Submitted:
15 July 2025
Posted:
17 July 2025
You are already at the latest version
Abstract
Lipoprotein(a) [Lp(a)] has emerged as a significant independent risk factor for atherosclerotic cardiovascular disease (ASCVD). While plasma Lp(a) levels remain relatively stable throughout life, their clinical impact varies depending on age and concentration. This comprehensive review examines the age-dependent clinical relevance of Lp(a), from childhood through adulthood. In pediatric populations, elevated Lp(a) levels are associated with early indicators of vascular dysfunction, and with conditions like familial hypercholesterolemia. In adults, elevated Lp(a) is consistently linked to an increased risk of myocardial infarction, stroke, and calcific aortic valve disease, particularly in those with additional cardiovascular risk factors. We also discuss emerging therapies targeting Lp(a) that may significantly alter long-term cardiovascular risk if implemented early. Understanding the lifelong implications of elevated Lp(a) highlights the need for age-specific strategies for screening, monitoring, and intervention. Future research should prioritize identifying high-risk pediatric populations, refining risk thresholds, and determining optimal timing for therapeutic initiation to improve long-term cardiovascular outcomes.
Keywords:
lipoprotein a
; cardiovascular disease
1. Introduction
Lp(a), predominately genetically determined, has been described as a risk factor for cardiovascular disease in all ages. Lp(a) has been investigated in young adults with no traditional cardiovascular risk factors, and even in children, who experienced cardiovascular events such as stroke [1]. In some of these cases, Lp(a) was found to be elevated, identifying it as a possible risk factor. With further investigation, it was confirmed that Lp(a) either contributes directly to cardiovascular disease or exists as a residual cardiovascular risk factor for future events [2]. Lp(a) is particularly important in individuals with a family history of premature ASCVD and in those with familial hypercholesterolemia (FH), as emphasized in current clinical guidelines [3]. The measurement of Lp(a) in these populations supports earlier identification of at-risk individuals and may guide the implementation of more aggressive lifestyle modifications and, eventually, targeted pharmacologic interventions once effective Lp(a)-lowering therapies become available.
2. Biology and Genetics of Lipoprotein(a)
Lp(a) is structurally similar to low-density lipoprotein (LDL) in terms of size, lipid content, and the presence of apolipoprotein B100 (apoB). The key distinguishing feature of Lp(a) is the addition of apolipoprotein(a) [apo(a)], which is another protein covalently linked to apoB via a disulfide bond. Apo(a) shares remarkable structural similarity with plasminogen, with approximately 94% amino acid sequence homology. Apo(a) contains an enzymatically inactive protease domain and several kringle domains—looped protein structures named for their resemblance to Scandinavian pastries. Two main kringle types are present: Kringle V (KV): Found as a single copy, identical in sequence to plasminogen by 91% and Kringle IV (KIV). The KIV domain can appear in 10 distinct subforms (KIV types 1–10). Among these, KIV type 2 is highly repetitive and can appear 10 to 40 times within apo(a). The number of KIV type 2 repeats is genetically determined and highly variable among individuals, ranging from 12 to 51 copies. This variability results in at least 34 different apo(a) isoforms, influencing the size of the Lp(a) particle and its plasma concentration, with smaller isoforms generally associated with higher Lp(a) levels and increased cardiovascular risk [4].
In addition to the KIV repeat polymorphisms, copy number variations (CNVs) within the LPA gene also influence Lp(a) concentrations [5]. CNVs are duplications or deletions in the LPA gene, that can decrease or increase the Lp(a) concentrations. The 1-copy LPA gene variant has been found to be protective for cardiovascular disease (CVD) for example, in a Chinese case-control study [6].
Another important factor influencing total plasma Lp(a) levels is the presence of single nucleotide polymorphisms (SNPs) in the LPA gene. Over 2.000 SNPs have been linked to Lp(a) concentrations, but two in particular—rs10455872 and rs3798220—have emerged as the most strongly associated. These SNPs do not directly alter the production of Lp(a), but they are closely linked to the presence of small apo(a) isoforms, which are known to result in higher plasma Lp(a) levels. In fact, approximately half of individuals carrying small apo(a) isoforms also carry one of these genetic variants. Due to their strong predictive value for elevated Lp(a) and associated cardiovascular risk, these SNPs have become key targets in genomic research [7]. SNPs have also been found to strongly participate in valvular heart disease, especially aortic stenosis [8].
3. Lp(a) Expression and Measurement over the Lifespan
Children and Adolescents
Lp(a) levels are low at birth, with the Lp(a) gene primarily becoming active and expressed by the age of two. These levels continue to fluctuate and stabilize, reaching adult concentrations around five years of age. After this point, Lp(a) levels remain relatively stable throughout life. Approximately 20% of children have increased Lp(a) in childhood and 17% of them do not have increased LDL-C levels [9]. Lp(a) levels are independent of age, sex and body weight across childhood [10].
Adults and Elders
Lp(a) evels remain relatively stable over time in adulthood and are minimally influenced by lifestyle or most medications [11]. Exceptions may occur in specific clinical contexts, such as chronic kidney disease or certain endocrine disorders. In the general adult population, Lp(a) levels greater than 50 mg/dL (approximately 125 nmol/L) are considered elevated and are associated with an increased risk of ASCVD. Approximately 28% of individuals have Lp(a) levels above this threshold, while around 10% have levels exceeding 100 mg/dL (≈250 nmol/L) [2].
Population Variations
Lp(a) levels and isoform distributions vary significantly among ethnic groups, largely due to genetic differences. African populations typically have higher Lp(a) levels, but their isoform patterns differ from other groups. Europeans are more commonly carriers of specific SNPs (such as rs10455872 and rs3798220) that significantly influence Lp(a) concentrations. In contrast, Asian populations tend to have lower Lp(a) levels and distinct isoform profiles. These variations underscore the fact that genetic factors account for over 90% of the variability in Lp(a) levels across individuals and populations.
Special consideration should be given to sex-related differences that may influence Lp(a) levels. Endogenous sex hormones appear to have minimal to no impact on Lp(a) concentrations. However, physiological states such as pregnancy can significantly elevate Lp(a) levels, in some cases nearly doubling them. Menopause itself does not substantially alter Lp(a) levels, but postmenopausal hormone replacement therapy has been shown to reduce Lp(a) by approximately 25% [11]. Additionally, chronic kidney disease and thyroid dysfunction can influence Lp(a) levels, highlighting the importance of evaluating and managing underlying endocrine conditions when interpreting Lp(a) values [2].
