Submitted:
30 July 2025
Posted:
07 August 2025
You are already at the latest version
Abstract
We aim to provide a thorough description of the healthcare system of the United States Department of Defense (DOD), also known as the Military Health System (MHS). The MHS Data Repository (MDR) is a highly valuable and well-published data source that has been in existence for many years; however, it has not been thoroughly presented in the literature in a way that would allow real world researchers outside the MHS to assess its fit for pharmaceutical research initiatives. The MDR offers a unique and powerful real-world data platform, distinguished by its closed clinical ecosystem, complete insurance claims data, Electronic Health Records (structured and unstructured), longitudinal familial linkage, and integration with biospecimen repositories, making it ideal for diverse retrospective and prospective research applications.
Keywords:
military health system
; Department of Defense
; familial linkage
; real world data
; fit-for-purpose research
; electronic health records
INTRODUCTION
The increased interest in and accessibility of real-world data (RWD) necessitates a focus on the critical appraisal and comparison of RWD platforms. Rapid expansion of RWD platforms--to include social media, wearable devices, claims data, disease registries, electronic health records (EHR) data, and other technology driven services--has come with increased scrutiny targeting the real world data quality and validity (Cooper JD, Shou K, Sunderland K, Pham K, Thornton JA, DeStefano CB). A fit-for-purpose assessment of the RWD is critical so that the optimal pairing of the data source with the research question of interest can occur and ensure that a reliable and robust study is performed (Reynolds MW, Bourke A, Dreyer NA) (Hall GC, Sauer B, Bourke A, Brown JS, Reynolds MW, LoCasale R). We aim to provide a thorough description of the healthcare system of the United States Department of Defense (DOD), also known as the Military Health System (MHS). The MHS Data Repository (MDR) is a highly valuable and well-published data source that has been in existence for many years; however, while elements of its underpinnings have been described (Rhon), it has not been thoroughly presented in the literature in a way that would allow real world researchers outside the MHS to assess its fit for research initiatives that may be otherwise difficult to study. Our goal is to provide a clear and deep understanding of this RWD source for both retrospective and prospective study applications. We aim to address its strengths and limitations as it pertains to research capabilities and generalizability.
The Military Health System of the United States Department of Defense
At any given time, the MHS supports a patient population of over 9.5 million beneficiaries via direct care (care provided directly via a Military Treatment Facility) and private care under the TRICARE program and is managed by the Defense Health Agency (DHA) (Tanielian T, Farmer C). Direct care, in this context, is free care from the MHS, while private care is care from civilian organizations. DHA data not only encompasses workload, cost, enrollment, demographic, and clinical reference data, but it additionally leverages the ability to link this data to biorepository samples (Health.mil). In 2023 alone, the MHS supported 850,400 inpatient admissions, 87,900,000 outpatient visits, 3,962,600 emergency department visits, 101,700,000 prescriptions, and 89,200 births across the direct care and private sector care systems, with records that can be queried dating back to the early 1990s (Health.mil).
In addition to providing data to assist in direct patient care, the MHS also leverages this data for public health initiatives. Combining MHS data with the Automated Central Tumor Registry (ACTUR), researchers have demonstrated the value of universal access via reporting on social determinants of health and clinical outcomes in colon, breast, and prostate cancer (Hofmann LJ, Lee S, Waddell B, Davis K); (Rizzo JA, Sherman WE, Arciero CA). Pregnancy data is also robust, as highlighted by a recent study assessing exposure of anti-malarial prophylaxis in over 200,000 pregnant women (Gutman JR, Hall C, Khodr ZG, Bukowinski AT, Gumbs GR, Conlin AMS, Wells NY, Tan KR).
An additional powerful public health tool unique to the MHS is the Department of Defense Serum Repository (DODSR), which is managed by the Armed Forces Health Surveillance Directorate (AFHSD). Instituted in 1989, the AFHSD oversees storage of over 74 million serum specimens with an increase of 2 million samples annually (Military Health System). The DODSR’s serial sampling enables assessment of the “pre-diagnosis” state by tracking biomarker changes over time, potentially revealing early disease signatures. Additionally, its broad, population-wide coverage supports large-scale health surveillance, trend analysis, and risk factor identification across diverse demographics and exposures (Perdue CL, Eick Cost AAE, Rubertone MV, Lindler LE, Ludwig SL), (Woeller CF, Thatcher TH, Van Twisk D, Pollock SJ, Croasdell A, Kim N, Hopke PK, Xia X, Thakar J, Mallon TM, Utell MJ, Phipps RP), (Ellis GC, Lanteri CA, Hsieh HC, Graf PCF, Pineda G, Crum-Cianflone NF, Berjohn CM, Sanders T, Maves RC, Deiss R), (Costenbader KH, DiIorio M, Chu SH, Cui J, Sparks JA, Lu B, Moss L, Kelmenson L, Feser M, Edison J, Clish C, Lasky-Su J, Deane KD, Karlson EW).
