Submitted:
12 August 2025
Posted:
15 August 2025
You are already at the latest version
Abstract
Background/Objectives: Identifying the optimal positive end-expiratory pressure (PEEP) is a major challenge in implementing strategies to prevent ventilator-induced lung injury in newborns. In this study, we assessed the validity of volumetric capnography based on the neonatal patient monitor (Vcap,PM) technique and investigated the impact of PEEP on newborns. Methods: Analysis 1 evaluated the validity of Vcap,PM technique with data from pediatric patients receiving invasive respiratory support. Linear regression and Bland–Altman analyses were performed on Vcap,PM and HAMILTON-C1 data. Analysis 2 evaluated the impact of PEEP on newborns. The PEEP level was increased from mild to high (the incremental phase) and then decreased from high to mild (the decremental phase) while performing the Vcap,PM technique on term and preterm infants. Results: Analysis 1 included 31 children (age, 9 [interquartile range (IQR), 0–36] months; weight, 6.0 [IQR, 3.8–10.5] kg). Regression and Bland–Altman analyses demonstrated the accuracy of Vcap,PM. Analysis 2 included 28 term (mean gestational age, 38 [IQR, 38–40] weeks; weight, 2,924 [IQR, 2,725–3,109] g) and 21 preterm (mean gestational age, 33 [IQR, 31–34] weeks; weight, 1,918 [IQR, 1,356–2,186] g) newborns. Despite no difference in tidal volume, high PEEP significantly increased airway dead space and decreased alveolar tidal volume compared to mild PEEP in each phase in term and preterm neonates. Conclusions: High PEEP induced airway dilation in newborns, as determined using a novel Vcap technique. This technique, which requires no special equipment, has the potential for wider clinical application in neonatal care.
Keywords:
1. Introduction
2. Materials and Methods
2.1 Study Design
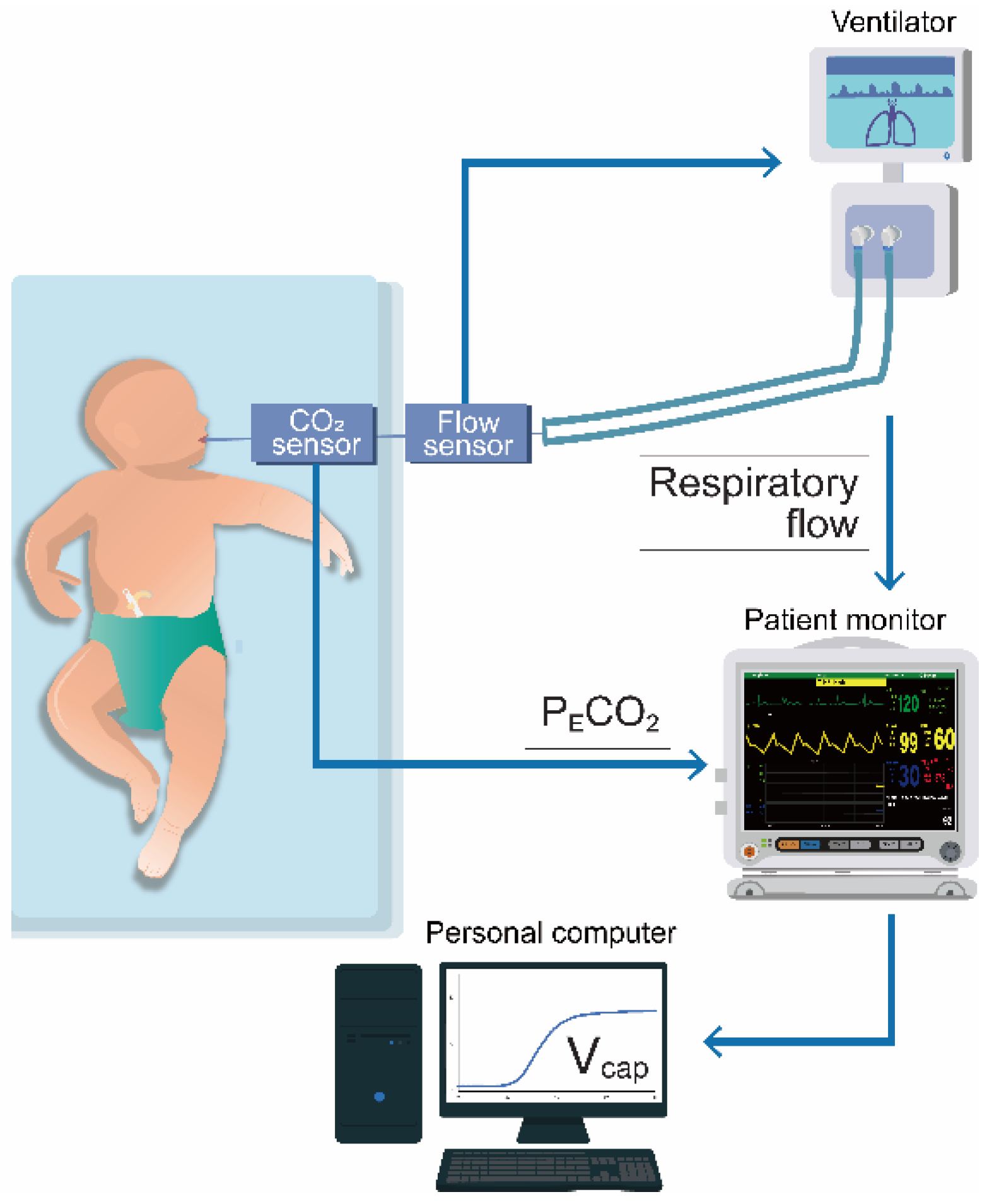
2.2 Methodology of Vcap,PM
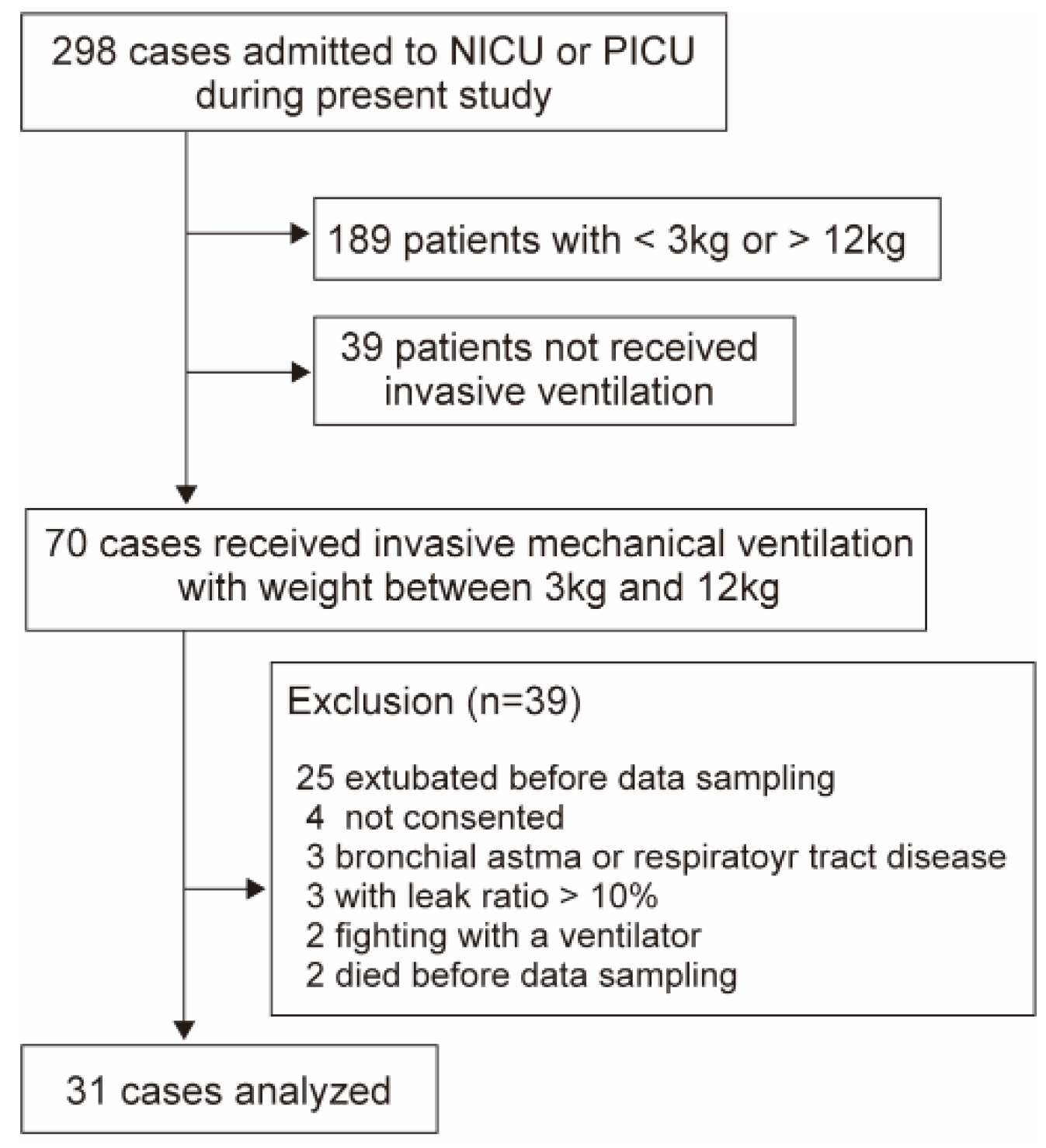
