Submitted:
23 August 2025
Posted:
25 August 2025
You are already at the latest version
Abstract
Cardiac resynchronization therapy (CRT) represents a cornerstone in the management of patients with heart failure and electrical dyssynchrony, improving symptoms, reducing hospitalizations, and prolonging survival. CRT can be delivered via a pacemaker (CRT-P) or an ICD (CRT-D). Despite its widespread use, the mortality benefit of CRT-D over CRT-P remains uncertain, as no head-to-head randomized trials have been designed to directly compare the two modalities, making device selection a frequent clinical dilemma. In practice, CRT-D accounts for 70–80% of CRT implantations in developed countries, yet solid evidence demonstrating its superiority over CRT-P is lacking. Specific patient groups including those with non-ischemic cardiomyopathy, advanced age, multiple comorbidities, or limited life expectancy, may derive limited incremental benefit from CRT-D, which should be balanced against device specific risks such as lead failure and inappropriate shocks. The present review aims to provide a comprehensive comparison between CRT-D and CRT-P, focusing on the existing body of evidence, criteria for patient selection, comparative clinical outcomes, and risk-benefit considerations for clinical decision-making.
Keywords:
CRT‑D
; CRT‑P
; sudden cardiac death
1. Introduction
Heart failure remains a leading cause of morbidity and mortality worldwide, affecting 1-2% of the adult population, with a rising prevalence mainly due to ageing [1,2,3]. Patients with heart failure and left ventricular dysfunction commonly exhibit significant intraventricular conduction delay, resulting in electrical dyssynchrony, exacerbating cardiac function [4,5]. Cardiac Resynchronization Therapy (CRT) has emerged as a cornerstone therapeutical intervention for such patients, aiming to achieve coordinated biventricular contraction and improve hemodynamic performance [6,7,8,9], raising the number of CRT implantations up to 76% from 2010 to 2019 [10]. Multiple randomized clinical trials (RCTs) have shown reduced mortality and hospitalizations as well as improvement of symptoms and quality of life in patients with heart failure and reduced left ventricular ejection fraction (LVEF) receiving a CRT device [6,7,9,11,12].
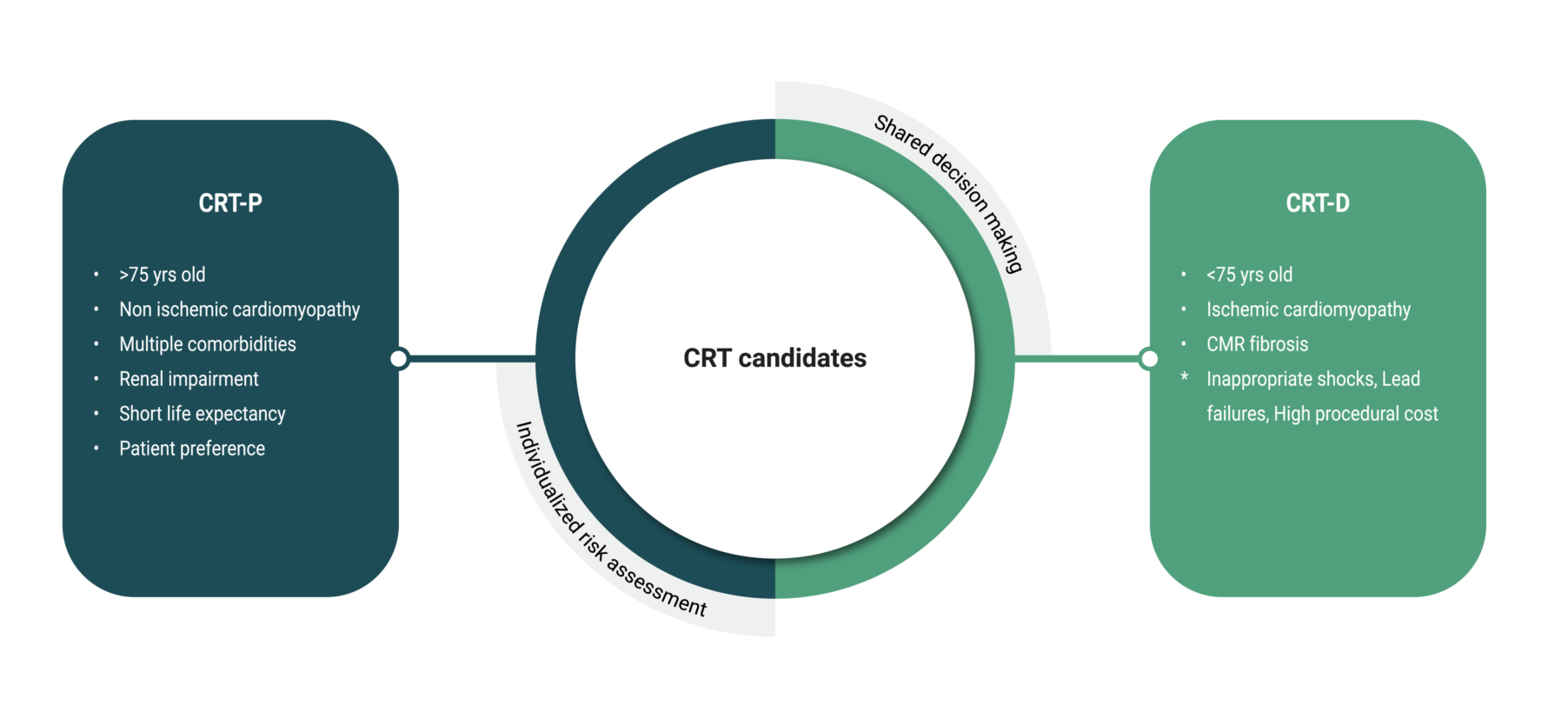
CRT can be delivered via cardiac resynchronization therapy with a pacemaker (CRT-P) and cardiac resynchronization therapy with a defibrillator (CRT-D). The mortality benefit of CRT-D compared to CRT-P remains uncertain, primarily due to the absence of head-to-head RCTs specifically designed to compare these two therapeutic modalities. Selecting the most appropriate device type requires an individualized risk assessment that takes into account multiple factors, including the underlying etiology, presence of myocardial scar tissue, patient age, comorbidities, and overall life expectancy. ICD-specific risks such as inappropriate shocks, lead failure and high cost should also be considered.
This review aims to provide a comprehensive comparison between CRT-D and CRT-P, focusing on the existing body of evidence, criteria for patient selection, comparative clinical outcomes, and key considerations for clinical decision-making.
2. Clinical Effectiveness of CRT
Current understanding and clinical use of CRT is based on landmark RCTs conducted since 2002. The MIRACLE trial was the first prospective study to demonstrate the effectiveness of CRT over a six-month follow-up period in patients with moderate-to-severe heart failure and intraventricular conduction delay, as compared with medical treatment [11]. Similar results were reported in CARE-HF trial, where patients at NYHA III-IV receiving CRT experienced significant improvement in quality of life and clinical outcomes as opposed to those treated with medication alone [13,14]. Along this line, patients with advanced heart failure, wide QRS interval and CRT exhibited reduced combined risk of death from any cause or hospitalization in the COMPANION trial, the only study to randomize patients to CRT-D or CRT-P, however the study was designed to assess the effectiveness of CRT compared to medical treatment [7]. Patients with mild heart failure (NYHA I-II) also benefit from CRT, as shown in MADIT-CRT [8], RAFT [9] and REVERSE [12] clinical trials. The major clinical trials of CRT are summarized in Table 1.
3. CRT Indications
CRT is recommended in selected patients with heart failure who remain symptomatic despite optimal guideline-directed medical therapy (OGMT). According to the 2021 ESC Guidelines on cardiac pacing and resynchronization therapy, CRT-D is indicated in patients with left ventricular ejection fraction (LVEF) ≤ 35%, sinus rhythm, and a widened QRS complex, particularly with left bundle branch block (LBBB) morphology [21]. The greatest benefit is observed among those with QRS duration ≥ 150 ms. Additionally, patients with atrial fibrillation (AF) may be candidates for CRT, given that adequate biventricular pacing can be ensured, either with medical treatment or following AV nodal ablation [21]. Patients who have received a conventional ICD and who subsequently develop symptomatic HF with LVEF≤ 35% despite OGMT, and who have a significant proportion of RV pacing, should be considered for CRT upgrade [22,23].
