Submitted:
05 September 2025
Posted:
09 September 2025
You are already at the latest version
Abstract
Background: Women’s reproductive health conditions such as endometriosis, menopause, and polycystic ovary syndrome (PCOS)—along with related disorders like restless legs syndrome (RLS) and bladder dysfunction—are traditionally viewed through a gynaecological lens. However, growing evidence demonstrates their substantial neurological and cognitive consequences, which remain under-recognised in clinical practice and policy. This integrative review explores the interplay between reproductive health conditions and brain function across the female life course, focusing on shared mechanisms, clinical manifestations, and implications for healthcare and policy. Methods: A comprehensive review of peer-reviewed literature, guidelines, and grey literature was undertaken to synthesise evidence on the neurological, cognitive, and psychosocial impacts of common reproductive health conditions. Evidence was mapped to a life-course and biopsychosocial framework. Results: Shared mechanisms included hormonal fluctuations, neuroinflammation, central sensitisation, and neuroendocrine disruption, all of which influence cognition, mood, and quality of life. Endometriosis was identified as a central pain syndrome with structural and functional brain alterations, psychiatric comorbidity, and associations with RLS. Menopause, driven by oestrogen withdrawal, was linked to “brain fog,” sleep disturbance, mood instability, and increased dementia risk. PCOS contributed to neurocognitive impairment through androgen excess, hypothalamic–pituitary–ovarian dysfunction, and metabolic abnormalities, increasing risks of depression, anxiety, and cognitive decline. Bladder dysfunction reflected wider neural network disruption and further compromised well-being. Conclusion: Despite their high prevalence, these conditions are underdiagnosed, poorly integrated into neurology and mental health care, and worsened by cultural stigma and systemic inequalities, especially in low- and middle-income countries. Urgent need exists for routine neurocognitive assessments, interdisciplinary care, and gender-sensitive policies. Recognising the brain–body interface and adopting a life-course, biopsychosocial perspective are key to advancing clinical practice, research, and global health equity for women.
Keywords:
polycystic ovary syndrome
; restless legs syndrome
; bladder dysfunction
; endometriosis
; menopause
Introduction
Endometriosis is a chronic, oestrogen-dependent inflammatory condition characterised by the growth of endometrial-like tissue outside the uterine cavity. Emerging evidence indicates that endometriosis, an estrogen-dependent inflammatory condition, can induce significant alterations in brain structure and function, potentially mediated by hormonal dysregulation. Animal studies have demonstrated that endometriosis can lead to changes in brain electrophysiology and gene expression, particularly in regions associated with pain and emotion regulation, such as the insula, hippocampus, and amygdala. These neural alterations are linked to increased pain sensitivity, anxiety, and depression-like behaviours (1). It affects an estimated 10% of women of reproductive age globally, approximately 195 million individuals (2). While traditionally associated with pelvic pain, infertility, and fatigue, there is growing recognition that endometriosis also has neurological and cognitive dimensions, impacting brain structure, function, and mental health.
Chronic Pain Processing: Neuroplastic Changes and Central Sensitisation in Endometriosis
In humans, neuroimaging studies have revealed that women with endometriosis-associated chronic pelvic pain exhibit decreased grey matter volume in key pain-processing regions, including the thalamus, mid-cingulate cortex, and posterior insula. These structural changes correlate with heightened pain perception and emotional distress. The pathophysiology underlying these brain changes may involve sustained estrogen exposure, which can alter neurotrophin balance and activate pathways like BDNF-NTRK2, contributing to neural remodelling. Additionally, chronic inflammation associated with endometriosis may exacerbate these neural alterations, further impacting pain perception and emotional well-being (3).
These findings underscore the complex interplay between hormonal imbalances, inflammation, and neural plasticity in endometriosis, highlighting the need for comprehensive approaches that address both peripheral and central mechanisms in the management of this condition (4) (Table 1)
The impact of this neurological process impacts both cognition and mood (Figure 1). There’s a growing recognition of cognitive and mood dysfunction in women with endometriosis, frequently manifesting as “brain fog”, a constellation of memory lapses, concentration difficulties, impaired executive function, and reduced verbal fluency. Functional MRI findings indicating altered activity in key brain regions such as the dorsolateral prefrontal cortex, hippocampus, and anterior cingulate, lend biological plausibility to these symptoms, as these areas underpin cognitive control and emotional regulation. The proposed role of neuroinflammation via increased brain cytokine levels and gene expression changes in the hippocampus and amygdala offers a compelling mechanistic explanation linking peripheral pelvic inflammation to central nervous system dysfunction. However, while this neuro-inflammatory hypothesis is promising, more longitudinal and mechanistic human studies are needed to determine causality and disentangle hormonal, inflammatory, and psychosocial contributors. This insight calls for a biopsychosocial approach to endometriosis care, integrating cognitive and mental health assessments into routine management.
Based on previous evidence and significant gaps, in this review, we aim to synthesise evidence on the neurological, cognitive, and psychosocial dimensions of women’s reproductive health across the life course. Also, to guide this synthesis, we applied a neuro-gynaecology conceptual framework that integrates biological, psychosocial, and policy dimensions across women’s health conditions.
Methods
Study Design
This study employed an integrative review methodology to explore the neurological and cognitive dimensions of reproductive health in women, with a particular focus on endometriosis, menopause, and mental health. Integrative reviews are well-suited for synthesising evidence from diverse sources, including quantitative, qualitative, and theoretical studies, thereby enabling a comprehensive understanding of complex phenomena that span biological, psychological, and socio-cultural domains. This approach was chosen because brain function in relation to reproductive health encompasses multiple disciplines, neuroscience, gynaecology, psychiatry, and public health, requiring a synthesis that goes beyond the limits of single-study designs.
Search Strategy
A systematic and structured search was conducted across seven electronic databases of PubMed, Embase, PsycINFO, Web of Science, Scopus, CINAHL, and the Cochrane Library. The search covered literature published from January 1990 to December 2024, ensuring inclusion of both foundational and recent evidence. A combination of Medical Subject Headings (MeSH) and free-text terms was used. The main search strings combined three domains: (i) reproductive health conditions (e.g., “endometriosis,” “menopause,” “polycystic ovary syndrome,” “perimenopause”), (ii) neurological and cognitive outcomes ( “cognition,” “brain fog,” “restless legs syndrome,” “neuroinflammation,” “cognitive decline”), and (iii) mental health outcomes (“depression,” “anxiety,” “quality of life”). Boolean operators “AND” and “OR” were applied to refine the queries. Grey literature, including WHO reports, national policy documents, and professional guidelines, was also reviewed to capture policy and practice-relevant insights.
Inclusion and Exclusion Criteria
Eligible studies were those that investigated neurological, cognitive, or mental health outcomes in women with endometriosis, menopause, or related reproductive conditions such as polycystic ovary syndrome (PCOS). Studies were included if they reported outcomes across any stage of the life course, from adolescence through to post-menopause, and if they comprised peer-reviewed empirical research, whether quantitative, qualitative, or mixed-method studies. Studies were excluded if they focused exclusively on fertility outcomes without reporting neurological or psychological endpoints, if they were animal studies not directly linked to mechanistic insights relevant to human health, or if they were published in languages other than English due to translation limitations
Study Selection and Screening
All identified citations were imported into EndNote X9 for duplicate removal. Two reviewers independently screened titles and abstracts against eligibility criteria. Full texts were retrieved for potentially relevant studies and assessed independently by both reviewers. Disagreements were resolved through discussion, and if consensus was not achieved, a third reviewer adjudicated. A PRISMA flow diagram was constructed to illustrate the selection process (supplement Figure 1)
Data Extraction
A structured data extraction form was developed to capture study characteristics (author, year, country, study design, sample size), participant demographics, reproductive health condition(s), neurological and mental health outcomes, and key findings. Extraction also recorded contextual factors such as comorbidities, health system characteristics, and policy considerations. Where quantitative data were available, these were extracted for descriptive synthesis. Qualitative findings were summarised thematically to capture experiential dimensions such as “brain fog,” stigma, and health system barriers.
Quality Appraisal
The methodological quality of included studies was appraised using the Newcastle–Ottawa Scale (NOS). It is shown in Supplement Table 2.