2.3 Examination for Validity of Vcap,PM (Analysis 1)
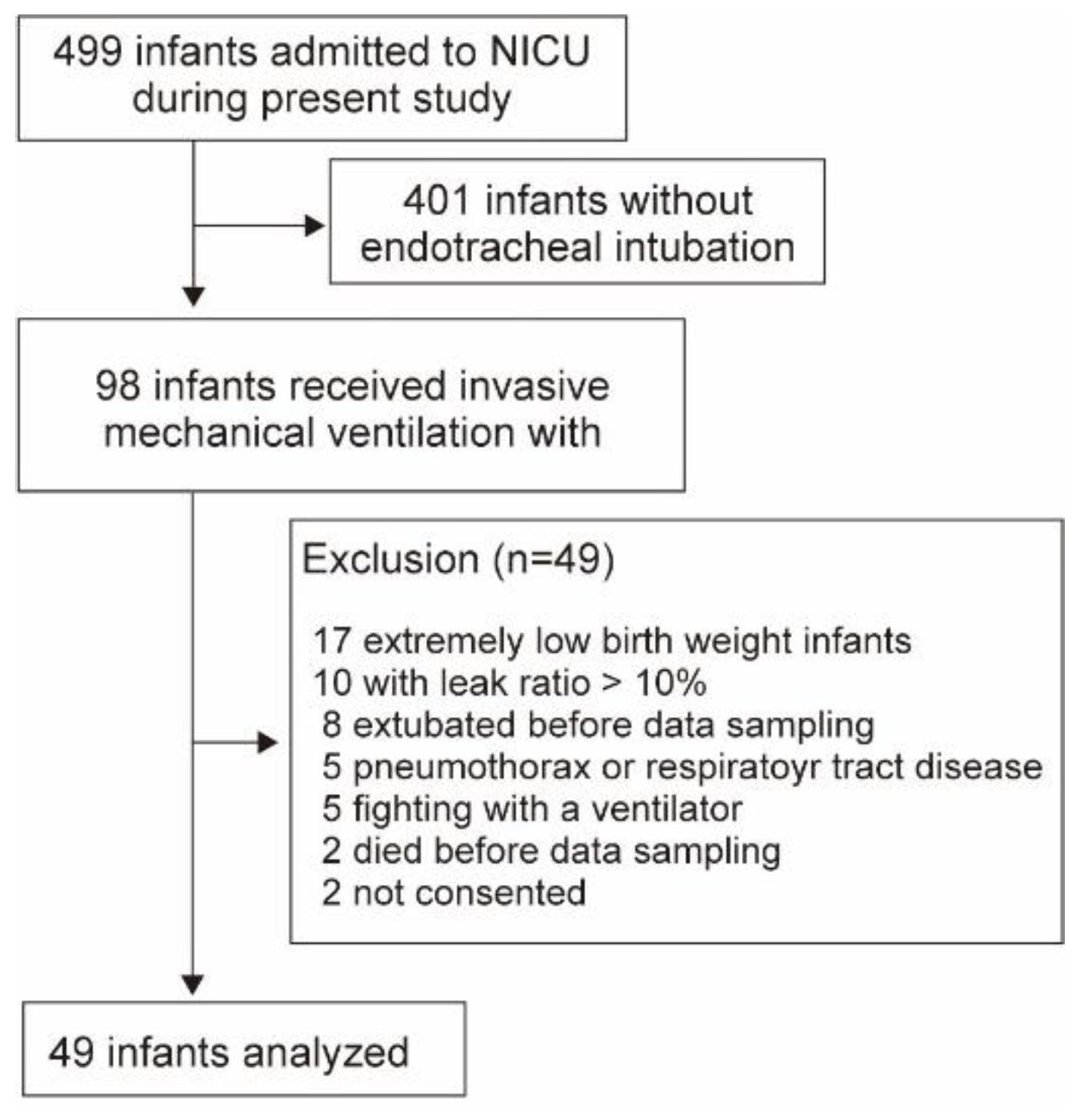
2.4 Impact of PEEP on Term and Preterm Newborns (Analysis 2)
2.5 Statistical Analyses
3. Results
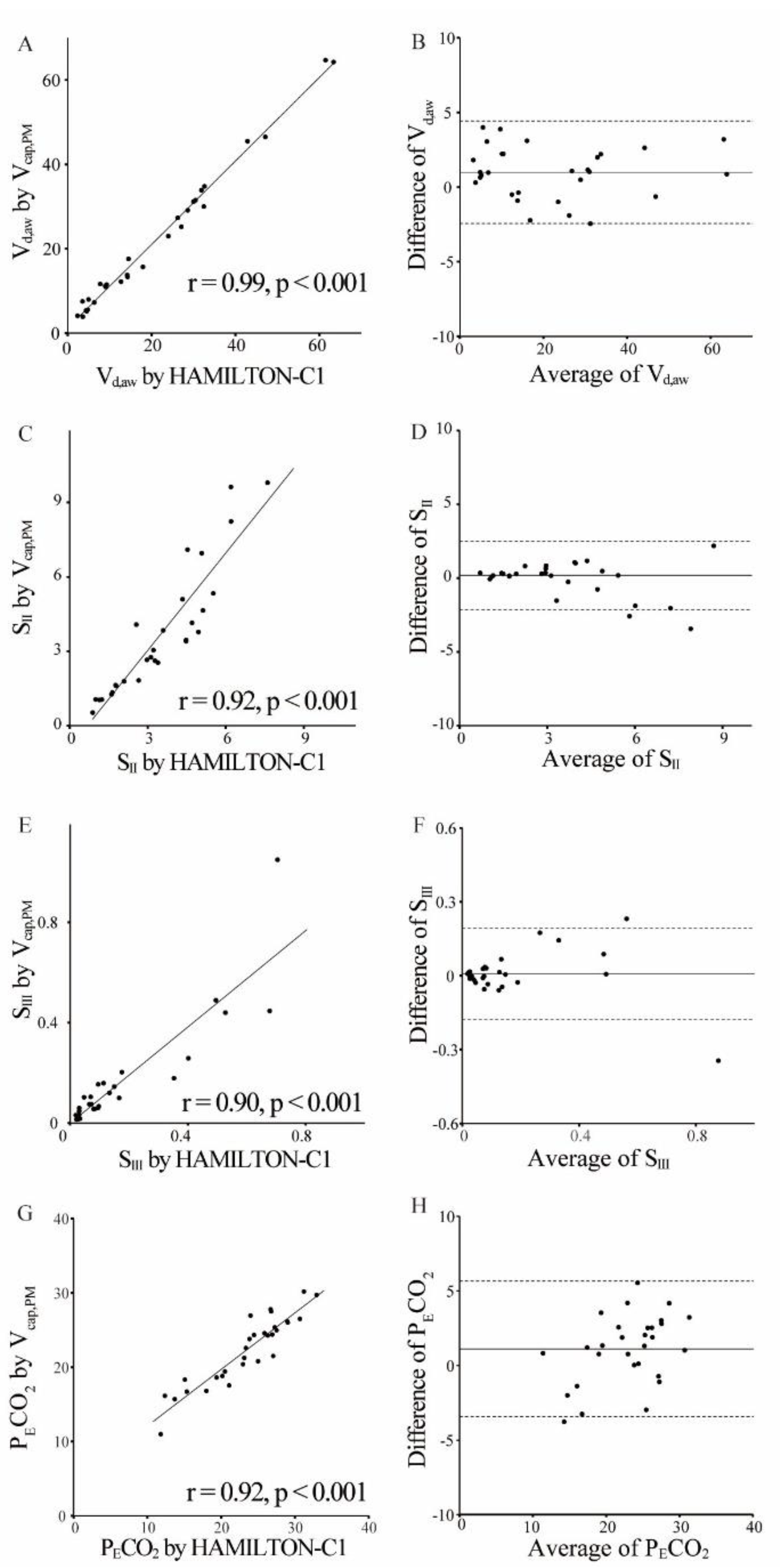
3.1 Analysis 1
3.2 Analysis 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CO2 | Carbon dioxide |
| IQR | Interquartile range |
| KPIV | Capnographic index |
| NICU | Neonatal intensive care unit |
| PECO2 | Partial pressure expiratory CO2 |
| PEEP | Positive end-expiratory pressure |
| PICU | Pediatric ICU |
| SII | Capnographic slope of phase II |
| SIII | Capnographic slope of phase III |
| VILI | Ventilator-induced lung injury |
| Vcap | Volumetric capnography |
| Vcap,PM | Vcap based on the patient monitor |
| Vd,alv | Alveolar dead space |
| Vd,aw | Airway dead space volume |
| Vd,app | Apparatus dead space volume |
| Vd,Fowler | Fowler dead space volume |
| VT | tidal volume |
| VT,E | Expired tidal volume |
References
- Thekkeveedu, R.K.; El-Saie, A.; Prakash, V.; Katakam, L.; Shivanna, B. Ventilation-induced lung injury (VILI) in neonates: evidence-based concepts and lung-protective strategies. J. Clin. Med. 2022, 11, 557. [Google Scholar] [CrossRef]
- Keszler, M. Mechanical ventilation strategies. Semin. Fetal. Neonatal. Med. 2017, 22, 267–274. [Google Scholar] [CrossRef]
- Rouby, J.J.; Ferrari, F.; Bouhemad, B.; Lu, Q. Positive end-expiratory pressure in acute respiratory distress syndrome: should the ‘open lung strategy’ be replaced by a ‘protective lung strategy’? Crit. Care 2007, 11, 180. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L. New goals for positive end-expiratory pressure in acute respiratory distress syndrome: a paradigm shift or the end of an area of uncertainty? Am. J. Respir. Crit. Care Med. 2010, 181, 528–530. [Google Scholar] [CrossRef] [PubMed]
