Submitted:
13 August 2025
Posted:
14 August 2025
You are already at the latest version
Abstract
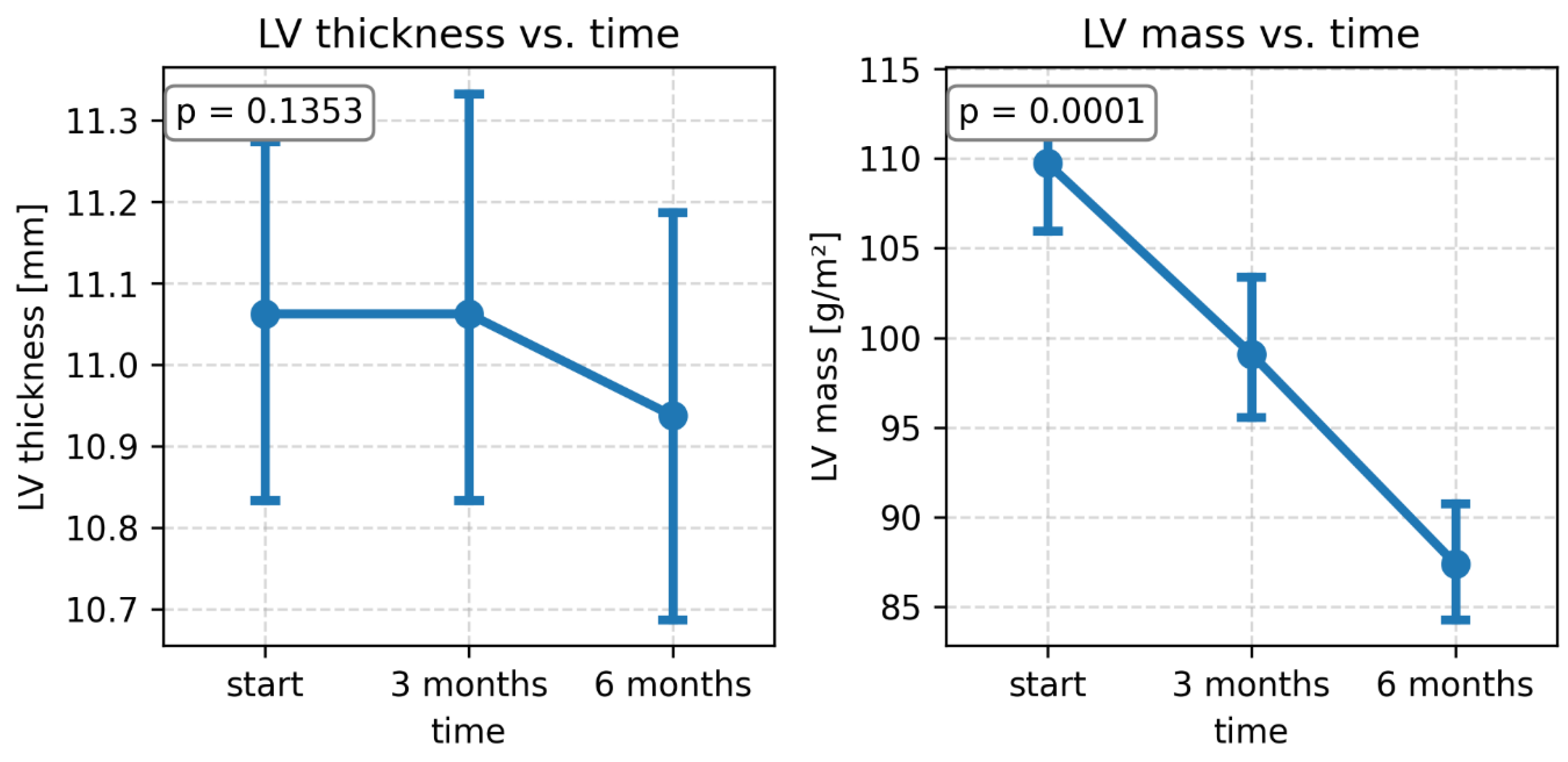
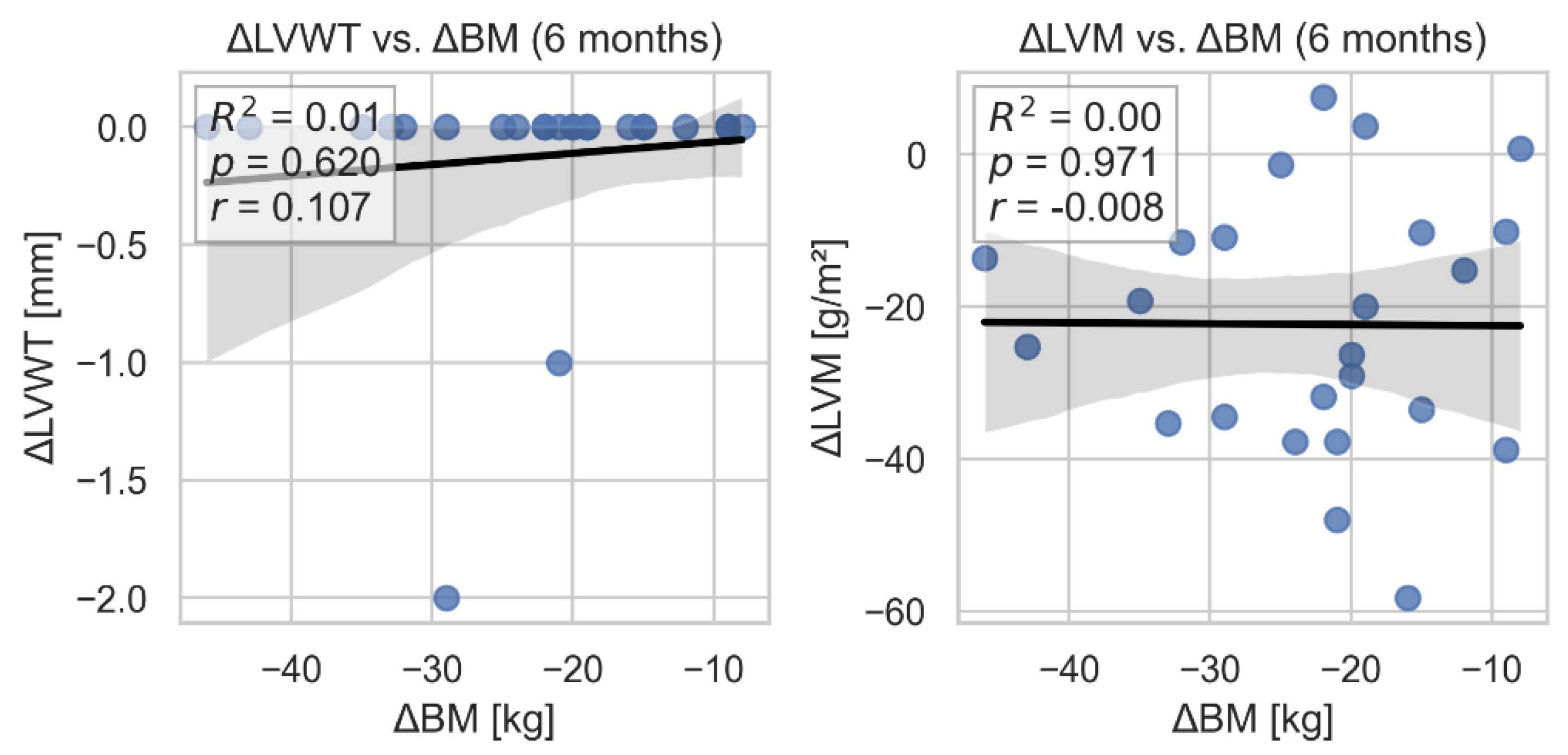
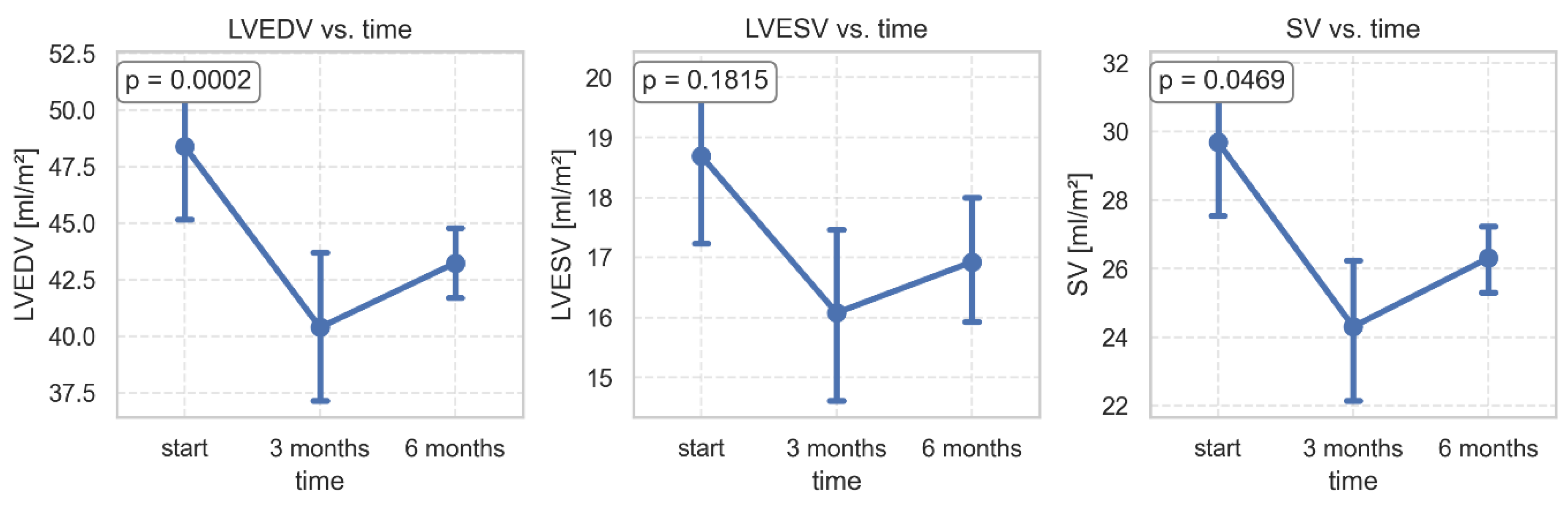
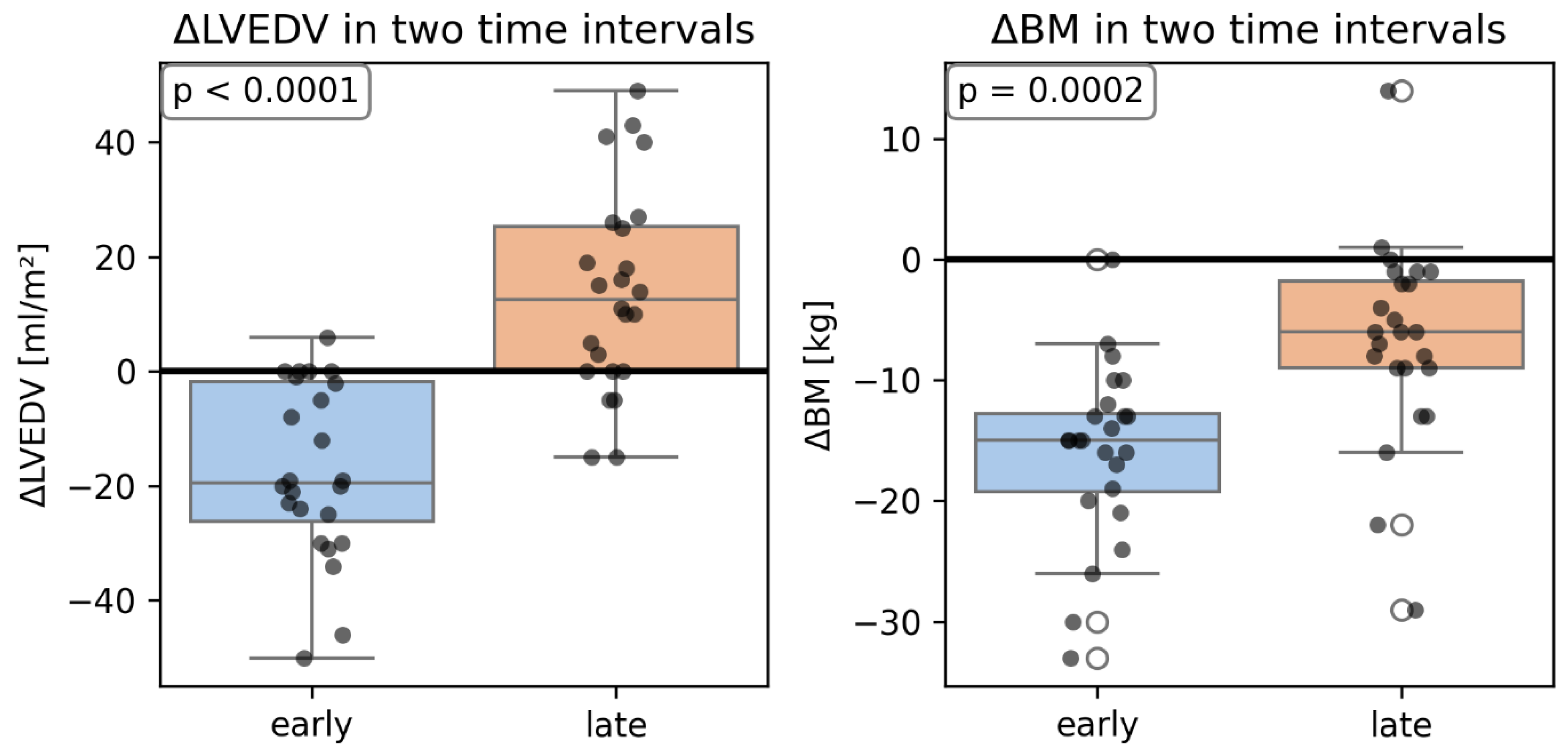
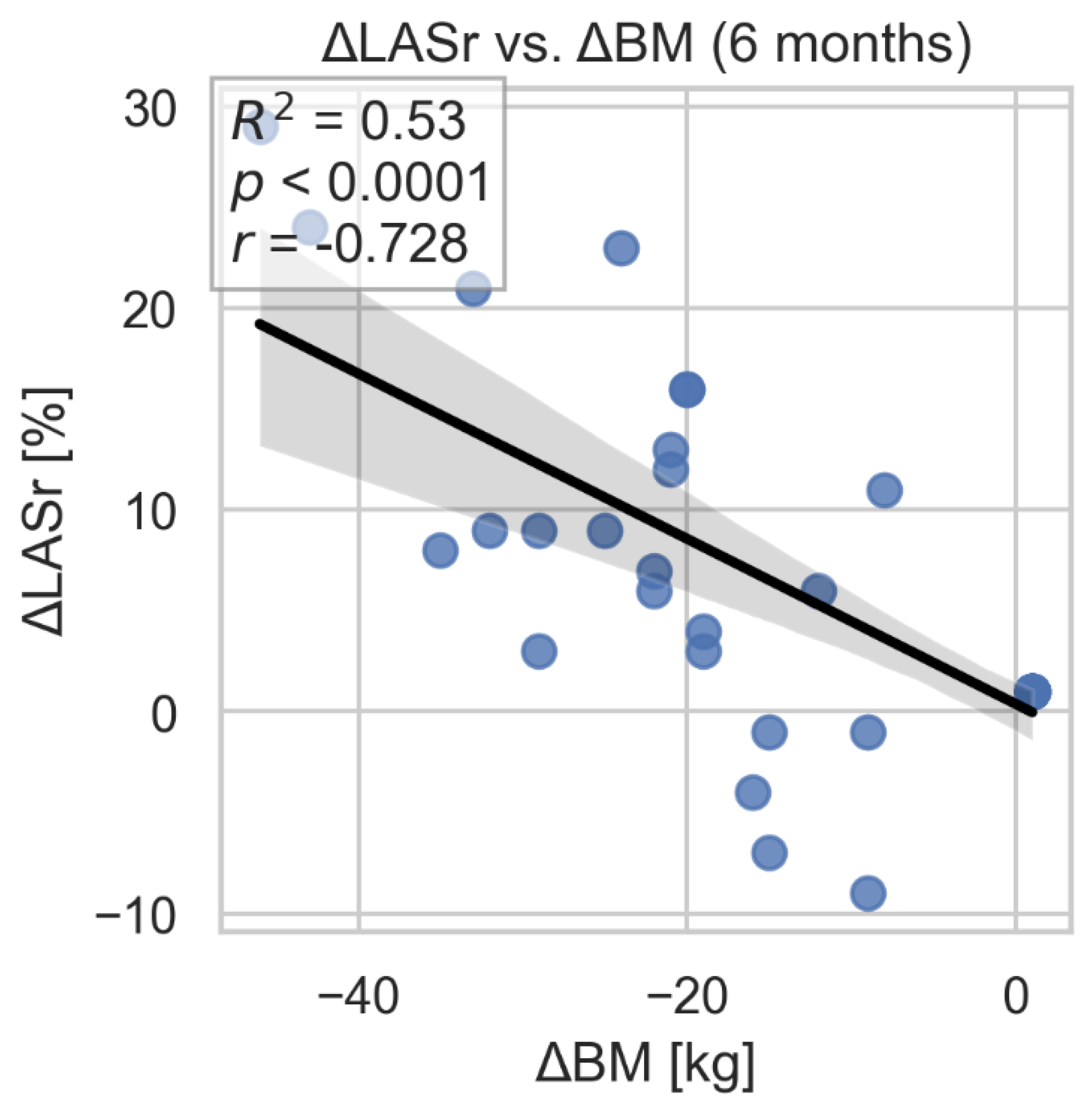
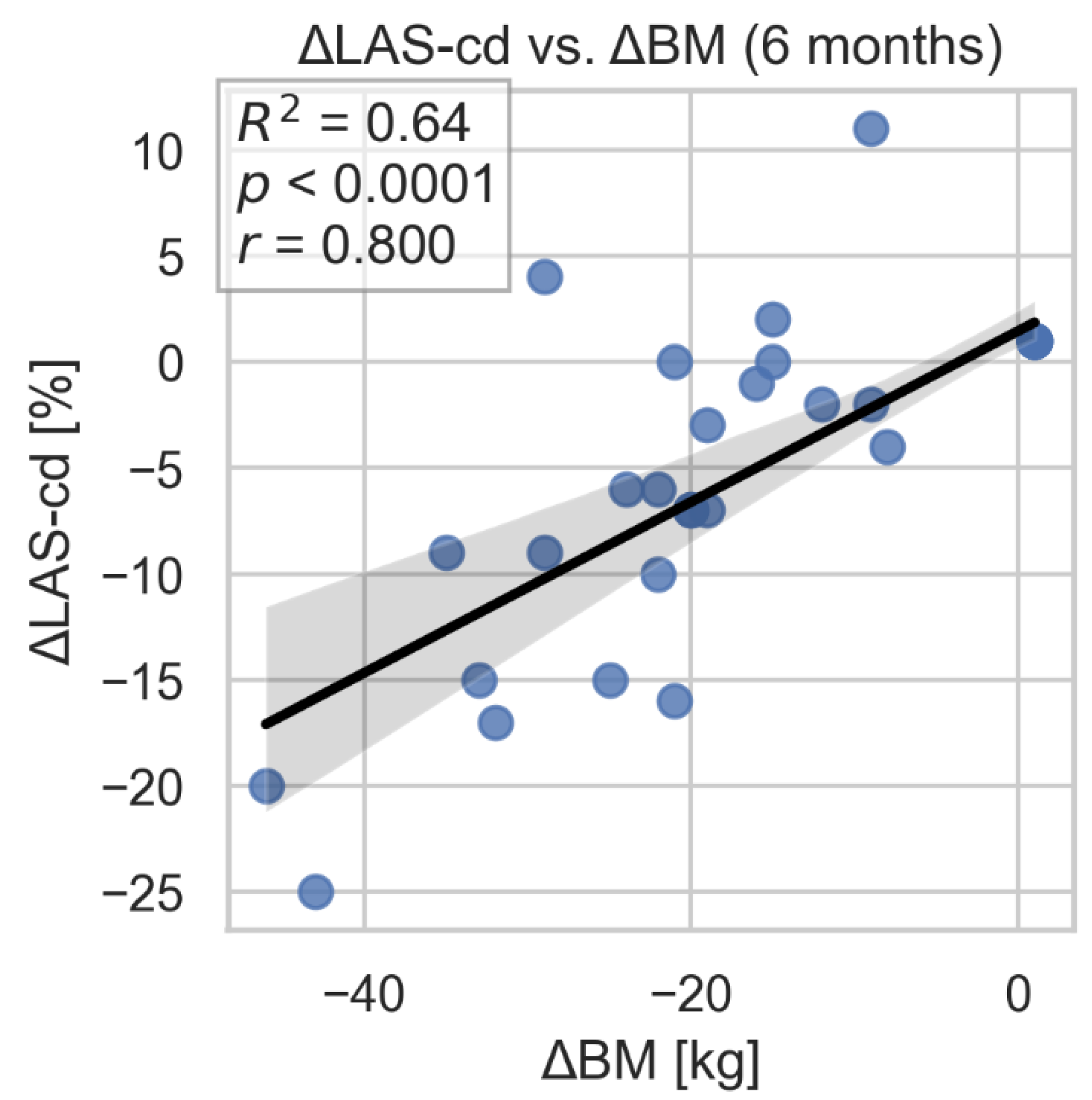
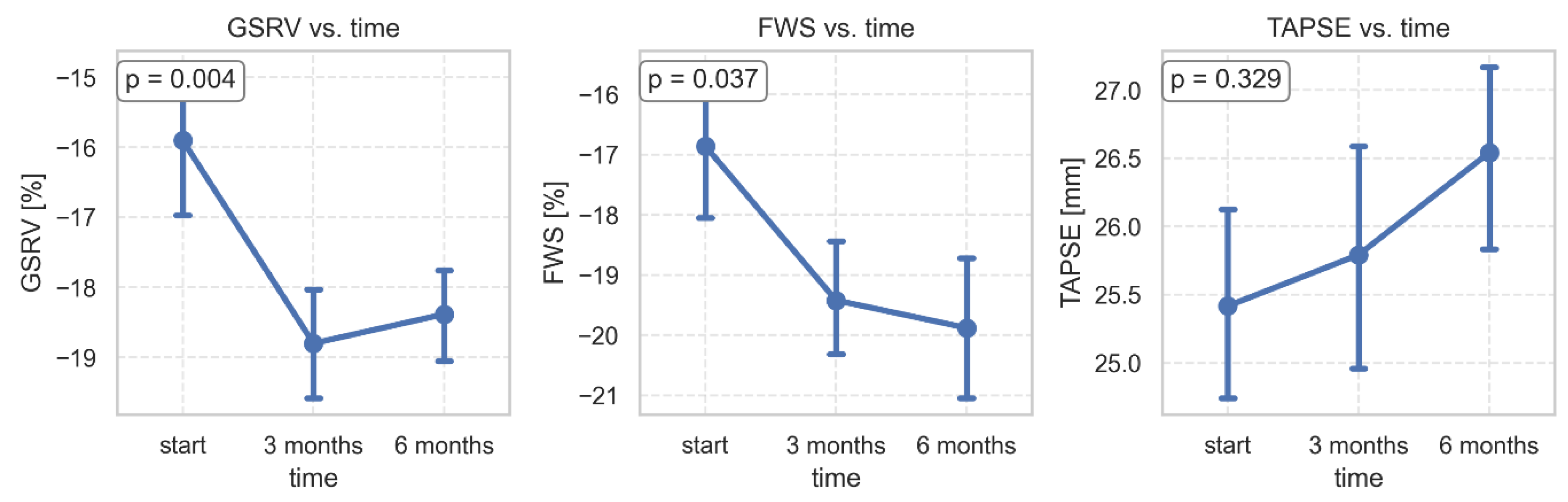
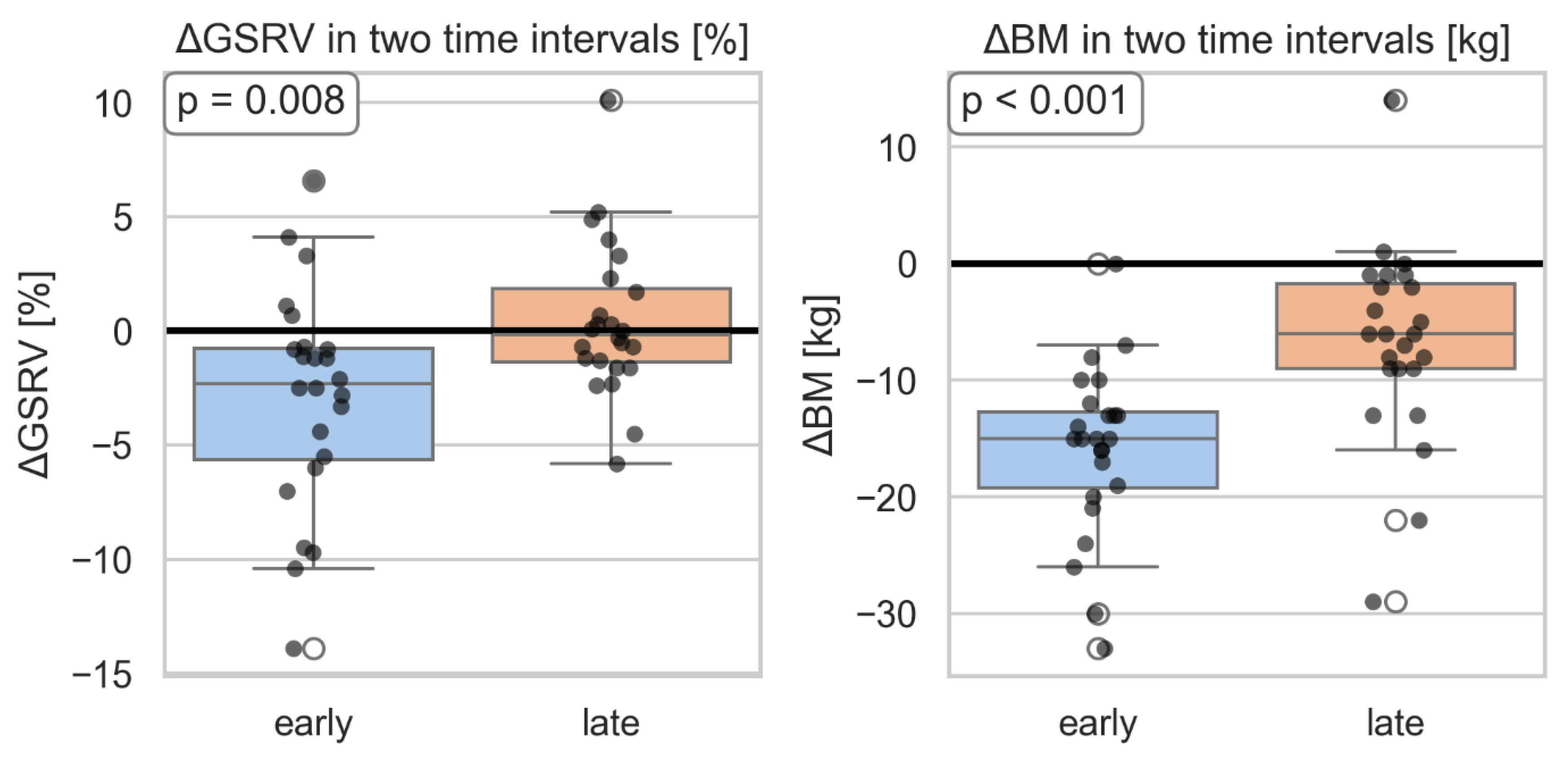
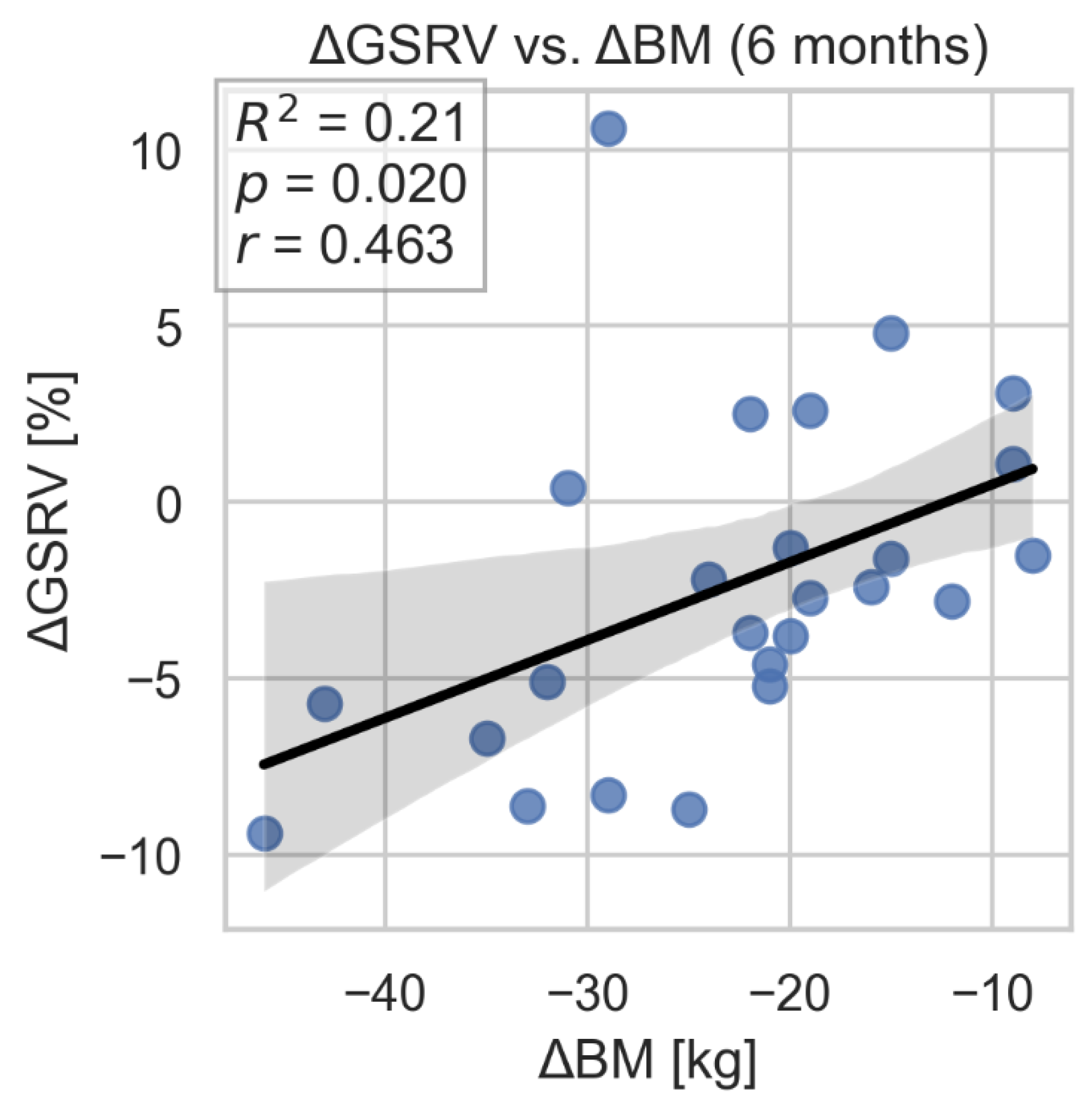
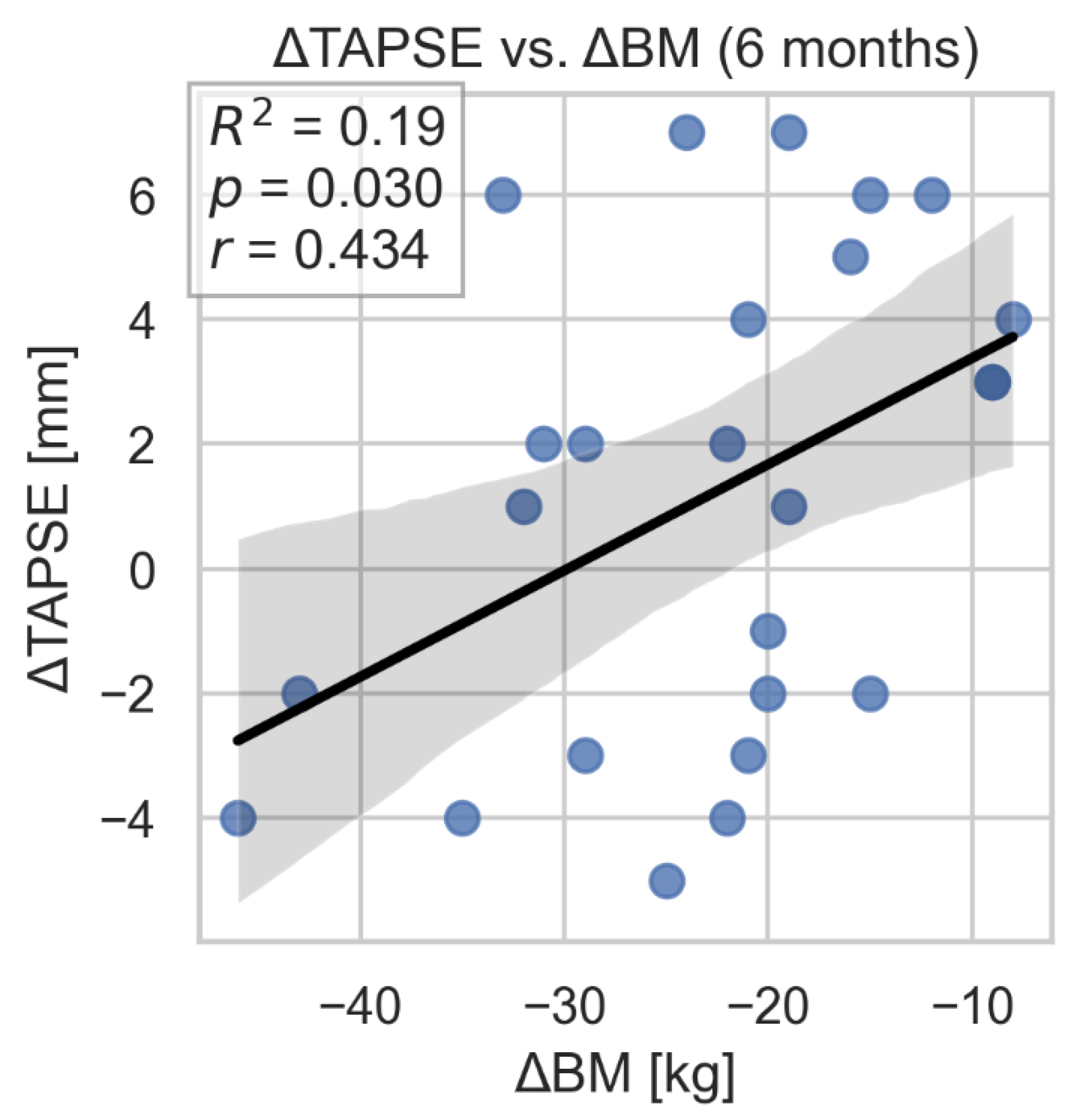
