
Submitted:
26 August 2025
Posted:
27 August 2025
You are already at the latest version
Abstract
Purpose. Evaluation of the results of glaucoma surgery performed by the same surgeon in the non-pandemic period (2019, 2021 and the first 3 months of 2022) vs. the pandemic one (2020). Evaluation of the effects of glaucoma surgery: release of intraocular pressure, intra and postoperative complications, measurement of success rate and postoperative failure rate and its implications. Material and method: Out of a total of 66 patients ad-mitted between November 2019 and March 2022, 45 patients met the inclusion and ex-clusion criteria and were included in the study. All underwent glaucoma surgery per-formed by the same surgeon using the same technique (trabeculectomy ± iridectomy, ± mitomycin C). Clinical parameters evaluated: preoperative and postop-erative, pre-operative IOP and first postoperative day; early / late intraoperative and postoperative complications; postoperative success and failure rates. Results: Most cases of glaucoma were in 2021 (38%). In 2019, cases of pseudoexfoliative glaucoma predominated (41.7%), while in 2020 cases of closed uncle secondary glaucoma pre-dominated (61.1%). In 2019, pseudoexfoliative glaucoma was the most prevalent sub-type (50%), whereas in 2020, neovascular glaucoma predominated (40%). In contrast, in 2021 (45.5%) and 2022 (40%), the most frequent diagnosis was primary open-angle glaucoma. Over years of study, it is found that retrobulbar anesthesia was performed more frequently in 2019. The failure rate was not significantly influenced by complications, age, comorbidities and type of intervention. Conclusions: Glaucoma surgery encountered a number of difficulties during the pandemic vs. non-pandemic period even though they were considered an emergency due to their low addressability. The share of early intraoperative and post-operative complications was reduced, with early intraocular hypotonia predominating in 10 cases. In all study groups, over 80% had qualified success and only 18% failed. According to the AAO and EGS recommendations, glaucoma is an emergency and surgery is urgently needed when IOP is uncontrolled to prevent severe functional loss, regardless of the existing pandemic or non-pandemic situation.
Keywords:
trabeculectomy
; pandemic period
; peripheral iridectomy
; mitomycin C
; neovascular glaucoma
; pseudo exfoliative glaucoma
; success rate
1. Introduction
The Covid-19 pandemic imposed the necessity of rapid adaptation in the face of unprecedented adversity. According to the World Health Organization, as of May 20, 2021, a total of 164,523,894 confirmed cases and 3,412,032 deaths were reported globally, underscoring the profound disruption caused to humanity. Beyond its respiratory manifestations, the virus also affected other organs, generally with favorable outcomes, except in elderly individuals and children with pre-existing conditions, where compli-cations required urgent medical intervention [1,2]. The most effective strategies for limiting the transmission of this airborne disease included maintaining physical dis-tancing, adhering to mask-wearing protocols, hand hygiene and disinfection, compli-ance with respiratory etiquette, and, most crucially, ensuring accurate public infor-mation about the virus [3,4]. During the pandemic, elderly patients with glaucoma en-countered significant difficulties due to constricted visual fields and comorbidities, which impeded their ability to monitor intraocular pressure (IOP) locally and regularly. In an effort to reduce disease transmission and optimize resource allocation, numerous ophthalmological societies issued guidelines for categorizing procedures as urgent or non-urgent, with non-urgent interventions being postponed accordingly [5,6]. Moreo-ver, certain ophthalmology departments were converted into COVID-19 units, ad-mit-ting exclusively SARS-CoV-2-positive patients and consequently restricting access to ophthalmic care (3–6). Non-adherence to treatment regimens among patients with Primary Open-Angle Glaucoma (POAG) was widely reported during the pandemic in various studies conducted in India (8), Croatia (9), the United States [10], Egypt [11], and Pakistan [12]. As strict lockdown measures were enforced, adherence rates declined due to factors such as unavailability or inaccessibility of medications [8,13,14,15], travel re-strictions [8], financial hardship resulting from the pandemic’s economic impact [8,11], and limited understanding or awareness of glaucoma [8,10,11]. In India, trabeculectomy and bleb-related procedures were the most frequently performed surgical interventions, with secondary glaucoma accounting for the majority of cases necessitating surgery (62.5%) during the pandemic. In the post-pandemic period, the frequency of minimally invasive glaucoma surgeries (MIGS) increased, while the number of trabeculectomy procedures declined [4,16]. In the United Kingdom, although trabeculectomy remained a standard procedure, its usage diminished during the pandemic due to the high number of required postoperative visits and follow-up procedures. As a result, alter-native interventions, such as conventional laser therapy, micropulse diode laser, glau-coma drainage devices, deep sclerectomy, and Preserflo implants, were increasingly preferred [7]. In Romania, during the same period, a significant number of private practices and clinics suspended operations, while many public hospitals either closed or scaled down their services, leading to a marked decline in ophthalmic surgical activity. The present study aims to evaluate the outcomes of glaucoma surgery performed by the same surgeon between October 2019 and March 2022, comparing the pandemic and non-pandemic periods in a Tertiary Hospital in the region of Moldova—the only facility that remained operational during the Covid-19 crisis. The study focuses on assessing the effects of antiglaucoma surgery (trabeculectomy), specifically the reduction of intraoc-ular pressure, intraoperative and postoperative complications, the measurement of postoperative success and failure rates, and the implications associated with surgical failure.
2. Materials and Methods
Patients with various types of glaucoma who were admitted as emergencies (in-flammatory, neovascular, pseudo exfoliative, post-traumatic) and operated on by the same surgeon (Anton Nicoleta) during the non-pandemic period (2019, 2021, 2022) versus the pandemic year (2020) were included in this study. The surgical procedures consisted of trabeculectomy with or without iridectomy (±IP), with or without mito-mycin C (±MMC), and with or without tenonectomy. All patients were evaluated pre- and postoperatively according to a standardized protocol.
Inclusion criteria. All glaucoma cases presented as emergencies underwent tra-beculectomy surgery. Exclusion criteria. Patients with phacomorphic glaucoma (emer-gency admissions) who underwent a different surgical technique (lens extraction in-stead of trabeculectomy) were excluded from the study.
The clinical parameters assessed included: preoperative intraocular pressure (IOP), IOP on the first postoperative day, and at one-month follow-up; baseline and postop-erative visual acuity (VA); intraoperative and early/late postoperative complications; and postoperative success and failure rates.
Additional data recorded included the type of anesthesia used (general anesthesia vs. topical/retrobulbar injectable anesthesia), whether surgery was performed on an only eye, and the number of antiglaucoma medications prescribed pre- and postopera-tively.
2.1. Preoperative Preparation
For the purpose of local or general anesthesia (depending on factors such as sin-gle-eye status, patient age - young or elderly - associated comorbidities, or anxiety), a series of preoperative evaluations were conducted. Laboratory tests included: complete blood count, liver function tests, urea, creatinine, electrolyte panel, and coagulation profile. A cardiology consultation was required to assess surgical fitness. Additional considerations included close attention to anticoagulant therapy, which needed to be discontinued prior to surgery, and chest radiography in preparation for general anes-thesia. General anesthesia was considered in cases involving antiglaucoma surgery on a single functional eye, in anxious patients, or when there was an elevated risk of bleed-ing, in order to ensure surgical safety.
2.2. Surgery Technique - the Surgical Protocol Consisted of the Following Steps
Localization: The first trabeculectomy was consistently performed at the 12 o’clock position. Subsequent interventions were localized either superonasally or superotem-porally.
In cases where mitomycin C (MMC) was used, a concentration of 0.2 mg/mL was applied. The MMC was delivered via a sponge soaked in the solution and placed be-tween the conjunctiva and sclera, with an average exposure time of 3 minutes. Fol-lowing removal of the sponge, the surgical area was thoroughly irrigated with balanced salt solution (BSS) to ensure complete removal of the antimetabolite.

Table 1.
The surgical protocol consisted of the following steps.
| Surgical protocol | Type of anesthesia used |
| Wide fornix-based conjunctival incision, 8 mm in length | General anesthesia (depending on factors such as single-eye status, patient age - young or elderly - associated comorbidities, or anxiety) |
| Delineation of a superficial scleral flap (50% thickness), rectangular, 4 × 4 mm | Topical/retrobulbar injectable anesthesia |
| Application of MMC (Mitomycin C – antifibrotic agent) | |
| Delineation of a deep scleral flap, 3 × 2 mm | |
| Paracentesis of the anterior chamber (AC), intraocular miotic administration | |
| Excision of the deep scleral block (3 × 2 mm), peripheral iridectomy | |
| Suturing of the superficial flap with 5/3 sutures, placement of a releasable suture in selected cases | |
| Restoration of ocular tone with BSS, assessment of filtration | |
| Continuous conjunctival suture at the peripheral cornea |
The surgery was performed by the same surgeon (Anton Nicoleta), following proper patient preparation and after a thorough discussion with the patient regarding the surgical technique, potential intraoperative and postoperative complications, as well as postoperative recommendations and expected outcomes. All patients provided written informed consent regarding the surgical procedure.
3. Results
Out of a total of 66 patients admitted between November 2019 and March 2022, 45 patients met the inclusion and exclusion criteria and were included in the study. All underwent glaucoma surgery performed by the same surgeon using the same technique (trabeculectomy ± iridectomy, ± mitomycin C) (Figure 1).
A total of 21 patients were excluded from the study due to having phacomorphic glaucoma, which required a different surgical intervention (lens extraction. In 2019, pseudoexfoliative glaucoma was the most prevalent subtype (50%), whereas in 2020, neovascular glaucoma predominated (40%). In contrast, in 2021 (45.5%) and 2022 (40%), the most frequent diagnosis was primary open-angle glaucoma (p = 0.067) (Figure 2).