- Terragni, P.P.; Rosboch, G.; Tealdi, A.; Corno, E.; Menaldo, E.; Davini, O.; Gandini, G.; Herrmann, P.; Mascia, L.; Quintel, M.; Slutsky, A.S.; Gattinoni, L.; Ranieri, V.M. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2007, 175, 160–666. [Google Scholar] [CrossRef]
- Vieillard-Baron, A.; Price, L.C.; Matthay, M.A. Acute cor pulmonale in ARDS. Intensive Care Med. 2013, 39, 1836–1838. [Google Scholar] [CrossRef]
- Bamat, N.; Fierro, J.; Wang, Y.; Millar, D.; Kirpalani, H. Positive end-expiratory pressure for preterm infants requiring conventional mechanical ventilation for respiratory distress syndrome or bronchopulmonary dysplasia. Cochrane Database Syst. Rev. 2019, 2, CD004500. [Google Scholar] [CrossRef] [PubMed]
- Verscheure, S.; Massion, P.B.; Verschuren, F.; Damas, P.; Magder, S. Volumetric capnography: lessons from the past and current clinical applications. Crit. Care 2016, 20, 184. [Google Scholar] [CrossRef]
- Blankman, P.; Shono, A.; Hermans, B.J.; Wesselius, T.; Hasan, D.; Gommers, D. Detection of optimal PEEP for equal distribution of tidal volume by volumetric capnography and electrical impedance tomography during decreasing levels of PEEP in post cardiac-surgery patients. Br. J. Anaesth. 2016, 116, 862–869. [Google Scholar] [CrossRef]
- Tusman, G.; Gogniat, E.; Madorno, M.; Otero, P.; Dianti, J.; Ceballos, I.F.; Ceballos, M.; Verdier, N.; Böhm, S.H.; Rodriguez, P.O. Effect of PEEP on dead space in an Experimental model of ARDS. Respir. Care 2020, 65, 11–20. [Google Scholar] [CrossRef]
- Yang, Y.; Huang, Y.; Tang, R.; Chen, Q.; Hui, X.; Li, Y.; Yu, Q.; Zhao, H.; Qiu, H. Optimization of positive end-expiratory pressure by volumetric capnography variables in lavage-induced acute lung injury. Respiration 2014, 87, 75–83. [Google Scholar] [CrossRef]
- Schmalisch, G. Current methodological and technical limitations of time and volumetric capnography in newborns. Biomed. Eng. OnLine 2016, 15, 104. [Google Scholar] [CrossRef]