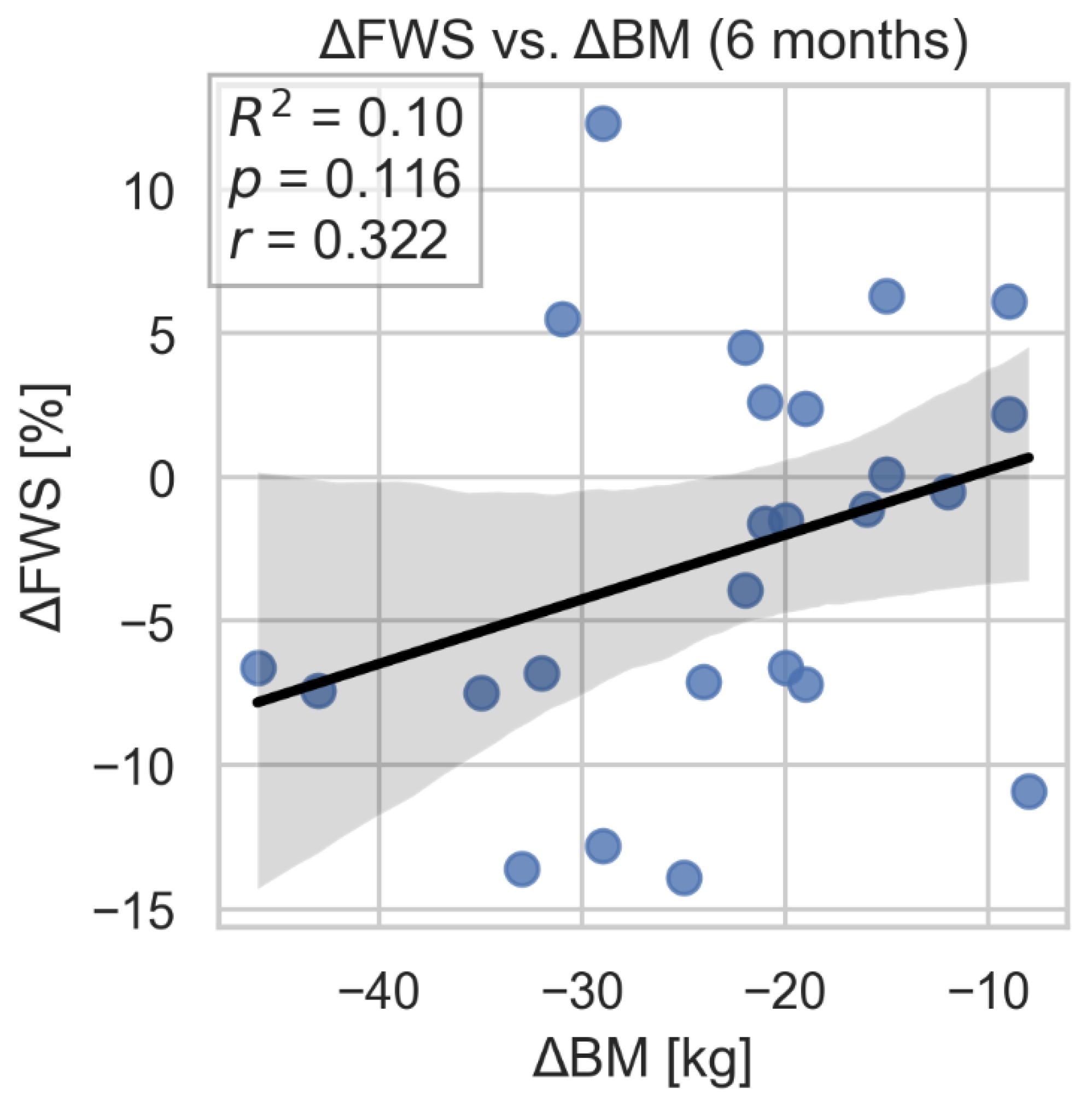
Background: Severe obesity causes hemodynamic changes in the circulatory system, which leads to the development of heart failure with either preserved or reduced ejection fraction. Weight loss achieved through bariatric surgery is likely to possibly reverse many of hemodynamic and structural abnormalities caused by obesity. Methods: Detailed echocardiographic parameters assessing left and right ventricular function in severely obese patients undergoing bariatric surgery were analyzed. The following