Submitted:
18 June 2025
Posted:
19 June 2025
You are already at the latest version
Abstract
Cefiderocol (FDC) presents challenges in antimicrobial susceptibility testing (AST). The broth microdilution (BMD) method with iron-depleted cation-adjusted Mueller-Hinton broth (ID-CAMHB), is the reference standard but cumbersome for routine clinical la-boratory use, while variable accuracy has been reported with available commercial systems. Variability in interpretive criteria and areas of technical uncertainty (ATUs) further complicate assessments. This review and expert opinion firstly presents an overview on non-susceptibility to FDC and then deeps into the performance of current FDC AST methods for Enterobacterales, Pseudomonas aeruginosa, and Acinetobacter bau-mannii complex, proposing decision frameworks to guide clinical microbiologists in making informed choices. For Enterobacterales, including carbapenem-resistant Enter-obacterales (CRE), and Pseudomonas aeruginosa, we propose disk diffusion (DD) as a preliminary screening tool to classify isolates as susceptible (S) or resistant (R). Con-firmatory testing using the UMIC® FDC system or the ID-CAMHB BMD method is recommended for R isolates. In cases of discrepancy, repeating the test with ID-CAMHB BMD is advised. Additionally, isolates falling within the ATU during DD testing should be retested using either the UMIC® system or ID-CAMHB BMD. For A. baumannii complex, since EUCAST breakpoints have not been defined yet,, we propose a stepwise framework based on the first DD result; isolates with inhibition zones.
Keywords:
cefiderocol
; antimicrobial susceptibility testing
; clinical microbiology
1. Introduction
Antimicrobial resistance (AMR) among MDR Gram-negative (GN) bacteria represents a major global health concern, particularly in hospital and critical care settings. In Intensive Care Units (ICUs), MDR-GNs—primarily carbapenem-resistant Enterobacterales, Pseudomonas aeruginosa, and Acinetobacter baumannii—account for over one-third of nosocomial infections. These pathogens, complicate treatment decisions, increase mortality, and contribute to substantial healthcare costs [1,2].
Recent antimicrobial resistance surveillance data in Europe collected by the Central Asian and European Surveillance of Antimicrobial Resistance (CAESAR) network and the European Antimicrobial Resistance Surveillance Network (EARS-Net), revealed that in this time frame third-generation cephalosporin resistance in Klebsiella pneumoniae was widespread in the WHO European Region, with 42% of the countries, especially in the southern and eastern parts, reporting high resistance levels of 50% or above [1]. Conversely, only 16% of the countries had resistance levels below 10%. According to the ECDC, carbapenem resistance in K. pneumoniae is substantially more common than in Escherichia coli: 33% of reporting countries documented resistance rates ≥25% in K. pneumoniae, and 18% reported rates ≥50%, while resistance in E. coli remains rare and generally below 1%. Resistance to carbapenems in P. aeruginosa and Acinetobacter spp. also showed significant geographic variability [1,2]. Specifically, 14% of countries reported high levels of carbapenem resistance in P. aeruginosa (50% or more), while in Acinetobacter spp. 56% of the countries reported 50% or above resistance levels, predominantly in the southern and eastern parts of Europe [1].
Despite the introduction of new β-lactamase inhibitor combinations, the demand for effective antibacterial drugs continues to increase. In this context, the introduction in 2019 of cefiderocol (FDC, Shionogi & Co., Ltd.), a siderophore cephalosporin, is a pivotal advancement in the treatment of MDR-GN infections. FDC is approved for a broad spectrum of serious infections caused by GN pathogens, including strains resistant to available treatments, as it is relatively stable against hydrolysis by many serine- and metallo- β -lactamases (MBLs) [3,4,5,6].
The dual penetration mechanism of FDC, through passive diffusion and active transport via the iron transport system, promotes effective delivery and achievement of high concentrations within the bacterial periplasm. This allows FDC to bypass common resistance mechanisms such as porin loss in carbapenemase-resistant (CR) strains, a feature that may confer an advantage over other β-lactams like ceftolozane or meropenem. As other β-lactams, FDC binds penicillin-binding proteins, disrupts cell wall synthesis, and induces bacterial cell death [3,4,7].
Implementing and using standardized and reproducible methods for antibiotic susceptibility testing (AST) for FDC is crucial for its clinical application, patient safety, and resistance surveillance. However, it remains a complex and challenging endeavor [8]. This review and expert opinion aims to offer an overview of global prevalence and general mechanisms of non-susceptibility to FDC and evaluate the performance of current AST practices proposing decision frameworks for FDC AST with Enterobacterales, P. aeruginosa, and A. baumannii complex.
2. Materials and Methods
First, a comprehensive state-of-the-art review was conducted on the mechanisms of resistance and the types of AST methodologies.
A focused search was then conducted in PubMed using the keywords "antimicrobial susceptibility testing," "cefiderocol susceptibility testing," "Cefiderocol," and "Gram-negative bacteria” to center on studies evaluating AST performances. These terms were combined using Boolean operators, such as AND and OR, to cover the spectrum of AST methodologies and resistance mechanisms associated with FDC.
Studies were included in the final evaluation if:
- focused on Enterobacterales, P. aeruginosa, and A. baumannii complex clinical isolates.
- reported on comparing AST methodologies specifically for FDC versus broth microdilution method (BMD).
Studies were excluded if not written in English or if they were editorials, reviews or meta-analyses.
All authors independently screened all titles, abstracts, and content to select eligible studies. Discrepancies at any stage were discussed and resolved unanimously.
Our search strategy identified 53 papers on PubMED, of which 13 were selected for our final review.
2.1. Data Synthesis Approach
Data from the selected studies were qualitatively synthesized, summarizing findings related to the performance (in terms of Categorical Agreement [CA], Essential Agreement [EA], Very Major Errors [VME], Major Errors [ME], minor errors [mE], and bias parameters). This synthesis aimed to highlight trends, consensus points among studies, and notable discrepancies in results or methodologies.