Data Synthesis
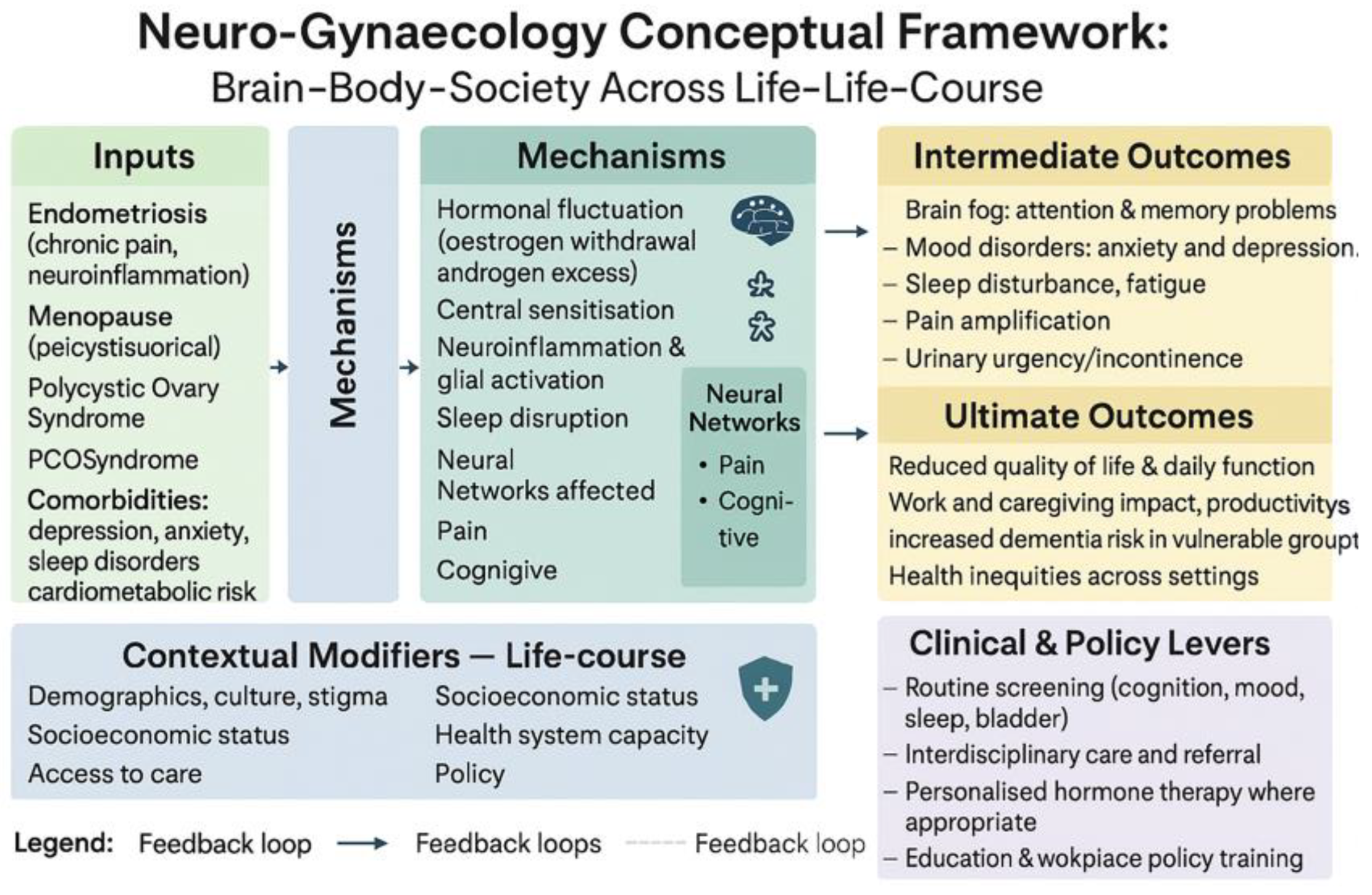
Findings were synthesised using a narrative and thematic approach. Quantitative data were tabulated and summarised descriptively, highlighting prevalence, associations, and effect sizes. Qualitative and mixed-methods evidence was integrated using thematic synthesis, drawing out recurrent patterns of neurological, cognitive, and psychosocial impact across reproductive conditions. Evidence was then mapped onto a life-course framework to explore how endometriosis, menopause, PCOS, and mental health intersect with brain function from adolescence to older age. Finally, policy and practice implications were identified through triangulation of empirical findings with global guidance documents (e.g., WHO recommendations). Also, we developed the Neuro-Gynaecology Conceptual Framework (Figure 3) to guide synthesis, mapping biological, psychosocial, and policy dimensions across the life course
Results
A total of 14 original articles were selected for inclusion in the manuscript through a comprehensive systematic search. These articles were subsequently synthesised using both narrative and thematic analytical approaches to provide a thorough understanding of the subject matter.
Women’s Mental Health: Depression, Cognition and Quality of Life
Mental health conditions in women, particularly depressive and anxiety disorders, are a major component of reproductive health-related brain function. Depression is not only more common in women, but it often correlates with reproductive life events (such as postnatal and perimenopausal periods). Globally, about 6% of adult women have depression versus 4% of men (7). This sex gap emerges by adolescence and persists across the lifespan, reflecting biological factors (e.g. hormonal fluctuations, immune differences) and psychosocial factors. Notably, postpartum depression is a worldwide concern: roughly 1 in 10 women experience significant depression after childbirth (7), with higher rates in some regions. Likewise, women in the menopausal transition have up to a 2–3 fold increased risk of a major depressive episode compared to pre-menopause (8). These examples illustrate how women’s mental health is often intertwined with reproductive physiology.
Neurologically, cognitive symptoms are a core feature of depression and anxiety. Patients frequently report poor concentration, indecisiveness, memory blanks, or mental slowing. Indeed, the WHO identifies poor concentration as one of the common symptoms of depressive episodes (7). Many women with depression describe a “foggy” feeling or difficulty performing complex tasks – this is sometimes termed pseudodementia in severe cases, as it can mimic organic cognitive impairment. Research confirms that depression can measurably reduce cognitive function: studies have found deficits in working memory, executive function, and processing speed in depressed individuals (9). For example, functional MRI shows reduced prefrontal activity during attention tasks in depression, and neuropsychological tests often reveal slowed information processing. Importantly, in younger adults, these cognitive effects are usually reversible with remission of depression. In older women, however, depression might herald or accelerate neurodegenerative decline. A longitudinal study of postmenopausal women (Table 1: Goveas et al.) found that those with depressive symptoms had roughly double the risk of developing mild cognitive impairment or dementia over the next five years (10). While part of this association could be an early symptom of dementia (i.e. emerging Alzheimer’s causing low mood), a body of evidence suggests depression itself can contribute to cognitive decline – via stress hormones, vascular damage, or lifestyle factors. Thus, maintaining good mental health is likely protective for the ageing brain.
Mental health issues also have significant links to RLS and sleep disorders. Depression and anxiety commonly co-occur with insomnia and conditions like RLS – often in a bidirectional manner. On one hand, chronic sleep disturbance (from causes such as RLS) can precipitate or worsen depression; on the other, certain antidepressants (SSRIs) can trigger or aggravate restless legs symptoms in some patients. The Swedish survey noted earlier illustrated that women with RLS had higher odds of depressed mood (11). In fact, many clinicians screen for RLS in patients presenting with unexplained fatigue or depression, since treating it can improve sleep and mood. This intersection of mood and movement disorders again underscores the intricate mind-body connection in women’s health.
Finally, it must be emphasised that the quality of life is profoundly affected by mental health disorders. Depression and anxiety can erode nearly all domains of life – work, relationships, self-care – and are leading causes of disability in women worldwide (12). Unlike menopause brain fog, untreated major depression can be debilitating. Women with chronic depression report poor life satisfaction and impaired social functioning, comparable or worse than many chronic physical illnesses. One meta-analysis shows depression reduces quality-of-life scores by 25–30%. Coexisting depression or anxiety in conditions like endometriosis amplifies perceived disability and pain. Effective mental health treatment can greatly improve quality of life, even if physical symptoms remain. Recognising and treating mental health is crucial for women’s overall health, especially in low-resource settings where up to 75% of those with mental disorders receive no treatment (7). This treatment gap urgently needs addressing, given the huge personal and economic toll of depression. These neuropsychological effects are not isolated but intersect with specific gynaecological conditions, beginning with endometriosis.
Endometriosis: Cognitive, Neurological, and Psychological Impact
Endometriosis, long recognised as a chronic gynaecological condition of pelvic pain and inflammation, also has significant neurological and psychological dimensions throughout the life course (Table 2 and Table 3). Many women with endometriosis report cognitive difficulties often described as “brain fog” (13). In fact, recent surveys indicate that over half of endometriosis patients experience memory lapses or trouble concentrating, with 60–80% reporting clinically significant cognitive impairment in daily life (13,14). These cognitive complaints, while subjective, are non-trivial: they are strongly associated with the severity of endometriosis symptoms – women in greater pain, fatigue, or with more depressive symptoms tend to report worse cognitive function (13). Notably, preliminary neuropsychological research finds that despite these self-reported issues, objective cognitive testing has yet to consistently demonstrate deficits in endometriosis patients (14). This paradox may reflect compensatory neural mechanisms (e.g. patients working harder to maintain performance (14)) or the difficulty of standard tests to capture subtle real-world cognitive inefficiencies. Regardless, the pervasive perception of cognitive dysfunction in endometriosis – sometimes severe enough to affect work and study (13) – underscores an often overlooked burden of the disease.
Neurological changes in the central nervous system have been observed in endometriosis, likely driven by chronic pain signalling. Neuroimaging studies, though few, suggest altered activity and connectivity in brain regions that process pain and emotions (such as the insula and cingulate cortex) in women with endometriosis (15). There is also emerging evidence of neuroinflammation: one study found widespread glial activation in the brains of mice with induced endometriosis (16), hinting that endometriosis’s impact extends beyond the pelvis to the brain’s immune environment. Such changes could plausibly contribute to the cognitive and mood symptoms reported.
Mental Health Correlations
Multiple studies indicate that up to 67% of women with endometriosis have at least one mental health diagnosis, most commonly depression, anxiety, or post-traumatic stress symptoms (20). These psychological comorbidities are often driven by a combination of chronic and unpredictable pain, infertility, sexual dysfunction, repeated surgical interventions, and the emotional toll of dismissive or invalidating medical encounters, particularly during adolescence or early adulthood. The relationship between pain and mental health is bidirectional: worsening psychological symptoms can heighten the perception of pain, while persistent physical discomfort can erode emotional resilience. This dynamic interplay contributes to central sensitisation, reinforcing a self-perpetuating pain–mood–brain feedback loop that deepens distress and complicates treatment outcomes (21).