4. CRT-D or CRT-P
Should all patients with a CRT indication receive a defibrillator lead? The choice between the two is a frequent clinical dilemma. Recent survey studies have shown that CRT-D devices account for over 70–80% of all CRT implantations in developed countries [24,25,26]. However, this widespread use of CRT-D is not supported by solid evidence demonstrating its superiority over CRT-P.
In a post-hoc analysis of the COMPANION study, CRT-D was associated with 36% mortality risk reduction as compared to CRT-P and regarding the cause of death, CRT-D rather than CRT-P significantly reduced sudden cardiac death (SCD) [(HR 0.44, 95% CI 0.23 - 0.86; P = 0.02) and (HR 1.21, 95% CI 0.7-2.07; P = 0.50) respectively] [7]. Importantly though, the COMPANION trial was underpowered to detect a survival benefit from CRT-D. A network meta-analysis of 13 randomized clinical trials including >12.000 patients found that CRT-D reduced total mortality by 19% (95% CI 1-33%, unadjusted) compared with CRT-P [27]. Similar results were reported in a propensity-matched cohort, where CRT-D was associated with a significantly lower all-cause mortality than CRT-P in patients with heart failure of ischemic etiology and in patients with non-ischemic heart failure below 75 years of age [28]. Accordingly, recently published meta-analysis of 26 observational studies including 55.469 CRT-P patients and 72.561 CRT-D patients, showed that patients with CRT-D had 26% lower risk of all-cause mortality compared with CRT-P. However, patients aged > 75 years old and those with non-ischemic heart failure were less-likely to benefit from a CRT-D [29]. Along this line, a previous meta-analysis focused on non-ischemic cardiomyopathy (NICM) reported that the addition of a defibrillator was not significantly associated with a reduction in all-cause mortality in CRT-eligible patients [30]. The DANISH trial had similarly reported no significant difference in mortality risk in patients with NICM between the ICD and no-ICD arm, irrespective of CRT [31]. Likewise, data from observational studies from Kutyifa et al. and Barra et al. suggest substantial (24–30%) mortality benefit from CRT-D only in patients with ischemic cardiomyopathy [32,33]. Contradictory though results were reported in another meta-analysis assessing the effect of CRT-P versus CRT-D on mortality in patients with NICM, where CRT-D was associated with significantly lower all-cause mortality (log HR − 0.169, SE 0.055; p = 0.002) as compared to CRT-P [34]. CRT with pacing only was reported to be non-inferior to CRT-D in the retrospective observational RESET-CRT study, in an overall population of 3.569 patients with both ischemic and non-ischemic heart failure [20].
Although CRT-D may offer additional survival benefit over CRT-P reducing sudden cardiac death (SCD) risk [7], there is data that CRT-P alone could confer SCD risk reduction. In particular, in the CARE HF extended study CRT-P reduced SCD risk by 5.6% [35]. Accumulating data from subgroup analyses from RCTs suggest that SCD risk is related to the extent of reverse LV remodeling with CRT, thus CRT responders are at lower risk for malignant ventricular arrhythmias and SCD than non-responders [36,37]. Women are shown to be better responders with higher percentage of biventricular pacing, improved rates of death and fewer hospitalizations, as compared to male counterparts, although they are underrepresented in CRT trials and less likely to receive CRT-D [38]. Current medical treatment may mitigate ventricular arrhythmia risk, particularly the use of sacubitril/valsartan and sodium-glucose co-transporter-2 inhibitors (SGLT2i) [39,40]. Increasing comorbidities on the other hand are associated with a mortality risk that competes with sudden arrhythmic death. The incremental benefit of an ICD is questioned in certain clinical settings. High comorbidity burden such as advanced age, chronic kidney disease, diabetes and peripheral vascular disease, is significant predictor of mortality in CRT-D recipients, attenuating survival benefit of ICD therapy [41,42,43,44]. Data from observational studies suggest that the addition of ICD has no impact on survival in elderly patients undergoing implantation of a CRT device [45,46]. Adding ICD to CRT seems a better option for the younger patients with good survival prognosis. Contrast-enhanced CMR-guided scar adds valuable information concerning the risk of ventricular arrhythmia. According to Gaudi CRT study, the presence of myocardial scar independently can predict appropriate ICD therapies and SCD in CRT patients [47]. Similarly, patients with NICM and left ventricular midwall fibrosis in CMR benefit from CRT-D than CRT-P [48].
As no head-to-head RCTs directly comparing CRT-D to CRT-P have been developed, the mortality benefit of CRT-D is not established. Defibrillator-specific complications, including inappropriate shocks, lead failures, and increased procedural costs are important issues to be considered [21]. It is crucial thus to reassess and refine patient selection criteria in order to identify which individuals will truly benefit from the addition of a defibrillator component. Table 2 and Table 3 summarizes existing studies and meta-analyses respectively on the effect of CRT on mortality in patients with ischemic and non-ischemic cardiomyopathy.
5. Our 2-Step Approach
A two-step, multifactorial, electrophysiology (EP)-guided approach was proposed for risk stratification and management of post-myocardial infarction patients [49]. According to current guidelines ICD is suggested in patients with LVEF<35% for primary prevention. However, the PRESERVE EF study revealed a high-risk subpopulation among those with preserved LVEF, who received an ICD following inducible sustained monomorphic ventricular tachycardia during PVS. The authors propose a stepwise approach, involving the assessment of non-invasive risk factors (NIRFs) such as LVEF, late potentials, ventricular premature beats, non-sustained ventricular tachycardia, heart rate variability, T wave alternans, QT prolongation, deceleration capacity and heart rate turbulence [49,50]. The presence of at least one NIRF leads to subsequent programmed ventricular stimulation (PVS), and according to inducibility of sustained monomorphic ventricular tachycardia (SMVT), to ICD implantation. Risk stratification for SCD in NICM is also traditionally based on LVEF, although LVEF as sole criterion cannot accurately identify truly high-risk individuals [51]. The results from the DANISH trial questioned the utility of ICDs in NICM and low LVEF [31], while at the same time a considerable SCD risks exists among those with mildly reduced and preserved LVEF [52,53]. Similar to ICM two-step EP-guided risk stratification approach has been suggested for patients with NICM and preserved ejection fraction, with pending results [54,55]. Unexplained syncope and LGE presence have been added in the risk stratification algorithm of the ReCONSIDER study [54,56]. A recently published comparative analysis of ICD efficacy in patients with ICM and NICM showed clear benefit in ICM whereas no significant reduction in mortality or ventricular arrhythmias was shown in ICM [57]. Thus, patients with a CRT-D indication who are questionable whether they will benefit from a defibrillator lead, such as the elderly, or patients with multiple comorbidities, or patients with NICM, could be subjected to this multifactorial strategy, in order to assess SCD risk, facilitating decision making. Likewise, patients with a pacemaker who become eligible for CRT upgrade could be subjected to non-invasive programmed stimulation (NIPS) via the device in order to assess arrhythmic risk and proceed to CRT-D implantation [58].
