Submitted:
23 July 2025
Posted:
14 August 2025
You are already at the latest version
Abstract
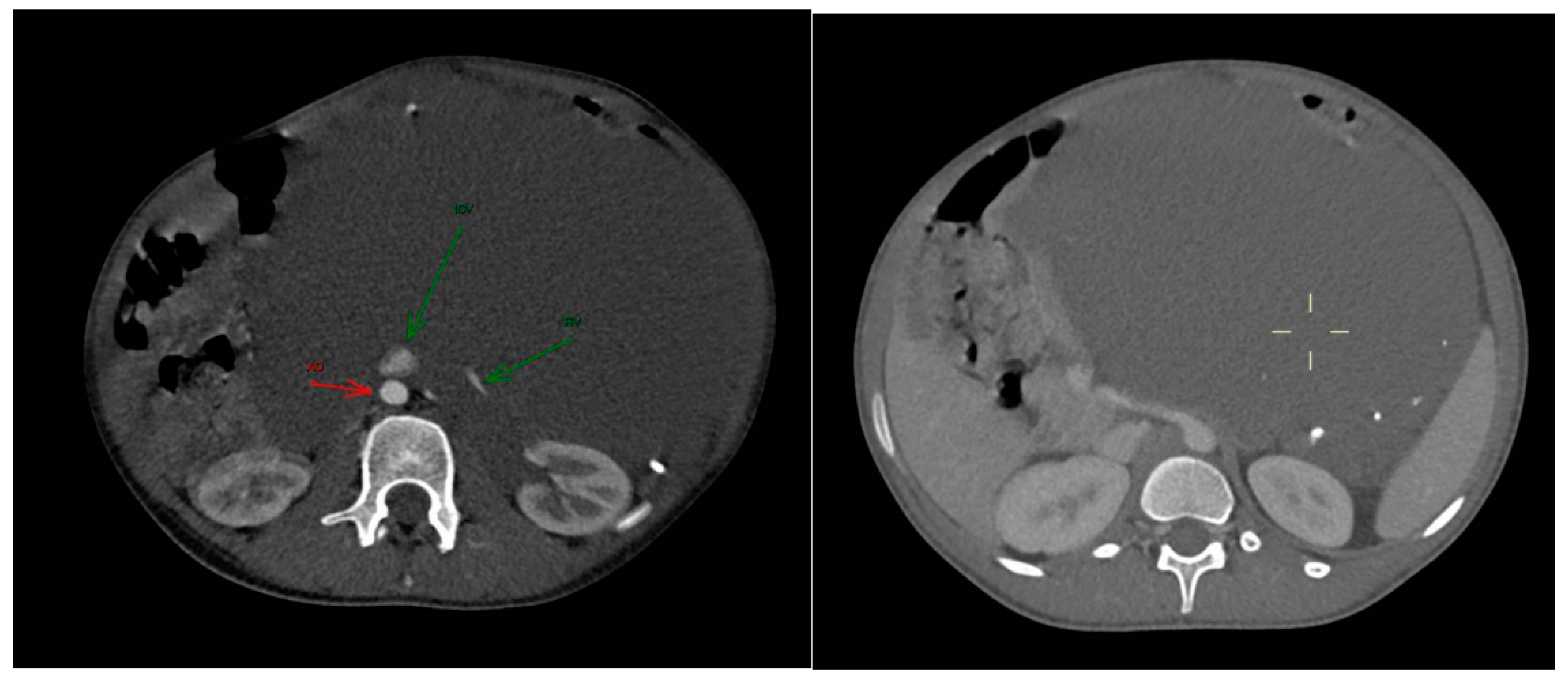
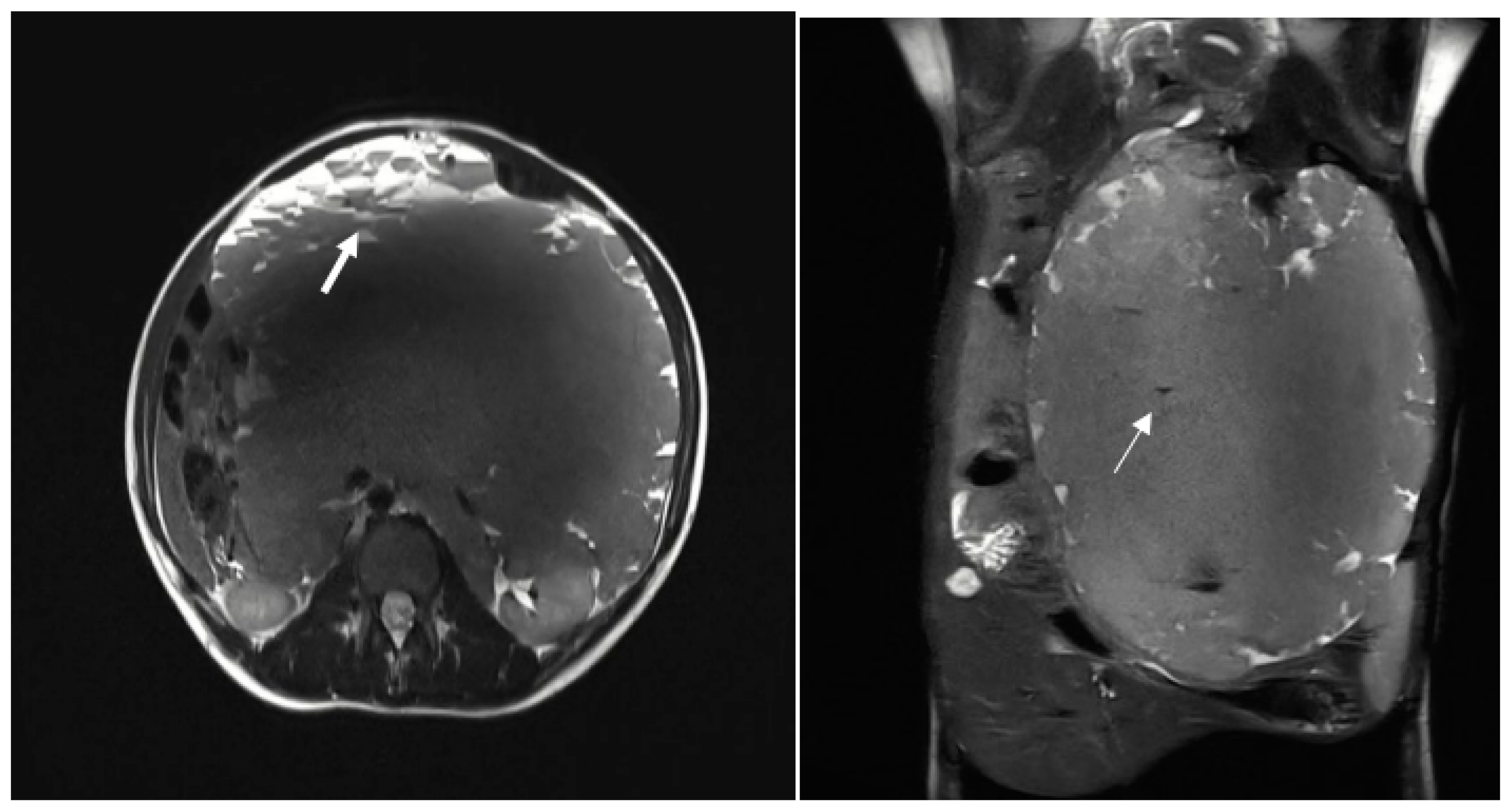
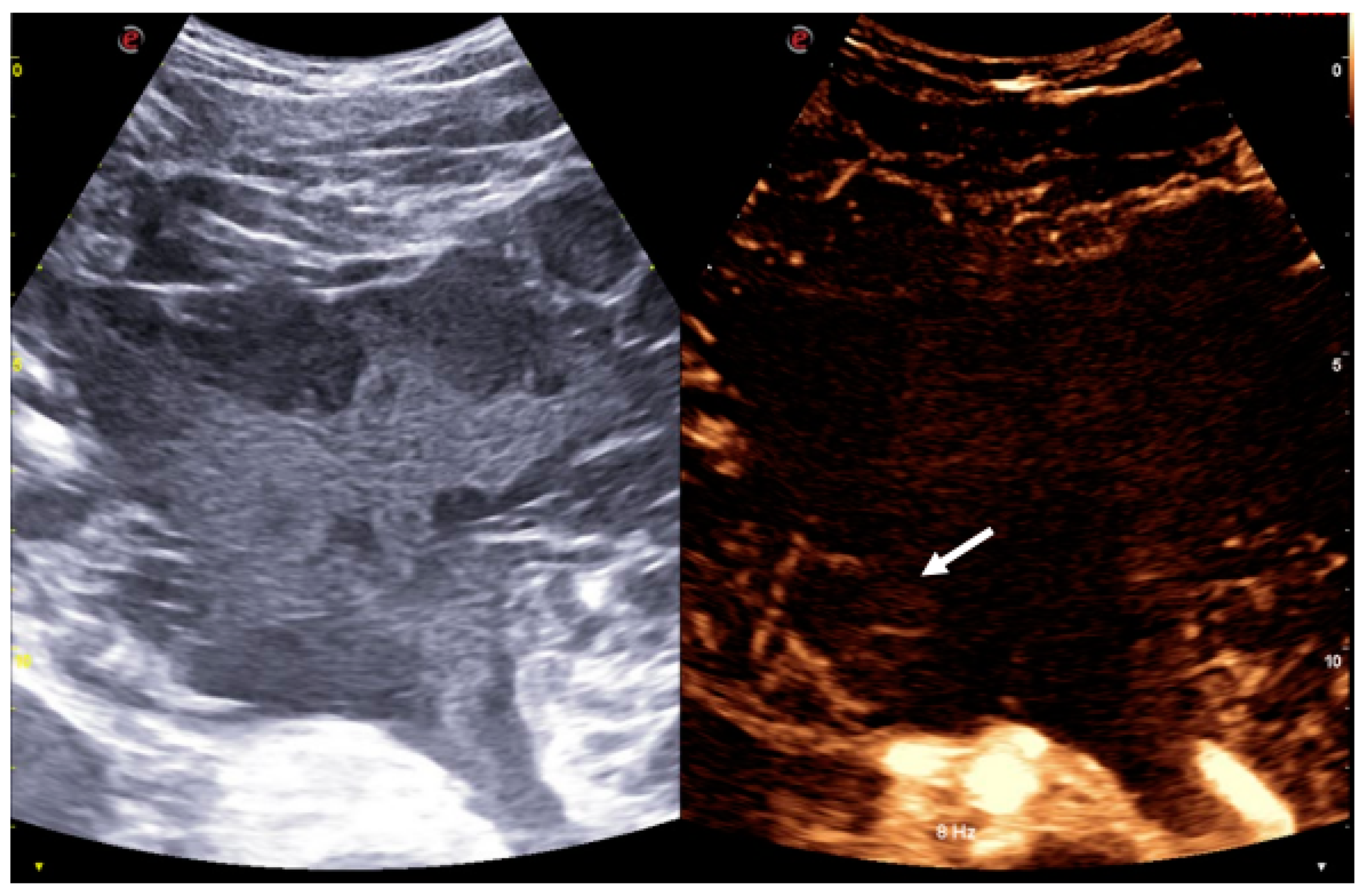
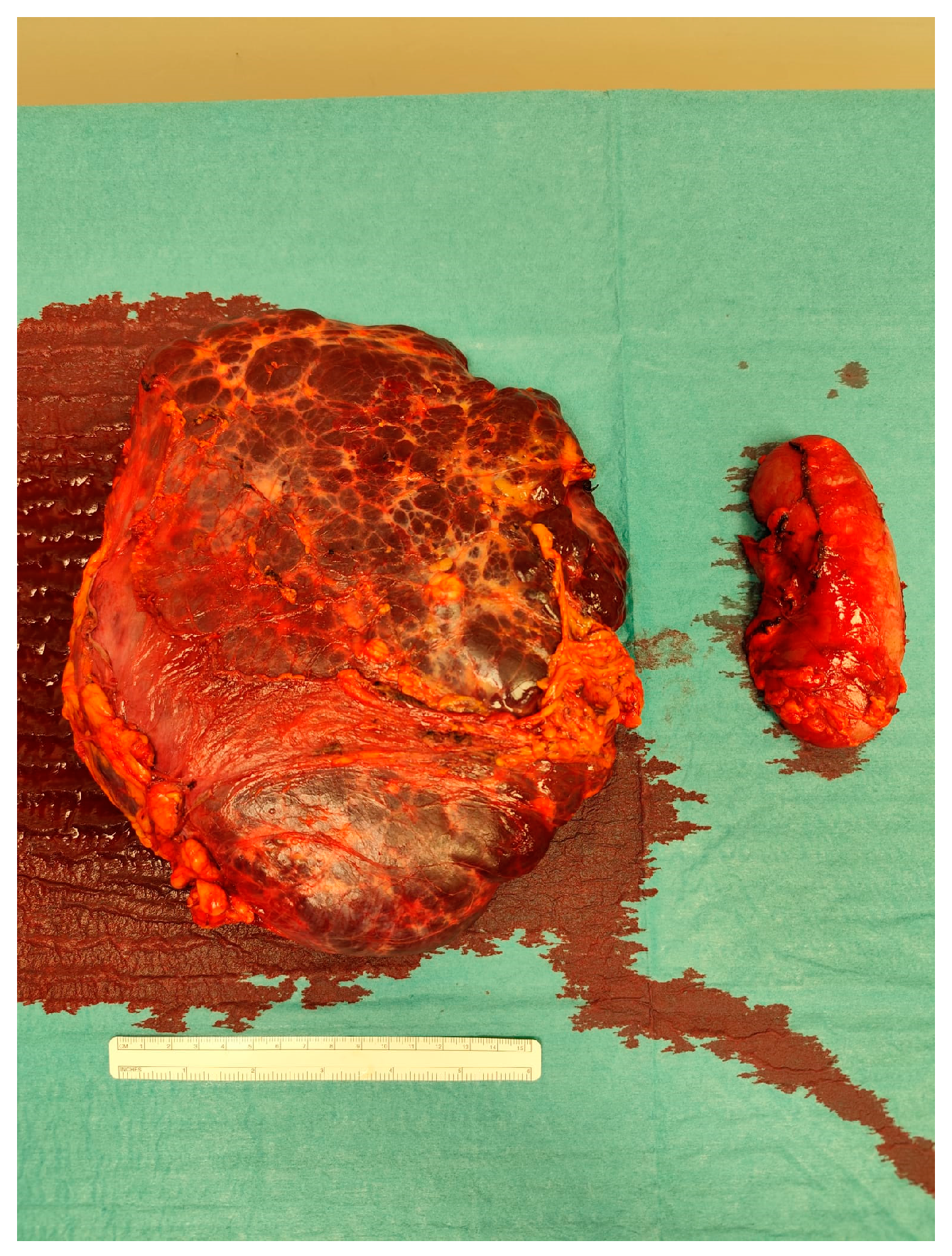
Lymphatic-venous malformations (LVMs) are rare congenital low-flow vascular anomalies characterized by abnormal, interconnected lymphatic and venous vessels. These malformations can occur anywhere in the body, but they are most commonly found in areas rich in lymphatic tissue, such as the head and neck, axilla, mediastinum, and groin1. Fewer than 5% of LVMs are located intra-abdominally, typically arising from the mesentery, retroperitoneum, or greater omentum. Patients with intra-abdominal LVMs may be asymptomatic, but they can also pre-sent with symptoms such as acute abdominal pain, chronic discomfort, palpable masses, or progressive abdominal distension. The diagnosis of LVMs can be challenging and requires a combination of imaging techniques, including ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI), along with histological con-firmation. This case describes a 24-year-old female who presented to our Emergency Depart-ment with progressive abdominal distension, nausea, and vomiting.
