Submitted:
18 August 2025
Posted:
20 August 2025
You are already at the latest version
Abstract
Primary mitral regurgitation (PMR) is the most common mitral valve disorder in clinical practice. Although several prognostic indicators derived from resting transthoracic echocardiography (TTE) and exercise stress echocardiography (ESE) are available, patient out-comes remain highly variable, with substantial differences in the risk of complications and mortality. Identifying individuals at lower cardiovascular risk is therefore clinically relevant, as they represent a large proportion of cases. Current guidelines recommend an integrative approach—combining qualitative, semiquantitative, and quantitative indices—to determine the timing of intervention, but they do not specifically address risk stratification of low-risk PMR populations. Recent studies from our group have demonstrated the prognostic importance of chest wall configuration, assessed noninvasively us-ing the modified Haller index (MHI). Defined as the ratio of latero-lateral thoracic diame-ter to the antero-posterior (A-P) sternum–spine distance, MHI has been shown to signifi-cantly affect myocardial deformation indices obtained by speckle tracking echocardiography (STE). Patients with PMR due to mitral valve prolapse (MVP) often present with reduced A-P thoracic diameter caused by sternal depression. Among these, individuals with MHI >2.5 or A–P diameter ≤13.5 cm displayed greater impairment in global and basal myocardial strain, particularly in longitudinal and circumferential directions. These ab-normalities appear to reflect extrinsic compressive forces and cardiac displacement lead-ing to intraventricular dyssynchrony, rather than intrinsic myocardial dysfunction. A reduced A-P diameter (≤13.5 cm) was also independently associated with mitral annular disjunction (MAD) in MVP and emerged as a key determinant of impaired strain in this subgroup. In a retrospective cohort of 424 symptomatic MVP patients with moderate MR undergoing ESE, positive tests and exercise-induced severe MR were uncommon (9.8% and 13.2%). Importantly, multivariable analysis revealed that MHI >2.5 or A–P diameter ≤13.5 cm was strongly linked to favorable medium-term prognosis, with very few adverse cardiovascular events. These findings suggest that chest wall assessment using MHI may help distinguish compression-related symptoms from hemodynamically significant MR and identify symptomatic PMR patients with a benign prognosis. This narrative review summarizes the evidence regarding conventional and novel echocardiographic prognostic markers and their implications for risk stratification in PMR.
Keywords:
primary mitral regurgitation
; prognostic risk stratification
; myocardial strain parameters
; mitral annular disjunction
; exercise stress echocardiography
1. Introduction
Mitral regurgitation (MR) is the second most prevalent valvular heart condition in Europe, surpassed only by aortic stenosis, with primary mitral regurgitation (PMR) accounting for approximately 61%–67% of cases [1,2]. PMR is characterized by systolic regurgitant flow from the left ventricle (LV) to the left atrium (LA), arising from intrinsic abnormalities of the mitral valve (MV) apparatus, including the leaflets, chordae tendineae, or papillary muscles. Structural lesions affecting one or more of these components define PMR. In Western countries, degenerative etiologies, particularly fibroelastic deficiency and Barlow disease, represent the predominant causes [1,3,4].
Chronic significant PMR frequently induces progressive LV remodeling and dysfunction, ultimately predisposing to heart failure and other adverse cardiac outcomes [5]. This disease course often necessitates repeated clinical evaluations, hospital admissions, and surgical intervention [6]. With the aging of the general population, the burden of PMR is anticipated to increase further [7]. Determining the optimal timing for surgical intervention has been the subject of longstanding debate. Current practice increasingly supports earlier surgical referral, as earlier intervention is associated with superior postoperative outcomes. For instance, surgery is now recommended at a left ventricular end–systolic diameter (LVESD) threshold of 40 mm, rather than waiting until it reaches 45 mm [8]. According to current guidelines, the presence of symptoms or LV dysfunction constitutes a Class I indication for surgery in patients with PMR [8,9]. However, reliance on left ventricular ejection fraction (LVEF) and LVESD has limitations, as these indices are influenced by LV geometry, loading conditions, and heart rate [10]. Consequently, these measures may overestimate systolic function in PMR, highlighting the need for more sensitive and reliable markers to guide surgical timing.
Despite numerous prognostic markers evaluated through resting transthoracic echocardiography (TTE) and exercise stress echocardiography (ESE), outcomes in PMR remain heterogeneous, with wide variability in reported rates of complications and mortality [11,12,13,14]. Identifying patients at lower risk is therefore as important as recognizing those at higher risk.
Recent work from our group has drawn attention to chest wall morphology as a potential modifier of cardiac function, assessed using the Modified Haller Index (MHI) [15]. Previous investigations demonstrated that MHI influences myocardial strain parameters in diverse populations, including healthy infants [16] and adults [17] with pectus excavatum, healthy individuals with mitral valve prolapse (MVP) [18], healthy adults with obesity [19], and healthy third–trimester pregnant women [20], even in the presence of preserved biventricular systolic performance. Specifically, individuals with a concave chest wall (MHI >2.5) [21] consistently showed impaired LV strain, particularly in basal segments, both longitudinally and circumferentially. These alterations were attributed to external compression and displacement of the heart caused by chest wall deformity, leading to intraventricular dyssynchrony rather than intrinsic myocardial disease. Furthermore, in a recent study, we demonstrated that symptomatic patients with MVP–related moderate MR and MHI ≥2.7 exhibited excellent prognosis following ESE during medium–term follow–up [22].
Based on these findings, we hypothesize that incorporating chest wall assessment with MHI into clinical practice may help distinguish compressive causes of symptoms from true pathological dysfunction in symptomatic PMR patients, and further allow identification of a subgroup with more favorable prognosis. The present narrative review summarizes available evidence regarding conventional and novel echocardiographic prognostic markers, with emphasis on their threshold values, in order to refine risk stratification and inform clinical decision–making in PMR.
2. Traditional Prognostic Indicators Assessed by Transthoracic Echocardiography
2.1. Echocardiographic criteria of PMR severity recommended by current guidelines
Echocardiography remains the cornerstone imaging modality for grading PMR. Current recommendations emphasize an integrative approach that combines qualitative, semiquantitative, and quantitative parameters, together with assessment of LV and LA size [23,24]. Identifying the precise anatomical lesion responsible for MR has clear prognostic significance [4,25] and is critical in determining the feasibility of surgical or transcatheter repair [26,27].
Several echocardiographic criteria derived from TTE are widely used in clinical practice [8]. These include morphological assessment of the MV apparatus, quantification of regurgitant severity, and evaluation of associated cardiac chamber enlargement, diastolic function, and pulmonary hemodynamics. The guideline–endorsed echocardiographic indicators of PMR severity are summarized in Table 1.
2.2. Left ventricular size
In longitudinal studies, measurements of LV linear internal diameters demonstrated higher reproducibility and minimal test–retest variability, which enables a more precise determination of clinically relevant cut-off values for individual patients [28].
LVESD is one of the most established prognostic parameters in patients undergoing MV surgery [29]. Pre–operative LVESD has consistently been shown to predict deterioration in LVEF [30], incidence of cardiac events [31], and both early and late mortality [32,33]. Based on evidence supporting its predictive value [32,34,35], both American and European guidelines recognize LVESD ≥40 mm as a Class I indication for surgical intervention in chronic PMR [8,9]. Other LV dimensional indices have also been evaluated; for example, left ventricular end–diastolic diameter (LVEDD) >60 mm has been associated with recurrent MR several years after surgery (HR 1.88 [1.06–3.34], p = 0.03) [33].
2.3. Left ventricular function
LVEF remains a classical measure of LV systolic performance. Numerous studies have confirmed the prognostic significance of pre–operative LVEF in predicting postoperative LV dysfunction [36,37,38,39,40], recurrent MR [33], and mortality [33,41]. Consequently, guidelines from both the ACC/AHA and ESC/EACTS recommend surgical referral when LVEF falls below 60% as a Class I indication for intervention in chronic PMR [8,9].
2.4. Left atrial size
The left atrium (LA) undergoes adaptive remodeling in response to chronic volume overload from MR [42]. Pre–operative LA enlargement has been strongly linked to adverse postoperative outcomes [43,44,45], including atrial fibrillation (AF) [45,46] and increased mortality [43,44,47]. Accordingly, the ESC/EACTS guidelines recommend surgical consideration in patients with LA volume index ≥60 mL/m² or LA diameter ≥55 mm as a Class IIa indication [8].
2.5. Pulmonary hypertension
In chronic PMR, elevated LA pressure is transmitted retrogradely to the pulmonary veins, potentially leading to pulmonary hypertension (PH) [48]. Persistent PH increases right ventricular (RV) afterload and may cause right heart remodeling, functional tricuspid regurgitation (FTR), and eventual RV dysfunction [48]. Approximately 20–30% of patients with severe PMR present with significant PH, defined as systolic pulmonary artery pressure (sPAP) ≥50 mmHg [49,50]. PH has been shown to predict poor outcomes, including early operative mortality [51], long–term all–cause and cardiovascular mortality [49,50,52,53,54], major adverse events [53], reoperation [55], and persistent postoperative PH [56]. sPAP provides incremental prognostic information for mortality [50,56]. For these reasons, both European and American guidelines list resting PH as a Class IIa indication for surgical intervention in PMR [8,9].
2.6. Right ventricular size and function
RV dilation and dysfunction generally indicate more advanced disease progression [48]. Multiple studies have demonstrated strong associations between RV indices and adverse surgical outcomes. RV end–diastolic diameter (RVEDD) >35 mm independently predicted prolonged intensive care unit (ICU) stay after MV replacement [57]. RV fractional area change (FAC) was inversely associated with in–hospital mortality or circulatory failure following left–sided valve surgery [58]. Similarly, RV myocardial performance index (MPI) ≥0.50 was linked to adverse postoperative outcomes [58]. Reduced RV ejection fraction (≤35%) was associated with higher cardiovascular mortality in chronic PMR [59]. Furthermore, tissue Doppler–derived s′ velocity <8.75 mm/s and tricuspid annular plane systolic excursion (TAPSE) <17.5 mm correlated with postoperative declines in LVEF [60]. These data underscore the prognostic importance of comprehensive RV assessment in PMR patients.
2.7. Functional tricuspid regurgitation
Functional tricuspid regurgitation (FTR) is frequently encountered among patients undergoing MV surgery, with reported prevalence rates ranging between 25% and 59% [61,62], while moderate or severe FTR is observed in approximately 8% to 45% of cases [63,64]. Increasing preoperative severity of FTR has been shown to correlate with worse postoperative outcomes, including reduced long–term survival [65,66,67], higher incidence of congestive heart failure [62,63], and progression of FTR during follow–up [62]. Owing to these adverse prognostic implications, combined surgical or transcatheter management of FTR has become increasingly common in recent years [68]. According to current ESC/EACTS and ACC/AHA guidelines, in patients with FTR secondary to left–sided valve disease, tricuspid valve surgery is strongly recommended in the presence of severe regurgitation at the time of concomitant left–sided valve surgery (Class I) [9]. Surgical intervention is also advised for patients with progressive FTR accompanied by a tricuspid annular end–diastolic diameter greater than 40 mm or with clinical evidence of right heart failure when left–sided valve surgery is indicated (Class IIa) [9]. Furthermore, isolated tricuspid valve surgery is recommended in cases of severe FTR caused by annular dilation in the presence of right heart failure symptoms (Class IIa) [8,9].
3. Prognostic Indicators Assessed by Speckle Tracking Echocardiography
3.1. Left ventricular global longitudinal strain
Most studies consistently show that preoperative impairment in left ventricular global longitudinal strain (LV–GLS) is a reliable prognostic indicator in PMR [69,70,71,72,73]. LV–GLS values between –17.9% and –20.5% are generally considered the thresholds associated with worse postoperative outcomes. Importantly, LV–GLS has been demonstrated to provide incremental prognostic value beyond conventional indices [72,74,75].
Some heterogeneity exists, however. Pandis et al. [75] reported that patients with preoperative LV–GLS less negative than –20.5% experienced a greater postoperative decline in LVEF, while LV–GLS values less negative than –17.9% predicted >10% reduction in LVEF and postoperative LVEF below 50%. Conversely, Song et al. [31] found no significant association between preoperative GLS and early postoperative LV dysfunction, possibly due to immediate postoperative hemodynamic instability and variability in patient populations. Overall, impaired LV–GLS appears to be a sensitive marker of adverse outcomes in PMR, although the precise cut–off values vary slightly depending on the imaging platform and analysis software.
3.2. Left atrial reservoir strain
Left atrial strain (LASr) has emerged as a sensitive marker of atrial function and remodeling [76]. Several studies have shown that reduced LASr is independently associated with postoperative adverse outcomes, including mortality, cardiac events, LV dysfunction, and impaired functional capacity [74,77,78,79]. A LASr cut–off of ~21% has been reported to predict postoperative cardiac events [80], while a threshold of ~22% has been linked to increased long–term all–cause mortality [79].
Interestingly, LASr impairment may precede changes in LV strain. Cameli et al. [81] proposed that because of the thin atrial wall and chronic volume overload, the LA is particularly vulnerable, and LASr abnormalities may appear earlier than LV strain impairment. Future investigations should consider the absence of universal normal values across vendors and technical challenges related to thin atrial walls [82].
3.3. Right ventricular strain
Evidence regarding RV strain in PMR remains limited. Kislitsina et al. [74] reported that impaired RV free–wall longitudinal strain correlated with postoperative LV dysfunction, and the combination of LV–GLS, RV strain, and LASr improved prognostic accuracy. However, RV strain did not independently predict survival in multivariable Cox regression analysis. Further studies are required to clarify the role of RV strain in prognostic stratification of PMR patients.
Figure 1 illustrates all principal 2D–TTE and 2D–STE derived echocardiographic parameters, independently associated with adverse cardiovscular events (negative prognostic indicators) in PMR individuals.
4. Prognostic Indicators Assessed by Exercise Stress Echocardiography
4.1. Exercise stress echocardiography
ESE enables dynamic assessment of mitral regurgitant volume and pulmonary pressures at peak exercise, and is particularly valuable in patients with discordance between symptoms and resting MR severity [83,84]. One of its primary roles is to unmask latent symptoms in patients who report being asymptomatic, while also guiding recommendations for physical activity and athletic participation. Despite its recognized utility and safety, registry data (e.g., the VHD II survey) indicate that stress testing is underutilized in asymptomatic patients [1].
ESE may clarify the cardiac origin of exertional dyspnea and carries prognostic relevance in MR [85]. In patients with PMR undergoing ESE followed by MV surgery, lower achieved metabolic equivalents were associated with poorer long–term outcomes [86]. Stress echocardiography has also proven useful in detecting subclinical ventricular dysfunction, identified either as abnormal echocardiographic parameters or lack of contractile reserve during stress. Accordingly, guidelines recommend stress echocardiography in PMR patients when discrepancies exist between resting MR severity, LV function, and symptoms [8,9].
Several exercise–derived parameters have prognostic significance. Exercise–induced LVEF <68% [87], LV end–systolic volume index (LVESVi) ≥25 mL/m² [87], and LV–GLS normalized for LVESD worse than –5.7%/cm [88] predict postoperative LV dysfunction. Exercise–induced pulmonary hypertension (sPAP >60 mmHg), reduced TAPSE (<26 mm), elevated E/e′ ratio, larger effective regurgitant orifice area (EROA), and positive stress echocardiography responses have all been associated with adverse outcomes after surgery [89,90]. Furthermore, contractile reserve of LVEF (Δ ≥4%) and LV–GLS (Δ ≥1.9%) independently predict postoperative LV dysfunction [91].