4. Risk-Stratification According to Age
Children and Adolescents
Lp(a) has been extensively studied for its role in influencing cardiovascular risk and contributing to premature cardiovascular events, particularly stroke, early in life. The historically significant Bogalusa Heart Study was among the first to highlight the role of Lp(a) in the pathogenesis of atherosclerosis. In a cohort of 2,438 children aged 8–17 years, Lp(a) levels were found to be significantly higher in those with a positive family history of myocardial infarction (MI) compared to those without (22.4 vs. 17.1 mg/dL). This association was even stronger among children with Lp(a) levels above 25 mg/dL. The authors concluded that Lp(a) measurement is crucial for early coronary artery disease (CAD) risk assessment beginning in childhood [12]. Numerous other studies and meta-analyses in recent years have consistently supported the role of elevated Lp(a) as a risk factor for premature atherosclerosis starting early in life [13,14,15,16]. Zawacki et al. notably found that Lp(a) was a stronger predictor of premature CVD than LDL-C in relatives of children with FH [17]. This was further confirmed in a cohort of 700 pediatric patients with FH from the LIPIGEN study, which demonstrated a clear association between both high Lp(a) and LDL-c levels with early-onset CVD [18]. Additionally, results from the Cardiovascular Risk in Young Finns Study, have shown that elevated Lp(a) levels in youth are linked to an increased risk of major cardiovascular events later in adulthood [19].
Moreover, early signs of vascular dysfunction and atherosclerosis may be detected in children with elevated Lp(a), especially those with FH. As early as 1998, a small case-control study reported impaired flow-mediated dilation (FMD) in children with FH compared to healthy peers [20]. In 2015, another study found an inverse relationship between Lp(a) levels and FMD in 11-year-old children, suggesting early vascular impairment. Notably, this association was also seen in children who received dietary counseling from early life [21]. Furthermore, a 20-year randomized controlled trial involving 200 children with FH showed that elevated Lp(a) levels were linked to increased carotid intima-media thickness (IMT) over time, supporting the value of early Lp(a) screening [22]. However, findings are controversial. A recent retrospective study of 113 children aged 6–18 found no relationship between elevated Lp(a) and IMT, even when LDL was also high [23]. Similarly, the Young Finns study, which measured Lp(a) at ages 17 and 38, found no association between Lp(a) and progression of atherosclerosis as assessed by IMT and FMD [24]. Additionally, a more recent study in young adults with FH found no correlation between Lp(a) and arterial stiffness measured by carotid pulse wave velocity (PWV) [25]. A study from Greece involving 27 children with elevated Lp(a) levels around the age of ten compared to age-matched controls assessed vascular function using carotid IMT, PWV, augmentation index (AIx), and subendocardial viability ratio (SEVR). The study found no significant differences in these vascular indices between the two groups [26].
Interestingly, elevated Lp(a) has been associated with hyperinsulinemia and insulin resistance, even in healthy, normal-weight prepubertal children [27]. Additionally, a study from Greece reported higher spexin levels—a peptide hormone involved in lipid metabolism, adiposity, and appetite regulation—in post-menarcheal adolescent females with elevated Lp(a) [28]. Emerging research has also linked Lp(a) to other early-life factors. For instance, a study examining vascular function in children conceived through assisted reproductive technologies (ART) found significantly higher Lp(a) levels in the ART group compared to spontaneously conceived peers, suggesting potential long-term cardiovascular implications [29]. Moreover, elevated Lp(a) levels have been associated with low birth weight, indicating a possible role of prenatal factors in Lp(a) regulation [30].
Adults
In adults, studies have clearly and consistently associated high Lp(a) with increased risk for myocardial infarction, coronary death, and ischemic stroke [31,32,33]. Specifically, in patients with acute myocardial infarction, persistently elevated Lp(a) levels were associated with a significantly increased risk of major adverse cardiovascular and cerebrovascular events over a 50-month follow-up period [34]. In one study, Lp(a) levels >150 mg/dL were linked to higher rates of ASCVD events in both individuals with and without prior cardiovascular history [35]. In a sub-analysis of the PROMISE trial, Lp(a) levels >50 mg/dL were associated with an increased risk of obstructive CAD, independent of LDL cholesterol levels. However, this association did not extend to high-risk plaque features when analyses were limited to cases with ≥50 or ≥70% coronary stenosis [36]. Additionally, elevated Lp(a) has been associated with coronary artery calcification, as demonstrated by coronary computed tomography imaging [37]. In the ATTICA study, Lp(a) levels were associated with a higher incidence of ASCVD over a 20-year follow-up in unadjusted models [38]. Notably, the added risk conferred by elevated Lp(a) on top of traditional cardiovascular risk factors was quantified as a 68%, 41%, and 14% increase in individuals at low, intermediate, and high baseline risk, respectively [7]. Lp(a) has also been investigated as a marker for subclinical atherosclerosis. In a recent Chinese study involving a general health check-up population, elevated Lp(a) levels were significantly associated with increased carotid intima-media thickness, the presence of carotid plaques, subclinical brain infarcts, and coronary artery calcification [39]. Beyond atherosclerosis, Lp(a) has also been implicated in aortic valve stenosis, with significantly higher levels observed in affected patients [40]. Emerging evidence suggests associations between elevated Lp(a) and other cardiovascular morbidities, including heart failure [41,42]—potentially due to coexisting coronary artery disease—and atrial fibrillation [43], possibly mediated by atrial structural remodeling.
Elders
The association between Lp(a) levels and cardiovascular events in older adults remains less well-defined, as traditional risk factors often lose predictive power in this population. However, emerging evidence suggests that elevated Lp(a) continues to be a significant and independent risk factor for adverse cardiovascular outcomes in the elderly [44]. In a prospective study involving 5888 patients, increased Lp(a) levels were found to be an independent predictor of stroke, vascular death and death by any cause in older men, but this association was observed in women [45]. Ιn another study, patients aged ≥ 80years old with ST elevation myocardial infarction, those with Lp(a) >30 mg/dL had 1.5-fold higher risk of cardiovascular death compared to those with Lp(a) ≤10 mg/dL, with no major sex differences reported [46]. Similarly, a U.S. prospective cohort study showed that patients over 70 years had an increased absolute incidence of acute coronary syndromes over an 8-year follow-up period [47].
