Submitted:
19 July 2025
Posted:
21 July 2025
You are already at the latest version
Abstract
Background: VEGF regulates tumor vascularization in response to hypoxia and inflam-matory signals while curcumin is anti-inflammatory. We investigated this interaction in breast cancer cell lines and gene expression databases. Methods: VEGF in cell cultures was detected by ELISA. Kinase activation was investigated by Western blotting. Gene ex-pression databases were analyzed by correlation tests. Results: VEGF secretion and kinase signaling in response to IL-1β and curcumin varied significantly for the cell lines. All cell lines increased VEGF secretion under hypoxia, but IL-1β increased VEGF secretion only in MCF-7 cells. VEGF secretion was inhibited by curcumin in MDA-MB-231 cells but in-creased in MCF-7- and UACC-3199 cells. Inhibitor experiments in MCF-7 cells demon-strated that curcumin-induced ERK- phosphorylation was important for VEGF secretion. In a retrospective cohort, VEGF detected by immunohistochemistry correlated with ductal- versus lobular morphology but showed no prognostic significance. Gene expression data of the METABRIC study showed highest VEGFA mRNA expression in triple negative breast cancer. Analysis of HIF-, NF-kB-signaling and VEGF expression on the mRNA level showed no clear correlation but suggested crosstalk of these pathways. Conclusion: These dissimilar responses of breast cancer cell lines suggest that therapy efficiency with an-ti-VEGF, anti-IL-1β or curcumin will also vary within breast cancers.
Keywords:
Breast cancer
; curcumin
; Interleukin-1β
; p38-MAPK
; ERK
; VEGF
1. Introduction
Breast cancer (BC) is a heterogeneous neoplasm representing the most frequent cancer in women with about 2.2 million new cases (in 2020) worldwide. It is still the leading cause of mortality in women [1]. Besides morphological characteristics, four biomarkers are required for defining the most important BC subtypes in a clinical setting. Thus, besides morphological characteristics, breast cancers are classified according to the expression of receptors for estrogen (ER), progesterone (PgR), epidermal growth factor receptor-2 (HER2/neu, erb-b2) and the proliferation marker Ki67. These biomarkers define the intrinsic molecular subtypes [2] of breast cancer without extensive gene expression analysis in a clinical setting [3]. The molecular subtypes of BC are the luminal A subtype, expressing the estrogen receptor α (ER) and/or the progesterone receptor (PgR) without HER2/neu-overexpression and a low percentage of Ki67-positive, proliferating cells. Luminal B also expresses the ER/PgR receptors and is characterized by either high Ki67 frequency or HER2/neu-overexpression [4]. The next type, overexpressing HER2/neu in the absence of ER/PgR is called HER2/neu-positive (non-luminal). Finally the absence of these three receptors is known as triple negative breast cancer (TNBC) and closely resembles the molecularly defined basal subtype [5,6].
Estrogen receptor-expressing tumors are the most frequently occurring class representing about two out of three cancers. PgR is mostly expressed in ER-positive cases, but rare cases expressing PgR in the absence of ER have also been described [7]. Patients with ER-expressing tumors have a far better prognosis than the other subtypes and can be treated by endocrine therapy, either with selective estrogen mediators such as tamoxifen for premenopausal women or aromatase inhibitors for postmenopausal patients [8]. Luminal B cases represent a more aggressive form of luminal breast cancer, which is often treated by additional chemo- and/or radiotherapy or an HER2/neu targeted therapy. The decision to use an additional cytotoxic and potentially harmful chemotherapy can be hard to take and several gene expression tests have been developed to assess the tumor recurrence rate better than with hormone receptor expression and Ki67 alone [9,10]. For HER2/neu-over-expressing cases, a targeted therapy using monoclonal anti-HER2/neu-antibodies (e.g., Trastuzumab) has been approved by the FDA in 1998. This therapy has greatly improved the outcome of this type of cancer and other opportunities even for low and ultra-low Her2/neu expressing cases are now available [11]. No targeted therapy for the remaining heterogeneous group [12] of TNBC patients (10-20%) is available; thus chemo- and radiotherapy are typically applied. This type of cancer has the worst outcome [13]. Nevertheless, with the introduction of immunotherapy using checkpoint inhibitors, an additional treatment option is available [14]. A subgroup of BC is caused by germ-line mutations. Patients with inherited breast cancer often carry mutations in BRCA1 and BRCA2 (about 5%) and have a TNBC-like appearance.
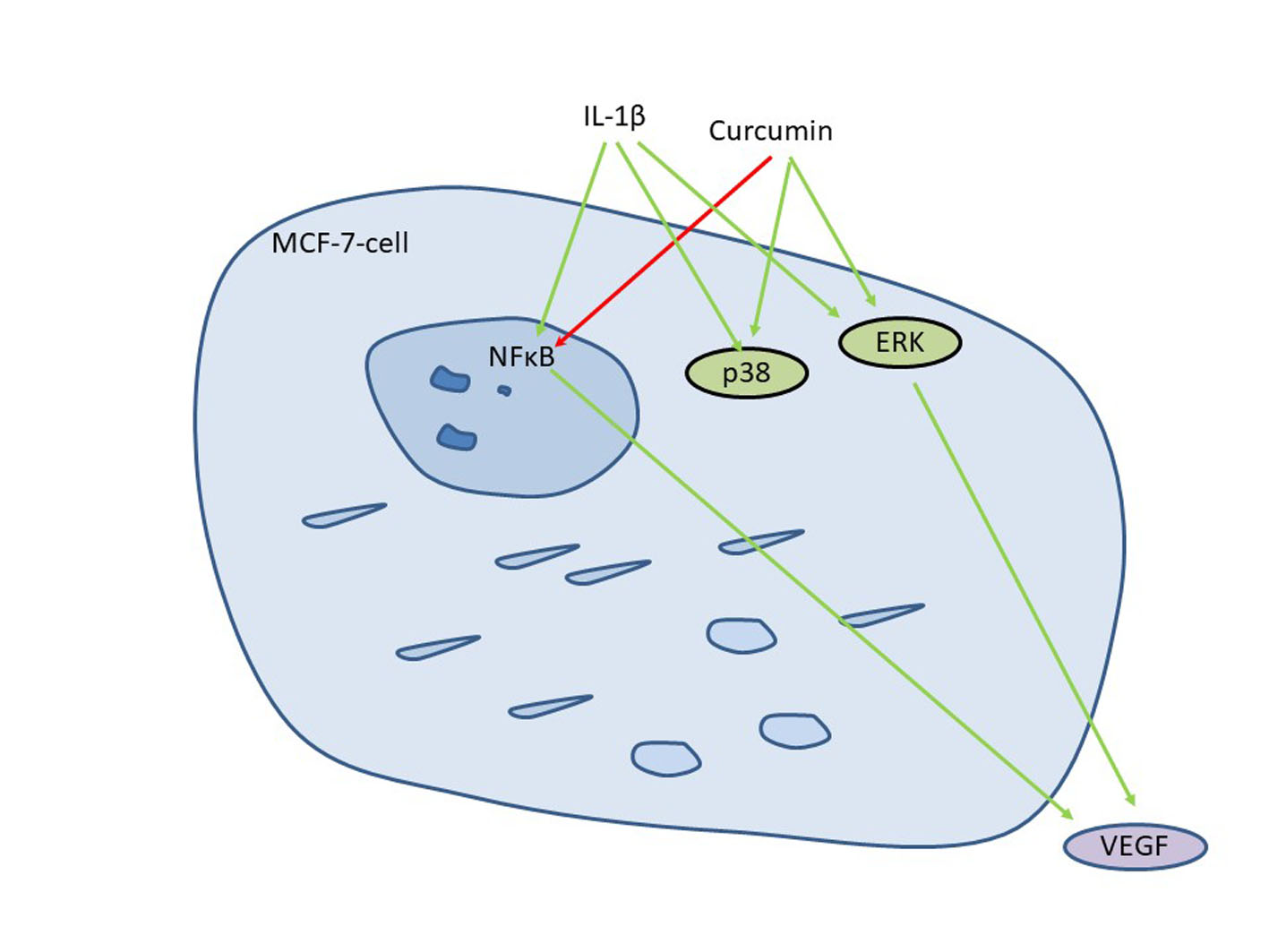
Interactions of tumor cells with the microenvironment including immune cells [15], cancer associated fibroblasts [16] and mesenchymal stem cells [17] have a significant impact on the effectiveness of therapy. An important factor produced in the tumor microenvironment is Interleukin 1β (IL-1β). It is involved in malignant and inflammatory processes [18] and, besides other effects, regulates the expression of the vascular endothelial growth factor (VEGF-A) in several cancer entities via activation of the transcription factor NF-kB [19,20,21]. VEGF in turn influences the prognosis of several cancer entities as it regulates angiogenesis and therefore nutrient and oxygen supply, especially of larger tumors [22]. Besides VEGF regulation by IL-1β its expression is triggered by hypoxia, mediated by the expression of hypoxia-induced factor (HIF1A) [23]. We have recently shown that IL-1β-induced VEGF-A secretion in chondrosarcoma cells can be inhibited by the natural compound curcumin [19]. This phenolic compound causes the yellow color of turmeric, the major constituent of curry [24]. Curcumin has been attributed a magnitude of positive effects, ranging from anti-cancer, anti-oxidative effects to plasma cholesterol control [25,26]. Curcumin inhibits IL-1β-receptor signaling by preventing the recruitment of interleukin-associated kinase (IRAK) and is therefore anti-inflammatory [27] but a multitude of other targets has been described [24]. In chondrosarcoma- [19] and fibrosarcoma [28] cell lines, curcumin downregulates VEGF and other NF-kB-regulated genes at concentrations that inhibit NF-kB activation. For breast cancer, an inhibition of VEGF expression in the triple negative MDA-MB-231 [29] and the estrogen receptor positive T47D cell line has also been observed [30].
The relevance of Il-1β signaling for VEGF secretion and the influence of curcumin in BC subtypes is still not completely understood. We therefore investigated the interplay of IL-1β, curcumin and VEGF production in cell lines representing the major BC subtypes. Furthermore, we correlated VEGF expression with BC subtype and outcome in a retrospective BC cohort. Finally, to further assess the importance of this signaling cascade, we explored the METABRIC breast cancer dataset [31] and the cancer Cell Line Encyclopedia [32] for expression of IL-1β signaling pathway members and HIF1A. Using these data, we intended to estimate how effective an anti-IL-1β/-VEGF directed therapy i.e., by curcumin in the breast cancer subclasses could be.
2. Materials and Methods
2.1. Cells and Cell Culture
Cell-lines were obtained from ATCC and maintained at 37°C with 5% CO2 enriched atmosphere in RPMI-1640 medium without phenol-red (Biochrom, Berlin, Germany) but supplemented with 9 % fetal calf serum (FCS, Biochrom, Berlin, Germany) and glutamax (Gibco-Thermo) as recommended. Cells were transferred weekly by using trypsin/EDTA (Biochrom).
