
Submitted:
01 September 2025
Posted:
03 September 2025
You are already at the latest version
Abstract
According to the CDC’s National Center for Health Statistics, type 2 diabetes mellitus (T2DM) remains a major public health issue with a considerable impact on human life, affecting over 38 million Americans of all ages, and an estimated 529 million people worldwide. It is a significant risk factor for polyneuropathy, eye problems, coronary artery disease (CAD), renal disease, heart disease, stroke, and peripheral artery disease (PAD). Nearly 9 million Americans with diabetes are unaware of their condition and, therefore, do not receive health care to prevent disease progression and complications. With T2DM being a condition that leads to increased demand for healthcare services due to its long-term, persistent nature and its incremental impact on the body, making early diagnosis and timely initiation of effective treatments essential. Despite the effect of metabolic memory in the development of diabetes-related complications, early in-tervention helps to decelerate disease progression, reduce complications, and ulti-mately improve survival. During the past few decades, various blood-based bi-omarkers have been identified, which hold great promise to streamline the mecha-nisms underlying T2DM and its progression from insulin resistance and prediabetes to diabetes and end-stage diabetes. However, the greatest need is to identify and utilize reliable biomarkers that can help to assess pharmacological treatment response and guide efforts to improve insulin sensitivity, preserve pancreatic beta-cell function, and prevent or delay complications. In this review, we explore the clinical utility of prom-ising biomarkers and assess their potential to support more personalized pharmaco-logical approaches tailored to the individual characteristics of T2DM patients.
Keywords:
antihyperglycemic agents
; microvascular disease
; macrovascular disease
; predictive biomarkers of T2DM
; diabetes complications
; neovasculogenesis
; atherosclerosis
1. Introduction
The recent International Diabetes Federation (IDF) Atlas (2025) estimates that 1 in 9 adults aged 20–79 is affected by diabetes, with nearly 4 in 10 individuals unaware that they have the condition [1]. T2DM is the 8th leading cause of preventable death and disability worldwide and is a major global risk factor for cardiovascular diseases [2]. It is estimated that T2DM accounts for nearly 90% of the global burden of diabetes and can increase the risk of kidney disease [3], hypertension [4], heart disease [5], vasculopathy [6], and neuropathy [7], often with devastating consequences. According to a report by the World Health Organization (WHO), diabetes and kidney disease are responsible for at least 2 million deaths due to diabetes [8]. Evidence indicates that diabetic patients are nearly twice as likely to have a stroke compared to adults without diabetes [9].
The diagnosis of T2DM is based on current classification criteria, including consistent fasting blood glucose levels greater than 130 mg/dL, glycated hemoglobin A1c (HbA1c) greater than 7% (an average blood glucose level of 154 mg/dL), and lifestyle assessment. Blood glucose levels vary considerably and tend to increase with age. The risk of microvascular and macrovascular complications rises with uncontrolled hyperglycemia [10]. Many neuroendocrine factors are involved in blood glucose regulation, including activation of the sympathetic and parasympathetic nervous systems, pancreatic hormones (insulin and glucagon secretion), hepatic processes (glycogenolysis, gluconeogenesis, glycogenesis), and lipolysis in adipose tissue [11]. Key organs involved in glucose homeostasis include the liver, pancreas, and gastrointestinal tract.
Approximately 90% of patients with hyperosmolar hyperglycemic state (HHS) have a known diagnosis of T2DM [12]. These patients are considered to have decompensated diabetes [13]. Hyperglycemic crises can result from increased gluconeogenesis, elevated glycogenolysis, and decreased glucose uptake in tissues such as the liver, muscles, and fat. These distinct metabolic disruptions can lead to glucosuria, elevated serum osmolality [14], dehydration, impaired renal function [15], and a prothrombotic state [16,17]. HHS is a major cause of morbidity and mortality [18], with contributing factors including severe dehydration, advanced age, and the presence of comorbidities [19].
Many medications can have severe undesirable effects, and prescription antihyperglycemic drugs are no exception. For instance, SGLT2 inhibitor-induced glucosuria is associated with osmotic diuresis, lower limb amputation, and diabetic ketoacidosis (due to insulin deficiency), which can lead to diabetic coma or even death. Therefore, to ensure that T2DM patients receiving antihyperglycemic medications achieve maximum therapeutic benefit, effective biomarkers should be used to guide clinical evaluation. This would not only improve patient care but also help identify individuals at greatest risk for drug-induced tissue damage.
In order to identify biomarkers a search is performed using PubMed, Science Direct, Google, and Google Scholar in tandem to cover the most thorough results. Both Google and Google Scholar are used because of their broad search capabilities for locating various document types: conference papers, patents, government reports and statistics [20,21]. The major keywords used to perform the search are the following: “imaging and circulating biomarkers”, “established biomarkers in diabetes/chronic diseases”, “pharmacodynamic biomarker”, “monitoring biomarkers in diabetes”, “predictive biomarkers in diabetes”, and “safety biomarkers”.
Therefore, in this review, we examine the applicability of various blood biomarkers studied for their potential to identify and explore the effectiveness, safety, and clinical endpoints of medical treatments in patients with T2DM. A schematic representation of the topics covered in this review is shown in Figure 1.
2. Biomarkers Help Monitor Responses to Medications
Potential biomarkers for the risk of diabetes are classified into two categories: genetic and nongenetic [22]. Biomarkers are measurable characteristics found in various biological compartments (blood, fluids, and tissues) in patients, and their diagnostic spectrums differ. While some circulating biomarkers serve as early indicators of improved outcomes and opportunities to optimize dosing in specific populations with diabetes, only a few meet clinical requirements. Abnormal elevation of key biomarkers that signal diabetes may also play a harmful mediating role in type 2 diabetes mellitus (T2DM) and associated cardiovascular risk factors.
Different countries take diverse approaches to diabetes care. However, clinical endpoints meaningful to both clinicians and patients − such as health and well-being − remain essential [23]. Although many biomarkers have been identified over the years, only some consistently predict relevant clinical outcomes in diabetes treatment across different ethnic groups.
Therefore, in this review, we examine the applicability of various blood biomarkers studied for their potential to identify and evaluate the effectiveness, safety, and clinical endpoints of medical treatments in patients with T2DM. A schematic representation of the topics covered in this review is shown in Figure 1.
3. Emerging Theories of the Pathophysiology of T2DM
Precision T2DM is an emerging field focused on improving the diagnosis, prognosis, and management of T2DM-related conditions by providing personalized and precise treatments that enhance individual clinical outcomes. It is well known that patients with T2DM may respond differently to the same treatment due to genetic variations and environmental factors. Precision T2DM has its conceptual roots in several scientific fields, including genomics, proteomics, molecular profiling, physiology, environmental factor analysis (via statistical methods), lifestyle, and big data analysis. Here, we briefly discuss the application of this translational paradigm, dating back to the mid-1960s and emphasize the need to identify new predictive biomarkers that reflect disease progression or treatment efficacy.
While the WHO has published guidelines for the diagnosis and classification of diabetes since 1965 [24], it established the first international guidelines for the management of diabetes in 1980. The American Diabetes Association (ADA) published its first Standards of Care in Diabetes clinical practice guidelines a few years later [25]. In defining diabetes, these guidelines have taken two approaches: either basing their definition on a specific threshold for initiating pharmacological treatment or on blood glucose levels above which the risk of complications increases.
The US, Asian, and European guidelines focus on lifestyle changes and have chosen a cut-off level of fasting plasma glucose above which the benefits of treatment, as reported by interventional clinical trials of blood glucose-lowering therapy, are considered to outweigh the harms. However, a thorough risk-benefit evaluation in older adults with T2DM should be performed to assess the potential advantages and disadvantages of treatments, due to the U-shaped relationship between HbA1c and the risk of mortality [26]. Using this approach, the cut-off point that defines diabetes is glycated hemoglobin (HbA1c) <7%, using standard clinical methods of measurement [27].
Traditionally, T2DM is characterized by a gradual decline in insulin secretion from the pancreas, against a background of insulin resistance. Recently, modifications have been made regarding the diagnosis of impaired fasting glucose [28]. This study emphasizes the range of severity in T2DM by stratifying patients into five subgroups with differing disease progression and risks of diabetes complications (Figure 2). The classification includes five clinical subgroups:
- Subtype 1 – Severe autoimmune diabetes mellitus
- Subtype 2 – Severe insulin-deficient diabetes mellitus
- Subtype 3 – Severe insulin-resistant diabetes mellitus
- Subtype 4 – Mild obesity-related diabetes
- Subtype 5 – Mild age-related diabetes
Severe autoimmune diabetes mellitus (Subtype 1) and severe insulin-deficient diabetes mellitus (Subtype 2) are the least common subtypes, representing 6–14% and 9–15% of the study cohorts, respectively [28]. While individuals in Subtype 1 are positive for autoimmune response, those in Subtype 2 exhibit inadequate insulin production. Both subtypes share characteristics similar to type 1 diabetes mellitus, including lower body mass index, higher rates of diabetic ketoacidosis, and faster progression to insulin therapy.
Individuals with severe insulin-resistant diabetes mellitus (Subtype 3), characterized by insulin resistance, represented 11–17% of the study cohorts. They had a higher risk of progression to chronic kidney disease and were prone to increased risk for coronary events.
Mild obesity-related diabetes (Subtype 4) and mild age-related diabetes (Subtype 5) are the most common subtypes, representing 18–23% and 34–47% of the study cohorts, respectively. Individuals in these two subtypes tend to experience metabolic derangement [29]. This suggests that individual metabolites and a metabolomic network are significantly associated with T2DM in these two cohorts.
The findings of this study change the definition of T2DM by emphasizing its heterogeneity. This suggests that to effectively manage T2DM subgroups, a new approach is essential—one that emphasizes a comprehensive understanding of biomarkers and targeted interventions to optimize care.
A link between glycemic control and diabetes complications was initially recognized in the late 1980s [30,31,32]. The benefit of lowering blood glucose to prevent diabetes-related complications and reduce cardiovascular events and mortality is unequivocal in patients with substantial elevations in blood glucose levels. Over two decades ago, the Diabetes Control and Complications Trial (DCCT) [33] on patients with type 1 diabetes and the United Kingdom Prospective Diabetes Study (UKPDS) [34] on patients with T2DM reported that maintaining optimal HbA1c levels, an indicator of mean glycemia, helps prevent disease progression and is crucial for reducing the risk of macrovascular and microvascular complications.
The first randomized controlled interventional study of anti-diabetes therapy in patients with elevated blood glucose levels is shown in the DCCT report. Subsequent studies, which have mostly used measures of clinic blood glucose levels, have shown the benefit of glucose-lowering therapy when HbA1c is above 7% in all patients up to age 80 years [35,36,37], with a caveat: severe hypoglycemia is a frequent event in the elderly population, and increased mortality risk becomes apparent among those with HbA1c values of 6.4% [38].
The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial elegantly demonstrated the benefits and risks of intensive glucose control, intensive blood pressure control, and lipid management in high-risk patients with T2DM [39]. The ACCORD trial showed the highest burden of excess deaths at both extremes of HbA1c compared to the average HbA1c level for adults with diabetes. HbA1c can be highly variable within an individual and is not well characterized from a single or limited number of measurements. Moreover, HbA1c levels vary disproportionately in certain groups of patients with T1DM [40,41] and T2DM [41,42,43].
Thus, recent guidelines have redefined hyperglycemia based on the degree of HbA1c associated with increased cardiovascular risk. They recommend individualization of HbA1c targets to reduce the risk of cardiovascular events [44,45]. While HbA1c is considered efficient in assessing the prevalence of pre-diabetes and undiagnosed diabetes [46], and a reliable marker for assessing long-term blood glucose control, it is influenced by numerous factors, including population differences, hemoglobin variants, anemia, and other medical conditions.
Studies also suggest that T2DM is a broad term encompassing a complex range of conditions that affect blood glucose regulation [5] (Figure 2). Since individual treatment decisions are more complex than a definition, new biomarkers and targeted interventions are essential for advancing treatment strategies in patients with T2DM and in critically ill diabetic patients.
4. Prescription Antihyperglycemic Drugs
4.1. Current Landscape of Oral Antihyperglycemic Drugs in T2DM Management
This section addresses a practical review of the available evidence on the different benefits of oral antihyperglycemic agents beyond their blood glucose-lowering effect, with an emphasis on the differences found between the biomarkers associated with different classes of drugs and the biological pathways they influence, with specific reference to the co-morbidities and anti-atherogenic mechanisms (Table 1). We also summarize the available data and information on risks of antidiabetic medications that can range from mild to severe reactions and occasionally pose life-threatening risks. Moreover, we focus on potential biomarkers, as indispensable tools, for antidiabetic medication associated risk that hold increasingly important roles in drug development, prediction of treatment response, and improving patient outcomes.
T2DM remains a major global health challenge. Although there have been significant advancements in research and technology in diabetes management, nonetheless it remains a major preventable death and morbidity risk factor. If not diagnosed early and managed properly, diabetes can be associated with several complications such as renal failure, heart failure (HF), hepatic dysfunction, metabolic disorders, loss of vision, and vascular complications. Reducing blood glucose using lifestyle modifications and/or antihyperglycemic drugs can significantly decrease the risk of cardiovascular morbidity, retinal and renal dysfunction as well as premature mortality.
The metabolic hormones play an important role in the pathophysiology of hyperglycemia and is closely related with cardio- and cerebrovascular events and chronic kidney diseases [89,90]. Each oral antihyperglycemic agent is important in the treatment of patients with T2DM, according to the results of glycemic control over the recent years.
HbA1c levels-is crucial to diabetes management, as persistent hyperglycemia not only promotes advanced glycation end-product (AGE) formation, but also it induces oxidative stress and chronic low-grade inflammation, the two major factors involved in vascular complications [17]. The longitudinal HbA1c trends in patients with diabetes exhibits unstable patterns that include increasing HbA1c, decreasing HbA1c, and non-linear behavior [91,92]. It appears to be associated with numerous factors such as age, gender, ethnicity, diabetes duration, disease management frequency, cardiovascular risk factors, and family environment [93]. For instance, diabetic patients with T2DM who maintain mean HbA1c between 6% − 8% can significantly lower the risk of major cardiovascular events [94]. Tilting HbA1c levels of high-risk patients to values lower than 7% or values higher than 8% can lead to worst overall outcomes for the patients, indicating the presence of intricate systems, each governed by a delicate balance of hormones.
Although oral antihyperglycemic drugs are available, it remains suboptimal within various populations in terms of glucose/HbA1c control and prognosis. A systemic review supports the notion that poor glycemic control remains a significant concern in T2DM management, contributing to increased risks of complications and healthcare burdens globally [95]. Despite the availability of oral antihyperglycemic agents, evidence-based recommendations endorsed by several guidelines as mentioned earlier, and HbA1c control, 50% to 70% of people with T2DM globally fail to achieve recommended HbA1c targets [95]. Thus, it is essential to consider and apply potential novel biomarkers to provide information on disease risk, prediction of response to ease therapeutic decision making and improve diabetic patients’ clinical outcomes.
While many studies have been conducted to deepen our understanding of the pathophysiology of T2DM and the effectiveness of antidiabetic medications, there is need to synthesize this available evidence to acquire an aggregate and holistic picture of the impacts of current antihyperglycemic agents on the pathophysiology of T2DM. Antihyperglycemic agents are being characterized by complex physiological changes that are reflected in biomarker alterations detectable in blood, in urine, or with cardiovascular imaging. As shown in Table 1, each class of antihyperglycemic agent exerts its therapeutic benefits through a specific pathway and a mechanism of action (s), and an example of a drug in each class. While all antihyperglycemic medications offer similar therapeutic efficacy and safety and their risks on intracellular signaling processes may be informative across multiple drug classes, some of them cause risks that are due to their unique effect or insufficient research on their effects (Figure 3). Identification of these risks associated with each drug not only provides a powerful method for dose-to-function analysis but also may point out to yet uncharacterized metabolic pathway, offering deeper insights from antihyperglycemic medication-cell perturbation interaction. It is feasible to propose that collection of antihyperglycemic medications’ risks can serve as early biomarkers to predict physiological response to previously untested drug that would benefit the discovery of combination therapies in diabetes or sensitive populations including children, pregnant women, and the high-risk patients.
4.2. Mechanisms of Action, Benefits, and Risks of Oral Antihyperglycemics
4.2.1. Metformin
Several recent large randomized controlled trials have significantly improved our knowledge about the impact of medications for T2DM on patient-oriented clinical endpoints. The current pharmacotherapy options are mainly evaluated based on safety, tolerability, effectiveness, and prevention of diabetes-induced complications. The first-line treatment option, metformin, is safe and fairly well-tolerated, has excellent long-term effectiveness (Table 1). It reduces glucose production in the liver (gluconeogenesis) and improves insulin sensitivity in peripheral tissues. Metformin produces both AMP-activated kinase (AMPK) dependent and independent effects [96]. It offers potential benefits against heart failure, neuropathy, and retinopathy, and remains safe [96]. However, meta-analyses cast a shadow on the effectiveness of metformin in reducing the risk of adverse cardiovascular outcomes [97]. While metformin-induced lactic acidosis is a rare event that occurs in patients with eGFR less than 30 ml/min/1.73m2 [98,99], it is associated with serious conditions such as hypotension and resistant bradyarrhythmia. In some cases, metformin is reported to cause changes in vitamin B12, blood coagulation system, hepatotoxicity, and acute pancreatitis [54] . Interestingly, altered secretion of growth factors, reduced anabolic pathways, and activated metabolic stress pathways are demonstrated in fetal hepatocytes [100]. A meta-analysis shows that neonates exposed to metformin exhibit significantly lower birthweight [101,102]. The FDA has not removed the acute or unstable congestive heart failure from the warning labels on metformin therapies used to treat T2DM. It is contraindicated in patients with severe renal impairment due to associated cardiovascular concerns [103].
4.2.2. Sulfonylureas
Sulfonylureas have the capability to lower blood glucose levels [104] and are associated with the reduced risk of diabetic retinopathy [105], indicating a beneficial microvascular effect. Their effects are primarily due to stimulating insulin secretion and suppressing hepatic glucose output [106], leading to a reduction in the glycation of hemoglobin A1c. Effective elevation of insulin sensitivity is reported at peripheral target sites [107]. While hypoglycemia is associated with the first-generation and second-generation sulfonylureas due to their ability to bind to the blood’s carrier proteins, glimepiride (the third-generation sulfonylureas) poses a lower risk of hypoglycemia due to reduced protein binding. WHO, International Diabetes Federation (IDF) recommend sulfonylureas after metformin or in combination with drugs such as SGLT2 inhibitors or DPP4 inhibitors [108]. However, they fails to stimulate the release of insulin in individuals with certain mutations in the KCNJ11 gene [93].
A well-designed study shows that incidences of microvascular complications are higher in patients treated with sulfonylurea compared with the vildagliptin (a dipeptidyl peptidase-4 inhibitor) study arm [109]. Sulfonylureas have been associated with an increased risk of cardiovascular events and mortality [110], including myocardial infarction [58], ventricular arrhythmias and sudden cardiac death [111], though others report no such association [112].
4.2.3. Meglitinide
Postprandial glucose has been recognized as a greater risk factor for cardiovascular disease than fasting plasma glucose for over two decades [113,114]. Meglitinides are one of the commonly prescribed class of anti-hyperglycemic agents that trigger pancreatic beta cells to release insulin [115] to target postprandial glucose excursions [114]. Thus, repaglinide is a prandial glucose regulator. The release of insulin is due to the inhibition of the adenosine triphosphate (ATP)-dependent potassium channels that depolarize beta cells [116,117].
Repaglinide, a meglitinide, decreases HbA1c by 0.7% in patients with T2DM [118]. Repaglinide improves homocysteine, plasma activator inhibitor, and lipoprotein (a) [119]. Improved glucose metabolism is recognized as a major driving force in reducing these metabolic parameters. Repaglinide is inactivated in the liver and primarily excreted via the bile, and as such, its excretion is not affected by renal disorders. This class of drug is a safe antidiabetic agent for the elderly [120] and renally impaired patients [115]. Patients who cannot tolerate metformin can switch to repaglinide. Repaglinide in combination with sitagliptin, a dipeptidyl peptidase-4 inhibitor, has been found to be effective without any clinical safety issues in diabetic patients [121]. However, it has been linked to increased cardiovascular event risk [122], including coronary heart disease, ischemic heart disease [123]. Unlike metformin, repaglinide might lead to an increased risk of adverse cardiovascular events in a Danish nation-wide registry-based observational analysis [119].
4.2.4. Thiazolidinedione
The TZDs amongst the therapeutic options in the treatment of hyperglycemia have been recognized as a new milestone in the history of diabetes treatment prior to the discovery of DPP4-inhibitors, SGLT2 inhibitors, and GLP-1R inhibitors. Pioglitazone, a TZDs, directly improves insulin sensitivity [124], has an effective HbA1C-lowering property [64], provides durable glycemic effects, and carries a low risk of hypoglycemia [125]. Pioglitazone has demonstrated benefit in patients with atherosclerotic cardiovascular disease and stroke risk [126,127,128]. Pioglitazone can effectively serve as a valuable second-line agent with unique cardiovascular advantages [126].
4.2.5. Dipeptidyl Peptidase-4 (DPP-4) Inhibitors
DPP-4, an endogenous aminopeptidase enzyme, metabolizes incretin hormones, resulting in decreased insulin secretion. DPP-4 exists in two isoforms [129]. One is free in the plasma and the other is anchored in the membrane of numerous cell types, including endothelial cells, T cells, and kidney tubular cells [130]. While the circulating DPP-4 is responsible for the metabolism of circulating GLP-1, it appears that the membrane bound DPP-4 involves in the cleavage of several substrates, including pronatriuretic brain peptide, Y-neuropeptide, stromal derived factor alpha as well [131].
The two incretin hormones, namely glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are involved in the pathophysiology of both obesity and T2DM. The elevated concentrations of incretin hormones lead to increased insulin secretion, decreased in glucagon, and reduction in the production of glucose in the liver [132]. GLP-1 and GIP exert insulinotropic and glucagonostatic effects [133] via the GLP-1 receptor – and GIP receptor -mediated stimulation, thus ensuring optimal maintenance of plasma glucose levels. While the biological effectiveness of GIP is significantly reduced in inducing insulin secretion by pancreatic β-cells in T2DM patients, the insulinotropic and glucagonostatic effects of GLP-1 are maintained in unaltered condition in these patients [132].