ESE also identifies dynamic MR, defined as a marked increase in regurgitation during exertion. Up to one–third of patients with at least moderate MR at rest may develop severe MR during exercise [92,93]. Dynamic MR frequently coincides with exercise–induced pulmonary hypertension, given the close link between increased regurgitant volume and elevated sPAP. Exercise sPAP >60 mmHg has been shown to predict symptom onset [94,95].
Another key application of ESE is the detection of latent LV dysfunction. Limited contractile reserve, particularly blunted increase in LV–GLS (<2%) during exercise, identifies patients at risk of early postoperative decompensation [88]. In this context, GLS is often the earliest parameter to decline in subclinical myocardial dysfunction, preceding changes in LVEF.
Diastolic stress echocardiography adds complementary information by identifying abnormal LV filling pressures during exercise. In healthy subjects, proportional increases in mitral inflow and annular velocities maintain a stable E/e′ ratio with exercise [96]. By contrast, in patients with diastolic dysfunction, increases in E/e′ ratio and/or sPAP correlate with invasive measures of elevated LV filling pressures [97]. Criteria for abnormal diastolic stress echocardiography include septal E/e′ >15, average E/e′ >14, exercise tricuspid regurgitation velocity (TRV) >2.8 m/s, and reduced baseline e′ velocities [98]. Normal findings are defined by septal E/e′ <10 and TR velocity <2.8 m/s at rest and during exercise.
Overall, exercise–induced increases in MR severity (ΔEROA ≥10 mm² and ΔRV ≥10 mL) [93], development of pulmonary hypertension (sPAP ≥60 mmHg) [94], and absence of LV contractile reserve [92,99] are among the most robust predictors of adverse cardiovascular outcomes. Emerging data also support the prognostic role of exercise RV dysfunction, with TAPSE ≤18 mm at peak exercise identifying patients at increased risk [100].
Table 2. ESE-derived prognostic indicators in PMR individuals. CV, cardiovascular; EROA, effective regurgitant orifice area; ESE, exercise stress echocardiography; GLS, global longitudinal strain; LV, left ventricular; LVEF, left ventricular ejection fraction; LVESD, left ventricular end–systolic diameter; LVESVi, left ventricular end–systolic volume index; MR, mitral regurgitation; PH, pulmonary hypertension; PMR, primary mitral regurgitation; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion; TRV, tricuspid regurgitation velocity.
In summary, ESE is particularly valuable in asymptomatic or oligosymptomatic PMR patients with equivocal resting echocardiographic findings. Although its use is limited by time and operator expertise, its prognostic yield makes it a crucial adjunct in patient selection and timing of intervention.
5. Laboratory Prognostic Indicators
Natriuretic peptides, particularly B–type natriuretic peptide (BNP) and its precursor fragments, have emerged as important biomarkers in mitral regurgitation. Plasma BNP levels rise in proportion to MR severity and are consistently higher in symptomatic compared with asymptomatic patients, even when LVEF remains preserved [101].
In organic MR, BNP activation primarily reflects the hemodynamic burden imposed on the ventricles and atria rather than the regurgitant volume itself. Elevated BNP levels have been shown to predict adverse outcomes under conservative management, regardless of MR grade [102]. This highlights BNP as a marker not only of disease severity but also of poor prognosis in patients managed medically. As such, BNP assessment is increasingly regarded as a valuable adjunct for risk stratification in PMR.
In asymptomatic patients with significant PMR and preserved LVEF undergoing MV surgery, the combination of BNP levels and LV–GLS has demonstrated complementary prognostic value. Together, these measures provide a synergistic framework for risk stratification beyond traditional markers [69].
6. Surgical or Percutaneous Treatment of PMR
Management of severe primary mitral regurgitation is traditionally guided by LV dimensions and ejection fraction. However, recent evidence suggests that LV–GLS provides incremental prognostic information in patients undergoing surgical repair [47,72].
To further refine risk stratification, the Mitral Regurgitation International Database (MIDA) score was developed to predict all–cause mortality in patients with severe PMR due to flail leaflet, whether managed surgically or medically [103]. The score incorporates variables such as symptoms, LVEF ≤60%, LVESD ≥40 mm, AF, right ventricular systolic pressure ≥50 mmHg, LA diameter ≥55 mm, and age ≥65 years. Of note, LVESD ≥40 mm and LA diameter ≥55 mm are now recognized thresholds in current guidelines.
Surgery is the treatment of choice in patients with symptomatic severe PMR and acceptable operative risk, as determined by the Heart Team. Independent of symptomatic status, triggers for intervention include LVEF ≤60%, LVESD ≥40 mm [103], LA diameter ≥55 mm or volume ≥60 mL/m² [104], systolic pulmonary artery pressure (sPAP) >50 mmHg [49], and AF [105,106]. In asymptomatic patients without these risk features, watchful waiting remains appropriate, ideally within a Heart Valve Clinic setting [107].
When surgery is indicated, mitral valve repair is generally preferred over replacement, provided durable results are achievable, as it is associated with superior long–term survival [108,109]. Segmental prolapse due to degenerative disease can typically be repaired with excellent durability and low reoperation rates [109,110]. In contrast, rheumatic lesions, extensive prolapse, leaflet calcification, or severe annular calcification present greater challenges and may reduce reparability [111,112]. For complex lesions, surgery should be performed in high–volume repair centers with demonstrated expertise and outcomes. If repair is not feasible, valve replacement with preservation of the subvalvular apparatus is the recommended alternative.
In patients with contraindications to surgery or high operative risk, transcatheter approaches represent a safe alternative. Transcatheter mitral valve implantation has been demonstrated to be feasible and effective in high–risk cohorts [113,114]. Among these techniques, transcatheter edge–to–edge repair (TEER) is currently the most widely validated, with additional transcatheter strategies under evaluation in smaller studies [115,116].
Indications for TEER in PMR are currently limited to patients with severe symptoms, high or prohibitive surgical risk, and suitable valve anatomy [117]. For asymptomatic individuals with severe PMR and preserved LVEF (>60%), close follow–up every six months with echocardiography is advised, preferably in a Heart Valve Center [118]. Additional tools such as BNP measurement, ESE, Holter monitoring, and cardiac magnetic resonance (CMR) imaging may provide complementary value in guiding risk stratification and timing of intervention [24].
7. Innovative Anthropometric Prognostic Indicators of PMR Severity
7.1. Modified Haller Index
The Modified Haller Index (MHI) is a simple, noninvasive anthropometric measure of chest wall conformation that avoids ionizing radiation while yielding information comparable to radiographic indices [15]. It is computed as the ratio between the latero–lateral external thoracic diameter, measured with a rigid ruler and level, and the antero–posterior (A–P) internal thoracic diameter acquired during standard transthoracic echocardiography from the parasternal long–axis view as the distance between the true apex of the sector and the posterior wall of the descending aorta visualized behind the left atrium (Figure 2).
Over recent years, we have examined how chest wall configuration affects myocardial mechanics, MR grading, and ESE findings in individuals with PMR secondary to MVP. We posited that a concave thorax, defined echocardiographically as MHI >2.5 or A–P diameter ≤13.5 cm [21], could exert external compressive effects on cardiac chambers and the mitral annulus, thereby influencing two–dimensional speckle–tracking echocardiography (2D–STE), conventional echocardiography, and exercise hemodynamics. In a prospective study of healthy MVP subjects without severe MR compared with matched controls, MVP participants exhibited a narrower A–P thoracic diameter consistent with a tendency toward mild–to–moderate chest deformity and showed more pronounced impairment of LV–GLS and global circumferential strain (GCS), particularly in basal segments, despite preserved biventricular systolic function on conventional echocardiography [18]. When stratified by MHI, MVP individuals with MHI >2.5 demonstrated lower magnitudes of both longitudinal and circumferential strain and more abnormal LV twist mechanics than those with MHI ≤2.5, with these differences most evident at the basal level. MVP participants with MHI >2.5 were predominantly women with small body surface area and small cardiac chambers, more often had nonclassic MVP without myxomatous degeneration and late–systolic mild or mild–to–moderate MR, and more frequently exhibited isolated ventricular premature beats and nonspecific ST–T abnormalities on resting ECG. Across MVP and control groups, MHI correlated linearly and strongly with LV–GLS and LV–GCS.
Figure 3 illustrates an example of MVP individual with concave–shaped chest wall conformation, mild MR and mild–to–moderate impairment of LV–GLS, more enhanced at the level of basal myocardial segments.
These findings differ from earlier reports that attributed reduced basal strain in MVP primarily to annular dilation [119,120,121]. In our cohort, MVP with concave chest morphology had shorter mitral annular A–P diameters yet worse global and regional strain, implicating thoracic mechanics rather than intrinsic myocardial disease. The mechanistic interpretation is that strain abnormalities typically precede overt contractile impairment, especially for GLS, with concomitant reductions across longitudinal, circumferential, and radial components usually reflecting more advanced systolic dysfunction and reduced ejection fraction [122,123,124]. In our MVP cohort, LVEF and RVEF were preserved while all strain measures were attenuated, which challenges a purely intrinsic myocardial explanation. The preserved apex–to–base deformation gradient, a pattern maintained from infancy to adulthood [125] and usually altered in cardiomyopathies and ischemia [126], also argues against primary myopathic dysfunction. Instead, our observations align with prior work indicating smaller biventricular chamber dimensions and lower strain in individuals with concave chest walls [127,128,129]. As demonstrated by CMR [129], relatively higher mid–apical strain in concave chest morphology likely represents compensation to maintain stroke volume against basal sternal compression. The graded relationship between MHI and strain impairment reproduces previous data in healthy subjects with pectus excavatum [16,17], supporting an extrinsic compressive mechanism. In MVP with MHI >2.5, increased apical rotation with blunted basal rotation suggests a rocking motion around a fulcrum near the shortest A–P chest diameter, a kinematic pattern that can confound speckle–tracking algorithms and reduce estimated strain despite preserved intrinsic contractility.
7.2. Relationship between chest wall conformation and MAD distance in PMR with MVP
The association of PMR with sudden cardiac death and ventricular arrhythmias remains debated [130,131]. Mitral annular disjunction (MAD), defined as atrial displacement of the mitral hinge line away from the ventricular myocardium, has been linked to ventricular arrhythmias and increased arrhythmic risk in MVP, often in the absence of severe MR [130,132,133]. Given the frequent coexistence of MVP with thoracic skeletal anomalies and the observed enrichment of MAD in MVP populations [134,135,136,137,138,139,140,141], we hypothesized that MAD would be more prevalent in individuals with narrow A–P thoraces and concave chest morphology. In a prospective monocentric study of MVP with and without MAD, patients with MAD had significantly smaller A–P thoracic diameters on TTE, smaller cardiac chambers, a higher prevalence of classic (floppy) MVP, and more impaired LV–GLS and LV–GCS despite similar LVEF when compared with those without MAD [142]. Multivariable analyses identified A–P thoracic diameter, classic MVP, and end–systolic mitral annular A–P diameter as independent predictors of MAD. MAD distance correlated strongly with MHI and A–P diameter but not with latero–lateral diameter. Among MAD–positive patients, MHI correlated inversely with both LV–GLS and LV–GCS, whereas this relationship was not evident in MAD–negative subjects. These findings suggest that a narrow A–P chest is associated with MAD and is a major determinant of impaired myocardial deformation in MAD–positive MVP, without commensurate differences in resting MR severity between groups that both exhibited moderate MR.
Among the MVP patients included in the present study, those with MAD exhibited the greater impairment in myocardial strain parameters, especially at basal level, in both longitudinal and circumferential directions (Figure 4).
The basal pattern of strain attenuation in MAD further supports the dominant influence of anterior chest wall mechanics in restricting basal motion and producing regional dyssynchrony [17,18]. These features can be misinterpreted as intrinsic basal hypokinesia even by experienced readers. The strong inverse associations between MHI and both LV–GLS and LV–GCS in MAD patients, concordant with our prior studies across different populations [16,17,18,20], favor a mechanical explanation over a primary myocardial substrate. This interpretation contrasts with reports ascribing basal strain impairment in MAD to annular dilation and intrinsic LV remodeling using 2D–STE, 3D transesophageal echocardiography, and CMR [119,143,144]. In our MAD cohort, approximately one third had MAD distance ≥8.5 mm, three quarters had isolated ventricular premature beats on resting ECG, and more than four fifths had classic MVP with enlarged annular diameters and paradoxical systolic annular unsaddling. These features support the concept that disjunction amplifies leaflet stress and may contribute to myxomatous degeneration [145,146,147,148], while excessive leaflet mobility and paradoxical annular dynamics may promote inferobasal and papillary muscle stretch, hypertrophy, fibrosis, and scar formation, with arrhythmogenic consequences [130,149,150,151,152]. The inverse relationship between MAD distance and A–P diameter suggests that chronic anterior chest mechanics may contribute to both MVP and MAD. As others have proposed [153,154], a concave chest wall or pectus excavatum, MVP, and MAD may cluster as a syndromic trait in some individuals.
7.3. Potential link between concave chest morphology and a “benign MAD phenotype”
In early 2025 we reported an MVP case with significant MAD and moderate MR that underwent a comprehensive imaging work–up including TTE, transesophageal echocardiography, CMR, coronary CT angiography, and ESE [155]. The patient had a concave chest configuration (MHI >2.5; A–P diameter <13.5 cm), non–hemodynamically significant MR on ESE, no late gadolinium enhancement on CMR, and a low arrhythmic burden. These observations led us to hypothesize that MHI might help identify a subset of MVP with MAD who carry a relatively favorable prognosis. In a subsequent series, MVP patients with MAD and MHI >2.5 or A–P diameter <13.5 cm exhibited a low prevalence of complex ventricular arrhythmias and favorable mid–term outcomes, supporting the concept of a “benign MAD phenotype” associated with concave chest morphology [156].
7.4. Influence of chest wall conformation on ESE results
To explore how chest wall anatomy influences ESE findings, we carried out a retrospective analysis of a consecutive cohort of 424 consecutive symptomatic patients with MVP and moderate MR who underwent ESE at our center between February 2014 and February 2021 [22]. The primary reason for testing was a mismatch between reported symptoms (dyspnea at rest or during exertion, chest pain, and/or palpitations) and resting echocardiographic evidence consistent with only moderate MR. MHI was measured noninvasively in all patients. At peak exercise, positive ESE was observed in 9.8% and exercise-induced severe MR (ΔEROA ≥0.13 cm²) in 13.2%. During a mean follow-up of 3.2 ± 1.7 years, 75 cardiovascular events occurred, including 55 hospitalizations (heart failure, acute coronary syndromes, or arrhythmias) and 20 mitral valve interventions. Univariate Cox analysis identified several clinical, ECG, and Doppler predictors of MACE, with MHI showing a significant inverse correlation with outcomes. Multivariate analysis confirmed that age, diabetes, peak exercise E/e′ ratio, and peak exercise EROA were independently associated with adverse events, while MHI and beta-blocker therapy were protective. ROC analysis indicated an MHI ≥2.7 predicted event-free survival with high accuracy (AUC = 0.98). Unlike previous studies [91,97-99,102,157,158], this investigation assessed both conventional ESE prognostic markers and a novel anthropometric parameter (MHI), measured by a non-radiological method [15]. Patients with concave chest wall (MHI ≥2.7) had fewer MACE, consistent with literature showing that age, diabetes, impaired stress echo indices, and lack of beta-blocker use predict worse outcomes [159,160]. Both univariate and multivariate models confirmed MHI >2.5 as independently protective.
Figure 5 reports an example of dynamic MR assessment by ESE performed in a symptomatic MVP individual with concave–shaped chest wall conformation (A–P thoracic diameter ≤13.5 cm) affected by resting mild–to–moderate MR. ESE revealed mild increase in MR degree (estimated moderate at peak exercise), with no evidence of severe PH (sPAP <60 mmHg).
