Submitted:
25 July 2025
Posted:
28 July 2025
You are already at the latest version
Abstract
Background: Reduced-dose prasugrel is widely used in East Asia for acute coronary syndrome (ACS), but real-world data in diverse Asian populations are limited. This study evaluated its effectiveness and safety in Taiwanese patients.
Methods: The PROMISE-TW Registry was a multicenter, retrospective study including 1,167 patients with ACS or chronic coronary syndrome (CCS) treated with reduced-dose prasugrel (20 mg loading, 3.75 mg maintenance) across 13 hospitals in Taiwan from 2018 to 2022. The primary endpoint was 1-year major adverse cardiovascular events (MACE: cardiovascular death, non-fatal myocardial infarction, non-fatal stroke). Secondary outcomes included composite ischemic events and major bleeding (BARC 3–5).
Results: Among enrolled patients (mean age 63.9 years, 81.2% male, 83% ACS), percutaneous coronary intervention was performed in 90.8%. At one year, MACE occurred in 1.9%, composite ischemic events in 8.2%, and major bleeding in 0.8%. Subgroup analysis identified prior stroke, diabetes, and chronic total occlusion intervention as predictors of bleeding. Male sex, chronic kidney disease, and left circumflex artery intervention predicted higher ischemic risk.
Conclusions: Reduced-dose prasugrel provided effective ischemic protection and low bleeding rates in Taiwanese patients, especially those with ACS. These findings support the clinical utility of dose-adjusted prasugrel in East Asian populations and highlight the importance of individualized risk assessment.
Keywords:
prasugrel
; acute coronary syndrome
; chronic coronary syndrome
; antiplatelet therapy
; PROMISE-TW Registry
; Taiwan
1. Introduction
Dual antiplatelet therapy (DAPT), comprising aspirin and a P2Y12 inhibitor, is the cornerstone of secondary prevention in patients with acute coronary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) [1,2,3]. Prasugrel and ticagrelor have demonstrated superior efficacy over clopidogrel in preventing thrombotic complications, but their higher bleeding risk necessitates careful patient selection [4,5]. Recognizing these concerns in East Asian populations, who have a higher propensity for bleeding events., Taiwan has adopted a reduced-dose prasugrel regimen (20 mg loading, 3.75 mg maintenance), similar to that used in Japan [6]. However, data about the real-world effectiveness and safety of this regimen show conflicting results and remain underexplored [7,8,9,10]. While global trials such as TRITON-TIMI 38 have established full-dose prasugrel’s efficacy, the applicability of reduced-dose prasugrel to Taiwanese patients remains uncertain. Given the variations in genetic polymorphisms affecting drug metabolism and the unique bleeding profile in East Asian populations, the Prasugrel Reduced-dose Observation for Measuring Improvement in Safety and Effectiveness in Taiwan (PROMISE-TW) Registry was designed to evaluate the clinical outcomes of reduced-dose prasugrel in Taiwanese patients, providing essential data to inform treatment decisions and guideline development. By investigating a real-world cohort in Taiwan, this study seeks to bridge this knowledge gap and offer insights that may refine antithrombotic strategies in the region.
2. Methods
2.1. Study Design and Population
PROMISE-TW is a multicenter, retrospective cohort study conducted across 13 hospitals in Taiwan. Eligible patients were ≥18 years old, diagnosed with ACS or chronic coronary syndrome (CCS), and received reduced-dose prasugrel between January 2018 and November 2022 [11]. Patients were included regardless of PCI status or concomitant oral anticoagulant (OAC) use. Those with incomplete clinical data were excluded. The definition of complex PCI includes any one of the following criteria: left main (LM) lesion, bifurcation lesion, stent length >30 mm, chronic total occlusion (CTO) lesion, implantation of ≥3 stents, or SYNTAX score ≥33. The definition of a fragile patient group includes those who meet all three of the following criteria: age >75 years, body weight <50 kg, and impaired renal function with an estimated glomerular filtration rate (eGFR) <50 mL/min/1.73 m².
2.2. Clinical Outcomes
The primary outcome was the incidence of major adverse cardiovascular events (MACE), including cardiovascular death, non-fatal myocardial infarction (MI), and non-fatal stroke within one year after receiving prasugrel. Secondary outcomes included 1-year composite ischemic events (MACE plus unplanned revascularization), all-cause mortality, stent thrombosis, unplanned revascularization, major bleeding defined as Bleeding Academic Research Consortium (BARC) type 3 to 5 bleeding, and combined major and minor bleeding events. Cardiovascular death was defined as death due to cardiac causes, including MI, heart failure (HF), or fatal arrhythmias. Unplanned revascularization was defined as any repeat revascularization procedure, including PCI or coronary artery bypass grafting (CABG), which was not scheduled as part of the initial treatment plan.
2.3. Data Collection
Data were retrospectively recorded using a standardized online case report form. Local study coordinators at each site will gather additional information by completing an electronic data capture form based on patient medical records. Clinical data will be extracted from both hospital and outpatient records, including demographic information, comorbidities, lifestyle factors, medications, echocardiographic findings, angiographic data, and clinical outcomes [11]. A detailed list of study variables is provided in Supplementary Table 1. This study was approved by the institutional review boards of all participating hospitals. As this was a retrospective analysis using de-identified clinical data, the requirement for written informed consent was waived by each institutional review board.
2.4. Calculation of Sample Size
This study is a retrospective analysis, and all patients meeting the specified inclusion criteria are eligible for enrollment. According to the Japanese PRASFIT-PRACTICE II study, the one-year incidence of MACE following reduced-dose prasugrel treatment was 1.7% [8]. Additionally, the Taiwan Acute Coronary Syndrome Full Spectrum Registry (2008–2010) reported a one-year MACE rate of 12.7% in patients with ACS [12]. Given advancements in clinical techniques and pharmacological therapies for ACS in recent years, we estimate that the one-year MACE incidence for the same patient population enrolled in Taiwan between 2018 and 2022 may be approximately 3.5%. For a non-inferiority study design with a type I error of 0.025 and 80% power, a minimum of 969 ACS patients undergoing interventional treatment is required. However, considering the real-world use of reduced-dose prasugrel in CCS populations within Taiwan’s clinical setting, we plan to increase the total sample size to 1,100 patients.
2.5. Statistical Analysis
Continuous data were expressed as the mean ± standard deviation (SD), while categorical data were expressed as numbers with percentages. Categorical data were compared by using the Chi-square test or Fisher's Exact test in two independent groups. Logistic regression analysis was used to determine the variables affecting prognosis. Upon completion of the univariable analyses, we select variables for the multivariable analysis. Any variable whose univariable test has a p-value < 0.25 is a candidate for the multivariable model along with all variables of know clinical importance. Once the variables have been identified, we begin with a model containing all of then selected variables. A 2-tailed P value < 0.05 was considered statistically significant. All analyses were performed using the SAS 9.4 statistical package (SAS Institute Inc., Cary, NC, USA).
