Submitted:
15 July 2025
Posted:
16 July 2025
You are already at the latest version
Abstract
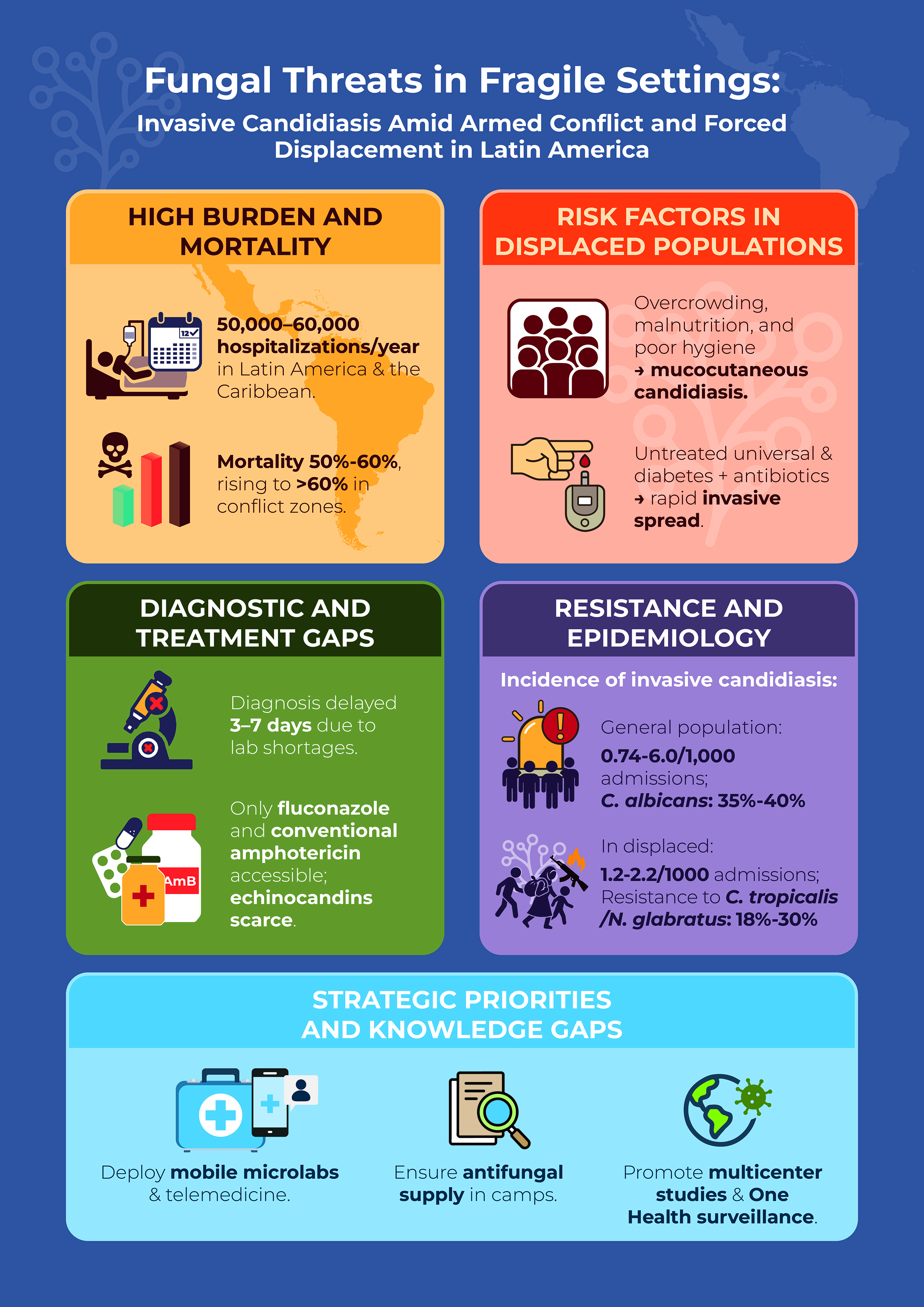
Invasive candidiasis (IC), characterized by the most common clinical manifestation of candidemia, is a fungal infection with a high mortality rate and a significant impact on global public health. It is estimated that each year there are between 227,000 and 250,000 hospitalizations related to IC, with more than 100,000 associated deaths. In Latin America and the Caribbean (LA&C), the absence of a standardized surveillance system has led to multicenter studies documenting incidences ranging from 0.74 to 6.0 cases per 1,000 hospital admissions, equivalent to 50,000–60,000 hospitalizations annually, with mortality rates of up to 60% in certain high-risk groups. Armed conflicts and structural violence in LA&C cause forced displacement, collapse of health systems, and poor living conditions—such as overcrowding, malnutrition, and lack of sanitation—which increase vulnerability to opportunistic infections, such as IC. The lack of specialized laboratories, adequate diagnostic technology, and properly trained personnel delays the identification of the pathogen and prevents the timely initiation of antifungal treatments. Furthermore, the empirical use of broad-spectrum antibiotics and the limited availability of echinocandins and lipid formulations of amphotericin B have promoted the emergence of resistant non-albicans strains, such as Candida tropicalis, Candida parapsilosis, and, in recent outbreaks, Candidozyma auris.
Keywords:
invasive candidiasis
; candidemia
; armed conflict
; forced displacement
; Latin America and the Caribbean
; antifungal resistance
; vulnerable populations
; epidemiological surveillance
1. Introduction
Invasive candidiasis (IC), which includes both candidemia and other deep forms of Candida infection, is among the most common hospital-acquired fungal infections. A high disease burden and mortality characterize it, often linked to prolonged hospitalizations and the coexistence of various comorbidities, thus posing a major challenge to healthcare systems globally [1]. Over the past twenty years, there has been a steady increase in the number of individuals at risk of developing IC, driven by the growing use of immunosuppressive therapies, stays in intensive care units (ICUs), and frequent administration of broad-spectrum antibiotics. This situation is further complicated by the emergence of non-albicans strains that are resistant to antifungal agents, making it difficult to treat these infections effectively [2]. Empirical and prolonged use of broad-spectrum antibiotics in critically ill patients promotes the development and spread of antifungal-resistant Candida strains, including C. tropicalis and C. parapsilosis. In recent years, outbreaks of the emerging isolates C. auris have also been documented, characterized by its resistance and difficult control in hospital settings [1,3,4].
It is estimated that, worldwide, IC causes around 227,300 hospitalizations each year, with at least 100,000 confirmed deaths. However, if unreported cases and those not diagnosed in time are included, estimates could rise to 1,565,000 episodes and nearly 995,000 deaths, underscoring its relevance as a critical public health priority [5,6,7]. In the LA&C region, the timely detection of IC faces multiple obstacles, including a high concentration of risk factors and restricted access to effective antifungal treatments. This situation is estimated to cause around 50,000 hospitalizations annually and between 15,000 and 35,000 deaths attributable to the infection [1,8].
Over the past two decades, many countries in LA&C have experienced prolonged crises linked to armed conflict, structural violence, and forced displacement. These situations have significantly deteriorated health systems, leading to drug shortages and severe limitations in medical care. It has been documented that these conditions significantly increase the susceptibility of affected populations to invasive fungal infections (IFI), including IC [5,9,10]. It is estimated that more than 1.6 million deaths worldwide each year are the result of serious fungal diseases, with areas affected by forced displacement having the highest mortality rates [5,10,11]. Despite the significant regional burden of candidiasis, there are still no specific studies measuring its incidence in vulnerable populations affected by violence, which highlights a notable gap in both scientific knowledge and operational response capacity [5,10,11,12].
Invasive candidiasis represents a particularly severe health challenge in contexts marked by armed conflict and high levels of violence in LA&C. The adverse conditions that characterize these environments—such as forced displacement, overcrowding in shelters, lack of basic sanitation, and limited access to health services—significantly increase both exposure to risk factors and the speed at which the infection progresses. In these areas, diagnoses are often delayed due to a lack of mycology laboratories, a lack of automated technology for blood cultures, and a shortage of trained personnel, which hinders the timely administration of antifungal treatments. In addition, the limited availability of echinocandins and lipid formulations of amphotericin B (AmB) increases the risk of unfavorable outcomes in infections caused by resistant non-albicans Candida isolates, such as C. tropicalis, C. parapsilosis, and C. auris [1,3,4]. Given this scenario, it is crucial to establish mechanisms for early diagnosis, ensure the continuous supply of essential antifungal drugs, and strengthen health infrastructure in these areas to reduce the impact of IC on the most vulnerable populations.
2. Historical Context of Armed Conflict and High Levels of Violence in Latin America and the Caribbean (LA&C) (Last 25 Years)
In recent decades, the LA&C region has experienced multiple forms of violence and armed conflict, with significant consequences for public health. The recent history of the area is marked by prolonged political conflicts—such as those in Peru and Colombia—as well as the so-called “war on drugs” in Mexico. Added to these are episodes of chronic urban violence in countries such as El Salvador and Honduras, the rise of gangs in Brazil, and deep institutional crises in nations such as Venezuela and Haiti. In addition, large-scale infrastructure projects and recurring natural disasters have contributed to new waves of displacement. These conditions have facilitated territorial control by armed actors and led to serious human rights violations, particularly affecting rural, indigenous, and Afro-descendant communities [13,14]. By the end of 2024, global figures showed that approximately 83.4 million people were living in situations of internal displacement, with around 14.5 million of these in the Americas, due to conflicts and natural disasters [13,15]. At the same time, LA&C also hosted more than 20 million migrants and asylum seekers, most notably approximately 8 million Venezuelan citizens and 1.2 million migrants residing in Peru [16].
In 2021, at least eight countries in the Americas were facing active armed conflicts. In North America and the Caribbean, these were Mexico and Haiti; in Central America, El Salvador, Guatemala, and Honduras; and in South America, Brazil, Colombia, and Venezuela. Over the past four years, the number of deaths associated with these conflicts has remained relatively stable in the region [17]. It is estimated that more than 21 million people in LA&C have been forced to displace themselves due to violence, conflict, or persecution, representing a historic high that clearly illustrates the gravity of the situation [18]. In settings marked by armed conflict and structural violence, the destruction of hospital facilities, shortages of medical personnel, and sustained shortages of medicines are common, severely restricting the affected population's access to basic health services [19]. These conditions lead to an increase in preventable infectious diseases and a lack of attention to chronic diseases, creating a favorable environment for the emergence of opportunistic infections, such as IC, particularly in impoverished or immunocompromised communities. Table 1 and Figure 1 complement this description: the former lists the countries in the region that have experienced armed conflict since 2000, along with regional data on displacement [20,21,22,23,24,25], while the latter visually represents the main conflicts that occurred between 2005 and 2025 and the associated internal displacement flows.
2.1. Conflicts in North America and the Caribbean
Mexico is experiencing multiple forms of armed violence mainly associated with drug trafficking and organized crime, which since the early 2000s have led to a significant increase in internal displacement and mass migration. The federal strategy against drug trafficking, formally implemented in 2006, intensified confrontations between criminal groups such as the Sinaloa, Jalisco Nueva Generación (Jalisco New Generation), and Zetas cartels and state security forces, resulting in the militarization of large areas of the country. Although there is no officially declared armed conflict, the conditions that have been created—including homicides, forced disappearances, and the use of high-powered weapons—resemble those of war zones [26]. According to a 2020 report by the International Committee of the Red Cross (ICRC), violence in Mexico has had both obvious and subtle impacts: from homicides and acts of physical violence to severe restrictions on mobility and a persistent climate of fear among communities, effects that together have created a suffocating environment for the population [26]. However, the Mexican government has not officially recognized the existence of internal displacement due to violence, which has made accurate measurement of the phenomenon difficult. Estimates by the Internal Displacement Monitoring Centre (IDMC) and non-governmental organizations (NGOs) indicate that every year, hundreds of thousands of people are forced to leave their homes as a result of large-scale violent events. In 2022 alone, 9,171 people were internally displaced by armed groups, who were responsible for 96% of the events recorded; the rest corresponded to expulsions or attacks resulting from human rights violations (<1%) [26]. Recent reports indicate that armed conflicts between cartels have caused the forced displacement of more than 500 people from communities in the state of Chiapas to Guatemalan territory [27]. Similarly, in June 2024, approximately 7,000 inhabitants left the municipality of Tila, also in Chiapas, as a direct result of confrontations between armed groups fighting for territorial control [28].
Haiti is in the midst of a serious humanitarian crisis that has intensified following the assassination of President Jovenel Moïse in 2021. Since then, the absence of a functioning government has facilitated the expansion and consolidation of at least 200 armed gangs, particularly in Port-au-Prince and other regions of the country. Despite the government's use of military drones, which have caused the deaths of more than 300 civilians, the leaders of these criminal groups continue to operate without being captured [29]. The ICRC has documented multiple attacks targeting government institutions and health centers in Haiti. As a result, less than 40% of health facilities in the capital, Port-au-Prince, are operating under normal conditions, evidencing the partial collapse of the health system amid the crisis [30]. The International Organization for Migration (IOM) states that the outbreaks of violence in November 2024 triggered the displacement of more than 300,000 people in just one month, bringing the total number of internally displaced persons due to violence in Haiti to over one million [31]. On the other hand, the United Nations Office for the Coordination of Humanitarian Affairs (UN OCHA) has stated that since March 2024, the number of displaced persons has almost doubled, with continuous flows of families fleeing to makeshift camps on the outskirts of Port-au-Prince and other areas of the country [32].
2.1.1. Conflicts in Central America
The Northern Triangle of Central America—comprising El Salvador, Guatemala, and Honduras—has historically been one of the regions most affected by structural and criminal violence, manifested through armed conflicts and the actions of criminal groups known as maras. This combination has triggered both forced displacement within countries and mass migration to other nations in the region and across the continent. In El Salvador (1980–1992) and Guatemala (1960–1996), armed conflicts between left-wing and right-wing groups left more than one million internally displaced persons in each country, with mass migrations of rural populations to urban areas following the signing of the Peace Accords. Since the beginning of the 21st century, the countries of the Northern Triangle have faced sustained confrontations with gangs, especially MS-13 and Barrio 18, which exercise territorial control through violent practices such as extortion, murder, and kidnapping. This dynamic has created conditions of insecurity so severe that, in several regions, the situation has been compared to that experienced in armed conflict scenarios [33]. By the end of 2022, El Salvador, Guatemala, and Honduras together had nearly 318,600 internally displaced persons due to violence generated by organized crime and gangs [23]. That same year, the IDMC reported around 171,000 additional displacements linked to episodes of extreme violence in the region [33]. At the international level, by the end of 2022, approximately 665,200 people from these three countries had been registered as refugees or asylum seekers, mainly in Mexico, the United States, and other Central American countries [23].
2.1.2. Conflicts in South America
The internal armed conflict that has affected Colombia for more than half a century has left a deep mark on the country's social life and has caused one of the highest levels of internal displacement and migration globally. Beginning in the mid-20th century, this conflict involved actors such as the FARC-EP and ELN guerrilla groups, as well as paramilitary groups. The prolonged struggle for territorial and resource control led to serious human rights violations, murders, the systematic use of anti-personnel mines, and direct impacts on rural and indigenous communities in the disputed areas [34]. For decades, Colombia has led global statistics on internal displacement. Between 1985 and 2015, an estimated 5.6 million people were forced to leave their homes, moving from rural areas to urban centers such as Bogotá, Medellín, and Cali [35]. Various studies have shown that, for more than a decade, the country ranked first or second in the world in terms of the number of internally displaced persons, a phenomenon intensified by the convergence of armed conflict and drug trafficking [36]. Recent events, such as the mass displacement of more than 40,000 people in Catatumbo in January 2025, reflect the persistence of this problem [37].
The humanitarian situation in Venezuela has been deeply marked by state repression and the actions of irregular armed groups, which have caused both internal displacement and mass migration to neighboring countries. During Nicolás Maduro's administration, various organizations have documented the systematic use of force by security agencies such as the FANB, FAES, and GNB. This pattern of violence includes extrajudicial executions, torture, and arbitrary detentions, which have led thousands of people to leave the country to protect their lives [38]. Investigations carried out by the UN mission and Human Rights Watch (HRW) have found evidence of crimes against humanity in Venezuela, including more than 19,000 deaths classified as “resistance to authority” between 2016 and 2019, and more than 15,000 arbitrary detentions since 2014 [38]. In one of the most serious incidents, during military operations against FARC dissidents in the state of Apure (March-April 2021), more than 5,800 people were forced to cross the Arauca River into Colombia, fleeing bombings and human rights violations. Many of them ended up in makeshift shelters and precarious conditions [39]. Since 2014, approximately 5.1 million Venezuelans have left the country, driven by the economic, political, and social crisis [40]. This migration process has accelerated significantly since 2015, with an estimated 8 million Venezuelans having emigrated by 2024, with Colombia, Peru, and other countries in LA&C being the main destinations [41].
Brazil experiences various forms of violence that affect both urban and rural areas and indigenous communities. Although the country has not undergone formal armed conflict, it does experience chronic violence that has led to internal displacement, migration induced by megaprojects, and a significant influx of Venezuelan refugees. In urban areas, such as the favelas of Rio de Janeiro, gang violence and police operations have established informal or “parastatal” territorial control, creating a constant climate of insecurity [42]. In rural areas of Brazil, land conflicts have intensified due to invasions and evictions in the Amazon region, exacerbated by poor implementation of the Rural Environmental Registry. This situation has encouraged irregular land occupation and forced displacement of peasant communities [43]. Indigenous populations, such as the Yanomami, have also been severely affected by illegal extractive activities, such as gold mining, which has triggered health emergencies and multiple violations of their fundamental rights [44]. In 2019, Brazil accounted for around 295,000 new internal displacements caused by natural disasters such as floods and landslides [45]. However, displacement associated with violence is not systematically recorded due to limitations in data collection. Large infrastructure projects have also forced rural communities to abandon their homes; for example, the construction of the Belo Monte dam forced thousands of people to resettle, severely affecting their livelihoods [46]. On the other hand, since 2015, Brazil has received approximately 1 million Venezuelan migrants, who have settled mainly in the states of Roraima, Amazonas, and São Paulo [47].
Between 1980 and 2000, Peru faced a prolonged internal conflict involving the armed groups Sendero Luminoso (Shining Path) and the Movimiento Revolucionario Túpac Amaru (Túpac Amaru Revolutionary Movement) (MRTA). This period was marked by high levels of violence, serious human rights violations, and mass displacement, which particularly affected rural and indigenous communities [48]. The conflict left an estimated 70,000 dead and profound social sequelae [48]. The Truth and Reconciliation Commission (CVR) in Peru documented the devastating effects of the conflict, including the collapse of the social fabric in the most affected communities. The report highlighted how violence fractured networks of solidarity and community support and underscored the fundamental role played by indigenous women in rebuilding these social structures after the conflict [49]. Since 2017, Peru has received more than 1,200,000 Venezuelan migrants and refugees, becoming one of the main destinations for this flow in LA&C [50].
3. Epidemiology and Burden of IC Disease in LA&C
Invasive candidiasis, especially in its manifestation as candidemia, is one of the most severe fungal infections and a major concern for international public health. Globally, there are an estimated 250,000 cases per year, with mortality rates ranging from 30% to 60% in high-income countries. In these regions, the availability of automated blood cultures and early access to echinocandins have helped reduce treatment delays, thereby improving survival rates [5]. A multicenter study conducted between 2008 and 2010 in seven Latin American countries reported an average rate of 1.18 cases per 1,000 hospitalizations, compared to 0.3–0.7 per 1,000 admissions in developed regions during the same period. Colombia had the highest incidence (1.96/1,000), while Chile reported the lowest (0.33/1,000) [1]. Subsequent studies showed significant variations between countries [1]. Subsequent studies showed significant variations between countries. In Brazil, a prospective observational study conducted between 1994 and 2004 in four tertiary hospitals in São Paulo reported an incidence of candidemia of 1.66 cases per 1,000 hospital admissions [51]. In Mexico, hospital surveys estimated rates between 1.2 and 1.5 per 1,000 admissions in high-complexity centers (2005–2015), while in the Caribbean, the incidence ranged from 0.5 to 0.8 per 1,000, with marked differences between hospitals [52,53]. Recent data from Brazil and Argentina (2020–2023) suggest a slight increase in cases in patients with severe COVID-19, possibly related to prolonged use of corticosteroids, mechanical ventilation (MV), and total parenteral nutrition (TPN) [54].
In 2017, the global burden attributed to IC was estimated at 1.6 million disability-adjusted life years (DALYs), with LA&C contributing 8% of that total, despite representing only 13% of the world's population. This disproportion reflects a high prevalence of predisposing conditions such as untreated HIV, poorly controlled diabetes, malnutrition, prolonged use of broad-spectrum antibiotics (OR > 2.5), TPN (OR 4.5), and the presence of CVCs (OR 3.8) [5]. In Colombia, the incidence of candidemia has been estimated at approximately 12–13 cases per 100,000 inhabitants per year [55], a figure considerably higher than that observed in many high-income countries. In Venezuela, recent studies suggest an even higher rate, around 16 cases per 100,000 inhabitants, likely reflecting the deterioration of the health system in the context of crisis [6]. The pediatric population accounts for a significant fraction of this burden. According to data from the LAMNet (Latin America Invasive Mycosis Network), 44% of candidemia episodes in the region occur in children, including newborns. Neonatal and pediatric ICUs are critical foci of infection, where Candida spp. accounts for between 85% and 88% of nosocomial fungal infections, making it a leading cause of hospital-acquired sepsis [1,9]. The treatment of a case of candidemia in Colombia, managed with echinocandins followed by fluconazole (FCZ), can cost between USD 40,000 and 60,000, considering prolonged stays in the ICU (≥14 days) and renal complications [9]. In Brazil, average hospital costs for adults with IC range from USD 20,000–25,000 in private centers and USD 5,000–8,000 in public institutions, differences attributable to the prices of antifungals and the length of hospitalization [56]. Despite their favorable cost-effectiveness profile, the widespread use of echinocandins (USD 1,000–1,500/day) and L-AmB (USD 5,000 per vial) in public hospitals faces significant barriers, such as their high initial cost and the structural limitations of the healthcare system, which can increase the infectious disease budget by 20%–30 [9,57]. In addition, indirect costs resulting from lost productivity due to prolonged hospital stays have been estimated at USD 10,000–15,000 per patient in the Andean region [58].
