Submitted:
04 August 2025
Posted:
05 August 2025
You are already at the latest version
Abstract
Ukraine’s healthcare system shows remarkable resilience in continuing newborn screening (NBS) program, beyond war challenges. Amid the conflict, a Ukrainian newborn screened positive for an extremely rare severe combined immunodeficiency (SCID) —purine nucleoside phosphorylase (PNP) deficiency. Ukraine successfully carried out NBS on neonatal dried blood spot (DBS) by real-time PCR, which showed remarkably reduced T-cell receptor and kappa-deleting recombination excision circles (TREC/KREC). Retesting was delayed due to difficult communication with the family. Whole exome sequencing on a new DBS confirmed the diagnosis. The newborn was candidate for al-logeneic hematopoietic stem cell transplantation (HSCT), the only curative treatment. HSCT is a complex procedure still ongoing in Ukraine despite the conflict. However, due to the psychosocial strain, the family sought medical support in Germany, where HSCT was performed successfully at 6 months. As part of a collaborative initiative with Italy, PNP biomarkers were quantified on the same DBSs using tandem mass spectrometry, according to the protocols established for SCID NBS in Tuscany, serving as a proof of concept of its diagnostic performance. This case highlights the importance of sustaining preventive and life-saving healthcare services, and reflects the key role of international partnerships in upholding the right to healthcare in times of crisis.
Keywords:
newborn screening
; purine nucleoside phosphorylase deficiency
; severe combined immunodeficiency
; war
; public health
; tandem mass spectrometry
; dried blood spot
1. Introduction
Ukraine’s healthcare system is showing a remarkable resilience in continuing preventive health programs, such as newborn screening (NBS) for inherited disorders of the metabolism and immunity, despite the difficulties of the ongoing nation-wide armed conflict. In this paper, we report the case of a Ukrainian male, born amid the war and screened positive at NBS for an extremely rare severe combined immunodeficiency (SCID) —purine nucleoside phosphorylase (PNP) deficiency.
PNP deficiency is an extremely rare autosomal recessive disease, its estimated incidence being of 1 in 50,000–100,000 live births, and it accounts for around 4% of all cases of SCID [1,2]. The disease is due to loss-of-function mutations in the PNP gene located at chromosome 14q11.2, encoding a key enzyme catalysing the reversible phosphorolysis of guanosine (Guo), deoxyguanosine (dGuo), inosine (Ino), and deoxyinosine (dIno), and to their respective purine bases and pentose-1-phosphates. In the presence of a defective PNP function, its substrates undergo alternative metabolic pathways, with accumulation of toxic metabolites. Among them, intracellular accumulation of deoxyguanosine triphosphate (dGTP) derived from dGuo can interfere with DNA synthesis and repair, thus affecting lymphocyte maturation and resulting in a progressive immunodeficiency. The genetic heterogeneity in terms of mutations in the PNP gene results in various levels of residual enzyme activity, determining a wide spectrum of clinical phenotypes ranging from mild adult-onset forms to neonatal-onset SCID [3].
The clinical suspicion of PNP deficiency arises in the presence of recurrent infections caused by common pathogens or opportunistic organisms; also, neurological abnormalities and autoimmunity can occur in up to two-thirds and one-third of the patients, respectively, with hematologic malignancies and developmental delay occurring in some cases [4]. From a laboratory point-of-view, the disease is characterized by T-lymphopenia, varied B-cell abnormalities, and low serum uric acid [5]. Supportive treatments to reduce the risk of infections include immunoglobulin replacement therapy, antimicrobial prophylaxis (i.e., to prevent pneumocystis pneumonia), and the withhold of life vaccines [6,7]. However, hematopoietic stem cell transplantation (HSCT) is considered the only curative treatment for the underlying immunodeficiency [7]. Early HSCT intervention, ideally within the first months of life, is crucial to promptly restore PNP activity, thus allowing immune cell proliferation and metabolic detoxification, before irreversible damage has occurred. Early detection of PNP deficiency by NBS programs is therefore crucial to promptly consider HSCT and avoid severe complications [8,9].