The overall profile of this cohort helps explain the favorable outcomes. Most participants had well–controlled blood pressure and a modest burden of other cardiovascular risk factors, thereby limiting the additive mechanical load that hypertension imposes on LV pressure and regurgitant volume [161]. The majority exhibited mid–late systolic rather than holosystolic MR, the latter being more strongly associated with adverse prognosis [158]. MR severity may be overestimated on resting TTE in concave thoraces, especially when LA size is small, because single–frame measures such as vena contracta width and proximal isovelocity surface area can be influenced by jet eccentricity and suboptimal alignment, particularly in MVP with tunneling jets and spray effects within a small receiving chamber [162,163]. Purely mid–late systolic MR has lower regurgitant volume and milder hemodynamic consequences than holosystolic MR; in such cases, regurgitant volume is a more reliable reflection of severity than instantaneous EROA. Accordingly, clinical decisions should incorporate MR timing and consequences rather than single–frame jet parameters [162]. Finally, beta–blocker therapy was associated with a 64% reduction in cardiovascular events, an effect plausibly mediated by attenuating sympathetic activation in MVP [164,165].
7.5. Implications for clinical practice
In a middle–aged, otherwise healthy MVP individual—particularly a woman—with narrow A–P thorax (MHI >2.5) and preserved LVEF, detection of regional (especially basal) and/or global strain impairment should prompt consideration of chest conformation artifacts on 2D–STE rather than automatic attribution to intrinsic myocardial dysfunction. A diffuse basal reduction or a global strain decrement does not respect coronary territories and may avert unnecessary testing for myocardial ischemia. Within MVP populations, a narrow A–P diameter (≤13.5 cm) confers a higher probability of detecting MAD on standard TTE, while a more circular transverse thorax (A–P diameter >13.5 cm) lowers MAD likelihood but often associates with older male sex, comorbidity, larger chambers (especially LA), and moderate–to–severe, potentially hemodynamically significant MR during exertion (Figure 6).
The inverse relationship between MHI and both LV–GLS and LV–GCS is most evident in narrow A–P chests, again suggesting that reduced strain values may derive from chest–wall–related mechanics and tracking limitations rather than primary myocardial disease. Speckle–tracking algorithms assume that the motion of gray–scale kernels remains within the imaging plane throughout the cardiac cycle [166]. When external thoracic geometry displaces the heart, alters its motion pattern, and changes the instantaneous insonation angle, out–of–plane motion can be misinterpreted as in–plane displacement, leading to apparent strain reduction similar to tangential interrogation of a normally contracting wall [166]. Clinicians should therefore recognize that strain decrements can arise from geometric and kinematic factors, not solely from altered myocardial mechanics. Among MVP patients, those with MAD typically have shorter A–P diameters and more impaired deformation indices despite normal LVEF on conventional echocardiography. The compressive and kinematic effects of a narrow A–P chest can induce global and regional motion patterns that confound tracking and simulate intrinsic dysfunction. Incorporating a quick chest shape assessment into routine MVP evaluation can therefore refine interpretation of 2D–STE findings.
These principles also inform the use of ESE in moderate PMR. In centers without external rulers and levels, the A–P diameter can be derived from parasternal long–axis TTE alone to flag concave morphology or pectus excavatum. In patients with MHI >2.5, small LV and LA sizes out of proportion to apparent MR grade, and non–holosystolic MR, clinicians should weigh the risk of overestimating MR and, in some cases, defer ESE for MR hemodynamic assessment or ischemia testing, given the low medium–term event rates and excellent prognosis in such individuals [156,167]. In symptomatic moderate PMR undergoing ESE, chest conformation correlates with outcomes; concave thoraces show fewer MACE over medium–term follow–up. An MHI ≥2.7 may identify a subgroup with particularly favorable prognosis in whom ESE may be unnecessary.
8. Conclusions
Systematic physical examination complemented by chest shape assessment should be routine in MVP. Noninvasive estimation of MHI can help identify symptomatic PMR individuals who are predisposed to moderate basal longitudinal strain attenuation attributable to sternal compression and narrow A–P chest configuration (MHI >2.5 or A–P diameter ≤13.5 cm), a nonmalignant MAD phenotype, and non–hemodynamically significant MR on ESE. As a group, these patients appear to have favorable medium– to long–term outcomes. The present observations warrant validation in adequately powered multicenter prospective studies. In particular, the prognosis of MAD–positive patients with concave chest morphology should be evaluated over extended follow–up to clarify the long–term clinical significance of this anthropometric–mechanical interaction.
Author Contributions
Conceptualization, A.S. and G.L.N.; methodology, A.S. and G.L.N.; software, A.S.; validation, G.L.N.; formal analysis, A.S.; investigation, A.S.; resources, A.S.; data curation, A.S. and G.L.N..; writing—original draft preparation, A.S.; writing—review and editing, G.L.N.; visualization, M.L. and M.B.; supervision, M.L. and M.B.; project administration, A.S.; funding acquisition, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Italian Ministry of Health, Ricerca Corrente IRCCS MultiMedica.
Institutional Review Board Statement
In accordance with the guidelines by the Comitato Etico Territoriale Lombardia 5, ethical review and approval were not required for this retrospective study.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data extracted from included studies will be publicly available on Zenodo (https://zenodo.org).
Acknowledgments
The authors wish to thank Monica Fumagalli for their graphical support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Prothero, A.; Wilson, J.; Kennedy, A.; Brubert, J.; Masters, M.; Newton, J.D.; Dawkins, S.; Enriquez-Sarano, M.; Prendergast, B.D.; et al. Community Prevalence, Mechanisms and Outcome of Mitral or Tricuspid Regurgitation. Heart 2021, 107, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Yadgir, S.; Johnson, C.O.; Aboyans, V.; Adebayo, O.M.; Adedoyin, R.A.; Afarideh, M.; Alahdab, F.; Alashi, A.; Alipour, V.; Arabloo, J.; et al. Global, Regional, and National Burden of Calcific Aortic Valve and Degenerative Mitral Valve Diseases, 1990–2017. Circulation 2020, 141, 1670–1680. [Google Scholar] [CrossRef] [PubMed]
- Dziadzko, V.; Dziadzko, M.; Medina-Inojosa, J.R.; Benfari, G.; Michelena, H.I.; Crestanello, J.A.; Maalouf, J.; Thapa, P.; Enriquez-Sarano, M. Causes and Mechanisms of Isolated Mitral Regurgitation in the Community: Clinical Context and Outcome. Eur. Heart J. 2019, 40, 2194–2202. [Google Scholar] [CrossRef]
- Ling, L.H.; Enriquez-Sarano, M.; Seward, J.B.; Tajik, A.J.; Schaff, H.V.; Bailey, K.R.; Frye, R.L. Clinical Outcome of Mitral Regurgitation Due to Flail Leaflet. N. Engl. J. Med. 1996, 335, 1417–1423. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Baron, G.; Butchart, E.G.; Delahaye, F.; Gohlke-Bärwolf, C.; Levang, O.W.; Tornos, P.; Vanoverschelde, J.L.; Vermeer, F.; Boersma, E.; et al. A Prospective Survey of Patients with Valvular Heart Disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur. Heart J. 2003, 24, 1231–1243. [Google Scholar] [CrossRef] [PubMed]
- Figlioli, G.; Sticchi, A.; Christodoulou, M.N.; Hadjidemetriou, A.; Amorim Moreira Alves, G.; De Carlo, M.; Praz, F.; Caterina, R.; Nikolopoulos, G.K.; Bonovas, S.; et al. Global Prevalence of Mitral Regurgitation: A Systematic Review and Meta-Analysis of Population-Based Studies. J. Clin. Med. 2025, 14, 2749. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [CrossRef]
- Wang, C.L.; Chan, Y.H.; Wu, V.C.; Lee, H.F.; Hsiao, F.C.; Chu, P.H. Incremental Prognostic Value of Global Myocardial Work over Ejection Fraction and Global Longitudinal Strain in Patients with Heart Failure and Reduced Ejection Fraction. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 348–356. [Google Scholar] [CrossRef]
- Freed, L.A.; Levy, D.; Levine, R.A.; Larson, M.G.; Evans, J.C.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and Clinical Outcome of Mitral-Valve Prolapse. N. Engl. J. Med. 1999, 341, 1–7. [Google Scholar] [CrossRef]
- Avierinos, J.F.; Gersh, B.J.; Melton, L.J., III; Bailey, K.R.; Shub, C.; Nishimura, R.A.; Tajik, A.J.; Enriquez-Sarano, M. Natural History of Asymptomatic Mitral Valve Prolapse in the Community. Circulation 2002, 106, 1355–1361. [Google Scholar] [CrossRef]
- Dziadzko, V.; Clavel, M.A.; Dziadzko, M.; Medina-Inojosa, J.R.; Michelena, H.; Maalouf, J.; Nkomo, V.; Thapa, P.; Enriquez-Sarano, M. Outcome and Undertreatment of Mitral Regurgitation: A Community Cohort Study. Lancet 2018, 391, 960–969. [Google Scholar] [CrossRef]
- Tsang, W. Recent Advances in Understanding and Managing Mitral Valve Disease. F1000Res. 2019, 8, F1000. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Baravelli, M.; Vincenti, A.; Trevisan, R.; Zompatori, M.; Nicolosi, G.L.; Lombardo, M.; Anzà, C. A New Modified Anthropometric Haller Index Obtained without Radiological Exposure. Int. J. Cardiovasc. Imaging 2018, 34, 1505–1509. [Google Scholar] [CrossRef]
- Sonaglioni, A.; Nicolosi, G.L.; Braga, M.; Villa, M.C.; Migliori, C.; Lombardo, M. Does Chest Wall Conformation Influence Myocardial Strain Parameters in Infants with Pectus Excavatum? J. Clin. Ultrasound 2021, 49, 918–928. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Nicolosi, G.L.; Granato, A.; Lombardo, M.; Anzà, C.; Ambrosio, G. Reduced Myocardial Strain Parameters in Subjects with Pectus Excavatum: Impaired Myocardial Function or Methodological Limitations Due to Chest Deformity? Semin. Thorac. Cardiovasc. Surg. 2021, 33, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Nicolosi, G.L.; Lombardo, M.; Gensini, G.F.; Ambrosio, G. Influence of Chest Conformation on Myocardial Strain Parameters in Healthy Subjects with Mitral Valve Prolapse. Int. J. Cardiovasc. Imaging 2021, 37, 1009–1022. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Nicolosi, G.L.; Trevisan, R.; Granato, A.; Zompatori, M.; Lombardo, M. Modified Haller Index Validation and Correlation with Left Ventricular Strain in a Cohort of Subjects with Obesity and without Overt Heart Disease. Intern. Emerg. Med. 2022, 17, 1907–1919. [Google Scholar] [CrossRef]
- Sonaglioni, A.; Esposito, V.; Caruso, C.; Nicolosi, G.L.; Bianchi, S.; Lombardo, M.; Gensini, G.F.; Ambrosio, G. Chest Conformation Spuriously Influences Strain Parameters of Myocardial Contractile Function in Healthy Pregnant Women. J. Cardiovasc. Med. 2021, 22, 767–779. [Google Scholar] [CrossRef]
- Archer, J.E.; Gardner, A.; Berryman, F.; Pynsent, P. The Measurement of the Normal Thorax Using the Haller Index Methodology at Multiple Vertebral Levels. J. Anat. 2016, 229, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Nicolosi, G.L.; Rigamonti, E.; Lombardo, M. Impact of Chest Wall Conformation on the Outcome of Primary Mitral Regurgitation Due to Mitral Valve Prolapse. J. Cardiovasc. Echogr. 2022, 32, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Tribouilloy, C.; Hagendorff, A.; Popescu, B.A.; Edvardsen, T.; Pierard, L.A.; Badano, L.; Zamorano, J.L.; Scientific Document Committee of the European Association of Cardiovascular Imaging. Recommendations for the Echocardiographic Assessment of Native Valvular Regurgitation: An Executive Summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 611–644. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Samad, Z.; Shaw, L.K.; Phelan, M.; Glower, D.D.; Ersboll, M.; Toptine, J.H.; Alexander, J.H.; Kisslo, J.A.; Wang, A.; Mark, D.B.; et al. Long-Term Outcomes of Mitral Regurgitation by Type and Severity. Am. Heart J. 2018, 203, 39–48. [Google Scholar] [CrossRef]
- Carpentier, A. Cardiac Valve Surgery—The “French Correction”. J. Thorac. Cardiovasc. Surg. 1983, 86, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Gavazzoni, M.; Taramasso, M.; Zuber, M.; Russo, G.; Pozzoli, A.; Miura, M.; Maisano, F. Conceiving MitraClip as a Tool: Percutaneous Edge-to-Edge Repair in Complex Mitral Valve Anatomies. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Nicolosi, G.L. Why Are Left Ventricular Linear Internal Diameters Still So Important for Clinical Decision-Making to Undergo Surgery in Asymptomatic Patients with Chronic Severe Aortic or Primary Mitral Regurgitation? J. Cardiovasc. Med. 2022, 23, 304–307. [Google Scholar] [CrossRef]
- Flemming, M.A.; Oral, H.; Rothman, E.D.; Briesmiester, K.; Petrusha, J.A.; Starling, M.R. Echocardiographic Markers for Mitral Valve Surgery to Preserve Left Ventricular Performance in Mitral Regurgitation. Am. Heart J. 2000, 140, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhao, Y.; Zhou, T.; Wang, Y.; Zhu, K.; Zhai, J.; Sun, Y.; Lai, H.; Wang, C. Mitral Valve Repair for Degenerative Mitral Regurgitation in Patients with Left Ventricular Systolic Dysfunction: Early and Mid-Term Outcomes. J. Cardiothorac. Surg. 2020, 15, 284. [Google Scholar] [CrossRef]
- Song, J.M.; Kang, S.H.; Lee, E.J.; Shin, M.J.; Lee, J.W.; Chung, C.H.; Kim, D.H.; Kang, D.H.; Song, J.K. Echocardiographic Predictors of Left Ventricular Function and Clinical Outcomes after Successful Mitral Valve Repair: Conventional Two-Dimensional versus Speckle-Tracking Parameters. Ann. Thorac. Surg. 2011, 91, 1816–1823. [Google Scholar] [CrossRef]
