Submitted:
18 August 2025
Posted:
19 August 2025
You are already at the latest version
Abstract
The Public Opinion Survey of Human Attributes–Stuttering (POSHA–S) Database, intermittently updated, currently contains 25,739 respondents from 46 countries with responses in 31 languages, representing 11 world regions. Among public and selected population samples, more than 600 self-identified stutterers are included. The Microsoft Excel database file features more than 150 columns of POSHA–S results. Some data, such as state/province and country of respondents’, primary job or occupation, languages known, race, and religion are included as text. Other demo-graphic and all attitude items are numeric data. The POSHA–S has check boxes or 1-5 scales for other demographic variables and general ratings that compare stuttering to four other attributes (intelligent, left handed, obese, and mentally ill). All subsequent stuttering attitude items are scored on a 1-3 scale reflecting “no,” “not sure,” and “yes.” All scaled ratings are converted to a uniform -100 to +100 scale, with some item ratings inverted so that, uniformly, higher ratings reflect more positive attitudes, and lower ratings reflect more negative attitudes. All respondents are classified according to population, category within population, region or continent, country, language, and other distinctive features.
Keywords:
public attitudes
; stuttering
; POSHA–S
; international
; obesity
; mental illness
; left handed
; intelligence
1. Summary
1.1. Rationale
Stuttering is primarily a genetically caused problem of speech fluency [1] that typically manifests as sound or syllable repetitions, sound or syllable prolongations, or silent or audible blocks or stoppages [2]. With some parallels to Wendell Johnson’s classic interaction hypothesis [3], stuttering can be conceptualized as a two-pillar condition. The first, personal pillar relates to a speaker’s stuttering and that speaker’s reactions to his or her stuttering. The second, societal pillar relates to a listener’s reaction to the speaker’s stuttering and his or her subsequent reaction to the listener’s reaction [4]. It is within the societal pillar that stereotypes, stigma, and even discrimination evolve. Since the mid-1970s, research has shown that the general public [5], teachers [6], high school and university students [7], elementary students [8], preschool children [9], and even speech-language pathology trainees and practitioners [10] hold stereotypic or stigmatizing beliefs and reactions regarding the disorder of stuttering and a person who stutters. For example, stuttering is typically regarded as a psychological problem, and stutterers are commonly perceived as being more nervous, shy, and fearful than nonstutterers by all of these groups. As a result of negative public attitudes, self-stigma can occur [11], wherein people who stutter comes to believe that they are “less than” or, in Goffman’s words, possess a “spoiled identity” [12].
Using a variety of measures, such as semantic differential scales [13], nearly all research studies on public attitudes toward stuttering from the mid-1970s to 2000 reported examples of negative attitudes [14]. It was, however, impossible to ascertain what “average” public attitudes toward stuttering are or to directly compare results from one study to the next. Accordingly, in 1999 a task force was formed at West Virginia University to develop what was intended to become a standard measure of explicit public attitudes [15] toward stuttering and selected other human conditions [16]. The name adopted for the initiative was the International Project on Attitudes Toward Human Attributes (IPATHA), and the primary and first instrument to be developed was the Public Opinion Survey of Human Attributes—Stuttering (POSHA–S). IPATHA’s stated vision at that time was to understand and improve public attitudes toward stuttering and other stigmatizing conditions worldwide through objective measures, and its mission was to foster effective use of the POSHA–S in comparing public attitudes and reducing stigma related to negative public opinion [14]. Six principles were adopted to guide the development of the POSHA–S, namely, to (a) permit comparison of attitudes toward stuttering to attitudes toward other human attributes using accepted epidemiological methods; (b) be sufficiently short, understandable, and easy to complete for adults and older children or average literacy; (c) possess satisfactory psychometric qualities such as reliability and validity; (d) provide information that would be useful to potential stakeholders such as speech-language pathologists and the stuttering self-help community; (e) contain simple, grammatical, and slang-free language that would foster accurate translations to other languages; and (f) permit easy and efficient scoring and interpretation of results [17].
1.2. Pilot Studies
The first research effort of the IPATHA initiative was to gather data from a variety of countries on the first experimental prototype. It was termed the POSHA–E [17] (and later termed the POSHA–E1 [18]). Following an extensive demographic section, this first version included a general section asking four questions about nine different human attributes (stuttering, obesity, mental illness, wheelchair use, old age, multilingualism, left handedness, good talking, and intelligence). Next, for each of these attributes, a detailed section was developed. The demographic, general, and detailed section for stuttering contained 148 items or questions. In the first US sample, 165 respondents rated the POSHA–E1 for stuttering plus parallel POSHAs pertaining to two of the other eight attributes in counterbalanced order in order that respondents would not be “primed” to think only about stuttering. A quasi-continuous scale with labels at 0 to 100, with 50 in the middle, followed each item. Respondents were instructed to mark through the line to depict their response to each item. Research assistants scored 165 returned questionnaires using a transparent “ruler” to convert respondents’ vertical marks to numbers from 0 to 100. Errors in both responding and in measuring the scales occurred, but a careful analysis revealed that they had virtually no effect on the overall results. Additionally, the questionnaires were determined to contain language that was appropriate for readability, i.e., from 2nd to 8th grade reading level, The order of the stuttering section, appearing first, second, or third in the total questionnaire, also had no effect on the results [17].
“IPATHA partners” who were recruited or volunteered then administered experimental versions of the POSHA to public samples in the US and seven other countries, in two of which were after translation of the instrument to Bulgarian and Brazilian Portuguese [19]. A total of 744 respondents in 15 samples from six countries filled out the POSHA–E1 [20]. Soon, it became clear that the POSHA–E1 was too difficult and time-consuming for respondents to complete, and its quasi-continuous scale invited too many errors in both responding and data reduction [18].
Thus, the second experimental version (POSHA–E2) was developed wherein the quasi-continuous scale was replaced throughout with a 1-9 scale for all ratings in the demographic, general, and detailed stuttering sections. It fostered somewhat shorter administration time, far fewer errors in responding, and much less time in data reduction [18]. The POSHA–E2 was administered to 26 different samples, with six of them followed by a second administration for reliability assessment or a post-intervention appraisal. A total of 1103 respondents from eight different samples in six different languages [20].
