Submitted:
05 September 2025
Posted:
08 September 2025
You are already at the latest version
Abstract
Background: Recent advancements in heart failure (HF) therapy have significantly enhanced the management of patients across all phenotypes of left ventricular ejection fraction. However, these multidrug regimens frequently induce alterations in renal function by influencing intrarenal hemodynamics, thereby modifying glomerular ca-pillary pressures. This phenomenon could result in a mild to moderate decline in esti-mated glomerular filtration rate (eGFR), often classified as “worsening kidney function.” This nomenclature stems from consistent observations of eGFR reductions recorded during HF treatment in clinical trials. This review aims to clarify the implications of renal function changes linked to therapies that modify glomerular hemodynamics, and their relationship with patient outcomes. Methods: By a comprehensive re-examination of data from HF clinical trials conducted with various classes of medications, all affecting eGFR, we sought to provide evidence that the decline in eGFR is associated with the activation of specific mechanisms that collectively contribute to a reduction in glomerular filtration pressure, a prominent factor in maladaptive neurohormonal responses. Results: Since the investigation of angiotensin-converting enzyme inhibitors to the more recent non-steroidal mineralocorticoid receptor antagonist, the renal effects of these therapeutic regimens correlate with improvements in patient outcomes. The data consistently indicate that an early decline in eGFR, when coupled with an enhancement in HF outcomes, is associated with a more gradual decline in eGFR during long-term follow-up. Conclusion: Clinicians should recognize early declines in eGFR as indicators of favorable intra-glomerular hemodynamic adjustments that mitigate maladaptive neurohormonal re-sponses and contribute to improved long-term outcomes in patients with HF.
Keywords:
heart failure
; glomerular filtration rate
; chronic kidney disease
; renin‐angiotensin‐aldosterone system
; sodium‐glucose cotransporter
; mineralocorticoid antagonist
1. Introduction
Recent advances in heart failure (HF) therapies have revolutionized patient management across the spectrum of left ventricular ejection fraction (LVEF). However, changes in renal function—reflected by alterations in creatinine levels and glomerular filtration rate (GFR)—are commonly observed during treatment with evidence-based multi-drug regimens. This is expected, given the close physiological interplay between the heart and kidneys in HF. Chronic kidney disease (CKD) markedly worsens HF outcomes [1], while HF itself is a leading driver of CKD progression in the general population [2]. Consequently, CKD is the most prevalent comorbidity among patients with HF [3].
Moreover, specific pharmacodynamic properties of HF therapies influence intra-renal hemodynamics, affecting the kidney’s capacity to maintain glomerular filtration pressures and regulate electrolyte and protein handling. This can lead to reductions in GFR, termed “worsening renal function” (WRF), often associated with HF medications endorsed by international guidelines [4]. Numerous studies have consistently reported declines in estimated GFR (eGFR) during HF treatment, ranging from 5–10 mL/min/1.73 m2 with angiotensin-converting enzyme inhibitors (ACEi) [5] and angiotensin receptor blockers (ARBs) [6], to approximately 4 mL/min/1.73 m2 with sodium-glucose cotransporter 2 inhibitors (SGLT2i) [7], and 2.4–6 mL/min/1.73 m2 with mineralocorticoid receptor antagonists (MRA) [8].
The term WRF also encompasses acute declines in renal function that may occur during decongestive therapy. Importantly, it is essential to distinguish these hemodynamically driven reductions in GFR from progressive, irreversible declines due to pathological loss of functioning glomeruli. The implications of WRF arising from structural nephron loss differ substantially from those of GFR reductions observed during guideline-directed HF therapy, which often raise concerns among clinicians, particularly when CKD coexists [9]. Understanding the underlying pathophysiological mechanisms during HF treatment is critical for accurately interpreting changes in GFR and serum creatinine (sCr), thereby optimizing the use of available therapies to improve HF outcomes.
2. Renal Physiology and Heart Failure Hemodynamics
At birth, each kidney contains approximately 950,000 nephrons, with no capacity for new nephron formation. As individuals mature, nephron size increases to meet rising metabolic demands. Despite significant fluctuations in systemic blood pressure, renal physiology maintains stable filtrate production through autoregulatory mechanisms [10].
This autoregulation, governed by the renal Starling forces, preserves glomerular filtration by modulating glomerular capillary pressure and filtration rate. Local and systemic neurohormonal pathways adjust the tone of the afferent arteriole (AA), efferent arteriole (EA), as well as podocytes and mesangial cells within the glomerular capillary network. This intricate system maintains the hydraulic conductivity of the filtration barrier, allowing plasma molecules up to 42 nm to pass into the filtrate while restricting larger molecules, such as albumin (approximately 75 nm) [11,12]. The oncotic pressure generated by plasma albumin counteracts the hydrostatic filtration pressure, finely tuning the filtration rate and capillary surface area. The coordinated function of these glomerular components enables efficient filtration even amid systemic hemodynamic variations. For simplicity, assuming constant barrier conductivity and stable oncotic forces tied to plasma albumin, the single nephron GFR primarily depends on glomerular capillary pressure.
Loss of nephrons due to injury or aging leads to compensatory increases in filtration pressure and glomerular hypertrophy, preserving the “renal reserve” via Starling adaptations [10,11,12]. However, in HF, reduced cardiac output and arterial underfilling activate baroreceptors, signaling diminished effective circulating volume to the kidneys. This triggers a nephron-centric response characterized by elevated norepinephrine spillover and excessive activation of the renin-angiotensin-aldosterone system (RAAS). These processes preferentially dilate the AA while constricting the EA, thereby sustaining glomerular filtration pressure to preserve filtrate production [13].
This compensatory mechanism, however, becomes maladaptive. The intimate link between glomerular filtration dynamics and neurohormonal activation fosters sodium retention, volume overload, and further renal endocrine stimulation [11,13,14]. During acute HF decompensation, the resultant surge in glomerular filtration pressure often leads to functional proteinuria, especially when preexisting damage impairs mesangial, podocyte, or tubular integrity. Excessive intraglomerular pressures compromise the filtration barrier, accelerating nephron loss [11,14].
Multiple factors disrupting glomerular filtration homeostasis help explain why different endogenous modulators may independently elevate the single nephron GFR, influencing renal reserve and contributing to GFR decline. This review aims to elucidate why observed eGFR declines in clinical practice may represent either loss of functioning glomeruli or pharmacologically mediated reductions in intraglomerular pressure that ultimately safeguard long-term renal and cardiovascular outcomes [15]
3. Angiotensin-Converting Enzyme Inhibitors (ACEi) and Angiotensin Receptor Blockers (ARB)
Renal concerns in advanced heart failure (HF) have been noted since the CONSENSUS trial in 1987, which first evaluated ACE inhibitors (ACEi) in HF. sCr initially increased by 10–15% (10–20 mmol/L) within three weeks, persisting up to six months. At 24 weeks, sCr rose by 20% in patients with baseline sCr <1.43 mg/dL versus 11% in those >1.43 mg/dL, with low blood pressure being the strongest predictor of sCr rise in severe HF [16].
A 2000 analysis of the SOLVD trial in patients with HF and reduced ejection fraction (HFrEF) and moderate renal impairment treated with enalapril found declining creatinine clearance was associated with increased mortality (HR per 30 mL/min decrease, 1.24; 95% CI 1.09–1.42) [17], raising concerns over ACEi-induced creatinine elevations. However, a subsequent SOLVD analysis over a decade later showed that early eGFR declines (>20% at day 14) were not linked to worse outcomes, and continued therapy conferred survival benefits (HR 0.66; 95% CI 0.5–0.9) [18]. A later post hoc SOLVD analysis confirmed lower hazard rates with enalapril, whereas placebo was associated with higher mortality, concluding that early renal worsening with ACEi initiation is generally benign and does not negate long-term benefits. Moreover, the rate of kidney function decline during follow-up independently predicted mortality, regardless of baseline renal function or HF worsening [19].
The introduction of ARBs further clarified the impact of angiotensin II blockade. In the CHARM trial, involving patients with HFrEF (<40% LVEF) or HF with mildly reduced (HFmrEF) or preserved (HFpEF) eiection fraction (>40% LVEF) and creatinine <3.0 mg/dL, eGFR was a stronger prognostic indicator than LVEF. Risks of the primary endpoint (cardiovascular death or hospitalization for HF) and all-cause mortality significantly increased when eGFR was <60 mL/min/1.73 m2, independent of ARB treatment effects [20].
Further CHARM analyses showed greater eGFR declines with candesartan versus placebo in both HFrEF and HFpEF, without a treatment-by-outcome interaction [21]. An evaluation of albuminuria revealed microalbuminuria (30%) and macroalbuminuria (11%) were prevalent across phenotypes and associated with increased hazard ratios (HR 1.43; 95% CI 1.21–1.69 and HR 1.75; 95% CI 1.39–2.20, respectively), underscoring urinary albumin-creatinine ratio (UACr) as a robust HF outcome marker [22].
Val-HeFT data on HFrEF patients highlighted proteinuria’s independent association with mortality (HR 1.2; 95% CI 1.01–1.62) and first morbid event (HR 1.28; 95% CI 1.06–1.55), independent of CKD status [23]. Valsartan similarly reduced eGFR in CKD (mean -3.6 mL/min/1.73 m2) and non-CKD patients (mean -4.0 mL/min/1.73 m2), but still lowered adverse event risks, distinguishing drug-induced eGFR changes from disease progression [23,24].
4. Angiotensin Receptor Neprilysin Inhibitor (ARNI, Sacubitril/Valsartan)
In the PARADIGM-HF trial, sacubitril/valsartan reduced the primary composite outcome and all-cause mortality by ~20% compared to enalapril in HFrEF [25]. The cohort had a mean eGFR of 70±20 mL/min/1.73 m2; 33% had CKD and 24% had micro/macroalbuminuria. During the run-in, eGFR declined more with enalapril (-0.6 vs 0.0 mL/min/1.73 m2), suggesting potential long-term renal benefits. However, during follow-up, sacubitril/valsartan showed slower eGFR decline (-1.61 vs -2.04 mL/min/1.73 m2/year) despite a greater increase in UACr (1.20 vs 0.90 mg/mmol) [26].
