
Submitted:
29 July 2025
Posted:
30 July 2025
You are already at the latest version
Abstract
Background and Objectives: The anesthetic nerve block test is a surgical technique that can assist in the differential diagnosis of forefoot pain, particularly in cases where clinical presentation is complex and diagnostic uncertainty is common. So, the aim of this study was to propose an alternative to the current procedure, which is known to produce a high rate of false positives in suspected cases of Morton’s neuroma. Material and methods: An experimental anatomical study was conducted on six fresh cadaveric feet. Under ultrasound guidance, the second, third, and fourth metatarsophalangeal joints were infiltrated with progressively increasing volumes of radiopaque contrast medium. Additionally, the third common digital nerve was injected in a healthy segment of the nerve within the third intermetatarsal space. Standard radiographs were then obtained to evaluate the distribution and proximal spread of the injected fluid. Results: A volume of 0.3 ml was sufficient to fully reach the intra-articular cavity and induce effective localized anesthesia. When the third common digital plantar nerve was injected in an anatomically healthy region, the contrast medium showed a proximal diffusion pattern extending up to the mid-diaphyseal level of the third and fourth metatarsal bones. Conclusions: Low intra-articular volumes of anesthetic may be sufficient to achieve a targeted clinical response, whereas injection into a Morton’s neuroma leads to a broader proximal spread, potentially anesthetizing adjacent anatomical structures and thus reducing diagnostic specificity. This refined technique may enhance the accuracy of therapeutic decision-making and reduce treatment failures in patients with suspected Morton’s neuroma.
Keywords:
Morton´s neuroma
; metatarsalgia
; ultrasound-guided injection
; differential diagnosis
; peripheral neuropathy
1. Introduction
Metatarsalgia is one of the most prevalent causes of forefoot pain, with an estimated incidence of approximately 10% in the general population, affecting females more frequently (1). It is a multifactorial clinical syndrome characterized by plantar pain in the region of the metatarsal heads, whose etiology may involve structural, mechanical, neurological, or inflammatory alterations. One of the conditions associated with metatarsalgia is Morton’s neuroma, defined as a compressive neuropathy of the common plantar digital nerve, with a higher prevalence in the third intermetatarsal space. Clinically, it presents as a burning pain radiating to the adjacent toes, often accompanied by paresthesias, electric shock-like sensations, and exacerbation when wearing tight footwear. Its pathogenesis involves perineural fibrosis, axonal degeneration, and degenerative vascular changes, potentially resulting from chronic repetitive trauma to the forefoot and biomechanical factors such as compression by the deep transverse intermetatarsal ligament (2–4). Nevertheless, the diagnosis of Morton’s neuroma should not be established without considering a broader spectrum of differential diagnoses, among which mechanical metatarsalgia stands out—typically secondary to overload of the metatarsal heads. This condition may arise from various factors, including first ray insufficiency, digital malalignment, hallux valgus, plantar fat pad atrophy, and inappropriate footwear. In this context, plantar plate injury or degeneration—a key stabilizing structure of the metatarsophalangeal (MTP) joint—is a frequent yet often underdiagnosed cause, requiring a markedly different clinical and therapeutic approach than neuroma (5,6). Other differential diagnoses to be considered include intermetatarsal bursitis (7), MTP joint synovitis, interosseous myofascial pain, stress fractures (8,9), distal peripheral neuropathies (such as tarsal tunnel syndrome), and inflammatory arthritides such as rheumatoid arthritis in patients with systemic disease (10), which typically affect the forefoot bilaterally and early in the disease course (11). The diagnostic complexity in distinguishing between these entities arises from overlapping symptoms, which can lead to diagnostic uncertainty and suboptimal therapeutic decision-making (2,4). The differential diagnosis is particularly challenging due to the convergence of symptoms originating from various anatomical structures—including MTP joints, plantar digital nerves, ligaments, tendons, and bursae—all of which may produce similar pain patterns. Correctly identifying the pain-generating structure is essential, as it directly influences the treatment strategy. For instance, metatarsalgia due to plantar plate rupture may benefit from reconstructive surgery or retrocapital