Evidence has confirmed a prominent role of DPP-4 in the pathophysiology of T2DM [134]. Inhibitors of DPP-4 are capable of manipulating a range of interrelated biochemical pathways to decrease glucagon, postprandial glucose levels, promote satiety, and improve glycemic control [66]. The role of DPP-4 inhibitors in delaying gastric emptying remains a point of debate among researchers with varying evidence supporting different perspectives [66,135]. Clinical studies further provide evidence that DPP-4 inhibitors could exert both anti-inflammatory and immunomodulatory effects [67] and exhibit protective effects in renal disease progression [68,69].
Notably, a recent data mining of the public version of the FDA Adverse Event Reporting System (FAERS) indicates that sitagliptin, saxagliptin, linagliptin, vildagliptin (not approved by the FDA) are disproportionally associated with gastrointestinal nonspecific inflammation and dysfunctional conditions, pancreas, musculoskeletal disorders [70] and upper respiratory infection [71]. A meta-analysis of cardiovascular outcome trials provides supporting evidence that DPP-4 inhibitors are a significant risk factor for atrial flutter [72]. Saxagliptin has repeatedly been shown to be associated with an increased rate of hospitalization for heart failure [136,137], although this association remains debated due to insufficient number of large-scale trials [138] or selection of diabetic patients with incomparable CV risk category, which is not in accord with the 2019ESC-EASD guidelines (very high risk, high risk, moderate risk) [139].
4.2.6. Glucagon-Like Peptide-1 (GLP-1) Agonist
GLP-1-induced GLP-1R activation leads to a complex intracellular signaling cascade, which at the end activates protein kinase A (PKA) pathway via production of cyclic adenosine monophosphate (cAMP) [140]. They are associated with weight loss and a low risk of hypoglycemia.
GLP-1 agonists are recognized as neuroprotective and cardioprotective agents by reducing inflammation, stimulating nerve growth and affecting lipid metabolism [141]. GLP-1 is capable of lowering glucose through multiple mechanisms including insulin release stimulation and suppression of glucagon secretion [142]. Thus, GLP-1 agonists offer cardioprotective and neuroprotective effects. Recently, a systematic review and meta-analysis of randomized clinical trials reports that semaglutide may elevate the risk of diabetic retinopathy [143], suggesting this medication might worsen the patients’ microvascular complication.
4.2.7. Sodium-Glucose Co-Transporter-2 Inhibitors
Sodium-glucose co-transporter-2 (SGLT2) inhibitors reduce blood glucose by increasing urinary glucose excretion [142] and improve cardiovascular and renal outcomes, especially in patients with high cardiovascular risk, as demonstrated in EMPA-REG OUTCOME and other trials [80,144]. SGLT2 [145] inhibitors, also known as gliflozins, reduce HbA1c by 0.5–1.0%, enhance insulin sensitivity, and exhibit pleiotropic benefits, including diverse cardiovascular- and kidney- protective effects [145,146,147]. SGLT2 inhibitors are shown to lower hyperuricemia, epicardial fat mass, as well as oxidative stress [144]. They also promote autophagy and lysosomal degradation, and contribute to the elevation of erythropoietin levels via SIRT1-dependent mechanisms [148], circulating pro-vascular progenitor cells [149], and improving vascular function.
In summary, Oral antihyperglycemic agents differ significantly in their mechanisms of action, safety profiles, and systemic effects. While metformin remains the first-line therapy, other agents offer complementary benefits and risks that must be considered in individualized care. The integration of novel biomarkers into clinical practice may refine risk assessment and guide therapeutic choices, especially in patients with comorbidities or organ dysfunction. It is essential to monitor renal function and adjust drug dosing accordingly, and to recognize that overly aggressive glycemic control may be detrimental in specific patient populations. A broader HbA1c target range may be more appropriate in elderly individuals or those with advanced renal or cardiovascular complications.
5. Emerging Biomarkers in T2DM
While growing evidence supports the utility of biomarkers in improving diabetes diagnosis, the prognostic value of only a few biomarkers appears to influence therapy, and current guidelines do not recommend their routine measurement for risk stratification or to assess the comparative effectiveness of dosing and combination therapies in people with T2DM. A recent systematic review indicates that changes in hematological protein, cytokine, and lipid profiles are evident in T2DM patients [150].
Markers of Chronic or Low-Grade Inflammation
In T2DM, obesity-induced macrophage infiltration causes low-grade inflammation, leading to the release of proinflammatory mediators [151]. Interleukin-6 (IL-6) is produced by activated leukocytes, endothelial cells, and adipocytes [152], whereas C-reactive protein (CRP), an acute-phase plasma protein, is synthesized by the liver and released into the bloodstream in response to IL-6 exposure [153]. CRP exists in two isoforms with opposing actions: native pentameric (pCRP), an anti-inflammatory form, and monomeric (mCRP), a proinflammatory form [154,155]. mCRP has been found to cause platelet activation [156,157], leukocyte recruitment [156], and endothelial dysfunction [158], all of which are implicated in the pathogenesis of various diseases, including diabetes. IL-6 and monomeric CRP, two of the most commonly assayed inflammatory biomarkers, are used to refine diabetes risk prediction. IL-6 primarily reflects the severity of inflammation, the link between inflammation and diabetes, and the prevalence of associated diabetic complications.
However, CRP levels may be elevated due to various conditions, including both acute and chronic responses to infection, noninfectious triggers, or factors such as moderate-to-vigorous physical activity and increased sedentary time [154]. Neither IL-6 nor CRP levels alone accurately reflect the diabetic patient’s response in terms of vascular health (e.g., atherosclerosis, insulin resistance), changes in hematological parameters, dyslipidemia, beta (β) cell responsiveness, cardiovascular disease (CVD), or variability in drug response. Notably, the impact of the IL-6 pathway on diabetes risk in the general population appears to be small [159]. Similarly, CRP is not considered an independent risk factor for T2DM [160]. However, CRP has shown a statistically significant association with a favorable effect of metformin in T2DM patients [161].
6. Vascular Complications Associated with T2DM
Hyperglycemia-induced vascular injury in type 2 diabetes mellitus (T2DM) is classified into two categories: microvascular and macrovascular complications (Figure 1). Individuals living with diabetic panvascular disease are markedly more susceptible to a broad spectrum of microvascular complications affecting organs such as the heart, brain, eyes, and kidneys. Moreover, they face an increasing risk of developing macrovascular complications. The macrovascular triad in diabetes encompassing coronary artery disease, cerebrovascular disease, and peripheral artery disease contributes substantially to morbidity and mortality. These widespread vascular impairments lead to poor circulation, a strong predictor of cardiovascular mortality, emphasizing the urgent need for early detection and precise prognostic tools. Biomarkers reflecting the presence and severity of vascular complications in diabetes have shown great promise in improving prognostic accuracy. This section will examine both microvascular and macrovascular complications of uncontrolled T2DM, with a particular focus on emerging biomarkers for the non-invasive diagnosis and treatment of diabetes.
6.1. Microvascular Complications
6.1.1. Retinopathy
Diabetic retinopathy, a common detrimental microvascular complication of diabetes, involves damage to the blood vessels within the retina [162]. It is a progressive condition that can worsen over time and lead to significant visual impairment or complete vision loss if not adequately treated [163]. Persistent long-term hyperglycemia contributes to the development of diabetic retinopathy by inducing morphological, structural, and functional changes in the small retinal blood vessels, a condition known as microangiopathy [164,165]. If left untreated, this damage can lead to various clinical manifestations.
Hyperglycemia is the main driver in the development of non-proliferative diabetic retinopathy (NPDR), which is characterized by microaneurysms, retinal hemorrhages, and retinal exudates [166]. It can progress to proliferative diabetic retinopathy (PDR), the most advanced stage of diabetic eye disease in T2DM, marked by the proliferation of abnormal new blood vessels on the surface of the retina [167]. This advanced stage poses a serious risk of significant visual impairment.
While genetic predisposition may influence an individual’s vulnerability to retinopathy [168], several risk factors including the duration of diabetes, poor glycemic control, hypertension, and dyslipidemia are also associated with the development and progression of diabetic retinopathy [169].
Potential Biomarker Options of Retinopathy
- Proangiogenic agents
Endothelial peroxisome proliferator-activated receptor γ coactivator (PGC1α)-mediated activation of estrogen-related receptor alpha (ERRα) under hypoxic conditions leads to the stimulation of angiogenic factor expression, which in turn triggers angiogenesis [170]. This signaling pathway also plays a significant role in regulating numerous genes involved in fatty acid metabolism and oxidative phosphorylation in the adult myocardium [171], as well as mitochondrial regulation [172]. Notably, this pathway has been identified as a promising therapeutic target in the treatment of diabetes [173], underscoring the pleiotropic nature of PGC1α. Interestingly, analysis of vitreous fluid samples from patients with proliferative diabetic retinopathy (PDR), non-diabetic individuals, and epiretinal fibrovascular membranes from PDR patients suggests that the PGC1α/ERRα pathway is suppressed in individuals with PDR [174].
Erythropoietin, a potent angiogenic factor induced by ischemia, appears at higher concentrations in the eyes of patients with diabetic macular edema compared to those with age-related macular degeneration (AMD) or non-diabetic individuals [175].
- Proinflammatory agents
Patients with diabetic retinopathy exhibit elevated serum levels of irisin and intercellular adhesion molecule-1 (ICAM-1) in the early stages of the disease, with levels decreasing in later stages [176]. These molecules may serve as potential biomarkers for the proliferative stage of diabetic retinopathy.
Another study explored the association between C-peptide (CP)-related parameters and diabetic retinopathy in T2DM [177]. Findings indicate that impaired β-cell function, rather than insulin resistance, is more closely linked with diabetic retinopathy. In particular, the postprandial C-peptide to glucose ratio may serve as a valuable systemic marker for identifying T2DM patients at high risk for developing diabetic retinopathy, especially vision-threatening forms.
Finally, a study was conducted to evaluate and compare the potential of several inflammatory markers, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio, systemic inflammation index, and red blood cell distribution width (RDW), as predictors of diabetic retinopathy severity in a U.S. population [178]. Results indicate that RDW combined with NLR presents a promising approach for predicting diabetic retinopathy severity.
- Metabolite- and lipid-derived biomarkers
There is broad consensus that metabolic dysregulation plays a crucial role in the development of diabetic vascular complications. A comprehensive study identifies six metabolites, including creatinine, albumin, tyrosine, glutamine, lactate, and the ratio of phospholipids to total lipids in small LDL, as being correlated with macrovascular complications. Eight additional metabolites, including glucose, tyrosine, very large high-density lipoprotein particles, valine, free cholesterol to total lipids in very small very low-density lipoprotein, alanine, albumin, and isoleucine are associated with microvascular complications [179]. These findings provide compelling evidence that circulating metabolites can be utilized as predictive biomarkers for vascular complications in diabetic patients.
Sphingomyelin (SM) appears to play a role in the early stages of diabetic retinopathy. Evidence shows that average plasma levels of total SM are significantly lower in individuals with T2DM compared to those with prediabetes and healthy controls [180]. Additionally, lower plasma SM levels are associated with reduced retinal sensitivity in diabetic individuals, suggesting that SMs could be promising biomarkers for detecting diabetic retinal neurodegeneration at early disease stages.
Another study highlights that dodecanoylcarnitine, linoleylcarnitine, stearylcarnitine, decanoic acid, and proline could potentially serve as independent biomarkers for predicting therapeutic outcomes following vitrectomy in patients with type 2 diabetic retinopathy [181].
The visceral adiposity index, lipid accumulation product, and atherogenic index of plasma are established biomarkers for predicting metabolic disorders such as diabetes mellitus and associated microvascular complications, particularly diabetic kidney disease (DKD) and diabetic retinopathy. While a study shows these indices are significant predictors of DKD in individuals with diabetes mellitus, their utility in detecting diabetic retinopathy is limited [182].
- Thickness changes in outer plexiform layer may correlates with renal-related diseases such as diabetes
Given the similar pathophysiology of microvascular complications in diabetic kidney disease and diabetic retinopathy, a study was conducted to assess the relationship between outer plexiform layer (OPL) thickness and kidney function indicators such as estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) [183]. Perifoveal OPL thickness was found to be inversely associated with eGFR and positively associated with UACR. The authors suggest that OPL thickening could serve as a potential indicator for diabetic kidney disease, with optical coherence tomography (OCT) imaging offering a noninvasive means of exploring retinal-renal interactions.
6.1.2. Nephropathy
Diabetic nephropathy is the most frequent complication of T2DM that affects kidney function, leading to a gradual decline in the renal capacity to filter waste products from the bloodstream [184]. It contributes to the development of end-stage renal disease (ESRD) [185], the final stage of chronic kidney disease, which results in permanent renal failure, underscoring its significant clinical importance. While the pathogenesis of diabetic nephropathy is not fully understood, its development involves multiple factors, including metabolic, hemodynamic, growth factors, and proinflammatory and profibrotic pathways, all of which play significant roles [186,187,188]. Over time, persistent hyperglycemia can lead to deterioration of various kidney compartments, including the glomeruli, tubules, interstitium, and vasculature [189]. Besides hypertension and certain immune disorders, elevated blood glucose levels can cause microalbuminuria, characterized by the presence of small amounts of albumin in the urine. This condition leads to glomerular hyperfiltration and overt proteinuria, the hallmark of diabetic kidney disease and a risk factor for cardiovascular disease.
Potential Biomarker Options of Nephropathy
- Dysregulated miRNA in diabetic kidney disease
Numerous miRNAs have been identified as either risk or protective factors in diabetes-related complications [190]. One study revealed a significant positive association between serum hsa-miR-221 and fasting insulin, fasting glucose, HOMA-IR, ACR, and BMI, with high specificity and sensitivity in patients with diabetic nephropathy [191]. Additionally, the expression levels of miR-132, miR-133a and lnc-MGC, and their correlations with LDH and HbA1C, have been shown to serve as biomarkers distinguishing diabetic patients with reduced cardiovascular disease risk from those in early-stage diabetes [192]. hsa-miR-221, in particular, appears to be a promising prognostic and diagnostic biomarker in diabetic nephropathy.
- Growth Factors
Circulating levels of vascular endothelial growth factor (VEGF) family members are often elevated in individuals with T2DM. A study examining placental growth factor (PlGF), soluble fms-like tyrosine kinase-1 (sFLT-1), and VEGF-A highlighted their involvement in cardiorenal complications in patients with T2DM [193]. The study found elevated PlGF levels, as well as increased sFLT-1 and PlGF/sFLT-1 ratios, to be useful indicators of cardiorenal events in T2DM and diabetic kidney disease. However, treatment with canagliflozin did not reduce these biomarkers.
Additionally, elevated circulating levels of adipocyte fatty acid-binding protein (AFABP), fibroblast growth factor 21, and pigment epithelium-derived factor are positively correlated with markers of metabolic syndrome and microvascular complications, including the progression of nephropathy in Chinese patients with T2DM [194,195,196,197]. Notably, serum AFABP has shown stronger predictive value for incident sight-threatening diabetic retinopathy than for nephropathy.
- Biomarkers of oxidative stress and inflammation
Circulating biomarkers such as IL-6, IL-10, CD163, CXCL9, CCL22, GDF15, IL-33, FGF21, follistatin, and neurofilament light chain (NfL) have been associated with both microvascular and macrovascular complications; including neuropathy, nephropathy, retinopathy, and major adverse cardiovascular events (MACE) [198]. Among these, CXCL9, GDF15, NfL, and FGF21 have been identified as independent predictors of mortality in T2DM.
A targeted proteomics approach compared inflammatory profiles between individuals with T1DM, T2DM, and healthy controls [199]. The results revealed that inflammatory proteins linked to nephropathy were similar across both types of diabetes. Specifically, FLT3L and EN-RAGE were associated with cardiovascular disease in T2DM. While both T1DM and T2DM showed elevated levels of inflammatory proteins, the increase was more pronounced in T2DM.
Circulating activin A, an inflammatory mediator implicated in profibrotic kidney injury, is elevated in diabetic kidney disease and correlates with kidney damage. Animal studies suggest that activin A promotes kidney injury through macrophage-driven inflammation [200]. Inhibitors targeting activin A reduce senescence markers (e.g., p19), pro-inflammatory and pro-fibrotic markers, improve kidney morphology, restore podocyte markers (nephrin and Wilms tumor-1), and reduce albuminuria and fibrosis.
Growth differentiation factor 15 (GDF-15), a homeostatic cytokine, also plays a protective role in diabetic nephropathy [201] . Its anti-inflammatory actions and upregulation of renal-protective pathways suggest that GDF-15 may serve as both a diagnostic and prognostic biomarker.
Elevated levels of serum adhesion molecule-like protein, coupled with reduced levels of nesfatin-1 and 25-hydroxy vitamin D (25(OH)D), have been linked to a higher risk of diabetic kidney disease in T2DM patients [202].
Oxidative stress is a key factor in the development and progression of T2DM. Peroxiredoxin-4, an antioxidant protein, was found to be associated with increased risk of nephropathy independent of low-grade inflammation, but not with new-onset retinopathy or neuropathy [203].
Ischemia-modified albumin is a novel marker of oxidative stress. Elevated levels have been detected in patients with T2DM and are associated with the severity of diabetic complications such as retinopathy, nephropathy, and peripheral arterial disease [204]. Despite its low specificity, this assay may still be useful for risk assessment.
The oxidative stress-related metabolite 8-hydroxy-2’-deoxyguanosine (8-OHdG) has also been evaluated in diabetic patients with and without renal complications. Serum 8-OHdG levels were significantly higher in those with diabetic kidney disease, supporting its potential as a biomarker for oxidative DNA damage in diabetes-related renal dysfunction [205].
- Hepatic and cardiac biomarkers
Cardiac biomarkers such as N-terminal prohormone of B-type natriuretic peptide and troponin T have shown associations with the progression of diabetic nephropathy [206]. Elevated levels of these markers in diabetic patients indicate advancing kidney dysfunction.
Angiopoietin-like protein 8, a hepatic-derived protein, has also been identified as a risk factor for diabetic nephropathy. Its significant elevation in affected patients suggests its utility as a potential biomarker[200].
6.1.3. Neuropathy
Diabetic neuropathy, a debilitating complication of T2DM, encompasses a broad range of clinical pathologies manifested through a set of nerve disorders caused by nerve fiber damage due to abnormally high levels of blood glucose. Prolonged hyperglycemia can induce neuronal injury through several biochemical pathways, including oxidative stress, polyol pathway alteration, protein kinase C activation, and advanced glycation end-products formation [207]. There is a link between the severity of diabetes and both peripheral somatic and central neurodegeneration [208,209]. Diabetic neuropathy in T2DM is associated with dyslipidemia, central obesity, hypertension, insulin resistance, hormonal imbalance, and poor glucose control. It can affect multiple components of the nervous system, from the cerebral cortex to skeletal muscle, leading to a broad range of symptoms.
Diabetic neuropathy refers to various conditions involving damage to the autonomic or peripheral nervous systems. It involves both tissues (large and small vessels) and fibers (large and small nerve fibers) [210]. Autonomic neuropathy is a condition that impairs the normal functioning of the autonomic nervous system, leading to cardiovascular morbidity and mortality, with a clinical course that damages the nerves of the cardiovascular system, digestive system, thermoregulation, kidneys, and bladder [211,212]. While its causes are multifactorial, prolonged elevation of blood glucose levels can damage nerves over time. Common symptoms of this condition may include dizziness, an irregular heart rate, gastrointestinal disturbances, and bladder dysfunction.
Diabetic peripheral neuropathy, a form of peripheral nerve dysfunction, involves multiple types of nerve fibers and is classified into three subclasses according to fiber diameter: small-fiber, large-fiber, and mixed-fiber neuropathies [213]. It is associated with neuromuscular dysfunction and primarily affects large fibers or a combination of small and large fibers. The condition may result not only in skeletal muscular dysfunction but also in morphological alterations of the plantar tissue [214]. It reflects the complex interplay of immune, inflammatory, and vascular mechanisms. Due to its complexity, there is currently no effective treatment available, apart from maintaining a healthy lifestyle and tight control of blood glucose levels. There is a need to identify biomarkers that reflect the progression of the disease and improve therapeutic strategies.
Potential Biomarker Options in Neuropathies
- Neuroinflammatory mediators
Chemokines play a key role in the pathogenesis of various neuropathies and neuropathic pain processes. Plasma levels of CXCL9, CXCL10, and CXCL11 have been measured in patients with neuropathy [215]. Among these, CXCL10 levels are significantly elevated in T2DM patients with neuropathy. It is suggested that CXCL10 may serve as an early detection biomarker, potentially aiding the development of therapeutic strategies to reverse or prevent diabetic neuropathy.
Netrin-1, a neurotrophic factor, has also been studied in relation to early diabetic neuropathy in patients with T2DM [216]. Serum netrin-1 levels show a gradual decline corresponding to the severity of small nerve fiber damage. This suggests that netrin-1 may serve as a biomarker for small fiber neuropathy in diabetes.
Glial Fibrillary Acidic Protein (GFAP), expressed in non-myelinating Schwann cells in the peripheral nervous system, and Ubiquitin C-terminal hydrolase L1 (UCH-L1), a neuron-expressed stress protein, are also of interest [217,218]. A study evaluating circulating GFAP and UCH-L1 levels in patients with and without diabetic polyneuropathy (DPN) found that serum GFAP levels were significantly reduced in individuals with DPN compared to controls and those without DPN [219]. This suggests that lower GFAP may indicate small nerve fiber damage, positioning GFAP as a potential biomarker for small fiber neuropathy.
Advanced glycation end products (AGEs) and their interaction with receptors for AGE (RAGE) are central to the pathogenesis of diabetic foot (DF), particularly in patients with neuropathy [220,221]. A study examined asymmetric dimethylarginine (ADMA), fructosamine, nitric oxide (NO), and soluble RAGE (sRAGE) in diabetic patients with and without neuropathy. Circulating sRAGE levels were significantly elevated in T2DM patients without DF compared to healthy controls. In contrast, ADMA and fructosamine levels were significantly higher in patients with DF, and NO levels were lower in this group compared to both non-DF diabetics and healthy individuals. The study suggests that sRAGE may act as an endogenous protective factor against the development of DF, with reduced levels potentially contributing to diabetic foot complications associated with neuropathy.