2.2. Cell Stimulation and Viability Assay
Cells were seeded in 24- (for VEGF-secretion) or 48-well (for viability) plates (Greiner Bio-One, Germany) to a confluence of about 50% (80,000 or 40,000 cells, respectively). After 24h, medium was removed and replaced with fresh medium containing the compound under study or solvent (0.1%). Preincubation with kinase inhibitors UO126 (1 µM) and SB 203580 (1 µM) (both from Merck-Calbiochem, Darmstadt, Germany) or curcumin (#C1386, Sigma-Aldrich, Munich, Germany) was done for 2.5 hours before IL-1β or curcumin was added. For short time stimulation and determination of early signaling events, cells were grown to confluence and serum-starved for 24 h. IL-1β (10 ng/mL) was added for ten minutes before medium was aspirated and cells lysed with TRIS/Cl 50 mM, pH 6.8 containing SDS (2%) and phosphatase and protease inhibitors (Sigma-Aldrich, Munich, Germany). For VEGF-secretion studies, cells were incubated with curcumin, IL-1β or DMSO for further 24 h with or without the presence of serum. Then, the culture supernatant was sampled for VEGF-determination and cells lysed for Western blot analysis as described. In some cases, resazurin (final concentration: 10 µg/mL) was added after collecting the supernatant to control the viability of the cells [33]. For hypoxia, 80,000 cells per well were seeded into 24 well plates, The next day, medium was changed and the plate was placed into a hypoxic bag (Anaerocult A mini), sealed with an anaeroclip and controlled for hypoxic conditions using anaerotest (all Merck-Millipore) for 24 h whereas a control plate was kept under normoxic conditions.
2.3. Western Blotting
From cell cultures, total protein was obtained by lysis with TRIS/Cl (50 mM, pH 6.8) supplemented with SDS (2%) and protease- as well as phosphatase-inhibitors (both Sigma-Aldrich, Munich, Germany). For VEGF-determination by Western blot, serum free cell culture supernatant was concentrated 100-fold by ultrafiltration as described [19]. Denatured and reduced proteins were separated on denaturing polyacrylamide gels (15% for VEGF and 12 % for all other applications). Transfer to nitrocellulose membranes (Millipore) was performed by semi dry blotting in CAPS-buffer (50 mM, pH 10) supplemented with methanol (10%) and 3-mercaptopropionic acid (1 mM) as described earlier [34]. Filters were blocked with TBS/NP40/BSA (TRIS/Cl 50 mM, pH 7.4 containing BSA (2%) NP-40 (0.2%)) and sodium azide (0.03 %). Primary antibodies were applied in the same buffer overnight at 4°C. Washing (3 x 15 min) and incubation with a secondary antibody (1h) conjugated to horseradish peroxidase (Jackson-Immuno via Dianova, Germany) and three further washes (15 min) were performed at room temperature in TBS/NP40 with reduced BSA concentration (0.1%) before detection of the signals by enhanced chemiluminescence (Millipore) in a GeneGnome (Syngene) or INTAS Chemostar (Intas, Göttingen, Germany) CCD-camera system.
2.4. VEGF-Determination
VEGF-A in the cell culture supernatants was determined by a commercial ELISA, according to the manufacturer’s recommendations (VEGF-DuoSet, DY293B, R&D, Wiesbaden, Germany). 10 or 50 µL of the cell culture supernatant were analyzed by this assay, depending on the cell line under study and the expected VEGF amount. Data were either presented as VEGF concentration in the cell culture supernatant to directly compare the cell lines with each other or we presented relative VEGF concentrations, where we set the basal VEGF concentration in controls to 1 (relative VEGF concentration). This better represents the changes that were invoked by the treatments for the respective cell line.
2.5. VEGF Determination by Immunohistochemistry in Clinical Samples
VEGF was stained in formaldehyde-fixed paraffin-embedded (FFPE) tissue of 204 breast cancer patients. This collective has been described earlier [35], and the study has been approved by the local ethics committee (AKZ 114/13). After deparaffinisation, epitopes were demasked with TRIS/EDTA buffer (pH 9) for 20 sec at 125°C in a pressure cooker. Primary rabbit polyclonal antibody A20 (Antibody registry: AB_2212984, St. Cruz Biotechnology, Heidelberg, Germany) was applied in Ventana dilution buffer in a dilution of 1:50. Detection was performed in an automated slide staining system (Ventana, Mannheim, Germany) using the iView DAB staining reagents (Ventana). An immunoreactive score (IRS) was determined according to Remmele [36] by assessing staining intensity (0 = no staining, 1 = weak staining, 2 = intermediate staining, 3 = strong staining) and percentage of positive tumor cells (1= <10%, 2 = 11-50%, 3 = 51-80%, 4 = >80%) followed by multiplication of these two parameters. The IRS therefore ranges from 0 to 12. VEGF “high” expression was defined for tumors with an IRS higher than 7 based on the optimal cutoff value in Kaplan Meier survival analysis.
2.6. Statistical Analysis
For the determination of significance, SPSS version 24 (IBM, Armonk, NY: IBM Corp. USA) was used. Means were compared by one-way ANOVA with post-hoc analysis by the Tamhane T2 method, assuming unequal variances. When relative values were averaged, the geometrical mean was used. Data are given +/- standard error when not indicated otherwise in the figures or tables. For comparing inhibitory effects on the IL-1β-induced stimulation of VEGF secretion, this inhibition was calculated relative to the increase in VEGF of the individual experiment. For correlation analysis of VEGF immunoreactive score with hormone receptor status, cross tabulation analysis was performed with significance level p determined by Pearson’s R test (interval by interval). Crosstabulation analysis with Fisher’s exact test was applied to show correlation of categorical parameters.
2.7. Analysis of Public Gene Expression Databases
Gene expression data were either analyzed with the tools provided at the cbioportal [37] website or downloaded (http://www.cbioportal.org/) and imported into SPSS (vers. 24, IBM, Armonk, NY: IBM Corp. USA) and then used for cross-tabulation, correlation and survival analysis. Cluster analysis was performed using the online tools at CIMminer (https://discover.nci.nih.gov/cimminer/home.do) [38].
2.8. Visualisation of Interactions Using Cytoscape
Cytoscape vers. 3.8.0 [39] was used for visualization of correlation data. The network was enriched with data from the string database using a confidence cut-off value of 0.4 with no request for additional interactors.
2.9. RNA Extraction and qRT-PCR
RNA was extracted from cell cultures using the NucleoSpin RNA kit (Macherey and Nagel, Düren, Germany) according to the manufacturer’s recommendations. cDNA was synthesized using Script Reverse Transcriptase and oligodT primers from 1 µg of total RNA (Jenabioscience, Jena Germany). Real time PCR was performed using a Roche light cycler 1.0 and the LightCycler® FastStart DNA Master SYBR Green I (Roche-Life Science, Mannheim, Germany) reagents. For VEGFA, forward primer TGCATTGGAGCCTTGCCTTG and reverse primer CGGCTCACCGCCTCGGCTTG were used. For HIF1A forward primer TGCTGGATCACAGACAGCTCA and reverse primer ACCACGTACTGCTGGCAAAGC were used. Normalization was done using RPL13 (forward primer: CCTGGAGGAGAAGAGGAAAGAGA, reverse primer: TTGAGGACCTCTTGTGTATTTGTCAA). Annealing temperature for both PCRs was 60°C.
3. Results
3.1. VEGF-Secretion by Mammary Carcinoma Cell Lines
We first showed that VEGF secretion into the medium occurred under serum-free conditions for the MCF-7 cell line by Western blotting (Figure 1A) as applied for chondrosarcoma cell lines before [19]. Under serum-free conditions, MCF-7 cells do not proliferate further. We used a renal cell carcinoma cell line designated N109 known to secrete high amounts of VEGF as a positive control for the procedure [40]. The observed pattern of VEGF isoforms was comparable to N109 as well as chondrosarcoma cell lines SW1353 and C3842 [19]. β-actin was detected as a positive control for the blotting process, although intact cells were not present in the concentrated growth media. Nevertheless, β-actin is always present in cell culture supernatants due to ongoing cell death and therefore, a slight increase with incubation time was observed.
For further experiments, we applied ELISA for VEGF detection in serum-containing medium as this method provides quantitative data and curcumin was also less toxic to the cells in the presence of serum. The investigated breast cancer cell lines secreted significantly different amounts of VEGF (Figure 1B). The triple negative cell line MDA-MB-231 produced the highest amounts of VEGF followed by the ER-negative, but HER2/neu positive SK-BR-3 and the ER-positive MCF-7 and the ER-negative, but highly DNA-methylated UACC-3199 cell line. IL-1β treatment increased the amount of secreted VEGF only in the MCF-7 cell line (Figure 1B). We repeated this experiment also in serum-depleted medium to exclude effects of signals coming from the serum. The result was essentially as before with MCF-7 being the only cell line showing a significant increase in extracellular VEGF upon IL-1β stimulation (Figure S1).
3.2. VEGF-Expression in Tumor Tissue Samples
As the next step, we stained tumor specimens of our BC cohort [35,41,42,43,44] for VEGF-expression using immunohistochemistry (Figure 2) and correlated the VEGF-status using a cut off of VEGF-IRS ≥ 6 with clinico-pathological parameters and survival (Table 1). VEGF was significantly higher in ductal, compared to lobular BC but no other statistically significant association was found. For survival, we also found no significant correlation of VEGF-expression as detected by IHC (log rank p < 0.05), neither for the whole study population nor in subtype analysis. However, according to the kmplot webtool [45] (kmplot.com, 2nd August 2025) VEGF-mRNA is a negative prognostic factor for disease free survival (HR = 1.43, 95%CI: 1.29 – 2.59, p = 2.4 e-11) for all subtypes included (n= 4,929).
As the TNBC cell line secreted the highest amounts of VEGF, we investigated whether this correlates with the VEGF-IRS of our clinical samples. For this, we correlated the ER- and VEGF-scores by Spearman’s correlation analysis. There was indeed a significant negative correlation, but the correlation factor was low (ρ = -0.13, p = 0.047). To obtain further evidence for this observation and to correlate VEGF-mRNA abundance with the expression of key signaling molecules, we analyzed gene expression data from the METABRIC study [31] and the Cell Line Encyclopedia [32]. In METABRIC, VEGFA mRNA abundance was also highest in triple-negative tumors. In addition, HER2/neu-positive tumors also exhibited high VEGFA mRNA expression (Table 2, Figure 3). We also included IL1B and HIF1A, which encode important VEGFA-regulating signaling molecules, in this analysis (Table 2). IL1B was significantly higher in ER-, HER2/neu-negative cases, including those with TNBC. HIF1A was highly expressed in ER-, PR-negative and TNBC cases. Pearson’s correlation factors were -0.18 (p < 0.01) for HIF1A to VEGFA, 0.03 for IL1B to VEGFA and 0.21 (p < 0.01) for HIF1A to IL1B.
In data from the Cell Line Encyclopedia [32], TNBC cell lines exhibited varying amounts of VEGFA-mRNA (Table S1). Nevertheless, on average, VEGFA was highest in HER2- followed by TNBC- and ER-positive cell lines. Only the difference between ER-positive and TNBC cell lines was significant (p = 0.016, ANOVA, Games-Howell post hoc test). HIF1A correlated with VEGFA (0.274, p = 0.052) and IL1B (0.339, p = 0.015), whereas IL1B correlated highly with VEGFA (0.518, p < 0.001). In cluster analysis using these three genes, TNBC cell lines also do not cluster together (Figure S2).
3.3. IL-1β Activates NF-kB Signaling in Breast Cancer Cell Lines
We then tested whether IL-1β was able to activate NF-κB and thereby cause an increase in VEGF secretion in MCF-7, SK-BR-3 and MDA-MB-231 cell lines. NF-κB activity was estimated by determining the amount of phosphorylated and non-phosphorylated IκBα and p65 (RELA) by Western blotting. By these means, strong activation of NF-κB by IL-1β could be demonstrated in MCF-7, MDA-MB-231, but only moderately in SK-BR-3
Figure 4.