RLS in Endometriosis Patients
RLS, or Willis-Ekbom Disease, is a chronic neurological disorder characterised by an irresistible urge to move the legs, often with unpleasant sensations that worsen at night and improve with movement. It affects 5–10% of adults in Western countries, with higher prevalence in women due to hormonal, iron-related, and neurochemical factors, and women with surgically confirmed endometriosis are up to 2.5 times more likely to report RLS symptoms (22). Shared mechanisms—iron deficiency, inflammation, hormonal imbalance, and sleep disruption—worsen pain, sleep, mood, and daily function, yet the condition remains underdiagnosed and under-recognised in both gynaecology and neurology. Greater awareness, screening, and multidisciplinary care are needed, alongside policy efforts to expand access to diagnosis and treatment (Table 4).
Clinical Relevance and Life Impact.
RLS adds substantially to the burden of endometriosis, worsening sleep, pain tolerance, cognition, and daily functioning. Fatigue, poor concentration, and irritability affect productivity and relationships, while severe symptoms heighten risks of depression, anxiety, and suicidal thoughts. Yet RLS often remains undiagnosed, as leg symptoms are overlooked or overshadowed by pelvic pain, underscoring the need for greater awareness and integrated care. Table 5 shows briefly the diagnosis and management of RLS in endometriosis cases based on current evidence.
Global and Regional Considerations
Data on RLS in endometriosis is limited but shows regional differences. Prevalence is higher in Western and urban populations, likely due to better diagnosis, while underdiagnosis occurs in Asian and African regions where endometriosis is often overlooked because of stigma, normalisation of menstrual pain, and poor specialist access. In rural and low-resource areas, the lack of trained sleep or neurology providers further decreases RLS diagnosis, except in severe cases (24,25). Healthcare systems should adopt an interdisciplinary approach to managing RLS in endometriosis patients. In LMICs, this may require greater involvement of community health workers and enhanced telemedicine services for diagnosis and follow-up (Figure 2).
Menopause: Hormonal Transitions and the Brain
While endometriosis exemplifies a central pain syndrome, similar neurological dimensions emerge in menopause. Menopause is a universal life stage that marks the cessation of ovarian function and menstrual cycles, typically occurring between the ages of 45 and 55. By 2025, over 1.1 billion women worldwide will be postmenopausal (27), representing a significant and growing demographic. Despite this, menopause has long been under-addressed in clinical practice, public health policy, and neuroscience. The decline in oestrogen, an essential neurosteroid, has substantial implications for brain function, mental health, and cognitive ageing.
Cognitive Symptoms and Functional Impact
Many women report experiencing “brain fog” during the perimenopausal transition, a constellation of symptoms that includes forgetfulness, difficulty concentrating, reduced verbal fluency, and slower information processing (28). These issues are often transient but can be disruptive, particularly for women balancing demanding professional roles, caregiving responsibilities, and societal expectations.
Longitudinal research from the SWAN (Study of Women’s Health Across the Nation) cohort found that verbal memory and processing speed often decline during perimenopause but tend to recover post menopause in many women. However, for others, especially those with coexisting risk factors (e.g., poor sleep, depression, early menopause), symptoms may persist or worsen with age (29). You can see the neurological implications of menopause in Table 6.
RLS and Menopausal Hormones
Menopausal hormonal changes may also intersect with RLS and other neurological conditions. RLS can emerge or worsen during perimenopause for some women (33). Epidemiological data are somewhat conflicting: a Swedish study found a strong link between menopausal night sweats and RLS prevalence, implying that women who suffer significant vasomotor symptoms are more prone to restless legs. However, the same study did not find a significant difference in RLS rates before vs. after menopause in general (11). This suggests it is not menopause per se that causes RLS, but rather the indirect effects (e.g. fragmented sleep, or perhaps iron level changes). It is known that RLS frequency increases with age and has a female predominance (34). In one cohort of 53-year-old women, over 25% reported new-onset RLS symptoms around menopausal age (35). Clinically, many women describe their restless legs as starting or getting worse during perimenopause (33). One theory is that oestrogen modulates dopamine pathways involved in RLS; as oestrogen levels drop, RLS symptoms might be unmasked. Additionally, the sleep deprivation from menopause symptoms can exacerbate RLS sensations, creating a vicious cycle. Quality of life can be significantly affected: untreated RLS “interferes with sleep, causes daytime drowsiness and negatively affects patients’ quality of life” (36,37). Combined with menopausal insomnia, this can severely impair daily functioning. Therefore, addressing sleep disorders (including RLS) is an important aspect of menopause care.
Hormone Therapy (HT): Cognitive Potential and Limitations
Hormone therapy (HT) remains the most effective intervention for managing vasomotor symptoms such as hot flashes and for treating genitourinary syndrome of menopause. However, its role in preserving or improving cognitive health is more complex.
Evidence supports the “critical window” hypothesis, which suggests that initiating HT close to the onset of menopause may help stabilise neuronal function and enhance verbal memory (38). Conversely, beginning HT later in life—particularly after the age of 65—has not been shown to provide cognitive benefits and may even increase the risk of dementia, especially when using combined oestrogen-progestogen formulations (39).
Transdermal oestrogen and micronised progesterone are emerging as potentially safer alternatives with fewer systemic risks. In light of this complexity, current clinical guidelines advocate for a personalised, symptom-focused approach to HT, balancing the individual’s risk profile, therapeutic goals, and timing of initiation.
Mental Health and Vasomotor Symptoms
Hormonal fluctuations during perimenopause may destabilise neurotransmitter systems (e.g., serotonin, GABA, dopamine), leading to mood disorders. Up to 25–30% of women report moderate to severe anxiety or depressive symptoms during this period (40). Vasomotor symptoms like night sweats and insomnia significantly disrupt sleep architecture, contributing to fatigue and worsened cognitive performance.
Untreated insomnia is a modifiable risk factor for dementia. Therefore, improving sleep through behavioural therapies, HT, or pharmacologic support may have downstream cognitive benefits (41).
Intersectionality and Social Determinants
Cognitive and psychological responses to menopause are shaped by intersecting social determinants, including race, ethnicity, education level, culture, and socioeconomic status. Black and Latina women, for example, report more severe vasomotor symptoms and are less likely to be offered HT (42). Low-income women frequently face restricted access to specialist services or adequate insurance coverage for menopause-related care, while cultural norms can influence whether symptoms are interpreted as medical problems or a “natural” life stage, thereby affecting care-seeking behaviour (43). These inequities are compounded by limited training in menopause management among healthcare providers, which perpetuates under-recognition and undertreatment across diverse populations
Workplace and Policy Implications
Despite its prevalence, menopause is rarely considered in workplace policy. Surveys in the UK indicate that 1 in 10 women have considered leaving their job due to menopause symptoms, yet only 14% of employers offer menopause-friendly accommodations (44). Encouraging developments include the UK Women’s Health Strategy (2022), which identifies menopause as a core priority (45), the work of Australia’s Jean Hailes Foundation in raising awareness and providing education on menopause, and calls from the WHO and other public health bodies to integrate menopause into non-communicable disease prevention frameworks (26).
Policies must address flexible work, education, HT access, and mental health as key to midlife women's health. Menopause, a neurobiological transition, impacts memory, attention, and emotions, increasing risks of cognitive decline and mood disorders. While many women have transient symptoms, others with early or surgical menopause, sleep issues, or mental health conditions face long-term effects.
Despite this, menopause remains marginalised in care and discourse. Evidence supports personalised hormone therapy within the “critical window” and combined strategies for sleep and mood issues. Responses vary by race, income, and healthcare access, with Black, Latina, and low-income women often underserved. Policy must reframe menopause as a public health and workplace priority, promoting informed policies, flexible work, education, and equitable care to safeguard cognitive health, support workforce participation, and ensure long-term brain health, especially for vulnerable groups.
PCOS and Neurological Impact
Beyond menopause, neuroendocrine disruption is also central to PCOS. PCOS is the most common endocrine-metabolic disorder affecting women of reproductive age, with an estimated global prevalence of 6–13% (46). Though traditionally considered a reproductive and metabolic disorder, PCOS has increasingly been recognised as a neuro-gynaecological condition due to its significant effects on brain structure, cognitive function, mood regulation, and long-term neurological health.
PCOS is characterised by hyperandrogenism, oligo/anovulation, and polycystic ovarian morphology, but its systemic effects extend far beyond the ovaries. Women with PCOS are more likely to experience neurocognitive challenges, mental health disorders, and even accelerated brain ageing, particularly when metabolic dysfunction is present (Table 7).