Keywords:
1. Introduction
2. Case Presentation
Follow Up
3. Discussion
Conclusion
Author Contributions
References
- Kalwani, N.M.; Rockson, S.G. Management of lymphatic vascular malformations: A systematic review of the literature. J. Vasc. Surgery: Venous Lymphat. Disord. 2021, 9, 1077–1082. [Google Scholar] [CrossRef] [PubMed]
- Shayesteh, S.; Salimian, K.J.; Fouladi, D.F.; Blanco, A.; Fishman, E.K.; Kawamoto, S. Intra-abdominal lymphangioma: A case report. Radiol. Case Rep. 2021, 16, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Qiu, T.; Yang, M.; Zhou, J.; Gong, X.; Yang, K.; Zhang, Z.; Lan, Y.; Zhang, X.; Zhou, Z.; et al. Clinical characteristics and risk factors for acute abdomen in patients with abdominal lymphatic malformations. J. Vasc. Surgery: Venous Lymphat. Disord. 2024, 13, 101969. [Google Scholar] [CrossRef] [PubMed]
- ISSVA Classification for Vascular Anomalies ©.
- Schacht, V.; Dadras, S.S.; Johnson, L.A.; Jackson, D.G.; Hong, Y.-K.; Detmar, M. Up-Regulation of the Lymphatic Marker Podoplanin, a Mucin-Type Transmembrane Glycoprotein, in Human Squamous Cell Carcinomas and Germ Cell Tumors. Am. J. Pathol. 2005, 166, 913–921. [Google Scholar] [CrossRef]
- Makni, A.; Chebbi, F.; Fetirich, F.; Ksantini, R.; Bedioui, H.; Jouini, M.; Kacem, M.; Ben Safta, Z. Surgical Management of Intra-Abdominal Cystic Lymphangioma. Report of 20 Cases. World J. Surg. 2012, 36, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Maghrebi, H.; Yakoubi, C.; Beji, H.; Letaief, F.; Megdich, S.; Makni, A.; Boukriba, S.; Frikha, W.; Ayadi, M.; Kacem, M. Intra-abdominal cystic lymphangioma in adults: A case series of 32 patients and literature review. Ann. Med. Surg. 2022, 81, 104460. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, A.H.; Mulliken, J.B.; Fishman, S.J.; Quatrano, N.A.; Zurakowski, D.; Greene, A.K. Lymphatic Malformation. J. Craniofacial Surg. 2012, 23, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Morais, F.P.; Carvalho, I.R.; Luppi, A.M.; Dornelas, B.C. Child Abdominal Distension Due to a Massive Retroperitoneal Lymphangioma: A Cyto-Histopathological and Clinical Correlation. Cureus 2024, 16, e72874. [Google Scholar] [CrossRef] [PubMed]
- Elbaaly, H.; Piché, N.; Rypens, F.; Kleiber, N.; Lapierre, C.; Dubois, J. Intra-abdominal lymphatic malformation management in light of the updated International Society for the Study of Vascular Anomalies classification. Pediatr. Radiol. 2021, 51, 760–772. [Google Scholar] [CrossRef] [PubMed]
- Abebe, D.M.; Nureta, T.H.; Gima, T. A rare case of huge intra-abdominal cystic lymphangioma arising from rectovesical pouch; a case report. Int. J. Surg. Case Rep. 2023, 106, 108275. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