Ukraine has an established NBS for SCID, based on the measurement of T-cell receptor excision circles (TREC) and kappa-deleting recombination excision circles (KREC) levels by quantitative real-time PCR on neonatal dried blood spot (DBS) [10]. The newborn described in this case report was correctly identified as screen positive for SCID at NBS based on TREC/KREC analysis. However, following the confirmed diagnosis, the family seeked for medical help in Germany looking for a safer place to live and care for their child. Biochemical monitoring of markers of PNP deficiency in the pre- and post-HSCT phase was further performed in collaboration with Tuscany (Italy).
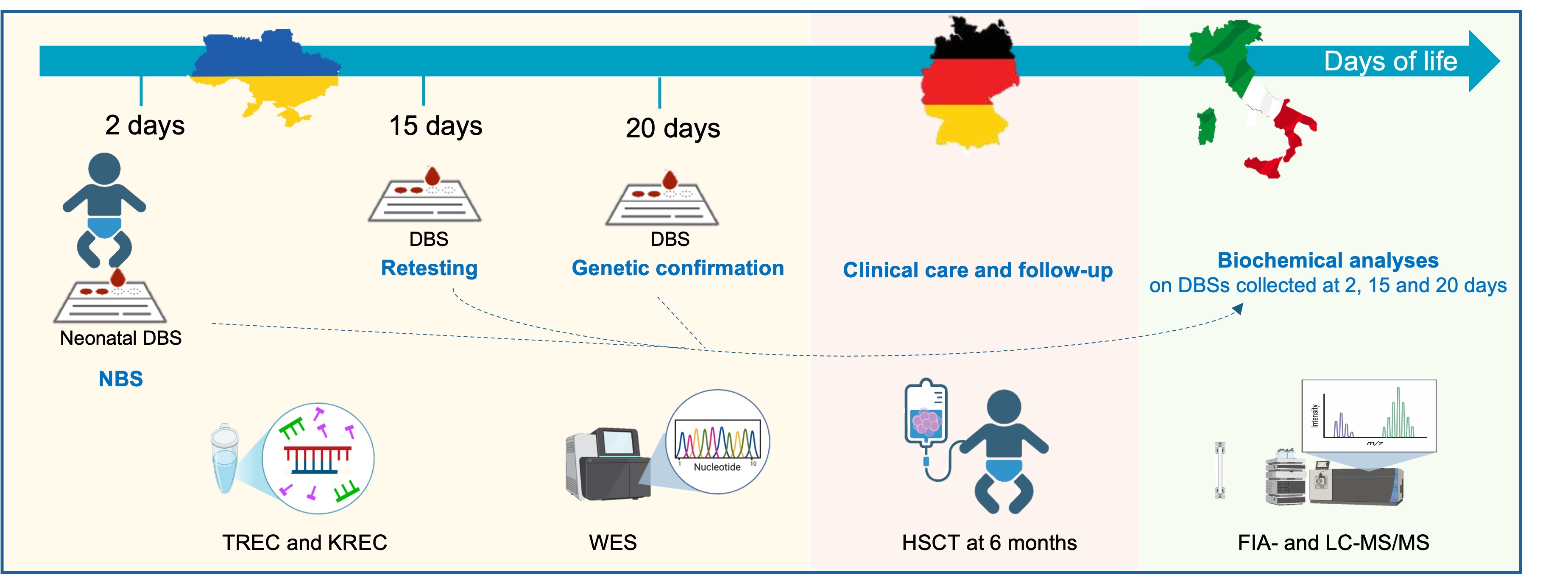
In Tuscany, NBS for SCID is performed by flow injection analysis-tandem mass spectrometry (FIA-MS/MS), via the quantification of Guo, dGuo, Ino and dIno metabolite levels, and second tier test for biochemical confirmatory purposed by liquid chromatograph—tandem mass spectrometry (LC-MS/MS) [11,12,13,14]. Following the implementation of PNP SCID in NBS programs in Tuscany in 2014, no new case of PNP deficiency has been identified out of about 250.000 tests, likely due to the rarity of the disease. In the framework of this international partnership (Figure 1), the neonatal DBS sample of this patient was sent from Ukraine to Tuscany and re-analysed by MS/MS, as a proof-of-concept analysis to confirm the feasibility of MS/MS-based NBS for the detection of this rare SCID.