Refinement of patient selection criteria is particularly warranted in NICM, where adjunctive tools such as CMR and genetic testing are gaining ground and together with EPS provide valuable guidance for risk stratification and clinical decision-making [59,60]. CMR provides reliable information about biventricular function and myocardial substrate through late gadolinium enhancement (LGE) and advanced tissue mapping techniques. The extent and distribution of myocardial scar, especially in ischemic cardiomyopathy, are closely linked to the risk of ventricular arrhythmias and sudden cardiac death; in such patients, the addition of defibrillator therapy may be justified. In NICM, mid-wall fibrosis detected by LGE or diffuse fibrosis identified by T1 mapping has also been associated with increased arrhythmic risk, potentially favoring CRT-D over CRT-P. A range of CMR parameters have been associated with SCD, including presence and extent of LGE, T1 relaxation times, and myocardial strain [61,62]. For example, 252 patients with NICM and CRT, of whom 68 had LGE, were prospectively followed and what was observed was that CRT-D was associated with significantly higher survival than CRT-P only in patients with LGE. In patients without LGE, with their low arrhythmic risk, CRT-D offered no benefit compared with CRT-P [10]. Parallel advances in cardiogenetics have improved our understanding of the complex genetic architecture of dilated cardiomyopathy [63]. Identifying a causative gene variant in a patient with DCM improves prognostic accuracy regarding disease progression and may contribute to the indications for device implantation. In specific, variants in genes such as LMNA, RBM20, PLN, and BAG3 are consistently associated with a worse prognosis and are recognized as risk modifiers for the primary prevention of sudden cardiac death [64,65]. Similarly, pathogenic or likely pathogenic variants in FLNC or desmosomal genes (e.g., DSP, DES) confer an increased susceptibility to ventricular arrhythmias and/or progression to heart failure [66]. Of note, previously published guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death, proposed PVS as a risk factor along with syncope, LGE in CMR and pathogenic mutations in certain genes, in the suggested SCD risk stratification algorithm [67]. Currently, artificial intelligence (AI) is emerging as a complementary tool to imaging and genomics in cardiomyopathies [63,68]. By integrating multimodal data, AI may provide new insight advancing our understanding of cardiomyopathies and potentially refining the choice between CRT-D and CRT-P. Although early in clinical use, AI offers a promising path toward precision medicine.
6. CRT Non-Responders
Non-responders to CRT comprise a rather non negligeable amount of CRT receivers and nonresponse to CRT has been related to right ventricular dysfunction. Approximately 30% of patients fail to exhibit clinical or echocardiographic improvement with CRT [69], partly attributed to the non-physiologic electrical resynchronization between an epicardial wavefront from the CS lead and the RV endocardium, suboptimal lead position, presence of LV scar, and latency due to localized conduction delay [70]. Moreover, in 5-7% of the case CS lead implantation may be unsuccessful, because of anatomic challenges, high pacing thresholds, or phrenic nerve stimulation [71]. Several approaches have been proposed to address this issue, including direct pacing of the conduction system (His bundle or left bundle branch pacing), pacing the left ventricle from multiple sites within the coronary sinus (multipoint pacing), or preferential LV pacing [72,73,74].
It is noteworthy that biventricular pacing may be complicated by ventricular proarrhythmia in the early post implantation period, a rare but clinically significant phenomenon [75,76,77,78,79]. For example, VT storm occurred in 4% of the 191 patients included in a prospective study examining the incidence of VT storm after CRT-D implantation [77]. Similarly, 5 of 145 consecutive patients (3.4%) receiving a CRT device over a 4-year period experienced ventricular tachyarrhythmia after initiation of biventricular pacing, in a case series study [80]. The causes of the proarrhythmogenicity are multiple. The reversal of the direction of the activation of the LV wall, from the epicardium to the endocardium, results in prolongation of repolarization that may trigger polymorphic VT. Secondarily, pacing close to or within myocardial scar and regions of slow conduction may increase the likelihood of VT. CRT responders though are less likely to experience ventricular proarrhythmia, compared to non-responders [81]. Data suggest a modest effect of biventricular pacing on the incidence of new-onset atrial fibrillation as well [75]. Conduction system pacing through more physiological pacing and more effective resynchronization promotes remodeling providing a less arrhythmogenic substrate compared with biventricular pacing.
7. Role of Conduction System Pacing
Conduction system pacing (CSP)—whether His bundle pacing (HBP) or left bundle branch area pacing (LBBAP)—has emerged as a possible alternative to achieve cardiac resynchronization [72,82,83,84]. HBP has been associated with higher pacing thresholds, lower implantation success rates, and significant rates of crossover to other pacing modalities [85,86]. Recently, LBBAP has been proposed as viable and effective alternative to HBP, offering higher procedural success and lower pacing thresholds [87,88]. In LEVEL-AT, a single-center, prospective, randomized, parallel, controlled, clinical trial patients allocated to biventricular pacing or CSP (either HBP or LBBP) presented similar degrees of cardiac resynchronization, ventricular reverse remodeling, and clinical outcomes [72]. LBBP-CRT demonstrated greater LVEF improvement than BiVP-CRT in heart failure patients with nonischemic cardiomyopathy and LBBB in a prospective randomized trial of 40 patients [82]. Data from an observation retrospective study including 1.778 eligible patients, suggest improved clinical outcomes in those receiving LBBAP compared with BVP [89]. Along this line, findings from a systematic review and meta-analysis including 3141 patients indicate reduced mortality and hospitalizations in LBBAP receivers compared to BVP [90]. Upgrading to LBBP is feasible and effective in CRT non-responders, achieving marked cardiac function improvement and better clinical outcomes, rendering it a reasonable alternative pacing strategy [75]. Table 4 summarizes clinical trials on CSP vs CRT.
8. Conclusions
Due to lack of robust clinical evidence, the choice between CRT-D and CRT-P should be based on shared decision making and individualized risk assessment. The two step EP-guided approach could serve as a risk stratification tool. Factors that should be taken into account are age, the etiology of heart failure, life expectancy, major comorbidities, poor renal function, and of course, patient preference. Conduction system pacing is an emerging pacing modality as an alternative to CRT. Further studies are needed to identify subpopulations of patients with indications for CRT who will benefit the most from CRT-D implantation, justifying device related risks as compared to CRT-P alone.
Author Contributions
Conceptualization, D.T. and KA.G.; data curation, CK.A., A.K., P.A., O.K, AI.V.; writing—original draft preparation, A.L., I.D., A.X., writing—review and editing, A.L.,D.T., KA.G.; visualization, A.E.K., N.M., S.A., P.D; supervision, D.T., KA.G, C.T.; project administration P.X, S.S., S.S. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CRT | Cardiac Resynchronization Therapy |
| RCTs | Randomized clinical trials |
| LVEF | Left ventricular ejection fraction |
| LBBB | Left bundle branch block |
| AF | Atrial fibrillation |
| RV | Right ventricular |
| OGMT | Optimal guideline-directed medical therapy |
| PVS | Programmed ventricular stimulation |
| NIRFs | Non-invasive risk factors |
| NIPS | Non-invasive programmed stimulation |
| EP | Electrophysiology |
| SCD | Sudden cardiac death |
| SMVT | Sustained monomorphic ventricular tachycardia |
| CSP | Conduction system pacing |
| HBP | His bundle pacing |
| LBBAP | Left bundle branch area pacing |
| CMR | Cardiac magnetic resonance |
| NICM | Non ischemic cardiomyopathy |
| ICM | Ischemic cardiomyopathy |
| LGE | Late gadolinium enhancement |
| DCM | Dilated cardiomyopathy |
References
- Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. 2018 Feb 10;391(10120):572–80.
- Dunlay SM, Weston SA, Jacobsen SJ, Roger VL. Risk factors for heart failure: a population-based case-control study. Am J Med. 2009 Nov;122(11):1023–8.
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020 Mar 3;141(9):e139–596.
- Leclercq C, Hare JM. Ventricular resynchronization: current state of the art. Circulation. 2004 Jan 27;109(3):296–9.
- Leclercq C, Kass DA. Retiming the failing heart: principles and current clinical status of cardiac resynchronization. J Am Coll Cardiol. 2002 Jan 16;39(2):194–201.
- Cleland JGF, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005 Apr 14;352(15):1539–49.
- Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004 May 20;350(21):2140–50.
- Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009 Oct 1;361(14):1329–38.
- Tang ASL, Wells GA, Talajic M, Arnold MO, Sheldon R, Connolly S, et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med. 2010 Dec 16;363(25):2385–95.
