Submitted:
08 August 2025
Posted:
11 August 2025
You are already at the latest version
Abstract
Alone or combined with clavulanic acid, amoxicillin is widely prescribed. Therapeu-tic indications include a broad spectrum of infections. Combination with clavulanic acid kept the known activity of amoxicillin against strains producing β-lactamase. Only poor studies exist on adverse reactions and antibiotic resistance by using databanks reporting spontaneous signals caused by amoxicillin or the combination amoxicillin/clavulanic acid. Antimicrobial resistance is an overlooked adverse event and pharmacovigilance da-tabases could serve as a tool in tracking resistance. On this basis, a study to define the safety profile of amoxicillin and amoxicillin/clavulanic acid and to increase the knowledge necessary to support the battle against antimicrobial resistance was undertook through the analysis of pharmacovigilance databases. Signals of suspected adverse reac-tions to amoxicillin and to the combination amoxicillin/clavulanic acid of the data system EudraVigilance in the years 2020-2024, were analyzed. A disproportionality analysis for hepatotoxic reactions and for drug inefficiency was performed comparing data of the two medicinal products. Most frequent signals were about “Skin and subcutaneous disorders” for both the drugs. Disproportionate analysis of cases signaling “Hepatobiliary disor-ders” or “Drug inefficiency”, indicates significant increase of these signals with the com-bination amoxicillin/clavulanic acid compared to amoxicillin. The combination amoxicil-lin/clavulanic acid has previously been associated with higher risk of hepatotoxicity, however, it is the first time that a post-marketing surveillance shows that antimicrobial resistance has a greater probability to occur with the combination in comparison to amoxicillin.
Keywords:
amoxicillin
; amoxicillin/clavulanic acid
; antimicrobial resistance
; antibiotic resistance
; hepatotoxicity
; liver toxicity
; pharmacovigilance
; adverse reactions
1. Introduction
The semisynthetic penicillin amoxicillin was generated with the addition of an extra amino group to penicillin with the aim to fight against the development of antibiotic resistance [1]. Alone or combined with the b-lactamase inhibitor clavulanic acid, this drug is the most widely prescribed penicillin in Europe and other many countries [2]. Amoxicillin binds irreversibly to penicillin-binding protein 1A, that is fundamental for the synthesis of cell wall in bacteria. This binding inactivates penicillin-binding protein 1A and leads to lysis of cell lysis [3]. Clavulanic acid is a suicide inhibitor binding the active site of the beta-lactamase, causing its reorganization [4]. Therapeutic indications for amoxicillin include infections induced by beta-lactamase–negative bacteria, such as higher and lower respiratory tract infections, urinary tract infections, Helicobacter pylori treatment and skin infections [5]. Combination of amoxicillin with clavulanic acid kept the known activity of amoxicillin against β-lactamase-negative strains and reinstated its action against β-lactamase-producing strains. Furthermore, the combination espanded amoxicillin action versus other strains producing β-lactamase, such as Klebsiella pneumoniae and anaerobic Bacteroides fragilis [6]. Combination of amoxicillin with clavulanic acid has been shown to be efficacious against infections of urinary, respiratory and soft tissues due to β-lactamase producing bacteria, as well as in the treatment of gonorrhoea and chancroid [7]. Amoxicillin and amoxicillin/clavulanic acid are generally considered as well tolerated medicinal products with an established safety profile, based on extensive clinical worldwide use. However, it is known that patients with recognized hypersensitivity to penicillin should not be treated with amoxicillin. Furthermore, the combination amoxicillin/clavulanate should be prescribed with caution in patients presenting hepatic dysfunction and it is contraindicated in patients with a previous history of cholestatic jaundice/hepatic dysfunction [8]. Only poor studies have been conducted on real world data investigating on adverse reactions and antibiotic resistance by using databanks reporting spontaneous signals of adverse reactions to medicinal products with amoxicillin and the combination amoxicillin/clavulanic acid. It has also been suggested that antimicrobial resistance is an overlooked adverse event and that pharmacovigilance databases could serve as a tool in tracking antimicrobial use and resistance [9]. On this basis, a study to define the safety profile related to signal of adverse reactions and to investigate the potential role of pharmacovigilance databases in supporting the battle against antimicrobial resistance, was undertook. In particular, aim of this study was to collect the spontaneous reports of suspected adverse reactions (SARs) to medicinal products based on amoxicillin and amoxicillin/clavulanic acid in the years 2020-2024 real-world data of the database EudraVigilance. On these data, a descriptive analysis of more common SARs, will be performed. Moreover, a disproportionate analysis comparing SARs described as “Hepatobiliary disorders” and “Drug ineffective” of the two medicinal products, will be operated.
2. Results
2.1. Serious/Non Serious Suspected Adverse Reactions Percentage and Ratio
A total of 7900 Individual Cases Safety reports (ICSRs) related to amoxicillin and the combination amoxicillin/clavulanic acid prescription were identified in the Eudravigilance database as signals of adverse reactions in the period from january 2020 to 31 December 2024. In the same years, 10329 ICSRs were identified for the combination amoxicillin/clavulanic acid. Of these reports, 3685 ICSRs linked to amoxicillin prescription were categorized as serious cases (46.6% of the total number of ICSRs amoxicillin-related). Serious ICSRs related to amoxicillin/clavulanic acid combination were 5114 (49.5% of the total number of ICSRs combination-related). The evaluation of adverse reactions to amoxicillin and to the combination amoxicillin clavulanic acid, shows as the ratio between the reports of serious and non-serious adverse reactions is less than 1 for both the medicinal products. It is 0.87 and 0.98, for amoxicillin alone and the combination, respectively (Table 1).
2.2. Serious Suspected Adverse Reactions to Amoxicillin and Amoxicillin/Clavulanic Acid Combination According to System Organ Class (SOC) Level
Aggregation of SARs to amoxicillin and to amoxicillin/clavulanic acid combination according to the SOC level shows that most frequent adverse reactions among those signaled in the years 2020-2024, are the group of “Skin and subcutaneous disorders” followed “Immune system disorders” for both the category of medicinal products. However, after these two groups of SARs, in descending order we find “General disorders and administration site conditions” for amoxicillin, while for the combination, the group of “Hepatobiliary disorders” is the third among groups of signaled SARs. These groups and the other groups of more frequently signaled SARs are represented in the Figure 1 and Figure 2.