- Hyperglycemia-induced molecules affecting metabolic and hemodynamic pathways
Heat shock protein 27 (Hsp27) is a small heat shock protein known for its role in protecting cells from apoptosis under stress. A study evaluated plasma Hsp27 levels in T2DM patients with and without microvascular complications such as diabetic retinopathy, diabetic nephropathy, and diabetic neuropathy [222]. Notably, Hsp27 levels were highest in the diabetic nephropathy group compared to controls and other complication groups, suggesting that plasma Hsp27 may serve as a potential biomarker for diabetic nephropathy.
Persistent hyperglycemia also alters hemoglobin (Hb) and red blood cell deformability, impairing hemorheology in T2DM [223]. Glycated hemoglobin reflects prolonged hyperglycemia. Another study found evidence of RBC breakdown and low-grade intravascular hemolysis (IVH) in T2DM patients [224]. Increased heme-related absorbance was associated with peripheral sensory neuropathy, but not with other vascular complications. These findings support an association between T2DM and low-grade IVH, which may contribute to the development of diabetic neuropathy.
6.2. Macrovascular Complications
6.2.1. Coronary Artery Disease
Coronary artery disease (CAD), a macrovascular complication, occurs when plaque buildup (atherosclerosis) in the arteries of the heart restricts blood flow. Atherosclerosis is a progressive condition that affects multiple arteries throughout the body. CAD is associated with diabetes, hypertension, metabolic disturbances, lifestyle factors, and older age [225].
Individuals with T2DM may develop cardiovascular complications such as CAD, cardiac autonomic neuropathy, or diabetic cardiomyopathy [5]. Risk factors unique to diabetes increase the likelihood of CAD, contributing to atherosclerotic plaque formation and thrombosis [226,227,228]. Diabetes-accelerated CAD is complex and involves numerous metabolic and molecular signaling pathways, including hyperglycemia, oxidative stress, chronic inflammation, and epigenetic dysfunction within the coronary arteries [229].
Atherosclerosis-induced reduction in blood flow to the heart results in angina. It encompasses a broad range of conditions, including stable angina, unstable angina, myocardial infarction (MI), and sudden death [230,231,232]. The Framingham study indicates that diabetic patients are more likely to experience MI than those without diabetes [233]. Diabetic individuals without a prior history of MI are still at high risk of myocardial ischemia, heart attacks, and strokes [234]. Thus, T2DM-induced atherosclerosis is a significant global health concern.
Potential Biomarkers in Coronary Arterial Disease
- Hormones as biomarkers
There is a strong association between the early stages of chronic kidney disease (CKD), vascular remodeling, and coronary artery calcification. Adropin, a nutritionally regulated peptide hormone primarily synthesized in the liver, is also produced in other tissues such as the brain, heart, and gastrointestinal tract [235]. Adropin plays a regulatory role in several cardiovascular pathologies [236]. A study has shown an association between adropin levels and asymptomatic coronary calcification in patients in the early stages of CKD [237]. Patients with known asymptomatic coronary artery calcification exhibited significantly reduced levels of circulating adropin. This suggests that low adropin levels may serve as a potential biomarker for predicting the risk of coronary artery calcification in early-stage CKD patients.
Endothelin-1 (ET-1), an endogenous vasoconstrictor, also plays a significant role in coronary artery disease (CAD) and diabetes. Its prognostic value has been evaluated in patients with stable CAD across different states of glucose metabolism [238]. Elevated ET-1 levels are significantly associated with an increased risk of cardiovascular events, suggesting that ET-1 could serve as a potential predictor in CAD patients with impaired glucose metabolism.
- Oxidative stress
Endothelial dysfunction and oxidative stress are key contributors to the initiation and progression of atherosclerosis. A study investigated their roles in patients with severe CAD undergoing coronary artery bypass graft (CABG) surgery, comparing those with and without T2DM [239]. Although serum levels of superoxide dismutase 1 (SOD-1) and lectin-like oxidized low-density lipoprotein receptor-1 (LOX-1) were not affected by the presence of T2DM, diabetic patients exhibited significant endothelial dysfunction, as evidenced by impaired brachial flow-mediated dilation and altered serum serotonin (5-HT) levels. The study found that circulating 5-HT levels were markedly influenced by T2DM and could potentially serve as a biomarker for CAD severity.
Ischemia with non-obstructive coronary arteries (INOCA) is a frequent cause of hospital admissions [240], with diabetes-induced coronary microvascular dysfunction playing a role in its complications. MicroRNAs (miRNAs) are emerging biomarkers for endothelial dysfunction and cardiovascular diseases. One study examined circulating miRNAs involved in endothelial regulation in INOCA patients with and without diabetes [241]. It found that miR-363-5p and miR-92a-3p were significantly dysregulated in INOCA patients with diabetes, suggesting their potential as biomarkers for monitoring and predicting endothelial dysfunction in this group.
Another study highlighted an association between circulating calprotectin, a protein secreted by activated monocytes and neutrophils, and the development of atherosclerotic cardiovascular disease (ASCVD), defined by events such as myocardial infarction, stroke, coronary revascularization, or cardiovascular death [242,243]. Calprotectin, involved in inflammatory processes, was associated with several risk factors, including elevated hemoglobin A1c, triglycerides, very low-density lipoprotein (VLDL) cholesterol, and reduced HDL cholesterol and cholesterol efflux capacity. The findings suggest that calprotectin may serve as a mechanistically relevant biomarker for ASCVD, independent of conventional cardiovascular risk factors.
- Metabolic messengers
Dyslipidemia is a well-established risk factor for ASCVD, particularly in T2DM patients. One study explored the association between dyslipidemia, dysglycemia, and subclinical coronary atherosclerosis [244]. It found that HDL diameter, free cholesterol, phospholipids, and total lipids in extra-large HDL were inversely associated with coronary artery calcium score. These findings indicate that alterations in HDL composition and concentration are linked to both dysglycemia and subclinical coronary atherosclerosis.
Sphingosine 1-phosphate (S1P) is a lipid signaling molecule with potent immunomodulatory and anti-inflammatory effects. A study revealed that altered circulating levels of S1P and its precursors are associated with increased cardiovascular risk in T2DM [245], suggesting their potential use as biomarkers for coronary atherosclerosis.
Another study investigated the oxLDL/LDL-C ratio and its relationship with the severity of coronary atherosclerosis in T2DM patients [246]. Results indicated that a higher oxLDL/LDL-C ratio was positively associated with more severe coronary atherosclerosis, supporting its potential use as a biomarker for early detection and intervention.
- Indicators of cell damage
Small leucine-rich proteoglycans (SLRPs), a type of matrix protein, have been associated with atherosclerotic plaque development [247]. One study examined the relationship between circulating lumican, a proteoglycan member of SLRPs, levels and CAD severity [248]. Serum lumican levels were elevated in patients with advanced CAD and demonstrated moderate predictive value (sensitivity: 64%, specificity: 65%) for disease severity.
Diabetes is a known risk factor for both CAD and chronic heart failure. Endothelial progenitor cells (EPCs), derived from bone marrow, play a critical role in vascular repair following injury. A study examined the response of circulating EPCs (cEPCs) to empagliflozin, an SGLT2 inhibitor, in diabetic patients with stable CAD [249]. Treatment resulted in increased cEPC levels and enhanced function, suggesting that EPC levels could serve as an indicator of therapeutic effectiveness.
A separate study evaluated the effects of empagliflozin versus placebo on high-sensitivity cardiac troponin-I (hs-cTnI) and lipid profile markers [250]. While the drug had a modest effect on lipid biomarkers, it significantly reduced circulating hs-cTnI levels, indicating improved cardiomyocyte function in T2DM patients with CAD.
6.2.2. Cerebrovascular Disease
T2DM increases the risk of cerebrovascular disease, a macrovascular complication. The progression of diabetes perturbs metabolic pathways [251], intracellular lipids [252], and blood glucose levels [253], leading to structural and functional alterations in the endothelial and smooth muscle cells of cerebral blood vessels. Moreover, insulin resistance combined with persistent hyperglycemia and lipotoxicity triggers macrophage-derived foam cell formation [254,255,256]. Diabetes-induced macrovascular dysfunction promotes atherosclerosis, leading to luminal narrowing [257]. Ultimately, diabetic atherosclerosis contributes to ischemic processes when a cerebral blood vessel becomes blocked. Ischemic stroke can result from an embolus originating in the heart or a more proximal artery, which then obstructs a cerebral artery already affected by an atherosclerotic plaque, increasing stroke risk.
A second type of stroke is hemorrhagic stroke. While hemorrhagic strokes have been observed in individuals with diabetes [258], their occurrence is associated with abnormally high HbA1c levels (≥72 mmol/mol). Poorly controlled blood glucose appears to significantly contribute to the risk of hemorrhagic stroke. These findings suggest that one of the primary vascular changes in T2DM is the development of atherosclerosis, which can lead to serious health complications.
Potential Biomarkers of Cerebrovascular Disease
- Biochemical indicators
Subclinical atherosclerosis begins to develop years before cardiovascular and cerebrovascular diseases become symptomatic. A study examined the effects of subclinical atherosclerosis on carotid intima-media thickness (CIMT) in patients with prediabetes and T2DM [259]. The results showed a significant elevation of circulating oxidized LDL (oxLDL), soluble lectin-like oxidized LDL receptor-1 (sLOX-1), and proprotein convertase subtilisin/kexin type 9 (PCSK9) levels in T2DM patients with macrovascular complications compared to controls, prediabetes, and uncomplicated diabetes groups. Concentrations of oxLDL, sLOX-1, and PCSK9 were significantly associated with CIMT. These findings suggest that these biomarkers may serve as potential indicators for cardiovascular risk assessment in patients with prediabetes and T2DM.
Chitotriosidase, a glycosyl hydrolase, is primarily synthesized by macrophages and epithelial cells [260]. It is secreted in response to local microenvironmental cues and plays a role in immune-driven processes, including inflammation. Studies show that serum chitotriosidase levels are associated with the severity of atherosclerotic lesions in patients with atherothrombotic stroke and ischemic heart disease [261], suggesting its potential as a marker for atherosclerotic burden.
Chronic kidney disease (CKD) is an independent risk factor for major adverse cardiovascular events (MACEs) and negatively impacts cerebrovascular function. Given the association between CKD progression and increased sympathetic tone, research has explored the relationship between cerebrovascular risk and renalase (RNL), a catecholamine-metabolizing enzyme, in pre-dialysis CKD patients [262]. Serum RNL levels were strongly associated with estimated glomerular filtration rate (eGFR), especially in relation to CKD progression. These findings suggest that RNL may serve as a predictor of renal and cerebrovascular outcomes.
Klotho is involved in the regulation of mineral metabolism, including phosphate and calcium. Mutations in the klotho gene have been linked to hypertension and kidney disease. Evidence indicates that klotho suppresses oxidative stress [263], improves endothelial function, and provides vascular protection [264]. Studies investigating its role in diabetic vascular complications found that elevated klotho levels are associated with a reduced risk of coronary artery disease and cerebrovascular events [264]. Notably, klotho levels independently predicted the development of macroangiopathies over a seven-year period. Circulating klotho is thus considered a valuable predictor of long-term macrovascular outcomes in T2DM patients.
- Neovasculogenesis
A separate study investigated the number and function of circulating endothelial progenitor cells (EPCs) in various vascular complications of T2DM and their association with vascular endothelial function [265]. The study found a reduction in both the number and function of circulating EPCs in T2DM patients, with the degree of reduction varying across different vascular diseases. EPC counts were correlated with endothelial function, suggesting that circulating EPCs may be used as a surrogate biomarker for vascular endothelial function in T2DM.
Moyamoya disease (MMD) is a chronic cerebrovascular disorder characterized by progressive occlusion of the internal carotid arteries or their branches [266]. A study explored the presence of EPCs and circulating endothelial cells (CECs) in patients with MMD [267]. CEC counts were significantly elevated in patients compared to controls. EPC counts were independently associated with patient age, while CEC counts were negatively associated with comorbid conditions such as hypertension, diabetes mellitus, and coronary heart disease.
6.2.3. Peripheral Artery Disease
Peripheral artery disease (PAD), a macrovascular complication, is characterized by the narrowing of arteries due to plaque buildup. As a chronic condition, PAD can lead to partial or total peripheral vascular occlusion. It involves atherosclerosis of the lower extremity arteries, the severity of which depends on the angiogenic response that triggers the development of collateral circulation to reduce ischemia and improve outcomes. However, functional impairment may increase the risk of atherothrombosis—the formation of a blood clot at the site of an atherosclerotic plaque.
Diabetes significantly contributes to PAD through various mechanisms, including glycation, inflammation, lipid abnormalities, insulin resistance, and endothelial dysfunction [268,269]. There is a significant association between PAD and male gender, former smoking, cerebrovascular disease, age, duration of diabetes, and high-density lipoprotein (HDL) levels [270].
PAD may cause multiple symptoms. In individuals with type 2 diabetes mellitus (T2DM), intermittent claudication may occur via nociceptive, inflammatory, and neuropathic mechanisms [271,272,273]. Intermittent claudication is classified into two subtypes: intermediate neurogenic claudication and intermediate vascular claudication [274]. Diabetic patients with PAD may present with variable intermittent claudication. Evidence suggests that some individuals with diabetes may not exhibit typical symptoms, as vascular claudication can be masked by peripheral neuropathy [270], while others may present with claudication and arterial ulceration. Notably, an association has been observed between plasma fibrinogen levels and diabetic foot ulcers, along with various clinical and inflammatory biomarkers [275].
Other symptoms include cold extremities due to poor circulation, reflecting reduced arterial blood flow, along with the development of non-healing ulcers or sores on the lower limbs [276,277]. Potential complications of PAD in individuals with diabetes include heart attack and stroke, which are among the leading causes of disability and death worldwide.
Potential Biomarker Options for Peripheral Arterial Disease
- Blood-based factors
Peripheral artery disease (PAD) is a common vascular condition. A study utilizing high-throughput proteomic profiling identified biomarkers associated with PAD [278]. Notably, plasma beta2-microglobulin (B2M) levels were significantly higher in PAD patients compared to non-PAD patients with coronary artery disease. B2M levels correlated with disease severity independently of other risk factors, as well as with the ankle-brachial index and functional capacity. These findings suggest B2M may serve as a promising biomarker for PAD.
Another study evaluated the predictive potential of circulating endothelium-enriched microRNA-126 (miR-126) in T2DM patients, both with and without coronary artery disease (CAD) [279]. miR-126 showed a strong association with both T2DM and CAD.
Endostatin, a cleavage fragment of collagen XVIII, is known to inhibit angiogenesis [280]. A study investigated the relationship between circulating endostatin levels and lower limb PAD symptoms [281]. Results showed elevated serum endostatin in older men experiencing intermittent claudication, supporting its role as a potential PAD biomarker.
- Inflammatory mediators
The relationship between vascular indices and circulating inflammatory biomarkers was explored in T2DM patients with poor glycemic control and no known cardiovascular disease [282]. Chitinase-3-like protein 1 (YKL-40) and neutrophil gelatinase-associated lipocalin (NGAL) emerged as novel indicators of vascular inflammation, showing associations with subclinical atherosclerosis in this population.
Adiponectin, a protein primarily secreted by adipocytes, circulates in peripheral blood [283]. Low levels of adiponectin (<4 µg/mL), or hypoadiponectinemia, are linked to several diseases, including coronary artery disease, stroke, and PAD. Adiponectin is therefore considered a biomarker of atherosclerosis.
Soluble urokinase plasminogen activator receptor (suPAR) is a marker of immune activation and is associated with atherosclerosis. A study assessed the relationship between suPAR and prevalent PAD [284], finding that elevated plasma suPAR levels predicted both existing PAD and future cardiovascular and PAD-related events.
- Cell-derived molecules
Patients with PAD are at increased risk for major adverse cardiovascular events (MACE). Insulin-like growth factor-binding protein 1 (IGFBP-1), mainly produced in the liver, was found to be significantly elevated in patients who experienced MACE [285]. IGFBP-1 emerged as the only biomarker independently associated with MACE over a two-year follow-up in both male and female PAD patients.
Adipocyte fatty acid-binding protein (FABP4), a fatty acid chaperone secreted by adipocytes and macrophages, is elevated in T2DM. It contributes to lipolysis and acts as an adipokine involved in insulin resistance and atherosclerosis [286]. A study investigating circulating FABP4 levels and endothelial function in T2DM patients found a negative association, suggesting that elevated FABP4 may directly impair vascular endothelium and serve as a valuable marker of vascular integrity [287]. Additionally, circulating miR-126 has been proposed as a biomarker for predicting T2DM patients with diabetic CAD.
A separate study evaluated biomarkers predictive of MACE in PAD patients [288]. While matrix metalloproteinase-10 (MMP-10) was associated with MACE in diabetic individuals, matrix metalloproteinase-7 (MMP-7) was independently associated with 2-year MACE prognosis in PAD patients.
7. Conclusions
T2DM is a complex chronic disorder and a major risk factor for neuropathy, nephropathy, retinopathy, coronary artery disease, cerebrovascular disease, and peripheral vascular disease. The concept of personalized medicine is emerging as a transformative approach to tailor medical treatment to the specific needs and characteristics of each patient. Since the treatment of T2DM is primarily based on HbA1c levels, improved glycemic control, and the reduction of long-term complications, circulating predictive biomarkers may prove useful in assessing patient responses to specific treatments, helping to ensure optimal therapeutic benefit with minimal side effects.
The image shown in Figure 4 illustrates the biomarkers discussed in this review and their potential roles in T2DM. A range of genetic and non-genetic biomarkers already have established roles in T2DM, though not all are suitable for routine clinical use due to various limitations. For instance, in monogenic diabetes, genetic testing can identify mutations that not only confirm a diagnosis of maturity-onset diabetes of the young (MODY) but also enable targeted therapy based on the patient’s genetic profile. For individuals with MODY1 or MODY3, low-dose sulfonylureas are considered first-line treatments. Similarly, circulating biomarkers may guide drug choices in broader T2DM populations and contribute to reducing morbidity and mortality. Notably, high-sensitivity C-reactive protein has been identified as a sensitive test to help distinguish MODY from T2DM.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, F.M. and Z.Sh.; validation, F.M. and Z.Sh.; writing—original draft preparation, Z.Sh.; writing—review and editing, F.M. and Z.Sh. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions to the study are included in the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACCORD | Action to Control Cardiovascular Risk in Diabetes |
| ADA | American Diabetes Association |
| CV | Cardiovascular |
| CNS | Central nervous system |
| CAD | Coronary artery disease |
| DCCT | Diabetes Control and Complications Trial |
| DPP-4 | Dipeptidyl peptidase-4 |
| FDA | Food and Drug Administration |
| GLP-1 | Glucagon-like peptide-1 |
| GIP | Glucose-dependent insulinotropic polypeptide |
| HbA1c | Plasma glycosylated hemoglobin A1C |
| HHS | Hyperosmolar hyperglycemic state |
| IDF | International Diabetes Federation |
| SGLT2 | Sodium-glucose co-transporter-2 |
| T1DM | Type 1 diabetes mellitus |
| T2DM | Type 2 diabetes mellitus |
| UKPDS | United Kingdom Prospective Diabetes Study |
| WHO | World Health Organization |
References
- Diabetes Facts and Figures | The International Diabetes Federation (IDF). 2025, https://idf.org/about-diabetes/diabetes-facts-figures/ .
- MARKANDU, K.; DEKHNE, A.; ISLAM, H.; ISLAM, R.; MADDINENI, K.; POTLURI, G.; PARISAPOGU, A.; TEJA CHINTHAPALLI, M.; DINESHBHAI DESAI, H. 1420-P: Global Burden and Trend of Type 2 DM in 38 OECD Countries from 1990–2019—A Benchmarking Systematic Analysis. Diabetes 2024, 73, (Supplement_1).
- Koya, D.; Araki, S.; Haneda, M. Therapeutic management of diabetic kidney disease. J Diabetes Investig 2011, 2, 248–254. [Google Scholar]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can J Cardiol 2018, 34, 575–584. [Google Scholar]
- Rajbhandari, J.; Fernandez, C.J.; Agarwal, M.; Yeap, B.X.Y.; Pappachan, J.M. Diabetic heart disease: A clinical update. World J Diabetes 2021, 12, 383–406. [Google Scholar]
- Mota, R.I.; Morgan, S.E.; Bahnson, E.M. Diabetic vasculopathy: macro and microvascular injury. Curr Pathobiol Rep 2020, 8, 1–14. [Google Scholar]
- Galiero, R.; Caturano, A.; Vetrano, E.; Beccia, D.; Brin, C.; Alfano, M.; Di Salvo, J.; Epifani, R.; Piacevole, A.; Tagliaferri, G.; Rocco, M.; Iadicicco, I.; Docimo, G.; Rinaldi, L.; Sardu, C.; Salvatore, T.; Marfella, R.; Sasso, F.C. Peripheral Neuropathy in Diabetes Mellitus: Pathogenetic Mechanisms and Diagnostic Options. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Diabete | World Health Organization (WHO). 2024, https://www.who.int/en/news-room/fact-sheets/detail/diabetes .