Globally, Candida albicans remains the most frequently isolated yeast in cases of candidemia, accounting for between 45% and 50% of episodes in high-income countries. It is followed by Nakaseomyces glabratus (10%–15%), C. parapsilosis (15%–20%), and C. tropicalis (8%–12%) [59]. However, in LA&C, the proportion of C. albicans has decreased, standing at around 35%–40%, although it remains the predominant species [1,8,51,60]. In the region, C. parapsilosis has increased in frequency to 25%–30%, especially in neonatal and pediatric ICUs [8,60]. C. tropicalis accounts for 15%–20% of cases, with a higher prevalence in hematology and oncology patients [1,61], while N. glabratus has a frequency of 5%–10%, with sustained growth in Brazil and Mexico since 2015 [1,62].
The emerging fungal pathogen C. auris has demonstrated a rapid and concerning global spread. By December 2023, it had been identified in at least 61 countries across six continents, with outbreaks documented in ICUs, rehabilitation centers, and nursing homes. In the United States, confirmed cases increased from 479 in 2019 to 4,514 in 2023, while significant outbreaks have been reported in India, South Africa, and several European countries, with associated mortality rates ranging from 30% to 60% [63,64]. In LA&C America, following its initial detection in Venezuela in 2012, C. auris has spread rapidly, although with varying prevalence between countries. In Brazil, some ICUs have reported that C. auris accounts for between 5% and 10% of all Candida isolates, while Colombia, with more than 2,000 cases recorded, is currently the country with the highest number of reports, accounting for approximately 26.1% of isolates documented in seven high-complexity hospitals [65,66].
Mortality associated with IC: the mortality rate associated with candidemia in LA&C remains alarmingly high. In referral hospitals, it is estimated that between 45% and 60% of affected patients die, figures higher than those reported in North America and Europe, where mortality ranges between 30% and 40% [67]. This disparity has also been documented in an epidemiological meta-analysis that included studies published between 2000 and 2019, which identified an average 30-day mortality rate of 37.5% for candidemia in Europe, with consistent rates in ICUs, general hospitals, and tertiary centers, in contrast to rates close to 50% in middle- and low-income countries and peaks above 60% in regions such as sub-Saharan Africa and Southeast Asia [5,68]. In LA&C, several national studies confirm this trend. A multicenter study in 10 hospitals in seven countries in the region reported a 30-day mortality rate of 40.7%, reaching up to 50.5% in some centers [1]. In Brazil, a retrospective multicenter study conducted between 2007 and 2010 in 16 hospitals documented extremely high hospital mortality from nosocomial candidemia (72.2%), reaching 85% in ICUs, figures that far exceed those reported in high-income countries [69]. In Colombia, a retrospective cohort of 123 patients with candidemia between 2008 and 2014 showed an attributable mortality rate of 49% [70]. In neonatal ICUs, mortality from IC in newborns varies between 25% and 30% in the region, while in high-income countries it is generally between 10% and 15% [71]. In a retrospective multicenter study conducted in Brazilian neonatal ICUs, a mortality rate of 46.15% associated with candidemia was reported, with frequent use of broad-spectrum antibiotics (100%), TPN (97.7%), prematurity (93.2%), and CVC (52.3%), although only the latter showed a statistically significant association with mortality (OR: 10.67; p = 0.02) [72].
The coexistence of diseases such as HIV and diabetes is a factor that worsens the prognosis in cases of candidemia. In a retrospective observational study conducted at a university hospital in Colombia (2008–2014), diabetes mellitus was present in 23% and HIV infection in 5% of patients with candidemia, with no significant association with hospital mortality [70]. In a six-year retrospective study conducted at a tertiary hospital in northeastern Brazil, a 30-day mortality rate of 55.9% was reported, higher in ICU patients and those with N. glabratus, with no significant association with diabetes mellitus (present in 25% of cases) or HIV infection (5.9%), with advanced age, severe sepsis, and hypotension being the only independent prognostic factors for mortality [73].
The high mortality rate due to candidemia in the region is closely linked to a combination of structural barriers, diagnostic limitations, and clinical factors [1,68]. Among the main determinants identified are:
- Delay in diagnosis: the speed with which candidemia is detected varies depending on the fungal species. While C. albicans can be detected in an average of 35 hours, N. glabratus requires up to 80 hours, which significantly delays the start of effective antifungal treatment [74].
- Age and clinical status at admission: a high APACHE II score and a diagnosis of septic shock are negative prognostic factors. On average, patients who die from candidemia are around 60 years old [79].
Epidemiology, Disease Burden in the Context of Armed Conflict and High Violence
Displaced persons and migrants in contexts of violence and conflict in LA&C face conditions that favor the onset and rapid progression of IC. Overcrowding in shelters, lack of access to safe drinking water and basic sanitation, malnutrition, and irregular medical care create an environment conducive to Candida colonization of the skin and mucous membranes. These factors act in conjunction with predisposing conditions, such as untreated HIV or immunosuppression due to severe malnutrition, to precipitate invasive infections [80,81]. Furthermore, the lack of mycological surveillance and early studies in migratory or resettlement phases makes it difficult to quantify the problem in these populations [80,81]. In referral hospitals located near violent areas or on displacement routes, such as the Colombia-Venezuela border or rural regions of Brazil, incidences of candidemia of 1 to 2 cases per 1,000 admissions have been observed, higher than in safer urban areas, with 30-day mortality rates that can reach 50%, especially in patients with malnutrition or co-infections. 000 admissions, higher than in safer urban areas, with 30-day mortality rates reaching 50%, especially in patients with malnutrition or co-infections [1,51,82].
Although studies are scarce, some series report similar incidences in specific settings: Between 2008 and 2010, border hospitals in Colombia observed rates of 1.2–1.8 episodes per 1,000 admissions in patients from camps or shelters, compared with 1.0 in non-displaced patients [83]. Between 2012 and 2015, in rural areas of Brazil affected by gangs, the incidence was 1.5–2.0/1,000 admissions, with a predominance of C. parapsilosis and C. tropicalis. [84] In field clinics in Mexico (2015–2018), an estimated 1.3 to 1.6 cases per 1,000 admissions were seen in young migrant adults with malnutrition and HIV [85]. Between 2020 and 2023, outbreaks in Port-au-Prince, Haiti, affected 2.2 patients per 1,000 admissions in centers caring for internal refugees [86].
These data, although limited and fragmented, suggest that the incidence of IC in displaced and migrant populations in LA&C may be comparable to or higher than in conventional clinical settings. Figure 1 illustrates this comparison between the general population and the migrant/displaced population.
Each episode of candidemia implies a significant burden on health systems in LA&C. It has been estimated that it prolongs hospital stays by at least 10 days, generating costs that exceed US$10,000 even in public hospitals [9]. In regions affected by conflict and mass displacement, where resources are already committed to caring for the wounded or refugees, this situation is unsustainable. The lack of standardized mycological surveillance networks makes it difficult to accurately identify areas of high incidence. However, recent outbreaks of C. auris in mobile clinics and field hospitals highlight the urgent need to strengthen diagnostic capacity through mobile laboratories and trained personnel, as well as to improve access to broad-spectrum antifungals [57,65]. In the migrant population, episodes of candidemia tend to extend hospitalization by an additional 10 to 14 days, with an estimated daily cost of between USD 300 and 500 in public hospitals in Brazil and Colombia, reaching between USD 7,000 and 10,000 for complete treatment [87]. Despite this, empirical treatment with FCZ remains common, with a therapeutic failure rate of around 25%, particularly in the case of resistant strains, such as C. tropicalis and N. glabratus. In these cases, when echinocandins such as caspofungin (CAS), anidulafungin (ANF), or micafungin (MCF) are required, the full course of treatment (14–21 days) can exceed USD 2,500, a figure that is unattainable for many healthcare systems in settings of armed conflict or sustained violence [88]. The long-term consequences for displaced patients who survive include sequelae such as chronic organ failure, which can reduce their ability to work by 40% to 60% [89]. Since these individuals often lack health insurance, indirect expenses—transportation, medication purchases—can represent up to 80% of monthly family income [90]. NGOs and mobile clinics must take on a large part of the treatment of these infections, allocating a considerable portion of their resources to the care of fungemia, which restricts the funds available for essential services such as vaccination and maternal and child care [91].
In displaced and migrant populations, a different distribution of Candida spp. and antifungal resistance patterns is observed compared to stable clinical settings in the region. Although C. albicans remains common (35%–45%), its prevalence is lower than that of non-albicans strains, which show higher resistance rates, especially in contexts of poor healthcare [92]. C. parapsilosis accounts for between 25% and 30% of isolates in migrants treated in Brazil and Colombia. This species is associated with prolonged use of CVCs and with TPN procedures performed under suboptimal conditions, which are common in mobile clinics or makeshift camps [93]. C. tropicalis reaches a frequency of 20%–25% in mobile hospitals located in areas of displacement, with FCZ resistance ranging from 18% to 22% [94]. N. glabratus is identified in 8%–10% of cases, with FCZ resistance rates of up to 30%, especially in migrants with untreated HIV or in diabetic patients with poor metabolic control [95]. C. auris has been responsible for documented outbreaks in displacement camps in Colombia and Venezuela between 2017 and 2023. In these situations, up to 5% of isolates have shown simultaneous resistance to azoles, echinocandins, and AmB, highlighting the therapeutic challenge in these settings [64,96].
Mortality in vulnerable populations: mortality related to IC in contexts of violence and displacement significantly exceeds that observed in local populations. A multicenter study in Colombia (2008–2010) revealed a 30-day mortality rate of 52% in displaced persons with candidemia, compared to 40% in non-displaced patients. This difference was associated with late diagnosis and the presence of comorbidities such as untreated HIV/AIDS [97]. Subsequent investigations in camps for people displaced by violence in Colombia reported a mortality rate from candidemia of over 65%, considerably higher than the 45%–60% observed in general hospitals. The identified causes were delays of more than 72 hours in initiating antifungal treatment and the administration of inadequate therapeutic regimens, such as the use of FCZ in N. glabratus infections [98,99]. In mobile ICUs in Brazil (2012–2015), the migrant population with candidemia had an overall mortality rate of 58%. Factors such as the administration of TPN in makeshift conditions, prolonged use of CVCs, and coinfection with FCZ-resistant C. tropicalis contributed significantly to this outcome [100]. During the period 2016–2019, mobile clinics along migratory routes in Central America recorded a 30-day mortality rate of 55% in migrant patients with candidemia. This high mortality rate was attributed to the lack of rapid diagnostic tests and adequate treatments, such as limited access to FCZ or echinocandins [101]. In high-violence urban areas in El Salvador and Honduras, it has been documented that mucocutaneous Candida infections, if not treated promptly, progress to disseminated forms in approximately 12% of patients with HIV or poorly controlled diabetes, significantly increasing the need for intensive care [102,103]. In the context of the humanitarian crisis in Haiti (2020–2023), refugees treated in field hospitals had a mortality rate of 60% in cases of confirmed candidemia. This level of lethality was associated with outbreaks of C. auris and the lack of echinocandins in these centers [104].
4. Factores Risk Factors for IC in the General Population and in Contexts of Forced Displacement in LA&C
Globally, various conditions predispose individuals to Candida infections, notably chronic metabolic disorders (such as diabetes and obesity), immunosuppression (advanced HIV, neutropenia), hormonal factors (use of contraceptives, pregnancy), and certain habits such as smoking. Diabetes mellitus is the main risk factor for both mucocutaneous and invasive forms of candidiasis. In hospitalized diabetic patients, a relative risk (RR) of 2.5 (95% CI: 2.0–3.1) has been observed for recurrent vaginitis and 3.2 (95% CI: 2.4–4.3) for candidemia [2,98,105,106]. In sub-Saharan Africa, the impact is particularly severe in people with advanced HIV, where oral candidiasis reaches a prevalence of 60%, compared to only 4% in the general population, representing an RR of 15 (95% CI: 10–22). In individuals with HIV and neutropenia, candidemia has been documented with attributable mortality between 35% and 45% [107,108,109].
In Europe, the use of combined oral contraceptives has been linked to a 40% increase in the risk of vulvovaginal candidiasis (RR = 1.4; 95% CI: 1.2–1.6) [110]. On the other hand, a meta-analysis in Asia and Europe found that up to 25% of pregnant women experience vulvovaginal candidiasis, with a higher risk during the second and third trimesters (RR = 1.7; 95% CI: 1.4–2.0) [110]. In North America, chronic smokers have an 80% increase in the likelihood of developing oral candidiasis (OR = 1.8; 95% CI: 1.3–2.5), while people with obesity (BMI > 30 kg/m²) have approximately twice the risk of developing interdigital candidiasis (RR = 2.1; 95% CI: 1.5–2.9) [60,106,107,111].
Unlike the global picture, in LA&C, socioeconomic determinants have a specific impact on susceptibility to Candida infections. Among these factors, limited access to antiretroviral treatments, an increase in gestational diabetes, and the widespread use of hormonal contraceptives and corticosteroids stand out. In a multicenter study conducted in Brazil and Argentina, it was observed that 28% of women with recurrent vulvovaginal candidiasis had type 2 diabetes, compared to 10% in healthy controls (OR = 3.4; 95% CI: 2.1–5.6); in addition, 15% had candidemia associated with uncontrolled diabetes [1,2,107,112]. In Colombia, patients with HIV and CD4 counts below 200 cells/μL had a prevalence of oral candidiasis of 35%, compared to 5% in those with levels above 500 cells/μL (OR = 9.8; 95% CI: 5.2–18.5). In cases of candidemia in patients with advanced HIV, mortality reached 60%, compared to 45% in patients without HIV (p = 0.02) [55,109,113]. Research conducted on pregnant women in Colombia indicated a prevalence of vulvovaginal candidiasis of 17%, with a higher risk in multiparous women (OR = 1.8; 95% CI: 1.1–2.9) and in those with gestational diabetes (OR = 2.6; 95% CI: 1.4–4.8) [55,106]. In Mexico, prolonged use of oral contraceptives for more than six months was linked to an increase in the recurrence of vulvovaginal candidiasis (OR = 2.2; 95% CI: 1.3–3.8), while uncontrolled use of topical corticosteroids was associated with intertriginous candidiasis (OR = 1.9; 95% CI: 1.1–3.3) [2,5,18]. Studies conducted in Peru established an association between obesity (BMI > 30 kg/m²) and intertriginous candidiasis in 22% of cases, compared to 8% in people with a BMI below 25 kg/m² (OR = 3.1; 95% CI: 1.6–6.0). Similarly, smoking was linked to an increased risk of oral candidiasis in adults (OR = 1.7; 95% CI: 1.1–2.6) [1,105,114].
The factors that predispose hospitalized patients to developing IC and candidemia vary significantly depending on the region and have a direct impact on morbidity and mortality. Internationally, a history of broad-spectrum antibiotic use during the previous 30 days—especially carbapenems, fluoroquinolones, or β-lactams combined with β-lactamase inhibitors—significantly increases the risk of candidemia, with an estimated odds ratio (OR) of 2.5 (95% CI: 1.8–3.4) [2,72,98]. The presence of a CVC increases the risk of candidemia by 4.1 times (OR 4.1; 95% CI: 3.0–5.7), while a stay in the ICU longer than 10 days doubles this risk (OR 2.1; 95% CI: 1.6–2.8) [108]. The use of TPN is one of the most important determinants: in North American contexts, it has been observed that patients receiving prolonged TPN have a 12% incidence of candidemia, with an OR of 6.8 (95% CI: 4.5–10.2) [2,98,105]. On the other hand, complex surgical procedures, such as major abdominal surgery and acute necrotizing pancreatitis, significantly increase the risk of both intra-abdominal candidiasis (OR = 4.7; 95% CI: 3.1–7.2) and candidemia (OR = 3.3; 95% CI: 2.1–5.3). Patients with immunosuppression—particularly those with febrile neutropenia secondary to prolonged chemotherapy (more than 7 days)—have an incidence of candidemia of approximately 8%, compared with less than 2% in those with neutropenia lasting less than 7 days (p < 0.001). In addition, prolonged use of high-dose corticosteroids (more than 20 mg daily of prednisone or its equivalent for a period longer than 14 days) has been associated with an increased risk of CI, with an estimated OR of 2.3 (95% CI: 1.5–3.5) [2].
In LA&C, the prevalence of predisposing factors for candidemia, such as the use of broad-spectrum antibiotics, the use of CVCs, and the administration of TPN, exceeds that reported in global studies. A prospective multicenter study conducted in eight countries in the region (Argentina, Brazil, Chile, Colombia, Ecuador, Honduras, Mexico, and Venezuela) showed that 82% of patients with candidemia had received broad-spectrum antibiotics—such as third-generation cephalosporins or carbapenems—in the previous 30 days, compared with only 45% among hospitalized patients without candidemia [107]. In this same cohort, candidemia was linked to the presence of CVCs in more than 70% of cases, representing a significantly higher risk (OR 3.8; 95% CI: 2.1–6.9) compared to patients without this device. Similarly, TPN was identified as an independent factor in 60% of cases of candidemia, while only 18% of controls received it (OR 4.5; 95% CI: 2.3–8.7). A prolonged stay in ICUs (more than 14 days) was also associated with an elevated risk of developing candidemia (OR 2.9; 95% CI: 1.5–5.6), probably due to sustained exposure to invasive treatments and empirical antibiotics. In addition, a recent history of major abdominal surgery (within the previous 30 days) was associated with intra-abdominal candidiasis in 25% of cases, compared with only 6% in controls (OR 5.1; 95% CI: 2.2–11.8). Finally, neutropenia (neutrophil count < 500 cells/µL) in cancer patients or patients with hematological diseases was associated with a fivefold increased risk of candidemia (OR 5.2; 95% CI: 2.4–11.1) [9,55,82,107].
In the region, multiple social, economic, and health factors converge to increase the vulnerability of certain populations to Candida infections [10,12]. In contexts marked by malnutrition, essential micronutrient deficiencies, overcrowding, and poor basic sanitation, gaps in early diagnosis and restricted access to modern antifungal treatments are key determinants in the onset and progression of the disease [105,113,115,116,117]. Added to this is the high prevalence of comorbidities such as untreated HIV/AIDS and poorly controlled diabetes, which compromise the patient's immunity and promote fungal invasion. Furthermore, the widespread use of broad-spectrum antibiotics without prior microbiological evaluation promotes imbalances in the microbiota, and favors the selection of resistant strains [118,119,120,121]. This scenario has led to IC no longer being a strictly nosocomial phenomenon and becoming established as a public health problem in the region, yet to be recognized or prioritized by government authorities.
4.1. Health Conditions and Risk of Fungal Infection in Migrant and Displaced Populations
In LA&C, structural conditions of inequality—including chronic poverty, insufficient access to safe drinking water and basic sanitation, geographic isolation of rural communities, and systemic violence—create a favorable environment for the development of both mucocutaneous and IC [10,122]. These vulnerabilities are exacerbated by a high burden of chronic and infectious diseases, such as HIV/AIDS, diabetes, tuberculosis (TB), and malnutrition, which weaken the immune system and increase susceptibility to colonization by Candida spp. The situation is further complicated by fragmentation in health systems, limited availability of mycological diagnostic laboratories, and logistical and economic barriers to obtaining adequate antifungal treatments. These deficiencies prolong diagnostic times and delay the initiation of timely treatment, increasing the risk of severe complications, especially among the most marginalized populations [12,105,116,123].
Migrants and displaced persons living in environments of conflict and extreme violence face multiple social and health conditions that increase their vulnerability to Candida infections, both in their mucocutaneous and invasive forms. The combination of overcrowding in informal camps, deficiencies in drinking water and sanitation, and malnutrition compromises immune function and creates conditions conducive to fungal colonization of the skin and mucous membranes, facilitating the onset of superficial infections and their progression to more severe forms [10,80,105,124,125]. This situation is exacerbated by the high burden of poorly controlled chronic diseases—such as untreated HIV/AIDS, unregulated diabetes mellitus, and tuberculosis—which aggravate immune deterioration, reduce the effectiveness of epithelial barriers, and accelerate the clinical progression of candidiasis [105,116,118,119,126,127]. The precarious nature of health services, especially in mobile clinics or border facilities, promotes the empirical and prolonged use of antibiotics without diagnostic support, as well as the improper handling of invasive devices, both of which alter the microbiota and increase the risk of candidemia [121,128,129]. In addition, certain demographic and environmental determinants—such as advanced or neonatal age, gender, ethnicity, and occupational exposure to humid or tropical environments—act as catalysts for fungal colonization and the development of infections [10,122,130,131]. Table 2 compares the main clinical conditions and risk factors for IC between the general population and migrant or displaced groups. [1,50,114,127,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155].