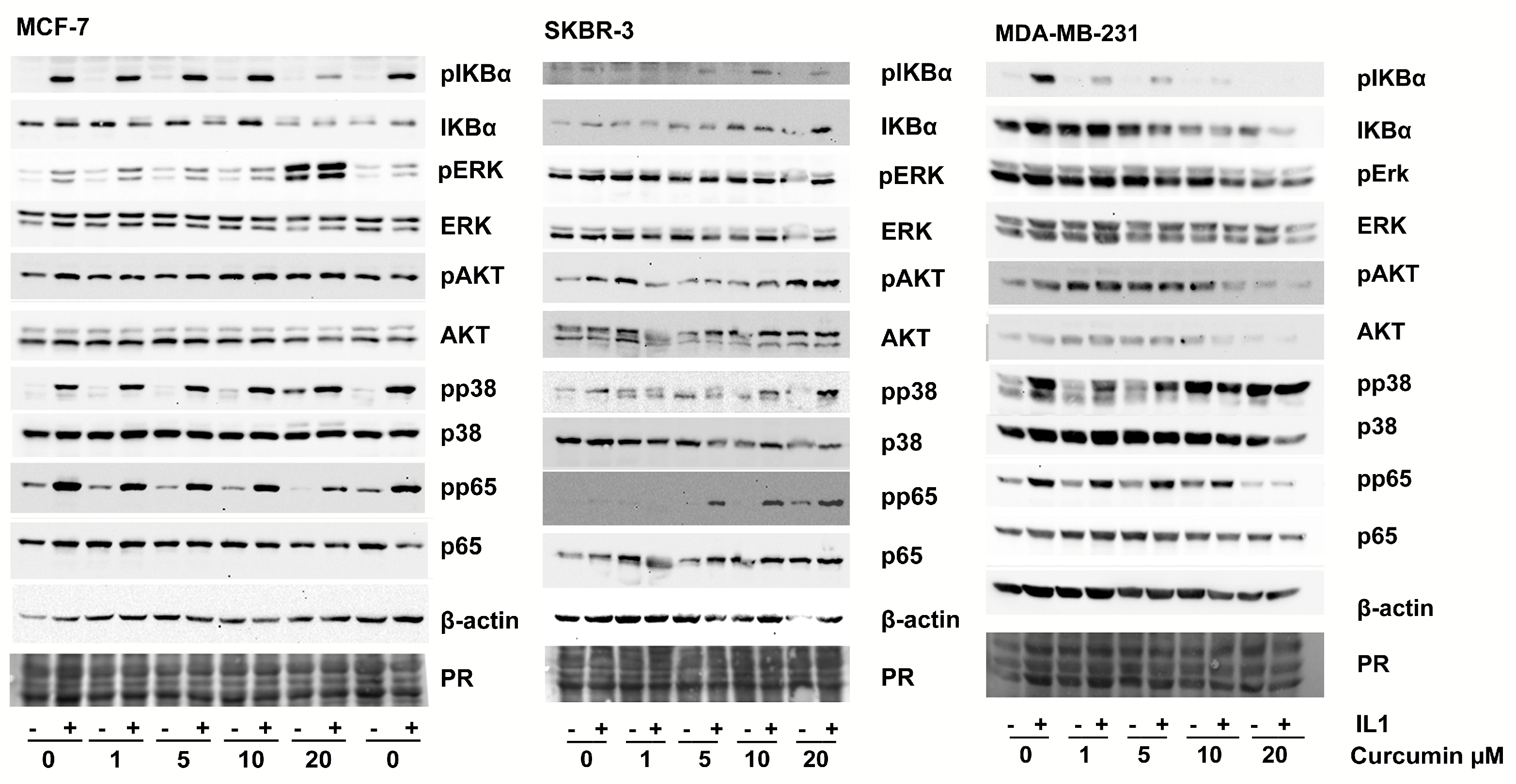
Phosphorylation of signaling proteins in response to curcumin and IL-1β analyzed by Western blotting. Cells were pre-incubated with DMSO (solvent) or curcumin for 2 h before IL-1β (10 ng/mL) was added for 10 minutes. Cells were lysed and total protein subjected to Western blot analysis. One representative result of three replicates is shown. PR: Protein stain.
Figure 4.
Phosphorylation of signaling proteins in response to curcumin and IL-1β analyzed by Western blotting. Cells were pre-incubated with DMSO (solvent) or curcumin for 2 h before IL-1β (10 ng/mL) was added for 10 minutes. Cells were lysed and total protein subjected to Western blot analysis. One representative result of three replicates is shown. PR: Protein stain.
3.4. Curcumin Affects IL-1-Mediated Activation of NF-kB and VEGF Secretion
In parallel, we investigated whether curcumin might interfere with IL-1β-mediated VEGF secretion as seen in the chondrosarcoma cell lines. Similar to this study, our first goal was to find a curcumin concentration that inhibited NF-kB signaling but caused only moderate viability loss for the cells. Curcumin showed similar toxicity to the four cell lines and concentrations below 20 µM resulted in less than 40 % viability loss in 24h (Figure 5A).
MCF-7 turned out to be slightly more tolerant to curcumin as the other cell lines; nevertheless, the differences between the cell lines in this assay were not substantial (Figure 5A). Thus, we continued this study with curcumin concentrations up to 20 µM. Surprisingly, increasing concentrations of curcumin alone resulted in elevated extracellular VEGF in some cell lines (Figure 5B). Especially MCF-7 cells showed this effect between 10 to 20 µM, UACC-3199 showed a nearly linear increase of VEGF secretion and there was no change in SK-BR-3 cells. Only in MDA-MB-231 cells, VEGF secretion was strongly reduced by curcumin at 10 and 20 µM curcumin.
In our analysis of NF-κB and MAP-kinase activation (Figure 4), we detected an inhibition of NF-kB activation (phosphorylation of IκBα and p65) by curcumin in the tolerable concentrations applied in this study for MCF-7 and MDA-MB-231. However, in SK-BR-3, phosphorylation of IκBα and p65 was increased at higher concentrations of curcumin (Figure 4). Phosphorylation of p38-MAPK also responded to IL-1β in MCF-7 and MDA-MB-231 but there was no significant effect seen in SK-BR-3. In MCF-7 and MDA-MB-231 curcumin alone increased p38 MAPK-phosphorylation at concentrations above 10 µM. In MCF-7, ERK was also phosphorylated in response to IL-1β and curcumin. In SK-BR-3 no effect on ERK was apparent and MDA-MB-231 showed a moderate decrease in pERK. AKT was not phosphorylated in response to IL-1β or curcumin in all cell lines tested.
To further investigate the function of ERK and p38-MAPK for the VEGF secretion, we pre-incubated MCF-7 cells with specific inhibitors for p38-MAPK (SB203580, [46]) and ERK (U0126, [47]) before curcumin was added. The applied inhibitor concentrations were established in a previous study and shown to have only a weak effect on cell viability, but significantly inhibited the target kinases [48]. U0126, showed a significant inhibitory effect (0.76-fold of curcumin-induced increase in VEGF, p = 0.01 ANOVA, Tamhane T2-post hoc test) on VEGF secretion into the medium but not SB203580 (0.94-fold, p = 0.93, Figure 5C).
3.5. Effect of Hypoxia on VEGF Secretion
We then became interested in whether VEGF secretion upon hypoxia was also different in the cell lines. However, in these experiments, all cell lines were able to increase VEGF in response to hypoxia (Figure 6), though to varying extents, with MDA-MB-231 displaying the lowest relative increase. In parallel, we analyzed the HIF1A mRNA in this experiment and observed a significant decrease in HIF1A mRNA under hypoxia in all cell lines tested (Figure S3).
4. Discussion
VEGF contributes to tumor vascularization and is prognostic [49] in primary breast cancer, especially the TNBC subtype [50,51]. Anti-angiogenic treatment in combination with chemotherapy of TNBC has therefore attracted considerable interest; however, the results were not completely conclusive [22,52,53]. Whereas in the E2100 trial, the anti VEGF antibody bevacizumab combined with chemotherapy approximately doubled the time until relapse [54], the effect on overall survival was not significant. This was also valid in the BEATRICE trial focusing on early TNBC patients [55]. Recently, a combination with check-point inhibitor directed therapy has been evaluated in a phase II study showing promising results [56].
Two important pathways control VEGF expression. On one hand the hypoxia responsive HIF1α [23,57], on the other hand, VEGF is responsive to inflammatory signals such as IL-1β [58,59]. Indeed, IL-1β increases the invasiveness of TNBC cells via NF-κB and this cytokine is also regulated by NF-κB in a positive regulatory loop [60]. IL-1β is also known as a driver of breast cancer growth and is especially associated with bone metastasis [61,62].
Besides investigating model cell lines, we determined VEGF by immunohistochemistry in our retrospective cohort; however, this did not indicate a significant correlation with relapse and overall survival. However, a high VEGF score correlated significantly with ductal compared to lobular BC. The association with the estrogen receptor or TNBC was also not significant, and we attribute this to the low number of TNBC cases (n = 32, p = 0.18) in our cohort. We also observed a significantly lower VEGF score in cases that did not undergo radiotherapy. This result is hard to explain and we propose that this is caused by the selection criteria of patients for radiotherapy at the time the cohort was established.
The MDA-MB-231 cell line, representing the aggressive TNBC, secreted the highest VEGF amounts. This correlated with VEGF expression in TNBC in clinical samples from the METABRIC study [31]. VEGF, therefore, likely contributes to the unfavorable outcome of TNBC by improving the nutrient and oxygen supply for such fast-growing tumors. However, the BRCA-1 deficient UACC-3199 [63] TNBC cell line secreted significantly less VEGF than MDA-MB-231. Data from the Cell Line Encyclopedia [32] also support the observation that VEGF expression varies within the TNBC cell lines, maybe reflecting the different subtypes of TNBC [64].
This investigation was based on the hypothesis that IL-1β activates VEGF secretion in breast cancer via NF-κB signaling, a process that can potentially be inhibited by curcumin. Thus, curcumin could be beneficial for breast cancer patients. However, we observed a differential response of VEGF to IL-1β as well as to curcumin in the cell models tested. Only the Luminal A cell line MCF-7 responded to IL-1β by significantly increasing VEGF secretion, whereas all cell lines responded to hypoxia by increasing VEGF secretion. Curcumin inhibited or even increased VEGF secretion and NF-κB signaling depending on the cell line. Nevertheless, MDA-MB-231 and MCF-7 were both responsive to IL-1β as shown by NF-kB activation. Curcumin on the other hand, inhibited IL-1β-mediated NF-kB activation in MDA-MB-231 and MCF-7 as proposed. However, MCF-7 and UACC-3199 responded to curcumin by increased VEGF secretion, and SK-BR-3 exhibited a higher IL-1β-mediated and IL-1β-independent NF-kB activation when curcumin was added.
Consistent with our data for the triple negative MDA-MB-231 cell line, a decreased expression of VEGF by curcumin has been reported in-vitro [29] as well as curcumin caused decreased angiogenesis in a xenotransplant model [65,66] based on the same cell line. Our data on curcumin toxicity are also consistent with studies published earlier by Shao [29], Liu [67] or Prasad [68]. These authors associated curcumin toxicity and control of VEGF secretion with NF-κB activity [67] or the Wnt/β-catenin pathway [68]. Other studies showed that promoter methylation of DLC1 [69] can be the target of curcumin resulting in growth inhibition. It is also noteworthy that curcumin interacted with estrogen signaling [29] in estrogen receptor expressing MCF-7 cells and curcumin was also able to restore tamoxifen sensitivity [70] in MCF-7 derived tamoxifen resistant cells. In the ER-positive T47-D cell line, curcumin reduced medroxyprogesterone-induced VEGF secretion [30].
To understand the mechanism of curcumin induced VEGF secretion in MCF-7 further, we investigated the signaling events further using inhibitors.
