Submitted:
07 July 2025
Posted:
08 July 2025
You are already at the latest version
Abstract
Background/Objectives: The COVID-19 pandemic supposed an increase of burnout vulnerability to the healthcare workers, which often translated into higher potential risks for their personal safety and that of their patients. This study is based on the JD-R model to explore emotional exhaustion and stress as a result of a lack of personal re-sources such as self-efficacy to cope with stress, unhealthy lifestyle, poor emotion reg-ulation, and work demands. Methods: The sample was composed by 189 emergency healthcare workers from Spain, aged between 26 and 59 years old. A cross-sectional and correlational study was carried out through an online platform. Results: The me-diation, moderation and Structural Equation Modelling analyses supported the pro-posed model, demonstrating good fit to the data. Work demands showed both a posi-tive direct effect and an indirect effect on emotional exhaustion through emotion reg-ulation and stress. In turn, self-efficacy to cope with stress and healthy lifestyle showed indirect effects on emotional exhaustion, also through emotion regulation and stress. Further, healthy lifestyle moderated the relationship between stress and emotional ex-haustion, by mitigating the negative influence of stress on emotional exhaustion. Con-clusion: The study highlights the importance of incorporating selfcare in coping with stress and preventing burnout and should be considered when designing interventions in the emergency healthcare context to improve wellbeing in its workers.
Keywords:
emergency healthcare workers
; job demands-resources model
; structural equation modeling
; burnout
; personal resources
1. Introduction
The COVID-19 pandemic supposed an unprecedented challenge for our society, [1] revealing how healthcare professionals were exposed to risks to their safety and to their mental health. Throughout this threatening episode, the incidence of anxiety and post-traumatic stress disorder was high among medical staff, especially among female medical staff and female nurses in China [2]. Similar results were found in the United States, where more than half of the healthcare workers sample had mild psychiatric symptoms and at least 40% had symptoms consistent with an emotional disorder, [3] and in eight European countries, where about one-third of health professionals reported experiencing moderate to extremely severe level of distress [4].
Healthcare workers (HCW) have been identified as more vulnerable to stress due the potential consequences of their actions and their responsibility for human lives [5]. Additionally, Wang et al. [6] explained that professionals who provide direct patient care in crisis situations experience increased demands and patient volume against a resource-constrained environment which has been associated with increased psychological stress.
Previous research offers clear evidence that healthcare and emergency workers face significant levels of stress, which can lead to dysfunctional reactions such as psychosomatic disorders, disturbances in sleep patterns, fatigue, irritability, nervousness, distractibility, among others [7]. Stress is also known to generate a greater propensity to suffer from depression, [8] work injuries, [9] risks of accidents and work-related illnesses [10]. Physician burnout has shown to have an impact both on their health, the health care system, and the quality of patient treatment, resulting on negative outcomes that include lower patient satisfaction, depression, poor self-care, reduced productivity, among others [11]. WHO and ILO [12] have highlighted that this ineffective care and potential medical errors could also lead to negative patient safety outcomes.
The stress inherent to these demanding settings is often not managed effectively, which can contribute to the development of burnout, [13] characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment. Emotional exhaustion has been found to act as a precursor to the other two dimensions, [14] which is why burnout studies often consider it its central core [15,16,17].
Almutairi and Azza [18] have shown that emergency medical service (EMS) professionals experience high levels of emotional exhaustion and depersonalization, and low levels of accomplishment as a result of chronic occupational stress. Purvanova and Muros [19] have addressed gender differences on burnout dimensions in their meta-analysis, where women showed a tendency to be more emotionally exhausted than men, while men showed higher levels of depersonalization than women. As noted by García-Herrero et al. [20], women show higher levels of occupational stress than men, which has been related to their home-career workload and lack of time for personal activities.
The job demands-resources (JD-R) [21] model of burnout is frequently used to address factors that influence the well-being of employees. It assumes that there are two categories applicable to any occupational settings: job demands and job resources. The first refers to the physical, social, or organizational aspects of the job that require sustained physical or mental effort and are associated with physiological and/or psychological costs, while the latter refers to the physical, psychological, social or organizational aspects of the job that may help to accomplish work objectives, minimize the costs associated with job demands, and promote personal growth [22]. Additionally, personal resources, understood as an individuals’ ability to control and successfully impact their environment, has a reciprocal relationship with job resources and is expected to reduce the negative effects of work demands on employee well-being [23]. This model predicts that job demands, whether they are high or unfavorable, are positively related to burnout, while job resources are negatively related to job disengagement. Moreover, it predicts that employees with more personal resources have access to more job resources, thus better dealing with job demands.
Under the JD-R theoretical framework, stress and emotional exhaustion cannot be adequately discussed without bringing to the table those resources that may counteract their effect, such as self-efficacy. In the occupational context, this concept refers to “the confidence that one can employ the skills necessary to deal with job-specific tasks and cope with job-specific challenges, job-related stress, and its consequences” [24] (p. 368). In the healthcare sector, self-efficacy has been found to influence how new graduate nurses interact with their workplace, preventing the development of burnout and turnover in demanding working conditions [25]. Additionally, self-efficacy was found to be a predictor of burnout in healthcare workers and a key focus point when designing interventions in healthcare personnel during the COVID-19 pandemic [26]. Since specific self-efficacy predicts behavior better than general self-efficacy, [27] it becomes relevant to explore how self-efficacy to cope with stress relates to emotional exhaustion, which to the best of our knowledge has not been studied in emergency healthcare workers.
In this sense, emotion regulation has been defined as the processes and strategies used to modulate emotional arousal and emotional reactions in order to meet environmental demands [28,29]. Emotional arousal has been considered to play an important role in relation to psychological stress [30]. Using self-regulatory strategies or emotion regulation techniques such as mindfulness has been associated with a reduction of burnout in doctors [31]. Another interesting finding was that of Martín-Brufau et al. [32], who found that similar workload conditions resulted on different levels of burnout depending on the emotion regulation strategies carried out by healthcare residents. Additionally, emotion regulation has been found to be a predictor of burnout: Gagnon et al. [33] study showed that self-regulation skills negatively predicted the three dimensions of burnout, while a regression analysis by Martínez-Iñigo et al. [34] found that emotion regulation was negatively associated with the emotional exhaustion component of burnout. Moreover, emotion regulation has been found to act as a mediator in the relationship established between job demands and emotional exhaustion [35].
Habits are another variable to consider when referring to personal resources. It is known that adopting healthy lifestyle habits, such as regular exercise, maintaining a balanced diet, and getting sufficient rest, can help to effectively cope with stressors. A recent study carried out in China during the pandemic among HCW showed that becoming less physically active and getting less sleep were significant predictors of moderate to severe anxiety symptoms, while poor nutrition and low physical activity were both significant predictors of moderate to severe depressive symptoms [36]. In this line, Balatoni et al. [37] highlighted the importance of promoting healthy lifestyles in healthcare workers, given the high vulnerability of this population to stress and burnout and the particularity of their schedules (e.g., rotating shifts, working longer than 8 hours). Additionally, a healthy lifestyle was found to be a significant moderator in the association between emotional exhaustion and work-life boundaries, meaning that those who committed to healthy habits were less prone to experience the negative impact of blurred work-life boundaries on emotional exhaustion [38]. In the same way, healthy lifestyle habits have been shown to moderate the stress-burnout relationship: lower healthy lifestyle habits increase the negative impact of stress on burnout [39].