2. Case Presentation
A male Ukrainian child was born at term in good general conditions. NBS from DBS was performed according to routine protocols at 2 days of life [10]. Shortly after birth, he also received Bacillus Calmette-Guérin (BCG) vaccination, a live attenuated vaccine to prevent mycobacterial infections, according to standard vaccination programs in Ukraine. The result from NBS (available at 5 days) showed remarkably reduced TREC and KREC copy levels (TREC 62 copies; KREC 23 copies; n.v. > 2000 copies), compatible with a SCID profile (Table 1).
According to standard NBS protocols, screen-positive cases should undergo retesting on a new DBS sample. In this case, retesting was delayed due to difficult communication with the parents, and was finally performed at 15 days (with results available at 19 days), confirming the profile (TREC 398 copies; KREC 17 copies). Also, flow cytometry analysis identified the typical phenotype with reduced T and B cells, suggestive of SCID. Genetic test by whole exome sequencing (WES) on a new DBS (collected at 20 days) confirmed the diagnosis of PNP deficiency [c.751delA (p.Ser251Alafs*11)+/+], which was finally made at 40 days of life. The family was counselled about the diagnosis and preventive measures to protect the child from early infections. Live attenuated vaccines (such as BCG) should be withheld in these patients; however, the newborn had been vaccinated immediately after birth, according to routine practice, before NBS results were available. The patient started supportive prophylactic treatments to reduce the risk of infections, including immunoglobulin replacement therapy, and antimicrobial prophylaxis against pneumocystis pneumonia. The child was candidate to allogenic (allo) HSCT with chemotherapy-based conditioning, as first-line curative therapeutic option. Receiving a diagnosis of an extremely rare, progressive and life-threatening disorder which requires such a complex therapeutic approach is always dramatic. To receive it amidst the chaos of a nation-wide war is nothing short of soul-shattering. Allogeneic HSCT is a complex procedure, that is still ongoing in Ukraine despite the logistical and technical difficulties of the conflict. However, to date in Ukraine, there is still no safe place to live or receive medical care. This emotional and physical exhaustion prompted the family to seek clinical help in Germany, looking for a safer, peaceful and confident place to care for their child. The patient was taken in charge at the University Hospital of Freiburg (Germany) at 11 weeks of age. He was in good medical conditions and was continuously free from infections including absence of BCG vaccine-related complications. Flow cytometry analysis confirmed the phenotype of severely reduced T and B cells, including very low naïve T cells. Allogenic HSCT from HLA-matched unrelated donor was finally successfully performed at 6 months of age.
The University Hospital of Freiburg has a longtime established collaboration with the Laboratory of Newborn Screening, Clinical Biochemistry and Clinical Pharmacy (Meyer Children Hospital IRCCS, Florence, Italy) for the quantification of biochemical markers of SCID for diagnostic and follow-up purposes. Quantification of PNP biomarkers Guo, dGuo, Ino, and dIno was performed on the same DBS samples used for TREC/KREC analysis (collected at 2, 15 and 20 days of life), for biochemical confirmation of the profile. After obtaining ad hoc written informed parental consent, we contacted the National Newborn Screening Laboratory in Ukraine, asking to retrieve and send the stored neonatal DBS that had been collected at patient’s birth (2 days of life). Moreover, DBS collected at 15 and 20 days of life were also retrieved and sent to the Meyer children Hospital IRCSS (Florence). The DBS samples were prepared as previously described [11,12], and both first-tier test by FIA-MS/MS and second-tier test by LC-MS/MS were performed according to the published methods [11,12]. Beside PNP biomarkers, also adenosine (Ado) and 2-deoxyadenosine (dAdo), the biomarkers of adenosine deaminase (ADA) deficiency, were quantified [11], due to the similarity between the two syndromes. High levels of purine metabolites Guo, dGuo, Ino, and dIno, were found in all three DBS samples collected at different times, as shown in Table 1 and Figure 2 (for the neonatal DBS). Particularly, analyses on neonatal DBS indicated that the patient would have been classified as screen positive if NBS for PNP deficiency by FIA- and LC-MS/MS was performed.