2.2. Collection of Expert Opinions
Expert opinions were gathered through a blend of face-to-face and virtual meetings (three in total) orchestrated by the coordinator, Stefania Stefani. These meetings involved key microbiology experts delving into their practical experiences, challenges faced, and evaluations on AST for FDC.
3. Non-Susceptibility to FDC: Global Prevalence and General Mechanisms
According to recent surveillance data, the prevalence of non-susceptibility to FDC (NS-FDC) remains low overall [2,9]. A recent systematic review and meta-analysis encompassing 82,035 clinical isolates (period 2020-2023) revealed that the prevalence of NS-FDC, according to EUCAST breakpoints, exhibited variability across different bacterial species. For instance, rates among Enterobacterales, P. aeruginosa, and A. baumannii were 3.0% (95%CI 1.5-6.0%), 1.4% (95%CI 0.5-4.0%), and 8.8% (95%CI 4.9-15.2%), respectively. Higher rates were found in carbapenem-resistant NDM-producing Enterobacterales with a prevalence of 38.8% (95%CI 22.6-58.0%) [9].
Four potential factors may contribute to the emergence of NS-FDC:
- Expression of metallo-β-lactamase NDM and/or β-lactamases (e.g., SHV, PER and VEB) [10,11,12,13,14,15,16,17,18,19]. In A. baumannii, combining FDC with avibactam has been shown to reduce MIC, indicating that β -lactamase activity in this species contributes to resistance [20]. In addition, increased copy numbers of the blaNDM-5 gene due to translocation events have been shown to enhance NDM production, leading to decreased activity of FDC. However, the extent to which blaNDM-5 expression contributes to FDC resistance remains to be fully elucidated [21].
- Structural alterations in β-lactamases, such as AmpC, for example, the region encoding the R2 loop [22,23,24]. Furthermore, comparable variations in Oxacillinases include specific point mutations in the Ω loop of OXA-2 (Ala149Pro and Asp150Gly) and the OXA-10 subgroup (Trp154Cys and Gly157Asp). Additionally, the OXA-10 subgroup exhibits a duplication of Thr206 and Gly207 in the β5-β6 loop.25 Also, in vivo and in vitro emergence of NS-FDC due to KPC variants (e.g., KPC-41 and KPC-50) has also been reported [19].
- Mutations in FDC's PBP3 target (i.e., 4- amino acid insertion at position 333) reduce the access of FDC to the specific transpeptidase pocket [26,27,28]. Mutations like these do not directly confer resistance but are commonly observed in isolates that produce β-lactamases, such as NDM-type. Such mutations can contribute to reaching a certain level of clinical resistance when associated with other mechanisms [26,27,28].
In addition, emerging mechanisms such as CpxS-mediated regulation of iron uptake have been implicated in FDC resistance, particularly in P. aeruginosa. Such adaptations have been observed in the context of both cooperative protection via siderophores and the selection of heteroresistant subpopulations under prolonged FDC therapy. These findings underscore the need to consider enzymatic and structural resistance determinants, regulatory pathways, and population dynamics when evaluating FDC activity [37,38].
Reduced susceptibility to FDC development during treatment has been observed mainly through translocation events that result in multiple copies of blaNDM genes in Enterobacterales [39]. High-level resistance may also arise in NDM producers due to the selection of mutants in the iron transport systems [40]. Clinical isolates may exhibit various resistance mechanisms [41,42]. Further, P. aeruginosa clinical isolates prone to ceftolozane-tazobactam and ceftazidime-avibactam resistance overall have high cefiderocol MICs, suggesting a role of the pseudomonal-derived cephalosporinase and MexAB systems in cefiderocol non-susceptibility [43]. Notably, for all of these Gram-negative classes, literature emphasize that FDC susceptibility loss is generally via multiple mechanisms compounded rather than one [33,44].
In addition, recent studies have identified clinical carbapenem-resistant Enterobacterales isolates with increased MICs of FDC (MIC > 4 mg/L) that have never been exposed to the drug [45].This may be expected, given that FDC targets the same PBP3 as other cephalosporins and monobactams. Additionally, variants in the omega loop of β-lactamases can also develop following exposure to other β-lactams.
These various proposed resistance mechanisms observed in patients without prior FDC exposure, together with numerous reports of low-barrier resistance emergence to cefiderocol—both in vitro and in clinical settings—underscore the urgent need to refine AST methodologies and better inform clinical treatment decisions.
4. Current Standards and AST Methodologies for FDC
Broth Microdilution (BMD) is the gold standard for assessing FDC susceptibility. This method necessitates using an Iron–Depleted–Cation–Adjusted Mueller-Hinton Broth (ID-CAMHB) with a final iron concentration of ≤0.03 μg/mL, requiring lengthy preparation and posing challenges for routine implementation [46]. However, concerns have been raised regarding variability in BMD results even when using ID-CAMHB prepared according to standards. In particular, differences among commercial reagents—such as the use of manufacturer-supplied versus pure reference cefiderocol powder—may impact MIC values, sometimes skewing results toward higher in vitro activity [47].
Furthermore, the interpretation of the BMD method is complex due to the requirement, specific to the European Committee on Antimicrobial Susceptibility Testing (EUCAST), to observe the first well where a reduction (not absence) of growth occurs, indicated by a button size of less than 1 mm in diameter or the presence of a light haze/turbidity. Interpreting BMD results for FDC can be even more challenging with certain microorganisms, such as Acinetobacter spp., owing to potential trailing effects [8,48] characterized by weak growth across multiple wells [49,50,51].
Several commercial tests have been developed to determine the MIC of FDC using BMD, each offering specific tailored features. However, some of these methods have raised concerns regarding accuracy and reproducibility. In August 2022, EUCAST highlighted the difficulty in interpreting results from certain commercial FDC tests due to these limitations [50]. Similarly, the CLSI Antimicrobial Susceptibility Testing Subcommittee emphasized the need for careful interpretation and standardization of testing procedures [47].
