Submitted:
18 July 2025
Posted:
21 July 2025
You are already at the latest version
Abstract
Arthroscopy offers numerous benefits in the management of various shoulder conditions. One such condition is acromioclavicular joint separation, which is more commonly seen in young individuals who engage in sports. This injury involves the separation of the clavicle from the acromion, typically due to the rupture of the acromioclavicular and coracoclavicular ligaments. Modern anatomical repair techniques often utilize suspensory fixation devices to reconstruct the coracoclavicular ligaments and, in some cases, address the acromioclavicular joint as well. Arthroscopy provides minimally invasive access to the joint, allowing for comprehensive visualization and treatment of associated intra-articular pathologies, including direct access to the underside of the coracoid process where implants are placed. This approach is achieved with small incisions and minimal disruption to surrounding tissues. Despite its clear advantages, arthroscopy also has drawbacks, such as increased costs due to the advanced technology used and the requirement for specialized surgical expertise. Nevertheless, surgeons trained in shoulder arthroscopy are now able to manage this condition with relative ease and high precision.
Keywords:
acromioclavicular separation
; shoulder
; clavicle
; scapula
; surgery
; arthroscopy
1. Introduction
Modern arthroscopy originated in Japan, pioneered by Kenji Takagi—widely regarded as the father of arthroscopy—and later advanced by his student, Masaki Watanabe [1]. In 1955, Watanabe performed the first documented arthroscopic procedure, which focused on knee pathology [2,3]. From its origins in Japan, arthroscopy quickly gained global adoption. Its application to shoulder conditions was inevitable. The first reported shoulder arthroscopy was performed by Lanny Johnson in 1980 [4]. Initially, this technique was primarily used to treat shoulder instability and subacromial impingement [5]. Over time, the range of shoulder pathologies addressed through arthroscopy expanded. In 1985, Mathews et al. introduced the anterior portal [6], while Eugene Wolfe later emphasized the need for anterosuperior and anteroinferior portals to improve visualization of the anterior glenoid [7].
The first recorded use of arthroscopy to treat acromioclavicular (AC) joint separation occurred in 2001 [8]. Since then, the technique has been increasingly adopted, sometimes in combination with open surgical procedures.
The AC joint is a diarthrodial joint formed by the distal clavicle and the acromion. The acromial surface is concave, while the clavicular surface is convex, allowing for gliding, shearing, and rotational movements. Both articular surfaces are covered in hyaline cartilage, and a fibrocartilaginous disc lies between them—first described by de Palma [9]. With age or as a result of dislocation, this disc can degenerate or be damaged, which may hinder proper clavicle reduction.
The joint is enclosed in a capsule, which is more robust superiorly and often referred to as the AC ligament. The posterior and superior sections of this capsule are critical in preventing anterior and posterior translation of the distal clavicle.
The coracoclavicular (CC) ligaments—composed of the conoid ligament (medial) and the trapezoid ligament (lateral)—anchor the clavicle to the scapula and stabilize the joint. These ligaments cover approximately 15–30% of the distal clavicle. Their clavicular insertions are located roughly 15–16 mm from the lateral end, and together they have a footprint of about 25–26 mm [10,11]. The trapezoid ligament primarily prevents the clavicle from being compressed against the acromion, while the conoid ligament restricts superior and anterior displacement [12,13,14].
From an epidemiological standpoint, AC joint separation accounts for approximately 9% of shoulder injuries, occurring most often in men aged 20 to 40, largely due to participation in high-risk sports [15]. The injury mechanism typically involves a direct blow to the lateral aspect of the shoulder, which transmits force to the distal clavicle and can rupture both the capsule and ligaments. In some cases, AC separation may result from indirect trauma, such as falling with the arm adducted or extended.
Diagnosis is based primarily on physical examination and X-rays. Patients typically report localized pain at the AC joint, which intensifies with cross-body arm movement but improves with local anesthetic infiltration [16]. A visible deformity—elevation of the clavicle—may be present. This deformity can temporarily resolve with downward pressure on the clavicle and return once pressure is released, a phenomenon known as the “piano key sign” (Figure 1).
X-rays can indicate an acromioclavicular (AC) joint separation when the joint space widens beyond 5–8 mm. The most widely used system for classifying this injury is the Rockwood classification, a six-type model based on radiographic views (AP, axillary, and Zanca) that assesses both the direction and extent of clavicular displacement relative to the unaffected shoulder [17].
This classification system is helpful in guiding treatment decisions. Type I and II injuries are typically managed conservatively, while Types IV to VI usually require surgical intervention [18]. Type III injuries remain controversial. The International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) Upper Extremity Committee has proposed a subclassification [19]:
- Type IIIA involves a stable joint and is often treated nonoperatively.
- Type IIIB indicates joint instability and may benefit from surgical management.
Over time, more than 150 surgical techniques have been described, reflecting ongoing debate regarding optimal treatment [20]. Several older methods used for acute injuries (less than 3 weeks old)—such as K-wires, Bosworth screws, or hook plates—have been associated with long-term complications including AC joint arthritis, infection risk, and often require a second surgery for hardware removal [21,22].
In recent years, suspensory fixation devices have emerged as a preferred approach for acute AC separations [23,24]. These systems, which offer anatomical reconstruction and stable fixation without the need for later removal, have become a new standard. Initially performed via open surgery, the technique is now frequently done with arthroscopic assistance, which provides better visualization of the coracoid process and allows for simultaneous treatment of associated glenohumeral pathology.
For chronic AC separations (those older than 3–4 weeks), where the joint and ligament healing capacity is significantly reduced, simple fixation is insufficient. These cases require additional stabilization measures to ensure long-term success.
