Submitted:
15 July 2025
Posted:
17 July 2025
You are already at the latest version
Abstract
Cytomegalovirus (CMV) represents the most prevalent cause of congenital viral infection in newborns and the leading non-genetic etiology of sensorineural hearing loss (SNHL) in children. Notably, only 10%-15% of congenitally infected infants possibly present with classic clinical symptoms at birth, including Small for gestational age, Microcephaly, Petechiae or purpura, Blueberry muffin rash, Jaundice, Hepatomegaly, Splenomegaly and abnormal neurologic signs. In contrast, approximately 90% of infected neonates exhibit no apparent symptoms initially. Current research predominantly focuses on symptomatic cases due to their severe acute presentations and high rates of long-term sequelae (40%-60%), including SNHL and neurodevelopmental impairments. However, significant controversy persists regarding the management of asymptomatic infants. Emerging evidence reveals that 8%-15% of asymptomatic carriers develop Late-onset Hearing Loss (LOHL) beyond the neonatal period.Additionally 5%-10% may manifest neurodevelopmental abnormalities including mild intellectual disability, learning difficulties, or motor coordination disorders. Crucially, given the substantial population of asymptomatic cCMV cases, these delayed complications account for 30%-40% of all cCMV-related long-term morbidity, underscoring their considerable public health impact. This review synthesizes current evidence and controversies regarding cCMV-related SNHL in asymptomatic or mildly symptomatic children, with a focus on screening, di-agnostic classification, and antiviral management gaps, to heighten clinical awareness of this underrecognized cause of hearing loss.
Keywords:
congenital cytomegalovirus infection
; sensorineural hearing loss
; universal screening
; antiviral therapy
; delayed-onset hearing loss
; valganciclovir
; ganciclovir
1. Introduction
Cytomegalovirus (CMV), a member of the human herpesvirus family, represents the most prevalent viral etiology of congenital infections. The global prevalence of congenital CMV (cCMV) ranges between 0.2% and 2.5%, with higher seroprevalence observed among women, elderly populations, and populations in low-to-middle-income countries. As a leading preventable cause of childhood SNHL and a major non-genetic contributor to severe congenital malformations and neurodevelopmental delays [1,15], cCMV infection manifests clinically detectable symptoms in 10-15% of neonates at birth, while 85%-90% present without discernible clinical findings [23]. Although asymptomatic cases account for the majority of infections, they contribute to 30%–40% of cCMV-related long-term morbidity and still lack standardized management approaches. The 2017 European consensus established diagnostic classifications: asymptomatic denotes absence of CMV-related signs (including Small for gestational age, Microcephaly, Petechiae or purpura, Blueberry muffin rash, Jaundice, Hepatomegaly, Splenomegaly, Microcephaly, Lethargy, Hypotonia, Seizures, or Impaired sucking reflex); mild encompasses isolated (≤2 transient/non-significant) manifestations; moderate involves persistent hematologic/biochemical abnormalities or ≥2 mild features; severe indicates central nervous system involvement or life-threatening conditions. Notably, classification of isolated SNHL remains contentious - most experts at the consensus meeting opposed antiviral treatment for mild isolated presentations due to insufficient RCT evidence supporting therapeutic benefit [6].While symptomatic neonates with overt infection demonstrate clear treatment indications and higher risks of long-term sequelae, which have traditionally driven research efforts, recent investigations have increasingly shifted toward asymptomatic or mildly symptomatic cohorts. This shift acknowledges their substantial population burden: 10-15% develop delayed-onset SNHL [25], 5-10% exhibit neurodevelopmental impairments (intellectual disability, learning deficits, motor dysfunction), and 30-40% ultimately experience chronic complications. Emerging clinical perspectives advocate universal neonatal screening to capture this high-risk population and propose antiviral intervention for isolated SNHL to mitigate sequelae, though these approaches remain debated. This review synthesizes current perspectives on diagnosis, screening, treatment, and follow-up of hearing loss in children with asymptomatic or mild congenital CMV infection, highlighting controversies, critical knowledge gaps, and actionable research priorities to inform management strategies.
2. Epidemiology
Cytomegalovirus (CMV) demonstrates a global birth prevalence of 0.5%–1.3%. Seroprevalence reaches 58%–79% among North American women of childbearing age and ~86% worldwide [13]. Higher seropositivity is observed in females, older populations, and low-to-middle-income countries. The infection affects 1/200 live births in high-income nations compared to 1/71 in resource-limited settings [13]. CMV transmission occurs via vertical, horizontal, and sexual routes [11,12]. Postnatally acquired infections typically result from contact with infected bodily fluids (urine, saliva, semen, cervical secretions, breast milk) or medical procedures solid organ/allogeneic hematopoietic cell transplantation (HCT)), transfusion-mediated transmission is relatively uncommon [5]. Congenital CMV infection primarily stems from maternal vertical transmission during either primary infection (24%–40% fetal transmission risk) or non-primary infection (0.5%–2% transmission risk) [41,61,62]. Definitive diagnosis of congenital CMV requires viral detection within 21 postnatal days [2], as later identification may indicate postnatal acquisition, frequently via breast milk. SNHL develops in 40%–60% of symptomatic and 10%–14% of asymptomatic cCMV-infected infants [63], manifesting unilaterally or bilaterally [64]. Notably, 10%–20% of cCMV-associated SNHL cases present with late-onset, exhibiting threshold fluctuations or progression [6 5]. While First-trimester maternal infection confers substantially elevated risks of severe SNHL, third-trimester exposures may induce mild auditory deficits. Importantly, the potential for severe neurological sequelae remains exclusively associated with maternal infections occurring during the initial gestational trimester. [7,14,24].
3. Diagnosis and Screening
Congenital cytomegalovirus (cCMV) infection is implicated in approximately 10% of childhood cerebral palsy cases [8] and 25% of SNHL cases [9]. However, only 15% of infected infants exhibit clinical manifestations at birth [4,5]. The majority of cases remain undetected unless severe symptoms emerge, resulting in fewer than 25% identification within the first postnatal month [6]. Among those classified as asymptomatic at birth, up to 20% develop late-onset SNHL, developmental delays, or neurocognitive impairments, with diagnoses typically delayed beyond 12 months of age [10,19,20]. Early identification is critical, as delayed diagnosis may exacerbate adverse neurodevelopmental outcomes.