3. Discussion
This case report underscores the importance of continuing routine preventive health programs, such as NBS, despite critical geo-political scenarios. Indeed, this successful story confirms the key role of NBS for pre-symptomatic diagnosis of PNP deficiency and early therapeutic intervention. A positive screening has a well-known burden on parental well-being and psychosocial functioning, irrespectively of social setting [15,16,17]. We can well imagine how the emotional impact is amplified in families already burdened by a war conflict, as confirmed by the difficulties of initially approaching this family for retesting and confirmatory analyses, further advocating the need to improve multidisciplinary communication strategies. The exodus lived by this family underlines the humanitarian crisis of war, and emphasizes the vital importance of international partnerships between healthcare organizations. Concomitantly, this case offered the opportunity to conduct a proof-of-concept analysis, confirming the diagnostic performance of MS/MS-based NBS for the detection of PNP deficiency on neonatal DBS.
Author Contributions
Conceptualization, R.G. and G.l.M.; Investigation, R.D., N.M., N.S., G.C., C.S. and N.O.; Resources, C.S., N.O. and G.l.M.; Data Curation, R.D.; Writing—Original Draft Preparation, A.B. and R.D.; Writing—Review & Editing, R.D., N.M., N.S., G.C., C.S., N.O., R.G. and G.l.M.; Visualization, A.B. and R.D.; Supervision, G.l.M.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this type of study.
Informed Consent Statement
Informed consent was obtained from the subject’s parents. Written informed consent has been obtained from the patient’s parents to publish this paper.
Data Availability Statement
All data related to this case report are available within the main text of this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NBS | Newborn screening |
| SCID | Severe combined immunodeficiency |
| PNP | Purine nucleoside phosphorylase |
| Guo | Guanosine |
| dGuo | Deoxyguanosine |
| Ino | Inosine |
| dIno | Deoxyinosine |
| dGTP | Deoxyguanosine triphosphate |
| HSCT | Hematopoietic stem cell transplantation |
| TREC | T-cell receptor excision circles |
| KREC | kappa-deleting recombination excision circles |
| DBS | Dried blood spot |
| FIA | Flow injection analysis |
| MS/MS | Tandem mass spectrometry |
| LC | Liquid chromatography |
| BCG | Bacillus Calmette-Guérin |
| WES | Whole exome sequencing |
| Allo | Allogenic |
| Ado | Adenosine |
| dAdo | 2-deoxyadenosine |
| ADA | Adenosine deaminase |
References
- Tangye, S.G.; Al-Herz, W.; Bousfiha, A.; Cunningham-Rundles, C.; Franco, J.L.; Holland, S.M.; Klein, C.; Morio, T.; Oksenhendler, E.; Picard, C.; Puel, A.; Puck, J.; Seppänen, M.R.J.; Somech, R.; Su, H.C.; Sullivan, K.E.; Torgerson, T.R.; Meyts, I. Human Inborn Errors of Immunity: 2022 Update on the Classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol 2022, 42, 1473–1507. [Google Scholar] [CrossRef] [PubMed]
- Hirschhorn, R.; Grunebaum, E.; Roifman, C.; Candotti, F. Immunodeficiency Due to Defects of Purine Metabolism: Territorial Administration under Attack in Orleans and Washington. In Primary Immunodeficiency Diseases: A Molecular and Genetic Approach, 3rd ed.; Ochs, H.D.; Smith, C.I.E.; Puck, J.M. Eds; Oxford Academic: 2013.
