Submitted:
16 July 2025
Posted:
17 July 2025
You are already at the latest version
Abstract
Background/Objectives: Capnography monitoring in the Post-Anesthesia Care Unit (PACU) plays a crucial role in the early detection of respiratory complications, being fundamental for patient safety. It provides objective and continuous data on ventila-tion, enabling timely interventions to optimize health outcomes. This scoping review aims to map the available evidence regarding barriers and facilitators to the use of capnography for respiratory monitoring by nurses in Phase I PACU. Methods: A scoping review was conducted following the methodology proposed by the Joanna Briggs Institute (JBI). The search was performed in the MEDLINE and CINAHL Com-plete databases and the Portuguese Open Access Scientific Repository (RCAAP). Stud-ies in Portuguese, English, and Spanish were included, with no time restrictions. The search strategy combined indexing terms and natural language, adapted to each data-base. Results: Seven studies were included in the sample. The main identified barriers were high workload, perceived lack of patient adherence, and lack of knowledge. Key facilitators included alarm sound, patient education, anticipating patient clinical in-stability, increased nurse confidence, perception of enhanced safety, targeted training for nurses, continuous improvement in care delivery, effective communication and feedback, promotion of sustainable care practices, and prior knowledge and exposure. Conclusions: The use of capnography in the PACU allows for respiratory function as-sessment and early detection of clinical events. Its implementation should be based on current scientific evidence, promoting a culture of safety and quality improvement in patient care.
Keywords:
capnography
; nursing
; post-anesthesia care unit
; respiratory monitoring
1. Introduction
The Post-Anesthesia Care Unit (PACU) is dedicated to the continuous monitoring and care of patients following anesthetic and surgical procedures, aiming to minimize complications and ensure a safe transition to subsequent care units [1,2,3].
Most complications occur within the first five hours after anesthesia [4] and may be surgical, anesthetic, or patient-related origin [5,6]. Phase I of the postoperative period refers to the immediate phase following surgery, during which the patient is transferred to the PACU. The primary goal is to ensure initial recovery from anesthesia and facilitate a safe transition to Phase II, thereby promoting continuity of care [7]. This phase requires close monitoring and specialized interventions to maintain hemodynamic stability, prevent complications, and ensure patient safety [7].
In the PACU, nurses hold a critical role in managing the immediate recovery of patients following anesthesia. Their responsibilities necessitate autonomous clinical monitoring, proficiency in the early identification of complications, and the capacity for prompt decision-making, all underpinned by the advanced specialized knowledge of perioperative nursing [8].
Common respiratory complications during this phase include post-extubation hypoxemia, bronchospasm, atelectasis, acute respiratory failure, pneumothorax, pleural effusion, exacerbation of underlying diseases, and airway obstruction [9,10].
Capnography is a non-invasive, continuous technique that assesses the effectiveness of ventilation [11] and enables early detection of respiratory changes, being more sensitive than pulse oximetry in identifying adverse events [11,12].
Studies show that capnography can detect respiratory adverse events 8 to 11 minutes earlier than conventional monitoring [13], identify more episodes of postoperative respiratory depression compared to oximetry, and is six times more accurate than other methods [14].
While not universally mandatory, the use of capnography is strongly recommended for patients receiving opioid analgesia, individuals with obstructive sleep apnea (OSA), and those requiring supplemental oxygen therapy, due to their increased risk for respiratory complications [15,16,17,18].
Despite its clinical relevance, capnography is not yet widely implemented in PACU [19,20]. Identifying barriers and facilitators can support a more effective and sustained implementation of this monitoring tool in clinical practice, ultimately enhancing patient safety and quality of care.
The methodology employed is a scoping review, following the methodology proposed by JBI. This scoping review aims to map the evidence on barriers and facilitators to the use of capnography for respiratory monitoring by nurses in Phase I PACU.
2. Methods
This scoping review was conducted in accordance with the methodological guidelines established by the Joanna Briggs Institute (JBI) [21]. Advance registration of the review protocol was not undertaken.
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) reporting guidelines [22].
2.1. Identifying the Research Question
The JBI guidelines recommend employing the Population/Concept/Context (PCC) framework to guide the formulation of review questions (see Table 1).
The review question was: “What are the barriers and facilitators to the use of capnography for respiratory monitoring by nurses in Phase I PACU?”.
2.2. Identifying Relevant Studies
The literature search was conducted in MEDLINE (via PubMed), CINAHL Complete (via EBSCOhost), and Portuguese Open Access Scientific Repository (RCAAP). Search terms included: nurs*, capno*, "respiratory monitoring", "carbon dioxide", "end tidal carbon dioxide", "respiratory assessment", "respiratory complications", "postanesthesia", "recovery", "postoperative", PACU, "post anesthesia care unit", and "immediate postoperative". These were combined with specific Medical Subject Headings (MeSH) and CINAHL Subject Headings for each respective database, as detailed in Appendix A (see Table A1, Table A2 and Table A3). The search was conducted on January 2024.
2.3. Study Selection
Inclusion and exclusion criteria were based on population, concept, and context. Studies that included nurses—irrespective of their area of specialization—or multidisciplinary teams involving nurses were considered for inclusion. To be eligible, studies were required to focus on respiratory monitoring using capnography, addressing relevant barriers, facilitators, challenges, and limiting factors. Only studies conducted in perioperative settings involving adult patients (aged 18 and older) within Phase I PACU environments, defined as the immediate postoperative period, were included. Studies limited to preoperative or exclusively intraoperative contexts were excluded.
Only studies published in Portuguese, English, or Spanish were included, as these were the languages spoken by the reviewers. No time restrictions were applied.
All results from the different databases were exported to Rayyan QCRI (Qatar Computing Research Institute), where duplicates records were removed. A blinded and independent screening of titles and abstracts was conducted in duplicate by two reviewers (A.A. and L.C.) on January 18, 2024 to apply inclusion criteria.