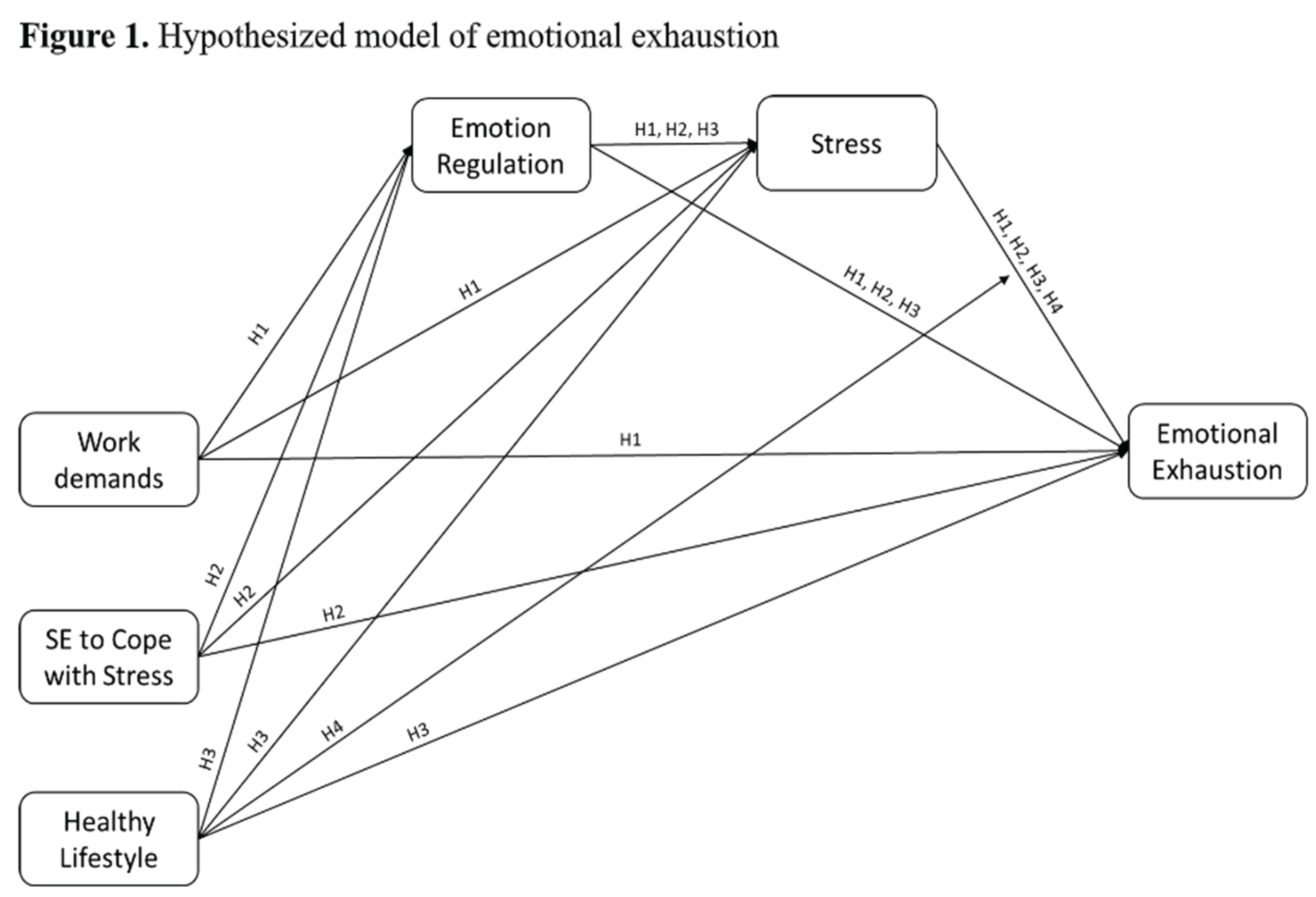
This highlights the need to assess psychosocial risks in a context as demanding as the emergency healthcare sector, as well as potential protective factors and coping mechanisms, for developing interventions that promote well-being of its workers. Therefore, we aim to identify predictors, mediators, and moderators that have an impact on emotional exhaustion in emergency healthcare workers. Specifically, this study bases on the JD-R model to explore how job demands (work demands), and personal resources (self-efficacy to cope with stress, emotion regulation and healthy habits) interact with emotional exhaustion. Considering the reviewed literature, the following hypotheses are proposed:
As works demands are associated to emotion regulation [35] and to emotional exhaustion [21]; as emotion regulation is related to both stress [30] and emotional exhaustion [35]; and as stress is related to emotional exhaustion [18], it is hypothesized that:
H1
: Emotion regulation and stress act as serial mediators in the relationship established between work demands and emotional exhaustion.
Moreover, as self-efficacy to cope with stress is related to emotion regulation, stress, and burnout [25,26], it is hypothesized that:
H2
: Emotion regulation and stress act as serial mediators in the relationship established between self-efficacy to cope with stress and emotional exhaustion.
As well, as healthy lifestyle has been shown be associated with emotion regulation, stress and burnout [33,34,37], it is hypothesized that:
H3:
Emotion regulation and stress act as serial mediators in the relationship established between healthy lifestyle and emotional exhaustion.
As well, as healthy lifestyle has been shown to moderate the stress-burnout relationship [39], it is hypothesized that:
H4:
Healthy lifestyle will moderate the strength of the relationship between stress and emotional exhaustion.
In brief, we hypothesize the predictive model of emotional exhaustion presented in Figure 1.
2. Materials and Methods
2.1. Participants and Procedure
The sample was composed by 189 Spanish emergency healthcare workers, of which 49.7% were male and 50.3% were female, aged between 26 and 59 (M = 49; SD = 8.88). Regarding their marital status, 53.4% reported being married, 20.6% single, 11.1% common-law partner, 11.6% divorced, and 3.2% separated. Out of the 189 respondents, 138 have completed university studies. In terms of job categories, the majority of the respondents were medical staff (34.9%), followed by nursing staff (28%), technical staff (23.3%) and managers (13.8%). Regarding the type of activity, 36.5% of participants work exclusively in the Emergency Team, which work directly with patients, 36% in coordination and emergency team or health intervention, 26.5% exclusively in call management or coordination, and 1.1% work exclusively in health intervention.
The study was approved by a research ethics committee and it conforms to the principles outlined in the Declaration of Helsinki [40]. Participation was totally anonymous and voluntary, and participants were informed of the objectives of the research before they provided consent for participation. Participants respond through a link hosted on the organization’s intranet to the questionnaire created using Unipark (v. 10.9).
2.2. Instruments
Sociodemographic data. Sex, age, job category and type of activity were included in the survey.
Work demands. Work demands were assessed with 9 items of the Job Content Questionnaire [41], specifically, from the psychological demands subscale (e.g., “My job requires a great mental effort”, “I don’t have enough time to do my job”). Cronbach’s alpha coefficient is acceptable (α = .78).
Stress. It was measured with 6 items (e.g., “I have been tired”, “I have been irritable”) from the Spanish version of the Copenhagen Psychosocial Questionnaire [42] with a five-point Likert scale. Cronbach’s alpha coefficient is excellent (α = .94).
Emotional exhaustion was measured with 5 items (e.g., “I feel emotionally exhausted because of my job”, “Working all day is really stressful for me”) of the Spanish version of the Maslach Burnout Inventory-General Survey (MBI-GS) [43]. The whole scale consists of three subscales (i.e., emotional exhaustion, cynicism, and professional efficacy), and its reliability ranges from α = .85 to α = .89.