offloading orthoses, whereas Morton’s neuroma typically responds better to anesthetic injections, radiofrequency ablation, or even neurectomy (2,12). This underscores the importance of an accurate functional diagnosis to complement imaging findings. From an anatomical standpoint, the studies by Sarrafian and Kelikian provide a foundational description of the neural and articular arrangement of the forefoot (13). The MTP joints are innervated by dorsal and plantar articular branches arising from the superficial and deep peroneal nerves, as well as the medial and lateral plantar nerves. These articular branches emerge proximal to the formation of the common plantar digital nerve, implying that an intra-articular anesthetic injection should not block a neuroma located distally in the intermetatarsal space. This functional separation is key to understanding the diagnostic utility of selective injections (13). Regarding available diagnostic tools, ultrasound and magnetic resonance imaging (MRI) are the most frequently employed imaging modalities (9), with fluoroscopy also demonstrating good results (14). Ultrasound demonstrates high sensitivity for detecting interdigital nerve thickening and associated bursitis, with the added advantage of enabling dynamic and bilateral comparative assessment. However, its specificity is limited by the presence of nonspecific findings in asymptomatic individuals and its operator dependency. MRI, on the other hand, offers superior visualization of the integrity of the plantar plate, bursae, synovitis, or stress fractures, although it has a high false-positive rate for neuromas, particularly in studies lacking clinical correlation (15). To overcome these limitations, several functional tests have been developed, such as ultrasound-guided diagnostic anesthetic blocks. These procedures involve the selective administration of local anesthetic into specific regions of the forefoot—such as the MTP joint or the neuroma site—followed by clinical evaluation of symptom relief. If intra-articular injection alleviates pain, an articular source is confirmed; if not, a neuropathic origin is more likely. The literature supports these tests as highly predictive diagnostic tools, validated in the knee, hip, lumbar spine, and more recently in the foot, as demonstrated by Ruiz Santiago et al (3) and El-Khoury et al (16).
Currently, the nerve suppression test is performed by injecting local anesthetic into the intermetatarsal space, directing the needle from dorsal to plantar, perpendicular to the course of the common digital plantar nerve. This technique aims to block Morton’s neuroma, so that if the patient experiences relief, the pain is considered to be of neuropathic origin (3,16,17). However, this approach may present a high rate of false positives, as observed in our experimental series. The contrast injection demonstrated a wide proximal spread of the anesthetic along the course of the lateral plantar nerve, reaching the plantar articular branches of the metatarsophalangeal joint capsule. This phenomenon implies that the clinical improvement after infiltration may not be due to the effect on the neuroma itself, but rather to the unintentional blockade of neighboring intra-articular structures.
As an alternative, we propose a technique based on ultrasound-guided diagnostic intra-articular infiltration of the metatarsophalangeal joint, a sealed cavity that allows the anesthetic effect to be confined exclusively to the articular compartment. If the patient does not experience improvement after this infiltration, it can be deduced that the pain does not originate from the joint and that the most likely cause is neuropathic. This sequential strategy—first infiltrating the joint and, only in the absence of response, performing the nerve suppression test—could improve diagnostic specificity and reduce the risk of misinterpretation. In addition, the use of ultrasound ensures anatomical precision and technical safety (3).
This type of strategy could evolved beyond diagnostic application, as it could also servee as a predictor of therapeutic response. For example, a patient experiencing significant pain relief after neuroma infiltration may be a good candidate for percutaneous radiofrequency ablation or selective neurotomy, whereas a positive response to joint blockade may indicate the need for focal orthopedic procedures. Thus, anatomical-clinical and radiological correlation—as proposed in this study through contrast-enhanced dispersion analysis—offers a more objective interpretation of the pain origin and facilitates more individualized treatment planning. Thus, ehe aim of this study was to propose an alternative to the current procedure, evaluating the rx results in cadaveric specimens.