2.3. Sex Distribution of Cases Reporting Serious Suspected Adverse Reactions (SARs) to Amoxicillin and Amoxicillin/Clavulanic acid Combination According to System Organ Class (SOC) Level
Table 2 and Table 3 show sex distribution of serious adverse reactions aggregated according to SOC level signaled for amoxicillin and the combination amoxicillin/clavulanic acid, respectively. Signals related to amoxicillin prescription show statistically significant difference in sex distribution of “Skin and subcutaneous tissue disorders”, “Gastrointestinal disorders” and “Respiratory, thoracic and mediastinal disorders” with the prevalence of female cases (Table 2). Signals related to the prescription of the combination amoxicillin/clavulanic acid show statistically significant difference in sex distribution of “Skin and subcutaneous tissue disorders” with prevalence of male cases. A significant difference through the analysis of data of the combination was observed for “Gastrointestinal disorders” and “Respiratory, thoracic and mediastinal disorders” with female prevalence in both the SOC groups (Table 3). Disproportionate analysis of ICSRs signaling adverse reactions to the combination amoxicillin/clavulanic acid vs the adverse reactions to amoxicillin, aggregated according to the SOC) level and performed by using Reporting Odds Ratio (ROR), indicates an increase of risk of Hepatobiliary disorders related to the use of the combination amoxicillin/clavulanic acid in comparison to the use of amoxicillin alone (Table 4).
2.4. Evaluation of Adverse Reactions to Amoxicillin and Amoxicillin/Clavulanic Acid Signaled as “Hepatobiliary Disorders”
Serious reactions belonging to the SOC group of “Hepatobiliary disorders” were detected in 257 and 834 cases for amoxicillin and for the combination amoxicillin/clavulanic acid, respectively. Statistical analysis shows an asymmetric sex distribution, since “Hepatobiliary disorders” are more frequent in females for amoxicillin and in males for the combination amoxicillin/clavulanic acid (Table 5). Disproportionate analysis of serious ICSRs signaling “Hepatobiliary disorders”, performed by using Reporting Odds Ratio (ROR), indicates significant increase of risk of this signal with the use of the combination amoxicillin/clavulanic acid in comparison to the use of amoxicillin alone (Table 6).
2.5. Evaluation of Adverse Reactions to Amoxicillin and Amoxicillin/Clavulanic acid Signaled as “Drug Ineffective”
For this evaluation, difference between serious and not serious cases was not maintained. The reaction signaled as “drug ineffective” was detected in 45 and 156 serious and non serious cases for amoxicillin and for the combination amoxicillin/clavulanic acid, respectively. Statistical analysis shows that frequency of male and female cases are overlapping for amoxicillin, while sex distribution between the sexes for the combination amoxicillin/clavulanic acid indicates that inefficiency against infections is more frequent in females (Table 7). Disproportionate analysis of ICSRs signaling “Drug ineffective”, performed by using Reporting Odds Ratio (ROR), indicates an increase of risk of this signal with the use of the combination amoxicillin/clavulanic acid in comparison to the use of amoxicillin alone (Table 8).
3. Discussion
In the present study we analyzed data on SARs signaled in European countries related to amoxicillin and the combination amoxicillin/clavulanic acid prescription in the years 2020-2024. These medicinal products show a serious/non serious ratio almost overlapping and close to 1, generally accepted as acceptable [10]. “Serious” adverse events are defined as any untoward medical occurrence that at any dose results in death, requires hospital admission or prolongation of existing hospital stay, results in persistent or significant disability/incapacity, is life threatening, results in cancers, congenital anomalies or birth defects, as well as any medical event that would be regarded as serious if they had not responded to acute treatment [11].
The most frequent signals in the EudraVigilance database, in the years taken in consideration, concern the group of “Skin and subcutaneous disorders” followed by “Immune system disorders” for both amoxicillin and the combination amoxicillin/clavulanic acid. It is not a novelty, since a 10-month prospective cohort study including all hospitalized patients and designed to identify those with adverse cutaneous drug reactions showed that medicinal products containing amoxicillin were the drugs with the highest reaction rate [12].
Other authors, through a mixed prospective- retrospective cohort study conducted to assess the safety profile of amoxicillin, amoxicillin-clavulanic acid, found that the skin and subcutaneous system, together with the gastrointestinal system, were commonly affected by the use of amoxicillin or of the combination, while respiratory thoracic disorders, nervous system and general disorders were uncommonly involved [13]. Prevalence of “Skin disorders and subcutaneous disorders”, at least as far as pediatric age is concerned and limited to the combination amoxicilli/clavulanic acid, has been explained by the presence of sodium benzoate, contained in the suspension formulation as a preservative. According with this hypothesis, sodium benzoate probably acts through a non-immunologic mechanism and care should be given to children allergic to sodium benzoate containing pharmaceutical formulations [14].
Skin and immune disorders caused by medicinal products containing amoxicillin are probably closely related. Amoxicillin is frequently involved drug in sensitization among all beta-lactams [15] and it has been shown that the combination amoxicillin/clavulanic acid is one of the most important drug triggering allergic reactions in younger people accounting for up to 80% of beta-lactams allergy cases [16]. Among mechanisms through amoxicillin can alter the immune e system activity, it has been shown that amoxicillin decreases phagocytosis and macrophage chemotaxis [17], and that early life amoxicillin exposure can alter immune response locally and systemically, long after withdrawal [18].
Sex distribution shows the prevalence of female cases of “Gastrointestinal disorders” and “Respiratory, thoracic and mediastinal disorders” about signals of SARs to both amoxicillin and amoxicillin/clavulanic acid. While signals about “Skin and subcutaneous tissue disorders” show an asymmetry in sex distribution of the two categories of medicinal products, because there is a prevalence of female cases for amoxicillin against a male prevalence of cases for the combination. Disproportionate analysis performed by ROR indicates a potential increase of risk of Hepatobiliary disorders related to the use of the combination amoxicillin/clavulanic acid in comparison to the use of amoxicillin alone.
Hepatobiliary adverse drug reactions are an important issue in the field of drug safety and pharmacovigilance, because they are the leading cause of acute liver failure in the United States and Europe [19,20]. Amoxicillin, alone or in combination with clavulanic acid, has previously been described as hepatotoxic substance in paediatrics [21]. Other authors, through two previous population-based studies in adults on drug-induced liver injury, indicated as the combination amoxicillin/clavulanic acid displays a higher risk of acute liver injury with respect to amoxicillin alone [22,23]. Moreover, another finding suggested that Class I and II HLA genotypes affect susceptibility to amoxicillin/clavulanic acid-induced hepatic injury, indicating the importance of the adaptive immune response in pathogenetic mechanism [24]. Recently, a retrospective study analyzing the ICSRs of the global pharmacovigilance database VigiBase, signaled in Switzerland from 2010 to 2020, indicated as the combination amoxicillin/clavulanic acid was among the most frequently suspected drugs for severe drug-related hepatic disorders. Authors concluded that the cause of hepatotoxicity induced by the prescription of the combination amoxicillin/clavulanate is still unknown, postulating an immunoallergic mechanism [25]. Analysis of data obtained from EudraVigilance seem to confirm that the combination amoxicillin/clavulanic acid is less safe of amoxicillin, since the comparison of signals for “Hepatobiliary disorders” of the combination showed, through a ROR of 2.78 (95% C.I. 2.41-3.24) a stronger association between liver disorders and use of medicinal products based on amoxicillin/clavulanic acid.