To understand how social determinants and environmental conditions amplify the risk of Candida infection in displaced populations, it is essential to identify the most relevant factors involved. The following are the main elements that, together, create a scenario conducive to the onset and worsening of candidiasis in these highly vulnerable contexts:
4.1.1. Socio-Environmental Conditions and Social Determinants
- Overcrowding and informal settlements: in contexts such as Venezuelan refugee camps in Colombia and Haitian migrant settlements in the Dominican Republic, it is common for families to live in extremely small spaces (less than 5 m² per person). These overcrowded conditions not only make privacy and hygiene difficult but also increase body moisture and skin maceration, promoting the development of fungal infections. In a recent survey, 28% of adult women in these environments reported intertriginous or vulvovaginal candidiasis [156]. An institutional report (2019–2020) on Mexico's southern border with Guatemala revealed that Central American migrants housed in shelters without adequate ventilation showed a high prevalence of skin infections. Microbiological field studies found that 33% of cases with interdigital rashes tested positive for Candida, mainly C. parapsilosis, highlighting how the tropical climate, combined with poor hygiene, increases susceptibility to these infections [157].
- Limited access to drinking water and sanitation: in the Northern Triangle of Central America (Honduras, El Salvador, and Guatemala), recent studies have shown that more than 40% of informal settlements do not have a continuous supply of chlorinated water. This limitation prevents adequate hand and surface hygiene, creating conditions conducive to the proliferation of yeasts in the environment. Such microenvironments become potential reservoirs for infections such as cutaneous and vulvovaginal candidiasis [158]. In Bolivia, data collected between 2018 and 2019 in rural areas inhabited by returning migrants showed that only 35% of homes had adequate latrines. This deficiency in basic sanitation increases the environmental microbial load and favors fungal colonization of the skin and moist areas of the body, especially in crowded conditions and hot climates [159].
- Malnutrition and immune deficiency: an internal epidemiological surveillance report conducted between 2018 and 2019 among the displaced population in the department of Arauca, Colombia, revealed that 42% of children and 28% of pregnant women suffered from acute or chronic malnutrition. In this context, 30% of children with oral candidiasis showed signs of malnutrition, and within this group, 18% developed candidemia within less than ten days [160,161]. The lack of essential micronutrients—such as vitamins A and D and zinc—impairs both cellular and humoral immunity, promoting the transition of Candida from superficial colonization to systemic infection. This risk is exacerbated in displaced adults with irregular access to basic nutritional supplements [160].
4.1.2. Prevalent Comorbidities in Migrants and Displaced Persons
- HIV/AIDS: according to an institutional report for the period 2018–2019, the prevalence of HIV among Venezuelan migrants settled in Colombia was 3.2%, of whom 45% were not receiving antiretroviral treatment and had CD4 counts below 200 cells/µL. In this cohort, 38% developed oral candidiasis, and 12% developed esophageal candidiasis during the first year of follow-up [162]. A retrospective analysis conducted after the 2010 earthquake in Haitian displacement camps revealed that many people were living with HIV patients in advanced stages of the disease and without access to antiretroviral therapy. In this group, 55% were diagnosed with recurrent mucocutaneous candidiasis, and 12% had candidemia, which was associated with a 65% mortality rate due to the lack of timely diagnosis and effective antifungal drugs [163].
- Type 2 diabetes mellitus: in agricultural export plantations in Central America, studies conducted among migrant workers showed a prevalence of undiagnosed diabetes of 16%. Of this group, 30% had candidal vulvovaginitis and 8% developed complicated forms of cutaneous candidiasis, including infected ulcers [119,120]. Similarly, an internal epidemiological surveillance report on displaced indigenous communities in Peru documented that 14% of older adults had uncontrolled diabetes (fasting glucose greater than 126 mg/dL). In these patients, interdigital candidiasis occurred in 27% of cases, and an RR of 2.8 (95% CI: 1.6–4.9) was estimated for the development of disseminated candidiasis after hospitalization [164].
- Tuberculosis and co-infections: in camps for displaced persons located in the border areas between Venezuela and Colombia, a prevalence of tuberculosis (TB) of 350 cases per 100,000 inhabitants has been documented, with a high frequency of HIV/TB co-infection. This combination increases the risk of IC. A retrospective study conducted in Bogotá revealed that 22% of patients with TB/HIV coinfection developed candidemia, with an associated mortality rate of 58% [165]. On the other hand, a descriptive study in Guatemala observed that, in co-infected individuals, the presence of extrapulmonary TB—particularly in its peritoneal or gastrointestinal forms—caused damage to the digestive mucosa, facilitating the translocation of Candida spp. into the body. As a result, 14% of these patients developed intra-abdominal candidiasis [166].
4.1.3. Exposure to Iatrogenic Factors
- Use of antibiotics in mobile clinics and shelters: between 2019 and 2020, in mobile clinics providing medical care to Nicaraguan migrants in Mexican territory, it was observed that 78% of patients with fever were treated with broad-spectrum antibiotics, such as ceftriaxone or carbapenems, without prior blood cultures. This practice was associated with the onset of mucocutaneous candidiasis in 26% of cases and candidemia in approximately 5%, although significant underreporting is presumed due to the lack of diagnostic laboratories in these settings [167]. The widespread empirical use of antibiotics without proper assessment of the risk of fungal infection has contributed to the disruption of normal microbiota, facilitating the overgrowth of Candida spp.
- Use of invasive devices in border hospitals: an internal surveillance report from 2020, based on data from migrant reception units in Tapachula (Mexico–Guatemala region), found that 42% of patients hospitalized for sepsis required CVC insertion. Among these patients, 12% developed candidemia, which corresponds to a significantly elevated risk (OR 3.5; 95% CI: 2.0–6.1). Furthermore, due to a lack of specialized personnel, protocols for early catheter removal are not properly implemented, prolonging exposure to fungal biofilm and increasing the likelihood of invasive infections [168].
4.1.4. Demographic and Vulnerability Factors
- Age and gender: an epidemiological surveillance study in Colombia (2018–2019), focusing on displaced children, revealed that 18% of newborns from temporary shelters developed oral candidiasis in their first week of life. This finding was related to low birth weight (less than 2,500 g) and maternal malnutrition, conditions that are common in contexts of forced displacement [160]. On the other hand, a study on reproductive health in migrant women (2019) found that 34% of women living in border settlements experienced episodes of vulvovaginal candidiasis in the last year, mainly linked to malnutrition, pregnancy, and limited access to adequate gynecological services [169].
- Ethnicity and inequalities: in displaced Guaraní indigenous communities in Paraguay, the rate of cutaneous candidiasis was almost three times higher than that observed in nearby urban populations. This difference has been attributed to difficulties in accessing adequate health services and language barriers that limit timely care [170]. Similarly, an internal report on Haitian migrants in the Dominican Republic reported that 46% of adults with HIV developed oral candidiasis, compared to 28% of the non-migrant population. Language barriers and experiences of discrimination contribute significantly to delays in diagnosis and treatment [171].
4.1.5. Environmental and Occupational Conditions
- Agricultural work and environmental exposure: among Central American migrants employed on sugar cane plantations in Guatemala, a 15% prevalence of skin colonization by C. parapsilosis has been identified, which is associated with repeated contact with humid environments and contaminated surfaces, such as wet soil and stagnant water [172]. On the other hand, an epidemiological surveillance report conducted in fruit-growing areas in Peru found that 22% of migrant workers of Peruvian and Bolivian origin developed interdigital candidiasis. This condition could be related to repeated exposure to insecticides, which alter the normal microbial flora of the skin [173].
- Climate and microenvironments: according to an epidemiological surveillance report, climatic conditions in coastal areas of Central America—characterized by humidity levels above 80% and constant temperatures around 28°C—are favorable for the growth of yeast on the skin and mucous membranes. In Honduras, migrants traveling along routes near the coast were found to have intertriginous candidiasis in 31% of cases, a figure considerably higher than the 12% reported among those traveling along mountainous routes [174].
5. Diagnosis of IC in LA&C: Barriers and Diagnostic Methods in Resource-Limited Settings
In LA&C, the diagnosis of candidiasis, both mucosal and invasive, is hampered by poor healthcare infrastructure, a lack of trained personnel, and the high costs associated with state-of-the-art reagents. Although conventional methods such as direct microscopy with KOH or Gram staining and Sabouraud agar cultures are available, the absence of more sophisticated diagnostic tools—such as chromogenic media (CHROMagar™Candida), automated blood culture systems (BacT/ALERT, BACTEC), MALDI-TOF spectrometry, serum biomarkers (1,3-β-D-glucan [BDG]), and molecular techniques (qPCR, LAMP)—hinders early detection, especially in rural areas [12,117,175,176,177,178,179,180].
Table 3 presents a detailed comparison between the availability of diagnostic and therapeutic methods, as well as the burden of disease, among the general population and migrant or displaced groups in various countries in LA&C [1,12,51,117,175,180,181,182].
In settings with limited resources, mucocutaneous candidiasis—in its oral, vulvovaginal, and intertriginous forms—is usually diagnosed solely by clinical evaluation, observing signs such as whitish plaques, erythema, intense itching, or maceration in the folds. This practice leads to diagnostic errors and delays in treatment [183,184]. Similarly, candidemia is often suspected presumptively in patients with persistent fever without an apparent source and signs of sepsis, especially in settings where blood cultures are not available. This form of delayed diagnosis delays the start of antifungal treatment and can raise mortality rates to over 60% in vulnerable populations [185,186].
In intermediate-level health centers, clinical suspicion is complemented by direct microscopy (KOH 10% or Gram staining), a method that shows sensitivities of 70%–85% for mucocutaneous forms, but without identification of the species involved [180]. To diagnose invasive infections, many regional hospitals use manual blood cultures, which take 3–5 days to produce results. However, these methods have limited sensitivity (≈ 70%–80%) and depend on correct inoculation techniques; deficiencies such as inadequate incubators or breaks in the cold chain can lead to false negatives in up to 30% of cases [12,180,187].
In high-complexity hospitals, such as those located in São Paulo, Mexico City, or Bogotá, automated blood culture systems—such as BacT/ALERT and BACTEC—are available, significantly reducing detection times to 24 and 48 hours. In addition, the use of chromogenic media facilitates the rapid identification of non-albicans isolates [117,188]. However, rural centers often lack these technologies due to budget constraints and power supply problems [12,175]. In reference laboratories in large cities, advanced techniques such as mass spectrometry (MALDI-TOF), BDG quantification, and molecular methods (qPCR) are also used, offering sensitivities greater than 80% and results in less than 8 hours. Their adoption is limited by the high cost per test (≈ USD 100 for BDG) and dependence on imported supplies [111,117,177,179].
In scenarios of mass displacement, overcrowding, lack of sanitation, malnutrition, and access barriers cause significant delays in the diagnosis and treatment of mucocutaneous and IC [180,189]. Although the implementation of direct microscopy (KOH 10%, Gram staining) with clinical-microscopic algorithms adapted to resource-limited settings has improved initial detection, these methods do not allow for species identification [12,61,111,175,176]. Deficiencies persist due to a lack of incubators, unstable power supplies, a shortage of specialized personnel, and the costs associated with reagents such as BDG or CHROMagar™. In addition, many centers do not have access to automated blood culture or qPCR systems [111,175,179].
To understand and address the limitations that affect the timely diagnosis of Candida infections in resource-poor settings, the main obstacles associated with poor infrastructure, shortage of trained personnel, difficulties in providing diagnostic supplies, and sociocultural factors that impact medical care are described below:
5.1. Barriers and Limitations in the Diagnosis of Candidiasis
5.1.1. Infrastructure and Logistics
- Lack of local laboratories: mobile health centers and small shelters are not equipped with adequate biosafety facilities or protocols for mushroom cultivation. As a result, samples must be sent to reference laboratories, which are often located far away. This involves transportation without a cold chain, which increases the risk of contamination or decreases the viability of the fungi, reducing crop yields to less than 50% [9,12].
5.1.2. Human Resources and Training
- High turnover of volunteer staff: in NGOs operating in camps, constant staff turnover prevents continuity in the use of protocols and hinders the transfer of specialized knowledge. Although there are no exact figures, this recurring problem has been documented in border environments [111,190,191,192].
5.1.3. Costs and Availability of Reagents
- Scarce and expensive basic reagents: in many countries in the Andean region and the Caribbean, essential reagents such as KOH 10% solutions and Gram stains must be imported, which increases the cost of each test by approximately USD 5–10. This is a difficult expense for mobile clinics with limited resources to bear [111,176,180,189,193].
- Limited access to state-of-the-art testing: serological tests such as BDG or molecular methods such as qPCR are not covered by public health systems and are only offered in reference laboratories, usually located in capital cities. This situation forces patients to travel long distances to access these diagnostics [9,117,176,194].
5.1.4. Social and Cultural Limitations
- Distrust of the healthcare system: many displaced persons have been victims of violence or discrimination, which generates mistrust of medical services and reduces their willingness to participate in procedures such as blood tests. Although there are no specific data on candidiasis, reproductive health studies show that more than 40% of displaced populations avoid going to official centers for this reason [12,41,125,142,192].
- Language and communication barriers: in Haitian refugee shelters in the Dominican Republic and also in Venezuelan indigenous communities, a lack of fluency in Spanish hinders communication with healthcare personnel. Qualitative studies indicate that up to 30% of consultations are postponed or interrupted due to language problems or a lack of interpreters [11,131,192,195,196].
To ensure timely and efficient diagnosis in forced displacement settings, the following recommendations are proposed to optimize resources, train local staff, and strengthen care networks:
5.2. Recommendations for Strengthening Diagnosis in Areas of Forced Displacement
5.2.1. Optimization of Low-Cost Methods
- Technical training in KOH: it is recommended to train local staff through weekly workshops focused on the processing and interpretation of exudates using 10% potassium hydroxide (KOH 10%). The implementation of this strategy in areas with limited resources has been shown to improve diagnostic accuracy [106,180,189,195,197].
- Rotary direct microscopy with calcofluor: several studies have shown that calcofluor is consistently more sensitive than KOH and sometimes comparable to more sophisticated diagnostic methods. Its usefulness as a rapid diagnostic technique makes it especially valuable in resource-limited environments. In this context, the possibility of sharing UV equipment between nearby camps is suggested to facilitate the assessment of mucocutaneous lesions. This strategy could be applied in countries such as Haiti to reduce the false negative rate [180,189,198,199].
5.2.2. Implementation of Simplified Algorithms
- Adapted use of the “modified Candida Score” in primary care: in community settings where state-of-the-art testing is not available, a simplified version of the “Candida Score” is proposed for initiating empirical treatment. In patients with fever without apparent source and at least three of the following criteria—recent antibiotic use, presence of CVC, and malnutrition—it is recommended to initiate FCZ if the KOH test is positive. If BDG is available, consider echinocandins when this marker is positive. Studies in ICUs in Latin America show that a score equal to or greater than 3 predicts candidemia with a sensitivity of 70% [117,188].
- Creation of multilingual visual guides: designing and distributing illustrative materials on clinical signs of candidiasis, translated into Spanish, Haitian Creole, and indigenous languages, can be key to improving recognition of the infection. Experiences in community health programs have shown that incorporating these guides improves early detection by 18% [7,12,189,200].
5.2.3. Surveillance and Reference Networks
- Development of collaborative networks for sample processing: it is proposed to implement a referral system between camps and laboratories located in nearby urban areas, ensuring the transport of samples under appropriate cold chain conditions. This measure, accompanied by regular exchanges of volunteer microbiologists, has proven effective: in Latin America, agreements between mobile units and universities reduced the analysis time for mycological samples from seven to three days [6,12,111,175,176,187].
- Strengthening tele-mycology networks: the use of technology to share diagnostic images (cultures, smears, lesions) in real-time via mobile networks or satellite connections can significantly improve diagnostic accuracy. Creating virtual links with regional mycology experts would enable constant supervision and technical support, with at least one specialist recommended for every 5,000 displaced persons [178,197,201,202,203].
5.2.4. Funding and Strategic Alliances
- Ensure donations of basic supplies: we propose coordinating with organizations such as GAFFI and PAHO to deliver essential supplies (KOH, dyes, culture media) to mobile clinics in border areas and hard-to-reach camps. Since 2019, these initiatives have made it possible to supply resources to more than 20 mobile units in Colombia and Peru, strengthening their diagnostic capacity [6,7,106,176,189,200,204]
- Formalize agreements with regional universities: emphasis is placed on the need to integrate essential diagnostics and strengthen national and hospital diagnostic networks. It is also proposed to establish biannual agreements with local universities for the provision of diagnostic supplies to reduce and lower transportation expenses and expand diagnostic coverage in remote areas [7,12,106,175,176,187,200].
6. Antifungal Treatment of IC in LA&C: Availability of Antifungals and Antifungal Resistance
Globally, echinocandins and L-AmB are included in the essential drug lists of most high-income countries, and their cost is often covered by health systems or insurance. As a result, mortality from candidemia is reduced to 25%–40%, in contrast to the higher figures observed in LA&C [111,176,193,205,206,207]. Although resistance to FCZ in N. glabratus (25%–33%) and C. tropicalis (8%–12%) is similar to the figures recorded in the region [1,8,59,60,105,182], the availability of broad-spectrum azoles—such as voriconazole (VCZ), posaconazole (PCZ), and isavuconazole (ISZ)—allows for more effective management of infections caused by non-albicans isolates. In the specific case of C. auris, a yeast (with more than 90% resistance to FCZ and 30%–40% resistance to AmB, echinocandins are the only effective treatment available [63,64,208].
In the LA&C region, empirical treatment of IC continues to be based on generic FCZ, which is available in most second-level hospitals [6,175,194,209]. However, growing resistance in clinical isolates of C. tropicalis (12%–15% in Brazil and Argentina) [210,211], N. glabratus (10%–12% of resistant or reduced-sensitivity strains) [51,72] and C. parapsilosis (8%–10% resistant strains in multicenter studies) [1,51,61,72,212] has forced a rethinking of the use of this regimen. Echinocandins (CAS, ANF, MCF), recommended for severe candidemia or infections caused by non-albicans strains, are only available in high-complexity urban hospitals due to their high cost (~$1,000–$1,500/day) [56,57,213]. In places where these molecules are not available, conventional AmB (D-AmB) continues to be used despite its nephrotoxicity, while L-AmB, which is preferred for critically ill patients, remains out of reach for most secondary hospitals (~$5,000 per vial) [56,193,205,209]. It has been shown that a delay of more than 48 hours in starting treatment with an echinocandin or L-AmB, or when resistant strains are managed with FCZ, is associated with significant clinical worsening [117,185,214]. Table 3 summarizes the treatment options for IC in the general population and displaced persons or migrants in LA&C countries.
At the regional level, less than 5% of C. albicans isolates are resistant to FCZ, while the figures for C. tropicalis (12%–15%) and N. glabratus (10%–12%) are considerably higher [210,211,215]. As for echinocandins, resistance remains below 5%, although mutations in the FKS1 gene of N. glabratus have been detected in Brazil and Argentina that could affect their efficacy and clinical isolates of echinocandin-resistant N. glabratus strains resistant to echinocandins have been reported in Colombia, associated with the R665G substitution, a rare mutation linked to resistance mechanisms (data in press). C. auris, which has caused outbreaks in Colombia and Venezuela, exhibits resistance to FCZ greater than 90% and resistance to AmB of 30%–40%, according to local reports [65,216,217].
In migrant and displaced populations, antifungal treatment is mainly restricted to the use of generic FCZ and, in some cases, D-AmB. The high cost and lack of equipment to administer continuous infusions make it difficult to access echinocandins and L-AmB—indicated for severe candidemia—in camps and mobile clinics [176,218,219]. Although more than 90% of isolates are FCZ-sensitive C. albicans, the presence of C. tropicalis and N. glabratus complicates empirical therapy, resulting in a high mortality rate of 55%–65% when only azoles (FCZ) and D-AmB are available [6,111,218,219]. In contrast, in refugee camps with greater logistical capacity, especially in Europe and North America, humanitarian organizations often have access to echinocandins for non-neutropenic candidemia, L-AmB for critical cases, and broad-spectrum azoles such as VCZ or PCZ for refractory infections, reducing mortality to 30%–40% [80,122,142]. In a narrative review of 15 original Lebanese studies published between 1998 and 2023, it was found that isolates from blood represent approximately 17% of all Candida isolates, but have a higher proportion of resistant profiles, especially in N. glabratus and C. auris. Resistance to FCZ in C. albicans is moderate (2%–33%), while in cases of candidemia caused by N. glabratus, it can reach up to 100%, with additional reports of high resistance to echinocandins. Meanwhile, C. auris, which emerged in hospitals during the pandemic, has shown resistance to most antifungal agents except echinocandins, even in blood isolates [128].
In situations of forced displacement and limited resources, there are critical barriers that hinder the adequate treatment of Candida infections:
- Restricted availability of essential antifungals: in most LA&C countries, access to antifungals is limited mainly to generic FCZ, due to its low cost and early inclusion in national essential medicines lists [10,193,206]. Although this drug is available, it is not the ideal option for candidemia in critically ill patients, as up to 50% of non-albicans isolates—such as N. glabratus, P. kudriavzevii, and C. auris—have reduced sensitivity or intrinsic resistance to FCZ.
- Suboptimal administration of D-AmB: in the absence of echinocandins, D-AmB is frequently used as an alternative. However, to ensure its safe use, constant monitoring of renal function and electrolyte balance is required, as well as continuous administration of intravenous fluids and potassium salts [207]. In hospitals with limited resources, such conditions are often inadequate. This has led many professionals to reduce doses as a precaution, especially when there is no access to ICUs or adequate laboratories. Additionally, D-AmB depends on a cold chain, which is challenging in hot environments with unstable power supplies.
- Increase in antifungal-resistant strains: during the C. auris outbreak in Venezuela, all isolates showed resistance to FCZ and VCZ, and 50% had high minimum inhibitory concentrations (MIC) against AmB [208]. Although echinocandins are considered the almost exclusive therapeutic resource in these cases, strains with reduced sensitivity to these drugs are beginning to be detected [65,217]. At the same time, N. glabratus shows increased resistance to azoles, and C. parapsilosis shows mutations associated with prolonged treatment with echinocandins [215,220,221,222]. In Brazil, clusters of FCZ-resistant C. parapsilosis have been documented [8,221,222,223], and in areas of armed conflict, the absence of surveillance and infection control facilitates their unnoticed spread.