Three neonatal screening strategies exist for cCMV: targeted screening, expanded targeted screening, and universal screening. Testing within 21 days of birth is essential to differentiate congenital from postnatal infections, which pose lower risks of SNHL and developmental deficits [4,6]. The 2017 European consensus recommends CMV testing only for symptomatic neonates or those with confirmed SNHL, primarily due to cost constraints, management uncertainties for asymptomatic cases, and parental anxiety concerns [6,35]. This approach misses >75% of asymptomatic infants. Universal screening has been advocated as the sole method capable of enabling early intervention for all cCMV-positive infants at risk of late-onset hearing loss [72]. Notably, the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) issued a 2024 position statement endorsing universal cCMV newborn screening, emphasizing its potential to improve hearing outcomes through early diagnosis (https://www.entnet.org/). Recent large-scale studies provide supporting evidence: Leruez-Ville et al. [27] identified a 0.37% cCMV prevalence (51 confirmed cases) among 11,740 screened neonates, with 4 infants developing unilateral/bilateral SNHL. Similarly, Barkai et al. [28] reported a 0.49% prevalence (47 confirmed cases) in 9,845 neonates, where initial pass rates on newborn hearing screening failed to predict subsequent SNHL detected during follow-up. These findings underscore universal screening’s capacity to identify at-risk asymptomatic infants requiring longitudinal audiological monitoring.
Dried blood spot (DBS) PCR has emerged as a practical tool for universal screening, leveraging existing newborn metabolic screening infrastructure [68,73]. DBS offers logistical advantages including cost-effectiveness, ease of storage, and retrospective diagnostic potential for late-onset SNHL. Minnesota became the first U.S. state to implement universal DBS-based cCMV screening in 2023, with 13 additional states (including New York) subsequently adopting similar programs, though methodological standardization remains lacking [70,71]. However, DBS PCR has lower sensitivity than saliva PCR (75% vs. >98%), potentially missing up to one-third of cases due to lower viral DNA loads in blood [58,68]. Boppana et al. [73] prospectively compared single- versus dual-primer DBS PCR with rapid saliva culture, revealing that even optimized dual-primer protocols failed to detect 80% of cCMV cases. While recent DBS sensitivity improvements (75% detection rate) represent progress, one-quarter of infections remain undiagnosed [70], necessitating methodological refinements. Conversely, saliva PCR achieves >98% sensitivity but faces challenges with false positives from breastmilk CMV DNA contamination, requiring confirmatory urine PCR [7,8,21]. Cost barriers further limit saliva PCR’s scalability for universal screening [76]. Israel’s pooled saliva testing strategy addresses these limitations by batch-testing multiple samples followed by individual retesting of positive pools, achieving a 55.6% detection rate for asymptomatic cCMV cases missed by targeted screening [77].
Cost-effectiveness analyses yield conflicting perspectives. A Singaporean study comparing three screening strategies over two years estimated total direct costs at S$104,445.79 (no screening), S$146,656.30 (targeted), and S$853,890.16 (universal) [33]. Similarly, Gantt et al. [37] calculated per-case identification costs of $566–$2,832 (targeted) versus $2,000–$10,000 (universal). However, when accounting for lifetime costs of undiagnosed SNHL, universal screening demonstrated greater net savings in most models [36,37]. A Japanese decision-tree analysis further supported universal screening’s superior cost-effectiveness compared to targeted approaches [36].
Prenatal diagnosis requires early first-trimester maternal. serology testing(IgG/IgM + IgG avidity), as fetal sequelae correlate strongly with first-trimester transmission [74]. CMV IgG/IgM serology with IgG avidity testing confirms primary infection in IgM-positive cases. Amniotic fluid PCR after 17 weeks is the gold standard [8]. Late-gestation fetal MRI and ultrasound provide prognostic insights, demonstrating high negative predictive values (96.9–98.5%) for severe outcomes when normal. Notably, 46% of asymptomatic neonates exhibit abnormal neuroimaging, though imaging poorly predicts late-onset SNHL [57].
For delayed-onset SNHL beyond 21 days, retrospective DBS analysis confirms cCMV. Differential diagnosis incorporates maternal infection history, characteristic neuroimaging findings (e.g., periventricular calcifications), and exclusion of genetic, anatomical, or alternative infectious etiologies to optimize diagnostic accuracy. The detailed diagnosis and treatment process is shown in Figure 1.
4. Classification
The 2017 European Consensus Committee defines isolated SNHL as asymptomatic cCMV infection in the absence of concurrent clinical, laboratory, or neuroimaging abnormalities [4]. In contrast, the European Society for Paediatric Infectious Diseases (ESPID) classifies isolated CMV-associated SNHL as a manifestation of CNS involvement [6].
5. Prevention and Treatment
5.1. Three-Tiered Prevention Measures for cCMV Infection
Primary prevention spans the entire pregnancy period, particularly preconception and early gestation, including vaccination and behavioral prophylaxis. Secondary prevention targets primary CMV infection during pregnancy, especially in the first trimester, involving antivirals, hyperimmune globulin, and monoclonal antibodies. Tertiary prevention involves using valacyclovir during pregnancy after amniocentesis-confirmed fetal CMV infection to reduce maternal viral load and vertical transmission risk. Confirmed fetal CMV infection may present as: asymptomatic, mild/isolated symptoms, or moderate/severe clinical symptoms at birth (refer to Table 1 for details).
5.2. Antiviral Treatment for Moderate/Severe Symptoms
Since 2017, antiviral therapy has been recommended for infants with moderate/severe symptoms [6,8,30]. Kimberlin et al. compared 6-week intravenous ganciclovir versus no treatment for hearing outcomes in neonates [31]. Among 100 enrolled infants, 47 were randomized to the treatment group and 50 to the control group. The treatment group received ganciclovir (6 mg/kg IV q12h for 6 weeks), while controls received no treatment. At 6 months: 84% (21/25) treated vs 59% (10/17) controls improved/maintained hearing; 0% vs 41% deteriorated. At ≥1-year follow-up, 21% (5/24) of treated versus 68% (13/19) control patients showed hearing deterioration. Grade 3/4 neutropenia: 63% (29/46) treated vs 21% (9/43) controls (P<0.01).
Yang et al. [56] conducted an RCT comparing 6-week IV ganciclovir (control) versus oral valganciclovir (intervention). Both groups showed significant reductions in abnormal hearing rates (20.83% control vs 29.17% intervention). Kimberlin et al. [60] conducted a pharmacokinetic comparison between intravenous ganciclovir and oral valganciclovir, demonstrating that the Oral valganciclovir had lower neutropenia risk than IV ganciclovir. A subsequent study compared 6-week vs 6-month oral valganciclovir [55]. At the 6-month assessment, both treatment groups exhibited comparable improvements in best-ear hearing outcomes. By 12 months, however, the 6-month treatment group demonstrated a higher proportion of ears maintaining or achieving normal hearing across all auditory frequencies compared to the 6-week cohort. Longitudinal follow-up at 24 months further revealed superior neurodevelopmental scale scores in the 6-month treatment group, underscoring the sustained benefits of prolonged antiviral therapy. While both regimens showed comparable short-term hearing improvement, the longer course appeared to moderately improve long-term hearing and developmental outcomes [55]. Current clinical practice typically employs 6-month oral valganciclovir for symptomatic cCMV, with individualized adjustments. Overall, for infants with moderate/severe congenital CMV, antiviral therapy (IV ganciclovir or oral valganciclovir) can improve/maintain hearing and reduce deterioration risk, despite neutropenia side effects. However, ganciclovir/valganciclovir use remains controversial for asymptomatic/mild cases [54].