Pharmacovigilance is defined as the science and the activities related to the detection, assessment, understanding and prevention of adverse effects or any other drug-related problems [9]. It has been suggested as pharmacovigilance databases could serve as a tool in measuring antibiotic resistance with the aim of tracking resistant microorganisms and reduce therapy failures and, finally to give a contribute in ensuring appropriate prescription of existing antibiotics [26]. On this basis, part of the present research was devoted to identify cases of antimicrobial resistance to the combination amoxicillin/clavulanic acid and of amoxicillin alone in the database EudraVigilance. This research was conducted through the identification of cases reporting the adverse reaction “Drug ineffective” for both the medicinal products in the years 2020-2024.
The combination amoxicillin/clavulanic acid is prescribed more frequently than amoxicillin in many countries. Amoxicillin alone has fewer side effects and can be prescribed in higher oral doses [2]. Antimicrobial resistance occurs when the antibiotic is not able to treat certain bacterial infections because the pathogens causing these infections have developed mechanisms to prevent the drug from functioning counteracting the antibiotic's effectiveness. Mechanisms involved in resistance to amoxicillin treatment are target alteration, antibiotic inactivation and reduced permeability to the drug [27]. This association offers broader coverage by combining amoxicillin, a penicillin derivative effective against gram-positive and gram-negative bacteria, with clavulanic acid, which counteracts β-lactamase–producing strains [28]. However, amoxicillin/clavulanic acid resistance keeps to be a concern as well as happens for amoxicillin. Resistance is often linked to the production of beta-lactamases, but other mechanisms like outer membrane protein modifications can play a role [29,30]. Disproportionate analysis of the association of the signal/adverse reaction “Drug ineffective”, produced in the present work, indicates a higher potential risk of inefficiency of the combination amoxicillin/clavulanic acid, ROR being 2.78 (95% C.I. 1.92-3.73). ROR represents a disproportionality measure use to identify the association between an adverse event with the exposure to a certain medicinal product. When ROR is more than one, it means that we have greater odds that the adverse event occurs with the exposure to the medicinal product [31]. In our case, results of disproportionality analysis suggest that we have more than 2.5 times the probability that drug inefficiency occurs with the combination amoxicillin/clavulanic acid in comparison with the use of amoxicillin alone. Since efficiency of these two medicinal products is prevalently measured against infections, thus it means that antibiotic resistance is probably more commonly occurring with the combination.
The results produced with the present study need to be interpreted with care due to the known limitations of pharmacovigilance research using data systems of spontaneous signals for drugs adverse reactions. Limitations include arbitrary choice of the years analyzed, the lack of a denominator, under-reporting, the minor quality of information, the uncertainty of causal relationships, and, finally, the difficulty in controlling confounding factors such as comorbidities or, sometimes, dosage and frequency duration of exposure, which may have an influence on health/pathology condition. Moreover, although care and attention were taken to identify and remove duplicates, they may still exist after data extraction. A different safety profile for the two medicinal products has been previously described. Amoxicillin/clavulanic acid has been associated with a higher risk of Stevens–Johnson syndrome, purpura, and with a reporting rate of hepatitis on average 9-fold higher for amoxicillin/clavulanic acid than for amoxicillin alone [32]. However, it is the first time that a post-marketing surveillance study shows through real-world data of spontaneous reports of adverse reactions that antimicrobial resistance has a greater probability to occur with the combination in comparison to amoxicillin.
In conclusion, beyond the limitations described above, this research focuses on two aspects related to the safety of prescribing amoxicillin and the amoxicillin/clavulanic acid combination. The data confirm previous research indicating that prescribing the amoxicillin/clavulanic acid combination carries an increased risk of hepatobiliary disorders. Even more interesting is the finding that the combination, developed to combat amoxicillin resistance, appears to be, in many cases, even less effective than amoxicillin itself in combating antibiotic resistance. Given the exploratory nature of the disproportionality analysis conducted in this study, which does not allow for a precise quantification of the identified risk, both aspects relating to the safety of amoxicillin/clavulanic acid use, hepatotoxicity and antibiotic resistance, deserve further investigation.
4. Materials and Methods
EudraVigilance is a database containing suspected adverse reactions (SARs) related to medicines authorized for the market or currently undergoing clinical trials in the European Union (EU). In this data system, SARs are traceable in individual cases (Individual Cases Safety Reports; ICSRs) signaled by national drug regulatory authorities in the EU or by marketing authorization holders. It is noteworthy that EudraVigilance collects reports of “suspected” adverse reactions, meaning unwanted medical events that have been observed following the use of a medicine, but which are not necessarily related to or caused by the medicine itself [33].
4.1. Design of the Study
In the present study, ICSRs reporting SARs that occurred in patients to whom amoxicillin or the combination amoxicillin/clavulanic acid was prescribed, signaled from 1 January 2020 to 31 December 2024, were collected and analyzed. The public version of the EudraVigilance database was used, and the collection of data on SARs was conducted according to the following inclusion criteria: only serious SARs and reports sent only from healthcare professionals in cases regarding all ages (from 0 to >85 years) and signaled from the European Economic Area, including the United Kingdom. Reports submitted in EudraVigilance originated from EEA and non-EEA countries, but for this study, we selected only reports originating from the European Economic Area (EEA). All serious and non serious cases were analyzed to evaluate in more depth the adverse reaction signaled as “Drug ineffective” and reflecting any case of resistance to treatment. We mention the UK separately because in EudraVigilance, it continues to be included within the EEA. Signals were excluded from the analysis when reported by not healthcare professionals, or coming from non-European countries. For all cases, information was provided on patient characteristics (age group and sex), the type of adverse reaction (often more than one for each ICSR), and the qualification of the primary source. The terms “sex” and “gender” are used interchangeably here because only the field containing the term “sex” is available in EudraVigilance; consequently, the information collected refers to biological sex [34]. Regarding the criteria for the collection of data from ICSRs, SARs selection was based on the Medical Dictionary for Regulatory Activities (MedDRA). MedDRA is an international standardized and clinically validated medical terminology used by regulatory authorities and the biopharmaceutical industry. It is used to code cases of adverse effects in pharmacovigilance databases and to facilitate searches in databases on adverse drug reactions. For the present study, each ICSR was analyzed, and every mentioned SAR was extracted and counted from every single case. MedDRA has a hierarchy of terms to describe adverse reactions. Adverse reactions were grouped under the terms of the SOC (System Organ Classification) level in the MedDRA hierarchy such as, for example, musculoskeletal and connective tissue disorders and vascular disorders. The SOC system organ classification is the highest level of the hierarchy that captures the broadest concept useful for retrieving data. It is a way of grouping medical terms based on body systems or functions. Single adverse reaction, as well as “Drug ineffective”, used in this study, has been used as a so-called “term” (PT) listed in MedDRA and reported by the National Center for Biomedical Ontology. A PT is a distinct descriptor (single medical concept) for an adverse symptom or sign. We selected all single adverse reaction recorded in the ICSRs as “Drug ineffective”, and we counted them all and analyzed its frequency for amoxicillin or for the combination amoxicillin/clavulanic acid [35].