1.3. Final Version of the POSHA–S
The subsequent process of developing the final version of the POSHA–S was informed by the fact that some of the 1-9 rating choices, most notably 4 and 6, were rarely selected. Also, the process of deciding about numerous items on such a long scale resulted in too many respondents going back and changing previous items, something they were instructed not to do unless they realized they had made an error. These limitations led the author to strive for a shorter, more user-friendly questionnaire. First, the demographic and general item ratings were changed to a 1-5 scale, and the detailed stuttering item scale was changed to a 1-3 rating wherein 1 = “No,” 2 = “Not Sure,” and 3 = “Yes,” [2005]. Second, an item analysis was carried out to change or eliminate items that had been worded ambiguously (e.g., “ignore stuttering” versus “try to act like the person was talking normally”), items that did not translate well (e.g., “my younger child’s teacher” must include “younger than who?” in Spanish), items that were quite invariable in different populations, and items unlikely to change after interventions to improve attitudes. Final item selection was also informed by standard factor analysis [18].
The demographic section of the final POSHA–S includes a wide variety of variables that might predict more positive versus less positive stuttering attitudes. It asks respondents to identify their country and state/province/district of birth and current residence, age, years of education, sex (or gender if the respondent interpreted “sex” in that way), marital status currently or in the past, parental status, work or student status, primary occupation or the one in which they were best trained, native and later languages known, religion, and race. This section also asked for ratings of the respondents’ income relative to their friends and family as well as relative to all the people in their country. From these two 1-5 ratings, a relative income score is generated that is weighted more heavily on the latter country rating. Next, respondents are asked to rate their physical health, mental health, ability to learn, and ability to speak. Finally, it asks them to rate 12 different life priorities, such as “being free” or “attending parties and social events.”
The general section asks for three ratings and one “select all that apply” item for the attributes of stuttering, obesity, mental illness, left handedness, and intelligence. For each attribute, respondents are asked to rate their overall impression, desire to which they would like to be or have (the attribute), amount if know about it. The fourth item asks who the respondent knows with each of the attributes with choices (and weightings) to generate a score follows: nobody, acquaintance, close friend, relative, me (oneself), or other.
The final POSHA–S contains 33 demographic open-ended questions and ratings, 15 general ratings and five checklists, and 35 ratings in the detailed stuttering section. The stuttering items are presented after different prompts (e.g., “I believe stuttering is caused by…”). Four additional stuttering items are taken from the general section, that is, overall impression, wanting to have stuttering, amount known, and persons known who stutter. In standard scoring of the POSHA–S, all these items are averaged into eight components. Means for four components (i.e., Traits/Personality, Help From, Cause, and Potential) are averaged into a Beliefs subscore. Beliefs are regarded as external in the sense that respondents must rely on what they have learned, heard, or intuited without needing to think about themselves. The other four components (i.e., Accommodating/Helping, Social Distance/Sympathy, Knowledge/Experience, and Knowledge Source) are averaged into a Self Reactions subscore that is internal. In this case, respondents must consider their own likely reactions to a person stuttering or their knowledge about the disorder. The mean of these two stuttering subscores, Beliefs and Self Reactions, is the Overall Stuttering Score.
A third subscore, Obesity/Mental Illness, is included to place stuttering within the context of other, typically undesired, attributes. The mean of items for obesity and mental illness become components of overall impression, want to be or have, and amount known for these two attributes. The three components are averaged for the Obesity/Mental Illness subscore. Ratings for the remaining two general attributes, left handedness and intelligence are not included in the standard scoring of the POSHA–S.
All ratings on the POSHA–S are converted to a -100 to +100 scale. Moreover, based on the extant literature on the nature of stuttering, accuracy, and sensitivity as reported by stutterers [21], higher scores on the -100 to +100 scale reflect more positive attitudes and lower scores, less positive attitudes. Accordingly, converted scores for some items, such as “If it were talking with a person who stutters, I would fill in the person’s words” are inverted such that scores of 3 (“yes”) is considered a negative attitude while a 1 (“no”) is considered positive.
2. Data Description
2.1. POSHA–S Database Overview and Standard Scoring
The current POSHA–S Database in Table S1 contains 25,739 respondents obtained from 261 different samples representing 46 countries and 11 world regions, with responses in 31 languages. The mean number of respondents in individual samples was 99.
Figure 1 is a radial graph that displays the lowest (least positive) and highest (most positive) mean values from any sample (not an individual respondent) in the database. Importantly, these lowest and highest values did not come from the same samples; each individual score was considered separately. Figure 1 also shows the median of all the sample means for each variable as the best current estimate of “average” attitudes toward stuttering. These three scores are displayed for the three subscores and components within them. Data points closer to the center are more negative; those closer to the periphery are more positive. Typically, in professional presentations and research articles, individual samples being analyzed are superimposed on this graph in order that investigators can compare the positivity/negativity of attitudes of their sample to all the previous samples in the Database [14]. Numeric values for these subscores and components, as well as Overall Stuttering Scores, on the -100 to +100 scale are listed in Table 1. The table also shows the means and standard deviations for all 25,739 respondents combined. It can be seen that the combined mean values are quite similar to the median of the 261 sample means, with a mean difference of only 3.4 units on the 201-unit scale (-100 to +100), with a range of 0-10 units.
Figure 2 and Figure 3 display the individual items for each component in line graphs for Beliefs and for Self Reactions, respectively. Figure 4 is a similar graph showing the first three items for the five attributes from the general section of the POSHA–S.
Table S1 is the POSHA–S Database. It is a Microsoft Excel file in which columns identify by most of the POSHA–S variables at the top. Each row contains results for one respondent. Numeric results, highlighted in orange, are ratings that have been inverted so that the higher -100 to +100 converted scores represent more positive attitudes, and lower converted scores reflect more negative attitudes. Numeric ratings that have not been inverted are highlighted in pink. Component scores are shown in green, subscores in red, and Overall Stuttering Scores in a brighter red. Text values are listed in the form that individual research partners wrote them. Most are in English, but some have not been translated. If users of the database wish to translate non-English text, at the far right for each respondent, the language of the POSHA–S is listed. Also provided for each respondent are the country, continent or region, population sampling group, and, in some cases, an additional description.
At the bottom of the Excel file, summary data for each of the 261 samples are provided. They are identified by country (and sometimes state or region) and population group as well as language of the POSHA–S. The individual respondents above are listed in random order to add another layer of anonymity protection. Accordingly, whereas the mean sample values are provided, identifying the individuals making up those samples would be virtually impossible.
When respondents—or sometime investigators—omitted an item, it is shown by a period. The 1-5 ratings were followed by an “I don’t know” choice. When those were circles or otherwise selected electronically, a “u” is entered in the database.
Importantly, despite great care in correcting them, there are no doubt errors in the Database. For example, a non-recognized number has been entered by researchers who entered their data in an Excel workbook or a space was added before or after a number resulting it not being counted. Early analysis of a much more difficult rating and scoring system yielded considerable errors, but those made virtually no difference in means after they had either been corrected or deleted [17]. No doubt as well, occasional respondents did not respond with the care that was anticipated for a variety of reasons [18]. Nevertheless, consistency in numerous similar samples generating very similar results privides evidence that occasional errors have little if any effect on mean values.