At a system level, these data resources are routinely used to produce reports for the DoD in the form of Medical Surveillance Monthly Reports (MSMR) and serve as a global resource for reportable events or diagnoses of interest (Military Health System). The MSMR includes updates on rare diseases or diagnoses that affect the military; however, it also offers a starting point to look deeper into topics such as HIV-care, behavioral health, reproductive health, traumatic brain injury, environmental injuries, tropical illness, and many other health conditions.
The unique availability of multiple core real world research components including complete medical claims, prescription claims, Electronic Health Record (EHR) data (both structured and unstructured text data), mortality, over-the-counter medications, linkage to DOD registries and tissue banking, the ability to identify targeted patients for prospective study enrollment (registries, trials, surveys), and more makes the DOD an optimal consideration for most real world study applications, including fit-for-purpose regulatory activities (Sicignano NM, Revel FB, Petruschke R, Barbone FP, Nickolson K, Edison, JD).
DESCRIPTION OF THE DATA SOURCE
The MHS provides two types of care to its beneficiaries. It provides direct care through military treatment facility networks that contain 45 military hospitals and 572 clinics (Health.Mil). It also provides private sector care delivered by civilian institutions and civilian providers, which is globally financed through managed care contracts, primarily with fee-for-service (FFS) reimbursements, though some capitated arrangements exist. Direct care accounts for approximately 35% of the total care provided, with the balance being purchased from civilian providers via TRICARE, the healthcare program and “insurance arm” of the DOD. Data from these distinct DOD-funded care categories is extracted into the MDR (Health.Mil).
The MHS uses electronic health records (EHR) and administrative systems to manage and operate the healthcare system. In 2017, the MHS began replacing its legacy systems (the Composite Healthcare System (CHCS) and Armed Forces Health Longitudinal Technology Application (AHLTA)) with a new commercial EHR from Oracle Cerner. There was a phased implementation of the Oracle Cerner product, MHS GENESIS, which completed in 2024.
The MDR, a data warehouse containing the most complete collection of data about healthcare provided to the beneficiaries of the MHS, receives data from a wide variety of sources throughout the entire enterprise and processes these sources according to a set of published rules called Functional Specifications. These standard processes are managed by the Analytics and Evaluation Division of the DHA. Data in the MDR is made available to a set of “super-users” via an interface platform accessed by a secured portal to allow engagement with the MDR through SAS programming language. Broader access is allowed for proxy query tools such as MHS Mart (M2). The data input and flow through MDR and these proxy tools is illustrated in Figure 1 and described in more detail below.
Defense Enrollment Eligibility Reports System (DEERS)
The Defense Enrollment Eligibility Reports System (DEERS) is a component of the DoD responsible for managing information about benefits received through a DoD association. DEERS provides MDR with a beneficiary level file that contains start/stop dates, type of eligibility (active duty, dependent), and linkage information to all beneficiaries enrolled under a sponsor’s plan. DEERS data are sent and processed monthly.
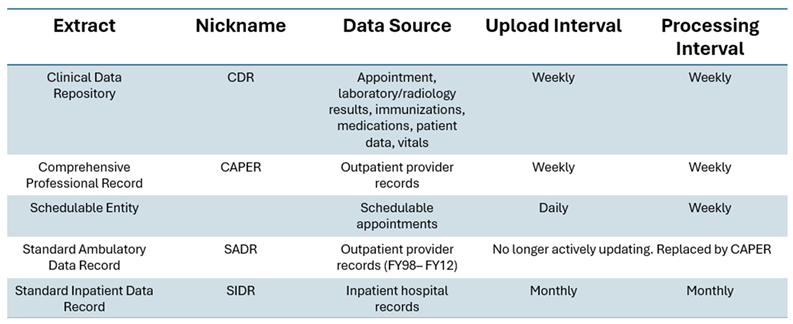
Clinical Data Repository (CDR)
The Clinical Data Repository (CDR) is a warehouse that stores clinical data from the global EHR of the MHS; until 2015, the global EHR was the Armed Forces Health Longitudinal Technology Application (AHLTA). MHS GENESIS subsequently superseded AHLTA (Mukherjee S). Containing more than administrative data, the CDR includes more detailed clinical data, inclusive of: vital signs, radiology, laboratory/pathology orders and results, medication/prescribing orders and fills, clinical notes (structured and unstructured), and immunizations. The CDR data is no longer processed since AHLTA was replaced by MHS GENESIS.