In elderly men hospitalized with chronic heart failure, high Lp(a) levels were associated with the presence of cardio-renal syndrome, further complicating their clinical course [47]. Another important finding comes from a study of older adults without prior cardiovascular disease: individuals in the highest quartile for both LDL cholesterol (>4.90 mmol/L) and Lp(a) (>276 mg/L) had nearly double the risk of developing coronary heart disease compared to those with lower levels. Interestingly, the study concluded that in elderly individuals with low Lp(a), elevated LDL might not necessitate aggressive lipid-lowering therapy, suggesting a potential role for Lp(a) in guiding treatment decisions [48]. Additionally, Lp(a) has been implicated in the pathogenesis and severity of aortic valve stenosis (AVS) among older adults. Those with elevated Lp(a) tend to have more advanced AVS compared to their healthy peers [49]. Elevated Lp(a) levels have also been linked to the occurrence of first-time ischemic or non-embolic stroke in older patients, independently of other cardiovascular risk factors [50].
Table 1 summarizes the main studies according to age group and cardiovascular event.
5. Screening
Children and Adolescents
Measurement of Lp(a) in children is not recommended as part of routine clinical assessments. However, targeted screening may be appropriate in children with a family history of FH, elevated Lp(a), or premature ASCVD. In such cases, early identification of elevated Lp(a) can help recognize individuals at lifelong increased cardiovascular risk [51].
Adults and Elders
Current guidelines recommend measuring Lp(a) once in adulthood in order to identify individuals with inherited high Lp(a) and increased risk for CVD as they had heterozygous FH, or to re-evaluate those with intermediate to high risk [2].
Current cardiovascular risk calculators, such as SCORE2 [52] and the ASCVD Risk Estimator [53], do not incorporate Lp(a) in their formal risk scoring algorithms. Instead, they rely on traditional risk factors such as age, sex, blood pressure, cholesterol levels, smoking status, and diabetes. Although Lp(a) is not yet formally included in standard risk prediction models, its increasingly recognized role in cardiovascular pathology, along with the development of targeted Lp(a)-lowering therapies, may lead to greater clinical emphasis and potential inclusion in future versions of these calculators [2].
6. Therapy
Lifestyle Modifications and Current Pharmacological Options
Currently, there is no approved treatment specifically targeting elevated Lp(a) in either children or adults. Most management strategies are derived from adult data and focus primarily on reducing overall cardiovascular risk rather than lowering Lp(a) itself [54].
Lifestyle modifications—including maintaining a healthy diet, engaging in regular physical activity, and avoiding smoking—are universally recommended. While these measures have minimal direct effect on Lp(a) concentrations, they help reduce the burden of other cardiovascular risk factors such as hypertension, obesity, and diabetes. Family counseling is also an essential component of care.
Lipid-lowering therapies commonly used in children with familial hypercholesterolemia and adults, such as statins and ezetimibe, do not significantly reduce Lp(a) levels [55]. Similarly, monoclonal antibody proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9is), which are sometimes prescribed in pediatric familial hypercholesterolemia or adults, have only modest or inconsistent effects on Lp(a) [56,57,58,59]. For individuals with extremely elevated Lp(a) and progressive cardiovascular disease despite maximal medical therapy, lipoprotein apheresis has been used in very few specialized centers [60]. This extracorporeal procedure can reduce Lp(a) concentrations by more than 70%, but it is invasive, costly, requires frequent sessions, and is only available in selected institutions [61].
Given these limitations, attention has shifted to novel Lp(a)-targeted therapies currently under investigation. These agents show promising results, with potential reductions in Lp(a) levels exceeding 70% [62]. However, emerging data suggest that to achieve a meaningful reduction in cardiovascular risk, an absolute Lp(a) decrease of over 100 mg/dL may be required—equivalent in clinical benefit to a 40% reduction in LDL [63]. Emerging therapies are in advanced clinical trials in adults but are not yet studied or approved for pediatric use.
Novel Treatments
The most promising results in Lp(a) reduction come from novel RNA-based therapies, particularly antisense oligonucleotides (ASOs) and small interfering RNAs (siRNAs). These therapies target the production of apo(a), a key component of Lp(a) particles [64].
Antisense Oligonucleotides (ASOs)
ASOs work by binding to the complementary apo(a) mRNA sequence, promoting degradation via RNase H1, an intracellular enzyme that recognizes and cleaves RNA-DNA hybrids. The most advanced ASO is pelacarsen, which in a phase II trial involving 288 patients with established CVD, reduced Lp(a) levels by up to 80% with a 20 mg subcutaneous dose administered every 4 weeks [65]. Pelacarsen is now being evaluated in a large phase III randomized controlled trial to determine whether Lp(a) lowering translates into reduced cardiovascular events [66].
Small Interfering RNAs (siRNAs)
siRNAs bind within cells with the RNA-induced silencing complex (RISC). After removing the sense strand, RISC binds to the antisense strand, which guides the complex to the target mRNA, resulting in its degradation and inhibition of protein synthesis. This mechanism allows for sustained effects with infrequent dosing [67].
Olpasiran has demonstrated Lp(a) reductions of 70–90%, sustained for over six months [68].
Lepodisiran, another siRNA agent, achieved a 94% Lp(a) reduction in a phase II trial and maintained this reduction for over a year after a single repeated dose [69]. Zerlasiran, in a phase II trial of 178 patients with established CVD, reduced Lp(a) by over 90%, with levels remaining 80–85% lower even at week 60 [70]. Zerlasiran is currently being tested in a phase III trial—the first to include individuals without established CVD, assessing its role in primary prevention [71]. All aforementioned RNA therapies are subcutaneous therapies.
Oral Therapy – Muvalaplin
Muvalaplin is a novel oral small molecule that blocks the noncovalent interaction between apo(a) and apoB, preventing Lp(a) particle formation. It has shown an average 65% reduction in Lp(a) levels. While its clinical benefit remains unproven, the ease of oral administration makes it an attractive candidate for further development [72].
