Submitted:
01 July 2025
Posted:
02 July 2025
You are already at the latest version
Abstract
The immune system is crucial in protecting against disease, but it can also contribute to chronic illnesses when it malfunctions, with different conditions involving either inflammation or immune suppression. Current treatments often fall short due to limited effectiveness and side effects. Nanomedicine, particularly cerium oxide nanoparticles (nanoceria), offers promising potential due to its unique therapeutic properties and role in modulating macrophages. Nanoceria (<5 nm) possess the catalytic ability to mimic natural enzymes such as superoxide dismutase, peroxidase, and catalase, enabling effective scavenging of reactive oxygen species (ROS), which play a central role in the pathogenesis of chronic inflammation and cancer. This review comprehensively summarizes the current advances in the application of nanoceria for inflammatory and anti-inflammatory therapy, including their modulatory effects on immune cell activation, cytokine production, and resolution of inflammatory responses. We discuss the mechanisms underlying their immunomodulatory actions in various disease contexts, such as rheumatoid arthritis, women’s health conditions (e.g., endometriosis), wound healing, and cancer. Additionally, the review highlights biocompatibility, therapeutic efficacy, adaptability in imaging (theranostics), and challenges in translating nanoceria-based therapies into clinical practice. The multifunctionality of nanoceria positions them as innovative candidates for next-generation immunotherapy aimed at efficiently controlling inflammation and promoting tissue repair.
Keywords:
immune system
; inflammation
; nanoceria
; reactive oxygen species
; immune response
; imaging
; therapy
1. Introduction
Inflammation and immune suppression are essential processes that maintain health in an individual. The immune system is an intricate network comprising cells, signaling molecules, and pathways that protect the body from external threats, such as pathogens and foreign substances, while preventing vital immune cells from damaging healthy tissue. Typically, this system balances pro-inflammatory and anti-inflammatory responses to achieve homeostasis in the body. Inflammation is commonly recognized by visible signs such as swelling, heat, loss of function, redness, and pain, collectively known by the acronym SHARP or the Latin terms tumor, calor, rubor, and dolor [1]. Inflammation has two primary forms: acute inflammation, a short-term response driven by the innate immune system, and chronic inflammation, which involves prolonged activation mainly by the adaptive immune system [2].
Acute inflammation is a vital response that supports survival and tissue repair. It begins when the innate immune system detects specific triggers, such as microbial molecules like lipopolysaccharides or proteins released from damaged cells. Mast cells serve as early detectors, commencing a signaling cascade [3], but neutrophils play a central role by engulfing pathogens and debris and releasing cytokines that recruit additional immune cells [4]. Subsequently, macrophages and T cells arrive, evolving to secrete chemokines and cytokines that amplify the immune response [5]. CD8 T cells primarily release cytotoxic agents to kill infected cells, whereas CD4 T cells regulate and recruit other immune cells in the area [6]. Macrophages adjust their function according to signals received, such as interferon-gamma (IFN-γ) from CD4 T cells, which can polarize them into pro-inflammatory M1 macrophages. These cells further engage neutrophils in a positive feedback loop that sustains inflammation [5].
To ensure healing and limit prolonged inflammation, this same cytokine signaling system activates anti-inflammatory pathways (Figure 1). While CD4 T cells produce IFN-γ to stimulate macrophages, this cytokine also attracts B cells that release anti-inflammatory cytokines and growth factors critical for resolving acute inflammation. B cells counterbalance the inflammatory loop by encouraging macrophages to shift towards the M2 anti-inflammatory macrophage phenotype [5,7]. Interleukin-10 (IL-10) is particularly important, as it signals mast cells to reduce neutrophil recruitment, suppresses CD4 T cells’ pro-inflammatory activity, and prompts macrophages to become anti-inflammatory. As inflammation subsides, cytokines such as tumor necrosis factor-alpha (TNFα) promote new blood vessel formation and improved blood flow, supporting tissue repair and return to normal function [8].
Disruptions to this delicate immune equilibrium can lead to health problems. Chronic inflammatory diseases, known for persistent pain and often a lifelong burden, include conditions like rheumatoid arthritis, which affects about 1% of the global population [9]. Other chronic inflammatory disorders range from relatively mild ailments such as psoriasis to severe illnesses like cardiovascular disease, which may result in heart attacks or strokes [10,11]. Respiratory diseases, including asthma and chronic obstructive pulmonary disease (COPD), cause significant healthcare burden with numerous hospitalizations annually [12,13]. Moreover, chronic inflammation has been implicated in neurodegenerative diseases such as Alzheimer’s disease and dementia, which profoundly impair cognitive and emotional functions [14].
While chronic inflammation is widely recognized, excessive or inappropriate anti-inflammatory responses also pose significant risks. For instance, in certain cancers, such as breast, kidney, and liver tumors, the tumor microenvironment is rich in M2 anti-inflammatory macrophages, often referred to as tumor-associated macrophages (TAMs). These cells secrete cytokines, such as IL-10 and TNFα, which support tumor growth and help tumors evade immune detection [15]. Similarly, compromised immune environments may fail to clear pathogens effectively, allowing infections to worsen and cause greater harm [16].
Current treatments for inflammation, although widely available, often have limitations in effectiveness. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, aspirin, and naproxen, work by inhibiting COX enzymes, reducing common symptoms like pain and swelling [17,18,19]. These medications are effective for acute inflammation but can have significant side effects, including gastrointestinal ulcers, kidney complications, liver damage, and increased bleeding risk [20,21,22]. Due to these concerns, alternative options are often sought, especially for long-term management. Steroids, specifically corticosteroids like hydrocortisone and prednisone, represent another major class of anti-inflammatory agents [23]. Hydrocortisone is commonly used topically for skin conditions such as eczema and psoriasis, offering relief from redness and itching with minimal side effects at low doses [24,25]. Systemic corticosteroids, like prednisone, are more potent and prescribed for conditions ranging from asthma exacerbations to autoimmune diseases [26,27,28]. However, they carry risks including acne, facial swelling known as “moon face,” and psychological effects such as mood disturbances [29,30]. Another option, opioid pain relievers, while not anti-inflammatory, are also frequently used to manage pain associated with inflammation. These drugs work by altering pain perception rather than addressing the underlying immune response [31]. Although valuable in severe or traumatic cases, opioids have significant drawbacks, notably their high potential for addiction [32]. The opioid crisis in the United States, marked by hundreds of thousands of overdose deaths over recent decades [33], highlights the urgent need for safer, more effective treatments that can control inflammation and associated pain without risking dependence.
While current therapeutic modalities for inflammation, including physical therapies and pharmacologic agents like NSAIDs and opioids, offer symptom relief, they face critical limitations mainly due to incomplete efficacy and significant safety concerns. There is an increasing need for novel therapies that focus on modulating specific inflammatory and resolution pathways, offering better safety and tailored approaches to address complex inflammatory conditions. Emerging biologics, resolution pharmacology, and precision medicine represent promising avenues for future inflammation management.
Although not as common as anti-inflammatory treatments, inflammatory treatments for immune-suppressed conditions are also available. Adjuvants, substances known to elicit a strong inflammatory response when injected, are the simplest of these [34]. Used in vaccines to promote a robust response to pathogens, adjuvants are powerful tools that allow for the development of robust immunity [35]. For this reason, they have also been employed in immune-suppressed cancers to engage the immune system with mixed results [36]. Immunotherapies, which broadly enhance the immune response, have shown success in various conditions, including diabetes, allergies, and cancer [37,38,39]. For allergies, immunotherapies show great promise, with symptom improvements typically observed after 2-4 months and complete cycles of treatment taking 3-5 years [38]. In cancers, however, immunotherapies have had more mixed results, with some cancers responding well to the treatment and others showing limited or no response [39]. Table 1 represents the existing treatments for inflammation, along with their advantages and adverse effects.
2. Nanoparticles for Immune Applications
The deliberate and precise engineering of nanoparticles enables the customization of their structural and functional attributes, making them highly suitable for specific biomedical applications. Nanoparticles, due to their nanoscale dimensions, possess unique physicochemical properties that make them promising candidates for addressing diseases modulated by the immune system. In scenarios where conventional therapeutic approaches prove inadequate or produce undesirable side effects, nanoparticles offer compelling alternatives, particularly for both pro- and anti-inflammatory interventions. Different types of nanoparticles, due to their modular and tunable design, can be tailored for distinct therapeutic roles, thereby enhancing treatment precision and minimizing systemic toxicity. Although the development of immune-targeted nanotherapeutics is relatively nascent, a rapidly growing body of research supports their significant potential in clinical immunomodulation [40]. A foundational application of nanoparticles lies in their role as drug delivery systems. Numerous pharmacological agents are currently available for treating immune-related disorders; however, their clinical use is frequently limited by challenges such as low bioavailability, systemic toxicity, and off-target effects. Nanoparticles offer a platform for overcoming these limitations by enabling controlled release, targeted delivery, and protection of drug payloads from premature degradation [41]. Nanocarriers are broadly categorized into polymeric, inorganic, and lipid-based systems, each offering unique advantages and subtypes optimized for specific therapeutic contexts [42]. The role of nanoparticles and their immune applications are represented in Figure 2.
Nanoparticle drug carriers can be formulated based on different components of the material used (Figure 2A). Polymeric nanoparticles, particularly nanocapsules, are widely utilized due to their structural flexibility. Composed of a biodegradable polymer shell surrounding a central cavity, nanocapsules can encapsulate both hydrophilic and hydrophobic drugs. Their synthesis enables the fine-tuning of properties such as size, charge, and responsiveness to local stimuli, which supports site-specific release and reduced systemic off-targeting [43]. Inorganic nanoparticles, especially mesoporous silica nanoparticles, are favored for their high surface area-to-volume (S/V) ratios, ease of synthesis (e.g., via the Stöber method), and capacity to load and slowly release therapeutic molecules [44,45]. Surface modifications, such as polyethylene glycol (PEG) coatings, can be employed to extend circulation time and evade immune detection, further enhancing therapeutic outcomes [46]. Additionally, lipid-based nanoparticles, particularly liposomes, offer a biocompatible and biomimetic alternative to synthetic systems [47]. Structurally analogous to biological membranes, liposomes can encapsulate diverse payloads within their phospholipid bilayers [48]. Modified with targeting ligands or membrane-anchored adjuvants, liposomes can facilitate selective tissue targeting and extended systemic retention [49]. Their resemblance to endogenous extracellular vesicles minimizes immune clearance and enhances delivery to specific pathological sites, including tumors and inflamed tissues [50,51].
In addition to their efficacy as drug carriers, nanoparticles also hold intrinsic therapeutic potential beyond simple cargo transport. Their physicochemical properties can be harnessed to produce direct therapeutic effects. Treatments such as magnetic hyperthermia and photothermal therapy exemplify this concept (Figure 2B) [52]. Magnetic hyperthermia involves the administration of superparamagnetic nanoparticles to pathological sites, followed by exposure to alternating magnetic fields, which induces localized heating [53]. This thermal effect can destroy pathological tissues such as tumors or bacterial biofilms without affecting adjacent healthy structures [52,54]. Photothermal therapy employs photoactive nanoparticles that generate heat upon exposure to specific wavelengths of light, typically in the near-infrared range [55]. Both modalities not only exert direct cytotoxic effects via thermal ablation but also promote immunogenic cell death [56,57]. The resulting release of intracellular contents into the extracellular space stimulates innate immune responses, thereby converting immunologically ‘cold’ environments, such as certain tumors, into immunologically ‘hot’ sites that are more amenable to immune surveillance and clearance.
Beyond these modalities, certain nanoparticles, particularly lipid-based systems, can also act as direct immunostimulants. These particles can incorporate immunological components such as adjuvants and antigens within their structure or on their surface, thereby mimicking the behavior of natural pathogens or vesicles (Figure 2C) [58,59]. This allows them to stimulate the immune system in a manner that closely resembles physiological immune activation. One notable application is in the formulation of mRNA vaccines, such as those developed for COVID-19 by Pfizer and Moderna. These lipid nanoparticles encapsulate mRNA sequences that encode specific antigens. Upon cellular uptake, the mRNA is translated into protein antigens that elicit both innate and adaptive immune responses [60]. This approach has demonstrated exceptional efficacy and has revolutionized vaccine development by reducing dependence on attenuated or inactivated pathogens, which carry inherent safety risks [61,62].
A particularly innovative application of nanoparticles in immune modulation involves nanozymes—nanoscale structures that mimic enzymatic functions (Figure 2D) [63]. These artificial enzymes can catalyze biochemical reactions relevant to both diagnostics and therapy. In diagnostics, nanozymes are used in biosensors for rapid, point-of-care detection of disease biomarkers. For instance, cholesterol assays may utilize nanozymes that catalyze the formation of hydrogen peroxide, which can be easily detected [64]. In therapeutic contexts, nanozymes are particularly valued for their ability to scavenge reactive oxygen species (ROS), making them potent agents in the treatment of inflammation-driven diseases [65]. Materials such as cerium oxide nanoparticles (nanoceria) can mimic the activity of key antioxidant enzymes like superoxide dismutase, catalase, and peroxidase, neutralizing oxidative stress in pathological conditions such as neurodegenerative disorders (e.g., Alzheimer’s and Parkinson’s disease), autoimmune diseases like rheumatoid arthritis, and ischemic injuries including stroke and myocardial infarction [66,67,68,69]. Additionally, nanozymes such as Prussian blue nanoparticles and iron oxide nanozymes have been employed to reduce inflammation and oxidative stress in the tumor microenvironment during photothermal or radiation therapies [70,71]. By alleviating hypoxia and mitigating oxidative damage, nanozymes enhance the therapeutic response and improve overall patient outcomes. A list of nanoparticles with their role in immunomodulatory performances is provided in Table 2.
3. Nanoceria as Potential Nanomedicine
Cerium, which holds the atomic number 58 on the periodic table, is a lanthanide and a rare earth metal characterized by its light grey, soft, and highly reactive nature in its pure solid form [92]. It commonly forms two types of oxides: CeO2, where cerium is in the +4 oxidation state, and Ce2O3, with cerium in the +3 state. These cerium oxides have distinct appearances and properties; CeO2 appears almost white or pale yellow, while Ce2O3 exhibits a richer yellow-gold [93]. Among these, CeO2 is more prevalent and interestingly contains some Ce3+ ions, which enhance its catalytic properties [94]. Nanoscale cerium oxide (nanoceria) has gained attention for its medical applications due to its unique ability to switch between Ce3+ and Ce4+ on its surface, conferring enzyme-like antioxidant activity and the capacity to neutralize reactive oxygen species (ROS), thereby offering long-lasting anti-inflammatory effects [95]. In nanoparticle form, cerium oxide surfaces display a mixture of Ce3+ and Ce4+ ions. As the particle size decreases, the number of surface oxygen vacancies and Ce3+ ions increases; this occurs because, to compensate for surface oxygen loss, two cerium ions transition from Ce4+ to Ce3+ [96,97]. The oxygen vacancies, also known as “catalytic hot spots”, exhibit a size-dependent increase, with smaller nanoparticles tending to have a higher Ce3+ content [66,98].
The Ce3+ ions play a significant role in conferring reactive oxygen species (ROS) scavenging capabilities and other enzyme-like functions, making nanoceria effective antioxidants [94]. In addition to redox switching and oxygen vacancies in nanoceria, further scientific investigations are underway to elucidate their antioxidant activity. For instance, research by Celardo et al. demonstrated that modifying the redox state without affecting oxygen vacancies, such as doping with samarium, significantly reduced the antioxidant performance of nanoceria [99]. More recent studies by Wang et al. suggest that the antioxidant properties of nanoceria are linked to transient surface defect states (TSDSs) found in the electronic band structure of short-lived intermediate species [100]. Besides mimicking enzymes like superoxide dismutase (SOD) and catalase, nanoceria also utilizes non-catalytic chemical reduction pathways to neutralize superoxide ions and hydrogen peroxide, acting as reducing agents rather than catalysts [100]. This multifaceted mechanism underpins the extensive range of biomedical applications for nanoceria.
3.1. Uptake and Localization of Nanoceria
Understanding how nanoceria is absorbed and distributed within biological systems is essential, as these particles play significant roles in applications like drug delivery, imaging, and cancer treatment. The physical characteristics of nanoparticles, including size, shape, and surface features, strongly influence their cellular uptake [101]. It has been found that nanoparticles smaller than 70 nm enter cells more swiftly, with those under 10 nm being particularly effective for targeted drug delivery [41]. Surface modification with PEG or targeting ligands can enhance uptake efficiency, prevent particle aggregation, and extend blood circulations [46,102]. Factors such as surface coating, size, electrolyte levels, and environmental pH greatly affect nanoparticle aggregation in biological fluids and overall systemic targeting efficiency.
Nanoparticles can cross cellular membranes through active or passive means. While lipid-based nanoparticles may enter cells via passive diffusion involving lipid interactions with the membrane [60], most nanoparticle uptake involves energy-dependent processes. This active uptake involves invaginations of the plasma membrane, forming vesicles through endocytosis or phagocytosis. The endocytic internalization pathways are diverse, including clathrin-mediated, caveolin-mediated, and other types of endocytosis, as well as micropinocytosis [103]. Tracking these uptake processes often relies on labeling nanoparticles with fluorescent dyes or radioactive tags, since nanoceria doesn’t possess an intrinsic fluorescence [104,105].
Self et al. demonstrated that fluorescently labeled nanoceria, with an average size of 3-5 nm, can localize in mitochondria, lysosomes, and the endoplasmic reticulum. The nanoceria were conjugated with CruzFluor fluorophores and shortly after exposure to HaCat cells, fluorescence microscopy imaging revealed that the cells internalized the particles faster than adherent ones (Figure 3A,B). The uptake occurs mainly through clathrin-mediated endocytosis and involves localization within the cytoplasm, with no observed toxicity at imaging concentrations [103]. In another study, Nadezda et al. used nanoceria conjugated with rhodamine B (~10 nm) as a sensor for ROS and as an antioxidant in human cell lines (Figure 3C) [104]. The NPs showed enhanced fluorescence in the cytoplasm, indicating its ability to stain cytoplasm rather than mitochondria (Figure 3D,E). These dye-tagged particles demonstrated antioxidant activity and successfully detected oxidative stress via fluorescence, underscoring their potential as multifunctional probes combining therapy and diagnostics (Figure 3F).
3.2. Factors Affecting Different Activities of Nanoceria
The catalytic efficiency and functional roles of nanomaterials are strongly influenced by their physical and chemical properties, including dimensions, morphology, and surface composition. In a study conducted by Lord et al., nanoceria were synthesized in sizes ranging from 3 to 94 nanometers to assess their capability to neutralize ROS in human monocytes and macrophages [106]. The findings indicated that robust antioxidant activity appeared to be independent of both particle size and oxygen vacancy concentration. Complementing this, Vassie and coworkers explored how the particle size of nanoceria affected cellular uptake, internalization, and ROS scavenging in cancer cells, concluding that larger particles (~94 nm) had enhanced ROS-neutralizing performance [107]. They also uncovered that nanoceria enter cells through energy-dependent mechanisms involving clathrin-mediated endocytosis, caveolae, and other non-specific routes.
Lee and colleagues examined ultrasmall nanoceria (~4 nm) and noted their potent antioxidant capabilities, which were further modulated by the thickness of polymer coatings [108]. Thinner coatings promoted more rapid interaction between Ce3+ ions and hydrogen peroxide. Meanwhile, Patil’s group analyzed the impact of surface charge on protein binding and cellular uptake, revealing that positively charged nanoparticles had a higher affinity for protein adsorption, whereas negatively charged ones demonstrated more efficient entry into A549 cells [109]. In related work, Celardo demonstrated that nanoceria can mitigate apoptosis triggered by various toxic agents in a dose-responsive manner, with protective effects closely tied to the presence of Ce3+ ions and their ROS-scavenging function [99]. Research by Asati et al. emphasized that negatively charged nanoceria were preferentially internalized by cancer cells and that their cytotoxic impact was enhanced when the particles accumulated in lysosomes instead of remaining in the cytosol [110].
Further insights into the activity of nanoceria revealed that enzyme-mimetic behavior depends on their surface crystal facets. Yang et al. synthesized nanocubes and nanorods with consistent Ce3+/Ce4+ ratios and oxygen vacancy levels but differing exposed facets; nanocubes with 100 surfaces exhibited greater peroxidase-mimicking activity, while nanorods with 110 facets showed stronger superoxide dismutase (SOD)-like activity [111]. Additionally, Gubernatorova’s team explored the potential of enhancing cerium oxide antioxidant properties through doping. Incorporating europium (Eu) into the cerium oxide structure increased oxygen vacancy levels leading to improved ROS mitigation, particularly in a model of intestinal injury caused by ischemia-reperfusion [112].
3.3. Enzyme-Mimetic Properties of Nanoceria
X-ray photoelectron spectroscopy (XPS), Fourier-transform infrared spectroscopy (FTIR), and ultraviolet-visible (UV–Vis) analyses demonstrated that treating nanoceria with hydrogen peroxide (H2O2) reduces the proportion of Ce3+ relative to Ce4+ ions and indicates the formation of peroxyl groups on the nanoparticle surface [68,113,114]. The primary mechanism for neutralizing reactive oxygen species (ROS) by nanoceria relies on redox reactions and oxygen exchange occurring at their surface. The simultaneous presence of Ce3+ and Ce4+ allows these nanoparticles to catalytically interact with superoxide anions (O2−) and H2O2 by oxidizing Ce3+ and reducing Ce4+ [115,116], thereby scavenging a wide array of ROS types [117,118].
While much research has focused on the ROS-scavenging capabilities of nanoceria, particularly their reactivity toward hydrogen peroxide, studies quantifying oxygen transport and specific ROS species in biological contexts remain limited. Evidence shows that exposure to H2O2 leads to the oxidation of surface Ce3+ ions into Ce4+ and the generation of superoxide (O2−) complexes on the nanoparticle surface, as verified by FTIR and XPS data [93]. Changes in the XPS spectra after H2O2 treatment confirm the dynamic redox behavior [68]. Furthermore, the detection of O22− stretching vibrations at 852 cm−1 in FTIR spectra after H2O2 exposure supports the hypothesis of superoxide adsorption onto the surface of nanoceria, highlighting a surface-bound mechanism of ROS interaction. The catalytic behavior of nanoceria is largely governed by the dynamic redox cycling between Ce³⁺ and Ce⁴⁺ ions. This reversible redox interplay acts like a seesaw, enabling fine-tuning of their enzyme-mimicking activities. Typically, nanoceria exhibits four major types of enzyme-like functions: superoxide dismutase (SOD)-like, catalase (CAT)-like, oxidase (OXD)-like, and peroxidase (POD)-like activities. A general schematic for the enzyme-mimetic properties of nanoceria is represented in Scheme 1A.