Analysis by year of study shows that retrobulbar anesthesia (RB) was more frequently administered in 2019 (75%), 2021 (86.4%), and 2022 (60%) (p = 0.323) (Figure 3).
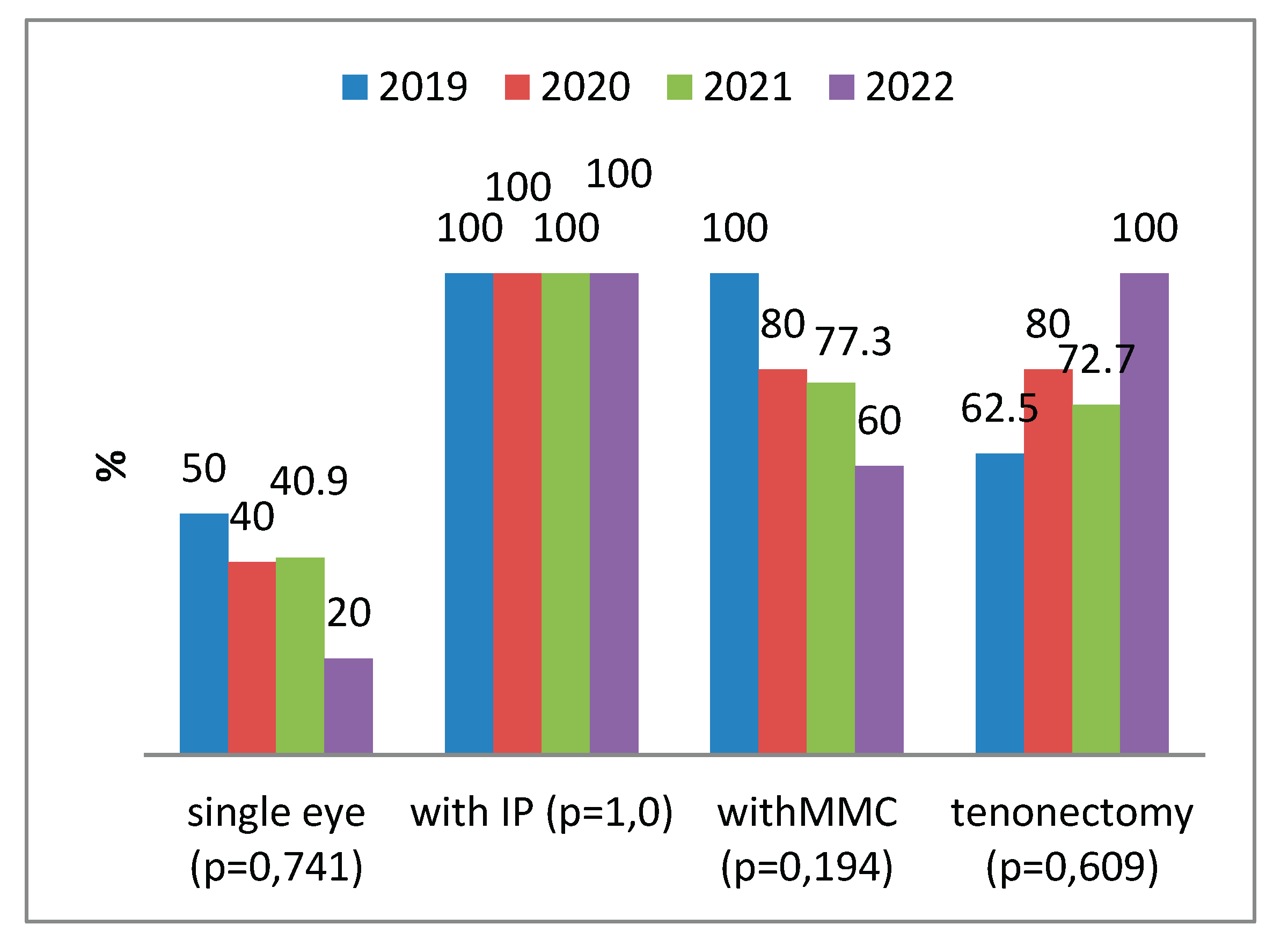
Figure 4 shows the types of surgical interventions performed, specifically trabeculectomy, which may be combined with peripheral iridectomy (PI), mitomycin C (MMC), and with or without tenonectomy. These variations were determined based on the type of glaucoma, conjunctival appearance, and intraoperative particularities
Seventy-five percent of the total cases in 2019, 75% in 2021, and 80% in 2022 received three types of antiglaucoma medications preoperatively, whereas 40% of the glaucoma cases in 2019 had not received any antiglaucoma treatment prior to surgery (p = 0.024). Among the four patients without preoperative treatment, three (75%) were discharged without antiglaucoma medication. Similarly, of the 28 patients who had received a combination of three medications preoperatively, 21 (75%) were discharged without the need for antiglaucoma therapy (p = 0.677) (Figure 5).
Among the associated systemic conditions reported were arterial hypertension, diabetes mellitus, and ankylosing spondylitis (with two cases of inflammatory glaucoma identified). In a very limited number of cases, 5-fluorouracil (5-FU), an antifibrotic agent, was administered via subconjunctival injection adjacent to the filtering bleb, and ocular massage was rarely recommended.
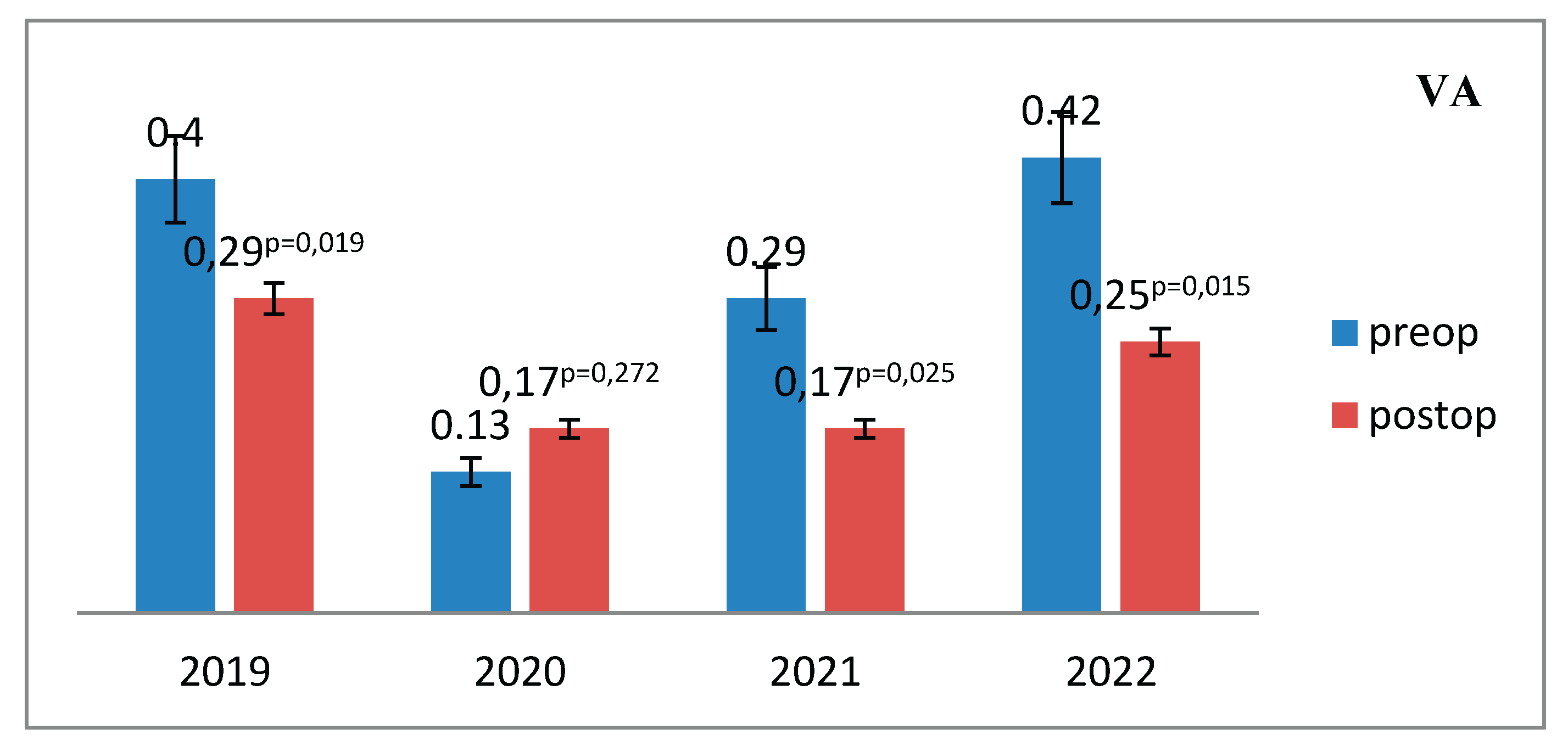
Visual acuity showed minimal change in the postoperative period compared to the preoperative status (Figure 6).
Figure 7.
Mean values of visual acuity, both preoperative and postoperative, were recorded for each year of the study period (2019–2022).
Figure 7.
Mean values of visual acuity, both preoperative and postoperative, were recorded for each year of the study period (2019–2022).
The level of intraocular pressure (IOP) was evaluated preoperatively versus post-operatively. A significant postoperative reduction in IOP was observed, indicating effective pressure relief following surgery (Figure 8).
The mean level of intraocular pressure (IOP) reduction at discharge across the study years revealed the following: the highest mean IOP was recorded in 2019, while the lowest was observed in 2022 (17.0 vs. 12.60; p = 0.544) (Figure 9).