At the end bottom of the Database, values for lowest, highest, and median of sample means are provided. In cases where investigators administered the POSHA–S two or more times, only the values for the first (pre-test) administration are considered. It can be noted that there have been 65 second (post-test) administrations that are not included in this database.
2.2. Data Conversions
The 1-5 ratings in the demographic and general sections are converted to the -100 to +100 scales by subtracting 3 from the rating and multiplying the difference by 50. The “u” or blank cells are not included in the calculations. For the 1-3 ratings in the detailed stuttering section, the -100 to +100 conversion involves subtracting 2 from rating and multiplying the difference by 100. Only two other weighted scores are calculated differently. As noted earlier, for the identification of “people I have known who...” general item for the five attributes, each item checked is recorded with a “1” in the Excel worksheet. A preliminary rating from 0 to 100 units is generated as the sum of Me = 60, Close Friend = 20, Relative = 10, Acquaintance = 5, Other = 5, and Nobody = 0. This value is then converted to -100 to +100 by subtracting 50 and then multiplying by 2. This personal experience score for stuttering (me, friends, family, others), is included in the Knowledge component of the Self Reactions subscore.
Converted means are shown for 1-5 ratings of respondents’ income compared to their family and friends and compared to all the people in their country. However, the Relative Income score is calculated only when both the 1-5 ratings for both comparisons have been filled in. They are converted to a -100 to +100 scale according to the formula, ((((B x 5)+A)-5)-13) x 100/12. The country value is weighted much more heavily than the family/friend value as shown in Table 2.
2.3. Using the POSHA–S Database
Comparisons of any given sample to the Database’s highest, lowest, and median sample means at the time of the research were reported in the large majority of POSHA–S published and unpublished studies [14]. In nearly all of these studies, this paper’s author sent an Excel workbook to the investigators in which to enter their POSHA–S data. Once sent back to him for entry into the Database, he then generated graphs (as shown in Figure 1, Figure 2, Figure 3 and Figure 4), descriptive statistics (i.e., means and standard deviations) of their samples; and percentile comparisons of all items, components, subscores, and Overall Stuttering Score relative to the extant samples in the Database. After data entry, the most recent version, the Data Entry & Graphs Excel workbook [22,23], generates graphs, descriptive statistics, and percentiles automatically.
Research has also utilized selected data from the POSHA–S Database itself. Sorting it by country and by professions, studies by Arnold, Li, and others compared stuttering attitudes of teachers versus nonteachers [24,25] and police or other protection workers versus controls [26]. They also explored the relationship between Beliefs and Self Reactions [27]. Hughes et al. selected males and females who were parents or not in various countries and showed that Middle Eastern fathers had more positive attitudes than mothers whereas the opposite was true of North American and European mothers and fathers [28]. St. Louis explored the extent to which the various general ratings for overall impression, want to be/have, amount known, and persons known for all five of the attributes (stuttering, obesity, mental illness, left handedness, and intelligence) could predict Overall Stuttering Scores [29]. St. Louis also analyzed the Database to identify and rank the predictive power of 34 different POSHA–S variables, showing that subscores for Beliefs and Self Reactions were best predicted by different combinations of variables [4]. A study of English and French speakers from Canada and Cameroon were compared to a control group of monolingual English speakers in the US selected from the Database [30]. Although pre- versus post-test samples are not available in the POSHA–S database reported herein, data from 41 different intervention and non-intervention pre versus post studies have shown that respondents’ attitudes toward stuttering are less stable than previously assumed [31,32,33].
As explained, the respondents from all the samples in the Database are listed in random order to render it virtually impossible to reconstruct individual samples. Therefore, in order to identify selected groups, the Database must be sorted according to various criteria. This can be done in most statistical programs, such as SPSS, but it can also be done in Excel. For example, Hughes et al. [28] first made a copy of the listed respondents. Second, they utilized the Sort function in Excel to first sort the data by region. Third, they deleted all the rows that were not either Middle East, Western Europe, Eastern Europe, and North America. Fourth, they created two files, one for the Middle East and another for Europe and North America. Fifth, they sorted each of the two files with the first variable of sex (male versus female) and the second variable of parent (yes versus no). This yielded all the respondents who were male and female parents as well as male and female nonparents. Sixth, the Overall Stuttering Scores for each of these four groups in the two different files were analyzed with descriptive and inferential statistics.
In similar manner, the POSHA–S Database can be sorted to answer an indefinite number of research questions. For example, a simple study might be to determine the percentage of left handedness in self-identified stutterers versus nonstuttering respondents who identified a relative who stutters versus nonstutterers who know nobody who stutters.
A more complicated but time-consuming study might involve socieoeconomic class (SES). Most previous studies of SES have considered relative income and years of education [34]. A researcher may wish to explore the effect of SES as a predictor of stuttering attitudes more systematically by including occupation. It might follow the model of an unpublished study when the database contained only 3751 respondents from 56 samples [35]. In that study, the text answers to “The job that I am best trained to do, or the job I worked at the longest, is (was):“ were categorized according to Hauser and Warren’s “Total Socioeconomic Index” (TSEI) [36]. Differences in TSEI were then used to determine differential effects on Overall Stuttering Scores. A comprehensive study of the influence of SES on stuttering attitudes might well involve developing a formula for combining relative income, education, and a measure of vocational status (e.g., TSEI) and its effect on stuttering attitudes in various regions of the world.
3. Methods
3.1. POSHA–S Psychometric and Practical Characteristics
After pilot studies using the first experimental prototype (POSHA–E1), the author and his student research assistants as well as international partners carried out experiments with the POSHA–E2 and, soon after, the POSHA–S. These studies have documented satisfactory psychometric and other characteristics of the instrument, namely, test retest reliability [18,32,37,38], construct and concurrent validity [39], and internal consistency [18,40]. Investigations also established comparable results from the POSHA–S versus the POSHA–E2 [18], translatability [30], important considerations in sampling strategies [41], and paper-and-pencil versus electronic survey methods [42].
3.2. Obtaining Data from IPATHA Partners
For more than 20 years, interested researchers have contacted the author about using the instrument to measure attitudes of the public or various subgroups of populations of interest to them (e.g., university students, teachers, or parents) in their countries or regions. At the outset, a decision was made that the instrument would be made available to researchers at no cost, provided three conditions were agreed upon beforehand: (a) all appropriate protections for human subject research must precede the data sampling, (b) an anonymous copy of the researchers’ raw data would be entered into a POSHA–S Excel workbook provided by the author would be filled out and a copy sent to the author to include the results in a growing database, and (c) presentations or publications of the research would acknowledge that the instrument was used by permission. Importantly, continue up to the present time, and the same requirement for free use in exchange for adding raw data to the database have been consistently applied. This means that the database is not static; it is updated about every year. The version herein described was updated in August, 2025.