Various synthetic ligaments are available as alternatives to autografts or allografts, including materials such as carbon fiber, polyethylene terephthalate (e.g., Dacron, LARS), and polytetrafluoroethylene (e.g., Gore-Tex). These synthetic grafts aim not only to restore mechanical stability but also to support biological healing through fibroblast ingrowth [25]. However, the risk of material rejection remains a significant concern in some patients [26].
Despite advancements in synthetic options, autografts and allografts have been shown in numerous studies to outperform synthetic materials, offering both biomechanical strength and biological integration comparable to native coracoclavicular ligaments [27,28,29]. A range of tendons has been used—including tibialis anterior, flexor carpi radialis, palmaris longus, and peroneus longus—but the hamstring tendons (semitendinosus and gracilis) remain the most commonly employed. These grafts are effective in both acute and chronic cases, especially in chronic separations where biological augmentation is critical for healing.
Arthroscopic techniques provide several advantages, including minimal invasiveness, improved intra-articular visualization, and the ability to manage coexisting shoulder pathology effectively.
2. Materials and Methods
The aim of this paper is to present the technique used by the senior author for treating acromioclavicular (AC) joint separations—a method that is both reproducible and accessible to most surgeons with basic skills in shoulder arthroscopy (all surgeries were performed by one surgeon). We believe that the ideal reconstruction approach involves achieving accurate reduction of the displaced clavicle (sometimes requiring AC joint opening to remove a damaged intra-articular disc), followed by arthroscopically assisted reconstruction of the coracoclavicular (CC) ligaments using suspensory fixation devices, with augmentation using autografts or synthetic materials when needed.
Over the past seven years, we have treated 30 cases of AC separation using this arthroscopic technique. The surgery was addressed to the patients with type IV, V, VI dislocation and for athletes with type III dislocation. In rest o situations, the treatment was conservative. During surgeries, in acute cases, suspensory devices alone were used, while in chronic cases, the procedure was augmented with allografts for additional stability.
The procedure is performed under either general or loco-regional anesthesia, with the patient positioned in the beach-chair position (Figure 2a.b). We favor this position because it allows for a rapid conversion to open surgery if complications arise (see Figure 2). A fluoroscopy unit is set up to provide full visualization of the shoulder. Under fluoroscopic guidance, we assess the manual reduction of the AC joint. If the reduction is complete, we proceed with arthroscopy alone. However, if reduction is not possible, we open the AC joint to remove any soft tissue obstructing proper alignment of the clavicle.
After the shoulder is sterilized and draped, key bony landmarks are marked with a sterile skin marker. A small incision (2–3 cm) is made approximately 2–3 cm medial to the lateral end of the clavicle. Using electrocautery, soft tissues are released from the clavicle from anterior to posterior to expose the bone. This exposure facilitates the arthroscopic procedure. In cases where reduction is not possible through closed means, this incision can be extended toward the AC joint for direct access.
The procedure begins with a standard posterior arthroscopic approach to access the shoulder joint. A thorough diagnostic evaluation is then performed to identify any associated pathologies, such as labral tears, cartilage damage, or rotator cuff injuries—which are present in approximately 40% of cases [30]. From the posterior portal, the rotator interval is clearly visualized.
Next, anterosuperior and anteroinferior portals are established using a spinal needle through the rotator interval (Figure 3a). One portal is designated for the arthroscope, and the other for instruments such as the electrocautery device. The anterosuperior portal is typically placed just superior and slightly medial to the biceps tendon within the rotator interval.
For enhanced visualization, especially of the anterior structures, a 70-degree arthroscope can be used, which may allow the entire procedure to be performed through a single working portal.
The inferior surface of the coracoid process is then carefully exposed (skeletonized) using electrocautery (Turbovac) and a 4.5 mm shaver. During this dissection, it is critical to proceed cautiously and avoid extending too far medially, as this could risk injury to the brachial plexus (Figure 3b).
The anterosuperior portal should be placed as laterally as possible to ensure proper access to the inferior border of the coracoid process. Similarly, the posterior portal should be positioned slightly lateral to enable a medial view toward the base of the coracoid. The skin incision must be large enough to accommodate the necessary instruments; however, we have often found the working space to be limited and, for this reason, prefer to avoid routine use of a cannula.
For the next step, we utilize a surgical guide, typically provided by Arthrex. Through the anterosuperior portal, the inferior limb of the guide is placed beneath the coracoid at its junction with the scapular body (commonly referred to as the “knee” of the coracoid), while the superior limb rests over the clavicle, with its cannula positioned centrally on the clavicle at approximately 25 mm from the AC joint (Figure 4).
A thin drill is then passed through both the clavicle and coracoid. It is crucial that the drill exits precisely at the center of the knee of the coracoid (Figure 5a), as improper positioning increases the risk of coracoid fracture [31].
Once the drill trajectory is confirmed satisfactory, a larger cannulated guidewire is inserted over it (Figure 5b). The initial drill is then removed, and a FiberStick (Arthrex) passing suture is advanced through the cannulated guidewire and retrieved through the anterior portal to facilitate placement of the AC fixation device, which includes suture tapes and cortical buttons (Figure 6a).
The Dog Bone Button, or a TightRope device is then passed through the prepared bone tunnels. One cortical button is seated just beneath the coracoid (Figure 6b), while the second button rests on top of the clavicle.
The construct is then tensioned to reduce the clavicle and secured with multiple surgical knots (Figure 7a). Final confirmation of proper reduction is achieved with fluoroscopic imaging using a C-arm X-ray system (Figure 7b).