Self-efficacy to cope with stressful situations. This scale by Tabernero et al. [44] assess the capacity that professionals feel for managing stress effectively (e.g., “I feel capable of persisting in what I have proposed despite the adversities”, “I feel capable of effectively handling unexpected events”). Cronbach’s alpha coefficient for the items of this scale was α = .91.
Regulatory Emotional Self-Efficacy. The participants capability to manage their emotional life was assessed with 8 items from the Regulatory Emotional Self-Efficacy scale (RESE) [45] for negative affect, which consists of a five-point Likert scale ranging from being unable to fully capable (e.g., “Avoid flying off the handle when you get angry”, “Avoid getting discouraged by strong criticism”). Cronbach’s alpha coefficient was .91.
Healthy lifestyle. To assess the habits of healthcare emergency workers, the Healthy lifestyle questionnaire was applied (EVS) [46]. It consists of a five-point Likert scale ranging from totally disagree to totally agree (e.g. “I feel good when I smoke”, “I sleep enough hours for my body to be rested”, “Normally, I eat vegetables and fruits everyday”). The twelve items of the scale are grouped into the following factors: tobacco use (α = .85), rest habits (α = .71), respecting meal times (α =.71), and balanced diet (α = .75).
2.3. Statistical Analyses
To test the serial mediating and moderating hypotheses, three different mediating models were tested by using the sixth model of the Process for SPSS macro, with 10.000 bootstrap resamples and a confidence interval of 95%. For hypotheses 1 to 3 (mediational hypotheses), in the 3 models explored, emotional exhaustion was introduced as the dependent variable (DV), emotional regulation as the first serial mediating variable, and stress as the second serial mediating variable. The independent variables (IV) introduced were work demands in the first model explored, self-efficacy to cope with stress in the second model explored, and healthy lifestyle in the third model explored, to respond to the first, second and third hypotheses, respectively. Finally, for hypothesis 4, about the moderating role of healthy lifestyle in the relationship between stress and emotional exhaustion, the test for interaction between healthy lifestyle and stress was included in the third mediating model explored.
Moreover, to test the hypothesized model on emotional exhaustion, with all the relationships together, a SEM model was explored with Mplus 8 [47]. The fit of the model was analyzed using the chi-square test and its p probability level, and the RMSEA (root mean squared error of approximation), CFI (comparative fit index), and TLI (Tucker-Lewis index).
3. Results
3.1. Preliminary Analyses
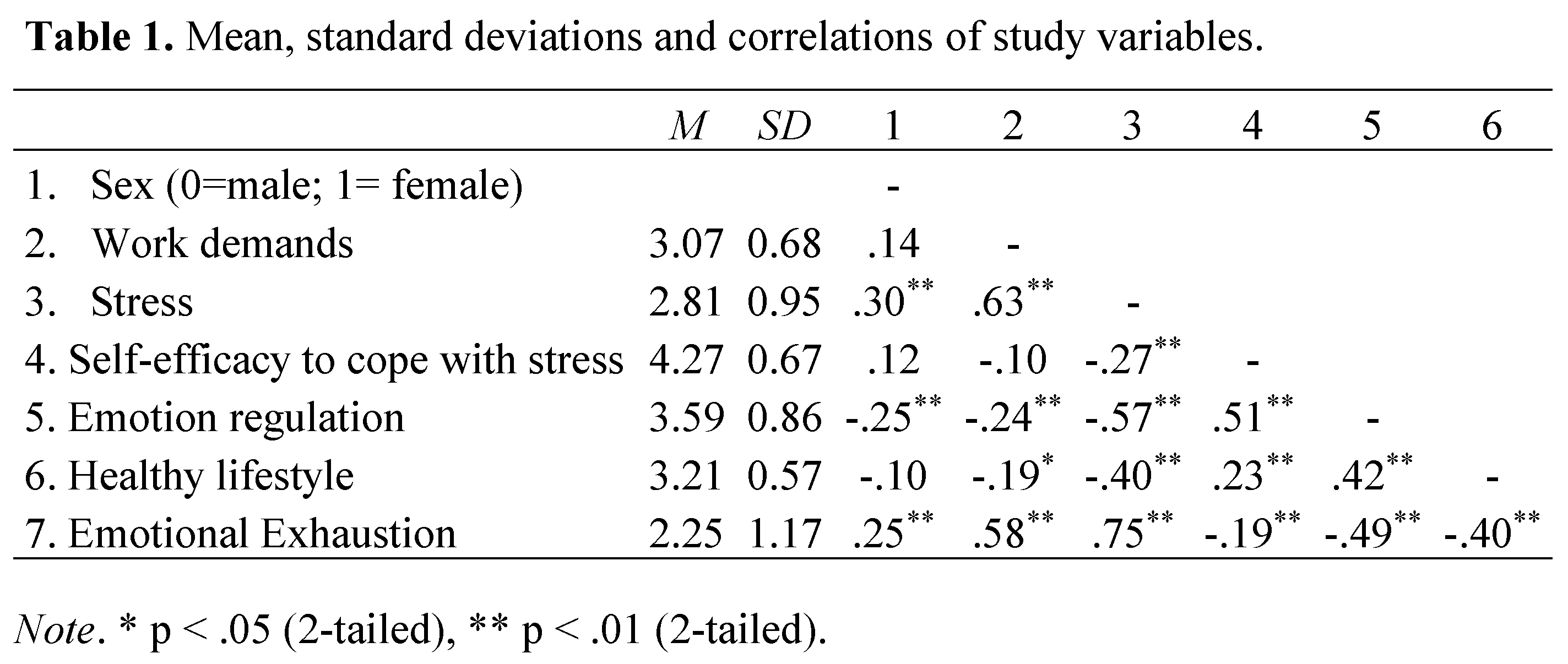
Table 1 shows the correlations among the variables of the study. Results revealed significant intercorrelations in the predicted directions, providing preliminary evidence of the hypotheses of this study. Higher work demands were strongly associated with higher levels of stress, and the latter resulted strongly associated with emotional exhaustion. Moreover, carrying a healthy lifestyle was moderately associated with lower stress, higher emotion regulation and lower emotional exhaustion. Another notable aspect was that significant sex differences were found in correlation with stress, emotion regulation and emotional exhaustion.
