
Submitted:
01 August 2025
Posted:
04 August 2025
You are already at the latest version
Abstract
New-onset postoperative atrial fibrillation (POAF) is common after cardiac and major noncardiac surgery, and significantly associated with short- and long-term adverse events. Multiple management strategies have been described but the lack of evidence from large randomized controlled trials and the lack of consensus regarding best practices has led to major variations in practice patterns. Considering on the one hand its serious adverse effects and complex drug interactions, and on the other hand discrepancies among recent international guidelines, the indications of amiodarone to both prevent and treat POAF should be reserved to patients at high risk of POAF only, or patients with hemodynamic instability and/or severely reduced left ventricular ejection fraction. Perioperative optimization of oral and intravenous cardio-selective beta-blockers to prevent POAF, and control heart rate when POAF occurs with a rapid ventricular response is the recommended first-line strategy, simultaneously with the treatment of associated factors. Given their efficient and safety profile, ultra-short-acting intravenous beta-blockers like esmolol or landiolol could be preferentially used in acute care patients. Besides, and waiting for the results of ongoing RCTs in cardiac and noncardiac surgery, the use of oral anticoagulation in patients with POAF should take into account the individualized thromboembolic/hemorrhagic risk ratio.
Keywords:
new-onset atrial fibrillation
; postoperative atrial fibrillation
; amiodarone
; beta-blockers
; landiolol
Introduction
Postoperative atrial fibrillation (POAF) is defined as new-onset atrial fibrillation that occurs within the first postoperative days following cardiac and noncardiac surgery. POAF is a common complication that occurs in 30%-50% of patients undergoing cardiac surgery [1,2,3], in 5%-30% of patients undergoing major noncardiac surgery, and in 5%-45% of critically ill patients [4]. The reported incidence of POAF has remained remarkably steady over recent decades. POAF is a serious complication that increases postoperative cardiac, cerebral, and renal morbidity, short- and long-term mortality, lengths of stay in intensive care unit (ICU) and in hospital, and healthcare cost [5,6,7,8,9]. Numerous risk factors of POAF have been well identified. They can be divided in non-modifiable risk factors related to atrial myopathy and patients characteristics and comorbidities (age, gender, obesity, alcohol, sleep apnea, hypertension, valvular disease, ventricular dysfunction) [10], and in transient modifiable stress factors accompanying acute illness (sympathetic activity, hypo/hypervolemia, hypo/hypertension, anemia, pain, electrolyte disturbances, metabolic alterations, hypo/hyperthermia, hypoxia, inflammation) [11,12,13]. From a clinical point of view, POAF is a paroxysmal phenomenon whose peak frequency occurs at postoperative day 2 (interquartile range: 1-3) [14]. More than 90% of patients with POAF return to normal sinus rhythm within the first seven postoperative days [5], even if a second acute episode is observed in 20 to 40% of cases [15]. When paroxysmal POAF lasts beyond postoperative day 7, it becomes persistent POAF. Noteworthy, POAF is associated with 4-5 times increase in recurrent atrial fibrillation during the next five years [16,17]. POAF is most often hemodynamically well tolerated and rarely responsible for acute circulatory failure or shock state. While multiple strategies to prevent POAF with pre-treatment or acute drug treatment have been described, there is a lack of evidence from large randomized controlled trials (RCTs). Besides, various treatment strategies have been described and diversely recommended in numerous international guidelines over the last twenty past years. The lack of consensus regarding best practices for the management of POAF has led to major variations in practice patterns [1,18,19,20,21].
Prevention of POAF
Amiodarone: A Dead Man Walking [22]
Amiodarone has been proving superiority on placebo in preventing POAF after cardiac surgery for a long time [23,24,25,26], and is currently recommended in several international guidelines, especially when beta-blockers are contra-indicated [27,28]. Noteworthy, the latest 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS), but without the European Society of Anaesthesiology and Intensive Care (ESAIC), still recommend using perioperative amiodarone therapy where drug therapy is desired to prevent POAF after cardiac surgery (Class I recommendation, Level of Evidence A) [29] on the basis of old studies [23,24,25,26]. This is however at the cost of potentially serious adverse hemodynamic effects following cardiopulmonary bypass, as high-grade atrioventricular blocks, refractory hypotension, or cardiogenic shock. In addition, there are as much as schemes of administration than existing published studies, so that it is currently impossible to provide a clear and consensual protocol that could be used on a routine basis. Especially, when to start amiodarone preoperatively, at which dose, and for how long are unresolved practical questions. Moreover, amiodarone and its metabolites accumulate in tissues at high concentrations, and are responsible for serious potential adverse non-hemodynamic effects including pulmonary, ophthalmic, hepatic, thyroid, and numerous drug interactions. In a retrospective study including 137 consecutive patients who underwent lung or heart-lung transplant, the prevalence of POAF within 26 days after surgery was high (45%) and the use of amiodarone was an independent predictor of short-term mortality in multivariate analysis (HR 2.97 [95% CI: 1.19-7.41], P=0.02) [30]. Even though the lungs account for less than 5% of all amiodarone-related complications, pulmonary involvement has the most clinically significant impact, and can contribute to patient mortality [31]. Thus, the individual benefit/risk ratio analysis of amiodarone therapy to prevent POAF pleads most often against rather than in favor of its preoperative systematic use, the risks outweighing the benefits (Figure 1) [22]. The joint recommendations for best practice around prevention and management of POAF in patients undergoing cardiac surgery from both Society of Cardiovascular Anesthesiologists (SCA) and European Association of Cardiothoracic Anaesthetists (EACTA) suggest using prophylactic amiodarone only in patients deemed at high risk of developing POAF (Class IIa recommendation, level of evidence A/B) [32]. Nonetheless, they are unable to recommend a specific dose or administration algorithm because referral and practice patterns markedly differ between institutions and countries.
