Submitted:
26 June 2025
Posted:
30 June 2025
You are already at the latest version
Abstract
Background/Objectives: Pacinian corpuscles are end organs complexes associated with rapidly adapting low-threshold mechanoreceptors abundant in the human hand. Pathological conditions involving Pacinian corpuscles are rare and normally appear as subcutaneous painful nodules. Diagnostics of those pathologies is usually throughout cutaneous biopsy. This study aimed to investigate whether human hand Pacinian corpuscles can be visualized using non-invasive high-resolution ultrasound. Methods: Five adult subjects were evaluated using high-resolution ultrasound following the digital nerves in the palm, and Pacinian corpuscles were identified based on their localization and morphology. Moreover, a structural, immunohistochemical, immunofluorescence associated with confocal laser microscopy and optic-densitometry was performed in palm cutaneous samples (n = 5) from the same areas as in ultrasonographic study. Results: Pacinian corpuscles were visualized within the intermetacarpal fat pads between flexor tendons and dorsal to the neurovascular bundles. They appeared as subcutaneous, oval, hypoechoic structures with an echogenic central structure which correspond, structurally, to the inner core and the outer capsule core, as demonstrated by immunohistochemistry and immunofluorescence associated with confocal laser microscopy and optical densitometry. Conclusions: Pacinian corpuscles can be identified, visualized, and counted in the human hand using high-resolution ultrasound. Furthermore, the neural and non-neural compartments of these corpuscles can be distinguished. Present results open the possibility of carrying out mapping studies of the Pacinian corpuscles of the hand as well as analyzing their size and structure under normal and pathological conditions.
Keywords:
pacinian corpuscles
; high-resolution ultrasound
; human hand
1. Introduction
The glabrous skin of the palm and fingers is richly innervated by mechanoreceptors and nociceptors whose somas are placed in the dorsal root ganglia of the roots of the brachial plexus [1,2,3]. Low-threshold mechanoreceptors (LTMRs) terminate in the dermis and hypodermis associated with glial, endoneurial, and perineurial cells to form different morphotypes of sensory corpuscles or cutaneous end-organ complexes (CEOCs) [4,5,6]. Among CEOCs are Pacinian corpuscles, which are large ovoid structures present in most organs and tissues, including the deep dermis and hypodermis, and have a typical “onion bulb” appearance [7,8,9]. Pacinian corpuscles consist of one axon, frequently branched, from a type II rapidly adapting Aβ-LTMR, surrounded by periaxonal cells that form two distinct compartments: the inner core (formed by terminal glial cells; TGCs), and the outer core-capsule formed by perineurial cells, both separated by an intermediate cell layer, known as the intermediate or growth layer [10,11]. The inner core consists of hemilamellae of non-myelinating TGCs symmetrically arranged while the outer core and the capsule are composed of concentrically arranged flattened lamellae of perineurial fibroblast-like cells. The interlamellar spaces of the capsule typically contain capillaries and macrophages [5,12], and between the lamellae of the inner core and the outer core-capsule there is chemically complex extracellular matrix. Previous studies have thoroughly characterized the protein composition of the different compartments of Pacinian corpuscles [5,6,13].
The functional and structural complexity of Pacinian corpuscles underscores their importance in tactile perception and vibration sensing. Their specialized lamellar architecture allows for rapid adaptation to mechanical stimuli, making them essential for interpreting changes in pressure and texture. As such, any pathological alteration in their form or number can lead to clinically significant sensory disturbances. The different cell types forming Pacinian corpuscles can proliferate or hypertrophy and give rise to different painful pathologies. These include heterotopic Pacinian corpuscles [14], hyperplasia [15,16,17,18], hypertrophy [19], hypertrophy and hyperplasia [20], and neuroma [19,21,22,23]. Also, hand Pacinian corpuscles are altered in Dupuytren’s disease [24,25,26] or neurofibromatosis [27,28]. Thus, given the abundance of Pacinian corpuscles in the fingers and palm [29], the appearance of painful nodules in the hand should prompt consideration of pathologies involving these sensory structures—or their exclusion—to determine the most appropriate treatment strategy.
Most of the available information on Pacinian corpuscles was obtained from histological, electron microscopy, and immunohistochemical studies of cadaveric specimens, surgical resections, and biopsies [7,13,30]. However, for clinical and research purposes, it would be of the utmost interest to be able to study Pacini's corpuscles in vivo using imaging techniques. The seminal works of Rhodes et al. [31,32], and the subsequent studies of Germann et al. [33], showed that magnetic resonance images, but not ultrasonography, could be successfully used to study the Pacini corpuscles of the hand. But almost simultaneously Riegler et al. [34] showed that high-resolution ultrasound (HRUS) techniques can also be a suitable method in the identification of Pacinian corpuscles; this was confirmed very recently [35]. Surely the use of HRUS will also be of great interest in the diagnosis of the pathologies of these sensory formations.
The aim of this study was to evaluate the possibility of visualizing Pacinian corpuscles in the hand using a cheap, innocuous, and easily reproducible and repeatable method, specifically HRUS. The study does not intend to map the distribution of Pacinian corpuscles in the hand but demonstrate and confirm that Pacinian corpuscles can be clearly identified and distinguished from other anatomical structures based on their sonographic appearances. This study might serve as a baseline for future research.
2. Materials and Methods
2.1. Patients and Scanner Procedure
Five patients were fully informed of the procedure, and verbal consent was obtained. The explorations were carried out by the same experienced radiologist, using the same scanner (Aplio i800, Canon Medical System Corporation, Otawara, Japan) equipped with a high-frequency hockey-stick linear array transducer (19–22 MHz). The patients were comfortably seated in front of the sonographer, with the arm fully extended, the elbow slightly flexed, and the hand resting on the examination table with the palm facing upward to ensure a stable and relaxed position.
Prior to imaging, coupling gel was generously applied to avoid excessive pressure on superficial tissues, thereby improving image quality and reducing artifact. The frequency and focus of the transducer were adjusted to optimize resolution and depth of field, allowing clear visualization of the dermis, hypodermis, and deeper palmar structures. This facilitated the identification of relevant anatomical landmarks including lumbrical muscles, flexor tendons, palmar aponeurosis, transverse ligament, and digital neurovascular bundles.
The examination began in the transverse (short axis) view at the level of the middle palm (proximal transverse crease) and advanced distally toward the proximal digital crease. The probe was kept perpendicular to the common digital nerves to avoid anisotropy and maintain consistent image clarity. Upon localizing a nerve, it was traced cranially to observe its branching and caudally to study associated subcutaneous tissue. Once potential Pacinian corpuscles were identified, they were assessed in both longitudinal and transverse axes. Dynamic imaging techniques, including passive and active finger flexion-extension, were applied to evaluate gliding behavior of nerves and corpuscles. Gentle transducer pressure was used to assess the compressibility of the corpuscles. Finally, Doppler-based microvascularity options were employed, although no internal vascular signals were visualized, suggesting the avascular nature of these corpuscles.