parameters were compared in the examinations performed before surgery and 3 and 6 months after surgery: left ventricular ejection fraction (LVEF), left ventricle (LV) and right ventricle (RV) global longitudinal strain (GLS and GSRV) with right ventricular free wall strain (FWSRV), peak early (e’) and late (a’) diastolic annular velocities (lateral and septal) with calculation of E/e’ ratios, left atrium volume index (LAVI), left atrial strain (LAS) including LAS conduit ( LAS-cd) and LAS tricuspid regurgitation velocity (TRV), tricuspid annular plane systolic excursion (TAPSE), maximum systolic velocity of the lateral part of the tricuspid annulus-s’ and accelerated pulmonary time (AcT). Results: Forty consecutive obese patients undergoing bariatric surgery from December 2022 till June 2023 were enrolled to the study. Finally 39 patients were included. The study population consisted of 76% women with mean BMI of 40.3 (SD 5.6) and mean age of 42.4 (SD 11.9). BMI after 3 months was 35,3 kg/m2, after 6 months was 31.2 kg/m2 (SD 5.1). At 3- and 6-month follow-up after bariatric surgery there was a reduction in left ventricular mass (109.7 vs. 99.1 vs. 87.4 kg/m2; p<0.001), LVEDV (47.1 vs. 30.0 vs. 43.7; p<0.001) and SV (29.7 vs. 24.3 vs. 26.3; p=0.05). Simultaneously an improvement in GLS (-14.38 vs. -16.79 vs. -18.01) and an increase in LAS parameters (reservoir : 22.5 vs. 28.0 vs. 31.1; p<0.001 and conduit: -12.8 vs. -16.5 vs. -19.6) were observed. Comparison of right ventricular parameters before and after bariatric surgery showed improvement in GSRV (-15.9 vs. -18.8 vs. -18.38%; p=0.005), FWS (-18.38 vs. -19.70 vs. -19.50; p=0.042) and reduction in TRV (1.84 vs. 1.67 vs. 1.46±0.52; p=0.01). Conclusions: Weight loss contributes to rapid improvement in left and right ventricular function. Some changes of echocardiographic parameters: LVEDV, LAS-r, LAS-cd, GSRV and TAPSE correlate with the degree of weight loss. New echocardiographic parameters earlier detect subclinical hemodynamic changes associated with obesity and weight loss after bariatric surgery.