This pattern mirrored the PARAMOUNT findings [27], with albuminuria increases attributed to heightened natriuretic peptide activity, as also seen in studies where atrial natriuretic peptide raised albuminuria, which reversed upon ARNI withdrawal [28]. A PARADIGM-HF subanalysis stratified by KDIGO risk showed that patients with high/very-high risk (26%) had the highest CV event rates (HR 14.9 per 100 person-years; 95% CI 12.7–17.6). Across KDIGO strata, sacubitril/valsartan maintained a consistent safety and efficacy profile [29,30].
The PARAGON-HF trial in HFpEF nearly reached statistical significance for reducing hHF or CV mortality (HR 0.87; 95% CI 0.75–1.01). Sacubitril/valsartan reduced renal decline by 1.4% vs 2.7% with valsartan (HR 0.50; 95% CI 0.33–0.77) [31]. eGFR initially fell in ~10% of PARAGON-HF versus 11% of PARADIGM-HF run-in participants but partially recovered by week 16 regardless of treatment changes [32].
Longitudinal analyses showed sacubitril/valsartan consistently slowed chronic eGFR decline versus valsartan (–2.0 vs –2.7 mL/min/1.73 m2/year) [33]. Further evaluation indicated accelerated eGFR decline started 12 months before hHF, continued thereafter, and only modestly slowed in patients without subsequent hospitalizations [34]. These findings emphasize sacubitril/valsartan’s nephroprotective role and its renal contributions to cardiovascular benefits [35].
Notably, in PARAGON-HF, women (51.6% of HFpEF patients) experienced greater early eGFR dips with ARNI (p=0.006) yet derived pronounced reductions in heart failure hospitalizations (hHF) risk (HR 0.67; 95% CI 0.53–0.85), a benefit not seen in men (HR 1.07; 95% CI 0.85–1.34) [32,36]. This suggests early eGFR declines in women should not deter guideline-recommended ARNI use.
Table 1 summarizes the effects of ACEi, ARBs and ARNI.
5. Mineralocorticoid Receptor Antagonists (MRAs)
5.1. Steroid MRAs
Early studies in the 1950s demonstrated that spironolactone, the first steroidal MRA, effectively reduced salt retention and cardiac necrosis in animal models [37]. However, it was not until the RALES trial in 1999 that the clinical benefits of spironolactone in HFrEF were firmly established. This landmark study, which enrolled 1,663 patients with LVEF <35% and NYHA class III–IV symptoms, found that spironolactone (25 mg/day) reduced all-cause mortality by 30% compared to placebo (HR 0.70; 95% CI, 0.60–0.82), leading to early termination due to efficacy despite an acceptable rise in hyperkalemia [38].
Following RALES, spironolactone prescriptions surged, but this was accompanied by a sharp increase in hyperkalemia-related hospitalizations, rising from 2.4 per 1,000 patients in 1994 to 11.0 per 1,000 in 2001, with mortality climbing from 0.3 to 2.0 per 1,000 [39]. This trend was likely due to spironolactone use in patients with advanced CKD, a group excluded from RALES.
To improve safety, eplerenone, a next-generation steroidal MRA with greater receptor selectivity and reduced affinity for progesterone and androgen receptors, was developed to mitigate hyperkalemia risk. The EMPHASIS-HF trial, published in 2011, investigated eplerenone in 2,737 patients with NYHA class II symptoms, LVEF <30%, eGFR >30 ml/min/1.73 m2, and serum potassium <5.0 mmol/L, all receiving ACEi/ARBs and beta-blockers. Eplerenone significantly reduced all-cause mortality (HR 0.76; 95% CI, 0.62–0.93), cardiovascular death (HR 0.76; 95% CI, 0.61–0.94), and hHF, with a modest increase in hyperkalemia (8% vs. 3.7%) [40].
Despite these strong outcomes, MRA use remained limited, primarily due to concerns over hyperkalemia and WRF in high-risk patients. A prespecified analysis showed that with careful monitoring, eplerenone was both safe and beneficial even in patients at elevated risk for hyperkalemia or WRF [41] (Table 2).
MRA underutilization is also linked to the 2014 TOPCAT trial, which evaluated spironolactone in HFpEF (LVEF >40%). Although the study narrowly missed its primary endpoint (HR 0.89; 95% CI, 0.77–1.04) for hHF and cardiovascular mortality, critiques centered on regional variations and adherence issues. Subgroup analyses revealed reductions in cardiovascular mortality and HF events among patients with lower natriuretic peptide levels and among women [43,44]. However, elevated rates of hyperkalemia (18.7% vs. 9.1%) and increased serum creatinine led to discontinuation in roughly one-third of participants, limiting guideline endorsement even after post hoc analyses demonstrated benefit in North American cohorts [45] (Table 2).
Despite this, a TOPCAT sub-analysis in patients with repeated UACr measurements found spironolactone reduced UACr by 39% overall and by 76% in those with microalbuminuria at one year. These reductions correlated with declines in hHF (HR 0.90; 95% CI, 0.82–0.98) and all-cause mortality (HR 0.91; 95% CI, 0.84–0.98), highlighting the association between eGFR decline, albumin leakage, and HF outcomes [46] (Table 3).
5.2. Non-Steroid MRAs
Given the antialbuminuric effects of MRAs, research has focused on developing non-steroidal agents to minimize adverse effects. Finerenone, a novel non-steroidal MRA, has lower affinity for sex hormone receptors and a reduced risk of hyperkalemia [47].
Initial trials, FIDELIO-DKD and FIGARO-DKD, assessed finerenone’s impact on renal and cardiovascular outcomes in patients with T2D and CKD. Finerenone led to an early eGFR decline at 4 months (-3.18 vs. -0.73 ml/min/1.73 m2), but by study end, the treated group showed less decline compared to controls (-2.66 vs. -3.97 ml/min/1.73 m2), alongside significant reductions in CKD progression, albuminuria, and cardiovascular events, including a 22% reduction in hHF (HR 0.78; 95% CI, 0.66–0.92), independent of baseline HF status [48].
A pooled analysis of EMPHASIS-HF and TOPCAT confirmed an acute eGFR decline (average 2–2.4 ml/min/1.73 m2) after steroidal MRAs without long-term differences in slope versus placebo, indicating no sustained renal harm [8]. Encouraged by these findings, finerenone was evaluated in HF patients in the FINEARTS-HF trial, which enrolled 6,001 patients with HFpEF or HFmrEF (mean eGFR 63 ml/min/1.73 m2; 45% women; 45.5% with diabetes). Finerenone significantly reduced total HF events and cardiovascular death (HR 0.84; 95% CI, 0.74–0.95), with low rates of significant hyperkalemia (>6.0 mmol/L: 3% vs. 1.4%) [49].
Interestingly, 23.0% of finerenone-treated patients experienced >15% eGFR declines, compared to 13.4% in the placebo group (HR 1.95; 95% CI, 1.69–2.24). However, increased risk of adverse outcomes was only seen with eGFR decline in the placebo arm (adjusted HR 1.50; 95% CI, 1.20–1.89), not with finerenone (adjusted rate ratio 1.07; 95% CI, 0.84–1.35; p interaction = 0.04), suggesting finerenone’s renal safety across eGFR trajectories and LVEF ranges [50] (Table 2).
The FINEARTS-HF study revealed an early, drug-induced eGFR decline that stabilized by 90 days, mirroring sustained reductions in albuminuria (-30%) and risk of new-onset micro- and macroalbuminuria (-38%). Although the composite renal endpoint was not significantly affected, the parallel changes in UACr and eGFR slopes underscored their interconnected pathophysiology [51].
A subsequent meta-analysis in The Lancet confirmed the prognostic benefits of MRAs across HF phenotypes, despite an increased frequency of eGFR declines >30% in treated groups. Importantly, large MRA trials typically excluded patients with eGFR <45 ml/min/1.73 m2, highlighting the context needed when interpreting these declines [52] (Table 2 and Table 3).
Collectively, these data indicate that eGFR declines under MRA therapy often reflect reductions in intraglomerular pressure, particularly in patients with diabetes or HF, where decreased albuminuria translates into long-term renal and cardiovascular benefits [22,23,24,48,50]

Table 2.
Effect or mineralcorticoid receptor antagonists on renal function and cardiovascular outcome in heart failure patients.
Table 2.