These studies showed that ERK activation was at least partly responsible for curcumin-induced VEGF secretion whereas p38-MAPK was not. That ERK activation is involved in VEGF production has already been shown for M-CSF induced VEGF production in monocytes [71]. Also another small molecule, the oncometabolite succinate was found to induce angiogenesis via ERK-mediated VEGF production [72]. Curcumin has been found to increase phosphorylation of MAP-kinases by inactivating protein phosphatases 2A and -5 [73] thereby leading to cell death in sarcoma and colon adenocarcinoma. As we observed an increase in MAPK-phosphorylation in the same concentration range, accompanied by decreasing cell viability, the curcumin-increased secretion of VEGF in MCF-7 cells might be a side effect of the same mechanisms. Nevertheless, further studies are needed to understand the different responses of the other breast cancer cell lines in detail. One difference might be the increased activity of STAT3 in TNBC and ER-negative breast cancer, which is a known target for curcumin [74,75]. However, it is not clear to what extend such cell based studies can indeed predict in-vivo effects.
A major drawback for the application of curcumin for therapy is its insufficient oral bioavailability; thus curcumin serum concentration might not exceed 1 µM after oral administration of even large amounts. However, new developments with improved bioavailability based i.e., on nano-emulsions, have the potential to achieve significantly higher curcumin serum levels [76,77]. In light of this improved bioavailability, we assume that testing curcumin in cell cultures at significantly higher concentrations than 1 µM can yield meaningful data. Our data suggest that TNBC patients might benefit from the curcumin-induced cell death and decreased VEGF secretion. Whereas, in luminal A tumors, represented by MCF-7, insufficient concentrations of curcumin might have adverse effects due to possibly increased tumor vascularization. To answer such questions additional clinical or animal studies are needed [78,79,80].
The most intriguing characteristic of curcumin is that it has been attributed to many effects ranging from inhibition of proliferation and inflammation to the modulation of cholesterol homeostasis. This seems quite intriguing, but in fact, several of these data could be misleading. Curcumin is usually not used as a pure substance and it is metabolized in cell cultures, however, to a different degree. Indeed, some researchers consider curcumin therefore a PAIN (panassays interfering compound) and an IMPS (invalid metabolic panaceas) [81]. Often, curcumin effects are observed near to toxic concentrations. We here identified curcumin effects at low concentrations where only limited cell death occurred. Although we could attribute the increased VEGF secretion in the MCF-7 cell line to ERK-phosphorylation, further studies are needed to understand this effect at the molecular level.
Under hypoxia, all cell-lines responded well by VEGF-secretion. This was accompanied by changes in HIF1A mRNA. Although HIF-1α activation is a post-transcriptional process, the mRNA of HIF1A was down-regulated under hypoxia in the four cell lines tested (Figure S3) suggesting an inhibitory feed-back loop.
We further investigated mRNA datasets for correlation of VEGF expression in breast cancer with IL-1β and HIF1α. Although protein abundance and modifications are more important for these pathways, mRNA expression often follows function because activation of signaling proteins regularly induce to higher turnover. We therefore reasoned that analyzing mRNA abundance could lead to meaningful results. Indeed in the METABRIC study, TNBC had the highest VEGFA as well as IL1B mRNA levels. However, there was no relevant correlation between VEGFA and IL1B RNA. In contrast to simply comparing averaged expression values, a correlation analysis investigates paired patient data and is therefore more indicative. This result holds against a direct regulatory interrelationship between VEGF and IL1B in tumors. In the breast cancer cell lines however, VEGFA correlated well with IL1B and this suggests that IL1B is more important for VEGFA under optimal normoxic in vitro conditions than in tumors, which are embedded in a supporting microenvironment. Altogether, these data suggest that in vitro, the VEGFA regulation via IL1B and NF-κB is more important than in patients’ tumors. On the other hand, a strong correlation between IL1B and HIF1A, present in both datasets, demonstrated a cross talk between the two pathways.
In conclusion, we observed significant variation in response to IL-1β and curcumin in only a small set of breast cancer cell lines. Especially curcumin had opposing effects on VEGF secretion although it caused cell death in all four cell lines within the same concentration range. Gene expression data from tumors suggest that VEGFA regulation is complex and involves an interplay of at least the two pathways NF-κB and HIF. These observations suggest that the outcome of a therapy approach based on curcumin as well as on α-IL-1β antibodies will vary within the breast cancer subtypes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Relative VEGF in serum-free medium after 24h with and without IL-1β; Table S1: VEGF mRNA expression in breast cancer cell lines; Figure S2: Breast cancer cell lines clustered according to gene expression of VEGFA, HIF1A and IL1B; Figure S3: HIF1A mRNA abundance in breast cancer cell lines under hypoxia.
Author Contributions
Conceptualization, N.N., A.I. and T.K.; methodology, N.N and T.K.; formal analysis, N.N.; investigation, N.N. and A.I; resources, A.I. and T.K. data curation, N.N and A.I.; writing—original draft preparation, N.N.; writing—review and editing, N.N., A.I. and T.K.; visualization, N.N.; supervision, T.K.; project administration, N.N. and T.K.; funding acquisition, T.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Deutsche Forschungsgemeinschaft (DFG) grant number (KA2663/3-1). TK and NN are currently supported by the Ministry of Science, Research and Cultural Affairs of the State of Brandenburg. The APC was funded by vouchers to N.N.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Otto von Guericke University, Medical Faculty (AKZ 114/13, 2013).
Informed Consent Statement
Patient consent was waived due to the sole use of residual material of diagnostic purposes according to the statement of the German Central Ethics Commission (Deutsches Ärzteblatt 100, 23, 2003).
Data Availability Statement
All necessary data are included into the manuscript and the supplements. Further details will be made available upon reasonable request.
Acknowledgments
The authors are grateful for excellent technical assistance by Mrs. Kerstin Werner and Martina Stoklasek as well as the members of the Magdeburg Institute of Pathology Histochemistry Laboratory.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wilkinson, L.; Gathani, T. Understanding Breast Cancer as a Global Health Concern. Br. J. Radiol. 2022, 95, 20211033. [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular Portraits of Human Breast Tumours. Nature 2000, 406, 747–752. [CrossRef]
- Goldhirsch, A.; Wood, W.C.; Coates, A.S.; Gelber, R.D.; Thürlimann, B.; Senn, H.-J.; Panel members Strategies for Subtypes--Dealing with the Diversity of Breast Cancer: Highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2011, 22, 1736–1747. [CrossRef]
- Duffy, M.J.; Harbeck, N.; Nap, M.; Molina, R.; Nicolini, A.; Senkus, E.; Cardoso, F. Clinical Use of Biomarkers in Breast Cancer: Updated Guidelines from the European Group on Tumor Markers (EGTM). Eur. J. Cancer Oxf. Engl. 1990 2017, 75, 284–298. [CrossRef]
- Anders, C.K.; Abramson, V.; Tan, T.; Dent, R. The Evolution of Triple-Negative Breast Cancer: From Biology to Novel Therapeutics. Am. Soc. Clin. Oncol. Educ. Book Am. Soc. Clin. Oncol. Meet. 2016, 35, 34–42. [CrossRef]
- Rakha, E.A.; Green, A.R. Molecular Classification of Breast Cancer: What the Pathologist Needs to Know. Pathology (Phila.) 2017, 49, 111–119. [CrossRef]
- Kuroda, H.; Muroi, N.; Hayashi, M.; Harada, O.; Hoshi, K.; Fukuma, E.; Abe, A.; Kubota, K.; Imai, Y. Oestrogen Receptor-Negative/Progesterone Receptor-Positive Phenotype of Invasive Breast Carcinoma in Japan: Re-Evaluated Using Immunohistochemical Staining. Breast Cancer Tokyo Jpn. 2018. [CrossRef]
- Miller, W.R. Aromatase and the Breast: Regulation and Clinical Aspects. Maturitas 2006, 54, 335–341. [CrossRef]
- Buus, R.; Sestak, I.; Kronenwett, R.; Denkert, C.; Dubsky, P.; Krappmann, K.; Scheer, M.; Petry, C.; Cuzick, J.; Dowsett, M. Comparison of EndoPredict and EPclin With Oncotype DX Recurrence Score for Prediction of Risk of Distant Recurrence After Endocrine Therapy. J. Natl. Cancer Inst. 2016, 108. [CrossRef]
- Martin, M.; Brase, J.C.; Ruiz, A.; Prat, A.; Kronenwett, R.; Calvo, L.; Petry, C.; Bernard, P.S.; Ruiz-Borrego, M.; Weber, K.E.; et al. Prognostic Ability of EndoPredict Compared to Research-Based Versions of the PAM50 Risk of Recurrence (ROR) Scores in Node-Positive, Estrogen Receptor-Positive, and HER2-Negative Breast Cancer. A GEICAM/9906 Sub-Study. Breast Cancer Res. Treat. 2016, 156, 81–89. [CrossRef]
- Buza, N. The Rapidly Evolving Landscape of Human Epidermal Growth Factor Receptor 2 (HER2) Testing in Endometrial Carcinoma and Other Gynecologic Malignancies. Arch. Pathol. Lab. Med. 2025. [CrossRef]
- Metzger-Filho, O.; Tutt, A.; de Azambuja, E.; Saini, K.S.; Viale, G.; Loi, S.; Bradbury, I.; Bliss, J.M.; Azim, H.A.; Ellis, P.; et al. Dissecting the Heterogeneity of Triple-Negative Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1879–1887. [CrossRef]
- Hennigs, A.; Riedel, F.; Gondos, A.; Sinn, P.; Schirmacher, P.; Marmé, F.; Jäger, D.; Kauczor, H.-U.; Stieber, A.; Lindel, K.; et al. Prognosis of Breast Cancer Molecular Subtypes in Routine Clinical Care: A Large Prospective Cohort Study. BMC Cancer 2016, 16, 734. [CrossRef]
- Singh, K.; Yadav, D.; Jain, M.; Singh, P.K.; Jin, J.-O. Immunotherapy for Breast Cancer Treatment: Current Evidence and Therapeutic Options. Endocr. Metab. Immune Disord. Drug Targets 2022, 22, 212–224. [CrossRef]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-Infiltrating Lymphocytes and Prognosis in Different Subtypes of Breast Cancer: A Pooled Analysis of 3771 Patients Treated with Neoadjuvant Therapy. Lancet Oncol. 2018, 19, 40–50. [CrossRef]
- Santos, R.P.C.; Benvenuti, T.T.; Honda, S.T.; Valle, P.R.; Katayama, M.L.H.; Brentani, H.P.; Carraro, D.M.; Rozenchan, P.B.; Brentani, M.M.; Lyra, E.C.; et al. Influence of the Interaction between Nodal Fibroblast and Breast Cancer Cells on Gene Expression. Tumor Biol. 2010, 32, 145–157. [CrossRef]
- Wan, S.; Liu, Y.; Weng, Y.; Wang, W.; Ren, W.; Fei, C.; Chen, Y.; Zhang, Z.; Wang, T.; Wang, J.; et al. BMP9 Regulates Cross-Talk between Breast Cancer Cells and Bone Marrow-Derived Mesenchymal Stem Cells. Cell. Oncol. Dordr. 2014, 37, 363–375. [CrossRef]
- Zhou, J.; Tulotta, C.; Ottewell, P.D. IL-1β in Breast Cancer Bone Metastasis. Expert Rev. Mol. Med. 2022, 24, e11. [CrossRef]
- Kalinski, T.; Sel, S.; Hütten, H.; Röpke, M.; Roessner, A.; Nass, N. Curcumin Blocks Interleukin-1 Signaling in Chondrosarcoma Cells. PloS One 2014, 9, e99296. [CrossRef]
- Kalinski, T.; Krueger, S.; Sel, S.; Werner, K.; Ropke, M.; Roessner, A. Differential Expression of VEGF-A and Angiopoietins in Cartilage Tumors and Regulation by Interleukin-1beta. Cancer 2006, 106, 2028–2038. [CrossRef]
- Voronov, E.; Shouval, D.S.; Krelin, Y.; Cagnano, E.; Benharroch, D.; Iwakura, Y.; Dinarello, C.A.; Apte, R.N. IL-1 Is Required for Tumor Invasiveness and Angiogenesis. Proc. Natl. Acad. Sci. U. S. A. 2003, 100, 2645–2650. [CrossRef]
- Aalders, K.C.; Tryfonidis, K.; Senkus, E.; Cardoso, F. Anti-Angiogenic Treatment in Breast Cancer: Facts, Successes, Failures and Future Perspectives. Cancer Treat. Rev. 2017, 53, 98–110. [CrossRef]
- Patel, S.A.; Hassan, M.K.; Naik, M.; Mohapatra, N.; Balan, P.; Korrapati, P.S.; Dixit, M. EEF1A2 Promotes HIF1A Mediated Breast Cancer Angiogenesis in Normoxia and Participates in a Positive Feedback Loop with HIF1A in Hypoxia. Br. J. Cancer 2024, 130, 184–200. [CrossRef]
- Kunnumakkara, A.B.; Bordoloi, D.; Padmavathi, G.; Monisha, J.; Roy, N.K.; Prasad, S.; Aggarwal, B.B. Curcumin, the Golden Nutraceutical: Multitargeting for Multiple Chronic Diseases. Br. J. Pharmacol. 2016. [CrossRef]
- Jha, A.; Mohapatra, P.P.; AlHarbi, S.A.; Jahan, N. Curcumin: Not So Spicy After All. Mini Rev. Med. Chem. 2017. [CrossRef]
- Peschel, D.; Koerting, R.; Nass, N. Curcumin Induces Changes in Expression of Genes Involved in Cholesterol Homeostasis. J. Nutr. Biochem. 2007, 18, 113–119. [CrossRef]
- Jurrmann, N.; Brigelius-Flohé, R.; Böl, G.-F. Curcumin Blocks Interleukin-1 (IL-1) Signaling by Inhibiting the Recruitment of the IL-1 Receptor-Associated Kinase IRAK in Murine Thymoma EL-4 Cells. J. Nutr. 2005, 135, 1859–1864.
