
Submitted:
01 August 2025
Posted:
04 August 2025
You are already at the latest version
Abstract
The concept of mechanical power (MP) has emerged as a comprehensive indicator of ventilator-induced lung injury (VILI), integrating the effects of tidal volume, airway pressures, respiratory rate, and flow. However, applying MP as an absolute threshold (e.g., 12 J/min) across heterogeneous patients with acute respiratory distress syndrome (ARDS) may be inadequate. This article explores a rheological model for the respiratory system that reconceptualizes the lung as a viscoelastic body and advocates for individualized MP thresholds. We propose adjusting MP based on ideal body weight (J/min/kg) and, more accurately, on static compliance (J/min/L), which better reflects functional lung size ("baby lung") and mechanical vulnerability. This normalization offers a more precise risk stratification and easier setting of ventilation targets, particularly in patients with low compliance or abnormal body composition. Emerging evidence suggests that normalized MP correlates more closely with mortality than absolute MP values and aligns with the physiological stress-strain behavior of pulmonary tissue. Adopting MP normalization within lung-protective strategies could enhance the safety and efficacy of mechanical ventilation, however clinical validation is still required. This review summarizes the theoretical foundations, supporting evidence, and clinical implications of this approach within the broader context of rheological modeling in ARDS.
Keywords:
acute respiratory distress syndrome
; ventilator-induced lung injury
; rheology
; mechanical ventilation
; driving pressure
; mechanical power
; strain
; stress
; lung protective ventilation
; materials science
1. Introduction
Rheology is the branch of physics that studies the deformation and flow of matter. It is a part of continuum mechanics that studies the data obtained when a force (load) is applied to a specific material in an experimental setting. Its primary objective is to find the "constitutive equations" of each material: mathematical models (generally differential equations of tensorial character) that describe the relationship between the stress suffered by the material and the strain induced by the applied force [1].
Acute respiratory distress syndrome (ARDS) represents one of the greatest challenges in the management of critically ill patients. For decades, ventilatory strategies have evolved based on concepts such as barotrauma, volutrauma, atelectrauma, and biotrauma. However, these models have shown limitations in fully understanding the pathophysiological mechanisms of ventilator-induced lung injury (VILI) [2,3].
The application of concepts derived from rheology and materials science, based on experimental evidence in laboratory animals and recent human research, has enabled the development of a new paradigm that explains the mechanisms of lung damage during mechanical ventilation more precisely than theories used in the past [4]. This rheological approach considers the lung as a viscoelastic body subject to deforming forces whose magnitude, frequency, and velocity determine the development of structural lesions (Table 1) [2,3].
Key concepts of rheological theory applied to the lung include the following:
Stress. Stress is the value of the maximum limit of force per unit area [1]. It corresponds to the transpulmonary pressure (PTP) difference between inspiration and expiration. PTP is the difference between alveolar pressure (Palv) and pressure within the pleural space (Ppl) [2]. It is assumed that clinically, pleural space pressure (mediastinal pressure) can be estimated by measuring esophageal pressure (Pes).
Strain, deformation, or relative displacement. This is the multidimensional deformation suffered by the body, i.e., the change in shape relative to the original state [1]. In classical respiratory physiology, the concept of strain does not exist, but its equivalent could be considered the quotient between tidal volume (VT) and functional residual capacity (FRC).
Young's Modulus (Figure 1). To generate knowledge about the physical behavior of each body, rheology performs what we call tensional experiments. Different solid materials are subject to increasing axial tension until fracture or rupture occurs. Each material’s behaviour is described by what is called the stress-strain curve. In all stress-strain curves, an initial zone that is linear can be identified, defining its elastic behavior [4,5]. The equation of this linear part is called the constitutive equation of an elastic solid (Hooke's Law). The proportionality constant (the slope of this line) EY (cmH₂O) is called the Young's modulus of elasticity of the solid. The Young's modulus of the respiratory system is called specific lung elastance (ESL).
Strain rate or deformation velocity. The velocity at which relative deformation occurs with respect to its original position [1]. In classical respiratory physiology, this would correspond to flow divided by FRC.
Driving pressure (DP). DP corelates the classic model with the rheological model. DP = plateau pressure – total positive end-expiratory pressure (total PEEP). Marini et al. [6] found a good correlation between stress (PTP) and DP. Chiumello et al. [7] corroborated this point and additionally determined a threshold DP value of 15 cmH₂O that would have very good diagnostic accuracy for detecting that the lung is being subjected to stress equal to or greater than 12 (strain of 1), the point from which VILI would begin.
Mechanical power (MP). In 2016, Gattinoni et al. [8] developed the concept of MP. To date, this is the model that has most successfully approximated rheological theory and classical respiratory physiology. It attempts to combine all parameters, both static and dynamic, that would play a role in generating the energy that the ventilator delivers to the lung and airways per unit time.
Resilience. This is the deformation per unit volume (J/m³) produced within a material when stress is applied from a base state to the yield point [1,4]. It constitutes the maximum capacity of a material to absorb energy when elastically deformed and then, upon unloading, completely recover this energy without losses (Figure 2).
Is it worth mentioning/providing a definition the Elastic Region? Haven’t seen anything specifically about it in other articles/talks
Figure 1.
Stress-strain curve. EY: Young's modulus of elasticity.
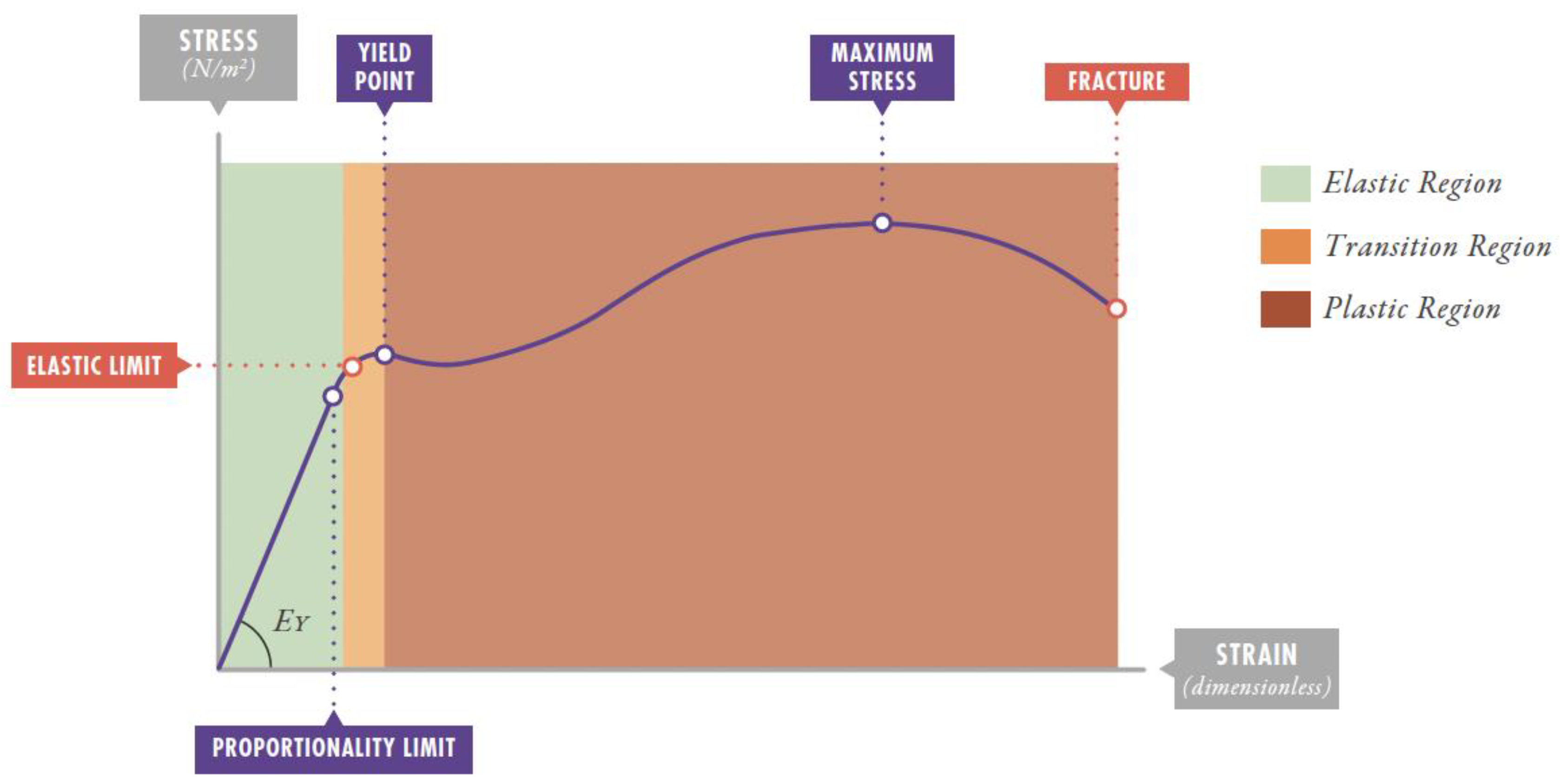
Figure 2.