2.2. Immunohistochemical Study
The structural and immunohistochemical study of Pacinian corpuscles was performed on palmar skin sections (5 samples, 5 sections per sample) collected from regions anatomically comparable to those examined during the ultrasonographic procedure. This histological material was obtained from the archives of the National Registry of Biobanks (Collections Section, Ref. C-0001627, SINPOS Research Group, Department of Morphology and Cell Biology, University of Oviedo). All samples were handled in accordance with ethical and procedural regulations and were preserved optimally to ensure antigen stability for immunostaining. Tissue samples were obtained in accordance with Spanish law (RD 1301/2006; Ley 14/2007; DR 1716/2011; Orden ECC 1414/2013). Informed consent of patients was obtained, and the study was approved by the Ethical Committee for Biomedical Research of the Principality of Asturias, Spain (Cod. Celm. Past: Proyecto 266/18).
The sections were processed for standard immunohistochemistry coupled with the EnVision antibody complex detection kit (Dako, Copenhagen, Denmark), following the manufacturer’s instructions, specifically targeting the S100 protein, a known marker for terminal glial cells that constitute the inner core of the Pacinian corpuscles [5,13]. The immunoreaction provided clear contrast between the inner Aβ-LTMR terminal and the surrounding TGC and outer structural components of the corpuscles (intermediate layer and the outer core-capsule complex). The primary antibodies against S100 protein used were a monoclonal antibody raised in mouse (Thermo Scientific, clone 4C4.9; Freemont, CA, USA) used at a dilution of 1:1000, and a polyclonal antibody raised in rabbit (Dako, Glostrup, Denmark) used diluted 1:2000.
Additionally, double immunofluorescence techniques were used to differentiate the various layers within the corpuscles. The intermediate lamina was highlighted with CD34 inmunostaining (mouse monoclonal antibody clone QB-END/10, purchased prediluted; Master Diagnostica, Granada, Spain), a marker expressed by perineurial and endothelial cells, demarcating the boundary between the S100-positive inner core and the outer lamellar capsule. This dual labeling technique was critical for assessing structural organization and for verifying the anatomical correlation between sonographic images and microscopic architecture. The protocols employed for both immunohistochemical and immunofluorescent analyses have been thoroughly validated and published by our group in previous studies [11,13]. These histological and molecular approaches serve as the gold standard for confirming sonographic findings and improving anatomical interpretation of Pacinian corpuscles in vivo.
2.3. Fluorescence Intensity Analysis
Pacinian corpuscles (n = 10) were acquired with a TCS SP8 X White Light Laser Confocal Microscope (Leica Biosystems, Madrid, Spain) using a HC PL APO CS2 40x/1.30 oil objective; Leica Application Suite X version 1.8.1 software was used for image acquisition and processing analysis (Copyright 1997–2015 Leica Microsystems CMS GmbH). Images of the S100 and CD34 double immunofluorescence experiment were acquired using a 488 nm line laser excitation and a fluorescence detection range of 499–541 nm for S100, and a 553 nm line laser excitation with a fluorescence detection range of 564–633 nm for CD34. The counterstain with DAPI was acquired using a 405 nm blue laser diode for excitation and a fluorescence detection range of 415–477 nm.
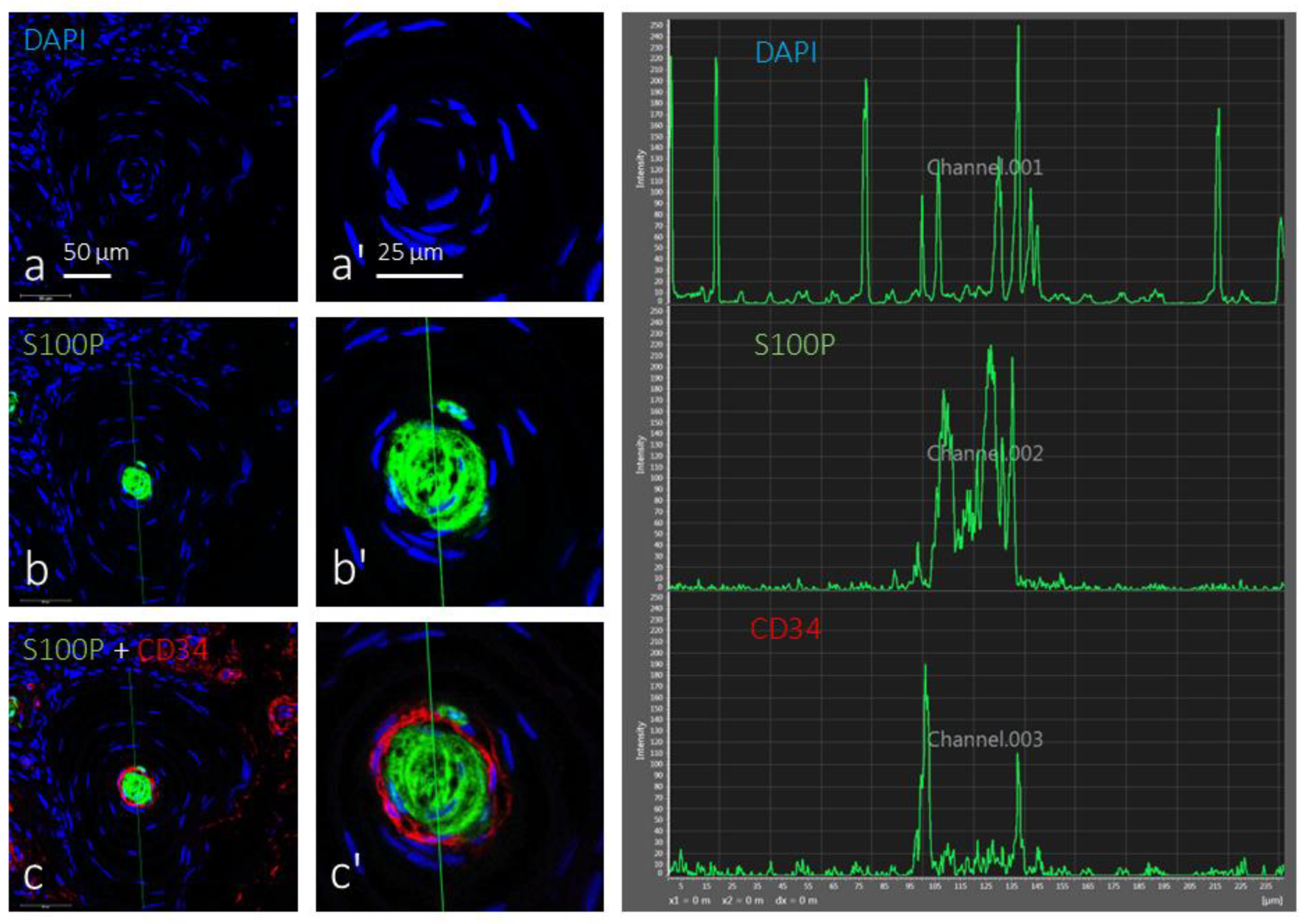
Fluorescence intensity of the three channels was analyzed using the line profile analytical tool to observe the spatial variation of signal intensity across the Pacinian corpuscles. A linear region of interest (ROI) was drawn across the entire corpuscle diameter, bisecting the inner core and extending through the intermediate and outer layers. The intensity peaks for each fluorophore were analyzed and plotted to evaluate compartmentalization and to quantify the contrast between glial-rich, CD34-positive, and nuclear-stained regions. This approach allowed objective assessment of lamellar density and thickness, revealing highly localized peaks in S100 and CD34 expression corresponding to inner and intermediate zones, respectively. DAPI distribution further highlighted the cellular architecture, confirming the densely packed nuclear arrangement within the inner core and a more diffuse pattern in the outer lamellae. These data supported structural compartmentalization previously observed in histological and sonographic studies and provided a quantitative molecular signature that may help in distinguishing normal versus pathological corpuscles in future investigations.