Intraoperative and early postoperative complications. Intraoperative complications were reported in 3 patients in 2020 and 2 patients in 2021. There were 2 cases of iridial hemorrhage, hyphema, and subsequent vitreous hemorrhage in a single functional eye in patients undergoing anticoagulant therapy and with diabetes. One case involved a suprachoroidal hemorrhage, which required rapid closure of the superficial flap using 9-0 nylon sutures, followed by postoperative treatment with cycloplegics, increased fluid intake, and analgesics. Early complications were observed in 6 patients (3 in 2019, 2 in 2020, 1 in 2021): hyphema, and early failure of the filtering bleb (flattened bleb, elevated IOP). No complications were reported in 2022, as all procedures were performed under analgosedation/general anesthesia. Late complications occurred in one case: a 31-year-old female patient from an urban area, diagnosed with inflammatory glaucoma, who experienced recurrent uveitis and moderately elevated IOP. Reinterventions: 2 cases of inflammatory glaucoma operated in 2019 required surgery for mature complicated cataract, which also led to glaucoma decompensation; 2 cases operated in 2022 required a second trabeculectomy approximately 20 years after the initial procedure (Figure 10).
Success and failure rates. The success rate - defined as an intraocular pressure (IOP) between 6 and 20 mmHg - reached approximately 85% in most cases. The failure rate - defined as an IOP <6 mmHg or >21 mmHg.
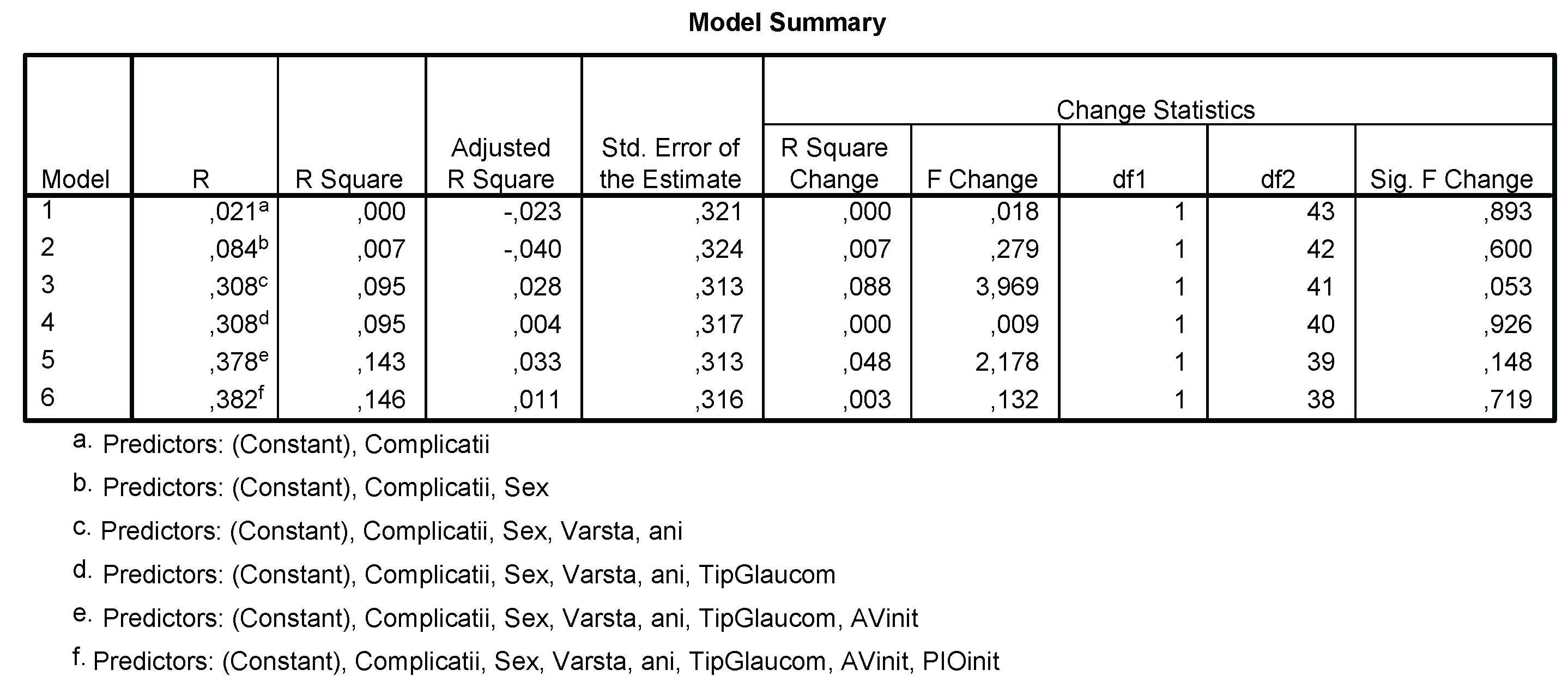
The linear regression model indicated that the failure rate was not significantly influenced by the presence of complications, sex, age, type of glaucoma, visual acuity, or preoperative IOP level (p = 0.719) (Figure 11).
The failure rate was slightly higher in male patients (60% vs. 47.5%; p = 0.597) and reached 100% in the age group over 60 years (p = 0.045), with no significant differences observed based on the presence of complications (20% vs. 17.5%; p = 0.892).
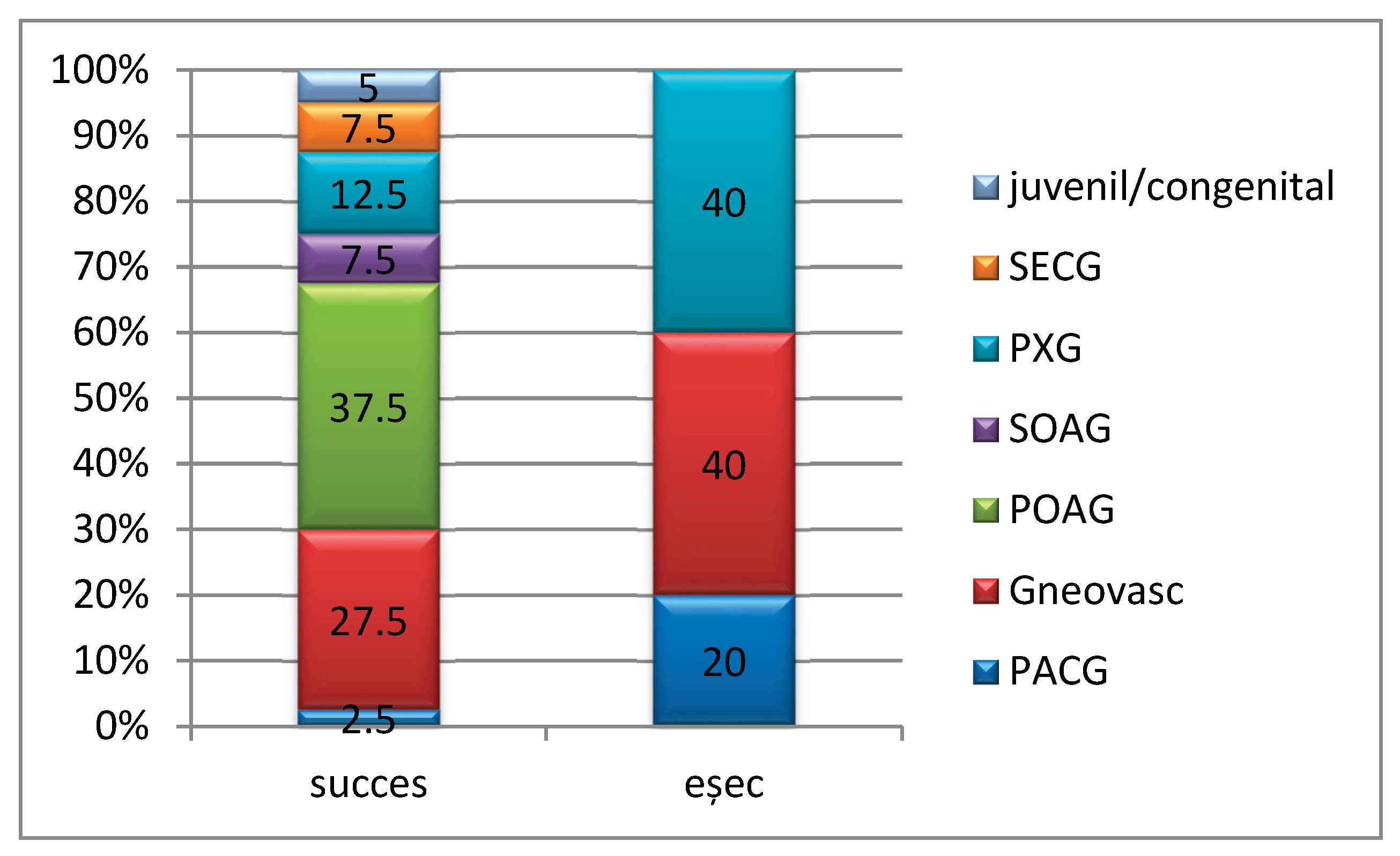
The failure rate was significantly higher among patients with neovascular glaucoma (40%) and pseudoexfoliative glaucoma (40%) (p = 0.169) (Figure 13).
Figure 12.
Distribution of success/failure cases according to epidemiological characteristics.