3. Results
This study enrolled 1,167 patients with a mean age of 63.9 ± 11.9 years, and 13.9% were age older than 75. The majority of participants (81.2%) were male. Most patients (83%) presented with ACS, categorized as ST-segment Elevation Myocardial Infarction (STEMI, 28.8%), Non–ST-segment Elevation Myocardial Infarction (NSTEMI, 26.9%), and unstable angina (23.0%), while the remaining 17% had CCS. DAPT including aspirin, was prescribed to only 81.5% of patients during hospitalization. Regarding P2Y12 inhibitor therapy, approximately half (49.9%) received prasugrel as the initial medication; however, 26.2% switched from clopidogrel and 23.9% from ticagrelor. The primary reasons for switching were dyspnea (50.9%), bleeding events (21.1%), thrombotic events (13.4%), and allergies (14.6%) (Figure 1). The overall duration of reduced-dose prasugrel therapy was 443.14 ± 329.02 days on average, with a median of 368 days (interquartile range: 271–525 days).
PCI was performed in 90.8% of patients, with coronary stenting conducted in 80.6%, including drug-eluting stents in 69.7% and bare-metal stents in 13.4%. Complex PCI procedures were performed in 70.2% of cases, including PCI to the left main artery (8.3%), true bifurcation lesions (34.2%), CTO lesions (16.0%), use of stent lengths ≥30 mm (48.5%), implantation of three or more stents (10.5%), and SYNTAX scores ≥33 (6.3%).
In addition, 12.7% of patients required mechanical circulatory support, and atherectomy for severely calcified plaques was performed in 9.0% of cases. Radial artery access was used in 72.4% of interventions, while femoral access was employed in 22.3%. The target coronary vessels included the left main artery (8.3%), left anterior descending artery (LAD, 56.0%), left circumflex artery (LCX, 28.7%), and right coronary artery (RCA, 32.0%).Three-vessel coronary artery disease (CAD) was identified in 27.9% of patients.
The most common comorbidities were hypertension (HTN, 60.8%), diabetes mellitus (DM, 38.2%), hyperlipidemia (27.4%), chronic kidney disease (CKD, eGFR <60, 19.0%), and a history of stroke (4.2%). Only 0.7% of the study population were classified as clinically fragile. (Table 1)
At the one-year follow-up, the overall incidence of MACE was 1.9%, with cardiovascular death occurring in 0.3%, non-fatal MI in 1.5%, and non-fatal stroke in 0.1%. When including unplanned revascularization, the composite ischemic event rate increased to 8.2%. Stent thrombosis was observed in 1.5% of patients, while all-cause mortality reached 1.3%. In terms of bleeding outcomes, major bleeding was recorded in 0.8%, whereas the overall rate of major plus minor bleeding was 1.7%. (Figure 2) Subgroup analysis (Figure 3, Figure 4, Figure 5 and Figure 6) identified significant predictors associated with various clinical outcomes. HTN (p=0.013), total stent length ≥30 mm (p=0.0454), and LCX as the target vessel (p=0.0068) were significantly associated with MACE. Composite ischemic outcomes (MACE plus unplanned revascularization) were significantly correlated with CKD (p=0.0086), total stent length ≥30 mm (p=0.0317), use of drug-eluting stents (DES) (p=0.0161), fragile patient group (p=0.0086), LM lesions (p=0.0034), and LCX lesions (p=0.0114). Additionally, major bleeding was significantly associated with DM (p=0.0315) and a history of stroke (p=0.0042), while combined major and minor bleeding was significantly linked to CCS versus ACS diagnosis (p=0.0109), stroke history (p=0.0001), and CTO lesions (p=0.0092). Other results from the subgroup analysis are presented in Supplementary Table S2.
Univariate and multivariate logistic regression analyses were performed to further identify independent predictors for each clinical outcome. Results from the univariate analysis are presented in Supplementary Table S3. In the multivariate model, HTN demonstrated a trend toward being an independent predictor of MACE, although it did not reach statistical significance (OR 2.45, 95% CI 0.81–7.44). Independent predictors of composite ischemic outcomes included male sex (OR 2.02, 95% CI 1.05–3.90), CKD (OR 2.17, 95% CI 1.40–3.37), and involvement of the LCX as the target vessel (OR 1.72, 95% CI 1.12–2.65). For major plus minor bleeding events, stroke history (OR 8.95, 95% CI 2.67–29.99) and the presence of CTO lesions (OR 4.12, 95% CI 1.45–11.68) were identified as independent predictors. Regarding major bleeding alone, independent predictors included a diagnosis of CCS versus ACS (OR 3.92, 95% CI 1.01–15.22), DM (OR 4.95, 95% CI 1.00–24.39), and stroke history (OR 10.53, 95% CI 2.45–45.22). (Figure 7)
4. Discussion
In this real-world, multicenter registry study conducted across Taiwan, we evaluated the clinical effectiveness and safety of reduced-dose prasugrel (loading dose 20 mg, maintenance dose 3.75 mg) in patients with both ACS and CCS. The PROMISE-TW Registry enrolled 1,167 patients, the majority with ACS and undergoing PCI. At one-year follow-up, the incidence of MACE was low (1.9%), and the rate of composite ischemic events was 8.2%. Major bleeding events occurred in only 0.8%, and overall bleeding (major + minor) was 1.7%, suggesting an acceptable ischemic–bleeding balance. These results support the feasibility of using reduced-dose prasugrel in daily practice for the Taiwanese population, particularly in the ACS setting.
The 1-year MACE rate observed in our cohort (1.9%) was notably lower than that reported in the PRASFIT-ACS randomized trial (9.4%) despite both studies using an identical reduced-dose prasugrel regimen [6]. Furthermore, compared with the JAMIR-KAMIR registry analysis, which reported a 1-year MACE rate of 4.7% in East Asian AMI patients treated with adjusted-dose prasugrel, our findings suggest even more favorable outcomes in the Taiwanese population [13]. Notably, JAMIR-KAMIR also showed a major bleeding rate of 0.43% in the reduced-dose group, compared to 1.71% in the standard-dose group, supporting the safety advantage of prasugrel dose adjustment in East Asian patients. The relatively low bleeding incidence in PROMISE-TW (0.8% major bleeding; 1.7% major + minor) supports the hypothesis of the "East Asian paradox," wherein East Asian patients exhibit lower thrombotic but higher bleeding tendencies [14]. This pharmacodynamic profile, along with CYP2C19 polymorphisms prevalent in East Asians, necessitates region-specific strategies. The clinical adoption of low-dose prasugrel in Taiwan mirrors Japan’s approach and reflects growing consensus on tailored antiplatelet therapy for this population.