Disagreements between reviewers were resolved through consultation with a third reviewer, ensuring impartiality and consensus. The third reviewer was not directly involved in the development of the manuscript and therefore is not listed as an author. However, they exclusively contributed by mediating decisions during the study selection process. The reviewers have academic training and clinical experience in post-anesthesia care, ensuring familiarity with the topic under study, and declared no conflicts of interest related to the included studies or the review topic.
Full texts of potentially eligible studies were obtained and analyzed in detail. Reference lists of included studies were also reviewed to identify additional relevant literature. Although a formal blinded review of full texts was not implemented, the combination of independent duplicate review with mediation by a third reviewer was adopted to minimize the risk of bias and increase the reliability of the process.
2.4. Data Extraction and Comprehensive Analysis
Data from the included studies were independently extracted by two reviewers using a customized data extraction matrix, which included: author, year of publication, title, country, study design, objectives, participants, setting, and main findings related to the barriers and facilitators of capnography use.
In this study, barriers are defined as factors that limit, hinder, or negatively affect the effective use of capnography for respiratory monitoring by nurses in Phase I of the PACU. Facilitators are elements that help promote or facilitate the use of capnography. Barriers and facilitators are essential factors influencing the implementation process of healthcare practices [23].
2.5. Reporting the Results
The results are summarized and presented in a tabular form aligned with the objective of this scoping review. A narrative summary accompanies the tables and describes how the findings relate to the review’s objective and question.
3. Results
The results of the search and article selection process are presented using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart, adapted for scoping reviews.
Figure 1.
PRISMA Flow Diagram for study selection.
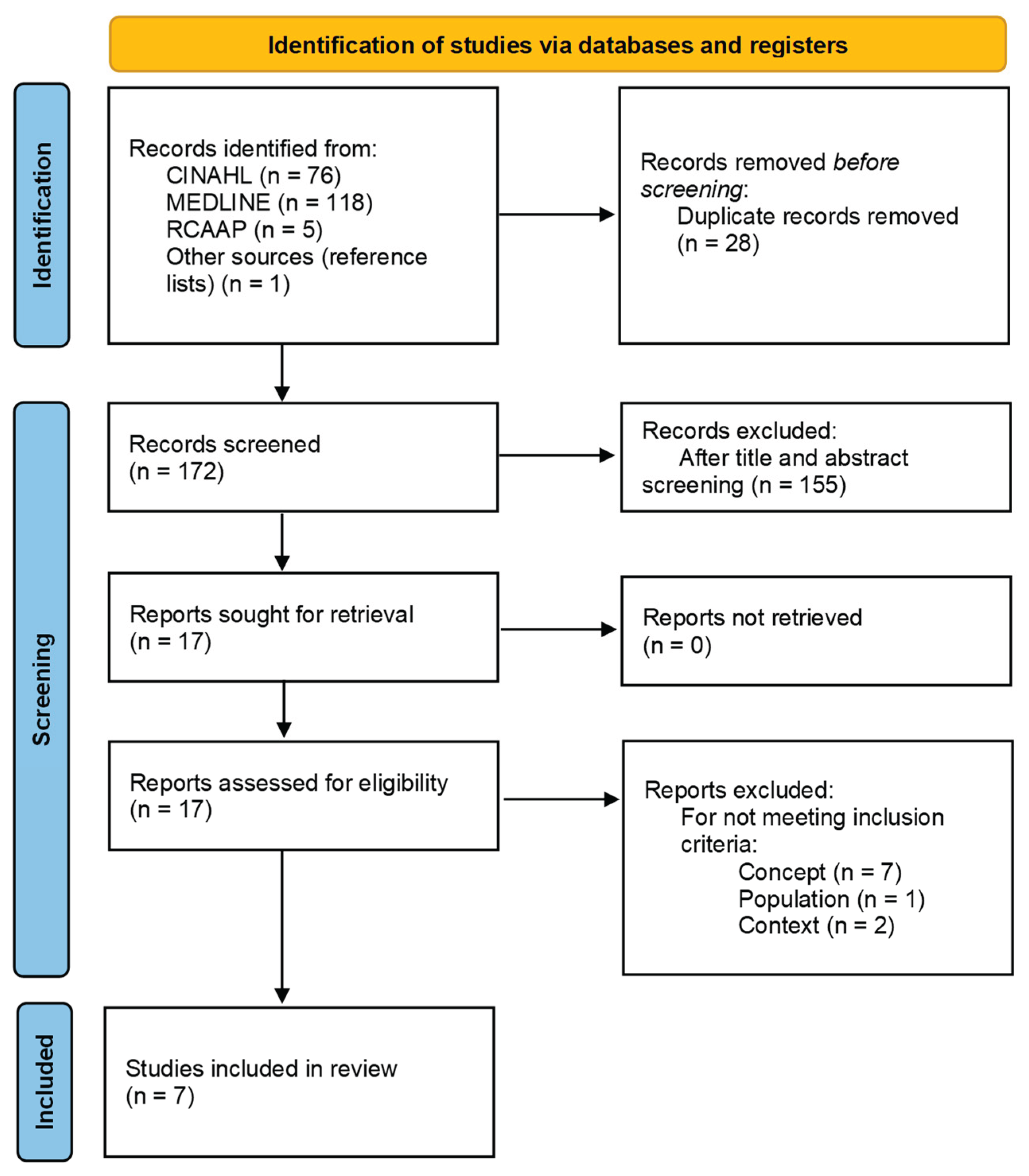
The search process initially identified 200 articles. Of these, 28 were excluded as duplicates, leaving 172 articles for title and abstract screening. From these, 155 were excluded. After full-text reading of the remaining 17 eligible articles and applying the inclusion criteria, seven articles were included in the review.