Sensititre™ EUMDROXF by Thermo Fisher, a semi-automated system, uses a standard culture medium rather than an iron-depleted medium, and has been withdrawn from the market due to concerns over its reliability. The ComASP® cefiderocol microdilution panel (Liofilchem, Roseto degli Abruzzi, Italy) and UMIC® cefiderocol strips (Bruker Daltonics GmbH & Co. KG, Bremen, Germany) are manual systems that employ a "ready-to-use" iron-depleted culture medium and are currently among the few available options complying with guideline requirements. Given the variability among BMD-based commercial systems and limited access to standardized testing, both EUCAST and CLSI currently recommend initiating FDC testing with the disk diffusion (DD) method as a first-line approach. If performed adequately with an FDC 30 µg disk according to EUCAST standard recommendations for non-fastidious organisms and calibrated with quality control strains, DD has been considered predictive of susceptibility and resistance outside areas of technical uncertainty (ATUs) [48]. Most studies to date have used the previous ATU definitions; the impact of the updated values remains to be fully evaluated. While narrowing ATUs may improve testing accuracy, some data suggest it could also increase the risk of false negatives [46,52].
Thus, the DD method, currently endorsed by EUCAST as a frontline approach, offers a practical alternative by circumventing the need for an iron-depleted medium [53]. This is because the iron in the standard Mueller-Hinton (MH) broth is believed to form complexes with the agar matrix, simulating an iron-depleted environment. In particular, it has been demonstrated that iron-regulated outer membrane proteins (iROMPs), which function as receptors for siderophore-iron complexes, are expressed on the surface of cells from colonies grown on agar plates. On the contrary, these proteins are absent from the cell membranes of bacteria cultured in standard CAMHB [54]. However, DD carries the burden of ATUs, where strains overlap with MICs on either side of the susceptibility/resistance breakpoint for FDC. This overlap can lead to ambiguity in interpretation of results, thus presenting a challenge for clinicians attempting to make informed treatment decisions [8]. EUCAST advised ignoring the ATU until alternative validated methods were developed to resolve interpretive uncertainties using the zone diameter breakpoints in the breakpoint table [53]. EUCAST also highlighted that the results depend on the quality of the materials used in all AST methods and antimicrobial agents. However, EUCAST did not systematically investigate all products, disks or MH media [53]. In the evaluation of FDC 30 µg disks from Liofilchem, Mast, and Oxoid alongside MH agars from BBL, bioMérieux, Bio-Rad, Liofilchem, and Oxoid, it was found that Oxoid disks and Bio-Rad MH agar produced zone diameters exceeding the acceptable limits for both quality control strains and clinical samples. Combining Oxoid disks with Bio-Rad MH agar further exacerbated this issue, leading to larger zone diameters [53]. CA, EA, and bias parameters were evaluated according to the ISO 20776-2:2021 guidelines for BMD. EUCAST breakpoints served as standards. Acceptable levels were set at 90% for CA and EA, with a permissible bias range of ±30% [53].
There are controversy over appropriate ATUs and narrowing setpoints; some suggesting changes will improve accuracy versus some citing risks of higher false negative rates. Importantly, discrepancies exist among CLSI guidelines (ed. 34, 2024), EUCAST (v.14, 2024) and FDA (version updated on 11/12/2024) as shown in Table 1, suggesting that even with DD AST, clinical microbiologist lack consensus on approaches to detecting FDC resistance. Further, EUCAST has yet to release BMD and DD breakpoints for two gram-negatives: Acinetobacter spp. and Stenotrophomonas maltophilia [50,55]. EUCAST provides an essential guide for interpreting inhibition zones, suggesting that diameters larger than 17 and 20 mm for disks containing 30 mcg FDC typically correspond to MIC values BELOW the PK/PD susceptibility breakpoint (<2 mg/L) for A. baumannii and S. maltophilia, respectively [55].
Regarding AST methods that rely on alternative approaches, different from BMD and DD, a recent study aimed to develop a rapid culture-based test (namely Rapid Cefiderocol NP test) to detect FDC resistance in MDR Enterobacterales [56]. This test leverages the metabolic activity of glucose in the presence of FDC at a concentration of 64 mg/L in an iron-depleted CAMHB medium. It also uses a color change from red to yellow in red phenol, a pH indicator, to visually signify bacterial growth [56]. Evaluated using 74 clinical enterobacterial isolates, the test demonstrated a high sensitivity of 98% and a specificity of 91%compared to the standard BMD method [55]. Remarkably, the Rapid Cefiderocol NP test delivered results within three hours, significantly reducing the time required for susceptibility testing [56]. Additional confirmation of this test across various laboratories, involving a broader and more varied collection of FDC-non susceptible and -susceptible enterobacterial isolates, is essential to comprehensively validate its efficacy and reliability. An equivalent Rapid Cefiderocol NP test for A. baumannii has been developed [57] This test relies on bacterial viable cells reducing resazurin to resorufin, which shifts the color from blue to violet or pink, indicating bacterial growth in the presence of FDC at a concentration of 38.4 mg/L. Using 95 randomly selected A. baumannii isolates, the test demonstrated a sensitivity of 95.5% and a specificity of 100% compared to BMD with only a single VME identified [57]. These findings suggest that NP-based methods may represent a rapid alternative for screening purposes. However, these tests are not currently commercially available, and further comparative studies—including functional in vitro assays and clinical correlation analyses—are required to establish their reliability, practical utility, and potential advantages over existing gold-standard methods.