4.2. Data Analysis
The source of data extraction is a line listing a structured table, where each row represents an ICSR and each column represents a specific data point associated with that case. The data were analyzed by aggregating the PTs of individual reports to a higher level of the MedDRA hierarchy by merging individual serious SARs in the SOC level (e.g., nausea and vomiting are classified in the same group as Gastrointestinal Symptoms). Only reports classified as serious were analyzed, except for the analysis of data related to the adverse reaction “Drug ineffective”. In accordance with the E2D guidelines of the International Council for Harmonization, ICSRs are classified as serious if they are life threatening, have resulted in death, have resulted in/prolonged hospitalization or disability, or are related to a congenital anomaly/birth defect or other medically important condition. The adequate stratification of signals by sex groups was performed to avoid biases caused by confounding effects and to analyze these two variables separately. Sex distribution were analyzed as ratio of relative risk. Duplicate and incomplete ICSRs were excluded from the analysis. A duplicate search was conducted based on the detection in the dataset of similarities in the adverse reaction, age, sex, suspected/interacting medicinal products, and EudraVigilance local report number. A disproportionate analysis of the potential association of the SOC group “Hepatobiliary disorders” and of the signal “Drug ineffective” was performed by reporting odds ratio (ROR) comparing SARs of the combination amoxicillin/clavulanic acid with those signaled for amoxicillin alone. Disproportionality analysis is a methodology used to detect signals of adverse drug reactions. It is based on the two-by-two contingency table. In this way, the differences between the occurrence frequency and background frequency for target drugs and target adverse events can be compared [36]. ROR is one of the well-established disproportionality analysis methods. It calculates the ratio of the odds of a selected drug versus other drugs for a certain adverse event [37].
4.3. Statistics
A descriptive statistical analysis and a disproportionality analysis based on the reporting odds ratio (ROR) were performed. The ROR is used here to establish the strength of disproportionality comparing SARs signaled for the combination amoxicillin/clavulanic with those signaled for amoxicillin alone. An ROR equal to 1 indicates the absence of a signal; conversely, an ROR greater than 1 indicates a signal and the existence of an association. The higher the ROR, the stronger the association. The ROR is statistically significant when the lower limit of its 95% CI is greater than 1 [38]. All statistical analyses were completed using SPSS statistical software, version 29.0 (SPSS, IBM, Armonk, NY, USA).
Author Contributions
Conceptualization, I.A., F.C., C.M., and G.C.; methodology, I.A., F.C., C.M., M.C.; software, I.A., F.C., M.C., G.C., P.M. and E.E.; validation, I.A. and F.C.; formal analysis, I.A., F.C., P.M. and L.C.; investigation, M.S., C.M., P.M., M.C. and L.C.; resources, data curation, E.E., C.M., F.C., P.M. and G.C.; writing—original draft preparation, I.A., F.C., C.M., and L.C.; writing—review and editing, F.C., C.M., L.C. and E.E.; supervision, G.C.; project administration, I.A., F.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data analyzed and presented in this study are available on the public EudraVigilance data system.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| SAR | Suspected adverse reaction |
| ICSR | Individual Case Safety Reports |
| SOC | System Organ Class |
| EEA | European Economic Area |
| ROR | Reporting Odds Ratio |
| HLA | Human leukocyte antigen |
| C.I. | Confidence intervals |
| EU | European Union |
| MedDRA | Medical Dictionary for Regulatory Activities |
| PT | Preferred Term |
References
- Akhavan BJ, Khanna NR, Vijhani P. Amoxicillin. 2023 Nov 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. [PubMed]
- Huttner A, Bielicki J, Clements MN, Frimodt-Møller N, Muller AE, Paccaud JP, Mouton JW. Oral amoxicillin and amoxicillin-clavulanic acid: properties, indications and usage. Clin Microbiol Infect. 2020 Jul;26(7):871-879. [CrossRef] [PubMed]
- Bodey GP, Nance J. Amoxicillin: in vitro and pharmacological studies. Antimicrob Agents Chemother. 1972 Apr;1(4):358-62. [CrossRef] [PubMed] [PubMed Central]
- Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005 Oct;18(4):657-86. [CrossRef] [PubMed] [PubMed Central]
- Hsu CK, Lai CC. Different Indications Between Fluoroquinolone and Amoxicillin. Clin Infect Dis. 2023 Jan 13;76(2):371. [CrossRef] [PubMed]
- Hsu LY, Chang SC, Luh KT, Hsieh WC. Antibacterial activities of amoxicillin alone and in combination with clavulanic acid correlated with beta-lactamase production. Zhonghua Min Guo Wei Sheng Wu Ji Mian Yi Xue Za Zhi. 1991 Aug;24(3):272-80. [PubMed]
- Todd PA, Benfield P. Amoxicillin/clavulanic acid. An update of its antibacterial activity, pharmacokinetic properties and therapeutic use. Drugs. 1990 Feb;39(2):264-307. [CrossRef] [PubMed]
- White AR, Kaye C, Poupard J, Pypstra R, Woodnutt G, Wynne B. Augmentin (amoxicillin/clavulanate) in the treatment of community-acquired respiratory tract infection: a review of the continuing development of an innovative antimicrobial agent. J Antimicrob Chemother. 2004 Jan;53 Suppl 1:i3-20. [CrossRef] [PubMed]
- Habarugira JMV, Figueras A. Pharmacovigilance network as an additional tool for the surveillance of antimicrobial resistance. Pharmacoepidemiol Drug Saf. 2021 Aug;30(8):1123-1131. [CrossRef] [PubMed]
- Moulis G, Sommet A, Durrieu G, Bagheri H, Lapeyre-Mestre M, Montastruc JL; French Association of PharmacoVigilance Centres. Trends of reporting of 'serious'vs. 'non-serious' adverse drug reactions over time: a study in the French PharmacoVigilance Database. Br J Clin Pharmacol. 2012 Jul;74(1):201-4. [CrossRef] [PubMed] [PubMed Central]
- Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet. 2000;356:1255–9. [CrossRef]