- Umemura, T.; Kawamura, T. Effect of diabetes on stroke symptoms and mortality: Lessons from a recent large population-based cohort study. J Diabetes Investig 2014, 5, 14–16. [Google Scholar]
- Lu, Y.; Wang, W.; Liu, J.; Xie, M.; Liu, Q.; Li, S. Vascular complications of diabetes: A narrative review. Medicine (Baltimore) 2023, 102, e35285. [Google Scholar] [CrossRef]
- Pan, S.; Worker, C.J.; Feng Earley, Y. The hypothalamus as a key regulator of glucose homeostasis: emerging roles of the brain renin-angiotensin system. Am J Physiol Cell Physiol 2023, 325, C141–c154. [Google Scholar] [CrossRef]
- Benoit, S.R.; Zhang, Y.; Geiss, L.S.; Gregg, E.W.; Albright, A. Trends in Diabetic Ketoacidosis Hospitalizations and In-Hospital Mortality - United States, 2000-2014. MMWR Morb Mortal Wkly Rep 2018, 67, 362–365. [Google Scholar] [CrossRef]
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic Crises in Adult Patients With Diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef]
- Scott, A.R.; Care, t. J. B. D. S. f. I.; group, t. J. h. h. g. Management of hyperosmolar hyperglycaemic state in adults with diabetes. Diabetic Medicine 2015, 32, 714–724. [Google Scholar]
- Umpierrez, G.E.; Davis, G.M.; ElSayed, N.A.; Fadini, G.P.; Galindo, R.J.; Hirsch, I.B.; Klonoff, D.C.; McCoy, R.G.; Misra, S.; Gabbay, R.A.; Bannuru, R.R.; Dhatariya, K.K. Hyperglycaemic crises in adults with diabetes: a consensus report. Diabetologia 2024, 67, 1455–1479. [Google Scholar]
- Wei, W.T.; Lin, S.M.; Hsu, J.Y.; Wu, Y.Y.; Loh, C.H.; Huang, H.K.; Liu, P.P. Association between Hyperosmolar Hyperglycemic State and Venous Thromboembolism in Diabetes Patients: A Nationwide Analysis in Taiwan. J Pers Med 2022, 12. [Google Scholar] [CrossRef]
- Arabshomali, A.; Bazzazzadehgan, S.; Mahdi, F.; Shariat-Madar, Z. Potential Benefits of Antioxidant Phytochemicals in Type 2 Diabetes. Molecules 2023, 28, 7209. [Google Scholar]
- Karslioglu French, E.; Donihi, A.C.; Korytkowski, M.T. Diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome: review of acute decompensated diabetes in adult patients. BMJ 2019, 365, l1114. [Google Scholar]
- Kitabchi, A.E.; Umpierrez, G.E.; Murphy, M.B.; Kreisberg, R.A. Hyperglycemic Crises in Adult Patients With Diabetes: A consensus statement from the American Diabetes Association. Diabetes Care 2006, 29, 2739–2748. [Google Scholar] [CrossRef]
- Shariff, S.Z.; Bejaimal, S.A.; Sontrop, J.M.; Iansavichus, A.V.; Haynes, R.B.; Weir, M.A.; Garg, A.X. Retrieving clinical evidence: a comparison of PubMed and Google Scholar for quick clinical searches. J Med Internet Res 2013, 15, e164. [Google Scholar]
- Morshed, T.; Hayden, S. Google Versus PubMed: Comparison of Google and PubMed’s Search Tools for Answering Clinical Questions in the Emergency Department. Ann Emerg Med 2020, 75, 408–415. [Google Scholar]
- Laakso, M. Biomarkers for type 2 diabetes. Molecular Metabolism 2019, 27, S139–S146. [Google Scholar]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tankova, T.; Tsapas, A.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar]
- Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia, World Health Organization (WHO)/IDF consultation, https://www.who.int/publications/i/item/definition-and-diagnosis-of-diabetes-mellitus-and-intermediate-hyperglycaemia; 9241594934; 2006.
- Standards of Medical Care for Patients With Diabetes Mellitus. Diabetes Care 1989, 12, 365–368. [CrossRef]
- Huang, E.S.; Liu, J.Y.; Moffet, H.H.; John, P.M.; Karter, A.J. Glycemic Control, Complications, and Death in Older Diabetic Patients: The Diabetes and Aging Study. Diabetes Care 2011, 34, 1329–1336. [Google Scholar]
- Bilal, A. Understanding Diabetes Overtreatment in Older Adults: Are We at an Intersection? Diabetes Care 2024, 48, 47–49. [Google Scholar]
- Ahlqvist, E.; Storm, P.; Käräjämäki, A.; Martinell, M.; Dorkhan, M.; Carlsson, A.; Vikman, P.; Prasad, R.B.; Aly, D.M.; Almgren, P.; Wessman, Y.; Shaat, N.; Spégel, P.; Mulder, H.; Lindholm, E.; Melander, O.; Hansson, O.; Malmqvist, U.; Lernmark, Å.; Lahti, K.; Forsén, T.; Tuomi, T.; Rosengren, A.H.; Groop, L. Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol 2018, 6, 361–369. [Google Scholar]
- Chen, Z.-Z.; Gerszten, R.E. Metabolomics and Proteomics in Type 2 Diabetes. Circulation Research 2020, 126, 1613–1627. [Google Scholar]
- Feldt-Rasmussen, B.; Mathiesen, E.R.; Deckert, T. Effect of two years of strict metabolic control on progression of incipient nephropathy in insulin-dependent diabetes. Lancet 1986, 2, 1300–1304. [Google Scholar]
- Reichard, P.; Berglund, B.; Britz, A.; Cars, I.; Nilsson, B.Y.; Rosenqvist, U. Intensified conventional insulin treatment retards the microvascular complications of insulin-dependent diabetes mellitus (IDDM): the Stockholm Diabetes Intervention Study (SDIS) after 5 years. J Intern Med 1991, 230, 101–108. [Google Scholar]
- Brinchmann-Hansen, O.; Dahl-Jørgensen, K.; Sandvik, L.; Hanssen, K.F. Blood glucose concentrations and progression of diabetic retinopathy: the seven year results of the Oslo study. Bmj 1992, 304, 19–22. [Google Scholar]
- Nathan, D.M.; Genuth, S.; Lachin, J.; Cleary, P.; Crofford, O.; Davis, M.; Rand, L.; Siebert, C. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993, 329, 977–986. [Google Scholar]
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998, 352, 837–853. [Google Scholar]
- Committee, A.D.A.P.P. 13. Older Adults: Standards of Care in Diabetes—2025. Diabetes Care 2024, 48, (Supplement_1), S266-S282.
- Mukonda, E.; van der Westhuizen, D.J.; Dave, J.A.; Cleary, S.; Hannan, L.; Rusch, J.A.; Lesosky, M. Understanding the relationship between the frequency of HbA1c monitoring, HbA1c changes over time, and the achievement of targets: a retrospective cohort study. BMC Endocrine Disorders 2025, 25, 3. [Google Scholar] [CrossRef]
- Nunes, J.P.L.; DeMarco, J.P. A 7.0-7.7% value for glycated haemoglobin is better than a .
- Gerstein, H.C.; Miller, M.E.; Byington, R.P.; Goff, D.C., Jr.; Bigger, J.T.; Buse, J.B.; Cushman, W.C.; Genuth, S.; Ismail-Beigi, F.; Grimm, R.H., Jr.; Probstfield, J.L.; Simons-Morton, D.G.; Friedewald, W.T. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008, 358, 2545–2559. [Google Scholar]
- Buse, J.B.; Bigger, J.T.; Byington, R.P.; Cooper, L.S.; Cushman, W.C.; Friedewald, W.T.; Genuth, S.; Gerstein, H.C.; Ginsberg, H.N.; Goff, D.C., Jr.; Grimm, R.H., Jr.; Margolis, K.L.; Probstfield, J.L.; Simons-Morton, D.G.; Sullivan, M.D. Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial: design and methods. Am J Cardiol 2007, (12a), 21i–33i. [Google Scholar]
- Stimson, R.H.; Dover, A.R.; Forbes, S.; Strachan, M.W.J.; McKnight, J.A.; Gibb, F.W. HbA1c Is Disproportionately Higher in Women and Older People With Type 1 Diabetes Compared With Flash Glucose Monitoring Metrics of Glycemic Control. J Diabetes Sci Technol 2022, 16, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Aceves, B.; Ezekiel-Herrera, D.; Marino, M.; Datta, R.; Lucas, J.; Giebultowicz, S.; Heintzman, J. Disparities in HbA1c testing between aging US Latino and non-Latino white primary care patients. Prev Med Rep 2022, 26, 101739. [Google Scholar] [PubMed]
- Zhou, B.; Sheffer, K.E.; Bennett, J.E.; Gregg, E.W.; Danaei, G.; Singleton, R.K.; Shaw, J.E.; Mishra, A.; Lhoste, V.P.F.; Carrillo-Larco, R.M.; Kengne, A.P.; Phelps, N.H.; Heap, R.A.; Rayner, A.W.; Stevens, G.A.; Paciorek, C.J.; Riley, L.M.; Cowan, M.J.; Savin, S.; Vander Hoorn, S.; Lu, Y.; Pavkov, M.E.; Imperatore, G.; Aguilar-Salinas, C.A.; Ahmad, N.A.; Anjana, R.M.; Davletov, K.; Farzadfar, F.; González-Villalpando, C.; Khang, Y.-H.; Kim, H.C.; Laatikainen, T.; Laxmaiah, A.; Mbanya, J.C.N.; Narayan, K.M.V.; Ramachandran, A.; Wade, A.N.; Zdrojewski, T.; Abbasi-Kangevari, M.; Rahim, H.F.A.; Abu-Rmeileh, N.M.; Adambekov, S.; Adams, R.J.; Aekplakorn, W.; Agdeppa, I.A.; Aghazadeh-Attari, J.; Agyemang, C.; Ahmadi, A.; Ahmadi, N.; Ahmadi, N.; Ahmed, S.H.; Ajlouni, K.; Al-Hinai, H.; Al-Lahou, B.; Al-Lawati, J.A.; Asfoor, D.A.; Al Qaoud, N.M.; Alarouj, M.; AlBuhairan, F.; AlDhukair, S.; Aldwairji, M.A.; Ali, M.M.; Alinezhad, F.; Alkandari, A.; Alomirah, H.F.; Aly, E.; Amarapurkar, D.N.; Andersen, L.B.; Anderssen, S.A.; Andrade, D.S.; Ansari-Moghaddam, A.; Aounallah-Skhiri, H.; Aris, T.; Arlappa, N.; Aryal, K.K.; Assah, F.K.; Assembekov, B.; Auvinen, J.; Avdičová, M.; Azad, K.; Azimi-Nezhad, M.; Azizi, F.; Bacopoulou, F.; Balakrishna, N.; Bamoshmoosh, M.; Banach, M.; Bandosz, P.; Banegas, J.R.; Barbagallo, C.M.; Barceló, A.; Baretić, M.; Barrera, L.; Basit, A.; Batieha, A.M.; Batista, A.P.; Baur, L.A.; Belavendra, A.; Ben Romdhane, H.; Benet, M.; Berkinbayev, S.; Bernabe-Ortiz, A.; Berrios Carrasola, X.; Bettiol, H.; Beybey, A.F.; Bhargava, S.K.; Bika Lele, E.C.; Bikbov, M.M.; Bista, B.; Bjerregaard, P.; Bjertness, E.; Bjertness, M.B.; Björkelund, C.; Bloch, K.V.; Blokstra, A.; Bo, S.; Bobak, M.; Boggia, J.G.; Bonaccio, M.; Bonilla-Vargas, A.; Borghs, H.; Bovet, P.; Brajkovich, I.; Brenner, H.; Brewster, L.M.; Brian, G.R.; Briceño, Y.; Brito, M.; Bugge, A.; Buntinx, F.; Cabrera de León, A.; Caixeta, R.B.; Can, G.; Cândido, A.P.C.; Capanzana, M.V.; Čapková, N.; Capuano, E.; Capuano, R.; Capuano, V.; Cardoso, V.C.; Carlsson, A.C.; Casanueva, F.F.; Censi, L.; Cervantes-Loaiza, M.; Chamnan, P.; Chamukuttan, S.; Chan, Q.; Charchar, F.J.; Chaturvedi, N.; Chen, H.; Cheraghian, B.; Chirlaque, M.-D.; Chudek, J.; Cifkova, R.; Cirillo, M.; Claessens, F.; Cohen, E.; Concin, H.; Cooper, C.; Costanzo, S.; Cowell, C.; Crujeiras, A.B.; Cruz, J.J.; Cureau, F.V.; Cuschieri, S.; D’Arrigo, G.; d’Orsi, E.; Dallongeville, J.; Damasceno, A.; Dastgiri, S.; De Curtis, A.; de Gaetano, G.; De Henauw, S.; Deepa, M.; DeGennaro, V.; Demarest, S.; Dennison, E.; Deschamps, V.; Dhimal, M.; Dika, Z.; Djalalinia, S.; Donfrancesco, C.; Dong, G.; Dorobantu, M.; Dörr, M.; Dragano, N.; Drygas, W.; Du, Y.; Duante, C.A.; Duboz, P.; Dushpanova, A.; Dziankowska-Zaborszczyk, E.; Ebrahimi, N.; Eddie, R.; Eftekhar, E.; Efthymiou, V.; Egbagbe, E.E.; Eghtesad, S.; El-Khateeb, M.; El Ati, J.; Eldemire-Shearer, D.; Elosua, R.; Enang, O.; Erasmus, R.T.; Erbel, R.; Erem, C.; Ergor, G.; Eriksen, L.; Eriksson, J.G.; Esmaeili, A.; Evans, R.G.; Fakhradiyev, I.; Fall, C.H.; Faramarzi, E.; Farjam, M.; Farzi, Y.; Fattahi, M.R.; Fawwad, A.; Felix-Redondo, F.J.; Ferguson, T.S.; Fernández-Bergés, D.; Ferrari, M.; Ferreccio, C.; Ferreira, H.S.; Ferrer, E.; Feskens, E.J.M.; Flood, D.; Forsner, M.; Fosse, S.; Fottrell, E.F.; Fouad, H.M.; Francis, D.K.; Frontera, G.; Furusawa, T.; Gaciong, Z.; Garnett, S.P.; Gasull, M.; Gazzinelli, A.; Gehring, U.; Ghaderi, E.; Ghamari, S.-H.; Ghanbari, A.; Ghasemi, E.; Gheorghe-Fronea, O.-F.; Ghimire, A.; Gialluisi, A.; Giampaoli, S.; Gianfagna, F.; Gill, T.K.; Gironella, G.; Giwercman, A.; Goltzman, D.; Gomula, A.; Gonçalves, H.; Gonçalves, M.; Gonzalez-Chica, D.A.; Gonzalez-Gross, M.; González-Rivas, J.P.; González-Villalpando, M.-E.; Gonzalez, A.R.; Gottrand, F.; Grafnetter, D.; Grodzicki, T.; Grøntved, A.; Guerrero, R.; Gujral, U.P.; Gupta, R.; Gutierrez, L.; Gwee, X.; Haghshenas, R.; Hakimi, H.; Hambleton, I.R.; Hamzeh, B.; Hanekom, W.A.; Hange, D.; Hantunen, S.; Hao, J.; Hari Kumar, R.; Harooni, J.; Hashemi-Shahri, S.M.; Hata, J.; Heidemann, C.; Henrique, R. d. S.; Herrala, S.; Herzig, K.-H.; Heshmat, R.; Ho, S.Y.; Holdsworth, M.; Homayounfar, R.; Hopman, W.M.; Horimoto, A.R.V.R.; Hormiga, C.; Horta, B.L.; Houti, L.; Howitt, C.; Htay, T.T.; Htet, A.S.; Htike, M.M.T.; Huerta, J.M.; Huhtaniemi, I.T.; Collaboration, N.C.D.R.F. Global variation in diabetes diagnosis and prevalence based on fasting glucose and hemoglobin A1c. Nature Medicine 2023, 29, 2885–2901. [Google Scholar]
- de Miranda, V.A.; Cruz Filho, R.A.; de Oliveira, T.S.; Moscavitch, S.D.; Kang, H.C.; Miranda Chagas, S.V.; Costa, D.M.; Vianna Araújo, D.; Garcia Rosa, M.L. Racial differences in HbA1c: a cross-sectional analysis of a Brazilian public primary care population. Prim Care Diabetes 2013, 7, 135–141. [Google Scholar] [CrossRef]
- Gorst, C.; Kwok, C.S.; Aslam, S.; Buchan, I.; Kontopantelis, E.; Myint, P.K.; Heatlie, G.; Loke, Y.; Rutter, M.K.; Mamas, M.A. Long-term Glycemic Variability and Risk of Adverse Outcomes: A Systematic Review and Meta-analysis. Diabetes Care 2015, 38, 2354–2369. [Google Scholar] [CrossRef]
- Teoh, H.; Home, P.; Leiter, L.A. Should A1C targets be individualized for all people with diabetes? Arguments for and against. Diabetes Care 2011, 34 Suppl 2, (Suppl 2), S191-6.
- Anderson, J.J.; Welsh, P.; Ho, F.K.; Ferguson, L.D.; Welsh, C.E.; Pellicori, P.; Cleland, J.G.F.; Forbes, J.; Iliodromiti, S.; Boyle, J.; Lindsay, R.; Celis-Morales, C.; Gray, S.R.; Katikireddi, S.V.; Gill, J.M.R.; Pell, J.P.; Sattar, N. Ethnic differences in prevalence of actionable HbA1c levels in UK Biobank: implications for screening. BMJ Open Diabetes Res Care 2021, 9. [Google Scholar]
- Oshima, M.; Jun, M.; Ohkuma, T.; Toyama, T.; Wada, T.; Cooper, M.E.; Hadjadj, S.; Hamet, P.; Harrap, S.; Mancia, G.; Marre, M.; Williams, B.; Chalmers, J.; Woodward, M.; Perkovic, V.; on behalf of the, A.C.G. The relationship between eGFR slope and subsequent risk of vascular outcomes and all-cause mortality in type 2 diabetes: the ADVANCE-ON study. Diabetologia 2019, 62, 1988–1997. [Google Scholar] [PubMed]
- Marx, N.; Federici, M.; Schütt, K.; Müller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; Di Angelantonio, E.; Eliasson, B.; Espinola-Klein, C.; Fauchier, L.; Halle, M.; Herrington, W.G.; Kautzky-Willer, A.; Lambrinou, E.; Lesiak, M.; Lettino, M.; McGuire, D.K.; Mullens, W.; Rocca, B.; Sattar, N.; Group, E.S.D. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes: Developed by the task force on the management of cardiovascular disease in patients with diabetes of the European Society of Cardiology (ESC). European Heart Journal 2023, 44, 4043–4140. [Google Scholar] [PubMed]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovascular Diabetology 2018, 17, 83. [Google Scholar] [PubMed]
- Alijla, F.; Buttia, C.; Reichlin, T.; Razvi, S.; Minder, B.; Wilhelm, M.; Muka, T.; Franco, O.H.; Bano, A. Association of diabetes with atrial fibrillation types: a systematic review and meta-analysis. Cardiovasc Diabetol 2021, 20, 230. [Google Scholar] [CrossRef]
- Reinstatler, L.; Qi, Y.P.; Williamson, R.S.; Garn, J.V.; Oakley, G.P., Jr. Association of Biochemical B12 Deficiency With Metformin Therapy and Vitamin B12 Supplements: The National Health and Nutrition Examination Survey, 1999–2006. Diabetes Care 2012, 35, 327–333. [Google Scholar]
- Wile, D.J.; Toth, C. Association of Metformin, Elevated Homocysteine, and Methylmalonic Acid Levels and Clinically Worsened Diabetic Peripheral Neuropathy. Diabetes Care 2009, 33, 156–161. [Google Scholar] [CrossRef]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A.W. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. New England Journal of Medicine 2008, 359, 1577–1589. [Google Scholar]
- Shurrab, N.T.; Arafa, E.-S. A. Metformin: A review of its therapeutic efficacy and adverse effects. Obesity Medicine 2020, 17, 100186. [Google Scholar]
- Wu, H.; Feng, K.; Zhang, C.; Zhang, H.; Zhang, J.; Hua, Y.; Dong, Z.; Zhu, Y.; Yang, S.; Ma, C. Metformin attenuates atherosclerosis and plaque vulnerability by upregulating KLF2-mediated autophagy in apoE−/- mice. Biochemical and Biophysical Research Communications 2021, 557, 334–341. [Google Scholar]
- McIntosh, B.; Cameron, C.; Singh, S.R.; Yu, C.; Dolovich, L.; Houlden, R. Choice of therapy in patients with type 2 diabetes inadequately controlled with metformin and a sulphonylurea: a systematic review and mixed-treatment comparison meta-analysis. Open Med 2012, 6, e62–e74. [Google Scholar]
- Riddle, M. Combining sulfonylureas and other oral agents. Am J Med 2000, 108 Suppl 6a, 15s-22s.