ATU limitations and discrepancies of breakpoints, prompt questions of best ways to assess FDC AST. The Gradient Strip Test (specifically the MIC Strip Test by Liofilchem) (Roseto degli Abruzzi, Italy) uses a strip with a gradient of FDC concentrations to determine MIC but is only validated for P. aeruginosa and should not be used with other pathogens (Enterobacterales or A. baumannii) as it may lead to reporting of false susceptibles (VME) [58,59,60]. Agar dilution was assessed by Albano et al. who using 610 gram-negative bacilli. While tested against standard and iron-depleted broth microdilution (BMD), the agar dilution method showed poor agreement with BMD, variable categorical agreement (47–93%), and frequent errors. It tended to yield higher MICs and failed to meet accuracy thresholds, indicating it is not reliable for FDC MIC testing [61].
However, it could be important to underline that while ID-BMD remains the reference method, limitations have been reported, particularly in non-fermenters such as A. baumannii, where reproducibility issues and incomplete alignment with clinical outcomes have been described elsewhere [62]. Ibrahim et al. developed the SuperFDC medium, which is not currently commercially available, to detect Enterobacterales, P. aeruginosa, and A. baumannii strains with FDC reduced susceptibility. The medium, which consisted of 8 mg/L FDC added to iron-deficient agar, was tested on 68 susceptible and 33 resistant GN bacteria with various β-lactam resistance mechanisms. The SuperFDC demonstrated 97% sensitivity and 100% specificity, with only 3% VME compared to the reference BMD. Furthermore, it showed satisfactory performance, with a 10–103 cfu/mL detection limit in spiked stool tests [63].
5. Variability in Testing Outcomes Across Different Microorganisms
Our analysis focused only on Enterobacterales, A. baumannii, and P. aeruginosa, as these are the primary GN bacteria responsible for difficult-to-treat infections. The MIC and inhibition zone diameters of these bacteria have been reported to fall below and above the susceptibility breakpoints, sometimes within ATU [46,64]. On the other hand, species such as Burkholderia pseudomallei, Achromobacter spp., and S. maltophilia are usually found to be susceptible to FDC, displaying low MIC90 values and wide inhibition zones, which facilitate a more straightforward interpretation of the data [46,64,65].
5.1. Enterobacterales
Table 2 details studies reporting the performance of various AST methods compared with the reference BMD method for Enterobacterales. Three out of eight studies utilized the standard homemade BMD method as their reference, whereas the others employed commercial BMD or frozen panels.
Matuschek et al. evaluated the reproducibility of FDC MIC determination using ID-CAMHB BMD (frozen 96-well microtitre plates - Thermo Scientific, Oakwood, USA) and EUCAST DD across 263 isolates, including E. coli and K. pneumoniae. Although not included in Table 2 due to the absence of CA or EA data, the study tested 30 μg FDC disks from two manufacturers (Liofilchem and Mastdisc) on cation unsupplemented MHA plates prepared in-house from two manufacturers (Oxoid, Thermo Fisher Scientific, Basingstoke, UK) and BBL (Becton Dickinson, Sparks, NV, USA). DD showed overall reproducibility and highlighted a zone overlap (18–22 mm) between susceptible (≤2 mg/L) and resistant (>2 mg/L) isolates, underscoring the relevance of confirmatory MIC testing within the ATU range. The study also noted high MIC variability in wild-type strains, potentially linked to differences in iron transporter and siderophore expression [66].
Accordingly, other authors have concluded that while BMD remains the reference standard for AST in Enterobacterales, DD can provide a reliable alternative for initial susceptibility testing [67]. Morris et al. used BMD and DD with research-use-only 30 μg cefiderocol Mastdiscs (Mast Group Ltd., Bootle, UK) to evaluate the susceptibility in 58 isolates of carbapenem-resistant Enterobacterales (CRE) and 50 isolates of non-fermentative GN bacilli [67]. Results indicated a susceptibility rate ranging from 72% (FDA criteria) to 90% (CLSI criteria), a variation that underscores the impact of different regulatory standards on susceptibility outcomes. With DD interpreted according to the EUCAST criteria, a non-susceptibility of 65% and 66% was found compared to 74% and 72% for the FDA criteria and 87% and 89% for CLSI, respectively, with HardyDisks and Mastdiscs. CA ranged from 75% to 90%, with ME present in percentages varying from 8% to 25%, mE from 0 to 19%, and VME from 0 to 20%, considering the variability of disks and breakpoints evaluated [67]. Bonnin et al. focused specifically on CRE, applying various methodologies including CE-IVD BMD plate (ThermoFisher) using regular MH broth, MTS (Liofilchem), and DD (Liofilchem), which were compared to a frozen BMD plate prepared with iron depleted MH broth. [60] Interestingly, the first phase of the study assessed comparability between commercial CE-IVD BMD (Sensititre™ EUMDROXF) and standard BMD.