Referral data are available from both the legacy administrative system, CHCS, and MHS GENESIS. The MHS GENESIS data are transmitted to the MDR weekly. Referral data can be linked to the initial appointment that generated the referral and any appointment made with a specialty provider or clinic for that referral within the MTF. Referral data can also be linked to TRICARE claims data. The referral data enables an understanding of referral patterns and access to care.
Private Sector Care
Encounter and provider files representing private sector care are available in the MDR. Information in the claims files are extracted from standard HIPAA 835/837 transactions by the MCSCs. The provider file is a list of providers who can bill TRICARE. Encounters are received daily but are processed into the MDR once a week. The types of files sent include:
• Institutional Claims: Inpatient institutional (hospital, rehab, skilled nursing facility, etc.) claims and home health claims.
• Non-Institutional Claims: All other TRICARE medical (and pharmacy) claims, including outpatient institutional claims.
• Provider Records: Providers who can bill TRICARE.
• Dental Care: Claims and Provider records for Active Duty and Retirees. Designated provider claims and provider files are sent from the designated provider data processing contractor to the MDR once a month.
PATIENT POPULATION AND GENERALIZABILITY
Patient Population
The patient population covered by the DOD via their TRICARE insurance plan is described in great detail via annual public reports, such as this one from Fiscal Year 2023: https://www.health.mil/Reference-Center/Reports/2024/09/23/Annual-Evaluation-of-the-TRICARE-Program-FY24. As noted in this summary, the DOD beneficiary population does include active military, but this accounts for only 15% of the total MHS population of 9.5 million beneficiaries. (Figure 2)
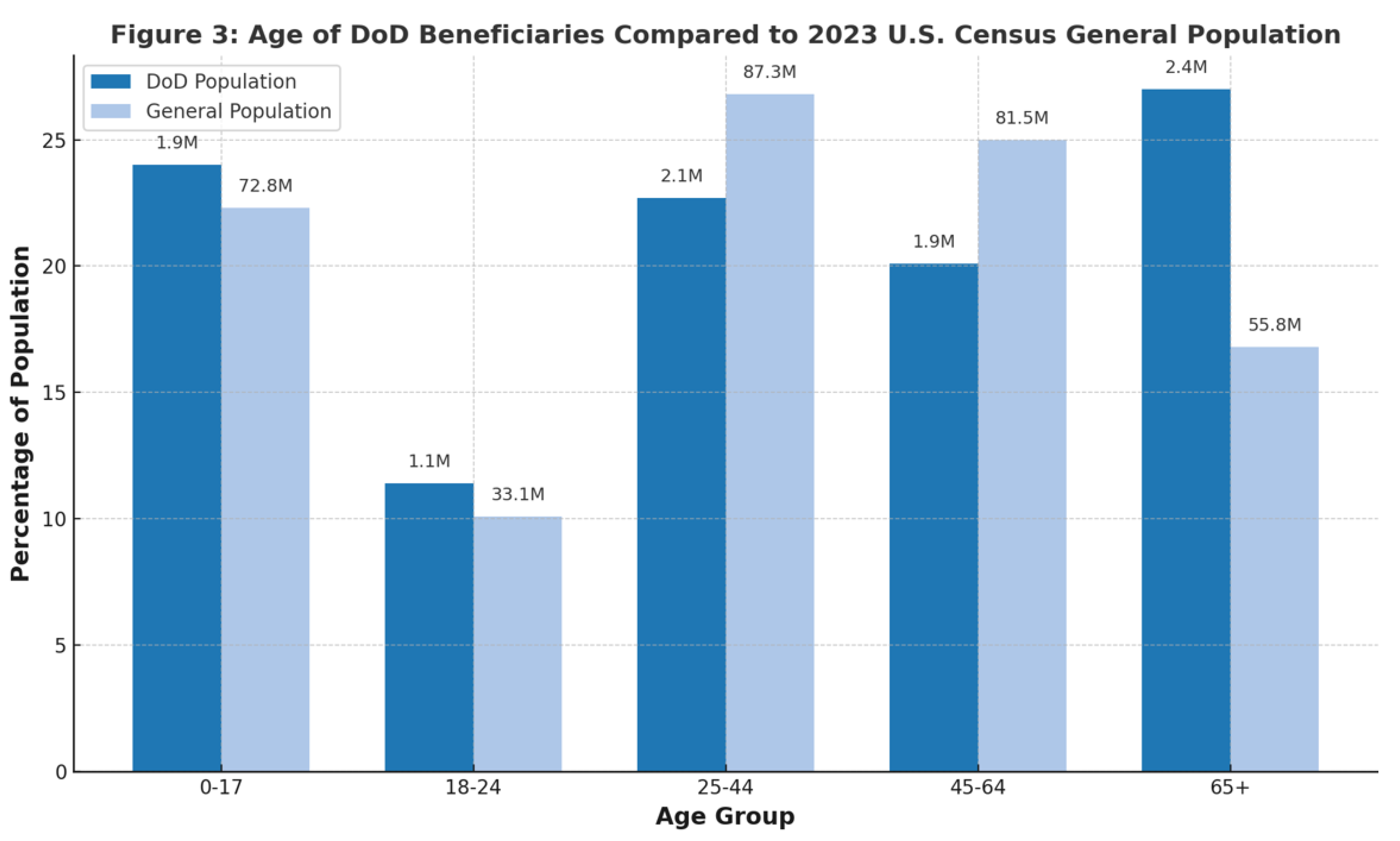
Overall, in the DOD beneficiary population, approximately 24% of all patient lives are aged 0-17 years, compared to 22.3% in the US general population (per 2023 US Census) (Figure 3). The US general population has a slightly higher percentage of patients in the 25-44 year age range (22.7% DOD vs 26.8% US population) and in the 45-64 year age range (20.1% DOD vs 25% US Population). The DOD has a higher percentage of beneficiaries in the 65 year and older range (27%) when compared to the US general population (17%).