- Douros, A.; Dell’Aniello, S.; Yu, O.H.Y.; Filion, K.B.; Azoulay, L.; Suissa, S. Sulfonylureas as second line drugs in type 2 diabetes and the risk of cardiovascular and hypoglycaemic events: population based cohort study. BMJ 2018, 362, k2693. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y.; Matsuda, M.; Tawaramoto, K.; Kawasaki, F.; Hashiramoto, M.; Matsuki, M.; Kaku, K. Effects of sulfonylurea drugs on adiponectin production from 3T3-L1 adipocytes: implication of different mechanism from pioglitazone. Diabetes Res Clin Pract 2008, 81, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Hasslacher, C.; Group, f. t. M. R. R. S. Safety and Efficacy of Repaglinide in Type 2 Diabetic Patients With and Without Impaired Renal Function. Diabetes Care 2003, 26, 886–891. [Google Scholar] [CrossRef]
- Garber, A.J.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.T.; Bush, M.A.; Dagogo-Jack, S.; DeFronzo, R.A.; Einhorn, D.; Fonseca, V.A.; Garber, J.R.; Garvey, W.T.; Grunberger, G.; Handelsman, Y.; Hirsch, I.B.; Jellinger, P.S.; McGill, J.B.; Mechanick, J.I.; Rosenblit, P.D.; Umpierrez, G.E. CONSENSUS STATEMENT BY THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY ON THE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM - 2018 EXECUTIVE SUMMARY. Endocr Pract 2018, 24, 91–120. [Google Scholar] [CrossRef]
- Chang, J.; Liu, B.; Cheng, Y.X.; Zhang, J.G.; Tao, S.; Yan, H.L. Effect of Repaglinide on Blood Glucose, Endothelial Function, Lipid Metabolism, and Inflammatory Reaction in a Rat Model of Atherosclerosis. Dose Response 2020, 18, 1559325820918762. [Google Scholar]
- Herrmann, B.L.; Erbel, R.; Janssen, O.E.; Mann, K. [Cardiovascular effects of oral hypoglycemie drugs]. Herz 2004, 29, 510–518. [Google Scholar]
- Bloomgarden, Z.T. Thiazolidinediones. Diabetes Care 2005, 28, 488–493. [Google Scholar]
- Smith, U. Pioglitazone: mechanism of action. Int J Clin Pract Suppl 2001, 13–18. [Google Scholar]
- Bohannon, N. Overview of the gliptin class (dipeptidyl peptidase-4 inhibitors) in clinical practice. Postgrad Med 2009, 121, 40–45. [Google Scholar]
- Drakul, M.; Čolić, M. Immunomodulatory activity of dipeptidyl peptidase-4 inhibitors in immune-related diseases. European Journal of Immunology 2023, 53, 2250302. [Google Scholar] [CrossRef]
- Kawanami, D.; Takashi, Y.; Takahashi, H.; Motonaga, R.; Tanabe, M. Renoprotective Effects of DPP-4 Inhibitors. Antioxidants (Basel) 2021, 10. [Google Scholar] [CrossRef]
- Gupta, S.; Sen, U. More than just an enzyme: Dipeptidyl peptidase-4 (DPP-4) and its association with diabetic kidney remodelling. Pharmacol Res 2019, 147, 104391. [Google Scholar] [PubMed]
- Huang, J.; Jia, Y.; Sun, S.; Meng, L. Adverse event profiles of dipeptidyl peptidase-4 inhibitors: data mining of the public version of the FDA adverse event reporting system. BMC Pharmacology and Toxicology 2020, 21, 68. [Google Scholar]
- Pathak, R.; Bridgeman, M.B. Dipeptidyl Peptidase-4 (DPP-4) Inhibitors In the Management of Diabetes. P t 2010, 35, 509–513. [Google Scholar] [PubMed]
- Patoulias, D.I.; Boulmpou, A.; Teperikidis, E.; Katsimardou, A.; Siskos, F.; Doumas, M.; Papadopoulos, C.E.; Vassilikos, V. Cardiovascular efficacy and safety of dipeptidyl peptidase-4 inhibitors: A meta-analysis of cardiovascular outcome trials. World J Cardiol 2021, 13, 585–592. [Google Scholar] [CrossRef]
- Sun, F.; Wu, S.; Wang, J.; Guo, S.; Chai, S.; Yang, Z.; Li, L.; Zhang, Y.; Ji, L.; Zhan, S. Effect of glucagon-like peptide-1 receptor agonists on lipid profiles among type 2 diabetes: a systematic review and network meta-analysis. Clin Ther 2015, 37, 225–241.e8. [Google Scholar] [CrossRef]
- Deacon, C.F.; Mannucci, E.; Ahrén, B. Glycaemic efficacy of glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors as add-on therapy to metformin in subjects with type 2 diabetes-a review and meta analysis. Diabetes Obes Metab 2012, 14, 762–767. [Google Scholar] [CrossRef]
- Scheen, A.J. GLP-1 Receptor Agonists and SGLT2 Inhibitors in Type 2 Diabetes: Pleiotropic Cardiometabolic Effects and Add-on Value of a Combined Therapy. Drugs 2024, 84, 1347–1364. [Google Scholar] [CrossRef]
- McLean, B.A.; Wong, C.K.; Kaur, K.D.; Seeley, R.J.; Drucker, D.J. Differential importance of endothelial and hematopoietic cell GLP-1Rs for cardiometabolic versus hepatic actions of semaglutide. JCI Insight 2021, 6. [Google Scholar]
- Saraiva, J.F.K.; Franco, D. Oral GLP-1 analogue: perspectives and impact on atherosclerosis in type 2 diabetic patients. Cardiovasc Diabetol 2021, 20, 235. [Google Scholar] [CrossRef]
- Seddio, A.E.; Vasudevan, R.S.; Gouzoulis, M.J.; Ansah-Twum, J.K.; Grauer, J.N.; Rubin, L.E. As Few as Three Months of Preoperative Semaglutide Exposure Prior to Total Knee Arthroplasty Is Associated With Reduced Postoperative Adverse Events in Patients With Type II Diabetes. J Arthroplasty 2025. [Google Scholar] [CrossRef] [PubMed]
- Lixi, F.; Calabresi, V.; Cukurova, F.; Giannaccare, G. Non-Arteritic Anterior Ischemic Optic Neuropathy in an Otherwise Healthy Young Adult Patient Treated with Liraglutide and Semaglutide for Weight Loss: A Cautionary Tale. Int Med Case Rep J 2025, 18, 991–995. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Inzucchi, S.E. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Kadowaki, T.; Heftdal, L.D.; Ko, H.J.; Overvad, M.; Shimomura, I.; Thamattoor, U.K.; Kim, K.K.; Investigators, O. Oral Semaglutide in an East Asian Population With Overweight or Obesity, With or Without Type 2 Diabetes: The OASIS 2 Randomized Clinical Trial. JAMA Intern Med 2025. [Google Scholar] [CrossRef]
- Suki, M.; Amer, J.; Milgrom, Y.; Massarwa, M.; Hazou, W.; Tiram, Y.; Perzon, O.; Sharif, Y.; Sackran, J.; Alon, R.; Lourie, N.E.E.; Raz, I.; Imam, A.; Khalaileh, A.; Safadi, R. Semaglutide in MASLD Patients: Improved Survival and Liver Outcomes. Pharmaceuticals (Basel) 2025, 18. [Google Scholar] [CrossRef]
- Aristizabal-Colorado, D.; Vernaza Trujillo, D.A.; Sierra Castillo, S.; Rivera Martinez, W.A.; Badiel, M.; Abreu Lomba, A. Semaglutide Versus Empagliflozin in Uncontrolled Type 2 Diabetes: A Cohort Study With 18 Months of Follow-Up (SEMPA18). Cureus 2025, 17, e83416. [Google Scholar] [CrossRef]
- Peng, L.; He, Y.; Zhang, Z.; Yin, J.; Fan, J. Efficacy and safety of empagliflozin for the acute myocardial infarction: a systematic review and meta-analysis of randomized controlled trials. Ann Med 2025, 57, 2514078. [Google Scholar] [CrossRef]
- Lewis, M.; Burrack, N.; Heymann, A.; Grossman, A.; Neuman, T.; Abuhasira, R. Sodium-Glucose Cotransporter 2 Inhibitors, Erythrocytosis, and Thrombosis in Adults With Type 2 Diabetes. JAMA Netw Open 2025, 8, e2517086. [Google Scholar] [CrossRef]
- Schmedt, N.; Alhamdow, A.; Tskhvarashvili, G.; Saarelainen, L.; Qiao, X.; Lobier, M.; Hoti, F. Post-authorisation safety study to assess the risk of urinary tract cancer in people with type 2 diabetes initiating empagliflozin: A multi-country European study. Diabetes Obes Metab 2025, 27, 4401–4414. [Google Scholar] [CrossRef]
- Liang, D.X.; Wu, H.T.; Yang, J.; Yang, M. [Efficacy and safety of empagliflozin in the treatment of glycogen storage disease-associated inflammatory bowel disease]. Zhongguo Dang Dai Er Ke Za Zhi 2025, 27, 929–935. [Google Scholar] [PubMed]
- Hauwanga, W.N.; Abdalhamed, T.Y.; Ezike, L.A.; Chukwulebe, I.S.; Ko Oo, A.; Wilfred, A.; Khan, A.; Chukwuwike, J.; Florial, E.; Lawan, H.; Felix, A.; McBenedict, B. The Pathophysiology and Vascular Complications of Diabetes in Chronic Kidney Disease: A Comprehensive Review. Cureus 2024, 16, e76498. [Google Scholar] [CrossRef] [PubMed]
- Shan, P.F.; Li, Q.; Khamaisi, M.; Qiang, G.F. Type 2 Diabetes Mellitus and Macrovascular Complications. Int J Endocrinol 2017, 2017, 4301461. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Tan, K.H.X.; Tan, C.S.; Lim, W.Y.; Tai, E.S.; Venkataraman, K. Longitudinal trends in HbA(1c) patterns and association with outcomes: A systematic review. Diabetes Metab Res Rev 2018, 34, e3015. [Google Scholar] [CrossRef]
- Li, K.; Yang, L.; Zhao, D. The relationship between HbA1c control pattern and atherosclerosis progression of diabetes: a prospective study of Chinese population. Diabetology & Metabolic Syndrome 2024, 16, 127. [Google Scholar]
- Bazzazzadehgan, S.; Shariat-Madar, Z.; Mahdi, F. Distinct Roles of Common Genetic Variants and Their Contributions to Diabetes: MODY and Uncontrolled T2DM. Biomolecules 2025, 15. [Google Scholar] [CrossRef]
- Colayco, D.C.; Niu, F.; McCombs, J.S.; Cheetham, T.C. A1C and Cardiovascular Outcomes in Type 2 Diabetes: A nested case-control study. Diabetes Care 2010, 34, 77–83. [Google Scholar] [CrossRef]
- Ahmed, Y.; Mohamed Abuelass, F.K.; Hamd Abdelwahab, S.B.; Mukhtar, M.; Ahmed, Y.; Elfahal, M.; Mohmed Elhussein, N.S. Determinants of Poor Glycemic Control Among Type 2 Diabetes Patients: A Systematic Review. Cureus 2025, 17, e82464. [Google Scholar] [CrossRef]
- Nesti, L.; Natali, A. Metformin effects on the heart and the cardiovascular system: A review of experimental and clinical data. Nutr Metab Cardiovasc Dis 2017, 27, 657–669. [Google Scholar] [CrossRef]
- Griffin, S.J.; Leaver, J.K.; Irving, G.J. Impact of metformin on cardiovascular disease: a meta-analysis of randomised trials among people with type 2 diabetes. Diabetologia 2017, 60, 1620–1629. [Google Scholar] [CrossRef] [PubMed]
- Salpeter, S.R.; Greyber, E.; Pasternak, G.A.; Salpeter, E.E. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus: systematic review and meta-analysis. Arch Intern Med 2003, 163, 2594–2602. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, B.; Wu, A.; Shin, J.I.; Sang, Y.; Alexander, G.C.; Secora, A.; Inker, L.A.; Coresh, J.; Chang, A.R.; Grams, M.E. Association of Metformin Use With Risk of Lactic Acidosis Across the Range of Kidney Function: A Community-Based Cohort Study. JAMA Intern Med 2018, 178, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Swenson, K.S.; Wang, D.; Jones, A.K.; Nash, M.J.; O’Rourke, R.; Takahashi, D.L.; Kievit, P.; Hennebold, J.D.; Aagaard, K.M.; Friedman, J.E.; Jones, K.L.; Rozance, P.J.; Brown, L.D.; Wesolowski, S.R. Metformin Disrupts Signaling and Metabolism in Fetal Hepatocytes. Diabetes 2023, 72, 1214–1227. [Google Scholar] [CrossRef]
- Tarry-Adkins, J.L.; Aiken, C.E.; Ozanne, S.E. Neonatal, infant, and childhood growth following metformin versus insulin treatment for gestational diabetes: A systematic review and meta-analysis. PLOS Medicine 2019, 16, e1002848. [Google Scholar] [CrossRef]
- Toft, J.H.; Økland, I. Metformin use in pregnancy: What about long-term effects in offspring? Acta Obstetricia et Gynecologica Scandinavica 2024, 103, 1238–1241. [Google Scholar] [CrossRef]
- European Medicine Agency Science Medicines Health. Use of metformin to treat diabetes now expanded to patients with moderately reduced kidney function. https://www.ema.europa.eu/en/medicines/human/referrals/metformin-metformin-containing-medicines#topics. Accessed October, 2016.
- Mohan, V.; Saboo, B.; Khader, J.; Modi, K.D.; Jindal, S.; Wangnoo, S.K.; Amarnath, S. Position of Sulfonylureas in the Current ERA: Review of National and International Guidelines. Clin Med Insights Endocrinol Diabetes 2022, 15, 11795514221074663. [Google Scholar] [CrossRef]
- Bahardoust, M.; Mehrabi, Y.; Hadaegh, F.; Khalili, D.; Delpisheh, A. Impact of duration of treatments with metformin and sulfonylureas, individually or in combination, on diabetic retinopathy among newly diagnosed type 2 diabetic patients: a pooled cohort’s analysis. Int J Retina Vitreous 2025, 11, 9. [Google Scholar] [CrossRef]
- Genuth, S. Should Sulfonylureas Remain an Acceptable First-Line Add-on to Metformin Therapy in Patients With Type 2 Diabetes? No, It’s Time to Move On! Diabetes Care 2014, 38, 170–175. [Google Scholar] [CrossRef]
- Lebovitz, H.E.; Feinglos, M.N. Mechanism of action of the second-generation sulfonylurea glipizide. The American Journal of Medicine 1983, 75, 46–54. [Google Scholar] [CrossRef]
- Aschner, P. New IDF clinical practice recommendations for managing type 2 diabetes in primary care. Diabetes Res Clin Pract 2017, 132, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Kolaczynski, W.M.; Hankins, M.; Ong, S.H.; Richter, H.; Clemens, A.; Toussi, M. Microvascular Outcomes in Patients with Type 2 Diabetes Treated with Vildagliptin vs. Sulfonylurea: A Retrospective Study Using German Electronic Medical Records. Diabetes therapy : research, treatment and education of diabetes and related disorders 2016, 7, 483–496. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, L.; Suissa, S. Sulfonylureas and the Risks of Cardiovascular Events and Death: A Methodological Meta-Regression Analysis of the Observational Studies. Diabetes Care 2017, 40, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.T.L.; Hui, J.M.H.; Lee, Y.H.A.; Satti, D.I.; Shum, Y.K.L.; Kiu, P.T.H.; Wai, A.K.C.; Liu, T.; Wong, W.T.; Chan, J.S.K.; Cheung, B.M.Y.; Wong, I.C.K.; Cheng, S.H.; Tse, G. Sulfonylurea Is Associated With Higher Risks of Ventricular Arrhythmia or Sudden Cardiac Death Compared With Metformin: A Population-Based Cohort Study. Journal of the American Heart Association 2022, 11, e026289. [Google Scholar] [CrossRef]
- Hau, K.T.; Mafauzy, M.; Bin, L.X. Systematic Review of Cardiovascular Outcomes with Sulfonylureas, GLP-1 RA, and DPP-4 Inhibitors in Type 2 Diabetes Mellitus. Journal of Diabetology 2024, 15, 266–272. [Google Scholar] [CrossRef]
- Gerich, J.E. Clinical significance, pathogenesis, and management of postprandial hyperglycemia. Arch Intern Med 2003, 163, 1306–1316. [Google Scholar] [CrossRef]
- Schmitz, O.; Lund, S.; Andersen, P.H.; Jønler, M.; Pørksen, N. Optimizing Insulin Secretagogue Therapy in Patients With Type 2 Diabetes: A randomized double-blind study with repaglinide. Diabetes Care 2002, 25, 342–346. [Google Scholar] [CrossRef]
- Philip, J.; Fernandez, C.J. Efficacy and Cardiovascular Safety of Meglitinides. Curr Drug Saf 2021, 16, 207–216. [Google Scholar] [CrossRef]
- DeFronzo, R.A. Pharmacologic therapy for type 2 diabetes mellitus. Ann Intern Med 1999, 131, 281–303. [Google Scholar] [CrossRef]
- Black, C.; Donnelly, P.; McIntyre, L.; Royle, P.L.; Shepherd, J.P.; Thomas, S. Meglitinide analogues for type 2 diabetes mellitus. Cochrane Database Syst Rev 2007, 2007, Cd004654. [Google Scholar] [CrossRef]
- Jovanovic, L.; Dailey, G., 3rd; Huang, W.C.; Strange, P.; Goldstein, B.J. Repaglinide in type 2 diabetes: a 24-week, fixed-dose efficacy and safety study. J Clin Pharmacol 2000, 40, 49–57. [Google Scholar]
- Schramm, T.K.; Gislason, G.H.; Vaag, A.; Rasmussen, J.N.; Folke, F.; Hansen, M.L.; Fosbøl, E.L.; Køber, L.; Norgaard, M.L.; Madsen, M.; Hansen, P.R.; Torp-Pedersen, C. Mortality and cardiovascular risk associated with different insulin secretagogues compared with metformin in type 2 diabetes, with or without a previous myocardial infarction: a nationwide study. Eur Heart J 2011, 32, 1900–1908. [Google Scholar] [CrossRef] [PubMed]
- Papa, G.; Fedele, V.; Rizzo, M.R.; Fioravanti, M.; Leotta, C.; Solerte, S.B.; Purrello, F.; Paolisso, G. Safety of Type 2 Diabetes Treatment With Repaglinide Compared With Glibenclamide in Elderly People : A randomized, open-label, two-period, cross-over trial. Diabetes Care 2006, 29, 1918–1920. [Google Scholar] [CrossRef] [PubMed]
- Kawamori, R.; Kaku, K.; Hanafusa, T.; Ioriya, K.; Kageyama, S.; Hotta, N. Clinical study of repaglinide efficacy and safety in type 2 diabetes mellitus patients with blood glucose levels inadequately controlled by sitagliptin. J Diabetes Investig 2016, 7, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-K.; Yeh, J.-I. Comparison of mortality and cardiovascular event risk associated with various insulin secretagogues: A nationwide real-world analysis. Diabetes Research and Clinical Practice 2019, 152, 103–110. [Google Scholar] [CrossRef]
- Huang, Y.; Abdelmoneim, A.S.; Light, P.; Qiu, W.; Simpson, S.H. Comparative cardiovascular safety of insulin secretagogues following hospitalization for ischemic heart disease among type 2 diabetes patients: a cohort study. Journal of Diabetes and its Complications 2015, 29, 196–202. [Google Scholar] [CrossRef]
- Soccio, R.E.; Chen, E.R.; Lazar, M.A. Thiazolidinediones and the promise of insulin sensitization in type 2 diabetes. Cell Metab 2014, 20, 573–591. [Google Scholar] [CrossRef]
- Leonard, C.E.; Han, X.; Brensinger, C.M.; Bilker, W.B.; Cardillo, S.; Flory, J.H.; Hennessy, S. Comparative risk of serious hypoglycemia with oral antidiabetic monotherapy: A retrospective cohort study. Pharmacoepidemiol Drug Saf 2018, 27, 9–18. [Google Scholar] [CrossRef]
- Bush, A.; Benny, T.; Hale, G.; Seamon, M. What is the role of pioglitazone for patients with type 2 diabetes in value-based care settings? Drugs & Therapy Perspectives 2024, 40, 131–136. [Google Scholar]
- Dormandy, J.A.; Charbonnel, B.; Eckland, D.J.; Erdmann, E.; Massi-Benedetti, M.; Moules, I.K.; Skene, A.M.; Tan, M.H.; Lefèbvre, P.J.; Murray, G.D.; Standl, E.; Wilcox, R.G.; Wilhelmsen, L.; Betteridge, J.; Birkeland, K.; Golay, A.; Heine, R.J.; Korányi, L.; Laakso, M.; Mokán, M.; Norkus, A.; Pirags, V.; Podar, T.; Scheen, A.; Scherbaum, W.; Schernthaner, G.; Schmitz, O.; Skrha, J.; Smith, U.; Taton, J. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet 2005, 366, 1279–1289. [Google Scholar] [CrossRef]
- Kernan, W.N.; Viscoli, C.M.; Furie, K.L.; Young, L.H.; Inzucchi, S.E.; Gorman, M.; Guarino, P.D.; Lovejoy, A.M.; Peduzzi, P.N.; Conwit, R.; Brass, L.M.; Schwartz, G.G.; Adams, H.P., Jr.; Berger, L.; Carolei, A.; Clark, W.; Coull, B.; Ford, G.A.; Kleindorfer, D.; O’Leary, J.R.; Parsons, M.W.; Ringleb, P.; Sen, S.; Spence, J.D.; Tanne, D.; Wang, D.; Winder, T.R. Pioglitazone after Ischemic Stroke or Transient Ischemic Attack. N Engl J Med 2016, 374, 1321–1331. [Google Scholar] [CrossRef]
- Daza-Arnedo, R.; Rico-Fontalvo, J.-E.; Pájaro-Galvis, N.; Leal-Martínez, V.; Abuabara-Franco, E.; Raad-Sarabia, M.; Montejo-Hernández, J.; Cardona-Blanco, M.; Cabrales-Juan, J.; Uparella-Gulfo, I.; Montiel, L.S. Dipeptidyl Peptidase-4 Inhibitors and Diabetic Kidney Disease: A Narrative Review. Kidney Medicine 2021, 3, 1065–1073. [Google Scholar] [CrossRef]
- Mulvihill, E.E.; Drucker, D.J. Pharmacology, physiology, and mechanisms of action of dipeptidyl peptidase-4 inhibitors. Endocr Rev 2014, 35, 992–1019. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, V.A. New developments in diabetes management: medications of the 21st century. Clin Ther 2014, 36, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.A.; Meier, J.J. Incretin hormones: Their role in health and disease. Diabetes Obes Metab 2018, 20 Suppl 1, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Deacon, C.F. Peptide degradation and the role of DPP-4 inhibitors in the treatment of type 2 diabetes. Peptides 2018, 100, 150–157. [Google Scholar] [CrossRef]
- Bayanati, M.; Ismail Mahboubi Rabbani, M.; Sirous Kabiri, S.; Mir, B.; Rezaee, E.; Tabatabai, S.A. Dipeptidyl Peptidase-4 Inhibitors: A Systematic Review of Structure-Activity Relationship Studies. Iran J Pharm Res 2024, 23, e151581. [Google Scholar] [CrossRef]
- Scheen, A.J. DPP-4 inhibitors in the management of type 2 diabetes: A critical review of head-to-head trials. Diabetes & Metabolism 2012, 38, 89–101. [Google Scholar]
- Green, J.B.; Bethel, M.A.; Armstrong, P.W.; Buse, J.B.; Engel, S.S.; Garg, J.; Josse, R.; Kaufman, K.D.; Koglin, J.; Korn, S.; Lachin, J.M.; McGuire, D.K.; Pencina, M.J.; Standl, E.; Stein, P.P.; Suryawanshi, S.; Van de Werf, F.; Peterson, E.D.; Holman, R.R. Effect of Sitagliptin on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2015, 373, 232–242. [Google Scholar] [CrossRef]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; Cavender, M.A.; Udell, J.A.; Desai, N.R.; Mosenzon, O.; McGuire, D.K.; Ray, K.K.; Leiter, L.A.; Raz, I. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013, 369, 1317–1326. [Google Scholar] [CrossRef]
- Mannucci, E.; Mosenzon, O.; Avogaro, A. Analyses of Results From Cardiovascular Safety Trials With DPP-4 Inhibitors: Cardiovascular Outcomes, Predefined Safety Outcomes, and Pooled Analysis and Meta-analysis. Diabetes Care 2016, 39, (Supplement_2), S196-S204.
- BERRA, C.C.; MANFRINI, R.; GHELARDI, R.; BOLLATI, P.M.; BUCCIARELLI, L.; MIRANI, M.; MURATORI, M.; FOLLI, F.; GROUP, A.S. 367-P: Cardiovascular Risk Categories in Patients with Diabetes According to 2019 ESC/EASD Guidelines in Clinical Practice: Use of a Dedicated App (AWARE). Diabetes 2021, 70, (Supplement_1).