Social Determinants and Policy
Despite its high prevalence, PCOS is often underdiagnosed and undertreated, especially in LMICs. Up to 70% of cases go unrecognised due to systemic and sociocultural barriers, including limited awareness among clinicians and patients, lack of adolescent health services, and cultural stigma linked to symptoms like irregular periods, acne, infertility, or hirsutism. Access to specialist care is limited by barriers to nutrition, mental health, and endocrinology services. These disparities are most severe where women’s health is narrowly focused on fertility or childbirth, neglecting the cognitive, metabolic, and emotional aspects of PCOS (50)
In response to these persistent challenges, the World Health Organisation (WHO) published its first-ever international guideline on PCOS in 2023. The guideline emphasises the need for early diagnosis using adolescent-appropriate criteria, the integration of mental health services and cognitive screening into routine PCOS care, and culturally sensitive interventions that prioritise lifestyle approaches. These include improving access to nutritional guidance, physical activity programmes, and reducing weight-related stigma, thereby promoting holistic management (51)
Crucially, PCOS is not just a reproductive or cosmetic disorder but a complex multisystem condition with neurological and psychosocial effects. Its impact on brain function, especially during adolescence and midlife, underscores the importance of early recognition and intervention to prevent cognitive decline and protect quality of life. Future research should focus on neuroimaging, hormone–brain interactions, and interventions across the lifespan.
Bladder Function and Neurology
In addition to previous hormone-mediated conditions, bladder dysfunction highlights the neurological control of pelvic function. Bladder dysfunction is a significant but often overlooked neuro-gynaecological concern, affecting millions of women globally. Common conditions include overactive bladder (OAB), urinary incontinence (UI), and chronic pelvic pain with urinary symptoms. These disorders frequently coexist with gynaecological conditions such as endometriosis, menopause, PCOS, and pelvic trauma, and they have important neurological underpinnings.
Neuroanatomy of Bladder Control
The central nervous system regulates bladder function through cortical areas (medial prefrontal cortex, insula, anterior cingulate), subcortical structures (periaqueductal grey, hypothalamus), and the pontine micturition centre. Peripheral control involves the pelvic, hypogastric, and pudendal nerves. Dysfunction at any of these levels can result in storage or voiding issues, especially when exacerbated by hormonal or structural changes (52).
Neuroimaging and functional evidence: fMRI studies show that women with OAB or chronic bladder pain have increased activity in pain-processing and emotional regulation areas, such as the insula and anterior cingulate cortex. Altered connectivity between prefrontal regions and the periaqueductal grey suggests impaired bladder control from central origins (53). Table 8 shows this.
Bladder dysfunction is a often overlooked but impactful aspect of women’s reproductive health, linked to conditions like endometriosis, PCOS, menopause, and indirectly to RLS through shared inflammation, hormonal, and neurological pathways. Endometriosis involves painful bladder symptoms due to nerve and lesion involvement, while PCOS's metabolic issues weaken pelvic strength and alter bladder signals. Menopause causes oestrogen decline, leading to atrophy, sphincter issues, and nerve symptoms, resulting in urgency, nocturia, or incontinence, significantly affecting women’s quality of life.
The psychosocial burden is substantial. Bladder symptoms can cause embarrassment, restrict mobility, disrupt sleep, and contribute to anxiety, depression, and social withdrawal. In conservative cultures or low-resource settings, stigma and normalisation of symptoms deter women from seeking care (57).
Effective treatments like behavioural therapy, pelvic floor physiotherapy, pharmacologic interventions, and neuromodulation such as sacral neuromodulation and PTNS are underused due to cost, lack of awareness, and workforce shortages, especially in LMICs (58). In many African and South Asian regions, bladder issues are worsened by untreated obstetric trauma, fistula, or FGM complications, exposing a gap in urogynaecological services.
Integrating bladder health into routine reproductive and postmenopausal care is crucial. Urinary symptom screening should be standard, particularly for women with pelvic pain, hormonal issues, or sleep problems. Education, provider training, and health system improvements are needed to recognise bladder dysfunction as a vital part of women’s health care (59).
The Neuro-Gynaecology Conceptual Framework
Together, these findings underscore the interdependence of reproductive health and neurological outcomes, synthesised through our conceptual framework (Figure 3). The Neuro-Gynaecology Conceptual Framework highlights the dynamic interplay between brain, body, and society in shaping women's health across the life course. It demonstrates how biological inputs, including gynaecological and neurological conditions, interact with psychosocial and health system factors to produce complex patterns of symptoms and outcomes. The model identifies points where interventions ranging from clinical care to policy reforms can disrupt negative feedback loops, reduce disparities, and improve quality of life. This framework supports a holistic approach to women's health, emphasising integrated care and equity-focused strategies. Figure 3 illustrates the interconnected pathways linking neuro-gynaecological conditions to health outcomes across the life course. Inputs such as endometriosis, menopause, PCOS, bladder dysfunction, and comorbidities trigger biological mechanisms, including hormonal fluctuations, neuroinflammation, and sleep disruption. These mechanisms affect neural networks, leading to intermediate outcomes such as brain fog, mood disorders, pain amplification, and urinary symptoms. Contextual modifiers such as socioeconomic status, access to care, and cultural factors shape these experiences. Clinical and policy levers can mitigate ultimate outcomes, which include reduced quality of life, productivity loss, increased dementia risk, and health inequities.
Figure 3.
The Neuro-Gynaecology Conceptual Framework.
Discussion
Women’s reproductive health conditions, long compartmentalised within the domain of gynaecology, are now recognised as multisystem disorders with extensive neurological, psychological, and metabolic dimensions. Conditions such as endometriosis, PCOS, menopause, RLS, and bladder dysfunction impact far more than fertility or pelvic anatomy; they alter brain structure, cognitive function, neuroendocrine pathways, pain processing, sleep, and emotional well-being. These disorders are increasingly understood as part of a broader neuro-gynaecological framework, where chronic inflammation, hormonal fluctuation, central sensitisation, and metabolic stress converge to produce functional disruption across multiple systems (60).
Neurological Impact and Central Sensitisation
In endometriosis, for example, central sensitisation is now recognised as a core mechanism of chronic pelvic pain, independent of lesion location. Functional neuroimaging reveals alterations in pain-processing regions such as the insula, anterior cingulate cortex, and thalamus, with neuroplastic changes that persist even postmenopausal (61). Similarly, PCOS is associated with subtle but significant reductions in brain volume and white matter integrity, linked to insulin resistance and elevated androgens. Cognitive performance deficits, particularly in memory, attention, and executive function, are reported even in young women with PCOS, often under-recognised amidst the focus on fertility and cosmetic symptoms (62).
In menopause, the neurological impact of oestrogen withdrawal includes reduced synaptic plasticity, impaired glucose metabolism, and increased amyloid deposition—factors that contribute to midlife “brain fog” and increased risk of cognitive decline or dementia. Restless legs syndrome, disproportionately affecting women and often comorbid with endometriosis, adds further neurological complexity. Shared pathways of iron deficiency, disrupted dopamine signalling, and poor sleep quality magnify the overall burden on cognitive and emotional health (63).
Bladder Dysfunction: The Overlooked Dimension
Bladder symptoms such as urgency, incontinence, and pelvic pressure are frequently reported in endometriosis, menopause, and PCOS, yet they remain underdiagnosed and underprioritized. Neurologically, bladder control involves an intricate network of cortical, subcortical, and spinal structures. Functional and anatomical disruptions arising from hormonal changes, pelvic nerve involvement, or inflammatory cytokines can impair bladder function and worsen psychosocial distress (64).
Bladder dysfunction is often misattributed to ageing or hygiene, leading to stigma and silence, especially in conservative or resource-limited settings. Sleep disruption, anxiety, social withdrawal, and depression commonly follow. Despite the availability of effective therapies including pelvic floor physiotherapy, antimuscarinic medications, and neuromodulation techniques, access is often limited, particularly in LMICs, due to cost, lack of trained personnel, and normalisation of female discomfort (65).
Health Inequities and Global Considerations
The challenges described are compounded by profound health inequities. Women from low-income, ethnic minority, rural, or refugee populations face longer diagnostic delays, reduced access to specialist care, and poorer outcomes. In LMICs, women are less likely to be screened for menstrual abnormalities, sleep disorders, cognitive decline, or bladder symptoms (Supplementary Table 2). Obstetric trauma, untreated fistula, and female genital mutilation (FGM) further exacerbate urological and neurological morbidity, especially in sub-Saharan Africa and South Asia (68).
Global initiatives, including the WHO’s women’s health and NCD strategies, have begun to acknowledge these gaps, but implementation remains limited. Routine screening for sleep, bladder, cognitive, and mood symptoms is rarely embedded in reproductive health programs, and neuro-gynaecological conditions remain absent from most public health curricula (69).
Based on the current evidence, we provide policy recommendations regarding the neurological burden in gynaecological conditions, as presented in Table 9.
Strengths and limitations
This review synthesises 35 years of global evidence up to mid-2025, incorporating both foundational and recent research across diverse populations, which strengthens the breadth and generalisability of our findings. A key limitation is the heterogeneity of included studies, from surveys to clinical trials, which restricted us to a primarily descriptive synthesis rather than a formal meta-analysis. Potential publication bias may also influence the evidence base, particularly the underreporting of studies that found no cognitive effects of menopause. Moreover, while we focused on depression and anxiety as central outcomes of women’s mental health, other important conditions such as postpartum psychosis and premenstrual dysphoric disorder (PMDD) remain underexplored in relation to reproductive brain function. Finally, the complex interplay between endometriosis, menopause, and mood disorders complicates causal interpretation; observational studies cannot always determine whether, for instance, endometriosis directly contributes to depression, or whether both arise from shared genetic, hormonal, or psychosocial factors. Further longitudinal and mechanistic studies are needed to clarify these relationships.