The DOD beneficiary population also tracks with the US general population regarding sex; 49% male and 51% female.
While the racial demographics for the full DOD beneficiary population are not readily available, it is reported that the active military population is 70% White, 17% Black, 6% Multi-Race, and 3.6% Asian (Department of Defense).
Mother-Child Linkage
The family linkage in the US DOD population is highly complete and detailed. As a part of that family linkage, the link between mother and children are a hallmark of the population data, resulting in high utility in pregnancy outcome research. Quantifying this, each year across the MHS, approximately 90,000 babies are born, of which about 20-40 percent of those births occur in MTFs, allowing for detailed clinical insight into the health of both mother and children.
A publication from 2017 reporting on the DOD Birth and Infant Health Registry (BIHR) from 2003 to 2014 used data from 1,304,406 infants among military families and 258,332 pregnancies among active duty women. They found that the rates of common adverse infant and pregnancy outcomes were comparable to or lower than those in the general U.S. population. These observations, along with prior BIHR analyses, provide insight that military service is not independently associated with increased risks for select adverse reproductive health outcomes (Bukowinski AT et al.).
Strengths and Limitations
The US DOD clinical ecosystem is a valuable real world data option for clinical and pharmaceutical research fit-for-purpose consideration. It includes a large patient population of approximately 9-10 million active patients at any given point in time, along with decades of retrospective data. The patient population’s clinical care is completely evaluable via a closed-claims network (TRICARE) that tracks all care for its beneficiaries and has almost 8 years of continuous enrollment per patient on average. Approximately 30-40% of all clinical care for this population is provided via DOD clinicians and medical staff at MTFs across the country and around the world. The MTF care is captured in a single consistent EHR that includes structured and unstructured clinical data for these patients, their diseases, and their clinical care. Additionally, since care in the MTF (including medications) is generally free, patients are motivated to fill their prescriptions at the MTFs, including OTC medications, making this a unique real world data source with rich OTC data at the patient longitudinal level.