3.2. Mediation and Moderation Hypotheses
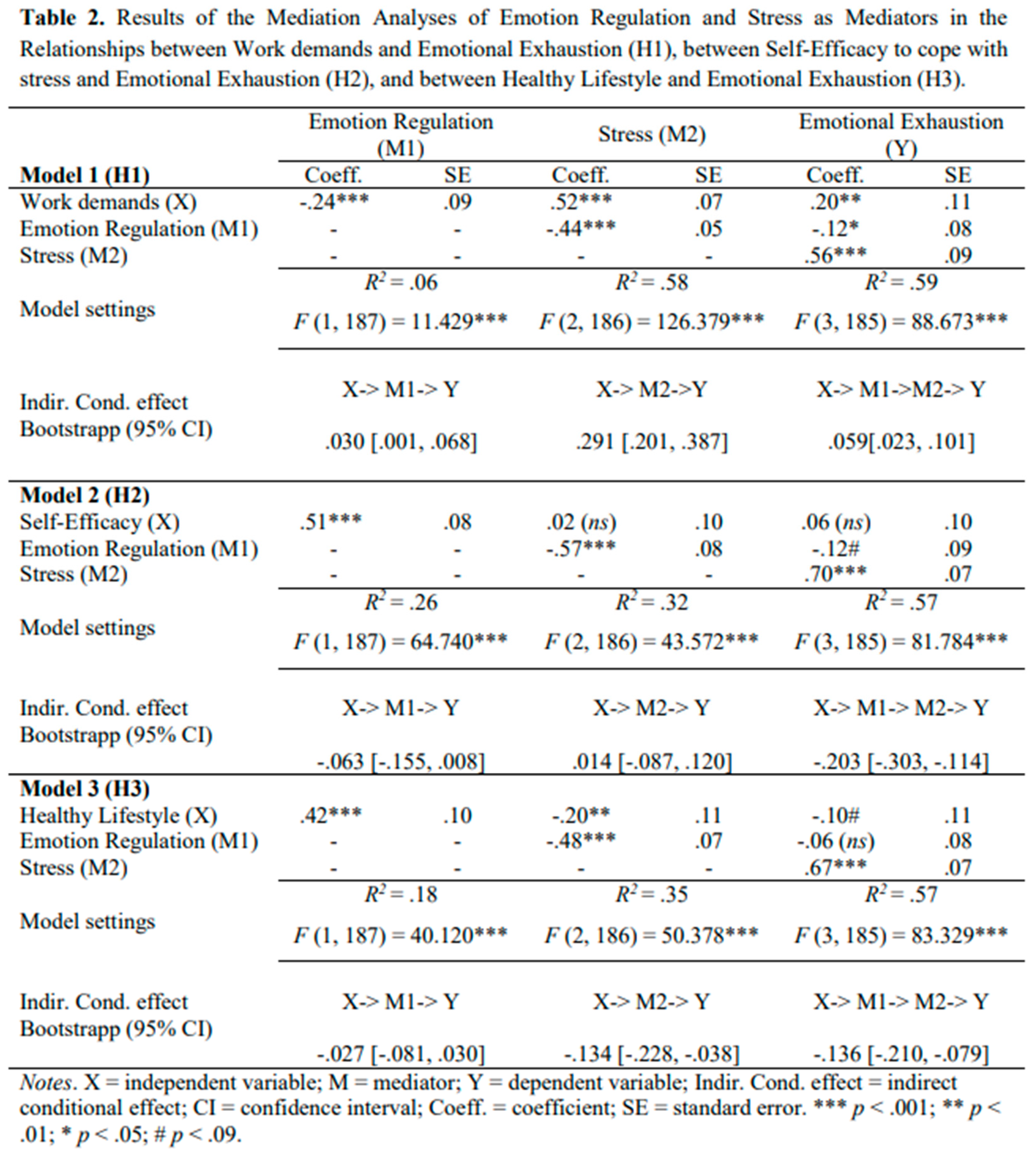
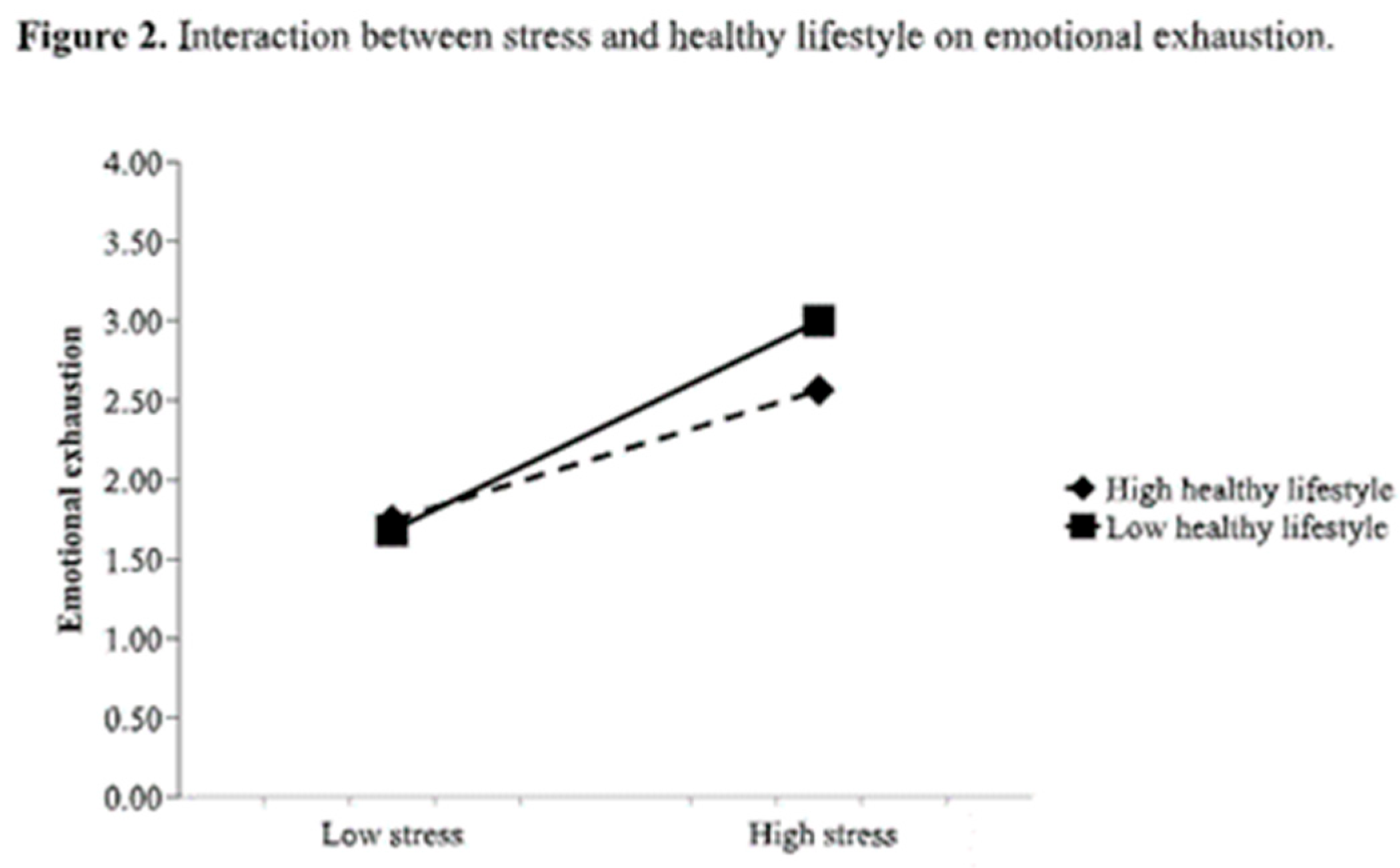
The results of the mediation analyses (Table 2) revealed that emotion regulation (first) and stress (second) mediated the relationships (a) between work demands and emotional exhaustion; (b) between self-efficacy to cope with stress and emotional exhaustion; and (c) between healthy lifestyle and emotional exhaustion, confirming H1, H2 and H3, respectively. Moreover, when performing the serial mediation analysis with healthy lifestyle as predictor (Model 3), the test for interaction between healthy lifestyle and stress on emotional exhaustion was significant (F (1, 184) = 5.719, p = .018), confirming H4 about the moderating role of healthy lifestyle on the relationship between stress and emotional exhaustion. The moderating role of healthy lifestyle can be observed in Figure 2.