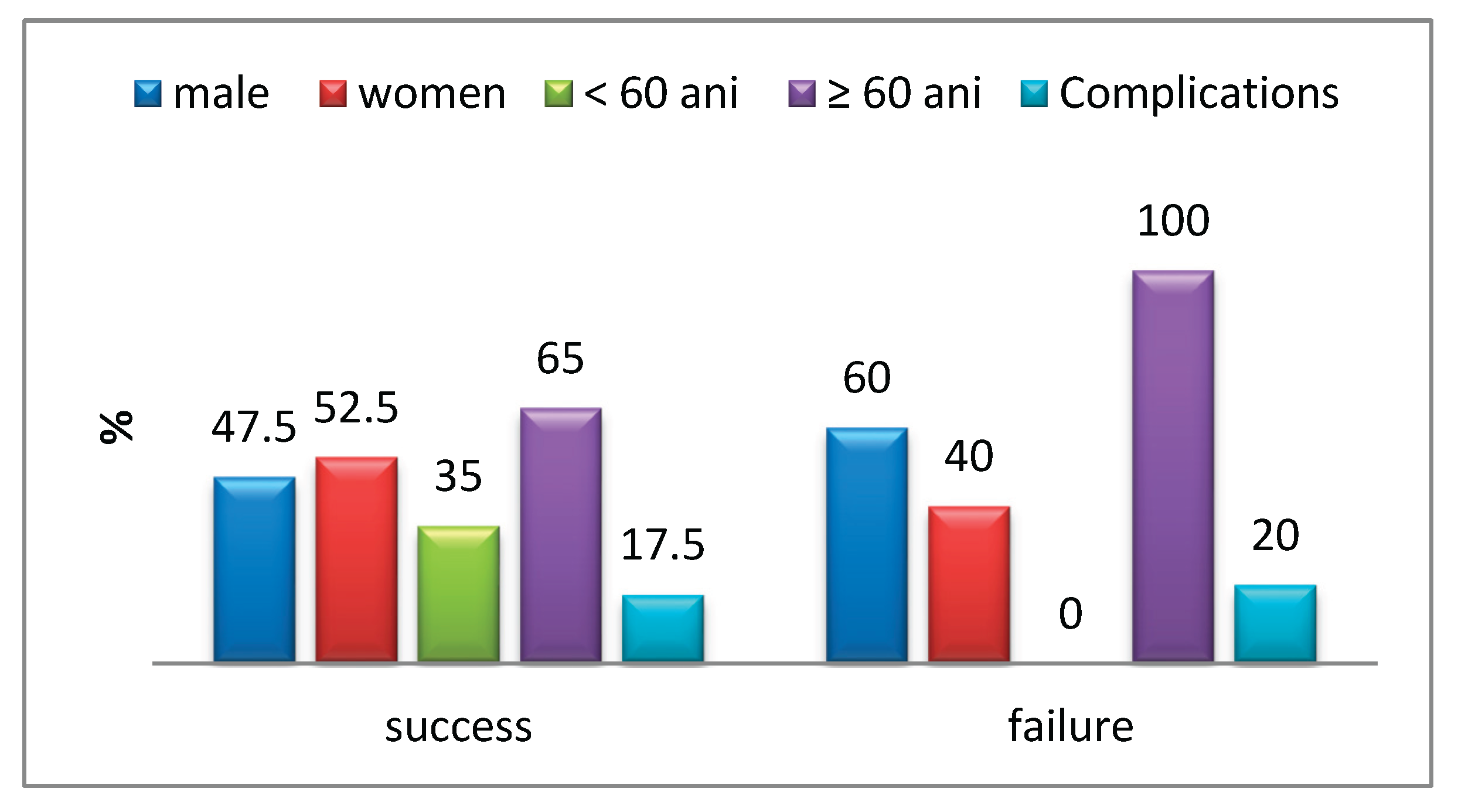
Figure 13.
Distribution of success/failure cases according to glaucoma type (p = 0.169) (Gsec – secondary glaucoma, PXG – pseudoexfoliative glaucoma, SOAG – sec-ondary open-angle glaucoma, POAG – primary open-angle glaucoma, PACG – primary angle-closure glaucoma).
Figure 13.
Distribution of success/failure cases according to glaucoma type (p = 0.169) (Gsec – secondary glaucoma, PXG – pseudoexfoliative glaucoma, SOAG – sec-ondary open-angle glaucoma, POAG – primary open-angle glaucoma, PACG – primary angle-closure glaucoma).
4. Discussion
The pandemic period posed significant challenges to healthcare systems world-wide. Various parameters were established to reduce the risk of contamination. The evaluation of glaucoma patients underwent several modifications to minimize the risk of transmission to examiners and other patients. Cross-contamination could be avoided through the use of disposable-tonometer tips [17]. Virtual reality perimetry has emerged as an alternative to conventional perimetry. For glaucoma suspects and con-firmed patients, imaging is preferred over visual field testing, as it carries a lower risk of cross-contamination, is easier to sanitize, and provides faster results [18]. Given that some studies suggest the potential presence of the virus in the conjunctival sac secre-tions of COVID-19 patients, instrument disinfection remains a critical recommendation [19,20]. Numerous studies from that period have emphasized the disruptive impact of the pandemic on the evaluation and management of glaucoma patients.
Our study is retrospective and includes patients who underwent surgery in a ter-tiary referral hospital in the region of Moldova, Romania - the only facility that remained operational during the pandemic, serving an extensive geographic area. According to our findings, the vast majority of cases treated during the pandemic were advanced and decompensated. This trend was attributed to reduced access to primary care providers, the absence of reimbursed prescriptions, and interruptions in treatment continuity. Furthermore, decompensation of associated systemic conditions such as hypertension and diabetes mellitus contributed to the increased incidence of decompensated neo-vascular glaucomas and proliferative diabetic retinopathies.
Globally, patterns of healthcare access during the pandemic differed markedly from the pre-pandemic period. A study conducted in India reported that, out of 8,296 glaucoma surgeries performed during the study period, secondary glaucoma accounted for the majority of cases requiring surgical intervention (62.5%) during the COVID-19 period. Among all surgical procedures, trabeculectomy and bleb-related interventions were the most commonly performed across all periods studied, including during the pandemic (42.6% in the pre-COVID period, 30% during COVID, and 39.8% post-COVID). Minimally invasive glaucoma surgeries (MIGS) increased in the post-COVID period, while the number of trabeculectomies decreased, paralleled by a rise in implant procedures during the pandemic - 11.7% (pre-COVID), 15% (COVID), and 10.8% (post-COVID) - correlating with the increased incidence of secondary glau-coma [4]. Another Indian study comparing surgical procedures demonstrated a pro-portional decrease in incisional glaucoma surgeries (60.86%) and a rise in emergency cataract surgeries (27.15%) and transscleral cyclophotocoagulation during 2020 com-pared to 2019 (8.16%).
In Poland, a study showed that the number of glaucoma surgeries dropped by 50% during the pandemic compared to a similar pre-pandemic period, with a significant difference in the types of procedures performed between the two groups. In the pre-pandemic group, the most common procedures were ExPress shunt implantation (33.7%) and trabeculectomy (31.5%). In the pandemic group, half of the eyes underwent trabeculectomy (50.0%), followed by Preserflo microshunt (11.6%), iStent (8.7%), and transscleral cyclophotocoagulation (TSCP) (8.7%). Thus, the COVID-19 pandemic was associated with a decline in extensive antiglaucoma procedures and an increase in shorter, less complex surgeries [3].
At a tertiary center in Verona, Italy, analysis of surgical volume and type during the pandemic year showed a 30% reduction in glaucoma surgeries. Only 24.3% of proce-dures were performed under general anesthesia, compared to 41.5% in the pre-pandemic period. The number of surgeries performed on eyes with advanced or end-stage glaucoma doubled. As in our study, most patients presented much later and with more advanced disease. The closure of the operating theater in the first quarter of the pandemic contributed to the increased number of advanced-stage cases [21].
In Germany, data from the Federal Joint Committee’s (G-BA) quality reports, which include information on glaucoma surgeries performed in 296 hospitals, were analyzed for the years 2019 through 2022. The total number of glaucoma surgeries decreased by 8.5% in 2020 compared to 2019 but returned to pre-pandemic levels in 2021. The number of traditional trabeculectomies steadily declined, while filtering devices that create blebs were used more frequently. Throughout all four years, cyclodestructive proce-dures remained the most commonly performed interventions [22].
In our study, all surgical procedures consisted of trabeculectomy. We observed a surge in advanced angle-closure glaucoma cases in 2021, along with an increase in surgeries on single functional eyes and lens-induced glaucomas. This contrasted with 2020, when secondary open-angle and primary open-angle glaucomas predominated. The pressure reduction rate was significant and comparable across all groups, with the highest reduction observed in 2021. The failure rate was significantly higher in patients with neovascular and pseudoexfoliative glaucoma. In all study groups, over 80% of cases achieved qualified success, while only 18% experienced failure. The incidence of in-traoperative and early postoperative complications was low, with early ocular hy-potony observed in 10 cases. Similar to our findings, literature from the same period highlights a predominance of secondary, neovascular, and acute glaucomas in advanced stages, often requiring emergency intervention. Prior to the COVID-19 pandemic, tra-beculectomy was the most preferred surgical technique for glaucoma [16,25], with var-ying rates of adoption among glaucoma specialists - 87% in the United Kingdom [24] and 62.8% in Italy [23].
Limitations and Perspectives. One ongoing challenge is ensuring that patients re-turn for follow-up visits to monitor disease progression. In the pre- and post-pandemic periods, telemedicine and teleconsultation have proven to be the most effective ap-proaches, although their effectiveness was limited during the pandemic. Due to the ongoing outbreak, routine outpatient services and elective procedures were suspended, with only emergency care being provided to hospitalized patients. Teleophthalmology, which had been a growing phenomenon for over a decade, became essential. Tele glaucoma may be useful for screening [26], diagnostic consultation [27,28], and long-term treatment monitoring [29,30,31]. This approach protects both the patient and physician by reducing physician exposure time and limiting patient visits to the hospital to only the most urgent situations.
5. Conclusions
Antiglaucoma surgery faced a series of challenges during the pandemic period compared to the non-pandemic period, despite being considered an emergency, due to reduced access to medical services. A notable increase in advanced angle-closure glaucoma cases was observed in 2021, along with a rise in surgeries on single functional eyes and lens-induced glaucomas, compared to 2020, when secondary open-angle and primary open-angle glaucomas were predominant.