- Tribouilloy, C.; Grigioni, F.; Avierinos, J.F.; Barbieri, A.; Rusinaru, D.; Szymanski, C.; Ferlito, M.; Tafanelli, L.; Bursi, F.; Trojette, F.; et al. Survival Implication of Left Ventricular End-Systolic Diameter in Mitral Regurgitation Due to Flail Leaflets: A Long-Term Follow-Up Multicenter Study. J. Am. Coll. Cardiol. 2009, 54, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Li, J.; Lai, H.; Zhu, K.; Sun, Y.; Ding, W.; Hong, T.; Wang, C. Benefits of Early Surgery on Clinical Outcomes after Degenerative Mitral Valve Repair. Ann. Thorac. Surg. 2018, 106, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, T.G.; Thomas, J.D.; Debonnaire, P.J.; Delgado, V.; Hoke, U.; Ewe, S.H.; Versteegh, M.I.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; et al. Global Longitudinal Strain Predicts Left Ventricular Dysfunction after Mitral Valve Repair. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Mascle, S.; Schnell, F.; Thebault, C.; Corbineau, H.; Laurent, M.; Hamonic, S.; Veillard, D.; Mabo, P.; Leguerrier, A.; Donal, E. Predictive Value of Global Longitudinal Strain in a Surgical Population of Organic Mitral Regurgitation. J. Am. Soc. Echocardiogr. 2012, 25, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Sarano, M.; Tajik, A.J.; Schaff, H.V.; Orszulak, T.A.; Bailey, K.R.; Frye, R.L. Echocardiographic Prediction of Survival after Surgical Correction of Organic Mitral Regurgitation. Circulation 1994, 90, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.M.; Shapiro, L.M.; Wells, F.C. Mortality and Morbidity after Mitral Valve Repair: The Importance of Left Ventricular Dysfunction. J. Heart Valve Dis. 1995, 4, 460–468. [Google Scholar] [PubMed]
- Tribouilloy, C.; Rusinaru, D.; Szymanski, C.; Mezghani, S.; Fournier, A.; Lévy, F.; Peltier, M.; Ben Ammar, A.; Carmi, D.; Remadi, J.P.; et al. Predicting Left Ventricular Dysfunction after Valve Repair for Mitral Regurgitation Due to Leaflet Prolapse: Additive Value of Left Ventricular End-Systolic Dimension to Ejection Fraction. Eur. J. Echocardiogr. 2011, 12, 702–710. [Google Scholar] [CrossRef]
- Hu, X.; Jiang, W.; Li, H.; Yan, G.; Wang, Y. Timing of Valve Repair for Asymptomatic Mitral Regurgitation and Preserved Left Ventricular Function. Ann. Thorac. Surg. 2021, 111, 862–870. [Google Scholar] [CrossRef]
- Kitai, T.; Okada, Y.; Shomura, Y.; Tani, T.; Kaji, S.; Kita, T.; Furukawa, Y. Timing of Valve Repair for Severe Degenerative Mitral Regurgitation and Long-Term Left Ventricular Function. J. Thorac. Cardiovasc. Surg. 2014, 148, 1978–1982. [Google Scholar] [CrossRef]
- Nair, V.V.; Das, S.; Nair, R.B.; George, T.P.; Kathayanat, J.T.; Chooriyil, N.; Radhakrishnan, R.; Thanathu Krishnan Nair, J. Mitral Valve Repair in Chronic Severe Mitral Regurgitation: Short-Term Results and Analysis of Mortality Predictors. Indian J. Thorac. Cardiovasc. Surg. 2021, 37, 506–513. [Google Scholar] [CrossRef]
- Kihara, Y.; Sasayama, S.; Miyazaki, S.; Onodera, T.; Susawa, T.; Nakamura, Y.; Fujiwara, H.; Kawai, C. Role of the Left Atrium in Adaptation of the Heart to Chronic Mitral Regurgitation in Conscious Dogs. Circ. Res. 1988, 62, 543–553. [Google Scholar] [CrossRef]
- Szymanski, C.; Bohbot, Y.; Rusinaru, D.; Touati, G.; Tribouilloy, C. Impact of Preoperative Left Atrial Dimension on Outcome in Patients in Sinus Rhythm Undergoing Surgical Valve Repair for Severe Mitral Regurgitation Due to Mitral Valve Prolapse. Cardiology 2019, 142, 189–193. [Google Scholar] [CrossRef]
- Essayagh, B.; Antoine, C.; Benfari, G.; Messika-Zeitoun, D.; Michelena, H.; Le Tourneau, T.; Mankad, S.; Tribouilloy, C.M.; Thapa, P.; Enriquez-Sarano, M. Prognostic Implications of Left Atrial Enlargement in Degenerative Mitral Regurgitation. J. Am. Coll. Cardiol. 2019, 74, 858–870. [Google Scholar] [CrossRef]
- Balachandran, P.; Schaff, H.V.; Lahr, B.D.; Nguyen, A.; Daly, R.C.; Maltais, S.; Pislaru, S.V.; Dearani, J.A. Preoperative Left Atrial Volume Index Is Associated with Postoperative Outcomes in Mitral Valve Repair for Chronic Mitral Regurgitation. J. Thorac. Cardiovasc. Surg. 2020, 160, 661–672.e5. [Google Scholar] [CrossRef]
- Di Gioia, G.; Mega, S.; Nenna, A.; Campanale, C.M.; Colaiori, I.; Scordino, D.; Ragni, L.; Miglionico, M.; Di Sciascio, G. Should Pre-Operative Left Atrial Volume Receive More Consideration in Patients with Degenerative Mitral Valve Disease Undergoing Mitral Valve Surgery? Int. J. Cardiol. 2017, 227, 106–113. [Google Scholar] [CrossRef]
- Kim, H.M.; Cho, G.Y.; Hwang, I.C.; Choi, H.M.; Park, J.B.; Yoon, Y.E.; Kim, H.K. Myocardial Strain in Prediction of Outcomes after Surgery for Severe Mitral Regurgitation. JACC Cardiovasc. Imaging 2018, 11, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, S.; Gibbs, J.S.; Wachter, R.; De Marco, T.; Vonk-Noordegraaf, A.; Vachiéry, J.L. Left Ventricular Heart Failure and Pulmonary Hypertension. Eur. Heart J. 2016, 37, 942–954. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, A.; Bursi, F.; Grigioni, F.; Tribouilloy, C.; Avierinos, J.F.; Michelena, H.I.; Rusinaru, D.; Szymansky, C.; Russo, A.; Suri, R.; et al. Prognostic and Therapeutic Implications of Pulmonary Hypertension Complicating Degenerative Mitral Regurgitation Due to Flail Leaflet: A Multicenter Long-Term International Study. Eur. Heart J. 2011, 32, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Le Tourneau, T.; Richardson, M.; Juthier, F.; Modine, T.; Fayad, G.; Polge, A.S.; Ennezat, P.V.; Bauters, C.; Vincentelli, A.; Deklunder, G. Echocardiography Predictors and Prognostic Value of Pulmonary Artery Systolic Pressure in Chronic Organic Mitral Regurgitation. Heart 2010, 96, 1311–1317. [Google Scholar] [CrossRef]
- Ghoreishi, M.; Evans, C.F.; DeFilippi, C.R.; Hobbs, G.; Young, C.A.; Griffith, B.P.; Gammie, J.S. Pulmonary Hypertension Adversely Affects Short- and Long-Term Survival after Mitral Valve Operation for Mitral Regurgitation: Implications for Timing of Surgery. J. Thorac. Cardiovasc. Surg. 2011, 142, 1439–1452. [Google Scholar] [CrossRef] [PubMed]
- Nozohoor, S.; Hyllén, S.; Meurling, C.; Wierup, P.; Sjögren, J. Prognostic Value of Pulmonary Hypertension in Patients Undergoing Surgery for Degenerative Mitral Valve Disease with Leaflet Prolapse. J. Card. Surg. 2012, 27, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Murashita, T.; Okada, Y.; Kanemitsu, H.; Fukunaga, N.; Konishi, Y.; Nakamura, K.; Koyama, T. The Impact of Preoperative and Postoperative Pulmonary Hypertension on Long-Term Surgical Outcome after Mitral Valve Repair for Degenerative Mitral Regurgitation. Ann. Thorac. Cardiovasc. Surg. 2015, 21, 53–58. [Google Scholar] [CrossRef]
- Genuardi, M.V.; Shpilsky, D.; Handen, A.; VanSpeybroeck, G.; Canterbury, A.; Lu, M.; Shapero, K.; Nieves, R.A.; Thoma, F.; Mulukutla, S.R.; et al. Increased Mortality in Patients with Preoperative and Persistent Postoperative Pulmonary Hypertension Undergoing Mitral Valve Surgery for Mitral Regurgitation: A Cohort Study. J. Am. Heart Assoc. 2021, 10, e018394. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, G.F.; Garcia, A.L.; Correia, P.M.; Branco, C.; Antunes, M.J. Negative Impact of Atrial Fibrillation and Pulmonary Hypertension after Mitral Valve Surgery in Asymptomatic Patients with Severe Mitral Regurgitation: A 20-Year Follow-Up. Eur. J. Cardiothorac. Surg. 2015, 48, 548–556. [Google Scholar] [CrossRef]
- Mentias, A.; Patel, K.; Patel, H.; Gillinov, A.M.; Sabik, J.F.; Mihaljevic, T.; Suri, R.M.; Rodriguez, L.L.; Svensson, L.G.; Griffin, B.P.; et al. Effect of Pulmonary Vascular Pressures on Long-Term Outcome in Patients with Primary Mitral Regurgitation. J. Am. Coll. Cardiol. 2016, 67, 2952–2961. [Google Scholar] [CrossRef]
- Gackowski, A.; Chrustowicz, A.; Kapelak, B.; Miszalski-Jamka, T.; El-Massri, N.; Sadowski, J. Forward Stroke Volume Is Predictor of Perioperative Course in Patients with Mitral Regurgitation Undergoing Mitral Valve Replacement. Cardiol. J. 2010, 17, 386–389. [Google Scholar]
- Haddad, F.; Denault, A.Y.; Couture, P.; Cartier, R.; Pellerin, M.; Levesque, S.; Lambert, J.; Tardif, J.C. Right Ventricular Myocardial Performance Index Predicts Perioperative Mortality or Circulatory Failure in High-Risk Valvular Surgery. J. Am. Soc. Echocardiogr. 2007, 20, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Le Tourneau, T.; Deswarte, G.; Lamblin, N.; Foucher-Hossein, C.; Fayad, G.; Richardson, M.; Polge, A.S.; Vannesson, C.; Topilsky, Y.; Juthier, F.; et al. Right Ventricular Systolic Function in Organic Mitral Regurgitation: Impact of Biventricular Impairment. Circulation 2013, 127, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Chrustowicz, A.; Gackowski, A.; El-Massri, N.; Sadowski, J.; Piwowarska, W. Preoperative Right Ventricular Function in Patients with Organic Mitral Regurgitation. Echocardiography 2010, 27, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Simon, R.; Oelert, H.; Borst, H.G.; Lichtlen, P.R. Influence of Mitral Valve Surgery on Tricuspid Incompetence Concomitant with Mitral Valve Disease. Circulation 1980, 62, I152–I157. [Google Scholar] [CrossRef]
- Murashita, T.; Okada, Y.; Kanemitsu, H.; Fukunaga, N.; Konishi, Y.; Nakamura, K.; Sakon, Y.; Koyama, T. Fate of functional tricuspid regurgitation after mitral valve repair for degenerative mitral regurgitation. Circ. J. 2013, 77, 2288–2294. [Google Scholar] [CrossRef]
- Chan, V.; Burwash, I.G.; Lam, B.K.; Auyeung, T.; Tran, A.; Mesana, T.G.; Ruel, M. Clinical and echocardiographic impact of functional tricuspid regurgitation repair at the time of mitral valve replacement. Ann. Thorac. Surg. 2009, 88, 1209–1215. [Google Scholar] [CrossRef]
- Di Mauro, M.; Bezante, G.P.; Di Baldassarre, A.; Clemente, D.; Cardinali, A.; Acitelli, A.; Salerni, S.; Penco, M.; Calafiore, A.M.; Gallina, S.; et al. Functional tricuspid regurgitation: An underestimated issue. Int. J. Cardiol. 2013, 168, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Yeates, A.; Marwick, T.; Deva, R.; Mundy, J.; Wood, A.; Griffin, R.; Peters, P.; Shah, P. Does moderate tricuspid regurgitation require attention during mitral valve surgery? ANZ J. Surg. 2014, 84, 63–67. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; David, C.M.; Fan, C.S.; Manlhiot, C. Tricuspid regurgitation is uncommon after mitral valve repair for degenerative diseases. J. Thorac. Cardiovasc. Surg. 2017, 154, 110–122.e1. [Google Scholar] [CrossRef]
- Essayagh, B.; Antoine, C.; Benfari, G.; Maalouf, J.; Michelena, H.I.; Crestanello, J.A.; Thapa, P.; Avierinos, J.-F.; Enriquez-Sarano, M. Functional tricuspid regurgitation of degenerative mitral valve disease: A crucial determinant of survival. Eur. Heart J. 2020, 41, 1918–1929. [Google Scholar] [CrossRef]
- Yasmin, F.; Najeeb, H.; Naeem, U.; Moeed, A.; Zaidi, F.; Asghar, M.S.; Aamir, M. Efficacy and safety of concomitant tricuspid repair in patients undergoing mitral valve surgery: A systematic review and meta-analysis. Curr. Probl. Cardiol. 2022, 47, 101360. [Google Scholar] [CrossRef] [PubMed]
- Alashi, A.; Mentias, A.; Patel, K.; Gillinov, A.M.; Sabik, J.F.; Popović, Z.B.; Mihaljevic, T.; Suri, R.M.; Rodriguez, L.L.; Svensson, L.G.; et al. Synergistic utility of brain natriuretic peptide and left ventricular global longitudinal strain in asymptomatic patients with significant primary mitral regurgitation and preserved systolic function undergoing mitral valve surgery. Circ. Cardiovasc. Imaging 2016, 9, e004451. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.J.; Park, S.J.; Yun, H.R.; Jeong, D.S.; Lee, S.C.; Park, S.W.; Park, P.W. Predicting left ventricular dysfunction after surgery in patients with chronic mitral regurgitation: Assessment of myocardial deformation by 2-dimensional multilayer speckle tracking echocardiography. Korean Circ. J. 2016, 46, 213–221. [Google Scholar] [CrossRef]
- Mentias, A.; Naji, P.; Gillinov, A.M.; Rodriguez, L.L.; Reed, G.; Mihaljevic, T.; Suri, R.M.; Sabik, J.F.; Svensson, L.G.; Grimm, R.A.; et al. Strain echocardiography and functional capacity in asymptomatic primary mitral regurgitation with preserved ejection fraction. J. Am. Coll. Cardiol. 2016, 68, 1974–1986. [Google Scholar] [CrossRef]
- Hiemstra, Y.L.; Tomsic, A.; van Wijngaarden, S.E.; Palmen, M.; Klautz, R.J.M.; Bax, J.J.; Delgado, V.; Ajmone Marsan, N. Prognostic value of global longitudinal strain and etiology after surgery for primary mitral regurgitation. JACC Cardiovasc. Imaging 2020, 13, 577–585. [Google Scholar] [CrossRef]
- Donal, E.; Mascle, S.; Brunet, A.; Thebault, C.; Corbineau, H.; Laurent, M.; Leguerrier, A.; Mabo, P. Prediction of left ventricular ejection fraction 6 months after surgical correction of organic mitral regurgitation: The value of exercise echocardiography and deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 922–930. [Google Scholar] [CrossRef]
- Kislitsina, O.N.; Thomas, J.D.; Crawford, E.; Michel, E.; Kruse, J.; Liu, M.; Andrei, A.C.; Cox, J.L.; McCarthy, P.M. Predictors of left ventricular dysfunction after surgery for degenerative mitral regurgitation. Ann. Thorac. Surg. 2020, 109, 669–677. [Google Scholar] [CrossRef]
- Pandis, D.; Sengupta, P.P.; Castillo, J.G.; Caracciolo, G.; Fischer, G.W.; Narula, J.; Anyanwu, A.; Adams, D.H. Assessment of longitudinal myocardial mechanics in patients with degenerative mitral valve regurgitation predicts postoperative worsening of left ventricular systolic function. J. Am. Soc. Echocardiogr. 2014, 27, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.K.; Poulsen, S.H. Left atrial systolic function by strain analysis—A new useful prognostic tool in primary severe mitral regurgitation? Int. J. Cardiol. 2021, 322, 204–205. [Google Scholar] [CrossRef] [PubMed]