- Bardou, M.L.D.; Henriques, M.T.; Grumach, A.S. Inborn errors of immunity associated with characteristic phenotypes. J Pediatr (Rio J) 2021, 97 (Suppl. 1), S75–S83. [Google Scholar] [CrossRef] [PubMed]
- Brodszki, N.; Svensson, M.; van Kuilenburg, A.B.; Meijer, J.; Zoetekouw, L.; Truedsson, L.; Toporski, J. Novel Genetic Mutations in the First Swedish Patient with Purine Nucleoside Phosphorylase Deficiency and Clinical Outcome After Hematopoietic Stem Cell Transplantation with HLA-Matched Unrelated Donor. JIMD Rep 2015, 24, 83–89. [Google Scholar] [PubMed]
- Kütükçüler, N.; Bölük, E.; Tökmeci, N.; Karaca, N.E.; Azarsız, E.; Aksu, G.; Aykut, A. Recurrent infections, neurologic signs, low serum uric acid levels, and lymphopenia in childhood: Purine nucleoside phosphorylase deficiency, an emergency for infants. Turk Pediatri Ars 2020, 55, 320–327. [Google Scholar] [PubMed]
- Alasmari, B.G.; Ibrahim, F.; Wafa, S.; Alshehri, A.; Saeed, M. Purine Nucleoside Phosphorylase Deficiency: A Case Report of an Extremely Rare Disorder. Cureus 2024, 16, e76220. [Google Scholar] [CrossRef] [PubMed]
- Grunebaum, E.; Cohen, A.; Roifman, C.M. Recent advances in understanding and managing adenosine deaminase and purine nucleoside phosphorylase deficiencies. Curr Opin Allergy Clin Immunol 2013, 13, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Martín-Nalda, A.; Rivière, J.G.; Català-Besa, M.; García-Prat, M.; Parra-Martínez, A.; Martínez-Gallo, M.; Colobran, R.; Argudo-Ramírez, A.; Marín-Soria, J.L.; García-Villoria, J.; Alonso, L.; Arranz-Amo, J.A.; la Marca, G.; Soler-Palacín, P. Early Diagnosis and Treatment of Purine Nucleoside Phosphorylase (PNP) Deficiency through TREC-Based Newborn Screening. Int J Neonatal Screen 2021, 7, 62. [Google Scholar] [CrossRef] [PubMed]