Effect or mineralcorticoid receptor antagonists on renal function and cardiovascular outcome in heart failure patients.
| Study | Population characteristics | Mean GFR* |
eGFR detected changes in study course | Relation between study outcome and detected eGFR changes |
|---|---|---|---|---|
| TOPCAT [45,69] | Number. 1767 LVEF 58± 7 |
53% GFR<60 | - Creatinine increase from baseline was greater in spironolacone than in. placebo group (+12.5% vs. +3.5%). - GFR mean reduction was greater in spironolactone than in placebo group (– 2.3 vs -0.7 ml/min/m2) |
- In 14% WRF was observed (Creatinine increase >0.3 mg/dl or >25% from baseline to 4 months). - WRF was associated with increased risk in whole population (HR 2.22 IC 1.67-2.96) - Patients developing WRF in the placebo group were at higher absolute risk of the primary endpoint compared to Spironolactone group: (39.6 events per 100 patient-years;95% CI: 25.5 to 61.3) vs. placebo group (16.7 events per 100 patient-years; 95% CI: 12.0 - 23.3) |
| Pooled analysis of EMPHASIS TOPCAT and EPHESUS [83] |
Number 12700 | 43% with GFR*<60 | 2.6% experienced eGFR< 30 ml/min/m2 across study period | - Randomization to MRA (vs placebo) increased stepwise the odds of developing WRF by 1.2- to 2.0-fold - The effect of MRAs vs placebo on the reduction of CV death / hHF was attenuated as GFR decreased (treatment-by-eGFR interaction P for trend¼ 0.033). - Primary outcome with MRA therapy was similar in those who experienced a decrease in GFR to <30 mL/min/1.73 m2 (HR: 0.65; 95% CI: 0.43-0.99) compared with those who did not (HR: 0.63; 95% CI: 0.56-0.71) |
| FINEARTS HF [49,50] | Number: 5587 Age 72 ± 10 years Males: 60% LVEF: 53±8% |
62 ± 19 | Early (1 month) GFR decline >15%: 23% in finerenone and 13.4% in placebo (OR: 1.95; 95% CI: 1.69-2.24; P < 0.001) |
Greater risk of hHF/CV death after early GFR decline in placebo group (RR: 1.56; 95% CI: 1.22-1.99; P < 0.01) than in finerenone group (RR: 1.14; 95% CI: 0.90-1.43; P= 0.27; P interaction = 0.06) |
*Expressed as ml/min*1.73 m2. CKD: chronic kidney disease; CV: cardiovascular; EMPHASIS HF: Eplerenone in mild patients hospitalization and survival study in heart failure; FINEARTS HF: Finerenone Trial to Investigate Efficacy and Safety Superior to Placebo in Patients With Heart Failure; GFR: estimated glomerular filtration rate; hHF: hospitalization for heart failure; HR: Hazard Raio; LVEF: left ventricular ejection fraction; RALES: Randomized aldactone evaluation study; TOPCAT: Americans Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist. WRF: Worsening renal function.
Table 3.
Table reports data generated by post-hoc analysis of heart failure trials and evaluating the effects of albuminuria on outcome and on therapy renal effect. On note, heart failure study design did not include albuminuria among the prespecified protocol analysis criteria.
Table 3.
Table reports data generated by post-hoc analysis of heart failure trials and evaluating the effects of albuminuria on outcome and on therapy renal effect. On note, heart failure study design did not include albuminuria among the prespecified protocol analysis criteria.
| Study |
Type of Analysis | Albuminuria n (%) |
Adverse outcome | All-Cause Mortality | Drug effects on renal function and albuminuria |
|---|---|---|---|---|---|
| Val-Heft [23] | Relationships between study outcomes and proteinuria in HFrEF patients | 405*/5010 (8%) |
- Proteinuria: HR: 1.28 (95%CI: 1.06- 1.55) for first morbid - Proteinuria and CKD: HR: 1.26 (95%CI: 1.01- 1.57) for first morbid - Proteinuria and no-CKD: HR: 1.42 (95%CI: 0.98 to 2.07) for first morbid |
- Proteinuria: HR: 1.28 (95%CI: 1.01- 1.62) for first morbid - Proteinuria and CKD: HR: 1.26 (95%CI: 0.96- 1.66) for first morbid - Proteinuria and no-CKD: HR: 1.37 (95%CI: 0.83 to 2.26) for first morbid |
Without Albuminuria GFR† change: -2.6±0.2 in placebo group vs. -6.5±0.2 in Valsartan group (mean difference -3.9). With Albuminuria GFR† change: -5.3±0.6 in placebo group vs. -6.6±0.6 mL in Valsartan group (mean difference -1.3) |
| PARADIGM-HF [26] | Renal effects of sacubitril/valsartan in patients with HFrEF | UACR‡: albuminuria in 441/1872 (24%) |
First morbid event, post-hoc prespecified composite renal outcome: sacubitril/valsartan vs Enalapril HR 0.94 (95%CI: 0.40–2.2) | Sacubitril/valsartan vs Enalapril HR 1.15 (95%CI: 0.78–1.71) |
Risk of albuminuria: - HR 1.20 (95% CI: 1.04- 1.36) after sacubitril/valsartan - HR 0.90 (95% CI: 0.77 -1.03) after Enalapril |
| EMPEROR POOLED [65] |
Secondary analysis of EMPEROR reduced and EMPEROR Preserved pooled data | 9673 patients with assessed UACR‡: Microalbuminuria in 32%, macroalbuminuria in 11% |
Empagliflozin vs Placebo for first and recurrent hHF: HR: 0.72; 95%CI: 0.63-0.82 |
Empagliflozin vs. Placebo: HR: 0.97 (95%CI: 0.87-1.08) |
Empagliflozin vs placebo GFR† slope difference: - UACr <30: −1.6 (95%CI: 1.2-1.9) - UACr 30- 300: −2.5 (95%CI: −2.9 - −2.2) - UACr >300: −4.0 (95%CI: −4.6 - −3.3) |
| TOPCAT [45] | Secondary analysis on a TOPCAT subpopulation focusing on UACr association with renal study outcome |
744 patients with UACR‡ detected at baseline and at 1-year visit (microalbuminuria in 35%, macroalbuminuria in 13%) | Crude Model for Efficacy Outcomes on hHF per UACR halving at the 1-Year Visit vs Baseline: HR: 0.89; 95%CI: 0.82-0.97 |
Crude Model for Efficacy Outcomes per UACr, Halving at the 1-Year Visit vs Baseline. HR: 0.90; 95%CI: 0.83–0.97 |
At 1-year visit, in patients with macroalbuminuria, spironolactone reduced albuminuria by 76% (Geometric Mean Ratio: 0.24; 95%CI: 0.10–0.56) |
| FINEARTS-HF [51] | UACr changes over time and the development of microalbuminuria and macroalbuminuria | 5797 patients with assessed UACr‡ (microalbuminuria in 30% macroalbuminuria in 10%) |
- | - | After Six months, reduction in UACr in finerenone group: Mean -30% (95%CI: 25%-34%) Composite kidney outcome (including >57% eGFR fall) in Placebo vs Finerenone: HR: 1.28; 95%CI: 0.80-2.05 |
* albuminuria detected with positive urine stick at baseline; † expressed as ml/min x 1.73m2; ‡ assessed by urine albumin to creatinine ratio and expressed as mg/g; ARNI: angiotensin receptor neprilisyn inhibitor; CI: confidence interval; EMPEROR POOLED: Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction and Empagliflozin in Heart Failure with a Preserved Ejection Fraction trials combined; FINEARTS: Finerenone Trial to Investigate Efficacy and Safety Superior to Placebo in Patients With Heart Failure; GFR: estimated glomerular filtration rate; hHF: hospitalization for heart failure. HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction; HR= hazard ratio; PARADIGM-HF: Prospective Comparison of ARNI with ACE inhibition to Determine Impact on Global Mortality and Morbidity in Heart Failure; TOPCAT: Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist; UACr= urine albumin creatinine ratio; Val-HeFT: Valsartan in HF Trial.
6. Sodium-Glucose Cotransporter Type 2 Inhibitors (SGLT2i)
Initially developed as glucose-lowering agents, SGLT2 inhibitors (SGLT2i, or gliflozins) demonstrated unexpected cardiovascular and renal benefits in diabetic patients, as shown in EMPA-REG OUTCOME, DECLARE, CANVAS, and CREDENCE trials. These findings led to their application in patients with HF and CKD, resulting in reduced risks of HF progression and CKD worsening [53]. Although early benefits were attributed to natriuretic effects, subsequent research highlighted more complex renal mechanisms [54], with consistent efficacy across HF phenotypes, irrespective of diabetes or CKD status.
Administration of SGLT2i typically induces a modest, transient decline in eGFR (approximately −3 to −5 mL/min/1.73 m2 within 2–4 weeks), reflecting reduced intraglomerular pressure. By restoring tubular Na+ concentrations, these agents enhance tubuloglomerular feedback and lower filtration pressure [55,56]. Unlike angiotensin II blockade, this mechanism complements sacubitril-valsartan, particularly in patients with reduced ejection fraction [57]. Importantly, this early eGFR dip signals hemodynamic efficacy and is associated with long-term cardiovascular and renal protection, not harm [55,56,58].
Following this initial dip, eGFR tends to stabilize or improve, and long-term therapy slows GFR decline relative to placebo across diverse cohorts [Table 4]. In DAPA-HF, dapagliflozin led to a smaller eGFR decrease (−1.09 vs. −2.85 mL/min/1.73 m2 with placebo) [59]. Similar patterns emerged in DELIVER (HFmrEF/HFpEF) [60] and in EMPEROR-Reduced and EMPEROR-Preserved, where treated patients consistently experienced less decline [61,62].
Conversely, post hoc analyses linked spontaneous eGFR decreases in placebo groups to higher cardiovascular, renal, and mortality risks [61,62], as noted in DAPA-HF [59]. In EMPEROR trials, eGFR rose after SGLT2i discontinuation, aligning treated patients with placebo outcomes within 30 days [63], mirroring reversibility seen in diabetes studies [64].
Empagliflozin also reduced macroalbuminuria incidence (HR 0.81; 95% CI: 0.70–0.94) and increased regression to normo- or microalbuminuria (HR 1.31; 95% CI: 1.07–1.59), particularly in diabetic patients with higher baseline UACr [65] [Table 3]. Additionally, SGLT2i lowered acute kidney injury rates and HF events across all investigated settings [53].
These drugs consistently produced early reductions in primary endpoints (by 21–25% within 30 days), with benefits comparable in scale to ACE inhibitors when first introduced for HF [56,66]. The direct modulation of renin release by SGLT2 inhibition may further explain these additive effects [56,58].
7. Discussion
CKD is the most prevalent comorbidity in patients with HF, followed by diabetes, which compounds disease burden [3,67,68]. Clinicians often interpret eGFR declines from evidence-based therapies as alarming signs of “worsening kidney function,” implying imminent renal failure. However, this overlooks the kidney’s physiological role in volume and toxin regulation and its unique vascular architecture—receiving 25% of cardiac output while comprising just 0.7% of body mass—to rapidly adjust filtration in response to circulatory demands [58,64,68].