- Leyva F, Zegard A, Patel P, Stegemann B, Marshall H, Ludman P, et al. Improved prognosis after cardiac resynchronization therapy over a decade. Europace. 2023 Jun 2;25(6):euad141.
- Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, et al. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002 Jun 13;346(24):1845–53.
- Linde C, Abraham WT, Gold MR, St John Sutton M, Ghio S, Daubert C, et al. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008 Dec 2;52(23):1834–43.
- Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, et al. The CARE-HF study (CArdiac REsynchronisation in Heart Failure study): rationale, design and end-points. Eur J Heart Fail. 2001 Aug;3(4):481–9.
- Cleland JGF, Freemantle N, Erdmann E, Gras D, Kappenberger L, Tavazzi L, et al. Long-term mortality with cardiac resynchronization therapy in the Cardiac Resynchronization-Heart Failure (CARE-HF) trial. Eur J Heart Fail. 2012 Jun;14(6):628–34.
- Auricchio A, Stellbrink C, Sack S, Block M, Vogt J, Bakker P, et al. The Pacing Therapies for Congestive Heart Failure (PATH-CHF) study: rationale, design, and endpoints of a prospective randomized multicenter study. Am J Cardiol. 1999 Mar 11;83(5B):130D-135D.
- Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001 Mar 22;344(12):873–80.
- Young JB, Abraham WT, Smith AL, Leon AR, Lieberman R, Wilkoff B, et al. Combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003 May 28;289(20):2685–94.
- Higgins SL, Hummel JD, Niazi IK, Giudici MC, Worley SJ, Saxon LA, et al. Cardiac resynchronization therapy for the treatment of heart failure in patients with intraventricular conduction delay and malignant ventricular tachyarrhythmias. J Am Coll Cardiol. 2003 Oct 15;42(8):1454–9.
- Kindermann M, Hennen B, Jung J, Geisel J, Böhm M, Fröhlig G. Biventricular versus conventional right ventricular stimulation for patients with standard pacing indication and left ventricular dysfunction: the Homburg Biventricular Pacing Evaluation (HOBIPACE). J Am Coll Cardiol. 2006 May 16;47(10):1927–37.
- Hadwiger M, Dagres N, Haug J, Wolf M, Marschall U, Tijssen J, et al. Survival of patients undergoing cardiac resynchronization therapy with or without defibrillator: the RESET-CRT project. European Heart Journal. 2022 Jul 14;43(27):2591–9.
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021 Sep 14;42(35):3427–520.
- Merkely B, Hatala R, Wranicz JK, Duray G, Földesi C, Som Z, et al. Upgrade of right ventricular pacing to cardiac resynchronization therapy in heart failure: a randomized trial. Eur Heart J. 2023 Oct 21;44(40):4259–69.
- Sideris S, Poulidakis E, Aggeli C, Gatzoulis K, Vlaseros I, Dilaveris P, et al. Upgrading pacemaker to cardiac resynchronization therapy: an option for patients with chronic right ventricular pacing and heart failure. Hellenic J Cardiol. 2014;55(1):17–23.
- Sridhar ARM, Yarlagadda V, Parasa S, Reddy YM, Patel D, Lakkireddy D, et al. Cardiac Resynchronization Therapy: US Trends and Disparities in Utilization and Outcomes. Circ Arrhythm Electrophysiol. 2016 Mar;9(3):e003108.
- Yokoshiki H, Shimizu A, Mitsuhashi T, Furushima H, Sekiguchi Y, Manaka T, et al. Trends and determinant factors in the use of cardiac resynchronization therapy devices in Japan: Analysis of the Japan cardiac device treatment registry database. J Arrhythm. 2016 Dec;32(6):486–90.
- Banks H, Torbica A, Valzania C, Varabyova Y, Prevolnik Rupel V, Taylor RS, et al. Five year trends (2008-2012) in cardiac implantable electrical device utilization in five European nations: a case study in cross-country comparisons using administrative databases. Europace. 2018 Apr 1;20(4):643–53.
- Woods B, Hawkins N, Mealing S, Sutton A, Abraham WT, Beshai JF, et al. Individual patient data network meta-analysis of mortality effects of implantable cardiac devices. Heart. 2015 Nov 15;101(22):1800–6.
- Liang Y, Wang J, Yu Z, Zhang M, Pan L, Nie Y, et al. Comparison between cardiac resynchronization therapy with and without defibrillator on long-term mortality: A propensity score matched analysis. J Cardiol. 2020 Apr;75(4):432–8.
- Veres B, Fehérvári P, Engh MA, Hegyi P, Gharehdaghi S, Zima E, et al. Time-trend treatment effect of cardiac resynchronization therapy with or without defibrillator on mortality: a systematic review and meta-analysis. Europace. 2023 Oct 5;25(10):euad289.
- Patel D, Kumar A, Black-Maier E, Morgan RL, Trulock K, Wilner B, et al. Cardiac Resynchronization Therapy With or Without Defibrillation in Patients With Nonischemic Cardiomyopathy: A Systematic Review and Meta-Analysis. Circ Arrhythm Electrophysiol. 2021 Jun;14(6):e008991.
- Køber L, Thune JJ, Nielsen JC, Haarbo J, Videbæk L, Korup E, et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N Engl J Med. 2016 Sep 29;375(13):1221–30.
- Kutyifa V, Geller L, Bogyi P, Zima E, Aktas MK, Ozcan EE, et al. Effect of cardiac resynchronization therapy with implantable cardioverter defibrillator versus cardiac resynchronization therapy with pacemaker on mortality in heart failure patients: results of a high-volume, single-centre experience. Eur J Heart Fail. 2014 Dec;16(12):1323–30.
- Barra S, Boveda S, Providência R, Sadoul N, Duehmke R, Reitan C, et al. Adding Defibrillation Therapy to Cardiac Resynchronization on the Basis of the Myocardial Substrate. J Am Coll Cardiol. 2017 Apr 4;69(13):1669–78.
- Al-Sadawi M, Aslam F, Tao M, Salam S, Alsaiqali M, Singh A, et al. Is CRT-D superior to CRT-P in patients with nonischemic cardiomyopathy? International Journal of Arrhythmia. 2023 Feb 1;24(1):3.
- Cleland JGF, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, et al. Longer-term effects of cardiac resynchronization therapy on mortality in heart failure [the CArdiac REsynchronization-Heart Failure (CARE-HF) trial extension phase]. Eur Heart J. 2006 Aug;27(16):1928–32.
- Gold MR, Daubert JC, Abraham WT, Hassager C, Dinerman JL, Hudnall JH, et al. Implantable defibrillators improve survival in patients with mildly symptomatic heart failure receiving cardiac resynchronization therapy: analysis of the long-term follow-up of remodeling in systolic left ventricular dysfunction (REVERSE). Circ Arrhythm Electrophysiol. 2013 Dec;6(6):1163–8.
- Gold MR, Linde C, Abraham WT, Gardiwal A, Daubert JC. The impact of cardiac resynchronization therapy on the incidence of ventricular arrhythmias in mild heart failure. Heart Rhythm. 2011 May;8(5):679–84.
- de Waard D, Manlucu J, Gillis AM, Sapp J, Bernick J, Doucette S, et al. Cardiac Resynchronization in Women: A Substudy of the Resynchronization-Defibrillation for Ambulatory Heart Failure Trial. JACC Clin Electrophysiol. 2019 Sep;5(9):1036–44.
- Zannad F, Ferreira JP, Pocock SJ, Anker SD, Butler J, Filippatos G, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: a meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet. 2020 Sep 19;396(10254):819–29.
- McMurray JJV, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014 Sep 11;371(11):993–1004.
- Pun PH, Al-Khatib SM, Han JY, Edwards R, Bardy GH, Bigger JT, et al. Implantable cardioverter-defibrillators for primary prevention of sudden cardiac death in CKD: a meta-analysis of patient-level data from 3 randomized trials. Am J Kidney Dis. 2014 Jul;64(1):32–9.