- Blom, M.; Soomann, M.; Soler-Palacín, P.; Šedivá, A.; Stray-Pedersen, A.; Zetterström, R.; Speckmann, C.; Gennery, A.R.; van der Burg, M. Newborn screening for SCID and severe T lymphocytopenia in Europe. J Allergy Clin Immunol 2025, 155, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Boyarchuk, O.; Yarema, N.; Kravets, V.; Shulhai, O.; Shymanska, I.; Chornomydz, I.; Hariyan, T.; Volianska, L.; Kinash, M.; Makukh, H. Newborn screening for severe combined immunodeficiency: The results of the first pilot TREC and KREC study in Ukraine with involving of 10,350 neonates. Front Immunol 2022, 13, 999664. [Google Scholar] [CrossRef] [PubMed]
- la Marca, G.; Canessa, C.; Giocaliere, E.; Romano, F.; Malvagia, S.; Funghini, S.; Moriondo, M.; Valleriani, C.; Lippi, F.; Ombrone, D.; Della Bona, M.L.; Speckmann, C.; Borte, S.; Brodszki, N.; Gennery, A.R.; Weinacht, K.; Celmeli, F.; Pagel, J.; de Martino, M.; Guerrini, R.; Wittkowski, H.; Santisteban, I.; Bali, P.; Ikinciogullari, A.; Hershfield, M.; Notarangelo, L.D.; Resti, M.; Azzari, C. Diagnosis of immunodeficiency caused by a purine nucleoside phosphorylase defect by using tandem mass spectrometry on dried blood spots. J Allergy Clin Immunol 2014, 134, 155–159. [Google Scholar] [CrossRef] [PubMed]
- la Marca, G.; Giocaliere, E.; Malvagia, S.; Villanelli, F.; Funghini, S.; Ombrone, D.; Della Bona, M.L.; Forni, G.; Canessa, C.; Ricci, S.; Romano, F.; Guerrini, R.; Resti, M.; Azzari, C. Development and validation of a 2nd tier test for identification of purine nucleoside phosphorylase deficiency patients during expanded newborn screening by liquid chromatography-tandem mass spectrometry. Clin Chem Lab Med 2016, 54, 627–632. [Google Scholar] [CrossRef] [PubMed]