In Taiwan, several observational studies have also demonstrated consistent results with our findings. A recent single-center registry from Chang et al. reported a 1-year MACE rate (defined as cardiac mortality, non-fatal MI, the need for target lesion revascularization, non-fatal ischemic stroke, and stent thrombosis ) of 7.1% and a major bleeding rate of 0.8% among 226 Taiwanese ACS patients receiving reduced-dose prasugrel [15]. Similarly, in the multicenter SWITCH study involving Taiwanese ACS patients, the 48-week incidence of MACE was low (1.0%), and the major bleeding rate remained acceptable (2.0%) following a switch from clopidogrel to prasugrel [16]. Collectively, these results align closely with our study, suggesting that the effectiveness and safety of reduced-dose prasugrel are consistently observed across different Taiwanese populations and clinical contexts.
Importantly, our multivariate analysis revealed that patients with prior stroke, diabetes mellitus, and those undergoing CTO interventions had significantly higher bleeding risk. Specifically, a prior history of stroke increased the odds of major bleeding by more than 10-fold (OR 10.53, 95% CI 2.45–45.22), aligning with the result of subgroup analysis in the TRITON-TIMI 38 study4 and current international guidelines. 2023 ESC guidelines for the management of acute coronary syndromes explicitly contraindicate the use of prasugrel in patients with prior stroke due to elevated bleeding risk [17]. Our study thus reinforces the importance of guideline adherence in high-risk subgroups. In addition, while prasugrel has been officially approved in Taiwan for ACS since 2018, our registry also included patients with CCS. Although ischemic events in CCS were infrequent, the increased bleeding risk—particularly among those with prior stroke, diabetes, or CTO lesions — raises concerns and supports a cautious approach. These findings underscore the need for further prospective studies before considering broader off-label use in CCS, and may inform future regulatory or guideline updates regarding expanded indications in the Taiwanese context.
Subgroup analysis of ischemic endpoints revealed several key predictors associated with adverse outcomes. For MACE, hypertension, stent length ≥30 mm, and LCX as the target vessel were significantly correlated with increased event rates. Notably, CKD (eGFR <60 mL/min/1.73m²), long total stent length (≥30 mm), DES use, LCX and LM lesions, and frailty were significantly associated with increased ischemic risk. Furthermore, multivariate analysis demonstrated that male sex, CKD, and LCX as target vessel emerged as independent predictors for composite ischemic outcomes. These findings reflect the interplay between anatomical complexity, comorbid conditions, and treatment strategies. For example, patients undergoing PCI to LCX or LM often present with more technically demanding lesions, which may result in residual ischemia or higher risk of restenosis. Likewise, frail patients may receive modified therapies or shorter durations of DAPT, further contributing to suboptimal outcomes.
Another key observation in this study was the frequent switching between P2Y12 inhibitors in real-world settings. Over half of the patients had previously received either clopidogrel or ticagrelor before transitioning to prasugrel. The leading causes for switching were dyspnea (especially from ticagrelor), bleeding, and intolerance. These patterns reflect the complexity of antiplatelet decision-making in clinical practice and highlight the need for practical algorithms to guide therapy adjustment based on side effects, genetic factors (e.g., CYP2C19 polymorphism), and patient risk profiles.
5. Limitations
Several limitations must be acknowledged. First, this was a retrospective, observational study and thus subject to potential selection and reporting bias. Second, while the overall sample size was sizable, some important subgroups—such as CCS patients, those with prior stroke, or those receiving oral anticoagulants—were relatively small, limiting the statistical power for subgroup analysis. Third, although clinical outcomes were carefully adjudicated, the possibility of underreporting events such as minor bleeding or asymptomatic restenosis cannot be excluded. Fourth, there was no clopidogrel or ticagrelor control group, which precludes direct comparative interpretation. Lastly, because reduced-dose prasugrel is not currently approved for CCS in Taiwan, our findings in this population should be considered exploratory and hypothesis-generating only. Future prospective, multicenter studies—ideally randomized—are needed to validate our findings and support potential label expansion or guideline refinement.
6. Conclusions
Our findings support the use of reduced-dose prasugrel in Taiwanese patients with ACS, demonstrating consistent ischemic protection and low bleeding rates in real-world practice. These results align with local and regional data, reinforcing its clinical utility in East Asian populations. Further research is warranted to confirm its safety in specific high-risk subgroups and to refine individualized antiplatelet strategies.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This work was supported by Daiichi Sankyo Co., Ltd.
Ethics Statement
This study was conducted in accordance with the ethical standards of the institutional review boards of all participating centers. Given the retrospective nature of the research and use of de-identified data, the requirement for written informed consent was waived by each institutional review board.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
References
- S Yusuf, F Zhao, S R Mehta, S Chrolavicius, G Tognoni, K K Fox. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345(7):494-502.
- Steven R Steinhubl, Peter B Berger, J Tift Mann 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA . 2002;288(19):2411-20.
- Mehta, S.R.; Yusuf, S.; Peters, R.J.; Bertrand, M.E.; Lewis, B.S.; Natarajan, M.K.; Malmberg, K.; Rupprecht, H.-J.; Zhao, F.; Chrolavicius, S.; et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet 2001, 358, 527–533. [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. New Engl. J. Med. 2007, 357, 2001–2015. [CrossRef]
- Lars Wallentin 1, Richard C Becker, Andrzej Budaj, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361(11):1045-57.
- Shigeru Saito, Takaaki Isshiki, Takeshi Kimura, et al. Efficacy and safety of adjusted-dose prasugrel compared with clopidogrel in Japanese patients with acute coronary syndrome: the PRASFIT-ACS study. Circ J. 2014;78(7):1684-92.
- Nakamura, M.; Iizuka, T.; Sagawa, K.; Abe, K.; Chikada, S.; Arai, M. Prasugrel for Japanese patients with acute coronary syndrome in short-term clinical practice (PRASFIT-Practice I): a postmarketing observational study. Cardiovasc. Interv. Ther. 2017, 33, 135–145. [CrossRef]
- Nakamura M, Kitazono T, Kozuma K, et al. "Prasugrel for Japanese Patients With Ischemic Heart Disease in Long-Term Clinical Practice (PRASFIT-Practice II) - 1-Year Follow-up Results of a Postmarketing Observational Study." Circ J. 2019;83(1):101-108.
- Akita, K.; Inohara, T.; Yamaji, K.; Kohsaka, S.; Numasawa, Y.; Ishii, H.; Amano, T.; Kadota, K.; Nakamura, M.; Maekawa, Y. Impact of reduced-dose prasugrel vs. standard-dose clopidogrel on in-hospital outcomes of percutaneous coronary intervention in 62 737 patients with acute coronary syndromes: a nationwide registry study in Japan. Eur. Hear. J. - Cardiovasc. Pharmacother. 2019, 6, 231–238. [CrossRef]
- Shoji, S.; Sawano, M.; Sandhu, A.T.; Heidenreich, P.A.; Shiraishi, Y.; Ikemura, N.; Ueno, K.; Suzuki, M.; Numasawa, Y.; Fukuda, K.; et al. Ischemic and Bleeding Events Among Patients With Acute Coronary Syndrome Associated With Low-Dose Prasugrel vs Standard-Dose Clopidogrel Treatment. JAMA Netw. Open 2020, 3, e202004–e202004. [CrossRef]
- Yu Chen Wang. J Taiwan Cardiovasc Interv 2024;15:63-72.