3.3. Predictive Model
To test the relationship between antecedents (work demands and self-efficacy to cope with stress), mediators (stress, emotion regulation), moderator (healthy lifestyle), and outcome (emotional exhaustion) simultaneously, we conducted a Structural Equations Modelling (SEM) analysis with Mplus. Figure 3 shows the path diagram, which has three exogenous variables (work demands, self-efficacy to cope with stress, and healthy lifestyle) and three endogenous variables (stress, emotion regulation, and emotional exhaustion). The following indices were used to assess the fit of the model: Chi-Square Statistic (χ2); Root Mean Square Error of Approximation (RMSEA); the Comparative Fix Index (CFI); Tucker-Lewis Index (TLI). The proposed model fit the data reasonably well with χ2=3.658 (p = .30), RMSEA=.034, CFI=.998, and TLI=.991, with all fit indexes above .97 and RMSEA below .05 [48].
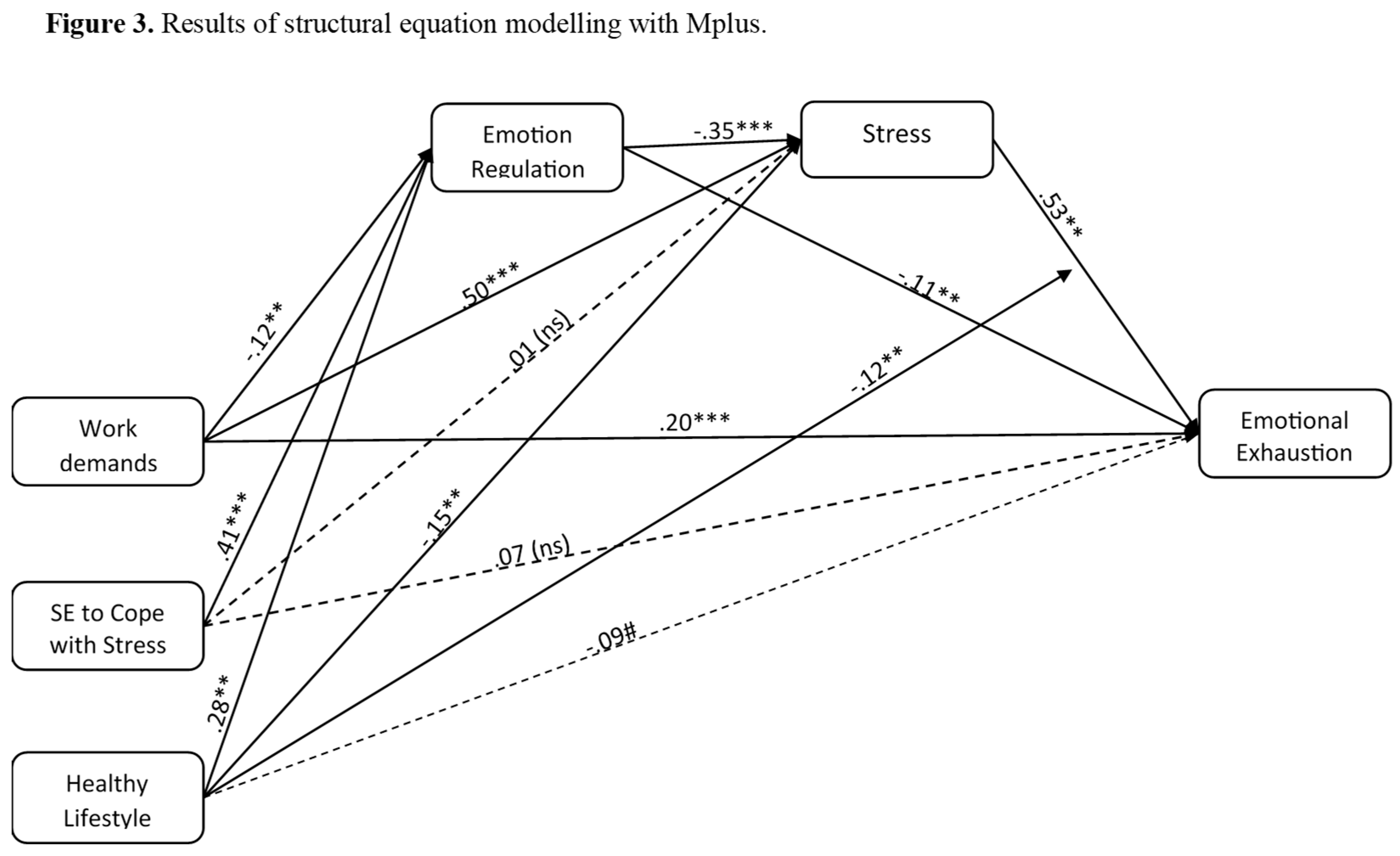
The results of the SEM analysis confirmed the previous findings in a model that integrate all the variables. Work demands are related to emotional exhaustion not only directly, with a positive relationship between themselves, but also indirectly through the serial effect that work demands have on emotion regulation first and in turn on stress. Moreover, self-efficacy to cope with stress showed an indirect effect on emotional exhaustion through emotion regulation and stress. Finally, healthy lifestyle has an indirect effect through emotion regulation and stress, and it has a moderating role between stress and emotional exhaustion. Figure 2 shows a depiction of this interaction. The slope between low stress and high stress was significant for both high healthy lifestyle (t = 4.90, p <.001) and low healthy lifestyle (t = 7.88, p < .001). When comparing both slopes and its t-values, it can be concluded that a less healthy lifestyle can increase susceptibility to stress and aggravate levels of emotional exhaustion, while a healthy lifestyle can have a mitigating or protective effect by reducing the influence of stress on emotional exhaustion.
Moreover, a statistically significant difference was found in the data when higher levels of stress were reported. Specifically, emotional exhaustion turned out lower when there was a high healthy lifestyle than when there was a low healthy lifestyle (t = -2.60, p = .009). This significant difference was not found when lower levels of stress were reported (t = .38, p = .702).
When controlling sex on stress in the SEM model, we found a statistically significant positive relationship (β = .13, p < .01). Additionally, when controlling sex on emotion regulation, we found a statistically significant negative relationship (β = -.15, p < .01). This indicates that there are discernible differences in stress levels and emotion regulation strategies among men and women. However, when controlling sex on emotional exhaustion, the relationship was not significant (β = .03, n.s.), which indicates that sex did not play a role in explaining the variability in emotional exhaustion perception.
4. Discussion
Healthcare professionals have shown to be particularly vulnerable to burnout, which is why several studies have identified organizational risk factors that contribute to its development, such as high work demands, long working hours, high or frequent rotations overtime, and individual factors as job experience, personality traits, coping styles and emotion regulation skills [49]. Burnout is known to have serious implications on their job performance, reducing empathy [50] affecting the quality of patient-treatment [51], and increasing rates of major medical errors [52].
Although burnout was already a significant concern for healthcare professionals, the COVID-19 pandemic supposed an increase of their vulnerability [53], which is why, basing on the JD-R model, this study explored how work demands and personal resources, such as self-efficacy to cope with stress, emotion regulation and healthy habits, interact and associate with the main component of burnout, emotional exhaustion. Specifically, the purpose of this study was to identify predictors, mediators, and moderators that have an impact on emotional exhaustion in emergency healthcare workers.
The results of this research provide support for H1, which predicted that emotion regulation and stress would act as serial mediators in the relationship established between work demands and emotional exhaustion. Moreover, the serial mediating role of emotion regulation and stress in the relationship established between self-efficacy to cope with stress and emotional exhaustion expected in H2 was also supported. Additionally, emotion regulation and stress showed to be significant mediators in the relationship between healthy lifestyle and emotional exhaustion, as stated in H3. Finally, healthy lifestyle moderated the strength of the mediated relationship between stress and emotional exhaustion, supporting H4.