Resilience: maximum energy that can be stored in an elastic body and subsequently recovered without any loss (left). Pathogenesis of ventilator-induced lung injury: deformation energy exceeds resilience (right). σy: stress at maximum elasticity point; εy: strain at maximum elasticity point; U: resilience.
Figure 2.
Resilience: maximum energy that can be stored in an elastic body and subsequently recovered without any loss (left). Pathogenesis of ventilator-induced lung injury: deformation energy exceeds resilience (right). σy: stress at maximum elasticity point; εy: strain at maximum elasticity point; U: resilience.
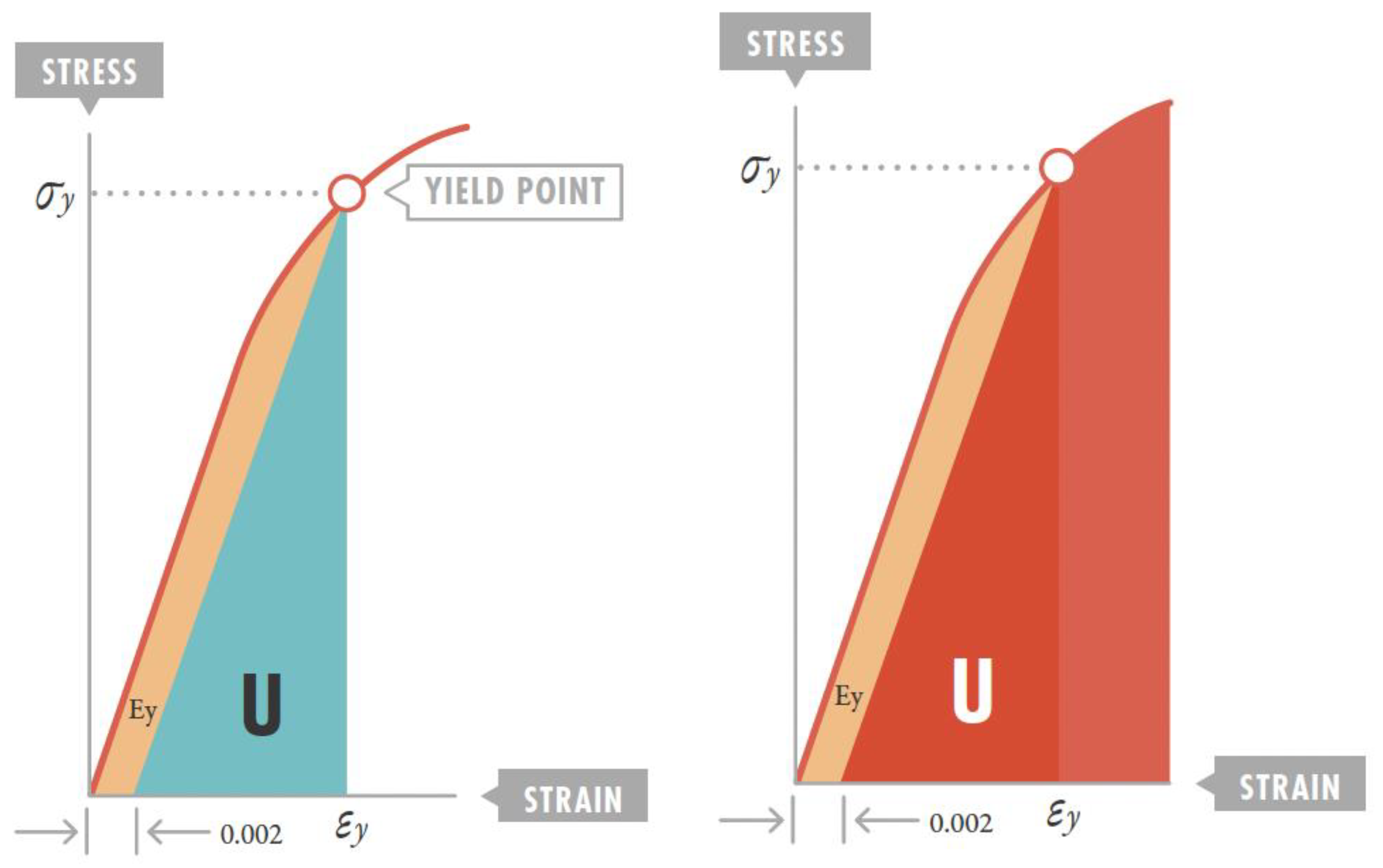

Table 1.
Fundamental concepts of rheology applied to the respiratory system.
| Concept | Physical Definition | Pulmonary Application | Units |
|---|---|---|---|
| Stress | Force per unit area (f/A) | Transpulmonary pressure (PTP) | cmH₂O |
| Strain | Relative deformation (dX-dX₀)/dX₀ | Tidal volume/Functional residual capacity (VT /FRC) | Dimensionless |
| Strain rate | Deformation velocity | Flow/FRC | s⁻¹ |
| Young's Modulus (EY) | Proportionality constant between stress and strain | Specific lung elastance (ESL) | cmH₂O |
| Driving pressure (DP) | Difference between plateau pressure and PEEP | Clinical approximation to pulmonary stress | cmH₂O |
| Mechanical power (MP) | Energy per unit time | Energy delivered to respiratory system per minute | J/min |
| Resilience | Maximum energy storable without permanent deformation | Energy threshold to prevent VILI | J/m³ |
F: force; A: area; PTP: transpulmonary pressure; cmH₂O: centimeters of water; VT: tidal volume; FRC: functional residual capacity; EY: Young's modulus; DP: driving pressure; ESL: specific lung elastance; MP: mechanical power; VILI: ventilator-induced lung injury.
2. Refutation of Classical VILI Theories. New VILI Concepts
Since the 1970s, two static variables have been fundamentally studied as VILI inducers: pressure and volume.
Initially, the concept of barotrauma emerged, relating excessive peak airway pressure (greater than 36 cmH₂O). A decade later, experimental studies demonstrated that when generated volumes were relatively low, pressures up to 45 cmH₂O did not induce lung injury, and high volumes did cause injury despite using low pressures [9].
Volume then became considered the main determinant of VILI. This concept continued developing, and in 2000, the ARDS Network trial was published in The New England Journal of Medicine, [10] proving that ventilating ARDS patients with volumes of 6 mL/kg ideal body weight versus 12 mL/kg reduced mortality.
Simultaneously with volutrauma studies, several works began investigating the modulating role that PEEP could have. In the 1990s, this idea gave rise to the concept of atelectrauma, which considers that periodic opening and closing of collapsed alveolar units also generates tissue damage. Marcelo Amato et al. [11] published in 1995 one of the first clinical studies in ARDS patients comparing this new ventilatory strategy, called "open-lung," with the classical strategy, giving weight to using PEEP above the lower inflection point of the pressure-volume curve.
In the late 1990s, Slutsky et al. [12] developed the concept of biotrauma, which attributes part of both local and systemic lesions to the inflammatory reaction triggered in damaged lung tissue.
In summary, the classical theories explaining VILI development have been:
4.Biotrauma: inflammatory response secondary to mechanical damage [12].
However, these theories present important limitations:
González-López et al. [14] demonstrated in 2012 that patients ventilated with lower driving pressures (22.6 ± 6 cmH₂O) but with lower PEEP experienced greater pulmonary inflammation despite receiving protective tidal volumes of 7 mL/kg. This finding directly contradicts barotrauma theory, suggesting that pressure alone does not explain lung damage.
Rahaman [15] provided mathematical proof that ventilation of healthy lungs with tidal volumes of 6-10 mL/kg should not cause VILI, since the generated strain (0.17-0.29) produces stress (2.31-3.86 cmH₂O) well below the harmful threshold. However, upon reaching total lung volume (strain of 1.5), the resulting stress (17 cmH₂O) exceeded the safety threshold, explaining why conventional ventilatory strategies do not cause damage in healthy lungs but can be injurious in ARDS.