In cases where the AC separation is older than 3–4 weeks (chronic cases), augmentation with an autograft, allograft, or synthetic material becomes necessary, as the natural healing potential of the joint and ligaments significantly declines over time. We prefer to use autografts, such as the gracilis tendon harvested from the ipsilateral knee or the palmaris longus tendon, ideally from the same side, but some others authographs can be used like plantaris longus tendon.
With the base of the coracoid process visualized arthroscopically, a cannulated guidewire is inserted from the posterior side of the clavicle, exiting at the medial side of the coracoid process. A suture is then passed through the guidewire to serve as a shuttle for graft passage. Next, another cannulated guidewire is inserted from the anterior side of the clavicle, exiting at the lateral side of the coracoid, and the shuttle suture is pulled through.
Following the previously described steps for AC joint stabilization, the graft is attached to the shuttle suture and passed over the clavicle and looped beneath the coracoid process. The two ends of the graft are tensioned, with the longer limb used to reconstruct the superior portion of the AC joint (Figure 8).
If the AC joint has been surgically opened, small drill holes are made through the distal clavicle and acromial process. Sutures are passed through these tunnels and tied securely. The graft can either be threaded through the bone tunnels or simply laid over the AC joint and secured with sutures.
Fluoroscopic imaging is used at the end of the procedure to confirm proper reduction. The deltotrapezial fascia is closed in a longitudinal fashion, and the skin is sutured in layers. Postoperatively, the arm is supported in a sling.
3. Results
Following surgery, patients are permitted to move their arm within shoulder-level range during the first six weeks to allow proper healing of the soft tissues. After this initial phase, they may begin lifting the arm overhead. Sutures are typically removed 10 to 14 days postoperatively.
Postoperative follow-up visits are scheduled for the day after surgery, at two weeks, six weeks, six months, one year and five years. During these appointments, we monitor pain levels, shoulder mobility, and strength. We also assess recovery using standardized scoring systems, such as the Constant and ASES scores.
Rehabilitation begins as early as possible, following the necessary precautions outlined for the initial healing period. An immediate postoperative control X-ray (A-P view) is performed to confirm proper implant placement and reduction.
Once full range of motion is restored, patients can gradually return to their previous athletic activities (Figure 9). Muscle strength usually returns relatively quickly, but lifting heavy objects (over 5 kg) is restricted for several months. High-intensity training is only permitted after six months post-surgery.
In some cases, particularly in lean patients, a small bump may be felt at the clavicle incision site due to the presence of the surgical knot. However, this is typically painless and does not affect shoulder function.
In one case, a fracture of the coracoid process occurred, caused by improper positioning of the button — placed too anteriorly rather than at the base (knee level) of the coracoid. The patient reported no pain, but after several weeks noticed a change in shoulder contour due to elevation of the lateral clavicle. Revision surgery was performed, and the button was correctly repositioned. The tip of the coracoid did not require fixation and did not lead to any further issues. Full shoulder mobility was eventually restored.
In four cases, a loss of reduction was observed. Radiographic imaging confirmed that the buttons remained securely in place, and patients did not report any functional limitations. The cause remains unclear, though it is possible that in the moist internal environment, the fixation wires may have loosened over time.
All patients regained full range of motion, experienced no pain, and returned to their previous activities, including sports such as tennis. Importantly, no infections were reported. The average Constant-Murley score was 95, and the average ASES score was 89. Aside from the patient who sustained a coracoid fracture, no other individual required further surgical intervention.
4. Discussion
As with all shoulder conditions, accurately identifying the type of AC (acromioclavicular) separation is crucial, since various shoulder or clavicle pathologies can mimic its symptoms. A thorough clinical examination is essential and cannot be replaced by imaging alone. X-rays help assess the degree of displacement, with only Rockwood types IV, V, and VI typically requiring surgical intervention. For type III injuries, treatment decisions—whether surgical or non-surgical—should be based on a detailed discussion with the patient, considering their functional demands and expectations.
Once an AC separation is diagnosed, the next step is to choose the most appropriate surgical technique—open or arthroscopic. Arthroscopy has several clear advantages:
- Minimally Invasive Approach: All surgeries cause some tissue damage, but arthroscopy minimizes trauma thanks to advanced instruments that allow internal access with small incisions. This generally leads to faster recovery, less pain, and a lower risk of infection.
- Enhanced Visualization: Arthroscopy magnifies the surgical field up to ten times, providing detailed views of the joint. This allows simultaneous diagnosis and treatment of associated injuries, such as ligament tears, labral damage, or rotator cuff pathology.
Precise placement of the fixation device is critical. In arthroscopy, the guide wire can be positioned accurately at the “knee” of the coracoid process—its strongest part—reducing the risk of fracture and ensuring stable reduction. In contrast, open surgery typically relies on tactile feedback, which can be less precise. However, arthroscopic treatment of AC separation has its challenges. It requires advanced surgical skills and should not be performed by inexperienced surgeons. Proper training and sufficient practice are essential. Surgeons must also be cautious to avoid injuring the brachial plexus or musculocutaneous nerve, especially when dissecting tissue near the coracoid [31]. Overly aggressive soft tissue removal can damage the conjoint tendon, leading to functional deficits and potential nerve injury. Adequate—but conservative—debridement ensures clear visualization without harming critical structures.
Another risk is clavicle fracture during insertion of the guide wire for the cannulated drill [32]. To minimize this, the wire must be centered in the bone, at the knee of coracoid process. Surgeons typically mark the correct spot at the beginning of the procedure through a small incision, ensuring the wire is neither too anterior nor posterior.
Arthroscopy has limitations. For instance, if the coracoid process is fractured, an alternative surgical method may be necessary. One often-overlooked issue is knot protrusion under the skin, particularly in thin patients. To address this, knotless systems—such as those developed by Arthrex—have been introduced to improve patient comfort and cosmetic outcomes.