To maintain a typical GFR near 125 mL/min, the kidney activates mechanisms—chiefly RAAS and sympathetic responses—whenever blood flow decreases. These adaptations elevate intraglomerular pressure to sustain filtration but at the cost of potential long-term damage, masking CKD progression while preserving GFR up to 130–140 mL/min/1.73 m2 [11,58,69,70].
Therapies such as ACEi/ARBs, ARNI, MRAs, and SGLT2i should thus be viewed not merely as agents altering GFR, but as modulators restoring physiologic intraglomerular pressures. Large trials consistently show that despite early eGFR variability, these agents preserve renal function and improve HF outcomes in patients with and without diabetes [11,51,53,55,58,59,70]. Notably, substantial eGFR declines (>30%) are rare, usually reversible, and infrequently linked to adverse renal events [4,63,64,68].
The extent and timing of eGFR dips vary by drug mechanism, patient characteristics, background therapy, and trial design. Larger acute eGFR reductions often occur in patients with better baseline kidney function, yet may still be beneficial in advanced CKD [53]. For instance, in type 2 diabetes studies, those with the greatest eGFR declines during early RAAS blockade had the best long-term renal preservation [72].
However, inconsistent definitions of WRF across HF trials have muddled interpretation of renal outcomes and drug effects on CKD progression [57,63,66,71]. A secondary analysis of over 28,000 HF patients from six trials of steroidal MRAs, ARNI, and SGLT2i demonstrated that, under standardized kidney endpoints, these therapies had neutral or beneficial impacts on renal outcomes [74]. This underscores the need for harmonized definitions, especially as most HF trials exclude patients with advanced CKD (stage IV), focusing on milder renal impairment. Consequently, HF events typically dictate trial endpoints, often censoring patients before long-term renal changes manifest [74,75].
Analyzing eGFR slopes offers a more robust indicator of drug effects than discrete events, though it requires adequate power and consistent analytic standards [75,76]. In HF patients with preserved eGFR, the early “dip” with SGLT2i often predicts longer-term benefits, as shown by improvements in both HF events and chronic eGFR trajectories [53,56,64,71,72,73,77]. The FINEARTS-HF trial further supported this, with a win ratio of 1.17 (95% CI: 1.04–1.32) that remained favorable despite early declines, stabilizing after roughly 12 months [78].
Albuminuria, a marker of glomerular injury driven by hypertension, insulin resistance, and hyperglycemia, is strongly linked to incident HF and exacerbations, especially with low eGFR [79]. RAAS and SGLT2 inhibitors mitigate albuminuria through distinct hemodynamic pathways (Figure 1), supporting combination strategies in HF management. Caution is needed in interpreting early rises in UACr with ARNI, often reflecting mesangial relaxation from natriuretic peptide effects rather than structural damage [26,27,28].
Longitudinal UACr monitoring, as recommended by KDIGO categories, enables better risk stratification and timely therapeutic adjustments [29,68,69,80]. Evidence from post hoc analyses shows that effective therapy rapidly alters albuminuria, linking changes to improved HF and renal outcomes [23,24,45,48,50,53,68,79].
Finally, it is crucial to challenge misconceptions that modest slowing of eGFR decline with RAAS or SGLT2 inhibitors lacks clinical significance. EMPA-Kidney demonstrated that greater relative benefits in chronic slope occur among higher-risk patients, emphasizing the value of this metric even when short-term changes appear modest [80].
Data also contest the notion that aging inherently leads to GFR loss. Longitudinal registries show stable renal function in healthy aging [81], suggesting preserved filtration is a meaningful endpoint tied to reduced HF exacerbations [34].
Regarding thresholds, while eGFR <30 mL/min/1.73 m2 often precludes RAAS or SGLT2 initiation, observational data suggest potential benefits with cautious monitoring, including in advanced CKD. Finerenone demonstrated safety and efficacy down to eGFR 25, while dapagliflozin and empagliflozin were safe and effective in HF patients with eGFR as low as 20–25 [48,49,54,82]. Nonetheless, steroidal MRA benefits wane near eGFR 30, and careful management is required to avoid limiting other key HF therapies [80,82].
8. Conclusions
Renal function plays a pivotal role in the progression, management, and outcomes of heart failure (HF), often complicating treatment strategies. The complex interplay among cardiac, renal, and metabolic systems frequently leads clinicians to rely on glomerular filtration rate (GFR) changes as primary indicators of therapeutic tolerance. This narrow focus can obscure a true understanding of drug efficacy in clinical practice. As a result, neurohormonal therapies are frequently underdosed or prematurely discontinued, particularly when eGFR approaches 30 mL/min/1.73 m2 [9]. Conversely, robust data from studies in diabetic patients with moderate renal impairment and albuminuria demonstrate that evidence-based treatments maintain a favorable safety profile even in these populations, underscoring the need to prioritize therapy optimization over eGFR fluctuations.
Misinterpretation of treatment-induced eGFR changes often places HF patients with CKD at greater risk by withholding essential therapies, thereby exacerbating their prognosis relative to patients without CKD [4,70,80,84]. This issue is compounded by inadequate clinical monitoring, which prevents timely dose adjustments and contributes to unnecessary treatment withdrawal.
Clinicians must appreciate that renal physiology is inherently designed to maintain filtration under varying circulatory conditions. The kidneys continuously monitor blood pressure and flow, rapidly deploying compensatory mechanisms to sustain glomerular filtration pressure and preserve filtrate production. While this response is initially protective, in chronic cardiovascular disease it becomes maladaptive, perpetuating neurohormonal activation and contributing to HF onset and progression.
By adhering to patient selection criteria established in major clinical trials and ensuring diligent follow-up, clinicians should recognize early declines in eGFR as indicative of favorable intraglomerular hemodynamic adjustments. These changes mitigate maladaptive neurohormonal responses and ultimately support improved long-term outcomes in patients with HF.
Supplementary Materials
No supplementary materials.
Author Contributions
Conceptualization, E.G.; methodology, E.G., M.I., A.P., S.C., A.A.; data curation, E.G., M.I., A.P., S.C., A.A; writing—original draft preparation, E.G., M.I., A.P., A.A; writing—review and editing, S.C., D.G., L.T.; visualization, E.G., M.I., A.P., S.C., A.A., D.G., L.T.; supervision, D.G., L.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AA | Afferent arteriole |
| ACEi | Angiotensin-converting enzyme inhibitors |
| ARB | Angiotensin receptor blockers |
| ARNI | Angiotensin Receptor Neprilysin Inhibitor |
| CKD | Chronic kidney disease |
| EA | Effeerent arteriole |
| eGFR | estimated glomerular filtration rate |
| HF | Heart Failure |
| hHF | Heart failure hospitalizations |
| HFmrEF | Heart failure with mildly reduced ejection fraction |
| HFpEF | Heart failure with preserved ejection fraction |
| HFrEF | Heart failure with reduced ejection fraction |
| LVEF | Left ventricular ejection fraction |
| MRA | Mineralocorticoid receptor antagonists |
| RAAS | Renin angiotensin aldosterone system |
| sCr | Serum creatinine |
| SGLT2i | Sodium-glucose cotransporter 2 inhibitors |
| WRF | Worsening renal function |
| UACr | Urinary albumin-creatinine ratio |
References
- Damman, K.; Valente, M.A.; Voors, A.A.; O'Connor, C.M.; van Veldhuisen, D.J.; Hillege, H.L. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J. 2014, 35, 455–469. [Google Scholar] [CrossRef] [PubMed]
- Mark, P.B.; Carrero, J.J.; Matsushita, K.; Sang, Y.; Ballew, S.H.; Grams, M.E.; et al. Major cardiovascular events and subsequent risk of kidney failure with replacement therapy: a CKD Prognosis Consortium study. Eur Heart J. 2023, 44, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- van Deursen, V.M.; Urso, R.; Laroche, C.; Damman, K.; Dahlstrom, U.; Tavazzi, L.; Maggioni, A.P.; Voors, A.A. Co-morbidities in patients with heart failure: an analysis of the European Heart Failure Pilot Survey. Eur J Heart Fail. 2014, 16, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Damman, K. When Kidney Function Declines But Therapy Still Works: The Case for Nonsteroidal MRA Therapy in Heart Failure. J Am Coll Cardiol 2025, 85, 186–189. [Google Scholar] [CrossRef]
- McCallum, W.; Tighiouart, H.; Ku, E.; Salem, D.; Sarnak, M.J. Trends in Kidney Function Outcomes Following RAAS Inhibition in Patients With Heart Failure With Reduced Ejection Fraction. Am J Kidney Dis 2020, 75, 21–29. [Google Scholar] [CrossRef]
- Damman, K.; Perez, A.C.; Anand, I.S.; Komajda, M.; McKelvie, R.S.; Zile, M.R.; Massie, B.; Carson, P.E.; McMurray, J.J. Worsening renal function and outcome in heart failure patients with preserved ejection fraction and the impact of angiotensin receptor blocker treatment. J Am Coll Cardiol 2014, 64, 1106–13. [Google Scholar] [CrossRef]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Zeller, C.; Anker, S.D.; Butler, J.; et al. Cardiac and Kidney Benefits of Empagliflozin in Heart Failure Across the Spectrum of Kidney Function: Insights From EMPEROR-Reduced. Circulation 2021, 143, 310–321. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Ferreira, J.P.; Rossignol, P.; Neuen, B.L.; Claggett, B.L.; Pfeffer, M.A.; et al. Effects of steroidal mineralocorticoid receptor antagonists on acute and chronic estimated glomerular filtration rate slopes in patients with chronic heart failure. Eur J Heart Fail 2022, 24, 1586–1590. [Google Scholar] [CrossRef]
- Shahim, A.; Linde, C.; Savarese, G.; Dahlstrom, U.; Lund, L.H.; Hage, C. Implementation of guideline-recommended therapies in heart failure with reduced ejection fraction according to heart failure duration: An analysis of 55‚Äâ581 patients from the Swedish Heart Failure (SwedeHF) Registry. Eur J Heart Fail 2025. [Google Scholar] [CrossRef]
- Dalal, R.; Bruss, Z.S.; Sehdev, J.S. Physiology, Renal Blood Flow and Filtration. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482248/.