- Fu, Z.; Chen, X.; Guan, S.; Yan, Y.; Lin, H.; Hua, Z.-C. Curcumin Inhibits Angiogenesis and Improves Defective Hematopoiesis Induced by Tumor-Derived VEGF in Tumor Model through Modulating VEGF-VEGFR2 Signaling Pathway. Oncotarget 2015, 6, 19469–19482. [CrossRef]
- Shao, Z.-M.; Shen, Z.-Z.; Liu, C.-H.; Sartippour, M.R.; Go, V.L.; Heber, D.; Nguyen, M. Curcumin Exerts Multiple Suppressive Effects on Human Breast Carcinoma Cells. Int. J. Cancer 2002, 98, 234–240.
- Carroll, C.E.; Ellersieck, M.R.; Hyder, S.M. Curcumin Inhibits MPA-Induced Secretion of VEGF from T47-D Human Breast Cancer Cells. Menopause N. Y. N 2008, 15, 570–574. [CrossRef]
- Curtis, C.; Shah, S.P.; Chin, S.-F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The Genomic and Transcriptomic Architecture of 2,000 Breast Tumours Reveals Novel Subgroups. Nature 2012, 486, 346–352. [CrossRef]
- Barretina, J.; Caponigro, G.; Stransky, N.; Venkatesan, K.; Margolin, A.A.; Kim, S.; Wilson, C.J.; Lehár, J.; Kryukov, G.V.; Sonkin, D.; et al. The Cancer Cell Line Encyclopedia Enables Predictive Modelling of Anticancer Drug Sensitivity. Nature 2012, 483, 603–607. [CrossRef]
- Nass, N.; Brömme, H.-J.; Hartig, R.; Korkmaz, S.; Sel, S.; Hirche, F.; Ward, A.; Simm, A.; Wiemann, S.; Lykkesfeldt, A.E.; et al. Differential Response to α-Oxoaldehydes in Tamoxifen Resistant MCF-7 Breast Cancer Cells. PloS One 2014, 9, e101473. [CrossRef]
- Ruhs, S.; Nass, N.; Somoza, V.; Friess, U.; Schinzel, R.; Silber, R.-E.; Simm, A. Maillard Reaction Products Enriched Food Extract Reduce the Expression of Myofibroblast Phenotype Markers. Mol. Nutr. Food Res. 2007, 51, 488–495. [CrossRef]
- Ignatov, A.; Ignatov, T.; Weissenborn, C.; Eggemann, H.; Bischoff, J.; Semczuk, A.; Roessner, A.; Costa, S.D.; Kalinski, T. G-Protein-Coupled Estrogen Receptor GPR30 and Tamoxifen Resistance in Breast Cancer. Breast Cancer Res. Treat. 2011, 128, 457–466. [CrossRef]
- Remmele, W.; Hildebrand, U.; Hienz, H.A.; Klein, P.J.; Vierbuchen, M.; Behnken, L.J.; Heicke, B.; Scheidt, E. Comparative Histological, Histochemical, Immunohistochemical and Biochemical Studies on Oestrogen Receptors, Lectin Receptors, and Barr Bodies in Human Breast Cancer. Virchows Arch. A Pathol. Anat. Histopathol. 1986, 409, 127–147.
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative Analysis of Complex Cancer Genomics and Clinical Profiles Using the cBioPortal. Sci. Signal. 2013, 6, pl1. [CrossRef]
- Weinstein, J.N.; Myers, T.G.; O’Connor, P.M.; Friend, S.H.; Fornace, A.J.; Kohn, K.W.; Fojo, T.; Bates, S.E.; Rubinstein, L.V.; Anderson, N.L.; et al. An Information-Intensive Approach to the Molecular Pharmacology of Cancer. Science 1997, 275, 343–349.
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A Software Environment for Integrated Models of Biomolecular Interaction Networks. Genome Res. 2003, 13, 2498–2504. [CrossRef]
- Reinecke, P.; Kalinski, T.; Mahotka, C.; Schmitz, M.; Déjosez, M.; Gabbert, H.E.; Gerharz, C.D. Paclitaxel/Taxol Sensitivity in Human Renal Cell Carcinoma Is Not Determined by the P53 Status. Cancer Lett. 2005, 222, 165–171. [CrossRef]
- Nass, N.; Walter, S; Jechorek, D; Weissenborn, C; Ignatov, A.; Haybaeck, J; Kalinski, T. High Neuronatin (NNAT) Expression Is Associated with Poor Outcome in Breast Cancer. Virchows Arch. 2017, 471(1), 23–30.
- Nass, N.; Ignatov, A.; Andreas, L.; Weißenborn, C.; Kalinski, T.; Sel, S. Accumulation of the Advanced Glycation End Product Carboxymethyl Lysine in Breast Cancer Is Positively Associated with Estrogen Receptor Expression and Unfavorable Prognosis in Estrogen Receptor-Negative Cases. Histochem. Cell Biol. 2016. [CrossRef]
- Scheifele, C.; Zhu, Q.; Ignatov, A.; Kalinski, T.; Nass, N. Glyoxalase 1 Expression Analysis by Immunohistochemistry in Breast Cancer. Pathol. Res. Pract. 2020, 216, 153257. [CrossRef]
- Czapiewski, P.; Cornelius, M.; Hartig, R.; Kalinski, T.; Haybaeck, J.; Dittmer, A.; Dittmer, J.; Ignatov, A.; Nass, N. BCL3 Expression Is Strongly Associated with the Occurrence of Breast Cancer Relapse under Tamoxifen Treatment in a Retrospective Cohort Study. Virchows Arch. Int. J. Pathol. 2022, 480, 529–541. [CrossRef]
- Győrffy, B. Integrated Analysis of Public Datasets for the Discovery and Validation of Survival-Associated Genes in Solid Tumors. Innov. Camb. Mass 2024, 5, 100625. [CrossRef]
- Cuenda, A.; Rouse, J.; Doza, Y.N.; Meier, R.; Cohen, P.; Gallagher, T.F.; Young, P.R.; Lee, J.C. SB 203580 Is a Specific Inhibitor of a MAP Kinase Homologue Which Is Stimulated by Cellular Stresses and Interleukin-1. FEBS Lett. 1995, 364, 229–233.
- Favata, M.F.; Horiuchi, K.Y.; Manos, E.J.; Daulerio, A.J.; Stradley, D.A.; Feeser, W.S.; Van Dyk, D.E.; Pitts, W.J.; Earl, R.A.; Hobbs, F.; et al. Identification of a Novel Inhibitor of Mitogen-Activated Protein Kinase Kinase. J. Biol. Chem. 1998, 273, 18623–18632.
- Nass, N.; Sel, S.; Ignatov, A.; Roessner, A.; Kalinski, T. Oxidative Stress and Glyoxalase-1 Activity Mediate Dicarbonyl Toxicity in MCF-7 Mamma Carcinoma Cells and a Tamoxifen Resistant Derivative. Biochim. Biophys. Acta 2016. [CrossRef]
- Gasparini, G.; Toi, M.; Gion, M.; Verderio, P.; Dittadi, R.; Hanatani, M.; Matsubara, I.; Vinante, O.; Bonoldi, E.; Boracchi, P.; et al. Prognostic Significance of Vascular Endothelial Growth Factor Protein in Node-Negative Breast Carcinoma. J. Natl. Cancer Inst. 1997, 89, 139–147.