3. Results
3.1. Ultrasound Identification
Pacinian corpuscles were visualized on high-resolution ultrasound as well-delineated, smoothly contoured, oval, hypoechoic structures embedded within the underlying subcutaneous tissue of the palm and fingers. When the transducer was aligned in the longitudinal axis of the digit or palm, each corpuscle adopted a characteristic orientation that was either gently oblique or almost perfectly parallel to the overlying skin surface, a feature that greatly facilitated their recognition during real-time scanning. The sensory corpuscles did not occur in isolation only; rather, they were frequently encountered either singly or clustered in compact groups, most commonly consisting of two, three, or at most six discrete elements. Within such clusters the individual corpuscles were often arranged in a neat linear series, reminiscent of beads on a string, and they appeared to be interconnected by slender, anechoic channels that suggested the presence of delicate connective-tissue pedicles linking one corpuscle to the next.
On transverse (short axis) sonographic sections, the corpuscles displayed a striking multilamellar internal echotexture. This pattern was characterised by a central hyperechoic point or, alternatively, by several blurred echogenic septa, all of which together produced an image evocative of a miniature onion bulb with concentric layers—an appearance that was readily identifiable during dynamic, real-time exploration of the palmar soft tissues (Figure 1). When the probe was rotated to obtain longitudinal (long axis) sonograms, the scans confirmed the presence of a thin, hyperechoic outer capsule enveloping each corpuscle; however, in this orientation the fine internal septations were less sharply resolved, making the multilamellar configuration less conspicuous than in the transverse plane.
In terms of spatial distribution, the corpuscles were observed mainly deep to the palmar aponeurosis in the mid-palmar region, whereas in the distal palm and along the fingers they lay at a slightly more superficial level, yet they remained consistently ventral to the digital neurovascular bundles that course toward the phalanges (Figure 2). This consistent anatomical relationship—with the corpuscles sheltered beneath the dense fibrous sheet of the palmar fascia in the mid-palm and positioned more superficially but still anterior to the nerves and vessels in the digits—proved to be a useful landmark configuration for reliable identification during sonographic examination.
Dynamic maneuvers involving active and passive finger movement demonstrated that the Pacinian corpuscles glided synchronously with surrounding soft tissues without significant displacement, confirming their structural integration into the subcutaneous tissue. Importantly, they maintained consistent shape and echotexture across patients and were found to be relatively non-compressible under gentle probe pressure, although minimal deformation could occasionally be observed, suggesting some degree of mechanical compliance. Doppler-based microvascular imaging failed to demonstrate internal flow, further supporting the avascular nature of these structures in their normal state. This absence of vascularity, coupled with their characteristic morphology, helped differentiate Pacinian corpuscles from small neuromas or vascular anomalies. These findings support the feasibility of using HRUS to identify Pacinian corpuscles in vivo, thereby establishing a reproducible imaging protocol for their study in health and disease.
3.2. Immunohistochemistry and Fluorescence Intensity Analysis
Histological analysis demonstrated Pacinian corpuscles both as isolated, individual entities and as compact clusters containing six or more corpuscles (Figure 3). Corpuscle diameter, longitudinal axis, and concentric lamellar architecture were highly variable across specimens. In several sections (Figure 3b), multiple corpuscles were encapsulated within a single, continuous connective-tissue sheath, indicating a localized aggregation of sensory units within a common capsule.
Histological examination confirmed the presence of Pacinian corpuscles either as solitary units or as groups of six or more elements, with wide variation in size, orientation, and lamellar organization. Simple immunohistochemistry using the S100 protein marker distinctly outlined the inner core, composed of terminal glial cells, providing strong contrast against the less intensely stained outer core-capsule system. This differentiation was evident under light microscopy and demonstrated the dense structural packing of the inner lamellae compared to the more widely spaced external layers (Figure 4).
Additional confirmation was achieved through dual immunofluorescence staining, where S100-positive cells defined the inner core and CD34-positive staining demarcated the intermediate lamina. Pacinian corpuscles and that CD34 fluorescent signal were localized in the intermediate layer (Figure 5). Nuclei were stained with DAPI and were localized in the inner core and in the intermediate and external lamellar cells of the Pacinian corpuscles. In Figure 5, line profile analytical tool on the confocal images showed that S100 protein and CD34 were concentrated in the inner core and the intermediate layer, while the graphic of DAPI alone confirmed that the lamellae of the inner core are more densely packed than the externals ones.
The correlation between immunohistochemical findings and previously obtained sonographic images was compelling. The echogenic central septum observed in ultrasonography likely corresponds to the inner core or to interfaces between tightly bound lamellae. Furthermore, these results provide strong morphological and molecular evidence to support HRUS as a reliable modality for the identification of Pacinian corpuscles. By combining structural, molecular, and imaging data, this study strengthens the diagnostic framework for evaluating these sensory corpuscles in both physiological and pathological states.
4. Discussion
The present research work was designed to find out if the Pacinian corpuscles of the human hand can be identified in situ by high-resolution ultrasonography. The results demonstrate that hand Pacini's corpuscles can indeed be identified by this technique, and our findings are in full agreement with previous studies by Riegler et al. and Miller et al. [34,35]. They contradict those of Rhodes et al. [31,32] and Germann et al. [33], who managed to identify them by MRI but not ultrasonography. Possibly, the sensitivity in the ultrasonography technique or differences in equipment resolution, operator experience, or anatomical variance across samples may account for these discrepancies. Further research will be necessary to resolve these differences definitively and determine the best parameters for consistent identification across clinical settings.
This paper is the third published report, to our knowledge, confirming that Pacini’s corpuscles can be visualized using high-resolution diagnostic ultrasound imaging. The capacity to detect such microscopic cutaneous end-organ complexes with a non-invasive, real-time imaging modality offers important diagnostic potential. Our study also indicates that the nervous and non-nervous components of Pacini's corpuscles can be distinguished by ultrasound and provides a plausible explanation for this differentiation. This is of potential clinical and research interest since it would be possible to distinguish between pathologies of Pacinian corpuscles involving the nervous part (greater echogenicity) and the non-nervous part (hypoechogenic) of the corpuscle.
The differences in echogenicity between the central-inner and peripheral-outer regions of the Pacinian corpuscles could be associated with the relatively denser packing of the inner core lamellae compared to the laxer, more heterogeneous structured outer core and capsule, which may also include interstitial fluid and fine collagen fibers. However, this cannot be directly attributed to cellular density, since the TGCs that form the central inner core are few, whereas fibroblasts and fibrocytes constituting the outer capsule are comparatively abundant and more widely distributed throughout the peripheral supporting matrix of the corpuscle [7,8,9,10].