Perioperative Optimization of Beta Blockers
Large cohort studies have previously shown that perioperative optimization of beta-blockers was strongly and independently associated with a reduction in POAF following cardiac and noncardiac surgery, especially in chronically treated patients [5]. Indeed, the withdrawal of treatment was responsible for a two-time increase in the incidence of POAF whereas continuing beta-blockers pre- and postoperatively was associated with a marked decrease in POAF (OR 0.49 [95% CI: 0.39-0.61], P<0.001) [5]. In a French multicentre prospective cohort study including 663 cardiac surgical patients, the odds of POAF were significantly reduced by restarting beta-blockers between 72 and 96h after surgery [33]. As well, a Cochrane systematic review of cardiac surgery RCTs reported that patients on beta-blocker therapy had a lower risk of POAF compared with control (RR 0.50 [95% CI: 0.42-0.59]) [34]. Focusing on landiolol, an ultra-short-acting intravenous highly cardio-selective beta-blocker, a systematic review of RCTs found a huge reduction in POAF following cardiac surgery in patients receiving a small dose of intravenous landiolol perioperatively when compared with control (13.7% versus 37.6%, P<0.001) [35]. Interestingly, the hemodynamic tolerance of landiolol was excellent, avoiding hypotension and its consequences [35]. Recently, a meta-analysis of RCTs confirmed the beneficial effect of landiolol for the prevention of POAF after cardiac surgery compared to patients allocated to control groups (RR 0.40 [95% CI: 0.30-0.54], P<0.001) [36]. Moreover, the use of landiolol was associated with a significant decrease in hospital length of stay. A similar beneficial effect of landiolol was also reported in a propensity score-matched analysis including 358 consecutive adult patients scheduled for aortic root, ascending aorta, and aortic arch surgery [37]. In this last study, the incidence of POAF was 18.9% versus 38.7% (P=0.002) in the landiolol group compared to control. All these studies provide a compelling evidence that perioperative optimization of beta-blockers, especially in chronically treated patients, is both efficient and safe in decreasing the incidence of POAF following cardiac and noncardiac surgery, and that perioperative administration of intravenous low-dose landiolol should be considered by physicians as a therapeutic option for POAF prevention after those surgeries.
Other Interventions
In the specific context of cardiac surgery, several RCTs and meta-analyses of RCTs have demonstrated the ability of posterior left pericardiotomy to prevent POAF [38,39]. The procedure is now recommended both in American and European guidelines (Class IIa recommendation, level of evidence B) [28,29]. Posterior left pericardiotomy is however not yet a routine practice worldwide.
Other medical interventions currently lack scientific evidence or showed conflicting results in the scientific literature, so that a wide use for medical practice cannot be recommended. Thus, the prophylactic benefit of magnesium sulfate (while commonly used by care providers), statins, sotalol, steroids, or botulium injection into the epicardial fat pad in cardiac surgery are controversial [40,41,42]. As well, the widespread practice that consists to maintain high-normal serum potassium concentration to avoid POAF after cardiac surgery can be abandoned [43]. Finally, the international multicentre RCT evaluating the effects of colchicine on POAF and myocardial injury in 3,209 patients undergoing noncardiac thoracic surgery (COP-AF trial) found no significant reduction in the incidence of clinically important POAF (6.4% versus 7.5%; HR 0.85 [95% CI: 0.65-1.10]; P=0.22), but an increased risk of mostly benign non-infectious diarrhea [44].
Treatment of POAF
Treatment of Associated Factors
The assessment and management of associated factors contributing to POAF and rapid ventricular response should reasonably be done as a prerequisite in the setting of cardiac and noncardiac surgery (Class IIa recommendation, level of evidence C) [45]. It includes treatment of hypovolemia or fluid overload, electrolytic disturbances as hypokalemia and hypomagnesemia, hypoxemia, anemia, pain, and management of sepsis or cardiogenic shock. Positive inotropic agents should be avoided when possible.
Considering a Rate Control Strategy
The largest multicentre RCT comparing rate control and rhythm control strategies to treat new-onset POAF after cardiac surgery found no significant difference in the total numbers of hospital days (median, 5.1 days and 5.0 days, respectively; P=0.76), complication rates, and rates of persistent atrial fibrillation 60 days after onset, and subsequently concluded that neither treatment strategy showed a net clinical advantage over the other [2]. Interestingly, about 25% of the patients in the rhythm-control group deviated from the assigned therapy because of amiodarone side effects or adverse drug reactions. Since surgical patients with POAF are most often in hemodynamically stable condition (hemodynamics is not compromised by the rhythm disorder), and given that i) spontaneous return to sinus rhythm is frequent, ii) amiodarone has serious and complex side effects, iii) postoperative sympathetic activation is constant, and iv) beta-blockers are efficient in heart-rate control, a rate control therapy using beta-blockers is recommended as initial strategy in the acute care setting (Class I recommendation, level of evidence B) [29]. Diltiazem or verapamil can also be used as first-choice drugs in patients with left ventricular ejection fraction > 40% to control heart rate and reduce symptoms (Class I recommendation, level of evidence B) [29]. They are preferred over digoxin because of their more rapid onset of action and dose-dependence effects [46,47,48]. More cardio-selective beta-blockers have a better efficacy and safety profile than unselective beta-blockers [49]. Intravenous esmolol and landiolol have the highest cardio-selectivity and shortest elimination half-life, suggesting they may be preferred in acute care patients who are hemodynamically unstable or with severely impaired left ventricular function (Table 1) (Class IIb recommendation, level of evidence B) [29]. In addition, landiolol could both increase and accelerate the rate of conversion of POAF when compared to control following cardiac surgery [35]. In a recent systematic review of new-onset atrial fibrillation in critical care, Levy et al. reported in 324 non-cardiac surgery patients from 17 studies that the use of landiolol was associated with a heart rate decrease of 18% to 51%, a mean conversion time of atrial fibrillation of 1.8h to 9.1h with 13% incidence of hypotension [4]. Combination of rate control therapy (cardio selective beta-blocker or diltiazem/verapamil plus digoxin) should be considered if a single drug does not control symptoms or heart rate. A lenient rate control with a resting heart rate of < 110 bpm should be considered as the initial target with stricter control reserved for patients with continuing atrial fibrillation-related symptoms (Grade IIa recommendation, level of evidence B) [29]. Combination of beta-blockers with diltiazem/verapamil should be avoided [50]. Amiodarone may be considered to achieve acute control of heart rate in selected patients who have hemodynamic instability and/or severely reduced left ventricular function or receiving positive inotropic agents (Class IIb recommendation, level of evidence B) [29], but due to its broad extracardiac adverse effects, the drug must be reserved as the last option when heart rate cannot be controlled even with maximal tolerated combination therapy.
Which Place for a Rhythm Control Strategy in the Acute Care Setting?
