Submitted:
10 August 2025
Posted:
13 August 2025
You are already at the latest version
Abstract
Introduction: Cervical disc diseases (CDD) are a significant cause of disability and diminished quality of life globally, with prevalence increasing with age. Two common surgical interventions for symptomatic CDD patients who do not respond to conservative treatments are Anterior Cervical Discectomy and Fusion (ACDF) and Cervical Disc Arthroplasty (CDA). While ACDF is more established and has a more extended history of use, CDA has been gaining popularity due to its motion-preserving benefits and comparable, if not superior, long-term outcomes. This study aims to compare these two procedures using a comprehensive dataset of 97,999 patients, focusing on patient demographics, complications, costs, length of hospital stay, and mortality rates to contribute valuable insights that can inform clinical practice and healthcare policy.
Methods: In this study, data were sourced from the Nationwide Inpatient Sample (NIS) database, covering the period from January 1st, 2016, to December 31st, 2019. The dataset comprised 97,999 patients, with 85,584 undergoing ACDF and 11,415 CDA. Patients were identified using ICD-10 codes, with exclusions for non-elective admissions and surgeries performed prior to admission. Statistical analyses, including crosstabs and t-tests, were conducted, with a significance level of p < 0.05. Propensity score matching was utilized to control selection bias, resulting in a refined cohort of 11,415 matched pairs. Comorbidities and clinical outcomes were analyzed using the NIS dataset, including mortality, length of stay, complications, and hospitalization costs. Results: The study observed a significant increase in the utilization of CDA surgeries compared to ACDF from 2016 to 2019. ACDF patients were older (55.6 vs. 47.2 years, P< 0.001) and more likely to have Medicare coverage (33.9% vs. 10.7%, P< 0.001). Comorbidities such as hypertension, dyslipidemia, and diabetes mellitus were more prevalent in ACDF patients (P< 0.001). Propensity score matching balanced both groups, confirming comparable demographic and comorbidity profiles, with no significant differences in major conditions like hypertension (P=0.59) and dyslipidemia (P=0.93). Hospitalization outcomes revealed a slightly longer length of stay for ACDF (1.39 vs. 1.32 days, P< 0.001), while CDA incurred higher mean charges ($82,431 vs. $58,472, P< 0.001). Postoperatively, ACDF patients experienced more dysphagia (4.90% vs. 3.60%, P< 0.001), venous thromboembolism (0.13% vs. 0.04%, P=0.03), and sepsis (0.04% vs. 0.00%, P=0.03). Cervical spinal cord injury and urinary tract infections were more frequent in the CDA group (P=0.04 and P=0.02, respectively).
Conclusions: This study highlights a growing trend in favor of CDA, particularly among younger patients and those with private insurance. The advantages of motion preservation, reduced adjacent-segment disease, shorter hospital stays, and lower complication rates make CDA an increasingly viable alternative to traditional ACDF, despite its higher initial costs. These findings align with recent literature, further supporting the adoption of CDA in appropriate patient populations.
Keywords:
cervical disc arthroplasty
; anterior cervical discectomy and fusion
; national inpatient sample
; big data
; NIS
1. Introduction
Cervical disc diseases (CDD) are a leading cause of disabilities and decreased quality of life [1,2,3] worldwide, with prevalence increasing with age [4,5,6]. The related pathologies are varied and highly common in the population [7,8,9,10,11]. Two widespread surgical interventions for symptomatic CDD patients who have failed or are not suitable for conservative treatment are ACDF and the newer, motion-preserving, Cervical Disc Arthroplasty (CDA). The ACDF is currently the most commonly performed procedure due to its extended history of use and a larger body of clinical evidence supporting its effectiveness. However, the popularity of CDA has been rising in recent years, and like ACDF, it can be used for both single-level and multi-level diseases.
Three major drawbacks of ACDFs for single-level disease post-surgery are limited neck mobility, the potential for adjacent segment disease, and longer recovery time. These drawbacks can be addressed with the more expensive CDA procedure [12], which has shown long-term results that are not inferior and even superior to those of ACDF [13,14,15,16,17,18]. Previous studies have attempted to characterize the patient population more likely to undergo the CDA procedure over ACDF for single-level disc disease and compare the inpatient outcomes [12]. These studies show shorter lengths of stay with CDA and highlight that younger patients, patients with private insurance, and patients with higher median household incomes are more likely to undergo this procedure [19,20,21,22].
Although previous studies have utilized the NIS database to compare CDA and ACDF, these investigations were conducted over a decade ago, employed the now outdated ICD-9 coding system, and did not account for advancements in CDA technology. In contrast, our study incorporates the updated ICD-10 coding system, includes a significantly more extensive and robust patient cohort, and reflects technological improvements in CDA, providing a more accurate and contemporary comparison. Our study utilizes a comprehensive dataset of 97,999 patients to compare ACDF with CDA. The primary objective is to contribute to the ongoing discourse regarding the efficacy of CDA by elucidating its practical implications, including patient demographics, complications, costs, length of hospital stay, and mortality rates. This investigation aims to provide valuable insights that can guide policymakers and ultimately enhance patient-centered care.
2. Methods
2.1. Data Source
This investigation employed data from the National Inpatient Sample (NIS), a nationally representative database developed by the Agency for Healthcare Research and Quality (AHRQ) as part of the Healthcare Cost and Utilization Project (HCUP). The NIS is the largest publicly accessible, all-payer inpatient healthcare dataset in the United States, systematically sampling approximately 20% of all hospital discharges from HCUP-affiliated institutions. This sampling framework encompasses roughly 7 million unweighted admissions annually and, when adjusted using the discharge-level sampling weights provided by HCUP, allows for the generation of robust national estimates and comprehensive epidemiological assessments.
For the present study, data spanning January 1, 2016, through December 31, 2021, were analyzed, representing the most recent and complete period available at the time of analysis. Within the NIS, each discharge record—referred to as a “case”—is assigned a statistical weight, with each weighted record corresponding to approximately five actual inpatient encounters nationwide. This methodology enables precise extrapolation to the national inpatient population, thereby enhancing both the external validity and statistical rigor of the study’s findings.
2.2. Cohort Definition and Selection Criteria
The National Inpatient Sample (NIS) database was queried for the period 2016–2021 to identify adult patients (aged ≥18 years) who underwent single-level anterior cervical discectomy and fusion (ACDF) or cervical disc arthroplasty (CDA). Procedural identification was performed using International Classification of Diseases, Tenth Revision (ICD-10) procedure codes specific to these operations, as detailed in the Appendix. The final cohort comprised 97,999 patients, including 85,584 who underwent ACDF and 11,415 who underwent CDA.
Patients with non-elective admissions or those who had undergone surgery prior to the index hospitalization were excluded. In addition, cases with incomplete or inconsistent records—such as missing procedural codes, demographic variables, or other critical data—were removed to preserve the accuracy and reliability of statistical analyses. This exclusion strategy minimized the potential for bias arising from incomplete datasets and ensured methodological rigor.
2.3. Outcome Variables (End Points)
Procedural identification was based on International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) codes specific to single-level ACDF and CDA, as detailed in the Table 1. Comorbidities were identified through review of patient-specific ICD-10-CM diagnosis codes.