- Baggio, L.L.; Drucker, D.J. Biology of incretins: GLP-1 and GIP. Gastroenterology 2007, 132, 2131–2157. [Google Scholar] [CrossRef]
- Zhao, X.; Wang, M.; Wen, Z.; Lu, Z.; Cui, L.; Fu, C.; Xue, H.; Liu, Y.; Zhang, Y. GLP-1 Receptor Agonists: Beyond Their Pancreatic Effects. Front Endocrinol (Lausanne) 2021, 12, 721135. [Google Scholar] [CrossRef]
- Drucker, D.J. The biology of incretin hormones. Cell Metab 2006, 3, 153–165. [Google Scholar] [CrossRef]
- Wen, S.; Yuan, Y.; Li, Y.; Xu, C.; Chen, L.; Ren, Y.; Wang, C.; He, Y.; Li, X.; Gong, M.; Yuan, X.; Xu, D.; Wang, C.; Zhou, L. The effects of non-insulin anti-diabetic medications on the diabetic microvascular complications: a systematic review and meta-analysis of randomized clinical trials. BMC Endocr Disord 2025, 25, 179. [Google Scholar]
- Lopaschuk, G.D.; Verma, S. Mechanisms of Cardiovascular Benefits of Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitors: A State-of-the-Art Review. JACC Basic Transl Sci 2020, 5, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Natale, P.; Tunnicliffe, D.J.; Toyama, T.; Palmer, S.C.; Saglimbene, V.M.; Ruospo, M.; Gargano, L.; Stallone, G.; Gesualdo, L.; Strippoli, G.F. Sodium-glucose co-transporter protein 2 (SGLT2) inhibitors for people with chronic kidney disease and diabetes. Cochrane Database Syst Rev 2024, 5, Cd015588. [Google Scholar] [PubMed]
- Chen, J.-Y.; Hsu, T.-W.; Liu, J.-H.; Pan, H.-C.; Lai, C.-F.; Yang, S.-Y.; Wu, V.-C. Kidney and Cardiovascular Outcomes Among Patients With CKD Receiving GLP-1 Receptor Agonists: A Systematic Review and Meta-Analysis of Randomized Trials. American Journal of Kidney Diseases 2025, 85, 555–569.e1. [Google Scholar] [CrossRef]
- Merovci, A.; Mari, A.; Solis-Herrera, C.; Xiong, J.; Daniele, G.; Chavez-Velazquez, A.; Tripathy, D.; Urban McCarthy, S.; Abdul-Ghani, M.; DeFronzo, R.A. Dapagliflozin lowers plasma glucose concentration and improves β-cell function. J Clin Endocrinol Metab 2015, 100, 1927–1932. [Google Scholar] [CrossRef]
- Packer, M. Mechanisms of enhanced renal and hepatic erythropoietin synthesis by sodium-glucose cotransporter 2 inhibitors. Eur Heart J 2023, 44, 5027–5035. [Google Scholar] [CrossRef]
- Hess, D.A.; Terenzi, D.C.; Trac, J.Z.; Quan, A.; Mason, T.; Al-Omran, M.; Bhatt, D.L.; Dhingra, N.; Rotstein, O.D.; Leiter, L.A.; Zinman, B.; Sabongui, S.; Yan, A.T.; Teoh, H.; Mazer, C.D.; Connelly, K.A.; Verma, S. SGLT2 Inhibition with Empagliflozin Increases Circulating Provascular Progenitor Cells in People with Type 2 Diabetes Mellitus. Cell Metabolism 2019, 30, 609–613. [Google Scholar] [CrossRef]
- Le, T.N.; Bright, R.; Truong, V.-K.; Li, J.; Juneja, R.; Vasilev, K. Key biomarkers in type 2 diabetes patients: A systematic review. Diabetes, Obesity and Metabolism 2025, 27, 7–22. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, S.P.; McCann, D.; Desai, M.; Rosenbaum, M.; Leibel, R.L.; Ferrante, A.W., Jr. Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest 2003, 112, 1796–1808. [Google Scholar] [CrossRef]
- Gabay, C. Interleukin-6 and chronic inflammation. Arthritis Research & Therapy 2006, 8, S3. [Google Scholar]
- Donath, M.Y.; Shoelson, S.E. Type 2 diabetes as an inflammatory disease. Nature Reviews Immunology 2011, 11, 98–107. [Google Scholar] [CrossRef]
- Singh, B.; Goyal, A.; Patel, B.C. C-Reactive Protein: Clinical Relevance and Interpretation. In StatPearls, StatPearls Publishing.
- Copyright © 2025, StatPearls Publishing LLC.: Treasure Island (FL), 2025.
- Rees, R.F.; Gewurz, H.; Siegel, J.N.; Coon, J.; Potempa, L.A. Expression of a C-reactive protein neoantigen (neo-CRP) in inflamed rabbit liver and muscle. Clin Immunol Immunopathol 1988, 48, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Khreiss, T.; József, L.; Potempa, L.A.; Filep, J.G. Opposing Effects of C-Reactive Protein Isoforms on Shear-Induced Neutrophil-Platelet Adhesion and Neutrophil Aggregation in Whole Blood. Circulation 2004, 110, 2713–2720. [Google Scholar] [CrossRef]
- Eisenhardt, S.U.; Habersberger, J.; Murphy, A.; Chen, Y.-C.; Woollard, K.J.; Bassler, N.; Qian, H.; von zur Muhlen, C.; Hagemeyer, C.E.; Ahrens, I.; Chin-Dusting, J.; Bobik, A.; Peter, K. Dissociation of Pentameric to Monomeric C-Reactive Protein on Activated Platelets Localizes Inflammation to Atherosclerotic Plaques. Circulation Research 2009, 105, 128–137. [Google Scholar] [CrossRef]
- Ji, S.-R.; Ma, L.; Bai, C.-J.; Shi, J.-M.; Li, H.-Y.; Potempa, L.A.; Filep, J.G.; Zhao, J.; Wu, Y. Monomeric C-reactive protein activates endothelial cells via interaction with lipid raft microdomains. The FASEB Journal 2009, 23, 1806–1816. [Google Scholar] [CrossRef]
- Bowker, N.; Shah, R.L.; Sharp, S.J.; Luan, J. a.; Stewart, I.D.; Wheeler, E.; Ferreira, M.A.R.; Baras, A.; Wareham, N.J.; Langenberg, C.; Lotta, L.A. Meta-analysis investigating the role of interleukin-6 mediated inflammation in type 2 diabetes. eBioMedicine 2020, 61. [Google Scholar] [CrossRef]
- Lee, C.C.; Adler, A.I.; Sandhu, M.S.; Sharp, S.J.; Forouhi, N.G.; Erqou, S.; Luben, R.; Bingham, S.; Khaw, K.T.; Wareham, N.J. Association of C-reactive protein with type 2 diabetes: prospective analysis and meta-analysis. Diabetologia 2009, 52, 1040–1047. [Google Scholar] [CrossRef]
- Anness, A.R.; Baldo, A.; Webb, D.R.; Khalil, A.; Robinson, T.G.; Mousa, H.A. Effect of metformin on biomarkers of placental- mediated disease: A systematic review and meta-analysis. Placenta 2021, 107, 51–58. [Google Scholar] [CrossRef]
- Wang, W.; Lo, A.C.Y. Diabetic Retinopathy: Pathophysiology and Treatments. Int J Mol Sci 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Al-Shabrawey, M.; Zhang, W.; McDonald, D. Diabetic retinopathy: mechanism, diagnosis, prevention, and treatment. Biomed Res Int 2015, 2015, 854593. [Google Scholar] [CrossRef] [PubMed]
- Mapanga, R.F.; Essop, M.F. Damaging effects of hyperglycemia on cardiovascular function: spotlight on glucose metabolic pathways. American Journal of Physiology-Heart and Circulatory Physiology 2016, 310, H153–H173. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wu, J.; Li, Z.; Han, J.; Xia, P.; Shen, Y.; Ma, J.; Liu, X.; Zhang, J.; Yu, P. Advances in the study of RNA-binding proteins in diabetic complications. Molecular Metabolism 2022, 62, 101515. [Google Scholar] [CrossRef]
- Duh, E.J.; Sun, J.K.; Stitt, A.W. Diabetic retinopathy: current understanding, mechanisms, and treatment strategies. JCI Insight 2017, 2. [Google Scholar] [CrossRef]
- Kropp, M.; Golubnitschaja, O.; Mazurakova, A.; Koklesova, L.; Sargheini, N.; Vo, T.K.S.; de Clerck, E.; Polivka, J., Jr.; Potuznik, P.; Polivka, J.; Stetkarova, I.; Kubatka, P.; Thumann, G. Diabetic retinopathy as the leading cause of blindness and early predictor of cascading complications-risks and mitigation. Epma j 2023, 14, 21–42. [Google Scholar] [CrossRef]
- Jeng-Miller, K.W.; Baumal, C.R. Chapter 5 - Genetics of Diabetic Retinopathy. In Current Management of Diabetic Retinopathy, Baumal, C.R.; Duker, J.S., Eds. Elsevier: 2018; pp 37-40.
- Gupta, S.; Thool, A.R. A Narrative Review of Retinopathy in Diabetic Patients. Cureus 2024, 16, e52308. [Google Scholar] [CrossRef]
- Fujiwara, T.; Takeda, N.; Hara, H.; Ishii, S.; Numata, G.; Tokiwa, H.; Katoh, M.; Maemura, S.; Suzuki, T.; Takiguchi, H.; Yanase, T.; Kubota, Y.; Nomura, S.; Hatano, M.; Ueda, K.; Harada, M.; Toko, H.; Takimoto, E.; Akazawa, H.; Morita, H.; Nishimura, S.; Komuro, I. PGC-1α–mediated angiogenesis prevents pulmonary hypertension in mice. JCI Insight 2023, 8. [Google Scholar] [CrossRef]
- Cunningham, K.F.; Beeson, G.C.; Beeson, C.C.; Baicu, C.F.; Zile, M.R.; McDermott, P.J. Estrogen-Related Receptor α (ERRα) is required for adaptive increases in PGC-1 isoform expression during electrically stimulated contraction of adult cardiomyocytes in sustained hypoxic conditions. International Journal of Cardiology 2015, 187, 393–400. [Google Scholar]
- Shoag, J.; Arany, Z. Regulation of Hypoxia-Inducible Genes by PGC-1α. Arteriosclerosis, Thrombosis, and Vascular Biology 2010, 30, 662–666. [Google Scholar] [PubMed]
- Willy, P.J.; Murray, I.R.; Qian, J.; Busch, B.B.; Stevens, W.C.; Martin, R.; Mohan, R.; Zhou, S.; Ordentlich, P.; Wei, P.; Sapp, D.W.; Horlick, R.A.; Heyman, R.A.; Schulman, I.G. Regulation of PPARγ coactivator 1α (PGC-1α) signaling by an estrogen-related receptor α (ERRα) ligand. Proceedings of the National Academy of Sciences 2004, 101, 8912–8917. [Google Scholar] [CrossRef] [PubMed]
- Abu El-Asrar, A.M.; Nawaz, M.I.; Ahmad, A.; Siddiquei, M.M.; Allegaert, E.; Gikandi, P.W.; De Hertogh, G.; Opdenakker, G. A key role of the PGC-1alpha/ERR-alpha pathway in regulation of angiogenic factors in proliferative diabetic retinopathy. Front Endocrinol (Lausanne) 2025, 16, 1615103. [Google Scholar] [CrossRef] [PubMed]
- Jonas, J.B.; Neumaier, M. Erythropoietin levels in aqueous humour in eyes with exudative age-related macular degeneration and diabetic retinopathy. Clin Exp Ophthalmol 2007, 35, 186–187. [Google Scholar] [CrossRef]
- Sherwin, A.A.R.; Jayashree, K.; Senthilkumar, G.P.; Thomas, S.E.; Babu, K.R. An Assessment of Serum Irisin and Intercellular Adhesion Molecule-1 as Potential Indicators of Retinopathy in Type 2 Diabetes Mellitus. Niger Postgrad Med J 2025, 32, 240–246. [Google Scholar]
- Zheng, Z.; Liu, N.; Zhang, Y.; Gu, X.; Li, H.; Yu, X. Postprandial C-Peptide to Glucose Ratio as a Promising Systemic Marker of Diabetic Retinopathy in Type 2 Diabetes. Transl Vis Sci Technol 2025, 14, 27. [Google Scholar]
- Wei, Z.M.; Zhao, Y.; Ding, R.R.; Zeng, Y.S.; Zeng, Z.; He, Z.T.; Hao, J.; Hu, J.J.; Yu, J.G.; You, C.Y. Combination of red blood cell distribution width and platelet-to-lymphocyte ratio for predicting severity of diabetic retinopathy. Int J Ophthalmol 2025, 18, 1506–1514. [Google Scholar]
- Li, Z.; Ren, Y.; Jiang, F.; Zhang, K.; Meng, X.; Zheng, Y.; He, M. Unveiling biomarkers via plasma metabolome profiling for diabetic macrovascular and microvascular complications. Cardiovasc Diabetol 2025, 24, 341. [Google Scholar]
- Jadhav, S.A.; Benedikter, B.J.; Mokhtar, S.B.A.; van der Heide, F.C.T.; Kumaramanickavel, G.; van Greevenbroek, M.M.J.; Webers, C.A.B.; Berendschot, T. Plasma Sphingomyelins as Biomarkers for Diabetic Retinal Neurodegeneration: The Maastricht Study. Ophthalmol Sci 2025, 5, 100870. [Google Scholar] [CrossRef]
- Hao, Y.; She, X.; Huang, G.; Chu, X.; Zhao, S.; Lv, Z.; Tao, J.; Zhang, Y. Metabolomic insights into vitreous humor with therapy outcome in type 2 diabetic retinopathy. BMC Ophthalmol 2025, 25, 460. [Google Scholar]
- Zooravar, D.; Shojaei, S.; Mousavi, A.; Soltani, P.; Amiri, B.S.; Radkhah, H. Novel Lipid Biomarkers and Microvascular Complications in Patients with Diabetes Mellitus: A Systematic Review and Meta-analysis. Clin Med Insights Endocrinol Diabetes 2025, 18, 11795514251365301. [Google Scholar]
- Cao, D.; Yang, Q.; Hong, Y.; Tan, R.; Ibrahim, F.N.I.; Lim, C.; Choo, J.; Sabanayagam, C.; Coffman, T.M.; Wong, T.Y.; Tan, G.S.W. Retinal Neuronal Changes and Kidney Dysfunction in Diabetes Mellitus. Clin Exp Ophthalmol 2025. [Google Scholar] [CrossRef]
- Conserva, F.; Gesualdo, L.; Papale, M. A Systems Biology Overview on Human Diabetic Nephropathy: From Genetic Susceptibility to Post-Transcriptional and Post-Translational Modifications. Journal of Diabetes Research 2016, 2016, 7934504. [Google Scholar] [CrossRef]
- Childs, B.P. Diabetic Nephropathy and End-Stage Renal Disease. In Complete Nurse’s Guide to Diabetes Care, Childs, B.P.; Cypress, M.; Spollett, G.R., Eds. American Diabetes Association: p 0.
- Agarwal, R. Pathogenesis of Diabetic Nephropathy. Compendia 2021, 2021, 2–7. [Google Scholar] [CrossRef]
- Natesan, V.; Kim, S.J. Diabetic Nephropathy - a Review of Risk Factors, Progression, Mechanism, and Dietary Management. Biomol Ther (Seoul) 2021, 29, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Hostetter, T.H.; Rennke, H.G.; Brenner, B.M. The case for intrarenal hypertension in the initiation and progression of diabetic and other glomerulopathies. Am J Med 1982, 72, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Ding, L.; Andoh, V.; Zhang, J.; Chen, L. The Mechanism of Hyperglycemia-Induced Renal Cell Injury in Diabetic Nephropathy Disease: An Update. Life (Basel) 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.; Zhang, Y.; Fang, X.; Zhang, Y.; Miao, R.; Yao, Y.; Guan, H.; Tian, J. Discovering diabetes complications-related microRNAs: meta-analyses and pathway modeling approach. BMC Med Genomics 2025, 18, 86. [Google Scholar] [CrossRef]
- Abdel-Tawab, M.S.; Mohamed, M.G.; Doudar, N.A.; Rateb, E.E.; Reyad, H.R.; Elazeem, N.A.A. Circulating hsa-miR-221 as a possible diagnostic and prognostic biomarker of diabetic nephropathy. Mol Biol Rep 2023, 50, 9793–9803. [Google Scholar] [CrossRef]
- Abdelgayed, G.; Hosni, A.; Abdel-Moneim, A.; Malik, A.; Zaky, M.Y.; Hasona, N.A. Integrated analysis of long non-coding RNA megacluster, microRNA-132 and microRNA-133a and their implications for cardiovascular risk and kidney failure progression in diabetic patients. Exp Ther Med 2025, 29, 35. [Google Scholar] [CrossRef]
- Januzzi, J.L., Jr.; Liu, Y.; Sattar, N.; Yavin, Y.; Pollock, C.A.; Butler, J.; Jardine, M.; Heerspink, H.J.L.; Masson, S.; Breyer, M.; Hansen, M.K. Vascular endothelial growth factors and risk of cardio-renal events: Results from the CREDENCE trial. Am Heart J 2024, 271, 38–47. [Google Scholar]
- Kralisch, S.; Fasshauer, M. Adipocyte fatty acid binding protein: a novel adipokine involved in the pathogenesis of metabolic and vascular disease? Diabetologia 2013, 56, 10–21. [Google Scholar]
- Xie, T.; Leung, P.S. Fibroblast growth factor 21: a regulator of metabolic disease and health span. Am J Physiol Endocrinol Metab 2017, 313, E292–e302. [Google Scholar]
- Wang, Y.; Liu, X.; Quan, X.; Qin, X.; Zhou, Y.; Liu, Z.; Chao, Z.; Jia, C.; Qin, H.; Zhang, H. Pigment epithelium-derived factor and its role in microvascular-related diseases. Biochimie 2022, 200, 153–171. [Google Scholar] [PubMed]
- Cheung, C.Y.Y.; Lee, C.-H.; Tang, C.S.; Xu, A.; Au, K.-W.; Fong, C.H.Y.; Ng, K.K.K.; Kwok, K.H.M.; Chow, W.-S.; Woo, Y.-C.; Yuen, M.M.A.; Hai, J.; Tan, K.C.B.; Lam, T.-H.; Tse, H.-F.; Sham, P.-C.; Lam, K.S.L. Genetic Regulation of Pigment Epithelium-Derived Factor (PEDF): An Exome-Chip Association Analysis in Chinese Subjects With Type 2 Diabetes. Diabetes 2018, 68, 198–206. [Google Scholar] [PubMed]
- Sbriscia, M.; Caccese, S.; Marchegiani, F.; Recchioni, R.; Matacchione, G.; Giordani, C.; Francini, E.; Salvioli, S.; Conte, M.; Landolfo, M.; Bonfigli, A.R.; Turchi, F.; Sabbatinelli, J.; Olivieri, F.; Giuliani, A. A scoring model integrating CXCL9, GDF15, FGF21, and NfL, predicts long-term mortality in type 2 diabetes: a retrospective study. Cardiovasc Diabetol 2025, 24, 270. [Google Scholar] [PubMed]
- van Heck, J.I.P.; Ajie, M.; Joosten, L.A.B.; Tack, C.J.; Stienstra, R. Circulating inflammatory proteins are elevated in type 1 and type 2 diabetes and associated to complications. Diabetes Obes Metab 2025, 27, 719–728. [Google Scholar]
- AlMajed, H.T.; Abu-Farha, M.; Alshawaf, E.; Devarajan, S.; Alsairafi, Z.; Elhelaly, A.; Cherian, P.; Al-Khairi, I.; Ali, H.; Jose, R.M.; Thanaraj, T.A.; Al-Ozairi, E.; Al-Mulla, F.; Al Attar, A.; Abubaker, J. Increased Levels of Circulating IGFBP4 and ANGPTL8 with a Prospective Role in Diabetic Nephropathy. Int J Mol Sci 2023, 24. [Google Scholar]
- Zhang, X.; Zhou, C.G.; Ma, L.J. Role of GDF-15 in diabetic nephropathy: mechanisms, diagnosis, and therapeutic potential. Int Urol Nephrol 2025, 57, 169–175. [Google Scholar] [CrossRef]
- Hou, Q.; Huang, K.; Liang, Y.; Yu, W.; Long, L.; Wang, K.; Yi, B. Associations between serum JAML, nesfatin-1, and 25(OH)D and the risk of diabetic kidney disease in patients with type 2 diabetes. Sci Rep 2025, 15, 27438. [Google Scholar]
- Bourgonje, A.R.; van Goor, H.; Bakker, S.J.L.; Hillebrands, J.L.; Bilo, H.J.G.; Dullaart, R.P.F.; van Dijk, P.R. Serum peroxiredoxin-4, a biomarker of oxidative stress, is associated with the development of nephropathy in patients with type 2 diabetes (Zodiac-65). Free Radic Biol Med 2024, 212, 186–190. [Google Scholar] [CrossRef]
- Ghareghani, O.; Ghareghani, S.; Takhshid, M.A. Diagnostic values of ischemia modified albumin in diabetes-related complications: a narrative review. J Diabetes Metab Disord 2023, 22, 35–46. [Google Scholar] [CrossRef]
- Spoto, B.; Politi, C.; Pizzini, P.; Parlongo, R.M.; Testa, A.; Mobrici, M.; Tripepi, G.L.; Mallamaci, F.; Zoccali, C. 8-hydroxy-2’-deoxyguanosine, a biomarker of oxidative DNA injury, in diabetic kidney disease. Nutr Metab Cardiovasc Dis 2025, 35, 103722. [Google Scholar] [CrossRef]
- Roointan, A.; Shafieizadegan, S.; Ghaeidamini, M.; Gheisari, Y.; Hudkins, K.L.; Gholaminejad, A. The potential of cardiac biomarkers, NT-ProBNP and troponin T, in predicting the progression of nephropathy in diabetic patients: A meta-analysis of prospective cohort studies. Diabetes Res Clin Pract 2023, 204, 110900. [Google Scholar] [CrossRef]
- Yagihashi, S.; Mizukami, H.; Sugimoto, K. Mechanism of diabetic neuropathy: Where are we now and where to go? J Diabetes Investig 2011, 2, 18–32. [Google Scholar] [CrossRef]
- Ferris, J.K.; Inglis, J.T.; Madden, K.M.; Boyd, L.A. Brain and Body: A Review of Central Nervous System Contributions to Movement Impairments in Diabetes. Diabetes 2019, 69, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Erus, G.; Battapady, H.; Zhang, T.; Lovato, J.; Miller, M.E.; Williamson, J.D.; Launer, L.J.; Bryan, R.N.; Davatzikos, C. Spatial patterns of structural brain changes in type 2 diabetic patients and their longitudinal progression with intensive control of blood glucose. Diabetes care 2015, 38, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Kawamura, N.; Dyck, P.J.; Dyck, P.J.B.; Kihara, M.; Low, P.A. Spectrum of diabetic neuropathies. Diabetol Int 2020, 11, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.Y.; Lee, M.K. Autonomic dysfunction, diabetes and metabolic syndrome. J Diabetes Investig 2021, 12, 2108–2111. [Google Scholar] [CrossRef]
- Serhiyenko, V.A.; Serhiyenko, A.A. Cardiac autonomic neuropathy: Risk factors, diagnosis and treatment. World J Diabetes 2018, 9, 1–24. [Google Scholar] [CrossRef]
- Itani, M.; Gylfadottir, S.S.; Krøigård, T.; Kristensen, A.G.; Christensen, D.H.; Karlsson, P.; Möller, S.; Andersen, H.; Tankisi, H.; Nielsen, J.S.; Jensen, T.S.; Thomsen, R.W.; Finnerup, N.B.; Sindrup, S.H. Small and large fiber sensory polyneuropathy in type 2 diabetes: Influence of diagnostic criteria on neuropathy subtypes. Journal of the Peripheral Nervous System 2021, 26, 55–65. [Google Scholar]
- Li, Y.; Wu, W.; Xue, L.; Zhao, T.; Lu, Y.; Qiao, X.; Ding, H. Plantar Tissue Characteristics in People With Diabetes With and Without Peripheral Neuropathy: A Novel Explanatory Model for DPN Risk Assessment. J Diabetes 2025, 17, e70094. [Google Scholar] [CrossRef] [PubMed]
- Ascaso, P.; Palanca, A.; Martinez-Hervas, S.; Sanz, M.J.; Ascaso, J.F.; Piqueras, L.; Real, J.T. Peripheral blood levels of CXCL10 are a useful marker for diabetic polyneuropathy in subjects with type 2 diabetes. Int J Clin Pract 2021, 75, e14302. [Google Scholar] [PubMed]
- Mondal, A.; Bose, C.; Pramanik, S.; Dash, D.; Mukherjee, B.; Malik, R.A.; Mukhopadhyay, S. Circulating netrin-1 levels are reduced and related to corneal nerve fiber loss in patients with diabetic neuropathy. J Diabetes Investig 2024, 15, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Wang, K.K.W. Glial fibrillary acidic protein: from intermediate filament assembly and gliosis to neurobiomarker. Trends in Neurosciences 2015, 38, 364–374. [Google Scholar] [CrossRef]
- Bishop, P.; Rocca, D.; Henley, J.M. Ubiquitin C-terminal hydrolase L1 (UCH-L1): structure, distribution and roles in brain function and dysfunction. Biochem J 2016, 473, 2453–2462. [Google Scholar] [CrossRef]
- Hviid, C.V.B.; Rasmussen, N.H.; Roikjer, J. Glial fibrillary acidic protein: a potential biomarker for small fiber neuropathy? Acta Diabetol 2025. [Google Scholar]
- Khalid, M.; Petroianu, G.; Adem, A. Advanced Glycation End Products and Diabetes Mellitus: Mechanisms and Perspectives. Biomolecules 2022, 12. [Google Scholar] [CrossRef]
- Chen, Y.; Meng, Z.; Li, Y.; Liu, S.; Hu, P.; Luo, E. Advanced glycation end products and reactive oxygen species: uncovering the potential role of ferroptosis in diabetic complications. Molecular Medicine 2024, 30, 141. [Google Scholar]
- Jakhotia, S.; Sivaprasad, M.; Shalini, T.; Reddy, P.Y.; Viswanath, K.; Jakhotia, K.; Sahay, R.; Sahay, M.; Reddy, G.B. Circulating levels of Hsp27 in microvascular complications of diabetes: Prospects as a biomarker of diabetic nephropathy. J Diabetes Complications 2018, 32, 221–225. [Google Scholar]
- Matuschik, L.; Riabov, V.; Schmuttermaier, C.; Sevastyanova, T.; Weiss, C.; Klüter, H.; Kzhyshkowska, J. Hyperglycemia Induces Inflammatory Response of Human Macrophages to CD163-Mediated Scavenging of Hemoglobin-Haptoglobin Complexes. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Le Jeune, S.; Sadoudi, S.; Charue, D.; Abid, S.; Guigner, J.M.; Helley, D.; Bihan, H.; Baudry, C.; Lelong, H.; Mirault, T.; Vicaut, E.; Dhote, R.; Mourad, J.J.; Boulanger, C.M.; Blanc-Brude, O.P. Low grade intravascular hemolysis associates with peripheral nerve injury in type 2 diabetes. PLoS One 2022, 17, e0275337. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.; Wang, J.; Tian, J.; Tang, Y.-d. Coronary Artery Disease: From Mechanism to Clinical Practice. In Coronary Artery Disease: Therapeutics and Drug Discovery, Wang, M., Ed. Springer Singapore: Singapore, 2020; pp 1-36.