When POAF is responsible for hemodynamic instability (nearly 10% of patients), a rhythm-control strategy using rapid external synchronized electrical cardioversion is imperative to improve immediate patient outcomes [4] (Grade I recommendation, level of evidence C) [29]. As well, in patients with hemodynamically stable POAF persisting beyond day 7, a rhythm-control strategy is also recommended as second-line therapy (Grade IIa recommendation, level of evidence B) [29], and the decision-making process must be shared with cardiologists. Depending on the existence or not of underlying coronary, valvular, or heart diseases, the antiarrhythmic drug strategy can be amiodarone, dronedarone, flecainide, or propafenone. A synthesis algorithm regarding the treatment of POAF is depicted in Figure 2. Percutaneous catheter ablation procedures may be considered in patients with persistent POAF albeit it is not clear whether first-line ablation is superior to drug therapy.
Prevention of Thromboembolic Events
International guidelines have been recommending for a long time to initially manage asymptomatic POAF with rate control and anticoagulation. Recently, the 2024 AHA/ACC/ACS/ASNC/HRS/SCA/SCCT/SCMR/SMV guideline for perioperative cardiovascular management for noncardiac surgery suggested initiation of postoperative anticoagulation therapy can be beneficial in patients with POAF after considering the competing risks associated with thromboembolism and perioperative bleeding (Class IIa recommendation, level of evidence C) [45]. The last version of the CHA2DS2-VASC risk score can help to consider the patient’s individual thromboembolic stroke risk (Table 2) [29]. The evidence for prevention of POAF-induced ischemic stroke by oral anticoagulants is however limited [51,52], and the bleeding risk soon after cardiac and major noncardiac surgery is high [52]. Moreover, it is unclear whether stroke mechanisms are the same in patients with POAF compared to those with nonsurgical atrial fibrillation. A recent meta-analysis reported a significant decrease in thromboembolic events following cardiac surgery when oral anticoagulants were used, at the expense of higher rates of bleeding [53]. Waiting for the results of ongoing RCTs in cardiac and noncardiac surgery, long-term oral anticoagulation should be considered only in patients with POAF at elevated thromboembolic risk to prevent ischemic stroke and thromboembolism (Class IIa recommendation, level of evidence B) [29].
Future Directions
The potential great interest of landiolol as first-line therapy to both prevent and treat POAF after cardiac and noncardiac surgery is the matter of ongoing RCTs whose results should be soon available. The LANDIPROTECT trial is a multicentre, prospective, randomized, controlled, double blinded, phase III study assessing the protective impact of a 24-hour-low-dose of landiolol (2 µg/kg/min) administered postoperatively at the arrival in ICU versus placebo on the incidence of POAF within seven days following conventional cardiac surgery with cardiopulmonary bypass (NCT04607122). The LANDI-POAF trial is another ongoing multicentre, prospective, randomized, controlled, double blinded, phase III, two parallel-arm study assessing the protective impact of a 72-hour-low-dose of landiolol (2 µg/kg/min) administered postoperatively versus placebo on the incidence of both POAF and mortality within 72h following adult cardiac surgery (NCT05084118). The FAAC trial is a multicentre, prospective, randomized, controlled, single blinded, two parallel-arm study, which planned to include 350 patients with a first episode of POAF after cardiac surgery. The aim is to compare landiolol to amiodarone with the hypothesis of both a higher rate of reduction to sinus rhythm with landiolol during the 48h after POAF and less adverse effects within one year after surgery (NCT04223739) [54].
The hemodynamic tolerance of POAF is currently defined as the absence of significant hypotension, pulmonary edema, or myocardial ischemia. However, patients experiencing POAF after cardiac surgery without any decrease in mean arterial pressure were found with both a lower pulse pressure (suggesting a decrease in cardiac output) and alterations in microcirculatory parameters during POAF, all values returning to baseline once normal sinus rhythm was restored [55]. Interestingly, intravenous esmolol tended to normalize microcirculatory variables in a dose dependent manner, and independently of its macrocirculatory effects [55]. Thus, POAF deemed as hemodynamically stable based on arterial blood pressure and usual clinical signs could be responsible for early, occult and reversible abnormalities in microcirculation [56] that may be improved by short-acting cardio-selective beta-blockers. Further studies are however mandatory to figure out the consequences of POAF-induced microcirculatory abnormalities on patient outcome and the potential beneficial or deleterious specific pharmacological effects of rate and rhythm control medications, especially beta-blockers.
The direct interrogation of atrial function by means of preoperative echocardiography has emerged as a new and promising method to identify patients at high risk of POAF following both cardiac and noncardiac surgery [57,58].
Finally, the definite benefit/risk ratio and optimal long-term use of oral anticoagulation among patients with POAF should be better informed by the results of ongoing RCTs conducted in cardiac surgery (NCT04045665) and noncardiac surgery (NCT03968393).
Conclusions
POAF is common after cardiac and major noncardiac surgery, and significantly associated with short- and long-term adverse events, thereby justifying an efficient proactive strategy of both prevention and treatment. Despite its great popularity among careproviders worldwide, discrepancies regarding the indications of amiodarone exist in the most recent international guidelines. Considering its serious side effects and complex drug interactions, amiodarone should be reserved to patients at high risk of POAF or with hemodynamic instability or severely reduced left ventricular ejection fraction. Perioperative optimization of cardio-selective beta-blockers to prevent POAF and control heart rate when POAF occurs is the recommended first-line strategy, in association with the treatment of associated factors. Ultra-short-acting intravenous beta-blockers like esmolol or landiolol could be preferentially used in acute care patients. Besides, and waiting for the results of ongoing RCTs in cardiac and noncardiac surgery, the use of oral anticoagulation in patients with POAF should take into account the individualized thromboembolic/hemorrhagic risk ratio.
In paroxysmal POAF without hemodynamic instability, a lenient rate control strategy (heart rate < 110 bpm) using cardio-selective beta-blockers should be the first-line treatment. Amiodarone may be considered in selected patients who have severely reduced left ventricular function or receiving positive inotropic agents.
The decision-making process regarding rhythm control strategy for the treatment of paroxysmal and/or persistent POAF should be shared with cardiologists.
Author Contributions
J.-L.F. wrote the manuscript, which was reviewed by M.-O.F., M.R., and M.J.-L. All authors have read and agreed to the published version of the manuscript.