In acute AC dislocations, simply reducing the clavicle and stabilizing it with suspensory devices like the TightRope or Dog Bone button is usually sufficient. In chronic cases, where natural healing has already occurred, additional augmentation with autografts, allografts, or synthetic materials is necessary to ensure stability.
Sometimes, damaged AC joint cartilage can obstruct reduction. If this is suspected, a preoperative reduction attempt under fluoroscopy can help guide the surgical plan. If the clavicle is easily reduced, the surgeon may proceed with the implant without opening the joint. If not, the joint must be surgically accessed and debrided. Reconstructing the AC ligament is also crucial to prevent anterior-posterior instability of the clavicle.
Overall, arthroscopic AC joint reconstruction is considered less invasive and often yields superior results when performed in a well-equipped facility by skilled surgeons. This approach allows full joint evaluation and management of coexisting pathologies. Suspensory devices offer biomechanical advantages, often outperforming other implants in anatomical accuracy and strength. In chronic separations, augmentation with autografts—particularly gracilis tendon, but also palmaris longus, or plantaris longus can be used—has shown reliable outcomes.
In the postoperative period, patients are required to protect the surgical repair for the first six weeks by limiting shoulder movement. Resumption of sports or physically demanding activities is generally advised after six months. Four patients experienced loosening of the fixation, and one patient sustained a coracoid process fracture. This complication was attributed to incorrect placement of the inferior button. The patient underwent revision surgery, during which the button was repositioned successfully, leading to favorable outcomes. All patients ultimately regained full shoulder range of motion and returned to their previous levels of activity, including sports like tennis.
Compared to open surgery, the arthroscopic approach involves smaller incisions and enables precise placement of the button beneath the coracoid process—an area that is accessed blindly during open procedures. This improved accuracy contributes to better tissue healing and a more efficient recovery process.
In the arthroscopic treatment of acromioclavicular (AC) joint dislocation, both synthetic neoligaments and autografts have been employed to restore joint stability. Clinical outcomes suggest that synthetic neoligaments offer shorter operative times and avoid donor-site morbidity, while providing immediate mechanical stability. However, concerns remain regarding long-term biocompatibility and the potential for foreign body reaction.
In contrast, autografts—typically harvested from the hamstring or other plases—demonstrate superior biological integration and long-term durability, though they are associated with longer surgical time and increased postoperative pain due to graft harvesting.
Studies indicate comparable functional outcomes in terms of range of motion and return to sports. However, autografts may show better long-term anatomical stability and lower rates of graft elongation or failure, particularly in high-demand patients. Ultimately, graft choice should be tailored to the patient’s activity level, surgical risk profile, and long-term expectations.
5. Conclusions
AC joint separation is particularly challenging for surgeons because it typically occurs in young, active individuals with high functional demands on their shoulders. In cases of type III displacement, according to the Rockwood classification, surgical intervention is generally reserved for specific cases, such as athletes. For more severe displacements (types IV to VI), surgery is typically the preferred treatment.
Over the years, many surgical techniques have been developed, but the best outcomes are usually achieved by closely restoring the joint’s normal anatomy. This is often done using suspensory fixation systems like the TightRope or Dog Bone button, sometimes reinforced with autografts, allografts, or synthetic ligaments when needed.
The procedure can be performed through an open or arthroscopic approach. Arthroscopy offers several benefits, including improved visualization of the underside of the coracoid process, which helps ensure accurate placement of the inferior fixation device and reduces the risk of fractures. Additionally, it enables simultaneous treatment of any other shoulder pathologies, requires only a small incision, and is associated with fewer complications and better cosmetic results.
The surgery should be carried out by a surgeon experienced in shoulder arthroscopy and performed in a facility with appropriate equipment. Anesthesia is a common concern among patients, particularly general anesthesia, though regional anesthesia is a viable alternative. Most complications can be avoided by strictly adhering to the surgical protocol.
When the procedure is done correctly, outcomes are generally excellent. Patients typically regain shoulder mobility and strength within a few weeks post-surgery. However, the first six weeks are critical for protecting the shoulder and allowing initial healing. Return to high-intensity sports should be delayed until at least six months after the operation.
Patient compliance is key to successful recovery. Following the surgeon’s recommendations and promptly starting a rehabilitation program are essential for restoring shoulder function.
Author Contributions
Conceptualization, M.T.G. and V.C.; methodology, M.T.G.; validation, C.S.; formal analysis, V.C.; investigation, M.T.G.; resources, M.T.G.; data curation, V.C.; writing— original draft preparation, M.T.G.; writing—review and editing, M.T.G.; visualization, M.T.G..; supervision, C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not necessary.
Data Availability Statement
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Takagi, K. The arthroscope. J Jpn Orthop Assoc. 1933, 8, 132. [Google Scholar] [CrossRef]
- Watanabe M, Takeda S. The number 21 arthroscope. J Jpn Orthop Assoc. 1960, 34, 1041. [Google Scholar]
- Watanabe M, Takeda S, Iqeuchi H. Tokyo: Atlas of Arthroscopy. Igaku Shoin Ltd.
- Johnson, LL. Arthroscopy of the shoulder. Orthop Clin North Am. 1980, 11, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Ellman, H. Arthroscopic subacromial decompression. Orthop Translat. 1985, 9, 8. [Google Scholar]
- Matthews LS, Zarins B, Michael RH, Helfet DL. Anterior portal selection for shoulder arthroscopy. Arthroscopy. 1985, 1, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, EM. Anterior portals in shoulder arthroscopy. Arthroscopy. 1989, 5, 201–208. [Google Scholar] [CrossRef] [PubMed]
- E M Wolf, W T Pennington Arthroscopic reconstruction for acromioclavicular joint dislocation Arthroscopy 2001 May;17,558-63. [CrossRef]
- DePalma, AF. Biologic aging of the shoulder. In: DePalma AF, editor. Surgery of the Shoulder. Philadelphia: J.B. Lippincott Co. 1983: 235-240.