In addition to the architectural differences observed, it is also necessary to consider the molecular and biochemical composition of the corpuscles, especially in relation to their extracellular matrix (ECM). The ECM composition—including collagen subtypes, proteoglycans, small leucin-rich proteoglycans and other glycoproteins—may influence acoustic impedance, hence affecting the echogenicity recorded by ultrasonography [5]. The composition of ECM in human digital Pacinian corpuscles is now rather well known [5]. Moreover, changes in hydration levels, protein cross-linking, and structural alignment of ECM fibers may also modulate the appearance of these structures in high-resolution scans. Future histological studies correlated with sonographic findings will be essential to unravel the exact source of these echogenic disparities and further validate the utility of this imaging method in clinical practice.
The results of our study are of significant clinical relevance, as they contribute to the non-invasive visualization and precise localization of both normal, and presumably also pathological, Pacini's corpuscles within the hand. This is particularly valuable in the context of conditions such as Pacinian neuroma or hypertrophy, where symptoms may include pain, hypersensitivity, or nodular formations. The identification of these structures in vivo allows for earlier diagnosis and a more targeted approach to treatment, potentially reducing the need for invasive diagnostic procedures, such as surgical biopsy. Additionally, accurate imaging of Pacini’s corpuscles may help clinicians distinguish between neuropathic pain syndromes and localized mechanical hypersensitivity due to corpuscular pathology.
Furthermore, the same ultrasonographic technique may be applicable to other anatomical locations rich in Pacinian corpuscles. These include the plantar surface of the foot, where such structures are highly concentrated, particularly in the heel and metatarsal pads [36,37]. In these locations, Pacinian corpuscle hyperplasia has been documented [38,39], often forming painful subcutaneous nodules [40]. These nodules are occasionally associated with connective tissue disorders such as Ledderhose’s disease, a type of plantar fibromatosis that affects the fascia of the sole [37]. High-resolution ultrasound may assist in distinguishing between corpuscular hyperplasia and fibromatous growth, aiding in the selection of appropriate treatment modalities, whether conservative, surgical, or pharmacological.
Another compelling aspect of our study is that it highlights ultrasound as a reliable, non-invasive, and cost-effective method for visualizing Pacinian corpuscles in situ. Unlike other imaging techniques that may require contrast enhancement or radioactive tracers, ultrasonography offers real-time, dynamic imaging that can be repeated as necessary without exposing the patient to ionizing radiation. This is particularly beneficial in pediatric, geriatric, and vulnerable populations. Additionally, it allows for the monitoring of corpuscular morphology over time, which may prove valuable in evaluating treatment outcomes or disease progression in pathologies affecting these mechanoreceptors.
It is also notable that alternative imaging techniques such as reflectance confocal microscopy, optical coherence tomography, or laser scanning microscopy—although effective for examining more superficial dermal structures such as Meissner corpuscles—are not applicable for in vivo assessment of Pacinian corpuscles due to their deeper dermal location [41,42,43]. Historically, the analysis of Pacinian corpuscles required excisional biopsies followed by histological processing, a time-consuming and often painful procedure with inherent risks of infection and scarring. Our study proposes an innovative and patient-friendly alternative, potentially shifting the diagnostic paradigm for mechanoreceptor-related disorders.
The anatomical and functional relevance of Pacinian corpuscles in sensory physiology cannot be overstated. These rapidly adapting mechanoreceptors are integral to the detection of vibration and deep pressure stimuli. Understanding their pathological changes and being able to monitor them non-invasively may open avenues for the study of various neuropathic disorders. For instance, early alterations in Pacinian corpuscle morphology or function might be linked to systemic diseases like diabetes mellitus, where peripheral neuropathy is common. Further investigations should explore whether changes in sonographic features of these corpuscles could serve as early biomarkers of peripheral sensory neuropathy.
Moreover, the capacity to differentiate nervous from non-nervous elements on high-resolution ultrasound holds a particular promise for regenerative-medicine research and clinical follow-up. In traumatic nerve disruption, entrapment neuropathy, or elective reconstructive microsurgery, serial ultrasonographic assessment of Pacinian corpuscles and adjacent sensory end-organs could complement electrophysiological testing by documenting structural integrity, lamellar continuity, and reinnervation status in real time. Such imaging feedback may help surgeons tailor postoperative rehabilitation protocols—adjusting mobilization schedules, splinting duration, or adjunct physiotherapy—according to objectively observed tissue recovery rather than fixed time points.
Likewise, experimental strategies that deploy autologous or allogenic nerve grafts, Schwann-cell–seeded scaffolds, mesenchymal stem-cell injections, or bioengineered hydrogel conduits to re-establish cutaneous sensation could incorporate ultrasonography as a non-invasive biomarker of success. In this way, real-time corpuscle imaging could bridge the translational gap between laboratory advances in sensory-nerve reconstruction and day-to-day patient management, guiding iterative improvements in both experimental design and surgical technique.
In conclusion, our findings add to the growing body of evidence that high-resolution ultrasonography is a viable tool for identifying Pacinian corpuscles in the human hand and potentially other locations. This technique enables detailed visualization of both the architecture and composition of these structures, supporting its use in both clinical diagnostics and anatomical research. Its safety, repeatability, and accessibility make it a valuable addition to the current imaging armamentarium. We encourage further longitudinal and comparative studies to optimize imaging protocols, validate diagnostic criteria, and explore the broader clinical applications of this promising modality.
Author Contributions
Conceptualization, E.G. and J.A.V.; methodology, I.A, E.G. and Y.G.-M.; validation, J.A.V., and Y.G-M.; formal analysis, I.A., E.G. and M.A.-G.; investigation, E.G. and Y.G-M.; resources, I.A., Y.G-M. and E.G.; writing—original draft preparation, I.A. and E.G.; writing—review and editing, J.A.V.; visualization, I.A., O.G.-S. and Y.G-M.; supervision, J.A.V.; project administration, I.A. and Y. G-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
These materials were obtained from the laboratory of the Peripheral Nervous System and Sense Organs Research Group (SINPOS) at the University of Oviedo (Registro Nacional de Biobancos, Sección Colecciones, Ref. C-0001627, Oviedo, Spain). The biological material was obtained in compliance with the Spanish Legislation (RD 1301/2006; Law 14/2007; RD 1716/2011; Order ECC/1404/2013) and in accordance with the guidelines of the Declaration of Helsinki II.
Informed Consent Statement
Verbal informed consent was obtained from all subjects involved in the ultrasonographic study.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
The authors have no acknowledgments to declare.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| LTMRs | Low-threshold mechanoreceptors |
| CEOCs | Cutaneous end-organ complexes |
| TGCs | Terminal glial cells |
| HRUS | High-resolution ultrasound |
| ROI | Region Of Interest |
| PC | Pacinian Corpuscle |
| ECM | Extracellular matrix |
References
- Li, L.; Rutlin, M.; Abraira, V.E.; Cassidy, C.; Kus, L.; Gong, S.; Jankowski, M.P.; Luo, W.; Heintz, N.; Koerber, H.R.; et al. The functional organization of cutaneous low-threshold mechanosensory neurons. Cell 2011, 147(7), 1615–1627. https://doi.org 10.1016/j.cell.2011.11.027.