Table B1, presented in Appendix B, contains the data extracted from the studies included in this scoping review, based on the customized data extraction matrix developed for this purpose. Table 2 provides a summary of the barriers and facilitators identified in each study regarding the use of capnography for respiratory monitoring by nurses in Phase I PACU.
The analysis of the seven studies included in this scoping review allowed the identification of a set of barriers and facilitators to the use of capnography for respiratory monitoring by nurses in Phase I of the PACU.
Among the identified barriers, high workload stands out, as nurses reported difficulties integrating capnography into daily practice due to competing demands, especially in the demanding PACU context, which can limit time and attention devoted to capnography monitoring [24]. Additionally, the perceived lack of patient adherence, caused by patients’ difficulties in complying with device use (e.g., keeping nasal cannulas in place) may discourage consistent monitoring [24,26,27]. Finally, lack of knowledge, manifested as limited understanding of the interpretation and application of capnography by nurses, constitutes a significant obstacle to its effective use [26,27].
Among the facilitators for the use of capnography, alarm sound plays a key role by enhancing vigilance and prompting timely interventions [24]. Patient education promotes adherence to capnography through patient instruction supporting successful monitoring and improving patients’ compliance with device use [24,26]. Nurses who anticipate patient clinical instability by using capnography to proactively identify deterioration perceive it as a valuable clinical tool [24,25,26,28]. Increased nurse confidence, gained through familiarity with the technology, boosts willingness to apply it in clinical practice [25,28]. The perception of enhanced safety leads nurses to associate capnography with increased patient safety [19,25,26,28,29]. Targeted nurse training equips professionals with the skills to interpret capnographic data and respond appropriately, with nurses receiving specific training demonstrating greater adherence to its use [19,25,27,28,29].
The integration of capnography supports continuous improvement in care delivery, aligning with broader goals of care optimization and innovation [28]. Effective communication and feedback, including sharing monitoring data and patient outcomes, strengthen interprofessional collaboration and reinforce capnography’s integration into practice [28]. Additionally, capnography promotes sustainable practices by supporting efficiency and resource stewardship in clinical settings, enabling early interventions, minimizing complications, and optimizing resources [28]. Finally, prior knowledge and exposure to capnography positively influence its adoption and routine use [29].
Table 3 provides a summary of the identified categories and the contributions of the seven included studies.
Discussion
This review synthesized current evidence from selected sources on the use of capnography by nurses in the Phase I PACU, identifying key barriers and facilitators that influence its implementation for respiratory monitoring. The findings highlight a complex interplay between individual, clinical, and organizational factors that shape nursing practice. While capnography is widely recognized for enhancing patient safety and enabling early detection of respiratory compromise, its consistent application is influenced by nurses’ knowledge, workload, perceived patient cooperation, and institutional support. These insights underscore the need for targeted interventions—such as structured training, communication strategies, and system-level support—to optimize the use of capnography and strengthen postoperative care quality.
The immediate postoperative period is a critical phase during which nurses must remain vigilant for respiratory events and early signs of respiratory depression such as tachycardia, drowsiness, or altered consciousness [30]. While opioid administration is a common cause of respiratory depression, other factors such as OSA also contribute, making capnography a more sensitive and accurate monitoring tool compared to pulse oximetry or respiratory rate evaluation [24,25]. Continuous, objective capnographic monitoring enables nurses to anticipate respiratory instability, thus preventing complications through early intervention [24,25,26,28]. The ongoing analysis of capnography data supports dynamic clinical decision-making, reinforcing the need for care plans to be regularly updated with timely, evidence-based interventions [19,27].
A prominent barrier identified is the lack of knowledge and training among PACU nurses regarding capnography interpretation and application. Many nurses report unfamiliarity with the technology and its clinical significance, which limits its integration into routine practice [27]. Consequently, structured and continuous education is essential for building the competencies required to interpret capnography accurately and make informed clinical decisions [19,24,28]. Targeted training not only enhances technical skills but also increases nurses’ confidence, which is pivotal for fostering critical thinking and clinical reasoning necessary for effective respiratory monitoring [25,28,29]. The implementation of standardized protocols and guidelines can further support nurses, providing a consistent framework for capnography use and facilitating evidence-based practice [19,32].
Beyond individual competencies, the role of healthcare organizations, leadership, and institutional culture is fundamental in supporting capnography adoption. Organizational support through policy development, resource allocation, and integration of monitoring protocols creates an enabling environment for nurses to utilize capnography effectively [32]. Leadership commitment is crucial for promoting a safety culture that prioritizes respiratory monitoring and encourages the uptake of new technologies. The presence of clinical champions and continuous quality improvement initiatives, such as audit and feedback cycles, fosters accountability and reinforces practice standards [25,28]. Effective communication within the healthcare team ensures shared understanding and alignment in respiratory monitoring practices, which is vital for cohesive and timely patient care.
The PACU is a multidisciplinary environment where collaboration between nurses, anesthesiologists, respiratory therapists, and other professionals influences the implementation of capnography. Interprofessional dynamics can either facilitate or hinder the consistent use of capnography, depending on the clarity of roles, mutual respect, and communication pathways. Encouraging collaborative decision-making and open dialogue enhances the acceptance of capnography data in clinical judgments and fosters coordinated responses to respiratory deterioration [25,28]. Feedback mechanisms that include the entire care team contribute to a shared responsibility for patient safety and promote continuous learning.
Patient-related barriers such as non-adherence due to discomfort from nasal cannulas or distress caused by alarm sounds present challenges to effective monitoring [24,25,27]. Patient education is therefore a critical facilitator, helping patients understand the importance of capnography and improving cooperation with device use [24]. Alarm fatigue among healthcare professionals is another significant concern; excessive or false alarms may desensitize nurses and delay responses, thereby compromising patient safety [31,32]. Strategies to optimize alarm settings and minimize unnecessary alerts, coupled with ongoing staff training, are essential to mitigate this issue.