The method showed strong concordance with the reference BMD (CA 95%, EA 87%, VME 2.8%, ME 1.6%), while MTS strips performed poorly, with a VME rate of 94.9%, highlighting their limited reliability in this setting [60]. However, test strips are not approved for Enterobacterales but only for P. aeruginosa. The second phase of the study was a prospective comparison between DD and CE-IVD BMD with EUCAST breakpoints among 827 Enterobacterales (76.7% carbapenemase producers including 426 OXA-48-like, 55 VIM-, 118 NDM- and 9 KPC-producers) [60]. The results revealed that 77% of the isolates were accurately categorized by DD, although with a considerable rate of VMEs (35.9%) and a MEs of 1.6%. Notably, of the VME cases, 21 out of 22 had MIC values of 4 mg/L, suggesting an acceptable edge of technical error within two dilutions. The study revealed wide MIC distributions and notable variability in inhibition zones, particularly among carbapenemase-producing or highly resistant strains. Approximately 21.3% of isolates fell within the ATU, requiring BMD confirmation. Overall, the method showed performance comparable to standard BMD for assessing FDC susceptibility [60]. Focusing on a set of 60 CRE, another study by Emeraud et al. concentrated on the performance of two commercial tests, ComASP® FDC microdilution panel and UMIC® FDC, compared with a frozen panel containing FDC in ID-CAMHB prepared by Thermo Fisher (Sensititre™ CML1FEUD plate) and stored according to EN ISO 20776-1:2019 and CLSI document M07, which was used as the reference method on 60 CREs [68]. The study revealed an FDC sensitivity rate of 70% when tested with ComASP® FDC microdilution panel, with an EA of 76.7% and a CA of 83%. However, the method also showed a high VME rate of 34.5% (10 strains falsely classified as susceptible), indicating discrepancies in resistance detection compared with the BMD standard. In contrast, UMIC® FDC aligned better with the BMD results, with a sensitivity rate of 58.3%, an EA of 91.7%, and a CA of 83.3%. The VME rates were 24.1% (7 strains falsely classified as susceptible) and 6.9% of the VMEs out of the EA, respectively [68]. The studies by Bianco et al. in 2023 and 2024 have also yielded significant findings on the AST for FDC in Enterobacterales, as well as other GN bacteria [69,70]. The 2023 study by Bianco et al. FDC testing was performed using DD according to EUCAST guidelines. Cation-adjusted MHA (Becton-Dickinson, Franklin Lakes, NJ, USA) and a FDC 30µg disk (Oxoid Ltd., Basingstoke, UK) were used. Sequentially, the ComASP® FDC microdilution panel and the reference BMD were used in parallel to test FDC on isolates that presented ATU or non-interpretable results by DD [69].
The ComASP® panel showed high concordance with BMD (CA 92.1%) in isolates with uninterpretable DD results, with only three discrepancies—one being a VME—all near the MIC threshold. Among CREs within the ATU, 20% were resistant by both methods [69]. DD method allowed the assessment of FDC susceptibility in 78.6% of Enterobacterales. Furthermore, 23.7% of strains exhibiting ATU results were found to be resistant according to the reference BMD method, with MICs ranging from 4 to 16 mg/L. Additionally, 20.5% of CRE showing ATUs were determined to be resistant by both the ComASP® FDC microdilution panel and the reference BMD technique [69].
In 2024, Bianco et al. evaluated UMIC® FDC and DD for assessing FDC susceptibility across a broader range of GN bacteria, including 90 Enterobacterales isolates. [70]. The UMIC® FDC demonstrated an EA of 81.1%, CA of 91.1%, and a bias of +26.7%. It showed only one VME where the MIC was 2 mg/L compared to the reference 4 mg/L, and seven MEs, primarily with MIC 4 mg/L versus reference 2 mg/L. A general trend of MIC overestimation was noted (bias + 24.2%), leading to 12 MEs (7.4%). The majority of VME and ME fell within the EA range (+2-fold dilution). For strains with a reference MIC below 0.5 mg/L, over 80% of MICs were outside the EA [70]. DD exhibited a CA of 81.1% and EA of 91.1% values. High rates of ATU were observed in the Enterobacterales (37.8%). Only 11.8% of cases falling into the ATU corresponded to MICs in the resistance range [70]. In 2023, a study by Bovo et al. specifically examined the performance of FDC ASTs on 75 clinical isolates of KPC-producing K. pneumoniae [71]. The authors utilized three testing methods: a standard BMD fresh panel, DD, and MTS. DD showed a CA of 92% and a ME of 16.7%. There were no VMEs, indicating that DD is a valuable method for the initial screening [71]. MTS had a CA of 90.7% and showed a higher rate of VME at 17.9%, indicating discrepancies in measuring the resistance. The agreement was even lower at 82.7% between DD and MTS, with ME significantly higher at 30.2%, reflecting the inconsistencies between these two methods [71]. Finally, another recent study, presented at ESCMID 2024 by Leonildi and colleagues, explored the susceptibility of 30 NDM-producing K. pneumoniae isolates to FDC by comparing ComASP® FDC microdilution panel and UMIC® FDC, alongside DD, to the BMD reference method. DD showed inhibition zones ranging from 20-24 mm, which in 74% of cases fell into the ATU, complicating the interpretation. The study found 100% EA and CA between BMD and commercial tests [52].
5.2. Pseudomonas aeruginosa
Table 3 details studies reporting the performance of various AST methods compared with the reference BMD method for P. aeruginosa. Two of the five studies utilized the standard homemade BMD method as their reference, while the others employed commercial BMD or frozen panels.