- Hernández-Salazar A, Rosales SP, Rangel-Frausto S, Criollo E, Archer-Dubon C, Orozco-Topete R. Epidemiology of adverse cutaneous drug reactions. A prospective study in hospitalized patients. Arch Med Res. 2006 Oct;37(7):899-902. [CrossRef] [PubMed]
- Mwamwitwa KW, Bukundi EM, Maganda BA, Munishi C, Fimbo AM, Buma D, Muro EP, Sabiiti W, Shewiyo DH, Shearer MC, Smith AD, Kaale EA. Adverse Drug Reactions Resulting From the Use of Chiral Medicines Amoxicillin, Amoxicillin-Clavulanic Acid, and Ceftriaxone: A Mixed Prospective-Retrospective Cohort Study. Inquiry. 2024 Jan-Dec;61:469580241273323. [CrossRef] [PubMed] [PubMed Central]
- Mori F, Barni S, Pucci N, Rossi ME, de Martino M, Novembre E. Cutaneous adverse reactions to amoxicillin-clavulanic acid suspension in children: the role of sodium benzoate. Curr Drug Saf. 2012 Apr;7(2):87-91. [CrossRef] [PubMed]
- Antúnez C, Martín E, Cornejo-García JA, Blanca-Lopez N, R-Pena R, Mayorga C, et al. Immediate hypersensitivity reactions to peni- cillins and other betalactams. Curr Pharm Des. 2006;12(26):3327- 33. [CrossRef]
- Kulhas Celik I, Guvenir H, Hurmuzlu S, Toyran M, Civelek E, Kocabas CN, et al. The negative predictive value of 5-day drug provocation test in nonimmediate beta-lactam allergy in children. Ann Allergy Asthma Immunol. 2020;124(5):494-9. [CrossRef]
- Fouhse JM, Yang K, More-Bayona J, Gao Y, Goruk S, Plastow G, Field CJ, Barreda DR, Willing BP. Neonatal Exposure to Amoxicillin Alters Long-Term Immune Response Despite Transient Effects on Gut-Microbiota in Piglets. Front Immunol. 2019 Sep 4;10:2059. [CrossRef] [PubMed] [PubMed Central]
- Miyata T, Shinohara M. Effect of antibiotics on rat leukocyte function. J Osaka Dent Univ. 1998 Apr;32(1):9-15. [PubMed]
- Lee, WM. Drug-induced acute liver failure. Clin Liver Dis. 2013 Nov;17(4):575-86, viii. [CrossRef] [PubMed] [PubMed Central]
- Larrey D, Pageaux GP. Drug-induced acute liver failure. Eur J Gastroenterol Hepatol. 2005 Feb;17(2):141-3. [CrossRef] [PubMed]
- Ferrajolo C, Verhamme KM, Trifirò G, 't Jong GW, Giaquinto C, Picelli G, Oteri A, de Bie S, Valkhoff VE, Schuemie MJ, Mazzaglia G, Cricelli C, Rossi F, Capuano A, Sturkenboom MC. Idiopathic acute liver injury in paediatric outpatients: incidence and signal detection in two European countries. Drug Saf. 2013 Oct;36(10):1007-16. [CrossRef] [PubMed]
- Ortland I, Mirjalili M, Kullak-Ublick GA, Peymani P. Drug-induced liver injury in Switzerland: an analysis of drug-related hepatic disorders in the WHO pharmacovigilance database VigiBase™ from 2010 to 2020. Swiss Med Wkly. 2021 May 12;151:w20503. [CrossRef] [PubMed]
- García Rodríguez LA, Stricker BH, Zimmerman HJ. Risk of acute liver injury associated with the combination of amoxicillin and clavulanic acid. Arch Intern Med. 1996 Jun 24;156(12):1327-32. [CrossRef] [PubMed]
- Lucena MI, Molokhia M, Shen Y, Urban TJ, Aithal GP, Andrade RJ, Day CP, Ruiz-Cabello F, Donaldson PT, Stephens C, Pirmohamed M, Romero-Gomez M, Navarro JM, Fontana RJ, Miller M, Groome M, Bondon-Guitton E, Conforti A, Stricker BH, Carvajal A, Ibanez L, Yue QY, Eichelbaum M, Floratos A, Pe'er I, Daly MJ, Goldstein DB, Dillon JF, Nelson MR, Watkins PB, Daly AK; Spanish DILI Registry; EUDRAGENE; DILIN; DILIGEN; International SAEC. Susceptibility to amoxicillin-clavulanate-induced liver injury is influenced by multiple HLA class I and II alleles. Gastroenterology. 2011 Jul;141(1):338-47. [CrossRef] [PubMed] [PubMed Central]
- de Abajo FJ, Montero D, Madurga M, García Rodríguez LA. Acute and clinically relevant drug-induced liver injury: a population based case-control study. Br J Clin Pharmacol. 2004 Jul;58(1):71-80. [CrossRef] [PubMed] [PubMed Central]
- Habarugira JMV, Figueras A. Antimicrobial stewardship: can we add pharmacovigilance networks to the toolbox? Eur J Clin Pharmacol. 2021 May;77(5):787-790. [CrossRef] [PubMed]
- Nong L, Liu X, Wang X, de Leeuw W, Jonker M, Brul S, Ter Kuile B. Driving factors for beta-lactam resistance gene amplification during de novoresistance evolution in E. coli. Antimicrob Agents Chemother. 2025 Jul 23:e0044125. [CrossRef] [PubMed]
- Benninger, MS. Amoxicillin/clavulanate potassium extended release tablets: a new antimicrobial for the treatment of acute bacterial sinusitis and community-acquired pneumonia. Expert Opin Pharmacother. 2003 Oct;4(10):1839-46. [CrossRef] [PubMed]
- Bader MS, Loeb M, Brooks AA. An update on the management of urinary tract infections in the era of antimicrobial resistance. Postgrad Med. 2017 Mar;129(2):242-258. [CrossRef] [PubMed]
- Pérez-Moreno MO, Centelles-Serrano MJ, Cortell-Ortolá M, Fort-Gallifa I, Ruiz J, Llovet-Lombarte MI, Picó-Plana E, Jardí-Baiges AM. Molecular epidemiology and resistance mechanisms involved in reduced susceptibility to amoxicillin/clavulanic acid in Klebsiella pneumoniae isolates from a chronic care centre. Int J Antimicrob Agents. 2011 May;37(5):462-6. [CrossRef] [PubMed]
- Hauben M, Zhou X. Quantitative methods in pharmacovigilance: focus on signal detection. Drug Saf. 2003;26(3):159-86. [CrossRef] [PubMed]
- Salvo F, De Sarro A, Caputi AP, Polimeni G. Amoxicillin and amoxicillin plus clavulanate: a safety review. Expert Opin Drug Saf. 2009 Jan;8(1):111-8. [CrossRef] [PubMed]
- Ammendolia I, Mannucci C, Cardia L, Calapai G, Gangemi S, Esposito E, Calapai F. Pharmacovigilance on cannabidiol as an antiepileptic agent. Front Pharmacol. 2023 Feb 10;14:1091978. [CrossRef] [PubMed] [PubMed Central]
- Sportiello L, Capuano A. Sex and gender differences and pharmacovigilance: a knot still to be untied. Front Pharmacol. 2024 Apr 17;15:1397291. [CrossRef] [PubMed] [PubMed Central]
- MedDRA and pharmacovigilance: a complex and little-evaluated tool. Prescrire Int. 2016 Oct;25(175):247-250. [PubMed]
- Hauben, M. Signal detection in the pharmaceutical industry: integrating clinical and computational approaches. Drug Saf. 2007;30(7):627-30. [CrossRef] [PubMed]
- Bate A, Evans SJ. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol Drug Saf. 2009 Jun;18(6):427-36. [CrossRef] [PubMed]
- Faillie, JL. Case-non-case studies: Principle, methods, bias and interpretation. Therapie. 2019 Apr;74(2):225-232. [CrossRef] [PubMed]
Figure 1.