Funding
No external funding.
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
JLF received consulting fees and honoraria for lectures from AOP Health. MOF has no conflict of interest to declare. MR has no conflict of interest to declare. MJL has no conflict of interest to declare.
References
- Echahidi, N.; Pibarot, P.; O’Hara, G.; Mathieu, P. Mechanisms, prevention, and treatment of atrial fibrillation after cardiac surgery. J Am Coll Cardiol 2008, 51, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Gillinov, A.M.; Bagiella, E.; Moskowitz, A.J.; et al. Rate control versus rhythm control for atrial fibrillation after cardiac surgery. N Engl J Med 2016, 374, 1911–1921. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, M.; Di Franco, A.; Rong, L.Q.; Piccini, J.; Mack, M. Postoperative atrial fibrillation: from mechanisms to treatment. Eur Heart J 2023, 44, 1020–1039. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Slama, M.; Lakbar, I.; et al. Landiolol for treatment of new-onset atrial fibrillation in critical care: A systematic review. J Clin Med 2024, 13, 2951. [Google Scholar] [CrossRef]
- Mathew, J.P.; Fontes, M.L.; Tudor, IC; et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA 2004, 291, 1720–1729. [Google Scholar] [CrossRef]
- Villareal, R.P.; Hariharan, R.; Liu, B.C.; et al. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol 2004, 43, 742–748. [Google Scholar] [CrossRef]
- Dobrev, D.; Aguilar, M.; Heijman, J.; Guichard, J.B.; Nattel, S. Postoperative atrial fibrillation: mechanisms, manifestations and management. Nat Rev Cardiol 2019, 16, 417–436. [Google Scholar] [CrossRef]
- Conen, D.; Wang, M.K.; Devereaux, PJ; et al. New-onset perioperative atrial fibrillation after coronary artery bypass grafting and long-term risk of adverse events: an analysis from the coronary trial. J Am Heart Assoc 2021, 10, e020426. [Google Scholar] [CrossRef]
- Wang, M.K.; Meyre, P.B.; Heo, R.; et al. Short-term and long-term risk of stroke in patients with perioperative atrial fibrillation after cardiac surgery: systematic review and meta-analysis. CJC Open 2021, 4, 85–96. [Google Scholar] [CrossRef]
- Staerk, L.; Sherer, J.A.; Ko, D.; Benjamin, E.J.; Helm, R.H. Atrial fibrillation: Epidemiology, pathophysiology, and clinical outcomes. Circ Res 2017, 120, 1501–1517. [Google Scholar] [CrossRef]
- Ascione, R.; Caputo, M.; Calori, G.; Lloyd, C.T.; Underwood, M.J.; Angelini, G.D. Predictors of atrial fibrillation after conventional and beating heart coronary surgery: A prospective, randomized study. Circulation 2000, 102, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- Ishida, K.; Kimura, F.; Imamaki, M.; et al. Relation of inflammatory cytokines to atrial fibrillation after off-pump coronary artery bypass grafting. Eur J Cardiothorac Surg 2006, 29, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.K.; Laurikka, J.; Vikman, S.; Nieminen, R.; Moilanen, E.; Tarkka, M.R. Postoperative interleukin-8 levels related to atrial fibrillation in patients undergoing coronary artery bypass surgery. World J Surg 2008, 32, 2643–2649. [Google Scholar] [CrossRef] [PubMed]
- Piccini, J.P.; Zhao, Y.; Steinberg, B.A.; et al. Comparative effectiveness of pharmacotherapies for prevention of atrial fibrillation following coronary artery bypass surgery. Am J Cardiol 2013, 112, 954–960. [Google Scholar] [CrossRef]
- Maesen, B.; Nijs, J.; Maessen, J.; Allessie, M.; Schotten, U. Post-operative atrial fibrillation: a maze of mechanisms. Europace 2012, 14, 159–174. [Google Scholar] [CrossRef]
- Lee, S.H.; Kang, D.R.; Uhm, J.S.; Shim, J.; et al. New-onset atrial fibrillation predicts long-term newly developed atrial fibrillation after coronary artery bypass graft. Am Heart J 2014, 167, 593–600. [Google Scholar] [CrossRef]
- Konstantino, Y.; Zelnik Yovel, D.; Friger, M.D.; Sahar, G.; Knyazer, B.; Amit, G. Postoperative atrial fibrillation following artery bypass graft surgery predicts long-term atrial fibrillation and stroke. Isr Med Assoc J 2016, 18, 744–748. [Google Scholar]
- Mitchell, L.B.; Crystal, E.; Heilbron, B.; Page, P. Atrial fibrillation following cardiac surgery. Can J Cardiol 2005, 21 Suppl. B, 45B–50B. [Google Scholar] [PubMed]
- Fuster, V.; Ryden, L.E.; Cannom, D.S.; et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the European Society of Cardiology Committee for practice guidelines. Circulation 2006, 114, e257–e354. [Google Scholar]
- Nair, S.G. Atrial fibrillation after cardiac surgery. Ann Card Anesth 2010, 13, 196–205. [Google Scholar] [CrossRef]
- Fuster, V.; Ryden, L.E.; Cannom, D.S.; et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2011, 123, e269–e367. [Google Scholar]