- Incomplete treatments: the minimum duration of treatment for candidemia should be 14 days from the last negative blood culture, extending in the presence of metastatic foci [112,117,185]. In displacement settings, it is common for patients to discontinue treatment after one week due to continuous displacement or depletion of medications in centers, which increases the risk of relapse and promotes the development of resistance.
- Inequality in costs and access: while FCZ is relatively affordable, echinocandins and L-AmB are too expensive for most centers and are only available in private clinics. In countries such as Haiti and Venezuela, public systems lack these drugs, and NGOs rarely include them in their emergency supplies due to budget constraints [121,193,194,206]. This means that, in many refugee camps, optimal treatment for candidemia remains inaccessible.
- Lack of complementary critical support: effective management of IC goes beyond the provision of antifungal agents. It requires intensive care, surgical interventions to control foci (such as valve replacement in endocarditis or abscess drainage), as well as life support—dialysis in cases of renal failure or MV [106,176,185]. In conflict-affected areas, these resources are often lacking [194], meaning that even with adequate antifungal treatment, the outcome can be fatal due to the lack of comprehensive clinical support or access to interventions that remove the source of infection.
7. Access to Health Services and Antifungal Treatment in Areas of Conflict and High Violence in LA&C
In LA&C, fragmented healthcare systems, uneven coverage, and scarce resources—both human and financial—seriously hinder access to medical care and antifungal treatments. Despite advances in the development of clinical practice guidelines and the implementation of antifungal optimization programs, difficulties persist in ensuring timely specialist consultations, quality diagnostic tests, and second-line therapies [12,175,224]. These limitations disproportionately affect rural, border, and vulnerable populations, where delays in treatment initiation and administration of suboptimal regimens significantly increase morbidity and mortality associated with IC [225].
A network of deficiencies—fragmented healthcare systems, delays in diagnosis, and a lack of effective therapies—contributes to high mortality rates and complications in candidiasis. In contexts of forced displacement, the lethality rate for candidemia exceeds 65%, compared to 45%–60% in general hospitals in the region, and up to 12% of cases of mucocutaneous candidiasis lead to invasive forms in patients with concomitant risk factors [119,140,226,227]. Early detection and treatment are essential: every delay in diagnosis and initiation of antifungal therapy significantly increases mortality from IC [106,194]. Wars and chronic violence undermine health systems in multiple ways: destruction of facilities, flight or attacks on health personnel, disruption of supply chains, and insecurity that prevents patients from attending health centers [11,35,38,80,228].
In situations of war, crisis, or forced displacement, healthcare for Candida infections faces serious obstacles that undermine its effectiveness:
- Forced internal migration and informal settlements: internally displaced persons and refugees living in temporary camps often have limited or no access to adequate healthcare services. In these contexts, cases of candidemia are rarely diagnosed or treated with antifungal medication, and deaths are often not officially reported [38,142,229].
- 2. Risks for patients and healthcare personnel: in areas of active violence, transfer to a medical center can pose a life-threatening risk (bombing, snipers, checkpoints). In conflicts such as the one in Syria, attacks on hospitals and healthcare personnel have been documented, interrupting essential treatments for severe mycoses [230].
8. Regional Perspective
In contexts of armed conflict and intense violence in LA&C, health systems are severely weakened: hospitals are attacked or closed [191,230,232], medical personnel are displaced [230,233], and laboratories cease to operate [191]. This situation favors the spread of fungal infections, such as mucocutaneous and IC, due to a combination of malnutrition [131,161], untreated HIV/AIDS [118,126,144], uncontrolled diabetes [119,120,140], overcrowding [11,124,125], and indiscriminate use of antibiotics in mobile or informal clinics [121,234].
8.1. Mexico
Cartel violence in states such as Sinaloa, Guerrero, and Tamaulipas has caused the collapse of multiple rural clinics and disrupted drug distribution routes [235,236], forcing many Central American migrants in transit through Chiapas and Oaxaca to seek care at mobile clinics in precarious conditions, where candidiasis is diagnosed solely based on clinical signs (white patches in the mouth, vaginal erythema) without microscopic confirmation [229], and between 2020 and 2021, an outbreak of IC associated with C. auris was identified in three ICUs at a referral hospital in Mexico, in intubated COVID-19 patients with CVCs, with more than 76% of isolates obtained from the catheter [54]; these clinics, lacking a stable power supply and incubators, use KOH 10% to diagnose mucocutaneous candidiasis (sensitivity ≈ 75%; specificity ≈ 85%), but do not have Sabouraud agar culture available, so empirical treatment with FCZ is chosen, which increases the risk of therapeutic failure against resistant strains such as N. glabratus [215,237].
8.2. Haiti:
In Haiti, political crisis and gang violence have rendered approximately 70% of health centers inoperable, forcing thousands of people to live in informal settlements without adequate medical care [31,153,190]. After the earthquake, in camps for displaced persons with intermittent access to antiretroviral therapy, 55% of patients with advanced HIV presented with recurrent mucocutaneous candidiasis, and 12% progressed to candidemia, with a mortality rate of 65% due to late diagnosis and lack of timely treatment [190]. The lack of functional laboratories means that blood samples must be sent to Port-au-Prince, with delays of 5–7 days, resulting in a loss of viability of up to 50% in Candida due to failures in the cold chain [238]. Since 2022, the implementation of mycological telemedicine via WhatsApp has made it possible to share KOH smear images with mycologists in Santiago, Chile, improving diagnostic accuracy by 30%, despite connectivity limitations and irregular supplies of reagents [201].
8.3. North Triangle (El Salvador, Guatemala, Honduras)
The humanitarian crisis resulting from gang violence and forced evictions continues to cause prolonged displacement in El Salvador, Guatemala, and Honduras. As a result, many people are forced to remain in urban shelters whose capacity has already been greatly exceeded [239,240]. In rural agricultural areas of Guatemala, workers face conditions that favor the onset of fungal infections, such as interdigital candidiasis, which has a prevalence of 15% to 22%. This phenomenon is mainly associated with frequent contact with humid environments and waterlogged soils, with a predominance of colonization by C. parapsilosis and C. tropicalis [23,130,172]. In shelters located in El Salvador, it has been documented that 33% of displaced women suffered from vulvovaginal candidiasis during the last year. This situation is exacerbated by chronic child malnutrition, which affects 25% of the population, and by the lack of adequate gynecological services. The treatments administered in these settings are usually empirical, mainly using FCZ and topical clotrimazole [241,242]. On the other hand, the widespread and unregulated use of broad-spectrum antibiotics in mobile clinics represents an added risk factor. In 78% of patients presenting with fever, ceftriaxone or carbapenems are administered without prior blood cultures, which promotes microbial imbalance and excessive yeast growth. As a result, there is a 26% incidence of mucocutaneous candidiasis and a 5% incidence of candidemia, although the latter could be significantly underreported due to limitations in clinical and diagnostic surveillance [121,167,243].
8.4. Colombia
After more than five decades of internal conflict, Colombia has more than six million internally displaced persons [244]. In Arauca, a cohort of children with oral candidiasis showed a 30% rate of malnutrition (z-score < –2); of these, 18% developed candidemia in less than 10 days, largely due to immunosuppression secondary to malnutrition [160,161]. In mobile clinics on the border with Venezuela, diagnosis is based on direct microscopy with KOH and manual blood cultures, with delays of 5–7 days and a sensitivity of around 70% [245]. In an observational study conducted in Cali, which analyzed 257 TB deaths in 2017, it was found that 24.5% corresponded to patients with HIV coinfection, which shows a significant mortality burden associated with this syndemic. The most affected population consisted of young men in highly vulnerable social conditions, with low health system coverage, malnutrition, and psychoactive substance use [126]. Although GAFFI has supplied echinocandins to public hospitals in border areas, these cover less than 15% of the demand, forcing the use of empirical FCZ against resistant non-albicans strains [209].
8.5. Venezuela
Venezuela's deep political and economic crisis has caused the collapse of the healthcare system, with shortages of supplies and medicines, mass migration, and virtually nonexistent epidemiological surveillance [154,155]. In the state of Táchira, 28% of displaced women suffered from vulvovaginal candidiasis, associated with malnutrition and lack of gynecological care. In informal clinics, resistance to FCZ was detected in up to 12% of C. parapsilosis isolates [11,39,246]. Migration to Colombia and Brazil has spread this burden: in Colombian shelters for Venezuelans, 3.2% of migrants with untreated HIV developed oral candidiasis in 38% of cases and esophageal candidiasis in 12% during the first year [192]. Access to echinocandins is practically nonexistent in Venezuela and very limited in referral centers such as Bogotá and São Paulo, which delays adequate treatment and places mortality from candidemia in migrants above 60% [11,40,156].
8.6. Brazil
Although Brazil is not experiencing formal conflict, violence in the favelas and lack of supplies in the Amazon create conditions that facilitate outbreaks of fungal infections [247]. In Manaus, cases of candidemia caused by echinocandin-resistant N. glabratus were documented, attributable to mutations in the FKS1 gene detected in 2022. This complicates treatment in regional hospitals without access to L-AmB [56,112,213]. In the favelas of Rio de Janeiro, there was a 31% incidence of intertriginous candidiasis in women, linked to overcrowding, poor sanitation, and malnutrition [42,112,248]. The Unified Health System (SUS) guarantees the supply of FCZ, but echinocandins are available in less than 20% of tertiary public hospitals, mainly in São Paulo and Brasília [248].
8.7. Peru
In regions of the Amazon and Andean areas affected by conflict, indigenous communities have a malnutrition rate of 25% and very limited access to medical care [48,114,139]. In migrant shelters in Lima, 22% of adults suffered from interdigital candidiasis, associated with construction work and lack of drinking water [114,139]. Mobile clinics in rural areas mainly use KOH and manual blood cultures; delays in results have led to undetected cases of candidemia, with a mortality rate of over 60% [249]. Although the Comprehensive Health Insurance (SIS) covers FCZ, the echinocandins and L-AmB are not available outside Lima, forcing the use of suboptimal regimens in areas with residual violence [250].
9. Recommendations for Future Research
People displaced by conflict and violence in LA&C live in adverse environments—overcrowded shelters, poor access to safe drinking water, malnutrition, and fragile health systems—that can increase the risk of fungal infections such as candidiasis [131,192,195]. While this infection is traditionally associated with the use of broad-spectrum antibiotics, diabetes, or HIV/AIDS, in these populations, psychosocial stress, overcrowding, and poor nutrition exacerbate the risk of both mucocutaneous candidiasis (oral and vulvovaginal) and invasive forms [8,41,49,124].
Few studies have explored this reality in depth: some have documented significant rates of vulvovaginal candidiasis, with the appearance of non-albicans isolates, and isolated cases of candidemia in camps following disasters [18,251]. However, these studies tend to focus on urban host populations, leaving out both camp dwellers and migrants in transit [252]. The lack of mycology laboratories in the field and limited access to antifungals hinder timely diagnosis and treatment [176,253].
To fill these gaps, multicenter studies in displaced camps are required that:
- Quantify the prevalence of candidiasis (mucocutaneous and invasive) and its distribution by species, including resistance profiles.
- Identify specific risk factors of displacement, such as hygiene conditions, sanitary access barriers, and psychological stress.
- Evaluate interventions such as improved sanitation, educational programs, and the use of broad-spectrum antifungals in vulnerable populations [125].
To design a comprehensive research plan on candidiasis in displaced populations, six strategic lines are proposed, ranging from prevalence studies and antifungal profiling to clinical trials and the integration of a One Health approach:
- 1.
-
Multicenter prevalence studies
- Conduct cross-sectional studies in camps and shelters to quantify the prevalence of oral and vulvovaginal candidiasis, itemized by sociodemographic factors, nutritional status, and HIV co-infection [228].
- 2.
-
Species identification and antifungal profile
- Create mobile laboratories or partnerships with regional laboratories (for example, in hospitals of host cities) to differentiate species and perform MIC sensitivity tests on dilution medium [256].
- Establish a regional registry of isolates from migrants and displaced persons in LA&C, including genetic typing using MLST (multilocus sequence typing) [257].
- 3.
-
Study of risk factors associated with displacement
- 4.
-
Design clinical trials to evaluate preventive and therapeutic interventions
- Conduct a randomized study in patients with recurrent vulvovaginal candidiasis to compare short treatment regimens with FCZ versus topical therapy with azoles (miconazole), evaluating adherence and tolerance [260].
- 5.
-
Systematic monitoring in camp health care centers
- 6.
-
Integration of a One Health approach
- Establish partnerships with veterinarians and local bioresource centers to identify environmental reservoirs of Candida in temporary settlement sites [106].
Author Contributions
Conceptualization, PR, JMO; Methodology, PR, JMO; Software, JCM; Validation, PR, JMO, JCO; Formal analysis, PR, JMO, JCM; Investigation, PR, JMO; Resources, PR, JMO; Data curation, PR, JCM, JMO; Drafting—preparation of the original draft, PR, JMO,JCM; Drafting—review and editing, PR, JMO, JCM; Visualization, PR, JMO; Supervision, PR; Project management, PR. All authors have read and approved the published version of the manuscript.
Funding
This research received no external funding.
Statement of the Institutional Ethics Committee
Not applicable.
Informed Consent Statement
Not applicable.
Declaration of Data Availability
Suggested statements on data availability are available in the section “MDPI Research Data Policies” in https://www.mdpi.com/ethics.
Acknowledgments
Not applicable. The authors have reviewed and edited the result and assume full responsibility for the content of this publication.
Conflicts of interest:
The authors declare no conflicts of interest.
References
- Nucci M, Queiroz-Telles F, Alvarado-Matute T, Tiraboschi IN, Cortes J, Zurita J, et al. Epidemiology of Candidemia in Latin America: A Laboratory-Based Survey. [cited 2025 Jun 13]; Available from: www.plosone.org.
- Yapar N. Therapeutics and Clinical Risk Management Dovepress Epidemiology and risk factors for invasive candidiasis. 2014 [cited 2025 Jun 13]. [CrossRef]
- Falci DR, Pasqualotto AC. Clinical mycology in Latin America and the Caribbean: A snapshot of diagnostic and therapeutic capabilities. Mycoses [Internet]. 2019 Apr 1 [cited 2025 Jun 13];62(4):368–73. Available from: https://pubmed.ncbi.nlm.nih.gov/30614600/.
- Desai AN, Ramatowski JW, Marano N, Madoff LC, Lassmann B. Infectious disease outbreaks among forcibly displaced persons: An analysis of ProMED reports 1996-2016. Confl Health [Internet]. 2020 Jul 22 [cited 2025 Jun 13];14(1). Available from: https://pubmed.ncbi.nlm.nih.gov/32704307/.
- Denning DW. Global incidence and mortality of severe fungal disease. Lancet Infect Dis [Internet]. 2024 Jul 1 [cited 2025 Jun 13];24(7):e428–38. Available from: https://pubmed.ncbi.nlm.nih.gov/38224705/.
- GAFFI. The burden of serious fungal infections in Latin America 5 https://life-slides-and-videos.s3.eu-west-2.amazonaws.com/LIFE+articles/Burden+of+serious+fungal+infections+in+Latin+America.pdf. 2021.
- GAFFI. Report on activities for 2015. [cited 2025 Jun 14]; 2016. Available from: https://gaffi.org/wp-content/uploads/GAFFI-2015-annual-report.pdf.
- Bays DJ, Jenkins EN, Lyman M, Chiller T, Strong N, Ostrosky-Zeichner L, et al. Epidemiology of Invasive Candidiasis. Clin Epidemiol [Internet]. 2024 [cited 2025 Jun 13];16:549–66. Available from: https://pubmed.ncbi.nlm.nih.gov/39219747/.
- Cortés JA, Ruiz JF, Melgarejo-Moreno LN, Lemos E V., Cortés JA, Ruiz JF, et al. Candidemia en Colombia. Biomédica [Internet]. 2020 [cited 2025 Jun 13];40(1):195–207. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0120-41572020000100195&lng=en&nrm=iso&tlng=es.
- Jenks JD, Prattes J, Wurster S, Sprute R, Seidel D, Oliverio M, et al. Social determinants of health as drivers of fungal disease. EClinicalMedicine [Internet]. 2023 Dec 1 [cited 2025 Jun 13];66. Available from: https://pubmed.ncbi.nlm.nih.gov/38053535/.
- Plataforma R4V. Refugiados y migrantes de Venezuela | R4V https://www.r4v.info/es/refugiadosymigrantes [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://www.r4v.info/es/refugiadosymigrantes.
- Rodriguez Tudela JL, Cole DC, Ravasi G, Bruisma N, Chiller TC, Ford N, et al. Integration of fungal diseases into health systems in Latin America. Lancet Infect Dis [Internet]. 2020 Aug 1 [cited 2025 Jun 13];20(8):890–2. Available from: https://pubmed.ncbi.nlm.nih.gov/32619435/.
- IDMC. IDMC | GRID 2022 | 2022 Global Report on Internal Displacement [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://www.internal-displacement.org/global-report/grid2022/.
- ICRC. Latin America: Armed violence, conflict, internal displacement, migration and disappearances were main humanitarian challenges in 2021 | International Committee of the Red Cross [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://www.icrc.org/en/document/latin-america-armed-violence-conflict-internal-displacement-migration-disappearances.
- IDMC. 2024 Global Report on Internal Displacement (GRID) | IDMC - Internal Displacement Monitoring Centre [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://www.internal-displacement.org/global-report/grid2024/.
- UNICEF. Number of unaccompanied and separated children migrating in Latin America and the Caribbean hits record high. 2024 [cited 2025 Jun 13]. Available from: https://www.unicef.org/lac/en/press-releases/number-unaccompanied-children-migrating-latin-america-caribbean-hits-record-high.
- Caparini M DI. The Americas — Key general developments in the region. En: SIPRI Yearbook 2022: Arm Conflict and Conflict Management 2021. Stockholm: Stockholm International Peace Research Institute; 2022. 2022;77–81.
- Gousy N, Adithya Sateesh B, Denning DW, Latchman K, Mansoor E, Joseph J, et al. Fungal Infections in the Caribbean: A Review of the Literature to Date. Journal of Fungi [Internet]. 2023 Dec 1 [cited 2025 Jun 13];9(12):1177. Available from: https://www.mdpi.com/2309-608X/9/12/1177/htm.
- Bernal O, Garcia-Betancourt T, León-Giraldo S, Rodríguez LM, González-Uribe C. Impact of the armed conflict in Colombia: consequences in the health system, response and challenges. Confl Health [Internet]. 2024 Dec 1 [cited 2025 Jun 13];18(1):1–9. Available from: https://conflictandhealth.biomedcentral.com/articles/10.1186/s13031-023-00561-6.
- Izcara-Palacios SP. Violencia contra inmigrantes en Tamaulipas. European Review of Latin American and Caribbean Studies. 2012;93:3–24.
- UNHCR. UNHCR Dataviz Platform - Haiti: A multi-dimensional crisis leading to continued displacement [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://dataviz.unhcr.org/product-gallery/2024/10/haiti-a-multi-dimensional-crisis-leading-to-continued-displacement/.
- Restrepo-Betancur LF, Restrepo-Betancur LF. Migración en Sudamérica en los últimos treinta años. El Ágora USB [Internet]. 2021 Sep 17 [cited 2025 Jun 13];21(1):61–74. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S1657-80312021000100061&lng=en&nrm=iso&tlng=es.
- UNHCR. El Salvador, Guatemala and Honduras situation | Global Focus https://reporting.unhcr.org/el-salvador-guatemala-and-honduras-situation-global-report-2022 [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://reporting.unhcr.org/el-salvador-guatemala-and-honduras-situation-global-report-2022.
- UNHCR. Situación en Colombia | Enfoque global [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://reporting.unhcr.org/operational/situations/colombia-situation.
- BID. Migración interna en Venezuela: en busca de oportunidades antes y durante la crisis https://publications.iadb.org/es/migracion-interna-en-venezuela-en-busca-de-oportunidades-antes-y-durante-la-crisis [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://publications.iadb.org/es/migracion-interna-en-venezuela-en-busca-de-oportunidades-antes-y-durante-la-crisis.
- ICRC. Armed violence in Mexico and Central America continues to cause large-scale suffering | International Committee of the Red Cross https://www.icrc.org/en/document/armed-violence-mexico-and-central-america-continues-cause-large-scale-suffering [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://www.icrc.org/en/document/armed-violence-mexico-and-central-america-continues-cause-large-scale-suffering.
- THE GUARDIAN. More than 500 Mexicans flee to Guatemala to escape cartel violence in Chiapas | Mexico | The Guardian https://www.theguardian.com/world/article/2024/jul/30/mexico-chiapas-flee-to-guatemala [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://www.theguardian.com/world/article/2024/jul/30/mexico-chiapas-flee-to-guatemala.
- THE TIME. The pilgrimage town that went to war when the drug cartels arrived https://www.thetimes.com/world/latin-america/article/a-town-that-went-to-war-local-feud-fuels-mexican-cartels-fight-for-control-fzqjmq302 [Internet]. 2025 [cited 2025 Jun 13]. Available from: https://www.thetimes.com/world/latin-america/article/a-town-that-went-to-war-local-feud-fuels-mexican-cartels-fight-for-control-fzqjmq302.
- WSJ. Haiti’s Beleaguered Government Launches Drones Against Gangs - WSJ https://www.wsj.com/world/americas/haiti-drones-gangs-fight-27e8341f [Internet]. 2025 [cited 2025 Jun 13]. Available from: https://www.wsj.com/world/americas/haiti-drones-gangs-fight-27e8341f.