- Abraira, V.E.; Ginty, D.D. The sensory neurons of touch. Neuron 2013, 79, 618–639. [CrossRef]
- Handler, A.; Ginty, D.D. The mechanosensory neurons of touch and their mechanisms of activation. Nat. Rev. Neurosci. 2021, 22, 521–537. [CrossRef]
- Zimmerman, A.; Bai, L.; Ginty, D.D. The gentle touch receptors of mammalian skin. Science 2014, 346, 950–954. https://doi.org 10.1126/science.1254229.
- Cobo, R.; García-Piqueras, J.; Cobo, J.; Vega, J.A. The human cutaneous sensory corpuscles: an update. J. Clin. Med. 2021, 10, 227. [CrossRef]
- Vega, J.A.; García-Mesa, Y.; Cuendias, P.; Martín-Cruces, J.; Cobo, R.; García-Piqueras, J.; Suazo, I.; García-Suárez, O. Development of vertebrate cutaneous end-organ complexes. Curr. Top. Dev. Biol. 2025, 154, [in press]. [CrossRef]
- Bell, J.; Bolanowski, S.; Holmes, M.H. The structure and function of Pacinian corpuscles: a review. Prog. Neurobiol. 1994, 42, 79–128. https://doi.org /10.1016/0301-0082(94)90022-1.
- Zelená, J. Nerves and Mechanoreceptors: The Role of Innervation in the Development and Maintenance of Mammalian Mechanoreceptors; Springer: Berlin, Germany, 1994; pp. 1–304.
- Malinovský, L. Sensory nerve formations in the skin and their classification. Microsc. Res. Tech. 1996, 34(4), 283–301. [CrossRef]
- Munger, B.L.; Ide, C. The structure and function of cutaneous sensory receptors. Arch. Histol. Cytol. 1988, 51(1), 1–34. [CrossRef]
- García-Piqueras, J.; García-Suárez, O.; Rodríguez-González, M.C.; Cobo, J.L.; Cabo, R.; Vega, J.A.; Feito, J. Endoneurial-CD34 positive cells define an intermediate layer in human digital Pacinian corpuscles. Ann. Anat. 2017, 211, 55–60. [CrossRef]
- Martín-Alguacil, N.; de Gaspar, I.; Schober, J.M.; Pfaff, D.W.; Vega, J.A. Somatosensation. In: Neuroscience in the 21st Century. In: Pfaff, D.W.; Volkow, N.D.; Rubenstein, J.L., Eds. Springer, Cham 2022, pp. 1143–1182.
- Vega, J.A.; García-Suárez, O.; Montaño, J.A.; Pardo, B.; Cobo, J.M. The Meissner and Pacinian sensory corpuscles revisited: new data from the last decade. Microsc. Res. Tech. 2009, 72(4), 299–309. [CrossRef]
- Irie, H.; Kato, T.; Yakushiji, T.; Hirose, J.; Mizuta, H. Painful heterotopic pacinian corpuscle in the hand: a report of three cases. Hand Surg. 2011, 16, 81–85. [CrossRef]
- Kumar, A.; Darby, A.J.; Kelly, C.P. Pacinian corpuscles hyperplasia—an uncommon cause of digital pain. Acta Orthop. Belg. 2003, 69(1), 74–76.
- Cho, H.H.; Hong, J.S.; Park, S.Y.; Park, H.S.; Cho, S.; Lee, J.H. Tender papule rising on the digit: Pacinian neuroma should be considered in differential diagnosis. Int. J. Med. Sci. 2012, 9, 83–85. [CrossRef]
- Garcia, F.C.; Acosta, D.R.; Diaz Gonzalez, J.M.; Lima, M.S. Hyperplasia and hypertrophy of Pacinian corpuscles: A case report. Am. J. Dermatopathol. 2015, 37, 100–101. [CrossRef]
- Stoj, V.J.; Adalsteinsson, J.A.; Lu, J.; Berke, A.; Lipner, S.R. Pacinian corpuscle hyperplasia: A review of the literature. Int. J. Womens Dermatol. 2020, 7(3), 335–341. [CrossRef]
- Yenidunya, M.O.; Yenidunya, S.; Seven, E. Pacinian hypertrophy in a type 2A hand burn contracture and Pacinian hypertrophy and hyperplasia in a Dupuytren's contracture. Burns 2009, 35(3), 446–450. [CrossRef]
- Reznik, M.; Thiry, A.; Fridman, V. Painful hyperplasia and hypertrophy of pacinian corpuscles in the hand: report of two cases with immunohistochemical and ultrastructural studies, and a review of the literature. Am. J. Dermatopathol. 1998, 20(2), 203–207. [CrossRef]
- Zanardi, F.; Cooke, R.M.; Maiorana, A.; Curti, S.; Farioli, A.; Bonfiglioli, R.; Violante, F.S.; Mattioli, S. "Is this case of a very rare disease work-related?" A review of reported cases of Pacinian neuroma. Scand. J. Work Environ. Health 2011, 37(3), 253–258. [CrossRef]
- Jiménez, I.; Marcos-García, A.; Muratore, G.; Medina, J. Pacinian Corpuscles Neuroma. An Exceptional Cause of Pain in the Hand. J. Hand Surg. Asian Pac. Vol. 2017, 22, 229–231. [CrossRef]
- Šedý, J.; Skalná, M. Incidental finding of multiple Pacinian neuroma in hand. J. Dermatol. 2015, 42(7), 743–744. https://doi.org10.1111/1346-8138.12886.
- Akyurek, N.; Ataoglu, O.; Cenetoglu, S.; Ozmen, S.; Cavusoglu, T.; Yavuzer, R. Pacinian corpuscle hyperplasia coexisting with Dupuytren’s contracture. Ann. Plast. Surg. 2000, 45, 220–222.