3.3.1. SOD-like Activity
Superoxide dismutase (SOD) is a key antioxidant enzyme that converts harmful superoxide radicals (O₂•⁻) into oxygen and hydrogen peroxide (H₂O₂). Despite its biological importance, natural SOD has clinical limitations due to high production costs and short half-life. Interestingly, nanoceria exhibit SOD-like activity, largely attributed to the redox cycling between Ce³⁺ and Ce⁴⁺ ions. Caputo et al. proposed that this redox switch enables nanoceria to mimic SOD by facilitating electron transfer. However, the slower transfer from Ce³⁺ to O₂•⁻ appears to limit the reaction rate, meaning higher Ce³⁺ content improves efficiency [119] (Scheme 1B,C). Heckert et al. confirmed via EPR that SOD-like activity increases with the Ce³⁺/Ce⁴⁺ ratio, which can be tuned by reducing nanoparticle size [120]. Baldim’s research further demonstrated that smaller nanoceria (4.5–28 nm) with higher Ce³⁺ content showed enhanced catalytic behavior following a Langmuir isotherm [121].
Doping nanoceria with low-valence ions, such as europium, boosts oxygen vacancies and Ce³⁺ levels, further enhancing enzymatic activity and enabling fluorescence-based biosensing [122]. Mechanistically, nanoceria either follow a dismutation pathway or an oxygen vacancy-mediated process where superoxide is adsorbed, and Ce(III) transfers electrons, generating H₂O₂. In turn, H₂O₂ participates in the redox cycling of Ce ions, allowing continuous superoxide scavenging. Although current evidence supports the positive role of Ce³⁺ in SOD-like activity, the detailed redox interactions with H₂O₂ remain poorly understood and warrant further experimental and theoretical investigation.
3.3.2. CAT-like Activity
Nanoceria exhibits catalase-like activity by breaking down H₂O₂ into water and oxygen, helping to reduce oxidative stress. This activity is influenced by the Ce⁴⁺/Ce³⁺ ratio, with higher Ce⁴⁺ levels generally enhancing the catalytic function. Studies suggest that Ce⁴⁺ plays a crucial role in electron transfer during H₂O₂ decomposition, potentially making it the rate-limiting step in the reaction [116] (Scheme 1D). Although further studies are needed to clarify this mechanism, experimental data show that CeO₂ with high Ce⁴⁺ content performs more effectively in biological environments than CeO₂ rich in Ce³⁺ [123]. For instance, in liver cells where natural catalase is inhibited, nanoceria significantly lowered H₂O₂ levels, indicating their therapeutic promise [123,124]. The accepted model for catalysis involves a two-step redox process between Ce⁴⁺ and Ce³⁺ during H₂O₂ interaction [125]. However, some studies challenge this by suggesting the reaction may not rely on localized Ce³⁺ but instead involve broader electron delocalization [100]. The dynamic behavior of oxygen vacancies further complicates pinpointing the exact reaction sites. Given these complexities, more in-depth mechanistic studies are essential to optimize enzymatic nanoceria for biomedical applications.
3.3.3. OXD-like Activity
Oxidase (OXD) enzymes play a vital role in human physiology by catalyzing the oxidation of substrates, including amino acids, amines, and alcohols, using molecular oxygen. This process produces hydrogen peroxide or water, and sometimes superoxide radicals, often accompanied by a visible color change, making OXD enzymes useful for biosensing applications. Despite their importance, reports of nanomaterials with strong oxidase-like activity remain limited. Nanoceria exhibit enzyme-like behaviors due to their unique redox “seesaw” mechanism, which is influenced by their size, shape, and surface chemistry (Scheme 1A). While nanoceria typically shows SOD and CAT activities depending on its Ce³⁺/Ce⁴⁺ ratio, studies have demonstrated that modifications like dextran or poly(acrylic acid) coatings enhance its OXD-like activity, especially under acidic conditions [126,127]. For example, acidic pH improves the ability of nanoceria to fully oxidize ampliflu, unlike the partial oxidation observed at neutral pH. Fluoride capping further boosts this activity by enhancing substrate binding, preventing product inhibition, and promoting electron transfer [128]. Mechanistic studies show that under acidic conditions, nanoceria adsorbs oxygen, facilitating its reduction to superoxide (O₂•–), which is subsequently converted to H₂O₂ and ultimately to hydroxyl radicals via a Fenton-like reaction. This explains the strong oxidase activity of nanoceria in acidic environments. Leveraging this, researchers have developed sensitive cancer biomarker detection methods by nanoceria, demonstrating their promise for diagnostics in clinical and point-of-care settings [126,129].
3.3.4. POD-like Activity
Peroxidases (PODs) are crucial enzymes in the antioxidant defense system, catalyzing the oxidation of various substrates using hydrogen peroxide as an oxidizing agent. This diverse group includes enzymes like glutathione peroxidase, which mitigates oxidative stress by neutralizing intracellular ROS, and myeloperoxidase, known for its role in immune defense against pathogens. Horseradish peroxidase (HRP) is widely employed in clinical diagnostics due to its ability to catalyze chromogenic reactions with specific substrates. Recently, increasing attention has been directed toward inorganic nanomaterials that emulate peroxidase activity. Nanoceria and their composites have shown significant promise [113,130,131,132]. For instance, Mn(II)/Ce composites have enabled the sensitive detection of hydrogen peroxide and glucose [133], while Ce-SrMOF-based sensors have been developed for assessing antioxidant levels in the saliva of lung cancer patients [134]. These advances highlight the need to understand better the mechanisms underlying their catalytic function.
Despite both utilizing H₂O₂, catalase and peroxidase differ mechanistically: catalase promotes H₂O₂ disproportionation into water and oxygen, whereas ceria-based peroxidase mimics decompose H₂O₂ into reactive radicals like hydroxyl and superoxide species, which then oxidize target substrates (Scheme 1E). Research by Heckert et al. revealed that Ce³⁺ surface sites play a vital role in H₂O₂ adsorption and radical generation during these reactions [135]. Furthermore, the enzyme-like activity of nanoceria correlates with its Ce³⁺ content and acidic conditions, enhancing hydroxyl radical production as evidenced by DNA relaxation assays. Building on this, Liu and colleagues developed porphyrin-modified ceria nanorods with superior POD-mimetic properties [66]. Their study demonstrated that porphyrin facilitated electron transfer to nanoceria under light activation, reducing recombination losses and enhancing the formation of reactive oxygen species. This synergistic approach opens new pathways for developing highly efficient nanozymes.
4. Biomedical Application for Nanoceria
Nanoceria exhibits a wide range of biomedical uses, including roles in antioxidant therapy [136,137], cancer treatment [138], antimicrobial action [139,140], as well as in drug and gene delivery [141], biosensing [142,143], medical imaging [144], and controlling inflammation [66,145]. Their favorable biocompatibility and selective cytotoxicity in diseased cells make them highly attractive for clinical use. Moreover, these nanoparticles have shown considerable potential in promoting wound repair [146,147] and tissue regeneration [148], primarily through their regulation of oxidative stress and inflammatory responses. In this review, we highlight the state of the art in using nanoceria for various biomedical applications related to their antioxidant and anti-inflammatory properties.
4.1. Nanoceria for Antiinflammation Applications
Nanoceria has emerged as a promising alternative to traditional non-steroidal anti-inflammatory drugs (NSAIDs). While conventional agents such as ibuprofen, naproxen, and corticosteroids are widely used to manage both acute and chronic inflammatory conditions, including minor injuries and severe diseases like asthma, they are often limited by significant side effects [22]. In contrast, nanoceria offers several therapeutic benefits, including selective localization at inflammation sites, redox-based catalytic activity, and prolonged retention in affected tissues [68,146]. Importantly, research suggests that nanoceria induces minimal toxicity, enhancing its appeal as a safer option. Its efficacy is particularly notable in addressing chronic inflammation, which can persist for extended periods and lead to tissue damage due to unresolved immune signaling. Unlike acute inflammation, chronic conditions often persist without resolution, causing a range of diverse symptoms that depend on the affected tissue. As existing treatments struggle to address long-term inflammatory diseases, nanoceria represents a compelling avenue for future therapeutic development. Nanoceria has shown significant potential in controlling inflammation across various disease conditions by lowering the levels of ROS. Its strong anti-inflammatory action stems from its ability to neutralize free radicals effectively. Additionally, nanoceria exerts its therapeutic effects by influencing key inflammatory pathways, including the suppression of NF-κB, IL-6, and IL-8, while also enhancing the expression of antioxidant enzymes like superoxide dismutase and catalase [149,150].
Rheumatoid Arthritis (RA) is a chronic autoimmune disorder which is characterized by persistent inflammation and ROS generation. Nanoceria has the potential for pain relief and ROS reduction in rheumatoid arthritis. In a recent study, Zhang et al. prepared silver-modified ceria nanoparticles loaded with celastrol (Ag-CeNP@Cel) for the treatment of RA [151]. The nanoformulation enhanced the water solubility of the drug celastrol, and synergistically scavenged excess ROS, thereby reprogramming M1 macrophages into M2 macrophages. These particles thereby mitigated inflammatory responses and improved the rheumatoid arthritis microenvironment. The nanoparticles were also conjugated with cyanine dye for diagnostic purposes and administered in adjuvant-induced arthritis mouse models. Results in these model organisms showed four times higher fluorescence in the inflamed legs as compared to the non-inflamed legs of normal mice.
From our group, Kalashnikova et al. showed that RA could be effectively treated using inflammation-targeting albumin-nanoceria. Small, crystalline nanoceria, rich in Ce3+, is fabricated onto albumin via a biomineralization process (Figure 4A) [68]. Albumin is a common blood protein that accumulates in sites of inflammation and offers nanoceria with excellent stability, non-toxicity, and safety for biological applications. Collagen-induced arthritis model mice treated with nanoceria showed reduced inflammation in the paws of the nanoceria-treated mice as compared to mice treated with PBS. Interestingly, the performance of the albumin-nanoceria was comparable to that of Methotrexate, a common anti-inflammatory drug (Figure 4B). Immunofluorescence staining studies showed that both PBS-treated and nanoceria-treated mice had high levels of macrophages (M0), as indicated by the presence of CD11b. Tissues from nanoceria-treated mice exhibited higher levels of Arg-1, an anti-inflammatory M2 marker, and lower levels of iNOS, a pro-inflammatory M1 marker (Figure 4C). Notably, the in vitro studies conducted in this study provide insight into the mechanism by which albumin-nanoceria treats RA. Flow cytometry performed on Raw264.7 macrophages and THP-1 monocytes reveals an immunomodulatory effect of the particles, allowing cells to transition from a pro-inflammatory to an anti-inflammatory phenotype (Figure 4D). This result highlights nanoceria being an effective, long-term anti-inflammatory drug in this condition. Xia et al. used manganese-doped nanoceria for RA [152]. Here, manganese enhances ROS scavenging while acting as a nanocarrier for the drug Methotrexate. To improve the targeting and delivery of the drug, the NPs were coated with BSA and dissolved in hyaluronic acid-based microneedles (Figure 4E). Flow cytometry analysis revealed that nanoparticles at a concentration of 25 µg/mL exhibited notable ROS scavenging capacity. A dose-dependent reduction in reactive oxygen species (ROS) levels was observed in macrophages, indicating the nanoparticles’ effectiveness in suppressing ROS generation. Additionally, measurements of immunofluorescence intensity further supported the ability of the nanoparticles to efficiently eliminate intracellular ROS.
RA is characterized by synovial inflammation, primarily driven by pro-inflammatory M1 macrophages [153]. Therapeutic strategies that reduce M1 and promote anti-inflammatory M2 macrophages are crucial. Hypoxia and elevated ROS in the RA synovium contribute to this M1/M2 imbalance. To address this, manganese ferrite–ceria nanoparticle-anchored mesoporous silica nanoparticles (MFC-MSNs) have been developed by Kim et al. [154]. These hybrid nanoplatforms synergistically scavenge ROS and generate oxygen, promoting macrophage polarization from M1 to M2 phenotypes. This is achieved through ceria nanoparticles neutralizing hydroxyl radicals produced by manganese ferrite during the Fenton-like reaction. In vitro and in vivo studies confirmed effective immune modulation, with intra-articular injection of MFC-MSNs in RA rat models alleviating joint hypoxia, inflammation, and damage. Additionally, methotrexate was loaded into MSNs for sustained release, further enhancing therapeutic outcomes. This multifunctional nanotherapeutic shows promise for RA by targeting oxidative stress and immune dysregulation simultaneously. Lin et al. showed that R-dihydrolipoic-acid stabilized cerium-modified gold nanoclusters (~3.4 nm) hold promise for treating advanced-stage RA [155]. In collagen-induced arthritis rat models, these nanoclusters normalized cytokine levels by modulating B cell activity within 24 hours and suppressed B cell memory responses. Notably, these NPs outperformed standard RA drugs like methotrexate and etanercept in reversing disease progression.
Chronic pancreatitis, though less frequently discussed, is a devastating and life-threatening condition characterized by irreversible pancreatic damage, excessive extracellular matrix (ECM) deposition, and impaired pancreatic function. A major complication of this chronic disease is pancreatic cancer, and individuals affected by chronic pancreatitis typically experience a significantly reduced lifespan. Currently, there are no curative treatments available; therapies merely aim to slow disease progression without halting or reversing it. However, promising research by Godgu and colleagues demonstrates that nanoceria may offer a novel therapeutic approach [156]. In their study, ~100 nm nanoceria particles were synthesized and administered to animal models of chronic pancreatitis. The treatment significantly reduced inflammation by lowering levels of key inflammatory markers, such as NF-κB, and inhibited pro-fibrotic signaling pathways. Notably, nanoceria treatment led to reduced ECM accumulation and endoplasmic reticulum (ER) stress. These results indicate that nanoceria not only alleviates inflammation but may also substantially slow or even halt disease progression. This groundbreaking approach holds great potential as a transformative therapy for chronic, irreversible pancreatic disorders, offering patients improved outcomes and enhanced quality of life. In a separate study, Luo and colleagues demonstrated that utilizing a combination of calcium-binding agents and cerium-based nanozymes carrying catalase effectively reduced excessive ROS and alleviated mitochondrial damage, resulting in comprehensive anti-inflammatory benefits [157]. This nanotherapeutic system also helped restore disrupted autophagic processes and reduced endoplasmic reticulum stress in the pancreas, aiding the recovery of damaged acinar cells. On a mechanistic level, treatment with the nanoplatform corrected metabolic disruptions within pancreatic tissue and suppressed key inflammatory signaling pathways involved in the progression of pancreatic inflammation.
4.2. Nanoceria for Immunotherapy Applications
Nanoceria has been explored in specific immunotherapy applications, primarily as an immunomodulatory nanodrug [68]. One could argue that the treatment of rheumatoid arthritis with nanoceria and its associated modulation of macrophages from an M1 pro-inflammatory to an M2 anti-inflammatory phenotype constitutes a form of immunotherapy; however, in these applications, it is not being utilized to its full potential to affect the entire immune environment. Other populations of cells can be activated or deactivated, including T cells, B cells, and NK cells. Early evidence supports the claim that nanoceria can be used to modulate these cell populations, in addition to macrophages and monocytes. For diseases with complex immune phenotypes, such as endometriosis and cancer, this makes nanoceria an attractive option for treatment [105,158]. To thoroughly examine the use of nanoceria as an immunotherapy, applications of nanoceria beyond the simple tuning of macrophages must be explored and characterized.
Generally, tumors are remarkably difficult to treat due to the complex nature of tumor microenvironment (TME). Tumors often have hypoxic cores with a lack of useable oxygen, which inhibits immune activity and prevents effective treatment [159]. Unfortunately, tumors are also known to have highly metabolically active exteriors with anti-inflammatory tumor-associated macrophages preventing an appropriate pro-inflammatory response to abnormal tumor cells [15,160]. Paradoxically, it has been shown that nanoceria can both be used to relieve tumor hypoxia by scavenging ROS and be used to generate ROS in tumor environments. This is due to the pH-responsive behavior of nanoceria, which allows for the scavenging of ROS in neutral or basic environments as commonly reported, and the generation of ROS in acidic environments like those found in tumors as demonstrated by Wang et al. [161]. These smart NPs show a 3-in-1 action, pH responsiveness, controlled release of doxorubicin, and TME-responsive combination therapy. Glycol Chitosan-coated nanoceria were loaded with doxorubicin, and for target specificity CXCR4 antagonist (AMD11070) on nanoceria. Blocking CXCR4 allows reducing the crosstalk between TME and tumor cells, which leads to the inhibition of tumor metastasis. The study showed, under acidic pH conditions, tumor cell apoptosis and reduced tumor growth in vitro in human retinoblastoma (Rb) cells and in vivo in mouse genetic RbLox/lox p107+/− p130−/− (p107s) and human xenograft Rb models. Nanoceria has a dual effect both protecting normal tissues from oxidative stress and unnecessary inflammation while triggering a much-needed inflammatory cascade in immune-suppressed cancers. As the hypoxic core of tumors does not have the same molecular environment as the acidic exterior, nanoceria instead restores oxygen to the area, allowing for greater efficacy of cancer therapies. Though research in nanoceria as an immunotherapy is still nascent, the particles hold enormous potential in a variety of immune modulated disease states beyond typical inflammatory conditions.
Fernández-Varo et al. demonstrated that 4–5 nm nanoceria, synthesized via co-precipitation, exert strong antioxidant and anti-inflammatory effects in Wistar rats with hepatocellular carcinoma [162]. Treatment improved survival by reducing macrophage infiltration and phosphorylated ERK1/2 levels, key components of the Ras/MAPK pathway. Nanoceria also helped restore disrupted fatty acid metabolism, which is crucial for cancer cell growth. In a breast tumor model, nanoceria reduced oxidative and inflammatory markers like MDA, MPO, and nitric oxide. While promising, further studies are needed to clarify how nanoceria regulates lipid metabolism in disease.
The therapeutic efficacy of nanoceria in cancer treatment has been explored across various preclinical models. In one study, Tian and colleagues demonstrated that intravenously delivered porous cerium oxide nanorods, synthesized using a hydrothermal technique, reduced tumor mass by 51.1% [163] (Figure 5A). This anti-tumor effect was further enhanced to 96.1% when the nanorods were coated with sodium polystyrene sulfonate (Figure 5B). Administration of nanoceria (~32 nm in size, carrying a surface charge of −26.3 mV intraperitoneally at a dose of 0.5 mg/kg to mice significantly inhibited the progression of WEHI164 tumors [164]. Additionally, a copper-doped version of nanoceria almost completely halted tumor growth, achieving 98.5% inhibition [165]. Reduced tumor cell proliferation was supported by the marked suppression of Ki67 expression in MDA-MB-231 tumors in mice [165] and hepatocellular carcinoma models in rats [162] after nanoceria treatment. Histological assessments using hematoxylin and eosin (H&E) staining indicated a greater presence of necrotic and apoptotic cells in treated tumor samples compared to controls (Figure 5C) [163]. Furthermore, TUNEL assays revealed extensive DNA fragmentation in nanoceria-treated tissues, highlighting increased levels of apoptosis (Figure 5C). Molecular analyses showed upregulation of pro-apoptotic genes such as Bax and caspase-3, alongside reduced expression of the anti-apoptotic gene Bcl-2. Elevated levels of reactive oxygen species (ROS), as indicated by dihydroethidium (DHE) staining, suggested that oxidative stress-induced apoptosis was a key mechanism of action (Figure 5C).
Nanoceria is also being evaluated as a non-steroidal anti-inflammatory drug for endometriosis theranostics. Endometriosis is a chronic inflammatory disease affecting approximately 10% of reproductive-aged women globally, characterized by the growth of endometrial-like tissue outside the uterus [166,167]. Studies have identified a strong link between oxidative stress (OS) and the development of endometriosis, with abnormal endometrial angiogenesis also playing a central role in the disease’s progression. In a notable study by Chaudhury et al., nanoceria were successfully employed to alleviate symptoms of endometriosis [168]. These nanoparticles, characterized by their dual oxidation states (Ce³⁺ and Ce⁴⁺), function as efficient scavengers of free radicals such as superoxide and hydrogen peroxide. When administered intraperitoneally at a single dose of 0.5 mg/kg in a murine model, nanoceria significantly reduced the formation of endometrial lesions. This therapeutic effect was attributed to a decrease in oxidative stress markers, including ROS, lipid peroxidation, and an improvement in total antioxidant capacity as well as suppressed angiogenesis, evidenced by lower levels of vascular endothelial growth factor and adrenomedullin. Compared to the commonly used antioxidant N-acetyl cysteine, administered at 250 mg/kg three times weekly for 15 days, nanoceria demonstrated superior outcomes. Additionally, the treatment helped improve oocyte quality, a key determinant of reproductive success in individuals with endometriosis.
Rahman and colleagues demonstrated the efficacy of nanoceria in the treatment of endometriosis, a disease characterized by complex immune interactions [158]. There are several differences between the immune profiles of healthy and diseased animals, including an increased prevalence of pro-inflammatory macrophages and T-cells as well as reduced NK cells and anti-inflammatory macrophages, which are present in endometrial lesions. Plausible treatments for endometriosis include common STAT and JAK inhibitors, which have been shown to reduce disease burden through limiting pro-inflammatory signaling. However, a major challenge present in the treatment of endometriosis is that lesions are phenotypically similar to normal uterine tissue. Unfortunately, the same inhibitors that are useful in reducing disease burden act on appropriate activation of STAT3 in the uterus, leading to many undesirable symptoms, including infertility [169]. For this reason, albumin-nanoceria was explored as a targeted STAT/JAK inhibitor and immunotherapy in endometriosis (Figure 5D). Nanoceria was able to have a distinct, targeted effect on endometrial lesions without affecting the uterus, as confirmed by fluorescence and photoacoustic signals from albumin-nanoceria conjugated with indocyanine green (ICG). These NPs enabled non-invasive detection of endometriosis lesions (Figure 5E). In model mice treated with albumin-nanoceria, there was a reduction in lesions comparable to the effect of the JAK inhibitor or Tofacitinib. The pSTAT3 (the activated form of STAT3) was reduced in the lesions of nanoceria-treated mice, and not only were M1 macrophages reduced and M2 macrophages increased, but T cells were reduced without an impact on NK cells. Fascinatingly, owing to its efficient targeting, nanoceria did not inhibit pregnancy in treated mice, whereas traditional therapeutics caused implantation failure (Figure 5F,G). These findings suggest that nanoceria can function as a STAT/JAK inhibitor, influencing the overall immune environment of lesions without compromising fertility, thereby positioning nanoceria as an excellent choice for treating endometriosis.