Our findings are consistent with previous research. In general, studies have shown that emotional exhaustion is positively related to job demands, such as work overload and emotional demands, while being negatively related to job resources [54]. Additionally, emotion regulation skills have been found to play a fundamental role in how healthcare workers cope with workplace stressors, influencing their overall well-being and ultimately their practice [31,55]. Although self-efficacy to cope with stress has been little studied, especially in emergency healthcare context, it is known that low levels of general self-efficacy led to stress and burnout [56,57]. Regarding healthy lifestyle, poor sleep quality as a result of workload has been found to relate to emotional exhaustion and struggles when recovering from stress [58]. In this sense, healthy habits and their promotion has been essential for the development of intervention programs for preventing burnout and substance use disorder in healthcare professionals [59].
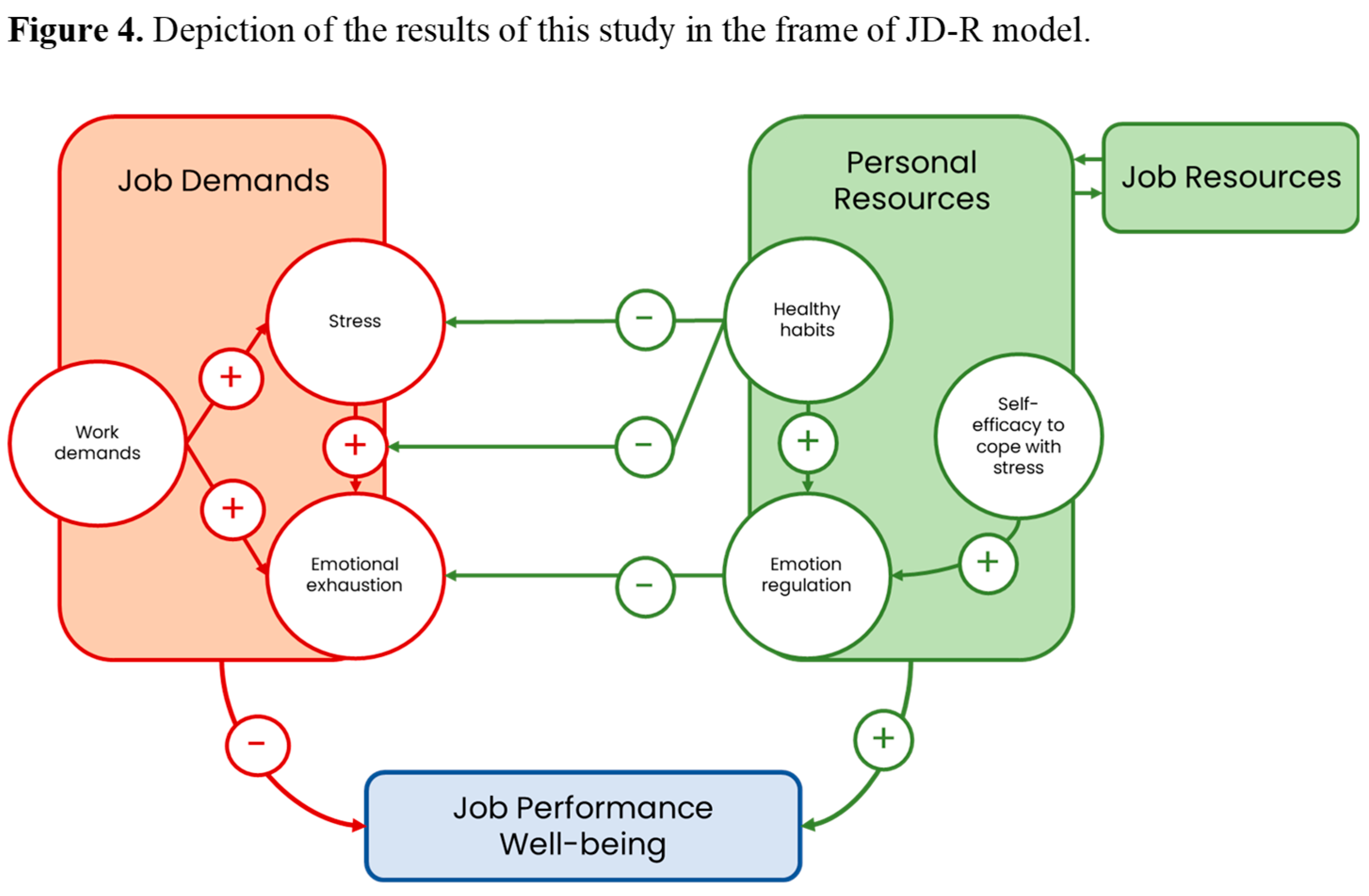
Our results provide empirical support for the JD-R model in the context of emergency healthcare, introducing personal resources as a process that impacts on the development of emotional exhaustion, thus providing relevant relationships that make job resources more effective (see Figure 4). Following [23], personal resources are known to moderate the impact of job demands on employee well-being. In this sense, the identification of healthy lifestyle as a significant moderator in the mediated relationship between stress and emotional exhaustion contributes to understand how personal resources can mitigate the negative effects of work demands.
Taken together, the interaction between personal resources and job demands has practical implications for emergency healthcare workers. Firstly, the importance of incorporating selfcare, both emotional and physical, in coping with stress and preventing burnout cannot be overstated. Encouraging workers to adopt healthy habits such as regular exercise, a balanced diet, and enough rest can help to reduce the effect of stress on emotional exhaustion. Secondly, training on stress management techniques and emotion regulation can help professionals to cope with such a demanding setting as the emergency healthcare sector [60].
One limitation of the present study is that the data were gathered in a period where COVID-19 cases were rising. The COVID-19 unpredictability and its unknown extent may have increased psychological stress [61], which is not related to work demands and could be acting as an extraneous variable. Additionally, by using a cross-sectional design behavioral changes could not be observed and causal inferences regarding the relationships tested are discarded. We suggest that future research aim for a longitudinal design to make comparisons over time.
Although personal resources are essential to prevent emotional exhaustion in the healthcare context, job resources such as workplace support, have shown a significant role in burnout prevention [32]. Furthermore, variables such as gender and age could be considered for a more extensive comprehension of emotional exhaustion, since older professionals have shown to be more engaged with their work, use more emotion regulation strategies and are more confident with their abilities, thus experiencing less emotional exhaustion in comparison to younger employees [62], and women appear to be more affected by job demands and psychological distress than men [63].
Nevertheless, this research contributes to the study of the variables that influence the development of emotional exhaustion in emergency healthcare workers by highlighting the importance of individual factors. It further implicates that healthcare organizations should implement interventions that promote healthy habits, emotion regulation skills and coping strategies to deal with high work demands in order to prevent the development of burnout and its consequences. Finally, this study suggests the incorporation of the aforementioned personal resources into future research that aim to provide an extensive frame of occupational stress and burnout in emergency healthcare professionals.
Author Contributions
Conceptualization, A.A. and C.T.; methodology, A.A. and E.C.; formal analysis, A.A. and E.C.; investigation, A.A. and V.T.; resources, A.A, C.T. and B.L.; data curation, R.C.; writing—original draft preparation, A.A. and V.T.; writing—review and editing, A.A., R.C. and B.L.; funding acquisition, A.A., C.T. and B.L. All authors have read and agreed to the published version of the manuscript.