- Chiang, F.-T.; Shyu, K.-G.; Wu, C.-J.; Mar, G.-Y.; Hou, C.J.-Y.; Li, A.-H.; Wen, M.-S.; Lai, W.-T.; Lin, S.-J.; Kuo, C.-T.; et al. Predictors of 1-year outcomes in the Taiwan Acute Coronary Syndrome Full Spectrum Registry. J. Formos. Med Assoc. 2014, 113, 794–802. [CrossRef]
- Honda, S.; Lee, S.; Cho, K.H.; Takegami, M.; Nishihira, K.; Kojima, S.; Asaumi, Y.; Saji, M.; Yamashita, J.; Hibi, K.; et al. Clinical outcomes of adjusted-dose versus standard-dose prasugrel in East Asian patients with acute myocardial infarction. Int. J. Cardiol. 2024, 410, 132197. [CrossRef]
- Kwon, O.; Park, D.-W. Antithrombotic Therapy After Acute Coronary Syndromes or Percutaneous Coronary Interventions in East Asian Populations. JACC: Asia 2022, 2, 1–18. [CrossRef]
- Chang, H.-H.; Hung, C.-F.; Chen, Y.-J.; Fang, C.-C. Clinical Efficacy and Safety of Reduced-Dose Prasugrel After Percutaneous Coronary Intervention for Taiwanese Patients with Acute Coronary Syndromes. J. Clin. Med. 2024, 13, 7221. [CrossRef]
- Liu, P.-Y.; Su, C.-H.; Kuo, F.-Y.; Lee, W.-L.; Wang, Y.-C.; Lin, W.-S.; Chu, P.-H.; Lu, T.-M.; Lo, P.-H.; Lee, C.-H.; et al. Prasugrel switching from clopidogrel after percutaneous coronary intervention for acute coronary syndrome in Taiwanese patients: an analysis of safety and efficacy. Cardiovasc. Interv. Ther. 2021, 37, 269–278. [CrossRef]
- Byrne, R.; Coughlan, J.J.; Rossello, X.; Ibanez, B.; Members of the Task Force for the 2023 ESC Guidelines for the management of acute coronary syndromes; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; et al. Key priorities for the implementation of the 2023 ESC Guidelines for the management of acute coronary syndromes in low-resource settings. Eur. Hear. J. - Qual. Care Clin. Outcomes 2025. [CrossRef]
Figure 1.
A. The percentage of switching from other P2Y12 inhibitors to prasugrel. B. Reasons for switching from other P2Y12 inhibitors to prasugrel.
Figure 1.
A. The percentage of switching from other P2Y12 inhibitors to prasugrel. B. Reasons for switching from other P2Y12 inhibitors to prasugrel.
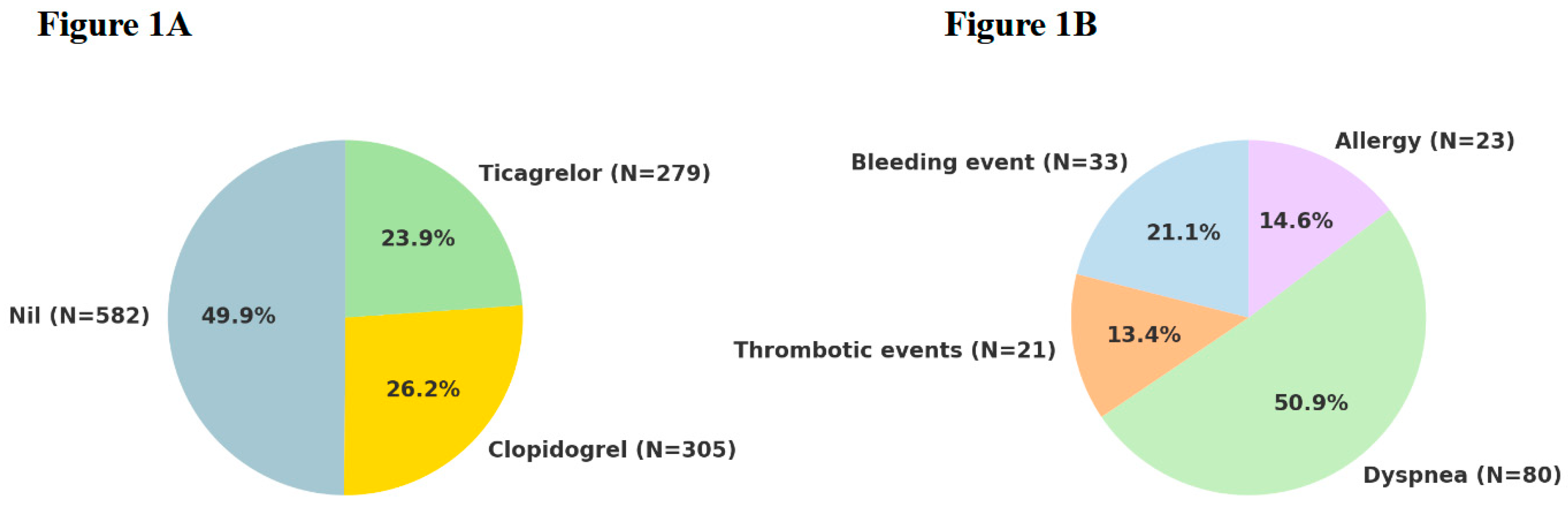
Figure 2.
One-year clinical outcomes. The incidences of MACE, composite ischemic events, stent thrombosis, major bleeding, and overall bleeding (major + minor) are shown. The overall safety and efficacy profile of reduced-dose prasugrel was favorable.
Figure 2.
One-year clinical outcomes. The incidences of MACE, composite ischemic events, stent thrombosis, major bleeding, and overall bleeding (major + minor) are shown. The overall safety and efficacy profile of reduced-dose prasugrel was favorable.