Morris et al. reported wide variability in FDC susceptibility rates for carbapenem-resistant P. aeruginosa (57–93%), depending on the breakpoint criteria used, with CLSI breakpoints yielding the highest susceptibility [67]. Correlation between DD (HardyDisks and Mastdiscs) and BMD showed variability: 4 of 9 isolates appeared more susceptible and 5 more resistant by DD, unlike Enterobacterales, which tended to show higher susceptibility by DD. Both DD methods demonstrated acceptable CA, ranging from 79%. (HardyDisks with EUCAST breakpoints) to 93% (HardyDisks and Mastdiscs with CLSI breakpoints) [67]. Dortet et al. evaluated the performance of UMIC® FDC against standard BMD in various GN bacteria, including P. aeruginosa, in terms of analytical (inter-operator, execution cycle, site, execution day, batch) and clinical performance. The overall reproducibility of the method was high (>95%) for all parameters and the overall clinical performance according to the ISO 20776-2.2021 target with EA >90% and -30%<bias<30%. In particular, the study found that UMIC® FDC provided reliable susceptibility testing results, showing a CA of 98.0% (95% CI: 89.3%–99.6%) and EA of 93.9% (95% CI: 83.5%–97.9%) for P. aeruginosa. The test performed better in non-fermenters than in Enterobacterales, where it tended to underestimate MICs—likely due to the higher prevalence of MBL producers, which were associated with elevated FDC MICs [72]. In Bianco et al. 2024, the UMIC® FDC method aligned closely with BMD, although, as already mentioned, the effectiveness varied between different approaches and bacterial strains [70]. It is worth underlining that before carrying out the evaluations on 13 FDC-susceptible non-fermenting GNB (MIC ≤2 mg/L), Bianco et al. 2024 carried out in vitro resistance induction experiments to have a greater breadth of MICs for testing [70]. With this step, 48 isolates with different degrees of reduced susceptibility or frank resistance to FDC were obtained and included for the evaluations of both methods. CA among P. aeruginosa strains was 90% (n = 36/40) with EA rate of 92.5% (n= 37/40). In this study, DD generally showed a high CA ranging from 94.9 to 100% regardless of the disk manufacturer in Enterobacterales, P. aeruginosa, and A. baumannii, according to EUCAST breakpoints. One VME was observed in P. aeruginosa for Oxoid (23 mm versus reference MIC, 16 mg/L). P. aeruginosa isolates with zone diameters falling within the ATU range of 14-22 mm demonstrated a higher resistance rate (68.7%) compared to Enterobacterales [70]. The ATU limit for P. aeruginosa was lowered to 20-21mm in the EUCAST v14 update, which would result in several cases being excluded. In contrast, the ATU defined by CLSI and FDA (14–22 mm) has not been modified to date. These discrepancies likely stem from differences in dataset size, clinical correlations, and timing of breakpoint updates. Further harmonization and prospective validation are needed to refine DD interpretive criteria across systems. In Bianco et al. 2023, 11.9% of P. aeruginosa isolates exhibited inhibition zones inside the ATU. All P. aeruginosa tested susceptible (MICs range: 0.06–2 mg/L) with ComASP® cefiderocol microdilution panel and reference BMD [69]. Disk diffusion allowed the determination of FDC susceptibility in 88.1% of strains, with all VIM-producing P. aeruginosa showing MIC values in the susceptible range (2 mg/L) [69]. Devoos et al. (2022) examined a collection of 150 clinical strains of P. aeruginosa resistant to ceftazidime (MIC>8 mg/L), imipenem (MIC>4 mg/L), and ceftolozane/tazobactam (MIC>4mg/L).73 FDC susceptibility was tested using DD (three disk brands on six MHAs), MTS, and Sensititre microplates, compared to reference BMD. Only DD achieved acceptable overall CA. Sensititre overestimated MICs (CA 86.7%, EA 69.3%, bias +68.2%), while MTS underestimated them (same CA and EA, bias –30.4%), correctly identifying just 50% of resistant strains [73]. Finally, the overall rate of CA for the 18 combinations of disks and MHA applied to the collection of clinical strains was 84.0%, with variations ranging from 78.0% to 89.3%. Acceptable CA rates, irrespective of the disk brand (excluding ATU), were achieved using Becton Dickinson (ranging from 94.0% to 95.5%), bioMerieux (ranging from 91.8% to 93.0%), and Mast MHA (ranging from 91.1% to 92.7%) [73]. It is worth noting that 20 isolates displayed microcolonies in the zone of inhibition for at least one combination of disks and MHA. These were more frequently observed with the Mast disc and MHA from Becton Dickinson, BioMérieux, Mast, and Oxoid [73]. While DD proved acceptable for assessing FDC susceptibility, substantial variability in inhibition zones was observed across disk–MHA combinations, including with the quality control strain—likely due to batch-dependent differences in MHA iron content (0.35- 1.03 mg/L) [73].
5.3. Acinetobacter baumannii
Studies comparing the performance of various AST methods to a reference BMD method for A. baumannii are detailed in Table 4. Four out of seven studies used the standard homemade BMD method as their reference, while the others used commercial BMD or frozen panels.
It is important to note that for Acinetobacter spp., although EUCAST (2024) has not set specific FDC clinical breakpoints, there is currently only a PK/PD breakpoint (≤2 mg/L or ≤17 mm) defined. Meanwhile, CLSI provides breakpoints for A. baumannii complex (≤4 mg/L or ≥15 mm as susceptible and ≥16 mg/L as resistant) [47,52]. Therefore, we refer to isolates with MICs exceeding the PK/PD breakpoint as "reduced susceptibility"; however, this does not mean clinical resistance and should be interpreted cautiously.
Jeannot et al. tested the standard BMD and DD with three types of disks (Mast Diagnostic, Liofilchem, and Oxoid), UMIC® FDC, and ComASP® cefiderocol microdilution panel among 97 clinical isolates of A. baumannii with reduced susceptibility to at least one carbapenem. DD assays were carried out following the EUCAST guidelines. Using the reference BMD method, 43.3% of the strains were classified as strains with a reduced susceptibility to FDC [58]. For the comparison between BMD and the ComASP® cefiderocol microdilution panel, EA was recorded at 81.4% and CA at 95.9%, with biases of -36.1% and +28.9%, respectively. In the matchup between BMD and UMIC® FDC, EA was 78.4%, CA was 93.8%, and bias was -42.3%. Four strains were sensitive to one of the two commercial BMD methods but not susceptible to the reference BMD; of these, two were misclassified by both [58].
In the comparison between BMD and MTS, EA was reported at 59.8%, with a CA of 76.3%. The bias was -48.4%; however, the lower value observed was -62.9%. Using gradient strips, 55% of strains with a reduced susceptibility to FDC were incorrectly classified as susceptible [58]. When comparing BMD with DD, CA varied between 72.2% and 81.4%, depending on the type of disk used. The study identified microcolonies within the inhibition zones on all three types of disks, affecting 10 isolates (eight non-susceptible and two susceptible). While susceptible strains were correctly identified, resistant strains were misclassified in 42.9% (MAST), 50% (Liofilchem), and 64.3% (Oxoid) of cases. These errors were unrelated to β-lactam resistance mechanisms or strain backgrounds but correlated with gene expression; notably, PER-type β-lactamase and NDM producers were frequently resistant [58]. In the same study Authors also suggest that DD inhibition zones between 17 and 22 mm may include isolates that are non-susceptible by BMD, and propose a higher cut-off of 22 mm to reduce the risk of underestimation of resistance [58]. EUCAST has recently received these suggestions and updated its guidelines accordingly, although official breakpoints have yet to be defined [74].