5.3. Management of Asymptomatic/Mild Cases
In the 2017 European consensus, most experts believe that asymptomatic children and children with mild isolated symptoms should not receive treatment, and there is no consensus on whether to treat isolated SNHL [6].The risk-benefit ratio of antiviral therapy must be carefully considered. Some cohort studies support potential benefits. Pui Khi Chung et al. conducted a non-randomized trial comparing valganciclovir versus no treatment in minimally symptomatic infants [32]. Among 37 analyzed participants (25 treatment, 12 control), controls were more likely to experience hearing decline. Mean best-ear hearing decreased by 13.7 dB in controls versus improved by 3.3 dB in the treatment group. Neutropenia occurred in 3/20 treated versus 1/8 control infants.
Lanzieri et al. [43] prospectively followed 92 asymptomatic cCMV infants and 51 controls from 3 months to 5 years. SNHL prevalence increased from 7% to 14% in cases versus 0% in controls; from 6-18 years, changes were 11% versus 8% respectively. By age 18, SNHL prevalence reached 25% (95% CI: 17%-36%) in cases versus 8% (95% CI: 3%-22%) in controls. Cases with unilateral congenital/early-onset SNHL had higher risk of delayed-onset loss in the initially normal ear. Among affected ears, 65% showed progressive deterioration, including 40% of better ears in bilateral cases.
Pasternak et al. [42] retrospectively studied 59 infants with isolated SNHL receiving valganciclovir/ganciclovir. Of 80 affected ears at baseline, 68.8% (55) improved (96.3% normalized), 2.5% (2) worsened; among 21 infants with bilateral loss, 76.1% (16) showed improvement (93.7% achieving normal functional hearing). Neutropenia (ANC ≤1000/mm³) occurred in 19 infants (30 episodes), primarily during the first 3 months, including one grade 3 case (ANC 400-599 cells/mm³).
Lackner et al. [50] followed 18 treated asymptomatic children; 89% (16) maintained normal hearing at 4-10 years. Turriziani Colonna et al. [48] reported no SNHL in 24 treated asymptomatic infants followed to 41.5 months. Villaverde et al. [18] retrospectively analyzed 196 mild cCMV infants (68 treated). Overall SNHL incidence at 24 months was 4.6% (9/196), with no difference between treated (4.4%) and untreated (4.7%) groups (P=0.658). Long-term drug effects and post-24-month hearing outcomes remain unclear. Dilek Yılmaz Çiftdoğan et al. [54] reported a case of asymptomatic cCMV with bilateral SNHL showing CMV pp65 antigenemia reduction after 1-week ganciclovir, undetectable levels after 5-week valganciclovir, and progressive SNHL improvement over 1-year follow-up. These observational data demonstrate hearing protection despite significant neutropenia risks (63% ganciclovir vs 12% valganciclovir).
5.4. Delayed-Onset Hearing Loss
Amir et al. [53] analyzed 21 infants with delayed-onset SNHL receiving ganciclovir/valganciclovir. Among 42 affected ears pretreatment: 52% (22) mild, 24% (10) moderate, 7% (3) severe loss. Post-treatment, only 5% (2) remained in each category, with 86% (36) normalizing and 69% (29) improving. Stronati et al. [45] reported an infant with normal newborn hearing who developed isolated left mild SNHL at 3 months. Without treatment, BERA at 6 months showed moderate bilateral deficit. After 6-week valganciclovir (15 mg/kg q12h), hearing normalized by 12 months. However, given the fluctuating nature of cCMV-related hearing loss, spontaneous recovery must be distinguished from treatment effects through long-term follow-up.
5.5. Current Perspectives
Current evidence suggests potential therapeutic benefits of antiviral treatment for children with isolated or delayed-onset SNHL. Although valganciclovir’s short-term toxicities (neutropenia, hepatotoxicity) are usually reversible, they require frequent hematologic monitoring [44]. The sustained benefits of neonatal antiviral therapy beyond age 2 remain unclear [51], as limited longitudinal follow-up data and insufficient safety surveillance preclude robust conclusions regarding universal intervention for isolated/delayed SNHL. Critical knowledge gaps persist, including: 1) the identification of reliable biomarkers for delayed-onset SNHL progression [52]; 2) comprehensive pharmacokinetic, efficacy, and safety profiling of oral valganciclovir regimens [54]; and 3) evidence-based criteria for initiating treatment in asymptomatic or minimally symptomatic cases. These unresolved issues underscore the imperative for targeted clinical investigations to optimize therapeutic protocols.
6. Follow-Up
Therapeutic management of cCMV infection has historically been constrained by limited long-term follow-up data. Prior studies lacked prospective audiologic evaluations beyond age 2 in infants with symptomatic cCMV disease receiving six-month valganciclovir (VGCV) therapy [59]. Recently, a Japanese investigator-initiated, single-arm, prospective multicenter trial evaluated long-term hearing outcomes in symptomatic cCMV infants treated with oral VGCV (16 mg/kg bid for six months), with three-year follow-up. At six months, 19 of 48 ears (40.0%) demonstrated hearing improvement, increasing to 27 ears (56.3%, p = 0.032) by three years. The proportion of ears achieving and sustaining normal hearing rose from 25 (52.5%) at six months to 35 (72.9%, p = 0.011) at three years, while stable hearing preservation rates remained comparable between timepoints. No delayed adverse effects were observed post-treatment [59]. These findings by Ichiro Morioka et al. suggest a favorable benefit-risk profile for antiviral therapy in maintaining or improving auditory function in symptomatic cases.
Delayed-onset hearing loss (DHL) is defined as postnatally acquired hearing deficits in infants passing newborn hearing screening programs (NHSP). Progressive hearing loss—deterioration to a more severe hearing category in ≥1 ear—also falls under DHL. Notably, 8-12% of asymptomatic cCMV infants develop isolated SNHL [34], underscoring the necessity for longitudinal monitoring. While current prenatal or neonatal tools cannot reliably predict DHL, neuroimaging markers of central nervous system involvement (e.g., ventriculomegaly, white matter lesions, or calcifications) correlate with elevated SNHL risk. Most existing studies feature ≤2-year follow-up periods, potentially missing late-onset DHL, while infrequent audiologic assessments may delay detection of early hearing declines [48,49].
According to longitudinal data by Lancrer [50], Fourgeaud [46], and Liesbeth [47], 40%-60% of symptomatic infants exhibit SNHL at birth (71% severe-to-profound), with 37.5% experiencing further auditory deterioration during follow-up, often necessitating cochlear implantation. Among asymptomatic cases, 8%-15% develop SNHL between 6 months and 6 years of age (50% unilateral; fluctuating/progressive in subset), yet 43% discontinue follow-up before age 3, increasing DHL underdiagnosis [46,47,50].