- Theuns DAMJ, Schaer BA, Soliman OII, Altmann D, Sticherling C, Geleijnse ML, et al. The prognosis of implantable defibrillator patients treated with cardiac resynchronization therapy: comorbidity burden as predictor of mortality. Europace. 2011 Jan;13(1):62–9.
- Goldenberg I, Vyas AK, Hall WJ, Moss AJ, Wang H, He H, et al. Risk stratification for primary implantation of a cardioverter-defibrillator in patients with ischemic left ventricular dysfunction. J Am Coll Cardiol. 2008 Jan 22;51(3):288–96.
- Leyva F, Zegard A, Okafor O, de Bono J, McNulty D, Ahmed A, et al. Survival after cardiac resynchronization therapy: results from 50 084 implantations. Europace. 2019 May 1;21(5):754–62.
- Wang Y, Sharbaugh MS, Althouse AD, Mulukutla S, Saba S. Cardiac resynchronization therapy pacemakers versus defibrillators in older non-ischemic cardiomyopathy patients. Indian Pacing Electrophysiol J. 2019;19(1):4–6.
- Döring M, Ebert M, Dagres N, Müssigbrodt A, Bode K, Knopp H, et al. Cardiac resynchronization therapy in the ageing population - With or without an implantable defibrillator? Int J Cardiol. 2018 Jul 15;263:48–53.
- Acosta J, Fernández-Armenta J, Borràs R, Anguera I, Bisbal F, Martí-Almor J, et al. Scar Characterization to Predict Life-Threatening Arrhythmic Events and Sudden Cardiac Death in Patients With Cardiac Resynchronization Therapy: The GAUDI-CRT Study. JACC Cardiovasc Imaging. 2018 Apr;11(4):561–72.
- Leyva F, Zegard A, Acquaye E, Gubran C, Taylor R, Foley PWX, et al. Outcomes of Cardiac Resynchronization Therapy With or Without Defibrillation in Patients With Nonischemic Cardiomyopathy. J Am Coll Cardiol. 2017 Sep 5;70(10):1216–27.
- Gatzoulis KA, Tsiachris D, Arsenos P, Antoniou CK, Dilaveris P, Sideris S, et al. Arrhythmic risk stratification in post-myocardial infarction patients with preserved ejection fraction: the PRESERVE EF study. Eur Heart J. 2019 Sep 14;40(35):2940–9.
- Gatzoulis KA, Arsenos P, Trachanas K, Dilaveris P, Antoniou C, Tsiachris D, et al. Signal-averaged electrocardiography: Past, present, and future. J Arrhythm. 2018 Jun;34(3):222–9.
- Milaras N, Dourvas P, Doundoulakis I, Sotiriou Z, Nevras V, Xintarakou A, et al. Noninvasive electrocardiographic risk factors for sudden cardiac death in dilated ca rdiomyopathy: is ambulatory electrocardiography still relevant? Heart Failure Reviews. 2023;28(4):865–78.
- Stecker EC, Vickers C, Waltz J, Socoteanu C, John BT, Mariani R, et al. Population-based analysis of sudden cardiac death with and without left ventricular systolic dysfunction: two-year findings from the Oregon Sudden Unexpected Death Study. J Am Coll Cardiol. 2006 Mar 21;47(6):1161–6.
- Gorgels APM, Gijsbers C, de Vreede-Swagemakers J, Lousberg A, Wellens HJJ. Out-of-hospital cardiac arrest--the relevance of heart failure. The Maastricht Circulatory Arrest Registry. Eur Heart J. 2003 Jul;24(13):1204–9.
- Gatzoulis KA, Dilaveris P, Arsenos P, Tsiachris D, Antoniou CK, Sideris S, et al. Arrhythmic risk stratification in nonischemic dilated cardiomyopathy: The ReCONSIDER study design - A two-step, multifactorial, electrophysiology-inclusive approach. Hellenic J Cardiol. 2021;62(2):169–72.
- Laina A, Gatzoulis KA, Soulaidopoulos S, Arsenos P, Doundoulakis I, Tsiachris D, et al. Time to reconsider risk stratification in dilated cardiomyopathy. Hellenic Journal of Cardiology. 2021;62(5):392–3.
- Doundoulakis I, Tsiachris D, Kordalis A, Soulaidopoulos S, Arsenos P, Xintarakou A, et al. Management of Patients With Unexplained Syncope and Bundle Branch Block: Predictive Factors of Recurrent Syncope. Cureus. 2023 Mar;15(3):e35827.
- Demir E, Köse MR, Şimşek E, Orman MN, Zoghi M, Gürgün C, et al. Comparative analysis of implantable cardioverter-defibrillator efficacy in ischemic and non-ischemic cardiomyopathy in patients with heart failure. Sci Rep. 2025 Jul 9;15(1):24631.
- Frontera A, Prolic Kalinsek T, Hadjis A, Della Bella P. Noninvasive programmed stimulation in the setting of ventricular tachycardia catheter ablation. J Cardiovasc Electrophysiol. 2020 Jul;31(7):1828–35.
- Kariki O, Antoniou CK, Mavrogeni S, Gatzoulis KA. Updating the Risk Stratification for Sudden Cardiac Death in Cardiomyopathies: The Evolving Role of Cardiac Magnetic Resonance Imaging. An Approach for the Electrophysiologist. Diagnostics (Basel). 2020 Jul 31;10(8):541.
- Xintarakou A, Kariki O, Doundoulakis I, Arsenos P, Soulaidopoulos S, Laina A, et al. The Role of Genetics in Risk Stratification Strategy of Dilated Cardiomyopathy. Reviews in Cardiovascular Medicine. 2022;23(9).
- Halliday BP, Gulati A, Ali A, Guha K, Newsome S, Arzanauskaite M, et al. Association Between Midwall Late Gadolinium Enhancement and Sudden Cardiac Death in Patients With Dilated Cardiomyopathy and Mild and Moderate Left Ventricular Systolic Dysfunction. Circulation. 2017 May 30;135(22):2106–15.
- Keil L, Chevalier C, Kirchhof P, Blankenberg S, Lund G, Müllerleile K, et al. CMR-Based Risk Stratification of Sudden Cardiac Death and Use of Implantable Cardioverter–Defibrillator in Non-Ischemic Cardiomyopathy. Int J Mol Sci. 2021 Jul 1;22(13):7115.
- Antonopoulos AS, Xintarakou A, Protonotarios A, Lazaros G, Miliou A, Tsioufis K, et al. Imagenetics for Precision Medicine in Dilated Cardiomyopathy. Circ Genom Precis Med. 2024 Apr;17(2):e004301.
- Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Barriales-Villa R, Basso C, et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J. 2023 Oct 1;44(37):3503–626.
- Gigli M, Merlo M, Graw SL, Barbati G, Rowland TJ, Slavov DB, et al. Genetic Risk of Arrhythmic Phenotypes in Patients With Dilated Cardiomyopathy. J Am Coll Cardiol. 2019 Sep 17;74(11):1480–90.
- Gasperetti A, Carrick RT, Costa S, Compagnucci P, Bosman LP, Chivulescu M, et al. Programmed Ventricular Stimulation as an Additional Primary Prevention Risk Stratification Tool in Arrhythmogenic Right Ventricular Cardiomyopathy: A Multinational Study. Circulation. 2022 Nov 8;146(19):1434–43.
- Zeppenfeld K, Tfelt-Hansen J, de Riva M, Winkel BG, Behr ER, Blom NA, et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022 Oct 21;43(40):3997–4126.
- Trayanova NA, Popescu DM, Shade JK. Machine Learning in Arrhythmia and Electrophysiology. Circ Res. 2021 Feb 19;128(4):544–66.
- Ellenbogen KA, Huizar JF. Foreseeing super-response to cardiac resynchronization therapy: a perspective for clinicians. J Am Coll Cardiol. 2012 Jun 19;59(25):2374–7.
- Daubert C, Behar N, Martins RP, Mabo P, Leclercq C. Avoiding non-responders to cardiac resynchronization therapy: a practical guide. Eur Heart J. 2017 May 14;38(19):1463–72.