- Debonnaire, P.; Leong, D.P.; Witkowski, T.G.; Al Amri, I.; Joyce, E.; Katsanos, S.; Schalij, M.J.; Bax, J.J.; Delgado, V.; Marsan, N.A. Left atrial function by two-dimensional speckle-tracking echocardiography in patients with severe organic mitral regurgitation: Association with guidelines-based surgical indication and postoperative (long-term) survival. J. Am. Soc. Echocardiogr. 2013, 26, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Candan, O.; Ozdemir, N.; Aung, S.M.; Hatipoglu, S.; Karabay, C.Y.; Guler, A.; Gecmen, C.; Dogan, C.; Omaygenc, O.; Bakal, R.B. Atrial longitudinal strain parameters predict left atrial reverse remodeling after mitral valve surgery: A speckle tracking echocardiography study. Int. J. Cardiovasc. Imaging 2014, 30, 1049–1056. [Google Scholar] [CrossRef]
- Stassen, J.; van Wijngaarden, A.L.; Butcher, S.C.; Palmen, M.; Herbots, L.; Bax, J.J.; Delgado, V.; Ajmone Marsan, N. Prognostic value of left atrial reservoir function in patients with severe primary mitral regurgitation undergoing mitral valve repair. Eur. Heart J. Cardiovasc. Imaging 2022, 24, 142–151. [Google Scholar] [CrossRef]
- Mandoli, G.E.; Pastore, M.C.; Benfari, G.; Bisleri, G.; Maccherini, M.; Lisi, G.; Cameli, P.; Lisi, M.; Dokollari, A.; Carrucola, C.; et al. Left atrial strain as a pre-operative prognostic marker for patients with severe mitral regurgitation. Int. J. Cardiol. 2021, 324, 139–145. [Google Scholar] [CrossRef]
- Cameli, M.; Mandoli, G.E.; Nistor, D.; Lisi, E.; Massoni, A.; Crudele, F.; Stricagnoli, M.; Lunghetti, S.; Mondillo, S. Left heart longitudinal deformation analysis in mitral regurgitation. Int. J. Cardiovasc. Imaging 2018, 34, 1741–1751. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, Z.; Fei, H.; Yu, Y.; Ren, S.; Lin, Q.; Li, H.; Tang, Y.; Hou, Y.; Li, M. Left atrial strain reproducibility using vendor-dependent and vendor-independent software. Cardiovasc. Ultrasound 2019, 17, 9. [Google Scholar] [CrossRef]
- Bakkestrøm, R.; Banke, A.; Christensen, N.L.; Pecini, R.; Irmukhamedov, A.; Andersen, M.; Borlaug, B.A.; Møller, J.E. Hemodynamic characteristics in significant symptomatic and asymptomatic primary mitral valve regurgitation at rest and during exercise. Circ. Cardiovasc. Imaging 2018, 11, e007171. [Google Scholar] [CrossRef]
- Utsunomiya, H.; Hidaka, T.; Susawa, H.; Izumi, K.; Harada, Y.; Kinoshita, M.; Itakura, K.; Masada, K.; Kihara, Y. Exercise-stress echocardiography and effort intolerance in asymptomatic/minimally symptomatic patients with degenerative mitral regurgitation: Combined invasive–noninvasive hemodynamic monitoring. Circ. Cardiovasc. Imaging 2018, 11, e007282. [Google Scholar] [CrossRef] [PubMed]
- Picano, E.; Pibarot, P.; Lancellotti, P.; Monin, J.L.; Bonow, R.O. The emerging role of exercise testing and stress echocardiography in valvular heart disease. J. Am. Coll. Cardiol. 2009, 54, 2251–2260. [Google Scholar] [CrossRef] [PubMed]
- Naji, P.; Griffin, B.P.; Barr, T.; Asfahan, F.; Gillinov, A.M.; Grimm, R.A.; Rodriguez, L.L.; Mihaljevic, T.; Stewart, W.J.; Desai, M.Y. Importance of exercise capacity in predicting outcomes and determining optimal timing of surgery in significant primary mitral regurgitation. J. Am. Heart Assoc. 2014, 3, e001010. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.; Griffin, B.P.; Stewart, W.J.; Cosgrove, D.M., 3rd; Thomas, J.D.; Marwick, T.H. Left ventricular function after valve repair for chronic mitral regurgitation: Predictive value of preoperative assessment of contractile reserve by exercise echocardiography. J. Am. Coll. Cardiol. 1996, 28, 1198–1205. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Cosyns, B.; Zacharakis, D.; Attena, E.; Van Camp, G.; Gach, O.; Radermecker, M.; Piérard, L.A. Importance of left ventricular longitudinal function and functional reserve in patients with degenerative mitral regurgitation: Assessment by two-dimensional speckle tracking. J. Am. Soc. Echocardiogr. 2008, 21, 1331–1336. [Google Scholar] [CrossRef]
- Vitel, E.; Galli, E.; Leclercq, C.; Fournet, M.; Bosseau, C.; Corbineau, H.; Bouzille, G.; Donal, E. Right ventricular exercise contractile reserve and outcomes after early surgery for primary mitral regurgitation. Heart 2018, 104, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Magne, J.; Donal, E.; Mahjoub, H.; Miltner, B.; Dulgheru, R.; Thebault, C.; Pierard, L.A.; Pibarot, P.; Lancellotti, P. Impact of exercise pulmonary hypertension on postoperative outcome in primary mitral regurgitation. Heart 2015, 101, 391–396. [Google Scholar] [CrossRef]
- Lee, R.; Haluska, B.; Leung, D.Y.; Case, C.; Mundy, J.; Marwick, T.H. Functional and prognostic implications of left ventricular contractile reserve in patients with asymptomatic severe mitral regurgitation. Heart 2005, 91, 1407–1412. [Google Scholar] [CrossRef]
- Magne, J.; Mahjoub, H.; Dulgheru, R.; Pibarot, P.; Pierard, L.A.; Lancellotti, P. Left ventricular contractile reserve in asymptomatic primary mitral regurgitation. Eur. Heart J. 2014, 35, 1608–1616. [Google Scholar] [CrossRef] [PubMed]
- Magne, J.; Lancellotti, P.; Piérard, L.A. Exercise-induced changes in degenerative mitral regurgitation. J. Am. Coll. Cardiol. 2010, 56, 300–309. [Google Scholar] [CrossRef]
- Magne, J.; Lancellotti, P.; Piérard, L.A. Exercise pulmonary hypertension in asymptomatic degenerative mitral regurgitation. Circulation 2010, 122, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Magne, J.; Lancellotti, P.; O’Connor, K.; Van de Heyning, C.M.; Szymanski, C.; Piérard, L.A. Prediction of exercise pulmonary hypertension in asymptomatic degenerative mitral regurgitation. J. Am. Soc. Echocardiogr. 2011, 24, 1004–1012. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.K.; Kane, G.C. Diastolic stress echocardiography: The time has come for its integration into clinical practice. J. Am. Soc. Echocardiogr. 2014, 27, 1060–1063. [Google Scholar] [CrossRef] [PubMed]
- Burgess, M.I.; Jenkins, C.; Sharman, J.E.; Marwick, T.H. Diastolic stress echocardiography: Hemodynamic validation and clinical significance of estimation of ventricular filling pressure with exercise. J. Am. Coll. Cardiol. 2006, 47, 1891–1900. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.W.; Andersen, O.S.; Smiseth, O.A. Diastolic stress test: Invasive and noninvasive testing. JACC Cardiovasc. Imaging 2020, 13, 272–282. [Google Scholar] [CrossRef]
- Haluska, B.A.; Short, L.; Marwick, T.H. Relationship of ventricular longitudinal function to contractile reserve in patients with mitral regurgitation. Am. Heart J. 2003, 146, 183–188. [Google Scholar] [CrossRef]
- Kusunose, K.; Popović, Z.B.; Motoki, H.; Marwick, T.H. Prognostic significance of exercise-induced right ventricular dysfunction in asymptomatic degenerative mitral regurgitation. Circ. Cardiovasc. Imaging 2013, 6, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Sutton, T.M.; Stewart, R.A.; Gerber, I.L.; West, T.M.; Richards, A.M.; Yandle, T.G.; Kerr, A.J. Plasma natriuretic peptide levels increase with symptoms and severity of mitral regurgitation. J. Am. Coll. Cardiol. 2003, 41, 2280–2287. [Google Scholar] [CrossRef]
- Detaint, D.; Messika-Zeitoun, D.; Avierinos, J.F.; Scott, C.; Chen, H.; Burnett, J.C., Jr.; Enriquez-Sarano, M. B-type natriuretic peptide in organic mitral regurgitation: Determinants and impact on outcome. Circulation 2005, 111, 2391–2397. [Google Scholar] [CrossRef]
- Grigioni, F.; Clavel, M.A.; Vanoverschelde, J.L.; Tribouilloy, C.; Pizarro, R.; Huebner, M.; Avierinos, J.F.; Barbieri, A.; Suri, R.; Pasquet, A.; et al. The MIDA mortality risk score: Development and external validation of a prognostic model for early and late death in degenerative mitral regurgitation. Eur. Heart J. 2018, 39, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Rusinaru, D.; Tribouilloy, C.; Grigioni, F.; Avierinos, J.F.; Suri, R.M.; Barbieri, A.; Szymanski, C.; Ferlito, M.; Michelena, H.; Tafanelli, L.; et al. Left atrial size is a potent predictor of mortality in mitral regurgitation due to flail leaflets: Results from a large international multicenter study. Circ. Cardiovasc. Imaging 2011, 4, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Grigioni, F.; Benfari, G.; Vanoverschelde, J.L.; Tribouilloy, C.; Avierinos, J.F.; Bursi, F.; Suri, R.M.; Guerra, F.; Pasquet, A.; Rusinaru, D.; et al. Long-term implications of atrial fibrillation in patients with degenerative mitral regurgitation. J. Am. Coll. Cardiol. 2019, 73, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Szymanski, C.; Magne, J.; Fournier, A.; Rusinaru, D.; Touati, G.; Tribouilloy, C. Usefulness of preoperative atrial fibrillation to predict outcome and left ventricular dysfunction after valve repair for mitral valve prolapse. Am. J. Cardiol. 2015, 115, 1448–1453. [Google Scholar] [CrossRef] [PubMed]
- Suri, R.M.; Vanoverschelde, J.L.; Grigioni, F.; Schaff, H.V.; Tribouilloy, C.; Avierinos, J.F.; Barbieri, A.; Pasquet, A.; Huebner, M.; Rusinaru, D.; et al. Association between early surgical intervention vs watchful waiting and outcomes for mitral regurgitation due to flail mitral valve leaflets. JAMA 2013, 310, 609–616. [Google Scholar] [CrossRef]
- Jung, J.C.; Jang, M.J.; Hwang, H.Y. Meta-analysis comparing mitral valve repair versus replacement for degenerative mitral regurgitation across all ages. Am. J. Cardiol. 2019, 123, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Lazam, S.; Vanoverschelde, J.L.; Tribouilloy, C.; Grigioni, F.; Suri, R.M.; Avierinos, J.F.; de Meester, C.; Barbieri, A.; Rusinaru, D.; Russo, A.; et al. Twenty-year outcome after mitral repair versus replacement for severe degenerative mitral regurgitation: Analysis of a large, prospective, multicenter, international registry. Circulation 2017, 135, 410–422. [Google Scholar] [CrossRef]
- David, T.E.; David, C.M.; Tsang, W.; Lafreniere-Roula, M.; Manlhiot, C. Long-term results of mitral valve repair for regurgitation due to leaflet prolapse. J. Am. Coll. Cardiol. 2019, 74, 1044–1053. [Google Scholar] [CrossRef]
- Donnellan, E.; Alashi, A.; Johnston, D.R.; Gillinov, A.M.; Pettersson, G.B.; Svensson, L.G.; Griffin, B.P.; Desai, M.Y. Outcomes of patients with mediastinal radiation-associated mitral valve disease undergoing cardiac surgery. Circulation 2019, 140, 1288–1290. [Google Scholar] [CrossRef] [PubMed]
- Vakamudi, S.; Jellis, C.; Mick, S.; Wu, Y.; Gillinov, A.M.; Mihaljevic, T.; Cosgrove, D.M.; Svensson, L.; Cho, L. Sex differences in the etiology of surgical mitral valve disease. Circulation 2018, 138, 1749–1751. [Google Scholar] [CrossRef]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous repair or surgery for mitral regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Sorajja, P.; Vemulapalli, S.; Feldman, T.; Mack, M.; Holmes, D.R., Jr.; Stebbins, A.; Kar, S.; Thourani, V.; Ailawadi, G. Outcomes with transcatheter mitral valve repair in the United States: An STS/ACC TVT Registry report. J. Am. Coll. Cardiol. 2017, 70, 2315–2327. [Google Scholar] [CrossRef]
- Gammie, J.S.; Bartus, K.; Gackowski, A.; D’Ambra, M.N.; Szymanski, P.; Bilewska, A.; Kusmierczyk, M.; Kapelak, B.; Rzucidlo-Resil, J.; Moat, N.; et al. Beating-heart mitral valve repair using a novel ePTFE cordal implantation device: A prospective trial. J. Am. Coll. Cardiol. 2018, 71, 25–36. [Google Scholar] [CrossRef]
- Praz, F.; Spargias, K.; Chrissoheris, M.; Büllesfeld, L.; Nickenig, G.; Deuschl, F.; Schueler, R.; Fam, N.P.; Moss, R.; Makar, M.; et al. Compassionate use of the PASCAL transcatheter mitral valve repair system for patients with severe mitral regurgitation: A multicentre, prospective, observational, first-in-man study. Lancet 2017, 390, 773–780. [Google Scholar] [CrossRef]
- Hahn, R.T.; Chan, V.; Adams, D.H. Current indications for transcatheter edge-to-edge repair in a patient with primary mitral regurgitation. Circulation 2022, 146, 1263–1265. [Google Scholar] [CrossRef] [PubMed]
- Zilberszac, R.; Heinze, G.; Binder, T.; Laufer, G.; Gabriel, H.; Rosenhek, R. Long-term outcome of active surveillance in severe but asymptomatic primary mitral regurgitation. JACC Cardiovasc. Imaging 2018, 11, 1213–1221. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, S.; Song, J.K.; Mahara, K.; Kuwaki, H.; Jang, J.Y.; Takeuchi, M.; Sun, B.J.; Kim, Y.J.; Miyamoto, T.; Oginosawa, Y.; et al. Basal Left Ventricular Dilatation and Reduced Contraction in Patients with Mitral Valve Prolapse Can Be Secondary to Annular Dilatation: Preoperative and Postoperative Speckle-Tracking Echocardiographic Study on Left Ventricle and Mitral Valve Annulus Interaction. Circ. Cardiovasc. Imaging 2016, 9, e005113. [Google Scholar] [CrossRef] [PubMed]
- Bulkley, B.H.; Roberts, W.C. Dilatation of the mitral anulus. A rare cause of mitral regurgitation. Am. J. Med. 1975, 59, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Chandra, S.; Salgo, I.S.; Sugeng, L.; Weinert, L.; Tsang, W.; Takeuchi, M.; Spencer, K.T.; O’Connor, A.; Cardinale, M.; Settlemier, S.; et al. Characterization of degenerative mitral valve disease using morphologic analysis of real-time three-dimensional echocardiographic images: Objective insight into complexity and planning of mitral valve repair. Circ. Cardiovasc. Imaging 2011, 4, 24–32. [Google Scholar] [CrossRef]