- Stine IA, Vangsness CT Jr. Analysis of the capsule and ligament insertions about the acromioclavicular joint: a cadaveric study. Arthroscopy. 2009, 25, 968–974. [CrossRef]
- Renfree KJ, Wright TW. Anatomy and biomechanics of the acromioclavicular and sternoclavicular joints. Clin Sports Med. 2003;22 (2):219–237. [CrossRef]
- Klimkiewicz JJ, Williams GR, Sher JS, Karduna A, Des Jardins J, Iannotti JP. The acromioclavicular capsule as a restraint to posterior translation of the clavicle: a biomechanical analysis. J Shoulder Elbow Surg. 1999, 8, 119–124. [CrossRef]
- Chahla J, Marchetti DC, Moatshe G, et al. Quantitative assessment of the coracoacromial and the coracoclavicular ligaments with 3-dimensional mapping of the coracoid process anatomy: a cadaveric study of surgically relevant structures. Arthroscopy. 2018, 34, 1403–1411. [CrossRef]
- Fukuda K, Craig EV, An K, et al. Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg [AM]. 1986, 68, 434–440.
- Chillemi C, Franceschini V, Dei Giudici L, et al. Epidemiology of isolated acromioclavicular joint dislocation. Emerg Med Int. 2013, 2013, 171609. [CrossRef]
- Johansen JA, Grutter PW, McFarland EG, Petersen SA. Acromioclavicular joint injuries: indications for treatment and treatment options. J Shoulder Elbow Surg. 2011, 20, S70–S82. [CrossRef]
- Rockwood CAJ. Fractures and Dislocations of the Shoulder. Philadelphia (PA): Lippincott; 1984.
- Marincek, Borut; Dondelinger, Robert F. (2007). Emergency Radiology: Imaging and Intervention. Springer Science & Business Media. p. 255. ISBN 9783540689089.
- Beitzel K, Mazzocca AD, Bak K, et al. ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014, 30, 271–278. [CrossRef]
- Kay, J. , Memon M. , Alolabi B. Return to sport and clinical outcomes after surgical management of acromioclavicular joint dislocation: A systematic review. Arthroscopy. 2018, 34, 2910–2924.e1. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya E, Arikan Y, Beng K, Mutlu H, Yalcinkaya M, Uzumcugil O. Bosworth and modified Phemister techniques revisited. A comparison of intraarticular vs extraarticular fixation methods in the treatment of acute Rockwood type III acromioclavicular dislocations. Acta Orthop Traumatol Turc. 2017, 51, 455–458. [CrossRef]
- Broos P, Stoffelen D, Van de Sijpe K, Fourneau I. Surgical management of complete Tossy III acromioclavicular joint dislocation with the Bosworth screw or the Wolter plate. A critical evaluation. Unfallchirurgie. 1997, 23, 153–159. [CrossRef]
- John Hayden Sonnier, Bryson Kemler, Carlo Coladonato, Ryan W Paul, Fotios P Tjoumakaris, Kevin B Freedman. Surgical management of acute, high-grade acromioclavicular joint separations: a systematic review, JSES Rev Rep Tech. 2022 Oct 29, 3, 10–20. [CrossRef]
- Ayyappan V. Nair D.Ortho., D.N.B., M.N.A.M.S, Bharath Bharadwaj M S M.S. Ortho, D.N.B. Ortho , Sreejith Thampy J M.S. Ortho, Maythilisharan Rambhojun M.S. Ortho, Aravind Rajan M.S. Ortho, D.N.B. Ortho, Kiran V M.S. Ortho, M.R.C.S. (Edinburgh), Prince Shanavas Khan D.Ortho, M.S. Ortho, Arthroscopic Acromioclavicular Joint Fixation in Acute High-Grade Injuries Using a Single Button Over the Clavicle and a FiberTape With Modified Cinch Loop Through the Coracoid With Acromioclavicular Reduction Using a Hohmann Retractor. [CrossRef]
- Tiefenboeck TM, Boesmueller S, Popp D, et al. The use of the LARS system in the treatment of AC joint instability—Long-term results after a mean of 7.4 years. Orthop Traumatol Surg Res. 2018, 104, 749–754. [CrossRef]
- Sinagra ZP, Kop A, Pabbruwe M, Parry J, Clark G. Foreign body reaction associated with artificial LARS ligaments: a retrieval study. Orthop J Sports Med. 2018, 6, 2325967118811604. [CrossRef]
- Fauci F, Merolla G, Paladini P, Campi F, Porcellini G. Surgical treatment of chronic acromioclavicular dislocation with biologic graft vs synthetic ligament: a prospective randomized comparative study. J Orthop Traumatol. 2013, 14, 283–290. [CrossRef]
- Lee SJ, Keefer EP, McHugh MP, et al. Cyclical loading of coracoclavicular ligament reconstructions: a comparative biomechanical study. Am J Sports Med. 2008, 36, 1990–1997. [CrossRef]
- Baran S, Belisle JG, Granger EK, Tashjian RZ. Functional and radiographic outcomes after allograft anatomic coracoclavicular ligament reconstruction. J Orthop Trauma. 2018, 32, 204–210. [CrossRef]
- Markel, J. , Schwarting T. , Malcherczyk D., Peterlein C.D., Ruchholtz S., El-Zayat B.F. Concomitant glenohumeral pathologies in high-grade acromioclavicular separation (type III-V) BMC Musculoskelet Disord. 2017, 18, 439. [Google Scholar] [CrossRef]
- Banaszek D, Pickell M, Wilson E, et al. Anatomical evaluation of the proximity of neurovascular structures during arthroscopically assisted acromioclavicular joint reconstruction: A cadaveric pilot study. Arthroscopy 2017, 33, 75–81.