Future Directions – Gene Editing
A potential long-term or even one-time solution could come from genome editing. In a mouse model, delivery of CRISPR-Cas9 via an adeno-associated virus vector successfully disrupted the LPA gene in the liver, nearly eliminating circulating apo(a) within 7 days [73]. While human applications are still in early development, genome editing offers exciting prospects for permanent Lp(a) reduction.
Figure 1 summarizes key clinical associations and implications of Lp(a) across different age groups.
7. Gaps in Evidence – Future Directions
Children and Adolescents
Special considerations apply to all clinical trials involving children, primarily related to safety and ethical concerns, as children are still growing and have different metabolic profiles compared to adults [74]. Therefore, dosing, efficacy, and long-term safety must be thoroughly evaluated before administering treatments to pediatric patients [75].
Moreover, pediatric clinical trials must carefully select appropriate endpoints, emphasizing early markers of atherosclerosis and vascular health to assess treatment efficacy in the absence of immediate clinical events [76].
Successful development and implementation of such trials depend on close collaboration among families, participants, and healthcare providers, with the ultimate goal of extending safe and effective Lp(a)-lowering therapies to children for improved cardiovascular prevention across lifespan.
Future research should focus on age-specific groups—such as preschool children, when Lp(a) levels stabilize, and adolescents undergoing puberty, when hormonal changes occur—to determine whether early intervention can effectively reduce cardiovascular risk and future events. However, it is important to consider that children may require prolonged or lifelong treatment, which could present challenges in adherence, require family consent, and potentially impact long-term outcomes [77].
Elders
Although, all current evidence derives primarily from studies focused on younger or middle-aged cohorts thus creating an underrepresentation of those older than 70 years old. This limits the ability to define age-specific thresholds or guide therapeutic strategies and underscores the need for dedicated studies in this population.
8. Discussion
The conception that Lp(a) is a major inherited cardiovascular risk factor has progressively advanced over the years, and evidence consistently demonstrates its association with heightened risk for ASCVD [2]. While most research has focused on adults, growing evidence in pediatric patients suggests that high Lp(a) levels established in early childhood may contribute to subclinical atherosclerosis, especially in genetically predisposed individuals with FH [4].
Despite the strong observational associations, a major limitation remains the lack of interventional data showing that lowering Lp(a) improves clinical outcomes. This is partly because there has been no specific therapy for elevated Lp(a), as current studies are still ongoing. Traditional lipid-lowering therapies have little or no effect on Lp(a), and lipoprotein apheresis, though effective, is invasive and limited in availability [60].
Studies on Lp(a) should also consider its heterogeneity across ethnic groups, age ranges, and comorbidities [37]. Pediatric research in this area poses additional challenges for many reasons, and early surrogate markers of vascular dysfunction may be difficult to assess reliably [35]. Therefore, there is a clear need for longitudinal studies starting in childhood and extending into adult life to fully understand the long-term vascular impact of elevated Lp(a). However, such studies are very difficult to carry out in practice.
Screening recommendations remain conservative in children, with targeted measurements advised only when FH or a family history of premature ASCVD is present, and a one-time measurement is typically recommended in adulthood [77]. Lp(a) is not yet incorporated into cardiovascular risk calculators, but this will likely change once effective treatments become available.
In Figure 2, we present a proposed algorithm for screening and managing Lp(a) levels across different stages of life.
9. Conclusions
In conclusion, Lp(a) is a predominantly genetically determined, lifelong risk factor for ASCVD, with substantial evidence supporting its role in the pathogenesis of atherosclerosis from childhood onward. Although routine screening and treatment have been limited by the absence of specific therapies, the landscape is rapidly evolving. As novel targeted agents advance through clinical studies, there is optimism that clinicians will soon have effective means to mitigate the cardiovascular burden associated with elevated Lp(a). Future research should continue to refine screening strategies, and determine the clinical benefits of targeted Lp(a) lowering interventions in both pediatric and adult populations.
Author Contributions
M.K.: conceptualization, project administration, writing original draft, writing, review, editing and supervision. A.N.: writing original draft, writing, review and editing. A.G., P.S.: writing, review and editing. E.K., D.P., and N.F.: review, editing, supervision.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| Lp(a) | Lipoprotein(a) |
| ASCVD | Atherosclerotic Cardiovascular Disease |
| FH | Familial Hypercholesterolemia |
| LDL | Low-Density Lipoprotein |
| ApoB | Apolipoprotein B100 |
| ApoA | Apolipoprotein A |
| KIV | Kringle IV |
| CNVs | Copy Number Variations |
| CVD | Cardiovascular Disease |
| SNPs | Single Nucleotide Polymorphisms |
| MI | Myocardial Infraction |
| CAD | Coronary Artery Disease |
| FMD | Flow-Mediated Dilation |
| IMT | Intima-Media Thickness |
| PWV | Pulse Wave Velocity |
| SEVR | Subendocardial Viability Ratio |
| ART | Assisted Reproductive Technologies |
| AVS | Aortic Valve Stenosis |
| PCSK9is | Proprotein Convertase Subtilisin/Kexin type 9 Inhibitors |
| ASOs | Antisense Oligonucleotides |
| siRNAs | Small Interfering RNAs |
| RISC | RNA-induced silencing complex |
References
- Kostner KM, Kostner GM. Lipoprotein (a): a historical appraisal. J Lipid Res 2016;58:1. [CrossRef]
- Kronenberg F, Mora S, Stroes ESG, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J 2022;43:3925–46. [CrossRef]
- Kronenberg F, Mora S, Stroes ESG. Consensus and guidelines on lipoprotein(a) - Seeing the forest through the trees. Curr Opin Lipidol 2022;33:342. [CrossRef]
- Lipoprotein(a) in atherosclerotic heart disease and familial hypercholesterolaemia. British Journal of Cardiology 2024. [CrossRef]
- Feingold KR, Grunfeld C. Introduction to Lipids and Lipoproteins. Endotext 2024.
- Wu Z, Sheng H, Chen Y, et al. Copy number variation of the Lipoprotein(a) (LPA) gene is associated with coronary artery disease in a southern Han Chinese population. Int J Clin Exp Med 2014;7:3669.