Conclusions
This review highlights the urgent need to reframe women’s health through a multisystem, life-course, and neurologically informed lens. Conditions such as endometriosis, PCOS, menopause, restless legs syndrome, and bladder dysfunction are not only reproductive or anatomical but also neuro-gynaecological, affecting the brain, cognition, and emotional well-being. Hormonal, metabolic, and psychosocial factors drive lasting brain and behavioural changes that begin in adolescence, intensify during reproductive transitions, and often persist into later life, with inequities shaped by socioeconomic and geographic disparities. To address this, women’s health must adopt an interdisciplinary and globally inclusive model that integrates neurological and cognitive screening, expands brain–body research, reforms medical education, and embeds workplace and policy support. Recognising the brain–body–society interface is both a scientific necessity and a matter of equity and justice.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
GD developed the ELEMI program and conceptualised this paper. GD wrote the first draft and furthered by all other authors. All authors critically appraised, reviewed and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Funding
Not funded.
Ethics Approval
Not applicable.
Availability of Data and Material
The data shared within this manuscript is publicly available.
Acknowledgments
Not applicable.
Conflicts of interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
Code availability
Not applicable.
Consent to Participate
No participants were involved in this paper.
Consent for Publication
All authors consented to publish this manuscript.
References
- Li, T.; Mamillapalli, R.; Ding, S.; Chang, H.; Liu, Z.-W.; Gao, X.-B.; Taylor, H.S. Endometriosis alters brain electrophysiology, gene expression and increases pain sensitization, anxiety, and depression in female mice†. Biol. Reprod. 2018, 99, 349–359. [CrossRef]
- Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014 May;10(5):261–75. [CrossRef]
- As-Sanie, S.; Kim, J.; Schmidt-Wilcke, T.; Sundgren, P.C.; Clauw, D.J.; Napadow, V.; Harris, R.E. Functional Connectivity Is Associated With Altered Brain Chemistry in Women With Endometriosis-Associated Chronic Pelvic Pain. J. Pain 2016, 17, 1–13. [CrossRef]
- Wessels, J.M.; Leyland, N.A.; Agarwal, S.K.; Foster, W.G. Estrogen induced changes in uterine brain-derived neurotrophic factor and its receptors. Hum. Reprod. 2015, 30, 925–936. [CrossRef]
- Endometriosis [Internet]. [cited 2025 Aug 31]. Available from: https://www.who.int/news-room/fact-sheets/detail/endometriosis.
- Facchin, F.; Barbara, G.; Dridi, D.; Alberico, D.; Buggio, L.; Somigliana, E.; Saita, E.; Vercellini, P. Mental health in women with endometriosis: searching for predictors of psychological distress. Hum. Reprod. 2017, 32, 1855–1861. [CrossRef]
- Depressive disorder (depression) [Internet]. [cited 2025 Aug 31]. Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
- Women are 40% more likely to experience depression during the perimenopause | UCL News - UCL – University College London [Internet]. [cited 2025 Aug 31]. Available from: https://www.ucl.ac.uk/news/2024/may/women-are-40-more-likely-experience-depression-during-perimenopause.
- Recognizing the Lesser-Known Symptoms of Depression | NAMI: National Alliance on Mental Illness [Internet]. [cited 2025 Aug 31]. Available from: https://www.nami.org/depression-disorders/recognizing-the-lesser-known-symptoms-of-depression/.
- Goveas, J.S.; Espeland, M.A.; Woods, N.F.; Wassertheil-Smoller, S.; Kotchen, J.M. Depressive Symptoms and Incidence of Mild Cognitive Impairment and Probable Dementia in Elderly Women: The Women's Health Initiative Memory Study. J. Am. Geriatr. Soc. 2011, 59, 57–66. [CrossRef]
- Wesström, J.; Nilsson, S.; Sundström-Poromaa, I.; Ulfberg, J. Restless legs syndrome among women: prevalence, co-morbidity and possible relationship to menopause. Climacteric 2008, 11, 422–428. [CrossRef]
- Cui, L.; Li, S.; Wang, S.; Wu, X.; Liu, Y.; Yu, W.; Wang, Y.; Tang, Y.; Xia, M.; Li, B. Major depressive disorder: hypothesis, mechanism, prevention and treatment. Signal Transduct. Target. Ther. 2024, 9, 30. [CrossRef]
- EndoNews.com: News & Research Portal for Endometriosis Foundation of America [Internet]. 2025 [cited 2025 Aug 31]. Cognitive Difficulties in Endometriosis. Available from: https://www.endonews.com/cognitive-difficulties-in-endometriosis.
- Berryman, A.; Machado, L. Cognitive Functioning in Females with Endometriosis-Associated Chronic Pelvic Pain: A Literature Review. Arch. Clin. Neuropsychol. 2025, 40, 1066–1080. [CrossRef]
- Maulitz, L.; Stickeler, E.; Stickel, S.; Habel, U.; Tchaikovski, S.; Chechko, N. Endometriosis, psychiatric comorbidities and neuroimaging: Estimating the odds of an endometriosis brain. Front. Neuroendocr. 2022, 65, 100988. [CrossRef]
- Bashir, S.T.; Redden, C.R.; Raj, K.; Arcanjo, R.B.; Stasiak, S.; Li, Q.; Steelman, A.J.; Nowak, R.A. Endometriosis leads to central nervous system-wide glial activation in a mouse model of endometriosis. J. Neuroinflammation 2023, 20, 59. [CrossRef]
- World population ageing 2019 [Internet]. New York: UN; 2020 [cited 2025 Aug 31]. Available from: https://digitallibrary.un.org/record/3907988.
- Epperson, C.N.; Sammel, M.D.; Freeman, E.W. Menopause Effects on Verbal Memory: Findings From a Longitudinal Community Cohort. J. Clin. Endocrinol. Metab. 2013, 98, 3829–3838. [CrossRef]
- Mosconi L, Berti V, Quinn C, McHugh P, Petrongolo G, Varsavsky I, et al. Sex differences in Alzheimer risk: Brain imaging of endocrine vs chronologic aging. Neurology. 2017 Sept 26;89(13):1382–90. [CrossRef]
- Rocca WA, Bower JH, Maraganore DM, Ahlskog JE, Grossardt BR, de Andrade M, et al. Increased risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause. Neurology. 2007 Sept 11;69(11):1074–83. [CrossRef]
- Maki, P.M.; Henderson, V.W. Hormone therapy, dementia, and cognition: the Women's Health Initiative 10 years on. Climacteric 2012, 15, 256–262. [CrossRef]
- Gupta, R.; Lahan, V.; Goel, D. Prevalence of restless leg syndrome in subjects with depressive disorder. Indian J. Psychiatry 2013, 55, 70–3. [CrossRef]
- Allen, R.P.; Picchietti, D.L.; Garcia-Borreguero, D.; Ondo, W.G.; Walters, A.S.; Winkelman, J.W.; Zucconi, M.; Ferri, R.; Trenkwalder, C.; Lee, H.B. Restless legs syndrome/Willis–Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria – history, rationale, description, and significance. Sleep Med. 2014, 15, 860–873. [CrossRef]
- Fenton, A.; Panay, N. Menopause and the workplace. Climacteric 2014, 17, 317–318. [CrossRef]
- Freeman, E.W. Associations of depression with the transition to menopause. Menopause 2010, 17, 823–827. [CrossRef]
- WHO Data [Internet]. [cited 2025 Aug 31]. Global Strategy for Women’s, Children’s and Adolescents’ Health Data Portal. Available from: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/mca/global-strategy.
- Bozdag, G.; Mumusoglu, S.; Zengin, D.; Karabulut, E.; Yildiz, B.O. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum. Reprod. 2016, 31, 2841–2855. [CrossRef]
- Hogervorst, E. Effects of Gonadal Hormones on Cognitive Behaviour in Elderly Men and Women. J. Neuroendocr. 2013, 25, 1182–1195. [CrossRef]
- Barry, J.; Kuczmierczyk, A.; Hardiman, P. Anxiety and depression in polycystic ovary syndrome: a systematic review and meta-analysis. Hum. Reprod. 2011, 26, 2442–2451. [CrossRef]
- Moore, A.M.; Campbell, R.E. The neuroendocrine genesis of polycystic ovary syndrome: A role for arcuate nucleus GABA neurons. J. Steroid Biochem. Mol. Biol. 2016, 160, 106–117. [CrossRef]
- Pletzer, B.; Kronbichler, M.; Nuerk, H.-C.; Kerschbaum, H. Hormonal contraceptives masculinize brain activation patterns in the absence of behavioral changes in two numerical tasks. Brain Res. 2014, 1543, 128–142. [CrossRef]
- Cosar, E.; Cosar, M.; Köken, G.; Sahin, F.K.; Caliskan, G.; Haktanir, A.; Eser, O.; Yaman, M.; Yilmazer, M. Polycystic ovary syndrome is related to idiopathic intracranial hypertension according to magnetic resonance imaging and magnetic resonance venography. Fertil. Steril. 2008, 89, 1245–1246. [CrossRef]
- Ghorayeb, I.; Bioulac, B.; Scribans, C.; Tison, F. Perceived severity of restless legs syndrome across the female life cycle. Sleep Med. 2008, 9, 799–802. [CrossRef]
- Tempest, N.; Boyers, M.; Carter, A.; Lane, S.; Hapangama, D.K. Premenopausal Women With a Diagnosis of Endometriosis Have a Significantly Higher Prevalence of a Diagnosis or Symptoms Suggestive of Restless Leg Syndrome: A Prospective Cross-Sectional Questionnaire Study. Front. Endocrinol. 2021, 12, 599306. [CrossRef]
- Restless Legs Perimenopause | Restless Legs Menopause [Internet]. 2023 [cited 2025 Aug 31]. Available from: https://www.mymenopausetransformation.com/restless-leg-syndrome/can-the-right-nutrients-calm-your-jumpy-restless-legs/.