For asymptomatic infants, selective oral VGCV therapy may be considered if DHL or progression emerges, accompanied by rigorous toxicity monitoring. However, robust long-term outcome data remain imperative to optimize prophylactic and therapeutic strategies for this population.
7. Conclusions
The management of congenital cytomegalovirus associated hearing loss necessitates a dual approach integrating early detection and evidence-based interventions. Current evidence supports antiviral therapy—specifically a six-month course of oral valganciclovir—for improving auditory and neurodevelopmental outcomes in symptomatic infants [1,2]. However, its use in asymptomatic or minimally symptomatic cases remains controversial. While observational studies suggest potential benefits in attenuating hearing deterioration [3], the absence of high-quality randomized controlled trial (RCT) data, coupled with risks of hepatotoxicity and other adverse effects, limits therapeutic consensus for this population [4,5]. Universal screening is currently the most effective measure to reduce the rate of missed diagnosis of asymptomatic children. Although some developed countries have begun to implement universal screening, its implementation still needs to make a balance between low screening cost and high positive rate, as well as the development of standardized management. The high rate of missed diagnosis of delayed-onset hearing loss exposes the shortcomings of the current follow-up system, and there is a need to formulate follow-up strategies and develop more methods to predict the risk of long-term sequelae.
Funding
This research is supported by the Key Program of the National Natural Science Foundation of China (No. 82430035), the National Key Research and Development Program of China (Nos. 2021YFF0702303, 2024YFC2511101, 2023YFE0203200), the Foundation for Innovative Research Groups of Hubei Province (No. 2023AFA038), and the Fundamental Research Funds for the Central Universities (No.2024BRA019).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lim, Y.; Lyall, H. Congenital cytomegalovirus-who, when, what-with and why to treat? J. Infect. 2017, 74, S89–S94. [Google Scholar] [CrossRef] [PubMed]
- Osterholm, E.A.; Schleiss, M.R. Impact of breast milk-acquired cytomegalovirus infection in premature infants: Pathogenesis, prevention, and clinical consequences? Rev. Med. Virol. 2020, 30, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Leruez-Ville, M.; Foulon, I.; Pass, R.; Ville, Y. Cytomegalovirus infection during pregnancy: State of the science. Am. J. Obstet. Gynecol. 2020, 223, 330–349. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, W.D.; Boppana, S.B.; Fowler, K.B.; Kimberlin, D.W.; Lazzarotto, T.; Alain, S.; Daly, K.; Doutré, S.; Gibson, L.; Giles, M.L.; et al. Congenital cytomegalovirus infection in pregnancy and the neonate: Consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect. Dis. 2017, 17, e177–e188. [Google Scholar] [CrossRef] [PubMed]
- Swartling, L.; Engman, M.L.; Eriksen, J.; Fischler, B.; Friman, V.; Hobell, H.; Ljungman, P.; Mellgren, K.; Navér, L.; Nyström, K.; et al. Management of cytomegalovirus infections-Swedish recommendations 2023. Infect. Dis. (Lond) 2024, 56, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Luck, S.E.; Wieringa, J.W.; Blázquez-Gamero, D.; Henneke, P.; Schuster, K.; Butler, K.; Capretti, M.G.; Cilleruelo, M.J.; Curtis, N.; Garofoli, F.; et al. Congenital cytomegalovirus: A European expert consensus statement on diagnosis and management. Pediatr. Infect. Dis. J. 2017, 36, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, W.D.; Boppana, S.B.; Fowler, K.B.; Kimberlin, D.W.; Lazzarotto, T.; Alain, S.; Daly, K.; Doutré, S.; Gibson, L.; Giles, M.L.; et al. Congenital cytomegalovirus infection in pregnancy and the neonate: Consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect. Dis. 2017, 17, e177–e188. [Google Scholar] [CrossRef] [PubMed]
- Leruez-Ville, M.; Chatzakis, C.; Lilleri, D.; Blazquez-Gamero, D.; Alarcon, A.; Bourgon, N.; Foulon, I.; Fourgeaud, J.; Gonce, A.; Jones, C.E.; et al. Consensus recommendation for prenatal, neonatal and postnatal management of congenital cytomegalovirus infection from the European congenital infection initiative (ECCI). Lancet Reg. Health Eur. 2024, 40, 100892. [Google Scholar] [CrossRef] [PubMed]
- Coskun, E.; Kakkar, F.; Riley, L.E.; Ciaranello, A.L.; Prabhu, M. Evaluation and management of congenital cytomegalovirus infection. Obstet. Gynecol. 2025, 145, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Buca, D.; Di Mascio, D.; Rizzo, G.; Giancotti, A.; D’Amico, A.; Leombroni, M.; Makatsarya, A.; Familiari, A.; Liberati, M.; Nappi, L.; et al. Outcome of fetuses with congenital cytomegalovirus infection and normal ultrasound at diagnosis: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2021, 57, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Weisblum, Y.; Panet, A.; Haimov-Kochman, R.; Wolf, D.G. Models of vertical cytomegalovirus (CMV) transmission and pathogenesis. Semin. Immunopathol. 2014, 36, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Navti, O.B.; Al-Belushi, M.; Konje, J.C. Cytomegalovirus infection in pregnancy-An update. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Heath, P.; Jones, C.; Soe, A.; Ville, Y.; Royal College of Obstetricians. Congenital cytomegalovirus infection: Update on screening, diagnosis and treatment: Scientific impact paper No. 56. BJOG 2025, 132, e42–e52. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Liu, X.; Sun, Y. The pathogenesis of cytomegalovirus and other viruses associated with hearing loss: Recent updates. Viruses 2023, 15, 1385. [Google Scholar] [CrossRef] [PubMed]
- Hilditch, C.; Liersch, B.; Spurrier, N.; Callander, E.J.; Cooper, C.; Keir, A.K. Does screening for congenital cytomegalovirus at birth improve longer term hearing outcomes? Arch. Dis. Child. 2018, 103, 988–992. [Google Scholar] [CrossRef] [PubMed]