- Ludovini, V.; Sidoni, A.; Pistola, L.; Bellezza, G.; Angelis, V.D.; Gori, S.; Mosconi, A.M.; Bisagni, G.; Cherubini, R.; Bian, A.R.; et al. Evaluation of the Prognostic Role of Vascular Endothelial Growth Factor and Microvessel Density in Stages I and II Breast Cancer Patients. Breast Cancer Res. Treat. 2003, 81, 159–168. [CrossRef]
- Sukumar, J.; Gast, K.; Quiroga, D.; Lustberg, M.; Williams, N. Triple-Negative Breast Cancer: Promising Prognostic Biomarkers Currently in Development. Expert Rev. Anticancer Ther. 2021, 21, 135–148. [CrossRef]
- Zhang, M.; Liu, J.; Liu, G.; Xing, Z.; Jia, Z.; Li, J.; Wang, W.; Wang, J.; Qin, L.; Wang, X.; et al. Anti-Vascular Endothelial Growth Factor Therapy in Breast Cancer: Molecular Pathway, Potential Targets, and Current Treatment Strategies. Cancer Lett. 2021, 520, 422–433. [CrossRef]
- Ayoub, N.M.; Jaradat, S.K.; Al-Shami, K.M.; Alkhalifa, A.E. Targeting Angiogenesis in Breast Cancer: Current Evidence and Future Perspectives of Novel Anti-Angiogenic Approaches. Front. Pharmacol. 2022, 13. [CrossRef]
- Miller, K.; Wang, M.; Gralow, J.; Dickler, M.; Cobleigh, M.; Perez, E.A.; Shenkier, T.; Cella, D.; Davidson, N.E. Paclitaxel plus Bevacizumab versus Paclitaxel Alone for Metastatic Breast Cancer. N. Engl. J. Med. 2007, 357, 2666–2676. [CrossRef]
- Bell, R.; Brown, J.; Parmar, M.; Toi, M.; Suter, T.; Steger, G.G.; Pivot, X.; Mackey, J.; Jackisch, C.; Dent, R.; et al. Final Efficacy and Updated Safety Results of the Randomized Phase III BEATRICE Trial Evaluating Adjuvant Bevacizumab-Containing Therapy in Triple-Negative Early Breast Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016. [CrossRef]
- Chen, M.; Huang, R.; Rong, Q.; Yang, W.; Shen, X.; Sun, Q.; Shu, D.; Jiang, K.; Xue, C.; Peng, J.; et al. Bevacizumab, Tislelizumab and Nab-Paclitaxel for Previously Untreated Metastatic Triple-Negative Breast Cancer: A Phase II Trial. J. Immunother. Cancer 2025, 13, e011314. [CrossRef]
- Huang, D.; Li, C.; Zhang, H. Hypoxia and Cancer Cell Metabolism. Acta Biochim. Biophys. Sin. 2014, 46, 214–219. [CrossRef]
- Carmi, Y.; Voronov, E.; Dotan, S.; Lahat, N.; Rahat, M.A.; Fogel, M.; Huszar, M.; White, M.R.; Dinarello, C.A.; Apte, R.N. The Role of Macrophage-Derived IL-1 in Induction and Maintenance of Angiogenesis. J. Immunol. Baltim. Md 1950 2009, 183, 4705–4714. [CrossRef]
- Carmi, Y.; Dotan, S.; Rider, P.; Kaplanov, I.; White, M.R.; Baron, R.; Abutbul, S.; Huszar, M.; Dinarello, C.A.; Apte, R.N.; et al. The Role of IL-1β in the Early Tumor Cell–Induced Angiogenic Response. J. Immunol. 2013, 190, 3500–3509. [CrossRef]
- Jeon, M.; Han, J.; Nam, S.J.; Lee, J.E.; Kim, S. Elevated IL-1β Expression Induces Invasiveness of Triple Negative Breast Cancer Cells and Is Suppressed by Zerumbone. Chem. Biol. Interact. 2016, 258, 126–133. [CrossRef]
- Holen, I.; Lefley, D.V.; Francis, S.E.; Rennicks, S.; Bradbury, S.; Coleman, R.E.; Ottewell, P. IL-1 Drives Breast Cancer Growth and Bone Metastasis in Vivo. Oncotarget 2016, 7, 75571–75584. [CrossRef]
- Tulotta, C.; Lefley, D.V.; Moore, C.K.; Amariutei, A.E.; Spicer-Hadlington, A.R.; Quayle, L.A.; Hughes, R.O.; Ahmed, K.; Cookson, V.; Evans, C.A.; et al. IL-1B Drives Opposing Responses in Primary Tumours and Bone Metastases; Harnessing Combination Therapies to Improve Outcome in Breast Cancer. NPJ Breast Cancer 2021, 7, 95. [CrossRef]
- Zajac, M.; Moneo, M.V.; Carnero, A.; Benitez, J.; Martínez-Delgado, B. Mitotic Catastrophe Cell Death Induced by Heat Shock Protein 90 Inhibitor in BRCA1-Deficient Breast Cancer Cell Lines. Mol. Cancer Ther. 2008, 7, 2358–2366. [CrossRef]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of Human Triple-Negative Breast Cancer Subtypes and Preclinical Models for Selection of Targeted Therapies. J. Clin. Invest. 2011, 121, 2750–2767. [CrossRef]
- Bimonte, S.; Barbieri, A.; Palma, G.; Rea, D.; Luciano, A.; D’Aiuto, M.; Arra, C.; Izzo, F. Dissecting the Role of Curcumin in Tumour Growth and Angiogenesis in Mouse Model of Human Breast Cancer. BioMed Res. Int. 2015, 2015, 878134. [CrossRef]
- Ferreira, L.C.; Arbab, A.S.; Jardim-Perassi, B.V.; Borin, T.F.; Varma, N.R.S.; Iskander, A.S.M.; Shankar, A.; Ali, M.M.; Zuccari, D.A.P. de C. Effect of Curcumin on Pro-Angiogenic Factors in the Xenograft Model of Breast Cancer. Anticancer Agents Med. Chem. 2015, 15, 1285–1296.
- Liu, Q.; Loo, W.T.Y.; Sze, S.C.W.; Tong, Y. Curcumin Inhibits Cell Proliferation of MDA-MB-231 and BT-483 Breast Cancer Cells Mediated by down-Regulation of NFkappaB, cyclinD and MMP-1 Transcription. Phytomedicine Int. J. Phytother. Phytopharm. 2009, 16, 916–922. [CrossRef]
- Prasad, C.P.; Rath, G.; Mathur, S.; Bhatnagar, D.; Ralhan, R. Potent Growth Suppressive Activity of Curcumin in Human Breast Cancer Cells: Modulation of Wnt/Beta-Catenin Signaling. Chem. Biol. Interact. 2009, 181, 263–271. [CrossRef]
- Liu, Y.; Zhou, J.; Hu, Y.; Wang, J.; Yuan, C. Curcumin Inhibits Growth of Human Breast Cancer Cells through Demethylation of DLC1 Promoter. Mol. Cell. Biochem. 2017, 425, 47–58. [CrossRef]
- Jiang, M.; Huang, O.; Zhang, X.; Xie, Z.; Shen, A.; Liu, H.; Geng, M.; Shen, K. Curcumin Induces Cell Death and Restores Tamoxifen Sensitivity in the Antiestrogen-Resistant Breast Cancer Cell Lines MCF-7/LCC2 and MCF-7/LCC9. Mol. Basel Switz. 2013, 18, 701–720. [CrossRef]
- Curry, J.M.; Eubank, T.D.; Roberts, R.D.; Wang, Y.; Pore, N.; Maity, A.; Marsh, C.B. M-CSF Signals through the MAPK/ERK Pathway via Sp1 to Induce VEGF Production and Induces Angiogenesis in Vivo. PloS One 2008, 3, e3405. [CrossRef]
- Mu, X.; Zhao, T.; Xu, C.; Shi, W.; Geng, B.; Shen, J.; Zhang, C.; Pan, J.; Yang, J.; Hu, S.; et al. Oncometabolite Succinate Promotes Angiogenesis by Upregulating VEGF Expression through GPR91-Mediated STAT3 and ERK Activation. Oncotarget 2017. [CrossRef]
- Han, X.; Xu, B.; Beevers, C.S.; Odaka, Y.; Chen, L.; Liu, L.; Luo, Y.; Zhou, H.; Chen, W.; Shen, T.; et al. Curcumin Inhibits Protein Phosphatases 2A and 5, Leading to Activation of Mitogen-Activated Protein Kinases and Death in Tumor Cells. Carcinogenesis 2012, 33, 868–875. [CrossRef]
- Banik, U.; Parasuraman, S.; Adhikary, A.K.; Othman, N.H. Curcumin: The Spicy Modulator of Breast Carcinogenesis. J. Exp. Clin. Cancer Res. CR 2017, 36, 98. [CrossRef]
- Banerjee, K.; Resat, H. Constitutive Activation of STAT3 in Breast Cancer Cells: A Review. Int. J. Cancer 2016, 138, 2570–2578. [CrossRef]
- Rahimi, H.R.; Nedaeinia, R.; Sepehri Shamloo, A.; Nikdoust, S.; Kazemi Oskuee, R. Novel Delivery System for Natural Products: Nano-Curcumin Formulations. Avicenna J. Phytomedicine 2016, 6, 383–398.
- Young, N.A.; Bruss, M.S.; Gardner, M.; Willis, W.L.; Mo, X.; Valiente, G.R.; Cao, Y.; Liu, Z.; Jarjour, W.N.; Wu, L.-C. Oral Administration of Nano-Emulsion Curcumin in Mice Suppresses Inflammatory-Induced NFκB Signaling and Macrophage Migration. PloS One 2014, 9, e111559. [CrossRef]
- Bachmeier, B.E.; Killian, P.H.; Melchart, D. The Role of Curcumin in Prevention and Management of Metastatic Disease. Int. J. Mol. Sci. 2018, 19. [CrossRef]
- Kotecha, R.; Takami, A.; Espinoza, J.L. Dietary Phytochemicals and Cancer Chemoprevention: A Review of the Clinical Evidence. Oncotarget 2016, 7, 52517–52529. [CrossRef]
- Fan, X.; Zhang, C.; Liu, D.; Yan, J.; Liang, H. The Clinical Applications of Curcumin: Current State and the Future. Curr. Pharm. Des. 2013, 19, 2011–2031.
- Nelson, K.M.; Dahlin, J.L.; Bisson, J.; Graham, J.; Pauli, G.F.; Walters, M.A. The Essential Medicinal Chemistry of Curcumin. J. Med. Chem. 2017, 60, 1620–1637. [CrossRef]
Figure 1.
A: Secretion of VEGF in response to IL-1β by MCF-7 cells as demonstrated by Western blotting. Cells were inoculated in serum-free medium and the medium sampled, concentrated and analyzed by Western blotting as described in the method section. N109 cell culture supernatant was applied as a positive control. B: VEGF in medium of breast cancer cells incubated for 24 hours with and without IL-1β as determined by ELISA. Average and standard deviation are shown. *: p < 0.05 (ANOVA).
Figure 1.
A: Secretion of VEGF in response to IL-1β by MCF-7 cells as demonstrated by Western blotting. Cells were inoculated in serum-free medium and the medium sampled, concentrated and analyzed by Western blotting as described in the method section. N109 cell culture supernatant was applied as a positive control. B: VEGF in medium of breast cancer cells incubated for 24 hours with and without IL-1β as determined by ELISA. Average and standard deviation are shown. *: p < 0.05 (ANOVA).
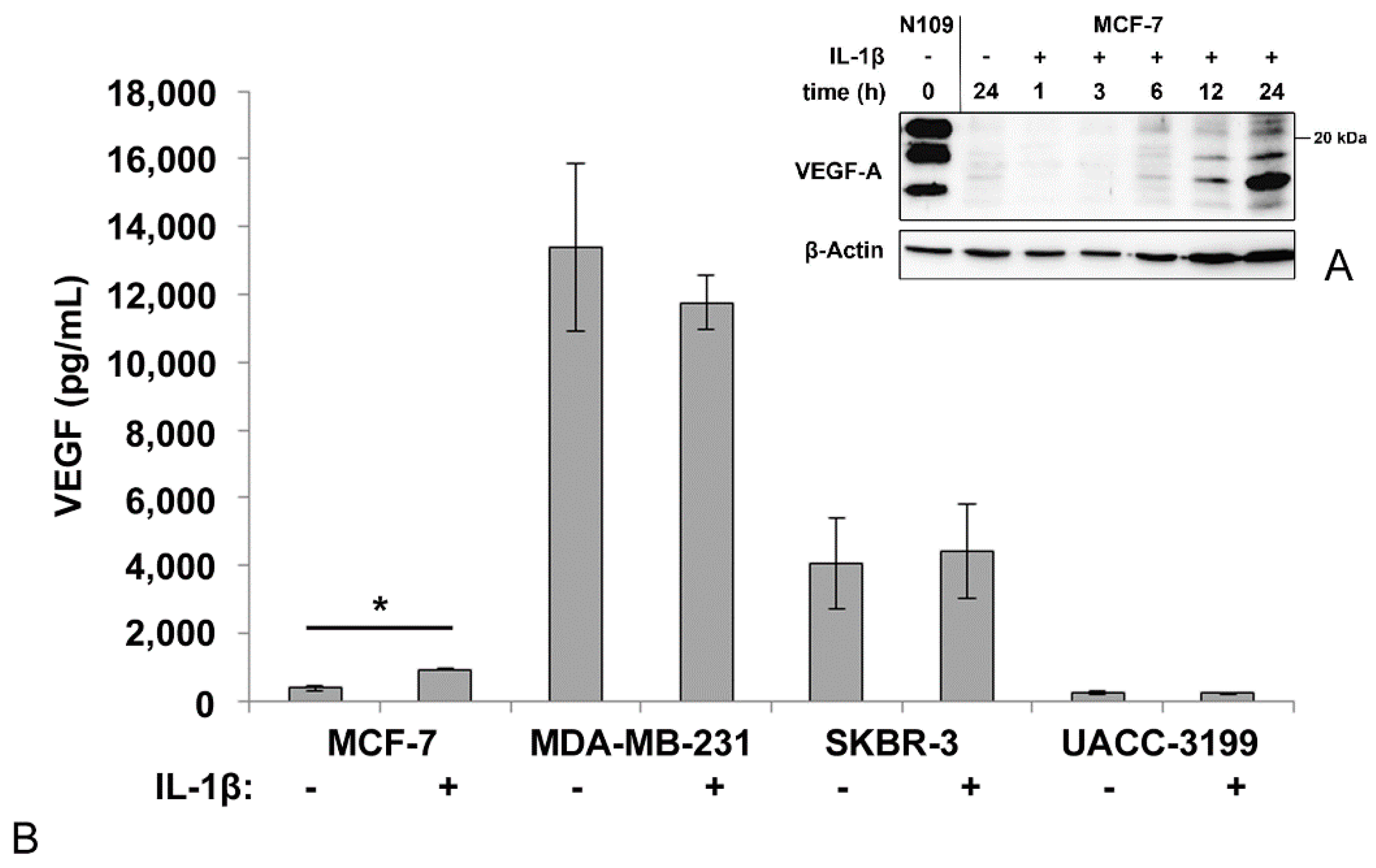
Figure 2.