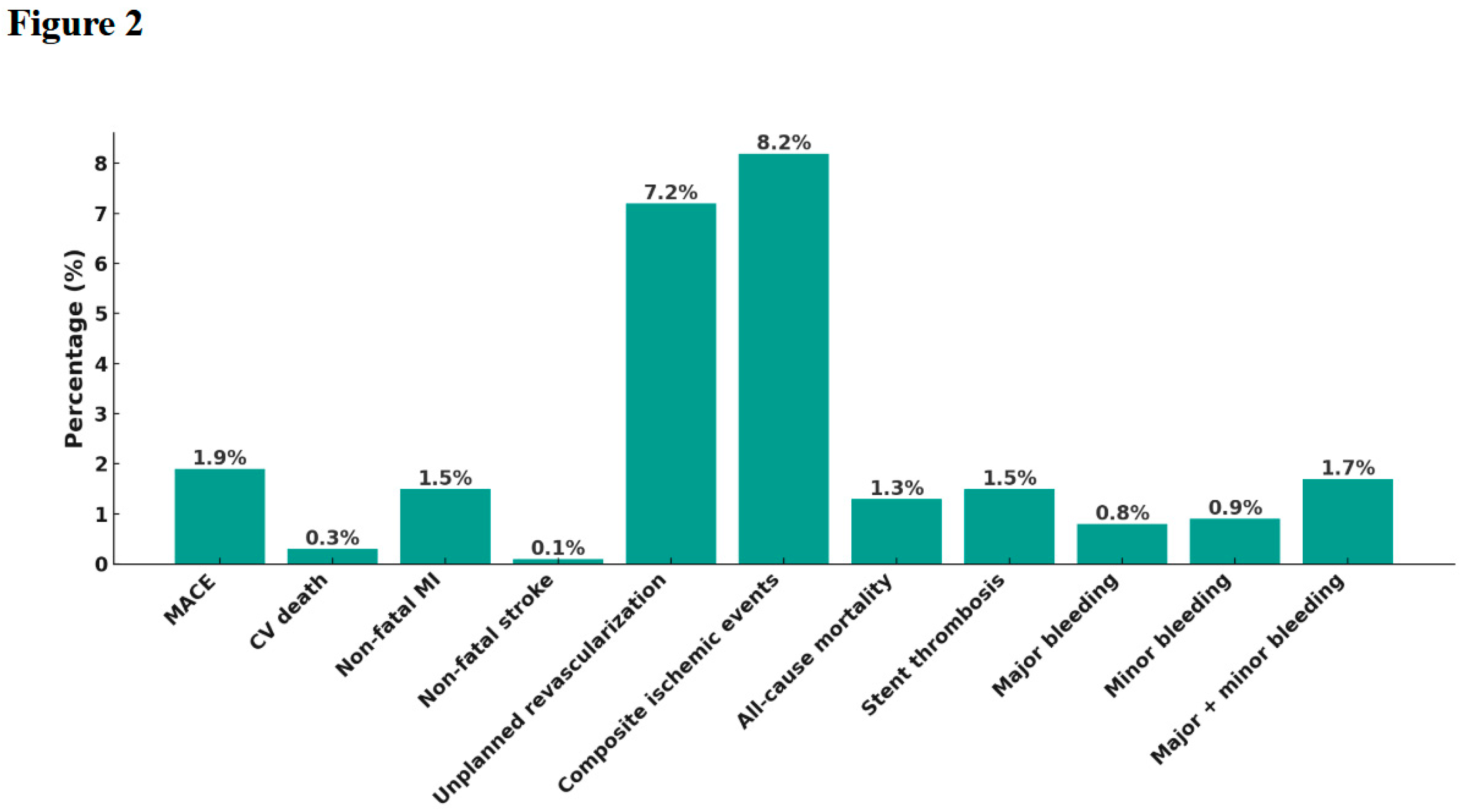
Figure 3.
Subgroup analysis of one-year MACE. Clinical characteristics such as hypertension, stent length ≥30 mm, and LCX as the target vessel were associated with higher MACE rates in exploratory analysis.
Figure 3.
Subgroup analysis of one-year MACE. Clinical characteristics such as hypertension, stent length ≥30 mm, and LCX as the target vessel were associated with higher MACE rates in exploratory analysis.
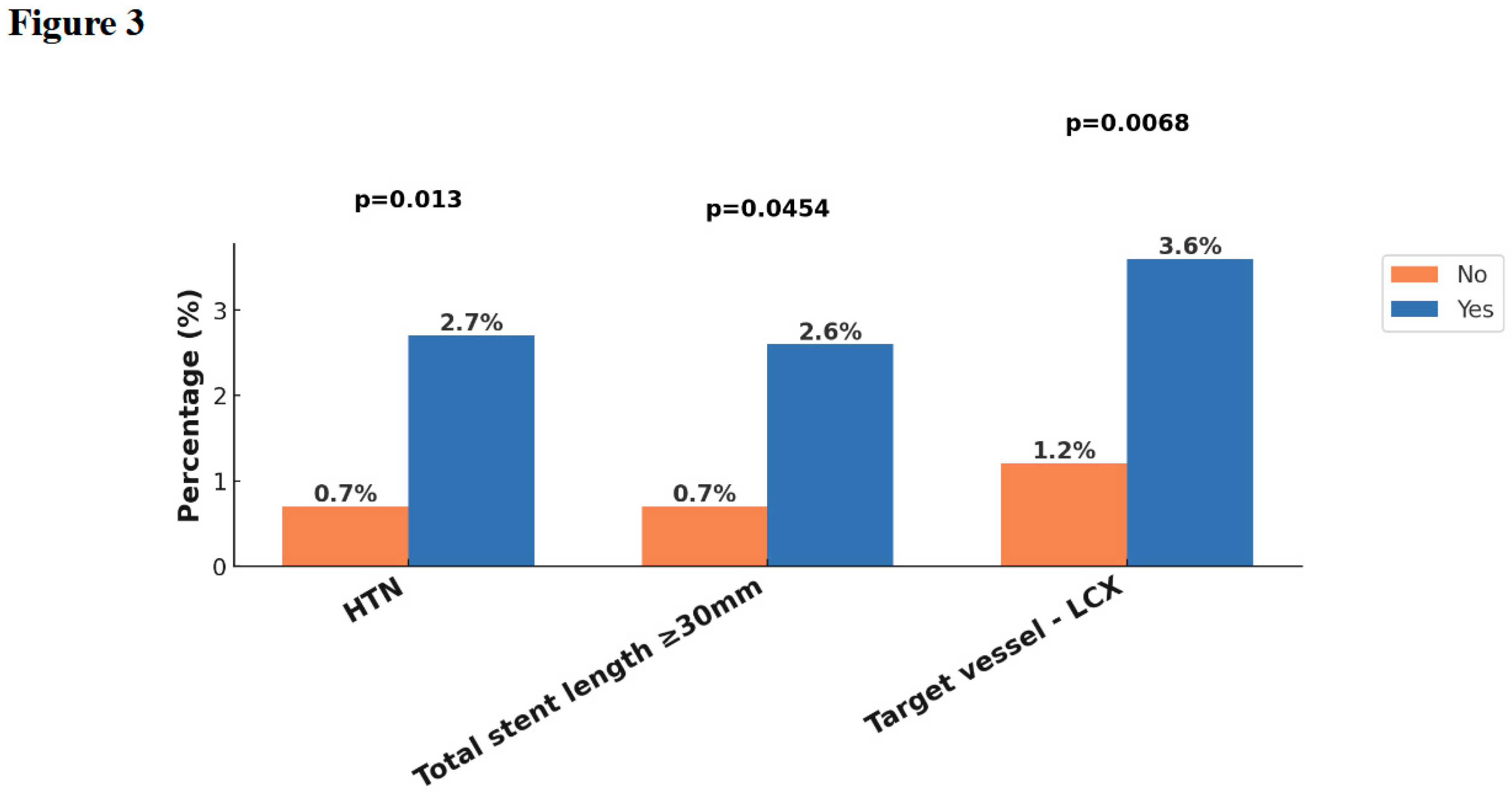
Figure 4.