- Dahl, J.S.; Videbæk, L.; Poulsen, M.K.; Rudbæk, T.R.; Pellikka, P.A.; Møller, J.E. Global strain in severe aortic valve stenosis: Relation to clinical outcome after aortic valve replacement. Circ. Cardiovasc. Imaging 2012, 5, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Mignot, A.; Donal, E.; Zaroui, A.; Reant, P.; Salem, A.; Hamon, C.; Monzy, S.; Roudaut, R.; Habib, G.; Lafitte, S. Global longitudinal strain as a major predictor of cardiac events in patients with depressed left ventricular function: A multicenter study. J. Am. Soc. Echocardiogr. 2010, 23, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Bertini, M.; Ng, A.C.; Antoni, M.L.; Nucifora, G.; Ewe, S.H.; Auger, D.; Marsan, N.A.; Schalij, M.J.; Bax, J.J.; Delgado, V. Global longitudinal strain predicts long-term survival in patients with chronic ischemic cardiomyopathy. Circ. Cardiovasc. Imaging 2012, 5, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.T.; El-Khuffash, A.; Patel, M.D.; Breatnach, C.R.; James, A.T.; Sanchez, A.A.; Abuchabe, C.; Rogal, S.R.; Holland, M.R.; McNamara, P.J.; et al. Maturational patterns of systolic ventricular deformation mechanics by two-dimensional speckle-tracking echocardiography in preterm infants over the first year of age. J. Am. Soc. Echocardiogr. 2017, 30, 685–698.e1. [Google Scholar] [CrossRef] [PubMed]
- Bijnens, B.H.; Cikes, M.; Claus, P.; Sutherland, G.R. Velocity and deformation imaging for the assessment of myocardial dysfunction. Eur. J. Echocardiogr. 2009, 10, 216–226. [Google Scholar] [CrossRef]
- Chao, C.J.; Jaroszewski, D.; Gotway, M.; Ewais, M.; Wilansky, S.; Lester, S.; Unzek, S.; Appleton, C.P.; Chaliki, H.P.; Gaitan, B.D.; et al. Effects of Pectus Excavatum Repair on Right and Left Ventricular Strain. Ann. Thorac. Surg. 2018, 105, 294–301. [Google Scholar] [CrossRef]
- Truong, V.T.; Li, C.Y.; Brown, R.L.; Moore, R.A.; Garcia, V.F.; Crotty, E.J.; Taylor, M.D.; Ngo, T.M.N.; Mazur, W. Occult RV systolic dysfunction detected by CMR derived RV circumferential strain in patients with pectus excavatum. PLoS ONE 2017, 12, e0189128. [Google Scholar] [CrossRef] [PubMed]
- Lollert, A.; Emrich, T.; Eichstädt, J.; Kampmann, C.; Abu-Tair, T.; Turial, S.; Düber, C.; Kreitner, K.F.; Staatz, G. Differences in myocardial strain between pectus excavatum patients and healthy subjects assessed by cardiac MRI: A pilot study. Eur. Radiol. 2018, 28, 1276–1284. [Google Scholar] [CrossRef] [PubMed]
- Dejgaard, L.A.; Skjølsvik, E.T.; Lie, Ø.H.; Ribe, M.; Stokke, M.K.; Hegbom, F.; Scheirlynck, E.S.; Gjertsen, E.; Andresen, K.; Helle-Valle, T.M.; et al. The mitral annulus disjunction arrhythmic syndrome. J. Am. Coll. Cardiol. 2018, 72, 1600–1609. [Google Scholar] [CrossRef]
- Nalliah, C.J.; Mahajan, R.; Elliott, A.D.; Haqqani, H.; Lau, D.H.; Vohra, J.K.; Morton, J.B.; Semsarian, C.; Marwick, T.; Kalman, J.M.; et al. Mitral valve prolapse and sudden cardiac death: A systematic review and meta-analysis. Heart 2019, 105, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Han, H.C.; Ha, F.J.; Teh, A.W.; Calafiore, P.; Jones, E.F.; Johns, J.; Koshy, A.N.; O’Donnell, D.; Hare, D.L.; Farouque, O.; et al. Mitral valve prolapse and sudden cardiac death: A systematic review. J. Am. Heart Assoc. 2018, 7, e010584. [Google Scholar] [CrossRef] [PubMed]
- Essayagh, B.; Sabbag, A.; Antoine, C.; Benfari, G.; Yang, L.T.; Maalouf, J.; Asirvatham, S.; Michelena, H.; Enriquez-Sarano, M. Presentation and outcome of arrhythmic mitral valve prolapse. J. Am. Coll. Cardiol. 2020, 76, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.J.; Bitkover, C.Y.; Omran, A.S.; David, T.E.; Ivanov, J.; Ali, M.J.; Woo, A.; Siu, S.C.; Rakowski, H. Mitral annular disjunction in advanced myxomatous mitral valve disease: Echocardiographic detection and surgical correction. J. Am. Soc. Echocardiogr. 2005, 18, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Carmo, P.; Andrade, M.J.; Aguiar, C.; Rodrigues, R.; Gouveia, R.; Silva, J.A. Mitral annular disjunction in myxomatous mitral valve disease: A relevant abnormality recognizable by transthoracic echocardiography. Cardiovasc. Ultrasound 2010, 8, 53. [Google Scholar] [CrossRef]
- Vaksmann, G.; Bouzguenda, I.; Guillaume, M.P.; Gras, P.; Silvestri, V.; Richard, A. Mitral annular disjunction and Pickelhaube sign in children with mitral valve prolapse: A prospective cohort study. Arch. Cardiovasc. Dis. 2023, 116, 514–522. [Google Scholar] [CrossRef]
- Figliozzi, S.; Georgiopoulos, G.; Lopes, P.M.; Bauer, K.B.; Moura-Ferreira, S.; Tondi, L.; Mushtaq, S.; Censi, S.; Pavon, A.G.; Bassi, I.; et al. Myocardial fibrosis at cardiac MRI helps predict adverse clinical outcome in patients with mitral valve prolapse. Radiology 2023, 306, 112–121. [Google Scholar] [CrossRef]
- Hussain, N.; Bhagia, G.; Doyle, M.; Rayarao, G.; Williams, R.B.; Biederman, R.W.W. Mitral annular disjunction; how accurate are we? A cardiovascular MRI study defining risk. Int. J. Cardiol. Heart Vasc. 2023, 49, 101298. [Google Scholar] [CrossRef]
- Perazzolo Marra, M.; Cecere, A.; Cipriani, A.; Migliore, F.; Zorzi, A.; De Lazzari, M.; Lorenzoni, G.; Cecchetto, A.; Brunetti, G.; Graziano, F.; et al. Determinants of ventricular arrhythmias in mitral valve prolapse. JACC Clin. Electrophysiol. 2024, 10, 670–681. [Google Scholar] [CrossRef]
- Blondeel, M.; L’Hoyes, W.; Robyns, T.; Verbrugghe, P.; De Meester, P.; Dresselaers, T.; Masci, P.G.; Willems, R.; Bogaert, J.; Vandenberk, B. Serial cardiac magnetic resonance imaging in patients with mitral valve prolapse—A single-center retrospective registry. J. Clin. Med. 2024, 13, 2669. [Google Scholar] [CrossRef]
- Figliozzi, S.; Stankowski, K.; Tondi, L.; Catapano, F.; Gitto, M.; Lisi, C.; Bombace, S.; Olivieri, M.; Cannata, F.; Fazzari, F.; et al. Mitral annulus disjunction in consecutive patients undergoing cardiovascular magnetic resonance: Where is the boundary between normality and disease? J. Cardiovasc. Magn. Reson. 2024, 26, 101056. [Google Scholar] [CrossRef]
- Sonaglioni, A.; Nicolosi, G.L.; Rigamonti, E.; Lombardo, M. The influence of chest wall conformation on myocardial strain parameters in a cohort of mitral valve prolapse patients with and without mitral annular disjunction. Int. J. Cardiovasc. Imaging 2023, 39, 61–76. [Google Scholar] [CrossRef]
- Lee, A.P.; Jin, C.N.; Fan, Y.; Wong, R.H.L.; Underwood, M.J.; Wan, S. Functional implication of mitral annular disjunction in mitral valve prolapse: A quantitative dynamic 3D echocardiographic study. JACC Cardiovasc. Imaging 2017, 10, 1424–1433. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.K.M.; Kwon, D.H.; Abou-Hassan, O.; Chetrit, M.; Harb, S.C.; Patel, D.; Kalahasti, V.; Popovic, Z.B.; Griffin, B.P.; Ayoub, C. Strain evaluation for mitral annular disjunction by echocardiography and magnetic resonance imaging: A case–control study. Int. J. Cardiol. 2021, 334, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Putnam, A.J.; Kebed, K.; Mor-Avi, V.; Rashedi, N.; Sun, D.; Patel, B.; Balkhy, H.; Lang, R.M.; Patel, A.R. Prevalence of mitral annular disjunction in patients with mitral valve prolapse and severe regurgitation. Int. J. Cardiovasc. Imaging 2020, 36, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Hutchins, G.M.; Moore, G.W.; Skoog, D.K. The association of floppy mitral valve with disjunction of the mitral annulus fibrosus. N. Engl. J. Med. 1986, 314, 535–540. [Google Scholar] [CrossRef]
- Mantegazza, V.; Tamborini, G.; Muratori, M.; Gripari, P.; Fusini, L.; Italiano, G.; Volpato, V.; Sassi, V.; Pepi, M. Mitral annular disjunction in a large cohort of patients with mitral valve prolapse and significant regurgitation. JACC Cardiovasc. Imaging 2019, 12, 2278–2280. [Google Scholar] [CrossRef] [PubMed]
- Wunderlich, N.C.; Ho, S.Y.; Flint, N.; Siegel, R.J. Myxomatous mitral valve disease with mitral valve prolapse and mitral annular disjunction: Clinical and functional significance of the coincidence. J. Cardiovasc. Dev. Dis. 2021, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Perazzolo Marra, M.; Rizzo, S.; De Lazzari, M.; Giorgi, B.; Cipriani, A.; Frigo, A.C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Arrhythmic mitral valve prolapse and sudden cardiac death. Circulation 2015, 132, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Nordhues, B.D.; Siontis, K.C.; Scott, C.G.; Nkomo, V.T.; Ackerman, M.J.; Asirvatham, S.J.; Noseworthy, P.A. Bileaflet mitral valve prolapse and risk of ventricular dysrhythmias and death. J. Cardiovasc. Electrophysiol. 2016, 27, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Perazzolo Marra, M.; Basso, C.; De Lazzari, M.; Rizzo, S.; Cipriani, A.; Giorgi, B.; Lacognata, C.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Morphofunctional abnormalities of mitral annulus and arrhythmic mitral valve prolapse. Circ. Cardiovasc. Imaging 2016, 9, e005030. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Perazzolo Marra, M. Mitral annulus disjunction: Emerging role of myocardial mechanical stretch in arrhythmogenesis. J. Am. Coll. Cardiol. 2018, 72, 1610–1612. [Google Scholar] [CrossRef] [PubMed]
- Brochhausen, C.; Turial, S.; Müller, F.K.; Schmitt, V.H.; Coerdt, W.; Wihlm, J.M.; Schier, F.; Kirkpatrick, C.J. Pectus excavatum: History, hypotheses and treatment options. Interact. Cardiovasc. Thorac. Surg. 2012, 14, 801–806. [Google Scholar] [CrossRef]
- Nomura, K.; Ajiro, Y.; Nakano, S.; Matsushima, M.; Yamaguchi, Y.; Hatakeyama, N.; Ohata, M.; Sakuma, M.; Nonaka, T.; Harii, M.; et al. Characteristics of mitral valve leaflet length in patients with pectus excavatum: A single center cross-sectional study. PLoS ONE 2019, 14, e0212165. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Nicolosi, G.L.; Muti-Schünemann, G.E.U.; Rispoli, G.A.; Lombardo, M.; Muti, P. Does preliminary chest shape assessment improve the prognostic risk stratification of individuals with mitral annular disjunction? A case report and narrative review. J. Clin. Med. 2025, 14, 2277. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Rigamonti, E.; Nicolosi, G.L.; Lombardo, M. Appropriate use criteria implementation with modified Haller index for predicting stress echocardiographic results and outcome in a population of patients with suspected coronary artery disease. Int. J. Cardiovasc. Imaging 2021, 37, 2917–2930. [Google Scholar] [CrossRef]
- Magne, J.; Pibarot, P.; Sengupta, P.P.; Donal, E.; Rosenhek, R.; Lancellotti, P. Pulmonary hypertension in valvular disease: A comprehensive review on pathophysiology to therapy from the HAVEC Group. JACC Cardiovasc. Imaging 2015, 8, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Naji, P.; Asfahan, F.; Barr, T.; Rodriguez, L.L.; Grimm, R.A.; Agarwal, S.; Thomas, J.D.; Gillinov, A.M.; Mihaljevic, T.; Griffin, B.P.; et al. Impact of duration of mitral regurgitation on outcomes in asymptomatic patients with myxomatous mitral valve undergoing exercise stress echocardiography. J. Am. Heart Assoc. 2015, 4, e001348. [Google Scholar] [CrossRef]
- Enriquez-Sarano, M.; Avierinos, J.F.; Messika-Zeitoun, D.; Detaint, D.; Capps, M.; Nkomo, V.; Scott, C.; Schaff, H.V.; Tajik, A.J. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N. Engl. J. Med. 2005, 352, 875–883. [Google Scholar] [CrossRef]
- Apostolidou, E.; Maslow, A.D.; Poppas, A. Primary mitral valve regurgitation: Update and review. Glob. Cardiol. Sci. Pract. 2017, 2017, e201703. [Google Scholar] [CrossRef] [PubMed]
- Katsi, V.; Georgiopoulos, G.; Magkas, N.; Oikonomou, D.; Virdis, A.; Nihoyannopoulos, P.; Toutouzas, K.; Tousoulis, D. The role of arterial hypertension in mitral valve regurgitation. Curr. Hypertens. Rep. 2019, 21, 20. [Google Scholar] [CrossRef]
- Topilsky, Y.; Michelena, H.; Bichara, V.; Maalouf, J.; Mahoney, D.W.; Enriquez-Sarano, M. Mitral valve prolapse with mid-late systolic mitral regurgitation: Pitfalls of evaluation and clinical outcome compared with holosystolic regurgitation. Circulation 2012, 125, 1643–1651. [Google Scholar] [CrossRef]
- Grayburn, P.A.; Weissman, N.J.; Zamorano, J.L. Quantitation of mitral regurgitation. Circulation 2012, 126, 2005–2017. [Google Scholar] [CrossRef] [PubMed]
- Taçoy, G.; Balcioğlu, A.S.; Arslan, U.; Durakoğlugil, E.; Erdem, G.; Ozdemir, M.; Cengel, A. Effect of metoprolol on heart rate variability in symptomatic patients with mitral valve prolapse. Am. J. Cardiol. 2007, 99, 1568–1570. [Google Scholar] [CrossRef] [PubMed]
- Slipczuk, L.; Rafique, A.M.; Davila, C.D.; Beigel, R.; Pressman, G.S.; Siegel, R.J. The role of medical therapy in moderate to severe degenerative mitral regurgitation. Rev. Cardiovasc. Med. 2016, 17, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Nicolosi, G.L. The strain and strain rate imaging paradox in echocardiography: Overabundant literature in the last two decades but still uncertain clinical utility in an individual case. Arch. Med. Sci. Atheroscler. Dis. 2020, 5, e297–e305. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Rigamonti, E.; Nicolosi, G.L.; Lombardo, M. Prognostic value of modified Haller index in patients with suspected coronary artery disease referred for exercise stress echocardiography. J. Cardiovasc. Echogr. 2021, 31, 85–95. [Google Scholar] [CrossRef]
Figure 1.
Echocardiographic predictors of adverse outcomes in primary mitral regurgitation, derived from conventional 2D transthoracic echocardiography and speckle tracking echocardiography. (A) Regurgitant volume. (B) Vena contracta width. (C) PISA radius. (D) Dominant transmitral E wave. (E) Dense holosystolic continuous–wave Doppler MR jet. (F) Increased tricuspid regurgitation velocity. (G) Enlarged LV end–systolic diameter. (H) Reduced LVEF. (I) Impaired LV–GLS. (L) Enlarged LA diameter. (M) Increased LA volume. (N) Reduced LASr. (O) Enlarged RV–EDD. (P) Reduced TAPSE. (Q) Moderate–to–severe FTR. FTR, functional tricuspid regurgitation; GLS, global longitudinal strain; LA, left atrial; LASr, left atrial reservoir strain; LV, left vetricular; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; PISA, proximal isovelocity surface area; RV–EDD, right ventricular end–diastolic diameter; TAPSE, tricuspid annular plane systolic excursion.