Funding
This work has been carried out under the projects “FireHealth: Monitorización de indicadores de estrés en el Cuerpo de Bomberos y utilización de una herramienta m-health para mejorar su bienestar” (Ref. PII2024/0019), “Fipsipro: m-health en la Prevención de Riesgos Psicosociales” (Ref. CTC-2022132186), “SALPRO, Analysis of physiological indicators and psychosocial factors in occupational health of health professionals” (Ref. PI-0098-2018) funded by Junta de Andalucía (Spain) whose main researcher is Alicia Arenas; and it was funded by the Spanish Ministry of Science, Innovation and Universities, grant number PDI2019-107304RB-I00, whose main researchers are Barbara Luque y Carmen Tabernero.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Hospital Reina Sofía’s ethics committee, with the protocol dated 1–6 January 2020 (committee reference: 5166; report no. 327; approved on 28 September 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to ethical reasons.
Acknowledgments
We acknowledge CES 061Andalucía for its collaboration in this research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Walton, M.; Murray, E.; Christian, M.D. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 201–207. [Google Scholar] [CrossRef]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of medical staff in a tertiary infectious disease hospital for COVID-19. Chin. J. Ind. Hyg. Occup. Dis. 2020, 38, 192–195. [Google Scholar] [CrossRef]
- Young, K.P.; Kolcz, D.L.; O’Sullivan, D.M.; Ferrand, J.; Fried, J.; Robinson, K. Health care workers’ mental health and quality of life during COVID-19: Results from a mid-pandemic, national survey. Psychiatr. Serv. 2021, 72, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Hummel, S.; Oetjen, N.; Du, J.; Posenato, E.; Resende de Almeida, R.M.; Losada, R.; Ribeiro, O.; Frisardi, V.; Hopper, L.; Rashid, A.; et al. Mental health among medical professionals during the COVID-19 pandemic in eight European countries: Cross-sectional survey study. J. Med. Internet Res. 2021, 23, e24983. [Google Scholar] [CrossRef] [PubMed]
- Koinis, A.; Giannou, V.; Drantaki, V.; Angelaina, S.; Stratou, E.; Saridi, M. The impact of healthcare workers’ job environment on their mental-emotional health. Coping strategies: The case of a local general hospital. Health Psychol. Res. 2015, 3. [Google Scholar] [CrossRef]
- Wang, L.; Norman, I.; Xiao, T.; Li, Y.; Li, Z.; Leamy, M. Evaluating a psychological first aid training intervention (Preparing Me) to support the mental health and wellbeing of Chinese healthcare workers during healthcare emergencies: Protocol for a randomized controlled feasibility trial. Front. Psychiatry 2022, 12, 809679. [Google Scholar] [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Coping with COVID-19: Emergency stress, secondary trauma and self-efficacy in healthcare and emergency workers in Italy. Front. Psychol. 2020, 11, 566912. [Google Scholar] [CrossRef]
- Yoshizawa, K.; Sugawara, N.; Yasui-Furukori, N.; Danjo, K.; Furukori, H.; Sato, Y.; Tomita, T.; Fujii, A.; Nakagam, T.; Sasaki, M.; Nakamura, K. Relationship between occupational stress and depression among psychiatric nurses in Japan. Arch. Environ. Occup. Health 2016, 71, 10–15. [Google Scholar] [CrossRef]
- Kim, Y.K.; Ahn, Y.S.; Kim, K.; Yoon, J.H.; Roh, J. Association between job stress and occupational injuries among Korean firefighters: A nationwide cross-sectional study. BMJ Open 2016, 6, e012002. [Google Scholar] [CrossRef]
- Jiménez-Paneque, R.J.; Pavés-Carvajal, J.R.P. Occupational hazards and diseases among workers in emergency services: A literature review with special emphasis on Chile. Medwave 2015, 15, e6239. [Google Scholar] [CrossRef]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; International Labour Organization. Caring for Those Who Care: Guide for the Development and Implementation of Occupational Health and Safety Programmes for Health Workers; WHO: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240040779 (accessed on 19 May 2025).
- Maslach, C.; Schaufeli, W.; Leiter, M. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Ito, J.; Brotheridge, C. Resources, coping strategies, and emotional exhaustion: A conservation of resources perspective. J. Vocat. Behav. 2003, 63, 490–509. [Google Scholar] [CrossRef]
- Edmondson, D.R.; Matthews, L.M.; Ambrose, S.C. A meta-analytic review of emotional exhaustion in a sales context. J. Pers. Sell. Sales Manag. 2019, 39, 275–286. [Google Scholar] [CrossRef]
- Fiabane, E.; Gabanelli, P.; La Rovere, M.T.; Tremoli, E.; Pistarini, C.; Gorini, A. Psychological and work-related factors associated with emotional exhaustion among healthcare professionals during the COVID-19 outbreak in Italian hospitals. Nurs. Health Sci. 2021, 23, 670–675. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of burnout among physicians: A systematic review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef]
- Almutairi, M.N.; Azza, A.A. Burnout and coping methods among emergency medical services professionals. J. Multidiscip. Healthc. 2020, 13, 271–279. [Google Scholar] [CrossRef]
- Purvanova, R.K.; Muros, J.P. Gender differences in burnout: A meta-analysis. J. Vocat. Behav. 2010, 77, 168–185. [Google Scholar] [CrossRef]
- García-Herrero, S.; Mariscal-Saldaña, M.Á.; García-Rodríguez, J.G.; Ritzel, D.O. Influence of task demands on occupational stress: Gender differences. J. Saf. Res. 2012, 43, 365–374. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E.; De Boer, E.; Schaufeli, W.B. Job demands and job resources as predictors of absence duration and frequency. J. Vocat. Behav. 2003, 62, 341–356. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E.; Sanz-Vergel, A. Job Demands-Resources Theory: Ten Years Later. Annu. Rev. Organ. Psychol. Organ. Behav. 2023, 10, 25–53. [Google Scholar] [CrossRef]
- Shoji, K.; Cieslak, R.; Smoktunowicz, E.; Rogala, A.; Benight, C.C.; Luszczynska, A. Associations between job burnout and self-efficacy: A meta-analysis. Anxiety Stress Coping 2016, 29, 367–386. [Google Scholar] [CrossRef]
- Laschinger, H.K.S.; Grau, A.L. The influence of personal dispositional factors and organizational resources on workplace violence, burnout, and health outcomes in new graduate nurses: A cross-sectional study. Int. J. Nurs. Stud. 2012, 49, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Cotel, A.; Golu, F.; Pantea Stoian, A.; Dimitriu, M.; Socea, B.; Cirstoveanu, C.; Davitoiu, A.M.; Jacota-Alexe, F.; Oprea, B. Predictors of burnout in healthcare workers during the COVID-19 pandemic. Healthcare 2021, 9. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; W.H. Freeman: New York, NY, USA, 1997; pp. 1–604. [Google Scholar]
- Thompson, R.A. Emotion regulation: A theme in search of definition. Monogr. Soc. Res. Child Dev. 1994, 59, 25–52. [Google Scholar] [CrossRef]
- Wang, M.; Saudino, K.J. Emotion regulation and stress. J. Adult Dev. 2011, 18, 95–103. [Google Scholar] [CrossRef]
- Lazarus, R.S. Stress and Emotions: A New Synthesis; Springer: New York, NY, USA, 2006; pp. 1–320. [Google Scholar]