- la Marca, G.; Canessa, C.; Giocaliere, E.; Romano, F.; Duse, M.; Malvagia, S.; Lippi, F.; Funghini, S.; Bianchi, L.; Della Bona, M.L.; Valleriani, C.; Ombrone, D.; Moriondo, M.; Villanelli, F.; Speckmann, C.; Adams, S.; Gaspar, B.H.; Hershfield, M.; Santisteban, I.; Fairbanks, L.; Ragusa, G.; Resti, M.; de Martino, M.; Guerrini, R.; Azzari, C. Tandem mass spectrometry, but not T-cell receptor excision circle analysis, identifies newborns with late-onset adenosine deaminase deficiency. J Allergy Clin Immunol 2013, 131, 1604–1610. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; la Marca, G.; Resti, M. Neonatal screening for severe combined immunodeficiency caused by an adenosine deaminase defect: a reliable and inexpensive method using tandem mass spectrometry. J Allergy Clin Immunol 2011, 127, 1394–1399. [Google Scholar] [CrossRef] [PubMed]
- Cazzorla, C.; Gragnaniello, V.; Gaiga, G.; Gueraldi, D.; Puma, A.; Loro, C.; Benetti, G.; Schiavo, R.; Porcù, E.; Burlina, A.P.; Burlina, A.B. Newborn Screening for Gaucher Disease: Parental Stress and Psychological Burden. Int J Neonatal Screen 2025, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Bush, L.W.; Levy, H.L. Past as Prologue: Predicting Potential Psychosocial-Ethical Burdens of Positive Newborn Screens as Conditions Propagate. Int J Neonatal Screen 2024, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, K.; Jukes, T.; Goobie, S.; DiRaimo, J.; Moran, G.; Potter, B.K.; Chakraborty, P.; Rupar, C.A.; Gannavarapu, S.; Prasad, C. Psychosocial impact on mothers receiving expanded newborn screening results. Eur J Hum Genet 2018, 26, 477–484. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Graphical representation of the clinical and analytical workflow in the framework of an international partnership between Ukraine, Germany and Italy.
Figure 1.
Graphical representation of the clinical and analytical workflow in the framework of an international partnership between Ukraine, Germany and Italy.
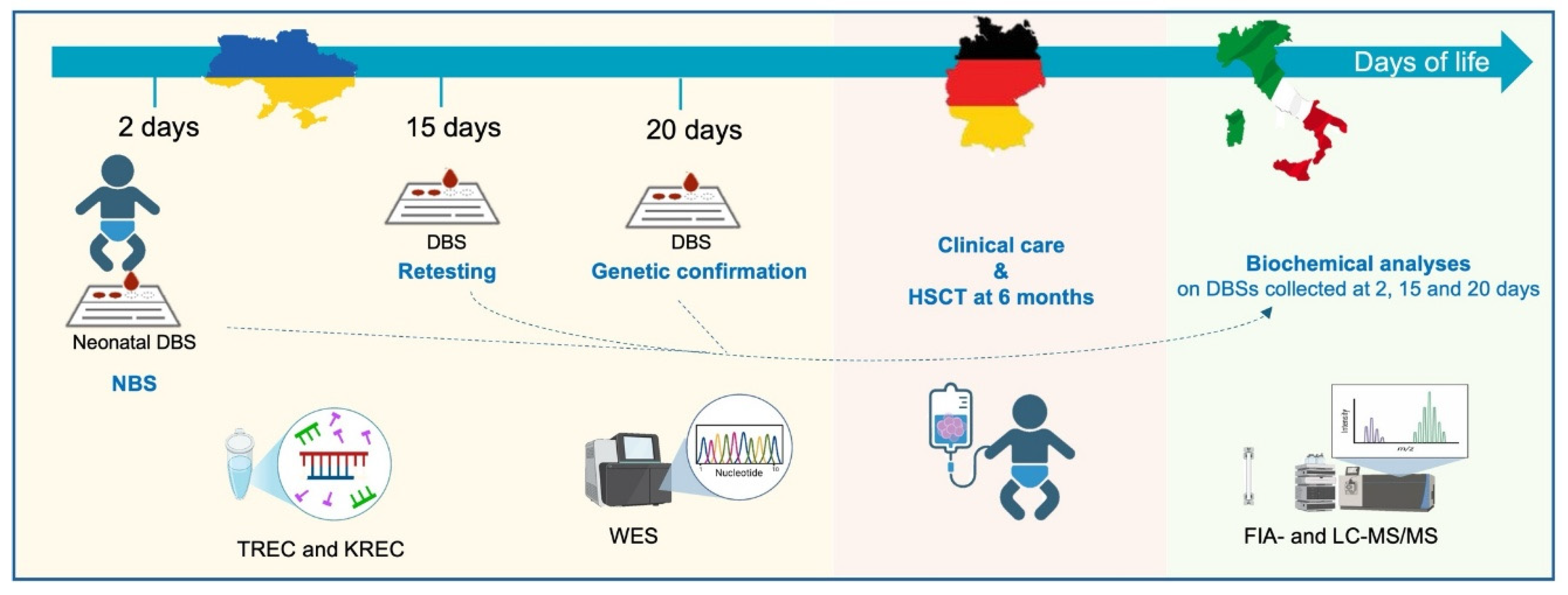
Figure 2.