- Fowler, K.; Mucha, J.; Neumann, M.; Lewandowski, W.; Kaczanowska, M.; Grys, M.; Schmidt, E.; Natenshon, A.; Talarico, C.; Buck, P.O.; et al. A systematic literature review of the global seroprevalence of cytomegalovirus: Possible implications for treatment, screening, and vaccine development. BMC Public Health 2022, 22, 1659. [Google Scholar] [CrossRef] [PubMed]
- Chatzakis, C.; Ville, Y.; Makrydimas, G.; Dinas, K.; Zavlanos, A.; Sotiriadis, A. Timing of primary maternal cytomegalovirus infection and rates of vertical transmission and fetal consequences. Am. J. Obstet. Gynecol. 2020, 223, 870–883. [Google Scholar] [CrossRef] [PubMed]
- Villaverde, S.; Pedrero-Tomé, R.; Papaevangelou, V.; Syridou, G.; Karagiannidou, S.; Lyall, H.; Payne, H.; Frick, M.A.; Soler-Palacín, P.; Baquero-Artigao, F.; et al. Antiviral treatment and risk of hearing loss in asymptomatic and mild symptomatic infants with congenital cytomegalovirus. Pediatr. Infect. Dis. J. 2025, 44, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Smyrli, A.; Raveendran, V.; Walter, S.; Pagarkar, W.; Field, N.; Kadambari, S.; Lyall, H.; Bailey, H. What are the neurodevelopmental outcomes of children with asymptomatic congenital cytomegalovirus infection at birth? A systematic literature review. Rev. Med. Virol. 2024, 34, e2555. [Google Scholar] [CrossRef] [PubMed]
- Korndewal, M.J.; Oudesluys-Murphy, A.M.; Kroes, A.C.; Van Der Sande, M.A.; De Melker, H.E.; Vossen, A.C. Long-term impairment attributable to congenital cytomegalovirus infection: A retrospective cohort study. Dev. Med. Child Neurol. 2017, 59, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Goderis, J.; Keymeulen, A.; Smets, K.; Van Hoecke, H.; De Leenheer, E.; Boudewyns, A.; Desloovere, C.; Kuhweide, R.; Muylle, M.; Royackers, L.; et al. Hearing in children with congenital cytomegalovirus infection: Results of a longitudinal study. J Pediatr. 2016, 172, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Goderis, J.; De Leenheer, E.; Smets, K.; Van Hoecke, H.; Keymeulen, A.; Dhooge, I. Hearing loss and congenital CMV infection: A systematic review. Pediatrics 2014, 134, 972–982. [Google Scholar] [CrossRef] [PubMed]
- Spekker-Bosker, K.; Ufermann, C.M.; Maywald, M.; Zimmermann, A.; Domröse, A.; Woite, C.; Däubener, W.; Eller, S.K. hCMV-mediated immune escape mechanisms favor pathogen growth and disturb the immune privilege of the eye. Int. J. Mol. Sci. 2019, 20, 858. [Google Scholar] [CrossRef] [PubMed]
- Seidenari, A.; Dionisi, C.; Nati, M.; Marsico, C.; Gabrielli, L.; Capretti, M.G.; Toni, F.; Lazzarotto, T.; Simonazzi, G. Follow-up of infants with congenital cytomegalovirus following maternal primary infection in the first trimester and normal fetal brain imaging at midgestation. Prenatal Diag. 2025, 45, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Schleiss, M.R.; Blázquez-Gamero, D. Universal newborn screening for congenital cytomegalovirus infection. Lancet Child Adolesc. Health 2025, 9, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Corazzi, V.; Fordington, S.; Brown, T.H.; Donnelly, N.; Bewick, J.; Ehsani, D.; Pelucchi, S.; Bianchini, C.; Ciorba, A.; Borsetto, D. Late-onset, progressive sensorineural hearing loss in the paediatric population: A systematic review. Eur. Arch. Otorhinolaryngol. 2024, 281, 3397–3421. [Google Scholar] [CrossRef] [PubMed]
- Leruez-Ville, M.; Magny, J.F.; Couderc, S.; Pichon, C.; Parodi, M.; Bussières, L.; Guilleminot, T.; Ghout, I.; Ville, Y. Risk factors for congenital cytomegalovirus infection following primary and nonprimary maternal infection: A prospective neonatal screening study using polymerase chain reaction in saliva. Clin. Infect. Dis. 2017, 65, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Barkai, G.; Roth, D.A.E.; Barzilai, A.; Tepperberg-Oikawa, M.; Mendelson, E.; Hildesheimer, M.; Kuint, J. Universal neonatal cytomegalovirus screening using saliva-report of clinical experience. J. Clin. Virol. 2014, 60, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Fowler, K.B.; Mccollister, F.P.; Sabo, D.L.; Shoup, A.G.; Owen, K.E.; Woodruff, J.L.; Cox, E.; Mohamed, L.S.; Choo, D.I.; Boppana, S.B.; et al. A targeted approach for congenital cytomegalovirus screening within newborn hearing screening. Pediatrics 2017, 139, e20162128. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, W.D.; Boppana, S.B.; Fowler, K.B.; Kimberlin, D.W.; Lazzarotto, T.; Alain, S.; Daly, K.; Doutré, S.; Gibson, L.; Giles, M.L.; et al. Congenital cytomegalovirus infection in pregnancy and the neonate: Consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect. Dis. 2017, 17, e177–e188. [Google Scholar] [CrossRef] [PubMed]
- Kimberlin, D.W.; Lin, C.Y.; Sánchez, P.J.; Demmler, G.J.; Dankner, W.; Shelton, M.; Jacobs, R.F.; Vaudry, W.; Pass, R.F.; Kiell, J.M.; et al. Effect of ganciclovir therapy on hearing in symptomatic congenital cytomegalovirus disease involving the central nervous system: A randomized, controlled trial. J Pediatr. 2003, 143, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.K.; Schornagel, F.A.; Soede, W.; Van Zwet, E.W.; Kroes, A.C.; Oudesluys-Murphy, A.M.; Vossen, A.C. Valganciclovir in infants with hearing loss and clinically inapparent congenital cytomegalovirus infection: A nonrandomized controlled trial. J Pediatr. 2024, 268, 113945. [Google Scholar] [CrossRef] [PubMed]
- Aldon, M.L.; Raveentheran, G.; Amin, Z.; Chan, S.M.; Aoyama, R.; Tee, N.; Ng, S.Y.; Lee, C.K.; Ng, P.G.; Low, J.M. Congenital cytomegalovirus screening in neonates born after 35 weeks gestation—is targeted screening beneficial? Front. Pediatr. 2025, 13, 1510612. [Google Scholar] [CrossRef] [PubMed]
- Andronaco, D.W. Congenital Cytomegalovirus (CMV) infection & hearing loss. J. Obstet. Gynecol. Neonatal Nurs. 2020, 49, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Schleiss, M.R. Newborn screening for congenital cytomegalovirus (cCMV) infection: Universal, targeted, expanded-targeted, or none-of-the-above? Neonatol. Today 2024, 19, 3. [Google Scholar] [PubMed]