The review underscores the necessity of developing specific competencies in capnography interpretation, clinical decision-making, and patient communication. Nursing education programs and continuing professional development should incorporate these components to prepare nurses for enhanced respiratory monitoring roles. Healthcare organizations must actively foster a culture that values innovation, supports training initiatives, and facilitates interprofessional collaboration to embed capnography into standard PACU care.
Future research should explore the impact of leadership styles, institutional policies, and team dynamics on capnography implementation. Additionally, evaluating the effectiveness of tailored educational interventions and protocol-driven care pathways will provide further evidence to optimize respiratory monitoring strategies.
5. Conclusions
The findings from this scoping review have successfully addressed the research question, underscoring the critical role of integrating capnography into Phase I PACU for respiratory monitoring. By mapping the barriers and facilitators associated with capnography use, this review provides valuable insights into how facilitators can be strengthened and barriers reduced.
Although barriers such as limited knowledge, high workload, and the perceived lack of patient adherence were identified, several facilitators also emerged, including specific nurse training, prior experience with capnography, the ability to anticipate clinical deterioration, and the perception of increased safety in care delivery.
The findings of this scoping review show that capnography, when used alongside other monitoring methods, is recognized by nurses as a fundamental tool for the early detection of respiratory complications, reinforcing its relevance in promoting patient safety. Moreover, institutional factors such as effective interprofessional communication, continuous quality improvement projects, regular audits and feedback, as well as the reinforcement of nurses’ knowledge through ongoing education based on current scientific evidence, are key elements in consolidating its practical application in the PACU.
This study provides an innovative contribution to understanding the factors that influence nurses’ adoption of capnography in Phase I PACU, offering valuable guidance for future interventions in nursing clinical practice and the development of health policies.
The primary limitations of this scoping review include the limited number of databases consulted and the language restrictions, which may have impacted the breadth of the evidence identified.
Author Contributions
Conceptualization, A.A. and L.C.; methodology, A.A. and L.C.; software, A.A. and L.C.; validation, A.A. and L.C.; formal analysis, L.C.; investigation, A.A.; data curation, A.A.; writing— original draft preparation, A.A.; writing—review and editing, L.C.; visualization, A.A.; supervision, L.C.; project administration, A.A. and L.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Public Involvement Statement
No public involvement in any aspect of this research.
Guidelines and Standards Statement
This manuscript was drafted in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guideline for systematic review research.
Use of Artificial Intelligence
AI or AI-assisted tools were not used in drafting any aspect of this manuscript.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PACU JBI RCAAP OSA PRISMA-ScR PCC QCRI PRISMA PCA etCO2 USA |
Post-Anesthesia Care Unit Joanna Briggs Institute Open Access Scientific Repositories of Portugal Obstructive Sleep Apnea Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews Population/Concept/Context Qatar Computing Research Institute Preferred Reporting Items for Systematic Reviews e Meta-Analyses Patient Controlled-Analgesia End-tidal Carbon Dioxide Concentration United States of America |
Appendix A. Search Strategy

Table A1.
Search strategy – MEDLINE (PubMed) - search performed on January 12, 2024.
| Search | Search terms | Results |
|---|---|---|
| #1 | nurs*[Title/Abstract] | 546,738 |
| #2 | "Postanesthesia Nursing"[MeSH Terms] OR "Nurses"[MeSH Terms] OR "Nursing"[MeSH Terms] | 338,351 |
| #3 | "nurs*"[Title/Abstract] OR "Postanesthesia Nursing"[MeSH Terms] OR "Nurses"[MeSH Terms] OR "Nursing"[MeSH Terms] | 696,705 |
| #4 | "capno*"[Title/Abstract] OR "respiratory monitoring"[Title/Abstract] OR "carbon dioxide"[Title/Abstract] OR "end tidal carbon dioxide"[Title/Abstract] OR "respiratory assessment"[Title/Abstract] OR "respiratory complications"[Title/Abstract] | 76,533 |
| #5 | "Capnography"[MeSH Terms] OR "blood gas monitoring, transcutaneous"[MeSH Terms] OR "Carbon Dioxide"[MeSH Terms] OR "Pulmonary Ventilation"[MeSH Terms] OR "signs and symptoms, respiratory"[MeSH Terms] | 322,554 |
| #6 | "capno*"[Title/Abstract] OR "respiratory monitoring"[Title/Abstract] OR "Carbon Dioxide"[Title/Abstract] OR "end tidal carbon dioxide"[Title/Abstract] OR "respiratory assessment"[Title/Abstract] OR "respiratory complications"[Title/Abstract] OR "Capnography"[MeSH Terms] OR "blood gas monitoring, transcutaneous"[MeSH Terms] OR "Carbon Dioxide"[MeSH Terms] OR "Pulmonary Ventilation"[MeSH Terms] OR "signs and symptoms, respiratory"[MeSH Terms] | 366,211 |
| #7 | "Postanesthesia"[Title/Abstract] OR "Recovery"[Title/Abstract] OR "Postoperative"[Title/Abstract] OR "PACU"[Title/Abstract] OR "Post anesthesia care unit"[Title/Abstract] OR "Immediate postoperative"[Title/Abstract] | 1,188,357 |
| #8 | "Postoperative Period"[MeSH Terms] OR "Postoperative Care"[MeSH Terms] OR "Recovery Room"[MeSH Terms] | 122,244 |
| #9 | "Postanesthesia"[Title/Abstract] OR "Recovery"[Title/Abstract] OR "Postoperative"[Title/Abstract] OR "PACU"[Title/Abstract] OR "Post anesthesia care unit"[Title/Abstract] OR "Immediate postoperative"[Title/Abstract] OR "Postoperative Period"[MeSH Terms] OR "Postoperative Care"[MeSH Terms] OR "Recovery Room"[MeSH Terms] | 1,244,717 |
| #10 | ("nurs*"[Title/Abstract] OR ("Postanesthesia Nursing"[MeSH Terms] OR "Nurses"[MeSH Terms] OR "Nursing"[MeSH Terms])) AND ("capno*"[Title/Abstract] OR "respiratory monitoring"[Title/Abstract] OR "Carbon Dioxide"[Title/Abstract] OR "end tidal carbon dioxide"[Title/Abstract] OR "respiratory assessment"[Title/Abstract] OR "respiratory complications"[Title/Abstract] OR ("Capnography"[MeSH Terms] OR "blood gas monitoring, transcutaneous"[MeSH Terms] OR "Carbon Dioxide"[MeSH Terms] OR "Pulmonary Ventilation"[MeSH Terms] OR "signs and symptoms, respiratory"[MeSH Terms])) AND ("Postanesthesia"[Title/Abstract] OR "Recovery"[Title/Abstract] OR "Postoperative"[Title/Abstract] OR "PACU"[Title/Abstract] OR "Post anesthesia care unit"[Title/Abstract] OR "Immediate postoperative"[Title/Abstract] OR ("Postoperative Period"[MeSH Terms] OR "Postoperative Care"[MeSH Terms] OR "Recovery Room"[MeSH Terms])) | 277 |
| #11 | #10 FILTERS: English, Portuguese, Spanish |
255 |
| #12 | #10 FILTERS: English, Portuguese, Spanish; Adult: 19+ years |
118 |
Table A2.