Primary outcomes included in-hospital mortality, length of stay, total hospitalization costs, and perioperative complication rates. Complications were identified using ICD-10 codes and encompassed dysphagia, postoperative anemia due to blood loss, cervical spinal cord injury, urinary tract infection, acute renal failure, pneumonia, blood transfusion requirement, venous thromboembolism, pulmonary edema, ileus, feeding tube placement, dural tear, sepsis, pulmonary embolism, and mortality. These definitions were applied consistently across both groups to ensure methodological uniformity and comparability of results.
2.4. Statistical Analysis
All statistical analyses were conducted using SPSS version 26 (IBM Corp., Armonk, NY, USA) and MATLAB 2024 (MathWorks, Natick, MA, USA). Categorical variables were compared using Pearson’s χ² test, and continuous variables were evaluated using independent-sample t-tests. A two-tailed p-value < 0.05 was considered statistically significant.
To minimize selection bias and control for confounding inherent in observational studies, propensity score matching (PSM) was employed. This method facilitated the creation of statistically comparable cohorts of patients undergoing anterior cervical discectomy and fusion (ACDF) or cervical disc arthroplasty (CDA) by matching individuals on key demographic, hospital-related, and clinical characteristics. PSM enhances the validity of causal inferences by approximating the balance achieved in randomized controlled trials, thereby improving the robustness and reliability of comparative analyses.
Propensity scores were estimated using a multivariable logistic regression model incorporating 34 covariates spanning three domains: (1) Hospital characteristics – hospital size, location (urban vs. rural), teaching status, geographic region, and total annual discharges. (2) Demographic and socioeconomic factors – patient location (urban vs. rural classification), median household income quartile, race, age, and primary payer status (Medicare, Medicaid, private insurance, self-pay, or other). (3) Preoperative comorbidities – 24 conditions including hypertension, dyslipidemia, obstructive sleep apnea, chronic anemia, alcohol abuse, osteoporosis, neurodegenerative disorders (Parkinson’s disease, Alzheimer’s disease, and dementia), chronic kidney disease, congestive heart failure, chronic lung disease, diabetes mellitus, inflammatory bowel disease, liver disease, obesity, fibromyalgia, thyroid disorders, prior myocardial infarction, peripheral vascular disease, prior cerebrovascular accident, any neoplasm, neoplasms of lymphoid and hematopoietic tissue, and any other recorded preoperative health condition.
Matching was performed using MATLAB, yielding two final cohorts of 11,415 patients each with comparable baseline characteristics. Matching criteria included hospital size, patient location (urban–rural classification), median household income quartile, hospital region, comorbidity profile, and total number of hospital discharges within the NIS dataset.
2.5. Ethical Consideration
This study received exempt status from the Institutional Review Board (IRB) owing to the fully de-identified nature of the National Inpatient Sample (NIS) dataset, in accordance with ethical standards for research involving human subjects. Artificial intelligence (AI) tools were employed exclusively for linguistic refinement, including improvements in clarity, grammatical precision, and stylistic coherence. These tools were not used for data analysis, statistical computation, or content generation, thereby ensuring the preservation of the study’s scientific integrity and methodological rigor.
3. Results
Over the past few years, cervical disc arthroplasty (CDA) has been used more often compared to anterior cervical discectomy and fusion (ACDF), as shown in Figure 1. From 2016 to 2019, the share of CDA among all CDA and ACDF procedures steadily increased, with the trend reaching statistical significance (p = 0.001). This rise reflects a growing preference for CDA in suitable patients, likely influenced by advances in technology, supportive clinical evidence, and increasing surgeon experience with the procedure.
Table 2 compares 85,584 patients who underwent anterior cervical discectomy and fusion (ACDF) with 11,415 patients who underwent cervical disc arthroplasty (CDA), detailing procedure distribution, demographic characteristics, and primary expected payer categories. Patients undergoing ACDF were, on average, significantly older than those undergoing CDA (55.6 vs. 47.2 years, p < 0.001). The proportion of female patients was similar between the groups (51.7% for ACDF vs. 52.5% for CDA, p = 0.108). Differences in primary payer status closely reflected the age disparity between cohorts. Medicare was the primary expected payer for 33.9% of ACDF patients compared with only 10.7% of CDA patients (p < 0.001), consistent with the older age profile of the ACDF group. Conversely, private insurance coverage was more prevalent among CDA patients (64.9%) than ACDF patients (44.5%) (p < 0.001), reflecting the younger, working-age demographic more commonly undergoing disc arthroplasty.
Table 3 presents a comparative analysis of preoperative comorbidities between patients undergoing anterior cervical discectomy and fusion (ACDF) and those undergoing cervical disc arthroplasty (CDA). The table details the prevalence of each condition and the statistical significance of differences between cohorts. Overall, ACDF patients exhibited a higher burden of comorbidities compared with CDA patients. Notably, the prevalence of hypertension (43.7% vs. 25.1%), dyslipidemia (30.0% vs. 17.3%), and diabetes mellitus (19.5% vs. 9.6%) was significantly greater in the ACDF group (p < 0.001 for all). Similarly, chronic lung disease (8.0% vs. 3.2%) and chronic kidney disease (3.8% vs. 1.1%) were more common among ACDF patients, with both differences reaching high statistical significance (p < 0.001). These patterns are consistent with the older mean age of the ACDF cohort and suggest that patients selected for CDA are generally younger and have fewer chronic health conditions, potentially reflecting stricter surgical candidacy criteria for arthroplasty compared with fusion.
To address potential selection bias and baseline differences in preoperative comorbidity profiles, a propensity score–matched (PSM) analysis was performed. This statistical technique balances observed covariates by pairing patients with comparable probabilities of undergoing either anterior cervical discectomy and fusion (ACDF) or cervical disc arthroplasty (CDA), thereby minimizing confounding and enhancing the validity of comparative analyses. By emulating the balance achieved through random assignment, PSM improves the reliability of conclusions drawn from observational data.
Following matching, the final analysis included 11,415 patients in each cohort, ensuring a balanced distribution of demographic and clinical characteristics. As shown in Table 4, no statistically significant differences were observed between groups across the evaluated parameters, confirming the effectiveness of the matching process.
Post-matching comparisons demonstrated that the cohorts were similar in mean age (47.3 years for ACDF vs. 47.2 years for CDA, p = 0.36) and sex distribution (52.1% female for ACDF vs. 52.5% female for CDA, p = 0.62). Primary expected payer status was also comparable, with private insurance—including health maintenance organizations (HMOs)—being the most common coverage type (64.5% for ACDF vs. 64.9% for CDA, p = 0.41). Likewise, the prevalence of common comorbidities such as hypertension (24.7% vs. 25.1%, p = 0.59) and dyslipidemia (17.2% vs. 17.3%, p = 0.93) showed no significant differences. Similar parity was observed across a range of additional comorbidities, underscoring that the matched cohorts were well-balanced and suitable for valid outcome comparisons.