The LUNG SAFE study [16] and Amato et al.'s meta-analysis [17] in 2015 revealed that DP was the factor most consistently associated with mortality, regardless of tidal volume, plateau pressure, or PEEP values used, thus questioning classical theories.
These findings suggest that traditional theories are incomplete and that a model based on rheological principles offers a more coherent explanation of VILI mechanisms.
Rheological theory considers the lung as a viscoelastic body whose behaviour can be described by Voigt's constitutive equation [18]:
Stress = EY × Strain + η × Strain rate
EY: Young's modulus (specific elastance); η: viscosity coefficient
Thus, from a physical standpoint, it is reasonable to assume that the respiratory system behaves as a viscoelastic body. In fact, in the context of mechanical ventilation, at least three phenomena related to the viscoelastic properties of the respiratory system have been identified:
Dynamic hysteresis (in the dynamic pressure-volume loop).
Relaxation index or stress relaxation (P1-P2 difference after a 5-second inspiratory pause).
Stress index.
3. New VILI Concepts Related to Rheological Theory
3.1. The Lung as an Elastic Solid
Gattinoni et al. [19] demonstrated in 2008 and Protti et al. [20] in 2011 that the lung behaves as an elastic solid, with a linear relationship between stress and strain, fulfilling Hooke's law:
ΔPTP = ESL × (VT /FRC)
ΔPTP: transpulmonary pressure increment; ESL: specific lung elastance; VT: tidal volume; FRC: functional residual capacity
3.2. Strain Threshold and VILI Development
The lung's stress-strain curve shows a linear relationship up to strain values near 1, losing linearity between 1.5 and 2. This point marks the elastic limit beyond which irreversible microfractures begin to occur in lung parenchyma [20].
In animal experiments, Protti et al. [20] demonstrated that VILI risk increased exponentially with strain value. Animals without VILI presented strain values of 1.29 ± 0.57, while those with VILI had values of 2.16 ± 0.58 (p < 0.001), with associated mortality of 86% after only 60 hours of mechanical ventilation.
3.3. Stress and Strain Estimation with the Ventilator
The rheological model and classical elastic-resistive model represent distinct and, in principle, incommensurable (mutually exclusive?) paradigms. The main limitation for applying the rheological model in clinical practice is the difficulty of estimating FRC at the bedside using a conventional ventilator. However, recent studies have established functional equivalence between both approaches [23].
Cortés-Puentes et al. [6] demonstrated a consistent relationship between rheological stress (ΔPTP) and driving pressure (DP), a parameter easily measurable clinically as the difference between plateau pressure (Pplat) and total PEEP, both measured under static conditions. The ΔPTP/DP ratio oscillates between 0.46 and 0.79, being approximately 0.75 in ARDS patients, and remains stable with PEEP changes, although it decreases with elevated intra-abdominal pressure (except in ARDS).
Chiumello et al. [23] replicated these findings and confirmed significant correlation between stress and DP (R² = 0.7; p < 0.001). In ARDS patients, stress represents between 73 and 85% of DP. Considering that lung Young's modulus (specific elastance) in human ARDS is 13 cmH₂O, it follows that pulmonary stress equal to or greater than this value can induce VILI.
Chiumello et al. [23] validated DP use as a marker of injurious stress, establishing a clinical threshold of 15 cmH₂O with high diagnostic capacity (AUC = 0.864; 95% CI: 0.80-0.93; sensitivity = 0.90; specificity = 0.78). This threshold identifies the presence of pulmonary stress ≥ 12 cmH₂O, associated with VILI risk.
In conclusion, DP represents the key parameter that allows establishing a connection between the classical elastic-resistive model and the rheological model, thus providing functional equivalence between both paradigms. A DP threshold value of 15 cmH₂O, which in humans is associated with an approximate strain of 1.5, appears to mark the elastic limit beyond which VILI is induced.
Along these lines, Rahaman et al. [15], applying rheological theory, offer a coherent explanation for a widely observed fact in clinical practice: conventional mechanical ventilation does not induce VILI in healthy lungs. Under physiological conditions, healthy lung FRC is approximately 35 mL/kg, while total lung capacity (TLC) reaches 85 mL/kg [24]. If a ventilatory strategy were applied that brought end-inspiratory volume to TLC and end-expiratory volume to FRC, the resulting strain would be 1.5. This deformation level translates, according to specific elastance modulus (ESL), into stress (ΔPTP) equivalent to a driving pressure clearly superior to the 15 cmH₂O threshold, thus positioning in a range capable of generating VILI even in a previously healthy lung.
Conversely, in the same lung, using tidal volumes of 6 mL/kg (strain = 0.17; stress = 2.31 cmH₂O; DP = 2.89 cmH₂O) or even 10 mL/kg (strain = 0.29; stress = 3.86 cmH₂O; DP = 4.82 cmH₂O) is considered safe, as it remains well below the injurious threshold. This practice is same as the ventilatory strategy traditionally employed in patients without lung disease, supporting its safety from a rheological perspective.
3.4. Mechanical Power and Injury Threshold
MP integrates all factors capable of producing VILI (VT, pressures, frequency, and flow) into a single physical magnitude representing energy transmitted to the respiratory system per unit time [25].
The simplified formula for its calculation is:
MP (J/min) = 0.098 × RR × VT × (PIP – DP/2)
MP: mechanical power; RR: respiratory rate; VT: tidal volume; PIP: peak inspiratory pressure; DP: driving pressure.
Gattinoni et al. [26] experimentally demonstrated the existence of an MP threshold (approximately 12 J/min) above which VILI occurs, regardless of the combination of ventilatory parameters used.
4. Ventilatory Strategy in ARDS from Rheological Perspective
4.1. Mechanical Power Adjustment by Ideal Weight or Compliance
MP adjustment by ideal body weight (IBW) or compliance (C) is a crucial aspect of the rheological model that deserves greater attention since MP as an absolute value (12 J/min) presents important limitations by not considering individual patient characteristics [25,26,27,28,29,30,31]:
1.It was derived primarily from studies in animal models with homogeneous anatomy/structural features.
2.Body size differences between patients were not accounted for.
3.Differences in the proportion of functional "baby lung" available in each ARDS case were not adjusted.
4.Differences in lung compliance between patients were not factored in.
Thus, MP could be normalized by patient's ideal weight [27,28,29,30,31], providing a more individualized value:
- Normalized MP (J/min/kg) = Total MP (J/min)/Ideal weight (kg).
Preliminary studies suggest that a threshold of approximately 0.25-0.3 J/min/kg might be more appropriate.
This approach is similar to VT normalization by ideal weight already routinely used.
Or it could be normalized by compliance [27,28,29,30,31], potentially more precise than ideal weight adjustment, as it directly reflects functional lung tissue:
- Specific MP (J/min/L) = Total MP (J/min)/Static compliance (L/cmH₂O)
The advantage of this approach is that it considers the severity of lung involvement in each individual patient, adjusting the "dose" of mechanical energy according to available functional tissue. This adjustment attempts to represent the theory of ARDS lung as a "baby lung" [33].
Some recent studies have begun exploring these normalizations (IBW and compliance):
Serpa Neto et al. [34] found that compliance-normalized MP showed better correlation with mortality than absolute MP.
Gattinoni et al. [33] subsequently proposed the concept of "specific mechanical power" that considers the baby lung.
Cressoni et al. [25] suggested that the injury threshold might be between 0.12-0.15 J/min per mL of functional lung tissue.
Ito et al.[29] have shown that weight adjustment underestimates MP compared to compliance-adjusted MP in pediatrics.
1.Patients with severe ARDS (lower compliance) would require lower absolute MP thresholds.
2.Patients with preserved compliance could tolerate higher absolute MP values.
3.Ventilatory strategy could be dynamically adjusted according to compliance evolution.
4.It would allow more precise comparisons between patients with different characteristics.
However, to implement this approach requires:
1.Clinical studies validating specific normalized MP thresholds.
2.Practical methods to estimate baby lung volume at bedside.
3.Algorithm development to automatically adjust ventilatory parameters according to normalized MP.
4.Validation in specific populations (pediatric, obese, etc.).