- Pedersini, R.; di Mauro, P.; Amoroso, V.; Castronovo, V.; Zamparini, M.; Monteverdi, S.; Laini, L.; Schivardi, G.; Cosentini, D.; Grisanti, S.; et al. Sleep disturbances and restless legs syndrome in postmenopausal women with early breast cancer given adjuvant aromatase inhibitor therapy. Breast 2022, 66, 162–168. [CrossRef]
- Haddadi, M.; Tabatabaei, F.-S.; Akbarzadeh, I.; Eftekhar, T.; Hantoushzadeh, S.; Hedayati, F.; Ahmadi, S.; Delbari, A. The sleep quality in women with surgical menopause compared to natural menopause based on Ardakan Cohort Study on Aging (ACSA). BMC Women's Heal. 2025, 25, 100. [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [CrossRef]
- Polycystic ovary syndrome [Internet]. [cited 2025 Aug 31]. Available from: https://www.who.int/news-room/fact-sheets/detail/polycystic-ovary-syndrome.
- Chesson, A.L.; Wise, M.; Davila, D.; Johnson, S.; Littner, M.; Anderson, W.M.; Hartse, K.; Rafecas, J. Practice Parameters for the Treatment of Restless Legs Syndrome and Periodic Limb Movement Disorder. Sleep 1999, 22, 961–968. [CrossRef]
- Trenkwalder C, Allen R, Högl B, Paulus W, Winkelmann J. Restless legs syndrome associated with major diseases: A systematic review and new concept. Neurology. 2016 Apr 5;86(14):1336–43. [CrossRef]
- Avis, N.E.; Colvin, A.; Karlamangla, A.S.; Crawford, S.; Hess, R.; Waetjen, L.E.; Brooks, M.; Tepper, P.G.; Greendale, G.A. Change in sexual functioning over the menopausal transition: results from the Study of Women's Health Across the Nation. Menopause 2017, 24, 379–390. [CrossRef]
- Hall L, Callister LC, Berry JA, Matsumura G. Meanings of menopause: cultural influences on perception and management of menopause. J Holist Nurs. 2007 June;25(2):106–18. [CrossRef]
- Griffiths, A.; MacLennan, S.J.; Hassard, J. Menopause and work: An electronic survey of employees’ attitudes in the UK. Maturitas 2013, 76, 155–159. [CrossRef]
- GOV.UK [Internet]. [cited 2025 Aug 31]. Women’s Health Strategy for England. Available from: https://www.gov.uk/government/publications/womens-health-strategy-for-england/womens-health-strategy-for-england.
- March, W.A.; Moore, V.M.; Willson, K.J.; Phillips, D.I.; Norman, R.J.; Davies, M.J. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum. Reprod. 2009, 25, 544–551. [CrossRef]
- Cooney, L.G.; Lee, I.; Sammel, M.D.; Dokras, A. High prevalence of moderate and severe depressive and anxiety symptoms in polycystic ovary syndrome: a systematic review and meta-analysis. Hum. Reprod. 2017, 32, 1075–1091. [CrossRef]
- Pastor, C.L.; Griffin-Korf, M.L.; Aloi, J.A.; Evans, W.S.; Marshall, J.C. Polycystic Ovary Syndrome: Evidence for Reduced Sensitivity of the Gonadotropin-Releasing Hormone Pulse Generator to Inhibition by Estradiol and Progesterone1. J. Clin. Endocrinol. Metab. 1998, 83, 582–590. [CrossRef]
- Wild, R.A.; Rizzo, M.; Clifton, S.; Carmina, E. Lipid levels in polycystic ovary syndrome: systematic review and meta-analysis. Fertil. Steril. 2011, 95, 1073–1079.e11. [CrossRef]
- Greenwood, E.A.; Pasch, L.A.; Cedars, M.I.; Legro, R.S.; Eisenberg, E.; Huddleston, H.G. Insulin resistance is associated with depression risk in polycystic ovary syndrome. Fertil. Steril. 2018, 110, 27–34. [CrossRef]
- Teede HJ, Tay CT, Laven JJE, Dokras A, Moran LJ, Piltonen TT, et al. Recommendations From the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2023 Sept 18;108(10):2447–69. [CrossRef]
- Griffiths, D.; Tadic, S.D. Bladder control, urgency, and urge incontinence: Evidence from functional brain imaging. Neurourol. Urodynamics 2007, 27, 466–474. [CrossRef]
- Komesu YM, Ketai LH, Mayer AR, Teshiba TM, Rogers RG. Functional MRI of the Brain in Women with Overactive Bladder: Brain Activation During Urinary Urgency. Female Pelvic Med Reconstr Surg [Internet]. 2011 [cited 2025 Aug 31];17(1):50–4. [CrossRef]
- Campin L, Borghese B, Marcellin L, Santulli P, Bourret A, Chapron C. [Urinary functional disorders bound to deep endometriosis and to its treatment: review of the literature]. J Gynecol Obstet Biol Reprod (Paris). 2014 June;43(6):431–42. [CrossRef]
- Kölükçü E, Gülücü S, Erdemir F. Association between lower urinary tract symptoms and polycystic ovary syndrome. Rev Assoc Med Bras (1992) [Internet]. [cited 2025 Aug 31];69(5):e20221561. [CrossRef]
- Robinson, D.; Cardozo, L.D. The role of estrogens in female lower urinary tract dysfunction. Urology 2003, 62, 45–51. [CrossRef]
- Coyne, K.S.; Wein, A.J.; Tubaro, A.; Sexton, C.C.; Thompson, C.L.; Kopp, Z.S.; Aiyer, L.P. The burden of lower urinary tract symptoms: evaluating the effect of LUTS on health-related quality of life, anxiety and depression: EpiLUTS. BJU Int. 2009, 103, 4–11. [CrossRef]
- Sukhu, T.; Kennelly, M.J.; Kurpad, R. Sacral neuromodulation in overactive bladder: a review and current perspectives. Res. Rep. Urol. 2016, ume 8, 193–199. [CrossRef]
- Abrams, P.; Andersson, K.; Apostolidis, A.; Birder, L.; Bliss, D.; Brubaker, L.; Cardozo, L.; Castro-Diaz, D.; O'COnnell, P.; Cottenden, A.; et al. 6th International Consultation on Incontinence. Recommendations of the International Scientific Committee: Evaluation and treatment of urinary incontinence, pelvic organ prolapse and faecal incontinence. Neurourol. Urodynamics 2018, 37, 2271–2272. [CrossRef]
- Harlow, B.L.; Wise, L.A.; Stewart, E.G. Prevalence and predictors of chronic lower genital tract discomfort. Am. J. Obstet. Gynecol. 2001, 185, 545–550. [CrossRef]
- van Rysewyk, S.; Blomkvist, R.; Chuter, A.; Crighton, R.; Hodson, F.; Roomes, D.; Smith, B.H.; Toye, F. Understanding the lived experience of chronic pain: A systematic review and synthesis of qualitative evidence syntheses. Br. J. Pain 2023, 17, 592–605. [CrossRef]
- Berkley KJ, Rapkin AJ, Papka RE. The pains of endometriosis. Science. 2005 June 10;308(5728):1587–9. [CrossRef]
- Cryan JF, O’Riordan KJ, Cowan CSM, Sandhu KV, Bastiaanssen TFS, Boehme M, et al. The Microbiota-Gut-Brain Axis. Physiol Rev. 2019 Oct 1;99(4):1877–2013. [CrossRef]
- Howard FM. Chronic pelvic pain. Obstet Gynecol. 2003 Mar;101(3):594–611.
- Giudice, L.C.; Oskotsky, T.T.; Falako, S.; Opoku-Anane, J.; Sirota, M. Endometriosis in the era of precision medicine and impact on sexual and reproductive health across the lifespan and in diverse populations. FASEB J. 2023, 37, e23130. [CrossRef]
- Schwab, R.; Stewen, K.; Ost, L.; Kottmann, T.; Theis, S.; Elger, T.; Schmidt, M.W.; Anic, K.; Kalb, S.R.; Brenner, W.; et al. Predictors of Psychological Distress in Women with Endometriosis during the COVID-19 Pandemic. Int. J. Environ. Res. Public Heal. 2022, 19, 4927. [CrossRef]
- Denny, E.; Mann, C.H. Endometriosis and the primary care consultation. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 139, 111–115. [CrossRef]
- Seear, K. The etiquette of endometriosis: Stigmatisation, menstrual concealment and the diagnostic delay. Soc. Sci. Med. 2009, 69, 1220–1227. [CrossRef]
- Jones G, Kennedy S, Barnard A, Wong J, Jenkinson C. Development of an endometriosis quality-of-life instrument: The Endometriosis Health Profile-30. Obstet Gynecol. 2001 Aug;98(2):258–64. [CrossRef]
- Gleason, C.E.; Dowling, N.M.; Wharton, W.; Manson, J.E.; Miller, V.M.; Atwood, C.S.; Brinton, E.A.; Cedars, M.I.; Lobo, R.A.; Merriam, G.R.; et al. Effects of Hormone Therapy on Cognition and Mood in Recently Postmenopausal Women: Findings from the Randomized, Controlled KEEPS–Cognitive and Affective Study. PLOS Med. 2015, 12, e1001833. [CrossRef]
- Krystal AD. Insomnia in women. Clin Cornerstone. 2003;5(3):41–50. [CrossRef]
- Strategy on women’s health and well-being in the WHO European Region [Internet]. [cited 2025 Aug 31]. Available from: https://www.who.int/europe/publications/i/item/WHO-EURO-2016-4173-43932-61910.