Table 5 summarizes hospitalization outcomes for anterior cervical discectomy and fusion (ACDF) and cervical disc arthroplasty (CDA) following propensity score matching. Both procedures were associated with short postoperative hospital stays; however, CDA demonstrated a statistically significant yet clinically modest reduction in length of stay compared with ACDF (1.32 vs. 1.39 days, p < 0.001). This difference may reflect procedural factors such as less invasive exposure, more rapid postoperative mobilization, or differences in perioperative management protocols favoring CDA. Despite the shorter hospitalization duration, CDA was associated with substantially higher total hospital charges ($82,431 vs. $58,472, p < 0.001). This cost disparity likely reflects increased expenditures related to surgical instrumentation, implant technology, and potentially higher reimbursement rates for arthroplasty procedures. These findings underscore the need to balance clinical advantages with economic considerations when selecting the optimal surgical strategy for cervical degenerative pathology.
Table 6 compares postoperative complication rates between patients undergoing anterior cervical discectomy and fusion (ACDF) and those receiving cervical disc arthroplasty (CDA) after propensity score matching. Dysphagia occurred more frequently in the ACDF cohort (4.90% vs. 3.60%, p < 0.001), potentially reflecting greater esophageal retraction inherent to the fusion technique. In contrast, cervical spinal cord injury, although rare, was observed slightly more often in the CDA group (0.30% vs. 0.17%, p = 0.04), which may be related to the technical precision required for prosthesis placement. Urinary tract infections were also more prevalent among CDA patients (0.39% vs. 0.22%, p = 0.02), possibly due to variations in perioperative management or urinary catheter utilization. ACDF patients demonstrated higher rates of perioperative blood transfusion (0.13% vs. 0.00%, p = 0.01) and venous thromboembolism (0.13% vs. 0.04%, p = 0.03), findings that may be attributable to greater intraoperative blood loss and longer postoperative immobilization. Additional complications—such as sepsis (0.04% vs. 0.00%, p = 0.03), pulmonary embolism (0.04% vs. 0.00%, p = 0.03), and feeding tube placement (0.08% vs. 0.00%, p = 0.01)—were also more common in the ACDF group, potentially reflecting the increased physiological stress and recovery demands associated with fusion procedures.
4. Discussion
Anterior cervical discectomy and fusion (ACDF) is a well-established surgical intervention for patients with severe or refractory cervical spine pathology who have not achieved symptomatic relief through conservative management [23]. While ACDF reliably decompresses the spinal cord and restores intervertebral disc height, the procedure eliminates motion at the fused segment, potentially increasing biomechanical stress on adjacent levels and predisposing to adjacent-segment disease (ASD). Cervical disc arthroplasty (CDA) was developed as a motion-preserving alternative designed to maintain cervical spine biomechanics, reduce stress transfer to adjacent segments, and thereby mitigate the risk of ASD [24,25]. Despite promising biomechanical and clinical rationale, the question of whether CDA offers superior long-term outcomes compared with ACDF remains the subject of ongoing debate [26].
This study leveraged a large, propensity score–matched cohort from the National Inpatient Sample (NIS) to evaluate the epidemiological trends and complication profiles of anterior cervical discectomy and fusion (ACDF) versus cervical disc arthroplasty (CDA). Our findings demonstrate a marked increase in CDA utilization over the past decade, consistent with previously published reports. One study [27] observed an increase in CDA procedures from 4.0% to 14.2% between 2010 and 2018, followed by a plateau from 2018 to 2021. Similarly, Singh BS et al. [28] documented a 25.25% rise in ACDF procedures from 2011 to 2014 and an extraordinary 654.24% increase in CDA procedures from 2011 to 2019, with subsequent stabilization in the rates of both interventions. The growing adoption of CDA over ACDF is likely influenced by earlier evidence suggesting superior postoperative functional mobility with arthroplasty, potentially mitigating biomechanical stress on adjacent segments and lowering the incidence of adjacent-segment degeneration [29,30].
In our cohort, patients undergoing cervical disc arthroplasty (CDA) were generally younger and demonstrated fewer comorbidities. CDA is frequently selected for younger individuals with preserved baseline segmental motion and without advanced degenerative changes of the cervical spine, as it offers the potential for greater postoperative mobility and segmental flexibility compared with anterior cervical discectomy and fusion (ACDF) [12]. The procedure’s success relies on the structural integrity of adjacent facet joints and spinal ligaments to maintain stability, rendering it less suitable for patients with poor bone quality, advanced spondylosis, or multi-level disc pathology. Older patients, who are more likely to present with comorbidities such as diabetes mellitus, hypertension, and dyslipidemia, often derive greater benefit from fusion procedures, which provide definitive stabilization of diseased segments [31,32]. These relative indications and contraindications help explain the higher prevalence of ACDF among older individuals with myelopathy and advanced disc degeneration in our study population.
Overall, cervical disc arthroplasty (CDA) demonstrated complication rates comparable to or lower than anterior cervical discectomy and fusion (ACDF), with overall incidences of 5.81% and 7.29%, respectively. ACDF was associated with a higher prevalence of dysphagia (4.90% vs. 3.60%) and a greater need for perioperative blood transfusion (0.13% vs. 0.00%). Conversely, CDA patients experienced slightly higher rates of cervical spinal cord injury (0.30% vs. 0.17%) and urinary tract infections. The existing literature presents mixed findings: several studies have reported fewer adverse events following CDA [33,34], whereas others have noted either no difference or higher complication rates compared with ACDF [35,36]. Given the similarities in surgical approach, both procedures demonstrated comparable rates of approach-related complications.
A recent systematic review and meta-analysis found that CDA was associated with a significantly lower incidence of secondary surgeries and adverse events compared with ACDF, without significant differences in neurological success [37]. Similarly, another study reported no statistically significant differences in the incidence of spinal cord injury or other major complications between the two techniques [38].
Although the present analysis identified statistically significant differences in certain complication rates between CDA and ACDF, the absolute rates were low for both procedures. These findings suggest that while statistical differences exist, their clinical impact may be limited. Future research should aim to determine whether these differences translate into meaningful variations in long-term patient outcomes, healthcare utilization, and quality of life.
In this study, a significantly greater proportion of cervical disc arthroplasty (CDA) patients (64.9%) were covered by private insurance compared with anterior cervical discectomy and fusion (ACDF) patients (44.5%). Similar trends have been reported in previous analyses. For example, a study utilizing the National Inpatient Sample (NIS) from 2006 to 2013 found that 66.2% of CDA patients had private insurance versus 55.4% of ACDF patients [19]. This disparity likely reflects differences in patient age and eligibility, as younger individuals—who are more likely to have private insurance—are also more likely to meet selection criteria for CDA. In contrast, older patients, particularly those covered by Medicare, may be less frequently considered for arthroplasty due to the presence of advanced degenerative changes or other contraindications. Additionally, variation in insurance coverage policies, including reimbursement rates and authorization practices, may contribute to the observed differences in payer distribution.
In terms of resource utilization, CDA patients in our cohort had a modestly shorter mean length of stay compared with ACDF patients (1.32 vs. 1.39 days) yet incurred substantially higher total hospital charges ($82,431 vs. $58,472). These findings are consistent with prior studies [19,39] that also demonstrated reduced length of stay for CDA relative to ACDF, while highlighting the potential impact of device costs, surgical instrumentation, and reimbursement structures on total expenditures.