Immunohistochemical staining of VEGF in breast cancer samples. Weak (A), intermediate (B) and strong staining intensity (C) is shown. Scale bar corresponds to 50 µM.
Figure 2.
Immunohistochemical staining of VEGF in breast cancer samples. Weak (A), intermediate (B) and strong staining intensity (C) is shown. Scale bar corresponds to 50 µM.
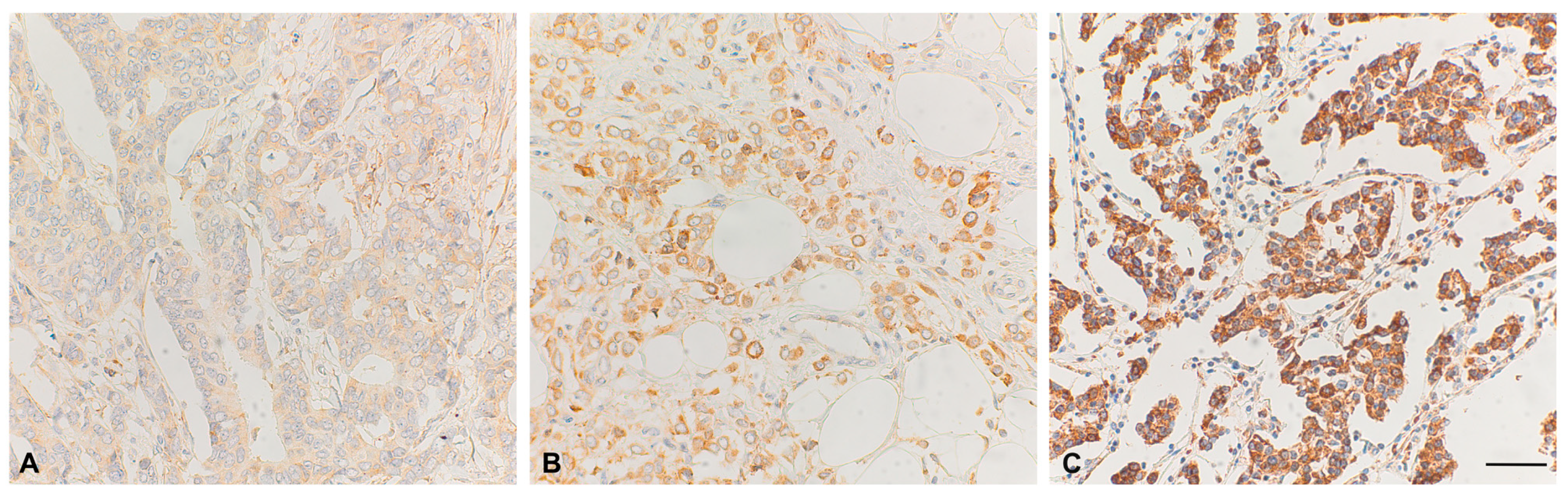
Figure 3.
mRNA expression in breast cancer specimens from the METABRIC study [31] in relation to receptor status. Data were obtained and analyzed using cBioportal [37].
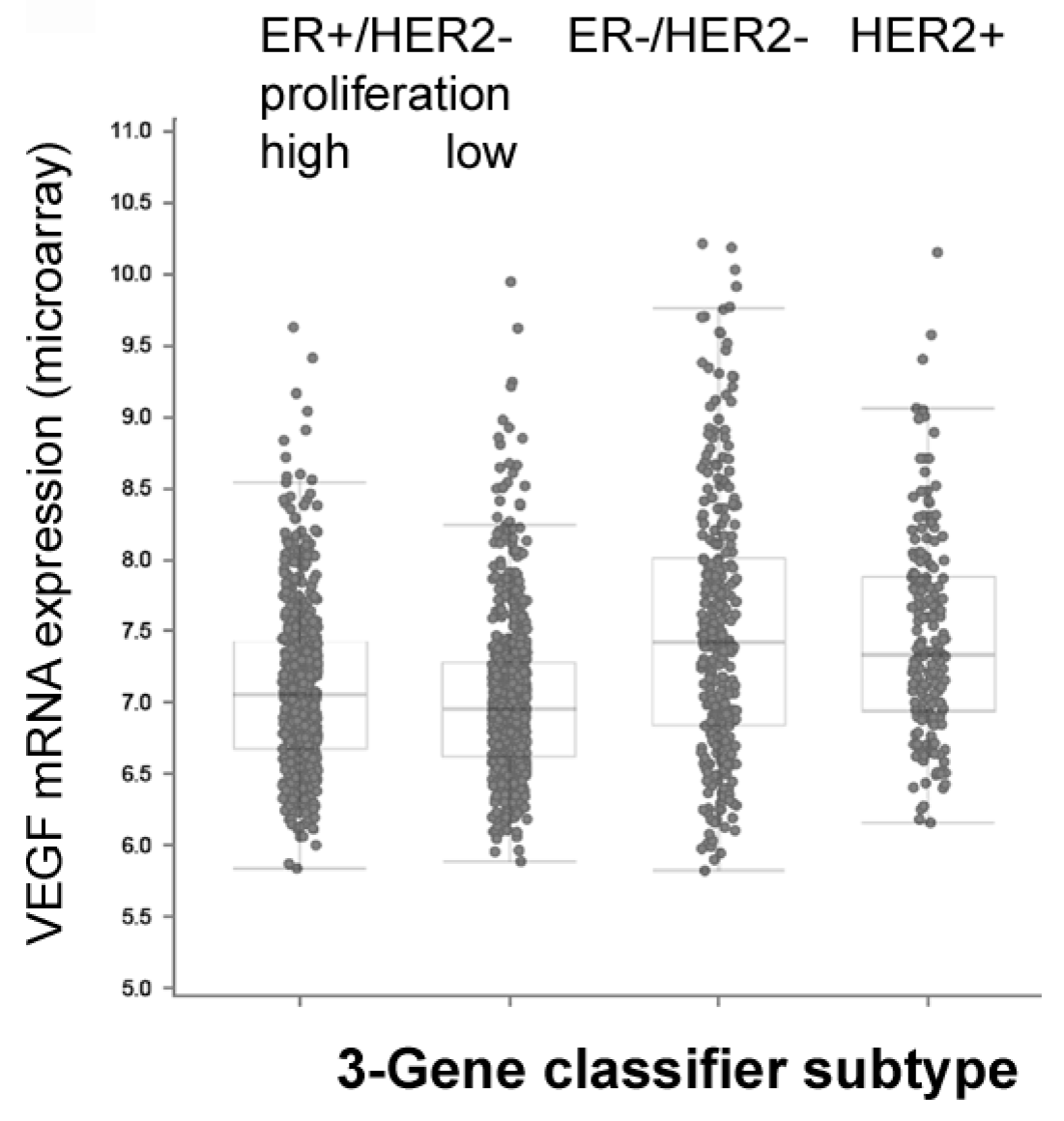
Figure 5.
A. Cell viability of cells exposed with curcumin for 24 hours. Viability was determined by the resazurin assay. Data averaged from three independent experiments. Standard deviation is shown. B. VEGF concentrations in cell culture supernatant upon 24h exposure to IL-1β, curcumin and combinations of both determined by ELISA. Data are averaged from three independent experiments and median and quartiles are shown. *: p < 0.05, ANOVA test. C. Effects of inhibition of MAP-kinases on curcumin-induced VEGF secretion in MCF-7. Data are expressed relative to solvent-treated cells. Data were averaged from three independent experiments and standard deviation is shown. *: p < 0.05, n.s. not significant.
Figure 5.
A. Cell viability of cells exposed with curcumin for 24 hours. Viability was determined by the resazurin assay. Data averaged from three independent experiments. Standard deviation is shown. B. VEGF concentrations in cell culture supernatant upon 24h exposure to IL-1β, curcumin and combinations of both determined by ELISA. Data are averaged from three independent experiments and median and quartiles are shown. *: p < 0.05, ANOVA test. C. Effects of inhibition of MAP-kinases on curcumin-induced VEGF secretion in MCF-7. Data are expressed relative to solvent-treated cells. Data were averaged from three independent experiments and standard deviation is shown. *: p < 0.05, n.s. not significant.