- Martetschlager F, Horan MP, Warth RJ, Millett PJ. Complications after anatomic fixation and reconstruction of the coracoclavicular ligaments. Am J Sports Med. 2013, 41, 2896–2903. [CrossRef]
Figure 1.
a) Clinical aspect and b) X-ray image of left AC separation.
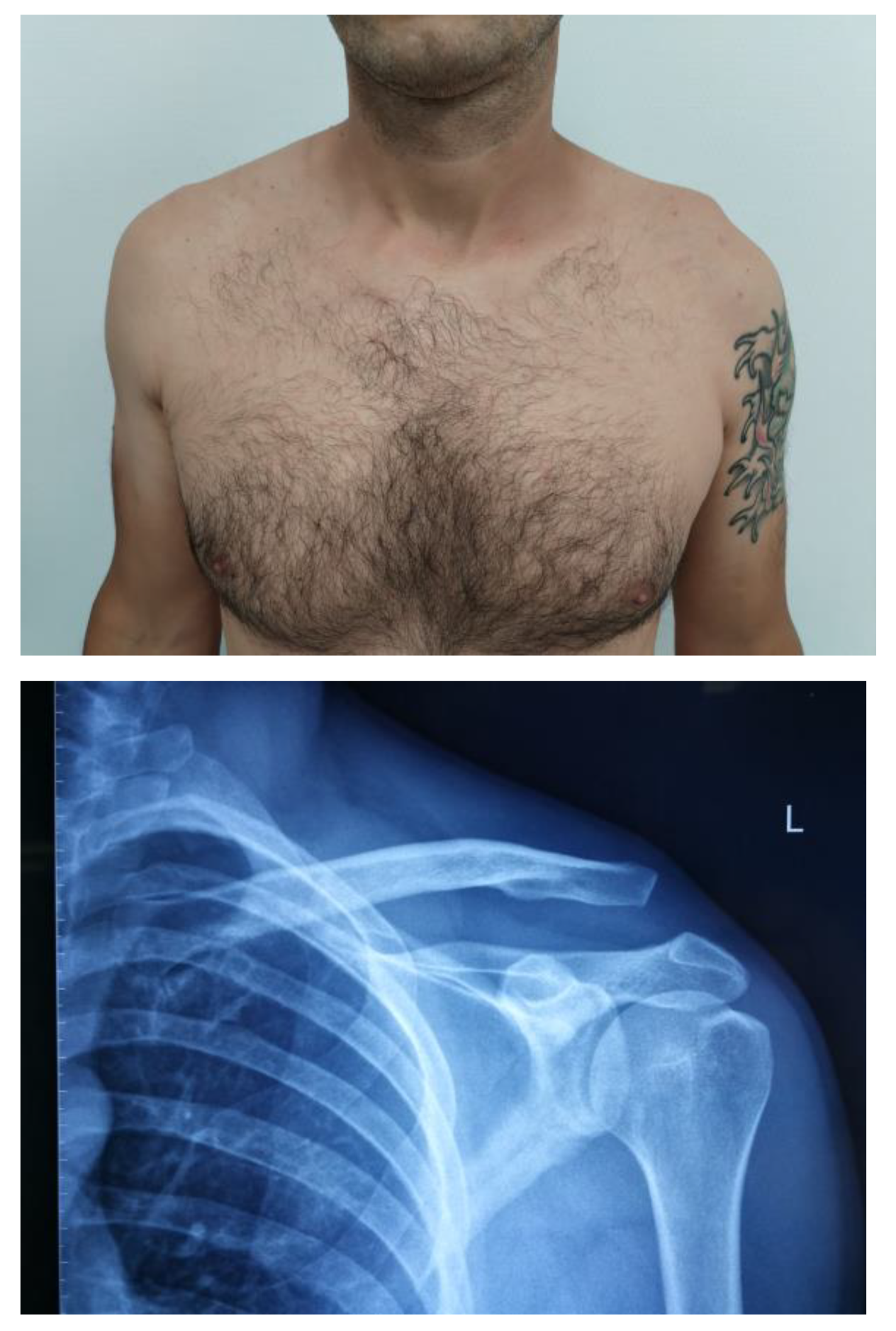
Figure 2.
Beach-chair position of the patient during arthroscopic AC repair with bony landmark drawn a) anterior, b) posterior.
Figure 2.
Beach-chair position of the patient during arthroscopic AC repair with bony landmark drawn a) anterior, b) posterior.

Figure 3.
a) anterosuperior postal, b) skeletonization of the inferior part of coracoid process.

Figure 4.
a) position of the Arthrex guide with superior limb over the clavicle and b) inferior limb under coracoid process.
Figure 4.
a) position of the Arthrex guide with superior limb over the clavicle and b) inferior limb under coracoid process.