Rather than tokenization, the data is linked via direct patient identifiers, and the data is traceable and auditable with regards to regulatory expectations and requirements. A complete enrollment and patient benefits portal with DEERS exists that supports familial linkage as well as insight into eligibility for TRICARE and other DOD benefits. Additionally, the DOD claims and EHR data are linkable to several DOD registries with rich consistently and completely collected data such as oncology (ACTUR/ONCOLOG) (Eaglehouse YL, Shriver CD, Lin J, Bytnar JA, Darmon S, McGlynn KA, Zhu K), HIV, tissue banking, and others.
While the DOD system offers a tremendous number of clear and unique benefits for research purposes, there exist a few limitations. While EHR data is available at MTFs, most care is private sector care provided outside of MTFs and only identifiable via TRICARE claims. As an example, if a beneficiary has other health insurance and uses it for care, TRICARE does not see the claim unless there is TRICARE cost sharing. This means for this pocket of patients we will lose preventive services, because those are free to patients per the Affordable Care Act (ACA). For regulatory studies, detailed charts can be requested by DOD PIs/clinicians, but these are not routinely directly available within the DOD system.
While the average length of continuous enrollment in this patient population is significantly longer than any commercial claims dataset, there remains the possibility of losing patients over time. Active military may opt to leave duty and not proceed to retirement eligibility (20 years of service). The average officer in 2009 had been in the military nearly 11 years, which is a slight increase from prior estimates. The average length of service for enlisted personnel has oscillated over the years, currently at an average of 6.7 years (Pew Research Center). This could explain the slightly lower percentage of patients in the 25-64 age groups, as this is the window when many leave active military service. It is possible that active-duty members could also sustain work-related injuries or disabilities, preventing them from continuing in active service. Depending on the injury/disability, it may drive service members to seek the bulk of their care via the Department of Veterans Affairs (VA) (which may or may not be identifiable in the DOD). However, this VA data can be linked to DHA dataset via a database called the DoD and VA Infrastructure for Clinical Intelligence (DaVINCI). This database is discussed in greater detail in other sources (PMID: 36461620.).
The Military Health System Data Repository (MDR) offers a unique and powerful real-world data platform, distinguished by its closed clinical ecosystem, longitudinal familial linkage, and integration with biospecimen repositories, making it ideal for diverse retrospective and prospective research applications. While the data are not available for commercial purchase, the Department of Defense welcomes collaboration through direct partnerships, including via Cooperative Research and Development Agreements (CRADAs), and supports extramural funding pursuits through mechanisms such as the Uniformed Services University (USU) and the Military Health System Research Symposium (MHSRS). Investigators are encouraged to engage with DoD-affiliated researchers to leverage these unparalleled resources for high-impact studies that advance both military and public health.
- Figure Legends
- Figure 1.
References
- Dreyer NA. Advancing a framework for regulatory use of real-world evidence: When real is reliable. Ther Innov Regul Sci. 2018;52(3): 362-368. [CrossRef]
- Reynolds MW, Bourke A, Dreyer NA. Considerations when evaluating real-world data quality in the context of fitness for purpose. Pharmacoepidemiol Drug Saf. 2020 Oct;29(10): 1316-1318.
- Hall GC, Sauer B, Bourke A, Brown JS, Reynolds MW, LoCasale R. Guidelines for good database selection and use in pharmacoepidemiology research. Pharmacoepidemiol Drug Saf. 2012 Jan;21(1): 1-10. [CrossRef]
- Tanielian T, Farmer C. The US Military Health System: Promoting readiness and providing health care. Health Affairs 2019 Aug;38(8). [CrossRef]
- Military Health System. Department of Defense serum repository. URL: https://www.health.mil/Military-Health-Topics/Health-Readiness/AFHSD/Functional-Information-Technology-Support/Department-of-Defense-Serum-Repository.