- Kronenberg, F. Lipoprotein(a): from Causality to Treatment. Curr Atheroscler Rep 2024;26:75–82. [CrossRef]
- Luo D, Björnson E, Wang X, et al. Distinct lipoprotein contributions to valvular heart disease: Insights from genetic analysis. Int J Cardiol 2025;431. [CrossRef]
- Giussani M, Orlando A, Tassistro E, et al. Is lipoprotein(a) measurement important for cardiovascular risk stratification in children and adolescents? Ital J Pediatr 2024;50. [CrossRef]
- Pac-Kozuchowska E, Krawiec P, Grywalska E. Selected risk factors for atherosclerosis in children and their parents with positive family history of premature cardiovascular diseases: a prospective study. BMC Pediatr 2018;18. [CrossRef]
- Simony SB, Mortensen MB, Langsted A, et al. Sex differences of lipoprotein(a) levels and associated risk of morbidity and mortality by age: The Copenhagen General Population Study. Atherosclerosis 2022;355:76–82. [CrossRef]
- Berenson, GS. Bogalusa Heart Study: A long-term community study of a rural biracial (Black/White) population. American Journal of the Medical Sciences 2001;322:267–74. [CrossRef]
- Qayum O, Alshami N, Ibezim CF, et al. Lipoprotein (a): Examination of Cardiovascular Risk in a Pediatric Referral Population. Pediatr Cardiol 2018;39:1540–6. [CrossRef]
- Giammanco A, Noto D, Nardi E, et al. Do genetically determined very high and very low LDL levels contribute to Lp(a) plasma concentration? Nutr Metab Cardiovasc Dis 2025;35. [CrossRef]
- de Boer LM, Wiegman A, van Gemert RLA, et al. The association between lipoprotein(a) levels and ischemic stroke in children: A case-control study. Pediatr Blood Cancer 2024;71. [CrossRef]
- Nave AH, Lange KS, Leonards CO, et al. Lipoprotein (a) as a risk factor for ischemic stroke: a meta-analysis. Atherosclerosis 2015;242:496–503. [CrossRef]
- Zawacki AW, Dodge A, Woo KM, et al. In pediatric familial hypercholesterolemia, lipoprotein(a) is more predictive than LDL-C for early onset of cardiovascular disease in family members. J Clin Lipidol 2018;12:1445–51. [CrossRef]
- Pederiva C, Capra ME, Biasucci G, et al. Lipoprotein(a) and family history for cardiovascular disease in paediatric patients: A new frontier in cardiovascular risk stratification. Data from the LIPIGEN paediatric group. Atherosclerosis 2022;349:233–9. [CrossRef]
- Raitakari O, Kartiosuo N, Pahkala K, et al. Lipoprotein(a) in Youth and Prediction of Major Cardiovascular Outcomes in Adulthood. Circulation 2023;147:23–31. [CrossRef]
- Sorensen KE, Celermajer DS, Georgakopoulos D, et al. Impairment of endothelium-dependent dilation is an early event in children with familial hypercholesterolemia and is related to the lipoprotein(a) level. J Clin Invest 1994;93:50–5. [CrossRef]
- Lapinleimu J, Raitakari OT, Lapinleimu H, et al. High Lipoprotein(a) Concentrations Are Associated with Impaired Endothelial Function in Children. J Pediatr 2015;166:947-952.e2. [CrossRef]
- de Boer LM, Wiegman A, Kroon J, et al. Lipoprotein(a) and carotid intima-media thickness in children with familial hypercholesterolaemia in the Netherlands: a 20-year follow-up study. Lancet Diabetes Endocrinol 2023;11:667–74. [CrossRef]
- Helk O, Böck A, Stefanutti C, et al. Lp(a) does not affect intima media thickness in hypercholesterolemic children -a retrospective cross sectional study. Atherosclerosis Plus 2022;51:1–7. [CrossRef]
- Kivimäki M, Magnussen CG, Juonala M, et al. Conventional and Mendelian randomization analyses suggest no association between lipoprotein(a) and early atherosclerosis: the Young Finns Study. Int J Epidemiol 2011;40:470–8. [CrossRef]
- van den Bosch SE, Boer LM de, Revers A, et al. Association Between Lipoprotein(a) and Arterial Stiffness in Young Adults with Familial Hypercholesterolemia. J Clin Med 2025;14:1611. [CrossRef]
- Papadopoulou-Legbelou K, Triantafyllou A, Vampertzi O, et al. Similar Myocardial Perfusion and Vascular Stiffness in Children and Adolescents with High Lipoprotein (a) Levels, in Comparison with Healthy Controls. Pulse (Basel) 2021;9:64–71. [CrossRef]
- Rodríguez-Moran M, Gamboa-Gómez CI, Preza-Rodríguez L, et al. Lipoprotein(a) and Hyperinsulinemia in Healthy Normal-weight, Prepubertal Mexican Children. Endocr Res 2021;46:87–91. [CrossRef]
- Bacopoulou F, Apostolaki D, Mantzou A, et al. Serum Spexin is Correlated with Lipoprotein(a) and Androgens in Female Adolescents. J Clin Med 2019;8. [CrossRef]
- Oberhoffer FS, Langer M, Li P, et al. Vascular function in a cohort of children, adolescents and young adults conceived through assisted reproductive technologies—results from the Munich heARTerY-study. Transl Pediatr 2023;12:1619–33. [CrossRef]
- Rodríguez-Moran M, Guerrero-Romero F. Low birthweight and elevated levels of lipoprotein(a) in prepubertal children. J Paediatr Child Health 2014;50:610–4. [CrossRef]