Figure 1.
Echocardiographic predictors of adverse outcomes in primary mitral regurgitation, derived from conventional 2D transthoracic echocardiography and speckle tracking echocardiography. (A) Regurgitant volume. (B) Vena contracta width. (C) PISA radius. (D) Dominant transmitral E wave. (E) Dense holosystolic continuous–wave Doppler MR jet. (F) Increased tricuspid regurgitation velocity. (G) Enlarged LV end–systolic diameter. (H) Reduced LVEF. (I) Impaired LV–GLS. (L) Enlarged LA diameter. (M) Increased LA volume. (N) Reduced LASr. (O) Enlarged RV–EDD. (P) Reduced TAPSE. (Q) Moderate–to–severe FTR. FTR, functional tricuspid regurgitation; GLS, global longitudinal strain; LA, left atrial; LASr, left atrial reservoir strain; LV, left vetricular; LVEF, left ventricular ejection fraction; MR, mitral regurgitation; PISA, proximal isovelocity surface area; RV–EDD, right ventricular end–diastolic diameter; TAPSE, tricuspid annular plane systolic excursion.
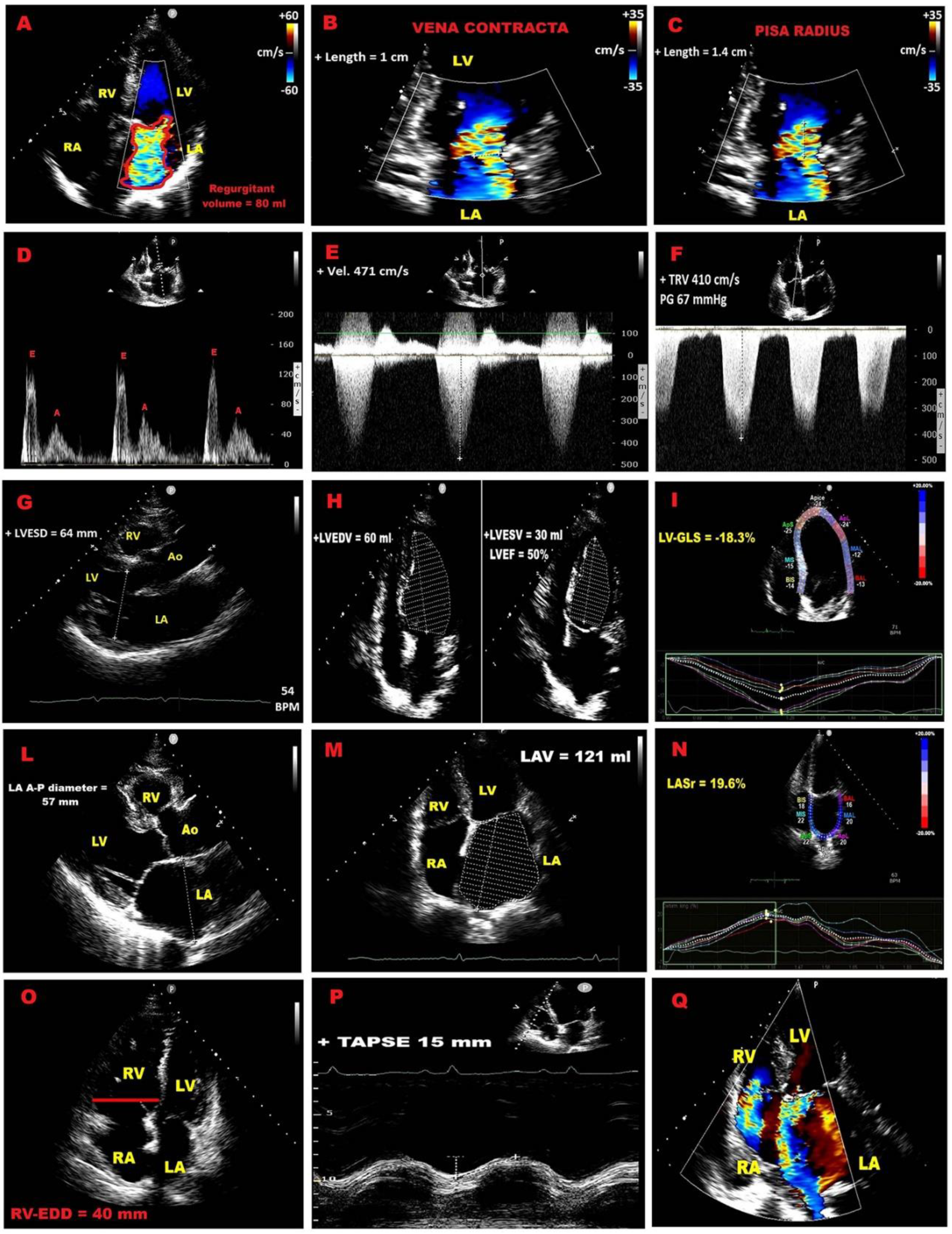
Figure 2.
Modified Haller Index. (A) Latero–lateral external thoracic diameter measured with a rigid ruler and level at the distal third of the sternum. (B) Antero–posterior internal thoracic diameter obtained on transthoracic echocardiography in the parasternal long–axis view, measured as the distance from the true apex of the ultrasound sector to the posterior wall of the descending aorta immediately behind the left atrium. Ao, aorta; Asc, ascending; Desc, descending; LA, left atrium; LV, left ventricle; RV, right ventricle.
Figure 2.
Modified Haller Index. (A) Latero–lateral external thoracic diameter measured with a rigid ruler and level at the distal third of the sternum. (B) Antero–posterior internal thoracic diameter obtained on transthoracic echocardiography in the parasternal long–axis view, measured as the distance from the true apex of the ultrasound sector to the posterior wall of the descending aorta immediately behind the left atrium. Ao, aorta; Asc, ascending; Desc, descending; LA, left atrium; LV, left ventricle; RV, right ventricle.
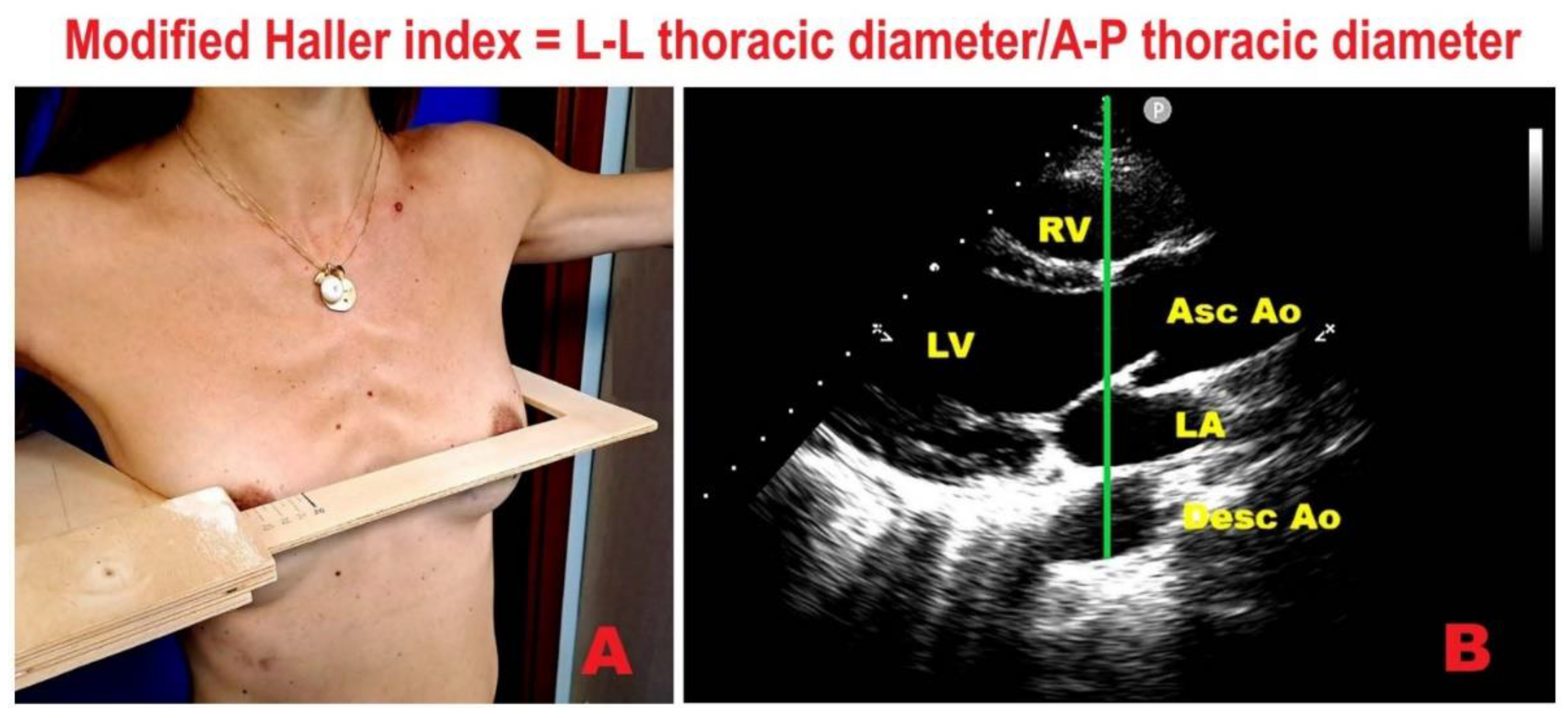
Figure 3.
Example of MVP with concave chest wall conformation (MHI >2.5 or A–P diameter ≤13.5 cm). (A) Narrow A–P thoracic diameter (≤13.5 cm) measured from the parasternal long–axis view. (B) Parasternal long–axis view showing mild MR on color Doppler. (C) 2D–STE bull’s–eye plot revealing mild–to–moderate impairment of LV–GLS, most marked in basal segments. 2D, two–dimensional; Ao, aorta; A–P, antero–posterior; Asc, ascending; Desc, descending; GLS, global longitudinal strain; LA, left atrium; LV, left ventricle; MHI, Modified Haller Index; MVP, mitral valve prolapse; MR, mitral regurgitation; RV, right ventricle; STE, speckle tracking echocardiography.
Figure 3.
Example of MVP with concave chest wall conformation (MHI >2.5 or A–P diameter ≤13.5 cm). (A) Narrow A–P thoracic diameter (≤13.5 cm) measured from the parasternal long–axis view. (B) Parasternal long–axis view showing mild MR on color Doppler. (C) 2D–STE bull’s–eye plot revealing mild–to–moderate impairment of LV–GLS, most marked in basal segments. 2D, two–dimensional; Ao, aorta; A–P, antero–posterior; Asc, ascending; Desc, descending; GLS, global longitudinal strain; LA, left atrium; LV, left ventricle; MHI, Modified Haller Index; MVP, mitral valve prolapse; MR, mitral regurgitation; RV, right ventricle; STE, speckle tracking echocardiography.
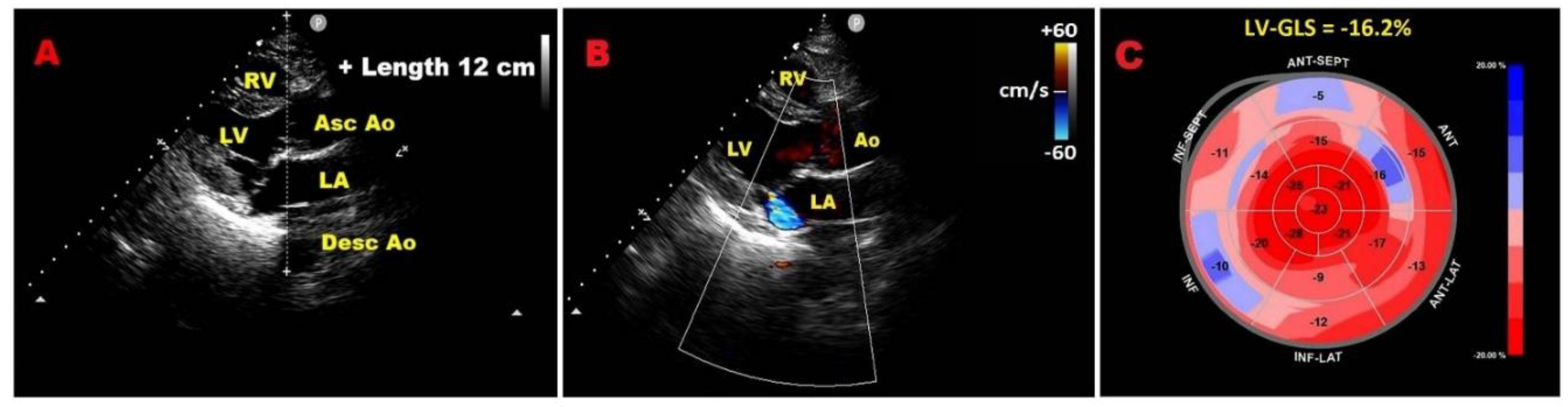
Figure 4.
Representative example of MVP individual with MAD, narrow A–P thoracic diameter and mild deterioration of LV–GLS with “apical sparing” pattern. (A) Parasternal long–axis view showing MVP, MAD, and reduced A–P diameter (red line indicates MAD distance; green line indicates A–P thoracic diameter). (B) 2D–STE bull’s–eye plot depicting mild LV–GLS reduction with predominant basal involvement and relative apical sparing. Ao, aorta; A–P, antero–posterior; Asc, ascending; Desc, descending; GLS, global longitudinal strain; LV, left ventricle; MAD, mitral annular disjunction; MVP, mitral valve prolapse; RV, right ventricle.
Figure 4.
Representative example of MVP individual with MAD, narrow A–P thoracic diameter and mild deterioration of LV–GLS with “apical sparing” pattern. (A) Parasternal long–axis view showing MVP, MAD, and reduced A–P diameter (red line indicates MAD distance; green line indicates A–P thoracic diameter). (B) 2D–STE bull’s–eye plot depicting mild LV–GLS reduction with predominant basal involvement and relative apical sparing. Ao, aorta; A–P, antero–posterior; Asc, ascending; Desc, descending; GLS, global longitudinal strain; LV, left ventricle; MAD, mitral annular disjunction; MVP, mitral valve prolapse; RV, right ventricle.