- Pollak, M.R.; Quaggin, S.E.; Hoenig, M.P.; Dworkin, L.D. The glomerulus: the sphere of influence. Clin J Am Soc Nephrol 2014, 9, 1461–9. [Google Scholar] [CrossRef]
- Romagnani, P.; Remuzzi, G.; Glassock, R.; Levin, A.; Jager, K.J.; Tonelli, M.; Massy, Z.; Wanner, C.; Anders, H.J. Chronic kidney disease. Nat Rev Dis Primers. 1708, 3, 17088. [Google Scholar] [CrossRef]
- Packer, M. Why do the kidneys release renin in patients with congestive heart failure? A nephrocentric view of converting-enzyme inhibition. Eur Heart J 1990, 11 Suppl D, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Butt, L.; Unnersjo-Jess, D.; Hohne, M.; Edwards, A.; Binz-Lotter, J.; Reilly, D.; et al. A molecular mechanism explaining albuminuria in kidney disease. Nat Metab. 2020, 2, 461–474. [Google Scholar] [CrossRef] [PubMed]
- Benghanem Gharbi, M.; Elseviers, M.; Zamd, M.; Belghiti Alaoui, A.; Benahadi, N.; Trabelssi el, H.; et al. Chronic kidney disease, hypertension, diabetes, and obesity in the adult population of Morocco: how to avoid "over"- and "under"-diagnosis of CKD. Kidney Int 2016, 89, 1363–71. [Google Scholar] [CrossRef]
- Ljungman, S.; Kjekshus, J.; Swedberg, K. Renal function in severe congestive heart failure during treatment with enalapril (the Cooperative North Scandinavian Enalapril Survival Study [CONSENSUS] Trial). Am J Cardiol 1992, 70, 479–87. [Google Scholar] [CrossRef] [PubMed]
- Dries, D.L.; Exner, D.V.; Domanski, M.J.; Greenberg, B.; Stevenson, L.W. The prognostic implications of renal insufficiency in asymptomatic and symptomatic patients with left ventricular systolic dysfunction. J Am Coll Cardiol 2000, 35, 681–9. [Google Scholar] [CrossRef]
- Testani, J.M.; Kimmel, S.E.; Dries, D.L.; Coca, S.G. Prognostic importance of early worsening renal function after initiation of angiotensin-converting enzyme inhibitor therapy in patients with cardiac dysfunction. Circ Heart Fail 2011, 4, 685–91. [Google Scholar] [CrossRef]
- Khan, N.A.; Ma, I.; Thompson, C.R.; Humphries, K.; Salem, D.N.; Sarnak, M.J.; Levin, A. Kidney function and mortality among patients with left ventricular systolic dysfunction. J Am Soc Nephrol 2006, 17, 244–53. [Google Scholar] [CrossRef]
- Hillege, H.L.; Nitsch, D.; Pfeffer, M.A.; Swedberg, K.; McMurray, J.J.; Yusuf, S.; et al. Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) Investigators. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation 2006, 113, 671–8. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; Solomon, S.D.; Pfeffer, M.A.; Swedberg, K.; Yusuf, S.; Young, J.B.; et al. Worsening renal function and outcome in heart failure patients with reduced and preserved ejection fraction and the impact of angiotensin receptor blocker treatment: data from the CHARM-study programme. Eur J Heart Fail 2016, 18, 1508–1517. [Google Scholar] [CrossRef]
- Jackson, C.E.; Solomon, S.D.; Gerstein, H.C.; Zetterstrand, S.; Olofsson, B.; Michelson, E.L.; e, al.; CHARM Investigators and Committees. Albuminuria in chronic heart failure: prevalence and prognostic importance. Lancet 2009, 374, 543–50. [Google Scholar] [CrossRef]
- Anand, I.S.; Bishu, K.; Rector, T.S.; Ishani, A.; Kuskowski, M.A.; Cohn, J.N. Proteinuria, chronic kidney disease, and the effect of an angiotensin receptor blocker in addition to an angiotensin-converting enzyme inhibitor in patients with moderate to severe heart failure. Circulation 2009, 120, 1577–84. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Mann, J.F.; Yi, Q.; et al. HOPE Study Investigators. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA 2001, 286, 421–6. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; et al. PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Damman, K.; Gori, M.; Claggett, B.; Jhund, P.S.; Senni, M.; Lefkowitz, M.P.; et al. Renal Effects and Associated Outcomes During Angiotensin-Neprilysin Inhibition in Heart Failure. JACC Heart Fail 2018, 6, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Voors, A.A.; Gori, M.; Liu, L.C.; Claggett, B.; Zile, M.R.; Pieske, B.; et al.; PARAMOUNT Investigators Renal effects of the angiotensin receptor neprilysin inhibitor LCZ696 in patients with heart failure and preserved ejection fraction. Eur J Heart Fail 2015, 17, 510–7. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Remuzzi, G. Combined neprilysin and RAS inhibition for the failing heart: straining the kidney to help the heart? Eur J Heart Fail 2015, 17(5), 468–71. [Google Scholar] [CrossRef]
- House, A.A.; Wanner, C.; Sarnak, M.J.; Pina, I.L.; McIntyre, C.W.; Komenda, P.; et al.; Conference Participants Heart failure in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2019, 95, 1304–1317. [Google Scholar] [CrossRef]
- Chatur, S.; Neuen, B.L.; Claggett, B.L.; Beldhuis, I.E.; Mc Causland, F.R.; Desai, A.S.; et al. Effects of Sacubitril/Valsartan Across the Spectrum of Renal Impairment in Patients With Heart Failure. J Am Coll Cardiol 2024, 83, 2148–2159. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Ge, J.; Lam, C.S.P.; Maggioni, A.P.; et al. PARAGON-HF Investigators and Committees. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N Engl J Med. 2019, 38, 1609–1620. [Google Scholar] [CrossRef]
- Chatur S, Claggett BL, McCausland FR, Rouleau J, Zile MR, Packer M, Pfeffer MA, Lefkowitz M, McMurray JJV, Solomon SD, Vaduganathan M. Variation in Renal Function Following Transition to Sacubitril/Valsartan in Patients With Heart Failure. J Am Coll Cardiol 2023, 81, 1443–1455. [Google Scholar] [CrossRef]
- Mc Causland, F.R.; Lefkowitz, M.P.; Claggett, B.; Anavekar, N.S.; Senni, M.; Gori, M.; et al. . Angiotensin-Neprilysin Inhibition and Renal Outcomes in Heart Failure With Preserved Ejection Fraction. Circulation 2020, 142, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Chatur, S.; Vaduganathan, M.; Peikert, A.; Claggett, B.L.; McCausland, F.R.; Skali, H.; et al. Longitudinal trajectories in renal function before and after heart failure hospitalization among patients with heart failure with preserved ejection fraction in the PARAGON-HF trial. Eur J Heart Fail 2022, 24, 1906–1914. [Google Scholar] [CrossRef] [PubMed]
- Pontremoli, R.; Borghi, C.; Perrone Filardi, P. Renal protection in chronic heart failure: focus on sacubitril/valsartan. Eur Heart J Cardiovasc Pharmacother 2021, 7, 445–452. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Jackson, A.M.; Lam, C.S.P.; Redfield, M.M.; Anand, I.S.; Ge, J.; et al. Effects of Sacubitril-Valsartan Versus Valsartan in Women Compared With Men With Heart Failure and Preserved Ejection Fraction: Insights From PARAGON-HF. Circulation 2020, 141, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Selye, H.; Hall, C.E.; Rowley, E.M. Malignant Hypertension Produced by Treatment with Desoxycorticosterone Acetate and Sodium Chloride. Can Med Assoc J 1943, 49, 88–92. [Google Scholar] [PubMed]
- Pitt, B.; Zannad, F.; Remme, W.J.; Cody, R.; Castaigne, A.; Perez, A.; Palensky, J.; Wittes, J. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999, 341(10), 709–17. [Google Scholar] [CrossRef]
- Juurlink, D.N.; Mamdani, M.M.; Lee, D.S.; Kopp, A.; Austin, P.C.; Laupacis, A.; Redelmeier, D.A. Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study. N Engl J Med 2004, 351, 543–51. [Google Scholar] [CrossRef]
- Zannad, F.; McMurray, J.J.; Krum, H.; van Veldhuisen, D.J.; Swedberg, K.; Shi, H.; et al.; EMPHASIS-HF Study Group Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 2011, 364, 11–21. [Google Scholar] [CrossRef]
- Eschalier, R.; McMurray, J.J.; Swedberg, K.; van Veldhuisen, D.J.; Krum, H.; Pocock, S.J.; et al.; EMPHASIS-HF Investigators Safety and efficacy of eplerenone in patients at high risk for hyperkalemia and/or worsening renal function: analyses of the EMPHASIS-HF study subgroups (Eplerenone in Mild Patients Hospitalization And SurvIval Study in Heart Failure). J Am Coll Cardiol 2013, 62, 1585–93. [Google Scholar] [CrossRef]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; et al.; TOPCAT Investigators Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 2014, 370, 1383–92. [Google Scholar] [CrossRef]
- Merrill, M.; Sweitzer, N.K.; Lindenfeld, J.; Kao, D.P. Sex Differences in Outcomes and Responses to Spironolactone in Heart Failure With Preserved Ejection Fraction: A Secondary Analysis of TOPCAT Trial. JACC Heart Fail 2019, 7, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Anand, I.S.; Claggett, B.; Liu, J.; Shah, A.M.; Rector, T.S.; Shah, S.J.; et al. Interaction Between Spironolactone and Natriuretic Peptides in Patients With Heart Failure and Preserved Ejection Fraction: From the TOPCAT Trial. JACC Heart Fail 2017, 5, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.A.; Claggett, B.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Clausell, N.; et al. Regional variation in patients and outcomes in the Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist (TOPCAT) trial. Circulation 2015, 131, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, S.; Claggett, B.; Shah, S.J.; Anand, I.; Rouleau, J.L.; O'Meara, E.; et al. Prognostic Value of Albuminuria and Influence of Spironolactone in Heart Failure With Preserved Ejection Fraction. Circ Heart Fail 2018, 11, e005288. [Google Scholar] [CrossRef]
- Bayer Healthcare Pharmaceuticals Inc. KERENDIA (finerenone) prescribing information. Accessed August 17, 2021. https://labeling. bayerhealthcare.com/html/products/pi/Kerendia_ PI.pdf.