3.3. Alternate Access to the Database and Related Materials
In addition to the current version in Table S1, the POSHA–S Database is also available from the www.teacherspayteachers.com (TPT) website for a fee at https://www.teacherspayteachers.com/Product/POSHAS-Database-11631862. Future versions with additional data from more countries will be made available at this website. As more data are acquired, the Database will be updated periodically; however, given its large size, mean values for the various scores are likely to change minimally. The TPT POSHA–S Database file also contains the limited databases for the two experimental versions, the POSHA-E1 and POSHA–E2. The author has made available for download numerous related files at TPT, including the POSHA–S in English [43] and 29 other languages, a child version (POSHA–S/Child) [44], and a POSHA for another fluency disorder known as cluttering (POSHA–Cl) [45]. Further, the Appraisal of the Stuttering Environment (ASE), which is an adaptation of the POSHA–E2 using a 1-9 scale, was developed for clinical use by speech-language pathologists rather than epidemiological investigations [46]. Extant translations and databases for these instruments are also available for download.
The POSHA has also been adapted for obesity (POSHA–Ob) and for mental illness (POSHA-MI). A recent study using three different POSHAs showed that public attitudes were the most negative for mental illness, less negative for stuttering, and least negative for obesity [29].
The Data Entry & Graphs Excel workbook for the POSHA–S is available in two versions for a fee from TPT. One version analyzes data for one sample [22]; the other analyzes and compares data for two samples [23]. Additionally, at no cost, users can download the following documents from TPT: Excel Workbook Data Entry & Analysis Assistance [47], Formula Explanations for POSHA Instruments and the ASE [48] and IPATHA Bibliography [49]. An IPATHA Instruments User’s Guide [50] is also available for a fee.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: POSHA–S Database.
Author Contributions
Conceptualization, St. Louis; methodology, St. Louis; software, St. Louis; validation, St. Louis; formal analysis, St. Louis.; investigation, St. Louis and IPATHA partners; resources, St. Louis and IPATHA partners; data curation, St. Louis.; writing—original draft preparation, St. Louis; writing—review and editing, St Louis.; visualization, St Louis.; supervision, St. Louis; project administration, St. Louis.; funding acquisition, NA. The author has read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The studies involved in this Database were conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of West Virginia University (protocol number 1801918277 approved January 10, 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is contained within the supplementary material. The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Acknowledgments
Cooperation of all the IPATHA partners is greatly appreciated.
Conflicts of Interest
The author declares no conflicts of interest except (a) owning the copyright of the POSHA–S and (b), since making it available for a fee from the TPT website, in 2022, receiving less than $1000 US in royalties.
References
- Frigerio-Domingues, C.; Drayna, D. Genetic contributions to stuttering: the current evidence. Molecular Genetics & Genomic Medicine 2017, 5, 95–102. [Google Scholar] [CrossRef]
- Manning, W.H.; DiLollo, A. Clinical Decision Making in Fluency Disorders. 5th ed. Plural Publishing, San Diego, CA, USA 2025.
- Johnson, W. ; Associates. The Onset of Stuttering: Research Finding and Implications; University of Minnesota Press, Minneapolis, MN, USA, 1959.
- St. Louis K.O. Predicting attitudes toward stuttering from an international database. J Commun Disord. 2024, 112, 106457. [Google Scholar] [CrossRef]
- Beilby, J.M.; Byrnes, M.; Meagher, E.L.; Yaruss, J.S. The impact of stuttering on adults who stutter and their partners. Jl Fluen Disord, 38, 2013), 14-29. [CrossRef]
- Irani, F.; Abdalla, F.; Gabel, R. Arab and American teachers’ attitudes toward people who stutter: A comparative study. Contemp Issues Commun Sci Disord 2012, 39, 12–20. [Google Scholar] [CrossRef]
- Flynn, T.W.; St. Louis K.O. Changing adolescent attitudes toward stuttering. J Fluen Disord 2011, 36, 110–121. [Google Scholar] [CrossRef]
- Yairi, E.; Williams, D.E. Speech clinician’s stereotypes of elementary-school boys who stutter. J Commun Disord 1970, 3, 161–70. [Google Scholar] [CrossRef]
- Weidner, M.E. ; St. Louis K.O.; Nakışcı E.; Özdemir S. A comparison of attitudes towards stuttering of non-stuttering preschoolers in the United States and Turkey. S Af J Commun Disord 2017, 64, 1–11. [Google Scholar] [CrossRef]
- Lee, K. Korean speech–language pathologists’ attitudes toward stuttering according to clinical experiences. Int J Lang Commun Disord 2014, 49, 771–779. [Google Scholar] [CrossRef]
- Boyle, M. P. , Cheyne, M. R., & Rosen, A. L. Self-stigma of stuttering: Implications for communicative participation and mental health. Journal of Speech, Language, and Hearing Research 2023, 66, 3328–3345. [Google Scholar] [CrossRef]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Penguin Random House, Englewood Cliffs, NJ, USA 1963.
- Woods, C.L.; Williams, D.E. Traits attributed to stuttering and normally fluent males. J Sp Hear Res 1976, 19, 267–278. [Google Scholar] [CrossRef]
- St. Louis K.O. Epidemiology of public attitudes toward stuttering. In Stuttering meets stereotype, stigma, and discrimination: An overview of attitude research; Editor St. Louis K.O.; West Virginia University Press, Morgantown, WV, USA 2015. pp. 7–42.
- Bohner, G.; Dickel, N. Attitudes and attitude change. Annual Review Psychol 2011, 62, 391–417. [Google Scholar] [CrossRef]
- St. Louis, K. O. The Public Opinion Survey of Human Attributes-Stuttering (POSHA–S): Summary framework and empirical comparisons. J Fluen Disord 2011, 36, 256–261. [Google Scholar] [CrossRef]
- St. Louis, K.O.; Lubker, B.B.; Yaruss, J.S.; Adkins, T.A.; Pill, J. C. St. Louis, K.O.; Lubker B.B.; Yaruss J.S.; Adkins, T.A.; Pill, J. C. Development of a prototype questionnaire to survey public attitudes toward stuttering: Principles and methodologies in the first prototype. Internet J of Epidemiol 2007, 5. [Google Scholar]
- St. Louis K.O. Research and development on a public attitude instrument for stuttering. J Commun Disord 2012, 45, 129–146. [Google Scholar] [CrossRef] [PubMed]
- St. Louis K.O.; Andrade C.R.F.; Georgieva D.; Troudt F.O. Experience and personal report about an international cooperation research—Brazil, Bulgaria and Turkey—Attitudes toward stuttering. Pró-Fono Revista de Atualização Cientifica 2005, 17, 413–416. [Google Scholar]
- St. Louis K.O. POSHA–S Database; Populore, Morgantown, WV, USA 2024. Available from https://www.teacherspayteachers.com/Product/POSHAS-Database-11631862.