In summary, this perspective of MP adjustment by ideal weight or compliance represents an important advance in individualized protective ventilation and is aligned with fundamental principles of the rheological model. However, it is important to note that research in this field continues evolving and more studies are needed to establish definitive normalized MP thresholds.
4.2. VILI Development Dynamics and Recruitment. Optimal PEEP
VILI is a time-dependent phenomenon. Gattinoni et al. [39] demonstrated in 2013 that VILI development follows a temporal relationship with applied strain:
With strain of 2.5: detectable VILI occurs at 6 hours with 100% mortality at 48 hours.
With strain of 1.154 and 0.556: VILI was detectable at 24 and 36 hours respectively.
With strain of 0.217: absence of VILI after 60 hours of ventilation despite using end-inspiratory volumes equal to TLC (with initial inspiratory Pplat values of 36 ± 3 cmH₂O), not only does VILI not appear, but Pplat values at experiment end were the lowest among the four cohorts.
It is important to highlight that none of the theories proposed to date to explain the etiopathogenic mechanism of VILI (barotrauma, volutrauma, atelectrauma, biotrauma) have explicitly considered a mechanism that included ventilation application time as an important responsible factor.
Therefore, VILI development occurs exponentially, initiating in interface zones of naturally non-homogeneous structures (subpleural microatelectasiae, peribronchial and intraparenchymal areas). These zones act as "stress multipliers" (stress raisers), similar to material fatigue mechanisms [2].
A crucial finding was that these initial VILI densities only appear in computed tomography images performed during expiration, indicating they are highly recruitable areas. This suggests that adequate PEEP use could prevent their appearance by maintaining more homogeneous parenchyma [40].
Protti et al. [18] observed that both low and high strain rate groups showed lower stress relaxation (P1-P2 difference) when ventilated with 10 cmH₂O PEEP compared to 0 cmH₂O PEEP (ZEEP). This effect was independent of strain rate, suggesting that PEEP reduces viscous behaviour of lung parenchyma during ventilation.
The use of sufficiently elevated PEEP level (so-called optimal PEEP) is the most relevant measure amongst those constituting lung protection strategy. It has been proved to have a very important effect (NNT = 5 patients; 95% CI = 3 to 10) in reducing mortality in severe ARDS patients [41]. Maintaining permanent opening of the highest possible percentage of recruitable alveoli through high continuous distending pressure prevents VILI because it prevents atelectrauma caused by cyclic collapse of these alveoli during expiratory phase [42]. To correctly apply open-lung strategy [11,43,44,45], high PEEP use must be optimized according to each patient's lung mechanics. For this, it is necessary that all patients have their static compliance curve analysed in its inspiratory ramp (for example, through "super-syringe" technique), prescribing a PEEP level 2 cmH₂O above the lower inflection point (LIP) of this curve. This is the transpulmonary pressure point corresponding to that patient's "functional residual capacity (FRC)." With this PEEP level, the entire respiratory cycle is performed above FRC, just as it happens in healthy lungs, atelectrauma is avoided, and intrapulmonary shunt is minimized (therefore, FiO₂ requirements are reduced).
Data from open lung strategy clinical trials, makes it possible to infere that this LIP is situated in 95% of cases between 12.35 and 13.43 cmH₂O. Therefore, to be 97.5% certain that the patient receives optimal PEEP, approximately 15 cmH₂O PEEP should be prescribed. This achieves a partial arterial oxygen pressure/inspired oxygen fraction (P/F) ratio between 170 and 200, indicating that shunt will have been reduced to 30-40%. High PEEP levels may be necessary, even using Pplat values above 32 cmH₂O, provided the 15 cmH₂O limit in DP is not exceeded.
Clinically, performing static compliance curve is usually not feasible, and therefore "optimal" PEEP level must be determined indirectly. Kacmarek, Amato, and other investigators [46] have verified that determining PEEP level based on static compliance curve LIP and doing so by measuring shunt degree produces results without statistically significant differences.
Therefore, in the clinical setting, it seems reasonable to determine "optimal" PEEP level based on the P/F ratio value obtained with it [47]. A P/F ratio > 150-175 seems a reasonable objective. Clinical trials using higher PEEP levels (super PEEP trials) have only managed to demonstrate very marginal survival improvement [48,49,50], particularly in the most severe patients [51,52]. Any further PEEP increase will result in a merely "cosmetic" effect and subject the patient to unnecessary hemodynamic compromise. Recently, it has been demonstrated that daily lung mechanics trends can be assessed based on real-time responses of respiratory system compliance, end-expiratory lung volume, and stress and strain with respect to PEEP changes using a non-invasive nitrogen washout technique [31]. It has also been demonstrated that, although PEEP increase up to 10 cmH₂O increases tension and stress, their levels remain below known harmful values in pediatric ARDS [32].
In summary, the hypothesis is that PEEP effect on VILI incidence, from rheological perspective, relates to its capacity to:
Increase FRC: by increasing the denominator in the strain equation (VT/FRC), it reduces strain for the same VT.
Homogenize lung parenchyma: prevents "stress multiplier" formation by maintaining recruited unstable alveolar units.
However, it is important to highlight that PEEP does not always increase FRC in ARDS patients, and its effect on lung recruitment is difficult to predict at bedside.
Furthermore, for now, PEEP effect on VILI production has not yet been perfectly established experimentally within the new rheological theory framework.
4.3. Importance of Respiratory Rate
Respiratory rate (RR) plays a fundamental role in VILI development. Marini et al. [53] first described in 2000 that elevated RR worsened VILI in an animal model.
Karolinska Institute researchers [54] demonstrated, using a "double hit" model (alveolar lavage followed by aggressive ventilation), that animals ventilated with 40 bpm RR presented worse P/F ratio and higher biochemical and anatomopathological VILI markers compared to those ventilated at 20 bpm, despite using protective strategies (6 mL/kg VT, 10 cmH₂O PEEP).
This effect is explained by RR contribution to total mechanical power:
MP = RR × VT × Pressures
MP: mechanical power; RR: respiratory rate; VT: tidal volume
Elevated RR linearly increases MP delivered to the respiratory system, potentially exceeding the safety threshold even with protective tidal volumes.
4.4. Importance of Flow
Gattinoni's group [55] demonstrated that not only strain magnitude is important, but also the velocity at which it occurs (strain rate). In experiments with pigs ventilated with similar strain (2.1 ± 0.9) but different flow velocities:
The high strain rate group (I:E ratios of 1:5 to 1:9) presented:
Worse compliance and P/F.
Higher inflammatory markers and anatomopathological signs of pulmonary oedema.
Higher VILI prevalence (73% vs 20%, p = 0.01).
Higher mortality at 54 hours (47% vs 13%).
These findings suggest that high inspiratory flows increase VILI risk by increasing strain rate, even maintaining other ventilatory parameters constant.
Additionally, the group with greater VILI presented higher values in dynamic pulmonary hysteresis index (Joules) and stress relaxation index (P1-P2, cmH₂O), parameters that can be monitored in clinical practice.
To illustrate the gas delivery problem, an example can be posed comparing VC and PC (Figure 3) in which we can see that, despite strain being the same, strain rate will be 3 times higher in PC in the first time constant.
4.5. Importance of Ventilatory Mode
Ventilatory mode choice significantly influences VILI development, mainly through its effect on flow pattern.
In a series of experiments [56,57,58] comparing continuous mandatory pressure-controlled modes with adaptive control scheme (PC-CMVa) versus continuous mandatory volume-controlled modes with fixed control scheme (VC-CMVs), clear superiority of VC-CMV modes was observed in both oxygenation parameters and anatomopathological findings. That is, PC-CMVa modes produced more VILI.
This finding is surprising but may be related to the higher peak flow necessary in PC-CMVa to introduce the same volume (same strain) inducing higher strain rate and, as Gattinoni's team has demonstrated [55].
Schmidt et al. [59] have also demonstrated that ventilation with expiratory flow control attenuates lung injury in a porcine ARDS model. This finding suggests that not only inspiratory flow is important, but also deformation velocity during expiration (expiratory strain rate).
High-frequency oscillatory ventilation (HFOV) use could be a typical example of daily practice. According to volu/barotrauma theories, HFOV use should be safer and cause less damage than conventional MV, since administered VT is below dead space with moderate continuous distending pressure. Contrary to this theory, currently available literature has not demonstrated superiority and has even shown worse results when using HFOV versus conventional mechanical ventilation, a paradox that can be explained by energy transmission in HFOV. Since the modality uses simple harmonic motion to provide ventilation, energy transmitted by this wave can exceed the MP threshold for VILI formation.