- ICRC. Haiti: Renewed clashes fuel humanitarian crisis | ICRC https://www.icrc.org/en/article/haiti-renewed-clashes-fuel-humanitarian-crisis-has-no-end-sight [Internet]. 2025 [cited 2025 Jun 13]. Available from: https://www.icrc.org/en/article/haiti-renewed-clashes-fuel-humanitarian-crisis-has-no-end-sight.
- PAHO/WHO. Caring for the Displaced in Haiti: Overcoming Health Challenges Amid Escalating Armed Violence - PAHO/WHO | Pan American Health Organization https://www.paho.org/en/stories/caring-displaced-haiti-overcoming-health-challenges-amid-escalating-armed-violence [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://www.paho.org/en/stories/caring-displaced-haiti-overcoming-health-challenges-amid-escalating-armed-violence.
- UN OCHA. Six things to know about the humanitarian crisis in Haiti | OCHA https://www.unocha.org/news/six-things-know-about-humanitarian-crisis-haiti [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://www.unocha.org/news/six-things-know-about-humanitarian-crisis-haiti.
- IDMC. Crime and displacement in Central America | IDMC - Internal Displacement Monitoring Centre https://www.internal-displacement.org/research-areas/crime-and-displacement-in-central-america/ [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://www.internal-displacement.org/research-areas/crime-and-displacement-in-central-america/.
- Franco S, Suarez CM, Naranjo CB, Báez LC, Rozo P. The effects of the armed conflict on the life and health in Colombia. Cien Saude Colet [Internet]. 2006 [cited 2025 Jun 13];11(2):349–61. Available from: https://www.scielo.br/j/csc/a/Hqcm7wXDMjwPjV8WhbJw3nt/?lang=en.
- IDMC. The Last Refuge: Urban Displacement in Colombia https://story.internal-displacement.org/colombia-urban/index.html [Internet]. 2020 [cited 2025 Jun 13]. Available from: https://story.internal-displacement.org/colombia-urban/index.html.
- Shultz JM, Garfin DR, Espinel Z, Araya R, Oquendo MA, Wainberg ML, et al. Internally Displaced “Victims of Armed Conflict” in Colombia: The Trajectory and Trauma Signature of Forced Migration. Curr Psychiatry Rep [Internet]. 2014 Oct 1 [cited 2025 Jun 13];16(10). Available from: https://pubmed.ncbi.nlm.nih.gov/25135775/.
- EL PAIS. Los 40.000 desplazados del Catatumbo marcan un quiebre en la larga historia del desplazamiento forzado en Colombia | EL PAÍS América Colombia https://elpais.com/america-colombia/2025-01-26/el-catatumbo-marca-un-record-en-la-larga-historia-del-desplazamiento-forzado-en-colombia.html [Internet]. 2025 [cited 2025 Jun 13]. Available from: https://elpais.com/america-colombia/2025-01-26/el-catatumbo-marca-un-record-en-la-larga-historia-del-desplazamiento-forzado-en-colombia.html.
- HRW. World Report 2021: Venezuela | Human Rights Watch https://www.hrw.org/world-report/2021/country-chapters/venezuela [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://www.hrw.org/world-report/2021/country-chapters/venezuela.
- HRW. Venezuela: Security Force Abuses at Colombia Border | Human Rights Watch https://www.hrw.org/news/2021/04/26/venezuela-security-force-abuses-colombia-border [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://www.hrw.org/news/2021/04/26/venezuela-security-force-abuses-colombia-border.
- IDMC. The impact of Covid-19 on the Venezuelan displacement crisis | IDMC - Internal Displacement Monitoring Centre https://www.internal-displacement.org/expert-analysis/the-impact-of-covid-19-on-the-venezuelan-displacement-crisis/ [Internet]. 2020 [cited 2025 Jun 13]. Available from: https://www.internal-displacement.org/expert-analysis/the-impact-of-covid-19-on-the-venezuelan-displacement-crisis/.
- Salas-Wright CP, Pérez-Gómez A, Maldonado-Molina MM, Mejia-Trujillo J, García MF, Bates MM, et al. Cultural stress and mental health among Venezuelan migrants: cross-national evidence from 2017 to 2024. Soc Psychiatry Psychiatr Epidemiol [Internet]. 2024 [cited 2025 Jun 13]; Available from: https://pubmed.ncbi.nlm.nih.gov/39579166/.
- Cruz MS, Silva ES, Jakaite Z, Krenzinger M, Valiati L, Gonçalves D, et al. Experience of neighbourhood violence and mental distress in Brazilian favelas: a cross-sectional household survey. The Lancet Regional Health - Americas [Internet]. 2021 Dec 1 [cited 2025 Jun 13];4:100067. Available from: https://www.thelancet.com/action/showFullText?pii=S2667193X21000636.
- Furumo PR, Yu J, Hogan JA, de Carvalho LTM, Brito B, Lambin EF. Land conflicts from overlapping claims in Brazil’s rural environmental registry. Proc Natl Acad Sci U S A [Internet]. 2024 Aug 13 [cited 2025 Jun 13];121(33):e2407357121. [CrossRef]
- Da Luz Scherf E, Viana da Silva MV. Brazil’s Yanomami health disaster: addressing the public health emergency requires advancing criminal accountability. Front Public Health [Internet]. 2023 [cited 2025 Jun 13];11:1166167. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10229808/.
- IDMC. Brazil - Internal Displacements Updates (IDU) (event data) | Humanitarian Dataset | HDX https://data.humdata.org/dataset/idmc-event-data-for-bra [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://data.humdata.org/dataset/idmc-event-data-for-bra.
- Randell H. Forced Migration and Changing Livelihoods in the Brazilian Amazon. Rural Sociol [Internet]. 2017 Sep 1 [cited 2025 Jun 13];82(3):548–73. Available from: https://pubmed.ncbi.nlm.nih.gov/29720771/.
- Chavez LJE, Lamy ZC, Veloso L da C, da Silva LFN, Goulart AMR, Cintra N, et al. Barriers and facilitators for the sexual and reproductive health and rights of displaced Venezuelan adolescent girls in Brazil. J Migr Health [Internet]. 2024 Jan 1 [cited 2025 Jun 13];10. Available from: https://pubmed.ncbi.nlm.nih.gov/39184240/.
- CLACS. PERU: The Shining Path and the Emergence of the Human Rights Community in Peru | Center for Latin American & Caribbean https://clacs.berkeley.edu/peru-shining-path-and-emergence-human-rights-community-peruStudies [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://clacs.berkeley.edu/peru-shining-path-and-emergence-human-rights-community-peru.
- Suarez EB. The association between post-traumatic stress-related symptoms, resilience, current stress and past exposure to violence: A cross sectional study of the survival of Quechua women in the aftermath of the Peruvian armed conflict. Confl Health [Internet]. 2013 [cited 2025 Jun 13];7(1). Available from: https://pubmed.ncbi.nlm.nih.gov/24148356/.
- IDMC. Peru | IDMC - Internal Displacement Monitoring Centre https://www.internal-displacement.org/countries/peru/ [Internet]. 2025 [cited 2025 Jun 13]. Available from: https://www.internal-displacement.org/countries/peru/.
- Colombo AL, Guimarães T, Silva LRBF, Monfardini LP de A, Cunha AKB, Rady P, et al. Prospective Observational Study of Candidemia in São Paulo, Brazil: Incidence Rate, Epidemiology, and Predictors of Mortality. Infect Control Hosp Epidemiol [Internet]. 2007 May [cited 2025 Jun 13];28(05):570–6. Available from: https://pubmed.ncbi.nlm.nih.gov/17464917/.
- CDC. Data and Statistics on Candidemia | Candidiasis | CDC https://www.cdc.gov/candidiasis/data-research/facts-stats/index.html [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://www.cdc.gov/candidiasis/data-research/facts-stats/index.html.
- Bonaldo G, Jewtuchowicz VM. Candidiasis invasiva en pacientes con Covid-19 [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://repositorio.uai.edu.ar/handle/123456789/400.
- Villanueva-Lozano H, Treviño-Rangel R de J, González GM, Ramírez-Elizondo MT, Lara-Medrano R, Aleman-Bocanegra MC, et al. Outbreak of Candida auris infection in a COVID-19 hospital in Mexico. Clinical Microbiology and Infection [Internet]. 2021 May 1 [cited 2025 Jun 14];27(5):813. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7835657/.
- Alvarez-Moreno CA, Cortes JA, Denning DW. Burden of Fungal Infections in Colombia. Journal of Fungi [Internet]. 2018 Jun 1 [cited 2025 Jun 13];4(2):41. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6023354/.
- Brasil. Ministério da Saúde. Comissão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde – CONITEC. Análise de custo-efetividade e impacto orçamentário do uso de anidulafungina como tratamento de primeira linha para candidíase invasiva no Brasil [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2025 jun 14]. p. 12–15. Disponible en: https://www.gov.br/conitec/pt-br. [cited 2025 Jun 13]; Available from: http://conitec.gov.br/.
- de Mello Vianna CM, Mosegui GBG, da Silva Rodrigues MP. Cost-effectiveness analysis and budgetary impact of anidulafungin treatment for patients with candidemia and other forms of invasive candidiasis in Brazil. Rev Inst Med Trop Sao Paulo [Internet]. 2023 [cited 2025 Jun 13];65. Available from: https://pubmed.ncbi.nlm.nih.gov/36722671/.
- Wan Ismail WNA, Jasmi N, Khan TM, Hong YH, Neoh CF. The Economic Burden of Candidemia and Invasive Candidiasis: A Systematic Review. Value Health Reg Issues [Internet]. 2020 May 1 [cited 2025 Jun 13];21:53–8. Available from: https://www.sciencedirect.com/science/article/pii/S2212109919300883.
- Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: A persistent public health problem. Clin Microbiol Rev [Internet]. 2007 Jan [cited 2025 Jun 13];20(1):133–63. Available from: https://pubmed.ncbi.nlm.nih.gov/17223626/.
- Sifuentes-Osornio J, Corzo-León DE, Ponce-De-León LA. Epidemiology of Invasive Fungal Infections in Latin America. Curr Fungal Infect Rep [Internet]. 2012 Mar [cited 2025 Jun 13];6(1):23. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3277824/.
- Márquez F, Iturrieta I, Calvo M, Urrutia M, Godoy-Martínez P, Márquez F, et al. Epidemiología y susceptibilidad antifúngica de especies causantes de candidemia en la ciudad de Valdivia, Chile. Revista chilena de infectología [Internet]. 2017 Oct 1 [cited 2025 Jun 13];34(5):441–6. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0716-10182017000500441&lng=es&nrm=iso&tlng=es.
- Groisman Sieben R, Paternina-de la Ossa R, Waack A, Casale Aragon D, Bellissimo-Rodrigues F, Israel do Prado S, et al. Risk factors and mortality of candidemia in a children’s public hospital in Sao Paulo, Brazil. Revista Argentina de Microbiología / Argentinean Journal of Microbiology [Internet]. 2024 Jul 1 [cited 2025 Jun 13];56(3):281–6. Available from: https://www.elsevier.es/es-revista-revista-argentina-microbiologia-argentinean-372-articulo-risk-factors-mortality-candidemia-in-S0325754124000397.
- Bhargava A, Klamer K, Sharma M, Ortiz D, Saravolatz L. Candida auris: A Continuing Threat. Microorganisms [Internet]. 2025 Mar 1 [cited 2025 Jun 13];13(3). Available from: https://pubmed.ncbi.nlm.nih.gov/40142543/.
- Chowdhary A, Sharma C, Meis JF. Candida auris: A rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLoS Pathog [Internet]. 2017 May 1 [cited 2025 Jun 14];13(5). Available from: https://pubmed.ncbi.nlm.nih.gov/28542486/.
- Lanna M, Lovatto J, de Almeida JN, Medeiros EA, Colombo AL, García-Effron G. Epidemiological and Microbiological aspects of Candidozyma auris (Candida auris) in Latin America: A literature review. Journal of Medical Mycology [Internet]. 2025 Jun 1 [cited 2025 Jun 13];35(2). Available from: https://pubmed.ncbi.nlm.nih.gov/40215876/.
- Ortiz-Roa C, Valderrama-Rios MC, Sierra-Umaña SF, Rodríguez JY, Muñetón-López GA, Solórzano-Ramos CA, et al. Mortality Caused by Candida auris Bloodstream Infections in Comparison with Other Candida Species, a Multicentre Retrospective Cohort. Journal of Fungi [Internet]. 2023 Jul 1 [cited 2025 May 12];9(7). Available from: https://pubmed.ncbi.nlm.nih.gov/37504704/.
- Toda M, Williams SR, Berkow EL, Farley MM, Harrison LH, Bonner L, et al. Population-Based Active Surveillance for Culture-Confirmed Candidemia — Four Sites, United States, 2012–2016. MMWR Surveillance Summaries [Internet]. 2020 [cited 2025 Jun 13];68(8):1–17. Available from: https://www.cdc.gov/mmwr/volumes/68/ss/ss6808a1.htm.
- Koehler P, Stecher M, Cornely OA, Koehler D, Vehreschild MJGT, Bohlius J, et al. Morbidity and mortality of candidaemia in Europe: an epidemiologic meta-analysis. Clinical Microbiology and Infection [Internet]. 2019 Oct 1 [cited 2025 Jun 13];25(10):1200–12. Available from: https://pubmed.ncbi.nlm.nih.gov/31039444/.
- Doi AM, Pignatari ACC, Edmond MB, Marra AR, Camargo LFA, Siqueira RA, et al. Epidemiology and microbiologic characterization of nosocomial candidemia from a Brazilian national surveillance program. PLoS One [Internet]. 2016 Jan 1 [cited 2025 Jun 13];11(1). Available from: https://pubmed.ncbi.nlm.nih.gov/26808778/.
- Barahona Correra JE, Calvo Valderrama MG, Romero Alvernia DM, Angulo Mora J, Alarcón Figueroa LF, Rodríguez Malagón MN, et al. Epidemiology of Candidemia at a University Hospital in Colombia, 2008-2014. Universitas Medica [Internet]. 2019 Dec 18 [cited 2025 Jun 13];60(1). Available from: https://revistas.javeriana.edu.co/index.php/vnimedica/article/view/24463.
- ME S, T A, F QT, AL C, J Z, IN T, et al. Erratum: Active surveillance of Candidemia in children from Latin America (Pediatric Infectious Disease Journal (2013) 33: 2 (e40-e44)). Pediatric Infectious Disease Journal [Internet]. 2014 Mar 1 [cited 2025 Jun 13];33(3):333. Available from: https://pubmed.ncbi.nlm.nih.gov/23995591/.
- da Silva CM, de Carvalho AMR, Macêdo DPC, Jucá MB, Amorim R de JM, Neves RP. Candidemia in Brazilian neonatal intensive care units: risk factors, epidemiology, and antifungal resistance. Brazilian Journal of Microbiology [Internet]. 2023 Jun 1 [cited 2025 Jun 13];54(2):817–25. Available from: https://pubmed.ncbi.nlm.nih.gov/36892755/.
- de Medeiros MAP, de Melo APV, de Oliveira Bento A, de Souza LBFC, de Assis Bezerra Neto F, Garcia JBL, et al. Epidemiology and prognostic factors of nosocomial candidemia in Northeast Brazil: A six-year retrospective study. PLoS One [Internet]. 2019 Aug 1 [cited 2025 Jun 13];14(8):e0221033. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0221033.
- Fernandez J, Erstad BL, Petty W, Nix DE. Time to positive culture and identification for Candida blood stream infections. Diagn Microbiol Infect Dis [Internet]. 2009 Aug [cited 2025 Jun 13];64(4):402–7. Available from: https://pubmed.ncbi.nlm.nih.gov/19446982/.
- Ortiz B, Varela D, Fontecha G, Torres K, Cornely OA, Salmanton-García J. Strengthening Fungal Infection Diagnosis and Treatment: An In-depth Analysis of Capabilities in Honduras. Open Forum Infect Dis [Internet]. 2024 Oct 1 [cited 2025 Jun 13];11(10). Available from: https://pubmed.ncbi.nlm.nih.gov/39421702/.
- Wu Y, Zou Y, Dai Y, Lu H, Zhang W, Chang W, et al. Adaptive morphological changes link to poor clinical outcomes by conferring echinocandin tolerance in Candida tropicalis. PLoS Pathog [Internet]. 2025 May 1 [cited 2025 Jun 13];21(5):e1013220. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12140413/.
- Khan S, Cai L, Bilal H, Khan MN, Fang W, Zhang D, et al. An 11-Year retrospective analysis of candidiasis epidemiology, risk factors, and antifungal susceptibility in a tertiary care hospital in China. Sci Rep [Internet]. 2025 Dec 1 [cited 2025 Jun 13];15(1):1–13. Available from: https://www.nature.com/articles/s41598-025-92100-x.
- Govender NP, Todd J, Nel J, Mer M, Karstaedt A, Cohen C, et al. HIV infection as risk factor for death among hospitalized persons with Candidemia, South Africa, 2012-2017. Emerg Infect Dis [Internet]. 2021 Jun 1 [cited 2025 Jun 13];27(6):1607–15. Available from: https://pubmed.ncbi.nlm.nih.gov/34014153/.
- González de Molina FJ, León C, Ruiz-Santana S, Saavedra P. Assessment of candidemia-attributable mortality in critically ill patients using propensity score matching analysis. Crit Care [Internet]. 2012 Jun 14 [cited 2025 Jun 13];16(3). Available from: https://pubmed.ncbi.nlm.nih.gov/22698004/.
- WHO. Health of refugees and migrants https://cdn.who.int/media/docs/default-source/documents/publications/health-of-refugees-migrants-paho-20181c89615b-3e93-4b59-9d25-2979e6b0cbcb.pdf?sfvrsn=2ca33a0b_1. 2021;.
- Ellis D, Marriott D, Hajjeh RA, Warnock D, Meyer W, Barton R. Epidemiology: surveillance of fungal infections. Med Mycol [Internet]. 2000 Dec 30 [cited 2025 Jun 13];38(1):173–82. Available from: https://www.researchgate.net/publication/12127348_Epidemiology_Surveillance_of_fungal_infections.
- Ortíz Ruiz G, Osorio J, Valderrama S, Álvarez D, Elías Díaz R, Calderón J, et al. Factores de riesgo asociados a candidemia en pacientes críticos no neutropénicos en Colombia. Med Intensiva [Internet]. 2016 Apr 1 [cited 2025 Jun 13];40(3):139–44. Available from: https://pubmed.ncbi.nlm.nih.gov/26725105/.
- Ministerio de Salud de Colombia. Incidencia de candidemia en migrantes desplazados en regiones fronterizas (2008–2010). Informe interno. Bogotá: Ministerio de Salud de Colombia; 2011. No publicado. Plan de Respuesta https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/COM/plan-respuesta-salud-migrantes.pdf. 2011.
- Ministério da Saúde de Brasil. Incidencia de candidemia en pacientes desplazados en zonas rurales afectadas por violencia de pandillas (2012–2015) -[informe interno] no publicado. Brasília; 2016.
- Secretaría de Salud (México). Incidencia de candidemia en migrantes en tránsito en estado fronterizo (2015–2018) [Informe interno] No publicado. Ciudad de México; 2019.
- Ministerio de Salud (Haití). Brotes de candidemia en refugiados internos en Puerto Príncipe (2020–2023) [Informe interno] No publicado. Puerto Príncipe; 2024.
- Ministério da Saúde de Brasil. Costos hospitalarios de candidemia en migrantes en hospitales públicos (2012–2015) [Informe interno] No publicado. Brasília; 2016.
- Ministerio de Salud (Colombia). Costos de tratamientos antifúngicos en candidemia de migrantes (2008–2010) [Informe interno] No publicado. Bogotá; 2011.
- OIM. Secuelas de candidemia en población desplazada: impacto en productividad (2016–2020) [informe técnico]. Ginebra: OIM; 2021. No publicado. https://publications.iom.int/system/files/pdf/IOM-AR-Abridged-2021-ES.pdf [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://publications.iom.int/system/files/pdf/IOM-AR-Abridged-2021-ES.pdf.
- ACNUR. Carga económica familiar de enfermedades fúngicas en refugiados de Centroamérica (2018–2019) [informe interno]. Ginebra: ACNUR; 2020. No publicado. https://www.acnur.org/?utm_content=HTML&gad_source=1&gad_campaignid=22375232861&gbraid=0AAAAA-tzzixwQOOs2SzPCsAjGws-8EHjg&gclid=Cj0KCQjwu7TCBhCYARIsAM_S3NgdvcxqtLZtvp8nji77TVL7RjsLTsST-Dzxs4qNNVlGeCPEt3m4RHcaAt0uEALw_wcB [Internet]. 2020 [cited 2025 Jun 13]. Available from: https://www.acnur.org/?utm_content=HTML&gad_source=1&gad_campaignid=22375232861&gbraid=0AAAAA-tzzixwQOOs2SzPCsAjGws-8EHjg&gclid=Cj0KCQjwu7TCBhCYARIsAM_S3NgdvcxqtLZtvp8nji77TVL7RjsLTsST-Dzxs4qNNVlGeCPEt3m4RHcaAt0uEALw_wcB.
- MSF. Asignación de recursos para fungemias en clínicas móviles en contextos de conflicto (2018–2022) [informe interno]. París: MSF; 2022. No publicado. https://www.msf.org.co/wp-content/uploads/2023/08/REPORTE-ANUAL-2022-MSF_CO.pdf. 2022.
- Ministério da Saúde de Brasil. Perfil de especies de Candida en pacientes desplazados atendidos en campañas móviles (2012–2015) [Informe interno] No publicado. Brasília; 2016.