- St. Louis, K. O. St. Louis, K. O., Irani, F., Gabel, R. M., Hughes, S., Langevin, M., Rodriguez, M., Scott, K. S., & Weidner, M. E. (2017). Evidence-based guidelines for being supportive of people who stutter in North America. Journal of Fluency Disorders, /: https. [CrossRef]
- St. Louis K.O. Data Entry & Graphs for One Group or Sample; Populore, Morgantown, WV, USA 2024. Available from https://www.teacherspayteachers.com/Product/POSHAS-Data-Entry-Graphs-for-One-Group-or-Sample-7759598.
- St. Louis K.O. Data Entry & Graphs for Two Groups or Samples; Populore, Available from https://www.teacherspayteachers.com/Product/POSHAS-Data-Entry-Graphs-for-One-Group-or-Sample-7759598Morgantown, WV, USA 2024.
- Arnold, H.S.; Li, J.; Goltl, K. Beliefs of teachers versus non-teachers toward people who stutter. J Fluen Disord 2015, 43, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Arnold, H. Reactions of teachers versus non-teachers toward people who stutter. J Commun Disord 2015. 56, 8–18. [CrossRef]
- Arnold, H.S.; Li, J.; Beste-Guldborg, A. Reactions of protective services workers towards people who stutter. J Fluen Disord 2016, 50, 1–12. [Google Scholar] [CrossRef]
- Arnold, H.S.; Li, J. Association between beliefs about and reactions toward people who stutter. J Fluen Disord 2016, 47, 27–37. [Google Scholar] [CrossRef]
- Hughes S,; Junuzović-Žunić L. ; Mostafa E.; Weidner M, Özdemir R.S.; Daniels D, Glover H.L.; Göksu A.; Konrot A.; & St. Louis K.O. Mothers’ and fathers’ attitudes toward stuttering in the Middle East compared to Europe and North America. Int J Lang Commun Disord 2024, 59, 354–68. [Google Scholar] [CrossRef]
- St. Louis K.O. Comparing and predicting public attitudes toward stuttering, obesity, and mental illness. Amer J Sp-Lang Pathol 2020, 29, 2023–2038. [Google Scholar] [CrossRef]
- St. Louis K.O.; Roberts P.M. Measuring attitudes toward stuttering: English-to-French translations in Canada and Cameroon. J Commun Disord 2010, 43, 361–377. [Google Scholar] [CrossRef]
- St. Louis K.O.; Węsierska K.; Przepiórka A.; Błachnio A.; Beucher C.; Abdalla F.; Flynn T.; Reichel I.; Beste-Guldborg A.; Junuzović-Žunić L.; Gottwald S.; Hartley J.; Eisert S.; Johnson K.; Bolton B.; Teimouri Sangani M.; Rezai H.; Abdi S.; Pushpavathi M.; Hudock D.; Spears S.; Aliveto E. Success in changing stuttering attitudes: A retrospective study of 29 intervention samples. J Commun Disord 2020, 84, 105972. [Google Scholar] [CrossRef]
- St. Louis,K.O.; Aliveto E.F.; Teimouri Sangan, M.; Abdi S.; Rezai H.; Abdalla F.; Przepiórka A.; Błachnio A.; Węsiersk; K., Junuzović-Žunić L.; Eisert S.; Roche C.K.; Reichel I.; Beste-Guldborg A.; Flynn T.; Bolton B.; Gottwald S.; Spears S.; Hudock D.; Hartley J.; Pushpavathi M.; Johnson K.N. Measuring public attitudes toward stuttering: Test-retest reliability revisited. Clinical Archives of Communication Disorders 2024, 9, 93–104. [Google Scholar] [CrossRef]
- St. Louis K.O.; Abdalla F.; Abdi S.; Aliveto E.; Beste-Guldborg A.; Błachnio A.; Bolton-Grant B.; Eisert S.; Flynn T.; Gottwald S.; Hartley J.; Hudock D.; Johnson K.N.; Junuzović-Žunić, L., Przepiórka, L., Pushpavathi, M., Reichel, I., Rezai, H., Roche, C., Spears S.; Teimouri Sangani M.; Węsierska K. Profiles of public attitude change regarding stuttering. Language and Health 2024, 2, 1–18. [Google Scholar] [CrossRef]
- Valente, A.R.S.; St. Louis, K.O.; Leahy M.; Hall A.; Jesus L. A country-wide probability sample of public attitudes toward stuttering in Portugal. J Fluen Disord 2017, 52, 37–52. [Google Scholar] [CrossRef]
- St. Louis K.O.; Rogers A.L. Predicting stuttering attitudes from socioeconomic indicators: Education, occupation, and income. Poster at the Annual Convention of the American Speech-Language-Hearing Association, San Diego, CA, USA (November, 2011. [Google Scholar]
- Hauser, R.M.; Warren, J.R. Socioeconomic indexes for occupations: A review, update, and critique. Sociological Methodol 1997, 27, 177–298. [Google Scholar] [CrossRef]
- St. Louis K.O.; Lubker B.B.; Yaruss J.S.; Aliveto E.F. Development of a prototype questionnaire to survey public attitudes toward stuttering: Reliability of the second prototype. Contemp Issues Commun Sci Disord 2009, 36, 101–107. [Google Scholar] [CrossRef]
- St. Louis K.O.; Williams M.J.; Ware M.B.; Guendouzi J.; Reichel I.K. The public opinion survey of human attributes-stuttering (POSHA-S) and bipolar adjective scale (BAS): aspects of validity. Journal of Communication Disorders 2014, 50, 36–50. [Google Scholar] [CrossRef]
- St. Louis K.O.; Reichel I.; Yaruss J.S.; Lubker B.B. Construct and concurrent validity of a prototype questionnaire to survey public attitudes toward stuttering. J Fluen Disord 2009, 34, 11–28. [Google Scholar] [CrossRef]
- Al-Khaledi, M.; Lincoln, M.; McCabe, P.; Packman, A.; Alshatti, T. The attitudes, knowledge and beliefs of Arab parents in Kuwait about stuttering. J Fluen Disord 2009, 34, 44–59. [Google Scholar] [CrossRef]
- Özdemir, R.S.; St. Louis K.O.; Topbaş S. Public attitudes toward stuttering in Turkey: Probability versus convenience sampling. Journal of Fluency Disorders 2011, 36, 262–267. [Google Scholar] [CrossRef] [PubMed]
- St. Louis K.O. POSHA–S public attitudes toward stuttering: Online versus paper surveys. Canad J Speech-Lang Pathol Audiol 2012, 36, 116–123. [Google Scholar]
- St. Louis K.O. Public Opinion Survey of Human Attributes–Stuttering (POSHA–S) in English. Populore. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/POSHAS-in-English-for-Stuttering-7759542.