2. Materials and Methods
An experimental and descriptive anatomical study was conducted, inspired by validated protocols described by Ruiz Santiago et al.(3), with the objective of documenting the radiological dispersion of iodinated contrast medium following ultrasound-guided injection into two key regions of the forefoot: the metatarsophalangeal (MTP) joint and the intermetatarsal (IM) space. This approach allows for anatomical validation of the clinical rationale behind the suppression test used to differentiate between Morton’s neuroma and other sources of metatarsalgia.
2.1. Anatomical Specimens and Inclusion Criteria
Six fresh human lower limbs were used, donated to institutional educational and research programs. All specimens were previously examined to confirm the anatomical integrity of the forefoot and to rule out signs of prior surgery, trauma, or deformities that could interfere with the technique.
2.2. Ultrasound-Guided Injection Technique
The procedure was performed using high-resolution ultrasound (10–15 MHz linear transducer) under real-time guidance (Figure 1), following the selective infiltration protocol described by Ruiz Santiago et al. for Morton’s neuroma (3). Three injections were performed on each anatomical specimen: 1- Metatarsophalangeal joint of the third ray (3rd MTP joint), 2- Metatarsophalangeal joint of the fourth ray (4th MTP joint) and 3- Intermetatarsal space between the third and fourth rays (IM space).
A 25G, 40 mm needle was used. A volume of 1 cc of iodinated contrast medium (iopamidol 300 mg/mL) was injected at each site. For the MTP joints, a dorsal longitudinal approach was employed, with the needle oriented parallel to the metatarsal shaft and advanced to the base of the proximal phalanx, avoiding the dorsal capsule and extensor tendons. For the IM space, a transverse dorsoplantar approach was used. The needle was positioned in the deep plane of the intermetatarsal space, just beneath the deep transverse intermetatarsal ligament and above the course of the common plantar digital nerve.
The selected volume of 1 cc was based on previous studies (16,17) and personal clinical experience, which indicate that this amount provides sufficient visualization without risk of extensive extravasation or pressure-related artifacts that could distort radiological interpretation.
2.3. Radiological Assessment
Digital radiographs were obtained in two projections (dorsoplantar and anteromedial oblique) after each injection. Images were acquired using a standardized exposure system (55 kV, 2.5 mAs). Two independent observers (second and fourth authors) with expertise in musculoskeletal imaging analyzed the images in a blinded fashion, evaluating the following parameters: a - Contrast dispersion: localized/intra-articular vs. diffuse/extra-articular, b- Margin definition: well-defined vs. irregular and c- Relationship with anatomical compartments as described by Sarrafian (13). Images were stored in DICOM format for subsequent review and were accompanied by static and video ultrasound recordings of each injection.
2.4. Quality Control and Reproducibility
To ensure replicability, the following quality control measures were implemented. All injections were performed by the same experienced operator. Each procedure was documented both sonographically and audiovisually. Two injections were randomly repeated to verify consistency of the dispersion pattern.
2.5. Ethical Considerations
All specimen donations complied with applicable legislation. This study was approved by the Research Ethics Committee of the University of Extremadura (ID 97//2022) and were carried out in accordance with institutional ethical protocols, aligned with the Declaration of Helsinki as adapted for cadaveric research.
3. Results
A total of 18 ultrasound-guided injections were performed across six fresh anatomical specimens: 6 into the third metatarsophalangeal (3rd MTP) joint, 6 into the fourth metatarsophalangeal (4th MTP) joint, and 6 into the third intermetatarsal (IM) space. All procedures were successfully executed under real-time ultrasound guidance and followed by standardized radiographic acquisition.