- Providencia, R.; Kukendra-Rajah, K.; Barra, S. Amiodarone for atrial fibrillation: a dead man walking? Eur Heart J 2024, 45, 389–392. [Google Scholar] [CrossRef]
- Daoud, E.G.; Strickberger, S.A.; Man, K.C.; et al. Preoperative amiodarone as prophylaxis against atrial fibrillation after heart surgery. N Engl J Med 1997, 337, 1785–1791. [Google Scholar] [CrossRef]
- Yagdi, T.; Nalbantgil, S.; Ayik, F.; et al. Amiodarone reduces the incidence of atrial fibrillation after coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003, 125, 1420–1425. [Google Scholar] [CrossRef]
- Auer, J.; Weber, T.; Berent, R.; et al. A comparison between oral antiarrhythmic drugs in the prevention of atrial fibrillation after cardiac surgery: the pilot study of prevention of postoperative atrial fibrillation (SPPAF), a randomized, placebo-controlled trial. Am Heart J 2004, 147, 636–643. [Google Scholar] [CrossRef]
- Buckley, M.S.; Nolan, P.E.; Slack, M.K.; Tisdale, J.E.; Hilleman, D.E.; Copeland, J.G. Amiodarone prophylaxis for atrial fibrillation after cardiac surgery: meta-analysis of dose response and timing of initiation. Pharmacotherapy 2007, 27, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the diagnosis and management of atrial fibrillation: A report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation 2024, 149, e1–e156. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024, 45, 3314–3414. [Google Scholar] [CrossRef]
- Isiadinso, I.; Meshkov, A.B.; Gaughan, J.; et al. Atrial arrhythmias after lung and heart-lung transplant: Effects on short-term mortality and the influence of amiodarone. J Heart Lung Transplant 2011, 30, 37–44. [Google Scholar] [CrossRef]
- vanErven, L.; Schalij, M.J. Amiodarone: an effective antiarrhythmic drug with unusual side effects. Heart 2010, 96, 1593–1600. [Google Scholar] [CrossRef]
- Muehlschlegel, J.D.; Burrage, P.S.; Ngai, J.Y.; et al. Society of Cardiovascular Anesthesiologists/European Association of Cardiothoracic Anaesthetists practice advisory for the management of perioperative atrial fibrillation in patients undergoing cardiac surgery. Anesth Analg 2019, 128, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Couffignal, C.; Amour, J.; Ait-Hamou, N.; et al. Timing of beta-blocker reintroduction and the occurrence of postoperative atrial fibrillation after cardiac surgery: a prospective cohort study. Anesthesiology 2020, 132, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Blessberger, H.; Lewis, S.R.; Pritchard, M.W.; et al. Perioperative beta-blockers for preventing surgery-related mortality and morbidity in adults undergoing non-cardiac surgery. Cochrane Database Syst Rev 2019, 9, CD-13438. [Google Scholar] [CrossRef]
- Fellahi, J.L.; Heringlake, M.; Knotzer, J.; Fornier, W.; Cazenave, L.; Guarracino, F. Landiolol for managing atrial fibrillation in post-cardiac surgery. Eur Heart J Suppl 2018, 20, A4–A9. [Google Scholar] [CrossRef]
- Cafaro, T.; Allwood, M.; McIntyre, W.F.; et al. Landiolol for the prevention of postoperative atrial fibrillation after cardiac surgery: a systematic review and meta-analysis. Can J Anesth 2023, 70, 1828–1838. [Google Scholar] [CrossRef] [PubMed]
- Kaminohara, J.; Hara, M.; Uehara, K.; Suruga, M.; Yunoki, K.; Takatori, M. Intravenous landiolol for the prevention of atrial fibrillation after aortic root, ascending aorta, and aortic arch surgery: A propensity score-matched analysis. JTCVS Open 2022, 11, 49–58. [Google Scholar] [CrossRef]
- Gaudino, M.; Sanna, T.; Ballman, K.V.; et al. Posterior left pericardiotomy for the prevention of atrial fibrillation after cardiac surgery: an adaptive, single-centre, single-blind, randomized, controlled trial. Lancet 2021, 398, 2075–2083. [Google Scholar] [CrossRef]
- Abdelaziz, A.; Hafez, A.H.; Elaraby, A.; et al. Posterior pericardiotomy for the prevention of atrial fibrillation after cardiac surgery: a systematic review and meta-analysis. EuroIntervention 2023, 19, e305–e317. [Google Scholar] [CrossRef]
- O’Brien, B.; Burrage, P.S.; Ngai, J.Y.; et al. Society of Cardiovascular Anesthesiologists/European Association of Cardiothoracic Anaesthetists practice advisory for the management of perioperative atrial fibrillation in patients undergoing cardiac surgery. J Cardiothorac Vasc Anesth 2019, 33, 12–26. [Google Scholar] [CrossRef]
- Piccini, J.P.; Ahlsson, A.; Dorian, P.; et al. Design and rationale of a phase 2 study of NeurOtoxin (Botulinum toxin type A) for the prevention of postoperative atrial fibrillation – the NOVA study. Am Heart J 2022, 245, 51–59. [Google Scholar] [CrossRef]