- Weidner, M.E. ; St. Louis K.O. Public Opinion Survey of Human Attributes–Stuttering/Child (POSHA–S/Child) in English. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/POSHASChild-in-English-for-Stuttering-7821535.
- St. Louis K.O. Public Opinion Survey of Human Attributes–Cluttering (POSHA–Cl) in English. Populore. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/POSHACl-in-English-for-Cluttering-7784844.
- St. Louis, K.O. St. Louis, K.O. Appraisal of the Stuttering Environment (ASE) in English. Populore. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/ASE-Appraisal-of-the-Stuttering-Environment-in-English-7759680.
- St. Louis, K.O. St. Louis, K.O. Excel Workbook Data Entry & Analysis Assistance. Populore. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/Excel-Workbook-Data-Entry-Analysis-Assistance-7846685.
- St. Louis, K.O. St. Louis, K.O. Formula Explanations for POSHA Instruments and the ASE. Populore. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/Formula-Explanations-for-POSHA-Instruments-the-ASE-7763337.
- St. Louis, K.O. St. Louis, K.O. IPATHA Bibliography. Populore. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/IPATHA-Bibliography-9016470.
- St. Louis, K.O. St. Louis, K.O. IPATHA Instruments User’s Guide. Populore. Morgantown, WV, USA 2022. Available at https://www.teacherspayteachers.com/Product/IPATHA-Instrument-Users-Guide-7935995.
Figure 1.
Radial graph showing the lowest sample mean value, the highest sample mean value, the median of all sample mean values, and the Overall Stuttering Scores for 261 samples utilizing the POSHA–S.
Figure 1.
Radial graph showing the lowest sample mean value, the highest sample mean value, the median of all sample mean values, and the Overall Stuttering Scores for 261 samples utilizing the POSHA–S.
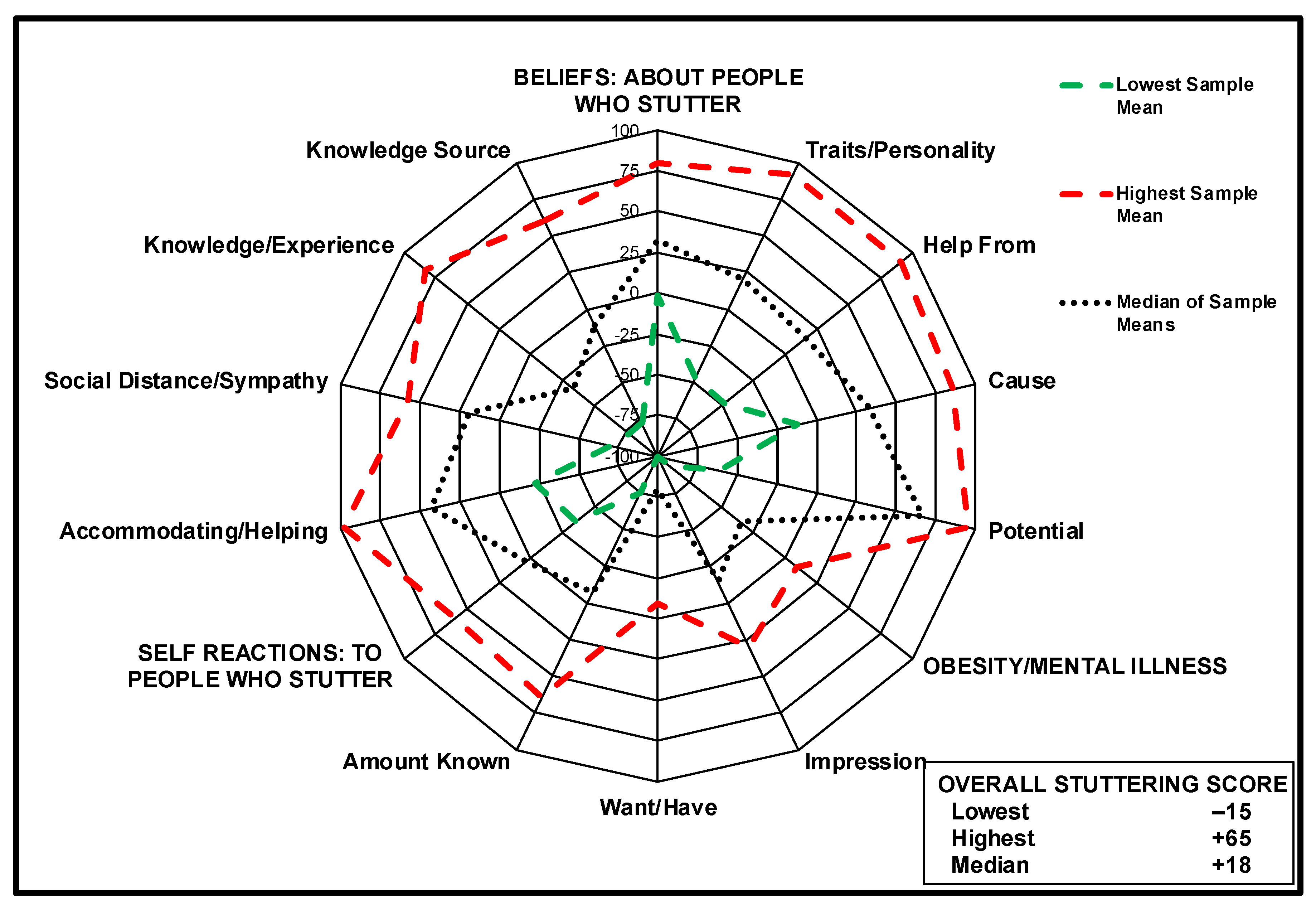
Figure 2.
Graph showing the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for all items in the Beliefs subscore for 261 samples utilizing the POSHA–S.
Figure 2.
Graph showing the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for all items in the Beliefs subscore for 261 samples utilizing the POSHA–S.