- Ministerio de Salud (Colombia). Aislamientos de C. parapsilosis en clínicas móviles para migrantes (2008–2010) [Informe Interno] No publicado. Bogotá; 2011.
- Instituto de Salud de Venezuela. Resistencia a fluconazol en C. tropicalis en campamentos de desplazados (2017–2021) [Informe interno] No publicado. Caracas; 2022.
- Secretaría de Salud de México. Resistencia a fluconazol en C. glabrata en migrantes VIH positivos y diabéticos sin control (2015–2018) [Informe interno] No publicado. Ciudad de México; 2019.
- INAS (Colombia), Ministerio de Salud (Venezuela). Brotes de Candida auris en campamentos de desplazados (2017–2023) [Informe interno] No publicado. Bogotá/Caracas; 2024.
- Ministerio de Salud (Colombia). Mortalidad a 30 días de candidemia en pacientes desplazados en regiones fronterizas (2008–2010) [Informe interno] No publicado. Bogotá; 2011.
- Cortés JA, Montañez AM, Carreño-Gutiérrez AM, Reyes P, Gómez CH, Pescador A, et al. Risk factors for mortality in Colombian patients with candidemia. Journal of Fungi [Internet]. 2021 Jun 1 [cited 2025 Jun 13];7(6). Available from: https://pubmed.ncbi.nlm.nih.gov/34073125/.
- Ministerio de Salud (Colombia). Informe interno sobre candidemia en poblaciones desplazadas [Informe interno] Datos no publicados. Bogotá; 2022.
- Ministério da Saúde de Brasil. Mortalidad en migrantes con candidemia atendidos en unidad de cuidados intensivos móvil en zonas rurales afectadas por violencia de pandillas (2012–2015) [Informe interno] No publicado. Brasília; 2016.
- Secretaría de Salud de Honduras en representación de la red de salud de Centroamérica. Mortalidad de candidemia en migrantes atendidos en clínicas móviles a lo largo de rutas migratorias (2016–2019) [Informe interno] No publicado. Tegucigalpa; 2020.
- Ministerio de Salud Pública (El Salvador). Guía de Manejo de Infecciones Fúngicas en Pacientes con VIH y Diabetes [Informe interno] No publicado. San Salvador; 2021.
- OPS/OMS. Informe epidemiológico de infecciones oportunistas en Honduras. Tegucigalpa: Organización Panamericana de la Salud; 2022. https://www.paho.org/es/honduras [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://www.paho.org/es/honduras.
- Ministerio de Salud Pública y Población de Haití. Mortalidad por candidemia en refugiados internos en hospitales de campaña tras crisis humanitaria (2020–2023)[Informe interno] No publicado. Puerto Príncipe; 2024.
- Nucci M, Queiroz-Telles F, Tobón AM, Restrepo A, Colombo AL. Epidemiology of opportunistic fungal infections in latin America. Clinical Infectious Diseases [Internet]. 2010 Sep 1 [cited 2025 Jun 13];51(5):561–70. Available from: https://pubmed.ncbi.nlm.nih.gov/20658942/.
- Rodrigues ML, Nosanchuk JD. Fungal diseases as neglected pathogens: A wake-up call to public health officials. PLoS Negl Trop Dis [Internet]. 2020 Feb 1 [cited 2025 Jun 13];14(2):e0007964. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7032689/.
- Colombo AL TLGJR. The north and south of candidemia: Issues for Latin America [Internet]. 2008 [cited 2025 Jun 13]. Available from: https://www.researchgate.net/publication/51433871_The_north_and_south_of_Candidemia_Issues_for_Latin_America.
- Eggimann P, Garbino J, Pittet D. Epidemiology of Candida species infections in critically ill non-immunosuppressed patients. Lancet Infectious Diseases [Internet]. 2003 [cited 2025 Jun 13];3(11):685–702. Available from: https://pubmed.ncbi.nlm.nih.gov/14592598/.
- Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: Candidiasis (Mucocutaneous) [Internet]. Washington, DC: Department of Health and Human Services; 2025 Feb [cited 2025 Jun 14]. Available from: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection/candidiasis-mucocutaneous . 2025 [cited 2025 Jun 13]; Available from: https://clinicalinfo.hiv.gov/.
- Sobel JD. Recurrent vulvovaginal candidiasis. Am J Obstet Gynecol [Internet]. 2016 Jan 1 [cited 2025 Jun 13];214(1):15–21. Available from: https://pubmed.ncbi.nlm.nih.gov/26164695/.
- GAFFI. Country fungal disease burdens [Internet]. Geneva: GAFFI; c2023 [citado 14 jun 2025]. Disponible en: GAFFI website, sección Country Fungal Disease Burdens https://gaffi.org/media/country-fungal-disease-burdens/ [Internet]. 2025 [cited 2025 Jun 13]. Available from: https://gaffi.org/media/country-fungal-disease-burdens/.
- Lopes Colombo A, Guimarães T, Aranha Camargo LF, Richtmann R, Queiroz-Telles F de, Costa Salles MJ, et al. Brazilian guidelines for the management of candidiasis: a joint meeting report of three medical societies – Sociedade Brasileira de Infectologia, Sociedade Paulista de Infectologia, Sociedade Brasileira de Medicina Tropical. The Brazilian Journal of Infectious Diseases [Internet]. 2012 Aug 1 [cited 2025 Jun 13];16(SUPPL. 1):S1–34. Available from: https://www.bjid.org.br/en-brazilian-guidelines-for-management-candidiasis-articulo-S1413867012703367.
- Castro LÁ, Álvarez MI, Martínez E. Pseudomembranous Candidiasis in HIV/AIDS Patients in Cali, Colombia. Mycopathologia [Internet]. 2013 Feb 1 [cited 2025 Jun 13];175(1–2):91–8. Available from: https://pubmed.ncbi.nlm.nih.gov/23086383/.
- MINSA (Perú). Análisis de Situación de Salud - Peru https://bvs.minsa.gob.pe/local/MINSA/6279.pdf [Internet]. 2021 [cited 2025 Jun 14]. Available from: www.dge.gob.pe.
- Flondor AE, Sufaru IG, Martu I, Burlea SL, Flondor C, Toma V. Nutritional Deficiencies and Oral Candidiasis in Children from Northeastern Romania: A Cross-Sectional Biochemical Assessment. Nutrients 2025, Vol 17, Page 1815 [Internet]. 2025 May 27 [cited 2025 Jun 13];17(11):1815. Available from: https://www.mdpi.com/2072-6643/17/11/1815/htm.
- Wirtz AL, Guillén JR, Stevenson M, Ortiz J, Talero MÁB, Page KR, et al. HIV infection and engagement in the care continuum among migrants and refugees from Venezuela in Colombia: a cross-sectional, biobehavioural survey. Lancet HIV [Internet]. 2023 Jul 1 [cited 2025 Jun 13];10(7):e461–71. Available from: https://pubmed.ncbi.nlm.nih.gov/37302399/.
- Oñate JM, Rivas P, Pallares C, Saavedra CH, Martínez E, Coronell W, et al. Consenso Colombiano Para el Diagnóstico, Tratamiento y Prevención de la Enfermedad por Candida Spp. en Niños y Adultos. Infectio [Internet]. 2019 [cited 2025 Jun 13];23(3):271–304. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0123-93922019000300271&lng=en&nrm=iso&tlng=en.
- UNAIDS. Informe regional 2022: VIH/SIDA https://www.unaids.org/sites/default/files/media_asset/2022-global-aids-update-summary_es.pdf [Internet]. 2022 [cited 2025 Jun 14]. Available from: https://www.unaids.org/sites/default/files/media_asset/2022-global-aids-update-summary_es.pdf.
- OPS. 2023. Panorama de la diabetes en la Región de las Américas https://iris.paho.org/bitstream/handle/10665.2/57197/9789275326336_spa.pdf?sequence=1&isAllowed=y.
- OPS/OMS. Diabetes - OPS/OMS | Organización Panamericana de la Salud https://www.paho.org/es/temas/diabetes [Internet]. 2023 [cited 2025 Jun 14]. Available from: https://www.paho.org/es/temas/diabetes.
- OPS/OMS. La OPS y GARDP colaborarán para hacer frente a la resistencia a los antibióticos en América Latina y el Caribe - OPS/OMS | Organización Panamericana de la Salud https://www.paho.org/es/noticias/26-9-2024-ops-gardp-colaboraran-para-hacer-frente-resistencia-antibioticos-america-latina [Internet]. 2024 [cited 2025 Jun 14]. Available from: https://www.paho.org/es/noticias/26-9-2024-ops-gardp-colaboraran-para-hacer-frente-resistencia-antibioticos-america-latina.
- WHO. Social determinants of health in countries in conflict https://applications.emro.who.int/dsaf/dsa955.pdf. 2008;.
- Nucci M, Engelhardt M, Hamed K. Mucormycosis in South America: A review of 143 reported cases. Mycoses [Internet]. 2019 [cited 2025 Jun 13];62(9):730. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6852100/.
- OMS. Hacinamiento en los hogares - https://www.ncbi.nlm.nih.gov/books/NBK583397/#:~:text=En%20resumen%2C%20la%20revisi%C3%B3n%20sistem%C3%A1tica,y%20otras%20enfermedades%20infecciosas%20respiratorias. 2022 [cited 2025 Jun 14]; Available from: https://www.ncbi.nlm.nih.gov/books/NBK583397/.
- WHO. Salud de los refugiados y migrantes https://www.who.int/es/health-topics/refugee-and-migrant-health#tab=tab_1 [Internet]. 2025 [cited 2025 Jun 14]. Available from: https://www.who.int/es/health-topics/refugee-and-migrant-health#tab=tab_1.
- Gómez-Vasco JD, Candelo C, Victoria S, Luna L, Pacheco R, Ferro BE, et al. Vulnerabilidad social, un blanco fatal de la coinfección tuberculosis-VIH en Cali. Infectio [Internet]. 2021 [cited 2025 Jun 14];25(4):207–11. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0123-93922021000400207&lng=en&nrm=iso&tlng=es.
- PAHO/OPS. Tuberculosis en las Américas. Informe regional 2021 [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://iris.paho.org/handle/10665.2/57084.
- Hassoun N, Kassem II, Hamze M, El Tom J, Papon N, Osman M. Antifungal Use and Resistance in a Lower–Middle-Income Country: The Case of Lebanon. Antibiotics 2023, Vol 12, Page 1413 [Internet]. 2023 Sep 6 [cited 2025 Jun 14];12(9):1413. Available from: https://www.mdpi.com/2079-6382/12/9/1413/htm.
- WHO. Sistema Mundial de Vigilancia de la Resistencia a los Antimicrobianos Protocolo de implementación temprana para la inclusión de Candida spp. 2019 [cited 2025 Jun 14]; Available from: http://apps.who.int/bookorders.
- Bezares Cóbar P. ORGANIZACIÓN PANAMERICANA DE LA SALUD /ORGANIZACIÓN MUNDIAL DE LA SALUD-OPS/OMS-SISTEMATIZACIÓN DEL MODELO DE VIGILANCIA Y ATENCIÓN A LA SALUD DEL TRABAJADOR AGRÍCOLA MIGRANTE Y SU FAMILIA EN GUATEMALA.
- UNICEF. Niños desplazados y migrantes | UNICEF https://www.unicef.org/es/ninos-desplazados-migrantes-refugiados#:~:text=Trabajamos%20con%20gobiernos%2C%20con%20el,y%20est%C3%A1n%20a%20nuestro%20alcance. [Internet]. 2023 [cited 2025 Jun 14]. Available from: https://www.unicef.org/es/ninos-desplazados-migrantes-refugiados.
- Thomas-Rüddel DO, Schlattmann P, Pletz M, Kurzai O, Bloos F. Risk Factors for Invasive Candida Infection in Critically Ill Patients: A Systematic Review and Meta-analysis. Chest [Internet]. 2022 Feb 1 [cited 2025 Jun 15];161(2):345–55. Available from: https://pubmed.ncbi.nlm.nih.gov/34673022/.
- ICBF. COLOMBIA. ENSIN: Encuesta Nacional de Situación Nutricional | Portal ICBF - Instituto Colombiano de Bienestar Familiar ICBF https://www.icbf.gov.co/bienestar/nutricion/encuesta-nacional-situacion-nutricional [Internet]. 2015 [cited 2025 Jun 13]. Available from: https://www.icbf.gov.co/bienestar/nutricion/encuesta-nacional-situacion-nutricional.
- UNAIDS. Colombia HIV Epidemiological Update 2023 https://www.unaids.org/en/regionscountries/countries/colombia [Internet]. 2023 [cited 2025 Jun 13]. Available from: https://www.unaids.org/en/regionscountries/countries/colombia.
- OPS/PAHO. OPS. PAHO Tuberculosis Surveillance 2023 https://www.paho.org/es/temas/tuberculosis#:~:text=En%202023%20se%20notificaron%3A,y%20las%20muertes%20un%2044%25.&text=222.039%20personas%20con%20TB%20conoc%C3%ADan,iniciaron%20tratamiento%20para%20TB%20farmacorresistente. [Internet]. 2023 [cited 2025 Jun 13]. Available from: https://www.paho.org/es/temas/tuberculosis.
- MINSA (Colombia). Boletín Desplazamiento Interno 2022 https://www.unidadvictimas.gov.co/las-cifras-que-presenta-el-informe-global-sobre-desplazamiento/ [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://www.unidadvictimas.gov.co/las-cifras-que-presenta-el-informe-global-sobre-desplazamiento/.
- MINSA (Colombia). Registro TB 2022. https://www.ins.gov.co/buscador-eventos/Lineamientos/Pro_Tuberculosis%202022.pdf [Internet]. 2022 [cited 2025 Jun 13]. [CrossRef]
- OPS. AMÉRICA LATINA Y EL CARIBE PANORAMA REGIONAL DE LA SEGURIDAD ALIMENTARIA Y NUTRICIONAL. 2022.
- MIDIS (Perú). PERÚ: EVALUACIÓN DE SEGURIDAD ALIMENTARIA ANTE EMERGENCIAS (ESAE), 2021 https://evidencia.midis.gob.pe/wp-content/uploads/2024/09/IFE-SEGURIDAD-ALIMENTARIA-ESAE-DEPLEG-22022023-F.pdf [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://siea.midagri.gob.pe/portal/.
- OPS/OMS. Perfiles Carga Enfermedad Diabetes 2023 | OPS/OMS | Organización Panamericana de la Salud [Internet]. 2023 [cited 2025 Jun 13]. Available from: https://www.paho.org/es/tag/perfiles-carga-enfermedad-diabetes-2023.
- FAO. FOOD SECURITY AND NUTRITION IN THE WORLD THE STATE OF REPURPOSING FOOD AND AGRICULTURAL POLICIES TO MAKE HEALTHY DIETS MORE AFFORDABLE [Internet]. 2022 [cited 2025 Jun 13]. [CrossRef]
- WHO. World report on the health of refugees and migrants https://www.who.int/publications/i/item/9789240054462. 2022.
- IBGE. Pesquisa Nacional de Saúde Nutricional 2019 (Brasil). https://www.ibge.gov.br/estatisticas/sociais/saude/9160-pesquisa-nacional-de-saude.html [Internet]. 2019 [cited 2025 Jun 13]. Available from: https://www.ibge.gov.br/estatisticas/sociais/saude/9160-pesquisa-nacional-de-saude.html.
- MS Brasil. Relatório VIH/SIDA 2020. https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2020/boletim-hiv_aids-2020-internet.pdf [Internet]. 2020 [cited 2025 Jun 13]. Available from: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2020/boletim-hiv_aids-2020-internet.pdf.
- Sharkawi N. PROTECTION BRIEF BRAZIL https://www.r4v.info/sites/g/files/tmzbdl2426/files/2025-01/Protection-Brief-Brazil_Oct2024.pdf. 2024 [cited 2025 Jun 13]; Available from: https://www.acnur.org/br/sites/br/files/2024-11/informe-mercado-trabalho-formal-haitianos-brasil-jun-2024.pdf.
- PAHO/WHO. Burden of Kidney Diseases - PAHO/WHO | Pan American Health Organization https://www.paho.org/en/enlace/burden-kidney-diseases [Internet]. 2019 [cited 2025 Jun 13]. Available from: https://www.paho.org/en/enlace/burden-kidney-diseases.
- UNAIDS. Peru | UNAIDS https://www.unaids.org/en/regionscountries/countries/peru [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://www.unaids.org/en/regionscountries/countries/peru.
- Rodriguez L, Bustamante B, Huaroto L, Agurto C, Illescas R, Ramirez R, et al. A multi-centric Study of Candida bloodstream infection in Lima-Callao, Peru: Species distribution, antifungal resistance and clinical outcomes. PLoS One [Internet]. 2017 Apr 1 [cited 2025 Jun 13];12(4):e0175172. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0175172.
- CONEVAL (México). Informe Pobreza Alimentaria 2022 https://www.coneval.org.mx/InformesPublicaciones/Documents/Pobreza_Multidimensional_2022.pdf [Internet]. 2022 [cited 2025 Jun 13]. Available from: https://www.coneval.org.mx/InformesPublicaciones/Documents/Pobreza_Multidimensional_2022.pdf.
- Alberto Cortés Cáceres F, Escobar Latapí A, Nahmad Sittón S, Scott Andretta J, María Teruel Belismelis G, Ejecutiva Gonzalo Hernández Licona Secretario Ejecutivo Thania Paola de la Garza Navarrete S, et al. 2 DIAGNÓSTICO SOBRE ALIMENTACIÓN Y NUTRICIÓN Investigadores académicos María del Rosario Cárdenas Elizalde Universidad Autónoma Metropolitana. [cited 2025 Jun 13]; Available from: www.coneval.gob.mx.
- SS México. EPOC en Población Rural 2019. https://www.gob.mx/cms/uploads/attachment/file/706945/PAE_IRC_cF_.pdf [Internet]. 2019 [cited 2025 Jun 13]. Available from: https://www.gob.mx/cms/uploads/attachment/file/706945/PAE_IRC_cF_.pdf.
- UNICEF. Update on the context and situation of children https://www.unicef.org/media/152411/file/Haiti-2023-COAR.pdf. 2023.
- Vega Ocasio D, Juin S, Berendes D, Heitzinger K, Prentice-Mott G, Desormeaux AM, et al. Cholera Outbreak — Haiti, September 2022–January 2023. MMWR Morb Mortal Wkly Rep [Internet]. 2024 Jan 13 [cited 2025 Jun 13];72(2):21–5. Available from: https://www.cdc.gov/mmwr/volumes/72/wr/mm7202a1.htm.
- FAO. Regional Overview of Food Security and Nutrition 2021 https://www.fao.org/family-farming/detail/en/c/1475760/#:~:text=According%20to%20the%20Regional%20Overview,hunger%20from%202019%20to%202020. | FAO [Internet]. 2021 [cited 2025 Jun 13]. Available from: https://www.fao.org/family-farming/detail/en/c/1475760/.
- FAO. Latin America and the Caribbean Regional Overview of Food Security and Nutrition 2024 https://www.fao.org/americas/publicaciones/panorama/en [Internet]. FAO; IFAD; PAHO; UNICEF; WFP; 2025 [cited 2025 Jun 13]. Available from: https://www.fao.org/americas/publicaciones/panorama/en.
- Ministerio de Salud (Colombia). Situación de candidiasis en campamentos de refugiados venezolanos (2018–2019) [Informe interno] No publicado. Bogotá; 2020.
- Secretaría de Salud (México). Estudio de erupciones interdigitales en migrantes centroamericanos en tránsito (2019–2020) [Informe interno] No publicado. Tuxtla Gutiérrez; 2021.
- UNICEF. Niñez en MOVIMIENTO Revisión de evidencia https://www.unicef.org/lac/media/40946/file/Ninez-en-movimiento-en-ALC%20.pdf [Internet]. [cited 2025 Jun 13]. Available from: www.unicef.org/lac.
- Ministerio de Salud (Bolivia). Condiciones sanitarias y candidiasis en comunidades rurales de retornados (2018–2019) [Informe interno] No publicado. La Paz; 2020.
- Ministerio de Salud (Colombia). Malnutrición y candidiasis en desplazados de Arauca (2018–2019) [Informe interno] No publicado. Bogotá; 2020.
- Delegada para la Infancia D, Juventud la Vejez Bogotá C la D. REPORTE DESNUTRICIÓN EN NIÑOS Y NIÑAS MENORES DE 5 AÑOS DE EDAD EN COLOMBIA https://www.defensoria.gov.co/documents/20123/1657207/REPORTE+DESNUTRICI%C3%93N+EN+NI%C3%91OS+Y+NI%C3%91AS+MENORES+DE+5+A%C3%91OS+DE+EDAD+EN+COLOMBIA.pdf/c16abb21-9e11-44d4-16e1-58ed50053ee3?t=1675107656750 [Internet]. 2023 [cited 2025 Jun 13]. Available from: https://www.ins.gov.co/buscador-eventos/Paginas/Info-Evento.aspx.
- Ministerio de Salud (Colombia). Prevalencia de VIH y candidiasis en migrantes venezolanos (2018–2019) [Informe interno] No publicado. Bogotá; 2020.
- Ministerio de Salud Pública y Población (Haití). Informe sobre salud en campamentos pos-terremoto (2010–2011) [Informe interno] No publicado. Puerto Príncipe; 2012.
- Ministerio de Salud (Perú). Diabetes y candidiasis en comunidades indígenas desplazadas (2018) [Informe interno] No publicado. Lima; 2019.
- INS (Colombia). Coinfección TB/VIH y candidemia en desplazados fronterizos (2017–2018) [Informe interno] No publicado. Bogotá; 2019.