Similarly, Kolesnik-Goldmann and colleagues utilized a collection of 100 carbapenem-resistant A. baumannii strains to compare the performance of BMD with fresh panels, DD on two commercial ID-CAMH agar plates (from bioMérieux and Liofilchem), and a homemade version, UMIC® FDC and ComASP® cefiderocol microdilution panel. Additionally, MTS was performed on two commercial CAMH agar plates (BioMerieux and Liofilchem) and a homemade ID-CAMH [59]. The study used both the CLSI clinical breakpoints and the EUCAST PK-PD breakpoint, and the methods were extended with whole-genome sequencing and typing for thorough evaluation [59]. In specific comparisons, BMD against the ComASP® cefiderocol microdilution panel yielded an EA of 76% and CA rates of 86% according to CLSI and 88% according to EUCAST standards, respectively, with VME reported at 6/100 with CLSI and 7/100 with EUCAST readings. UMIC® FDC showed 76% EA and CA values of 86% (CLSI) and 89% (EUCAST), with VMEs slightly higher under EUCAST (9%) than CLSI (3%), indicating variability across interpretive standards [59]. The MTS demonstrated variability influenced by the type of media used. Using the homemade ID-CAMH, the EA was the highest at 75%, while with commercial media from Biomerieux and Liofilchem, it dropped to 57% and 44%, respectively. The CA remained similar across all media types at 87%, 85%, and 88%. However, VME varied more substantially, recorded at 2%, 10%, and 6.9%, respectively, highlighting media choice's significant impact on the accuracy of susceptibility tests [59]. Morris et al. reported a CA of 64% for both CLSI and EUCAST when comparing DD to Sensititre™ BMD, with VMEs of 0% (CLSI) and 33% (EUCAST), and MEs of 20% and 25%, respectively [67].
The study by Bianco et al. 2023 showed a high CA of 97.9% with no VMEs, highlighting a highly reliable agreement between DD and the standard BMD reference method. Only a 2.1% occurrence of MEs suggests a strong performance in accurately categorizing strains [69]. MIC determinations obtained by ComASP® cefiderocol microdilution panel and reference BMD on the 7 A. baumannii isolates that achieved ATU by DD revealed that 6 isolates (85.7%) were NS (MICs range: 4–16 mg/L) [65].
Bianco and colleagues also detected high agreement rates in comparing DD and BMD in 2024, who reported a CA of 94.9% and a CA of 89.7% in comparing DD or UMIC® FDC with BMD, respectively. Also in this study, susceptibility was interpreted according to EUCAST clinical breakpoints (v. 13.0 2023) The study also noted MEs and VMEs at 3% for DD versus BMD, reflecting minor discrepancies that might affect interpretation but generally suggest a reliable testing method [70]. Dortet et al. reported 90% EA and 84.1% CA for UMIC® FDC, with a bias of –11.4% and an ME rate of 6.8%. Results were interpreted using non-species-specific PK/PD EUCAST breakpoints (susceptible ≤2 mg/L) [72].
Finally, Liu et al. compared DD with standard BMD using CLSI and EUCAST breakpoints. Overall CA was high: 98.1% (CLSI) and 97.0% (EUCAST), with VME rates of 0.9% and 1.9%, respectively. For carbapenem-susceptible A. baumannii, CA was 100% with no errors. In carbapenem-resistant strains, CA remained high (97.5% CLSI; 96.2% EUCAST), with low VMEs. Among difficult-to-treat isolates, CA was 97.6% (CLSI) and 95.7% (EUCAST), with VMEs of 1.2% and 3.1% [75].
6. Expert Opinion and Discussion
FDC represents a crucial option for treating infections caused by MDR GN bacteria, particularly due to its unique mechanism of action as a siderophore cephalosporin. Its ability to bypass many resistance mechanisms, including efflux pumps and porin loss, makes it especially effective against strains producing metallo-β-lactamases, which are typically resistant to most available β-lactams. Additionally, FDC shows promising activity against Acinetobacter spp., a pathogen often associated with severe MDR infections, positioning it as a valuable therapeutic option in challenging clinical scenarios. For carbapenem-resistant A. baumannii isolates, however, the interpretation of susceptibility results requires caution as, as we also report in this review, some discrepancies between MIC values and clinical outcomes have been observed [62]. These data highlight the importance of ongoing efforts to optimize AST methods and interpretive criteria for this specific pathogen, to better guide therapeutic decision-making.
Evaluating antimicrobial susceptibility to FDC involves unique challenges due to its dependency on low iron levels for efficacy, a mechanism designed to mimic the human body's low iron availability [67,76]. Consequently, the BMD method requires using ID-CAMHB, established as the reference standard. Nonetheless, preparing this medium proves cumbersome for the routine operations of clinical laboratories, highlighting the need for more adaptable and efficient methodologies. The variability in interpretive guidelines from standard-setting bodies like CLSI, FDA, and EUCAST further complicates susceptibility assessments for FDC. Moreover, wider MIC distributions observed in wild-type strains compared to other antibiotics might be attributable to variations in iron transporter and siderophore expression, which could modulate drug uptake leading to MIC variability rather than indicating poor reproducibility of the BMD method [66]. The ATU serves as an important indicator within the testing process, alerting to potential interpretative challenges. Results within this zone can prompt actions such as 1) retesting, 2) applying alternative methodologies, or 3) reporting uncertainties in the findings.
Given these complexities, we identified a need for developing guidance frameworks tailored to FDC AST, especially for pathogens like Enterobacterales, P. aeruginosa, and A. baumannii, the primary GN bacteria responsible for difficult-to-treat infections. These frameworks could be of use not only for addressing specific challenges clinical microbiologists face in their daily routines but also for facilitating rapid and effective clinical downstream decision-making in treating infections caused by MDR-GN bacteria.