- Dziopa, K.; Chaturvedi, N.; Asselbergs, F.W.; Schmidt, A.F. Identifying and ranking non-traditional risk factors for cardiovascular disease prediction in people with type 2 diabetes. Commun Med (Lond) 2025, 5, 77. [Google Scholar] [CrossRef] [PubMed]
- Morales-Villegas, E. Dyslipidemia, Hypertension and Diabetes Metaflammation. A Unique Mechanism for 3 Risk Factors. Curr Hypertens Rev 2014. [Google Scholar] [CrossRef]
- Jacoby, R.M.; Nesto, R.W. Acute myocardial infarction in the diabetic patient: Pathophysiology, clinical course and prognosis. Journal of the American College of Cardiology 1992, 20, 736–744. [Google Scholar] [CrossRef]
- Karakasis, P.; Theofilis, P.; Patoulias, D.; Vlachakis, P.K.; Antoniadis, A.P.; Fragakis, N. Diabetes-Driven Atherosclerosis: Updated Mechanistic Insights and Novel Therapeutic Strategies. Int J Mol Sci 2025, 26. [Google Scholar] [CrossRef]
- John, J.E.; Claggett, B.; Skali, H.; Solomon, S.D.; Cunningham, J.W.; Matsushita, K.; Konety, S.H.; Kitzman, D.W.; Mosley, T.H.; Clark, D.; Chang, P.P.; Shah, A.M. Coronary Artery Disease and Heart Failure With Preserved Ejection Fraction: The ARIC Study. Journal of the American Heart Association 2022, 11, e021660. [Google Scholar] [CrossRef]
- Braunwald, E.; Morrow, D.A. Unstable Angina. Circulation 2013, 127, 2452–2457. [Google Scholar] [CrossRef]
- Lange, R.A. Chapter 15 - Chronic Stable Angina. In Cardiology Secrets (Fifth Edition), Levine, G.N., Ed. Elsevier: 2018; pp 135-142.
- Kannel, W.B.; McGee, D.L. Diabetes and cardiovascular disease. The Framingham study. Jama 1979, 241, 2035–2038. [Google Scholar] [CrossRef]
- Wu, S.; Wu, Y.; Ning, Y.; Peng, X.; Zhao, H.; Feng, J.; Lin, L.; Ruan, C.; Chen, S.; Tian, J.; Jin, C. Modifiable Factors and 10-Year and Lifetime Risk of Cardiovascular Disease in Adults With New-Onset Diabetes: The Kailuan Cohort Study. Journal of the American Heart Association 2025, 14, e041223. [Google Scholar] [CrossRef]
- Jasaszwili, M.; Billert, M.; Strowski, M.Z.; Nowak, K.W.; Skrzypski, M. Adropin as A Fat-Burning Hormone with Multiple Functions-Review of a Decade of Research. Molecules 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Mushala, B.A.S.; Scott, I. Adropin: a hepatokine modulator of vascular function and cardiac fuel metabolism. Am J Physiol Heart Circ Physiol 2021, 320, H238–h244. [Google Scholar] [CrossRef] [PubMed]
- Berezina, T.A.; Berezin, O.O.; Novikov, E.V.; Berezin, A.E. The Association of Adropin with Asymptomatic Coronary Calcification in Patients in Early Stages of Chronic Kidney Disease. Int J Mol Sci 2025, 26. [Google Scholar] [CrossRef]
- Yang, C.; Zhu, C.G.; Guo, Y.L.; Wu, N.Q.; Dong, Q.; Xu, R.X.; Wu, Y.J.; Qian, J.; Li, J.J. Prognostic Value of Plasma Endothelin-1 in Predicting Worse Outcomes in Patients with Prediabetes and Diabetes and Stable Coronary Artery Diseases. Diabetes Metab J 2024, 48, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Boieriu, A.M.; Luca, C.D.; Neculoiu, C.D.; Bisoc, A.; Tint, D. Endothelial Dysfunction and Oxidative Stress in Patients with Severe Coronary Artery Disease: Does Diabetes Play a Contributing Role? Medicina (Kaunas) 2025, 61. [Google Scholar] [CrossRef]
- Hwang, D.; Park, S.-H.; Koo, B.-K. Ischemia With Nonobstructive Coronary Artery Disease. JACC: Asia 2023, 3, 169–184. [Google Scholar] [CrossRef]
- Ferrone, M.; Ciccarelli, M.; Varzideh, F.; Kansakar, U.; Guerra, G.; Cerasuolo, F.A.; Buonaiuto, A.; Fiordelisi, A.; Venga, E.; Esposito, M.; Rainone, A.; Ricciardi, R.; Del Giudice, C.; Minicucci, F.; Tesorio, T.; Visco, V.; Iaccarino, G.; Gambardella, J.; Santulli, G.; Mone, P. Endothelial microRNAs in INOCA patients with diabetes mellitus. Cardiovasc Diabetol 2024, 23, 268. [Google Scholar] [CrossRef]
- Zuo, Y.; NaveenKumar, S.K.; Navaz, S.; Liang, W.; Sugur, K.; Kmetova, K.; Ayers, C.R.; Kluge, L.; Chong, E.; Shah, A.M.; Rohatgi, A.; Berry, J.D.; Knight, J.S.; de Lemos, J.A. Epidemiological and Translational Study of Calprotectin and Atherosclerotic Cardiovascular Disease. JAMA Cardiol 2025, 10, 718–727. [Google Scholar] [CrossRef]
- Carnazzo, V.; Redi, S.; Basile, V.; Natali, P.; Gulli, F.; Equitani, F.; Marino, M.; Basile, U. Calprotectin: two sides of the same coin. Rheumatology (Oxford) 2024, 63, 26–33. [Google Scholar] [CrossRef]
- Gigante, B.; Chen, Q.; Bjorkbacka, H.; Bjornson, E.; Brinck, J.; Chorell, E.; Djekic, D.; Edsfeldt, A.; Engstrom, G.; Eriksson, J.W.; Gottsater, A.; Gummesson, A.; Hagstrom, E.; Hedin, U.; Jernberg, T.; Johnston, N.; Nilsson, L.; Nystrom, F.; Otten, J.; Rosengren, A.; Soderberg, S.; Haglow, J.T.; Ostgren, C.J. Lipoproteins and lipoprotein lipid composition are associated with stages of dysglycemia and subclinical coronary atherosclerosis. Int J Cardiol 2025, 419, 132698. [Google Scholar] [CrossRef]
- Le Goff, W.; Bourron, O.; Materne, C.; Galier, S.; Phan, F.; Tan-Chen, S.; Guillas, I.; Hartemann, A.; Salem, J.E.; Redheuil, A.; Foufelle, F.; Le Stunff, H.; Hajduch, E.; Guerin, M. Inverse relationship between circulating sphingosine-1-phosphate and precursor species and coronary artery calcification score in type 2 diabetes. Cardiovasc Diabetol 2025, 24, 85. [Google Scholar] [CrossRef]
- Xu, L.; Yan, X.; Tang, Z.; Feng, B. Association between circulating oxidized OxLDL/LDL-C ratio and the severity of coronary atherosclerosis, along with other emerging biomarkers of cardiovascular disease in patients with type 2 diabetes. Diabetes Res Clin Pract 2022, 191, 110040. [Google Scholar] [CrossRef]
- Hultgårdh-Nilsson, A.; Borén, J.; Chakravarti, S. The small leucine-rich repeat proteoglycans in tissue repair and atherosclerosis. J Intern Med 2015, 278, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Kirankaya, A.; Tugrul, S.; Ozcan, S.; Ince, O.; Donmez, E.; Atici, A.; Hancioglu, E.; Okuyan, E.; Sahin, I. Correlation between the serum lumican level and the severity of coronary artery disease. Eur Rev Med Pharmacol Sci 2023, 27, 2350–2357. [Google Scholar] [PubMed]
- Hershenson, R.; Nardi-Agmon, I.; Leshem-Lev, D.; Kornowski, R.; Eisen, A. The effect of empagliflozin on circulating endothelial progenitor cells in patients with diabetes and stable coronary artery disease. Cardiovasc Diabetol 2024, 23, 386. [Google Scholar] [CrossRef] [PubMed]
- Taheri, H.; Chiti, H.; Reshadmanesh, T.; Gohari, S.; Jalilvand, A.; Arsang-Jang, S.; Ismail-Beigi, F.; Ghanbari, S.; Dadashi, M.; Asgari, A.; Mahjani, M.; Karbalaee-Hasani, A.; Ahangar, H. Empagliflozin improves high-sensitive cardiac troponin-I and high-density lipoprotein cholesterol in patients with type 2 diabetes mellitus and coronary artery disease: a post-hoc analysis of EMPA-CARD Trial. J Diabetes Metab Disord 2023, 22, 1723–1730. [Google Scholar] [CrossRef]
- Jin, Q.; Ma, R.C.W. Metabolomics in Diabetes and Diabetic Complications: Insights from Epidemiological Studies. Cells 2021, 10. [Google Scholar] [CrossRef]
- Muriach, M.; Flores-Bellver, M.; Romero, F.J.; Barcia, J.M. Diabetes and the brain: oxidative stress, inflammation, and autophagy. Oxid Med Cell Longev 2014, 2014, 102158. [Google Scholar] [CrossRef]
- Eid, S.; Sas, K.M.; Abcouwer, S.F.; Feldman, E.L.; Gardner, T.W.; Pennathur, S.; Fort, P.E. New insights into the mechanisms of diabetic complications: role of lipids and lipid metabolism. Diabetologia 2019, 62, 1539–1549. [Google Scholar] [CrossRef]
- Reardon, C.A.; Lingaraju, A.; Schoenfelt, K.Q.; Zhou, G.; Cui, C.; Jacobs-El, H.; Babenko, I.; Hoofnagle, A.; Czyz, D.; Shuman, H.; Vaisar, T.; Becker, L. Obesity and Insulin Resistance Promote Atherosclerosis through an IFNγ-Regulated Macrophage Protein Network. Cell Reports 2018, 23, 3021–3030. [Google Scholar]
- Ding, P.F.; Zhang, H.S.; Wang, J.; Gao, Y.Y.; Mao, J.N.; Hang, C.H.; Li, W. Insulin resistance in ischemic stroke: Mechanisms and therapeutic approaches. Front Endocrinol (Lausanne) 2022, 13, 1092431. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhou, L.-Q.; Yang, S.; Dong, M.-H.; Chen, L.; Lu, Y.-L.; Zhang, L.-Y.; Zhang, L.; Chu, Y.-H.; Xu, L.-L.; Pang, X.-W.; Zhu, L.-F.; Xu, T.; Yong, T.-y.; Wang, W.; Tian, D.-S.; Qin, C. The foam cell-derived exosomes exacerbate ischemic white matter injury via transmitting metabolic defects to microglia. Cell Metabolism 2025, 37, 1636–1654.e10. [Google Scholar] [CrossRef] [PubMed]
- Edgar, L.; Akbar, N.; Braithwaite, A.T.; Krausgruber, T.; Gallart-Ayala, H.; Bailey, J.; Corbin, A.L.; Khoyratty, T.E.; Chai, J.T.; Alkhalil, M.; Rendeiro, A.F.; Ziberna, K.; Arya, R.; Cahill, T.J.; Bock, C.; Laurencikiene, J.; Crabtree, M.J.; Lemieux, M.E.; Riksen, N.P.; Netea, M.G.; Wheelock, C.E.; Channon, K.M.; Rydén, M.; Udalova, I.A.; Carnicer, R.; Choudhury, R.P. Hyperglycemia Induces Trained Immunity in Macrophages and Their Precursors and Promotes Atherosclerosis. Circulation 2021, 144, 961–982. [Google Scholar] [CrossRef] [PubMed]
- Mavridis, A.; Viktorisson, A.; Eliasson, B.; von Euler, M.; Sunnerhagen, K.S. Risk of Ischemic and Hemorrhagic Stroke in Individuals With Type 1 and Type 2 Diabetes: A Nationwide Cohort Study in Sweden. Neurology 2025, 104, e213480. [Google Scholar] [CrossRef]
- Dogan, Z.; Senyigit, A.; Durmus, S.; Duvarci, C.; Gelisgen, R.; Uzun, H.; Tabak, O. The relationship between oxLDL, sLOX-1, PCSK9 and carotid intima-media thickness in patients with prediabetes and type 2 diabetes. Sci Rep 2025, 15, 4554. [Google Scholar] [CrossRef]
- Chang, D.; Sharma, L.; Dela Cruz, C.S. Chitotriosidase: a marker and modulator of lung disease. European Respiratory Review 2020, 29, 190143. [Google Scholar] [CrossRef]
- Artieda, M.; Cenarro, A.; Gañán, A.; Jericó, I.; Gonzalvo, C.; Casado, J.M.; Vitoria, I.; Puzo, J.; Pocoví, M.; Civeira, F. Serum Chitotriosidase Activity Is Increased in Subjects With Atherosclerosis Disease. Arteriosclerosis, Thrombosis, and Vascular Biology 2003, 23, 1645–1652. [Google Scholar] [CrossRef]
- Cerqueira, A.; Quelhas-Santos, J.; Ferreira, I.; Sampaio, S.; Relvas, M.; Marques, N.; Dias, C.C.; Pestana, M. Circulating Renalase as Predictor of Renal and Cardiovascular Outcomes in Pre-Dialysis CKD Patients: A 5-Year Prospective Cohort Study. Life (Basel) 2021, 11. [Google Scholar] [CrossRef]
- Xu, Y.; Sun, Z. Molecular basis of Klotho: from gene to function in aging. Endocr Rev 2015, 36, 174–193. [Google Scholar] [CrossRef]
- Pan, H.C.; Chou, K.M.; Lee, C.C.; Yang, N.I.; Sun, C.Y. Circulating Klotho levels can predict long-term macrovascular outcomes in type 2 diabetic patients. Atherosclerosis 2018, 276, 83–90. [Google Scholar] [CrossRef]
- Chen, L.L.; Liao, Y.F.; Zeng, T.S.; Li, Y.M.; Yu, F.; Li, H.Q. [Number and function of circulating endothelial progenitor cell in diabetics with different vascular complications]. Zhonghua Yi Xue Za Zhi 2009, 89, 1234–1239. [Google Scholar] [PubMed]
- Zhang, X.; Xiao, W.; Zhang, Q.; Xia, D.; Gao, P.; Su, J.; Yang, H.; Gao, X.; Ni, W.; Lei, Y.; Gu, Y. Progression in Moyamoya Disease: Clinical Features, Neuroimaging Evaluation, and Treatment. Curr Neuropharmacol 2022, 20, 292–308. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.Y.; Fan, Y.N.; Liu, Y.; Wang, Q.N.; Zhang, Y.; Zhu, B.; Liu, B.; Duan, L. Circulating endothelial progenitor cells and endothelial cells in moyamoya disease. Brain Behav 2018, 8, e01035. [Google Scholar] [CrossRef] [PubMed]
- Paneni, F.; Beckman, J.A.; Creager, M.A.; Cosentino, F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Eur Heart J 2013, 34, 2436–2443. [Google Scholar] [CrossRef]
- Thiruvoipati, T.; Kielhorn, C.E.; Armstrong, E.J. Peripheral artery disease in patients with diabetes: Epidemiology, mechanisms, and outcomes. World J Diabetes 2015, 6, 961–969. [Google Scholar] [CrossRef]
- Abu-Jableh, W.; Younis, A.; Hjazeen, A.; Mashaqbeh, E.; Al-Sharif, E. Asymptomatic Peripheral Arterial Disease Among Jordanian Patients With Diabetic Foot Ulcer. Cureus 2024, 16, e73722. [Google Scholar] [CrossRef]
- Smolderen, K.G.; Ujueta, F.; Buckley Behan, D.; Vlaeyen, J.W.S.; Jackson, E.A.; Peters, M.; Whipple, M.; Phillips, K.; Chung, J.; Mena-Hurtado, C.; Disease, o. b. o. t. A. H. A. C. o. P. V.; Cardiovascular, C. o.; Nursing, S.; Care, C. o. Q. o.; Research, O. Understanding the Pain Experience and Treatment Considerations Along the Spectrum of Peripheral Artery Disease: A Scientific Statement From the American Heart Association. Circulation: Cardiovascular Quality and Outcomes 2025, 18, e000135. [Google Scholar] [CrossRef]
- Sangeeta, S.; Siripuram, C.; Konka, S.; Vaithilingam, K.; Periasamy, P.; Velu, R.K.; Kandimalla, R. Biomarkers of Inflammation, Oxidative Stress, and Endothelial Dysfunction in Early Detection of Diabetic Foot Ulcers. Cureus 2025, 17, e82174. [Google Scholar] [CrossRef]
- Jude, E.B. Intermittent claudication in the patient with diabetes. The British Journal of Diabetes & Vascular Disease 2004, 4, 238–242. [Google Scholar]
- Nadeau, M.; Rosas-Arellano, M.P.; Gurr, K.R.; Bailey, S.I.; Taylor, D.C.; Grewal, R.; Lawlor, D.K.; Bailey, C.S. The reliability of differentiating neurogenic claudication from vascular claudication based on symptomatic presentation. Can J Surg 2013, 56, 372–377. [Google Scholar] [CrossRef]
- Khan, Z.; Zeb, S.; Ashraf; Rumman; Ali, A.; Aleem, F.; Omair, F. The Relationship Between Plasma Fibrinogen Levels and the Severity of Diabetic Foot Ulcers in Diabetic Patients. Cureus 2025, 17, e81118.