- Ministerio de Salud (Guatemala). TB extrapulmonar y candidiasis intraabdominal en desplazados (2018) [Informe interno] No publicado. Ciudad de Guatemala; 2019.
- Secretaría de Salud (México). Uso de antibióticos y candidiasis en migrantes nicaragüenses (2019–2020) [Informe interno] No publicado. Ciudad de México; 2021.
- Instituto Nacional de Salud Pública (México). Candidemia asociada a catéteres en migrantes en Tapachula (2020) [Informe interno] No publicado. Cuernavaca; 2021.
- Ministerio de Salud (Nicaragua). Salud reproductiva y candidiasis en mujeres migrantes (2019) [Informe interno] No publicado. Managua; 2020.
- Ministerio de Salud (Paraguay). Candidiasis cutánea en comunidades indígenas guaraní desplazadas (2018) [Informe interno] No publicado. Asunción; 2019.
- Ministerio de Salud (República Dominicana). Candidiasis oral en migrantes haitianos con VIH (2019–2020) [Informe interno] No publicado. Santo Domingo; 2021.
- Ministerio de salud (Guatemala). Exposición a Candida parapsilosis en migrantes agrícolas de Guatemala (2019) [Informe interno] No publicado. Washington, DC; 2019.
- Ministerio de Salud (Perú). Candidiasis interdigital en trabajadores agrícolas expuestos a plaguicidas (2019) [Informe interno] No publicado. Lima; 2020.
- Secretaría de Salud (Honduras). Impacto del clima en candidiasis de migrantes en rutas costeras (2019) [Informe interno] No publicado. Tegucigalpa; 2020.
- GAFFI. Global Fungal Infection Forum 4 in Lima - Gaffi https://gaffi.org/global-fungal-infection-forum-4-in-lima/ [Internet]. 2019 [cited 2025 Jun 13]. Available from: https://gaffi.org/global-fungal-infection-forum-4-in-lima/.
- GAFFI. GAFFI ‘s Annual report outlines its new strategy – access to diagnostics and antifungals, the centerpiece of its efforts - Gaffi https://gaffi.org/gaffi-s-annual-report-outlines-its-new-strategy-access-to-diagnostics-and-antifungals-the-centerpiece-of-its-efforts/ [Internet]. 2025 [cited 2025 Jun 14]. Available from: https://gaffi.org/gaffi-s-annual-report-outlines-its-new-strategy-access-to-diagnostics-and-antifungals-the-centerpiece-of-its-efforts/.
- Koc Ö, Kessler HH, Hoenigl M, Wagener J, Suerbaum S, Schubert S, et al. Performance of Multiplex PCR and β-1,3-D-Glucan Testing for the Diagnosis of Candidemia. Journal of Fungi [Internet]. 2022 Sep 1 [cited 2025 Jun 14];8(9). Available from: https://pubmed.ncbi.nlm.nih.gov/36135696/.
- OPS/OMS. 2016. [cited 2025 Jun 13]. Marco de Implementación de un Servicio de Telemedicina https://iris.paho.org/bitstream/handle/10665.2/28413/9789275319031_spa.pdf. Available from: https://iris.paho.org/bitstream/handle/10665.2/28413/9789275319031_spa.pdf.
- Donato L, González T, Canales M, Legarraga P, García P, Rabagliati R, et al. Evaluación del rendimiento de 1,3-β-d-glucano como apoyo diagnóstico de infecciones invasoras por Candida spp. en pacientes críticos adultos. Revista chilena de infectología [Internet]. 2017 [cited 2025 Jun 13];34(4):340–6. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0716-10182017000400340&lng=es&nrm=iso&tlng=es.
- Pemán J, Ruiz-Gaitán A. Diagnosing invasive fungal infections in the laboratory today: It’s all good news? Rev Iberoam Micol [Internet]. 2025 [cited 2025 Jun 13]; Available from: https://pubmed.ncbi.nlm.nih.gov/40268631/.
- Cornely OA, Sprute R, Grothe JH, Koehler P, Meis JF, Reinhold I, et al. Global guideline for the diagnosis and management of candidiasis: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis [Internet]. 2025 May 1 [cited 2025 Jun 13];25(5):e280–93. Available from: https://www.thelancet.com/action/showFullText?pii=S1473309924007497.
- Hernández-Pabón JC, Tabares B, Gil Ó, Lugo-Sánchez C, Santana A, Barón A, et al. Candida Non-albicans and Non-auris Causing Invasive Candidiasis in a Fourth-Level Hospital in Colombia: Epidemiology, Antifungal Susceptibility, and Genetic Diversity. Journal of Fungi [Internet]. 2024 May 1 [cited 2025 Jun 13];10(5):326. Available from: https://www.mdpi.com/2309-608X/10/5/326/htm.
- Akpan A, Morgan R. Oral candidiasis. Postgrad Med J [Internet]. 2002 Aug 1 [cited 2025 Jun 13];78(922):455–9. [CrossRef]
- Belmokhtar Z, Djaroud S, Matmour D, Merad Y. Atypical and Unpredictable Superficial Mycosis Presentations: A Narrative Review. Journal of Fungi [Internet]. 2024 Apr 1 [cited 2025 Jun 13];10(4). Available from: https://pubmed.ncbi.nlm.nih.gov/38667966/.
- Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases [Internet]. 2015 Nov 4 [cited 2025 Jun 13];62(4):e1–50. Available from: https://pubmed.ncbi.nlm.nih.gov/26679628/.
- Kullberg BJ, Arendrup MC. Invasive Candidiasis. Campion EW, editor. New England Journal of Medicine [Internet]. 2015 Oct 8 [cited 2025 Jun 13];373(15):1445–56. Available from: https://www.nejm.org/doi/full/10.1056/NEJMra1315399.
- PAHO. 2024. 2024 [cited 2025 Jun 14]. GAFFI and PAHO Join Forces to Combat Fungal Disease in Latin America and the Caribbean - PAHO/WHO | Pan American Health Organization https://www.paho.org/en/news/14-5-2024-gaffi-and-paho-join-forces-combat-fungal-disease-latin-america-and-caribbean. Available from: https://www.paho.org/en/news/14-5-2024-gaffi-and-paho-join-forces-combat-fungal-disease-latin-america-and-caribbean.
- Tobar A. E, Silva O. F, Olivares C. R, Gaete G. P, Luppi N. M. Candidiasis invasoras en el paciente crítico adulto. Revista chilena de infectología [Internet]. 2011 [cited 2025 Jun 13];28(1):41–9. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0716-10182011000100008&lng=es&nrm=iso&tlng=es.
- OMS. La OMS publica sus primeros informes sobre pruebas y tratamientos relacionados con las micosis https://www.who.int/es/news/item/01-04-2025-who-issues-its-first-ever-reports-on-tests-and-treatments-for-fungal-infections [Internet]. [cited 2025 Jun 14]. Available from: https://www.who.int/es/news/item/01-04-2025-who-issues-its-first-ever-reports-on-tests-and-treatments-for-fungal-infections.
- OPS/OMS. [La OPS responde a la crisis humanitaria grado 3 de Haití] - OPS/OMS | Organización Panamericana de la Salud https://www.paho.org/es/crisis-humanitaria-haiti-grado-3 [Internet]. 2025 [cited 2025 Jun 14]. Available from: https://www.paho.org/es/crisis-humanitaria-haiti-grado-3.
- OPS/OMS. El Libro Rojo - Documento de orientación para los equipos médicos que responden a emergencias de salud en conflictos armados y otros entornos inseguros - OPS/OMS | Organización Panamericana de la Salud [Internet]. 2025 [cited 2025 Jun 14]. Available from: https://www.paho.org/es/documentos/libro-rojo-documento-orientacion-para-equipos-medicos-que-responden-emergencias-salud.
- OPS. SALUD Y MIGRACION EN LA REGION DE LAS AMERICAS Al 31 de Marzo de 2024 https://www.paho.org/sites/default/files/2024-04/sitrep-migracion-mar-2024-es.pdf [Internet]. 2024 [cited 2025 Jun 14]. Available from: https://www.paho.org/sites/default/files/2024-04/sitrep-migracion-mar-2024-es.pdf.
- GAFFI. Antifungal drug maps - Gaffi [Internet]. 2025 [cited 2025 Jun 14]. Available from: https://gaffi.org/antifungal-drug-maps/.
- Riera F, Cortes Luna J, Rabagliatti R, Scapellato P, Caeiro JP, Chaves Magri MM, et al. Antifungal stewardship: The Latin American experience. Antimicrobial Stewardship and Healthcare Epidemiology [Internet]. 2023 Dec 5 [cited 2025 Jun 14];3(1). Available from: https://pubmed.ncbi.nlm.nih.gov/38156226/.
- PAHO. 2023. 2023 [cited 2025 Jun 14]. Migración y Salud en las Américas - OPS/OMS | Organización Panamericana de la Salud https://www.paho.org/es/migracion-salud-americas. Available from: https://www.paho.org/es/migracion-salud-americas.
- USAID/OIM. SISTEMATIZACIÓN DE BUENAS PRÁCTICAS Y LECCIONES APRENDIDAS EN LA GESTIÓN DE CENTROS DE RECEPCIÓN DE PERSONAS MIGRANTES RETORNADAS https://lac.iom.int/sites/g/files/tmzbdl2601/files/documents/2024-10/sistematizacion-en-centros-de-recepcion_esp.pdf [Internet]. 2024 [cited 2025 Jun 14]. Available from: https://infounitnca.iom.int/.
- OPS/OMS. Ministerio de Salud Pública con apoyo de OPS/OMS lanza las primeras redes de telemedicina en tiempo real de Guatemala - OPS/OMS | Organización Panamericana de la Salud https://www.paho.org/es/noticias/10-12-2020-ministerio-salud-publica-con-apoyo-opsoms-lanza-primeras-redes-telemedicina [Internet]. 2020 [cited 2025 Jun 14]. Available from: https://www.paho.org/es/noticias/10-12-2020-ministerio-salud-publica-con-apoyo-opsoms-lanza-primeras-redes-telemedicina.
- Duque-Restrepo CM, Muñoz-Monsalve LV, Guerra-Bustamante D, Cardona-Maya WD, Gómez-Velásquez JC, Duque-Restrepo CM, et al. Blanco de calcoflúor: en búsqueda de un mejor diagnóstico. Revista Médica de Risaralda [Internet]. 2023 Mar 1 [cited 2025 Jun 14];29(2):39–48. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0122-06672023000200039&lng=en&nrm=iso&tlng=es.
- Gupta M, Chandra A, Prakash P, Banerjee T, Maurya OPS, Tilak R. Fungal keratitis in north India; Spectrum and diagnosis by Calcofluor white stain. Indian J Med Microbiol [Internet]. 2015 Jul 1 [cited 2025 Jun 14];33(3):462–3. Available from: https://pubmed.ncbi.nlm.nih.gov/26068366/.
- GAFFI. Report on activities for 2020 https://gaffidocuments.s3.eu-west-2.amazonaws.com/GAFFI+Annual+report+2020+final+2.pdf. 2021;.
- BRECHA CERO. 2020. [cited 2025 Jun 14]. Haití desarrolla plataforma de telemedicina - Brecha Cero https://brechacero.com/haiti-desarrolla-plataforma-de-telemedicina/. Available from: https://brechacero.com/haiti-desarrolla-plataforma-de-telemedicina/.
- Yarak S, Evandro I, Seron E, Ii R, Torres Pisa I. A Teledermatologia na Prática Médica. Rev Bras Educ Med [Internet]. 2017 Jun [cited 2025 Jun 14];41(2):346–55. Available from: https://www.scielo.br/j/rbem/a/h93wcmF8rqfw76YbdrrZhFQ/.
- Guadalupe González-Villalobos C, Alejandro Santana-Chávez L. PRÁCTICA CLÍNICO-QUIRÚRGICA Experiencia en el programa Telederma de una unidad de medicina familiar. Rev Med Inst Mex Seguro Soc. 2011;49(4):407–11.
- OPS/OMS. Guía de intervención humanitaria mhGAP - OPS/OMS https://www.paho.org/es/noticias/7-7-2016-guia-intervencion-humanitaria-mhgap| Organización Panamericana de la Salud [Internet]. 2016 [cited 2025 Jun 14]. Available from: https://www.paho.org/es/noticias/7-7-2016-guia-intervencion-humanitaria-mhgap.
- GAFFI. Antifungal echinocandins added to the WHO’s Essential Medicines List - Gaffi [Internet]. 2021 [cited 2025 Jun 14]. Available from: https://gaffi.org/antifungal-echinocandins-added-to-the-whos-essential-medicines-list/.
- WHO. WHO Model List of Essential Medicines - 23rd list, 2023 https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.02 [Internet]. 2023 [cited 2025 Jun 14]. Available from: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.02.
- Ndyetukira JF, Kwizera R, Ahimbisibwe C, Namujju C, Meya DB. Using single-dose liposomal amphotericin B for cryptococcal meningitis induction therapy: nurse pearls and practical perspectives. Wellcome Open Res [Internet]. 2024 May 15 [cited 2025 Jun 14];9:253. Available from: https://pubmed.ncbi.nlm.nih.gov/39386968/.
- Clancy CJ, Nguyen MH. Emergence of candida auris: An international call to arms. Clinical Infectious Diseases [Internet]. 2017 Jan 15 [cited 2025 Jun 14];64(2):141–3. Available from: https://pubmed.ncbi.nlm.nih.gov/27989986/.
- GAFFI. Mapas de fármacos antimicóticos - Gaffi [Internet]. [cited 2025 Jun 14]. Available from: https://gaffi.org/antifungal-drug-maps/.
- Spruijtenburg B, Baqueiro CCSZ, Colombo AL, Meijer EFJ, de Almeida JN, Berrio I, et al. Short Tandem Repeat Genotyping and Antifungal Susceptibility Testing of Latin American Candida tropicalis Isolates. Journal of Fungi [Internet]. 2023 Feb 1 [cited 2025 Jun 14];9(2). Available from: https://pubmed.ncbi.nlm.nih.gov/36836321/.
- Chen PY, Chuang YC, Wu UI, Sun HY, Wang JT, Sheng WH, et al. Mechanisms of azole resistance and trailing in candida tropicalis bloodstream isolates. Journal of Fungi [Internet]. 2021 Aug 1 [cited 2025 Jun 14];7(8). Available from: https://pubmed.ncbi.nlm.nih.gov/34436151/.
- Bonilla Oviedo D. Candida en la mira: Vigilancia de aislamientos resistentes en Colombia (julio – noviembre 2024) https://repositorio.uniandes.edu.co/entities/publication/7dcb6f4f-ad7b-463b-bb0b-f3198ad1e7cf [Internet]. [cited 2025 Jun 14]. Available from: https://repositorio.uniandes.edu.co/entities/publication/7dcb6f4f-ad7b-463b-bb0b-f3198ad1e7cf.
- Ministério da Saúde de Brasil. Acceso y costos de antifúngicos en hospitales terciarios (2021) [Informe interno] No publicado. Brasília; 2021.
- Rosenthal VD, Bat-Erdene I, Gupta D, Belkebir S, Rajhans P, Zand F, et al. International Nosocomial Infection Control Consortium (INICC) report, data summary of 45 countries for 2012-2017: Device-associated module. Am J Infect Control [Internet]. 2020 Apr 1 [cited 2025 Jun 14];48(4):423–32. Available from: https://pubmed.ncbi.nlm.nih.gov/31676155/.
- Frías-De-león MG, Hernández-Castro R, Conde-Cuevas E, García-Coronel IH, Vázquez-Aceituno VA, Soriano-Ursúa MA, et al. Candida glabrata Antifungal Resistance and Virulence Factors, a Perfect Pathogenic Combination. Pharmaceutics [Internet]. 2021 Oct 1 [cited 2025 Jun 14];13(10):1529. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8538829/.
- Ministerio de Salud (Colombia). Informe de brotes de Candida auris en campamentos de desplazados (2022) [Informe interno] No publicado. Bogotá; 2022.
- PAHO. Epidemiological Updates / Actualizaciones Epidemiológicas;October, 2016 https://iris.paho.org/handle/10665.2/50649. PAHO; 2016 [cited 2025 Jun 14]. Epidemiological Alert, Candida auris outbreaks in health care services (3 October 2016). Available from: https://iris.paho.org/handle/10665.2/50649.
- Ministerio de Salud (Colombia). Acceso a antifúngicos en poblaciones desplazadas y migrantes (2021) [Informe interno] No publicado. Bogotá; 2021.
- Ministério da Saúde de Brasil. Disponibilidad de antifúngicos en campamentos y clínicas móviles (2019) [Informe interno] No publicado. Brasília; 2019.
- Huang YC, Lin T-Y, Leu HS, Peng HL, Wu J-H, Chang HY. Outbreak of Candida parapsilosis fungemia in neonatal intensive care units: Clinical implications and genotyping analysis. Infection. 1999;27(2):97–102.
- Pinhati HMS, Casulari LA, Souza ACR, Siqueira RA, Damasceno CMG, Colombo AL. Outbreak of candidemia caused by fluconazole resistant Candida parapsilosis strains in an intensive care unit. BMC Infect Dis [Internet]. 2016 Aug 20 [cited 2025 Jun 14];16(1). Available from: https://pubmed.ncbi.nlm.nih.gov/27544427/.
- Berkow EL, Lockhart SR. Fluconazole resistance in Candida species: a current perspective. Infect Drug Resist [Internet]. 2017 Jul 31 [cited 2025 Jun 14];10:237. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5546770/.
- Thomaz DY, Del Negro GMB, Ribeiro LB, da Silva M, Carvalho GOMH, Camargo CH, et al. A Brazilian Inter-Hospital Candidemia Outbreak Caused by Fluconazole-Resistant Candida parapsilosis in the COVID-19 Era. Journal of Fungi [Internet]. 2022 Feb 1 [cited 2025 Jun 14];8(2). Available from: https://pubmed.ncbi.nlm.nih.gov/35205855/.
- Ministerio de Salud (Colombia). Barreras y desafíos en el acceso a tratamientos antimicóticos en zonas rurales y fronterizas [Informe interno] No publicado. Bogotá; 2020.
- Ministerio de Salud (México). Acceso a Consultas y Diagnósticos Especializados para Candidiasis en Poblaciones Vulnerables [Informe interno] No publicado. Ciudad de México; 2019.
- Ministerio de Salud (El Salvador). Mortalidad por Candidemia en Población Desplazada y General en Hospitales Públicos [Informe interno] No publicado. San Salvador; 2021.
- Ministerio de salud (El Salvador). Morbimortalidad de Candidiasis Mucocutánea en Pacientes con VIH y Diabetes en Contexto de Desplazamiento [Informe interno] No publicado. San Salvador; 2021.
- Harding E, Beckworth C, Fesselet JF, Lenglet A, Lako R, Valadez JJ. Using lot quality assurance sampling to assess access to water, sanitation and hygiene services in a refugee camp setting in South Sudan: A feasibility study. BMC Public Health [Internet]. 2017 Aug 8 [cited 2025 Jun 14];17(1):1–11. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-017-4656-2.
- MSF. Informe de Actividades de MSF México – Centroamérica 2022 - Médicos Sin Fronteras en México y Centroamérica https://www.msf.mx/document/informe-de-actividades-de-msf-mexico-centroamerica-2022/ [Internet]. 2022 [cited 2025 Jun 14]. Available from: https://www.msf.mx/document/informe-de-actividades-de-msf-mexico-centroamerica-2022/.
- Fouad FM, Sparrow A, Tarakji A, Alameddine M, El-Jardali F, Coutts AP, et al. Health workers and the weaponisation of health care in Syria: a preliminary inquiry for The Lancet–American University of Beirut Commission on Syria. The Lancet [Internet]. 2017 Dec 2 [cited 2025 Jun 14];390(10111):2516–26. Available from: https://www.thelancet.com/action/showFullText?pii=S0140673617307419.
- WHO. Rapid Grey Literature Evidence Review to Support the Guideline on Emergency Risk Communication https://www.who.int/publications/m/item/rapid-grey-literature [Internet]. 2017 [cited 2025 Jun 14]. Available from: https://www.who.int/publications/m/item/rapid-grey-literature.
- HRW. Informe Mundial 2022: Colombia | Human Rights Watch https://www.hrw.org/es/world-report/2022/country-chapters/colombia [Internet]. 2022 [cited 2025 Jun 14]. Available from: https://www.hrw.org/es/world-report/2022/country-chapters/colombia.
- Ministerio de Salud (Colombia). Desplazamiento forzado del personal sanitario en contextos de violencia [Informe interno] No publicado. Bogotá; 2021.
- Moreno Páez LF, Cortes Mendoza L. Estudio de utilización de antibióticos en una IPS de atención médica domiciliaria de la ciudad de Bogotá, durante la prestación de servicio médico a pacientes mayores de 18 años desde marzo de 2020 [Internet]. 2022 [cited 2025 Jun 14]. Available from: https://repository.udca.edu.co/server/api/core/bitstreams/95e506d0-a0d2-46d6-b2d7-53548928c620/content.
- HRW. 2025. [cited 2025 Jun 14]. México | Country Page | World | Human Rights Watch. Available from: https://www.hrw.org/es/americas/mexico.
- Secretaría de Salud (México). Informe sobre interrupción de cadenas de suministro de medicamentos en zonas de violencia [Informe interno] No publicado. Ciudad de México; 2021.
- Akinosoglou K, Livieratos A, Asimos K, Donders F, Donders GGG. Fluconazole-Resistant Vulvovaginal Candidosis: An Update on Current Management. Pharmaceutics [Internet]. 2024 Dec 1 [cited 2025 Jun 14];16(12):1555. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11678211/.