Search strategy – CINAHL (EBSCOhost) - search performed on January 12, 2024.
| Search | Search terms | Results |
|---|---|---|
| S1 | TI nurs* OR AB nurs* | 624,190 |
| S2 | (MH "Nurses+") OR (MH "Perianesthesia Nursing") OR (MH "Perioperative Nursing") | 254,721 |
| S3 | S1 OR S2 | 719,008 |
| S4 | TI capno* OR AB capno* OR TI “respiratory monitoring” OR AB “Respiratory monitoring” OR TI “carbon dioxide” OR AB “carbon dioxide” OR TI “end tidal carbon dioxide” OR AB “end tidal carbon dioxide” OR TI “respiratory assessment” OR AB “respiratory assessment” OR TI “respiratory complications” OR AB “respiratory complications” | 9,641 |
| S5 | (MH "Capnography") OR (MH "Carbon Dioxide") OR (MH "Signs and Symptoms, Respiratory+") OR (MH "Blood Gas Monitoring, Transcutaneous") | 44,729 |
| S6 | S4 OR S5 | 50,121 |
| S7 | TI “postanesthesia” OR AB “postanesthesia” OR TI “recovery” OR AB “recovery” OR TI “postoperative” OR AB “postoperative” OR TI PACU OR AB PACU OR TI “post anesthesia care unit” OR AB “post anesthesia care unit” OR TI “immediate postoperative” OR AB “immediate postoperative” | 212,894 |
| S8 | (MH "Post Anesthesia Care Units") OR (MH "Post Anesthesia Care") OR (MH "Postoperative Care") OR (MH "Anesthesia Recovery") OR (MH "Postoperative Period") | 42,008 |
| S9 | S7 OR S8 | 234,949 |
| S10 | S3 AND S6 AND S9 | 205 |
| S11 | S10 (Limited to English, Portuguese, and Spanish languages) | 197 |
| S12 | S10 (Limited to English, Portuguese, and Spanish languages; age group: all adults) | 74 |
Table A3.
Search strategy – RCAAP - search performed on January 20, 2024.
| Search | Search terms | Results |
|---|---|---|
| 1 | capnografia AND enfermagem | 5 |
Appendix B. Data Extraction from the Studies
Table B1.
Data extraction from the studies included in the scoping review.
| Study | Reference Number, First Author’s Surname, Year of Publication, Country | Type of study | Objetive(s) | Population | Context | Concept (Barriers and Facilitators use of capnography for respiratory monitoring by nurses in Phase I PACU) |
|---|---|---|---|---|---|---|
| S1 | [24] Hutchison et al. (2008), United States of America (USA) | Randomized prospective study | Determine whether capnography used in isolation is more sensitive than pulse oximetry (with assessment of respiratory rate through observation or auscultation) | 54 adult patients following orthopedic surgery, monitored for respiratory depression using capnography by nurses | PACU and general nursing care unit |
Barriers: - Capnography requires more time from professionals to be implemented; - Nurses perceived greater difficulty in patient adherence due to limitations in daily activities, such as walking in the postoperative period. Facilitators: - Educating patients to facilitate their adherence to monitoring (for example, about the importance of the cannula and the meaning of the alarms); - The alarm produced by the capnography monitor led to a quicker response from nurses; - Allowed early identification of changes in respiratory function. |
| S2 | [25] McCarter et al. (2008), USA | Quantitative, descriptive, cross-sectional study | Evaluate the effectiveness of monitoring in the postoperative period in patients with opioid PCA | 634 adult postoperative patients receiving PCA with opioids, monitored with capnography by nurses | Postoperative period (Phase I and Phase II) |
Facilitators: - Increased nurse awareness of respiratory changes; - Increased effectiveness of nursing interventions to minimize respiratory discomfort related to PCA; - Increased nurse confidence due to effective monitoring; - Quick response from the team to prevent serious consequences; - Increased perceived patient safety during this period. |
| S3 | [26] Lakdawala et al. (2017), USA | Quality improvement project | Assess patients using the STOP-Bang screening tool; Compare high-risk and low-risk groups with respect to respiratory complications; Use and evaluate capnography in the postoperative period; Evaluate nurses' perception of the OSA care protocol; Assess patient satisfaction with the OSA care protocol. |
161 adult neuro-surgical patients screened for OSA using STOP-Bang, monitored with capnography by nurses | Preoperative unit, PACU, and neuro-surgery unit |
Barriers: - Nurses observed greater patient resistance to adherence to capnography devices due to discomfort caused by the cannula and the nuisance of the alarm; - Nurses needed more knowledge about problem-solving methods related to the use of capnography in patients with OSA, to improve interpretation skills and response to each situation, as well as the indications for capnography and monitoring techniques. Facilitators: - Capnography proved to identify early signs of respiratory depression (such as apnea and snoring episodes), allowing for quick intervention; - Need to educate patients on the importance of using the device to ensure safety, raising awareness about the significance of monitoring, promoting adherence. |