- Wortmann, L.; Oertelt-Prigione, S. Teaching Sex- and Gender-Sensitive Medicine Is Not Just a Matter of Content. J. Med Educ. Curric. Dev. 2024, 11. [CrossRef]
Figure 1.
Demonstrates the Neurological Processes Involved in Cognitive and Mood Dysfunction.
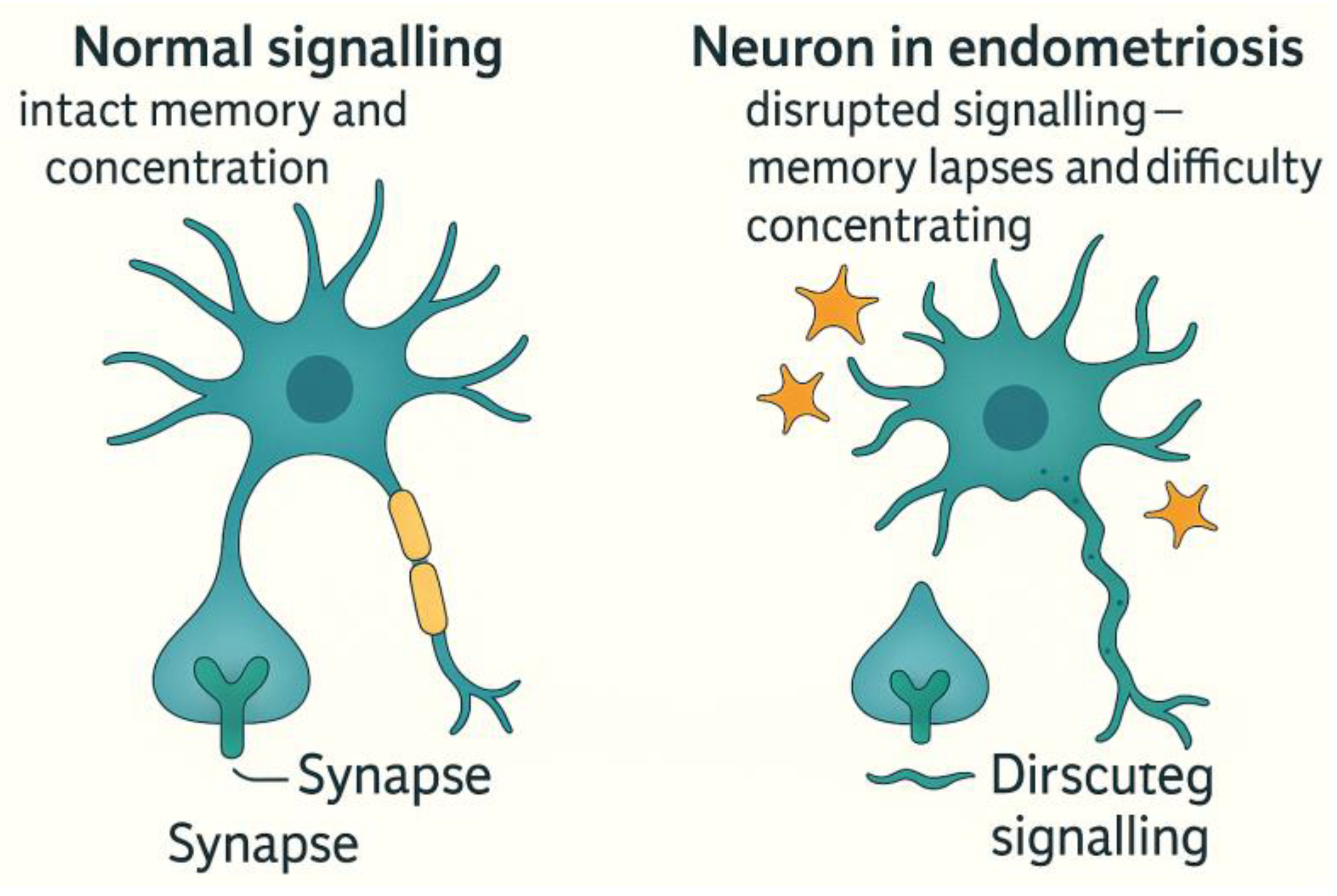
Figure 2.
Policy and Educational Recommendation for RLS in Endometriosis.
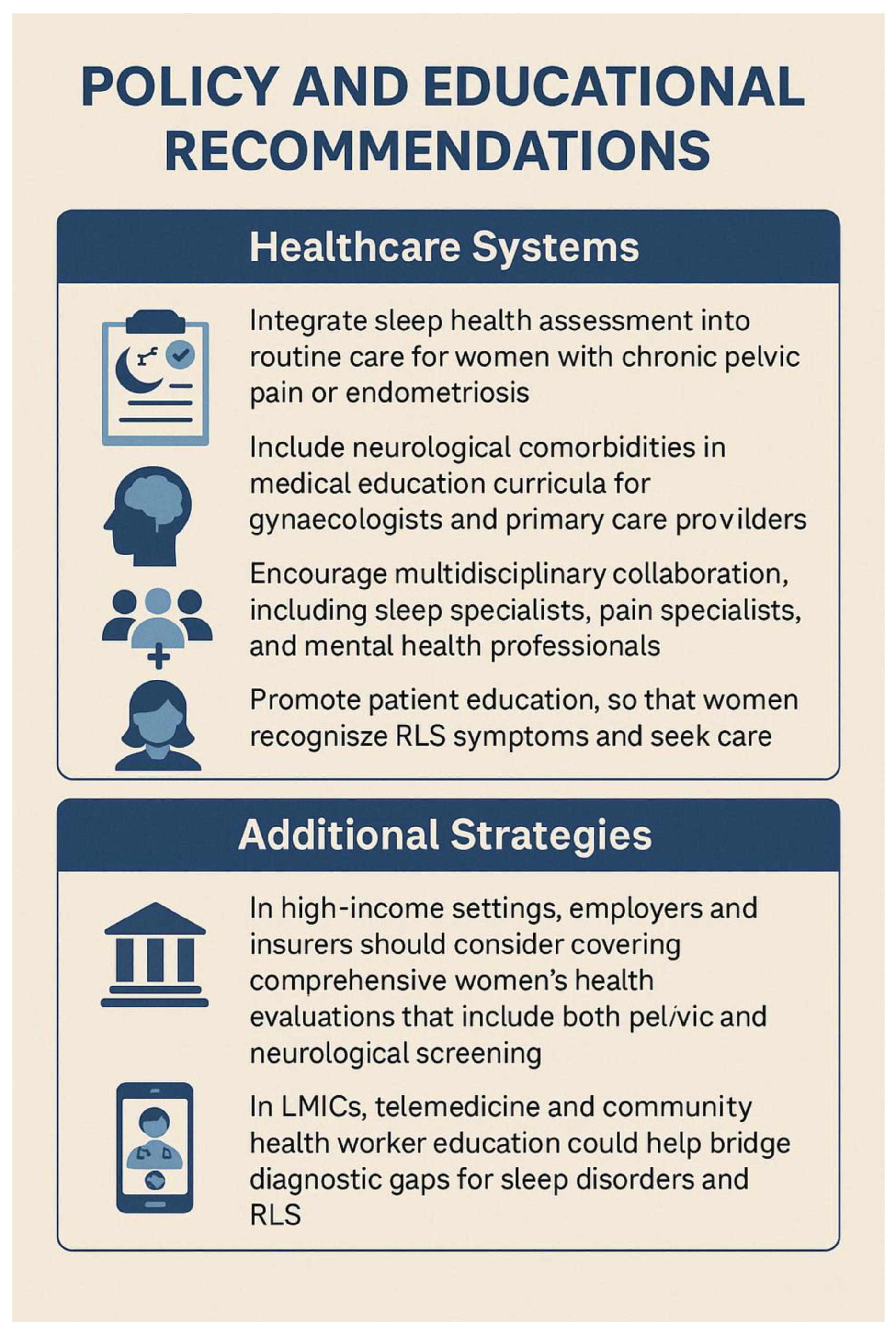

Table 1.