- Tipping RW, Ford CE, Simpson LM, et al. Lipoprotein(a) Concentration and the Risk of Coronary Heart Disease, Stroke, and Nonvascular Mortality. JAMA 2009;302:412–23. [CrossRef]
- Mitsis A, Myrianthefs M, Sokratous S, et al. Emerging Therapeutic Targets for Acute Coronary Syndromes: Novel Advancements and Future Directions. Biomedicines 2024, Vol 12, Page 1670 2024;12:1670. [CrossRef]
- Cesaro A, Acerbo V, Scialla F, et al. Role of LipoprotEin(a) in CardiovascuLar diseases and premature acute coronary syndromes (RELACS study): Impact of Lipoprotein(a) levels on the premature coronary event and the severity of coronary artery disease. Nutr Metab Cardiovasc Dis 2025;35. [CrossRef]
- Wang Z, Tang J, Shi Q, et al. Persistent lipoprotein(a) exposure and its association with clinical outcomes after acute myocardial infarction: a longitudinal cohort study. Ann Med 2025;57. [CrossRef]
- Patel AP, Wang M, Pirruccello JP, et al. Lp(a) (Lipoprotein[a]) Concentrations and Incident Atherosclerotic Cardiovascular Disease New Insights from a Large National Biobank. Arterioscler Thromb Vasc Biol 2021;41:465–74. [CrossRef]
- O’Toole T, Shah NP, Giamberardino SN, et al. Association Between Lipoprotein(a) and Obstructive Coronary Artery Disease and High-Risk Plaque: Insights From the PROMISE Trial. Am J Cardiol 2024;231. [CrossRef]
- Jackson CL, Garg PK, Guan W, et al. Lipoprotein(a) and coronary artery calcium in comparison with other lipid biomarkers: The multi-ethnic study of atherosclerosis. J Clin Lipidol 2023;17:538–48. [CrossRef]
- Kouvari M, Panagiotakos DB, Yannakoulia M, et al. Transition from metabolically benign to metabolically unhealthy obesity and 10-year cardiovascular disease incidence: The ATTICA cohort study. Metabolism 2019;93:18–24. [CrossRef]
- Man S, Zu Y, Yang X, et al. Prevalence of Elevated Lipoprotein(a) and its Association With Subclinical Atherosclerosis in 2.9 Million Chinese Adults. J Am Coll Cardiol 2025;85. [CrossRef]
- Pantelidis P, Oikonomou E, Lampsas S, et al. Lipoprotein(a) and calcific aortic valve disease initiation and progression: a systematic review and meta-analysis. Cardiovasc Res 2023;119:1641–55. [CrossRef]
- Wang HP, Zhang N, Liu YJ, et al. Lipoprotein(a), family history of cardiovascular disease, and incidence of heart failure. J Lipid Res 2023;64. [CrossRef]
- Kamstrup PR, Nordestgaard BG. Elevated lipoprotein(a) levels, LPA risk genotypes, and increased risk of heart failure in the general population. JACC Heart Fail 2016;4:78–87. [CrossRef]
- Mohammadi-Shemirani P, Chong M, Narula S, et al. Elevated Lipoprotein(a) and Risk of Atrial Fibrillation: An Observational and Mendelian Randomization Study. J Am Coll Cardiol 2022;79:1579–90. [CrossRef]
- Gaw A, Murray HM, Brown EA. Plasma lipoprotein(a) [Lp(a)] concentrations and cardiovascular events in the elderly: evidence from the prospective study of pravastatin in the elderly at risk (PROSPER). Atherosclerosis 2005;180:381–8. [CrossRef]
- Ariyo AA, Thach C, Tracy R. Lp(a) Lipoprotein, Vascular Disease, and Mortality in the Elderly. New England Journal of Medicine 2003;349:2108–15. [CrossRef]
- Zhang M, Liu HH, Jin JL, et al. Lipoprotein(a) and cardiovascular death in oldest-old (≥80 years) patients with acute myocardial infarction: A prospective cohort study. Atherosclerosis 2020;312:54–9. [CrossRef]
- Bartoli-Leonard F, Turner ME, Zimmer J, et al. Elevated lipoprotein(a) as a predictor for coronary events in older men. J Lipid Res 2022;63:100242. [CrossRef]
- Simons LA, Simons J, Friedlander Y, et al. LDL-cholesterol Predicts a First CHD Event in Senior Citizens, Especially So in Those With Elevated Lipoprotein(a): Dubbo Study of the Elderly. Heart Lung Circ 2018;27:386–9. [CrossRef]
- Yang N, Zhang G, Li X, et al. Correlation analysis between serum lipoprotein (a) and the incidence of aortic valve sclerosis. Int J Clin Exp Med 2015;8:19318.
- Milionis HJ, Filippatos TD, Loukas T, et al. Serum lipoprotein(a) levels and apolipoprotein(a) isoform size and risk for first-ever acute ischaemic nonembolic stroke in elderly individuals. Atherosclerosis 2006;187:170–6. [CrossRef]
- Khoury M, Clarke SL. The Value of Measuring Lipoprotein(a) in Children. Circulation 2023;147:32–4. [CrossRef]
- collaboration S working group and EC risk, Hageman S, Pennells L, et al. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. Eur Heart J 2021;42:2439–54. [CrossRef]
- Arnett DK, Roger Blumenthal C-CS, Michelle Albert C-CA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2019;74:1376–414. [CrossRef]
- de Boer LM, Wiegman A, Swerdlow DI, et al. Pharmacotherapy for children with elevated levels of lipoprotein(a): future directions. Expert Opin Pharmacother 2022;23:1601–15. [CrossRef]