The higher costs associated with cervical disc arthroplasty (CDA) compared with anterior cervical discectomy and fusion (ACDF) are primarily attributable to the increased expense of implants and surgical instrumentation required for arthroplasty. CDA implants, incorporating motion-preserving technology, are generally more costly than the devices used in ACDF [40,41]. A study published in World Neurosurgery reported that the mean supply cost for CDA was approximately $9,532, compared with $4,173 for ACDF, with the majority of this discrepancy attributable to the higher price of disc replacement implants [40]. Beyond implant costs, total intraoperative expenses are also greater for CDA; the same study found mean intraoperative costs of $12,026 for CDA versus $6,776 for ACDF. This difference reflects not only the increased cost of implants but also the additional operative time and resources required for arthroplasty [40].
Differences in hospital reimbursement policies further contribute to the economic disparity between CDA and ACDF. Reimbursement for CDA is often influenced by private insurance coverage, with some payers limiting approval due to the higher upfront cost and ongoing uncertainty regarding long-term benefits. These reimbursement structures can influence surgical decision-making and patient access to CDA, particularly for individuals with limited insurance coverage or financial constraints.
Economic trends further highlight the growing financial burden associated with CDA. Between 2009 and 2019, the mean total hospital charges for elective CDA increased by 73%, while the mean total cost for index hospital admissions rose by 26% [41]. Notably, this cost escalation has not been matched by a proportional rise in reimbursements, resulting in higher out-of-pocket expenses for patients and increased financial strain on healthcare systems. These findings underscore the importance of considering the long-term economic implications of CDA relative to ACDF when evaluating its broader adoption in clinical practice.
The shorter length of stay (LOS) observed in cervical disc arthroplasty (CDA) patients may reflect more standardized perioperative care protocols and implant-specific surgical workflows. In contrast, the higher costs associated with CDA are likely attributable to the advanced technology, specialized implants, and longer operative times required for these procedures. In resource-limited settings, such elevated costs can place substantial strain on healthcare budgets, potentially restricting the availability of CDA. Consequently, anterior cervical discectomy and fusion (ACDF) is often favored in such environments, as it demonstrates greater cost-effectiveness across various willingness-to-pay thresholds [42]. The financial burden associated with CDA may also disproportionately limit access for patients from lower socioeconomic backgrounds or those without comprehensive insurance coverage [12]. Future studies should investigate the long-term cost-effectiveness of CDA and ACDF, incorporating revision rates, patient-reported outcomes, indirect costs, and broader measures of healthcare utilization.
Accurate determination of indications and patient eligibility is essential when selecting between CDA and ACDF. Inappropriate selection for CDA can compromise surgical outcomes. For example, if the posterior longitudinal ligament is divided during the removal of posterior osteophytes, segmental fusion is generally preferred over disc replacement to avoid iatrogenic instability [43]. This underscores the importance of adhering to established surgical principles and tailoring procedural choice to individual anatomical and pathological characteristics.
CDA is most commonly indicated for patients with single- or two-level cervical disc disease between the C3 and C7 levels. Regulatory approval for CDA is based on clinical trials demonstrating non-inferiority to ACDF, with evidence indicating that, in appropriately selected patients, CDA can provide comparable or superior clinical and functional outcomes while preserving segmental motion [44,45]. Proper patient selection is critical, with absolute contraindications including severe osteoporosis, active infection, and significant cervical instability due to the heightened risk of implant failure and poor postoperative outcomes. Relative contraindications—such as segmental kyphosis or prior cervical spine surgery—require individualized assessment, as emerging evidence suggests that CDA may remain a viable option in select patients with outcomes comparable to standard candidates [46,47]. While preoperative segmental mobility has historically been regarded as a key criterion for CDA candidacy, recent studies suggest that even patients with reduced baseline mobility can achieve meaningful postoperative improvements in pain relief and functional status, challenging the traditional reliance on mobility as a strict determinant [48].
Collectively, these findings highlight the necessity of a nuanced, evidence-based approach to surgical decision-making. Patient-specific planning, careful evaluation of anatomical and biomechanical factors, and ongoing research into long-term cost-effectiveness, functional outcomes, and quality of life are essential to optimizing treatment strategies for cervical degenerative disease.
This study acknowledges several limitations inherent to its methodological approach, which is based on the use of a broad set of ICD-10 procedure and diagnosis codes applied to a large administrative dataset. While this strategy enables a macro-level assessment of national trends and facilitates the analysis of a substantial sample size—approximately 98,000 single-level CDA and ACDF cases—it does not permit granular, patient-level clinical detail. This reflects an inherent trade-off between the depth of individual patient information and the statistical power afforded by large-scale, population-based analyses. Additionally, the cost estimates reported in the National Inpatient Sample (NIS) are derived from hospital-specific cost-to-charge ratios, which may overestimate actual procedural expenses. However, these ratios undergo internal validation by the Agency for Healthcare Research and Quality, supporting their use in comparative economic analyses.
5. Conclusions
In conclusion, this study demonstrates a clear and sustained increase in the utilization of cervical disc arthroplasty (CDA), driven by younger patient demographics, higher rates of private insurance coverage, and the procedural advantages of motion preservation and reduced risk of adjacent-segment disease. Although CDA is associated with higher initial costs, its shorter hospital stays and lower complication rates make it an attractive option for appropriately selected patients. These findings align with current literature and support the growing adoption of CDA as a viable alternative to traditional anterior cervical discectomy and fusion (ACDF).
List of Abbreviations (A-Z)
| ACDF: | Anterior Cervical Discetomy and Fusion |
| CDA: | Cervical Disc Arthroplasty |
| HCUP: | Healthcare Cost and Utilization Project |
| ICD-10: | International Classification of Diseases, 10th Revision |
| NIS: | Nationwide Inpatient Sample |
| SPSS: | Statistical Package for the Social Sciences |
Author Contributions
Conceptualization, Assil Mahamid and David Maman; Data curation, Assil Mahamid and Ali Yassin; Formal analysis, David Maman; Investigation, Assil Mahamid and Ali Yassin; Methodology, Assil Mahamid and David Maman; Project administration, Assil Mahamid, David Maman and Hadar Gan-Or; Resources, Yaron Berkovich and Eyal Behrbalk; Software, Assil Mahamid and Amit Keren; Supervision, Yaron Berkovich and Eyal Behrbalk; Validation, Marah Hodruj and Hadar Gan-Or; Visualization, Saleem Samara; Writing – original draft, Assil Mahamid, David Maman and Dan Fishman; Writing – review & editing, Marah Hodruj, Amit Keren and Saleem Samara.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the complete anonymization of patient data, as ensured by the standardized methods developed by the Healthcare Cost and Utilization Project (HCUP).
Informed Consent Statement
Not applicable.
Data Availability Statement
Restrictions apply to the availability of these data. Data were obtained from HCUP and are available [https://hcup-us.ahrq.gov/] with the permission of HCUP.