The proportion of intraoperative and early postoperative complications was low, with early ocular hypotony being the most frequent, recorded in 10 cases. Additionally, in all study groups, more than 80% of patients achieved qualified success, with only 18% experiencing failure.
Glaucoma surgery requires in-depth knowledge of the procedure, awareness of potential intraoperative complications, and thorough preoperative preparation. Se-lecting the appropriate type of anesthesia (local or general), depending on the specific case (single functional eye, younger age, male sex, associated comorbidities), facilitates the surgeon’s task and helps to reduce cardiovascular risks.
Glaucoma surgery encountered a number of difficulties during the pandemic vs. non-pandemic period even though they were considered an emergency due to their low addressability. There has been an explosion of advanced cases of closed-angle glaucoma in 2021 and single-eye surgery as well as lens-induced glaucoma compared to 2020, where predominant open-angle and primary open-angle glaucoma predominated. The share of early intraoperative and postoperative complications was reduced, with early intraocular hypotonia predominating in 10 cases. In all study groups, over 80% had qualified success and only 18% failed. Although the study is based on a small number of patients, it reveals a low level of healthcare utilization among glaucoma patients who required surgical intervention during the pandemic compared to the non-pandemic period. This reduced access is primarily due to the limited number of healthcare insti-tutions available for evaluation, compounded by patients’ fear of contamination. As a result, a notable discrepancy emerged in the number of cases presented for assessment and treatment in the Moldavia region. Moreover, the absence of advanced home-based technologies for monitoring intraocular pressure (IOP), visual fields (e.g., home to-nometers, home visual field testing), along with the limited implementation of tele-medicine and teleophthalmology services, further impeded the evaluation of a broader patient population.
According to AAO and EGS guidelines, glaucoma is considered an ophthalmologic emergency, and surgery becomes imperative when intraocular pressure is uncontrolled, in order to prevent severe functional loss - regardless of whether the context is pan-demic or non-pandemic.
Author Contributions
Conceptualization, N.A. , F.C.D, A.V.F and M.D.; method-ology, I.-I.L.; soft-ware, M.D and, I.-I.L.; validation, N.A. and, R.I.B, F.C.D.; formal analysis, R.I.B. and R.A.P.; investigation, N.A., A.M.P and, F.C.D.; resources, N.A., R.E.C and A.M.P.; data curation, .; writing —original draft preparation, N.A., R.E.C, F.C.D; writ-ing—review and editing, N.A, and R.I.B, R.A.P, F.C.D .; visualization, N.A.; supervision, N.A.; project administration, N.A. and R.E.C; funding acquisition I-I.L and M.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Ethics Com-mission of the University Hospital Sf. Spiridon Iasi, approval no. 5657/7 March 2020, in compliance with the ethical and deontological rules for medical and research practice. This study was conducted in accordance with the Helsinki Declaration.
Informed Consent Statement
Written informed consent was obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets used and analyzed in this study are available from the corresponding author on reasonable request.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| VA | visual acuity |
| AAO | American Acadeny of Ophthalmology |
| EGS | European Glaucoma Society |
| IOP | Intraocular pressure |
| MMC | Mitomycin C |
References
- WHO, WHO Director-General’s opening remarks at the media briefing on COVID-19–11 March 2020, 2022, WHO, Geneva, Switzerland.
- Kshitija Mundle a , Brian Yu b, Monali S. Malvankar-Mehta c,d,*. Impact of the pandemic on clinical management of glaucoma . JFO Open Ophthalmology 5 (2024) 100080.
- Natalia Dub, Kinga Gołaszewska, Emil Saeed, Diana Anna Dmuchowska, Iwona Obuchowska and Joanna Konopi nska. Changes to glaucoma surgery patterns during the coronavirus disease 2019 pandemic: a shift towards less invasive procedures. ANNALS OF MEDICINE 2023, VOL. 55, NO. 1, 224–230 . [CrossRef]
- Aparna Rao, Sirisha Senthil. Effect of COVID-19 on glaucoma surgical practice in India: The challenges faced and the outcomes. . J Clin Ophthalmol Res 2023;11:114-8.
- Nguyen AX, Gervasio KA, Wu AY. Differences in SARSCoV- 2 recommendations from major ophthalmology societies worldwide. BMJ Open Ophthalmol. 2020;5(1):e000525.
- Gelman S, Cone FE, Pease ME, et al. The presence and distribution of elastin in the posterior and retrobulbar regions of the mouse eye. Exp Eye Res. 2010; 90(2):210–215.
- Frank Larkin. Effect of COVID-19 pandemic on glaucoma surgical practices in the UK. British Journal of Ophthalmology 2022; 106 i-ii Published Online First: 22 Sep 2022. [CrossRef]
- Subathra GN, Rajendrababu SR, Senthilkumar VA, Mani I, Udayakumar B. Impact of COVID-19 on follow-up and medication adherence in patients with glaucoma in a tertiary eye care centre in south India. Indian J Ophthalmol (2021) 69:1264–70. [CrossRef]
- Lešin Gaćina D, JandrokovićS, Vidas Pauk S, Škegro I, BoškovićJ, TomićM, et al. The medication adherence among glaucoma patients during the coronavirus disease 2019 pandemic in Croatia. Eur J Ophthalmol (2022) 32(5): 11206721221112150. [CrossRef]
- Racette L, Abu SL, Poleon S, Thomas T, Sabbagh N, Girkin CA. The impact of the coronavirus disease 2019 pandemic on adherence to ocular hypotensive medication in patients with primary open-angle glaucoma. Ophthalmology (2022) 129:258–66. [CrossRef]
- Awwad MA, Masoud M. Influence of COVID-19 on the prognosis and medication compliance of glaucoma patients in the Nile delta region. Clin Ophthalmol (2021) 15:4565–72. [CrossRef]
- Rizwan A, Ali M, Akhtar F, Sughra U, Naqvi SAH. Trickle down effects of covid-19 on glaucoma patients. Pak J Ophthalmol (2021) 37(3):274–8. [CrossRef]
- Killeen OJ, Pillai MR, Udayakumar B, Shroff S, Vimalanathan M, Cho J, et al. Understanding barriers to glaucoma treatment adherence among participants in south India. Ophthalmic Epidemiol (2020) 27(3):200–8. [CrossRef]
- Watane A, Yannuzzi NA, Sridhar J. Letter to the Editor: The impact of COVID-19 on the ophthalmic pharmaceutical supply. Optom Vis Sci (2021) 98:456–7. [CrossRef]
- Bala DS, Islam DNM, Mallick DS. Impact of Covid19 pandemic on visual field loss in glaucoma patients with irregular follow-up and medication adherence At a tertiary eye care centre in Eastern India(2022). Available at: https://www. wjpmr.com/abstract/4385 (Accessed August 16, 2022).
- Rajendrababu S, Durai I, Mani I, Ramasamy KS, Shukla AG, Robin AL. Urgent and emergent glaucoma care during the COVID-19 pandemic: An analysis at a tertiary care hospital in South India. Indian J Ophthalmol 2021;69:2215-21.
- Salvi SM, Sivakumar S, Sidiki SS. Use of disposable prism tonometry in routine clinical practice. Eye Lond Engl (2005) 19:743–6. [CrossRef]
- Tejwani S, Angmo D, Nayak BK, Sharma N, Sachdev MS, Dada T, et al. Preferred practice guidelines for glaucoma management during COVID-19 pandemic. Indian J Ophthalmol (2020) 68(7):1277–80. [CrossRef]
- Liang L, Wu P. There may be virus in conjunctival secretion of patients with COVID-19. Acta Ophthalmol (Copenh.) (2020) 98:223. [CrossRef]
- Seah IYJ, Anderson DE, Kang AEZ, Wang L, Rao P, Young BE, et al. Assessing viral shedding and infectivity of tears in coronavirus disease 2019 (COVID-19) patients. Ophthalmology (2020) 127:977–9. [CrossRef]
- Rosa Longo · Elia Franzolin · Emilio Pedrotti · Adriano Fasolo · Erika Bonacci · Giorgio Marchini. Glaucoma surgery during the first year of the COVID-19 pandemic. Int Ophthalmol (2022) 42:2881–2887 . [CrossRef]
- Philip Keye1,4 · Charlotte Evers2 · Timothy Gläser1 · Philip Braun1 · Patrick Thelen1 · Daniel Böhringer1 · Stefan Johann Lang3 · Thomas Reinhard1 · Jan Lübke. Impact of the COVID-19 pandemic on glaucoma surgery in German hospitals. Graefe’s Archive for Clinical and Experimental Ophthalmology . [CrossRef]
- Quaranta L, Micheletti E, Riva I. Glaucoma surgery during the COVID-19 pandemic in Italy: How novel coronavirus has changed the surgical management of glaucoma patients. J Glaucoma (2020) 29:831–2. [CrossRef]
- Holland LJ, Kirwan JF, Mercieca KJ. Effect of COVID-19 pandemic on glaucoma surgical practices in the UK. Br J Ophthalmol (2021) 0:1–5. [CrossRef]
- Gedde SJ, Feuer WJ, Shi W, Lim KS, Barton K, Goyal S, et al. Treatment outcomes in the primary tube versus trabeculectomy study after 1 year of follow-up. Ophthalmology (2018) 125:650–63. [CrossRef]
- Thomas S-M, Jeyaraman M, Hodge WG, Hutnik C, Costella J, Malvankar- Mehta MS. The effectiveness of teleglaucoma versus in-patient examination for glaucoma screening: A systematic review and meta-analysis. PloS One (2014) 9: e113779. [CrossRef]
- Kassam F, Sogbesan E, Boucher S, Rudnisky CJ, Prince W, Leinweber G, et al. Collaborative care and teleglaucoma: A novel approach to delivering glaucoma services in northern Alberta, Canada. Clin Exp Optom (2013) 96:577– 80. [CrossRef]
- Verma S, Arora S, Kassam F, Edwards MC, Damji KF. Northern Alberta remote teleglaucoma program: Clinical outcomes and patient disposition. Can J Ophthalmol (2014) 49:135–40. [CrossRef]
- Kotecha A, Baldwin A, Brookes J, Foster P. Experiences with developing and implementing a virtual clinic for glaucoma care in an NHS setting. J.Clin Ophthalmol Auckl NZ (2015) 9:1915–23. [CrossRef]
- Wright HR, Diamond JP. Service innovation in glaucoma management: using a web-based electronic patient record to facilitate virtual specialist supervision of a shared care glaucoma programme. Br J Ophthalmol (2015) 99:313–7. [CrossRef]
- Clarke J, Puertas R, Kotecha A, Foster PJ, Barton K. Virtual clinics in glaucoma care: face-to-face versus remote decision-making. Br J Ophthalmol (2017) 101:892–5. [CrossRef]
Figure 1.