4.6. Tidal Volume and Driving Pressure
In all mammalian species, [60] from bat to whale, physiological VT is 6.3 mL/kg. VT limitation to 6 mL/kg constitutes one of the fundamental aspects of lung protective ventilation strategy. Lung involvement in ARDS is very heterogeneous, with collapsed and non-recruitable zones coexisting with healthy or recruitable zones that remain open throughout the respiratory cycle. If very high VT are used, these ventilatable zones receive all inspired air (the volume that should come to them plus the remaining that should go to collapsed zones). VT limitation aims to avoid overdistention of these open zones and is a therapeutic measure that, although not proven to decrease barotrauma, has managed to moderately decrease ARDS patient mortality [10] (number needed to treat [NNT] = 12 patients; 95% CI: 8 to 36). But it is fundamental that this VT limitation be accompanied by adequate PEEP to maximize recruitment and decrease overdistention by distributing inspired air among the highest possible number of alveoli.
Since the beginnings of lung protective ventilation [61], in pressure control modes, VT limitation was established indirectly by limiting maximum Pplat (35 cmH₂O). This maximum Pplat correlates with PTP needed to insufflate lungs of a paralyzed and ventilated adult to obtain TLC [62]. However, experimental animal models have demonstrated that the main cause of overdistention is applied VT rather than maximum Pplat [9]. This implies that absence of VT limitation can cause VILI despite Pplat < 30 cmH₂O and, conversely, lower VT (6 mL/kg) using sufficient PEEP and recruitment maneuvers could make it possible for the patient to tolerate higher Pplat (40 cmH₂O) [49]. Although this topic is still controversial, in subsequent consensus guidelines for ARDS ventilatory management, for both adults and children, a maximum Pplat limit around 30 cmH₂O was established [63,64,65].
In relation to this, DP has been independently associated with mortality. Amato's study [66] reflects that Pplat increase is not always deleterious nor PEEP increase always protective, but rather the pressure difference between both that causes lung injury. A differential pressure below 15 cmH₂O has been established as a safety point [66].
On the other hand, it is not proven that using less than 6 mL/kg VT is positive for ARDS. In fact, since recruitment occurs through insufflation pressure (and is maintained by PEEP), using lower VT could be renouncing recruiting potentially recruitable zones and thereby worsening atelectrauma. In neonates with hyaline membrane disease, it has been seen that using 3 mL/kg VT versus 5 mL/kg produces greater pulmonary inflammation [67]. Consistent with this, Eichacker [68] published meta-analysis data indicating that VT < 5 mL/kg should not be used routinely since both high and low VT use can increase mortality. With Pplat of 28-32 cmH₂O being what most decreases mortality. This point has also been highlighted in the Cochrane meta-analysis published in 2013, which emphasizes that mortality does not increase until Pplat is greater than 32 cmH₂O [69].
Based on all the above and supported by Costa et al.'s 2021 meta-analysis [28], from a practical standpoint, initial VT should be 6 mL/kg ideal weight. If, having programmed adequate initial PEEP (15 cmH₂O), Pplat is equal to or greater than 32 cmH₂O, then VT should be decreased, with 4.5 mL/kg ideal weight recommended as lower limit.
Classically, in cases where VT is decreased below 6 mL/kg, minute volume loss was compensated with RR increase. However, it has been seen that resulting acidosis from permissive hypercapnia-based strategy is less injurious than VT increase necessary to correct it. And if accompanied by other lung protection measures (especially adequate PEEP level [70], it has demonstrated improving hemodynamics of adult patients ventilated for ARDS [71].
This supposed protective effect of permissive hypercapnia cannot be explained with classical VILI theories but may fit with the new vision provided by rheological theory. Considering that RR has a direct effect on MP increase, this can explain the beneficial effect of hypercapnia.
4.7. Resilience Implication in ARDS Ventilatory Strategy
Material resilience is deformation per unit volume (J/m³) produced within a material by deformation when stress is applied from a base state to the yield point. It constitutes the maximum capacity of a material to absorb energy when elastically deformed and then, upon unloading, completely recover this energy without losses. Since the first part of the stress-strain curve is linear, resilience is calculated as the geometric area of the triangle below the initial linear elastic region of that curve, up to the yield point (Figure 2). Therefore, it is half the product of stress and strain within that first segment [4,14,39].
When deformation energy remains within this elastic "comfort" zone, there is no energy loss. Then, there is no excess energy that leaks into the material producing microfractures and deformations, ending with material rupture (yield limit) (Figure 2) [25,26,72].
This threshold effect is a prediction of materials science. It requires staying in the deformation "comfort" zone to avoid creating microfractures. Therefore, to minimize VILI, it is important to adjust ventilator settings (in non-invasive and invasive ventilation) to maintain the energy level involved so that it is less than human lung resilience (J/m³), diseased or not. If deformation energy exceeds the safe zone, VILI appears [4].
4.8. Self-Inflicted Lung Injury (SILI)
Classically, preserving patient's spontaneous breaths was recommended; in fact, this is the basis for justifying Airway Pressure Release Ventilation (APRV) use. However, it has been demonstrated that muscle relaxant use in the most acute phase after intubation decreases mortality. [73] This data has been confirmed in a meta-analysis [74].
In recent years, the concept of self-inflicted lung injury (SILI) has been developed, extending the rheological model to patients with spontaneous breathing [30,75]. During respiratory effort, especially in ARDS, elevated negative pleural pressures are generated that can produce:
Increased regional strain. Especially in dependent zones, where negative pleural pressure can cause excessive local deformations.
Pendelluft. Air movement between lung regions with different time constants, increasing regional strain without changes in total VT.
Increased strain rate. Vigorous inspiratory efforts generate high flows that increase deformation velocity.
Increased mechanical power. The sum of patient's respiratory work and energy delivered by ventilator can exceed lung resilience threshold.
From rheological perspective, SILI can be prevented through:
Adequate sedation in initial phases of severe ARDS.
Ventilatory modes that limit inspiratory effort.
Trigger and cycling adjustment to avoid mismatches/asynchronies?.
Oesophageal pressure monitoring to estimate real stress.
Neuromuscular blockade consideration in selected cases.
5. Rheological Model Limitations
Some limitations of the new rheological theory are shown below:
5.1. Regional Lung Variability Not Captured by the Model
Current mathematical models of lung mechanics present important limitations for capturing regional lung heterogeneity, especially in pathological states like ARDS. This marked heterogeneity (areas of alveolar collapse, consolidation, and relatively preserved zones coexisting in the same lung) generates regional mechanical behaviours that cannot be adequately represented by global parameters. Current models, by assuming homogeneous properties, can lead to erroneous interpretations of global lung mechanics.
5.2. Interaction Between Mechanical Ventilation and Inflammation Not Completely Explained
Current models focus primarily on mechanical parameters, without adequately incorporating biological aspects of ventilator-lung interaction. Mechanical ventilation can induce or exacerbate pulmonary and systemic inflammatory response through mechanisms like biotrauma and mechanotransduction, processes that are not adequately integrated into conventional mechanical models.
Experimental studies by Chiumello et al. [76] have demonstrated that specific ventilation patterns can modulate gene expression and inflammatory mediator release, even in the absence of evident changes in mechanical parameters. This bidirectional interaction between mechanics and inflammation represents a significant challenge for current models.
5.3. Challenges for Determining the "Baby Lung" Precisely at Patient Bedside
The "baby lung" concept, introduced by Gattinoni, [33] has been essential to the understanding of ARDS pathophysiology and the adaptation of ventilatory strategies. However, precise quantification of functional lung tissue at bedside remains a significant challenge.
Currently, "baby lung" volume estimation requires advanced imaging techniques like quantitative computed tomography, which is not routinely available in intensive care units. Indirect methods, such as compliance-based or physiological dead space estimation, present important limitations and may not accurately reflect lung tissue truly available for ventilation.
In relation to these limitations, several solutions are proposed:
Implementation of multicompartmental models incorporating different time constants for different lung regions.
Integration of real-time functional imaging data to adjust regional model parameters.
Development of finite element-based computational simulations considering patient-specific geometry.
Development of integrated models incorporating real-time biological VILI parameters along with mechanical variables to adjust model parameters.
Creation of experimental models allowing characterization of the relationship between mechanical parameters and their specific biological response.
Validation of simplified methods to estimate "baby lung" based on lung mechanics parameters accessible at bedside.