Chronic Pain Processing and Endometriosis.
| Aspect | Details |
| Neuroimaging Findings | - Increased grey matter volume in the insula, thalamus, and anterior cingulate cortex. - Altered connectivity in the Default Mode Network (DMN) and Salience Network. These are associated with pain hypervigilance and cognitive inflexibility. |
| Central Sensitisation Manifestations | - Hyperalgesia: Heightened sensitivity to painful stimuli. - Allodynia: Pain in response to non-painful stimuli (e.g. light touch). - Pain Memory Consolidation: Persistent perception of pain even after the original cause is removed. |
| Comparative Syndromes | Similar CNS patterns observed in fibromyalgia and chronic migraine, indicating that endometriosis belongs to the spectrum of central pain syndromes (5,6). |
Table 2.
Impact of Endometriosis in Adolescents and Women of Reproductive Age.
| Category | Details |
| Onset and Diagnosis | - Often begins during adolescence. - Diagnosis typically delayed by 6–11 years due to symptom normalisation and lack of awareness (17). |
| Barriers to Diagnosis | - Dysmenorrhea frequently dismissed as normal. - Menstrual pain still stigmatised or minimised in schools and primary healthcare settings. |
| Consequences of Delay | - School absenteeism and academic disruption. - Social isolation and shame surrounding menstruation. - Early invalidation shapes long-term healthcare attitudes. |
| Neurodevelopmental Risk | - Chronic pain during critical brain development may lead to long-term cognitive-emotional dysregulation. |
| Intervention Priorities | - Early recognition and validation of menstrual pain. - Comprehensive pain management. - School-based accommodations and mental health support. |
Table 3.
Postmenopausal Legacy of Endometriosis.
| Category | Details |
| Persistent Risk Factors | Women may continue to experience symptoms postmenopausal if they: - Use menopausal hormone therapy (MHT) - Have deep-infiltrating lesions - Exhibit central sensitisation from long-standing pain (18). |
| Ongoing Symptoms | - Pelvic pain - Bladder or bowel dysfunction - Psychological distress including low mood, anxiety, and fatigue |
| Neurological Footprint | Long-term changes in brain function due to chronic pain may impact: - Concentration and processing speed - Pain perception - Emotional resilience |
| Ageing-Related Risks | Women with a history of endometriosis may have increased risks of: - Sleep disorders - Depression and anxiety - Reduced cognitive reserve in later life (19) |
| Research Needs | More longitudinal studies are needed to determine the extent of cognitive and emotional sequelae of chronic endometriosis after menopause. |
Table 4.
Underlying mechanism of RLS and endometriosis.
| Contributing Factor | Description and Impact |
| Iron Deficiency | - Iron is essential for dopamine synthesis in the central nervous system. - In endometriosis, heavy menstrual bleeding, inflammation, or malabsorption can lead to systemic and cerebral iron depletion (23). |
| Chronic Inflammation | - Endometriosis involves chronic pelvic and systemic inflammation. - Elevated cytokines such as IL-6 and TNF-α may impair dopaminergic signalling and peripheral nerve function, contributing to RLS pathophysiology. |
| Hormonal Fluctuations | - Oestrogen and progesterone regulate dopamine and GABAergic neurotransmission. - Hormonal imbalances in endometriosis may exacerbate or reveal underlying RLS symptoms (23). |
| Sleep Disruption | - Endometriosis-related pain leads to insomnia and fragmented sleep. - RLS symptoms typically worsen at night, compounding sleep loss and increasing fatigue, anxiety, and depression. |
Table 5.
Diagnosis and Management of RLS in Women with Endometriosis.
| Category | Details |
| Clinical Clues for RLS | - Insomnia or difficulty falling asleep - Nighttime leg restlessness or discomfort - Unexplained daytime fatigue - Unrefreshing sleep despite adequate duration |
| Recommended Workup | - Ferritin testing (target >75 ng/mL) - Medication review (e.g., antihistamines, SSRIs may worsen symptoms) - Assessment of sleep hygiene and circadian rhythm |
| Management Strategies | - Iron supplementation (oral or intravenous) - Dopaminergic agents (e.g., pramipexole, ropinirole) - Gabapentinoids (e.g., gabapentin, pregabalin—helpful with comorbid pain/anxiety) - Sleep behaviour therapy and lifestyle modification (avoid caffeine, alcohol, nicotine) |
Table 6.
Oestrogen and Brain Health: Neurological Implications of Menopause.
| Aspect | Details |
| Neuroprotective Functions of Oestrogen | - Enhances synaptic plasticity and supports memory consolidation - Maintains mitochondrial efficiency for neuronal energy needs - Promotes glucose metabolism in the brain, essential for cognitive performance (30) |
| Neuroimaging Findings in Menopause | - Reduced grey and white matter volumes, especially in the hippocampus and prefrontal cortex - Decreased glucose uptake in key brain areas - Increased amyloid-beta deposition, associated with Alzheimer’s disease (31) |
| Clinical Interpretation | Menopause may function as a “neurological transition state,” heightening vulnerability to accelerated brain ageing. |
| High-Risk Groups | Women experiencing early menopause (before age 45) or surgical menopause (e.g., oophorectomy) without hormone therapy are at greater risk of cognitive decline and dementia (32). |
Table 7.
Neurological and Cognitive Impacts of PCOS.
| Domain | Key Findings |
| Cognitive Function | - Lower brain volume in frontal and temporal lobes - Reduced white matter integrity, impairing inter-regional communication - 11–13% lower performance on tasks involving attention, memory, and processing speed (38) - Associated with insulin resistance, obesity, and chronic inflammation - Poor sleep quality (e.g., due to sleep apnoea) worsens cognitive symptoms - Often missed due to focus on cosmetic or fertility issues |
| Mood Disorders and Emotional Health | - 2–3x higher risk of depression, anxiety, dysthymia, and eating disorders (47) - Hormonal imbalances (e.g., high testosterone, LH/FSH disruption) affect serotonin and dopamine - Stigma and appearance concerns cause low self-esteem - Adolescents with PCOS face bullying, school absenteeism, and social isolation, increasing risk of long-term mental illness |
| Neuroendocrine Basis | - PCOS involves elevated GnRH pulse frequency and increased LH, leading to androgen excess (48) - Disrupted HPO axis feedback implies a central role of the brain in PCOS pathogenesis - Brain imaging shows altered activity in corticolimbic circuits (amygdala, nucleus accumbens, anterior cingulate), affecting: reward processing, impulse control, and mood regulation |
| Androgens and Cognition | - High testosterone levels linked to poorer verbal memory and attention (49) - In some young women, mild androgen excess may enhance spatial ability via androgen receptor activity in the hippocampus and PFC - In most cases, particularly with metabolic dysfunction, androgens impair rather than enhance cognition |
| Life-Course Risk | - PCOS is lifelong, starting in adolescence and continuing into older age - Increases risk of: Type 2 diabetes and metabolic syndrome (50–70%) Hypertension and CVD Stroke and cognitive decline {Citation} - Brain MRI in postmenopausal women with PCOS shows white matter lesions, silent infarcts, and microvascular disease - Early intervention may reduce neurovascular ageing |
Table 8.
Bladder Dysfunction in Women with Reproductive Health Conditions.
| Condition | Mechanisms and Effects on Bladder Function |
| Endometriosis and Bladder Symptoms | - Deep infiltrating endometriosis may involve the bladder wall, ureters, or pelvic nerves. - Contributes to painful bladder syndrome or interstitial cystitis. - Chronic inflammation and central sensitisation exacerbate urinary urgency, frequency, and nocturia—especially around menstruation. - May mimic recurrent UTIs, leading to misdiagnosis (54). |
| PCOS and Metabolic Contributions | - Obesity and insulin resistance in PCOS are linked to increased rates of urinary incontinence. - Excess abdominal pressure weakens pelvic floor neuromuscular support. - Metabolic inflammation may impact bladder sensory pathways, increasing urgency and frequency (55). |
| Menopause and Urogenital Atrophy | - Oestrogen deficiency causes thinning of bladder and urethral epithelium, reduced vascularity, and loss of collagen. - Results in reduced bladder capacity, increased urgency, and compromised sphincter control. - Neurologically, there is decreased afferent input and delayed cortical inhibitory control (56). |
Table 9.
Overall Policy Recommendations.
| Policy Recommendation | Key Actions |
| Integrate Neuropsychological Assessment into Women’s Health Services | Routine screening for cognitive symptoms, mood disorders, and sleep disturbances; use validated tools in consultations (70) |
| Promote Interdisciplinary and Life-Course Approaches | Develop interdisciplinary care pathways; ensure life-course continuity of care tailored to each stage. |
| Expand Research on Neuro-Gynaecological Conditions | Fund research on brain imaging, neuroendocrinology, and cognition in women’s health; close gender gaps in clinical trials |
| Address Health Inequities and Social Determinants | Address diagnostic delays via community outreach; invest in culturally sensitive care and accessible health communication (26) |
| Improve Menstrual and Menopause Literacy | Implement menstrual education in schools; standardise menopause care in healthcare systems and workplaces |
| Embed Sleep and Pain Management into Reproductive Health | Screen and manage sleep disorders and pain in reproductive health; train providers in sleep–hormone–pain links (71) |
| Develop Global Health Frameworks with Neurological Dimensions | Incorporate neurocognitive wellbeing into global women’s health policies; support LMIC capacity-building (72) |
| Promote Menopause- and Pain-Friendly Workplaces | Encourage workplace accommodations for menopausal symptoms and chronic pain; promote global adaptation of UK models. |
| Mandate Medical Education Reform | Integrate neuro-gynaecology and menstrual health into medical curricula; tackle gender bias in clinical training (73). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