- Hummel JD, Coppess MA, Osborn JS, Yee R, Fung JWH, Augostini R, et al. Real-World Assessment of Acute Left Ventricular Lead Implant Success and Complication Rates: Results from the Attain Success Clinical Trial. Pacing Clin Electrophysiol. 2016 Nov;39(11):1246–53.
- Pujol-Lopez M, Jiménez-Arjona R, Garre P, Guasch E, Borràs R, Doltra A, et al. Conduction System Pacing vs Biventricular Pacing in Heart Failure and Wide QRS Patients: LEVEL-AT Trial. JACC Clin Electrophysiol. 2022 Nov;8(11):1431–45.
- Antoniou CK, Chrysohoou C, Manolakou P, Tsiachris D, Kordalis A, Tsioufis K, et al. Multipoint Left Ventricular Pacing as Alternative Approach in Cases of Biventricular Pacing Failure. J Clin Med. 2025 Feb 7;14(4):1065.
- Dilaveris P, Antoniou CK, Chrysohoou C, Xydis P, Konstantinou K, Manolakou P, et al. Comparative Trial of the Effects of Left Ventricular and Biventricular Pacing on Indices of Cardiac Function and Clinical Course of Patients With Heart Failure: Rationale and Design of the READAPT Randomized Trial. Angiology. 2021 Nov;72(10):961–70.
- Herweg B, Sharma PS, Cano Ó, Ponnusamy SS, Zanon F, Jastrzebski M, et al. Arrhythmic Risk in Biventricular Pacing Compared With Left Bundle Branch Area Pacing: Results From the I-CLAS Study. Circulation. 2024 Jan 30;149(5):379–90.
- Fish JM, Brugada J, Antzelevitch C. Potential Proarrhythmic Effects of Biventricular Pacing. J Am Coll Cardiol. 2005 Dec 20;46(12):2340–7.
- Nayak HM, Verdino RJ, Russo AM, Gerstenfeld EP, Hsia HH, Lin D, et al. Ventricular tachycardia storm after initiation of biventricular pacing: incidence, clinical characteristics, management, and outcome. J Cardiovasc Electrophysiol. 2008 Jul;19(7):708–15.
- Bradfield JS, Shivkumar K. Cardiac Resynchronization Therapy–Induced Proarrhythmia. Circ Arrhythm Electrophysiol. 2014 Dec;7(6):1000–2.
- Vouliotis AI, Tsiachris D, Dilaveris P, Sideris S, Gatzoulis KA. Cardiac Resynchronization Therapy and Proarrhythmia: Weathering the Storm. Hospital Chronicles. 2012 Aug 24;7(4):234–40.
- Shukla G, Chaudhry GM, Orlov M, Hoffmeister P, Haffajee C. Potential proarrhythmic effect of biventricular pacing: fact or myth? Heart Rhythm. 2005 Sep;2(9):951–6.
- Deif B, Ballantyne B, Almehmadi F, Mikhail M, McIntyre WF, Manlucu J, et al. Cardiac resynchronization is pro-arrhythmic in the absence of reverse ventricular remodelling: a systematic review and meta-analysis. Cardiovasc Res. 2018 Sep 1;114(11):1435–44.
- Wang Y, Zhu H, Hou X, Wang Z, Zou F, Qian Z, et al. Randomized Trial of Left Bundle Branch vs Biventricular Pacing for Cardiac Resynchronization Therapy. J Am Coll Cardiol. 2022 Sep 27;80(13):1205–16.
- Upadhyay GA, Vijayaraman P, Nayak HM, Verma N, Dandamudi G, Sharma PS, et al. His Corrective Pacing or Biventricular Pacing for Cardiac Resynchronization in Heart Failure. J Am Coll Cardiol. 2019 Jul 9;74(1):157–9.
- Vinther M, Risum N, Svendsen JH, Møgelvang R, Philbert BT. A Randomized Trial of His Pacing Versus Biventricular Pacing in Symptomatic HF Patients With Left Bundle Branch Block (His-Alternative). JACC Clin Electrophysiol. 2021 Nov;7(11):1422–32.
- Archontakis S, Sideris K, Laina A, Arsenos P, Paraskevopoulou D, Tyrovola D, et al. His bundle pacing: A promising alternative strategy for anti-bradycardic pacing - report of a single-center experience. Hellenic J Cardiol. 2022;64:77–86.
- Lustgarten DL, Crespo EM, Arkhipova-Jenkins I, Lobel R, Winget J, Koehler J, et al. His-bundle pacing versus biventricular pacing in cardiac resynchronization therapy patients: A crossover design comparison. Heart Rhythm. 2015 Jul;12(7):1548–57.
- Vijayaraman P, Herweg B, Verma A, Sharma PS, Batul SA, Ponnusamy SS, et al. Rescue left bundle branch area pacing in coronary venous lead failure or nonresponse to biventricular pacing: Results from International LBBAP Collaborative Study Group. Heart Rhythm. 2022 Aug;19(8):1272–80.
- Vijayaraman P, Ponnusamy S, Cano Ó, Sharma PS, Naperkowski A, Subsposh FA, et al. Left Bundle Branch Area Pacing for Cardiac Resynchronization Therapy: Results From the International LBBAP Collaborative Study Group. JACC Clin Electrophysiol. 2021 Feb;7(2):135–47.
- Vijayaraman P, Sharma PS, Cano Ó, Ponnusamy SS, Herweg B, Zanon F, et al. Comparison of Left Bundle Branch Area Pacing and Biventricular Pacing in Candidates for Resynchronization Therapy. J Am Coll Cardiol. 2023 Jul 18;82(3):228–41.
- Leventopoulos G, Travlos CK, Anagnostopoulou V, Patrinos P, Papageorgiou A, Perperis A, et al. Clinical Outcomes of Left Bundle Branch Area Pacing Compared with Biventricular Pacing in Patients with Heart Failure Requiring Cardiac Resynchronization Therapy: Systematic Review and Meta-Analysis. Rev Cardiovasc Med. 2023 Nov 9;24(11):312.
- Vijayaraman P, Pokharel P, Subzposh FA, Oren JW, Storm RH, Batul SA, et al. His-Purkinje Conduction System Pacing Optimized Trial of Cardiac Resynchronization Therapy vs Biventricular Pacing: HOT-CRT Clinical Trial. JACC Clin Electrophysiol. 2023 Dec;9(12):2628–38.
- Pujol-López M, Graterol FR, Borràs R, Garcia-Ribas C, Guichard JB, Regany-Closa M, et al. Clinical Response to Resynchronization Therapy: Conduction System Pacing vs Biventricular Pacing. CONSYST-CRT trial. JACC Clin Electrophysiol. 2025 May 1;S2405-500X(25)00187-2.

Table 1.
Major CRT clinical trials.