Acknowledgments
The authors wish to acknowledge the use of artificial intelligence (AI) tools solely for the purpose of revising and improving the clarity, grammar, and style of the English language in this manuscript. The AI tools were not employed for data analysis, the interpretation of results, or the generation of original scientific content. The responsibility for the scientific integrity, accuracy, and interpretation of the manuscript remains solely with the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Safiri S, Kolahi AA, Hoy D, et al. Global, regional, and national burden of neck pain in the general population, 1990-2017: systematic analysis of the Global Burden of Disease Study 2017. BMJ. Published online March 26, 2020:m791.
- Yang L, Chen J, Yang C, et al. Cervical Intervertebral Disc Degeneration Contributes to Dizziness: A Clinical and Immunohistochemical Study. World Neurosurgery. 2018;119:e686-e693. [CrossRef]
- Cohen SP, Hooten WM. Advances in the diagnosis and management of neck pain. BMJ. Published online August 14, 2017:j3221. [CrossRef]
- Mesregah MK, Repajic M, Mgbam P, Fresquez Z, Wang JC, Buser Z. Trends and patterns of cervical degenerative disc disease: an analysis of magnetic resonance imaging of 1300 symptomatic patients. Eur Spine J. 2022;31(10):2675-2683. [CrossRef]
- Brinjikji W, Luetmer PH, Comstock B, et al. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. AJNR Am J Neuroradiol. 2015;36(4):811-816. [CrossRef]
- Suzuki A, Daubs MD, Hayashi T, et al. Patterns of Cervical Disc Degeneration: Analysis of Magnetic Resonance Imaging of Over 1000 Symptomatic Subjects. Global Spine Journal. 2018;8(3):254-259. [CrossRef]
- Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J. 2006;15(6):834-848. [CrossRef]
- Genebra CVDS, Maciel NM, Bento TPF, Simeão SFAP, Vitta AD. Prevalence and factors associated with neck pain: a population-based study. Brazilian Journal of Physical Therapy. 2017;21(4):274-280. [CrossRef]
- Woods BI, Hilibrand AS. Cervical Radiculopathy: Epidemiology, Etiology, Diagnosis, and Treatment. Journal of Spinal Disorders & Techniques. 2015;28(5):E251-E259.
- Nouri A, Tetreault L, Singh A, Karadimas SK, Fehlings MG. Degenerative Cervical Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine. 2015;40(12):E675-E693.
- Northover JR, Wild JB, Braybrooke J, Blanco J. The epidemiology of cervical spondylotic myelopathy. Skeletal Radiol. 2012;41(12):1543-1546.
- Ostrov PB, Reddy AK, Ryoo JS, Behbahani M, Mehta AI. Anterior Cervical Discectomy and Fusion Versus Cervical Disc Arthroplasty: A Comparison of National Trends and Outcomes. World Neurosurgery. 2022;160:e96-e110. [CrossRef]
- Sasso WR, Smucker JD, Sasso MP, Sasso RC. Long-term Clinical Outcomes of Cervical Disc Arthroplasty: A Prospective, Randomized, Controlled Trial. Spine. 2017;42(4):209-216.
- Murrey D, Janssen M, Delamarter R, et al. Results of the prospective, randomized, controlled multicenter Food and Drug Administration investigational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease. The Spine Journal. 2009;9(4):275-286. [CrossRef]
- Lavelle WF, Riew KD, Levi AD, Florman JE. Ten-year Outcomes of Cervical Disc Replacement With the BRYAN Cervical Disc: Results From a Prospective, Randomized, Controlled Clinical Trial. Spine. 2019;44(9):601-608.
- Burkus JK, Traynelis VC, Haid RW, Mummaneni PV. Clinical and radiographic analysis of an artificial cervical disc: 7-year follow-up from the Prestige prospective randomized controlled clinical trial: Clinical article. SPI. 2014;21(4):516-528. [CrossRef]
- Hisey MS, Zigler JE, Jackson R, et al. Prospective, Randomized Comparison of One-level Mobi-C Cervical Total Disc Replacement vs. Anterior Cervical Discectomy and Fusion: Results at 5-year Follow-up. Int J Spine Surg. 2016;10:10. [CrossRef]
- Nunley PD, Hisey M, Smith M, Stone MB. Cervical Disc Arthroplasty vs Anterior Cervical Discectomy and Fusion at 10 Years: Results From a Prospective, Randomized Clinical Trial at 3 Sites. Int J Spine Surg. 2023;17(2):230-240. [CrossRef]
- Saifi C, Fein AW, Cazzulino A, et al. Trends in resource utilization and rate of cervical disc arthroplasty and anterior cervical discectomy and fusion throughout the United States from 2006 to 2013. The Spine Journal. 2018;18(6):1022-1029. [CrossRef]
- Lu Y, McAnany SJ, Hecht AC, Cho SK, Qureshi SA. Utilization Trends of Cervical Artificial Disc Replacement After FDA Approval Compared With Anterior Cervical Fusion: Adoption of New Technology. Spine. 2014;39(3):249-255. [CrossRef]
- Nesterenko SO, Riley LH, Skolasky RL. Anterior Cervical Discectomy and Fusion Versus Cervical Disc Arthroplasty: Current State and Trends in Treatment for Cervical Disc Pathology. Spine. 2012;37(17):1470-1474.
- Kumar C, Dietz N, Sharma M, Wang D, Ugiliweneza B, Boakye M. Long-Term Comparison of Health Care Utilization and Reoperation Rates in Patients Undergoing Cervical Disc Arthroplasty and Anterior Cervical Discectomy and Fusion for Cervical Degenerative Disc Disease. World Neurosurgery. 2020;134:e855-e865. [CrossRef]
- Chen CM, Yang JJ, Wu CC. Cervical Disc Arthroplasty (CDA) versus Anterior Cervical Discectomy and Fusion (ACDF) for Two-Level Cervical Disc Degenerative Disease: An Updated Systematic Review and Meta-Analysis. J Clin Med. 2024 May 29;13(11):3203. [CrossRef]
- Demetriades AK, Ringel F, Meyer B (2014) Cervical disc arthroplasty: a critical review and appraisal of the latest available evidence. Adv Tech Stand Neurosurg 41:107–129.
- Fay LY, Huang WC, Tsai TY et al (2014) Differences between arthroplasty and anterior cervical fusion in two-level cervical degenerative disc disease. Eur Spine J 23(3):627–634.
- Rao, MJ., Nie, SP., Xiao, BW. et al. Cervical disc arthroplasty versus anterior cervical discectomy and fusion for treatment of symptomatic cervical disc disease: a meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg 135, 19–28 (2015). [CrossRef]
- Ratnasamy PP, Rudisill KE, Maloy GC, Grauer JN. Cervical Disc Arthroplasty Usage Has Leveled Out From 2010 to 2021. Spine (Phila Pa 1976). 2023 Oct 15;48(20):E342-E348. [CrossRef]
- Singh M, Balmaceno-Criss M, Anderson G, Parhar K, Daher M, Gregorczyk J, Liu J, McDonald CL, Diebo BG, Daniels AH. Anterior cervical discectomy and fusion versus cervical disc arthroplasty: an epidemiological review of 433,660 surgical patients from 2011 to 2021. Spine J. 2024 Aug;24(8):1342-1351. [CrossRef]
- Nunley PD, Kerr EJ 3rd, Cavanaugh DA, Utter PA, Campbell PG, Wadhwa R, Frank KA, Marshall KE, Stone MB. Adjacent Segment Pathology After Treatment With Cervical Disc Arthroplasty or Anterior Cervical Discectomy and Fusion, Part 1: Radiographic Results at 7-Year Follow-Up. Int J Spine Surg. 2020 Jun 30;14(3):269-277.