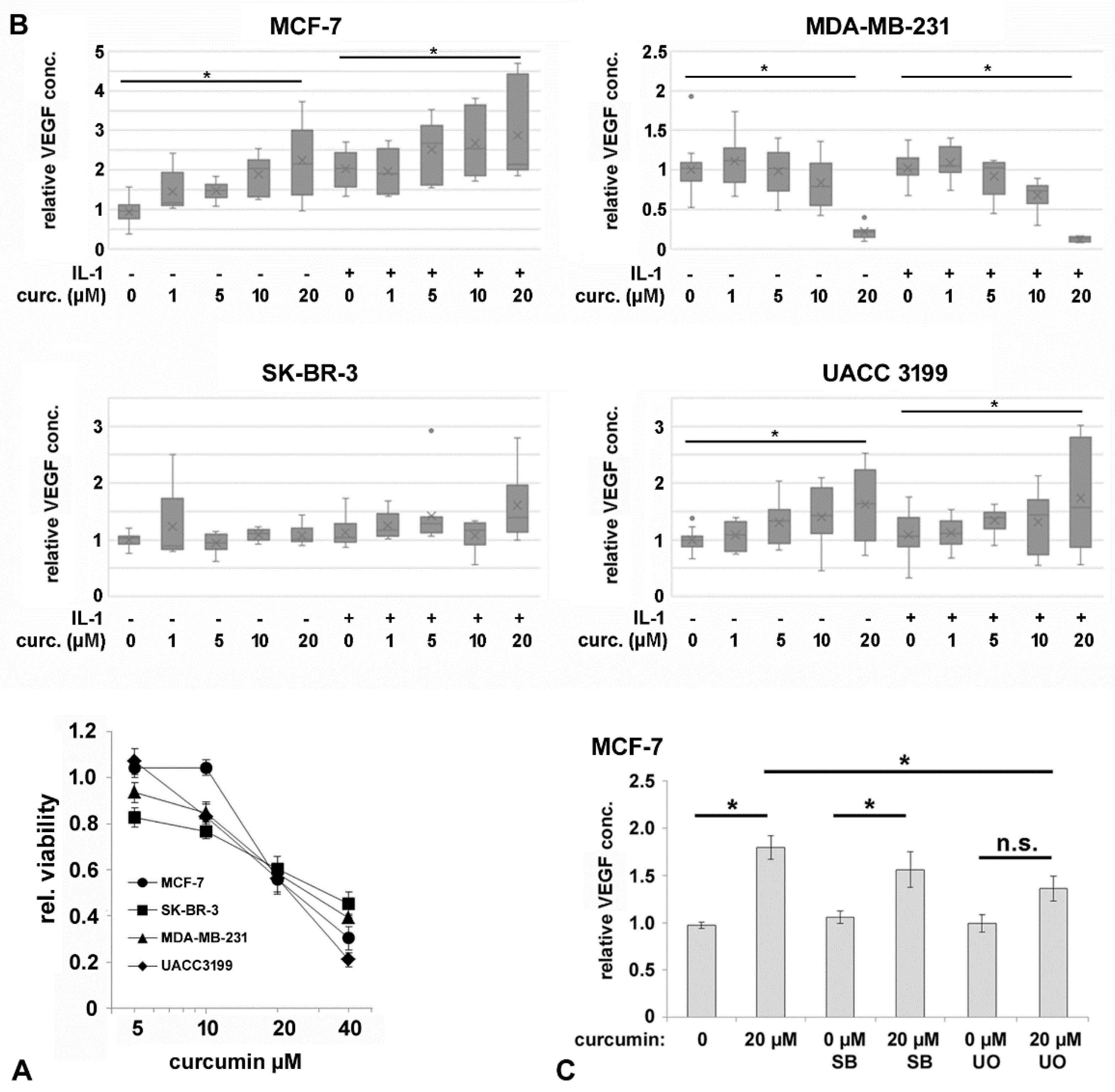
Figure 6.
VEGF secretion in response to hypoxia. Cells were exposed to hypoxic conditions for 24 h and VEGF was determined in the supernatant by ELISA. Data were averaged from three independent experiments, represented as box plots and the median and quartiles are shown. *: p < 0.05, ** p < 0.01 (ANOVA, Tamhane T2 post hoc analysis), °: outliers.
Figure 6.
VEGF secretion in response to hypoxia. Cells were exposed to hypoxic conditions for 24 h and VEGF was determined in the supernatant by ELISA. Data were averaged from three independent experiments, represented as box plots and the median and quartiles are shown. *: p < 0.05, ** p < 0.01 (ANOVA, Tamhane T2 post hoc analysis), °: outliers.
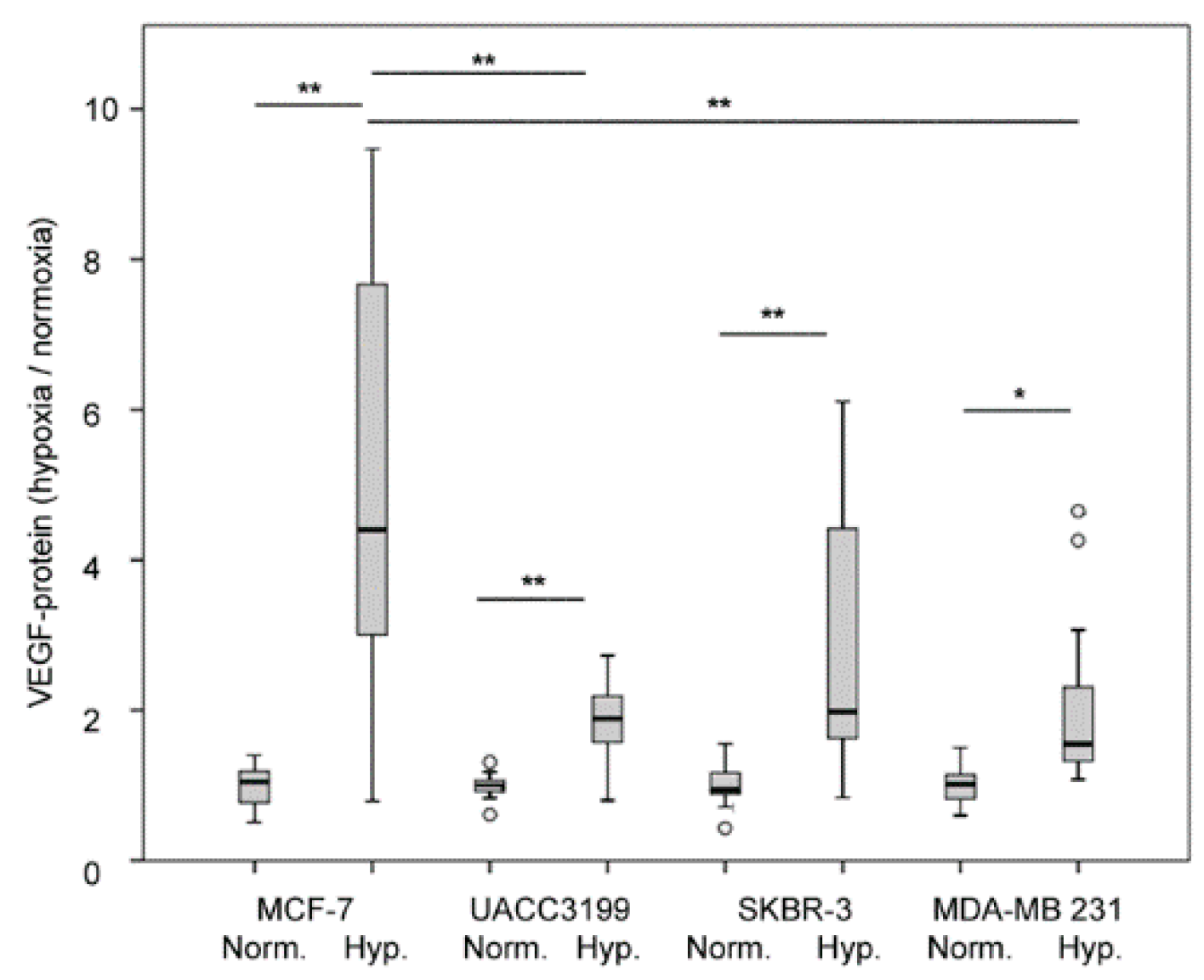

Table 1.
Clinico-pathological parameters and VEGF status. An IRS ≥ 6 was considered as “VEGF high” status. Total numbers may vary since not all parameters were available for every patient. For 2 x 2 contingency tables, Fisher’s exact p is provided; otherwise, significance was calculated using Pearson Chi Square $.
Table 1.
Clinico-pathological parameters and VEGF status. An IRS ≥ 6 was considered as “VEGF high” status. Total numbers may vary since not all parameters were available for every patient. For 2 x 2 contingency tables, Fisher’s exact p is provided; otherwise, significance was calculated using Pearson Chi Square $.
| Parameter | number | VEGF low/high | VEGF high % | p-value |
| All patients | 230 | 122 / 108 | 47.0 % | |
| Histology | ||||
| Ductal | 175 | 85 / 90 | 51.4 % | 0.005 |
| Lobular | 43 | 32 / 11 | 25.6 % | |
| Other | 11 | 4 / 7 | 63.6 % | |
| Menopausal - | 45 | 25 / 20 | 44.4 % | 0.741 |
| Menopausal + | 185 | 97 / 88 | 47.6 % | |
| T < 2 | 117 | 58 / 64 | 54.7 % | 0.294 |
| T ≥ 2 | 113 | 59 / 49 | 43.4 % | |
| Ki67 < 23 | 97 | 50 / 47 | 48.5 % | 0.306 |
| Ki67 ≥ 23 | 52 | 22 / 30 | 57.7 % | |
| N0 | 147 | 80 / 67 | 45.6 % | 0.581 |
| N1 | 82 | 41 / 41 | 50.0 % | |
| G1 | 27 | 14 / 13 | 48.1 % | 0.534 $ |
| G2 | 132 | 74 / 58 | 43.9 % | |
| G3 | 71 | 34 / 37 | 52.1 % | |
| ER - | 46 | 21 / 25 | 54.3 % | 0.322 |
| ER + | 184 | 101 / 83 | 45.1 % | |
| Luminal A | 127 | 74 / 53 | 41.7 % | 0.201 |
| Luminal B | 57 | 27 / 30 | 52.6 % | |
| PR - | 101 | 50 / 51 | 50.5 % | 0.355 |
| PR + | 129 | 72 / 57 | 44.2 % | |
| HER2 - | 182 | 98/ 84 | 46.2 % | 0.745 |
| HER2 + | 48 | 24 / 24 | 50.0 % | |
| No TNBC | 198 | 109 / 89 | 44.9 % | 0.181 |
| TNBC | 32 | 13 / 19 | 59.4 % | |
| No Radiotherapy | 72 | 49 / 23 | 31.9 % | 0.003 |
| Radiotherapy | 158 | 73 / 85 | 53.8 % | |
| No Chemotherapy | 122 | 69 / 53 | 43.4 % | 0.290 |
| Chemotherapy | 108 | 53 / 55 | 50.9 % | |
| No endocrine therapy | 39 | 17 / 22 | 56.4 % | |
| Tamoxifen | 126 | 70 / 56 | 44.4 % | 0.424 |
| Aromatase Inhibitor | 64 | 34 / 30 | 46.9 % | |
| No Tamoxifen relapse |
80 | 43 / 37 | 46.3 % | 0.710 |
| Tamoxifen relapse |
46 | 27 / 19 | 41.3 % |
Table 2.
Comparison of gene expression data from the METABRIC study according to receptor expression. Mean of expression of normalized mRNA abundance (log-scale) of IL-1β, VEGFA and HIFA, in breast cancer subtypes of the METABRIC cohort was calculated and significance determined by one-way ANOVA test.
Table 2.
Comparison of gene expression data from the METABRIC study according to receptor expression. Mean of expression of normalized mRNA abundance (log-scale) of IL-1β, VEGFA and HIFA, in breast cancer subtypes of the METABRIC cohort was calculated and significance determined by one-way ANOVA test.
| BC subtype | Expression levels in METABRIC study (log-scale) Mean ± standard error */ ** One Way ANOVA p < 0.05 / 0.01 |
| VEGF-A | |
| ER -/+ | 7.58 ± 0.04 / 7.07 ± 0.02 ** |
| PR -/+ | 7.36 ± 0.03 / 7.04 ± 0.02 ** |
| HER2 -/+ | 7.16 ± 0.02 / 7.41 ± 0.04 ** |
| TNBC -/+ | 7.11± 0.02 / 7.60± 0.05 ** |
| IL1B | |
| ER -/+ | 6.68 ± 0.03 / 6.54 ± 0.02 ** |
| PR -/+ | 6.59 ± 0.02 / 6.56 ± 0.02 |
| HER2 -/+ | 6.60 ± 0.02 / 6.37 ± 0.04 ** |
| TNBC -/+ | 6.53 ± 0.02 / 6.81 ± 0.04 ** |
| HIF1A | |
| ER -/+ | 7.00 ± 0.03 / 6.57 ± 0.02 ** |
| PR -/+ | 6.79 ± 0.02 / 6.56 ± 0.02 ** |
| HER2 -/+ | 6.62 ± 0.02 / 6.98 ± 0.04 |
| TNBC -/+ | 6.61± 0.02 / 6.97 ± 0.03 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