- Filippatos, G.; Anker, S.D.; Pitt, B.; Rossing, P.; Joseph, A.; Kolkhof, P.; et al. Finerenone and Heart Failure Outcomes by Kidney Function/Albuminuria in Chronic Kidney Disease and Diabetes. JACC Heart Fail 2022, 10, 860–870. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Vaduganathan, M.; Claggett, B.; Jhund, P.S.; Desai, A.S.; et al.; FINEARTS-HF Committees and Investigators Finerenone in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med 2024, 391, 1475–1485. [Google Scholar] [CrossRef]
- Matsumoto, S.; Jhund, P.S.; Henderson, A.D.; Bauersachs, J.; Claggett, B.L.; Desai, A.S.; et al. Initial Decline in Glomerular Filtration Rate With Finerenone in HFmrEF/HFpEF: A Prespecified Analysis of FINEARTS-HF. J Am Coll Cardiol 2025, 85, 173–185. [Google Scholar] [CrossRef]
- Mc Causland, F.R.; Vaduganathan, M.; Claggett, B.L.; Kulac, I.J.; Desai, A.S.; Jhund, P.S.; et al. Finerenone and Kidney Outcomes in Patients With Heart Failure: The FINEARTS-HF Trial. J Am Coll Cardiol 2025, 85, 159–168. [Google Scholar] [CrossRef]
- Jhund, P.S.; Talebi, A.; Henderson, A.D.; Claggett, B.L.; Vaduganathan, M.; Desai, A.S.; et al. Mineralocorticoid receptor antagonists in heart failure: an individual patient level meta-analysis. Lancet 2024, 404, 1119–1131. [Google Scholar] [CrossRef]
- Nuffield Department of Population Health Renal Studies Group; SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists' Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: collaborative meta-analysis of large placebo-controlled trials. Lancet 2022, 400(10365), 1788-1801. [CrossRef]
- Marton, A.; Saffari, S.E.; Rauh, M.; Sun, R.N.; Nagel, A.M.; Linz, P.; et al. Water Conservation Overrides Osmotic Diuresis During SGLT2 Inhibition in Patients With Heart Failure. J Am Coll Cardiol 2024, 83, 1386–1398. [Google Scholar] [CrossRef] [PubMed]
- Cherney, D.Z.; Perkins, B.A.; Soleymanlou, N.; Maione, M.; Lai, V.; Lee, A.; et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation 2014, 129, 587–97. [Google Scholar] [CrossRef] [PubMed]
- Gronda, E.; Iacoviello, M.; Arduini, A.; Benvenuto, M.; Gabrielli, D.; Bonomini, M.; Tavazzi, L. Gliflozines use in heart failure patients. Focus on renal actions and overview of clinical experience. Eur J Intern Med 2025, 132, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Pocock, S.J.; et al.; EMPEROR-Reduced Trial Committees and Investigators Influence of neprilysin inhibition on the efficacy and safety of empagliflozin in patients with chronic heart failure and a reduced ejection fraction: the EMPEROR-Reduced trial. Eur Heart J 2021, 42, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Vallon, V.; Kim, Y.C. Protecting the Kidney: The Unexpected Logic of Inhibiting a Glucose Transporter. Clin Pharmacol Ther 2022, 112, 434–438. [Google Scholar] [CrossRef]
- Adamson, C.; Docherty, K.F.; Heerspink, H.J.L.; de Boer, R.A.; Damman, K.; Inzucchi, S.E.; et al. Initial Decline (Dip) in Estimated Glomerular Filtration Rate After Initiation of Dapagliflozin in Patients With Heart Failure and Reduced Ejection Fraction: Insights From DAPA-HF. Circulation 2022, 146, 438–449. [Google Scholar] [CrossRef]
- Mc Causland, F.R.; Claggett, B.L.; Vaduganathan, M.; Desai, A.S.; Jhund, P.; de Boer, R.A.; et al. Dapagliflozin and Kidney Outcomes in Patients With Heart Failure With Mildly Reduced or Preserved Ejection Fraction: A Prespecified Analysis of the DELIVER Randomized Clinical Trial. JAMA Cardiol. 2023, 8, 56–65. [Google Scholar] [CrossRef]
- Zannad, F.; Ferreira, J.P.; Gregson, J.; Kraus, B.J.; Mattheus, M.; Hauske, S.J.; et al.; EMPEROR-Reduced Trial Committees and Investigators Early changes in estimated glomerular filtration rate post-initiation of empagliflozin in EMPEROR-Reduced. Eur J Heart Fail 2022, 24, 1829–1839. [Google Scholar] [CrossRef]
- Rastogi, T.; Ferreira, J.P.; Butler, J.; Kraus, B.J.; Mattheus, M.; Brueckmann, M.; et al. Early changes in estimated glomerular filtration rate post-initiation of empagliflozin in EMPEROR-Preserved. Eur J Heart Fail 2024, 26, 885–896. [Google Scholar] [CrossRef]
- Packer, M.; Butler, J.; Zeller, C.; Pocock, S.J.; Brueckmann, M.; Ferreira, J.P.; et al. Blinded Withdrawal of Long-Term Randomized Treatment With Empagliflozin or Placebo in Patients With Heart Failure. Circulation 2023, 148, 1011–1022. [Google Scholar] [CrossRef]
- Heerspink, H.J.; Perkins, B.A.; Fitchett, D.H.; Husain, M.; Cherney, D.Z. Sodium Glucose Cotransporter 2 Inhibitors in the Treatment of Diabetes Mellitus: Cardiovascular and Kidney Effects, Potential Mechanisms, and Clinical Applications. Circulation 2016, 134, 752–72. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Zannad, F.; Butler, J.; Filippatos, G.; Pocock, S.J.; Brueckmann, M.; et al. Association of Empagliflozin Treatment With Albuminuria Levels in Patients With Heart Failure: A Secondary Analysis of EMPEROR-Pooled. JAMA Cardiol 2022, 7, 1148–1159. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Nie, Z.; Shi, R.; Yu, D.; Wang, Q.; Shao, F.; et al. Time to Benefit of Sodium-Glucose Cotransporter-2 Inhibitors Among Patients With Heart Failure. JAMA Netw Open 2023, 6, e2330754. [Google Scholar] [CrossRef] [PubMed]
- Marx, N.; Federici, M.; Schott, K.; Muller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; et al.; ESC Scientific Document Group 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J 2023, 44, 4043–4140. [Google Scholar] [CrossRef] [PubMed]
- Beldhuis, I.E.; Lam, C.S.P.; Testani, J.M.; Voors, A.A.; Van Spall, H.G.C.; Ter Maaten, J.M.; Damman, K. Evidence-Based Medical Therapy in Patients With Heart Failure With Reduced Ejection Fraction and Chronic Kidney Disease. Circulation 2022, 145, 693–712. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, L.; Sun, L.; Arnold, M.; Bell, S.; Cho, K.; Kaptoge, S.K.; et al.; Emerging Risk Factors Collaboration/EPIC-CVD/Million Veteran Program Mild-to-Moderate Kidney Dysfunction and Cardiovascular Disease: Observational and Mendelian Randomization Analyses. Circulation 2022, 146, 1507–1517. [Google Scholar] [CrossRef]
- Tonneijck, L.; Muskiet, M.H.; Smits, M.M.; van Bommel, E.J.; Heerspink, H.J.; van Raalte, D.H.; Joles, J.A. Glomerular Hyperfiltration in Diabetes: Mechanisms, Clinical Significance, and Treatment. J Am Soc Nephrol 2017, 28, 1023–1039. [Google Scholar] [CrossRef]
- Neuen, B.L.; Tighiouart, H.; Heerspink, H.J.L.; Vonesh, E.F.; Chaudhari, J.; Miao, S.; et al.; CKD-EPI Clinical Trials Acute Treatment Effects on GFR in Randomized Clinical Trials of Kidney Disease Progression. J Am Soc Nephrol 2022, 33, 291–303. [Google Scholar] [CrossRef]
- Holtkamp, F.A.; de Zeeuw, D.; Thomas, M.C.; Cooper, M.E.; de Graeff, P.A.; et al. An acute fall in estimated glomerular filtration rate during treatment with losartan predicts a slower decrease in long-term renal function. Kidney Int 2011, 80, 282–287. [Google Scholar] [CrossRef]
- Khan, M.S.; Bakris, G.L.; Packer, M.; Shahid, I.; Anker, S.D.; Fonarow, G.C.; et al. Kidney function assessment and endpoint ascertainment in clinical trials. Eur Heart J 2022, 43, 1379–1400. [Google Scholar] [CrossRef]
- Butt, J.H.; McMurray, J.J.V.; Claggett, B.L.; Jhund, P.S.; Neuen, B.L.; McCausland, F.R.; et al. Therapeutic Effects of Heart Failure Medical Therapies on Standardized Kidney Outcomes: Comprehensive Individual Participant-Level Analysis of 6 Randomized Clinical Trials. Circulation 2024, 150, 1858–1868. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Heerspink, H.J.L.; Tighiouart, H.; Levey, A.S.; Coresh, J.; Gansevoort, R.T.; et al. GFR Slope as a Surrogate End Point for Kidney Disease Progression in Clinical Trials: A Meta-Analysis of Treatment Effects of Randomized Controlled Trials. J Am Soc Nephrol, 2019, 30, 1735–1745. [Google Scholar] [CrossRef] [PubMed]
- Mark, P.B.; Carrero, J.J.; Matsushita, K.; Sang, Y.; Ballew, S.H.; Grams, M.E.; et al. Major cardiovascular events and subsequent risk of kidney failure with replacement therapy: a CKD Prognosis Consortium study. Eur Heart J 2023, 44, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Gronda E, Palazzuoli A, Iacoviello M, Benevenuto M, Gabrielli D, Arduini A. Renal Oxygen Demand and Nephron Function: Is Glucose a Friend or Foe? Int J Mol Sci 2023, 24, 9957. [Google Scholar] [CrossRef]
- Kondo, T.; Jhund, P.S.; Henderson, A.D.; Claggett, B.L.; Desai, A.S.; Brinker, M.; et al. The efficacy of finerenone on hierarchical composite endpoint analysed using win statistics in patients with heart failure and mildly reduced or preserved ejection fraction: A prespecified analysis of FINEARTS-HF. Eur J Heart Fail 2025. [Google Scholar] [CrossRef]
- Vaduganathan, M.; Neuen, B.L.; McCausland, F.; Jhund, P.S.; Docherty, K.F.; McMurray, J.J.V.; Solomon, S.D. Why Has it Been Challenging to Modify Kidney Disease Progression in Patients With Heart Failure? J Am Coll Cardiol 2024, 84, 2241–2245. [Google Scholar] [CrossRef]
- EMPA-KIDNEY Collaborative Group. Effects of empagliflozin on progression of chronic kidney disease: a prespecified secondary analysis from the empa-kidney trial. Lancet Diabetes Endocrinol 2024, 12, 39–50. [Google Scholar] [CrossRef]
- Lindeman, R.D.; Tobin, J.; Shock, N.W. Longitudinal studies on the rate of decline in renal function with age. J Am Geriatr Soc 1985, 33, 278–85. [Google Scholar] [CrossRef]
- Ferreira, J.P.; Pitt, B.; McMurray, J.J.V.; Pocock, S.J.; Solomon, S.D.; Pfeffer, M.A.; Zannad, F.; Rossignol, P. Steroidal MRA Across the Spectrum of Renal Function: A Pooled Analysis of RCTs. JACC Heart Fail 2022, 10, 842–850. [Google Scholar] [CrossRef]
Figure 1.