3.1. Injections into the Metatarsophalangeal Joints (3rd and 4th MTP)
In all intra-articular injections (n = 12), iodinated contrast dispersion remained confined within the articular capsule (Figure 2). Radiographic images revealed a contained, symmetrical pattern with sharply defined margins and an ovoid or triangular morphology, depending on the projection plane. The distribution of contrast was homogeneous in all joints, with no evidence of extravasation into the collateral ligaments, dorsal capsule, or pericapsular regions. These findings support the hypothesis that the MTP joint functions as a closed, sealed cavity, offering a significant anatomical advantage for performing selective and reproducible diagnostic blocks.
3.2. Injections into the Intermetatarsal Space (IM)
In all specimens, IM space infiltration resulted in diffuse, uncontained dispersion with irregular expansion and poorly defined borders (Figure 3). The contrast extended both proximally and laterally into adjacent soft tissue planes, following fascial paths with no clear anatomical containment. Additionally, a tendency for contrast migration toward the plantar region was observed, following the trajectory of the common plantar digital nerve. The mobility and superficial location of this nerve within the IM space appear to facilitate the lack of containment. This pattern confirms that the IM space functions as an anatomically open cavity with higher permeability to infiltrated fluid.
3.3. Functional Comparison of Dispersion Patterns
The results obtained in the experimental study revealed clear and consistent differences in the anesthetic dispersion patterns depending on the injection technique used. In the case of intra-articular infiltrations of the metatarsophalangeal (MTP) joint, the contrast dispersion was consistently focal, well-defined, and reproducible, which aligns with the closed and encapsulated anatomical nature of the joint. The articular capsule acts as a physical barrier that contains the injected volume in a controlled manner, allowing the anesthetic effect to remain confined exclusively within the joint cavity. This containment facilitates precise diagnostic interpretation, as any clinical improvement can be attributed with a high degree of certainty to the blockade of articular structures, without interference from nervous or bursae tissues. In contrast, infiltrations performed in the intermetatarsal space—following the conventional pathway of the nerve suppression test—showed broad, irregular, and variable contrast dispersion, both distally and proximally. This behavior corresponds to the lack of anatomical encapsulation in this region, where the anesthetic can freely spread through soft tissues including fat, fascia, bursae, nerves, and articular branches. Such unpredictable diffusion carries a high risk of unintentionally anesthetizing adjacent structures, particularly the plantar articular branches, which can lead to nonspecific or falsely positive clinical responses.
The functional comparison between both techniques suggests that the MTP joint, due to its enclosed anatomical nature, provides an optimal environment for controlled diagnostic infiltration. In contrast, the intermetatarsal space, being anatomically loose and lacking defined boundaries, does not allow the anesthetic effect to be reliably isolated, thus complicating the subsequent clinical interpretation. These observations support the notion that the MTP joint provides an ideal setting for anatomically selective suppression testing, whereas neuroma infiltration—although clinically useful—may result in less specific responses due to variable anesthetic dispersion and possible coexistence of adjacent bursitis or fibrosis.
4. Discussion
Diagnosing metatarsal pain remains one of the greatest challenges in foot and ankle clinical practice due to symptom overlap among entities such as Morton’s neuroma, mechanical metatarsalgia, intermetatarsal bursitis, and plantar plate rupture. The findings of this study—by anatomically evaluating contrast dispersion following targeted infiltrations—provide a functional basis to improve discrimination between these conditions and reduce therapeutic errors.
In this study there were no of communication observed between the metatarsophalangeal (MTP) joint capsule and the intermetatarsal bursa, reinforcing the concept of the MTP joint as a sealed anatomical cavity. Contrast dispersion along the neural pathway may lead to anesthesia of adjacent structures, including the plantar branches innervating the joint capsule. This could produce misleading diagnostic results if infiltration is not accurately performed at the articular level.
This new technique offers a reproducible and minimally invasive tool to optimize the differential diagnosis between metatarsalgia and Morton’s neuroma, thereby enhancing treatment selection and potentially reducing the incidence of failed interventions. Morton’s neuroma results from entrapment of the common plantar digital nerve, which courses between the third and fourth metatarsals and bifurcates to supply sensory innervation to the adjacent toes. According to Sarrafian, this nerve lacks connections to the MTP joint capsule, which is instead innervated by articular branches of the medial and lateral plantar nerves, as well as the superficial peroneal nerve (13). This separation supports the ability of MTP joint infiltrations to block articular pain without affecting the neuroma. Conversely, infiltration targeting the neuroma—due to broader fluid dispersion—may anesthetize plantar articular branches and yield symptomatic improvement, thereby masking the true pain origin.