Keywords:
1. Introduction
2. Methods
Statistical Methods
3. Results
3.1. Left Ventricular and Left Atrium Parameters
3.2. Right Ventricular Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Grapsa J, Tan TC, Paschou SA, Kalogeropoulos AS, Shimony A, Kaier T, Demir OM, Mikhail S, Hakky S, Purkayastha S, Ahmed AR, Cousins J, Nihoyannopoulos P. The effect of bariatric surgery on echocardiographic indices: a review of the literature. Eur J Clin Invest 2013;43(11):1224–1230. [CrossRef]
- Alpert MA, Omran J, Bostick BP. Effects of Obesity on Cardiovascular Hemodynamics, Cardiac Morphology, and Ventricular Function. Curr Obes Rep 2016;5:424–434. [CrossRef]
- Shin, S.H.; Lee, Y.J.; Heo, Y.S.; Park, S.D.; Kwon, S.W.; Woo, S.I.; Kim, D.H.; Park, K.S.; Kwan, J. Beneficial Effects of Bariatric Surgery on Cardiac Structure and Function in Obesity. Obes. Surg. 2017; 27: 620–625. [CrossRef]
- Sorimachi H, Obokata M, Omote K, Reddy YNV, Takahashi N, Koepp KE, Ng ACT, Rider OJ, Borlaug BA. Long-Term Changes in Cardiac Structure and Function Following Bariatric Surgery. J Am Coll Cardiol 2022;80(16):1501–1512. [CrossRef]
- Mostfa, S.A. Impact of obesity and surgical weight reduction on cardiac remodeling. Indian Heart J 2018;70:S224–S228. [CrossRef]
- Esparham A, Shoar S, Kheradmand HR, Ahmadyar S, Dalili A, Rezapanah A, Zandbaf T, Khorgami Z. The Impact of Bariatric Surgery on Cardiac Structure and Function: A Systematic Review and Meta-analysis. Obes Surg 2023;33:345–361.
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015; 28:1-39.e14. [CrossRef]
- Aryee EK, Ozkan B, Ndumele CE. Heart Failure and Obesity: The Latest Pandemic. Prog Cardiovasc Dis. 2023;78:43. [CrossRef]
- Rodrigues MM, Falcão LM. Pathophysiology of heart failure with preserved ejection fraction in overweight and obesity - clinical and treatment implications. Int J Cardiol. 2025;1;430:133182. [CrossRef]
- Alpert MA, Karthikeyan K, Abdullah O, Ghadban R. Obesity and Cardiac Remodeling in Adults: Mechanisms and Clinical Implications. Prog Cardiovasc Dis. 2018; 61:114-123. [CrossRef]
- Wong CY, O’Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation. 2004 ;110:3081-3087. [CrossRef]
- Barbosa MM, Beleigoli AM, de Fatima Diniz M, Freire CV, Ribeiro AL, Nunes MC. Strain imaging in morbid obesity: insights into subclinical ventricular dysfunction. Clin Cardiol. 2011;34:288-293.
- Orhan AL, Uslu N, Dayi SU, Nurkalem Z, Uzun F, Erer HB, Hasdemir H, Emre A, Karakus G, Soran O, Gorcsan J 3rd, Eren M. Effects of isolated obesity on left and right ventricular function: a tissue Doppler and strain rate imaging study. Echocardiography. 2010;27:236–243.
- Kang X, Zhou L, Zhang Y, Kang C, Xue J. Myocardial mechanical changes before and after bariatric surgery in individuals with obesity and diabetes: a 1-year follow-up study. Sci Rep. 2025; 2;15:580. [CrossRef]
- Koshino, Y.; Villarraga, H.R.; Somers, V.K.; Miranda, W.R.; Garza, C.A.; Hsiao, J.F.; Yu, Y.; Saleh, H.K.; Lopez-Jimenez, F. Changes in myocardial mechanics in patients with obesity following major weight loss after bariatric surgery. Obesity 2013, 21, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Tuluce K, Kara C, Tuluce SY, Cetin N, Topaloglu C, Bozkaya YT, Saklamaz A, Cinar CS, Ergene O. Early Reverse Cardiac Remodeling Effect of Laparoscopic Sleeve Gastrectomy. Obes Surg. 2017;27:364-375. [CrossRef]
- Kemaloğlu Öz T, Ünal Dayı Ş, Seyit H, Öz A, Ösken A, Atasoy I, Yıldız U, Özpamuk Karadeniz F, İpek G, Köneş O, Alış H. The effects of weight loss after sleeve gastrectomy on left ventricular systolic function in men versus women. J Clin Ultrasound. 2016;44:492-499.
- Kossaify A, Nicolas N. Impact of overweight and obesity on left ventricular diastolic function and value of tissue Doppler echocardiography. Clin Med Insights Cardiol. 2013;7:43-50. [CrossRef]
- Lavie CJ, Alpert MA, Arena R, Mehra MR, Milani RV, Ventura HO. Impact of obesity and the obesity paradox on prevalence and prognosis in heart failure. J Am Coll Cardiol HF 2013;1:93-102. [CrossRef]
- Alpert MA, Omran J, Mehra A, Ardhanari S. Impact of obesity and weight loss on cardiac performance and morphology in adults. Prog Cardiovasc Dis 2014;56:391-400. [CrossRef]
- Alpert MA, Lavie CJ, Agrawal H, Kumar A, Kumar SA. Cardiac effects of obesity: pathophysiologic, clinical and prognostic consequences. J Cardiopulm Rehabil Prev. 2016; 36:1-11.
- Alpert MA, Terry BE, Kelly DL. Effect of weight loss on cardiac chamber size, wall thickness and left ventricular function in morbid obesity. Am J Cardiol. 1985 1;55:783-786. [CrossRef]
- Iacobellis G, Ribaudo MC, Leto G, Zappaterreno A, Vecci E, Di Mario U, Leonetti F. Influence of excess fat on cardiac morphology and function: study in uncomplicated obesity. Obes Res. 2002;10:767-773. [CrossRef]
- Hsuan CF, Huang CK, Lin JW, Lin LC, Lee TL, Tai CM, Yin WH, Tseng WK, Hsu KL, Wu CC. The effect of surgical weight reduction on left ventricular structure and function in severe obesity. Obesity (Silver Spring). 2010;18:1188-1193. [CrossRef]
- Willens HJ, Byers P, Chirinos JA, Labrador E, Hare JM, de Marchena E. Effects of weight loss after bariatric surgery on epicardial fat measured using echocardiography. Am J Cardiol 2007;99:1242–1245. [CrossRef]
- Valezi AC, Machado VH. Morphofunctional evaluation of the heart of obese patients before and after bariatric surgery. Obes Surg 2011;21:1693–1697. [CrossRef]
- Kardassis D, Bech-Hanssen O, Sch€onander M, Sj€ostr€om L, Karason K. The influence of body composition, fat distribution, and sustained weight loss on left ventricular mass and geometry in obesity. Obesity (Silver Spring) 2012;20:605–611. [CrossRef]
- Leichman JG, Wilson EB, Scarborough T, Aguilar D, Miller CC 3rd, Yu S et al. Dramatic reversal of derangements in muscle metabolism and left ventricular function after bariatric surgery. Am J Med 2008;121:966–973.