The figure depicts in the glomerular structure the sites and the mechanisms by which different molecules affect the intraglomerular filtration pressure, leading to the fall of the single nephron filtration rate, while they improve heart failure outcome in patients with and without diabetes and or chronic kidney disease, independently of left ventricular ejection fraction phenotype. 1. The ACEi decreases the angiotensin II by inhibiting the angiotensin-converting enzyme. The ARBs provide the same effect by blocking the angiotensin II receptor. Both agents prevent the angiotensin vasoconstrictive action on the efferent arteriole, thereby avoiding the rise in the intra-glomerular pressure gradient that leads to hyperfiltration. 2. The ARNI molecule is a composite product of the ARB valsartan that works as reported above and of the sacubitril enzyme that cleaves metalloproteins that have catabolic action on the atrial natriuretic peptides. The cardiac atria generate those molecules for the specific purpose of providing rapid fluid unloading. Those molecules not only exert fast natriuretic action, but also induce the mesangial structure relaxation, allowing the filtration of a mild amount of albumin that can be detected in the urine. By being a physiology-related effect, the albumin leak does not impact HF outcome but correlates with the intraglomerular vascular resistance decrease. 3. The MRAs not only reduce the sodium reabsorption in the renal collecting tubule, but exerts a potent anti-inflammatory, anti-oxidation and anti-fibrotic action on the glomerular mesangial structure, shielding the delicate sieve deputed to select plasma solutes that have to be preserved from filtration (i.e.,: albumin) and the amounts of electrolytes and molecules generating the filtrate. The MRAs contentive action over the filtration process importantly concurs to balance the intraglomerular filtration pressure. 4. In the early segment of the glomerular tubule, the SGLT2 is primarily involved in the reabsorption of filtered glucose, a pivotal body nutrient, coupling one glucose molecule with one atom of sodium. The SGLT2 contemporary combines the largest sodium reabsorption in the kidney through the intertwined action of NHE3, located in the apical membrane of the proximal tubule section. The contemporary sodium reuptake is not trivial since the sodium is the electrolyte that provides the electrical gradient to the cell membrane as the energy source for biological needs. On the basis of renal physiology, any condition entailing the rise of filtrate production results in an immediate increase of SGLT2 expression coupled with the activity of NHE3. The combined action largely impoverishes the sodium content in the filtrate. The low sodium concentration by reaching the juxtaglomerular apparatus affects the production of adenosine, the eutakoid deputed to interact with the specialized receptor in the afferent arteriole to raise the vessel muscular tone, leading to the restraint of the vessel section, taping down the intraglomerular pressure. On top of this the adenosine concentration provides braking action of renin production in the juxtaglomerular apparatus. The SGLT2 inhibitors affect the disproportioned glucose reabsorption in the proximal tubule, which can put under control the largest intrarenal asset of mechanisms involved in sodium retention and neurohormonal activation. (see text for details).
Figure 1.
The figure depicts in the glomerular structure the sites and the mechanisms by which different molecules affect the intraglomerular filtration pressure, leading to the fall of the single nephron filtration rate, while they improve heart failure outcome in patients with and without diabetes and or chronic kidney disease, independently of left ventricular ejection fraction phenotype. 1. The ACEi decreases the angiotensin II by inhibiting the angiotensin-converting enzyme. The ARBs provide the same effect by blocking the angiotensin II receptor. Both agents prevent the angiotensin vasoconstrictive action on the efferent arteriole, thereby avoiding the rise in the intra-glomerular pressure gradient that leads to hyperfiltration. 2. The ARNI molecule is a composite product of the ARB valsartan that works as reported above and of the sacubitril enzyme that cleaves metalloproteins that have catabolic action on the atrial natriuretic peptides. The cardiac atria generate those molecules for the specific purpose of providing rapid fluid unloading. Those molecules not only exert fast natriuretic action, but also induce the mesangial structure relaxation, allowing the filtration of a mild amount of albumin that can be detected in the urine. By being a physiology-related effect, the albumin leak does not impact HF outcome but correlates with the intraglomerular vascular resistance decrease. 3. The MRAs not only reduce the sodium reabsorption in the renal collecting tubule, but exerts a potent anti-inflammatory, anti-oxidation and anti-fibrotic action on the glomerular mesangial structure, shielding the delicate sieve deputed to select plasma solutes that have to be preserved from filtration (i.e.,: albumin) and the amounts of electrolytes and molecules generating the filtrate. The MRAs contentive action over the filtration process importantly concurs to balance the intraglomerular filtration pressure. 4. In the early segment of the glomerular tubule, the SGLT2 is primarily involved in the reabsorption of filtered glucose, a pivotal body nutrient, coupling one glucose molecule with one atom of sodium. The SGLT2 contemporary combines the largest sodium reabsorption in the kidney through the intertwined action of NHE3, located in the apical membrane of the proximal tubule section. The contemporary sodium reuptake is not trivial since the sodium is the electrolyte that provides the electrical gradient to the cell membrane as the energy source for biological needs. On the basis of renal physiology, any condition entailing the rise of filtrate production results in an immediate increase of SGLT2 expression coupled with the activity of NHE3. The combined action largely impoverishes the sodium content in the filtrate. The low sodium concentration by reaching the juxtaglomerular apparatus affects the production of adenosine, the eutakoid deputed to interact with the specialized receptor in the afferent arteriole to raise the vessel muscular tone, leading to the restraint of the vessel section, taping down the intraglomerular pressure. On top of this the adenosine concentration provides braking action of renin production in the juxtaglomerular apparatus. The SGLT2 inhibitors affect the disproportioned glucose reabsorption in the proximal tubule, which can put under control the largest intrarenal asset of mechanisms involved in sodium retention and neurohormonal activation. (see text for details).