- Von Campe, A.; Mende, K.; Omaren, H.; Meuli-Simmen, C. Painful nodules and cords in Dupuytren disease. J. Hand Surg. Am. 2012, 37, 1313–1318. [CrossRef]
- García-Martínez, I.; García-Mesa, Y.; García-Piqueras, J.; Martínez-Pubil, A.; Cobo, J.L.; Feito, J.; García-Suárez, O.; Vega, J.A. Sensory innervation of the human palmar aponeurosis in healthy individuals and patients with palmar fibromatosis. J. Anat. 2022, 240, 972–984. [CrossRef]
- Yan, S.; Horangic, N.J.; Harris, B.T. Hypertrophy of Pacinian corpuscles in a young patient with neurofibromatosis. Am. J. Dermatopathol. 2006, 28, 202–204. [CrossRef]
- Friedrich, R.E.; Hagel, C. Painful Vater-Pacini neuroma of the digit in neurofibromatosis type 1. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2019, 8, Doc03. [CrossRef]
- Stark, B.; Carlstedt, T.; Hallin, R.G.; Risling, M. Distribution of human Pacinian corpuscles in the hand. A cadaver study. J. Hand Surg. Br. 1998, 23(3), 370–372. [CrossRef]
- Handler, A.; Zhang, Q.; Pang, S.; Nguyen, T.M.; Iskols, M.; Nolan-Tamariz, M.; Cattel, S.; Plumb, R.; Sanchez, B.; Ashjian, K.; Shotland, A.; Brown B.; Kabeer, M.; Turecek, J.; DeLisle, M.M.; Rankin, G.; Xiang, W.; Pavarino, E.C.; Africawala, N.; Santiago, C.; Lee, W.A.; Xu, C.S.; Ginty, D.D. Three-dimensional reconstructions of mechanosensory end organs suggest a unifying mechanism underlying dynamic, light touch. Neuron 2023, 111, 3211–3229.e9. [CrossRef]
- Rhodes, N.G.; Murthy, N.S.; Lachman, N.; Rubin, D.A. Normal Pacinian corpuscles in the hand: radiology-pathology correlation in a cadaver study. Skeletal Radiol. 2019, 48(10), 1591–1597. [CrossRef]
- Rhodes, N.G.; Murthy, N.S.; Lehman, J.S.; Rubin, D.A. Pacinian corpuscles: an explanation for subcutaneous palmar nodules routinely encountered on MR examinations. Skeletal Radiol. 2018, 47(11), 1553–1558. [CrossRef]
- Germann, C.; Sutter, R.; Nanz, D. Novel observations of Pacinian corpuscle distribution in the hands and feet based on high-resolution 7-T MRI in healthy volunteers. Skeletal Radiol. 2021, 50, 1249–1255. [CrossRef]
- Riegler, G.; Brugger, P.C.; Gruber, G.M.; Pivec, C.; Jengojan, S.; Bodner, G. High-Resolution Ultrasound Visualization of Pacinian Corpuscles. Ultrasound Med. Biol. 2018, 44(12), 2596–2601. [CrossRef]
- Miller, N.J.; Meiling, J.B.; Walker, F.O.; Cartwright, M.S. Ultrasonographic Identification of Pacinian Corpuscles in the Hand: A Pilot Study of Technique and Reliability. Muscle Nerve 2025, [Epub ahead of print]. [CrossRef]
- Jin, Z.W.; Cho, K.H.; Xu, D.Y.; You, Y.Q.; Kim, J.H.; Murakami, G.; Abe, H. Pacinian corpuscles in the human fetal foot: A study using 3D reconstruction and immunohistochemistry. Ann. Anat. 2020, 227, 151421. [CrossRef]
- Feito, J.; Esteban, R.; García-Martínez, M.L.; García-Alonso, F.J.; Rodríguez-Martín, R.; Rivas-Marcos, M.B.; Cobo, J.L.; Martín-Biedma, B.; Lahoz, M.; Vega, J.A. Pacinian Corpuscles as a Diagnostic Clue of Ledderhose Disease—A Case Report and Mapping of Pacinian Corpuscles of the Sole. Diagnostics 2022, 12, 1705. [CrossRef]
- Chambers, A.R.; Dreyer, M.A.; Song, K.Y.; Lam, K.K. Bilateral symptomatic Pacinian corpuscle hyperplasia of the adult foot. Foot (Edinb.) 2021, 49, 101709. [CrossRef]
- Satge, D.; Nabhan, J.; Nandiegou, Y.; Hermann, B.; Goburdhun, J.; Labrousse, F. A Pacinian hyperplasia of the foot. Foot Ankle Int. 2001, 22(4), 342–344. [CrossRef]
- Goldman, F.; Garner, R. Pacinian corpuscles as a cause for metatarsalgia. J. Am. Podiatry Assoc. 1980, 70, 561–567. [CrossRef]
- Herrmann, D.N.; Boger, J.N.; Jansen, C.; Alessi-Fox, C. In vivo confocal microscopy of Meissner corpuscles as a measure of sensory neuropathy. Neurology 2007, 69, 2121–2127. [CrossRef]
- Creigh, P.D.; Du, K.; Wood, E.P.; Mountain, J.; Sowden, J.; Charles, J.; Behrens-Spraggins, S.; Herrmann, D.N. In Vivo Reflectance Microscopy of Meissner Corpuscles and Bedside Measures of Large Fiber Sensory Function: A Normative Data Cohort. Neurology 2022, 98, e750–e758. [CrossRef]
- Infante, V.H.P.; Bennewitz, R.; Klein, A.L.; Meinke, M.C. Revealing the Meissner Corpuscles in Human Glabrous Skin Using In Vivo Non-Invasive Imaging Techniques. Int. J. Mol. Sci. 2023, 24, 7121. [CrossRef]
Figure 1.
High-resolution images at the distal intermetacarpal space; images in the axial view of the palm in two different cases with magnification of the selected area. Pacinian corpuscles (PC) on the short axis sonogram show a central, echogenic blurred incomplete septa corresponding to the inner core. (a’) and (a’’), and (b’) and (b’’) are progressive enlargements of (a) and (b), respectively.
Figure 1.
High-resolution images at the distal intermetacarpal space; images in the axial view of the palm in two different cases with magnification of the selected area. Pacinian corpuscles (PC) on the short axis sonogram show a central, echogenic blurred incomplete septa corresponding to the inner core. (a’) and (a’’), and (b’) and (b’’) are progressive enlargements of (a) and (b), respectively.