(a and b) FIA-MS/MS and (c) LC-MS/MS experiments show increased concentrations of Guo, dGuo, Ino, and dIno in the neonatal DBS sample (collected at 2 days of life) of the patient with PNP SCID (b and c) as compared to a control newborn (a).
Figure 2.
(a and b) FIA-MS/MS and (c) LC-MS/MS experiments show increased concentrations of Guo, dGuo, Ino, and dIno in the neonatal DBS sample (collected at 2 days of life) of the patient with PNP SCID (b and c) as compared to a control newborn (a).
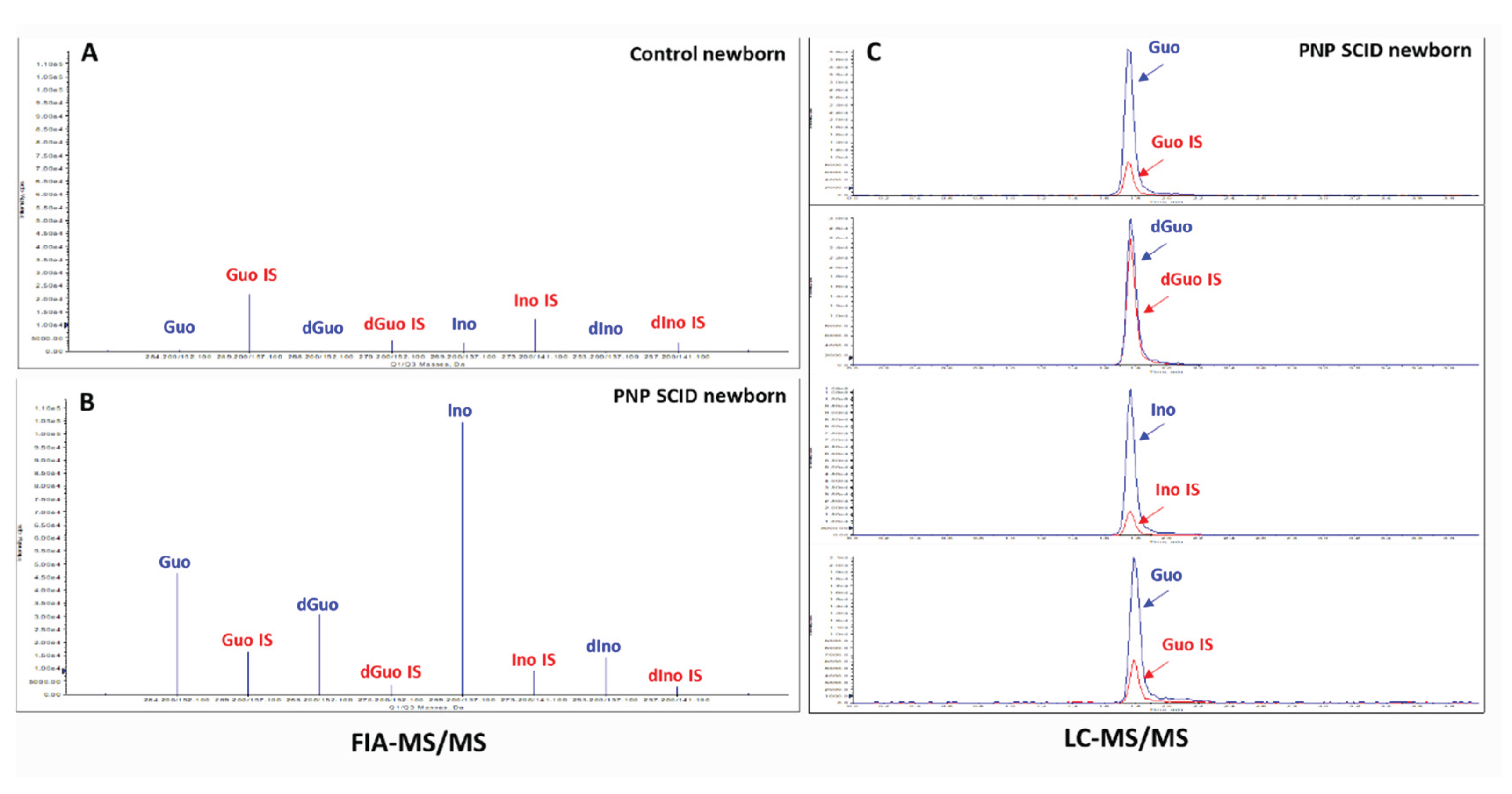

Table 1.
Molecular analysis of TREC and KREC levels, genetic testing and quantification of purine biomarkers of PNP deficiency by MS-MS, in the DBS samples collected at 2, 15 and 20 days of life.
Table 1.
Molecular analysis of TREC and KREC levels, genetic testing and quantification of purine biomarkers of PNP deficiency by MS-MS, in the DBS samples collected at 2, 15 and 20 days of life.
| Neonatal DBS (2 days) |
1st Retest (15 days) |
2nd Retest (20 days) |
|
|---|---|---|---|
| TREC § (n.v. > 2000 copies) | 62 | 398 | - |
| KREC § (n.v. > 2000 copies) | 23 | 17 | - |
| Whole exome sequencing (WES) § | - | - | c.751delA (p.Ser251Alafs*11)+/+ |
| First tiest test by FIA-MS/MS * | |||
| Guo (n.v. < 4.9 μmol/L) | 16.9 | 8.8 | 3.3 |
| dGuo (n.v. < 0.6 μmol/L) | 14.1 | 6.1 | 4.7 |
| Ino (n.v. < 61.5 μmol/L) | 67.9 | 66.8 | 97.7 |
| dIno (n.v. < 7.7 μmol/L) | 29.0 | 97.7 | 8.9 |
| Second tiest test by LC-MS/MS * | |||
| Guo (n.v. < 1.1 μmol/L) | 46.4 | 33.8 | 10.2 |
| dGuo (n.v. 0 μmol/L) | 12.5 | 6.7 | 4.3 |
| Ino (n.v. < 16.8 μmol/L) | 58.8 | 61.0 | 91.8 |
| dIno (n.v. < 0.1 μmol/L) | 36.5 | 14.5 | 10.1 |
§ Performed at the National Specialized Children’s Hospital “Ohmatdyt”, Kyiv, Ukraine. * Performed at the Meyer Children Hospital IRCCS, Florence, Italy. ADA SCID biomarkers (Ado and dAdo) were within normal range in FIA-MS/MS and LC-MS/MS.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