- Hofmann LJ, Lee S, Waddell B, Davis KG. Effect of race on colon cancer treatment and outcomes in the Department of Defense healthcare system. Diseases of the Colon & Rectum 2010 Jan;53(1): 9-15. [CrossRef]
- Rizzo JA, Sherman WE, Arciero CA. Racial disparity in survival from early breast cancer in the department of defense healthcare system. J. Surg. Oncol. 2015 Feb;111: 819-823. [CrossRef]
- Alexander M, Zhu K, Cullen J et al. Race and overall survival in men diagnosed with prostate cancer in the Department of Defense Military Health System, 1990–2010. Cancer Causes Control 2019 Apr;30: 627–635. [CrossRef]
- Gutman JR, Hall C, Khodr ZG, Bukowinski AT, Gumbs GR, Conlin AMS, Wells NY, Tan KR. Atovaquone-proguanil exposure in pregnancy and risk for adverse fetal and infant outcomes: A retrospective analysis. Travel Medicine and Infectious Disease 2019 Nov;32. [CrossRef]
- Perdue CL, Cost AAE, Rubertone MV, Lindler LE, Ludwig SL. Description and utilization of the United States Department of Defense Serum Repository: A review of published studies, 1985-2012. PLoS ONE 2015 Feb;10(2). [CrossRef]
- Woeller CF, Thatcher TH, Van Twisk D, Pollock SJ, Croasdell A, Kim N, Hopke PK, Xia X, Thakar J, Col. Mallon TM, Utell MJ, Phipps RP. Detection of serum microRNAs from Department of Defense Serum Repository: Correlation with cotinine, cytokine, and polycyclic aromatic hydrocarbon levels. Journal of Occupational and Environmental Medicine 2016 Aug;58(8): S62-S71. [CrossRef]
- Ellis GC, Lanteri CA, Hsieh HC, Graf PCF, Pineda G, Crum-Cianflone NF, Berjohn CM, Sanders T, Maves RC, Deiss R. Coccidioidomycosis seroincidence and risk among military personnel, Naval Air Station Lemoore, San Joaquin Valley, California, USA. Emerg Infect Dis. 2022 Sep;28(9):1842-1846. [CrossRef]
- Costenbader KH, DiIorio M, Chu SH, Cui J, Sparks JA, Lu B, Moss L, Kelmenson L, Feser M, Edison J, Clish C, Lasky-Su J, Deane KD, Karlson EW. Circulating blood metabolite trajectories and risk of rheumatoid arthritis among military personnel in the Department of Defense Biorepository. Annals of the Rheumatic Diseases 2021 Aug;80(8): 989-996. [CrossRef]
- Military Health System. Medical Surveillance Monthly Report. URL: https://www.health.mil/Military-Health-Topics/Health-Readiness/AFHSD/Reports-and-Publications/Medical-Surveillance-Monthly-Report.
- Military Health System. Interface Control Documents (ICDs) functional references and specifications. URL: https://www.health.mil/Military-Health-Topics/Technology/Support-Areas/MDR-M2-ICD-Functional-References-and-Specification-Documents/Interface-Control-Documents-Functional-References-and-Specifications.
- Mukherjee S. Cerner, Leidos, & Accenture win massive $4.3B Defense Department EHR contract. Healthcare Dive. URL: https://www.healthcaredive.com/news/cerner-leidos-accenture-win-massive-43b-defense-department-ehr-contra/403130/.
- Bukowinski AT et al. Department of Defense Birth and Infant Health Registry: Select reproductive health outcomes, 2003–2014. MSMR November 2017;24(11): 39-50.
- Eaglehouse YL, Shriver CD, Lin J, Bytnar JA, Darmon S, McGlynn KA, Zhu K. MilCanEpi: Increased capability for cancer care research in the Department of Defense. JCO Clin Cancer Inform. 2023 Aug;7. [CrossRef]
- Military Health System. Patient Care Numbers for the Military Health System. URL: https://www.health.mil/News/Media-Resources/Media-Center/Patient-Care-Numbers-for-the-MHS.
- Military Health System. MHS Health Facilities. URL: https://www.health.mil/News/Media-Resources/Media-Center/MHS-Health-Facilities.
- Military Health System. Patient Care Numbers for the Military Health System. URL: https://www.health.mil/News/Media-Resources/Media-Center/Patient-Care-Numbers-for-the-MHS.
- Department of Defense. 2023 Demographics: Profile of the Military Community. URL: https://download.militaryonesource.mil/12038/MOS/Reports/2023-demographics-report.
- Pew Research Center. Chapter 6: A Profile of the Modern Military. URL: https://www.pewresearch.org/social-trends/2011/10/05/chapter-6-a-profile-of-the-modern-military/.