4.3. Theranostic Application of Nanoceria
Theranostic approaches in modern medicine offer a dual advantage by enabling simultaneous disease diagnosis and treatment through non-invasive imaging [170,171]. Nanoceria, especially when doped with gadolinium or surface-modified with targeting ligands, combine potent antioxidative therapeutic properties with enhanced diagnostic imaging capabilities, primarily magnetic resonance imaging (MRI) and computed tomography (CT) contrast enhancement [172,173,174]. Their size tunability, biocompatibility, ability to scavenge ROS, and targeting capability make them highly promising theranostic agents for personalized diagnosis, image-guided therapy, and monitoring of inflammatory and cancerous diseases. For instance, Wu et al. engineered Fe₃O₄/CeO₂ core-shell nanoparticles that serve both diagnostic and therapeutic functions [175] (Figure 6A,B). In this system, iron oxide provided MRI contrast, while the cerium oxide shell delivered ROS-scavenging therapeutic benefits (Figure 6C,D). This multifunctional design not only facilitated MRI tracking and biodistribution analysis of the nanoparticles but also demonstrated high cellular uptake, a favorable Ce³⁺/Ce⁴⁺ ratio, and minimal cytotoxicity. These features make them promising tools for managing ROS-associated inflammatory disorders, including cardiovascular diseases, atherosclerosis, rheumatoid arthritis, and allergies (Figure 6E,F). The potential for targeted therapy was also discussed, highlighting the possibility of functionalizing these nanoparticles with antibodies or peptides targeting specific inflammatory markers, such as VCAM-1 and neutrophil cytosolic factor 1. Additionally, another study described magnetite-CeO₂ nanoconjugates formed by interlinking iron oxide and nanoceria, coated with polyethyleneimine (PEI) and crosslinked using glutaraldehyde [176]. These 8 nm-sized particles exhibited enhanced antioxidant activity both in vitro and in vivo, possessing superparamagnetic properties and effectively neutralizing ROS. The combination of magnetic responsiveness and potent antioxidant activity positions these nanostructures as valuable candidates for advanced theranostic applications. In a similar study, Eriksson et al. showed that a 5 nm-sized nanoceria dopped with gadolinium showed excellent T1 relaxivity with ROS scavenging property. The bioluminescence study showed an inhibitory effect of ROS in vivo with a higher concentration of Ce3+ at the nanoparticle surfaces [173]. At the same time, Saidi et al. showed the use of nanoceria for CT application for in vivo tumor tracking and treatment [177]. To improve stability and contrasting properties, the nanoparticles (1-3 nm in size) were coated with hydrophilic and biocompatible poly(acrylic acid) (PAA) and poly(acrylic acid-co-maleic acid). The nanoparticles showed distinctive CT contrast signals in the bladder, and interestingly injection dose is ∼10 times less than those of standard iodine contrast agents (Figure 6G,H). A redox-active gadolinium-doped nanoceria was synthesized by Kolmanovich et al. [178]. Using polyelectrolyte, a layer-by-layer capsule was prepared and used for cellular uptake and MRI imaging for human osteosarcoma, adenocarcinoma cells, and normal human mesenchymal stem cells.
Johnson et al. prepared theranostic nanoceria conjugated with fluorescein isothiocyanate (FITC)-tagged epidermal growth factor receptor for the diagnosis and treatment of melanoma [179]. The theranostic potential of the nanoformulation was validated using both two-dimensional (2D) monolayer cultures and three-dimensional (3D) spheroid models derived from parental and metastatic melanoma cell lines. Confocal microscopy confirmed the diagnostic capability of the system through clear visualization of cellular uptake and distribution. To assess therapeutic efficacy, cell viability assays and ROS measurements were performed. In 2D models, a marked increase in overall cellular ROS was observed, while mitochondrial ROS remained largely unaffected. In contrast, the 3D melanoma spheroids exhibited a significant rise in both total and mitochondrial ROS levels, with metastatic spheroids showing a more pronounced response compared to the parental ones. These findings suggest that the nanoformulation is particularly effective against metastatic melanoma, highlighting its promise as a dual function theranostic agent.
4.4. Nanoceria for Tissue Engineering Applications
Due to its strong antioxidant capabilities, nanoceria plays a crucial role in promoting tissue repair by aiding stem cell growth and guiding their transformation into specific cell types. It also encourages the formation of new blood vessels, thereby accelerating the healing of damaged tissues. When integrated into biomaterials and scaffold structures, nanoceria helps create environments that closely resemble natural tissue, which supports tissue regeneration and minimizes immune system rejection. Owing to its dual antioxidant and anti-inflammatory effects, nanoceria has emerged as a promising multifunctional tool for regenerating both soft and hard tissues, including skin, bone, nerve, and heart tissue [180,181,182].
Tissue repair facilitated by biomaterials generally follows two primary pathways: one involves regenerative remodeling, where damaged tissue is replaced with functionally similar parenchymal cells, and the other leads to the formation of fibrous tissue, resulting in scar-like structures. These outcomes are largely influenced by factors such as the regenerative capacity of resident cells and the severity of tissue damage, as well as the structural integrity or degradation of the extracellular matrix (ECM) at the implantation site [148,183]. A critical component in enhancing cellular regeneration lies in designing scaffolds that can replicate biochemical cues essential for parenchymal cell growth and ECM synthesis. Within the realm of regenerative medicine, stem cells serve as key agents for tissue reconstruction, often in combination with scaffolds that support their differentiation and integration [180]. The regenerative potential of these scaffolds often hinges on how well they interact with stem or progenitor cells. In this context, research has focused on exploring both the cellular microenvironment and the specific responses elicited by nanoceria, as detailed in Table 3.
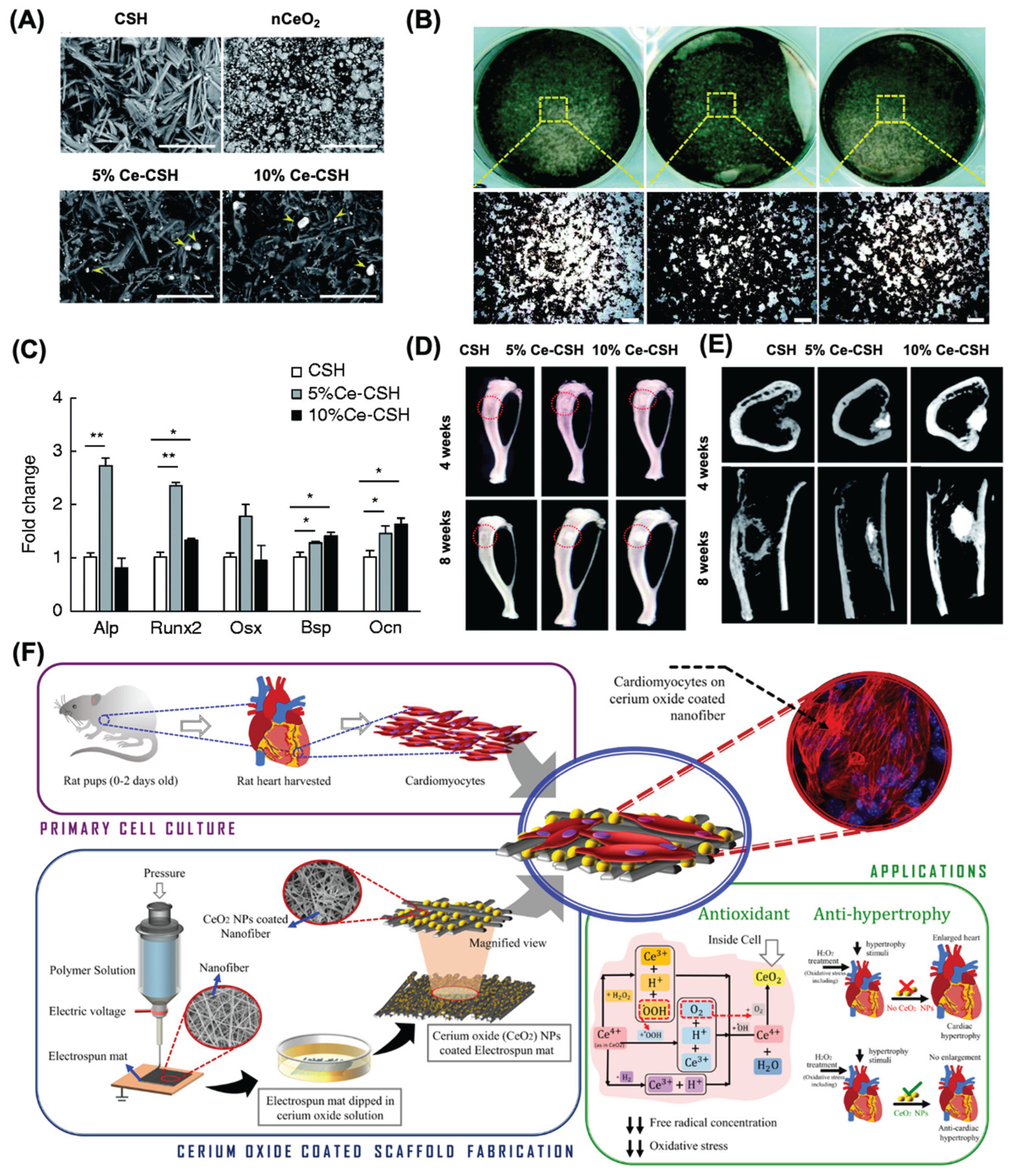
Numerous experimental studies have validated the therapeutic benefits of both pristine and surface-modified nanoceria in various biomedical applications. As a notable example, nanoceria doped with samarium and modified with polyethylene glycol (PEG) chains were shown to boost endothelial cell proliferation, activate key angiogenic signaling pathways such as p38 MAPK and HIF-1α, and stimulate blood vessel development in chick embryo models [184]. Furthermore, integrating nanoceria into polymer-based structures has emerged as a strategic approach for promoting wound closure and skin regeneration. In particular, 3D scaffolds embedded with nanoceria have demonstrated strong potential as biomimetic platforms for replacing injured dermal tissue [185,186]. The integration of nanoceria into α-calcium sulfate hemihydrate (α-CSH) at 5% and 10% concentrations were studied to develop a composite for bone repair (Figure 7A). Cell extracts from α-CSH and CeO₂/α-CSH composites were tested in vitro, revealing that the 5% CeO₂ composite notably enhanced cell proliferation, migration, and osteogenic gene expression in bone marrow stromal cells (Figure 7B,C). In vivo, critical bone defects in rats treated with the 5% CeO₂ composite showed improved bone regeneration, as evidenced by imaging (X-ray and micro-CT), mineral deposition at the bone interface, and increased osteocalcin expression (Figure 7D,E). Overall, the 5% CeO₂/α-CSH composite demonstrated superior osteogenic potential, suggesting its promise as a bone graft substitute [186].
Nanoceria has emerged as a promising candidate in treating cardiac conditions due to its antioxidant and anti-inflammatory actions. It shows potential in mitigating myocardial reperfusion injury by reducing elevated ROS levels and has demonstrated cardioprotective effects against oxidative damage. In CP-1 transgenic mice, intravenous delivery of 15 nmol nanoceria significantly curbed left ventricular dysfunction and dilation within two weeks [187]. Cardiac progenitor cells, essential for heart regeneration, require a controlled microenvironment for optimal growth. Nanoceria, due to its redox activity, can mitigate oxidative stress in cardiac progenitor cell cultures. Pagliari et al. found that exposure to nanoceria (5–50 μg/mL) for 24 hours did not impair CPC function and offered protection from H₂O₂-induced toxicity for up to a week [190]. The interplay between microRNAs and ROS plays a critical role in ischemia-reperfusion injury. A novel composite of silica-polydopamine/DNA/nanoceria was developed by Yang et al. to test in cell and animal models. Their findings confirmed a regulatory interaction between H₂O₂ and miR-21 via the PI3K/AKT pathway, offering new insights into oxidative stress signaling [194]. Additionally, nanoceria-loaded electrospun polycaprolactam PCL and PCL-gelatin nanofiber patches were designed as antioxidant cardiac scaffolds (Figure 7E) [195]. These patches supported various heart cells and helped prevent hypertrophy in cardiomyocytes by neutralizing ROS.

Table 3.
Application of various nanoceria formulations in tissue engineering scaffolds.
| Nano formulation | Role of nanoceria | Cell type | Tissue target | Tissue repiar | Outcome | Ref |
|---|---|---|---|---|---|---|
| Nanoceria-incorporated hydroxyapatite (HA) coatings | Additive to scaffold | Bone marrow stromal cells (BMSCs) | Bone | Constructive remodeling | Enhances cell viability and osteogenesis, restores antioxidant defenses and gene expression and inhibits apoptosis, osteoclastogenesis, and oxidative stress. | [188] |
| Cancellous bone containing poly-L-lactic acid and nanoceria | Additive to scaffold | Mesenchymal stem cells (MSCs) | Bone | Constructive remodeling | Improvement of cell proliferation ; Prevents apoptosis via calcium channel activation and HIF-1α stabilization |
[182] |
| Nanoceria |
Dispersion in medium | BMSCs Bone & adipose | Bone | Constructive remodeling | BMSC viability increased, while osteogenic and adipogenic differentiation were inhibited in a time- and dose-dependent manner | [189] |
| Nanoceria |
Dispersion in medium | Cardiac progenitor cells (CPCs) | Heart | Constructive remodeling |
No alteration of the cellular growth and differentiation; Protection of cells against oxidative insults | [190] |
| Citrate-stabilized nanoceria |
Dispersion in medium | Primary mouse embryonic fibroblasts | - | Constructive remodeling |
Enhanced proliferative activity of primary cells; Reduction of intracellular ROS during the lag phase of cell growth; Modulation of major antioxidant enzymes | [191] |
| Nanoceria |
Dispersion in medium | Human adipose derived-mesenchymal stem cells (hAd-MSCs) | Skin | Constructive remodeling | Improved tensile strength of acellular dermal matrices impregnated with nanoceria enhances hAd-MSC growth and survival, boosts free radical scavenging, and increases collagen content | [192] |
| Nanoceria & Samarium-doped nanoceria |
Dispersion in medium | Neural progenitor cells | Nerves | Constructive remodeling |
NPs enter cells and temporarily protect against oxidative stress. They hinder neuronal differentiation and disrupt the cytoskeleton, posing neurotoxicity risks. High collagen levels are observed. |
[193] |
Figure 7.
(A) scanning electron micrographs for fabricated α-calcium sulfate hemihydrate (CHS)-CeO2 nanocompoiste for bone tissue regeneration studies. (B) Quantitative analysis of mRNA levels for Alp, Runx2, Osx, Bsp, and Ocn in BMSCs after 7 days of incubation with extracts from various composite materials. Data represent triplicate samples per group (n = 3). (C) von Kossa staining results showing mineral deposition in BMSCs following 21 days of treatment with different composite extracts. Scale bar in the lower panel represents 1 mm. (D) X-ray images captured in the anteroposterior view at four- and eight-weeks following implantation, with the red circles indicating the site of the bone defect. (E) Micro-computed tomography (micro-CT) scans of the tibia at eight weeks after composite implantation. The top row displays cross-sectional (transverse) views, while the bottom row shows sagittal views of the tibial bone. (E) A schematic representation for the PCL-Gelatin-Ce nanofiber formation and its application for cardiovascular tissue engineering. Reproduced with permission from [186,195]. Copy Right, 2019, Sage Publishers and 2021, Elsevier.
Figure 7.
(A) scanning electron micrographs for fabricated α-calcium sulfate hemihydrate (CHS)-CeO2 nanocompoiste for bone tissue regeneration studies. (B) Quantitative analysis of mRNA levels for Alp, Runx2, Osx, Bsp, and Ocn in BMSCs after 7 days of incubation with extracts from various composite materials. Data represent triplicate samples per group (n = 3). (C) von Kossa staining results showing mineral deposition in BMSCs following 21 days of treatment with different composite extracts. Scale bar in the lower panel represents 1 mm. (D) X-ray images captured in the anteroposterior view at four- and eight-weeks following implantation, with the red circles indicating the site of the bone defect. (E) Micro-computed tomography (micro-CT) scans of the tibia at eight weeks after composite implantation. The top row displays cross-sectional (transverse) views, while the bottom row shows sagittal views of the tibial bone. (E) A schematic representation for the PCL-Gelatin-Ce nanofiber formation and its application for cardiovascular tissue engineering. Reproduced with permission from [186,195]. Copy Right, 2019, Sage Publishers and 2021, Elsevier.
4.5. Nanoceria for Wound Healing Applications
As the largest organ by surface area, the skin plays a critical role in safeguarding the body, making the rapid healing of topical wounds vital for restoring its protective function. Wound healing is a complex, staged process involving hemostasis, inflammation, proliferation, and remodeling [196]. During the inflammatory phase, various immune cells are recruited to secrete cytokines and chemokines that drive tissue repair. ROS, key signaling molecules in this phase, help eliminate pathogens and sustain the inflammatory response [197]. However, excessive or uncontrolled ROS production can prolong inflammation, leading to chronic, non-healing wounds. Nanoceria offers therapeutic potential by modulating ROS levels, thereby reducing oxidative stress and promoting the resolution of inflammation. Although they cannot penetrate intact skin, open wounds provide an ideal route for delivering nanoceria with high bioavailability [147,198].
Chigurupati et al. studied the use of bare nanoceria for wound healing applications [199]. Nanoceria, with an average size of 3-5 nm, were introduced to normal cutaneous wounds in mice. Nanoceria enhanced the in vitro proliferation and migration of keratinocytes, fibroblasts, and vascular endothelial cells. In vivo, topical application of these nanoparticles significantly reduced wound size in C57BL/6 mice compared to untreated controls. Histological analysis revealed an increased density of blood vessels and infiltration of mononuclear leukocytes, suggesting enhanced angiogenesis that may facilitate infection prevention and debris clearance: critical steps in the formation of new skin tissue. Additionally, the antioxidant properties of the nanoceria led to reduced lipid and protein oxidation at the wound site, as evidenced by lower levels of 4-hydroxynonenal and nitrotyrosine.
For topical and diabetic wound closure, nanoceria was mixed with various adhesives or incorporated into various hydrogel patches. This allows the slow release of nanoceria at the wound site and reduces their toxicity. Wu et al. prepared 5 nm-sized nanoceria and incorporated it into mesoporous silica nanoparticles (MSNs) for topical wound healing applications (Figure 8A) [200]. The nanocomposite showed ROS scavenging properties, accelerated wound closure, and reduced scar formation (Figure 8B). A higher expression of messenger ribonucleic acid (mRNA) levels of stearoyl-CoA desaturase 1, leucine-rich repeats and immunoglobulin-like domain 1, placenta-expressed transcript-1, and platelet-derived growth factor-α in Sprague–Dawley (SD) rats were observed after the administration of NPs. The combined action of nanoceria, functioning as a catalytic antioxidant, and MSNs serving as tissue adhesives, was further validated by a noticeable decrease in superoxide anion levels and reduced infiltration of CD68-positive macrophages at the wound site (Figure 8C,D).
In diabetic wounds, elevated glucose levels lead to protein glycation, triggering the release of proinflammatory cytokines and disrupting healing by increasing oxidative stress and altering the extracellular matrix. These chronic wounds are prone to infection, often requiring antibiotics and immune modulators. Nanoceria, with their catalytic antioxidant properties, help reduce inflammation and oxidative stress, promoting healing in both standard and diabetic chronic wounds. Wang et al. fabricated polymeric vesicles (PVs) for the incorporation of antibiotic ciprofloxacin (CIP) and nanoceria for the treatment of infected wounds in a streptozocin (STZ)-induced diabetic mouse model (Figure 8E) [201]. The study was based on the understanding that diabetic individuals often have diminished levels of SOD which controls oxidative stress. To address this, the researchers incorporated nanoceria, which possesses SOD-like properties, to promote more effective wound healing. To prepare the formulation, CIP-loaded PVs were incubated with cerium nitrate and sodium hydroxide, triggering the in-situ formation of nanoceria on the vesicle surface. These nanoparticles, approximately 4 nm in size, were embedded into the PVs, resulting in a hydrodynamic diameter of 539 nm. The nanoparticles exhibited SOD-mimicking activity and facilitated the sustained release of CIP. Notably, the surface of the nanoceria contained 40.4% Ce³⁺, which can be an added advantage for antioxidant properties. Topical application of the CIP–ceria–PV system to wounds infected with Staphylococcus aureus in diabetic mice markedly accelerated wound closure (Figure 8F). This therapeutic effect was attributed to a dual action: bacterial eradication by CIP and reduction of ROS levels through antioxidant activity of nanoceria. The combined effect led to full wound healing and re-epithelialization within 14 days, whereas untreated and control groups continued to exhibit unhealed, open wounds without new epidermal formation (Figure 8G).
Various hydrogel-based scaffolds embedded with nanoceria are used for various wound-healing applications. The hydrogel polymeric support will allow the slow release of nanoceria at the wound site. Hydrogels provide a 3D network structure which can provide moisture, promote cell migration, and provide the ideal architecture for cell growth and tissue engineering, while also promoting the antioxidant properties of nanoceria [202,203]. Augustine et al. fabricated ceria-loaded gelatin methacryloyl (GelMA) scaffolds to enhance the healing of diabetic wounds [204] (Figure 8G). This composite material showed inhibition of bacterial growth and enhancement of angiogenic activity, leading to an acceleration in the healing process of diabetic skin wounds in rats with a loading efficiency of 1% w/w cerium in Gelma. Similarly, in two independent studies, it was reported that cryogels loaded with microRNA-nanoceria showed enhanced cell proliferation and wound healing capability in diabetic wounds [205,206]. Nanoceria exhibit strong antioxidant capabilities, while microRNA-146a serves as a suppressor of the NF-κB-mediated inflammatory response. When combined, the CNP-miR146a formulation offers a dual-effect by simultaneously mitigating oxidative damage and inflammation. Administering this combination directly into the skin has been shown to improve collagen production, stimulate new blood vessel formation, and reduce inflammatory and oxidative markers leading to accelerated healing in diabetic wound models (Figure 8H).
To better understand the multifaceted roles of nanoceria, numerous studies have been performed into their biological behavior and potential therapeutic benefits for wound healing. Pandey et al. observed that temperature significantly influences the redox functionality of CeO₂ NPs, noting a decline in superoxide dismutase-like activity as temperature decreases [207]. Additionally, these nanoparticles demonstrated up to 60% inhibition of α-amylase at 1 mM, highlighting their relevance for antidiabetic applications, particularly in managing diabetic wounds due to their combined antioxidant, antimicrobial, and metabolic regulatory properties. In parallel, Bai et al. emphasized the enzyme-like capabilities of nanoceria, describing their redox mechanism involving the interconversion of Ce³⁺ and Ce⁴⁺ states, which creates oxygen vacancies [141]. This structural characteristic allows them to mimic multiple enzymatic functions, such as those of catalase, peroxidase, oxidase, and superoxide dismutase. These multienzyme-mimetic properties make nanoceria a promising tool in areas such as disease diagnostics, therapeutics, and broader biomedical applications, especially due to their capacity to neutralize nitric oxide and other reactive species. Further insights from He et al. explored the molecular underpinnings of nanoceria-mediated wound healing, identifying their role in modulating mitochondrial function via the NLRP3 inflammasome pathway [208]. Differential gene expression analysis pointed to involvement in immune regulation, metabolic pathways, and inflammatory signaling, including the TNFR2/NF-κB axis. Notably, CeO₂–Y@ZIF-8@Gel treatment helped prevent mitochondrial DNA escape and reduced inflammasome activation, leading to decreased IL-1β secretion and promoting an anti-inflammatory macrophage phenotype by limiting cGAS-STING signaling.