Comparative ultrasound-guided injections into the MTP joint and the intermetatarsal space provide a functional approach to identify the true source of pain. In our study, contained contrast dispersion in the MTP joint confirms its nature as a sealed cavity—ideal for precise diagnostic blockade. In contrast, the diffuse contrast pattern in the IM space reflects an open anatomy, making selective blockade of the interdigital nerve more difficult. This may explain the therapeutic failures seen with techniques such as radiofrequency ablation or neurectomy.
One of the most frequent errors is assuming that the presence of a neuroma on MRI or ultrasound always explains the patient’s pain. This structural misattribution—without functional confirmation—may result in unnecessary surgeries or ineffective treatments. Ruiz Santiago and Lucas et al. have shown that diagnostic infiltrations can alter surgical indications in up to 30% of cases (3,16). Similarly, procedures targeting the plantar plate or metatarsal overload will fail if the pain originates from an untreated interdigital neuropathy. This underscores the need for a stepwise diagnostic strategy that integrates structural imaging, clinical examination, and functional tests such as those proposed here.
As evidence continues to grow around complex metatarsal pain syndromes, it becomes increasingly imperative to adopt a structured diagnostic approach that combines targeted history-taking, expert physical examination, high-resolution imaging, and—crucially—functional testing with anatomical support, as described in this study. This integrated methodology not only enhances diagnostic precision but also reduces unnecessary interventions and improves functional outcomes and patient satisfaction.
5. Conclusions
The MTP joint behaves as a closed cavity with predictable contrast dispersion, allowing for effective diagnostic blockade. This contrasts with the open anatomy of the intermetatarsal (IM) space, where contrast spreads more diffusely and erratically, hindering accurate diagnosis of Morton’s neuroma. A correct new ultrasound-guided diagnostic injections can significantly reduce the rate of failed morton’s neuroma diagnosis. A positive response to intra-articular injection—i.e., pain relief following MTP blockade—suggests an intra-articular source or involvement of the plantar plate. In contrast, an ambiguous or limited response to neuroma injection
Author Contributions
Conceptualization, G. C-N. and A. M-N., methodology, A. F-G, H. P-S. and S. M.; resources, F. G., M. F-P, L. P-P.; writing—original draft preparation, G. C-N.; writing—review and editing, G. C-N, A. F-G, A. M-N.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of the University of Extremadura (Protocols code 97//2022, date of approval April, 16th of 2022).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Palka O, Guillin R, Lecigne R, Combes D. Radiological approach to metatarsalgia in current practice: an educational review. Insights Imaging. 2025;16(1):94.
- Kasparek M, Schneider W. Surgical treatment of Morton’s neuroma: Clinical results after open excision. Int Orthop. 2013;37(9):1857–61.
- Ruiz Santiago F, Moraleda Cabrera B, Láinez Ramos-Bossini AJ. Ultrasound guided injections in ankle and foot. J Ultrasound. 2024;27(1):153–9.
- Valisena S, Petri GJ, Ferrero A. Treatment of Morton’s neuroma: A systematic review. Foot Ankle Surg. 2018;24(4):271–81.
- Maceira E, Monteagudo M. Mechanical Basis of Metatarsalgia. Foot Ankle Clin. 2019;24(4):571–84.
- Nery C, Coughlin MJ, Baumfeld D, Mann TS. Lesser metatarsophalangeal joint instability: prospective evaluation and repair of plantar plate and capsular insufficiency. Foot Ankle Int. 2012;33(4):301–11.