- Haïti | OPS/OMS | Organisation panaméricaine de la santé [Internet]. [cited 2025 Jun 14]. Available from: https://www.paho.org/fr/haiti.
- OIM. El Salvador Crisis Response Plan 2023 - 2025 | Global Crisis Response Platform https://crisisresponse.iom.int/response/el-salvador-crisis-response-plan-2023-2025 [Internet]. [cited 2025 Jun 14]. Available from: https://crisisresponse.iom.int/response/el-salvador-crisis-response-plan-2023-2025.
- UNHCR. Situación de El Salvador, Guatemala y Honduras | Enfoque https://reporting.unhcr.org/operational/situations/el-salvador-guatemala-and-honduras-situationglobal [Internet]. 2024 [cited 2025 Jun 13]. Available from: https://reporting.unhcr.org/operational/situations/el-salvador-guatemala-and-honduras-situation.
- UNICEF. UNICEF El Salvador https://www.unicef.org/elsalvador/ [Internet]. [cited 2025 Jun 14]. Available from: https://www.unicef.org/elsalvador/.
- Alberto S, Rodríguez M, Noemy I, Medrano M, Carolina B, Tobías M. "PREVALENCIA DE INFECCIONES VAGINALES EN MUJERES. 2024.
- Kim SH, Mun SJ, Kang JS, Moon C, Kim HT, Lee HY. Multifaceted Evaluation of Antibiotic Therapy as a Factor Associated with Candidemia in Non-Neutropenic Patients. Journal of Fungi [Internet]. 2023 Feb 1 [cited 2025 Jun 14];9(2). Available from: https://pubmed.ncbi.nlm.nih.gov/36836385/.
- Unidad para las Víctimas de Colombia. Registro Nacional de Desplazados Internos, 2023. Bogotá: UV; 2023. https://www.unidadvictimas.gov.co/las-cifras-que-presenta-informe-global-sobre-desplazamiento-2024/#:~:text=El%20Gobierno%20colombiano%2C%20a%20trav%C3%A9s,vulnerabilidad%20asociadas%20a%20su%20desplazamiento. [Internet]. 2023 [cited 2025 Jun 14]. Available from: https://www.unidadvictimas.gov.co/las-cifras-que-presenta-informe-global-sobre-desplazamiento-2024/.
- Ombelet S, Barbé B, Affolabi D, Ronat JB, Lompo P, Lunguya O, et al. Best Practices of Blood Cultures in Low- and Middle-Income Countries. Front Med (Lausanne) [Internet]. 2019 Jun 18 [cited 2025 Jun 14];6. Available from: https://pubmed.ncbi.nlm.nih.gov/31275940/.
- MINSA (Colombia). Seguimiento a la situación de salud de la población migrante procedente de Venezuela, para el período comprendido entre el 1 de marzo de 2017 y el 31 de diciembre de 2022. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/ED/GCFI/informe-circular-029-dic-2022.pdf. 2022.
- Ministério da Saúde de Brasil. Violencia urbana y desabastecimiento en regiones amazónicas: impacto en infecciones fúngicas [Informe interno] No publicado. Brasília; 2022.
- Anvisa (Brasil). Resistência aos antimicrobianos é coisa séria! — Agência Nacional de Vigilância Sanitária - Anvisa https://www.gov.br/anvisa/pt-br/assuntos/noticias-anvisa/2024/resistencia-aos-antimicrobianos-e-coisa-seria [Internet]. 2024 [cited 2025 Jun 14]. Available from: https://www.gov.br/anvisa/pt-br/assuntos/noticias-anvisa/2024/resistencia-aos-antimicrobianos-e-coisa-seria.
- OPS. Informe anual OPS - https://www.paho.org/sites/default/files/2023-11/informe-anual-2022-slv.pdf. 2022. 2022;.
- Seguro Integral de Salud (SIS) (Perú). Cobertura de antifúngicos: fluconazol, equinocandinas y anfotericina B liposomal [Informe interno] No publicado. Lima; 2023.
- Villaseca R, Ovalle A, Amaya F, Labra B, Escalona N, Lizana P, et al. Infecciones vaginales en un Centro de Salud Familiar de la Región Metropolitana, Chile. Revista chilena de infectología [Internet]. 2015 [cited 2025 Jun 14];32(1):30–6. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0716-10182015000200005&lng=es&nrm=iso&tlng=es.
- Martinez Rosado LL, Cardona-Arias JA, Martinez Rosado LL, Cardona-Arias JA. Infecciones fúngicas en un hospital público de referencia para la atención de personas con VIH/ SIDA, Medellín 2013-2017. Medicas UIS [Internet]. 2020 Aug 31 [cited 2025 Jun 14];33(2):17–24. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0121-03192020000200002&lng=en&nrm=iso&tlng=es.
- OPS/OMS. Sistemas de Laboratorio - OPS/OMS | Organización Panamericana de la Salud https://www.paho.org/es/temas/sistemas-laboratorio [Internet]. [cited 2025 Jun 14]. Available from: https://www.paho.org/es/temas/sistemas-laboratorio.
- Pineda-Murillo J, Cortés-Figueroa A ángel, Uribarren-Berrueta T del NJ, Castañón-Olivares LR. Candidosis vaginal: Revisión de la literatura y situación de México y otros países latinoamericanos. Revista Médica de Risaralda [Internet]. 2017 [cited 2025 Jun 14];23(1):38–44. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0122-06672017000100009&lng=en&nrm=iso&tlng=es.
- Lynch T, Peirano G, Lloyd T, Read R, Carter J, Chu A, et al. Molecular Diagnosis of Vaginitis: Comparing Quantitative PCR and Microbiome Profiling Approaches to Current Microscopy Scoring. J Clin Microbiol [Internet]. 2019 [cited 2025 Jun 14];57(9):e00300-19. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6711928/.
- CVSP/OPS. Identificación y sensibilidad a los antifúngicos en levaduras del género Candida - 2021 | Campus Virtual de Salud Pública (CVSP/OPS) https://campus.paho.org/es/curso/Candida-Metodos-Identificacion-Sensibilidad [Internet]. 2021 [cited 2025 Jun 14]. Available from: https://campus.paho.org/es/curso/Candida-Metodos-Identificacion-Sensibilidad.
- Boonsilp S, Homkaew A, Phumisantiphong U, Nutalai D, Wongsuk T. Species distribution, antifungal susceptibility, and molecular epidemiology of candida species causing Candidemia in a tertiary care hospital in Bangkok, Thailand. Journal of Fungi [Internet]. 2021 [cited 2025 Jun 14];7(7):577. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8303137/.
- INAS (Colombia). Instituto Nacional de Salud | Colombia searchDTC [Internet]. 2019 [cited 2025 Jun 14]. Available from: https://www.ins.gov.co/Paginas/search.aspx?k=KOH#k=KOH#s=21.
- OMS. La OMS publica su primera lista de hongos que constituyen una amenaza para la salud https://www.who.int/es/news/item/25-10-2022-who-releases-first-ever-list-of-health-threatening-fungi [Internet]. 2025 [cited 2025 Jun 14]. Available from: https://www.who.int/es/news/item/25-10-2022-who-releases-first-ever-list-of-health-threatening-fungi.
- Donders G, Sziller IO, Paavonen J, Hay P, de Seta F, Bohbot JM, et al. Management of recurrent vulvovaginal candidosis: Narrative review of the literature and European expert panel opinion. Front Cell Infect Microbiol [Internet]. 2022 Sep 9 [cited 2025 Jun 14];12:934353. Available from: http://within3.com.
Figure 1.
Burden of Invasive Candidiasis and Migration in Latin America.
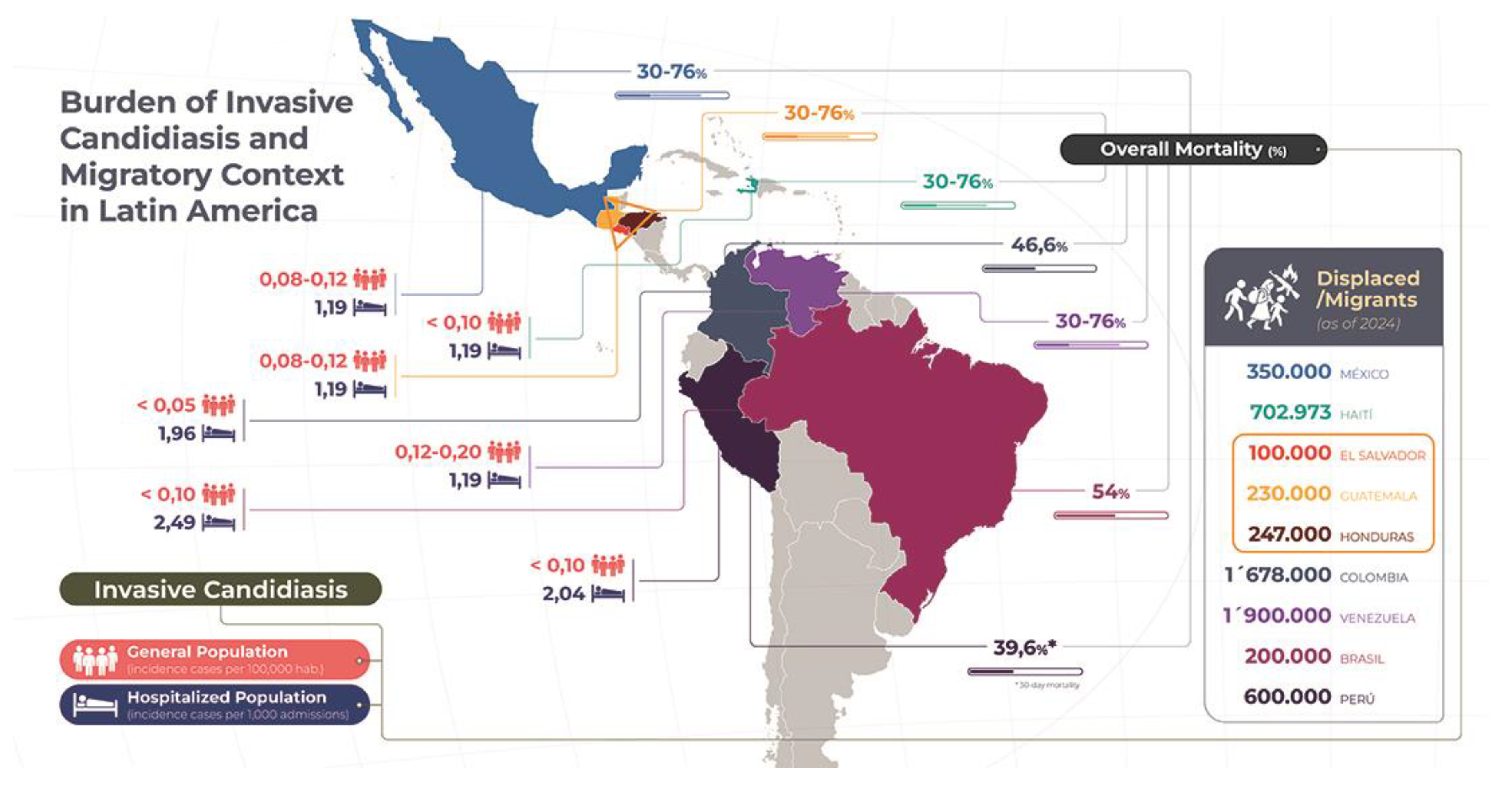

| Country | Type of conflict / violence | Key period | Internally displaced persons / Migrants-refugees (estimates) | Key findings |
|---|---|---|---|---|
| Mexico | Drug trafficking and violence by criminal groups | 2006–2020 | – / 127,796¹ |
|
| Haiti | Political instability, gang violence, and natural disasters | 2004–2020 | 702,973 / 350,000² |
|
| El Salvador | Gang violence (MS-13, Barrio 18) | 2000–2020 | 513,000 / 234,000³ |
|
| Guatemala | Civil war (1960–1996) and post-conflict violence | 1960–1996 / 2000–2020 |
|
|
| Honduras | Gang violence and organized crime | 2000–2020 |
|
|
| Colombia | Internal armed conflict (FARC, paramilitaries) | 2000–2020 | 6,900,000 / 3,000,000 + 2,900,000⁴ |
|
| Venezuela | Sociopolitical crisis and high levels of street violence | 2014–2020 | – / 7,770,000⁵ |
|
| Brazil | Urban violence and organized crime (favelas, militias) | 2000–2020 | – / 790,000⁶ |
|
| Peru | Internal conflict (Sendero Luminoso (Shining Path) and State response) | 1980–2000 | – / Not available |
|
FARC: Revolutionary Armed Forces of Colombia, UNHCR: United Nations High Commissioner for Refugees. ¹ No official figures available for internally displaced persons for 2023–2024 (National Victims Commission, UNHCR). ² Record number of internally displaced persons due to criminal violence in mid-2024. ³ No official figures for 2024; recent increase documented by regional analysts in Guatemala and Honduras. ⁴ Displacements reported since the signing of the peace agreement (November 2016) until June 2024. ⁵ Latest UNHCR estimate; unpublished internal displacement data for 2023–2024. ⁶ Localized displacement; no recent UNHCR report for 2024.
Table 2.
Health Conditions and IC Risk: General vs. Migrant / Displaced Population [1,50,114,127,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155].
| Country | Main risk factors for IC |
Common conditions and fungal risk General Population |
Common conditions and fungal risk Displaced/Migrant Population |
Comments |
|---|---|---|---|---|
| Mexico | - CVC - Broad-spectrum antibiotics - TPN - Colonization by Candida | - Infant malnutrition (13%) - HIV/AIDS (0.3 %) - TB (22/100,000) - Fungal risk: 1.19‰ (regional mean). associated to CVC and TPN |
- Malnutrition and anemia in Central American migrants - COPD in rural displaced - Fungal risk: probable aspergillosis and candidemia in detention centers |
The high rotation in shelters and the presence of wet soils increase the exposure to fungal spores. |
| Haiti | - Broad-spectrum antibiotics - CVC - TPN | - Severe malnutrition (22%) - Epidemics of cholera and diarrhea - Fungal risk: post-breakout mucocutaneous mycoses; limited data on IC |
- Critical post-disaster malnutrition - Cholera outbreaks in camps - Fungal risk: probable increase in mucocutaneous and systemic candidiasis |
Sanitary collapse and lack of available antifungals limit the management of deep infections. |
|
Central America Northern Triangle (El Salvador. Guatemala. Honduras) |
- Broad-spectrum antibiotics - CVC - TPN - Invasive procedures | - Chronic malnutrition (25–30%) - TB (≈ 100/100,000) - Trauma and violence - Fungal risk: skin cysts and candidemia in municipal ICUs |
- Malnutrition in rural displaced persons - TB in informal camps - Fungal risk: IC in burns and associated to CVC |
The insecurity and dispersion of the population make prevention and timely treatment interventions difficult. |
| Colombia | - Broad-spectrum antibiotics (OR 5.6) - CVC (OR 4.7) - TPN (OR 4.6) - Colonization by Candida | - Chronic malnutrition (10.5%) - HIV/AIDS (0.4%) - TB (21/100,000) - Fungal risk: candidemia associated to CVC. TPN. and antibiotics (OR 5.6) |
- Acute and chronic malnutrition - HIV/AIDS (~ 0.5%) - Elevated risk for pulmonary and extrapulmonary TB - Fungal risk: similar to the general hospitalized. aggravated by overcrowding and malnutrition |
The combination of malnutrition and overcrowding enhances immunosuppression. increasing susceptibility to HF. |
| Venezuela | Same as Colombia. but with scarce local data | - Infant malnutrition (11.3%) - Diabetes (8%) - TB (17/100,000) - Fungal risk: similar to Latin America, with local under-registration |
- Malnutrition due to food crisis - Chronic diseases (diabetes, HTN) - TB in returnees - Fungal risk: possible delay in diagnosis, with poor surveillance |
The humanitarian crisis hinders timely access to antifungal diagnosis and treatment. |
| Brazil | - CVC - Broad-spectrum antibiotics - TPN – Recent surgery | - Infant malnutrition (7.4%) - HIV/AIDS (0.4%) - TB (32/100,000) - Fungal risk: outbreaks of candidemia in the ICU; increased isolates of N. glabratus |
- Moderate malnutrition in Haitian refugees - HIV/AIDS in urban displaced persons - Chronic renal disease (dialysis) in Haitian refugees - Chronic kidney disease (dialysis) in Haitian refugees - Fungal risk: elevated in dialysis and ICU patients |
Migration from Haiti generates social stress and hinders the continuity of antifungal treatments. |
| Peru | - Broad-spectrum antibiotics - CVC - Recent surgery - MV - TPN | - Infant malnutrition (12 %) - TB (119/100 000) - HIV/AIDS (0.3%) - Fungal risk: incidence of 2.04‰ in ICU; mortality 39.6% |
- Malnutrition in rural displaced persons - Extrapulmonary TB - TB-HIV co-infection in migrants - Fungal risk: similar to general inpatients |
Internal-urban displacement delays seeking care, increasing fungal complications. |
* As no specific studies were found in this population, risk factors derived from social determinants of health are proposed. TB: tuberculosis, TPN: total parenteral nutrition, CVC: central venous catheter, VM: mechanical ventilation, IC: invasive candidiasis, COPD: chronic obstructive pulmonary disease, ICU: intensive care unit, HTN: hypertension; CKD: chronic kidney disease.
Table 3.
Gaps in Access to IC Diagnosis and Treatment: General vs. Migrant/Displaced Population [1,12,51,117,175,180,181,182].
| Country | IC Burden (Incidence; Mortality) | Diagnosis and Treatment General Population |
Diagnosis and Treatment Displaced/Migrant Population |
Comments |
|---|---|---|---|---|
| Mexico | 1,19‰; 30–76% (regional mean) |
Diagnosis: - Cultures and stains (48-72 h)- BDG/AGA (3 national institutes)- MALDI-TOF (5 high-complexity hospitals) Treatment: - FCZ- Standard AmB - L-AmB (limited)- Echinocandins (available, irregular distribution) |
Diagnosis: - Cultures and stains in large hospitals - BDG and MALDI-TOF almost absent at the second level Treatment: - FCZ- D-AmB- Echinocandins (very limited access) |
Existing national protocol, but uneven distribution of reagents and drugs delays the management of migrants and displaced persons. |
| Haiti | 1.19‰; 30–76% (regional mean) |
Diagnosis: - Cultures in 2 central laboratories (48–72 h)- No BDG, PCR, or MALDI-TOF. Treatment: - Generic AmB - FCZ (ONG) |
Diagnosis: - Clinical (lack of specialized laboratories) Treatment: - AmB- FCZ- Echinocandins (not available) |
Healthcare collapse and dependence on NGOs leave displaced persons without timely diagnosis and appropriate treatment. |
|
Central America Northern Triangle (El Salvador, Guatemala, Honduras) |
1,19‰; 30–76% (regional mean) |
Diagnosis: - Local cultures - No BDG, PCR, or MALDI-TOF Treatment: - D-AmB- FCZ- ITZ- Echinocandins (not included in the public service) |
Diagnosis: - Clinical and primary cultures - No immunological/molecular testing Treatment: - AmB- FCZ- Echinocandins (not accessible) |
Lack of training and equipment in local laboratories; diagnostic delays increase mortality among displaced persons. |
| Colombia | 1.19‰; 30–76% (regional mean) |
Diagnosis: - Cultures and stains (48–72 h)- BDG (reference)- MALDI-TOF (large hospitals) Treatment: - D-AmB, L-AmB (limited)- FCZ, ITZ- Echinocandins (expensive, scarce) |
Diagnosis: Cultures and stains (reference) – No BDG/MALDI-TOF in primary care Treatment: - AmB- FCZ- Echinocandins (not accessible) |
Delays in diagnosis and lack of echinocandins in the public system increase mortality in displaced persons. |
| Venezuela | 1.19‰; 30–76% (regional mean) |
Diagnosis: - Cultures (very slow) - No BDG nor MALDI-TOF Treatment: - Generic AmB - FCZ (unstable stock) |
Diagnosis: - Predominantly clinical - No immunological/molecular testing Treatment: - AmB- FCZ- Echinocandins (not available) |
Chronic shortage of reagents and antifungals aggravates delays in displaced persons. |
| Brazil | 2.49‰; 54% |
Diagnosis: - Cultures and stains (48–72 h) - BDG (2–3 reference laboratories) - MALDI-TOF (large hospitals) Treatment: - AmB (including liposomal) - FCZ, VCZ, echinocandins |
Diagnosis: - Cultures/stains in urban centers- Little BDG/MALDI-TOF outside of capitals - PCR almost null Treatment: - D-AmB- FCZ- Echinocandins (limited) |
Large health centers offer adequate care, but rural refugees and displaced persons are almost completely lacking these options. |
| Peru | 2.04‰; 39.6% (30 days) |
Diagnosis: - Cultures (48–72 h)- BDG (2 laboratories in Lima)- MALDI-TOF (1 university center) Treatment: - D-AmB, L-AmB (limited stock) - FCZ, ITZ, echinocandins (irregular stock) |
Diagnosis: - Cultures - Outside Lima without BDG/MALDI-TOF/PCR Treatment: - AmB- FCZ- Echinocandins (virtually inaccessible) |
Concentration of resources in Lima leaves displaced persons from the interior of the country with almost insurmountable barriers to diagnosis and treatment. |
Note: Regional incidences reflect the best available estimate where no specific national data are available. IC: invasive candidiasis; BDG: (1→3)-β-D-glycan, PCR - polymerase chain reaction; MALDI-TOF: mass spectrometry, FCZ: fluconazole, ITZ: itraconazole, AmB: Amphotericin, D-AmB: Amphotericin B deoxycholate, L-AmB: Liposomal Amphotericin B, VCZ: voriconazole.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