- Neumann, R.P.; Pillow, J.J.; Thamrin, C.; Larcombe, A.N.; Hall, G.L.; Schulzke, S.M. Influence of gestational age on dead space and alveolar ventilation in preterm infants ventilated with volume guarantee. Neonatology 2015, 107, 43–49. [Google Scholar] [CrossRef]
- Zuiki, M.; Yamano, A.; Kitamura, K.; Goda, T.; Oya, S.; Komatsu, H. Ventilated Infants Have Increased Dead Space and Lower alveolar Tidal Volumes during the Early versus Recovery Phase of Respiratory Distress. Neonatology 2020, 117, 189–192. [Google Scholar] [CrossRef]
- Zuiki, M.; Naito, Y.; Kitamura, K.; Tsurukawa, S.; Matsumura, U.; Kanayama, T.; Komatsu, H. Reduction in minute alveolar ventilation causes hypercapnia in ventilated neonates with respiratory distress. Eur. J. Pediatr. 2021, 180, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Zuiki, M.; Kume, R.; Matsuura, A.; Mitsuno, K.; Kitamura, K.; Kanayama, T.; Komatsu, H. Large difference between Enghoff and Bohr dead space in ventilated infants with hypoxemic respiratory failure. Pediatr. Pulmonol. 2021, 56, 2102–2107. [Google Scholar] [CrossRef] [PubMed]
- Fowler, W.S. Lung function studies; the respiratory dead space. Am. J. Physiol. 1948, 154, 405–416. [Google Scholar] [CrossRef]
- Strömberg, N.O.; Gustafsson, P.M. Ventilation inhomogeneity assessed by nitrogen washout and ventilation-perfusion mismatch by capnography in stable and induced airway obstruction. Pediatr. Pulmonol. 2000, 29, 94–102. [Google Scholar] [CrossRef]
- Dassios, T.; Dixon, P.; Hickey, A.; Fouzas, S.; Greenough, A. Physiological and anatomical dead space in mechanically ventilated newborn infants. Pediatr. Pulmonol. 2018, 53, 57–63. [Google Scholar] [CrossRef]
- Wenzel, U.; Wauer, R.R.; Schmalisch, G. Comparison of different methods for dead space measurements in ventilated newborns using CO2-volume plot. Intensive Care Med 1999: 25:705-13. [CrossRef]
- Mereness, J.A.; Mariani, T.J. The critical role of collagen VI in lung development and chronic lung disease. Matrix Biol. Plus 2021, 10, 100058. [Google Scholar] [CrossRef] [PubMed]