- Aga, Y.S.; Kroon, D.; Snelder, S.M.; Biter, L.U.; de Groot-de Laat, L.E.; Zijlstra, F.; Brugts, J.J.; van Dalen, B.M. Decreased Left Atrial Function in Obesity Patients without Known Cardiovascular Disease. Int. J. Cardiovasc. Imaging 2023, 39, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Chirinos JA, Sardana M, Satija V, Gillebert TC, De Buyzere ML, Chahwala J, De Bacquer D, Segers P, Rietzschel ER; Asklepios investigators. Effect of Obesity on Left Atrial Strain in Persons Aged 35-55 Years (The Asklepios Study). Am J Cardiol. 2019;123:854-861. [CrossRef]
- Strzelczyk J, Kalinowski P, Zieniewicz K, Szmigielski C, Byra M, Styczyński G. The Influence of Surgical Weight Reduction on Left Atrial Strain. Obes Surg. 2021;31:5243-5250. [CrossRef]
- Wong CY, O’Moore-Sullivan T, Leano R, Hukins C, Jenkins C, Marwick TH. Association of subclinical right ventricular dysfunction with obesity. J Am Coll Cardiol. 2006; 7;47:611-616. [CrossRef]
- Garza CA, Pellikka PA, Somers VK, Sarr MG, Collazo-Clavell ML, Korenfeld Y, Lopez-Jimenez F. Garza CA, Pellikka PA, Somers VK, Sarr MG, Collazo-Clavell ML, Korenfeld Y, Lopez-Jimenez F. Am J Cardiol. 2010; 15;105:550-556.
- Liu J, Li J, Yu J, Xia C, Pu H, He W, Li X, Zhou X, Tong N, Peng L. Regional Fat Distributions Are Associated With Subclinical Right Ventricular Dysfunction in Adults With Uncomplicated Obesity. Front Cardiovasc Med. 2022; 25:9:814505.
- Yuksel IO, Akar Bayram N, Koklu E, Ureyen CM, Kucukseymen S, Arslan S, Bozkurt E Assessment of Impact of Weight Loss on Left and Right Ventricular Functions. Echocardiography 2016; 33:854–861.
- Büber I, Aykota MR, Sevgican Cİ, Kaya D, Akarsu H, Tekin I, Kılıc ID. Impact of Laparoscopic Sleeve Gastrectomy on Pulmonary Arterial Stiffness and Right Ventricular Function. Obes Surg 2025;35:87–92. [CrossRef]

| Category | Count (%) |
| Gender | |
| Women | 32 (82.05%) |
| Men | 7 (17.95%) |
| Comorbidities | |
| Hypertension (HTN) | 17 (43.59%) |
| Ischemic Heart Disease (IHD) | 3 (7.69%) |
| Diabetes | 9 (23.08%) |
| Hypothyroidism | 11 (28.21%) |
| Type of procedure | |
| Sleeve Gastrectomy | 34 (87.18%) |
| Balloon | 3 (7.69%) |
| Mini-Gastric Bypass | 1 (2.56%) |
| Single Anastomosis Sleeve Ileal Bypass | 1 (2.56%) |
| Left ventricle Parameters |
Before surgery | 3 months after surgery | 6 months after surgery | P value |
|---|---|---|---|---|
| LV wall thickness | 11.1 +/- 1.2 | 11.1 +/- 1.2 | 10.9 +/- 1.2 | 0.14 |
| LV mass index (g/m2) | 109.7 +/- 20.3 | 99.1 +/-19.4 | 87.4 +/- 16.2 | <0.001 |
| LVEDV | 47.1 +/- 13.2 | 30.0 +/- 15.0 | 43.7 +/- 11.0 | <0.001 |
| LVESV | 18.7 +/- 5.4 | 16.1 +/- 5.3 | 16.9 +/- 3.8 | 0.18 |
| SV | 29.7 +/- 7.8 | 24.3 +/- 7.6 | 26.3 +/- 3.7 | 0.05 |
| LVEF (%) | 59±4.8 | 61±4.8 | 61.3±4,8 | 0.167 |
| GLS (%) | -14.38±2.47 | -16.79±2.21 | -18.01±2.32 | 0.001 |
| E/A | 1.1 +/- 0.3 | 1.1 +/- 0.4 | 1.2 +/- 0.3 | 0.38 |
| T dec | 194.8 +/- 33.4 | 214.8 +/- 45.2 | 197.1 +/- 33.9 | 0.06 |
| e’ sept (cm/s) | 9.88±2.54 | 10.04±2.31 | 11.00±2.65 | 0.15 |
| E/e’ sept | 8.17±1.69 | 7.58±2.36 | 7.46±1.69 | 0.39 |
| e’ lat (cm/s) | 13.5±2.70 | 13.46±3.51 | 15.21±4.42 | 0.13 |
| E/e’ lat | 6.71±1.52 | 6.58±1.61 | 6.04±1.27 | 0.14 |
| LAVI (ml/m2) | 24.3±9.17 | 23.9±8.77 | 22.8±7.19 | 0.32 |
| LAS-r | 22.5 +/- 7.5 | 28.0 +/- 6.1 | 31.1 +/- 8.6 | <0.001 |
| LAS-cd | -12.8 +/- 6.3 | -16.5 +/- 5.3 | -19.6 +/- 7.0 | <0.001 |
| LAS-ct | -8.3 +/- 7.0 | -11.5 +/- 3.8 | -10.8 +/- 5.8 | 0.18 |
| Right ventricle Parameters |
Before surgery | 3 months after surgery | 6 months after surgery |
P-value |
|---|---|---|---|---|
| GSRV [%] | -15.9+/-5.29 | -18.8+/-4.03 | -18.38+/-3.25 | 0.005 |
| FWSRV [%] | -18.38+/-6.17 | -19.7+/-5.00 | -19.5+/-5.182 | 0.042 |
| TAPSE [mm] | 25.4+/-3.3 | 25.8+.-4.0 | 26.5+/-3.3 | 0.36 |
| TRV max (m/s) | 1.84±0.62 | 1.67±0.59 | 1.46±0.52 | 0.01 |
| s’ [cm/s] | 14.7+/-3.52 | 14.2+/-2.9 | 14.9+/-2.32 | 0.55 |
| AcT [ms] | 108.4+/-13.5 | 110.3+/-12.3 | 109.9+/-12.3 | 0.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