6. Conclusions
In summary, the rheological described above explains how the lung, as a viscoelastic body, behaves more like a viscous liquid than an elastic solid when subject to rapid deformations, increasing energy dissipation as heat and structural damage.
Therefore, the rheological model provides a solid theoretical framework to understand VILI mechanisms in ARDS, integrating materials science and thermodynamics concepts. This approach explains why apparently safe ventilatory strategies can cause lung damage, and why interventions like limiting DP, reducing RR, or controlling flow are protective (Table 2).
Clinical application of these concepts suggests that:
1.DP should be maintained below 15 cmH₂O to avoid exceeding lung elastic limit.
2.Total MP should be limited to less than 12 J/min, adjusting tidal volume, respiratory rate, and flow.
3.PEEP should be optimized to homogenize parenchyma and prevent stress multiplier formation.
4.Inspiratory and expiratory flow control can reduce strain rate and minimize viscous component of lung damage.
5.In patients with spontaneous breathing, the additional effect of respiratory effort on total mechanical power should be considered, justifying muscle relaxant use in the most severe phases of disease.
Finally, this model offers a more solid scientific basis for developing personalized ventilatory strategies and could guide future research on ARDS prevention and treatment.
Author Contributions
All authors contributed equally to the conception and design of the study. All authors participated in the drafting and critical revision of the manuscript, and approved the final version for submission.
Funding
The authors declare that no funds, grants or other support were received during the preparation of this manuscript.
Acknowledgments
no acknowledgments is required.
Conflicts of Interest
No financial or non-financial benefits have been received.
References
- Lin, Y.H. Polymer viscoelasticity. Basics, molecular theories and simulations. 2nd ed Singapur: World Scientific Publishing Co; 2011.
- Mead, J.; Takishima, T.; Leith, D. Stress distribution in lungs: A model of pulmonary elasticity. J Appl Physiol. 1970, 28, 596–608. [Google Scholar] [CrossRef]
- Modesto, I.; Alapont, V.; Aguar Carrascosa, M.; Medina Villanueva, A. Stress, strain and mechanical power: Is material science the answer to prevent ventilator induced lung injury? Med Intensiva (Engl Ed). 2019, 43(3), 165-175.
- Modesto i Alapont, V.; Medina Villanueva, A.; Aguar Carrascosa, M.; et al. Stress, strain y potencia mecánica. La ciencia para prevenir la lesión inducida por el ventilador (VILI). Apéndice 1. Manual de Ventilación Mecánica Pediátrica y Neonatal. e-book. 6ª edición. Tesela Ediciones; 2022.
- Pilkey, W.D. Formulas for stress, strain and structural matrices. 2 nd ed John, Wiley & Sons, Inc; 2005.
- Cortés-Puentes, G.A.; Keenan, J.C.; Adams, A.B.; et al. Impact of chest wall modifications and lung injury on the correspondence between airway and transpulmonary driving pressure. Crit Care Med. 2015, 43, e287–95. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Carlesso, E.; Brioni, M.; et al. Airway driving pressure and lung stress in ARDS patients. Crit Care. 2016, 20, 276. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; et al. Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med. 2016, 42, 1567–75. [Google Scholar] [CrossRef]
- Dreyfuss, D.; Saumon, G. Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med. 1998, 157, 294–323. [Google Scholar] [CrossRef] [PubMed]
- Acute Respiratory Distress Syndrome Network; Brower, R. G.; Matthay, M.A.; Morris, A.; et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000, 342, 1301–8.
- Amato, MBP, Barbas, CSV, Medeiros, DM, et al. Beneficial effects of the “open lung approach“ with low distending pressures in acute respiratory distress syndrome: a prospective randomized study on mechanical ventilation. Am J Respir Crit Care Med 1995, 152, 1835–46.
- Slutsky, A.; Tremblay, L. Multiple system organ failure: is mechanical ventilation a contributing factor? Am J Respir Crit Care Med. 1998, 157, 1721–5. [Google Scholar] [CrossRef]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N Engl J Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- González López, A.; Garcia Prieto, E.; Batalla Solís, E.; et al. Lung strain and biological response in mechanically ventilated patients. Intensive Care Med. 2012, 38, 240–7. [Google Scholar] [CrossRef] [PubMed]
- Rahaman, U. Mathematics of ventilator-induced lung injury. Indian J Crit Care Med. 2017, 21, 521–4. [Google Scholar] [CrossRef]
- Laffey, J.F.; Bellani, G.; Pham, T.; et al. Potentially modificable factors contributing to outcome from acute respiratory distress syndrome: the LUNG SAFE study. Intensive Care Med. 2016, 42, 1865–76. [Google Scholar] [CrossRef]
- Amato, M.B.P.; Meade, M.O.; Slutsky, A.S.; et al. Driving pressure and survival in the Acute Respiratory Distress Syndrome. N Engl J Med. 2015, 372, 747–55. [Google Scholar] [CrossRef]
- Protti, A.; Votta, E.; Gattinoni, L. Which is the most important strain in the pathogenesis of ventilator-induced lung injury: dynamic or static? Curr Opin Crit Care. 2014, 20, 33–8. [Google Scholar] [CrossRef]
- Gattinoni, L.; Carlesso, E.; Cadringher, P.; et al. Lung stress and strain during mechanical ventilation for acute respiratory distress syndrome. Am J Respir Crit Care Med. 2008, 178, 346–55. [Google Scholar]
- Protti, A.; Cressoni, M.; Santini, A.; et al. Lung stress and strain during mechanical ventilation: Any safe threshold? Am J Respir Crit Care Med. 2011, 183, 1354–62. [Google Scholar] [CrossRef]
- Gattinoni, L.; Carlesso, E.; Cadringher, P.; et al. Lung stress and strain during mechanical ventilation for acute respiratory distress syndrome. Am J Respir Crit Care Med. 2008, 178, 346–55. [Google Scholar]
- Chiumello, D.; Chidini, G.; Calderini, E.; et al. Respiratory mechanics and lung stress/strain in children with acute respiratory distres syndrome. Ann Intensive Care. 2016, 6, 11. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Carlesso, E.; Brioni, M.; Cressoni, M. Airway driving pressure and lung stress in ARDS patients. Critical Care. 2016, 20, 276. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.; Roberts, F. Anaesthesia data. En: Allman, K.; editor. Oxford Handbook of anesthesia. 4 th ed. Oxford: Oxford University Press; 2016.