- Bush, D.; Juliano, C.; Bowler, S.; Tiozzo, C. Development and disorders of the airway in bronchopulmonary dysplasia. Children (Basel), 2023, 10, 1127. [Google Scholar] [CrossRef]
- Schittny, J.C. Development of the lung. Cell Tissue Res 2017: 367:427-44. [CrossRef]
- Krauss, B.; Deykin, A.; Lam, A.; Ryoo, J.J.; Hampton, D.R.; Schmitt, P.W.; Falk, J.L. Capnogram shape in obstructive lung disease. Anesth. Analg. 2005, 100, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Sahetya, S.K.; Goligher, E.C.; Brower, R.G. Fifty years of research in ARDS. Setting positive end-expiratory pressure in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1429–1438. [Google Scholar] [CrossRef]
- Vedrenne-Cloquet, M.; Khirani, S.; Khemani, R.; Lesage, F.; Oualha, M.; Renolleau, S.; Chiumello, D.; Demoule, A.; Fauroux, B. Pleural and transpulmonary pressures to tailor protective ventilation in children. Thorax 2023, 78, 97–105. [Google Scholar] [CrossRef]
- Pandey, M.; Gupta, D.; Gupta, N.; Sachdev, A. Use of transpulmonary pressure monitoring in the management of extrapulmonary pediatric acute respiratory distress syndrome with multi organ dysfunction syndrome (MODS): are we Peepophobic? Clin. Med. Insights Case Rep. 2019, 12, 1179547619842183. [Google Scholar] [CrossRef]
- Gleich, S.J.; Schiltz, B.M.; Ouellette, Y.; Baker, J.E.; Aganga, D.O. Improvement in oxygenation utilising transpulmonary pressure monitoring for optimal positive end-expiratory pressure in pediatric acute respiratory distress syndrome: a case report. A. A. Pract. 2019, 13, 114–117. [Google Scholar] [CrossRef]
- Ren, H.; Xie, L.; Wang, Z.; Tang, X.; Ning, B.; Teng, T.; Qian, J.; Wang, Y.; Fu, L.; Zhao, Z.; Xiang, L. Comparison of global and regional compliance-guided positive end-expiratory pressure titration on regional lung ventilation in moderate-to-severe pediatric acute respiratory distress syndrome. Front. Med. (Lausanne) 2022, 9, 805680. [Google Scholar] [CrossRef]