- Tsimikas S, Gordts PLSM, Nora C, et al. Statin therapy increases lipoprotein(a) levels. Eur Heart J 2020;41:2275–84. [CrossRef]
- Rivera FB, Cha SW, Linnaeus Louisse C, et al. Impact of Proprotein Convertase Subtilisin/Kexin Type 9 Inhibitors on Lipoprotein(a): A Meta-Analysis and Meta-Regression of Randomized Controlled Trials. JACC: Advances 2025;4. [CrossRef]
- Sahebkar A, Reiner Ž, Simental-Mendía LE, et al. Effect of extended-release niacin on plasma lipoprotein(a) levels: A systematic review and meta-analysis of randomized placebo-controlled trials. Metabolism 2016;65:1664–78. [CrossRef]
- Nasoufidou A, Stachteas P, Karakasis P, et al. Treatment options for heart failure in individuals with overweight or obesity: a review. Future Cardiol 2025. [CrossRef]
- Bytyçi I, Bytyqi S, Lewek J, et al. Management of children with heterozygous familial hypercholesterolaemia worldwide: a meta-analysis. European Heart Journal Open 2025;5. [CrossRef]
- Reijman MD, Kusters DM, Groothoff JW, et al. Clinical practice recommendations on lipoprotein apheresis for children with homozygous familial hypercholesterolaemia: An expert consensus statement from ERKNet and ESPN. Atherosclerosis 2024;392. [CrossRef]
- Gianos E, Duell PB, Toth PP, et al. Lipoprotein Apheresis: Utility, Outcomes, and Implementation in Clinical Practice: A Scientific Statement From the American Heart Association. Arterioscler Thromb Vasc Biol 2024;44. [CrossRef]
- Boffa MB, Koschinsky ML. Therapeutic Lowering of Lipoprotein(a). Circ Genom Precis Med 2018;11:e002052. [CrossRef]
- Burgess S, Ference BA, Staley JR, et al. Association of LPA Variants With Risk of Coronary Disease and the Implications for Lipoprotein(a)-Lowering Therapies: A Mendelian Randomization Analysis. JAMA Cardiol 2018;3:619–27. [CrossRef]
- Tsimikas S, Viney NJ, Hughes SG, et al. Antisense therapy targeting apolipoprotein(a): a randomised, double-blind, placebo-controlled phase 1 study. The Lancet 2015;386:1472–83. [CrossRef]
- Tsimikas S, Karwatowska-Prokopczuk E, Gouni-Berthold I, et al. Lipoprotein(a) Reduction in Persons with Cardiovascular Disease. New England Journal of Medicine 2020;382:244–55. [CrossRef]
- Cho L, Nicholls SJ, Nordestgaard BG, et al. Design and Rationale of Lp(a)HORIZON Trial: Assessing the Effect of Lipoprotein(a) Lowering With Pelacarsen on Major Cardiovascular Events in Patients With CVD and Elevated Lp(a). Am Heart J 2025;287:1–9. [CrossRef]
- Kosmas CE, Bousvarou MD, Tsamoulis D, et al. Novel RNA-Based Therapies in the Management of Dyslipidemias. Int J Mol Sci 2025;26. [CrossRef]
- Kaur G, Rosenson RS, Gencer B, et al. Olpasiran lowering of lipoprotein(a) according to baseline levels: insights from the OCEAN(a)-DOSE study. Eur Heart J 2025;46:1162–4. [CrossRef]
- Nissen SE, Ni W, Shen X, et al. Lepodisiran - A Long-Duration Small Interfering RNA Targeting Lipoprotein(a). N Engl J Med 2025;392. [CrossRef]
- Nissen SE, Wang Q, Nicholls SJ, et al. Zerlasiran—A Small-Interfering RNA Targeting Lipoprotein(a): A Phase 2 Randomized Clinical Trial. JAMA 2024;332:1992–2002. [CrossRef]
- Study Details | A Study to Investigate the Effect of Lepodisiran on the Reduction of Major Adverse Cardiovascular Events in Adults With Elevated Lipoprotein(a) - ACCLAIM-Lp(a) | ClinicalTrials.gov n.d. https://clinicaltrials.gov/study/NCT06292013 (accessed June 20, 2025).
- Nicholls SJ, Nissen SE, Fleming C, et al. Muvalaplin, an Oral Small Molecule Inhibitor of Lipoprotein(a) Formation: A Randomized Clinical Trial. JAMA 2023;330:1042–53. [CrossRef]
- Doerfler AM, Park SH, Assini JM, et al. LPA disruption with AAV-CRISPR potently lowers plasma apo(a) in transgenic mouse model: A proof-of-concept study. Mol Ther Methods Clin Dev 2022;27:337–51. [CrossRef]
- Clinical trials in children, n.d. https://www.who.int/tools/clinical-trials-registry-platform/clinical-trials-in-children (accessed July 1, 2025).
- Ethical considerations for clinical trials on medicinal products conducted with minors Recommendations of the expert group on clinical trials for the implementation of Regulation (EU) No 536/2014 on clinical trials on medicinal products for human use 2017.
- Gianos E, Duell PB, Toth PP, et al. Lipoprotein Apheresis: Utility, Outcomes, and Implementation in Clinical Practice: A Scientific Statement from the American Heart Association. Arterioscler Thromb Vasc Biol 2024. [CrossRef]
- Sbrana F, Dal Pino B, Corciulo C, et al. Pediatrics cascade screening in inherited dyslipidemias: a lipoprotein apheresis center experience. Endocrine 2025;88. [CrossRef]
Figure 1.
Age-Dependent Clinical Relevance of Lp(a).
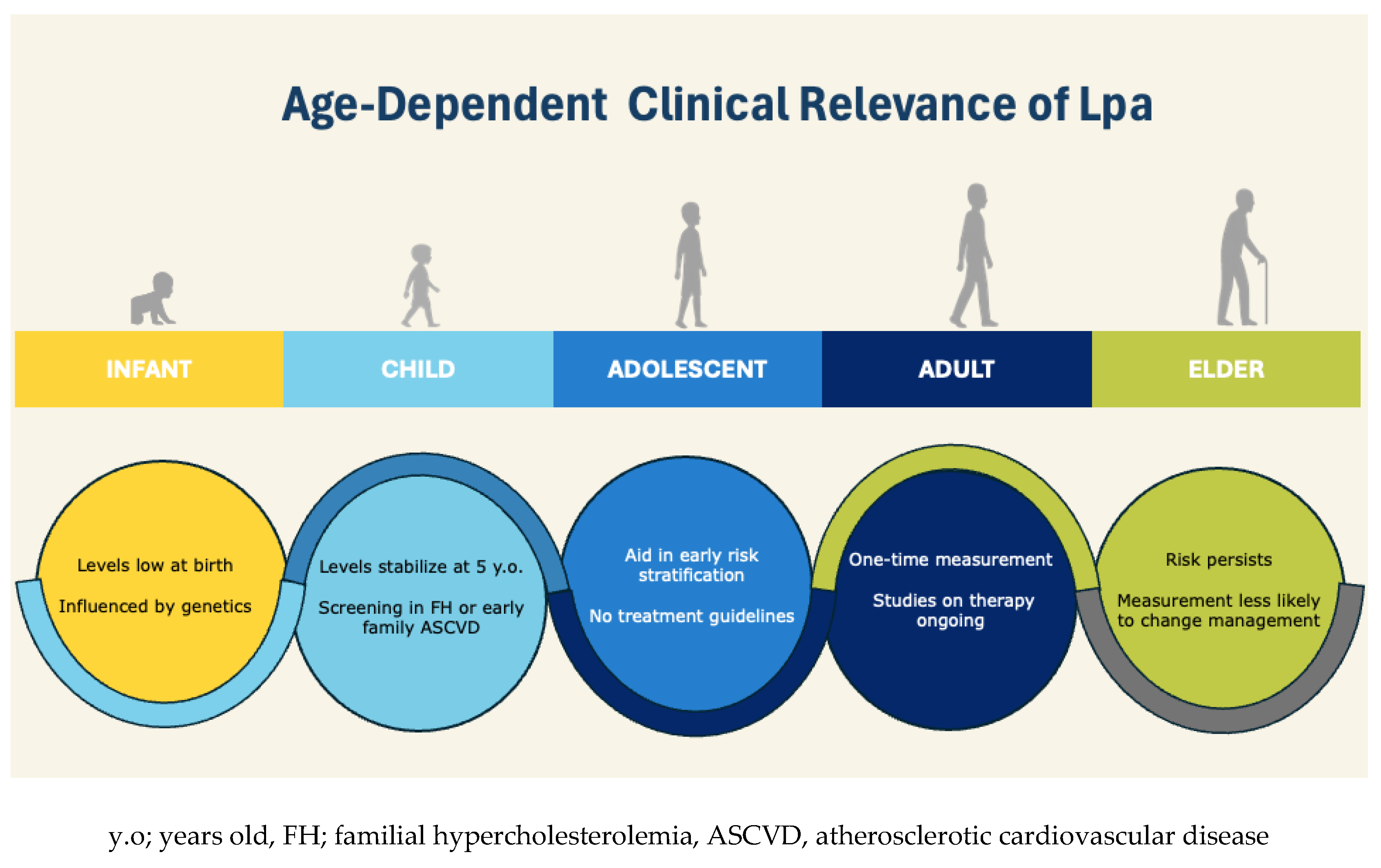
Figure 2.