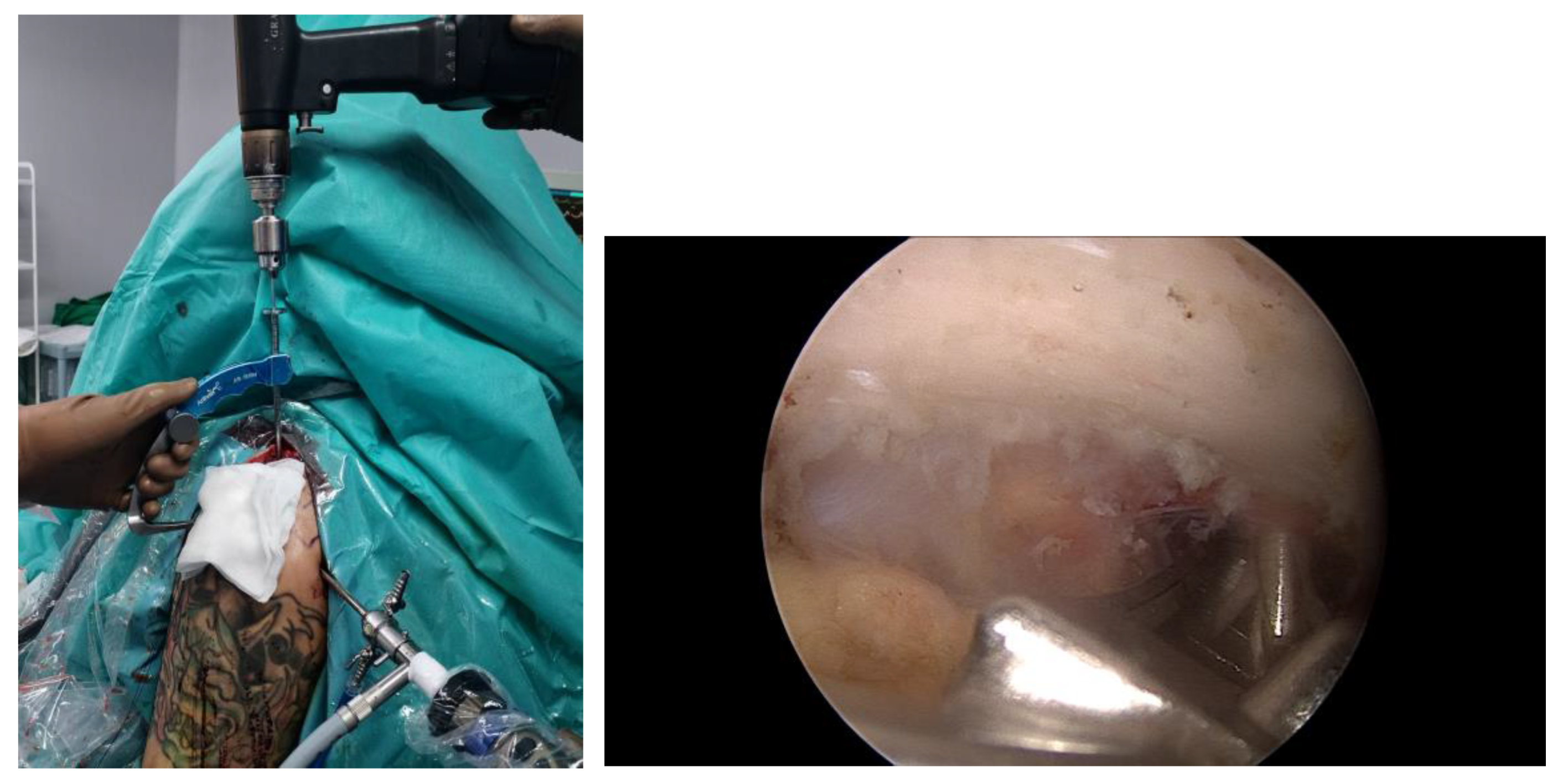
Figure 5.
a) The drill exits in the center of the knee of the coracoid; b) The large cannulated guide is inserted over it.
Figure 5.
a) The drill exits in the center of the knee of the coracoid; b) The large cannulated guide is inserted over it.
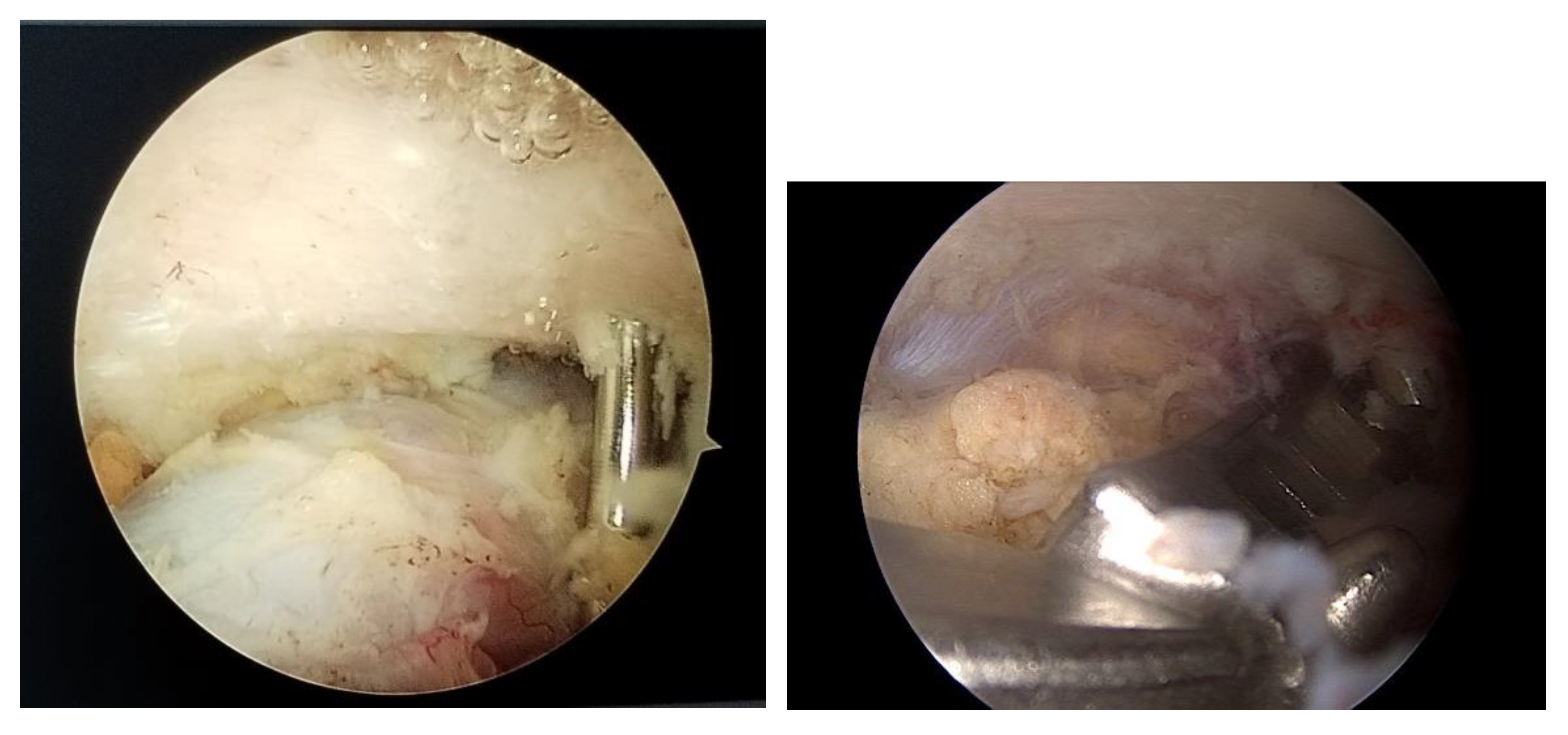
Figure 6.