- Xu S, Liang Y, Zhu Z, Qian Y, Liu H. Adjacent segment degeneration or disease after cervical total disc replacement: a meta-analysis of randomized controlled trials. J Orthop Surg Res. 2018 Oct 3;13(1):244. [CrossRef]
- Qureshi SA, Koehler SM, Lu Y, Cho S, Hecht AC. Utilization trends of cervical artificial disc replacement during the FDA investigational device exemption clinical trials compared to anterior cervical fusion. J Clin Neurosci. 2013 Dec;20(12):1723-6. [CrossRef]
- Lu Y, McAnany SJ, Hecht AC, Cho SK, Qureshi SA. Utilization trends of cervical artificial disc replacement after FDA approval compared with anterior cervical fusion: adoption of new technology. Spine (Phila Pa 1976). 2014 Feb 1;39(3):249-55. [CrossRef]
- Coric D, Cassis J, Carew JD, Boltes MO. Prospective study of cervical arthroplasty in 98 patients involved in 1 of 3 separate investigational device exemption studies from a single investigational site with a minimum 2-year follow-up. Clinical article. J Neurosurg Spine. 2010 Dec;13(6):715-21. [CrossRef]
- Zou S, Gao J, Xu B, Lu X, Han Y, Meng H. Anterior cervical discectomy and fusion (ACDF) versus cervical disc arthroplasty (CDA) for two contiguous levels cervical disc degenerative disease: a meta-analysis of randomized controlled trials. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2016. Epub 2016/06/18. [CrossRef]
- Heller JG, Sasso RC, Papadopoulos SM, Anderson PA, Fessler RG, Hacker RJ, Coric D, Cauthen JC, Riew DK. Comparison of BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion: clinical and radiographic results of a randomized, controlled, clinical trial. Spine (Phila Pa 1976).
- 36 Anderson PA, Sasso RC, Riew KD. Comparison of adverse events between the Bryan artificial cervical disc and anterior cervical arthrodesis. Spine (Phila Pa 1976). 2008 May 20;33(12):1305-12. [CrossRef]
- Quinto ES Jr, Paisner ND, Huish EG Jr, Senegor M. Ten-Year Outcomes of Cervical Disc Arthroplasty Versus Anterior Cervical Discectomy and Fusion : A Systematic Review With Meta-Analysis. Spine (Phila Pa 1976). 2024 Apr 1;49(7):463-469. [CrossRef]
- Abdelmalek G, Uppal H, Coban D, Patel N, Changoor S, Sahai N, Sinha K, Hwang K, Emami A. Is cervical disc arthroplasty an effective treatment option for patients with cervical spondylotic myelopathy? A matched cohort analysis compared to anterior cervical discectomy and fusion. Spine J. 2024 Nov 27:S1529-9430(24)01156-2. [CrossRef]
- Nunna RS, Ryoo JS, Ostrov PB, Patel S, Godolias P, Daher Z, Price R, Chapman JR, Oskouian RJ. Single-level cervical disc replacement (CDR) versus anterior cervical discectomy and fusion (ACDF): A Nationwide matched analysis of complications, 30- and 90-day readmission rates, and cost. World Neurosurg X. 2023 Oct 18;21:100242. [CrossRef]
- Leibold A, Glener S, Sarikonda A, Sami A, Self DM, Quraishi D, Ali DM, Isch EL, Heller J, Jallo J, Prasad SK, Sharan A, Vaccaro AR, Harrop J, Sivaganesan A. What is the True Cost of Motion Preservation? A Time-Driven Activity-Based Cost Analysis of Anterior Cervical Discectomy and Fusion versus Disc Replacement. World Neurosurg. 2024 Dec;192:e506-e512. [CrossRef]
- Du JY, Shafi K, Blackburn CW, Kim HJ, Iyer S, Qureshi S, Marcus RE, Albert TJ. Trends in costs, reimbursements, and surgeon payments for cervical disc arthroplasty cost of care from 2009 to 2019. J Neurosurg Spine. 2023 Jul 14;39(5):690-699. [CrossRef]
- Heijdra Suasnabar JM, Vleggeert-Lankamp CLA, Goedmakers CMW, de Vries F, Arts MP, van den Akker-van Marle ME. Cost effectiveness of implanting a prosthesis after anterior cervical discectomy for radiculopathy: results of the NECK randomized controlled trial. Spine J. 2023 Jun;23(6):851-858.
- Denaro V, Papalia R, Denaro L, Di Martino A, Maffulli N. Cervical spinal disc replacement. J Bone Joint Surg Br. 2009 Jun;91(6):713-9. [CrossRef]
- Bydon, M., Michalopoulos, G. D., Alvi, M. A., Goyal, A., & Abode-Iyamah, K. (2021). Cervical Total Disc Replacement: Food and Drug Administration-Approved Devices. Neurosurgery clinics of North America, 32(4), 425–435.
- Alves Ó. L. (2021). Cervical Total Disc Replacement: Expanded Indications. Neurosurgery clinics of North America, 32(4), 437–448. [CrossRef]
- Patel, N., Abdelmalek, G., Coban, D., Changoor, S., Sinha, K., Hwang, K., & Emami, A. (2024). Should patient eligibility criteria for cervical disc arthroplasty (CDA) be expanded? A retrospective cohort analysis of relatively contraindicated patients undergoing CDA. The spine journal : official journal of the North American Spine Society, 24(2), 210–218. [CrossRef]
- Auerbach, J. D., Jones, K. J., Fras, C. I., Balderston, J. R., Rushton, S. A., & Chin, K. R. (2008). The prevalence of indications and contraindications to cervical total disc replacement. The spine journal : official journal of the North American Spine Society, 8(5), 711–716. [CrossRef]
- Tu, T. H., Lee, C. Y., Kuo, C. H., Wu, J. C., Chang, H. K., Fay, L. Y., Huang, W. C., & Cheng, H. (2019). Cervical disc arthroplasty for less-mobile discs. Journal of neurosurgery. Spine, 31(3), 310–316. [CrossRef]
Figure 1.
Annual Proportion of Cervical Disc Replacement Surgeries Relative to Total Disc Arthroplasty and ACDF Procedures (2016–2019).
Figure 1.
Annual Proportion of Cervical Disc Replacement Surgeries Relative to Total Disc Arthroplasty and ACDF Procedures (2016–2019).