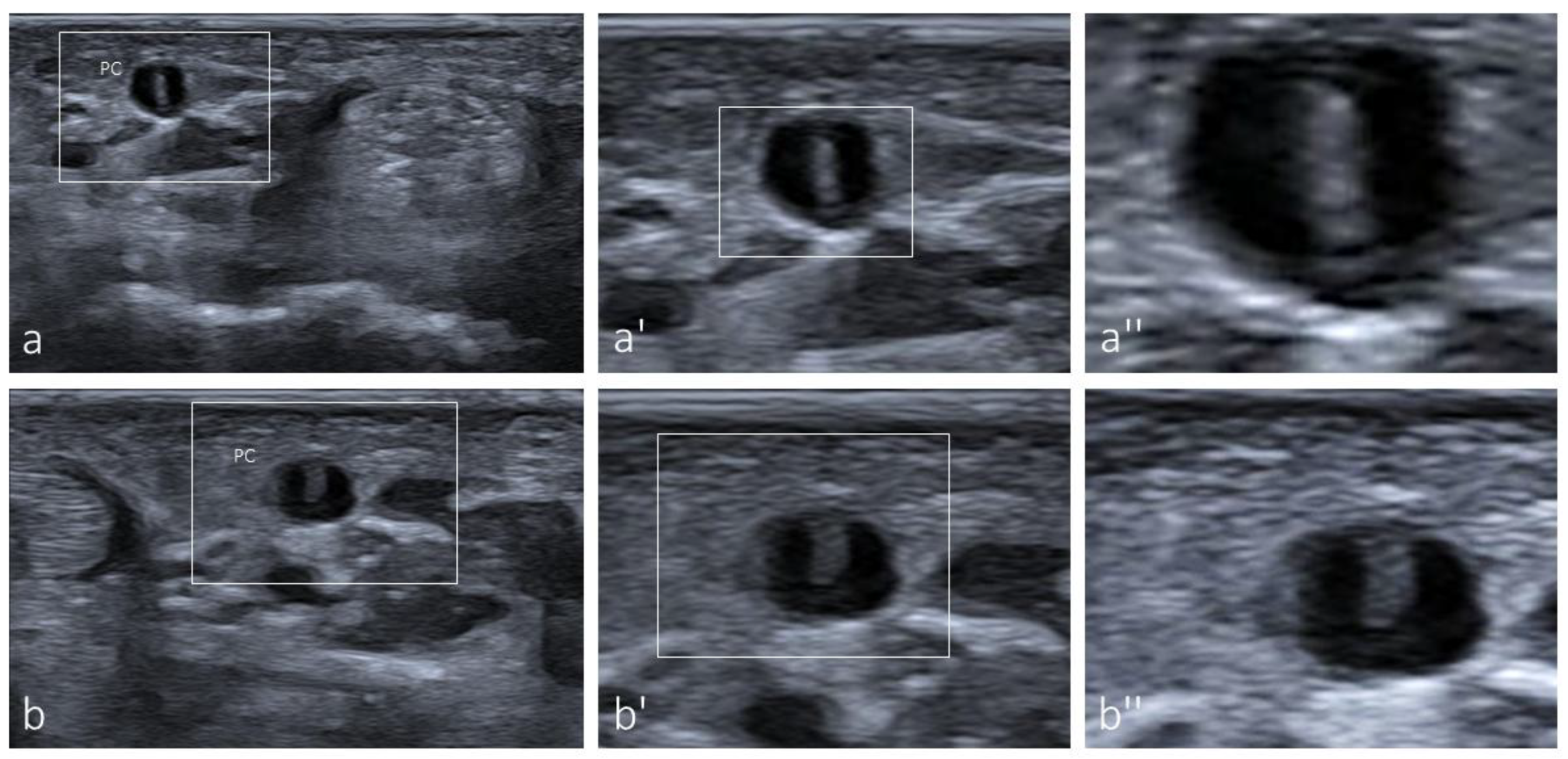
Figure 2.
High-resolution ultrasound images at the intermetacarpal space, short axis. (a) Flexor tendons (T) and lumbrical muscle (L); within the white-line square, a Pacinian corpuscle and the neurovascular bundle can be observed, which are enlarged in a’ and a’’. (a’) Magnified view of the squared area in (a), showing the lumbrical muscle (L), Pacinian corpuscle (PC), digital artery (a), digital vein (v) and digital nerves (discontinuous yellow line). (a’’) Higher magnification of the Pacinian corpuscle in the short axis view with a central echogenic core. (b) Longitudinal sonogram of Pacinian corpuscle with measurements. (b’’) Longitudinal sonogram of a Pacinian corpuscle showing the neural pedicle (white arrows).
Figure 2.
High-resolution ultrasound images at the intermetacarpal space, short axis. (a) Flexor tendons (T) and lumbrical muscle (L); within the white-line square, a Pacinian corpuscle and the neurovascular bundle can be observed, which are enlarged in a’ and a’’. (a’) Magnified view of the squared area in (a), showing the lumbrical muscle (L), Pacinian corpuscle (PC), digital artery (a), digital vein (v) and digital nerves (discontinuous yellow line). (a’’) Higher magnification of the Pacinian corpuscle in the short axis view with a central echogenic core. (b) Longitudinal sonogram of Pacinian corpuscle with measurements. (b’’) Longitudinal sonogram of a Pacinian corpuscle showing the neural pedicle (white arrows).
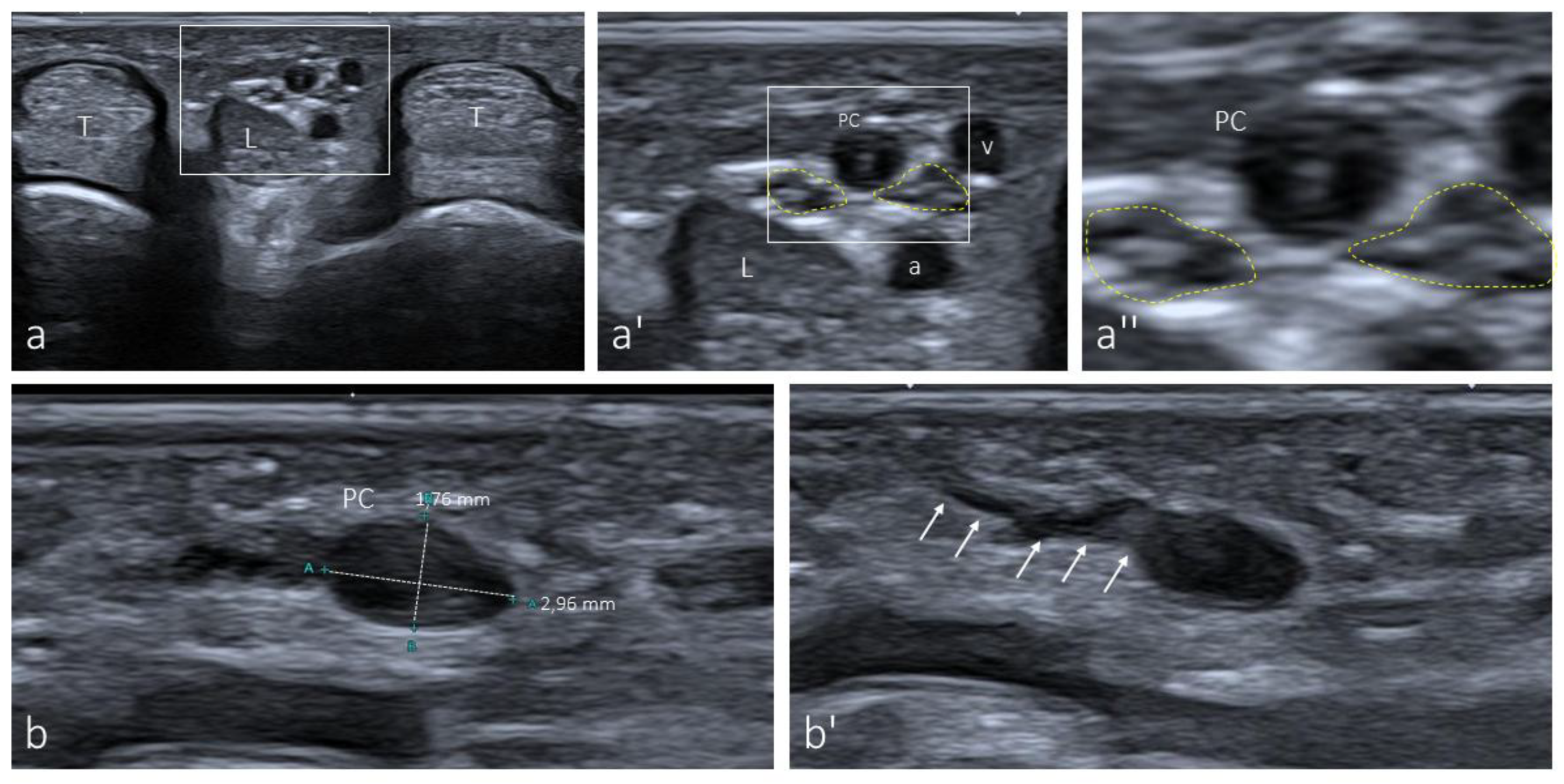
Figure 3.