The distribution of the patient group by year of surgery was as follows: 2019 – 18%, 2020 – 22%, 2021 – 49%, and 2022 – 11%.
Figure 1.
The distribution of the patient group by year of surgery was as follows: 2019 – 18%, 2020 – 22%, 2021 – 49%, and 2022 – 11%.
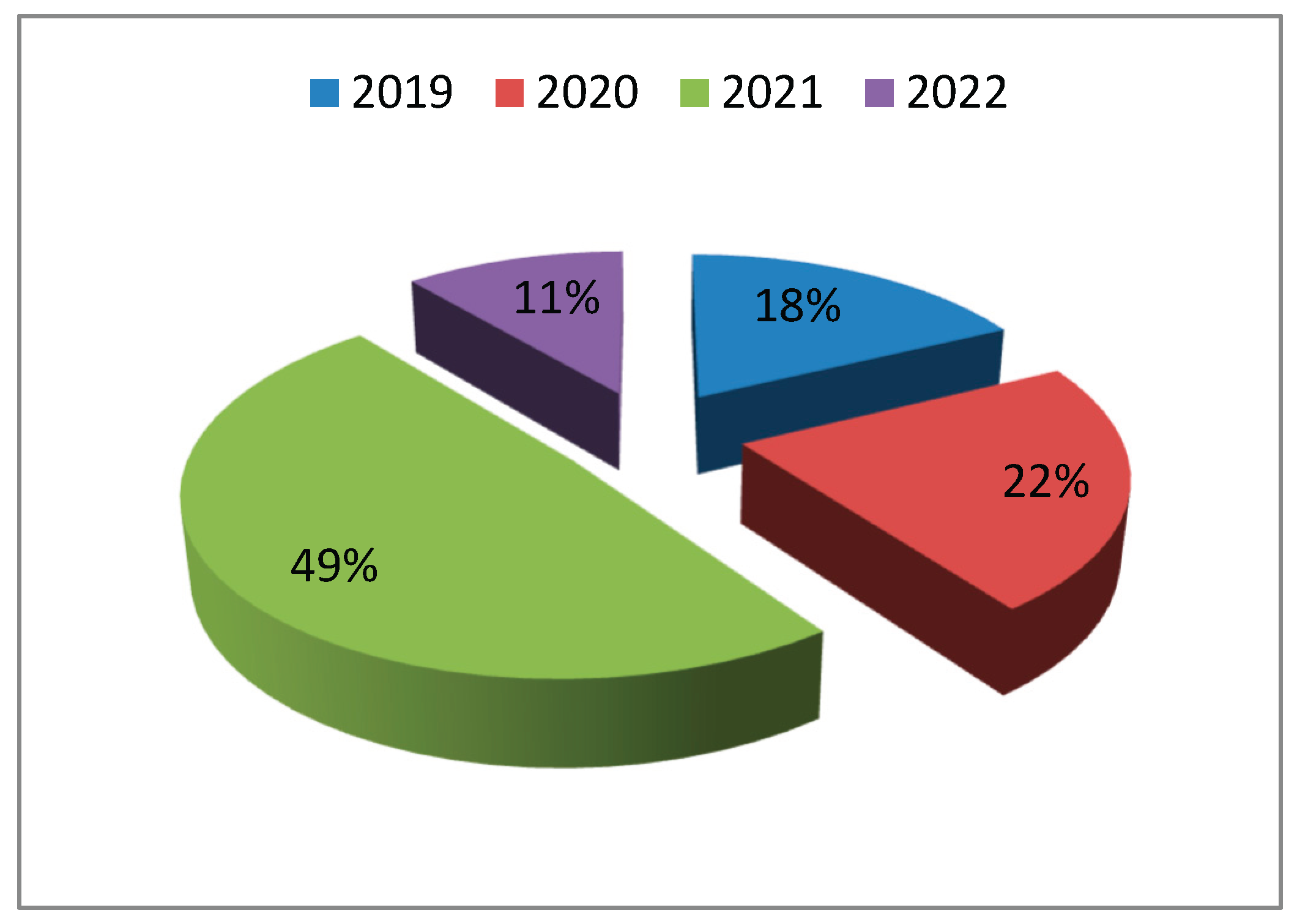
Figure 2.
The distribution of cases by year of study according to glaucoma type was as follows: Gsec – secondary glaucoma, PXG – pseudoexfoliative glaucoma, SOAG – secondary open-angle glaucoma, POAG – primary open-angle glaucoma, and PACG – primary angle-closure glaucoma.
Figure 2.
The distribution of cases by year of study according to glaucoma type was as follows: Gsec – secondary glaucoma, PXG – pseudoexfoliative glaucoma, SOAG – secondary open-angle glaucoma, POAG – primary open-angle glaucoma, and PACG – primary angle-closure glaucoma.
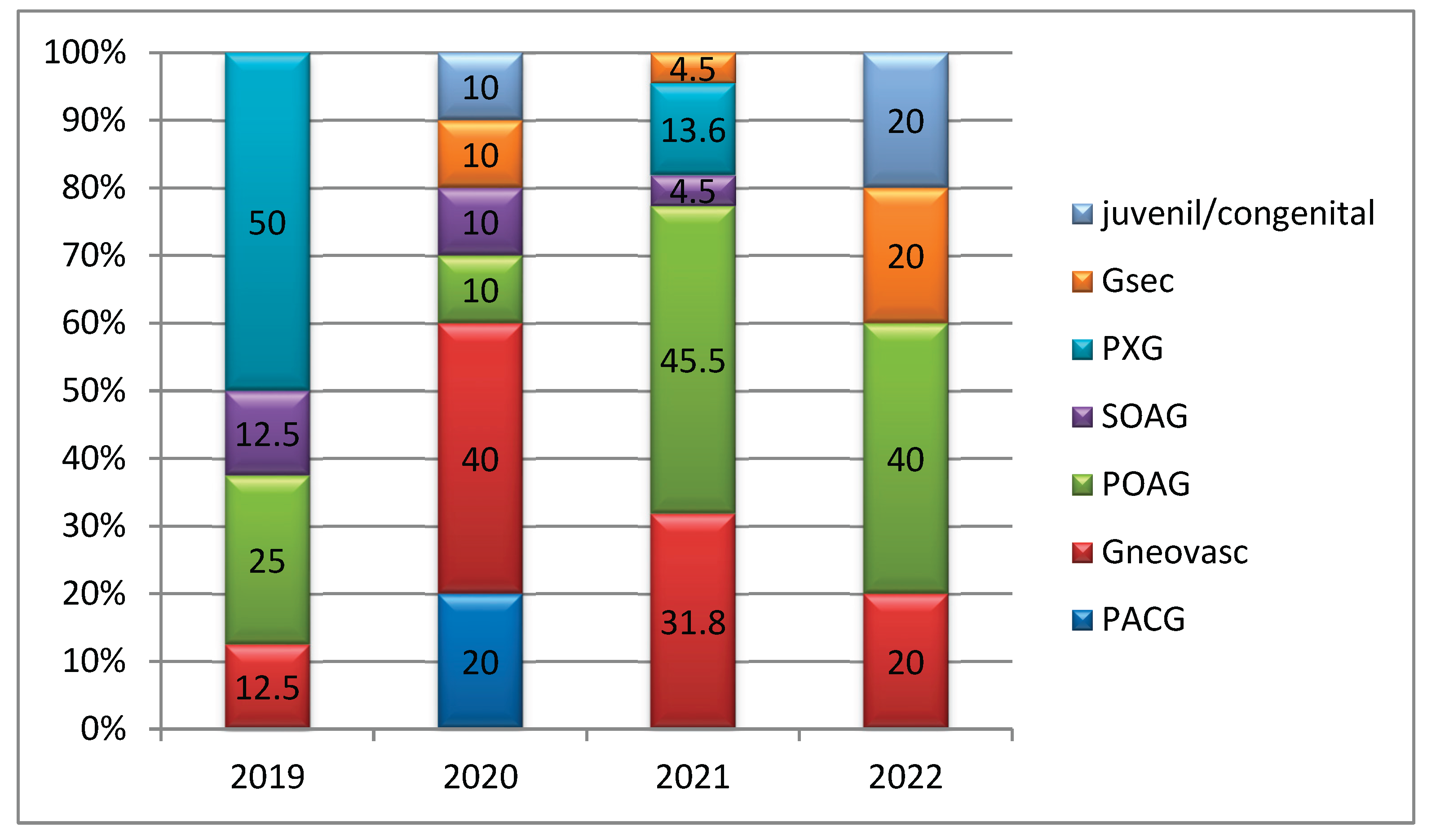
Figure 3.
The distribution of anesthesia types by year of study included the following categories: potentiated + retrobulbar, retrobulbar alone, topical, and general anesthesia.