Subgroup analysis of composite ischemic events (MACE plus unplanned revascularization). Factors such as CKD (eGFR <60), long stent length, DES use, LM and LCX lesions, and frailty were associated with increased ischemic risk in subgroup comparison.
Figure 4.
Subgroup analysis of composite ischemic events (MACE plus unplanned revascularization). Factors such as CKD (eGFR <60), long stent length, DES use, LM and LCX lesions, and frailty were associated with increased ischemic risk in subgroup comparison.
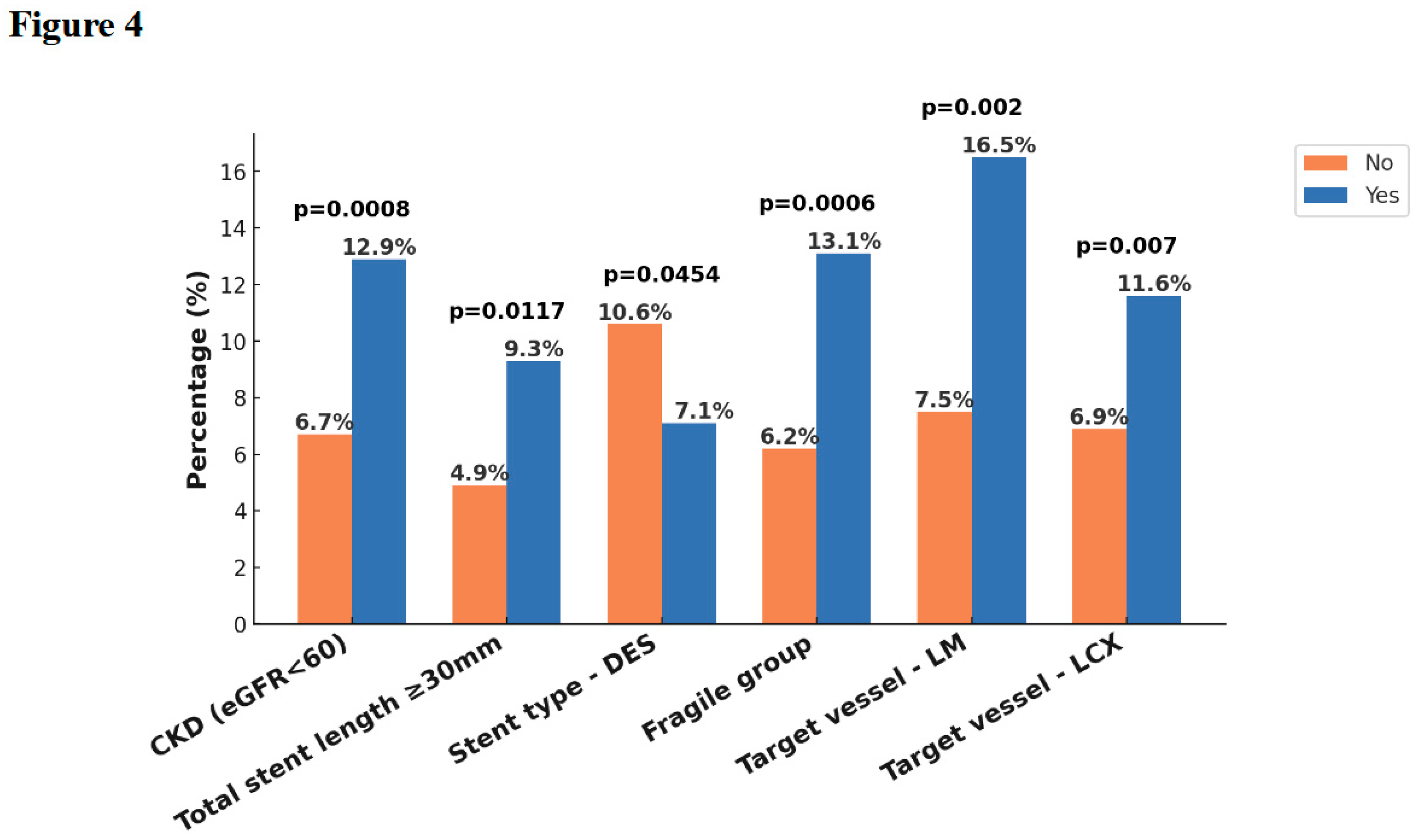
Figure 5.
Subgroup analysis of major bleeding. A history of stroke and the presence of diabetes mellitus were associated with increased risk of major bleeding events.
Figure 5.
Subgroup analysis of major bleeding. A history of stroke and the presence of diabetes mellitus were associated with increased risk of major bleeding events.