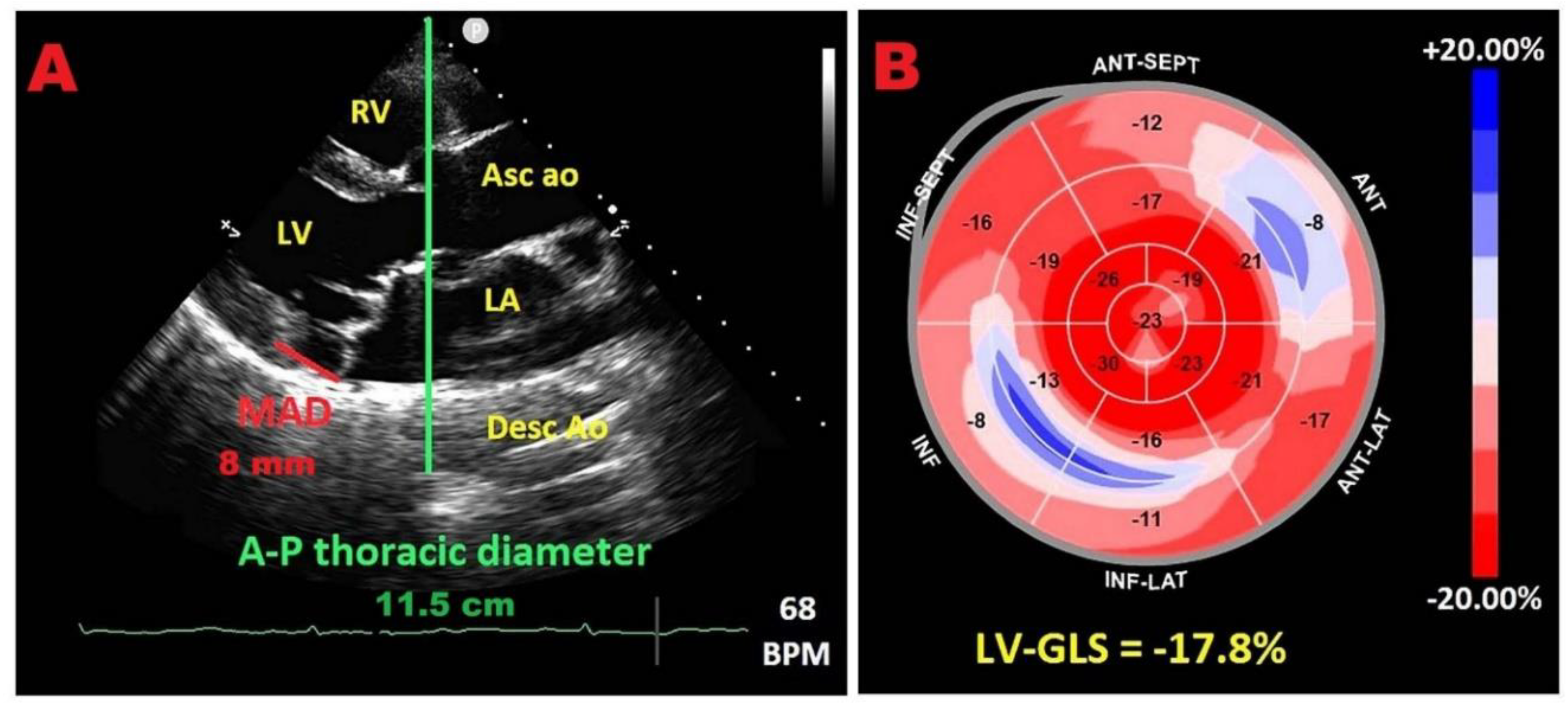
Figure 5.
Dynamic MR assessment by ESE in symptomatic MVP with concave thorax (A–P diameter ≤13.5 cm) and resting mild–to–moderate MR. (A) A–P diameter measurement in the parasternal long–axis view as the distance between the true sector apex and the posterior wall of the descending aorta. (B) Parasternal long–axis view showing resting mild–to–moderate MR. (C) Parasternal long–axis view revealing peak–exercise moderate MR. (D) Continuous–wave Doppler–derived peak exercise TRV of 3.2 m/s (RV–RA gradient 42 mmHg), excluding exercise–induced severe pulmonary hypertension (sPAP <60 mmHg). ESE, exercise stress echocardiography; MR, mitral regurgitation; MVP, mitral valve prolapse; PH, pulmonary hypertension; RA, right atrial; RV, right ventricular; sPAP, systolic pulmonary artery pressure; TRV, tricuspid regurgitation velocity.
Figure 5.
Dynamic MR assessment by ESE in symptomatic MVP with concave thorax (A–P diameter ≤13.5 cm) and resting mild–to–moderate MR. (A) A–P diameter measurement in the parasternal long–axis view as the distance between the true sector apex and the posterior wall of the descending aorta. (B) Parasternal long–axis view showing resting mild–to–moderate MR. (C) Parasternal long–axis view revealing peak–exercise moderate MR. (D) Continuous–wave Doppler–derived peak exercise TRV of 3.2 m/s (RV–RA gradient 42 mmHg), excluding exercise–induced severe pulmonary hypertension (sPAP <60 mmHg). ESE, exercise stress echocardiography; MR, mitral regurgitation; MVP, mitral valve prolapse; PH, pulmonary hypertension; RA, right atrial; RV, right ventricular; sPAP, systolic pulmonary artery pressure; TRV, tricuspid regurgitation velocity.
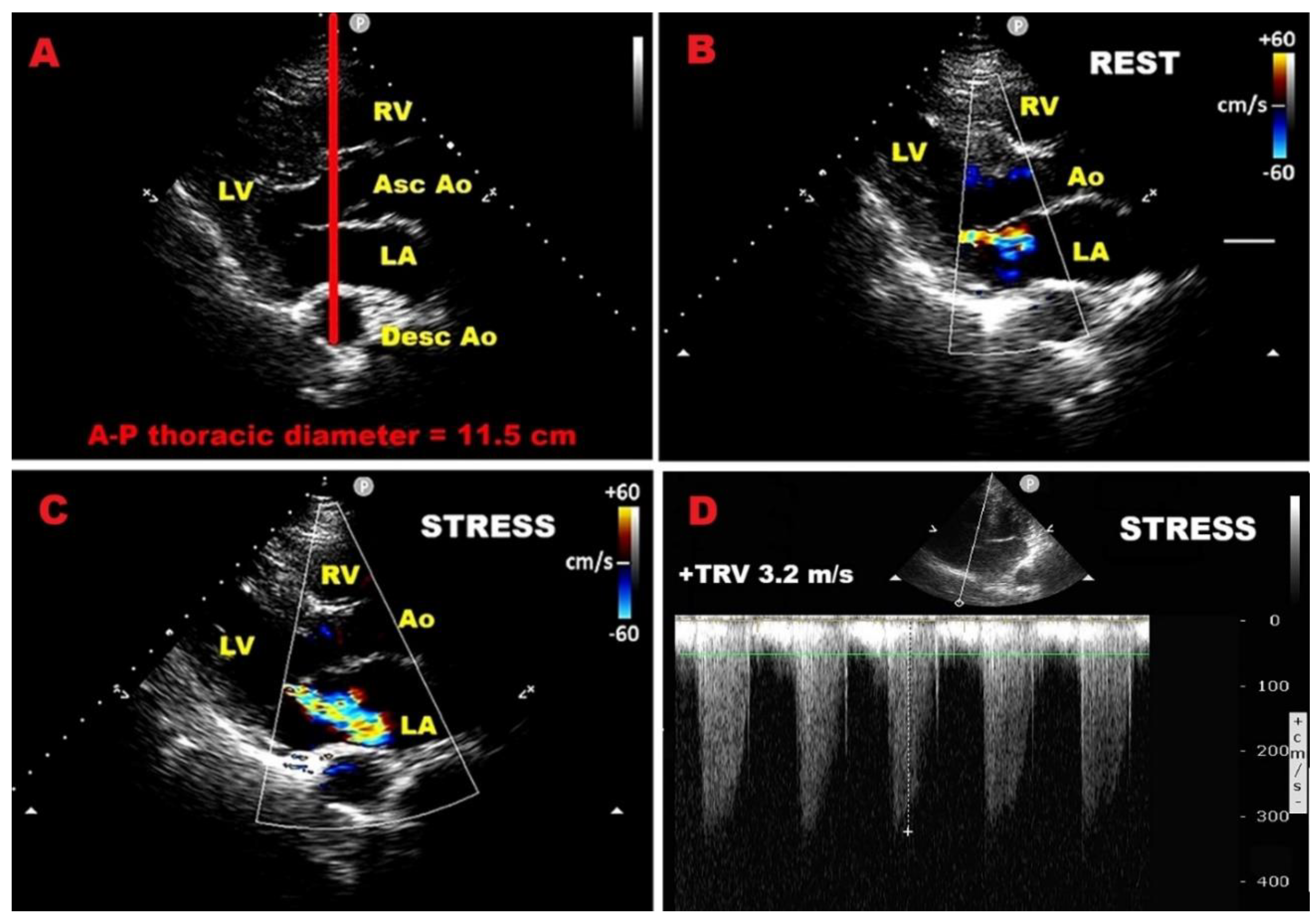
Figure 6.
Parasternal long–axis view illustrating A–P thoracic assessment in two MVP patients. (A) MVP individuals with narrow A–P diameter (≤ 13.5 cm) and mild MR. (B) MVP individual with a more circular transverse thoracic section and moderate–to–severe MR. Red lines indicate the A–P sterno–vertebral distance. Ao, aorta; A–P, antero–posterior; Asc, ascending; Desc, descending; LA, left atrium; LV, left ventricle; MR, mitral regurgitation; MVP, mitral valve prolapse; RV, right ventricle.
Figure 6.
Parasternal long–axis view illustrating A–P thoracic assessment in two MVP patients. (A) MVP individuals with narrow A–P diameter (≤ 13.5 cm) and mild MR. (B) MVP individual with a more circular transverse thoracic section and moderate–to–severe MR. Red lines indicate the A–P sterno–vertebral distance. Ao, aorta; A–P, antero–posterior; Asc, ascending; Desc, descending; LA, left atrium; LV, left ventricle; MR, mitral regurgitation; MVP, mitral valve prolapse; RV, right ventricle.
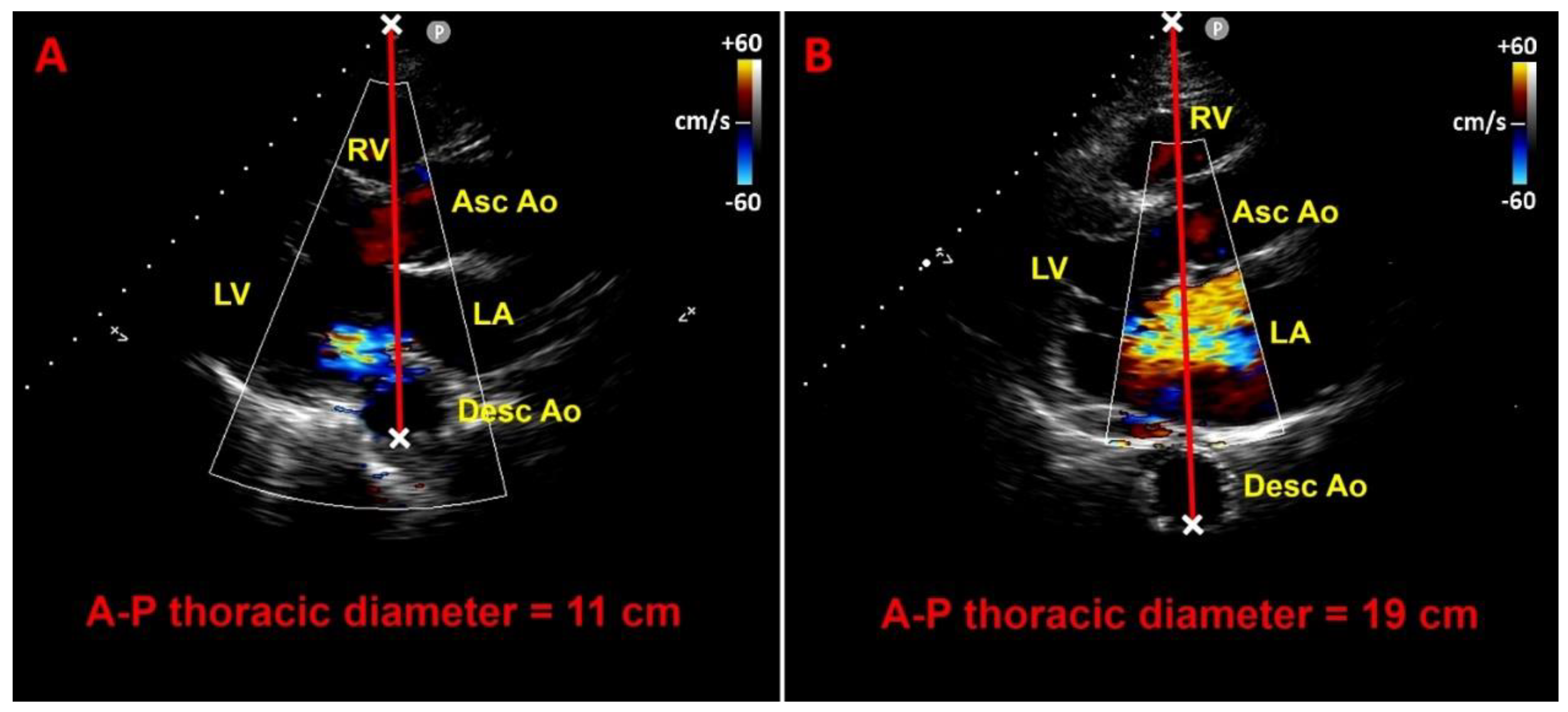

Table 1.
Principal qualitative, semiquantitative, quantitative and structural indicators of PMR severity. CW, continuous; wave; EROA, effective regurgitant orifice area; LA, left atrium/left atrial; LVESD, left ventricular end–systolic diameter; MV, mitral valve; PISA, proximal isovelocity surface area; PMR, primary mitral regurgitation; TVI, time–velocity integral.
Table 1.
Principal qualitative, semiquantitative, quantitative and structural indicators of PMR severity. CW, continuous; wave; EROA, effective regurgitant orifice area; LA, left atrium/left atrial; LVESD, left ventricular end–systolic diameter; MV, mitral valve; PISA, proximal isovelocity surface area; PMR, primary mitral regurgitation; TVI, time–velocity integral.
| Category | Criteria |
| Qualitative | MV morphology (flail leaflet, papillary rupture, severe retraction, perforation); Large central jet (>50% LA) or eccentric jet; Large systolic flow convergence; Dense holosystolic CW Doppler jet |
| Semiquantitative | Vena contracta ≥7 mm; Systolic pulmonary vein flow reversal; Dominant E–wave (>1.2 m/s); TVI mitral/TVI aortic >1.4 |
| Quantitative | PISA radius ≥1 cm; EROA ≥40 mm²; Regurgitant volume ≥60 mL/beat; Regurgitant fraction ≥50% |
| Structural | LVESD ≥40 mm; LA diameter ≥55 mm or volume ≥60 mL/m² |
Table 2.
summarizes all ESE-derived prognostic indicators in PMR individuals.
| Category | Prognostic Indicator | Threshold / Definition | Clinical Implication |
| LV systolic function | Exercise LVEF | < 68% | Predicts postoperative LV dysfunction |
| LVESVi | ≥ 25 mL/m² | Predicts postoperative LV dysfunction | |
| LV–GLS normalized for LVESD | Worse than –5.7%/cm | Predicts postoperative LV dysfunction | |
| Contractile reserve (LVEF) | Δ ≥ 4% | Protective; absence predicts adverse outcomes | |
| Contractile reserve (LV–GLS) |
Δ ≥ 1.9% | Protective; absence predicts adverse outcomes | |
| Blunted GLS increase | < 2% during exercise | Identifies early subclinical dysfunction | |
| Mitral regurgitation dynamics | Increase in EROA | Δ ≥ 10 mm² | Predicts adverse CV outcomes |
| Increase in regurgitant volume | Δ ≥ 10 mL | Predicts adverse CV outcomes | |
| Dynamic MR | MR worsens to severe during exercise | Linked with worse prognosis | |
| Pulmonary pressures | Exercise sPAP | > 60 mmHg | Predicts symptom onset & adverse outcomes |
| Right ventricular function | Exercise TAPSE | ≤ 18 mm (high-risk) | Associated with poor prognosis & CV events |
| Diastolic stress echo | Septal E/e′ | > 15 (abnormal) | Indicates elevated filling pressures |
| Average E/e′ | > 14 (abnormal) | Indicates elevated filling pressures | |
| TRV | > 2.8 m/s | Indicates exercise-induced PH | |
| Normal response | Septal E/e′ < 10 and TRV < 2.8 m/s |
Favourable prognosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