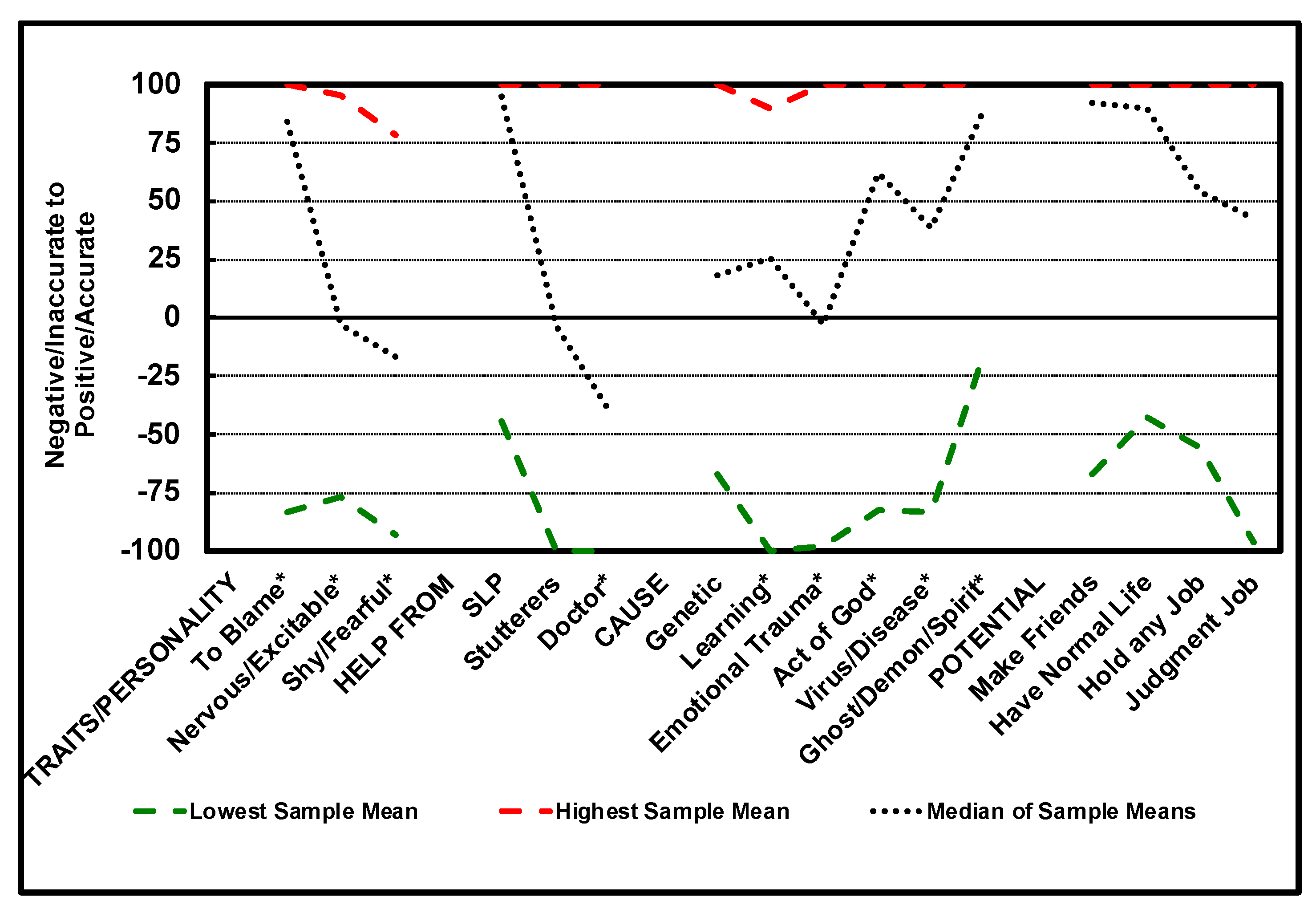
Figure 3.
Graph showing the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for all items in the Self Reactions subscore for 261 samples utilizing the POSHA–S.
Figure 3.
Graph showing the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for all items in the Self Reactions subscore for 261 samples utilizing the POSHA–S.
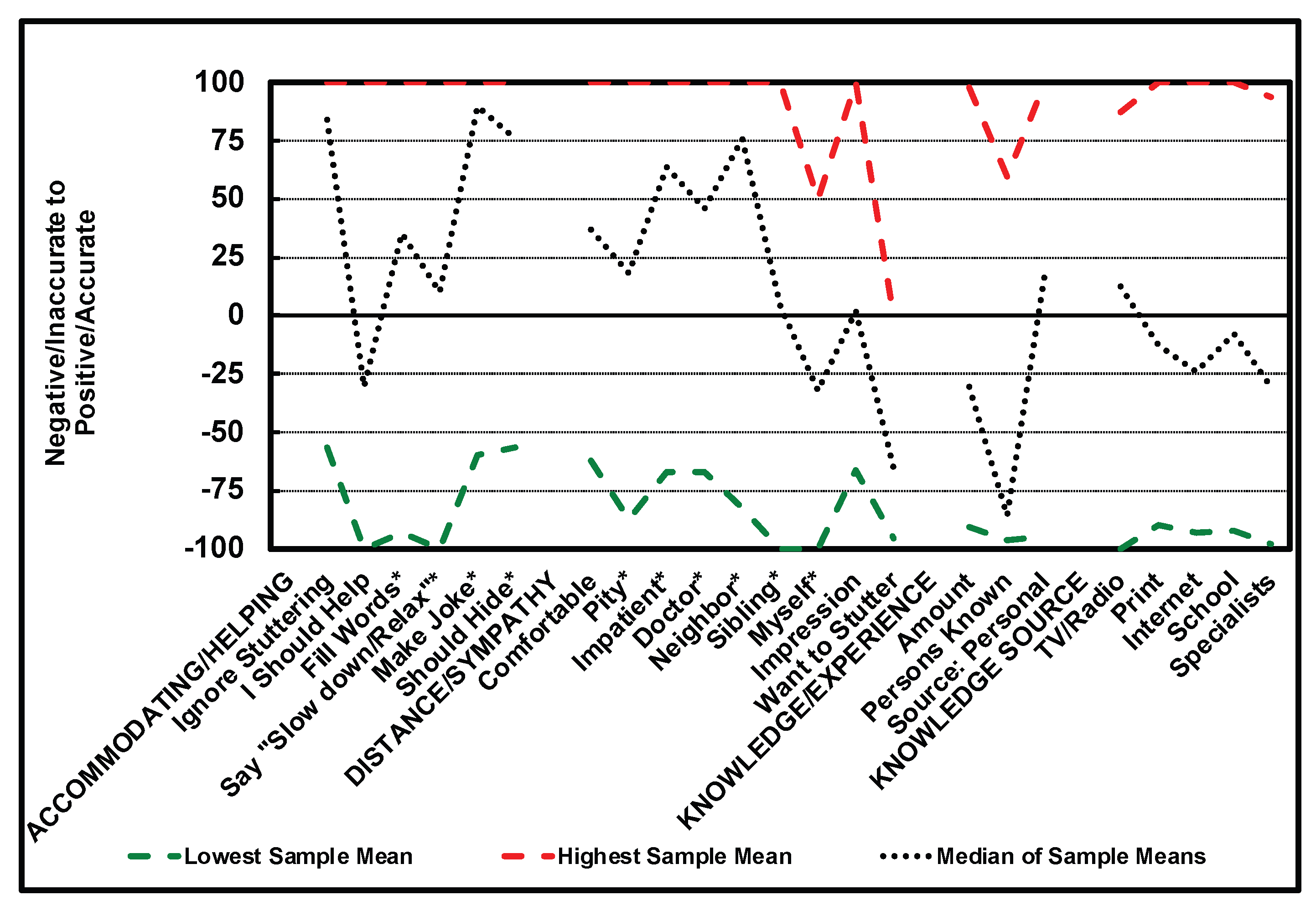
Figure 4.