Serious suspected adverse reactions to amoxicillin signaled in European Economic Area and United Kingdom in the years 2020-2024 and aggregated according to the System Organ Class (SOC) level.
Figure 1.
Serious suspected adverse reactions to amoxicillin signaled in European Economic Area and United Kingdom in the years 2020-2024 and aggregated according to the System Organ Class (SOC) level.
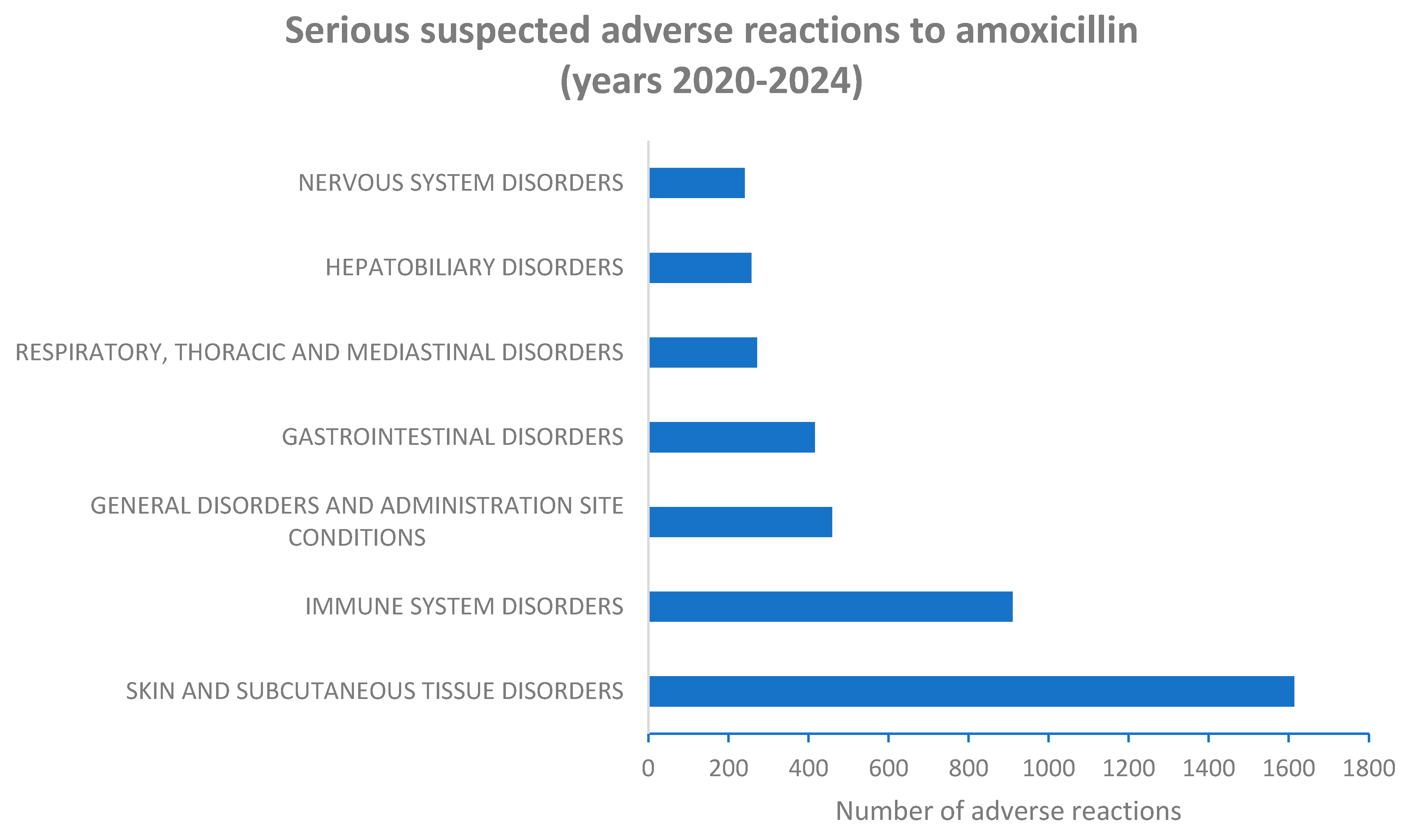
Figure 2.
Serious suspected adverse reactions to the combination amoxicillin/clavulanic acid signaled in European Economic Area and United Kingdom in the years 2020-2024 and aggregated according to the System Organ Class (SOC) level.
Figure 2.
Serious suspected adverse reactions to the combination amoxicillin/clavulanic acid signaled in European Economic Area and United Kingdom in the years 2020-2024 and aggregated according to the System Organ Class (SOC) level.