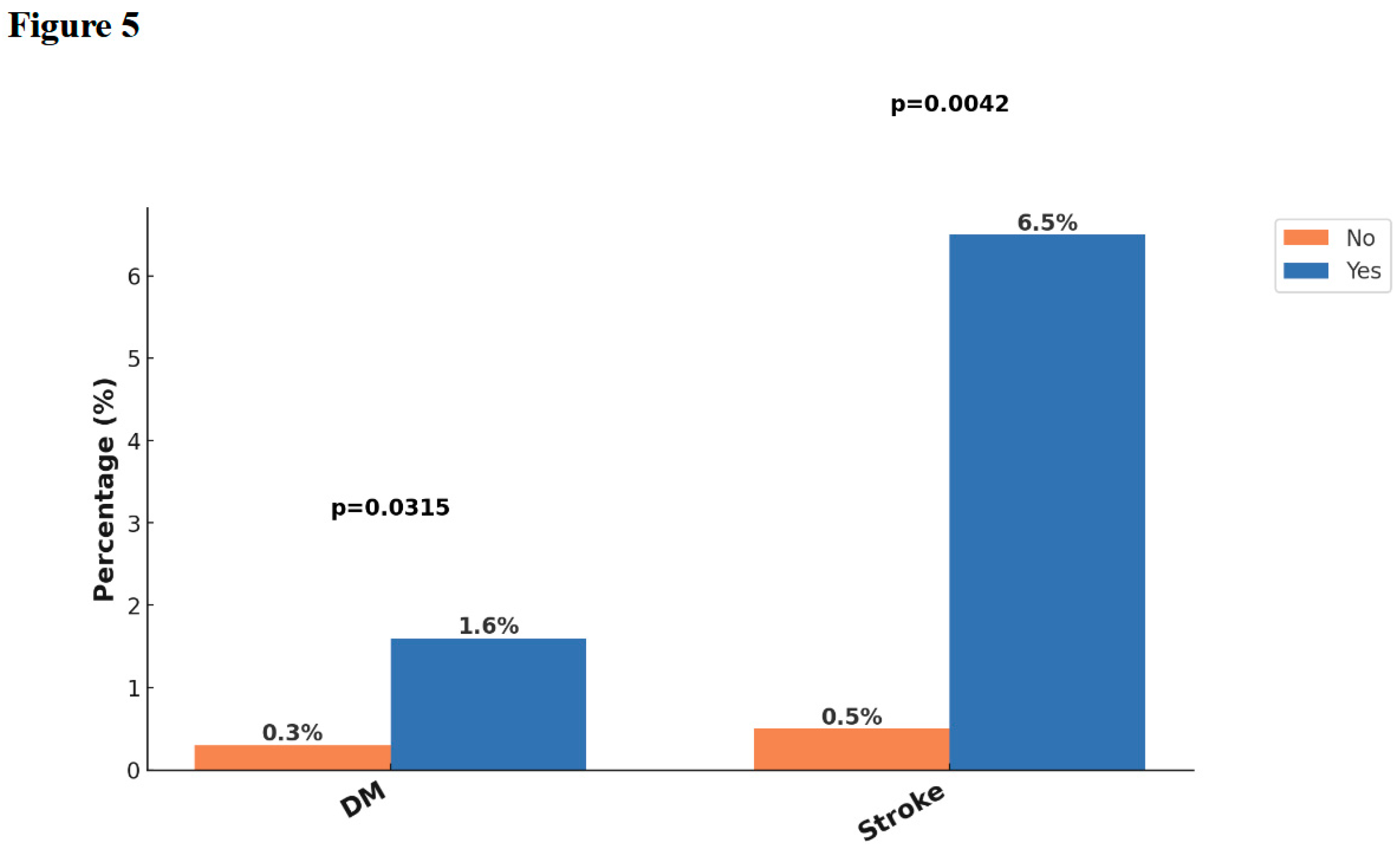
Figure 6.
Subgroup analysis of combined major and minor bleeding. Bleeding events were more frequent among patients with CCS, prior stroke, and those undergoing CTO intervention.
Figure 6.
Subgroup analysis of combined major and minor bleeding. Bleeding events were more frequent among patients with CCS, prior stroke, and those undergoing CTO intervention.
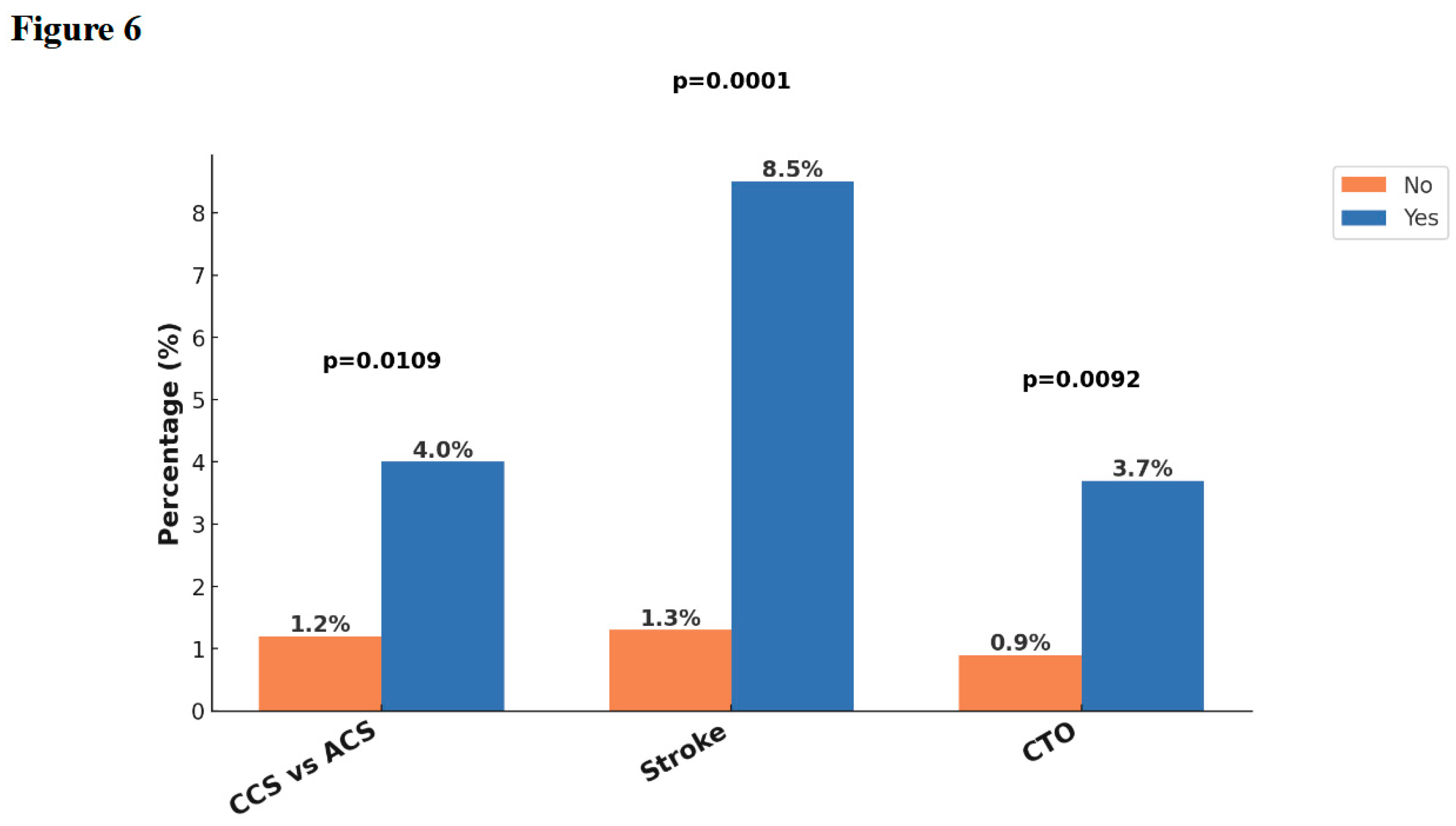
Figure 7.
Multivariate logistic regression analysis for clinical outcomes. Independent predictors of ischemic and bleeding events at 1 year are shown, including ORs and 95% CIs for MACE, composite ischemic events, major bleeding, and overall bleeding.