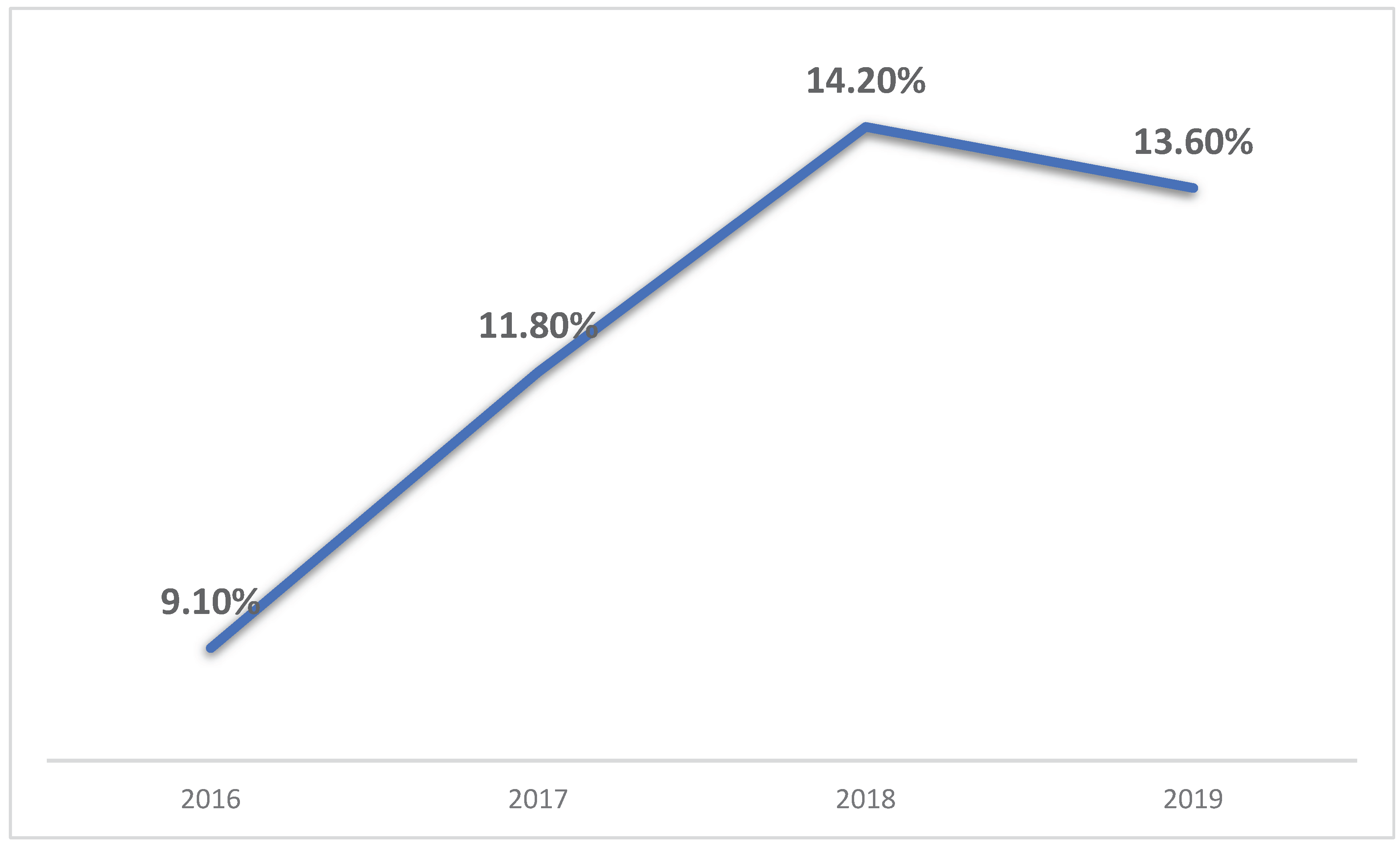

Table 1.
ICD-10 and Procedure Codes Used for Case Selection and Variable Definition.
| Category | ICD 10 CODES |
|---|---|
| Cervical Disc Arthroplasty (CDA) | 0RR30JZ, 0RR20JZ |
| Anterior Cervical Discectomy and Fusion (ACDF) | 0RG10A0, 0RG10A1, 0RG10A4, 0RG10J0, 0RG10J1, 0RG10J4 |
| Heart Failure | I5021, I5031, I5033, I5041, I5043 |
| Acute Kidney Injury | N170, N171, N172, N178, N179 |
| Acute Coronary Artery Disease | I2101, I2102, I2109, I211, I2119, I2111, I212, I2129, I213, I214, I219 |
| Stroke | I60, I61, I62, I63, I650, I688, O873, O2250, O2251, O2252 |
| Pulmonary Edema | J810, J811, I501 |
| Hypertension | I10(start with) |
| Blood Loss Anemia | D62 (start with) |
| Pneumonia | J189, J159, J22 |
| Pulmonary Embolism | I2602, I2609, I2692, I2699 |
| DVT | I82401, I82402, I82403, I82409, I82411, I82412, I82413, I82419, I82421, I82422, I82423, I82429 |
| Dyslipidemia | E78(start with) |
| Obstructive Sleep Apnea | G473 |
| Chronic Anemia | D64(start with) |
| Alcohol Abuse History | F10 |
| Osteoporosis | M81, M82 |
| Mental Disorders | F (start with) |
| Parkinson Disease | G20 (start with) |
| Type 2 Diabetes Mellitus | E11 (start with) |
| Chronic Kidney Disease | N18 (start with) |
| Congestive Heart Failure | I500, I501, I509 |
| Chronic Lung Disease | J44 (start with) |
| History of Myocardial Infarction | I252 |
| Peripheral Vascular Disease | I73 (start with) |
| History of Cerebrovascular Accident (CVA) | Z8673, I69 (start with) |
| Dementia | F03 (start with) |
| Peptic Ulcer Disease | K25-K28 |
| Hemiplegia | G81 |
| Neoplasms | C (start with) |
| Neoplasms of Lymphoid and Hematopoietic Tissue | C81-C96 |
Table 2.
Demographic and Payer Characteristics of Patients Undergoing ACDF and CDA.
| Parameter | ACDF | CDA | Significance |
|---|---|---|---|
| Total Surgeries (%) | 85,584 | 11,415 | - |
| Average Age (y) | 55.6 | 47.2 | P<0.001 |
| Female (%) | 51.7 | 52.5 | P=0.108 |
| Primary expected payer - Medicare (%) | 33.9 | 10.7 | P<0.001 |
| Primary expected payer - Medicaid (%) | 10.7 | 9.7 | |
| Pimary expected payer - private including HMO (%) | 44.5 | 64.9 | |
| Primary expected payer - self-pay (%) | 1.2 | 1.3 | |
| Primary expected payer - no charge (%) | 0.1 | 0 | |
| Primary expected payer - other (%) | 9.6 | 13.3 |
Table 3.