- Yachmaneni, A., Jr.; Jajoo, S.; Mahakalkar, C.; Kshirsagar, S.; Dhole, S. A Comprehensive Review of the Vascular Consequences of Diabetes in the Lower Extremities: Current Approaches to Management and Evaluation of Clinical Outcomes. Cureus 2023, 15, e47525. [Google Scholar] [CrossRef] [PubMed]
- Alsararatee, H.H.; Langley, J.C.S.; Thorburn, M.; Burton-Gow, H.; Whitby, S.; Powell, S. Assessment of the diabetic foot in inpatients. Br J Nurs 2025, 34, S12–S23. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.M.; Kimura, E.; Harada, R.K.; Nair, N.; Narasimhan, B.; Meng, X.Y.; Zhang, F.; Beck, K.R.; Olin, J.W.; Fung, E.T.; Cooke, J.P. Beta2-microglobulin as a biomarker in peripheral arterial disease: proteomic profiling and clinical studies. Circulation 2007, 116, 1396–1403. [Google Scholar] [CrossRef]
- Al-Kafaji, G.; Al-Mahroos, G.; Abdulla Al-Muhtaresh, H.; Sabry, M.A.; Abdul Razzak, R.; Salem, A.H. Circulating endothelium-enriched microRNA-126 as a potential biomarker for coronary artery disease in type 2 diabetes mellitus patients. Biomarkers 2017, 22, 268–278. [Google Scholar]
- Méndez-Valdés, G.; Gómez-Hevia, F.; Lillo-Moya, J.; González-Fernández, T.; Abelli, J.; Cereceda-Cornejo, A.; Bragato, M.C.; Saso, L.; Rodrigo, R. Endostatin and Cancer Therapy: A Novel Potential Alternative to Anti-VEGF Monoclonal Antibodies. Biomedicines 2023, 11. [Google Scholar]
- Golledge, J.; Clancy, P.; Hankey, G.J.; Yeap, B.B.; Norman, P.E. Serum endostatin concentrations are higher in men with symptoms of intermittent claudication. Dis Markers 2014, 2014, 298239. [Google Scholar]
- Naka, K.K.; Papathanassiou, K.; Bechlioulis, A.; Pappas, K.; Tigas, S.; Makriyiannis, D.; Antoniou, S.; Kazakos, N.; Margeli, A.; Papassotiriou, I.; Tsatsoulis, A.; Michalis, L.K. Association of vascular indices with novel circulating biomarkers as prognostic factors for cardiovascular complications in patients with type 2 diabetes mellitus. Clin Biochem 2018, 53, 31–37. [Google Scholar] [CrossRef]
- Kishida, K.; Funahashi, T.; Shimomura, I. Adiponectin as a routine clinical biomarker. Best Pract Res Clin Endocrinol Metab 2014, 28, 119–130. [Google Scholar] [CrossRef]
- Samman Tahhan, A.; Hayek, S.S.; Sandesara, P.; Hajjari, J.; Hammadah, M.; O’Neal, W.T.; Kelli, H.M.; Alkhoder, A.; Ghasemzadeh, N.; Ko, Y.A.; Aida, H.; Gafeer, M.M.; Abdelhadi, N.; Mohammed, K.H.; Patel, K.; Arya, S.; Reiser, J.; Vaccarino, V.; Sperling, L.; Quyyumi, A. Circulating soluble urokinase plasminogen activator receptor levels and peripheral arterial disease outcomes. Atherosclerosis 2017, 264, 108–114. [Google Scholar]
- Li, B.; Shaikh, F.; Younes, H.; Abuhalimeh, B.; Zamzam, A.; Abdin, R.; Qadura, M. The Prognostic Potential of Insulin-like Growth Factor-Binding Protein 1 for Cardiovascular Complications in Peripheral Artery Disease. J Cardiovasc Dev Dis 2025, 12. [Google Scholar] [CrossRef]
- Furuhashi, M. Fatty Acid-Binding Protein 4 in Cardiovascular and Metabolic Diseases. J Atheroscler Thromb 2019, 26, 216–232. [Google Scholar] [CrossRef]
- Aragones, G.; Ferre, R.; Lazaro, I.; Cabre, A.; Plana, N.; Merino, J.; Heras, M.; Girona, J.; Masana, L. Fatty acid-binding protein 4 is associated with endothelial dysfunction in patients with type 2 diabetes. Atherosclerosis 2010, 213, 329–331. [Google Scholar] [CrossRef]
- Li, B.; Shaikh, F.; Younes, H.; Abuhalimeh, B.; Zamzam, A.; Abdin, R.; Qadura, M. Matrix Metalloproteinases 7 and 10 Are Prognostic Biomarkers for Systemic Cardiovascular Risk in Individuals with Peripheral Artery Disease. Biomolecules 2025, 15. [Google Scholar] [CrossRef]
Figure 1.
A schematic representation of the main topics discussed in this review.
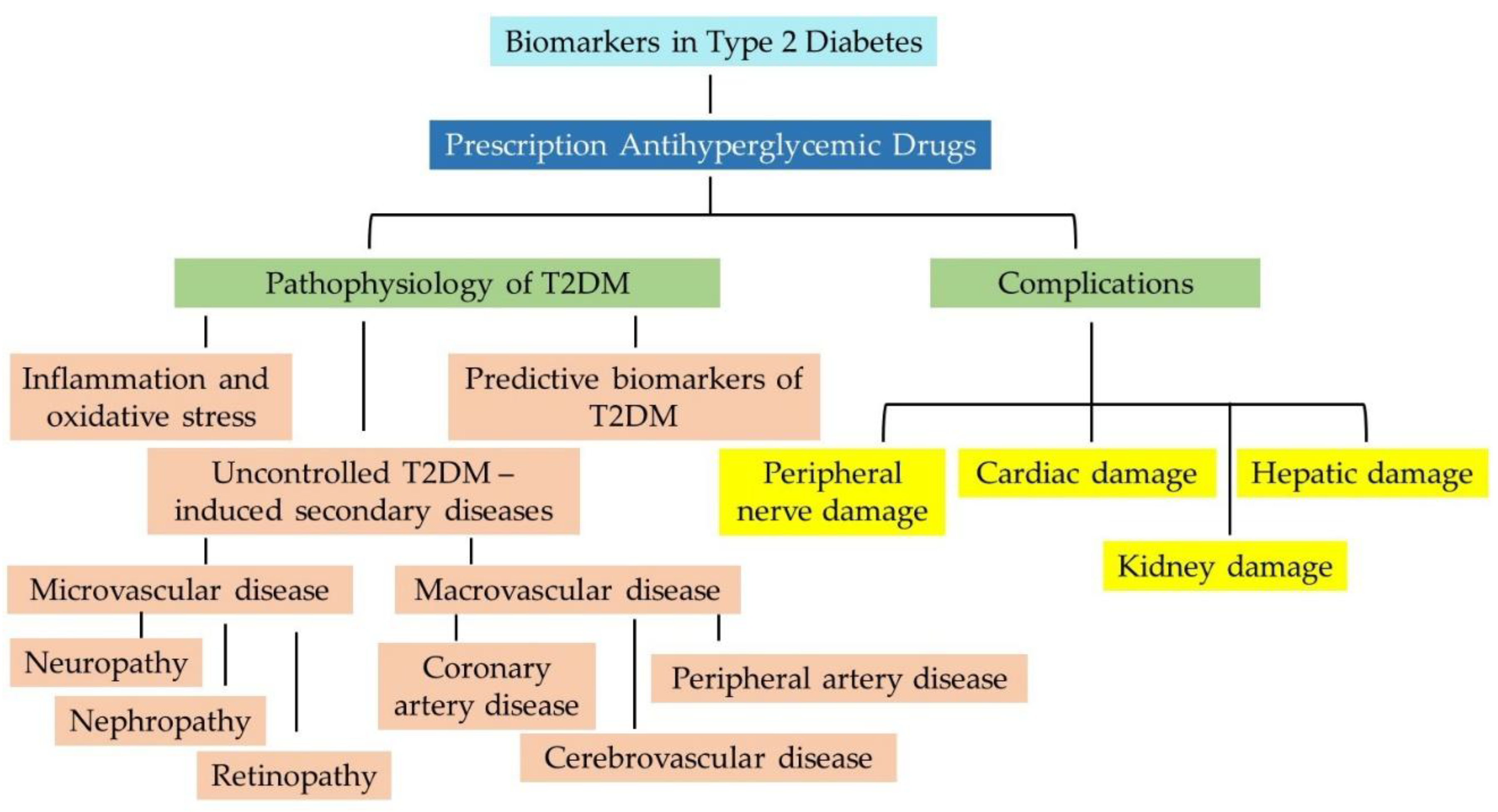
Figure 2.
Simplified schematic representation of five different subtypes of diabetes and their association with a range of health issues in patients with T2DM.
Figure 2.
Simplified schematic representation of five different subtypes of diabetes and their association with a range of health issues in patients with T2DM.
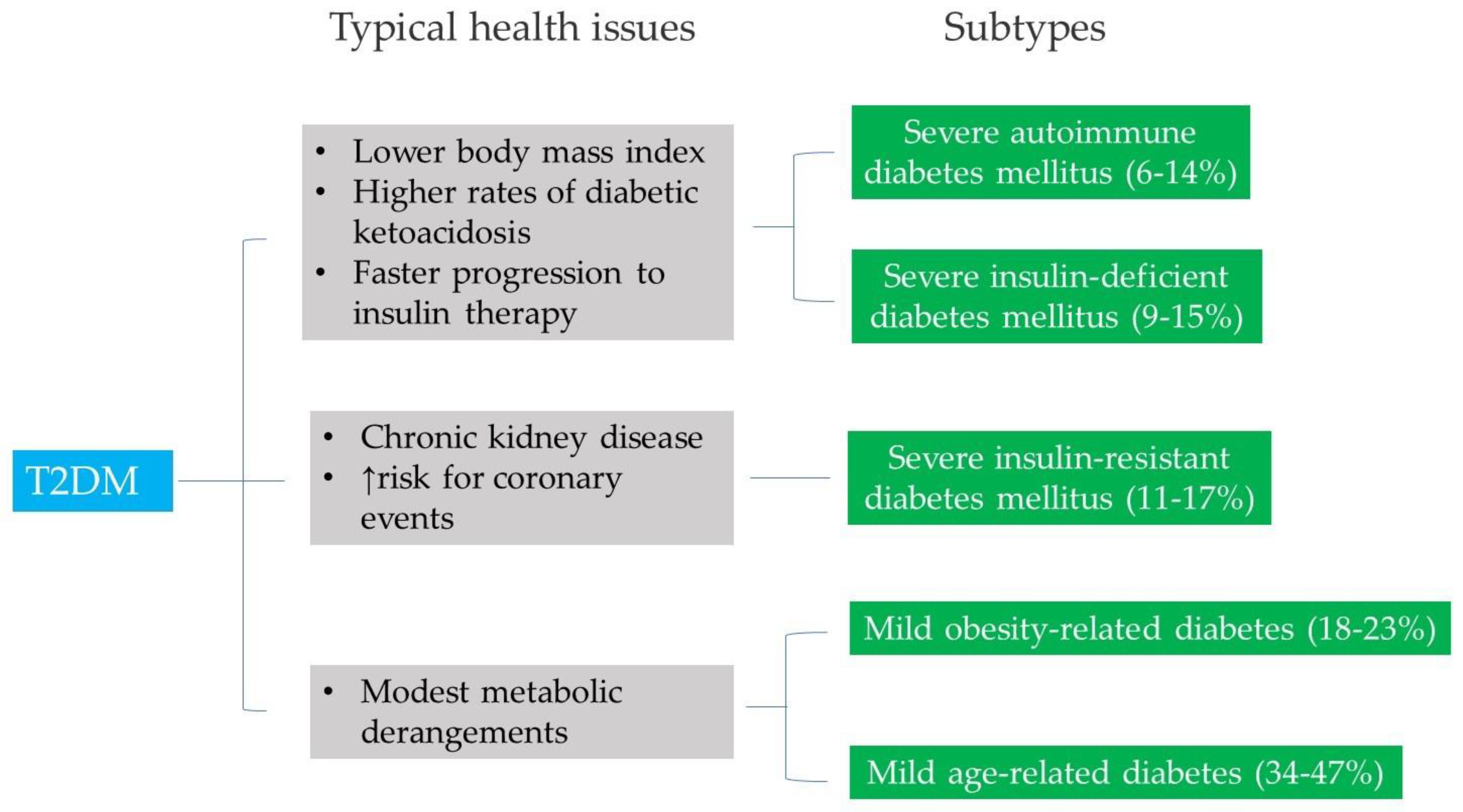
Figure 3.
Complications associated with the use of antihyperglycemic drugs.
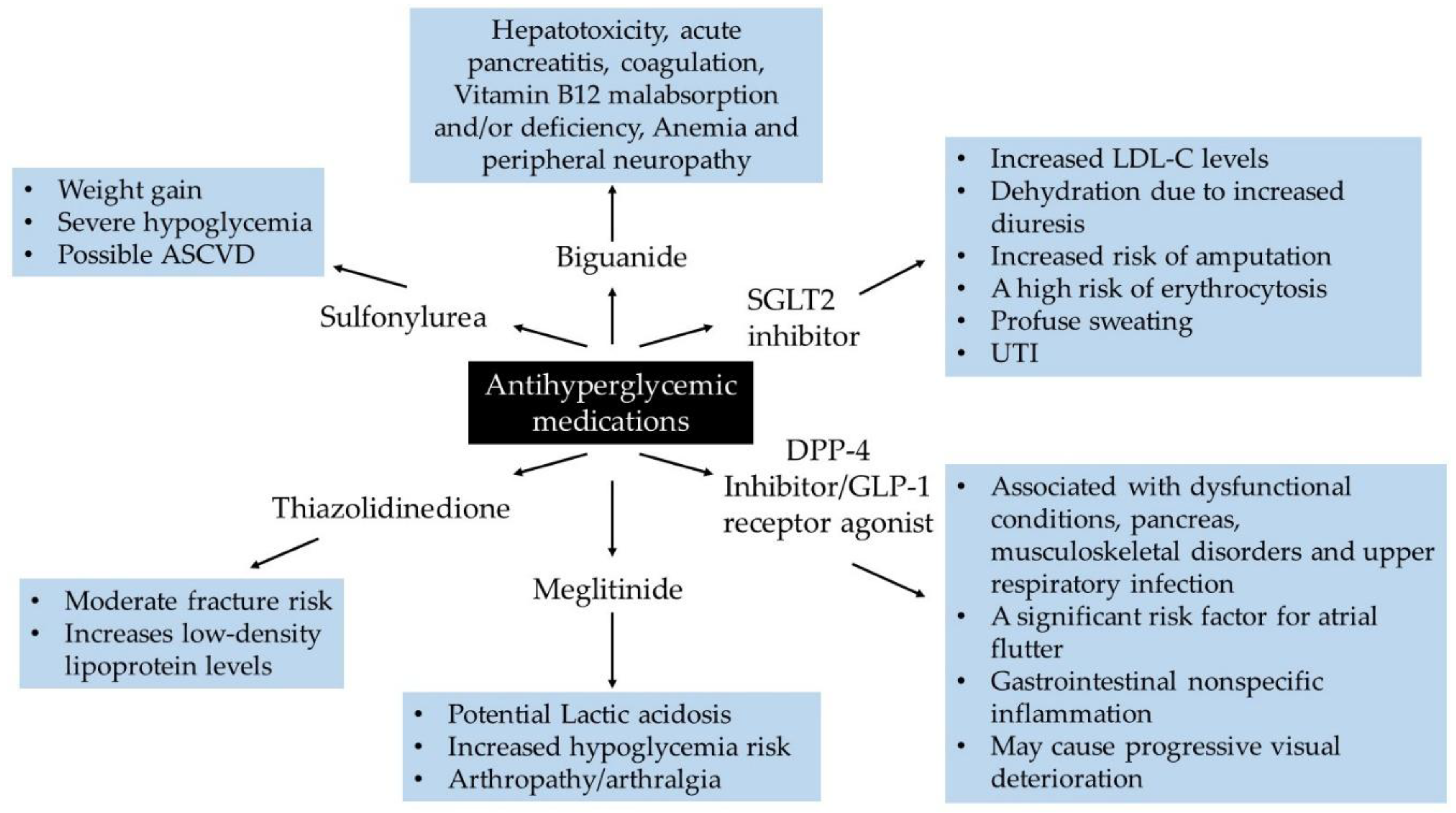
Figure 4.
The emerging role of biochemical indicators in diabetic microvascular and macrovascular dysfunction. A variety of risk factors promotes the development and progression of diabetic vasculopathy. Dyslipidemia combined with endothelial injury are precursors of atherosclerosis. The common indicator between CAD and PAD is shown in “Red”. The common indicators of microvascular or macrovascular are shown in “Dark Blue”. PAD; peripheral artery disease, CAD; coronary artery disease; CVD; cerebrovascular disease.
Figure 4.
The emerging role of biochemical indicators in diabetic microvascular and macrovascular dysfunction. A variety of risk factors promotes the development and progression of diabetic vasculopathy. Dyslipidemia combined with endothelial injury are precursors of atherosclerosis. The common indicator between CAD and PAD is shown in “Red”. The common indicators of microvascular or macrovascular are shown in “Dark Blue”. PAD; peripheral artery disease, CAD; coronary artery disease; CVD; cerebrovascular disease.
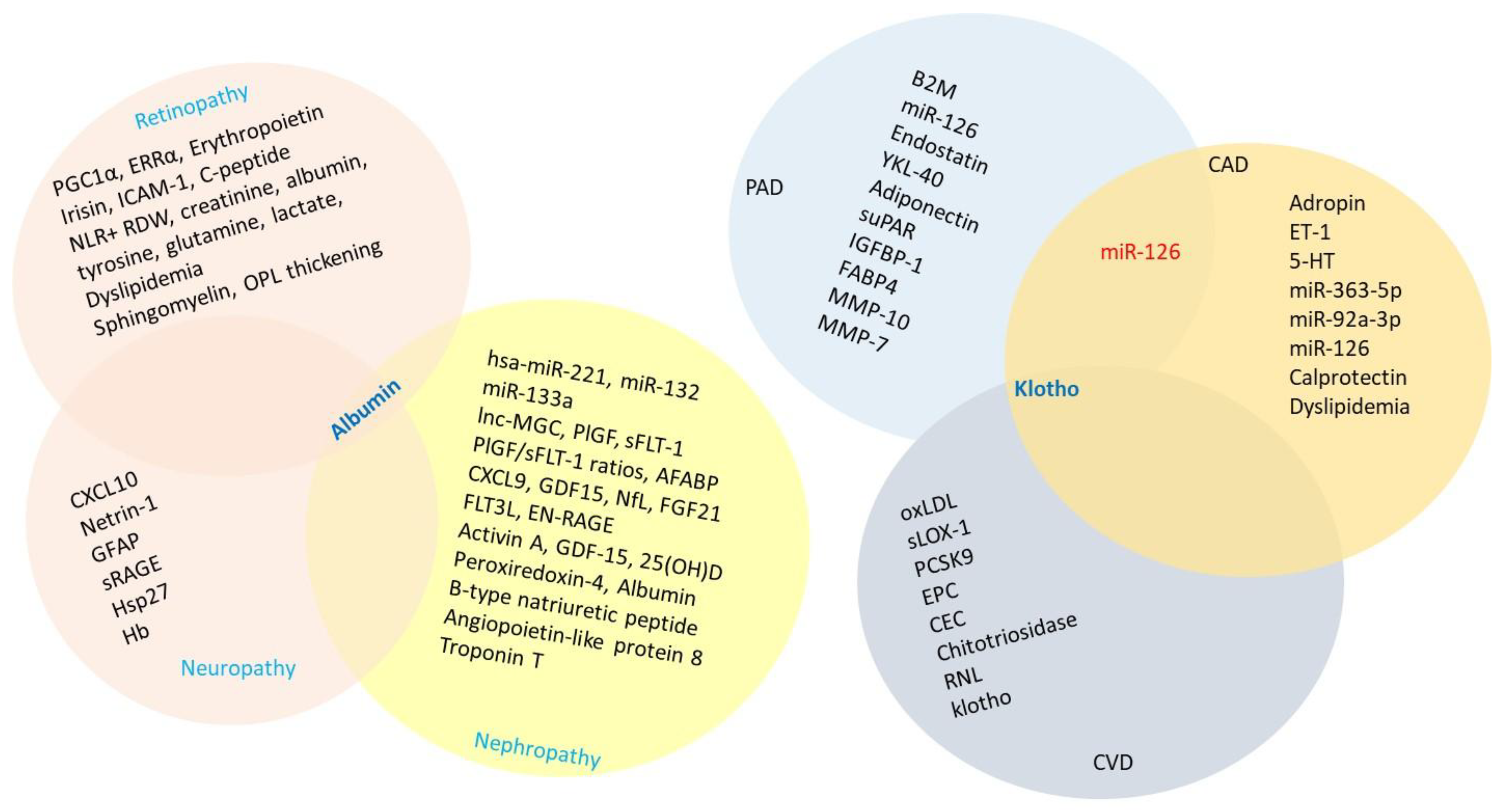

Table 1.
A summary of key hallmarks of common medications used for hyperglycemia that have been reported in clinical diabetes settings to guide therapeutic decision making.
Table 1.
A summary of key hallmarks of common medications used for hyperglycemia that have been reported in clinical diabetes settings to guide therapeutic decision making.
| Drug Class | Generic name | Clinical outcomes | Clinical condition of concern | Anti-atherogenic mechanisms | Ref. |
|---|---|---|---|---|---|
| Biguanide | Metformin, metformin extended release | Affects metabolic pathway (s):
|
|
|
[47,48,49,50,51,52,53,54,55] |
| Sulfonylurea | Glipizide |
|
|
|
[56,57,58,59] |
| Meglitinide | Repaglinide |
|
|
|
[60,61,62,63] |
| Thiazolidinedione | Pioglitazone |
|
|
|
[64,65] |
| DPP-4 inhibitor | Sitagliptin |
|
|
|
[66,67,68,69,70,71,72] |
| GLP-1 receptor agonist | Semaglutide |
|
|
|
[73,74,75,76,77,78,79] |
| SGLT2 inhibitor | Empagliflozin, Canagliflozin |
|
|
|
[80,81,82,83,84,85,86,87,88] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