- Aoki, H.; Bitnun, A.; Kitano, T. The cost-effectiveness of maternal and neonatal screening for congenital cytomegalovirus infection in Japan. J. Med. Virol. 2023, 95, e28391. [Google Scholar] [CrossRef] [PubMed]
- Gantt, S.; Dionne, F.; Kozak, F.K.; Goshen, O.; Goldfarb, D.M.; Park, A.H.; Boppana, S.B.; Fowler, K. Cost-effectiveness of universal and targeted newborn screening for congenital cytomegalovirus infection. JAMA Pediatr. 2016, 170, 1173–1180. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.; Crooks, C.M.; Permar, S.R.; Weimer, K.E.D. Neonatal cytomegalovirus infection: Advocacy, legislation, and changing practice. Clin. Perinatol. 2025, 52, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.R.; Wang, X.; Melvin, A.J. Timing of congenital cytomegalovirus diagnosis and missed opportunities. Front. Pediatr. 2025, 13, 1475121. [Google Scholar] [CrossRef] [PubMed]
- Boscarino, G.; Romano, R.; Tegoni, F.; Iotti, C.; Perrone, S.; Esposito, S.; Buonsenso, D. Congenital cytomegalovirus severity definitions and treatment decisions around the world: A systematic scoping review of the literature. J. Clin. Med. 2024, 13, 5997. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.; Crooks, C.M.; Permar, S.R.; Weimer, K.E.D. Neonatal cytomegalovirus infection: Advocacy, legislation, and changing practice. Clin. Perinatol. 2025, 52, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Pasternak, Y.; Ziv, L.; Attias, J.; Amir, J.; Bilavsky, E. Valganciclovir is beneficial in children with congenital cytomegalovirus and isolated hearing loss. J Pediatr. 2018, 199, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Lanzieri, T.M.; Chung, W.; Flores, M.; Blum, P.; Caviness, A.C.; Bialek, S.R.; Grosse, S.D.; Miller, J.A.; Demmler-Harrison, G.; Congenital Cytomegalovirus Longitudinal Study Group. Hearing loss in children with asymptomatic congenital cytomegalovirus infection. Pediatrics 2017, 139, e20162610. [Google Scholar] [CrossRef] [PubMed]
- Kimberlin, D.W.; Banerjee, R.; Barnett, E.D.; Lynfield, R.; Sawyer, M.H. Cytomegalovirus infection. In Red book: 2024– 2027 report of the committee on infectious diseases, 33rd ed.; Kimberlin, D.W., Banerjee, R., Eds.; American Academy of Pediatrics: New York, 2024; pp. 344–352. [Google Scholar]
- Stronati, M.; Garofoli, F.; Angelini, M.; Licari, A.; Manzoni, P.; Lombardi, G. Valganciclovir treatment in a 6-month-old infant with asymptomatic congenital cytomegalovirus infection and late hearing loss. Pediatr. Infect. Dis. J. 2011, 30, 1124–1125. [Google Scholar] [CrossRef] [PubMed]
- Fourgeaud, J.; Magny, J.F.; Couderc, S.; Garcia, P.; Maillotte, A.M.; Benard, M.; Pinquier, D.; Minodier, P.; Astruc, D.; Patural, H.; et al. Predictors of the outcome at 2 years in neonates with congenital cytomegalovirus infection. Pediatrics 2024, 153, e2023063531. [Google Scholar] [CrossRef] [PubMed]
- Royackers, L.; Christian, D.; Frans, D.; Ermelinde, R. Hearing status in children with congenital cytomegalovirus: Up-to-6-years audiological follow-up. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Turriziani Colonna, A.; Buonsenso, D.; Pata, D.; Salerno, G.; Chieffo, D.P.; Romeo, D.M.; Faccia, V.; Conti, G.; Molle, F.; Baldascino, A.; et al. Long-term clinical, audiological, visual, neurocognitive and behavioral outcome in children with symptomatic and asymptomatic congenital cytomegalovirus infection treated with valganciclovir. Front. Med. (Lausanne) 2020, 7, 268. [Google Scholar] [CrossRef] [PubMed]
- Palma, S.; Forli, F.; Rossi, C.; Filice, R.; D’Adamo, C.; Roversi, M.F.; Monzani, D.; Lorenzoni, F.; Botti, C.; Berrettini, S.; et al. The audiological follow-up of children with symptomatic congenital cytomegalovirus infection: An experience in two Italian centers. Children 2023, 10, 1136. [Google Scholar] [CrossRef] [PubMed]
- Lackner, A.; Acham, A.; Alborno, T.; Moser, M.; Engele, H.; Raggam, R.; Halwachs-Baumann, G.; Kapitan, M.; Walch, C. Effect on hearing of ganciclovir therapy for asymptomatic congenital cytomegalovirus infection: Four to 10 year follow up. J. Laryngol. Otol. 2009, 123, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Schleiss, M.R. Antiviral therapy and its long-term impact on hearing loss caused by congenital cytomegalovirus: Much remains to be learned! J. Pediatric Infect. Dis. Soc. 2022, 11, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Howard, A.; Nishikawa, J.K.; Sánchez, P.J. “Minimally symptomatic” congenital cytomegalovirus infection: Latest data and emerging concepts. Curr. Opin. Pediatr. 2024, 36, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Amir, J.; Attias, J.; Pardo, J. Treatment of late-onset hearing loss in infants with congenital cytomegalovirus infection. Clin. Pediatr. (Phila) 2014, 53, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Çiftdogan, D.Y.; Vardar, F. Effect on hearing of oral valganciclovir for asymptomatic congenital cytomegalovirus infection. J. Trop. Pediatr. 2011, 57, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Kimberlin, D.W.; Jester, P.M.; Sánchez, P.J.; Ahmed, A.; Arav-Boger, R.; Michaels, M.G.; Ashouri, N.; Englund, J.A.; Estrada, B.; Jacobs, R.F.; et al. Valganciclovir for symptomatic congenital cytomegalovirus disease. N. Engl. J. Med. 2015, 372, 933–943. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Qiu, A.; Wang, J.; Pan, Z. Comparative effects of valganciclovir and ganciclovir on the congenital cytomegalovirus infection and hearing loss: A randomized controlled trial. Iran. J. Pediatr. 2022, 32, e118874. [Google Scholar] [CrossRef]
- Buca, D.; Di Mascio, D.; Rizzo, G.; Giancotti, A.; D’Amico, A.; Leombroni, M.; Makatsarya, A.; Familiari, A.; Liberati, M.; Nappi, L.; et al. Outcome of fetuses with congenital cytomegalovirus infection and normal ultrasound at diagnosis: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2021, 57, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, M.; Kim, J.; Medoro, A.K.; Flint, K.; Kaptsan, I.; Wang, H.; Pifer, T.; Harris, R.; Cuartas, J.; Leber, A.; et al. Agreement between dried blood spot and plasma PCR in infants with congenital cytomegalovirus infection. J. Med. Virol. 2025, 97, e70257. [Google Scholar] [CrossRef] [PubMed]