| S4 | [27] Jungquist et al. (2019), USA | Prospective observational study | Explore the effectiveness of using pulse oximetry, capnography, and minute ventilation to identify and anticipate opioid-induced respiratory depression in the post-anesthesia period | 60 adult patients in PACU after spine, neck, hip, or knee surgery, monitored by nurses for opioid-induced respiratory depression | PACU |
Barriers: - Nurses' perception of patient non-adherence, related to discomfort, mask removal for nursing care, and other activities like eating and speaking; - Need for nurse training to instigate a change in the monitoring paradigm, reflecting limited knowledge of the technique and indications for capnography. |
| S5 | [28] Scully (2019), USA | Quality im-provement project (with mixed method) | Identify undiagnosed and high-risk patients with OSA in the preoperative period using the STOP-Bang screening tool; Train PACU nurses to recognize hypoventilation through capnography and intervene to prevent respiratory complications; Implement Practice Recommendation number 10 from |
314 adult patients diagnosed with OSA, monitored by multidisciplinary team | PACU |
Facilitators: - Training for professionals (introduction to capnography and monitoring); - Increased confidence in using capnography helped stimulate critical thinking (by applying it to other patients beyond the OSA population); - Improvement in care quality and patient safety are driving forces behind change; - Regular communication of results (via audit) motivated the team and promoted the implementation process; |
| the American Society of PeriAnesthesia Nurses (screening for OSA and monitoring of etCO2 in patients with OSA) | - Promoting sustainability by involving training and raising nurse awareness to provide the best care, integrating capnography monitoring into clinical practice; - Allowed the nurse to intervene before respiratory complications occurred. |
|||||
| S6 | [29] Atherton et al. (2022), USA | Quantitative, descriptive-correlational, and longitudinal study | Evaluate the effectiveness of an educational program on ventilatory patterns using devices that assess dioxid carbon levels in postoperative patients | 176 nurses | PACU |
Facilitators: - After the educational program, nurses reported greater confidence and consequent security in using etCO2 and transcutaneous carbon dioxide monitoring and interpreting the values; - Prior knowledge and training with etCO2 monitoring. |
| S7 | [19] Potvin et al. (2022), France | Randomized, controlled, prospective study | Study the rate of patients with alveolar hypoventilation before tracheal extubation or removal of the laryngeal mask through continuous capnography monitoring in the PACU | 52 adult patients with endotracheal tube orlaryngeal mask, monitored by nurses | PACU |
Facilitators: - Nurse training facilitated the accurate interpretation of capnography results and the overall layout of monitoring systems; - Training should be coupled with a standardized respiratory monitory protocol to ensure effective use of capnography; - Standard monitoring, together with capnography, can improve patient safety by providing a comprehensive assessment of respiratory function, allowing early detection of respiratory complications. |
References
- Ganter, M.T.; Blumenthal, S.; Dübendorfer, S.; Brunnschweiler, S.; Hofer, T.; Klaghofer, R.; Zollinger, A.; Hofer, C. The length of stay in the post-anaesthesia care unit correlates with pain intensity, nausea and vomiting on arrival. Perioper Med. 2014, 3, 1–9. [CrossRef]
- Mourão, J.; Pereira, L.; Alves, C.; Andrade, N.; Cadilha, S.; Perdigão, L. Indicadores de segurança e qualidade em anestesiologia. Rev. Soc. Port. Anestesiol. 2018, 27, 23–27. [CrossRef]
- Jaensson, M.; Nilsson, U.; Dahlberg, K. Methods and timing in the assessment of postoperative recovery: a scoping review. Br. J. Anaesth. 2022, 129, 92–103. [CrossRef]
- Mert, S. The significance of nursing care in the post-anesthesia care unit and barriers to care. Intensive Care Res. 2023, 3, 272-281. [CrossRef]
- Karcz, M.; Papadakos, P.J. Respiratory complications in the postanesthesia care unit: A review of pathophysiological mechanisms. Can J Respir Ther. 2013, 49, 21-29. Available from: https://pubmed.ncbi.nlm.nih.gov/26078599/.
- Sampaio, A.; Bernardino, A.; Campos, A.C.; Eufrásio, A.; Almeida, A.L.; Raimundo, A.; et al. Manual de cuidados pós-anestésicos, 2017. Available from: https://core.ac.uk/download/pdf/84995558.pdf.
- Clifford, T.L. Phase I and phase II recovery. In Perianesthesia nursing care: A bedside guide for safe recovery; Stannard, D., Krenzischek, D., Duarte, O., Martins, O., Eds.; Jones & Bartlett Learning, 2016, pp. 19-22. Available from: https://books.google.pt/books?hl=pt-PT&lr=&id=2hzrDAAAQBAJ&oi=fnd&pg=PA19&dq=phase+I+and+phase+II+recovery+clifford&ots=El0k6Q2nLC&sig=DfKr7iEIBVYlcfG0eEIYijXSRTo&redir_esc=y#v=onepage&q=phase%20I%20and%20phase%20II%20recovery%20clifford&f=false.