- Cooper JD, Shou K, Sunderland K, Pham K, Thornton JA, DeStefano CB. Real-World Pitfalls of Analyzing Real-World Data: A Cautionary Note and Path Forward. JCO Clin Cancer Inform. 2023 Sep;7:e2300097. [CrossRef]
- Rhon DI, Clewley D, Young JL, Sissel CD, Cook CE. Leveraging healthcare utilization to explore outcomes from musculoskeletal disorders: methodology for defining relevant variables from a health services data repository. BMC Med Inform Decis Mak. 2018 Jan 31;18(1):10. [CrossRef]
- Sicignano NM, Revel FB, Petruschke R, Barbone FP, Nickolson K, Edison, JD. Evaluating the Real-World Use of Topical Diclofenac Sodium Gel 1% Using US Longitudinal Electronic Health Records Database: A study supporting OTC switch. Pain Ther (2025). [CrossRef]
Figure 1.
Data Flow Through the MDR.
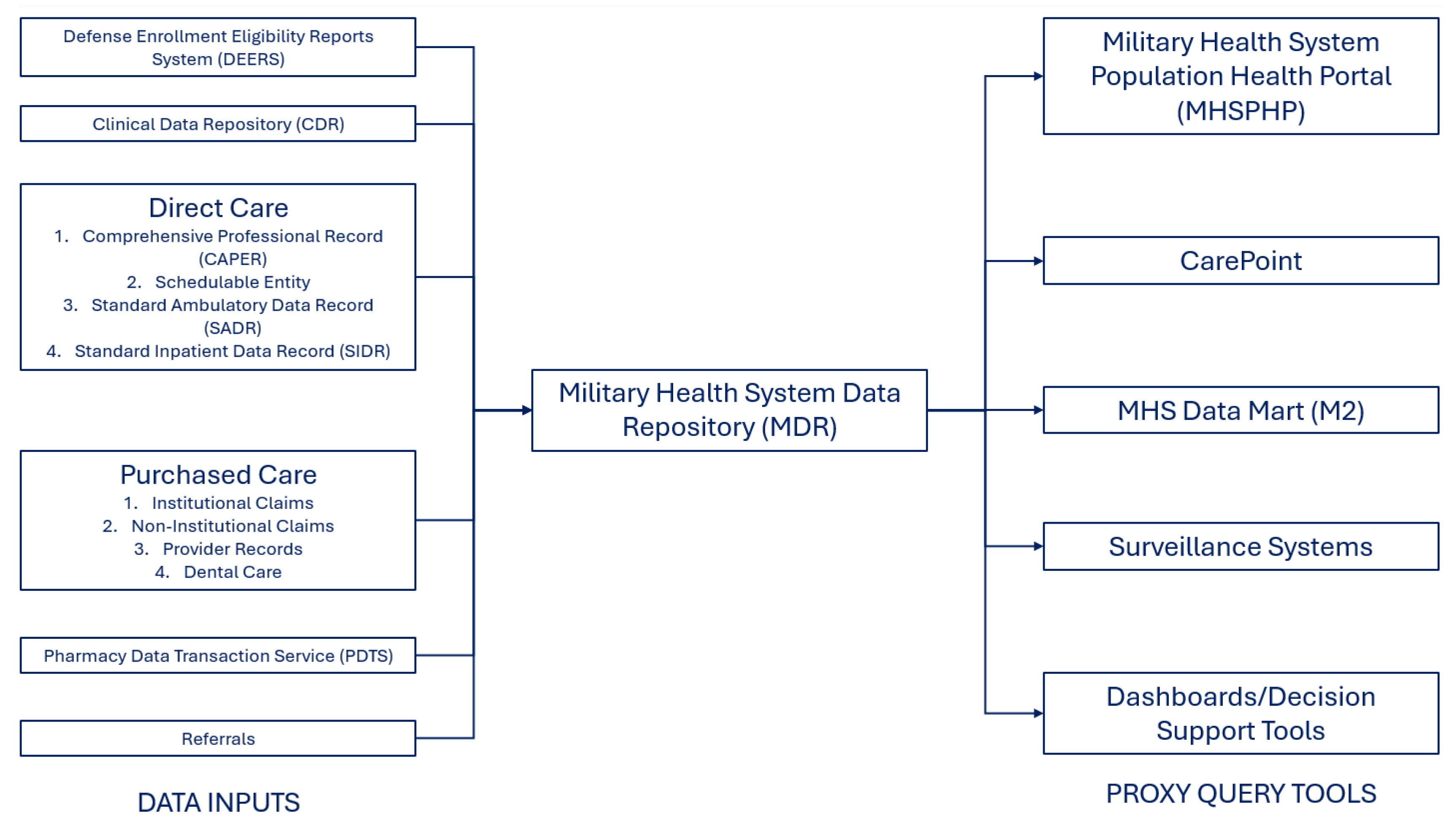
Figure 2.