- Pugh, C.P.; Ali, S.; Agarwal, A.; Matlock, D.N.; Sharma, M. Dynamic computed tomography for evaluation of tracheobronchomalacia in premature infants with bronchopulmonary dysplasia. Pediatr. Pulmonol. 2023, 58, 3255–3263. [Google Scholar] [CrossRef]
- Hysinger, E.; Friedman, N.; Jensen, E.; Zhang, H.; Piccione, J. Bronchoscopy in neonates with severe bronchopulmonary dysplasia in the NICU. J. Perinatol. 2019, 39, 263–268. [Google Scholar] [CrossRef]
- Dellacà, R.L.; Veneroni, C.; Vendettuoli, V.; Zannin, E.; Matassa, P.G.; Pedotti, A.; Pedotti, A.; Colnaghi, M.; Mosca, F. Relationship between respiratory impedance and positive end-expiratory pressure in mechanically ventilated neonates. Intensive Care Med. 2013, 39, 511–519. [Google Scholar] [CrossRef]

| Parameter | Clinical data of the study population (n = 31) |
|---|---|
| Age, months | 9 (0-36) |
| neonates, n (%) | 8 (26) |
| infants, n (%) | 11 (35) |
| children, n (%) | 12 (39) |
| Weight, kg | 6.0 (3.8-10.5) |
| Male/ Female, n | 12/ 19 |
| Reason for intubation | |
| Asphyxia or encephalopathy, n (%) | 17 (55) |
| respiratory failure, n (%) | 7 (23) |
| operation, n (%) | 7 (23) |
| Ventilator settings | |
| FIO2 | 0.21 (0.21-0.35) |
| PIP, cmH2O | 17.6 ± 2.7 |
| PEEP, cmH2O | 5.9 ± 1.5 |
| RR, /min | 28 ± 7 |
| MAP, cmH2O | 9.0 ± 2.3 |
| VT, ml/kg | 9.8 ± 2.5 |
| Parameter | Term infants (n=28) | Preterm infants (n=21) |
|---|---|---|
| Gestational age, weeks | 38 (38-40) | 33 (31-34) |
| Birth weight, g | 2,924 (2,725-3,109) | 1,918 (1,356-2,186) |
| Male / Female, n | 12 / 16 | 8 / 13 |
| Cesarean section, n (%) | 20 (71) | 18 (86) |
| Twin birth, n (%) | 4 (14) | 4 (19) |
| Apgar score at 1 min | 5 (1-8) | 5 (4-6) |
| Apgar score at 5 min | 6 (4-9) | 7 (6-8) |
| Postnatal surfactant, n (%) | 4 (14) | 10 (48) |
| Days of measurements, days | 2 (1-4) | 4 (3-5) |