- Dahlberg, K.; Brady, J.M.; Jaensson, M.; Nilsson, U.; Odom-Forren, J. Education, competence, and role of the nurse working in the PACU: An international survey. J Perianesth Nurs. 2021, 36, 224-331. [CrossRef]
- Eikermann, M.; Santer, P.; Ramachandran, S.K.; Pandit, J. Recent advances in understanding and managing postoperative respiratory problems. F1000Res. 2019, 8, 197. [CrossRef]
- Chandler, D.; Mosieri, C.; Kallurkar, A.; Pham, A.D.; Okada, L.K.; Kaye, R.J.; Cornett, E.M.; Fox, C.J.; Urman, R.D.; Kaye, A.D. Perioperative strategies for the reduction of postoperative pulmonary complications. Best Pract Res Clin Anaesthesiol. 2020, 34, 153-166. [CrossRef]
- Fink, R.J.; Mark J.B. Monitoração anestésica padrão e dispositivos. In Fundamentos de anestesiologia clínica; Barash, P.; Cullen, B.; Stoelting, R.; Cahalan, M.; Stock, M.; Ortega, R.; et al., Eds. Artmed Editora, Porto Alegre, 2017, pp. 277-297. Available from: https://books.google.pt/books?hl=pt-PT&lr=&id=LRcuDwAAQBAJ&oi=fnd&pg=PR1&dq=livro+anestesiologia+clinica&ots=6As0nnIfEP&sig=LUuMxn1tGjatPzupHHzcM36NvC4&redir_esc=y#v=onepage&q=livro%20anestesiologia%20clinica&f=false.
- Kerslake, I.; Kelly, F. Uses of capnography in the critical care unit. BJA Educ. 2017, 17, 178-183. [CrossRef]
- Chung, F.; Wong, J.; Mestek, M.L.; Niebel, K.H.; Lichtenthal, P. Characterization of respiratory compromise and the potential clinical utility of capnography in the post anesthesia care unit: a blinded observational trial. J Clin Monit Comput. 2020, 34, 541-551. [CrossRef]
- Lam, T.; Nagappa, M.; Wong, J.; Singh, M.; Wong, D.; Chung, F. Continuous pulse oximetry and capnography monitoring for postoperative respiratory depression and adverse events: A systematic review and meta-analysis. Anesth Analg. 2017, 125, 2019-2029. [CrossRef]
- Medtronic. Clinical society guidelines for Capnography monitoring, 2019. Available from: https://asiapac.medtronic.com/content/dam/covidien/library/emea/en/product/capnography-monitoring/18-emea-cs-guidelines-for-capnography-2922293.pdf.
- Royal College of Anaesthetists. Chapter 4: Guidelines for the provision of anaesthetic services for postoperative care 2019. GPAS Editorial, 2019. Available from: https://www.rcoa.ac.uk/sites/default/files/documents/2020-02/GPAS-2019-04POSTOP.pdf.
- Broens, S.; Prins, S.; Kleer, D.; Niesters, M.; Dahan, A.; Velzen, M. Postoperative respiratory state assessment using the integrated pulmonary index (IPI) and resultant nurse interventions in the post-anesthesia care unit: A randomized controlled trial. J Clin Monit Comput. 2021, 35, 1093-1102. [CrossRef]
- Wilks, C.; Foran, P. Capnography monitoring in the post anaesthesia care unit (PACU). J Perioper Nurs. 2021, 34, 29-35. [CrossRef]
- Potvin, J.; Etchebarne, I.; Soubiron, L.; Biais, M.; Roullet, S.; Nouette-Gaulain, K. Effects of capnometry monitoring during recovery in the post-anaesthesia care unit: a randomized controlled trial in adults (CAPNOSSPI). J Clin Monit Comput. 2022, 36, 379-385. [CrossRef]
- Wollner, E.; Nourian, M.M.; Booth, W.; Conover, S.; Law, T.; Lilaonitkul, M.; Gelb, A.W.; Lipnick, M.S. Impact of capnography on patient safety in high-and low-income settings: A scoping review. Br J Anaesth. 2020, 125, 88-103. [CrossRef]
- Peters, M.D.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping reviews (2020 version). In JBI manual for evidence synthesis; Aromatis, E.; Munn, Z., Eds. 2020. [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Int. Med. 2018, 169, 467–473. [CrossRef]
- Nilsen, P. Making sense of implementation theories, models and frameworks. Implementation Sci. 2015, 53, 1-13. [CrossRef]
- Hutchison, R.; Rodriguez, L. Capnography and respiratory depression. Am J Nurs. 2008, 108, 35-39. [CrossRef]
- McCarter, T.; Shaik, Z.; Scarfo, K.; Thompson, L.J. Capnography monitoring enhances safety of postoperative patient-controlled analgesia. Am Health Drug Benefits. 2008, 1, 28-35. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4115301/.
- Lakdawala, L.; Dickey, B.; Alrawashdeh, M. Obstructive sleep apnea screening among surgical patients: A quality improvement project. J Perianesth Nurs. 2018, 33, 814-821. [CrossRef]
- Jungquist, C.R.; Chandola, V.; Spulecki, C.; Nguyen, K.V.; Crescenzi, P.; Tekeste, D.; Sayapaneni, P.R. Identifying patients experiencing opioid-induced respiratory depression during recovery from anesthesia: The application of electronic monitoring devices. Worldviews Evid Based Nurs. 2019, 16, 186-194. [CrossRef]
- Scully, K.R.; Rickerby, J.; Dunn, J. Implementation science: Incorporating obstructive sleep apnea screening and capnography into everyday practice. J Perianesth Nurs. 2020, 35, 7-16. [CrossRef]
- Atherton, P.; Jungquist, C.; Spulecki, C. An educational intervention to improve comfort with applying and interpreting transcutaneous CO2 and end-tidal CO2 monitoring in PACU. J Perianesth Nurs. 2022, 37, 781-786. [CrossRef]
- Sajith, B. Respiratory depression: A case study of a postoperative patient with cancer. Clin J Oncol Nurs. 2018, 22, 453-456. [CrossRef]
- Ruskin, K.J.; Bliss, J.P. Alarm fatigue and patient safety. Anesth Patient Saf Found. 2019, 34, 1-6. Available from: https://www.apsf.org/article/alarm-fatigue-and-patient-safety/.