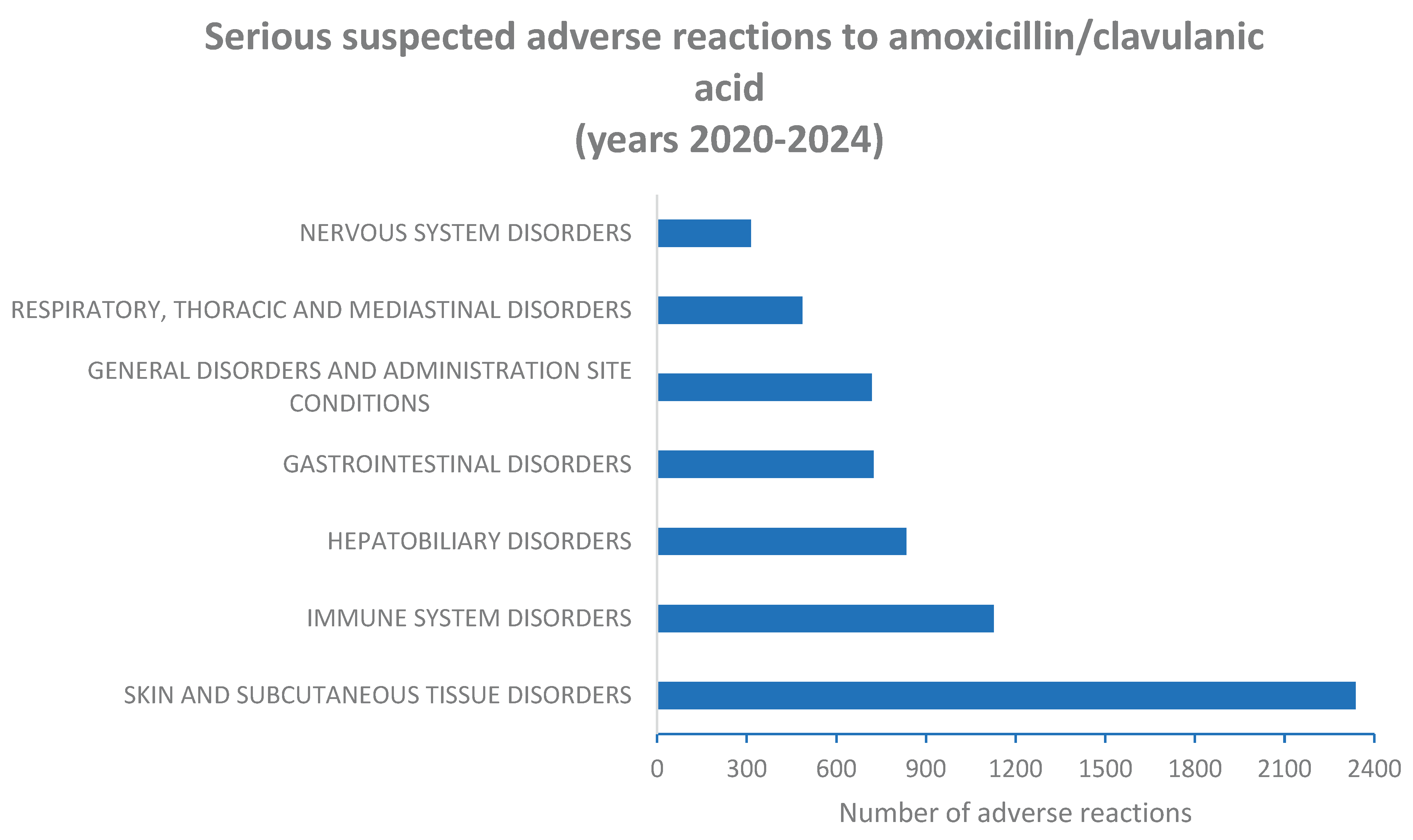

Table 1.
Serious and non-serious Individual Cases Safety Reports related to the prescription of amoxicillin and the combination amoxicillin/clavulanic acid signaled in the years 2020-2024 in the European Economic area and United Kingdom. .
Table 1.
Serious and non-serious Individual Cases Safety Reports related to the prescription of amoxicillin and the combination amoxicillin/clavulanic acid signaled in the years 2020-2024 in the European Economic area and United Kingdom. .
| Medicinal Product |
Total number of ICSRs | Serious ICSRs |
Non serious ICSRs | Serious/non serious ratio |
|---|---|---|---|---|
| Amoxicillin | 7900 | 3685 | 4215 | 0.87 |
| Amoxicillin/ clavulanic acid |
10329 | 5114 | 5215 | 0.98 |
Table 2.
Sex distribution of serious suspected adverse reactions (SARs) related to the prescription of amoxicillin signaled in the years 2020-2024 in the European Economic area and United Kingdom and aggregated according to the System Organ Class (SOC) level.
Table 2.
Sex distribution of serious suspected adverse reactions (SARs) related to the prescription of amoxicillin signaled in the years 2020-2024 in the European Economic area and United Kingdom and aggregated according to the System Organ Class (SOC) level.
| SOC | Male cases (N = 1658) |
Female cases (N = 2032) |
Male and female cases |
% of all serious cases | Significance level (P) |
|---|---|---|---|---|---|
| Skin and subcutaneous tissue disorders | 655 (40.6%) |
959 (59.4%) |
1614 | 43.7% | 0.0034* |
| Immune system disorders | 383 (42.1%) |
527 (57.9%) |
910 | 24.7% | 0.1226 |
| General disorders and administration site conditions | 186 (40.5%) |
273 (59.5%) |
459 | 12.4% | 0.0737 |
| Gastrointestinal disorders | 161 (38.7%) |
255 (61.3%) |
416 |
11.3% | 0.0158* |
| Respiratory, thoracic and mediastinal disorders | 98 (36.2%) |
173 (63.8%) |
271 | 7.3% | 0.0054* |
| Hepatobiliary disorders | 124 (48.2%) |
133 (51.8%) |
257 | 7.0% | 0.3017 |
| Nervous system disorders | 99 (41.2%) |
141 (58.8%) |
240 | 6.5% | 0.2669 |
*= P < 0.05 vs males.
Table 3.
Sex distribution of serious suspected adverse reactions (SARs) related to the prescription of the combination amoxicillin/clavulanic acid signaled in the years 2020-2024 in the European Economic area and United Kingdom and aggregated according to the System Organ Class (SOC) level.
Table 3.