Figure 3.
The distribution of anesthesia types by year of study included the following categories: potentiated + retrobulbar, retrobulbar alone, topical, and general anesthesia.
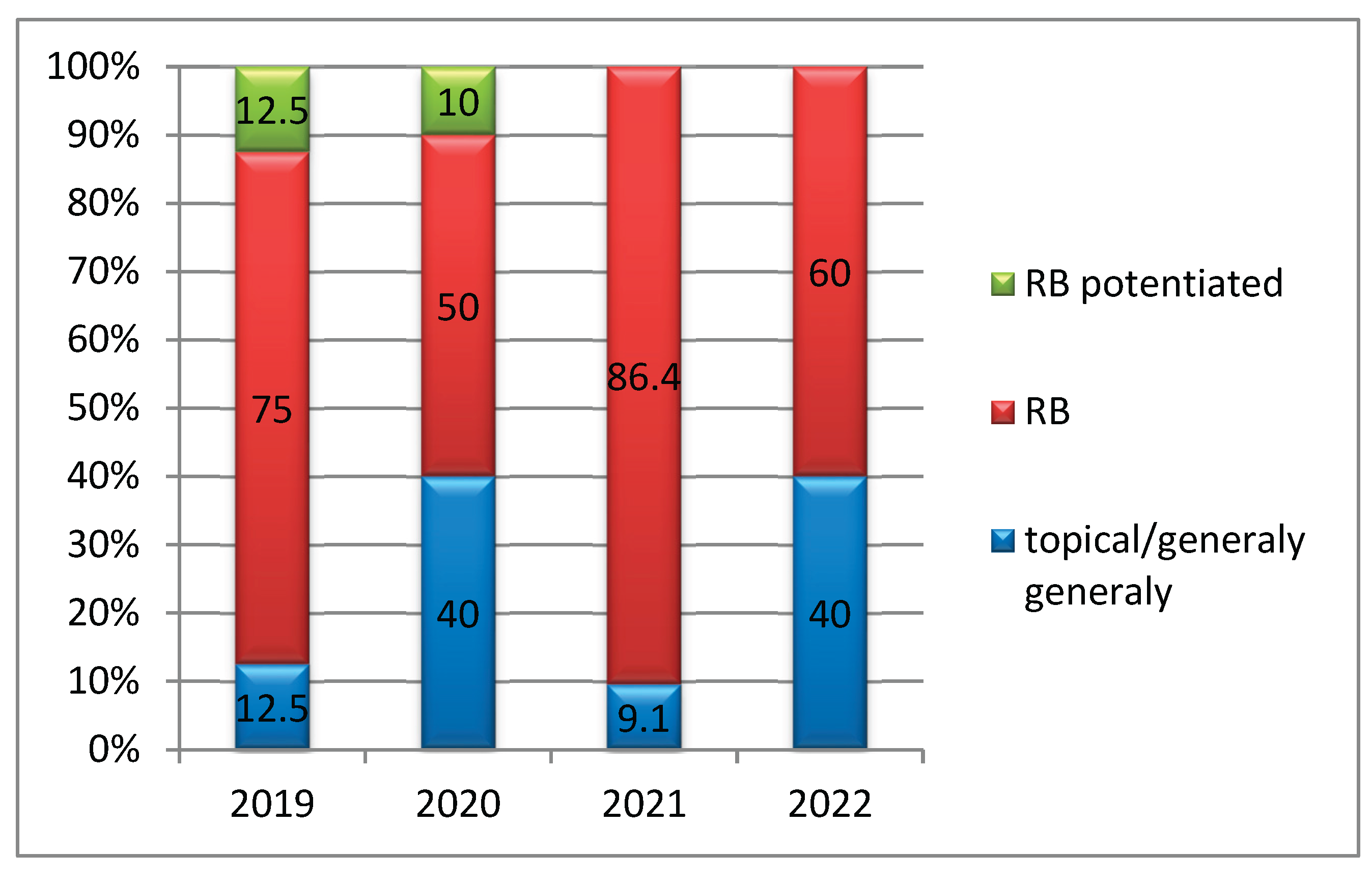
Figure 5.
The number of antiglaucoma medications administered to patients across all study years (2019–2022), both preoperatively and postoperatively, was recorded and analyzed.
Figure 5.
The number of antiglaucoma medications administered to patients across all study years (2019–2022), both preoperatively and postoperatively, was recorded and analyzed.
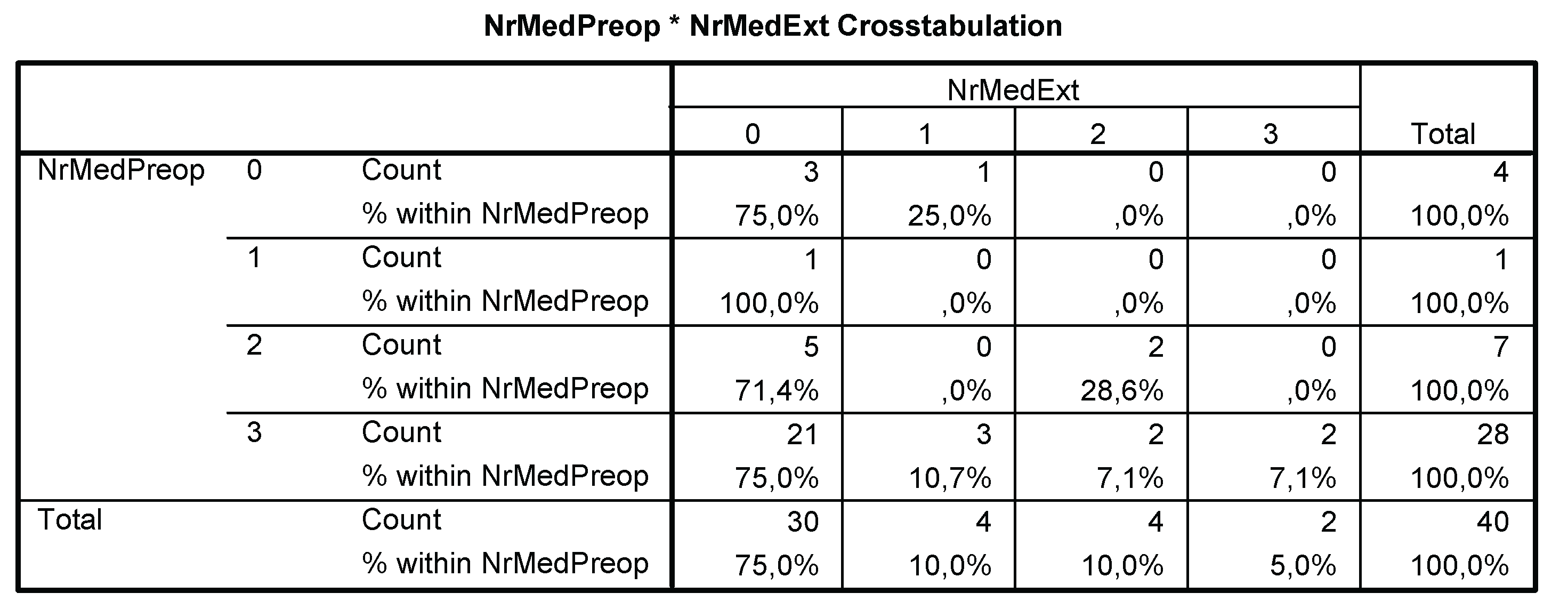
Figure 8.
The mean intraocular pressure (IOP) values, both preoperative and postoperative, were recorded for each year of the study period (2019–2022).
Figure 8.
The mean intraocular pressure (IOP) values, both preoperative and postoperative, were recorded for each year of the study period (2019–2022).
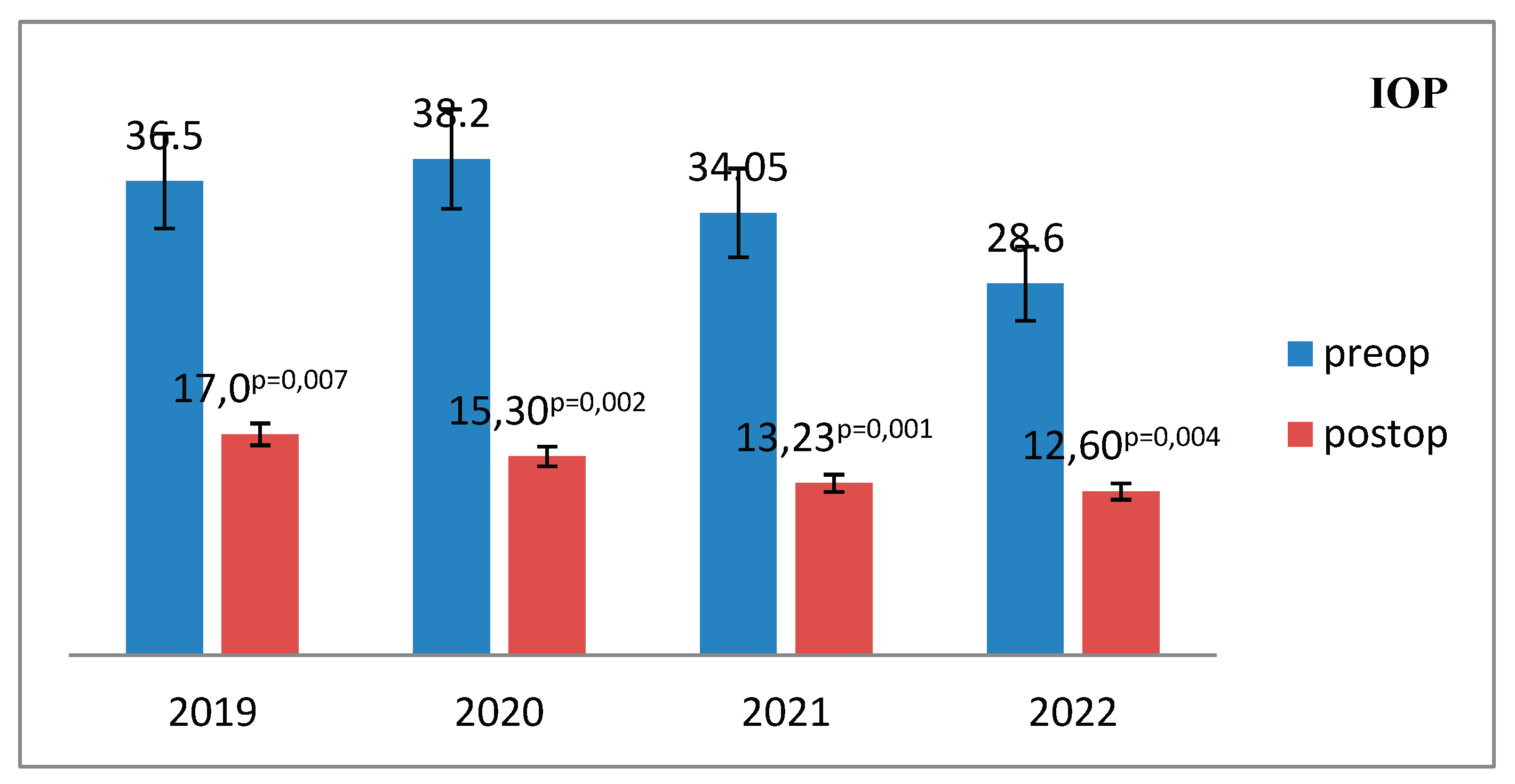
Figure 9.