- Curran, J.; Ross-White, A.; Sibley, S. Magnesium prophylaxis of new-onset atrial fibrillation: A systematic review and meta-analysis. Plos One 2023, 18, e029274. [Google Scholar] [CrossRef]
- O’Brien, B.; Campbell, N.G.; Allen, E.; et al. Potassium supplementation and prevention of atrial fibrillation after cardiac surgery. JAMA 2024, 332, 979–988. [Google Scholar] [CrossRef]
- Conen, D.; Wang, M.; Popova, E.; et al. Effect of colchicine on perioperative atrial fibrillation and myocardial injury after non-cardiac surgery in patients undergoing major thoracic surgery (COP-AF): an international randomized trial. Lancet 2023, 402, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.; Fleischmann, K.E.; Smilowitz, N.R.; et al. 2024 AHA/ACC/ACS/ASNC/HRS/SCA/SCCT/SCMR/SVM Guideline for perioperative cardiovascular management for noncardiac surgery. J Am Coll Cardiol 2024, 84, 1869–1969. [Google Scholar] [CrossRef] [PubMed]
- Tisdale, J.E.; Padhi, I.D.; Goldberg, A.D.; et al. A randomized, double-blind comparison of intravenous diltiazem and digoxin for atrial fibrillation after coronary artery bypass surgery. Am Heart J 1998, 135, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Siu, C.W.; Lau, C.P.; Lee, W.L.; Lam, K.F.; Tse, H.F. Intravenous diltiazem is superior to intravenous amiodarone or digoxin for achieving ventricular rate control in patients with acute uncomplicated atrial fibrillation. Crit Care Med 2009, 37, 2174–2179. [Google Scholar] [CrossRef]
- Scheuermeyer, F.X.; Grafstein, E.; Stenstrom, R.; et al. Safety and efficiency of calcium channel blockers versus beta-blockers for rate control in patients with atrial fibrillation and no acute underlying medical illness. Acad Emerg Med 2013, 20, 222–230. [Google Scholar] [CrossRef]
- Perrett, M.; Gohil, N.; Tica, O.; Bunting, K.V.; Kotecha, D. Efficacy and safety of intravenous beta-blockers in acute atrial fibrillation and flutter is dependent on beta-1 selectivity: a systematic review and meta-analysis of randomized trials. Clin Res Cardiol 2023, 113, 831–841. [Google Scholar] [CrossRef]
- Darby, A.E.; Dimarco, J.P. Management of atrial fibrillation in patients with structural heart disease. Circulation 2012, 125, 945–957. [Google Scholar] [CrossRef]
- Lin, M.H.; Kamel, H.; Singer, D.E.; Wu, Y.L.; Lee, M. Perioperative/postoperative atrial fibrillation and risk of subsequent strokeand/or mortality. Stroke 2019, 50, 1364–1371. [Google Scholar] [CrossRef]
- Taha, A.; Nielsen, S.J.; Bergfeldt, L.; et al. New-onset atrial fibrillation after coronary artery bypass grafting and long-term outcome: a population-based nationwide from the SWEDEHEART registry. J Am Heart Assoc 2021, 10, e017966. [Google Scholar] [CrossRef] [PubMed]
- Neves, I.A.; Magalhaes, A.; Lima da Silva, G.; et al. Anticoagulation therapy in patients with post-operative atrial fibrillation: systematic review with meta-analysis. Vascul Pharmacol 2022, 142, 106929. [Google Scholar] [CrossRef]
- Caspersen, E.; Guinot, P.G.; Rozec, B.; et al. Comparison of landiolol and amiodarone for the treatment of new-onset atrial fibrillation after cardiac surgery (FAAC) trial: study protocol for a randomized controlled trial. Trials 2023, 24, 353. [Google Scholar] [CrossRef]
- Fornier, W.; Jacquet-Lagreze, M.; Coolenot, T.; et al. Microvascular effects of intravenous esmolol in patients with normal cardiac function undergoing postoperative atrial fibrillation: a prospective pilot study in cardiothoracic surgery. Crit Care 2017, 21, 302. [Google Scholar] [CrossRef]
- Vacheron, C.H.; Allaouchiche, B. Illustration of the loss of haemodynamic coherence during atrial fibrillation using urethral photoplethysmography. BMJ Case Rep 2019, 12, e230757. [Google Scholar] [CrossRef]
- Pastore, M.C.; Degiovanni, A.; Grisafi, L.; et al. Left atrial strain to predict postoperative atrial fibrillation in patients undergoing coronary artery bypass grafting. Circulation: Cardiovascular Imaging 2024, 17, e015969. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, M.; Contreras, N.; Ramakrishna, S.; Zimmerman, J.M.; Varghese Jr, T.K.; Mitzman, B. Preoperative atrial deformation indices predict postoperative atrial fibrillation in patients undergoing lung resection surgery. Echocardiography 2025, 42, e70105. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Individual benefit/risk ratio of amiodarone to prevent and/or treat new-onset postoperative atrial fibrillation (POAF).
Figure 1.
Individual benefit/risk ratio of amiodarone to prevent and/or treat new-onset postoperative atrial fibrillation (POAF).
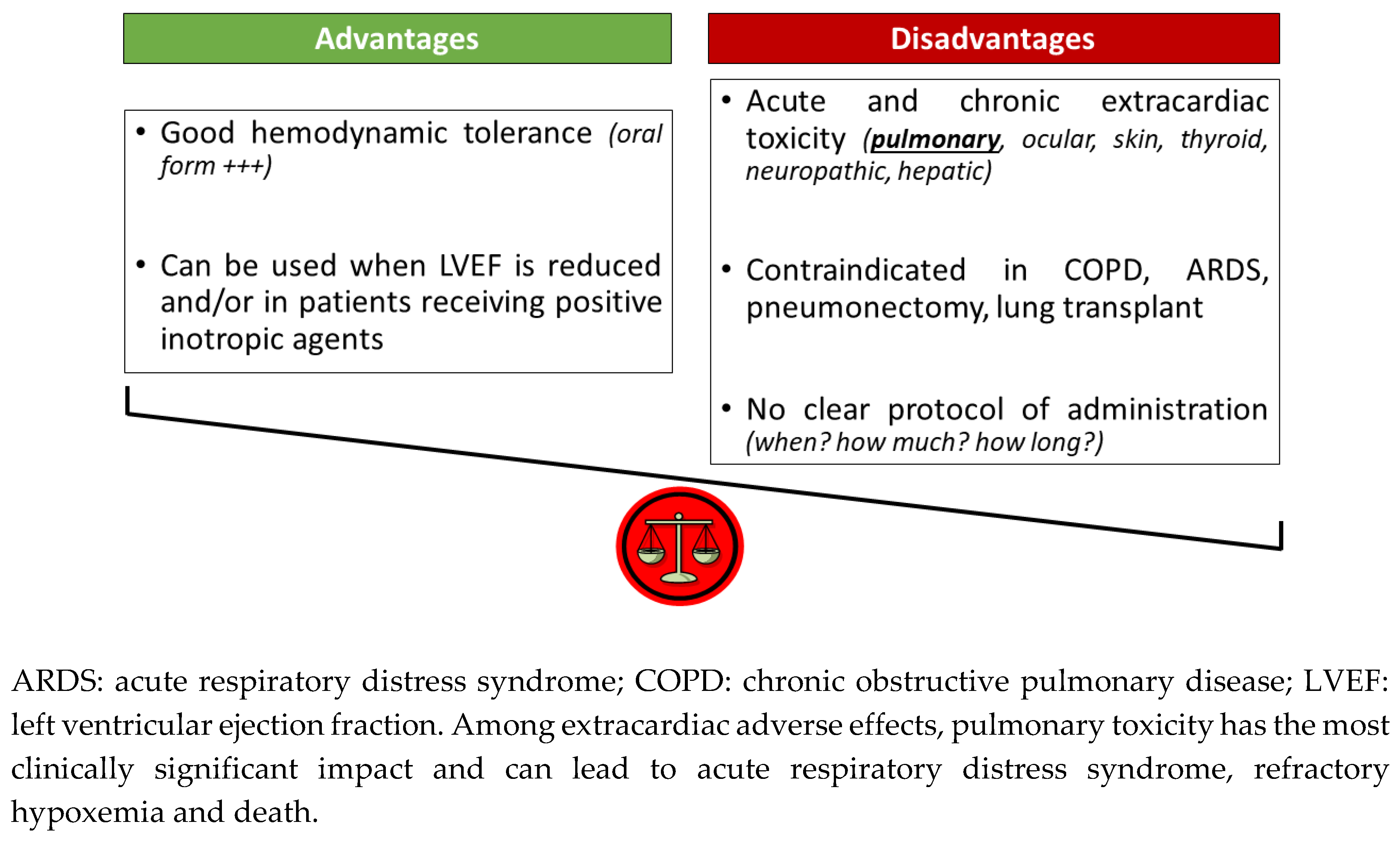
Figure 2.