Figure 8.
Application of nanoceria for wound healing applications. (A) Schematic showing accelerated wound healing using MSN-Ceria, a ROS-scavenging tissue adhesive that promotes wound closure by drawing wound edges together and mitigating oxidative stress to support tissue regeneration. (B) Stereomicroscopic images of wound surfaces on day 22 post-injury reveal healing progress. (C) DHE-stained cryosections on day 2 highlight superoxide anion production at the wound site. Scale bar: 100 μm. (D) Immunofluorescence images of CD68+ macrophages (green) on day 5 indicate immune cell infiltration in untreated, MSN-, and MSN-Ceria-treated groups. Scale bar: 50 μm. (D) schematic illustration of the preparation and working principle of CIP-Ceria-PVs for diabetic wound application. (E) In vivo superoxide levels monitored by fluorescence microscopy using CIP-Ceria-PVs. Scale bar: 100 μm. (F) Haematoxylin and eosin-stained (H&E) or Masson-stained mouse skin tissue of the wound area. Scale bar: 200 μm. (G) A schematic showing the Gelma-Cerium NP hydrogel patches for wound healing [application. (H) H and E staining results for diabetic wounds from rats. mRNA-Cerium NPs showed recued inflammation, oxidative stress, and enhanced angiogenesis after the treatment compared to control studies. Scale bar 50 μm. Reproduced with permission from [200,201,204,205]. Copyright 2018, Elsevier; 2021 and 2020, American Chemical Society; 2022, Elsevier respectively.
Figure 8.
Application of nanoceria for wound healing applications. (A) Schematic showing accelerated wound healing using MSN-Ceria, a ROS-scavenging tissue adhesive that promotes wound closure by drawing wound edges together and mitigating oxidative stress to support tissue regeneration. (B) Stereomicroscopic images of wound surfaces on day 22 post-injury reveal healing progress. (C) DHE-stained cryosections on day 2 highlight superoxide anion production at the wound site. Scale bar: 100 μm. (D) Immunofluorescence images of CD68+ macrophages (green) on day 5 indicate immune cell infiltration in untreated, MSN-, and MSN-Ceria-treated groups. Scale bar: 50 μm. (D) schematic illustration of the preparation and working principle of CIP-Ceria-PVs for diabetic wound application. (E) In vivo superoxide levels monitored by fluorescence microscopy using CIP-Ceria-PVs. Scale bar: 100 μm. (F) Haematoxylin and eosin-stained (H&E) or Masson-stained mouse skin tissue of the wound area. Scale bar: 200 μm. (G) A schematic showing the Gelma-Cerium NP hydrogel patches for wound healing [application. (H) H and E staining results for diabetic wounds from rats. mRNA-Cerium NPs showed recued inflammation, oxidative stress, and enhanced angiogenesis after the treatment compared to control studies. Scale bar 50 μm. Reproduced with permission from [200,201,204,205]. Copyright 2018, Elsevier; 2021 and 2020, American Chemical Society; 2022, Elsevier respectively.

Despite the potential of conventional nanozymes, their inability to continuously neutralize newly formed reactive oxygen species, especially hydroxyl radicals (·OH), poses limitations. Addressing this, Zhu et al. developed an advanced antioxidant nanoplatform by loading the NF-κB inhibitor JSH-23 into copper-doped ceria nanozymes [209]. To enhance tissue compatibility and adhesion in wound environments, these nanozymes were incorporated into a hydrogel spray composed of oxidized sodium alginate and methacrylated gelatin. This formulation not only activated Nrf2 pathways in macrophages, thereby suppressing oxidative stress at the source, but also maintained strong ROS-scavenging properties, significantly improving healing in diabetic wound models. Lastly, Carvajal et al. demonstrated that nanoceria can counteract oxidative stress-induced cellular changes by reversing H₂O₂-triggered phosphorylation events that regulate cell proliferation, stress signaling, and transcription [210].Their intervention notably impacted pathways involving mTOR, MAPK/ERK, CK2A1, and PKACA, further supporting the regulatory potential of nanoceria in oxidative stress-related cellular processes.
Even though there are multiple examples and applications of nanoceria for wound healing, future research on nanoceria should focus on optimizing their formulation and delivery, understanding their molecular mechanisms, ensuring biosafety, and translating preclinical successes into clinical therapies using standardized protocols. Additionally, regulatory compliance should be considered. Caution must be exercised regarding potential toxicity, immune responses, and chronic effects of particles to fully realize their promise in wound care.
5. Conclusions and Future Directions
The existing literature shows that nanoceria has emerged as a highly versatile nanomaterial with broad potential across diverse fields. Its distinctive redox and catalytic behavior has made nanoceria valuable in several biosensing and therapeutic applications. The excellent antioxidant properties of these nanoparticles were utilized as a diagnostic tool for detecting the COVID-19 virus and for targeting respiratory infections [211]. The potential use of nanoceria in medicine remains promising, particularly when considering strategies aimed at engineering their surface characteristics to enhance efficacy and biocompatibility. Notably, nanoceria demonstrates dual redox behavior, acting as either a reactive oxygen species (ROS) scavenger or an inducer, depending on the microenvironment. This duality is particularly advantageous in oncology, where nanoceria has shown selective toxicity towards cancer cells while shielding healthy tissues from chemotherapy-induced oxidative stress. Furthermore, nanoceria can be functionalized with various therapeutic and diagnostic agents, including small-molecule drugs, miRNAs, monoclonal antibodies, and imaging probes to enhance its biomedical performance. Some of these conjugate systems have already yielded encouraging results in preclinical models. Advancing the design of these surface-modified nanoceria platforms could offer significant breakthroughs in cancer therapy and beyond.
6. Future Direction and Prospects
Despite the immense therapeutic potential of nanoceria, significant concerns exist regarding its biological safety. One major hurdle is the variability introduced by different synthetic methods, which can alter the physicochemical characteristics of nanoceria and thereby influence its biological activity and safety. This inconsistency complicates the prediction of the nanomaterial’s behavior in biological systems. Additionally, regulatory frameworks for nanomaterials remain underdeveloped, and concerns about nanoparticle purity persist as contaminants can lead to unintended toxic effects.
Nanoceria has been known to have cytotoxic, genotoxic, and neurotoxic effects, particularly after prolonged exposure [212]. Extended contact with nanoceria may induce lung fibrosis and granulomas in both lung and liver tissues. Paradoxically, sustained exposure can also trigger inflammation and elevate oxidative stress in specific organs, including the brain, where neurotoxic effects persist even after cerium is no longer detectable [213]. These adverse outcomes highlight the delicate balance between the beneficial antioxidant roles nanoceria plays and its potential to cause harm within biological systems.
Another challenge with nanoceria in medicine is its rapid renal clearance. which is attributed to its nanoscale size [214]. While quick elimination is often beneficial in reducing toxicity, it limits the duration over which nanoceria can exert therapeutic effects detracting from its efficacy in treating chronic conditions. Ironically, the very features that make nanoceria attractive—small size, robust ROS scavenging activity, and surface valence cycling—also contribute to its toxicological risks and clearance issues [215]. Thus, the unique physicochemical traits that enable its medicinal promise simultaneously underpin the difficulties faced in safely harnessing nanoceria for long-term biomedical use.
Funding
There is no funding used for this review article.
Acknowledgments
The authors acknowledge the Department of Biomedical Engineering at Michigan State University.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Netea, M.G.; Balkwill, F.; Chonchol, M.; Cominelli, F.; Donath, M.Y.; Giamarellos-Bourboulis, E.J.; Golenbock, D.; Gresnigt, M.S.; Heneka, M.T.; Hoffman, H.M.; et al. A guiding map for inflammation. Nature Immunology 2017, 18, 826–831. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nature Medicine 2019, 25, 1822–1832. [Google Scholar] [CrossRef]
- Theoharides, T.C.; Alysandratos, K.D.; Angelidou, A.; Delivanis, D.A.; Sismanopoulos, N.; Zhang, B.; Asadi, S.; Vasiadi, M.; Weng, Z.; Miniati, A.; et al. Mast cells and inflammation. Biochim Biophys Acta 2012, 1822, 21–33. [Google Scholar] [CrossRef]
- Margraf, A.; Lowell, C.A.; Zarbock, A. Neutrophils in acute inflammation: current concepts and translational implications. Blood 2022, 139, 2130–2144. [Google Scholar] [CrossRef]
- Megha, K.B.; Joseph, X.; Akhil, V.; Mohanan, P.V. Cascade of immune mechanism and consequences of inflammatory disorders. Phytomedicine 2021, 91, 153712. [Google Scholar] [CrossRef]
- Seder, R.A.; Ahmed, R. Similarities and differences in CD4+ and CD8+ effector and memory T cell generation. Nature Immunology 2003, 4, 835–842. [Google Scholar] [CrossRef]
- Catalán, D.; Mansilla, M.A.; Ferrier, A.; Soto, L.; Oleinika, K.; Aguillón, J.C.; Aravena, O. Immunosuppressive Mechanisms of Regulatory B Cells. Front Immunol 2021, 12, 611795. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, J.; Zhang, X.; Wang, C.; Huang, Y.; Dai, K. TNF-α-induced LRG1 promotes angiogenesis and mesenchymal stem cell migration in the subchondral bone during osteoarthritis. Cell Death Dis 2017, 8, e2715. [Google Scholar] [CrossRef]
- Venetsanopoulou, A.I.; Alamanos, Y.; Voulgari, P.V.; Drosos, A.A. Epidemiology and Risk Factors for Rheumatoid Arthritis Development. Mediterr J Rheumatol 2023, 34, 404–413. [Google Scholar] [CrossRef]
- Raharja, A.; Mahil, S.K.; Barker, J.N. Psoriasis: a brief overview. Clin Med (Lond) 2021, 21, 170–173. [Google Scholar] [CrossRef]
- Henein, M.Y.; Vancheri, S.; Longo, G.; Vancheri, F. The Role of Inflammation in Cardiovascular Disease. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Cornwell, C.R.; Hsu, J.; Tompkins, L.K.; Pennington, A.F.; Flanders, W.D.; Sircar, K. Clinical outcomes among hospitalized US adults with asthma or chronic obstructive pulmonary disease, with or without COVID-19. J Asthma 2022, 59, 2509–2519. [Google Scholar] [CrossRef]
- Indicators of Environmental Health Disparites: Childhood Asthma Prevalence. 2023.
- Sartori, A.C.; Vance, D.E.; Slater, L.Z.; Crowe, M. The impact of inflammation on cognitive function in older adults: implications for healthcare practice and research. J Neurosci Nurs 2012, 44, 206–217. [Google Scholar] [CrossRef]
- Chen, Y.; Song, Y.; Du, W.; Gong, L.; Chang, H.; Zou, Z. Tumor-associated macrophages: an accomplice in solid tumor progression. Journal of Biomedical Science 2019, 26. [Google Scholar] [CrossRef]
- Dropulic, L.K.; Lederman, H.M. Overview of Infections in the Immunocompromised Host. Microbiol Spectr 2016, 4. [Google Scholar] [CrossRef]
- Cryer, B.; Feldman, M. Cyclooxygenase-1 and cyclooxygenase-2 selectivity of widely used nonsteroidal anti-inflammatory drugs. Am J Med 1998, 104, 413–421. [Google Scholar] [CrossRef]
- Ohashi, N.; Kohno, T. Analgesic Effect of Acetaminophen: A Review of Known and Novel Mechanisms of Action. Front Pharmacol 2020, 11, 580289. [Google Scholar] [CrossRef]
- Murphy, P.B.; Kasotakis, G.; Haut, E.R.; Miller, A.; Harvey, E.; Hasenboehler, E.; Higgins, T.; Hoegler, J.; Mir, H.; Cantrell, S.; et al. Efficacy and safety of non-steroidal anti-inflammatory drugs (NSAIDs) for the treatment of acute pain after orthopedic trauma: a practice management guideline from the Eastern Association for the Surgery of Trauma and the Orthopedic Trauma Association. Trauma Surg Acute Care Open 2023, 8, e001056. [Google Scholar] [CrossRef]
- Ghlichloo, I.; Gerriets, V. Nonsteroidal Anti-Inflammatory Drugs. Available online: (accessed on.
- Agrawal, S.; Khazaeni, B. Acetaminophen Toxicity. Available online: (accessed on.
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem Pharmacol 2020, 180, 114147. [Google Scholar] [CrossRef]
- Hodgens, A.; Sharman, T. Corticosteroids. Available online: (accessed on.
- Harvey, J.; Lax, S.J.; Lowe, A.; Santer, M.; Lawton, S.; Langan, S.M.; Roberts, A.; Stuart, B.; Williams, H.C.; Thomas, K.S. The long-term safety of topical corticosteroids in atopic dermatitis: A systematic review. Skin Health Dis 2023, 3, e268. [Google Scholar] [CrossRef]
- Coondoo, A.; Phiske, M.; Verma, S.; Lahiri, K. Side-effects of topical steroids: A long overdue revisit. Indian Dermatol Online J 2014, 5, 416–425. [Google Scholar] [CrossRef]
- Jones, C.J.; Morris, K.J.; Jayson, M.I. Prednisolone inhibits phagocytosis by polymorphonuclear leucocytes via steroid receptor mediated events. Ann Rheum Dis 1983, 42, 56–62. [Google Scholar] [CrossRef]
- Price, D.; Castro, M.; Bourdin, A.; Fucile, S.; Altman, P. Short-course systemic corticosteroids in asthma: striking the balance between efficacy and safety. Eur Respir Rev 2020, 29. [Google Scholar] [CrossRef]
- Boers, M.; Hartman, L.; Opris-Belinski, D.; Bos, R.; Kok, M.R.; Da Silva, J.A.; Griep, E.N.; Klaasen, R.; Allaart, C.F.; Baudoin, P.; et al. Low dose, add-on prednisolone in patients with rheumatoid arthritis aged 65+: the pragmatic randomised, double-blind placebo-controlled GLORIA trial. Ann Rheum Dis 2022, 81, 925–936. [Google Scholar] [CrossRef]
- Yasir, M.; Goyal, A.; Sonthalia, S. Corticosteroid Adverse Effects. Available online: (accessed on.
- Manubolu, S.; Nwosu, O. Exogenous Cushing’s syndrome secondary to intermittent high dose oral prednisone for presumed asthma exacerbations in the setting of multiple emergency department visits. Journal of Clinical and Translational Endocrinology: Case Reports 2017, 6, 4–8. [Google Scholar] [CrossRef]
- Manjiani, D.; Paul, D.B.; Kunnumpurath, S.; Kaye, A.D.; Vadivelu, N. Availability and utilization of opioids for pain management: global issues. Ochsner J 2014, 14, 208–215. [Google Scholar]
- Dydyk, A.M.; Jain, N.K.; Gupta, M. Opioid Use Disorder. Available online: (accessed on.
- Lyle Cooper, R.; Thompson, J.; Edgerton, R.; Watson, J.; MacMaster, S.A.; Kalliny, M.; Huffman, M.M.; Juarez, P.; Mathews-Juarez, P.; Tabatabai, M.; et al. Modeling dynamics of fatal opioid overdose by state and across time. Prev Med Rep 2020, 20, 101184. [Google Scholar] [CrossRef]
- Awate, S.; Babiuk, L.A.; Mutwiri, G. Mechanisms of action of adjuvants. Front Immunol 2013, 4, 114. [Google Scholar] [CrossRef]
- Apostólico Jde, S.; Lunardelli, V.A.; Coirada, F.C.; Boscardin, S.B.; Rosa, D.S. Adjuvants: Classification, Modus Operandi, and Licensing. J Immunol Res 2016, 2016, 1459394. [Google Scholar] [CrossRef]
- Dong, P.; Gewirtz, D.A. Editorial: Risks and Benefits of Adjuvants to Cancer Therapies. Front Oncol 2022, 12, 913626. [Google Scholar] [CrossRef]
- Esfahani, K.; Roudaia, L.; Buhlaiga, N.; Del Rincon, S.V.; Papneja, N.; Miller, W.H., Jr. A review of cancer immunotherapy: from the past, to the present, to the future. Curr Oncol 2020, 27, S87–s97. [Google Scholar] [CrossRef]
- Pavón-Romero, G.F.; Parra-Vargas, M.I.; Ramírez-Jiménez, F.; Melgoza-Ruiz, E.; Serrano-Pérez, N.H.; Teran, L.M. Allergen Immunotherapy: Current and Future Trends. Cells 2022, 11. [Google Scholar] [CrossRef]
- Allen, L.A.; Dayan, C.M. Immunotherapy for type 1 diabetes. Br Med Bull 2021, 140, 76–90. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, Z.; Pang, Y.; Zhou, H. The interaction between nanoparticles and immune system: application in the treatment of inflammatory diseases. Journal of Nanobiotechnology 2022, 20. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.J.; Billingsley, M.M.; Haley, R.M.; Wechsler, M.E.; Peppas, N.A.; Langer, R. Engineering precision nanoparticles for drug delivery. Nat Rev Drug Discov 2021, 20, 101–124. [Google Scholar] [CrossRef]
- Joudeh, N.; Linke, D. Nanoparticle classification, physicochemical properties, characterization, and applications: a comprehensive review for biologists. J Nanobiotechnology 2022, 20, 262. [Google Scholar] [CrossRef]
- Kothamasu, P.; Kanumur, H.; Ravur, N.; Maddu, C.; Parasuramrajam, R.; Thangavel, S. Nanocapsules: the weapons for novel drug delivery systems. Bioimpacts 2012, 2, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Bharti, C.; Nagaich, U.; Pal, A.K.; Gulati, N. Mesoporous silica nanoparticles in target drug delivery system: A review. Int J Pharm Investig 2015, 5, 124–133. [Google Scholar] [CrossRef]
- Dos Santos da Silva, A.; Dos Santos, J.H.Z. Stöber method and its nuances over the years. Adv Colloid Interface Sci 2023, 314, 102888. [Google Scholar] [CrossRef]
- Suk, J.S.; Xu, Q.; Kim, N.; Hanes, J.; Ensign, L.M. PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv Drug Deliv Rev 2016, 99, 28–51. [Google Scholar] [CrossRef]
- Andrade, S.; Ramalho, M.J.; Loureiro, J.A.; Pereira, M.C. Liposomes as biomembrane models: Biophysical techniques for drug-membrane interaction studies. Journal of Molecular Liquids 2021, 334. [Google Scholar] [CrossRef]
- Liu, P.; Chen, G.; Zhang, J. A Review of Liposomes as a Drug Delivery System: Current Status of Approved Products, Regulatory Environments, and Future Perspectives. Molecules 2022, 27. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Allemailem, K.S.; Almatroodi, S.A.; Almatroudi, A.; Rahmani, A.H. Recent strategies towards the surface modification of liposomes: an innovative approach for different clinical applications. 3 Biotech 2020, 10, 163. [Google Scholar] [CrossRef]
- Deshpande, P.P.; Biswas, S.; Torchilin, V.P. Current trends in the use of liposomes for tumor targeting. Nanomedicine (Lond) 2013, 8, 1509–1528. [Google Scholar] [CrossRef] [PubMed]
- Danila, D.; Pardo, P.S.; Misra, R.D.K.; Boriek, A.M. Liposomes as Imaging Agents of Inflammation and Oxidative Stress in Bone Implants. In Curr Issues Mol Biol; © 2025 by the authors.: 2025; Volume 47.