Figure 7.
Multivariate logistic regression analysis for clinical outcomes. Independent predictors of ischemic and bleeding events at 1 year are shown, including ORs and 95% CIs for MACE, composite ischemic events, major bleeding, and overall bleeding.
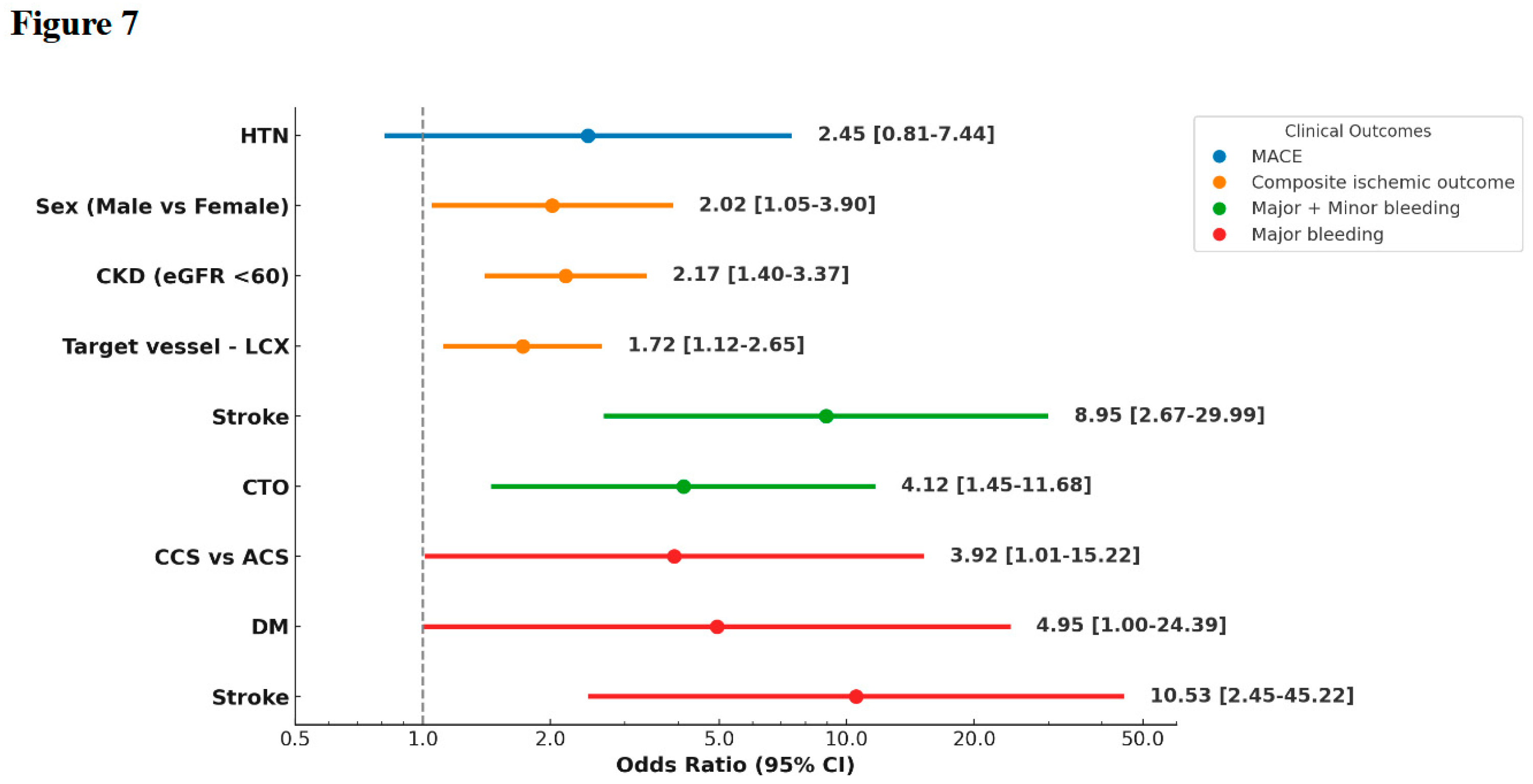

Table 1.
Baseline Clinical and Angiographic Characteristics of the Study Population.
| Characteristic | All N (=1167) |
| Age | 63.9 (11.9) |
| >75 | 162 (13.9) |
| Male | 948 (81.2) |
| ACS vs. CCS | |
| STEMI | 336 (28.8) |
| NSTEMI | 314 (26.9) |
| Unstable angina | 268 (23.0) |
| Chronic stable phase after ACS | 45 (3.9) |
| CCS | 198 (17.0) |
| Concomitant anti-thrombotic agents during the index event | |
| Nil | 185 (15.9) |
| Aspirin | 951 (81.5) |
| Warfarin | 3 (0.3) |
| DOAC | 14 (1.2) |
| Aspirin + warfarin | 2 (0.2) |
| Aspirin + DOAC | 12 (1.0) |
| PCI | 1060 (90.8) |
| Undergoing coronary stent implantation | 941 (80.6) |
| Drug-eluting stent | 813 (69.7) |
| Bare-metal stent | 156 (13.4) |
| Complex PCI | 819 (70.2) |
| Left main | 97 (8.3) |
| True bifurcation lesion | 400 (34.2) |
| CTO | 187 (16.0) |
| Stenting longer than 30mm | 566 (48.5) |
| ≥3 stents | 123 (10.5) |
| Syntax score ≥ 33 | 73 (6.3) |
| Calcified plaque requiring atherectomy | 105 (9.0) |
| Mechanical support | 148 (12.7) |
| Vascular access | |
| Radial arteries | 845 (72.4) |
| Femoral arteries | 260 (22.3) |
| The target coronary arteries during PCI | |
| Left main | 97 (8.3) |
| LAD | 653 (56.0) |
| LCX | 335 (28.7) |
| RCA | 373 (32.0) |
| SVG | 2 (0.2) |
| 3 vessel CAD | 326 (27.9) |
| Comorbidities | |
| Hypertension | 709 (60.8) |
| Diabetes | 446 (38.2) |
| Hyperlipidemia | 320 (27.4) |
| Chronic kidney disease | 222 (19.0) |
| Stroke | 49 (4.2) |
| Fragile population | 8 (0.7) |
Continuous variables are shown in mean (standard deviation); categorical variables are shown in number of patients (% of total patients). ACS = acute coronary syndrome; CCS = chronic coronary syndrome; STEMI = ST-segment elevation myocardial infarction; NSTEMI = Non–ST-segment elevation myocardial infarction; DOAC = direct oral anticoagulant; PCI = percutaneous coronary intervention; CTO = chronic total occlusion; LAD = left anterior descending artery; LCX = left Circumflex artery; RCA = right coronary artery; SVG = saphenous vein graft; CAD = coronary artery disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