- Oliveira, A.E.C.; Machado, A.B.; Santos, E.D.; Almeida, E.B. Fadiga de alarmes e as implicações para a segurança do paciente. Rev Bras Enferm. 2018, 71, 3211-3216. [CrossRef]
Table 1.
Application of the PCC Framework for the Scoping Review.
| Description | |
|---|---|
| Population | Nurses |
| Concept | Barriers and facilitators to the use of capnography for respiratory monitoring |
| Context | Phase I PACU |
Table 2.
Data extraction from the studies included in the scoping review based on the PCC.
| Reference Number | First Author’s Surname, Year of Publication | Population | Context | Concept (Barriers and Facilitators use of capnography for respiratory monitoring by nurses in Phase I PACU) |
|---|---|---|---|---|
| [24] | Hutchison et al. (2008) | 54 adult patients following orthopedic surgery, monitored for respiratory depression using capnography by nurses | PACU and general nursing care unit |
Barriers: - Capnography requires more time from professionals to be implemented; - Nurses perceived greater difficulty in patient adherence due to limitations in daily activities. Facilitators: - Educating patients to facilitate their adherence to monitoring; - The alarm produced by the capnography monitor led to a quicker response from nurses; - Allowed early identification of changes in respiratory function. |
| [25] | McCarter et al. (2008) | 634 adult postoperative patients receiving Patient Controlled-Analgesia (PCA), monitored with capnography by nurses | Postoperative period (Phase I and Phase II) |
Facilitators: - Increased nurse awareness of respiratory changes; - Increased effectiveness of nursing interventions to minimize respiratory discomfort related to PCA; - Increased nurse confidence due to effective monitoring; - Quick response from the team to prevent serious consequences; - Increased perceived patient safety during this period. |
| [26] | Lakdawala et al. (2017) | 161 adult neuro-surgical patients screened for OSA using STOP-Bang, monitored with capnography by nurses | Preoperative unit, PACU, and neuro-surgery unit |
Barriers: - Nurses observed greater patient resistance to adherence to capnography devices; - Nurses reported the need for increased knowledge on the use of capnography in patients with OSA. Facilitators: - Capnography proved to identify early signs of respiratory depression, allowing for quick intervention; - Need to educate patients on the importance of using the device to ensure safety and promote adherence. |
| [27] | Jungquist et al. (2019) | 60 adult patients in PACU after spine, neck, hip, or knee surgery, monitored by nurses for opioid-induced respiratory depression | PACU |
Barriers: - Nurses' perception of patient non-adherence, related to discomfort and mask removal for nursing care. - Need for nurse training due to limited knowledge of the technique and indications for capnography. |
| [28] | Scully (2019) | 314 adult patients diagnosed with OSA, monitored by multidisciplinary team | PACU |
Facilitators: - Training for professionals (introduction to capnography and monitoring); - Increased confidence in using capnography helped stimulate critical thinking (by applying it to other patients beyond the OSA population); - Improvement in care quality and patient safety drive change; - Regular communication of results (via audit) motivated the team and promoted the implementation process; - Promoting sustainability by involving training and raising nurse awareness to provide better care, integrating capnography monitoring into clinical practice; - Allowed the nurse to intervene early to prevent respiratory complications. |
| [29] | Atherton et al. (2022) | 176 nurses | PACU |
Facilitators: - The educational program increased nurses’ confidence and competence in using End-tidal Carbon Dioxide Concentration (etCO2) and transcutaneous carbon dioxide monitoring; - Prior knowledge and training with etCO2 monitoring. |
| [19] | Potvin et al. (2022) | 52 adult patients with endotracheal tube or laryngeal mask, monitored by nurses | PACU |
Facilitators: - Nurse training facilitated the accurate interpretation and the layout of monitoring systems; - Training should be accompanied by a standardized protocol; - Standard monitoring, together with capnography, can improve patient safety by allowing early detection of respiratory complications. |
Table 3.
Summary of the barriers and facilitators to the use of capnography for respiratory monitoring by nurses in the Phase I PACU.
Table 3.
Summary of the barriers and facilitators to the use of capnography for respiratory monitoring by nurses in the Phase I PACU.
| Hutchison et al. (2008) [24] |
McCarter et al. (2008) [25] |
Lakdawala et al. (2017) [26] |
Jungquist et al. (2019) [27] |
Scully et al. (2019) [28] |
Atherton et al. (2022) [29] |
Potvin et al. (2022) [19] |
||
|---|---|---|---|---|---|---|---|---|
| BARRIERS | High workload | X | ||||||
| Perceived lack of patient adherence | X | X | X | |||||
| Lack of knowledge | X | X | ||||||
| FACILITATORS | Alarm sound | X | ||||||
| Patient education | X | X | ||||||
| Anticipating patient clinical instability | X | X | X | X | ||||
| Increased nurse confidence | X | X | ||||||
| Perception of enhanced safety | X | X | X | X | X | |||
| Targeted nurse training | X | X | X | X | X | |||
| Continuous improvement in care delivery | X | |||||||
| Effective communication and feedback | X | |||||||
| Promotion of sustainable practices | X | |||||||
| Prior knowledge and exposure | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