- Glazer, E.S.; Curley, S.A. The ongoing history of thermal therapy for cancer. Surg Oncol Clin N Am 2011, 20, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Dulińska-Litewka, J.; Łazarczyk, A.; Hałubiec, P.; Szafrański, O.; Karnas, K.; Karewicz, A. Superparamagnetic Iron Oxide Nanoparticles-Current and Prospective Medical Applications. Materials (Basel) 2019, 12. [Google Scholar] [CrossRef]
- Sahli, C.; Moya, S.E.; Lomas, J.S.; Gravier-Pelletier, C.; Briandet, R.; Hémadi, M. Recent advances in nanotechnology for eradicating bacterial biofilm. Theranostics 2022, 12, 2383–2405. [Google Scholar] [CrossRef]
- Liao, S.; Yue, W.; Cai, S.; Tang, Q.; Lu, W.; Huang, L.; Qi, T.; Liao, J. Improvement of Gold Nanorods in Photothermal Therapy: Recent Progress and Perspective. Front Pharmacol 2021, 12, 664123. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhan, X.; Xiong, J.; Peng, S.; Huang, W.; Joshi, R.; Cai, Y.; Liu, Y.; Li, R.; Yuan, K.; et al. Temperature-dependent cell death patterns induced by functionalized gold nanoparticle photothermal therapy in melanoma cells. Scientific Reports 2018, 8. [Google Scholar] [CrossRef]
- Rock, K.L.; Kono, H. The inflammatory response to cell death. Annu Rev Pathol 2008, 3, 99–126. [Google Scholar] [CrossRef]
- Zhuang, J.; Holay, M.; Park, J.H.; Fang, R.H.; Zhang, J.; Zhang, L. Nanoparticle Delivery of Immunostimulatory Agents for Cancer Immunotherapy. Theranostics 2019, 9, 7826–7848. [Google Scholar] [CrossRef] [PubMed]
- Nsairat, H.; Khater, D.; Sayed, U.; Odeh, F.; Al Bawab, A.; Alshaer, W. Liposomes: structure, composition, types, and clinical applications. Heliyon 2022, 8, e09394. [Google Scholar] [CrossRef] [PubMed]
- Tenchov, R.; Bird, R.; Curtze, A.E.; Zhou, Q. Lipid Nanoparticles─From Liposomes to mRNA Vaccine Delivery, a Landscape of Research Diversity and Advancement. ACS Nano 2021, 15, 16982–17015. [Google Scholar] [CrossRef]
- Tretiakova, D.S.; Vodovozova, E.L. Liposomes as Adjuvants and Vaccine Delivery Systems. Biochem (Mosc) Suppl Ser A Membr Cell Biol 2022, 16, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Pöyhönen, L.; Bustamante, J.; Casanova, J.L.; Jouanguy, E.; Zhang, Q. Life-Threatening Infections Due to Live-Attenuated Vaccines: Early Manifestations of Inborn Errors of Immunity. J Clin Immunol 2019, 39, 376–390. [Google Scholar] [CrossRef]
- Deshwal, A.; Saxena, K.; Sharma, G.; Rajesh; Sheikh, F.A.; Seth, C.S.; Tripathi, R.M. Nanozymes: A comprehensive review on emerging applications in cancer diagnosis and therapeutics. Int J Biol Macromol 2024, 256, 128272. [CrossRef]
- Zhang, L.; Zhu, J.; Hong, W.; Li, G. Highly sensitive electrochemical detection of cholesterol based on Au-Pt NPs/PAMAM-ZIF-67 nanomaterials. Anal Sci 2024, 40, 37–45. [Google Scholar] [CrossRef]
- Li, Q.; Liu, Y.; Dai, X.; Jiang, W.; Zhao, H. Nanozymes Regulate Redox Homeostasis in ROS-Related Inflammation. Front Chem 2021, 9, 740607. [Google Scholar] [CrossRef]
- Saifi, M.A.; Seal, S.; Godugu, C. Nanoceria, the versatile nanoparticles: Promising biomedical applications. Journal of Controlled Release 2021, 164–189. [Google Scholar] [CrossRef]
- Estevez, A.Y.; Erlichman, J.S. The potential of cerium oxide nanoparticles (nanoceria) for neurodegenerative disease therapy. Nanomedicine (Lond) 2014, 9, 1437–1440. [Google Scholar] [CrossRef]
- Kalashnikova, I.; Chung, S.-J.; Nafiujjaman, M.; Hill, M.L.; Siziba, M.E.; Contag, C.H.; Kim, T. Ceria-based nanotheranostic agent for rheumatoid arthritis. Theranostics 2020, 10, 11863–11880. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.K.; Kim, T.; Choi, I.Y.; Soh, M.; Kim, D.; Kim, Y.J.; Jang, H.; Yang, H.S.; Kim, J.Y.; Park, H.K.; et al. Ceria nanoparticles that can protect against ischemic stroke. Angew Chem Int Ed Engl 2012, 51, 11039–11043. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.L.; Chung, S.J.; Woo, H.J.; Park, C.R.; Hadrick, K.; Nafiujjaman, M.; Kumar, P.P.P.; Mwangi, L.; Parikh, R.; Kim, T. Exosome-Coated Prussian Blue Nanoparticles for Specific Targeting and Treatment of Glioblastoma. ACS Appl Mater Interfaces 2024, 16, 20286–20301. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Chen, D.; Wang, Y.; Li, H.; Zhang, Y.; Chen, H.; Li, X.; Huo, M. Nanozymes-recent development and biomedical applications. Journal of Nanobiotechnology 2022, 20. [Google Scholar] [CrossRef]
- Mitchell, L.A.; Gao, J.; Wal, R.V.; Gigliotti, A.; Burchiel, S.W.; McDonald, J.D. Pulmonary and systemic immune response to inhaled multiwalled carbon nanotubes. Toxicol Sci 2007, 100, 203–214. [Google Scholar] [CrossRef]
- Mitchell, L.A.; Lauer, F.T.; Burchiel, S.W.; McDonald, J.D. Mechanisms for how inhaled multiwalled carbon nanotubes suppress systemic immune function in mice. Nat Nanotechnol 2009, 4, 451–456. [Google Scholar] [CrossRef]
- Tkach, A.V.; Shurin, G.V.; Shurin, M.R.; Kisin, E.R.; Murray, A.R.; Young, S.H.; Star, A.; Fadeel, B.; Kagan, V.E.; Shvedova, A.A. Direct effects of carbon nanotubes on dendritic cells induce immune suppression upon pulmonary exposure. ACS Nano 2011, 5, 5755–5762. [Google Scholar] [CrossRef]
- Inoue, K.; Koike, E.; Yanagisawa, R.; Hirano, S.; Nishikawa, M.; Takano, H. Effects of multi-walled carbon nanotubes on a murine allergic airway inflammation model. Toxicol Appl Pharmacol 2009, 237, 306–316. [Google Scholar] [CrossRef]
- Wang, X.; Podila, R.; Shannahan, J.H.; Rao, A.M.; Brown, J.M. Intravenously delivered graphene nanosheets and multiwalled carbon nanotubes induce site-specific Th2 inflammatory responses via the IL-33/ST2 axis. Int J Nanomedicine 2013, 8, 1733–1748. [Google Scholar] [CrossRef]
- Ryan, J.J.; Bateman, H.R.; Stover, A.; Gomez, G.; Norton, S.K.; Zhao, W.; Schwartz, L.B.; Lenk, R.; Kepley, C.L. Fullerene nanomaterials inhibit the allergic response. J Immunol 2007, 179, 665–672. [Google Scholar] [CrossRef]
- Tsao, N.; Luh, T.Y.; Chou, C.K.; Wu, J.J.; Lin, Y.S.; Lei, H.Y. Inhibition of group A streptococcus infection by carboxyfullerene. Antimicrob Agents Chemother 2001, 45, 1788–1793. [Google Scholar] [CrossRef] [PubMed]
- Cho, W.S.; Cho, M.; Jeong, J.; Choi, M.; Cho, H.Y.; Han, B.S.; Kim, S.H.; Kim, H.O.; Lim, Y.T.; Chung, B.H. Acute toxicity and pharmacokinetics of 13 nm-sized PEG-coated gold nanoparticles. Toxicol Appl Pharmacol 2009, 236, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Parween, S.; Gupta, P.K.; Chauhan, V.S. Induction of humoral immune response against PfMSP-1(19) and PvMSP-1(19) using gold nanoparticles along with alum. Vaccine 2011, 29, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.; Vanoirbeek, J.A.; Luyts, K.; De Vooght, V.; Verbeken, E.; Thomassen, L.C.; Martens, J.A.; Dinsdale, D.; Boland, S.; Marano, F.; et al. Lung exposure to nanoparticles modulates an asthmatic response in a mouse model. Eur Respir J 2011, 37, 299–309. [Google Scholar] [CrossRef]
- Alkilany, A.M.; Murphy, C.J. Toxicity and cellular uptake of gold nanoparticles: what we have learned so far? J Nanopart Res 2010, 12, 2313–2333. [Google Scholar] [CrossRef]
- Liu, H.; Yang, D.; Yang, H.; Zhang, H.; Zhang, W.; Fang, Y.; Lin, Z.; Tian, L.; Lin, B.; Yan, J.; et al. Comparative study of respiratory tract immune toxicity induced by three sterilisation nanoparticles: silver, zinc oxide and titanium dioxide. J Hazard Mater 2013, 248-249, 478–486. [Google Scholar] [CrossRef]
- Zhu, M.; Tian, X.; Song, X.; Li, Y.; Tian, Y.; Zhao, Y.; Nie, G. Nanoparticle-induced exosomes target antigen-presenting cells to initiate Th1-type immune activation. Small 2012, 8, 2841–2848. [Google Scholar] [CrossRef]
- Zhu, M.; Li, Y.; Shi, J.; Feng, W.; Nie, G.; Zhao, Y. Exosomes as extrapulmonary signaling conveyors for nanoparticle-induced systemic immune activation. Small 2012, 8, 404–412. [Google Scholar] [CrossRef]
- Shen, C.C.; Liang, H.J.; Wang, C.C.; Liao, M.H.; Jan, T.R. Iron oxide nanoparticles suppressed T helper 1 cell-mediated immunity in a murine model of delayed-type hypersensitivity. Int J Nanomedicine 2012, 7, 2729–2737. [Google Scholar] [CrossRef]
- Ban, M.; Langonné, I.; Huguet, N.; Guichard, Y.; Goutet, M. Iron oxide particles modulate the ovalbumin-induced Th2 immune response in mice. Toxicol Lett 2013, 216, 31–39. [Google Scholar] [CrossRef]
- Wingard, C.J.; Walters, D.M.; Cathey, B.L.; Hilderbrand, S.C.; Katwa, P.; Lin, S.; Ke, P.C.; Podila, R.; Rao, A.; Lust, R.M.; et al. Mast cells contribute to altered vascular reactivity and ischemia-reperfusion injury following cerium oxide nanoparticle instillation. Nanotoxicology 2011, 5, 531–545. [Google Scholar] [CrossRef]
- Srinivas, A.; Rao, P.J.; Selvam, G.; Murthy, P.B.; Reddy, P.N. Acute inhalation toxicity of cerium oxide nanoparticles in rats. Toxicol Lett 2011, 205, 105–115. [Google Scholar] [CrossRef]
- Chanan-Khan, A.; Szebeni, J.; Savay, S.; Liebes, L.; Rafique, N.M.; Alving, C.R.; Muggia, F.M. Complement activation following first exposure to pegylated liposomal doxorubicin (Doxil): possible role in hypersensitivity reactions. Ann Oncol 2003, 14, 1430–1437. [Google Scholar] [CrossRef] [PubMed]
- Hardy, C.L.; LeMasurier, J.S.; Belz, G.T.; Scalzo-Inguanti, K.; Yao, J.; Xiang, S.D.; Kanellakis, P.; Bobik, A.; Strickland, D.H.; Rolland, J.M.; et al. Inert 50-nm polystyrene nanoparticles that modify pulmonary dendritic cell function and inhibit allergic airway inflammation. J Immunol 2012, 188, 1431–1441. [Google Scholar] [CrossRef]
- Cerium. Available online: (accessed on.
- Xu, C.; Qu, X. Cerium oxide nanoparticle: a remarkably versatile rare earth nanomaterial for biological applications. NPG Asia Materials 2014, 6, e90–e90. [Google Scholar] [CrossRef]
- Gangopadhyay, S.; Frolov, D.D.; Masunov, A.E.; Seal, S. Structure and properties of cerium oxides in bulk and nanoparticulate forms. 2014, 584, 199-208.
- Hirst, S.M.; Karakoti, A.S.; Tyler, R.D.; Sriranganathan, N.; Seal, S.; Reilly, C.M. Anti-inflammatory properties of cerium oxide nanoparticles. Small 2009, 5, 2848–2856. [Google Scholar] [CrossRef] [PubMed]
- Dutta, P.; Pal, S.; Seehra, M.S.; Shi, Y.; Eyring, E.M.; Ernst, R.D. Concentration of Ce 3+ and Oxygen Vacancies in Cerium Oxide Nanoparticles. Chemistry of Materials 2006, 18, 5144–5146. [Google Scholar] [CrossRef]
- Cafun, J.-D.; Kvashnina, K.O.; Casals, E.; Puntes, V.F.; Glatzel, P. Absence of Ce 3+ Sites in Chemically Active Colloidal Ceria Nanoparticles. ACS Nano 2013, 7, 10726–10732. [Google Scholar] [CrossRef]
- Deshpande, S.; Patil, S.; Kuchibhatla, S.V.N.T.; Seal, S. Size dependency variation in lattice parameter and valency states in nanocrystalline cerium oxide. Applied Physics Letters 2005, 13. [Google Scholar] [CrossRef]
- Celardo, I.; De Nicola, M.; Mandoli, C.; Pedersen, J.Z.; Traversa, E.; Ghibelli, L. Ce 3+ Ions Determine Redox-Dependent Anti-apoptotic Effect of Cerium Oxide Nanoparticles. ACS Nano 2011, 5. [Google Scholar] [CrossRef]
- Wang, Z.; Shen, X.; Gao, X.; Zhao, Y. Simultaneous enzyme mimicking and chemical reduction mechanisms for nanoceria as a bio-antioxidant: a catalytic model bridging computations and experiments for nanozymes. Nanoscale 2019, 11, 13289–13299. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Liu, Y.; Huang, J.; Chen, K.; Huang, J.; Xiao, K. Uptake, distribution, clearance, and toxicity of iron oxide nanoparticles with different sizes and coatings. Scientific Reports 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Spada, A.; Emami, J.; Tuszynski, J.A.; Lavasanifar, A. The Uniqueness of Albumin as a Carrier in Nanodrug Delivery. Mol Pharm 2021, 18, 1862–1894. [Google Scholar] [CrossRef]
- Singh, S.; Kumar, A.; Karakoti, A.; Seal, S.; Self, W.T. Unveiling the mechanism of uptake and sub-cellular distribution of cerium oxidenanoparticles. Molecular Biosystems 2010, 6, 1813–1820. [Google Scholar] [CrossRef]
- Apostolova, N.; Rovira-Llopis, S.; Baldoví, H.G.; Navalon, S.; Asiri, A.M.; Victor, V.M.; Garcia, H.; Herance, J.R. Ceria nanoparticles with rhodamine B as a powerful theranostic agent against intracellular oxidative stress. RSC Advances 2015, 5, 79423–79432. [Google Scholar] [CrossRef]
- Tang, J.L.Y.; Moonshi, S.S.; Ta, H.T. Nanoceria: an innovative strategy for cancer treatment. Cell Mol Life Sci 2023, 80, 46. [Google Scholar] [CrossRef] [PubMed]
- Lord, M.S.; Jung, M.; Teoh, W.Y.; Gunawan, C.; Vassie, J.A.; Amal, R.; Whitelock, J.M. Cellular uptake and reactive oxygen species modulation of cerium oxide nanoparticles in human monocyte cell line U937. Biomaterials 2012, 33, 7915–7924. [Google Scholar] [CrossRef]
- Vassie, J.A.; Whitelock, J.M.; Lord, M.S. Endocytosis of cerium oxide nanoparticles and modulation of reactive oxygen species in human ovarian and colon cancer cells. Acta Biomater 2017, 50, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Song, W.; Cho, M.; Puppala, H.L.; Nguyen, P.; Zhu, H.; Segatori, L.; Colvin, V.L. Antioxidant Properties of Cerium Oxide Nanocrystals as a Function of Nanocrystal Diameter and Surface Coating. ACS Nano 2013, 7, 9693–9703. [Google Scholar] [CrossRef]
- Patil, S.; Sandberg, A.; Heckert, E.; Self, W.; Seal, S. Protein adsorption and cellular uptake of cerium oxide nanoparticles as a function of zeta potential. Biomaterials 2007, 28, 4600–4607. [Google Scholar] [CrossRef]
- Asati, A.; Santra, S.; Kaittanis, C.; Perez, J.M. Surface-Charge-Dependent Cell Localization and Cytotoxicity of Cerium Oxide Nanoparticles. ACS Nano 2010, 4, 5321–5331. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Mao, Z.; Huang, W.; Liu, L.; Li, J.; Wu, Q. Redox enzyme-mimicking activities of CeO(2) nanostructures: Intrinsic influence of exposed facets. Sci Rep 2016, 6, 35344. [Google Scholar] [CrossRef] [PubMed]
- Gubernatorova, E.O.; Liu, X.; Othman, A.; Muraoka, W.T.; Koroleva, E.P.; Andreescu, S.; Tumanov, A.V. Europium-Doped Cerium Oxide Nanoparticles Limit Reactive Oxygen Species Formation and Ameliorate Intestinal Ischemia-Reperfusion Injury. Adv Healthc Mater 2017, 6. [Google Scholar] [CrossRef]
- Wang, R.; Du, Y.; Fu, Y.; Guo, Y.; Gao, X.; Guo, X.; Wei, J.; Yang, Y. Ceria-Based Nanozymes in Point-of-Care Diagnosis: An Emerging Futuristic Approach for Biosensing. ACS Sensors 2023, 8, 4442–4467. [Google Scholar] [CrossRef]
- Ornatska, M.; Sharpe, E.; Andreescu, D.; Andreescu, S. Paper bioassay based on ceria nanoparticles as colorimetric probes. Anal Chem 2011, 83, 4273–4280. [Google Scholar] [CrossRef] [PubMed]
- Korsvik, C.; Patil, S.; Seal, S.; Self, W.T. Superoxide dismutase mimetic properties exhibited by vacancy engineered ceria nanoparticles. Chem Commun (Camb) 2007, 1056–1058. [Google Scholar] [CrossRef]
- Pirmohamed, T.; Dowding, J.M.; Singh, S.; Wasserman, B.; Heckert, E.; Karakoti, A.S.; King, J.E.; Seal, S.; Self, W.T. Nanoceria exhibit redox state-dependent catalase mimetic activity. Chem Commun (Camb) 2010, 46, 2736–2738. [Google Scholar] [CrossRef]
- Das, M.; Patil, S.; Bhargava, N.; Kang, J.F.; Riedel, L.M.; Seal, S.; Hickman, J.J. Auto-catalytic ceria nanoparticles offer neuroprotection to adult rat spinal cord neurons. Biomaterials 2007, 28, 1918–1925. [Google Scholar] [CrossRef]
- Karakoti, A.S.; Monteiro-Riviere, N.A.; Aggarwal, R.; Davis, J.P.; Narayan, R.J.; Self, W.T.; McGinnis, J.; Seal, S. Nanoceria as Antioxidant: Synthesis and Biomedical Applications. Jom (1989) 2008, 60, 33–37. [Google Scholar] [CrossRef]
- Caputo, F.; Mameli, M.; Sienkiewicz, A.; Licoccia, S.; Stellacci, F.; Ghibelli, L.; Traversa, E. A novel synthetic approach of cerium oxide nanoparticles with improved biomedical activity. Sci Rep 2017, 7, 4636. [Google Scholar] [CrossRef]
- Heckert, E.G.; Karakoti, A.S.; Seal, S.; Self, W.T. The role of cerium redox state in the SOD mimetic activity of nanoceria. Biomaterials 2008, 29, 2705–2709. [Google Scholar] [CrossRef] [PubMed]
- Baldim, V.; Bedioui, F.; Mignet, N.; Margaill, I.; Berret, J.-F. The enzyme-like catalytic activity of cerium oxide nanoparticles and its dependency on Ce 3+ surface area concentration. Nanoscale 2018, 10, 6971–6980. [Google Scholar] [CrossRef]
- Cioateră, N.; Pârvulescu, V.; Rolle, A.; Vannier, R.N. Effect of strontium addition on europium-doped ceria properties. Solid State Ionics 2009, 180, 681–687. [Google Scholar] [CrossRef]
- Singh, R.; Singh, S. Role of phosphate on stability and catalase mimetic activity of cerium oxide nanoparticles. Colloids Surf B Biointerfaces 2015, 132, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Singh, S. Redox-dependent catalase mimetic cerium oxide-based nanozyme protect human hepatic cells from 3-AT induced acatalasemia. Colloids Surf B Biointerfaces 2019, 175, 625–635. [Google Scholar] [CrossRef]
- Celardo, I.; Pedersen, J.Z.; Traversa, E.; Ghibelli, L. Pharmacological potential of cerium oxide nanoparticles. Nanoscale 2011, 3, 1411–1420. [Google Scholar] [CrossRef]
- Asati, A.; Kaittanis, C.; Santra, S.; Perez, J.M. pH-tunable oxidase-like activity of cerium oxide nanoparticles achieving sensitive fluorigenic detection of cancer biomarkers at neutral pH. Anal Chem 2011, 83, 2547–2553. [Google Scholar] [CrossRef] [PubMed]
- Asati, A.; Santra, S.; Kaittanis, C.; Nath, S.; Perez, J.M. Oxidase-like activity of polymer-coated cerium oxide nanoparticles. Angew Chem Int Ed Engl 2009, 48, 2308–2312. [Google Scholar] [CrossRef]
- Liu, B.; Huang, Z.; Liu, J. Boosting the oxidase mimicking activity of nanoceria by fluoride capping: rivaling protein enzymes and ultrasensitive F − detection. Nanoscale 2016, 8, 13562–13567. [Google Scholar] [CrossRef]
- Ni, P.; Wei, X.; Guo, J.; Ye, X.; Yang, S. On the origin of the oxidizing ability of ceria nanoparticles. 2015, 5, 97512-97519.
- Wu, J.; Wang, X.; Wang, Q.; Lou, Z.; Li, S.; Zhu, Y.; Qin, L.; Wei, H. Nanomaterials with enzyme-like characteristics (nanozymes): next-generation artificial enzymes (II). Chemical Society Reviews 2019, 48, 1004–1076. [Google Scholar]
- Jiang, D.; Ni, D.; Rosenkrans, Z.T.; Huang, P.; Yan, X.; Cai, W. Nanozyme: new horizons for responsive biomedical applications. Chemical Society Reviews 2019, 48, 3683–3704. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Zhang, A.; Wang, R.; Zhang, Q.; Cui, D. A Review on Metal- and Metal Oxide-Based Nanozymes: Properties, Mechanisms, and Applications. Nanomicro Lett 2021, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Wei, H.; Guo, J.; Yang, Y. Ceria-based peroxidase-mimicking nanozyme with enhanced activity: A coordination chemistry strategy. Colloids and Surfaces A: Physicochemical and Engineering Aspects 2021, 610. [Google Scholar] [CrossRef]
- Alshatteri, A.H.; Ali, G.K.; Omer, K.M. Enhanced Peroxidase-Mimic Catalytic Activity via Cerium Doping of Strontium-Based Metal-Organic Frameworks with Design of a Smartphone-Based Sensor for On-Site Salivary Total Antioxidant Capacity Detection in Lung Cancer Patients. ACS Appl Mater Interfaces 2023, 15, 21239–21251. [Google Scholar] [CrossRef]
- Heckert, E.G.; Seal, S.; Self, W.T. Fenton-like reaction catalyzed by the rare earth inner transition metal cerium. Environ Sci Technol 2008, 42, 5014–5019. [Google Scholar] [CrossRef]
- Nelson, B.C.; Johnson, M.E.; Walker, M.L.; Riley, K.R.; Sims, C.M. Antioxidant Cerium Oxide Nanoparticles in Biology and Medicine. Antioxidants (Basel) 2016, 5. [Google Scholar] [CrossRef]
- Banavar, S.; Deshpande, A.; Sur, S.; Andreescu, S. Ceria nanoparticle theranostics: harnessing antioxidant properties in biomedicine and beyond.