a) A passing suture is advanced through the cannulated guidewire; b) position of inferior button under coracoid cortical.
Figure 6.
a) A passing suture is advanced through the cannulated guidewire; b) position of inferior button under coracoid cortical.
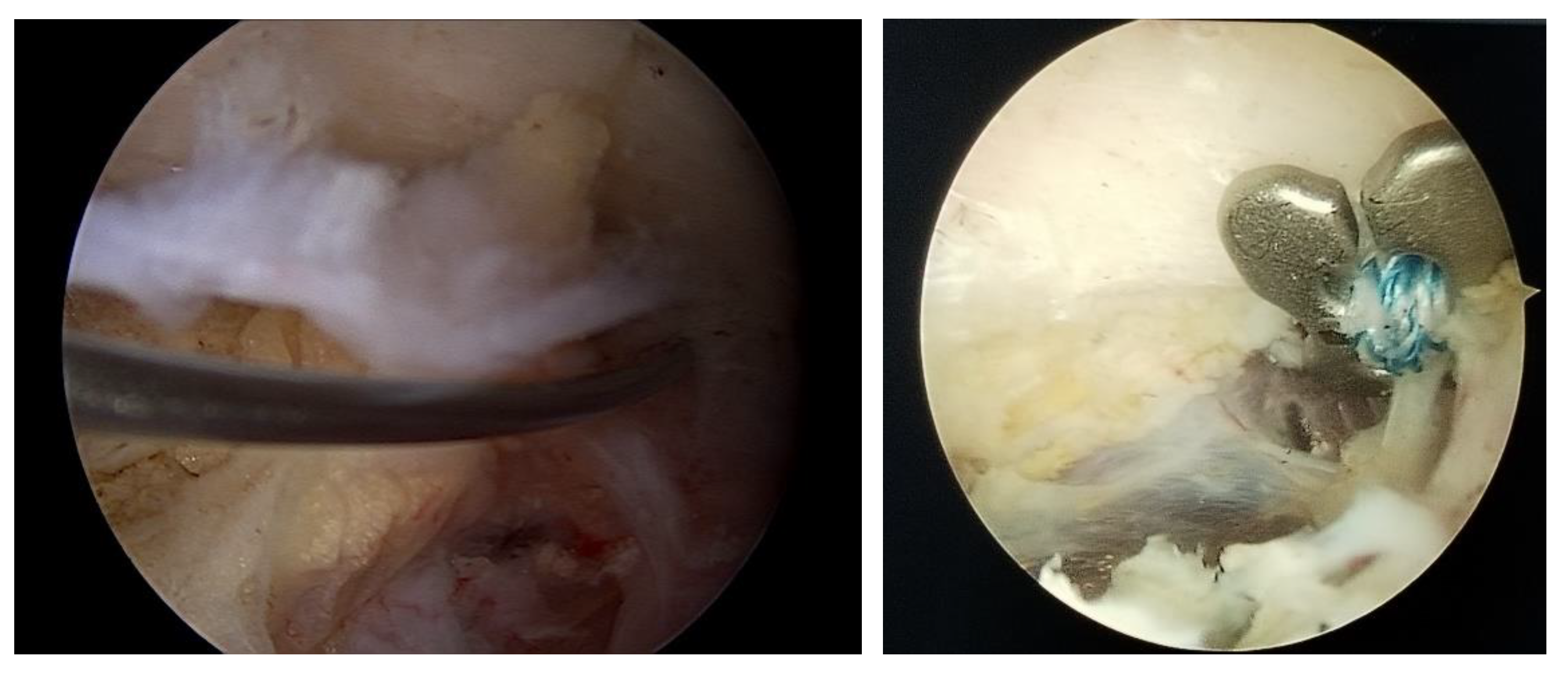
Figure 7.
a) superior button over the clavicle; b) final fluoroscopic imaging.

Figure 8.
For chronic cases it is used autographt from gracilis to reconstruct CC and AC ligaments.

Figure 9.
Clinical aspect after 6 weeks from surgery.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