The mean level of pressure reduction at discharge by year of study.
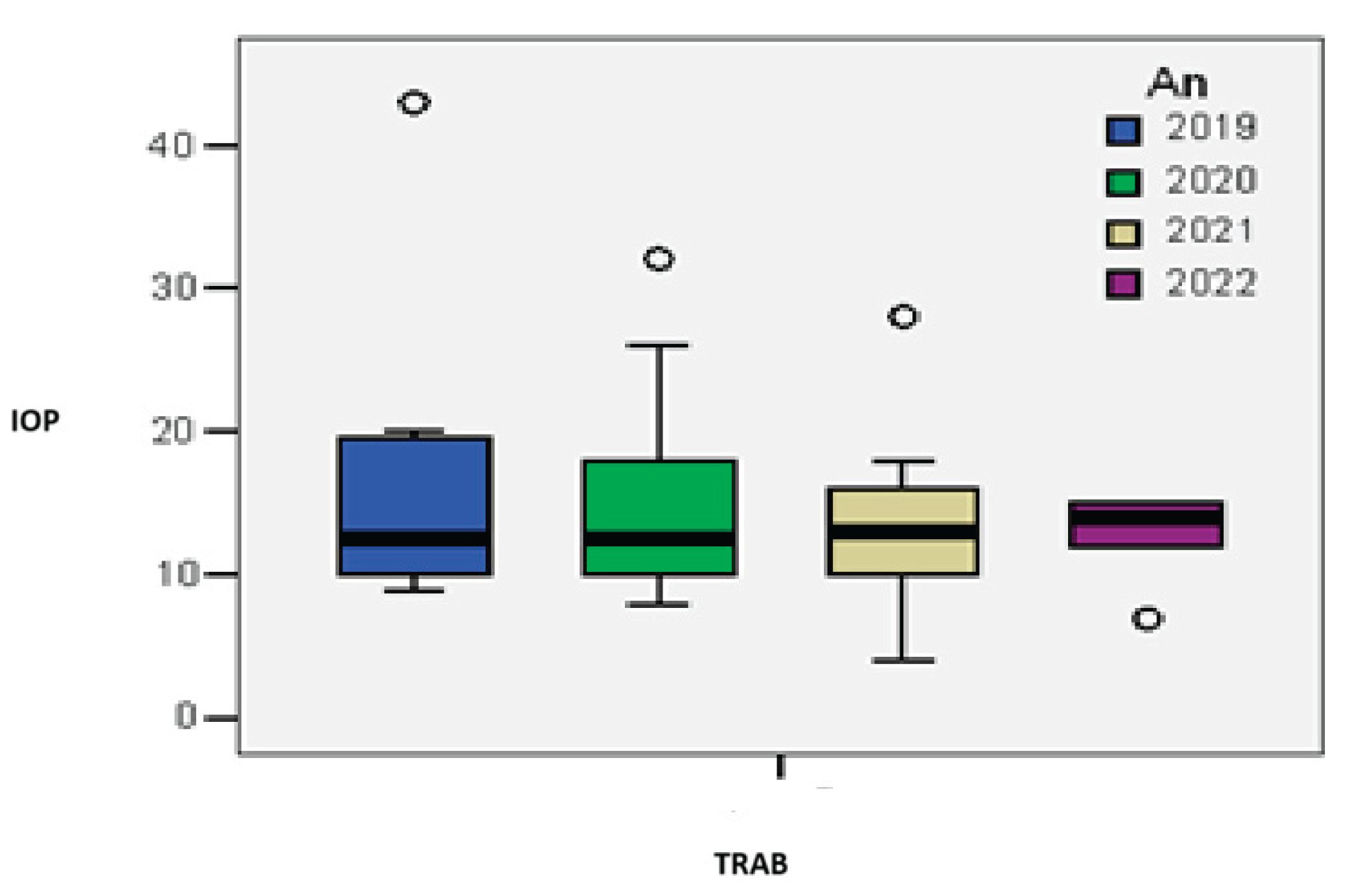
Figure 10.
Distribution of cases by year of study according to the presence of complications during the 2019–2022 study period (p = 0.026).
Figure 10.
Distribution of cases by year of study according to the presence of complications during the 2019–2022 study period (p = 0.026).
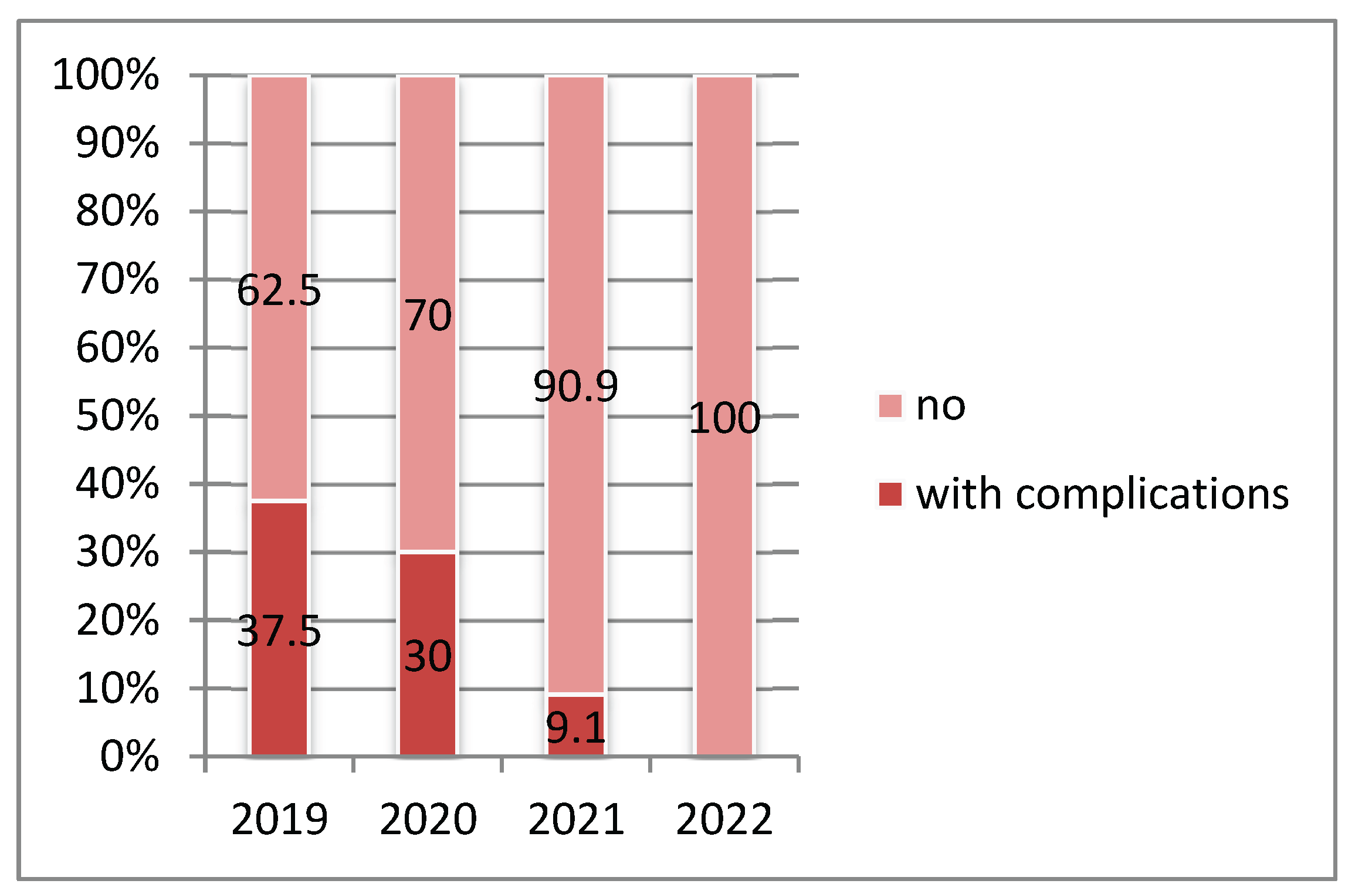
Figure 11.
Linear regression model of the failure rate based on the presence of complications.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