- Larsen SB, Søgaard SB, Nielsen MB, Torp-Pedersen ST. Diagnostic Considerations of Intermetatarsal Bursitis: A Systematic Review. Diagnostics. 2023;13(2):211.
- Goud A, Khurana B, Chiodo C, Weissman BN. Women’s musculoskeletal foot conditions exacerbated by shoe wear: an imaging perspective. Am J Orthop. 2011;40(4):183–91.
- Reijnierse M, Griffith JF. High-resolution ultrasound and MRI in the evaluation of the forefoot and midfoot. J Ultrason. 2023;23(95):e251–71.
- Bowen CJ, Culliford D, Dewbury K, Sampson M, Burridge J, Hooper L, et al. The clinical importance of ultrasound detectable forefoot bursae in rheumatoid arthritis. Rheumatology. 2010;49(1):191–2.
- Albtoush OM, Xenitidis T, Horger M. Intermetatarsal bursitis as first disease manifestation in different rheumatological disorders and related MR-imaging findings. Rheumatol Int. 2019;39(12):2129–36.
- Llombart-Blanco R, Mariscal G, Benlloch M, Barrios C, Llombart-Ais R. Systematic Review and Meta-analysis of Radiofrequency Ablation for Morton’s Neuroma: Outcomes and Predictors of Success. Am J Phys Med Rehabil. 2025;104(5):465–72.
- Sarrafian S, Kelikian A. Sarrafian’s Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2011. 373–384 p.
- Lucas PE, Hurwitz SR, Kaplan PA, Dussault RG, Maurer EJ. Fluoroscopically guided injections into the foot and ankle: localization of the source of pain as a guide to treatment--prospective study. Radiology. 1997;204(2):411–5.
- Ganguly A, Warner J, Aniq H. Central Metatarsalgia and Walking on Pebbles: Beyond Morton Neuroma. AJR Am J Roentgenol. 2018;210(4):821–33.
- Khoury NJ, El-Khoury GY, Saltzman CL, Brandser EA. Intraarticular foot and ankle injections to identify source of pain before arthrodesis. AJR Am J Roentgenol.1996;167(3):669–73.
- de Cesar Netto C, da Fonseca LF, Simeone Nascimento F, O’Daley AE, Tan EW, Dein EJ, et al. Diagnostic and therapeutic injections of the foot and ankle-An overview. Foot Ankle Surg. 2018;24(2):99–106.