- Feng, N.; Liu, Y.; Dai, X.; Wang, Y.; Guo, Q.; Li, Q. Advanced applications of cerium oxide based nanozymes in cancer. RSC Adv 2022, 12, 1486–1493. [Google Scholar] [CrossRef]
- Silina, E.V.; Ivanova, O.S.; Manturova, N.E.; Medvedeva, O.A.; Shevchenko, A.V.; Vorsina, E.S.; Achar, R.R.; Parfenov, V.A.; Stupin, V.A. Antimicrobial Activity of Citrate-Coated Cerium Oxide Nanoparticles. Nanomaterials (Basel) 2024, 14. [Google Scholar] [CrossRef]
- Gaio, S.; Svensson, F.; Breijaert, T.; Seisenbaeva, G.; Kessler, V. Nanoceria–nanocellulose hybrid materials for delayed release of antibiotic and anti-inflammatory medicines. Materials Advances 2022, 3, 7228–7234. [Google Scholar] [CrossRef]
- Bai, Y.; Li, Y.; Tian, L. Advanced Biological Applications of Cerium Oxide Nanozymes in Disease Related to Oxidative Damage. ACS Omega 2024, 9, 8601–8614. [Google Scholar] [CrossRef]
- Singh, K.R.; Nayak, V.; Sarkar, T.; Singh, R.P. Cerium oxide nanoparticles: properties, biosynthesis and biomedical application. RSC Adv 2020, 10, 27194–27214. [Google Scholar] [CrossRef]
- Qiyue, W.; Wang, B.; Shi, D.; Li, F.; Ling, D. Cerium Oxide Nanoparticles-Based Optical Biosensors for Biomedical Applications. Advanced Sensor Research 2023, 2. [Google Scholar]
- Dhall, A.; Self, W. Cerium Oxide Nanoparticles: A Brief Review of Their Synthesis Methods and Biomedical Applications. Antioxidants (Basel) 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Hong, G.; Mazaleuskaya, L.; Hsu, J.C.; Rosario-Berrios, D.N.; Grosser, T.; Cho-Park, P.F.; Cormode, D.P. Ultrasmall Antioxidant Cerium Oxide Nanoparticles for Regulation of Acute Inflammation. ACS Appl Mater Interfaces 2021, 13, 60852–60864. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.G.; Lee, Y.; Lee, N.; Soh, M.; Kim, D.; Hyeon, T. Ceria-Based Therapeutic Antioxidants for Biomedical Applications. Adv Mater 2024, 36, e2210819. [Google Scholar] [CrossRef]
- Chen, S.; Wang, Y.; Bao, S.; Yao, L.; Fu, X.; Yu, Y.; Lyu, H.; Pang, H.; Guo, S.; Zhang, H.; et al. Cerium oxide nanoparticles in wound care: a review of mechanisms and therapeutic applications. Front Bioeng Biotechnol 2024, 12, 1404651. [Google Scholar] [CrossRef]
- Hosseini, M.; Mozafari, M. Cerium Oxide Nanoparticles: Recent Advances in Tissue Engineering. Materials (Basel) 2020, 13. [Google Scholar] [CrossRef]
- Asano, S.; Arvapalli, R.; Manne, N.D.; Maheshwari, M.; Ma, B.; Rice, K.M.; Selvaraj, V.; Blough, E.R. Cerium oxide nanoparticle treatment ameliorates peritonitis-induced diaphragm dysfunction. Int J Nanomedicine 2015, 10, 6215–6225. [Google Scholar] [CrossRef]
- Manne, N.D.; Arvapalli, R.; Nepal, N.; Shokuhfar, T.; Rice, K.M.; Asano, S.; Blough, E.R. Cerium oxide nanoparticles attenuate acute kidney injury induced by intra-abdominal infection in Sprague-Dawley rats. J Nanobiotechnology 2015, 13, 75. [Google Scholar] [CrossRef]
- Zhang, X.; Fu, X.; Chen, W.; Chen, P.; Zhu, H.; Yang, B.; Liang, J.; Zeng, F. Amelioration of the rheumatoid arthritis microenvironment using celastrol-loaded silver-modified ceria nanoparticles for enhanced treatment. J Nanobiotechnology 2025, 23, 372. [Google Scholar] [CrossRef]
- Xia, T.; Zhu, Y.; Li, K.; Hao, K.; Chai, Y.; Jiang, H.; Lou, C.; Yu, J.; Yang, W.; Wang, J.; et al. Microneedles loaded with cerium-manganese oxide nanoparticles for targeting macrophages in the treatment of rheumatoid arthritis. J Nanobiotechnology 2024, 22, 103. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: pathological mechanisms and modern pharmacologic therapies. Bone Research 2018, 6. [Google Scholar] [CrossRef]
- Kim, J.; Kim, H.Y.; Song, S.Y.; Go, S.H.; Sohn, H.S.; Baik, S.; Soh, M.; Kim, K.; Kim, D.; Kim, H.C.; et al. Synergistic Oxygen Generation and Reactive Oxygen Species Scavenging by Manganese Ferrite/Ceria Co-decorated Nanoparticles for Rheumatoid Arthritis Treatment. ACS Nano 2019, 13, 3206–3217. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Gao, W.; Sun, J.; Gao, K.; Li, D.; Mei, X. Developing cerium modified gold nanoclusters for the treatment of advanced-stage rheumatoid arthritis. Mater Today Bio 2022, 15, 100331. [Google Scholar] [CrossRef]
- Khurana, A.; Saifi, M.A.; Godugu, C. Nanoceria Ameliorates Fibrosis, Inflammation, and Cellular Stress in Experimental Chronic Pancreatitis. ACS Biomater Sci Eng 2023, 9, 1030–1042. [Google Scholar] [CrossRef]
- Luo, T.; Tang, Y.; Xie, W.; Ma, Z.; Gong, J.; Zhang, Y.; Yang, T.; Jia, X.; Zhou, J.; Hu, Z.; et al. Cerium-based nanoplatform for severe acute pancreatitis: Achieving enhanced anti-inflammatory effects through calcium homeostasis restoration and oxidative stress mitigation. Mater Today Bio 2025, 31, 101489. [Google Scholar] [CrossRef]
- Rahman, M.S.; Hadrick, K.; Chung, S.J.; Carley, I.; Yoo, J.Y.; Nahar, S.; Kim, T.H.; Kim, T.; Jeong, J.W. Nanoceria as a non-steroidal anti-inflammatory drug for endometriosis theranostics. J Control Release 2025, 378, 1015–1029. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, L.; Li, X.F. Hypoxia and the Tumor Microenvironment. Technol Cancer Res Treat 2021, 20, 15330338211036304. [Google Scholar] [CrossRef] [PubMed]
- Galon, J.; Costes, A.; Sanchez-Cabo, F.; Kirilovsky, A.; Mlecnik, B.; Lagorce-Pagès, C.; Tosolini, M.; Camus, M.; Berger, A.; Wind, P.; et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 2006, 313, 1960–1964. [Google Scholar] [CrossRef]
- Gao, R.; Mitra, R.N.; Zheng, M.; Wang, K.; Dahringer, J.C.; Han, Z. Developing Nanoceria-Based pH-Dependent Cancer-Directed Drug Delivery System for Retinoblastoma. Adv Funct Mater 2018, 28. [Google Scholar] [CrossRef]
- Fernández-Varo, G.; Perramón, M.; Carvajal, S.; Oró, D.; Casals, E.; Boix, L.; Oller, L.; Macías-Muñoz, L.; Marfà, S.; Casals, G.; et al. Bespoken Nanoceria: An Effective Treatment in Experimental Hepatocellular Carcinoma. Hepatology 2020, 72, 1267–1282. [Google Scholar] [CrossRef] [PubMed]
- Tian, Z.; Liu, H.; Guo, Z.; Gou, W.; Liang, Z.; Qu, Y.; Han, L.; Liu, L. A pH-Responsive Polymer-CeO(2) Hybrid to Catalytically Generate Oxidative Stress for Tumor Therapy. Small 2020, 16, e2004654. [Google Scholar] [CrossRef]
- Nourmohammadi, E.; Khoshdel-Sarkarizi, H.; Nedaeinia, R.; Darroudi, M.; Kazemi Oskuee, R. Cerium oxide nanoparticles: A promising tool for the treatment of fibrosarcoma in-vivo. Mater Sci Eng C Mater Biol Appl 2020, 109, 110533. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.; Wang, S.; Zheng, H.; Yang, S.; Zhou, L.; Liu, K.; Zhang, Q.; Zhang, H. Cu-doped cerium oxide-based nanomedicine for tumor microenvironment-stimulative chemo-chemodynamic therapy with minimal side effects. Colloids Surf B Biointerfaces 2021, 205, 111878. [Google Scholar] [CrossRef] [PubMed]
- Vercellini, P.; Viganò, P.; Somigliana, E.; Fedele, L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol 2014, 10, 261–275. [Google Scholar] [CrossRef]
- Ellis, K.; Munro, D.; Clarke, J. Endometriosis Is Undervalued: A Call to Action. Front Glob Womens Health 2022, 3, 902371. [Google Scholar] [CrossRef]
- Chaudhury, K.; Babu, K.N.; Singh, A.K.; Das, S.; Kumar, A.; Seal, S. Mitigation of endometriosis using regenerative cerium oxide nanoparticles. Nanomedicine 2013, 9, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Kimura, T.; Koyama, S.; Ogita, K.; Tsutsui, T.; Shimoya, K.; Taniguchi, T.; Koyama, M.; Kaneda, Y.; Murata, Y. Mouse model of human infertility: transient and local inhibition of endometrial STAT-3 activation results in implantation failure. FEBS Lett 2006, 580, 2717–2722. [Google Scholar] [CrossRef]
- Chen, F.; Ehlerding, E.B.; Cai, W. Theranostic nanoparticles. J Nucl Med 2014, 55, 1919–1922. [Google Scholar] [CrossRef]
- Zhang, P.; Li, Y.; Tang, W.; Zhao, J.; Jing, L.; McHugh, K.J. Theranostic nanoparticles with disease-specific administration strategies. Nano Today 2022, 42. [Google Scholar] [CrossRef]
- García, A.; Cámara, J.A.; Boullosa, A.M.; Gustà, M.F.; Mondragón, L.; Schwartz, S., Jr.; Casals, E.; Abasolo, I.; Bastús, N.G.; Puntes, V. Nanoceria as Safe Contrast Agents for X-ray CT Imaging. Nanomaterials (Basel) 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, P.; Truong, A.; Brommesson, C.; Rietz, A.; Kokil, G.; Boyd, R.; Hu, Z.; Dang, T.; Persson, P.; Uvdal, K. Cerium Oxide Nanoparticles with Entrapped Gadolinium for High T 1 Relaxivity and ROS-Scavenging Purposes. ACS Omega 2022, 7, 21337–21345. [Google Scholar] [CrossRef]
- Eriksson, P.; Tal, A.A.; Skallberg, A.; Brommesson, C.; Hu, Z.; Boyd, R.D.; Olovsson, W.; Fairley, N.; Abrikosov, I.A.; Zhang, X.; et al. Cerium oxide nanoparticles with antioxidant capabilities and gadolinium integration for MRI contrast enhancement. Sci Rep 2018, 8, 6999. [Google Scholar] [CrossRef]
- Wu, Y.; Yang, Y.; Zhao, W.; Xu, Z.P.; Little, P.J.; Whittaker, A.K.; Zhang, R.; Ta, H.T. Novel iron oxide-cerium oxide core-shell nanoparticles as a potential theranostic material for ROS related inflammatory diseases. J Mater Chem B 2018, 6, 4937–4951. [Google Scholar] [CrossRef]
- Turin-Moleavin, I.A.; Fifere, A.; Lungoci, A.L.; Rosca, I.; Coroaba, A.; Peptanariu, D.; Pasca, S.A.; Bostanaru, A.C.; Mares, M.; Pinteala, M. In Vitro and In Vivo Antioxidant Activity of the New Magnetic-Cerium Oxide Nanoconjugates. Nanomaterials (Basel) 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Ali Al Saidi, A.K.; Ghazanfari, A.; Baek, A.; Tegafaw, T.; Ahmad, M.Y.; Zhao, D.; Liu, Y.; Yang, J.U.; Park, J.A.; Yang, B.W.; et al. Ultrasmall cerium oxide nanoparticles as highly sensitive X-ray contrast agents and their antioxidant effect. RSC Adv 2024, 14, 3647–3658. [Google Scholar] [CrossRef] [PubMed]
- Kolmanovich, D.D.; Chukavin, N.N.; Savintseva, I.V.; Mysina, E.A.; Popova, N.R.; Baranchikov, A.E.; Sozarukova, M.M.; Ivanov, V.K.; Popov, A.L. Hybrid Polyelectrolyte Capsules Loaded with Gadolinium-Doped Cerium Oxide Nanoparticles as a Biocompatible MRI Agent for Theranostic Applications. Polymers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- K, K.J.; Kopecky, C.; Koshy, P.; Liu, Y.; Devadason, M.; Holst, J.; K, A.K.; C, C.S. Theranostic Activity of Ceria-Based Nanoparticles toward Parental and Metastatic Melanoma: 2D vs 3D Models. ACS Biomater Sci Eng 2023, 9, 1053–1065. [Google Scholar] [CrossRef]
- Sadidi, H.; Hooshmand, S.; Ahmadabadi, A.; Javad Hosseini, S.; Baino, F.; Vatanpour, M.; Kargozar, S. Cerium Oxide Nanoparticles (Nanoceria): Hopes in Soft Tissue Engineering. Molecules 2020, 25. [Google Scholar] [CrossRef]
- Bhushan, S.; Singh, S.; Maiti, T.K.; Das, A.; Barui, A.; Chaudhari, L.R.; Joshi, M.G.; Dutt, D. Cerium oxide nanoparticles disseminated chitosan gelatin scaffold for bone tissue engineering applications. Int J Biol Macromol 2023, 236, 123813. [Google Scholar] [CrossRef]
- Xiang, J.; Li, J.; He, J.; Tang, X.; Dou, C.; Cao, Z.; Yu, B.; Zhao, C.; Kang, F.; Yang, L.; et al. Cerium Oxide Nanoparticle Modified Scaffold Interface Enhances Vascularization of Bone Grafts by Activating Calcium Channel of Mesenchymal Stem Cells. ACS Appl Mater Interfaces 2016, 8, 4489–4499. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Zhen, C.; Yang, J.; Wang, J.; Wang, S.; Fang, Y.; Shang, P. Recent advances of nanoparticles on bone tissue engineering and bone cells. Nanoscale Advances 2024, 6, 1957–1973. [Google Scholar] [CrossRef]
- Nethi, S.; Nanda, H.S.; T.W.J, S.; Patra, C. Functionalized nanoceria exhibit improved angiogenic properties. Journal of Materials Chemistry B 2017, 5, 9371–9383. [CrossRef]
- Augustine, R.; Dalvi, Y.B.; Dan, P.; George, N.; Helle, D.; Varghese, R.; Thomas, S.; Menu, P.; Sandhyarani, N. Nanoceria Can Act as the Cues for Angiogenesis in Tissue-Engineering Scaffolds: Toward Next-Generation in Situ Tissue Engineering. ACS Biomater Sci Eng 2018, 4, 4338–4353. [Google Scholar] [CrossRef]
- Xiang, H.; Wang, Y.; Chang, H.; Yang, S.; Tu, M.; Zhang, X.; Yu, B. Cerium-containing α-calcium sulfate hemihydrate bone substitute promotes osteogenesis. J Biomater Appl 2019, 34, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.; Azfer, A.; Rogers, L.M.; Wang, X.; Kolattukudy, P.E. Cardioprotective effects of cerium oxide nanoparticles in a transgenic murine model of cardiomyopathy. Cardiovascular Research 2007, 73. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Shen, Q.; Xie, Y.; You, M.; Huang, L.; Zheng, X. Incorporation of Cerium Oxide into Hydroxyapatite Coating Protects Bone Marrow Stromal Cells Against H(2)O(2)-Induced Inhibition of Osteogenic Differentiation. Biol Trace Elem Res 2018, 182, 91–104. [Google Scholar] [CrossRef]
- Zhang, Q.; Ge, K.; Ren, H.; Zhang, C.; Zhang, J. Effects of Cerium Oxide Nanoparticles on the Proliferation, Osteogenic Differentiation and Adipogenic Differentiation of Primary Mouse Bone Marrow Stromal Cells In Vitro. J Nanosci Nanotechnol 2015, 15, 6444–6451. [Google Scholar] [CrossRef]
- Pagliari, F.; Mandoli, C.; Forte, G.; Magnani, E.; Pagliari, S.; Nardone, G.; Licoccia, S.; Minieri, M.; Di Nardo, P.; Traversa, E. Cerium oxide nanoparticles protect cardiac progenitor cells from oxidative stress. ACS Nano 2012, 6, 3767–3775. [Google Scholar] [CrossRef]
- Popov, A.L.; Popova, N.R.; Selezneva, II; Akkizov, A.Y.; Ivanov, V.K. Cerium oxide nanoparticles stimulate proliferation of primary mouse embryonic fibroblasts in vitro. Mater Sci Eng C Mater Biol Appl 2016, 68, 406–413. [CrossRef]
- Pesaraklou, A.; Mahdavi-Shahri, N.; Hassanzadeh, H.; Ghasemi, M.; Kazemi, M.; Mousavi, N.S.; Matin, M.M. Use of cerium oxide nanoparticles: a good candidate to improve skin tissue engineering. Biomed Mater 2019, 14, 035008. [Google Scholar] [CrossRef]
- Gliga, A.R.; Edoff, K.; Caputo, F.; Källman, T.; Blom, H.; Karlsson, H.L.; Ghibelli, L.; Traversa, E.; Ceccatelli, S.; Fadeel, B. Cerium oxide nanoparticles inhibit differentiation of neural stem cells. Scientific Reports 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Ren, Y.; Pan, W.; Yu, Z.; Tong, L.; Li, N.; Tang, B. Fluorescent Nanocomposite for Visualizing Cross-Talk between MicroRNA-21 and Hydrogen Peroxide in Ischemia-Reperfusion Injury in Live Cells and In Vivo. Anal Chem 2016, 88, 11886–11891. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Behera, M.; Mahapatra, C.; Sundaresan, N.R.; Chatterjee, K. Nanostructured polymer scaffold decorated with cerium oxide nanoparticles toward engineering an antioxidant and anti-hypertrophic cardiac patch. Mater Sci Eng C Mater Biol Appl 2021, 118, 111416. [Google Scholar] [CrossRef]
- Rodrigues, M.; Kosaric, N.; Bonham, C.A.; Gurtner, G.C. Wound Healing: A Cellular Perspective. Physiol Rev 2019, 99, 665–706. [Google Scholar] [CrossRef]
- Cano Sanchez, M.; Lancel, S.; Boulanger, E.; Neviere, R. Targeting Oxidative Stress and Mitochondrial Dysfunction in the Treatment of Impaired Wound Healing: A Systematic Review. Antioxidants (Basel) 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Mauro, M.; Crosera, M.; Monai, M.; Montini, T.; Fornasiero, P.; Bovenzi, M.; Adami, G.; Turco, G.; Filon, F.L. Cerium Oxide Nanoparticles Absorption through Intact and Damaged Human Skin. Molecules 2019, 24. [Google Scholar] [CrossRef]
- Chigurupati, S.; Mughal, M.R.; Okun, E.; Das, S.; Kumar, A.; McCaffery, M.; Seal, S.; Mattson, M.P. Effects of cerium oxide nanoparticles on the growth of keratinocytes, fibroblasts and vascular endothelial cells in cutaneous wound healing. Biomaterials 2013, 34, 2194–2201. [Google Scholar] [CrossRef]
- Wu, H.; Li, F.; Wang, S.; Lu, J.; Li, J.; Du, Y.; Sun, X.; Chen, X.; Gao, J.; Ling, D. Ceria nanocrystals decorated mesoporous silica nanoparticle based ROS-scavenging tissue adhesive for highly efficient regenerative wound healing. Biomaterials 2018, 151, 66–77. [Google Scholar] [CrossRef]
- Wang, T.; Li, Y.; Cornel, E.J.; Li, C.; Du, J. Combined Antioxidant-Antibiotic Treatment for Effectively Healing Infected Diabetic Wounds Based on Polymer Vesicles. ACS Nano 2021, 15, 9027–9038. [Google Scholar] [CrossRef]
- Liu, Y.; Su, G.; Zhang, R.; Dai, R.; Li, Z. Nanomaterials-Functionalized Hydrogels for the Treatment of Cutaneous Wounds. Int J Mol Sci 2022, 24. [Google Scholar] [CrossRef]
- Allu, I.; Kumar Sahi, A.; Kumari, P.; Sakhile, K.; Sionkowska, A.; Gundu, S. A Brief Review on Cerium Oxide (CeO2NPs)-Based Scaffolds: Recent Advances in Wound Healing Applications.
- Augustine, R.; Zahid, A.A.; Hasan, A.; Dalvi, Y.B.; Jacob, J. Cerium Oxide Nanoparticle-Loaded Gelatin Methacryloyl Hydrogel Wound-Healing Patch with Free Radical Scavenging Activity. ACS Biomaterials Science & Engineering 2021, 7, 279–290. [Google Scholar]
- Dewberry, L.C.; Niemiec, S.M.; Hilton, S.A.; Louiselle, A.E.; Singh, S.; Sakthivel, T.S.; Hu, J.; Seal, S.; Liechty, K.W.; Zgheib, C. Cerium oxide nanoparticle conjugation to microRNA-146a mechanism of correction for impaired diabetic wound healing. Nanomedicine 2022, 40, 102483. [Google Scholar] [CrossRef] [PubMed]
- Sener, G.; Hilton, S.A.; Osmond, M.J.; Zgheib, C.; Newsom, J.P.; Dewberry, L.; Singh, S.; Sakthivel, T.S.; Seal, S.; Liechty, K.W.; et al. Injectable, self-healable zwitterionic cryogels with sustained microRNA - cerium oxide nanoparticle release promote accelerated wound healing. Acta Biomater 2020, 101, 262–272. [Google Scholar] [CrossRef]
- Pandey, S.; Kumari, S.; Manohar Aeshala, L.; Singh, S. Investigating temperature variability on antioxidative behavior of synthesized cerium oxide nanoparticle for potential biomedical application. J Biomater Appl 2024, 38, 866–874. [Google Scholar] [CrossRef]
- He, S.; Li, Z.; Wang, L.; Yao, N.; Wen, H.; Yuan, H.; Zhang, J.; Li, Z.; Shen, C. A nanoenzyme-modified hydrogel targets macrophage reprogramming-angiogenesis crosstalk to boost diabetic wound repair. Bioactive Materials 2024, 35, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Ding, J.; Qin, M.; Wang, L.; Jiang, D.; Zhao, J.; Wang, D.; Jia, W. Enhanced ·OH-Scavenging Activity of Cu-CeO(x) Nanozyme via Resurrecting Macrophage Nrf2 Transcriptional Activity Facilitates Diabetic Wound Healing. Adv Healthc Mater 2024, 13, e2303229. [Google Scholar] [CrossRef]
- Zuhrotun, A.; Oktaviani, D.J.; Hasanah, A.N. Biosynthesis of Gold and Silver Nanoparticles Using Phytochemical Compounds. Molecules 2023, 28. [Google Scholar] [CrossRef]
- Allawadhi, P.; Khurana, A.; Allwadhi, S.; Joshi, K.; Packirisamy, G.; Bharani, K.K. Nanoceria as a possible agent for the management of COVID-19. Nano Today 2020, 35, 100982. [Google Scholar] [CrossRef]
- Rajeshkumar, S.; Naik, P. Synthesis and biomedical applications of Cerium oxide nanoparticles – A Review. Biotechnology Reports 2018, 17, 1–5. [Google Scholar] [CrossRef]
- Yokel, R.A.; Hussain, S.; Garantziotis, S.; Demokritou, P.; Castranova, V.; Cassee, F.R. The Yin: An adverse health perspective of nanoceria: uptake, distribution, accumulation, and mechanisms of its toxicity. Environ Sci Nano 2014, 1, 406–428. [Google Scholar] [CrossRef] [PubMed]
- Soo Choi, H.; Liu, W.; Misra, P.; Tanaka, E.; Zimmer, J.P.; Itty Ipe, B.; Bawendi, M.G.; Frangioni, J.V. Renal clearance of quantum dots. Nature Biotechnology 2007, 25, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Younis, A.; Chu, D.; Li, S. Cerium Oxide Nanostructures and their Applications. InTech: 2016.