- Morioka, I.; Kakei, Y.; Imai, T.; Fujioka, K.; Takahashi, N.; Yoshikawa, T.; Moriuchi, H.; Ito, Y.; Oka, A.; Japanese Congenital Cytomegalovirus Study Group. Three-year hearing outcomes in infants with congenital cytomegalovirus disease treated with oral valganciclovir: Interim results of a six-year follow-up study in Japan. J. Clin. Virol. 2025, 177, 105778. [Google Scholar] [CrossRef] [PubMed]
- Kimberlin, D.W.; Acosta, E.P.; Sánchez, P.J.; Sood, S.; Agrawal, V.; Homans, J.; Jacobs, R.F.; Lang, D.; Romero, J.R.; Griffin, J.; et al. Pharmacokinetic and pharmacodynamic assessment of oral valganciclovir in the treatment of symptomatic congenital cytomegalovirus disease. J. Infect. Dis. 2008, 197, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Jenks, C.M.; Hoff, S.R.; Mithal, L.B. Congenital cytomegalovirus infection: Epidemiology, timely diagnosis, and management. Neoreviews 2021, 22, e606–e613. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B.L.; Gyamfi-Bannerman, C.; Society for Maternal-Fetal Medicine (SMFM). Diagnosis and antenatal management of congenital cytomegalovirus infection. Am. J. Obstet. Gynecol. 2016, 214, B5–B11. [Google Scholar] [CrossRef] [PubMed]
- Lanzieri, T.M.; Leung, J.; Caviness, A.C.; Chung, W.; Flores, M.; Blum, P.; Bialek, S.R.; Miller, J.A.; Vinson, S.S.; Turcich, M.R.; et al. J. Perinatol. 2017, 37, 875–880. [CrossRef] [PubMed]
- Singh, G.; Gaidhane, A. A review of sensorineural hearing loss in congenital cytomegalovirus infection. Cureus 2022, 14, e30703. [Google Scholar] [CrossRef] [PubMed]
- Aldè, M.; Binda, S.; Primache, V.; Pellegrinelli, L.; Pariani, E.; Pregliasco, F.; Di Berardino, F.; Cantarella, G.; Ambrosetti, U. Congenital cytomegalovirus and hearing loss: The state of the art. J. Clin. Med. 2023, 12, 4465. [Google Scholar] [CrossRef] [PubMed]
- Korndewal, M.J.; Oudesluys-Murphy, A.M.; Kroes, A.C.; Van Der Sande, M.A.; De Melker, H.E.; Vossen, A.C. Long-term impairment attributable to congenital cytomegalovirus infection: A retrospective cohort study. Dev. Med. Child Neurol. 2017, 59, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Payne, H.; Aaltoranta, M.; Veikkolainen, V.; Kent, N.; Gkouleli, T.; Lennon, A.; Ramgoolam, T.; Adams, S.P. A high-sensitivity, high-throughput newborn screening assay for congenital cytomegalovirus—is it time for universal screening in the United Kingdom? Front. Pediatr. 2025, 13, 1543132. [Google Scholar] [CrossRef] [PubMed]
- Boppana, S.B.; Ross, S.A.; Novak, Z.; Shimamura, M.; Tolan, R.W.; Palmer, A.L.; Ahmed, A.; Michaels, M.G.; Sánchez, P.J.; Bernstein, D.I.; et al. Dried blood spot real-time polymerase chain reaction assays to screen newborns for congenital cytomegalovirus infection. JAMA 2010, 303, 1375–1382. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.K.; Chakraborty, P.; Reuvers, E.; Gallagher, L.; Kernohan, K.D.; Lacaria, M.; Barton, M.; Leifso, K.; Pernica, J.M.; Santander, E. Outcomes of a population-based congenital cytomegalovirus screening program. JAMA Pediatr. 2025, 179, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Dollard, S.C.; Dreon, M.; Hernandez-Alvarado, N.; Amin, M.M.; Wong, P.; Lanzieri, T.M.; Osterholm, E.A.; Sidebottom, A.; Rosendahl, S.; Mccann, M.T.; et al. Sensitivity of dried blood spot testing for detection of congenital cytomegalovirus infection. JAMA Pediatr. 2021, 175, e205441. [Google Scholar] [CrossRef] [PubMed]
- Yassine, B.B.; Hulkower, R.; Dollard, S.; Cahill, E.; Lanzieri, T. A legal mapping assessment of cytomegalovirus-related laws in the United States. J. Public Health Manag. Pract. 2022, 28, E624–E629. [Google Scholar] [CrossRef] [PubMed]
- Pesch, M.H.; Brown, K.D.; Birath, A.L.; Demmler-Harrison, G.J.; Sapp, C.; Selleck, A.M.; Sweeney, A.D. American cochlear implant alliance position statement on newborn congenital cytomegalovirus screening. Otolaryngol. Head Neck Surg. 2025, 172, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Boppana, S.B.; Ross, S.A.; Novak, Z.; Shimamura, M.; Tolan, R.W.; Palmer, A.L.; Ahmed, A.; Michaels, M.G.; Sánchez, P.J.; Bernstein, D.I.; et al. Dried blood spot real-time polymerase chain reaction assays to screen newborns for congenital cytomegalovirus infection. JAMA 2010, 303, 1375–1382. [Google Scholar] [CrossRef] [PubMed]
- Faure-Bardon, V.; Magny, J.F.; Parodi, M.; Couderc, S.; Garcia, P.; Maillotte, A.M.; Benard, M.; Pinquier, D.; Astruc, D.; Patural, H.; et al. Sequelae of congenital cytomegalovirus following maternal primary infections are limited to those acquired in the first trimester of pregnancy. Clin. Infect. Dis. 2019, 69, 1526–1532. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, J.K.; Sánchez, P.J. Congenital cytomegalovirus infection and hearing loss: It’s time to screen. Otol. Neurotol. 2024, 45, e702–e709. [Google Scholar] [CrossRef] [PubMed]
- Del Valle Penella, A.; Miller, J.; Rochat, R.; Demmler-Harrison, G. Utility of dried blood spots for the diagnosis of congenital cytomegaloviruses within the first 21 days of life in a single center. Int. J. Neonatal. Screen. 2023, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Merav, L.; Ofek Shlomai, N.; Oiknine-Djian, E.; Caplan, O.; Livneh, A.; Sido, T.; Peri, A.; Shtoyer, A.; Amir, E.; Ben Meir, K.; et al. Implementation of pooled saliva tests for universal screening of cCMV infection. Nat. Med. 2024, 30, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Grosse, S.D.; Fleming, P.; Pesch, M.H.; Rawlinson, W.D. Estimates of congenital cytomegalovirus-attributable infant mortality in high-income countries: A review. Rev. Med. Virol. 2024, 34, e2502. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.; Sauve, R.S.; Davies, H.D. Congenital cytomegalovirus infection. J. Natl. Med. Assoc. 2003, 95, 213–218. [Google Scholar] [PubMed]
Figure 1.