| Ventilator settings at baseline | ||
| FIO2 | 0.22 ± 0.01 | 0.23 ± 0.02 |
| PIP, cmH2O | 11.8 ± 1.4 | 12.9 ± 1.3 |
| PEEP, cmH2O | 5.4 ± 0.6 | 5.4 ± 0.7 |
| RR, /min | 38 ± 4 | 41 ± 6 |
| MAP, cmH2O | 6.7 ± 0.8 | 7.2 ± 0.9 |
| Parameter | Term (n=28) | Preterm (n=21) | ||||
|---|---|---|---|---|---|---|
| mild | moderate | high | mild | moderate | high | |
| PEEP, cmH2O | 5.0 ± 0††† | 7.0 ± 0††† | 9.8 ± 0.4 | 5.0 ± 0††† | 7.0 ± 0††† | 9.6 ± 0.5 |
| PIP, cmH2O | 11.4 ± 1.0††† | 15.3 ± 1.2††† | 22.1 ± 1.8 | 12.4 ± 0.9††† | 15.4 ± 0.8††† | 22.5 ± 1.8 |
| MAP, cmH2O | 6.4 ± 0.3††† | 8.8 ± 0.4††† | 12.6 ± 0.5 | 6.8 ± 0.3††† | 9.0 ± 0.4††† | 13.0 ± 0.5 |
| FIO2 | 0.22 ± 0.02 | 0.22 ± 0.02 | 0.22 ± 0.02 | 0.25 ± 0.01 | 0.25 ± 0.01 | 0.25 ± 0.01 |
| SpO2, % | 98.8 ± 1.4 | 98.7 ± 1.5 | 98.5 ± 1.4 | 96.7 ± 1.8 | 96.8 ± 1.8 | 96.9 ± 1.7 |
| VT/kg, ml/kg | 6.5 (5.5-6.6) | 6.2 (5.4-6.6) | 6.5 (5.5-6.7) | 6.1 (5.6–6.8) | 6.3 (5.6–6.5) | 6.2 (5.4–6.5) |
| Vd,aw, ml/kg | 2.0 (1.8-2.2)††† | 2.1 (1.8-2.4)††† | 2.4 (2.2-2.7) | 2.6 (2.2–2.8)††† | 2.8 (2.4–3.1)††† | 3.1 (2.5–3.4) |
| Vd,aw/VT | 0.34 (0.27-0.39)††† | 0.36 (0.30-0.42)††† | 0.40 (0.34-0.46) | 0.40 (0.36–0.44)††† | 0.42 (0.39–0.45)††† | 0.48 (0.44–0.50) |
| VA, ml/kg | 3.6 (3.2-4.2)†† | 3.4 (3.1-3.9) | 3.0 (2.7-3.8) | 3.1 (2.7–3.7)††† | 2.9 (2.6–3.6)††† | 2.6 (2.2–3.0) |
| VA/VT | 0.59 (0.53-0.64)††† | 0.56 (0.50-0.62)†† | 0.52 (0.46-0.58) | 0.50 (0.46–0.55)†††† | 0.49 (0.45–0.52)††† | 0.43 (0.40–0.48) |
| SⅡ, mmHg/ml | 8.4 (6.4-9.5) | 9.3 (6.1-10.5) | 9.2 (6.6-10.6) | 12.5 (9.8–15.1) | 13.1 (10.3–18.2) | 13.0 (10.5–18.3) |
| SnⅡ, mmHg | 150 (123-173) | 158 (124-174) | 166 (139-194) | 135 (117–161) | 146 (138–174) | 156 (138–174) |
| SⅢ, mmHg/ml | 0.17 (0.12-0.26) | 0.18 (0.08-0.26) | 0.2 (0.11-0.33) | 0.37 (0.18–0.68) | 0.35 (0.20–0.71) | 0.22 (0.09–0.44) |
| SnⅢ, mmHg | 3.9 (1.9-4.5) | 3.2 (1.6-4.1) | 3.6 (2.2-5.0) | 4.7 (2.7–8.8)† | 4.2 (2.7–9.8) | 2.3 (1.5–3.7) |