DOD Beneficiary Classification.
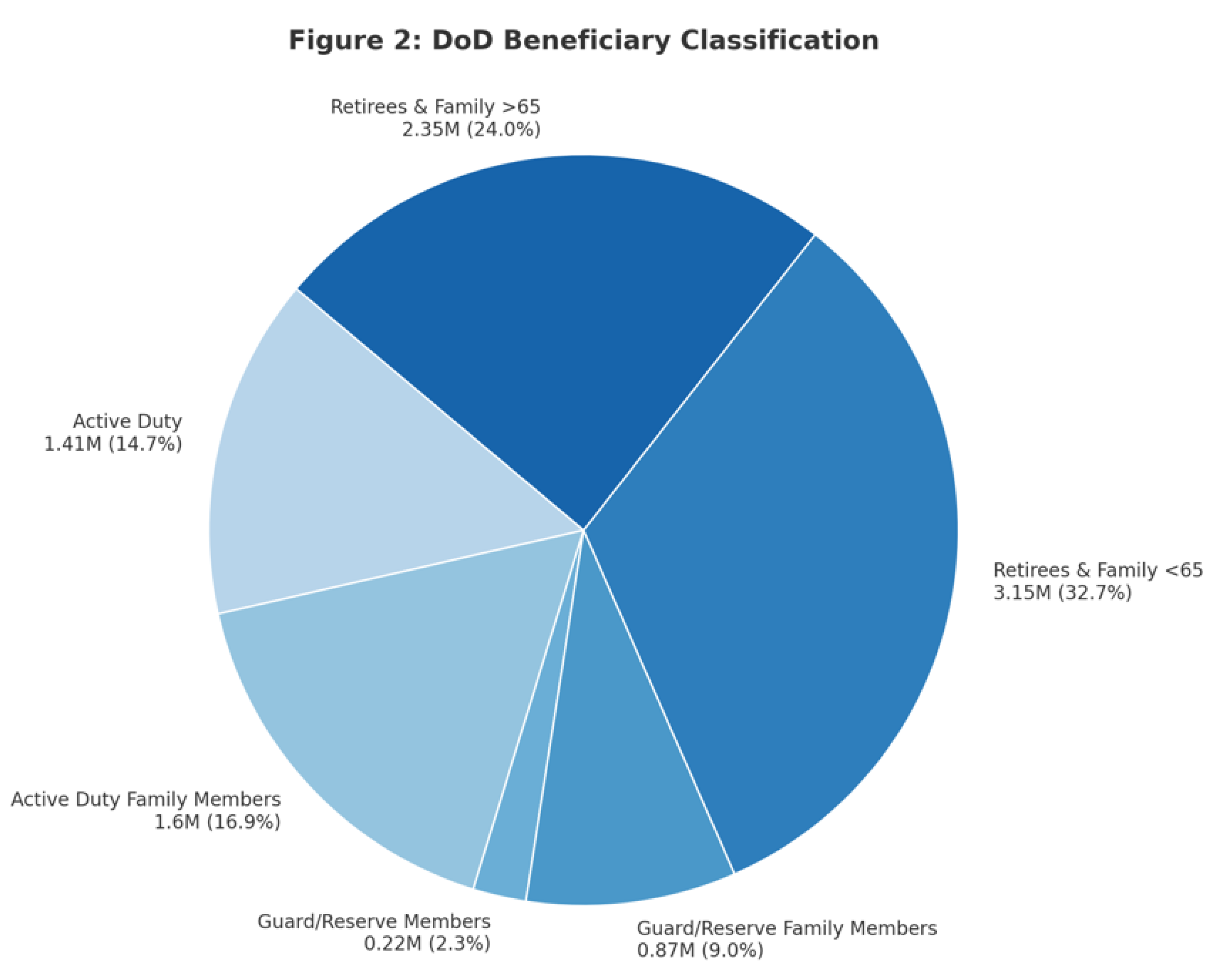
Figure 3.
Age of DOD Beneficiaries compared to the US General Population.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