Pacinian corpuscles forming clusters (a, b) or isolated (c) are regularly found in the hypodermis of both the palm and fingers. (*) indicate Pacini corpuscles; IC: inner core; OC-C: outer core-capsule complex.
Figure 3.
Pacinian corpuscles forming clusters (a, b) or isolated (c) are regularly found in the hypodermis of both the palm and fingers. (*) indicate Pacini corpuscles; IC: inner core; OC-C: outer core-capsule complex.
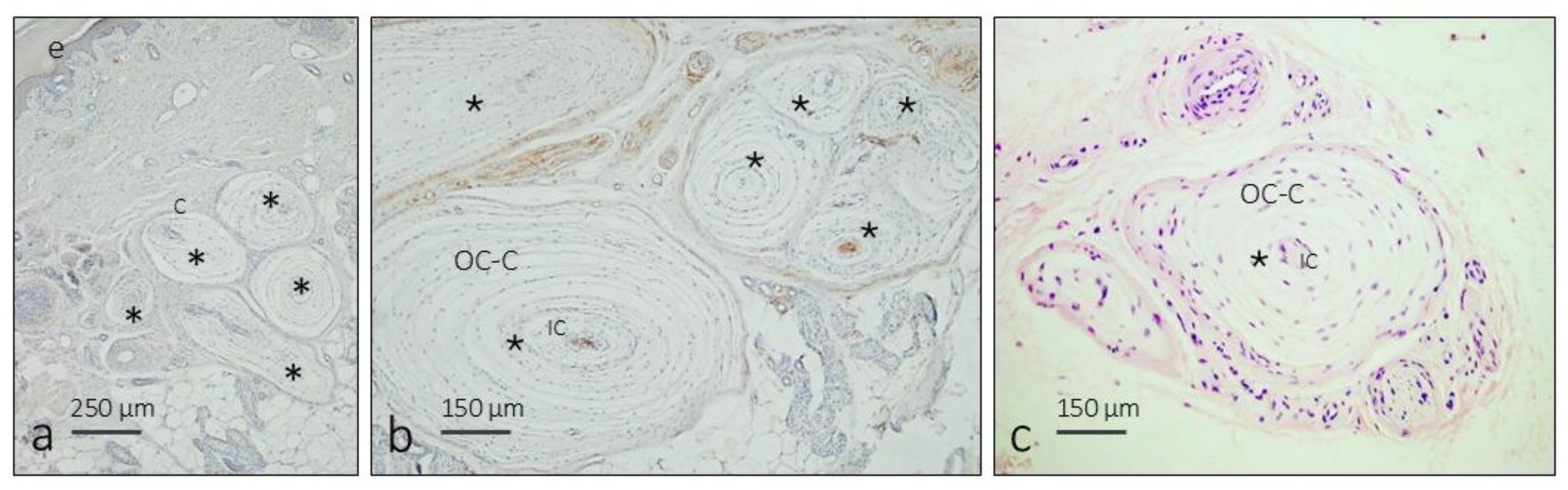
Figure 4.
Palmar Pacinian corpuscles in transversal (a, b) and oblique (c) sections showing an intense immunoreactivity for S100 protein in the inner core. C: capsule; E: epidermis; IC: inner core; OC: outer core.
Figure 4.
Palmar Pacinian corpuscles in transversal (a, b) and oblique (c) sections showing an intense immunoreactivity for S100 protein in the inner core. C: capsule; E: epidermis; IC: inner core; OC: outer core.
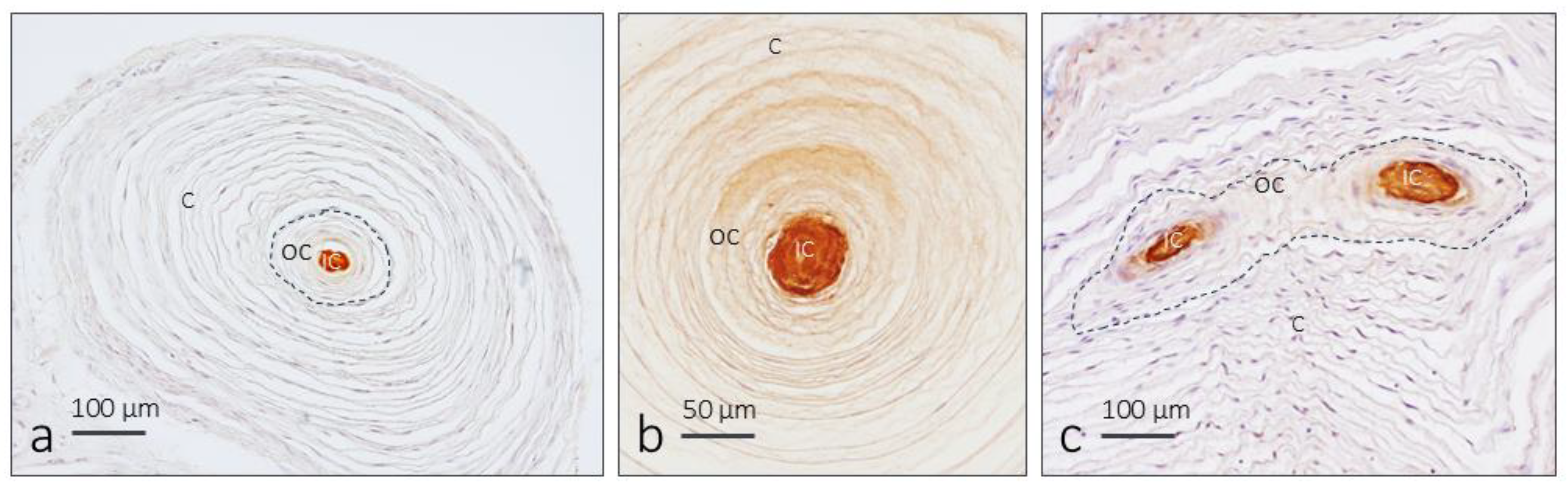
Figure 5.
Confocal images of two Pacinian corpuscles and position of the line profile tool. (a, a´) Fluorescence intensity graphics of DAPI. (b, b΄, c, c΄) Fluorescence intensity graphics of S100 / CD34 along a line drawn to the entire diameter of the Pacinian corpuscles passing through the inner core. (Left) Position of the line profile tool; X-axis: length of the line in µm; Y-axis: fluorescence intensity.
Figure 5.
Confocal images of two Pacinian corpuscles and position of the line profile tool. (a, a´) Fluorescence intensity graphics of DAPI. (b, b΄, c, c΄) Fluorescence intensity graphics of S100 / CD34 along a line drawn to the entire diameter of the Pacinian corpuscles passing through the inner core. (Left) Position of the line profile tool; X-axis: length of the line in µm; Y-axis: fluorescence intensity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