Flowchart for screening, diagnosis and treatment of congenital cytomegalovirus infection.
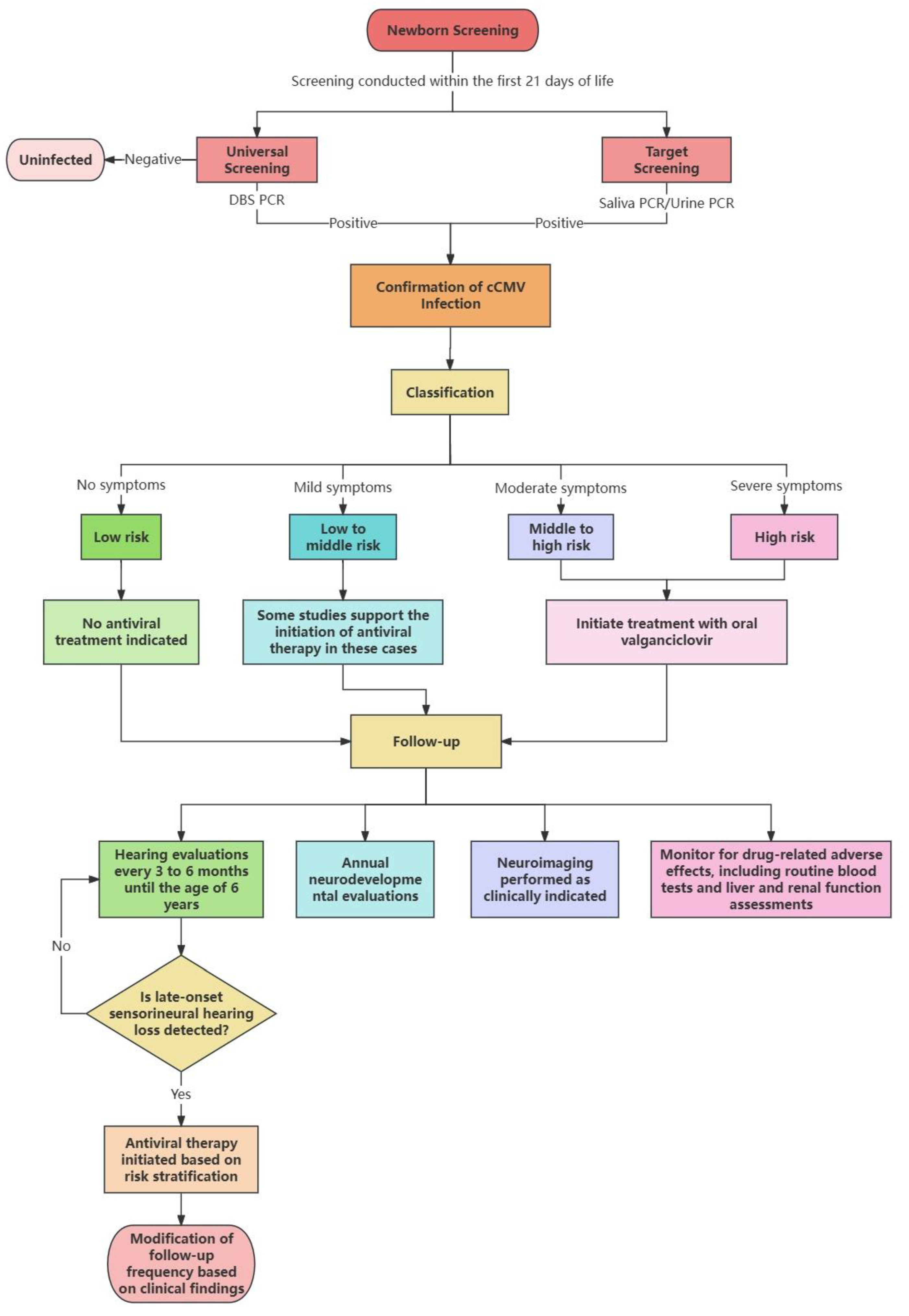

Table 1.
The difference between the 2017 ESPID criteria and recent perspectives.
| Classification Criteria | 2017 ESPID(Luck et al.) | 2024 ECCI(Leruez-Ville et al.)and recent views | Updates/Controversies |
| Severe Disease Definition | ·CNS involvement (microcephaly, neurologic signs, calcifications) ·Life-threatening organ failure ·Bilateral SNHL |
High-risk cCMV: ·Maternal primary infection in 1st trimester ·Severe CNS lesions (ventriculomegaly, cortical malformations on MRI) ·Multisystem involvement |
·Added “maternal primary infection in 1st trimester” as independent risk. ·isolated SNHL reclassified to moderate-risk. |
|
Moderate Disease Definition |
·Persistent laboratory abnormalities (>2 weeks) ·≥2 mild clinical features (e.g., jaundice + hepatosplenomegaly) |
Moderate-risk cCMV: · Isolated SNHL (unilateral/bilateral) · Non-CNS persistent abnormalities (hepatitis, thrombocytopenia) |
·Isolated SNHL now categorized as moderate-risk (previously “severe”). ·lab abnormalities require viral load correlation. |
|
Mild Disease Definition |
·Isolated/transient findings (petechiae, mild hepatomegaly) |
Low-risk cCMV: · Maternal non-primary or 3rd trimester infection · Asymptomatic with normal neuroimaging |
·”Mild disease” category removed. ·asymptomatic infants with normal imaging classified as low-risk (no treatment). |
|
Asymptomatic Infection Definition |
No clinical/laboratory abnormalities |
Expanded to: · Asymptomatic + normal imaging → low-risk · Asymptomatic + minor imaging anomalies → moderate-risk (requires monitoring) |
Controversy: Whether to treat subclinical imaging abnormalities (e.g., white matter changes) remains debated. |
|
Treatment Recommendations |
·Severe/moderate disease: 6-month antiviral therapy ·Mild/asymptomatic: No treatment |
·High-risk: 6-month valganciclovir · Moderate-risk (SNHL): 6-month therapy · Moderate-risk (non-CNS): 6-week therapy · Low-risk: No treatment |
Controversy: Prophylactic treatment for asymptomatic infants with imaging anomalies lacks RCT evidence. |
|
Role of Neuroimaging |
CrUSS (cranial ultrasound) as initial screening; MRI only if abnormalities detected |
Mandatory MRI: · All high/moderate-risk cases · Standardized scoring systems (e.g., white matter grading) |
· Debate: MRI accessibility vs. cost. ·new neuroimaging scoring systems |
|
Maternal Infection Impact |
No distinction between primary/non-primary maternal infections |
Independent risk factor: · Maternal primary infection (especially 1st trimester) → high-risk Non-primary → low or moderate-risk |
·Clear stratification by maternal infection type. · asymptomatic infants with 1st trimester exposure require long-term follow-up. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