Proposed Algorithm for Lp(a) Screening and Management Across the Lifespan.
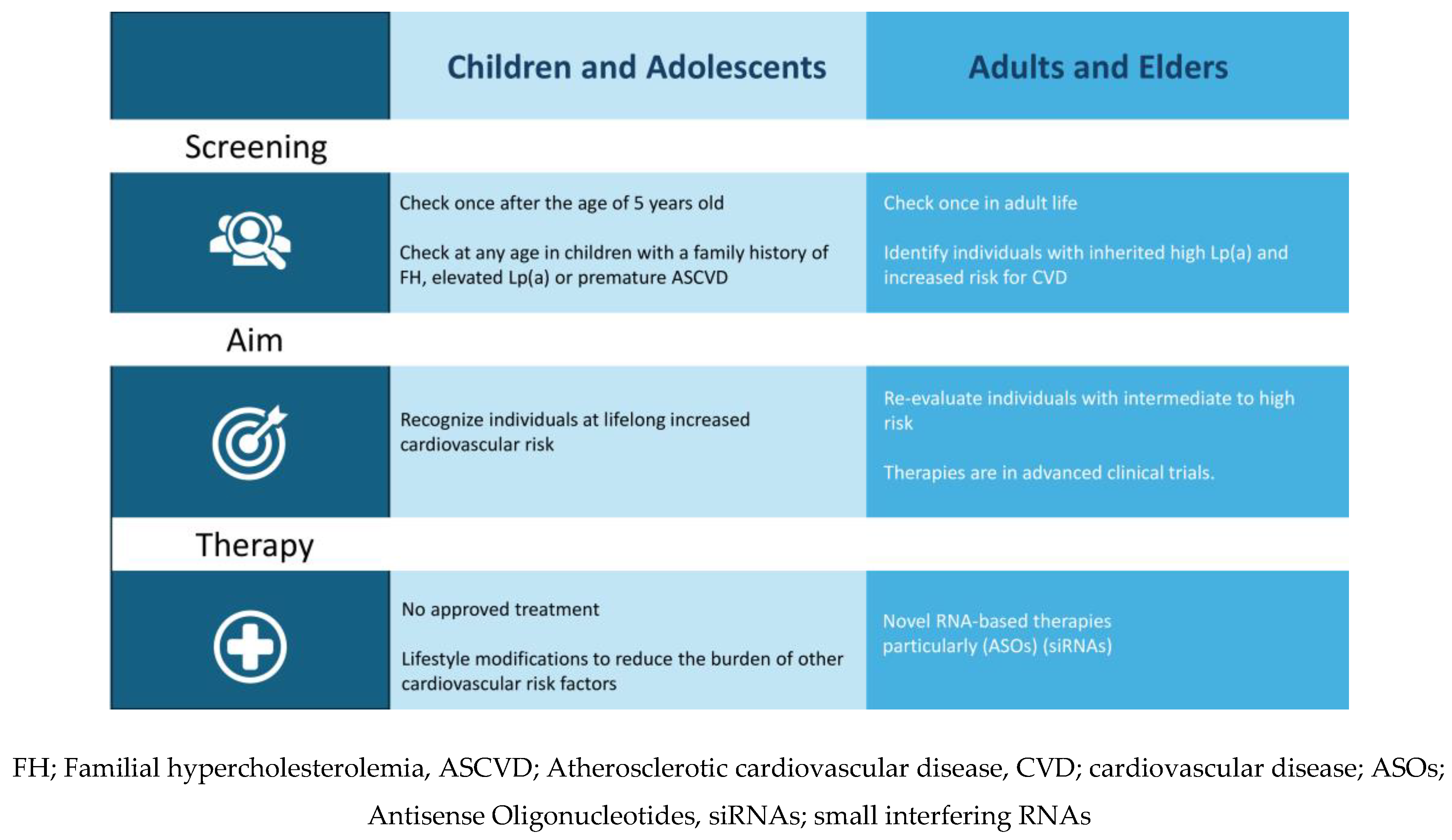

Table 1.
Summary of Main Studies Correlating Age-Specific Associations Between Elevated Lipoprotein(a) and Cardiovascular Events.
Table 1.
Summary of Main Studies Correlating Age-Specific Associations Between Elevated Lipoprotein(a) and Cardiovascular Events.
| Age | Stroke | MI | CAD | Atherosclerosis |
| Child | Bogalusa [12] | Bogalusa [12] Zawacki et al [17] LIPIGEN [18] |
de Boer LM et al [22] Young Finns [24] |
|
| Adolescent | Zawacki et al [17] | Young Finns [19] | ||
| Adult | Tipping [31] | Tipping [31] Wang [34] [35] |
PROMISE [36], ATTICA [38] | Jackson [37] |
| Elder | PROSPER [44] Ariyo [45] Milionis [50] |
Zhang [46] Bartoli [47] |
Simons [48] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