Synthesis algorithm for the treatment of new-onset postoperative atrial fibrillation (POAF).
Figure 2.
Synthesis algorithm for the treatment of new-onset postoperative atrial fibrillation (POAF).
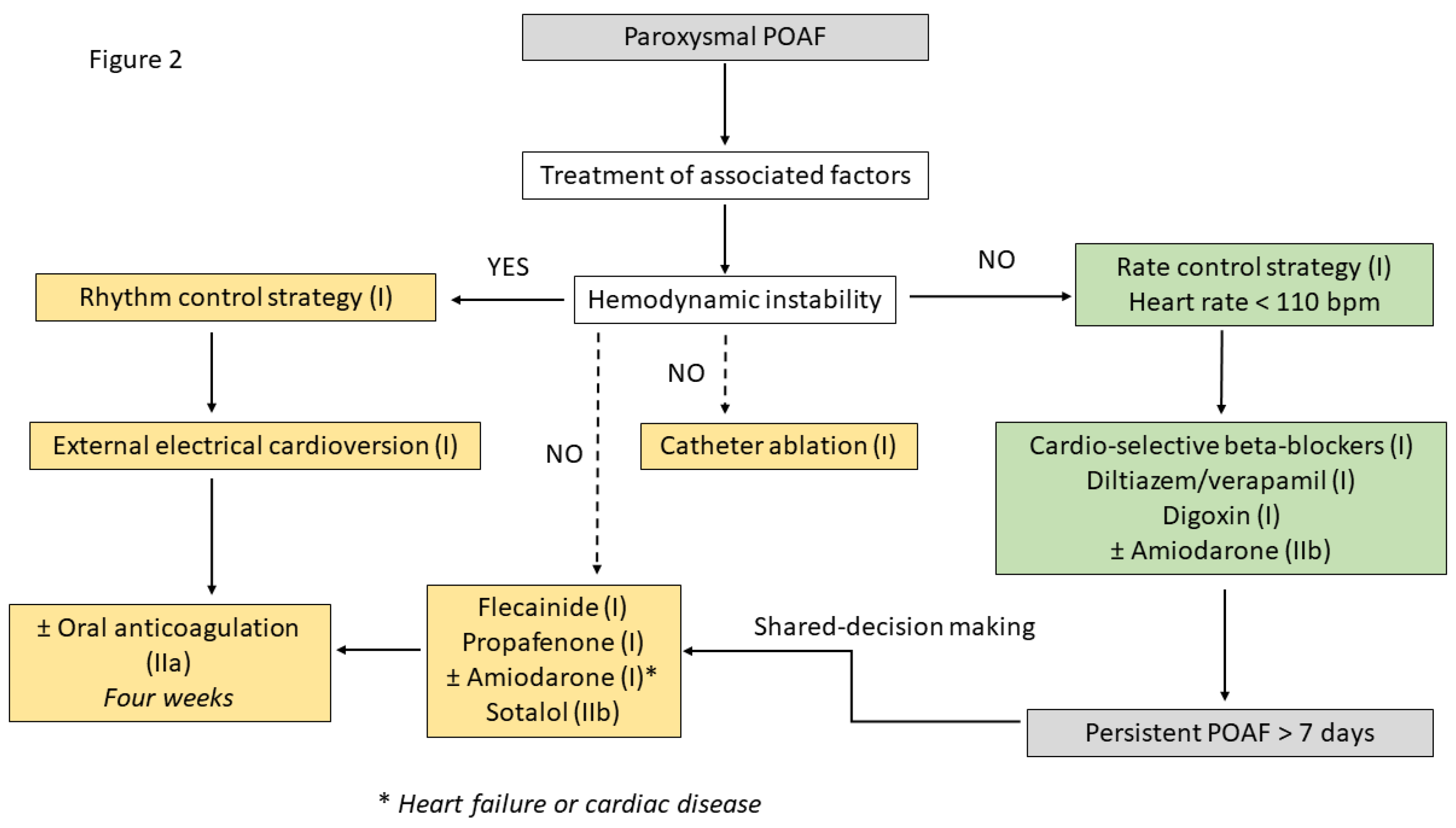

Table 1.
Pharmacological characteristics of intravenous beta-blockers used for acute rate control in new-onset postoperative atrial fibrillation (POAF).
Table 1.
Pharmacological characteristics of intravenous beta-blockers used for acute rate control in new-onset postoperative atrial fibrillation (POAF).