| Trial Name | Year | Population | Sample size | Comparison | Endpoints |
|---|---|---|---|---|---|
| PATH-CHF[15] | 1999 | NYHA III-IV | 42 | Univentricular pacing vs. BiVP | Trends for improvement regarding ˙VO2max and 6MWT |
| MUSTIC[16] | 2002 | NYHA III LVEF <35% QRS>150ms |
67 | BiVP vs. no pacing (sinus) BiVP vs. Univentricular (patients with Af) |
6MWT +20% VO2 max +10% LVEF +5% Mitral regurgitation improved by 45–50% |
| MIRACLE[11] | 2002 | NYHA III-IV LVEF ≤35% QRS >130 ms, |
453 | OMT vs CRT | Improved quality of life, 6MWT, NYHA class, LVEF |
| MIRACLE-ICD[17] | 2003 | NYHA III-IV LVEF ≤35% QRS >130 ms |
369 | BiVP+ICD vs. ICD | BiVP favorably affected quality of life, functional status, and exercise capacity No significant difference in LV function or survival |
| CONTAK-CD[18] | 2003 | NYHA) II -IV LVEF ≤35% QRS ≥120 ms |
490 | BiVP+ICD vs. ICD | 6MWT +20 m VO2max +0.8 mL/kg/min LVEF +2.3% |
| COMPANION[7] | 2004 | NYHA III-IV LVEF ≤35% QRS ≥120 ms |
1520 | OMT vs CRT/CRT-D | CRT-D reduced all-cause mortality by 36% CRT-P by 24% |
| CARE-HF[13] | 2005 | NYHA III-IV LVEF≤35% QRS ≥120 ms |
813 | OMT vs CRT | CRT-P reduced mortality and HF hospitalization |
| HOBIPACE[19] | 2006 | LVEF ≤40% Symptomatic bradycardia and impaired AV conduction |
33 | BiVP vs. Univentricular pacing | Favorable effects of BiVP on LV dimensions, LVEF, NT-proBNP levels, and functional status |
| MADIT-CRT[8] | 2009 | NYHA I-II LVEF ≤30% QRS ≥130 ms, |
1820 | CRT-D vs ICD | Reduced HF events and improved LV function, especially in LBBB |
| REVERSE[12] | 2008 | NYHA I-II LVEF ≤40% QRS ≥120 ms |
610 | OMT vs CRT | CRT-P improved LV function and reduced HF progression |
| RAFT[9] | 2010 | NYHA II-III LVEF ≤30% QRS ≥120 ms |
1798 | CRT-D vs ICD | CRT-D reduced mortality and HF hospitalizations |
| RESET-CRT[20] | 2023 | NYHA II-IV LVEF ≤35% QRS ≥120 ms |
3569 | CRT-P vs CRT-D | Non-inferior mortality with CRT-P vs CRT-D |
| Abbreviations: NYHA, New York Heart Association; LVEF, left ventricular ejection fraction; HF, heart failure; MWT, minute walking distance; OMT, optimal medical treatment; CRT, cardiac resynchronization | |||||
Table 2.
RCTS and observational on the effect of CRT on mortality.
| Study (Year) | Population | Study Period | Follow-up | CRT-P (n) | CRT-D (n) | Outcomes |
|---|---|---|---|---|---|---|
| RCTs | ||||||
| Køber (2016) | NICM | 2008-2014 | 67months (median) |
323 | 322 | No difference in all-cause mortality between patients who received CRT and patients who did not. |
| Doran (2021) | ICM and NICM | 2000–2002 | 16.5months (median) | 617 | 595 | The unadjusted and adjusted HRs for CRT-D versus CRT-P were both 0.84 (95% CI: 0.65-1.09) for all-cause mortality. NICM (n = 555): CRT-D reduced all-cause mortality compared to CRT-P (aHR: 0.54; 95% CI: 0.34-0.86) ICM (n = 657): CRT-D did not reduce all-cause mortality (aHR: 1.05; 95% CI: 0.77-1.44). |
| Observational studies | ||||||
|
Auricchio (2007) |
ICM and NICM | 1994–2004 | 34months (median) | 572 | 726 | CRT-D Non-significant decrease in mortality by 20% (HR 0.83, 95% CI 0.58-1.17, p = 0.284) Significant decrease of sudden cardiac death (HR 0.04, 95% CI 0.04-0.28, p <0.002). |
|
Morani (2013) |
ICM and NICM | 2004–2007 | 55months (median) | 108 | 266 | CRT-D significantly reduced all-cause mortality compared to CRT-P (73 CRT-D and 44 CRT-P patients died, rate 6.6 vs. 10.4%/year; log-rank test, P = 0.020). |
|
Kutyifa (2014) |
ICM and NICM | 2000–2011 | 28months (median) | 693 | 429 | No mortality benefit in patients with CRT-D compared with CRT-P in the total cohort (HR 0.98, 95% CI 0.73-1.32, P = 0.884). ICM: CRT-D was associated with 30% risk reduction in all-cause mortality compared with CRT-P (HR 0.70, 95% CI 0.51-0.97, P = 0.03). NICM: No mortality benefit of CRT-D over CRT-P (HR 0.98, 95% CI 0.73-1.32, P = 0.894). |
|
Looi (2014) |
ICM and NICM | 2006–10 | 29months (mean) | 354 | 146 | CRT-D did not offer additional survival advantage over CRT-P |
| Gold (2015) | ICM and NICM | 2004–06 | 60months (median) | 74 | 345 | 10% mortality among CRT-D patients and 11.8% among CRT-P patients. CRT-ON was predicted to increase survival 22.8% (CRT-ON 52.5% vs. CRT-OFF 29.7%; HR 0.45; p = 0.21), leading to expected survival of 9.76 years (CRT-ON) versus 7.5 years (CRT-OFF). |
| Marijon (2015) | ICM and NICM | 2008–10 | 222months (mean) | 535 | 1,170 | Increased mortality rate among CRT-P patients compared with CRT-D (relative risk 2.01, 95% CI 1.56–2.58). 95% of the excess mortality among CRT-P subjects was related to an increase in non-sudden death. |
|
Reitan (2015) |
ICM and NICM | 1999–12 | 59months (median) | 448 | 257 | Annual mortality differed between CRT-D and CRT-P (5.3% and 11.8%, respectively) After adjustment for covariates, CRT-D treatment (vs CRT-P) was not associated with better long-term survival. |
| Munir (2016) | ICM and NICM | 2002–13 | 40.8months (median) | 107 | 405 | CRT-P patients had higher unadjusted mortality compared to CRT-D (HR = 1.54, 95% CI 1.15–2.08, P = 0.004). After adjustment (age at implant, sex, prior myocardial infarction, Charlson index, pre-implant LVEF, QRS morphology, drugs) this effect lost statistical significance (HR 1.18, 95% CI 0.78–1.77, P = 0.435) |
|
Witt (2016) |
ICM and NICM | 2000–10 | 48months (median) |
489 | 428 | CRT-D reduced all-cause mortality in ICM (aHR 0.74, 95% CI, 0.56–0.97; P = 0.03) but not in NICM (aHR 0.96, 95% CI, 0.60–1.51; P = 0.85) |
|
Drozd (2016) |
ICM and NICM | 2008–12 | 36months (mean) | 544 | 251 | No survival benefit in CRT-D patients compared with CRT-P (HR 1.09, 95% CI 0.84-1.41, P = 0.51). |
| Laish-Farkas (2017) | Elderly with ICM and NICM | 2006–15 | 60months (median) |
142 | 104 | In octogenarians CRT-P is associated with similar morbidity and mortality outcomes as CRT-D. |
| Barra (2017) | ICM and NICM | 2002–12 | 41.4months (mean) | 1,270 | 4,037 | ICM: better survival with CRT-D vs CRT-P (HR 0.76; 95% CI: 0.62-0.92, P = 0.005) NICM: no such difference was observed (HR: 0.92; 95% CI: 0.73-1.16, P = 0.49). |
| Martens (2017) | ICM and NICM | 2008–15 | 38months (mean) | 361 | 326 | All-cause mortality was higher in patients with CRT-P versus CRT-D (21% vs 12%, p=0.003), even after adjusting for baseline characteristics (HR 2.5; 95% CI 1.36-4.60, P=0.003). Predominant non-cardiac mode of death in CRT-P recipients (n=47 (71%) vs n=13 (38%) in CRT-D, P=0.002). |
| Yokoshiki (2017) | ICM and NICM | 2011–15 | 21months (mean) | 97 | 620 | All-cause death or heart failure hospitalization diverged between the CRT-D and CRT-P groups with a rate of 22% vs. 42%, respectively, at 24 months (P=0.0011). However, this apparent benefit of CRT-D over CRT-P was no longer significant after adjustment for covariates. |
|
Leyva (2018) |