Figure 1.
Longitudinal (long-axis) ultrasound image of the ultrasound-guided injection into the second metatarsophalangeal joint.
Figure 1.
Longitudinal (long-axis) ultrasound image of the ultrasound-guided injection into the second metatarsophalangeal joint.
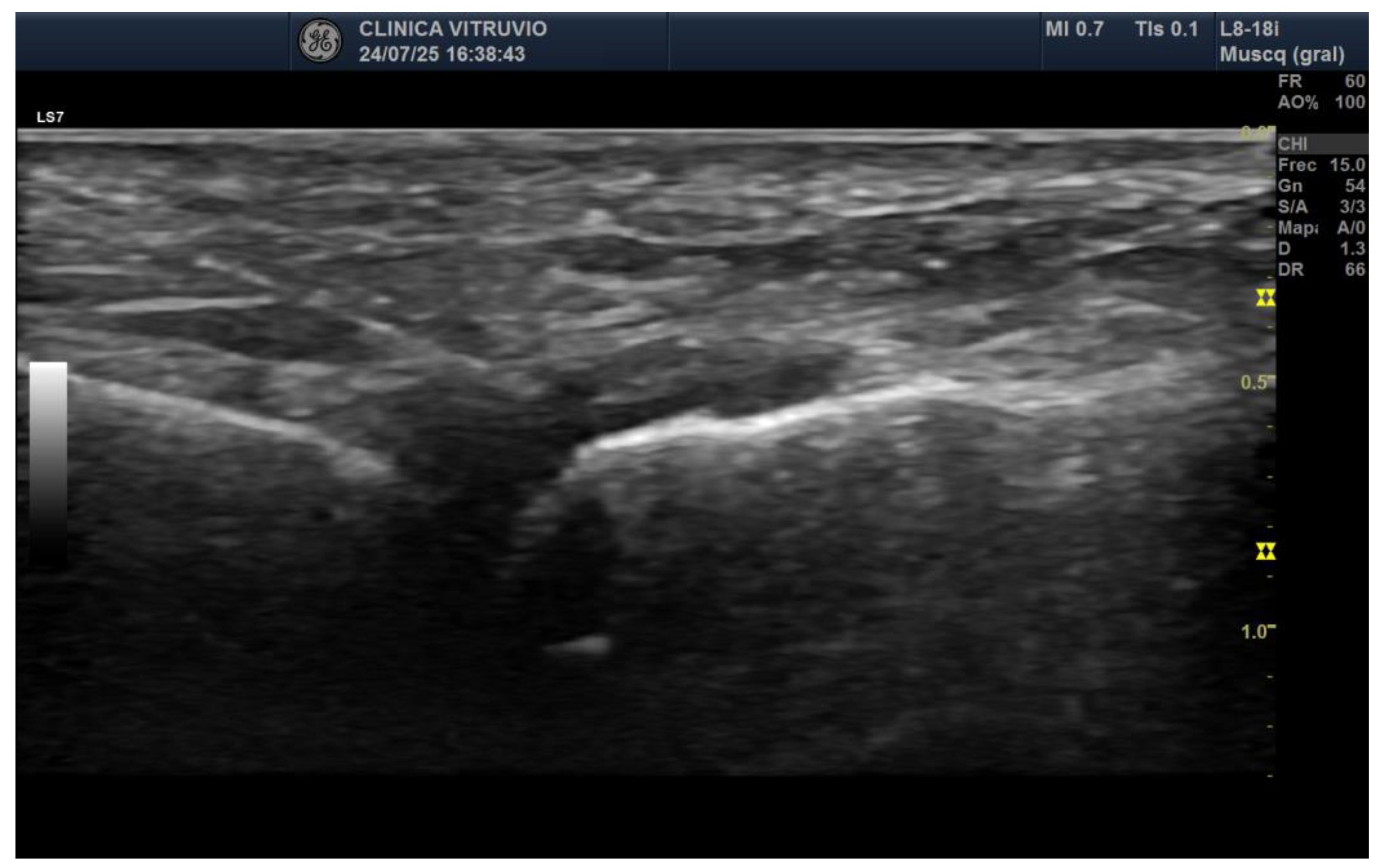
Figure 2.
Dorsoplantar radiograph of the right forefoot following intra-articular injection of radiopaque contrast. A volume of 0.5 cc was injected into the second metatarsophalangeal joint, 0.4 cc into the third, and 0.3 cc into the fourth. Complete filling of the joint cavities is observed without contrast extravasation, confirming the sealed capsular nature of each articulation.
Figure 2.
Dorsoplantar radiograph of the right forefoot following intra-articular injection of radiopaque contrast. A volume of 0.5 cc was injected into the second metatarsophalangeal joint, 0.4 cc into the third, and 0.3 cc into the fourth. Complete filling of the joint cavities is observed without contrast extravasation, confirming the sealed capsular nature of each articulation.

Figure 3.
Ultrasound-guided injection of 0.5 cc of radiopaque contrast targeting the third common plantar digital nerve. The injection was performed in long axis, with a distal-to-proximal trajectory parallel to the nerve. A) Dorsoplantar projection of the right forefoot. B) Oblique projection of the same injection, allowing better visualization of the contrast tracking along the interdigital space.
Figure 3.
Ultrasound-guided injection of 0.5 cc of radiopaque contrast targeting the third common plantar digital nerve. The injection was performed in long axis, with a distal-to-proximal trajectory parallel to the nerve. A) Dorsoplantar projection of the right forefoot. B) Oblique projection of the same injection, allowing better visualization of the contrast tracking along the interdigital space.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