| KPlV | 24 (12-35) | 20 (11-30) | 22 (11-33) | 35 (17–54)† | 28 (17–58) | 16 (9–26) |
| Parameter | Term (n=28) | Preterm (n=21) | ||||
|---|---|---|---|---|---|---|
| high | moderate | mild | high | moderate | mild | |
| PEEP, cmH2O | 9.8 ± 0.4 | 7.0 ± 0††† | 5.0 ± 0††† | 9.6 ± 0.5 | 7.0 ± 0††† | 5.0 ± 0††† |
| PIP, cmH2O | 22.0 ± 1.6 | 15.3 ± 1.0††† | 11.4 ± 0.9††† | 22.4 ± 1.7 | 15.2 ± 0.7††† | 12.2 ± 0.8††† |
| MAP, cmH2O | 12.7 ± 0.5 | 8.9 ± 0.4††† | 6.4 ± 0.3††† | 13.0 ± 0.5 | 9.0 ± 0.3††† | 6.7 ± 0.3††† |
| FIO2 | 0.22 ± 0.02 | 0.22 ± 0.02 | 0.22 ± 0.02 | 0.23 ± 0.01 | 0.23 ± 0.01 | 0.23 ± 0.01 |
| SpO2, % | 99.0 ± 1.3 | 98.7 ± 1.6 | 98.7 ± 1.6 | 98.1 ± 2.0 | 97.7 ± 2.0 | 97.1 ± 2.0 |
| VT/kg, ml/kg | 6.5 (5.5-6.6) | 6.5 (5.5-6.8) | 6.5 (5.6-6.9) | 6.2 (5.7-6.9) | 6.9 (6.3-7.5) | 6.1 (5.5-7.4) |
| Vd,aw, ml/kg | 2.4 (2.2-2.4) | 2.1 (1.9-2.3)††† | 2.0 (1.8-2.2)††† | 3.2 (2.5-3.5) | 2.6 (2.3-3.0)††† | 2.5 (2.1-2.7)††† |
| Vd,aw/VT | 0.40 (0.34-0.46) | 0.36 (0.31-0.39)††† | 0.33 (0.29-0.37)††† | 0.48 (0.44-0.5) | 0.39 (0.33-0.44)††† | 0.39 (0.34-0.42)††† |
| VA, ml/kg | 2.9 (2.6-3.7) | 3.1 (2.9-3.9) | 3.4 (2.9-4.1)† | 2.6 (2.2-3.0) | 3.5 (2.7-3.7)††† | 3.3 (2.8-4.0)††† |
| VA/VT | 0.52 (0.46-0.58) | 0.55 (0.52-0.60)†† | 0.56 (0.51-0.62)††† | 0.42 (0.40-0.47) | 0.52 (0.47-0.57)††† | 0.52 (0.48-0.57)††† |
| SⅡ, mmHg/ml | 9.2 (6.6-10.8) | 8.6 (6.1-10.3) | 8.5 (7.0-9.2) | 13.0 (10.4-18.3) | 13.5 (9.5-15.7) | 12.8 (9.3-15.4) |
| SnⅡ, mmHg | 166 (139-193) | 155 (124-176) | 152 (125-164) | 156 (138-174) | 162 (130-191) | 137 (125-164) |
| SⅢ, mmHg/ml | 0.2 (0.11-0.32) | 0.15 (0.09-0.19) | 0.17 (0.06-0.29) | 0.22 (0.09-0.44) | 0.28 (0.12-0.62) | 0.42 (0.25-0.77) |
| SnⅢ, mmHg | 3.6 (2.2-4.9) | 3.0 (1.7-4.0) | 3.5 (1.1-5.2) | 2.3 (1.5-3.7) | 4.3 (1.7-7.1) | 4.7 (3.1-10.1)† |
| KPlV | 22 (11-34) | 20 (11-23) | 24 (7-34) | 16 (9-27) | 20 (10-59) | 33 (23-58)† |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