Prevalence of Comorbidities Among Patients Undergoing ACDF and CDA.
| Parameter | ACDF (n=85,584) | CDA (n=11,415) | Significance |
|---|---|---|---|
| Hypertension (%) | 43.7 | 25.1 | P<0.001 |
| Dyslipidemia (%) | 30 | 17.3 | P<0.001 |
| Obstructive Sleep Apnea (%) | 9.5 | 6.9 | P<0.001 |
| Chronic Anemia (%) | 2.3 | 1.8 | P<0.001 |
| Alcohol Abuse (%) | 1.2 | 0.8 | P<0.001 |
| Osteoporosis (%) | 2.3 | 0.9 | P<0.001 |
| Parkinson Disease (%) | 0.5 | 0.1 | P<0.001 |
| Alzheimer Disease (%) | 0.1 | 0 | P=0.698 |
| Chronic Kidney Disease (%) | 3.8 | 1.1 | P<0.001 |
| Congestive Heart Failure (%) | 0.9 | 0.1 | P<0.001 |
| Chronic Lung Disease (%) | 8 | 3.2 | P<0.001 |
| Diabetes Mellitus (%) | 19.5 | 9.6 | P<0.001 |
| IBD (%) | 0.5 | 0.3 | P<0.001 |
| Liver Disease (%) | 1.1 | 0.7 | P<0.001 |
| Obesity (%) | 18.5 | 15.6 | P<0.001 |
| Fibromyalgia (%) | 3.8 | 3 | P<0.001 |
| Disorders of Thyroid (%) | 11.9 | 9.4 | P<0.001 |
| History of Myocardial Infarction (%) | 2.9 | 0.7 | P<0.001 |
| Peripheral Vascular Disease (%) | 1.3 | 0.6 | P<0.001 |
| History of Cerebrovascular Accident (%) | 3.9 | 1.3 | P<0.001 |
| Dementia (%) | 0.2 | 0.2 | P<0.001 |
| Neoplasms (%) | 0.8 | 0.3 | P<0.001 |
| Neoplasms of Lymphoid and Hematopoietic Tissue (%) | 0.3 | 0.1 | P<0.001 |
Table 4.
Comparison of Demographic and Clinical Characteristics in Propensity Score-Matched Cohorts Undergoing ACDF and CDA.
Table 4.
Comparison of Demographic and Clinical Characteristics in Propensity Score-Matched Cohorts Undergoing ACDF and CDA.
| Parameter | ACDF (n=11,415) | CDA (n=11,415) | Significance |
|---|---|---|---|
| Average Age (y) | 47.3 | 47.2 | P=0.36 |
| Female (%) | 52.1 | 52.5 | P=0.62 |
| Primary expected payer - Medicare (%) | 11.6 | 11.3 | P=0.41 |
| Primary expected payer - Medicaid (%) | 9.7 | 9.7 | |
| Primary expected payer - private including HMO (%) | 64.5 | 64.9 | |
| Primary expected payer - self-pay (%) | 1.5 | 1.3 | |
| Primary expected payer - no charge (%) | 0 | 0 | |
| Primary expected payer - other (%) | 12.7 | 12.7 | |
| Hypertension (%) | 24.7 | 25.1 | P=0.59 |
| Dyslipidemia (%) | 17.2 | 17.3 | P=0.93 |
| Obstructive Sleep Apnea (%) | 6.4 | 6.9 | P=0.05 |
| Chronic Anemia (%) | 1.6 | 1.8 | P=0.43 |
| Alcohol Abuse (%) | 0.7 | 0.8 | P=0.33 |
| Osteoporosis (%) | 0.9 | 0.9 | P=0.52 |
| Parkinson Disease (%) | 0 | 0.1 | P=0.20 |
| Alzheimer Disease (%) | 0 | 0 | P=1 |
| Chronic Kidney Disease (%) | 1 | 1.1 | P=0.51 |
| Congestive Heart Failure (%) | 0.1 | 0 | P=0.06 |
| Chronic Lung Disease (%) | 2.9 | 3.2 | P=0.09 |
| Diabetes Mellitus (%) | 8.9 | 9.6 | P=0.05 |
| Inflammatory Bowel Disease (%) | 0.4 | 0.3 | P=0.23 |
| Liver Disease (%) | 0.5 | 0.7 | P=0.19 |
| Obesity (%) | 16.4 | 15.6 | P=0.09 |
| Fibromyalgia (%) | 2.7 | 3 | P=0.11 |
| History of Myocardial Infarction (%) | 0.6 | 0.6 | P=0.18 |
| Peripheral Vascular Disease (%) | 0.6 | 0.6 | P=0.35 |
| History of Cerebrovascular Accident (%) | 1.3 | 1.3 | P=0.42 |
| Neoplasms (%) | 0.4 | 0.3 | P=0.09 |
| Neoplasms of Lymphoid and Hematopoietic Tissue (%) | 0.1 | 0.1 | P=1 |
Table 5.
Comparison of Hospitalization Outcomes in Propensity Score-Matched Cohorts Undergoing ACDF and CDA.
Table 5.
Comparison of Hospitalization Outcomes in Propensity Score-Matched Cohorts Undergoing ACDF and CDA.
| ACDF (n=11,415) | CDA (n=11,415) | Significance | |
|---|---|---|---|
| Length of stay mean in days | 1.39 (Std. deviation 1.52) | 1.32 (Std. deviation 1.27) | P<0.001 |
| Total charges mean in $ | 58,472 (Std. deviation 41703) | 82,431 (Std. deviation 53105) | P<0.001 |
Table 6.
Postoperative Outcomes in Patients Undergoing ACDF and CDA After Propensity Score Matching.
Table 6.
Postoperative Outcomes in Patients Undergoing ACDF and CDA After Propensity Score Matching.
| Parameter | ACDF (n=11,415) | CDA (n=11,415) |
Significance | Odds Ratio | Odds Ratio 95% Confidence |
|---|---|---|---|---|---|
| Dysphagia (%) | 4.90% | 3.60% | P<0.001 | 0.724 | 0.63 - 0.82 |
| Blood Loss Anemia (%) | 1.00% | 0.80% | P=0.17 | 0.825 | 0.62 - 1.08 |
| Cervical spinal cord injury (%) | 0.17% | 0.30% | P=0.04 | 1.752 | 1.01 - 3.03 |
| UTI (%) | 0.22% | 0.39% | P=0.02 | 1.803 | 1.1 - 2.94 |
| Acute Renal Failure (%) | 0.21% | 0.26% | P=0.50 | 1.201 | 0.7 - 2.04 |
| Pneumonia (%) | 0.17% | 0.17% | P=1.00 | 1.000 | 0.53 - 1.86 |
| Blood transfusion (%) | 0.13% | 0.00% | P=0.01 | 0.500 | 0.17 - 1.46 |
| Venous Thromboembolism (%) | 0.13% | 0.04% | P=0.03 | 0.308 | 0.12 - 0.75 |
| Pulmonary Edema (%) | 0.04% | 0.04% | P=1.00 | 1.000 | 0.28 - 3.45 |
| Ileus (%) | 0.08% | 0.17% | P=0.07 | 2.002 | 0.93 - 4.27 |
| Feeding Tube (%) | 0.08% | 0.00% | P=0.01 | 0.5 | 0.17 - 1.46 |
| Dural tear (%) | 0.04% | 0.04% | P=1.00 | 1.000 | 0.28 - 3.45 |
| Sepsis (%) | 0.04% | 0.00% | P=0.03 | 0.500 | 0.49 - 0.5 |
| Pulmonary Embolism (%) | 0.04% | 0.00% | P=0.03 | 0.500 | 0.49 - 0.5 |
| Mortality (%) | 0.00% | 0.00% | P=1.00 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