- Jackson-Koku, G.; Grime, P. Emotion regulation and burnout in doctors: A systematic review. Occup. Med. 2019, 69, 9–21. [Google Scholar] [CrossRef]
- Martín-Brufau, R.; Martin-Gorgojo, A.; Suso-Ribera, C.; Estrada, E.; Capriles-Ovalles, M.E.; Romero-Brufau, S. Emotion regulation strategies, workload conditions, and burnout in healthcare residents. Int. J. Environ. Res. Public Health 2020, 17. [Google Scholar] [CrossRef]
- Gagnon, M.C.J.; Durand-Bush, N.; Young, B.W. Self-regulation capacity is linked to wellbeing and burnout in physicians and medical students: Implications for nurturing self-help skills. Int. J. Wellbeing 2016, 6. [Google Scholar] [CrossRef]
- Martínez-Iñigo, D.; Totterdell, P.; Alcover, C.M.; Holman, D. Emotional labour and emotional exhaustion: Interpersonal and intrapersonal mechanisms. Work Stress 2007, 21, 30–47. [Google Scholar] [CrossRef]
- Yin, H.; Huang, S.; Wang, W. Work environment characteristics and teacher well-being: The mediation of emotion regulation strategies. Int. J. Environ. Res. Public Health 2016, 13, 907. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Zhang, N.; Zhu, J. Healthy lifestyle changes and mental health of healthcare workers during the COVID-19 pandemic in China. Curr. Psychol. In press. [CrossRef]
- Balatoni, I.; Szépné, H.V.; Kiss, T.; Adamu, U.G.; Szulc, A.M.; Csernoch, L. The importance of physical activity in preventing fatigue and burnout in healthcare workers. Healthcare 2023, 11, 1915. [Google Scholar] [CrossRef] [PubMed]
- Pluut, H.; Wonders, J. Not able to lead a healthy life when you need it the most: Dual role of lifestyle behaviors in the association of blurred work-life boundaries with well-being. Front. Psychol. 2020, 11, 607294. [Google Scholar] [CrossRef]
- Allen, H.K.; Barral, A.L.; Vincent, K.B.; Arria, A.M. Stress and burnout among graduate students: Moderation by sleep duration and quality. Int. J. Behav. Med. 2023, 28, 21–28. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Karasek, R. Job Content Instrument Questionnaire and User’s Guide, Version 1.1. 1985. [Google Scholar]
- Moncada, S.; Llorens, C.; Andrés, R.; Moreno, N.; Molinero, E. Manual del método CoPsoQ-istas21 (versión 2) para la evaluación y la prevención de los riesgos psicosociales en empresas con 25 o más trabajadores y trabajadoras, VERSIÓN MEDIA.; Instituto Sindical de Trabajo, Ambiente y Salud: Barcelona, Spain, 2014. [Google Scholar]
- Moreno-Jiménez, B.; Rodríguez-Carvajal, R.; Escobar Redonda, E. La evaluación del burnout profesional. Factorialización del MBI-GS. Un análisis preliminar. Ansiedad Estrés 2007, 7, 69–78. [Google Scholar]
- Tabernero, C.; Arenas, A.; Briones, E. Self-efficacy training programs to cope with highly demanding work situations and prevent burnout. In Handbook of Managerial Behavior and Occupational Health; Antoniou, A., Cooper, C., Chrousos, G., Spielberger, C., Eysenck, M., Eds.; Edward Elgar Publishing: Cheltenham, UK, 2009; pp. 278–291. [Google Scholar]
- Caprara, G.V.; Di Giunta, L.; Eisenberg, N.; Gerbino, M.; Pastorelli, C.; Tramontano, C. Assessing regulatory emotional self-efficacy in three countries. Psychol. Assess. 2008, 20, 227–237. [Google Scholar] [CrossRef]
- Leyton, M.; Lobato, S.; Batista, M.; Aspano, M.A.; Jiménez, R. Validación del cuestionario de estilo de vida saludable (EVS) en una población española. Rev. Iberoam. Psicol. Ejerc. Deporte 2018, 13, 23–31. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide. Statistical Analysis with Latent Variables, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017; Available online: http://www.statmodel.com/download/usersguide/MplusUserGuideVer_8.pdf.
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2009; pp. 1–816. [Google Scholar]
- Kinman, G.; Dovey, A.; Teoh, K. Burnout in Healthcare: Risk Factors and Solutions; Society of Occupational Medicine: London, UK, 2023; Available online: https://www.som.org.uk/sites/som.org.uk/files/Burnout_in_healthcare_risk_factors_and_solutions_July2023.pdf.
- Pavlova, A.; Wang, C.X.; Boggiss, A.L.; O’Callaghan, A.; Consedine, N.S. Predictors of physician compassion, empathy, and related constructs: A systematic review. J. Gen. Intern. Med. 2022, 37, 900–911. [Google Scholar] [CrossRef]
- Montgomery, A.; Panagopoulou, E.; Esmail, A.; Richards, T.; Maslach, C. Burnout in healthcare: The case for organisational change. BMJ 2019, 366, l4774. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, D.S.; Profit, J.; Morgenthaler, T.I.; Satele, D.V.; Sinsky, C.A.; Dyrbye, L.N.; Tutty, M.A.; West, C.P.; Shanafelt, T.D. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clin. Proc. 2018, 93, 1571–1580. [Google Scholar] [CrossRef]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi, R.S. Burnout among healthcare providers of COVID-19: A systematic review of epidemiology and recommendations. Arch. Acad. Emerg. Med. 2021, 9, e7. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Van Rhenen, W. How changes in job demands and resources predict burnout, work engagement, and sickness absenteeism. J. Organ. Behav. 2009, 30, 893–917. [Google Scholar] [CrossRef]
- Lee, M.; Jang, K.S. Nurses’ emotions, emotion regulation and emotional exhaustion. Int. J. Organ. Anal. 2019, 27, 1409–1421. [Google Scholar] [CrossRef]
- Cuadrado, E.; Tabernero, C.; Fajardo, C.; Luque, B.; Arenas, A.; Moyano, M.; Castillo-Mayén, R. Journal of Work and Organizational Psychology. J. Work Organ. Psychol. 2021, 37, 133–141. [Google Scholar] [CrossRef]
- Federici, R.A.; Skaalvik, E.M. Principal self-efficacy: Relations with burnout, job satisfaction and motivation to quit. Soc. Psychol. Educ. 2012, 15, 295–320. [Google Scholar] [CrossRef]
- Gillet, N.; Huyghebaert-Zouaghi, T.; Réveillère, C.; Colombat, P.; Fouquereau, E. The effects of job demands on nurses’ burnout and presenteeism through sleep quality and relaxation. J. Clin. Nurs. 2020, 29, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Kulchar, R.J.; Haddad, M.B. Preventing burnout and substance use disorder among healthcare professionals through breathing exercises, emotion identification, and writing activities. J. Interprof. Educ. Pract. 2022, 29, 100570. [Google Scholar] [CrossRef]
- Queirós, C.; Carlotto, M.S.; Kaiseler, M.; Dias, S.; Pereira, A.M. Predictors of burnout among nurses: An interactionist approach. Psicothema 2013, 25, 330–335. [Google Scholar] [CrossRef]
- Amanullah, S.; Ramesh Shankar, R. The impact of COVID-19 on physician burnout globally: a review. Healthcare 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.J.; Machowski, S.; Holdsworth, L.; Kern, M.; Zapf, D. Age, emotion regulation strategies, burnout, and engagement in the service sector: Advantages of older workers. J. Work Organ. Psychol. 2017, 33, 205–216. [Google Scholar] [CrossRef]
- Xie, X.; Huang, C.; Cheung, S.P.; Zhou, Y.; Fang, J. Job demands and resources, burnout, and psychological distress of social workers in China: Moderation effects of gender and age. Front. Psychol. 2021, 12, 741563. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