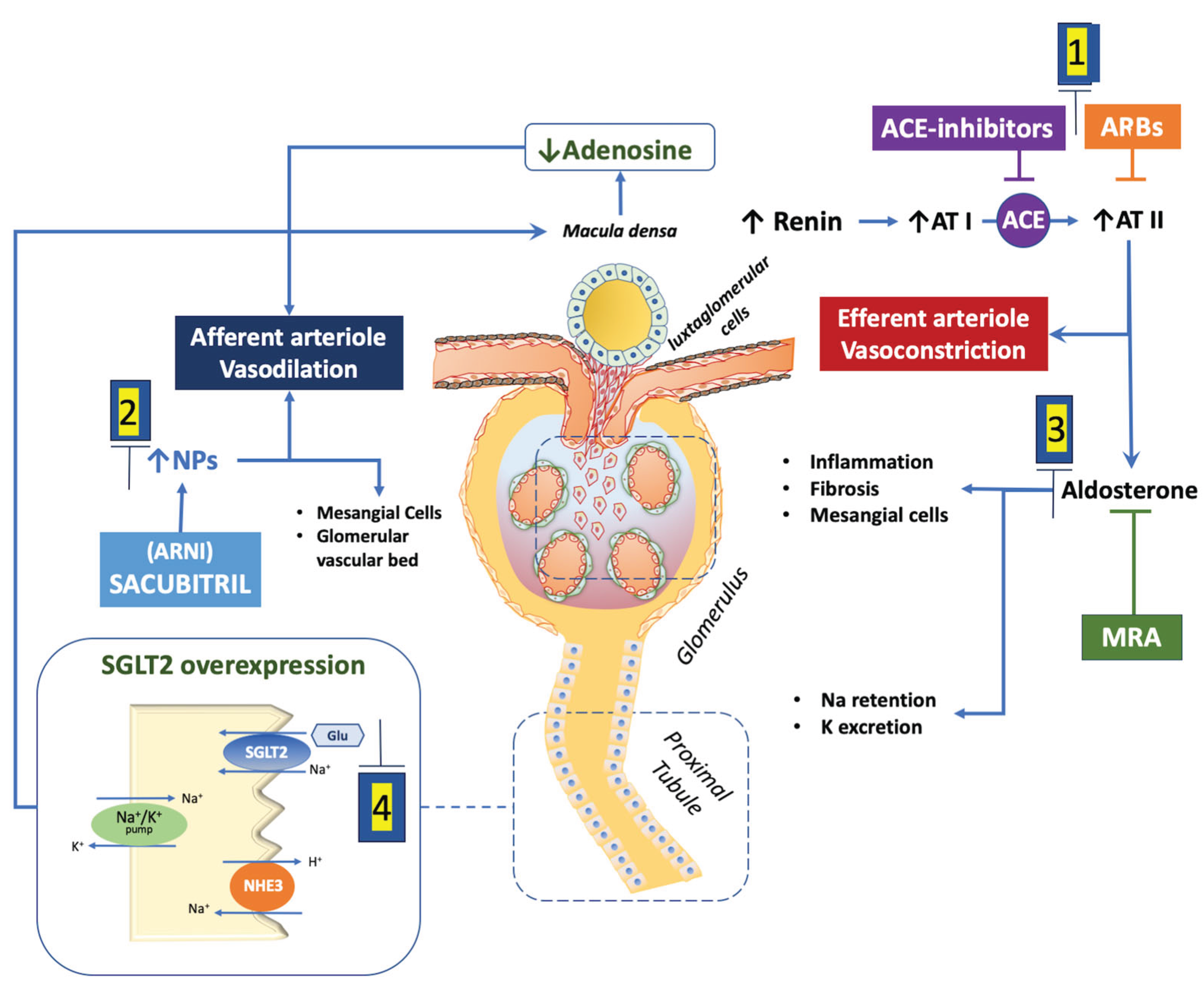
Table 1.
Effect on glomerular filtration rate and cardiovascular outcome in main studies performed with inhibitors of renin angiotensin system.
Table 1.
Effect on glomerular filtration rate and cardiovascular outcome in main studies performed with inhibitors of renin angiotensin system.
| Study | Population characteristics | Mean eGFR* |
Mean early renal function changes in treated arm vs. control arm |
|---|---|---|---|
| SOLVD Treatment and Prevention (cumulative): Enalapril vs. placebo [5] |
Number: 6245, Age: 59±10 years, LVEF: <35% | Treatment: 69.5±19 Prevention: 76.2±18 |
Treatment: -27.3(-33-21) Prevention: -12,8 (-17.4-8.4) |
| CHARM program Candesartan v. placebo [20] |
Number: 2405, Age: 65±12 years, Males: 68%, Diabetes: 38%, Mean LVEF 39 % | 71 ± 27 | Creatinine increase>25% at 6 weeks 16% vs. 25% |
| PARADIGM HF Sacubiril/valsartan vs Enalapril [32] |
Number: 8,096, Age: 64±11 years, Males: 78%, Diabetes: 35%, LVEF: 31% | 68 ± 19 | Run-in GFR decline >15% in 11% of patients. |
| PARAGON-HF Sacubiril/valsartan vs Enalapril [32] |
Number: 4665, Age: 73±8 years, Males: 52%, Diabetes: 43%, LVEF: 58% | 63±19 | Run-in GFR decline >15% in 10% of patients |
|
Mean chronic renal function changes in treated arm vs. control |
Cardiovascular outcomes | ||
| SOLVD Treatment and Prevention (cumulative): Enalapril vs. placebo [5] |
Treatment -27.3(-33-21) Prevention -12,8 (-17.4-8.4) |
Mortality in placebo vs. enalapril group: - CKD patients: 45% vs. 42% (HR, 0.88; CI, 0.73-1.06; p=0.164) - non CKD patients: 36% vs. 31% (HR, 0.82; 95% CI, 0.69-0.98; p=0.028) |
|
| CHARM program Candesartan v. placebo [20] |
Creatinine increase>25% at 6 weeks 16% vs. 25% |
Candesartan reduced both sudden death (HR 0.85 [0.73 to 0.99], P=0.036) and death from worsening HF | |
| PARADIGM HF Sacubiril/valsartan vs Enalapril [32] |
Run-in GFR decline >15% in 11% of patients. |
CV death/hHF: - Enalapril vs.sacubitril/valsartan in no GFR decline: 13.08 (95%CI: 12.27-13.96) vs. 10.46 (95%CI: 9.74-11.23) events/100 person years (HR: 0.79; 95%CI: 0.72-0.87)) - Enalapril vs.sacubitril/valsartan in GFR decline: 14.24 (95%CI: 11.93-17.08) vs. 9.70 (95%CI 7.93-11.96) events/100 person years (HR: 0.78; 95%CI: 0.61-1.01) |
|
| PARAGON-HF Sacubiril/valsartan vs Enalapril [32] |
Run-in GFR decline >15% in 10% of patients |
CV death/hHF: - Valsartan vs.sacubitril/valsartan in no GFR decline: 14.11 (95%CI:12.58-15.88) vs. 12.43 (95%CI: 11.12-13.93) events per 100 person years (HR 0.87; 95%CI: 0.74-1.03) - Valsartan vs.sacubitril/valsartan in GFR decline: 17.27 (13.59-22.27) vs. 15.16 (11.56-20.24) events per 100 person years (HR: 0.84; 95%CI: 0.58-1.20) |
|
*expressed as ml/min*1,73m2. Abbreviations: ARB angiotensin receptor blocker, ACEi angiotensin converting enzyme inhibitor; ARNI: Angiotensin II receptor Neprylisin inhibitors; CHARM: Candesartan in chronic heart failure CI: Confidence Interval; CKD: chronic kidney disease; CV cardiovascular, hHF heart failure hospitalization. GFR: estimated glomerular filtration rate; HR: Hazard Raio; LCZ696 sacubitril/valsartan (ARNI), RASi renin angiotensin system inhibitors, eGFR estimated glomerular filtration rate, LVEF: left ventricular ejection fraction; PARADIGM-HF: Efficacy and safety of LCZ696 compared to enalapril on morbidity and mortality of patients with chronic heart failure; PARAGON-HF: Prospective Comparison of ARNI with ACE inhibition to Determine Impact on Global Mortality and Morbidity in Heart Failure; SD: standard deviation; SOLVD: Effect of enalapril on survival in patients with reduced left ventricular ejection fraction.
Table 4.
Effect on glomerular filtration rate and cardiovascular outcome in main studies performed with inhibitors of type 2 sodium-glucose cotrasporter.
Table 4.
Effect on glomerular filtration rate and cardiovascular outcome in main studies performed with inhibitors of type 2 sodium-glucose cotrasporter.
| Study | Population characteristics | Mean early GFR* changes in treated arm vs. control arm |
Mean chronic GFR* changes in treated arm vs. control |
Cardiovascular outcomes |
|---|---|---|---|---|
| DAPA-HF Dapagliflozin vs. Placebo [59] |
Number: 4618 Age: 66 ± 11 years Males: 77% Diabetes: 42% LVEF: 31% Median eGFR*: 66 |
-4.19 (95%CI: -4.52/-3.87) vs. -1.09 (95%CI: -1.42/-0.77) | -1.09 (95%CI: 1.40 / -0.77) vs. - 2.85 (95%CI: -3.17 / -2.53) | CV death /hHF: 11.4 vs 15,6 per 100 pts/year (HR: 0.78; 95% CI: 0.61-1.00) |
| EMPEROR-R Empagliflozin vs. Placebo [61] |
Number: 3547 Age: 67 ± 11 years Males:76% Diabetes: 50% LVEF: 27% Mean eGFR*: 62±22 |
-3.5 (95%CI: -3.1/-3.9) vs. -1.0 (95%CI: -0,6/-1.4) |
-0.55 ±0.23 (SD) vs. -2.28±0.23(SD) |
CV death /hHF: 15.8 vs 21 per 100 pts/year (HR: 0.75; 95%CI: 0.65 0.86) |
| EMPEROR-P Empagliflozin vs. Placebo [62] |
Number: 5836 Age: 72 ± 9 years Males: 65% Diabetes: 49% LVEF: 54% Mean eGFR*: 61±20 |
−3.7 (95%CI: −4.0 / −3.4) vs. −0.5 (95%CI: −0.8 to−0.2) |
−1.25 ± 0.11(SD) vs. −2.62 ± 0.11(SD) |
CV death /hHF: 6,9 vs 8,7 per 100 pts/year (HR: 0.79; 95%CI: 0.69- 0.90) |
| DELIVER Dapagliflozin vs. Placebo [60] |
Number: 6262 Age: 72 ± 10 years Males 56% Diabetes: 45% LVEF: 54% Mean eGFR*: 61 ± 19 |
-3.7 (95%CI: -4.0/-3.3) vs. -0.4 (95%CI: -0,8/-0.0) |
-0.5(95%CI: −0.1 / -0.9) vs. −1.4 (95%CI: −1.0 / −1.8) |
CV death /hHF: 11,8 vs 15,4 per 100 pts/year (HR: 0.77; 95%CI: 0,67- 0,78) |
*expressed as ml/min*1,73m2. CI: Confidence Interval; CV cardiovascular; DAPA-HF: Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure; DELIVER: Dapagliflozin Evaluation to Improve the LIVEs of Patients With Preserved Ejection Fraction Heart Failure; EMPEROR-P: Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Preserved Ejection Fraction trials; EMPEROR-R: Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction; , hHF heart failure hospitalization. GFR: estimated glomerular filtration rate; HR: Hazard Ratio; LVEF: left ventricular ejection fraction. SGLT2i: inhibitors of type 2 sodium-glucose cotrasporter.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