Figure 1.
A depiction of how various immune cells interact through cytokine signaling and molecular communication pathways. Reproduced with permission from [5]. Copyright, 2021, Elsevier.
Figure 1.
A depiction of how various immune cells interact through cytokine signaling and molecular communication pathways. Reproduced with permission from [5]. Copyright, 2021, Elsevier.
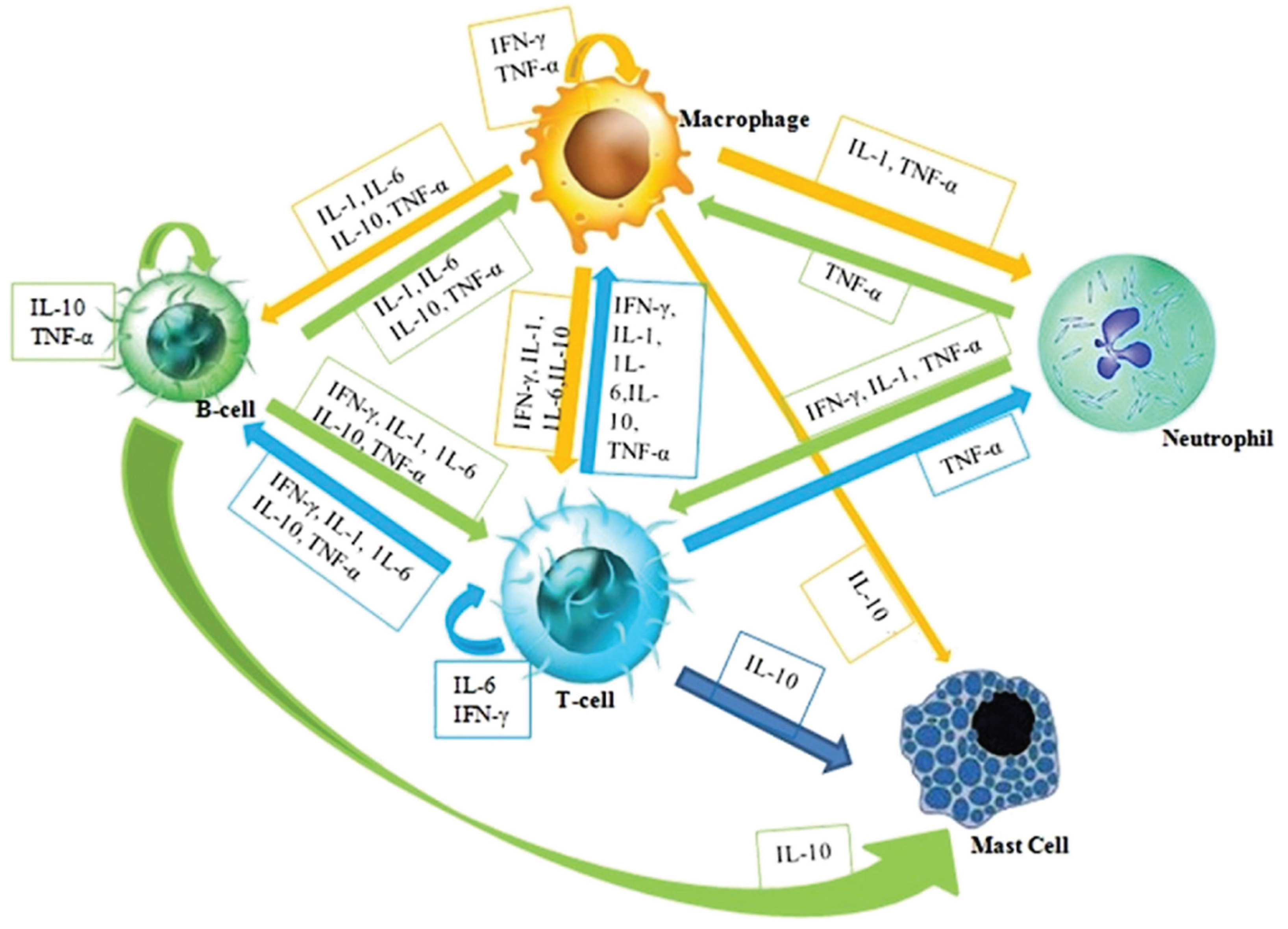
Figure 2.
Overview of major nanoparticle-based immunotherapeutic strategies, categorized by mechanism of action. (A) Drug delivery systems utilizing nanoparticles such as polymeric nanocapsules, mesoporous silica, and liposomes encapsulating therapeutic agents. (B) Thermal-based therapies, including magnetic hyperthermia (via superparamagnetic nanoparticles (SPION) activated by magnetic fields) and photothermal therapy (using Prussian blue nanoparticle (PBNP) activated by laser light to induce cell death). (C) Immunostimulatory liposomes with surface and/or core modifications for targeted delivery of immune-activating agents. (D) Nanozymes—engineered nanoparticles with intrinsic enzymatic activity employed for enzyme replacement or reactive species scavenging to modulate the immune microenvironment.
Figure 2.
Overview of major nanoparticle-based immunotherapeutic strategies, categorized by mechanism of action. (A) Drug delivery systems utilizing nanoparticles such as polymeric nanocapsules, mesoporous silica, and liposomes encapsulating therapeutic agents. (B) Thermal-based therapies, including magnetic hyperthermia (via superparamagnetic nanoparticles (SPION) activated by magnetic fields) and photothermal therapy (using Prussian blue nanoparticle (PBNP) activated by laser light to induce cell death). (C) Immunostimulatory liposomes with surface and/or core modifications for targeted delivery of immune-activating agents. (D) Nanozymes—engineered nanoparticles with intrinsic enzymatic activity employed for enzyme replacement or reactive species scavenging to modulate the immune microenvironment.
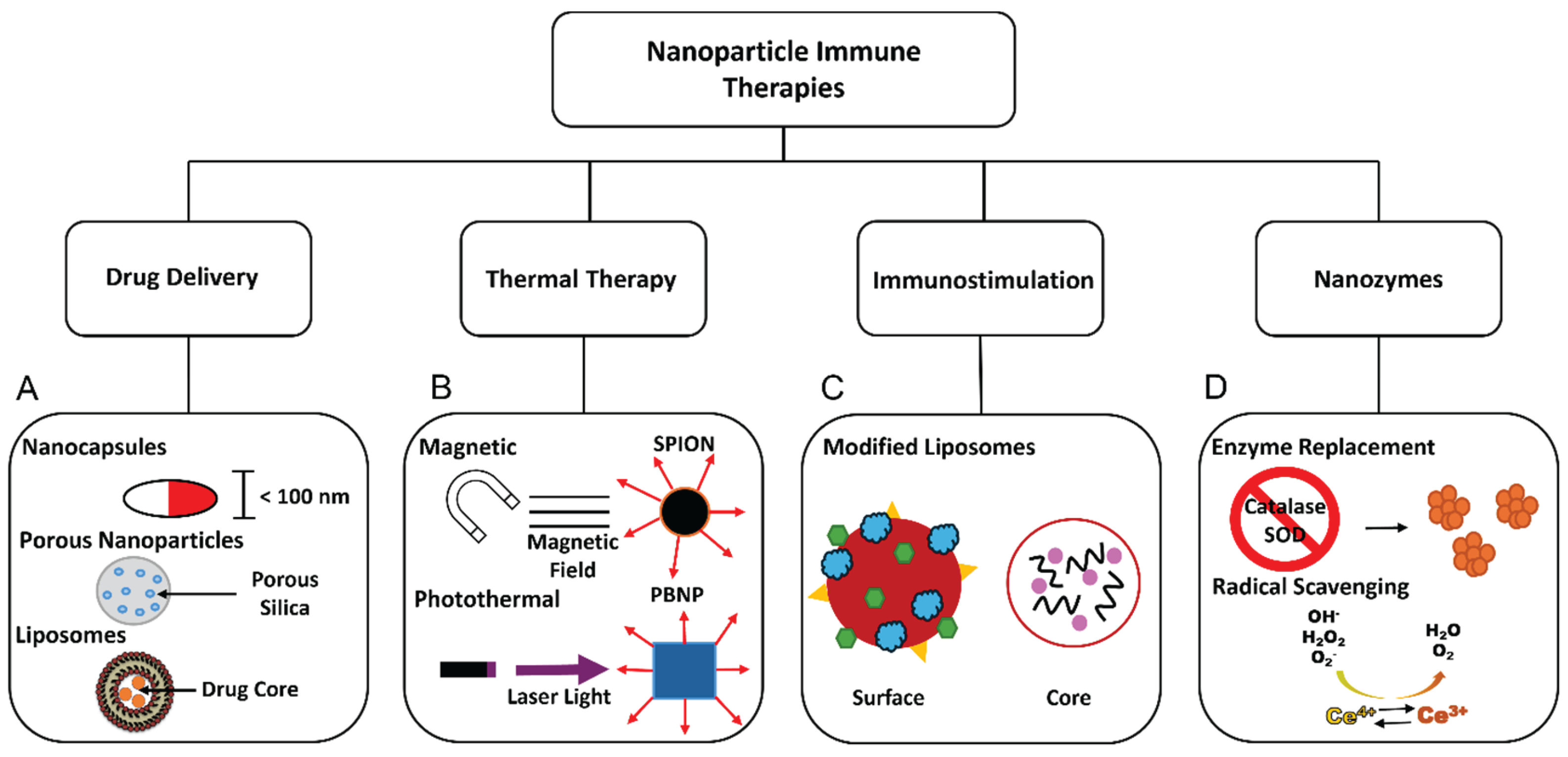
Figure 3.
Fluorescently labelled nanoceria. (A) Emission spectra for CruzFluor fluorophore labeled nanoceria. (B) Time-dependent cellular uptake of nanoceria observed within the first 1–3 hours of incubation. Cells were treated with nanoceria in PBS for 1 hour (ii), 3 hours (iii), and 6 hours (iv). Nuclei were counterstained with DAPI. Control cells not exposed to nanoceria (i) exhibited no significant fluorescence signals. Scale bar 50 μm. (C) Synthetic route for conjugation of nanoceria with Rhodamine B. (D) Confocal microscopy analysis of RhB-nanoceria uptake in HeLa cells following 3-hour incubation. Live-cell z-stack images (a–d) illustrate nanoparticle distribution. (E) Merged brightfield and fluorescence images reveal cytoplasmic staining with N-acridine orange (NAO), emitting green fluorescence. (E) Single-cell views highlight green fluorescence from SYTO80-labeled nucleic acids, while the red signal corresponds to the intrinsic fluorescence of RhB-nanoceria. (a–f) represents live-cell z-stack images. (F) Evaluation of the impact of nanoceria and RhB-nanoceria (both at 20 μg/mL) on rotenone-induced reactive oxygen species (ROS) generation in HeLa cells. Bar graphs depict DCFH fluorescence intensity as a measure of ROS levels across varying concentrations of rotenone. Data are presented as mean ± SEM from three independent experiments (n = 3) and analyzed using one-way ANOVA. Statistical significance compared to untreated control cells is indicated as *p < 0.05 and p < 0.01. Reproduced with permission from [103,104]. Copyright 2010 and 2015, RSC publishers.
Figure 3.
Fluorescently labelled nanoceria. (A) Emission spectra for CruzFluor fluorophore labeled nanoceria. (B) Time-dependent cellular uptake of nanoceria observed within the first 1–3 hours of incubation. Cells were treated with nanoceria in PBS for 1 hour (ii), 3 hours (iii), and 6 hours (iv). Nuclei were counterstained with DAPI. Control cells not exposed to nanoceria (i) exhibited no significant fluorescence signals. Scale bar 50 μm. (C) Synthetic route for conjugation of nanoceria with Rhodamine B. (D) Confocal microscopy analysis of RhB-nanoceria uptake in HeLa cells following 3-hour incubation. Live-cell z-stack images (a–d) illustrate nanoparticle distribution. (E) Merged brightfield and fluorescence images reveal cytoplasmic staining with N-acridine orange (NAO), emitting green fluorescence. (E) Single-cell views highlight green fluorescence from SYTO80-labeled nucleic acids, while the red signal corresponds to the intrinsic fluorescence of RhB-nanoceria. (a–f) represents live-cell z-stack images. (F) Evaluation of the impact of nanoceria and RhB-nanoceria (both at 20 μg/mL) on rotenone-induced reactive oxygen species (ROS) generation in HeLa cells. Bar graphs depict DCFH fluorescence intensity as a measure of ROS levels across varying concentrations of rotenone. Data are presented as mean ± SEM from three independent experiments (n = 3) and analyzed using one-way ANOVA. Statistical significance compared to untreated control cells is indicated as *p < 0.05 and p < 0.01. Reproduced with permission from [103,104]. Copyright 2010 and 2015, RSC publishers.
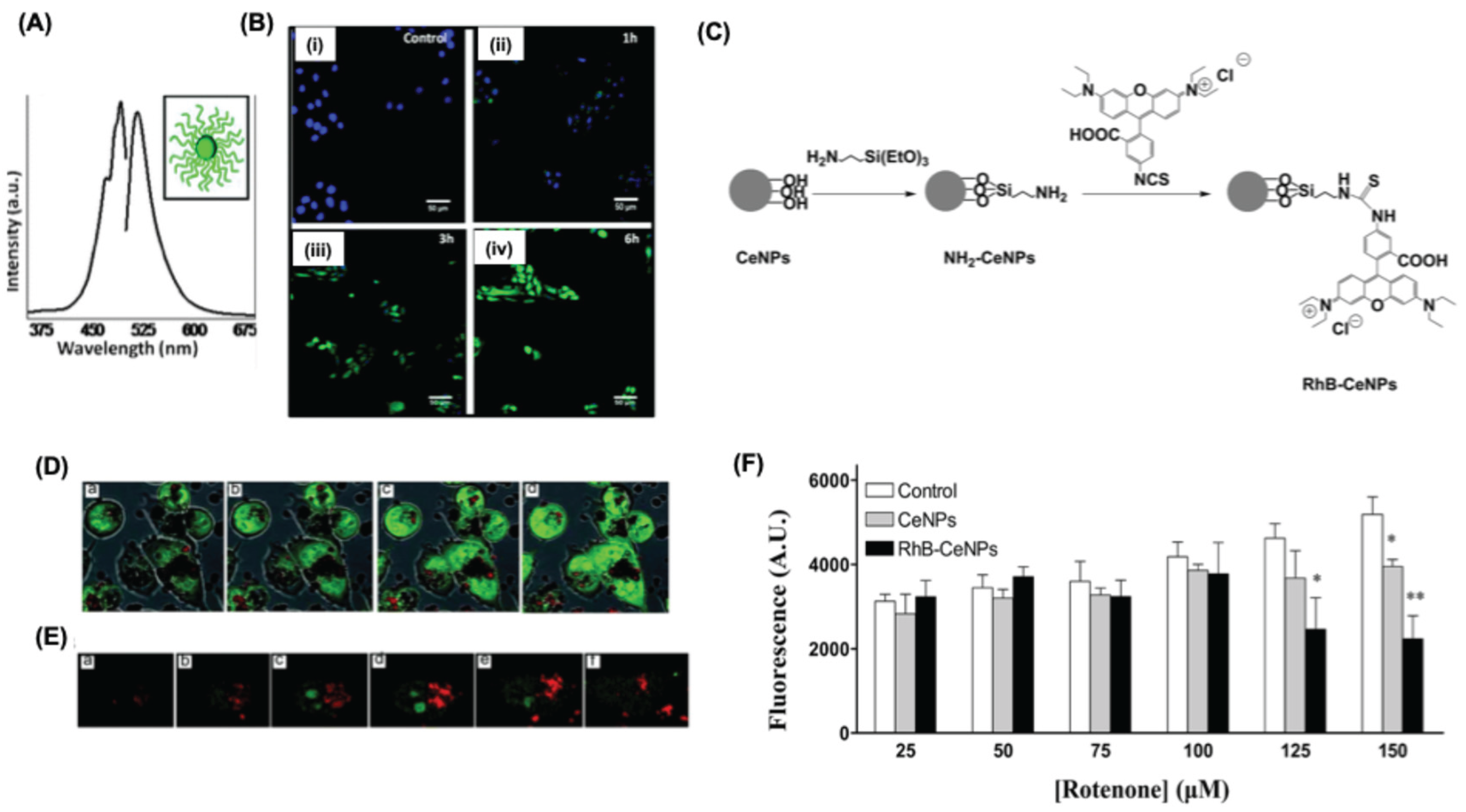
Scheme 1.
(A) A schematic representation of dynamic seesaw-like model of nanoceria and different enzyme-mimicking activities by ceria-based nanozymes. (B) Schematic representation of the SOD-mimetic mechanism of nanoceria: (C) The mechanism involves several redox steps at the nanoparticle surface: ① Oxygen vacancies present on the nanoceria surface act as active sites; ②H₂O₂ binds to surface Ce⁴⁺ sites; ③ This interaction leads to proton release and electron transfer, reducing Ce⁴⁺ to Ce³⁺; ④ Molecular oxygen (O₂) is subsequently released from the reduced vacancy site; ⑤ A superoxide (O₂⁻) radical binds to the exposed oxygen vacancy; ⑥ The radical undergoes dismutation to form H₂O₂, which is released from the surface. ⑦ A second superoxide anion binds and completes the redox cycle, mimicking native superoxide dismutase (SOD) activity by converting reactive oxygen species (ROS) into less harmful products. (D) Illustrated mechanisms of catalase-like activity by nanoceria: The steps involved in the oxidation reactions follow the same order as shown in Figure 3b (steps ① to ④). Step ⑤ represents the interaction of hydrogen peroxide (H₂O₂) with a site containing two Ce³⁺ ions, while step ⑥ denotes the uptake of two protons during the process. (E) Reaction pathway for peroxidase catalysis using nanoceria. Reproduced with permission from [113]. Copyright, 2023, American Chemical Society.
Scheme 1.
(A) A schematic representation of dynamic seesaw-like model of nanoceria and different enzyme-mimicking activities by ceria-based nanozymes. (B) Schematic representation of the SOD-mimetic mechanism of nanoceria: (C) The mechanism involves several redox steps at the nanoparticle surface: ① Oxygen vacancies present on the nanoceria surface act as active sites; ②H₂O₂ binds to surface Ce⁴⁺ sites; ③ This interaction leads to proton release and electron transfer, reducing Ce⁴⁺ to Ce³⁺; ④ Molecular oxygen (O₂) is subsequently released from the reduced vacancy site; ⑤ A superoxide (O₂⁻) radical binds to the exposed oxygen vacancy; ⑥ The radical undergoes dismutation to form H₂O₂, which is released from the surface. ⑦ A second superoxide anion binds and completes the redox cycle, mimicking native superoxide dismutase (SOD) activity by converting reactive oxygen species (ROS) into less harmful products. (D) Illustrated mechanisms of catalase-like activity by nanoceria: The steps involved in the oxidation reactions follow the same order as shown in Figure 3b (steps ① to ④). Step ⑤ represents the interaction of hydrogen peroxide (H₂O₂) with a site containing two Ce³⁺ ions, while step ⑥ denotes the uptake of two protons during the process. (E) Reaction pathway for peroxidase catalysis using nanoceria. Reproduced with permission from [113]. Copyright, 2023, American Chemical Society.

Figure 4.
Application of nanoceria for Rheumatoid Arthritis. (A) A pictorial representation for the albumin-nanoceria and its visual appearance. (B) Assessment of the therapeutic efficacy of Albumin-nanoceria in CIA mice through clinical scoring over a 3-week period (N = 6). Mice treated with Albumin-nanoceria (50 µL, blue line) exhibited an average clinical score of 4.8 ± 1.1, comparable to the methotrexate (MTX) group (50 µL, yellow line), and significantly lower by approximately 2.4-fold than the PBS control group (black line). The inset displays representative images of paw inflammation used for scoring. Error bars represent the standard error of the mean (SEM); statistical significance indicated as *p < 0.05, *p < 0.005 versus PBS control. (C) Fluorescence images of tissue sections from PBS and Albumin-nanoceria-treated mice show high macrophage infiltration (CD11b, red) in inflamed paws (DAPI, blue). Albumin-nanoceria treatment reduced pro-inflammatory M1 macrophages (iNOS, pink) and increased anti-inflammatory M2 macrophages (Arg-1, yellow). The lower panel represents quantified fluorescence signals of CD11b, iNOS, and Arg-1 across 25 ROIs (5 images from two mice per group; error bars = SD; ***p < 0.0005). (D) Mean fluorescence intensity data for THP-1 cells treated with albumin nanoceria. The Albumin-nanoceria treated cells showed lower CD80 than samples treated with IL4/IL13 (N = 3, error bars = SD, p-value: *p < 0.05). (E) A schematic representation and therapeutical application of manganese dopped nanoceria for RA. Reproduced with permission from [68,152]. Copy right 2020, Ivy spring Publishers. 2024, Springer publishers.
Figure 4.
Application of nanoceria for Rheumatoid Arthritis. (A) A pictorial representation for the albumin-nanoceria and its visual appearance. (B) Assessment of the therapeutic efficacy of Albumin-nanoceria in CIA mice through clinical scoring over a 3-week period (N = 6). Mice treated with Albumin-nanoceria (50 µL, blue line) exhibited an average clinical score of 4.8 ± 1.1, comparable to the methotrexate (MTX) group (50 µL, yellow line), and significantly lower by approximately 2.4-fold than the PBS control group (black line). The inset displays representative images of paw inflammation used for scoring. Error bars represent the standard error of the mean (SEM); statistical significance indicated as *p < 0.05, *p < 0.005 versus PBS control. (C) Fluorescence images of tissue sections from PBS and Albumin-nanoceria-treated mice show high macrophage infiltration (CD11b, red) in inflamed paws (DAPI, blue). Albumin-nanoceria treatment reduced pro-inflammatory M1 macrophages (iNOS, pink) and increased anti-inflammatory M2 macrophages (Arg-1, yellow). The lower panel represents quantified fluorescence signals of CD11b, iNOS, and Arg-1 across 25 ROIs (5 images from two mice per group; error bars = SD; ***p < 0.0005). (D) Mean fluorescence intensity data for THP-1 cells treated with albumin nanoceria. The Albumin-nanoceria treated cells showed lower CD80 than samples treated with IL4/IL13 (N = 3, error bars = SD, p-value: *p < 0.05). (E) A schematic representation and therapeutical application of manganese dopped nanoceria for RA. Reproduced with permission from [68,152]. Copy right 2020, Ivy spring Publishers. 2024, Springer publishers.