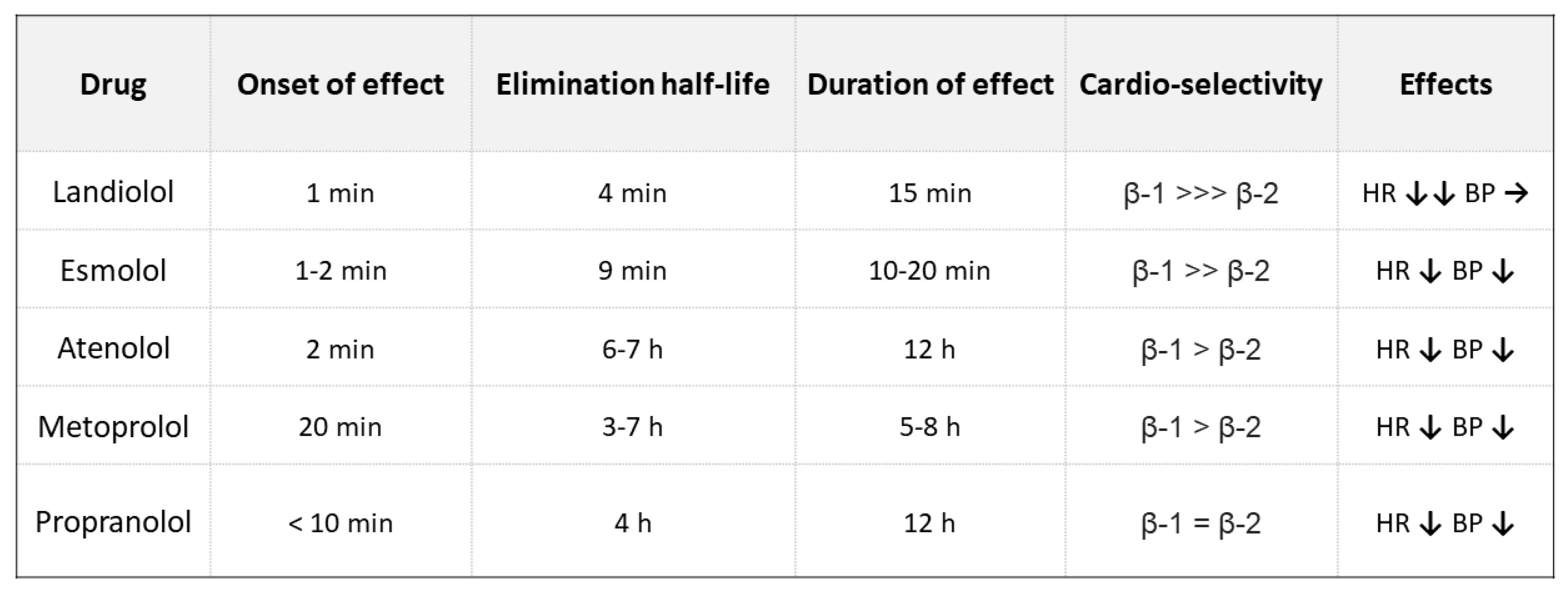 |
β-1/β-2: myocardial beta-agonist receptor; BP: blood pressure; HR: heart rate.
Table 2.
Update definitions for the CHA2DS2-VASC risk score. Adapted from [29].
Table 2.
Update definitions for the CHA2DS2-VASC risk score. Adapted from [29].
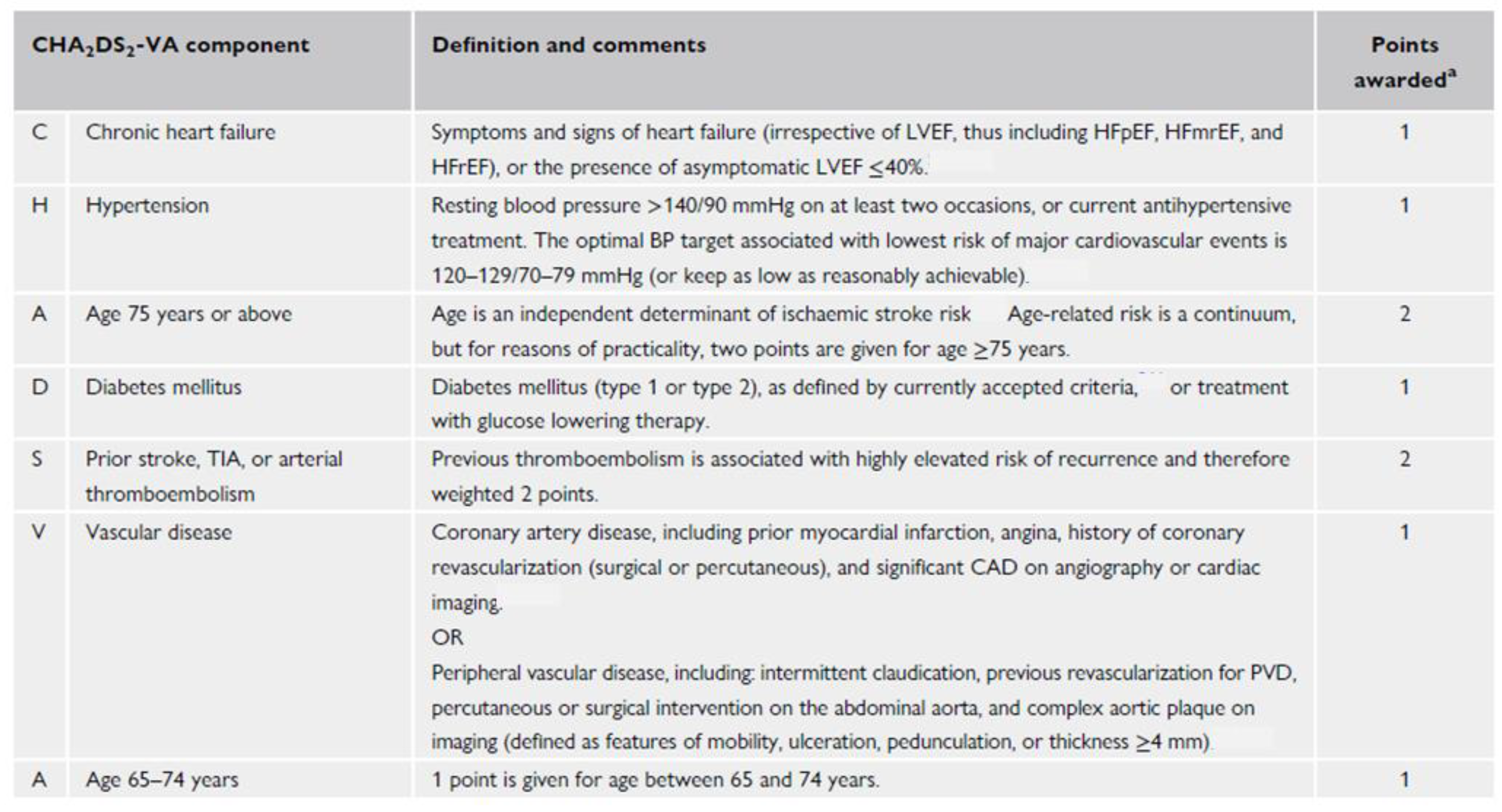 |
BP: blood pressure; CAD: coronary artery disease; HFmrEF: heart failure with mildly reduced ejection fraction; HFpEF: heart rate with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction; LVEF: left ventricular ejection fraction; PVD: peripheral vascular disease; TIA: transient ischemic attack. a In addition to these factors, other markers should be considered, including cancer, chronic kidney disease, ethnicity, cardiac biomarkers, atrial enlargement, hyperlipidemia, smoking, and obesity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