Graph showing the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for overall impression, want to have or be, and amount known about five human attributes for 261 samples utilizing the POSHA–S.
Figure 4.
Graph showing the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for overall impression, want to have or be, and amount known about five human attributes for 261 samples utilizing the POSHA–S.


Table 1.
POSHA–S summary scores for the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for 261 samples.
Table 1.
POSHA–S summary scores for the lowest sample mean value, the highest sample mean value, and the median of all sample mean values for 261 samples.
| POSHA–S Summary Scores | Lowest Sample Mean | Highest Sample Mean | Median of Sample Means | All Respondents: Mean | All Respondents: Standard Deviation |
| Overall Stuttering Score | -15 | +65 | +18 | +17 | 21 |
| Beliefs | -1 | +80 | +33 | +32 | 26 |
| Traits/Personality | -47 | +91 | +21 | +14 | 55 |
| Help From | -48 | +91 | +16 | +19 | 42 |
| Cause | -12 | +86 | +33 | +31 | 38 |
| Potential | -61 | +96 | +67 | +63 | 40 |
| Self Reactions | -36 | +60 | +3 | +3 | 26 |
| Accommodating/Helping | -22 | +98 | +44 | +41 | 36 |
| Social Distance/Sympathy | -71 | +57 | +19 | +9 | 42 |
| Knowledge/Experience | -77 | +83 | -34 | -33 | 44 |
| Knowledge Source | -76 | +60 | -11 | -5 | 60 |
| Obesity/Mental Illness | -90 | +2 | -35 | -31 | 29 |
| Impression | -100 | +26 | -15 | -10 | 44 |
| Want/Have | -100 | -10 | -79 | -77 | 37 |
| Amount Known | -75 | +53 | -9 | -5 | 46 |
Table 2.
Relative income conversions.
|
Countrymen Rating |
Family /Friends Rating |
Relative Income Score |
|||||||||||
| 1 | x 5 = | 5 | + | 1 | = | 6 | -5 = | 1 | -13 = | -12 | x (100/12) = | -100.00 | |
| 1 | x 5 = | 5 | + | 2 | = | 7 | -5 = | 2 | -13 = | -11 | x (100/12) = | -91.67 | |
| Lowest | 1 | x 5 = | 5 | + | 3 | = | 8 | -5 = | 3 | -13 = | -10 | x (100/12) = | -83.33 |
| 5th | 1 | x 5 = | 5 | + | 4 | = | 9 | -5 = | 4 | -13 = | -9 | x (100/12) = | -75.00 |
| 1 | x 5 = | 5 | + | 5 | = | 10 | -5 = | 5 | -13 = | -8 | x (100/12) = | -66.67 | |
| 2 | x 5 = | 10 | + | 1 | = | 11 | -5 = | 6 | -13 = | -7 | x (100/12) = | -58.33 | |
| 2 | x 5 = | 10 | + | 2 | = | 12 | -5 = | 7 | -13 = | -6 | x (100/12) = | -50.00 | |
| 2 | x 5 = | 10 | + | 3 | = | 13 | -5 = | 8 | -13 = | -5 | x (100/12) = | -41.67 | |
| 2 | x 5 = | 10 | + | 4 | = | 14 | -5 = | 9 | -13 = | -4 | x (100/12) = | -33.33 | |
| 2 | x 5 = | 10 | + | 5 | = | 15 | -5 = | 10 | -13 = | -3 | x (100/12) = | -25.00 | |
| 3 | x 5 = | 15 | + | 1 | = | 16 | -5 = | 11 | -13 = | -2 | x (100/12) = | -16.67 | |
| 3 | x 5 = | 15 | + | 2 | = | 17 | -5 = | 12 | -13 = | -1 | x (100/12) = | -8.33 | |
| Middle | 3 | x 5 = | 15 | + | 3 | = | 18 | -5 = | 13 | -13 = | 0 | x (100/12) = | 0.00 |
| 5th | 3 | x 5 = | 15 | + | 4 | = | 19 | -5 = | 14 | -13 = | 1 | x (100/12) = | +8.33 |
| 3 | x 5 = | 15 | + | 5 | = | 20 | -5 = | 15 | -13 = | 2 | x (100/12) = | +16.67 | |
| 4 | x 5 = | 20 | + | 1 | = | 21 | -5 = | 16 | -13 = | 3 | x (100/12) = | +25.00 | |
| 4 | x 5 = | 20 | + | 2 | = | 22 | -5 = | 17 | -13 = | 4 | x (100/12) = | +33.33 | |
| 4 | x 5 = | 20 | + | 3 | = | 23 | -5 = | 18 | -13 = | 5 | x (100/12) = | +41.67 | |
| 4 | x 5 = | 20 | + | 4 | = | 24 | -5 = | 19 | -13 = | 6 | x (100/12) = | +50.00 | |
| 4 | x 5 = | 20 | + | 5 | = | 25 | -5 = | 20 | -13 = | 7 | x (100/12) = | +58.33 | |
| 5 | x 5 = | 25 | + | 1 | = | 26 | -5 = | 21 | -13 = | 8 | x (100/12) = | +66.67 | |
| 5 | x 5 = | 25 | + | 2 | = | 27 | -5 = | 22 | -13 = | 9 | x (100/12) = | +75.00 | |
| Highest | 5 | x 5 = | 25 | + | 3 | = | 28 | -5 = | 23 | -13 = | 10 | x (100/12) = | +83.33 |
| 5th | 5 | x 5 = | 25 | + | 4 | = | 29 | -5 = | 24 | -13 = | 11 | x (100/12) = | +91.67 |
| 5 | x 5 = | 25 | + | 5 | = | 30 | -5 = | 25 | -13 = | 12 | x (100/12) = | +100.00 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