- Cressoni, M. ; Chiurazzi Ch, Gotti M et al. Lung inhomogeneities and time-course of ventilator-induced mechanical injuries. Anesthesiology. 2015, 123, 618–27. [Google Scholar] [PubMed]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; et al. Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med. 2016, 42, 1567–75. [Google Scholar] [CrossRef] [PubMed]
- Coppola, S.; Caccioppola, A.; Froio, S.; et al. Effect of mechanical power on intensive care mortality in ARDS patients. Crit Care. 2020, 24, 246. [Google Scholar] [CrossRef]
- Costa, E.L.V.; Slutsky, A.S.; Brochard, L.J.; et al. Ventilatory variables and mechanical power in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2021, 204, 303–11. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Takeuchi, M.; Inata, Y.; et al. Normalization to Predicted Body Weight May Underestimate Mechanical Energy in Pediatric Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2022, 205, 1360–3. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, T.; Vasques, F.; Rapetti, F.; et al. Driving pressure and mechanical power: new targets for VILI prevention. Ann Transl Med. 2017, 5, 286. [Google Scholar] [CrossRef] [PubMed]
- Ilia, S.; Geromarkaki, E.; Briassoulis, P.; et al. Effects of increasing PEEP on lung stress and strain in children with and without ARDS. Intensive Care Med. 2019, 45, 1315–7. [Google Scholar] [CrossRef]
- Ilia, S.; Geromarkaki, E.; Briassoulis, P.; et al. Longitudinal PEEP Responses Differ Between Children With ARDS and at Risk for ARDS. Respir Care. 2021, 66, 391–402. [Google Scholar] [CrossRef]
- Gattinoni, L.; Marini, J.J.; Pesenti, A.; et al. The "baby lung" became an adult. Intensive Care Med. 2016, 42, 663–75. [Google Scholar] [CrossRef] [PubMed]
- Serpa Neto, A.; Deliberato, R.O.; Johnson, A.E.W.; et al. Mechanical power of ventilation is associated with mortality in critically ill patients: an analysis of patients in two observational cohorts. Intensive Care Med. 2018, 44, 1914–22. [Google Scholar] [CrossRef]
- Becher, T.; van der Staay, M.; Schädler, D.; et al. Calculation of mechanical power for pressure-controlled ventilation. Intensive Care Med. 2019, 45(9), 1321–1323. [Google Scholar] [CrossRef]
- Chiumello, D.; Gotti, M.; Guanziroli, M.; et al. Bedside calculation of mechanical power during volume- and pressure-controlled mechanical ventilation. Crit Care. 2020, 24(1), 417. [Google Scholar] [CrossRef]
- Coppola, S.; Caccioppola, A.; Froio, S.; et al. Effect of mechanical power on intensive care mortality in ARDS patients. Crit Care. 2020, 24, 246. [Google Scholar] [CrossRef]
- Giosa, L.; Busana, M.; Pasticci, I.; et al. Mechanical power at a glance: a simple surrogate for volume-controlled ventilation. Intensive Care Med Exp. 2019, 7(1), 61. [Google Scholar] [CrossRef] [PubMed]
- Protti, A.; Andreis, D.T.; Monti, M.; Santini, A.; Sparacino, C.C.; Langer, T.; et al. Lung stress and strain during mechanical ventilation: Any difference between statics and dynamics? g Crit Care Med. 2013(41), 1046–1055. [CrossRef]
- Modesto, I.; Alapont, V.; Aguar Carrascosa, M.; Medina Villanueva, A. Clinical implications of the rheological theory in the prevention of ventilator-induced lung injury. Is mechanical power the solution? Med Intensiva. 2019, 43(6), 373–381. [Google Scholar]
- Gordo-Vidal, F.; Gómez-Tello, V.; Palencia-Herrejón, E.; et al. PEEP alta frente a PEEP convencional en el síndrome de distrés respiratorio agudo. Revisión sistemática y metaanálisis. Med Intensiva. 2007, 31, 491–501. [Google Scholar] [CrossRef]
- Farías, J.A.; Frutos, F.; Esteban, A.; et al. What is the daily practice of mechanical ventilation in pediatric intensive care units? A multicenter study. Intensive Care Med 2004, 30, 918–25. [Google Scholar] [CrossRef]
- Amato, M.; Valente Barbas, C.S.; Machado Medeiros, D.; et al. Effect of a Protective-Ventilation Strategy on Mortality in the Acute Respiratory Distress Syndrome. N Engl J Med 1998, 338, 347–54. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Suter, P.M.; Tortorella, C.; et al. Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1999 Jul 7;282, 54-61.
- Villar, J.; Kacmarek, R.M.; Pérez-Méndez, L.; et al. A high positive end- expiratory pressure, low tidal volume ventilatory syndrome: A randomized, controlled trial. Crit Care Med. 2006, 34, 1311–8. [Google Scholar] [CrossRef] [PubMed]
- Caramez, M.P.; Kacmarek, R.M.; Helmy, M.; et al. A comparison of methods to identify open-lung PEEP. Intensive Care Med. 2009, 35, 740–7. [Google Scholar] [CrossRef]
- Modesto i Alapont, V.; Medina Villanueva, A.; Del Villar Guerra, P.; et al. OLA strategy for ARDS: Its effect on mortality depends on achieved recruitment (PaO₂/FIO₂) and mechanical power. Systematic review and meta-analysis with meta-regression. Med Intensiva (Engl Ed). 2021, S0210-5691(21)00075-9.
- Brower, R.G.; Morris, A.; Maclntyre, N.; et al. Effects of recruitment maneuvers in patients with acute lung injury and acute respiratory distress syndrome ventilated with high positive end-expiratory pressure. Crit Care Med. 2003, 31, 2592–7. [Google Scholar]
- Meade, M.O.; Cook, D.J.; Guyatt, G.H.; et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008, 299, 637–45. [Google Scholar] [CrossRef]
- Mercat, A.; Richard, J.C.; Vielle, B.; et al. Expiratory Pressure (Express) Study Group. Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008, 299, 646–55. [Google Scholar]
- Briel, M.; Meade, M.; Mercat, A.; et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA. 2010, 303, 865–73. [Google Scholar] [CrossRef] [PubMed]
- Putensen, C.; Theuerkauf, N.; Zinserling, J.; et al. Meta-analysis: ventilation strategies and outcomes of the acute respiratory distress syndrome and acute lung injury. Ann Intern Med. 2009, 151, 566–76. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, J.R.; Blanch, L.; Murias, G.; Adams, A.B.; Olson, D.A.; Wangensteen, O.D.; et al. Effects of decreased respiratory frequency on ventilator-induced lung injury. Am J Resp Crit Care Med., 2000 (161), 463-468.
- Retamal, J.; Borges, J.B.; Bruhn, A.; et al. Open lung approach ventilation abolishes the negative effects of respiratory rate in experimental lung injury. Acta Anaesthesiol Scand. 2016, 60, 1131–41. [Google Scholar] [CrossRef]
- Protti, A.; Maraffi, T.; Milesi, M.; et al. Role of Strain rate in the pathogenesis of Ventilator-Induced Lung Edema. Crit Care Med. 2016, 44, e838–45. [Google Scholar] [CrossRef]
- Maeda, Y.; Fujino, Y.; Uchiyama, A.; Matsuura, N.; Mashimo, T.; Nishimura, M. Effects of peak inspiratory flow on development of ventilator-induced lung injury in rabbits. Anesthesiology. 2004(101), 722–728. [CrossRef]
- Fujita, Y.; Maeda, Y.; Fujino, Y.; Uchiyama, A.; Mashimo, T.; Nishimura, M. Effect of peak inspiratory flow on gas echange, pulmonary mechaniccs and lung histology in rabbits with injured lungs. J Anesth. 2006(20), 96–101.
- Fujita, Y.; Fujino, Y.; Uchiyama, A.; Mashimo, T.; Nishimura, M. High peak inspiratory flow can aggravate ventilator-induced lung injury. Med Sci Monit. 2007; (13):BR95-BR100. [Google Scholar]
- Schmidt, J.; Wenzel, C.; Spassov, S.; et al. Flow-controlled ventilation attenuates lung injury in a porcine model of acute respiratory distress syndrome: a preclinical randomized controlled study. Crit Care Med. 2020, 48, e241–8. [Google Scholar] [CrossRef]
- Villar, J.; Kacmarek, R.M.; Hedenstierna, G. From ventilator-induced lung injury to physician-induced lung injury: why the reluctance to use small tidal volumes? Acta Anaesthesiol Scand. 2004, 48, 267–71. [Google Scholar] [CrossRef]
- Slutsky, A.S. European Society of Intensive Care Medicine, the ACCP and the SCCM. Consensus conference on mechanical ventilation January 28-30, 1993 at Northbrook, Illinois, USA. Part, I.I. Intensive Care Med. 1994, 20, 150–62. [Google Scholar]
- Eisner, M.D.; Thompson, T.; Hudson, L.D.; et al. Efficacy of low tidal volume ventilation in patients with different clinical risk factors for acute lung injury and the acute respiratory distress syndrome. Am J Respir Crit Care Med. 2001, 164, 231–6. [Google Scholar] [CrossRef]
- Fan, E.; Del Sorbo, L.; Goligher, E.C.; et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017, 195, 1253–63. [Google Scholar] [CrossRef] [PubMed]
- Emeriaud, G.; López-Fernández, Y.M.; Iyer, N.P.; et al. Executive Summary of the Second International Guidelines for the Diagnosis and Management of Pediatric Acute Respiratory Distress Syndrome (PALICC-2). Pediatr Crit Care Med. 2023, 24, 143–68. [Google Scholar] [CrossRef]
- Kneyber, M.C.J.; de Luca, D.; Calderini, E.; et al. Recommendations for mechanical ventilation of critically ill children from the Paediatric Mechanical Ventilation Consensus Conference (PEMVECC). Intensive Care Med. 2017, 43, 1764–80. [Google Scholar] [CrossRef]
- Amato, M.B.P.; Meade, M.O.; Slutsky, A.S.; et al. Driving pressure and survival in the Acute Respiratory Distress Syndrome. N Engl J Med. 2015, 372, 747–55. [Google Scholar] [CrossRef]
- Lista, G.; Castoldi, F.; Fontana, P.; et al. Lung inflammation in preterm infants with respiratory distress syndrome: effects of ventilation with different tidal volumes. Pediatr Pulmonol. 2006, 41, 357–63. [Google Scholar] [CrossRef] [PubMed]
- Eichacker, P.Q.; Gerstenberger, E.P.; Banks, S.M.; et al. Meta-analysis of acute lung injury and acute respiratory distress syndrome trials testing low tidal volumes. Am J Respir Crit Care Med. 2002, 166, 1510–4. [Google Scholar] [CrossRef]
- Gillies, D.; Wells, D.; Bhandari, A.P. Positioning for acute respiratory distress in hospitalised infants and children. Cochrane Database of systematic reviews. 2012, 7, CD003645. [Google Scholar] [CrossRef] [PubMed]
- Rotta, A.T.; Gunnarsson, B.; Fuhrman, B.P.; et al. Comparison of lung protective ventilation strategies in a rabbit model of acute lung injury. Crit Care Med. 2001, 29, 2176–84. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.R.; Barbas, C.S.; Medeiros, DM; et al. Temporal hemodynamic effects of permissive hypercapnia associated with ideal PEEP in ARDS. Am J Respir Crit Care Med. 1997, 156, 1458–66. [Google Scholar] [CrossRef] [PubMed]
- Marini, J.J.; Rocco, P.R.M.; Gattinoni, L. Static and Dynamic Contributors to Ventilator-induced Lung Injury in Clinical Practice. Pressure, Energy, and Power. Am J Respir Crit Care Med. 2020, 201(7), 767-774.