Sex distribution of serious suspected adverse reactions (SARs) related to the prescription of the combination amoxicillin/clavulanic acid signaled in the years 2020-2024 in the European Economic area and United Kingdom and aggregated according to the System Organ Class (SOC) level.
| SOC | Males (N = 2238) |
Females (N = 2579) |
Male and female cases |
% of all serious cases | Significance level (P) |
|---|---|---|---|---|---|
| Skin and subcutaneous tissue disorders | 1189 (50.8%) |
1149 (49.2%) |
2338 | 48.5% | 0.0005* |
| Immune system disorders | 547 (48.5%) |
580 (51.5%) |
1127 | 23.4% | 0.2087 |
| Hepatobiliary disorders | 453 (54.3%) |
381 (45.7%) |
834 | 17.3% | 0.0001* |
| Gastrointestinal disorders | 300 (41.4%) |
425 (58.6%) |
725 |
15.0% | 0.0107* |
| General disorders and administration site conditions | 322 (44.8%) |
397 (55.2%) |
719 | 14.9% | 0.4007 |
| Respiratory, thoracic and mediastinal disorders | 202 (41.6%) |
284 (58.4%) |
486 | 10.1% | 0.0395* |
| Nervous system disorders | 147 (46.8%) |
167 (53.2%) |
314 | 6.5% | 0.9028 |
*= P < 0.05 vs males.
Table 4.
Reporting odds ratio (ROR) of Individual Cases Safety Reports (ICSRs) signaling adverse reactions to the combination amoxicillin/clavulanic acid vs the adverse reactions to amoxicillin in European Economic Area and United Kingdom in the years 2019-2024. Suspected adverse reactions (SARs) are aggregated according to the System Organ Class (SOC) level.
Table 4.
Reporting odds ratio (ROR) of Individual Cases Safety Reports (ICSRs) signaling adverse reactions to the combination amoxicillin/clavulanic acid vs the adverse reactions to amoxicillin in European Economic Area and United Kingdom in the years 2019-2024. Suspected adverse reactions (SARs) are aggregated according to the System Organ Class (SOC) level.
|
SOC |
Cases of SARs to amoxicillin/ clavulanic acid |
All other cases of SARs to amoxicillin/ clavulanic acid |
Cases of SARs to amoxicillin |
All other cases of SARs to amoxicillin |
ROR of cases of SARs to amoxicillin/ clavulanic acid vs amoxicillin (95% C.I.) |
|---|---|---|---|---|---|
| Skin and subcutaneous tissue disorders | 2338 | 7991 | 1614 | 6286 | 1.13 (1.06-1.22) |
| Immune system disorders | 1127 | 9202 | 910 | 6990 | 0.94 (0.86-1.03) |
| General disorders and administration site conditions | 719 | 9610 | 459 | 7441 | 1.21 (1.07-1.37) |
| Gastrointestinal disorders | 725 | 9604 | 416 | 7484 | 1.36 (1.20-1.54) |
| Respiratory, thoracic and mediastinal disorders | 486 | 9843 | 271 | 7629 | 1.39 (1.19-162) |
| Hepatobiliary disorders | 834 | 9495 | 257 | 7643 | 2.61 (2.26-3.01) |
| Nervous system disorders | 314 | 10015 | 240 | 7660 | 1.00 (0.84-1.19) |
Table 5.
Sex distribution of cases reporting the inefficiency of amoxicillin or of the combination amoxicillin/clavulanic acid, signaled in the European Economic Area and United Kingdom in the years 2020-2024. .
Table 5.
Sex distribution of cases reporting the inefficiency of amoxicillin or of the combination amoxicillin/clavulanic acid, signaled in the European Economic Area and United Kingdom in the years 2020-2024. .
|
Medicinal product |
Total number of serious cases |
Male cases |
Female cases |
Cases reporting “Hepatobiliary disorders” |
Male cases reporting “Hepatobiliary disorders” |
Female cases reporting “Hepatobiliary disorders” |
Significance level P |
| Amoxicillin/ clavulanic acid |
10329 | 4558 | 5771 | 834 | 453 |
381 |
0.00001 |
| Amoxicillin | 7900 | 3219 | 4681 | 257 | 124 |
133 |
0.02211 |
Table 6.
Reporting odds ratio (ROR) of Individual Cases Safety Reports (ICSRs) signaling “Hepatobiliary disorders” as adverse reaction to the combination amoxicillin/clavulanic acid vs amoxicillin in European Economic Area and United Kingdom in the years 2020-2024.
Table 6.
Reporting odds ratio (ROR) of Individual Cases Safety Reports (ICSRs) signaling “Hepatobiliary disorders” as adverse reaction to the combination amoxicillin/clavulanic acid vs amoxicillin in European Economic Area and United Kingdom in the years 2020-2024.
| Medicinal product |
Serious cases of “Hepatobiliary disorders” |
All other serious cases |
ROR of serious cases of “Hepatobiliary disorders” to amoxicillin/clavulanic acid vs amoxicillin (95% C.I.) |
| Amoxicillin/clavulanic acid | 834 | 3983 | 2.78 (2.41-3.24) |
| Amoxicillin | 45 | 3433 |
Table 7.
Sex distribution of cases reporting the inefficiency of amoxicillin or of the combination amoxicillin/clavulanic acid, signaled in the European Economic Area and United Kingdom in the years 2020-2024. .
Table 7.
Sex distribution of cases reporting the inefficiency of amoxicillin or of the combination amoxicillin/clavulanic acid, signaled in the European Economic Area and United Kingdom in the years 2020-2024. .
| Medicinal product |
Total number of cases (serious and non serious) | Male serious and non serious cases |
Female serious and non serious cases | Cases reporting “Drug ineffective” as adverse reaction |
Male cases reporting “Drug ineffective” as adverse reaction |
Female cases reporting “Drug ineffective” as adverse reaction |
Significance level P |
|---|---|---|---|---|---|---|---|
| Amoxicillin/ clavulanic acid |
10329 | 4558 | 5771 | 156 | 80 | 76 | 0.00001 |
| Amoxicillin | 7900 | 3219 | 4681 | 45 | 16 | 29 | N.S. |
Table 8.
Reporting odds ratio (ROR) of Individual Cases Safety Reports (ICSRs) signaling “Drug ineffective” as adverse reaction to the combination amoxicillin/clavulanic acid vs amoxicillin in European Economic Area and United Kingdom in the years 2020-2024.
Table 8.
Reporting odds ratio (ROR) of Individual Cases Safety Reports (ICSRs) signaling “Drug ineffective” as adverse reaction to the combination amoxicillin/clavulanic acid vs amoxicillin in European Economic Area and United Kingdom in the years 2020-2024.
| Medicinal product | Cases of “Drug ineffective” |
All other cases | ROR of cases of “Drug ineffective” to amoxicillin/clavulanic acid vs amoxicillin (95% C.I.) |
|---|---|---|---|
| Amoxicillin/clavulanic acid | 156 | 10173 | 2.68 (1.92-3.73) |
| Amoxicillin | 45 | 7855 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