ICM and NICM | 2000–17 | 56.4months (median) | 999 | 551 | CRT-D was associated with a lower total mortality (HR 0.72) ICM: CRT-D was associated with a lower total mortality (HR 0.62), total mortality or HF hospitalization (HR 0.63), and total mortality or hospitalization for MACE (HR 0.59) (all P < 0.001) NICM: No differences in outcomes between CRT-D and CRT-P |
|
Döring (2018) |
Elderly with ICM and NICM | 2008–14 | 26months (mean) | 80 | 97 | No significant difference in mortality between the two groups (P= 0.562) |
|
Wang (2019) |
NICM | 2002–13 | 46months (median) | 42 | 93 | CRT-P recipients had similar unadjusted mortality compared to CRT-D recipients (HR 1.04, 95% CI 0.56-1.93) Unchanged after adjusting for unbalanced covariates (HR 0.95, 95% CI 0.47-1.89) (LVEF, drugs, comorbidities) |
|
Saba (2019) |
NICM | 2007–14 | 60months | 1,236 | 4,359 | No difference between matched CRT-P and CRT-D recipients regarding the time to all-cause mortality (HR 0.90; 95% CI 0.74-1.09), any hospitalization (HR 1.13; 95% CI 0.98-1.30), and cardiac hospitalization (HR 0.98; 95% CI 0.83-1.17). CRT-P recipients had significantly lower medical costs at 12 and 24 months. |
|
Barra (2019) |
ICM and NICM | 2002–13 | 30months (mean) | 534 | 1,241 | ICM: better survival with CRT-D vs CRT-P (HR for mortality adjusted on propensity score and all mortality predictors: 0.76; 95% CI: 0.62 to 0.92; p = 0.005) NICM: no such difference was observed (HR: 0.92; 95% CI: 0.73 to 1.16; p = 0.49). |
| Leyva (2019) | 2009–17 | 32.4months (median) | 24,811 | 25,273 | Excess mortality was lower after CRT-D than after CRT-P in all patients (aHR 0.80, 95% CI 0.76-0.84] in subgroups with (aHR 0.79, 95% CI 0.74-0.84) or without (aHR 0.82, 95% CI 0.74-0.91) ICM |
|
| Liang (2020) | ICM and NICM | 2005–16 | 36 months (median) | 126 | 219 | No significant difference in the risk of mortality between CRT-D and CRT-P groups (HR 0.99, 95% CI 0.70-1.40, P= 0.95]. No significant difference between CRT-D and CRT-P in reducing mortality was observed in any pre-specified subgroups. |
|
Gras (2020) |
ICM and NICM | 2010–17 | 913 ± 841 days | 19,266 | 26,431 | Higher all-cause mortality in CRT-P (11.6%) than CRT-D patients (6.8%) (HR 1.70, 95% CI 1.63-1.76, P < 0.001). No difference in mortality in NICM patients >75 years old with CRT-P and CRT-D (HR 0.93, 95% CI 0.80-1.09, P = 0.39). Higher mortality in NICM CRT-P patients <75 years old (HR 1.22, 95% CI 1.03-1.45, P = 0.02). Higher mortality with CRT-P than with CRT-D irrespectively of age in patients with ICM (<75 years old: HR 1.22, 95% CI 1.08-1.37, P = 0.01; ≥75 years old: HR 1.13, 95% CI 1.04-1.22, P = 0.003). |
| Huang (2021) | ICM and NICM | 2012–13 | 27.7months (mean) | 237 | 362 | SCD rate was 8.0% in CRT-P group and 3.3% in CRT-D group No significant differences in all-cause death rate between the CRT-D and CRT-P groups (CRT-D vs. CRT-P, 20.4% vs. 19.4%, P = 0.840). |
| Schrage (2022) | ICM and NICM | 2000–16 | 28.2months (median) | 880 | 1,108 | CRT-D was associated with lower 1- and 3-year all-cause mortality (HR:0.76, 95% CI:0.58-0.98; HR: 0.82, 95% CI: 0.68-0.99, respectively). |
|
Hadwiger (2022) |
ICM and NICM | 2014–19 | 28.2months (median) |
847 | 2,722 | CRT-P treatment was not associated with inferior survival compared with CRT-D. |
| Farouq (2023) | NICM | 2005-2020 | 51.6months (median) | 2334 | 1693 | CRT-D was associated with higher 5-year survival (HR 0.72 95% CI 0.61–0.85, P < 0.001). CRT-P was associated with higher mortality in age groups <60 years and 70–79 years. |
| Abbreviations: ICM, ischemic cardiomyopathy; NICM, non-ischemic cardiomyopathy; SCD, sudden cardiac death; HF, heart failure; MACE, major adverse cardiac events; aHR, adjusted hazard ratio; CI, confidence interval | ||||||
Table 3.
Meta-analyses on the effect of CRT on mortality.
| Meta-analysis (year) | No of studies included | Population (n) | CRT-P (n) | CRT-D (n) |
Outcomes |
|---|---|---|---|---|---|
| Ischemic and non-ischemic cardiomyopathy | |||||
| Veres (2023) |
26 observational studies | 128.030 | 55.469 | 72.561 | CRT-D reduced all-cause mortality by 20% over CRT-P (aHR: 0.85; 95% CI: 0.76–0.94; P < 0.01] Not in NICM (HR: 0.95; 95% CI: 0.79–1.15; P = 0.19) Not in patients >75 years (HR: 1.08; 95% CI 0.96–1.21; P = 0.17). |
| Non-ischemic cardiomyopathy | |||||
|
Patel (2021) |
7 observational studies | 9.944 | 3.079 | 6.865 | CRT-D was not significantly associated with a reduction in all-cause mortality in CRT-eligible patients with NICM (aHR 0.92, 95% CI, 0.83–1.03) |
| Al Sadawi (2023) | 13 observational and 2 RCTs | 22.763 | 9.596 | 13.167 | CRT-D was associated with lower all-cause mortality (log HR − 0.169, SE 0.055; P = 0.002) as compared to CRT-P. |
|
Liu (2023) |
9 observational and 2 RCTs | 28.768 | 11.980 | 16.788 | CRT-D was associated with a modest but statistically significant survival benefit compared to CRT-P (aHR 0.90 95% CI, 0.81–0.99) |
|
Neto (2024) |
11 observational and 2 RCTs | 61.326 | 7.338 | 9.108 | CRT-D was associated with a significantly lower risk of all-cause mortality compared to CRT-P (pooled HR 0.74; 95% CI: 0.62-0.88; I2=84%). No statistically significant difference in mortality risk for patients > 75 years old (pooled HR 0.96; 95% CI: 0.811-1.15; I² = 39%, P<0.001). |
| Abbreviations: RCTs, randomized clinical trials; ICM, ischemic cardiomyopathy; NICM, non-ischemic cardiomyopathy; aHR, adjusted hazard ratio; CI, confidence interval | |||||
Table 4.
Clinical Trials on CSP vs CRT.
| Trial Name | Year | Study Type | Population | Intervention | Comparator | Key Findings |
|---|---|---|---|---|---|---|
| His-SYNC[83] | 2017 | RCT | 41 | HBP | BiV CRT | Similar improvements in LV function; HBP had higher crossover (48%) due to technical limitations. |
| His-Alternative[84] | 2021 | RCT | 50 | HBP or LBBAP | BiV CRT | CSP showed non-inferior clinical response and better electrical resynchronization. |
| LBBP-RESYNC[82] | 2022 | RCT | 40 | LBBAP | BiV CRT | LBBAP showed greater LVEF improvement and QRS narrowing than BiV CRT. |
| HOT CRT[91] | 2023 | RCT | 160 | HBP | BiV CRT | HBP superior to BiVP in LVEF; similar QRS narrowing and symptoms |
| LEVEL-AT[72] | 2023 | Prospective, non-randomized | 70 | LBBAP | CRT cohort | LBBAP showed better LVEF recovery and symptom improvement compared to historical BiV CRT. |
| CONSYST CRT[92] | 2025 | RCT | 134 | CSP | BiV CRT | Non inferiority in clinical and echocardiographic response |
| Abbreviations: RCT, randomized clinical trial; HBP, his bundle pacing; LBBAP, left bundle brunch area pacing; BiV, biventricular; CSP, conduction system pacing; CRT, cardiac resynchronization, LVEF, left ventricular ejection fraction; LV, left ventricular | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