- Papazian, L.; Forel, J.M.; Gacouin, A.; et al. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010, 363, 1107–16. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.T.N.; Patolia, S.; Guervilly, C. Neuromuscular blockade in acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials. J Intensive Care. 2020, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am J Respir Crit Care Med. 2017, 195(4), 438–442. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Pristine, G.; Slutsky, A.S. Mechanical ventilation affects local and systemic cytokines in an animal model of acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999, 160(1), 109–16. [Google Scholar] [CrossRef]
Figure 3.
Comparative example of gas delivery in pressure control (PC) and volume control (VC). Time constant (τ) is considered to be 0.2 seconds (5 time constants are completed in 1 second). Ideal weight is 30 kg and age 8 years. Estimated functional residual capacity is 1000 mL. Tidal volume (VT) to be delivered is 200 mL and plateau pressure (Pplat) or alveolar pressure (Palv) to be reached when gas delivery is completed is 20 cmH₂O. τ: time constant; Ti: inspiratory time; PG: generator pressure (working pressure); Paw: airway pressure; Palv: alveolar pressure; V: volume; SR: strain rate.
Figure 3.
Comparative example of gas delivery in pressure control (PC) and volume control (VC). Time constant (τ) is considered to be 0.2 seconds (5 time constants are completed in 1 second). Ideal weight is 30 kg and age 8 years. Estimated functional residual capacity is 1000 mL. Tidal volume (VT) to be delivered is 200 mL and plateau pressure (Pplat) or alveolar pressure (Palv) to be reached when gas delivery is completed is 20 cmH₂O. τ: time constant; Ti: inspiratory time; PG: generator pressure (working pressure); Paw: airway pressure; Palv: alveolar pressure; V: volume; SR: strain rate.
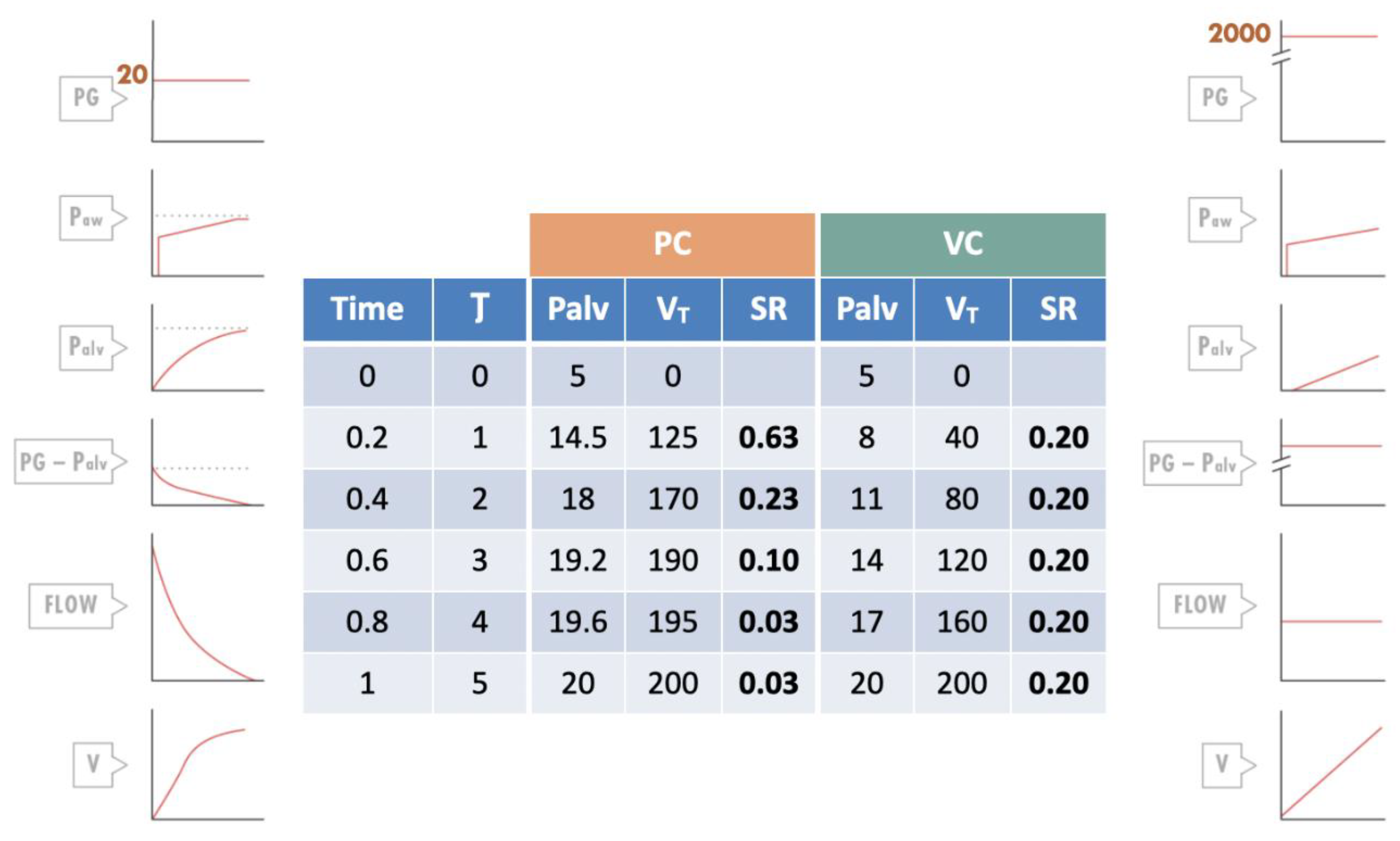
Table 2.
Ventilatory strategy based on rheological model to prevent ventilator-induced lung injury (VILI) in acute respiratory distress syndrome (ARDS).FRC: functional residual capacity; Pplat: plateau pressure; PEEP: positive end-espiratory pressure; J: Joules.
Table 2.
Ventilatory strategy based on rheological model to prevent ventilator-induced lung injury (VILI) in acute respiratory distress syndrome (ARDS).FRC: functional residual capacity; Pplat: plateau pressure; PEEP: positive end-espiratory pressure; J: Joules.
| Parameter | Recommendation | Rheological Justification |
|---|---|---|
| Driving pressure (DP) | < 15 cmH₂O | Maintains strain < 1 (elastic limit) |
| Tidal volume | Adjusted for DP < 15 cmH₂O Adjusted for Pplat = 28-32 cmH₂O |
Limits stress and strain |
| PEEP | PEEP titration to maximize homogeneity and recover pulmonary FRC | Reduces stress multipliers Reduces strain Reduces strain rate |
| Respiratory rate | Lowest possible allowing adequate ventilation | Limits mechanical power |
| Inspiratory flow | Moderate, avoiding high peaks | Reduces strain rate |
| Mechanical power | < 12 J/min | Below injury threshold |
| Inspiratory time | Prolonged (lower flow) | Reduces strain rate |
| Flow pattern | Constant and square | Optimizes stress distribution Decreases strain rate |
| Expiratory flow control | Consider if available | Reduces expiratory strain rate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