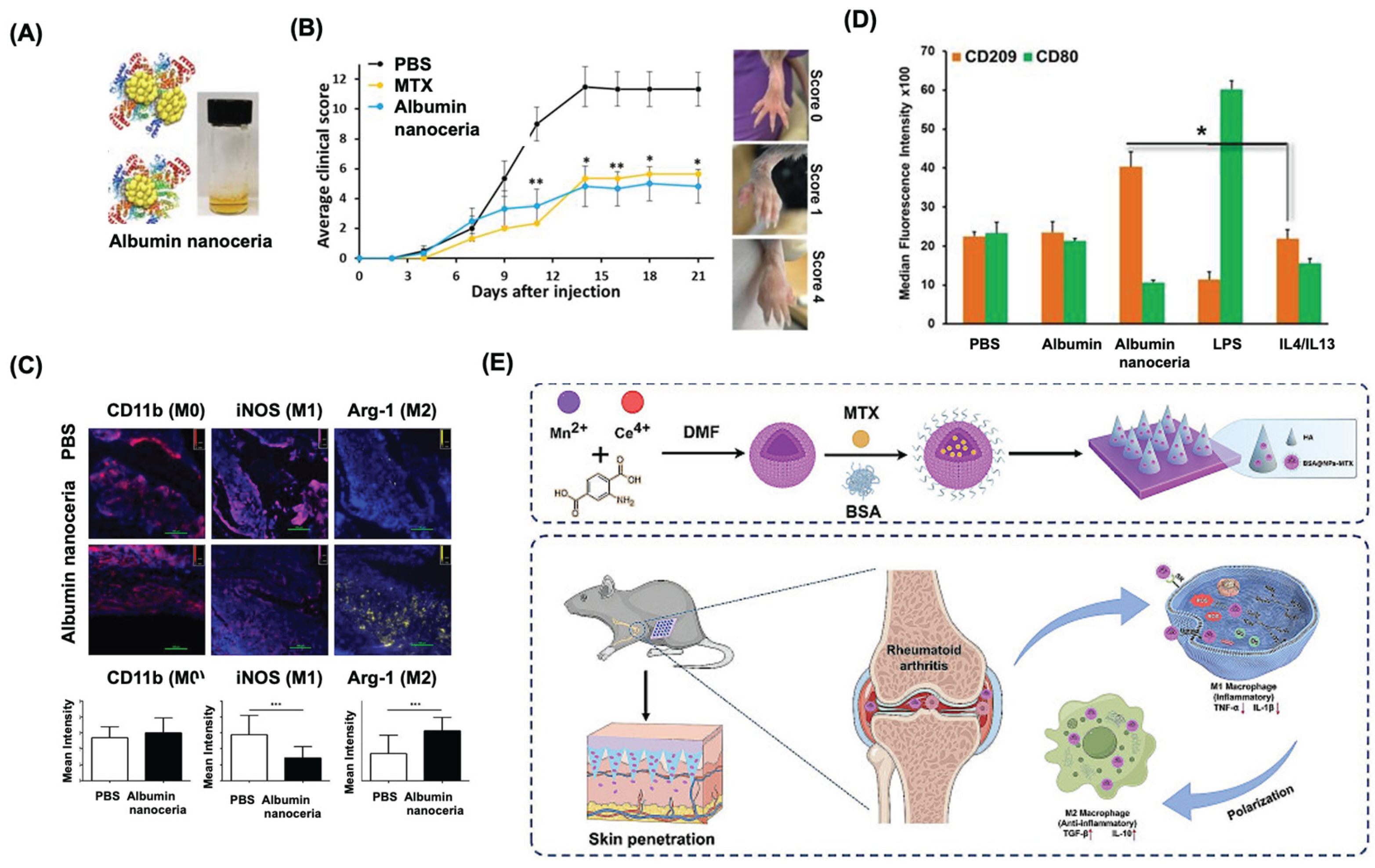
Figure 5.
Immunotherapy applications of nanoceria. (A) A schematic representation and catalytic activity of porous nanoceria (PN-CeO2). (B) tumor volume from the non-treated and treated mice (PN-CeO2 and sodium polystyrene sulfonate (PSS) coated PN-CeO2) after 20 days of treatment. *p < 0.05 and ***p < 0.001. Inset represents the Ex vivo images for the tumor for the non-treated and treated mice. (C) H&E staining, ROS staining and TUNEL staining for pathological changes of tumor tissues of each group after the 20-day treatments. All scale bars are 100 µm. (D) A pictorial representation for the theranostic application of albumin-nanoceria with indocyanine green (ICG) for non-invasive detection of endometriosis. (E) represents the photoacoustic and fluorescence microscopic images for mice injected with albumin-Ce-ICG nanoparticles. The arrows indicate the endometrial lesions in the mice. (F) Representative ex vivo images of uteri with implantation sites of treatment groups at gestation day 5.5. (Scale bar = 1 cm). (G) A graphical representation for the implantation sites for non-treated, albumin-nanoceria treated and Tofactinib treated mice uterine horns. A statistically significant reduction in implantation sites between vehicle treated and tofacitinib treated mice were observed but not between vehicle and albumin-nanoceria treated cells showing that albumin-nanoceria does not influence fertility (n=6) (*** p<0.001). Reproduced with permission from [158,163]. Copyright 2020, Springer publishers.; 2025, Elsevier respectively.
Figure 5.
Immunotherapy applications of nanoceria. (A) A schematic representation and catalytic activity of porous nanoceria (PN-CeO2). (B) tumor volume from the non-treated and treated mice (PN-CeO2 and sodium polystyrene sulfonate (PSS) coated PN-CeO2) after 20 days of treatment. *p < 0.05 and ***p < 0.001. Inset represents the Ex vivo images for the tumor for the non-treated and treated mice. (C) H&E staining, ROS staining and TUNEL staining for pathological changes of tumor tissues of each group after the 20-day treatments. All scale bars are 100 µm. (D) A pictorial representation for the theranostic application of albumin-nanoceria with indocyanine green (ICG) for non-invasive detection of endometriosis. (E) represents the photoacoustic and fluorescence microscopic images for mice injected with albumin-Ce-ICG nanoparticles. The arrows indicate the endometrial lesions in the mice. (F) Representative ex vivo images of uteri with implantation sites of treatment groups at gestation day 5.5. (Scale bar = 1 cm). (G) A graphical representation for the implantation sites for non-treated, albumin-nanoceria treated and Tofactinib treated mice uterine horns. A statistically significant reduction in implantation sites between vehicle treated and tofacitinib treated mice were observed but not between vehicle and albumin-nanoceria treated cells showing that albumin-nanoceria does not influence fertility (n=6) (*** p<0.001). Reproduced with permission from [158,163]. Copyright 2020, Springer publishers.; 2025, Elsevier respectively.
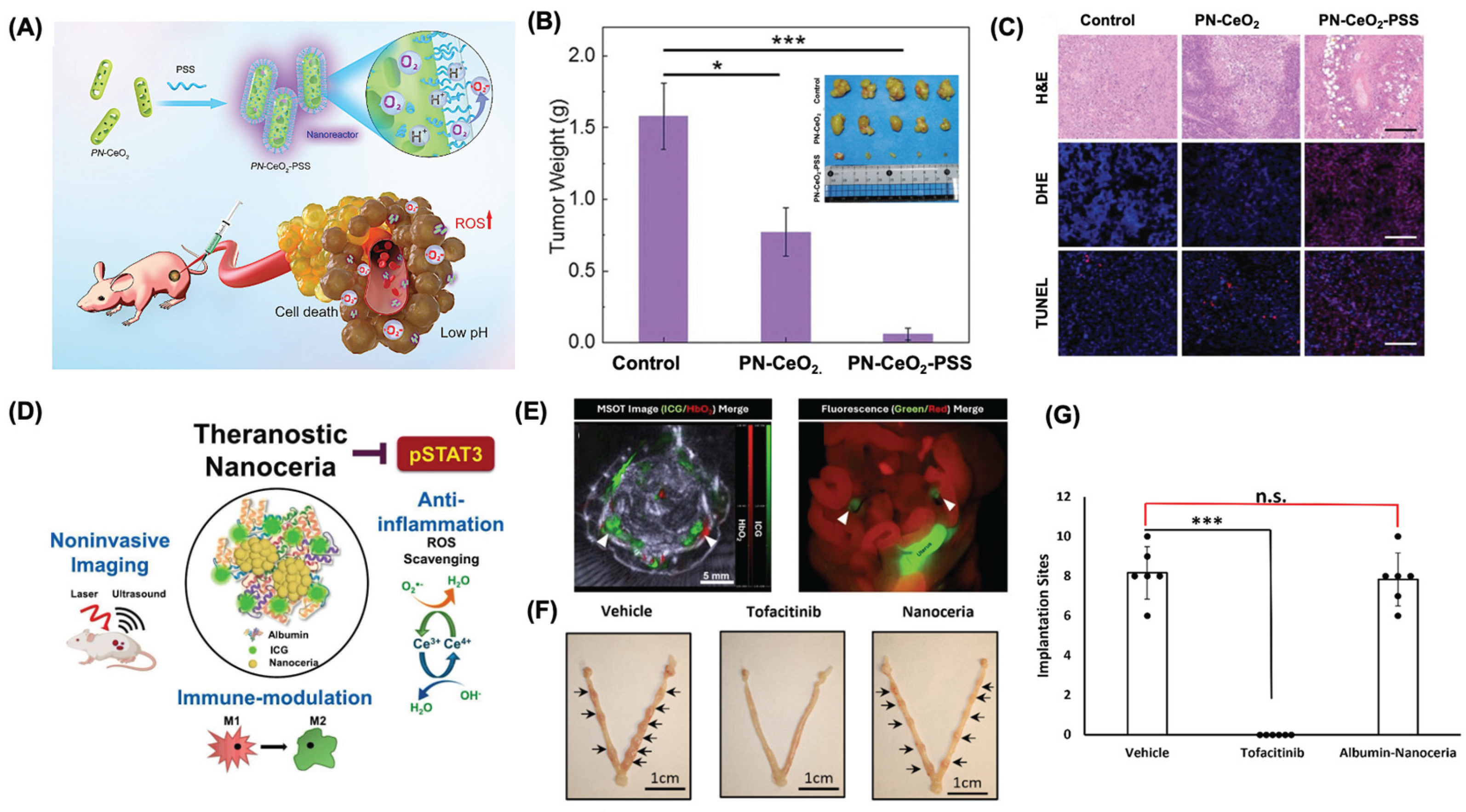
Figure 6.
(A) A schematic showing the SOD type activity for nanoceria. Cerium oxide exhibits regenerative antioxidant behavior by alternating between Ce³⁺ and Ce⁴⁺ states scavenging superoxide radicals as Ce³⁺ and neutralizing H₂O₂ as Ce⁴⁺. (B) A structural model illustrates iron oxide–cerium oxide core–shell nanoparticles (IO@CO). (C) MRI relaxation profile for non-treated and IO@CO treated macrophage cells. Treated cells with IO@CO1 and IO@CO2 showed a higher relaxation rate than untreated controls. ***P < 0.001. (D) MRI images revealed stronger dark signals in nanoparticle-treated cells, especially with IO@CO2 than untreated cells. (E) ROS scavenging ability of IO@CO NPs. ROS levels decreased significantly when cerium concentration reached 14 ng/100 μL or more than control. **P < 0.01, ***P < 0.001 (F) Fluorescence imaging confirmed reduced oxidative stress, as nanoparticle-treated cells emitted lower green fluorescence compared to H₂O₂-treated cells. Scale bar 200 μm. (G) In vivo CT images of the mice bladder before and after intravenous (IV) and intraperitoneal (IP) injections of an aqueous suspension sample of PAA-coated ultrasmall CeO2 nanoparticles at 70 kVp. The dotted circles at the bladder indicate the region of interest (ROI). (H) Contrast plots of the SNR-ROI of the bladder as a function of time. Reproduced with permission from [175,177]. Copyright, 2018, 2023, RSC publishing group.
Figure 6.
(A) A schematic showing the SOD type activity for nanoceria. Cerium oxide exhibits regenerative antioxidant behavior by alternating between Ce³⁺ and Ce⁴⁺ states scavenging superoxide radicals as Ce³⁺ and neutralizing H₂O₂ as Ce⁴⁺. (B) A structural model illustrates iron oxide–cerium oxide core–shell nanoparticles (IO@CO). (C) MRI relaxation profile for non-treated and IO@CO treated macrophage cells. Treated cells with IO@CO1 and IO@CO2 showed a higher relaxation rate than untreated controls. ***P < 0.001. (D) MRI images revealed stronger dark signals in nanoparticle-treated cells, especially with IO@CO2 than untreated cells. (E) ROS scavenging ability of IO@CO NPs. ROS levels decreased significantly when cerium concentration reached 14 ng/100 μL or more than control. **P < 0.01, ***P < 0.001 (F) Fluorescence imaging confirmed reduced oxidative stress, as nanoparticle-treated cells emitted lower green fluorescence compared to H₂O₂-treated cells. Scale bar 200 μm. (G) In vivo CT images of the mice bladder before and after intravenous (IV) and intraperitoneal (IP) injections of an aqueous suspension sample of PAA-coated ultrasmall CeO2 nanoparticles at 70 kVp. The dotted circles at the bladder indicate the region of interest (ROI). (H) Contrast plots of the SNR-ROI of the bladder as a function of time. Reproduced with permission from [175,177]. Copyright, 2018, 2023, RSC publishing group.
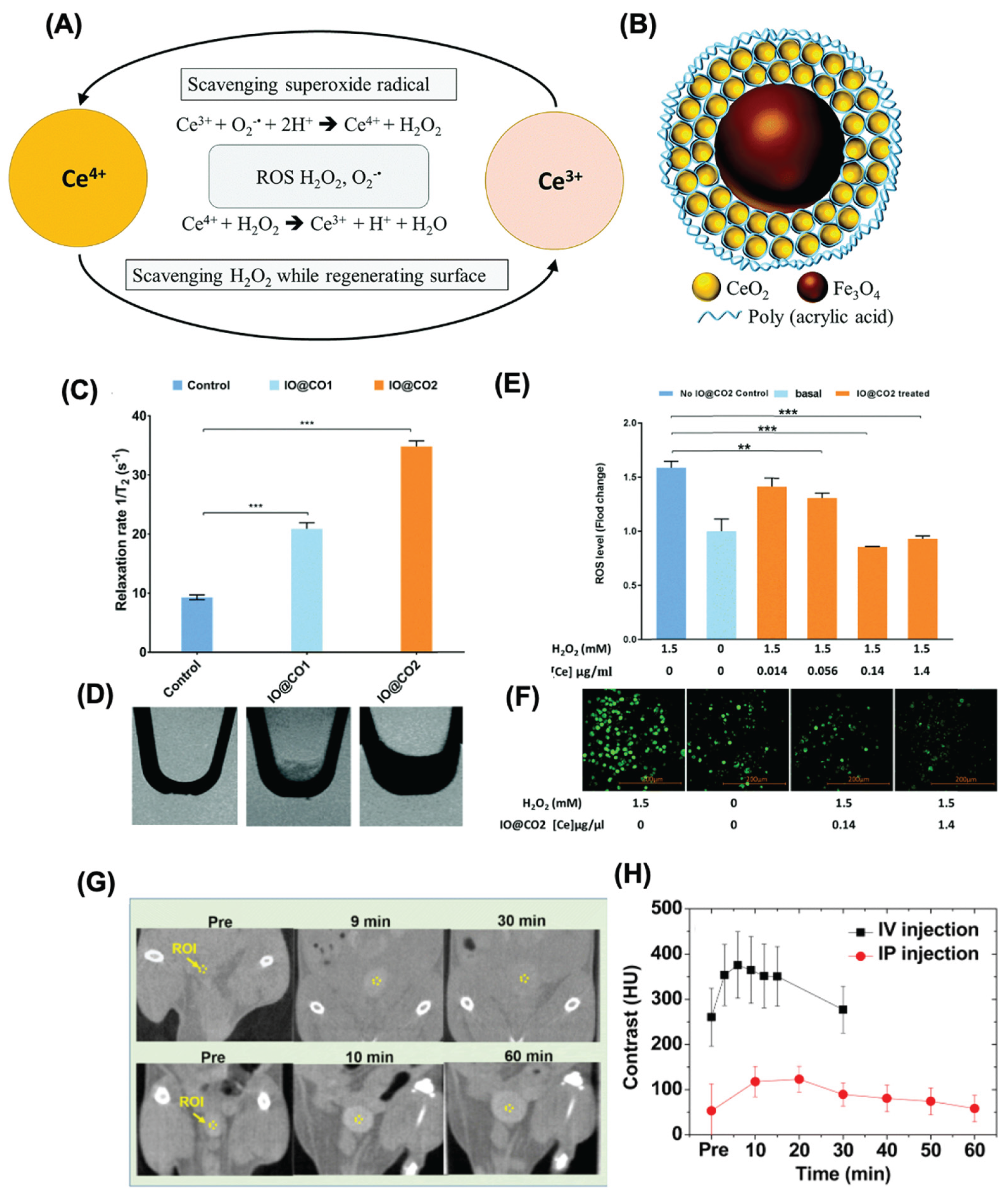
Table 1.
A list of various existing treatment methods for immune mediated conditions.
| Treatment | Non-Steroidal Anto-inflammatory Drugs (NSAIDs) | Steroids (Corticosteroids) | Opioid Pain Killers | Adjuvants | Immunotherapy |
|---|---|---|---|---|---|
| Pros | Simple to access; Very effective short term; Low cost | Available in many formulations; Well-characterized mechanism; Effective short and long-term | Do not interfere with healthy inflammation; Prevents shock and, in some cases, death from trauma; Work with anti-inflammatories | Simple mechanism; Common ; Many available |
Highly tunable; Useful for many diseases; Can treat away from site of administration |
| Cons | High doses cause side effects; Possible overdose; Can cause more inflammation | Prolonged use results in severe side effects; Rare side effects make them unusable for some patients | Not anti-inflammatory; Highly addictive; Inadequate for chronic conditions | Must be administered directly to the site of interest; Limited effects; Low tunability | Long timeframes; Unpredictable side effects; Limited efficacy |
| Examples | Ibuprofen (Advil) Naproxen (Aleve) Acetylsalicylic acid (Aspirin) |
Hydrocortisone Prednisone Beclomethasone |
Oxycodone Hydrocodone Morphine |
Aluminum salts Virosomes |
Allergy shots; Type-1 Diabetes Delay; Reversal of tumor immune privilege |
Table 2.
List of various nanoparticles and formulations used for inflammation studies.
| Nanomaterials | Size | Dose | Outcome | Cytokines/Chemokines | In vivo/In Vitro | Ref |
|---|---|---|---|---|---|---|
| MWCNT | L: 5–15 μm; D: 10–20 nm | Inhalation 5 mg/m3 | Immunosuppression | TGFβ↑, IL-10↑ | Male C57BL/6 | [72,73] |
| SWCNT | L: 1–3 μm; D: 1–4 nm | Pharyngeal aspiration 40-120 μg/mouse | Inflammation immunosuppression | TNF-α↑, IL-6↑, MCP1↑ | BALB/c C57BL/6 | [74] |
| SWCNT | L: 3–30 μm; D: 67 nm | Intratracheal 25, 50 μg | Allergic inflammation | IL-4↑, IL-5↑, IL-13↑, IFN-γ↑ | Male mice ICR | [75] |
| MWCNT | L: 15 ± 5 μm D: 25 ± 5 nm |
Intravenously 1 mg/kg | Inflammation | IL-4↑, IL-33↑ | C57BL/6 | [76] |
| Graphene | 4 ± 1 μm2 area | Intravenously 1 mg/kg | Th2 immune response | IL-33↑, IL-5↑, IL-13↑ | C57BL/6 | [76] |
| Fullerene C60 | N/A | Intravenously 50 ng/mouse | Immunosuppression | Serum histamine↓, Lyn↓, Syk↓, ROS↓ | C57BL/6 | [77] |
| Carboxyfullerene | NA | Peritoneum and air pouch 40 mg/kg | Activate immune system | NA | C57BL/6 | [78] |
| PEG coated AuNP | 13 nm | Intravenously 0-4.26 mg/kg | Acute inflammation | MCP-1/CCL-2↑, | BALB/c | [79] |
| PfMSP-119/PvMSP-119 coated AuNPs | 17 nm | Subcutaneously 25 μg/mouse | Poor immunogenic | N/A | BALB/c | [80] |
| Citrate-stabilized AuNPs | 40 nm | Oropharyngeal aspiration 0.8 mg/kg | Hypersensitivity | MMP-9↑, MIP-2↑, TNF-α↓, IL-6↓ | TDI-sensitised mice (BALB/c) | [81] |
| AgNPs | 22.18 ± 1.72 nm | Inhalation of particles/cm3 | Immunosuppression | Malt1 gene↓, Sema7a gene↓ | C57BL/6 | [82] |
| AgNPs | 52.25 ± 23.64 nm | Intratracheal instillation 3.5 or 17.5 mg/kg | Enhance immune function | IL-1↑, IL-6↑, TNF-α↑, GSH↓, NO↑ | Wistar rats | [83] |
| FeONP | 43 nm | Intratracheal instillation (4 or 20 μg × 3) | Activate immune response | IFN-γ↑, IL-4↑ | OVA-BALB/c | [84,85] |
| FeONP | 58.7 nm | Intravenously ≤10 mg iron/kg | Immunosuppression | IFN-γ↓, IL-6↓, TNF-α↓ | DTH mice | [86] |
| FeONP | 35 ± 14 nm | Intratracheally 500 μg/mouse | Immunosuppression | IgE↓, IL-4↓ | OVA-BALB/c | [87] |
| Nanoceria | D: 8 nm | Oropharyngeal instillation of 10-100 μg/mouse | Inflammation | TNF-α↑, IL-6↑, osteopontin↑ | C57BL/6 | [88] |
| Nanoceria | D: 55 nm | Inhalation of 641 mg/m3 | Inflammation | IL-1β↑, TNF-α↑, IL-6↑, MDA↑, GSH↓ | Wistar rats | [89] |
| Liposomal doxorubicin (Doxil) | 85–100 nm | Infuse in accordance with Doxil | Hypersensitivity reactions | NA | Patients with solid tumors | [90] |
| Polystyrene NP | 50 nm | Intratracheal 200 μg/mouse | Anti-inflammation immunosuppression | IL-4↓, IL-5↓, IL-13↓ | Allergen challenge mice | [91] |
Abbreviations: MWCNT: Multiwalled carbon nanotube; SWCNT: Single-walled carbon nanotube; L: Length; D: Diameter; FeONP: Iron oxide nanoparticles; AuNPs: gold nanoparticles; AgNPs: Silver nanoparticles. NA: Not reported.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