DD has emerged as a valuable initial screening method in the realm of FDC susceptibility testing for Enterobacterales and CRE. It typically achieves CA rates that exceed 88% and, in some cases, reach as high as 100% [67,70,71]. This level of reliability, coupled with the method's low or null rates of VMEs, underscores its suitability for assessing FDC susceptibility, particularly in settings where rapid and reliable results are crucial [67,70,71]. As VMEs were relatively uncommon, the occurrence of MEs suggests that confirmation with BMD should be focused on resistant results, which are more prone to misclassification and carry greater clinical implications [67,70,71]. This practice is encouraged to ensure the accuracy of antimicrobial susceptibility testing, given also the low rate of FDC resistance. However, it should be noted that the performance of DD can be significantly influenced by the choice of disks and media [60]. For example, studies have shown suboptimal results when using BioRad Mueller-Hinton agar combined with Liofilchem disks, particularly with a high incidence of VMEs among CRE isolates [60]. This finding points to the critical need for meticulous selection and standardization of materials in clinical laboratory settings to ensure test accuracy.
Among the MIC-based approaches, the UMIC® FDC system has shown to be reliable as an adjunct to DD, boasting EA rates above 90% and CA rates over 83%, although with VMEs noted in some isolates as high as 16.7% [52,68,70,72]. Its valid performances, which present only a slight tendency to undercall MICs, suggest that it could serve well in conjunction with DD when standard BMD is not feasible.
This integration approach, agreed upon by other authors, could provide a more comprehensive assessment of FDC susceptibility and offset some of the feasibility limitations observed with conventional BMD techniques [67,70].
On the other hand, MTS has been found inadequate for this testing context due to significant accuracy and reliability issues [60,67,71]- Likewise, the ComASP® cefiderocol microdilution panel has yielded limited and less satisfactory data than the UMIC® FDC system [68,69].
Similarly, for P. aeruginosa, the UMIC® FDC system emerges as the most accurate commercial BMD method currently available with CA and EA > 90% and no VME and low ME (2% and 8%) [70,72]. In contrast, the performance of MTS, which, despite being marketed explicitly for use with P. aeruginosa, tends to yield suboptimal results [73]. The reliance on DD as a standalone test is not suggested as while it shows performances in terms of CA rates ranging from 78% to 100% and low ME rates, significant variations in inhibitory zones depending on the disk and MHA combinations, even among quality control strain [67,69,70,73]. Furthermore, the ATU as a sole indicator does not adequately address the interpretative challenges associated with this testing.
Based on these considerations, our proposed decision-making framework for testing FDC susceptibility in Enterobacterales and P. aeruginosa initiates with DD to preliminarily screen isolates as susceptible, non-susceptible, or falling within the area of technical uncertainty (ATU) (Figure 1). For isolates deemed non-susceptible by DD, we suggest confirmatory testing using either the UMIC® FDC system or, where available, the standard BMD technique with iron-depleted media. Also, if feasible, we suggest sending the sample to a reference laboratory. Following this, if UMIC® is used and the result is susceptible, a standard BMD confirmation step is recommended. However, no further repetition is required if the initial confirmatory test has already been performed with standard BMD. For isolates within the ATU, we recommend retesting with UMIC® or standard BMD to refine the categorization. DD results indicating susceptibility do not routinely require confirmation. This structured approach to testing is designed to enhance the reliability of the results by systematically addressing the interpretative challenges posed by FDC susceptibility testing, thereby utilizing the strengths of each method in sequence to ensure accurate and dependable outcomes (Figure 1).
Considering the available data for A. baumannii complex. DD is applicable as it shows acceptable performance in terms of CA but is conditional on disk types and media, with maximum values reaching >90% [58,59,67,69,70,75]. In this setting, there is a critical need to reevaluate the sensitivity cutoffs because numerous strains, showing inhibition zone diameters ranging between 17 mm and 22 mm - which would categorize them as susceptible – prove to be non-susceptible when tested using the reference BMD method. Despite commercial BMD methods not fully meeting ISO standards, they do exhibit valuable CA rates of 88-95.9% and 89-97.4% for the ComASP® cefiderocol microdilution panel and UMIC® FDC system, respectively [59,70,72,73] MTS is not recommended in this context due to its limited accuracy [59].
For A. baumannii complex, we agreed on a decision-making framework that begins with disk diffusion (DD). We recommend the following stepwise approach: isolates with inhibition zones <17 mm are to be considered non-susceptible and should undergo confirmatory testing using a standard BMD method with iron-depleted media; those with zones between 17 and 22 mm should be retested using a commercial BMD method such as UMIC® or ComASP®. Importantly, we acknowledge that this approach may not eliminate the risk of VMEs, particularly in isolates near the current ECOFF, and we explicitly recommend further confirmation with BMD whenever possible, especially in critical clinical contexts or when inhibition zones fall within this intermediate range. Isolates with zones ≥23 mm may be considered susceptible without further testing (Figure 2). Although our proposed framework for A. baumannii susceptibility testing appears less complex than other pathogens, this reflects the currently limited availability of harmonized approaches and standardized breakpoints for this species.
The first note specifies that for inhibition zones equal to or greater than 17 mm, a footnote should be appended to the report indicating an expected MIC value of ≤ 2 mg/L. The second note addresses potential forthcoming adjustments in the reference values, suggesting a shift from the current epidemiological cut-off (ECOFF) of 18 to a new breakpoint of 19. These amendments aim to refine the interpretative accuracy of test results and ensure that susceptibility reporting remains aligned with evolving scientific standards.
The proposed decision-making frameworks aim to strike a pragmatic balance between diagnostic accuracy and practical feasibility. It is oriented toward reducing the likelihood of overestimating resistance, which could lead to unnecessary therapeutic exclusions. Moreover, while more conservative strategies—focused on minimizing the risk of false susceptibility—may offer advantages in selected contexts, they typically require broader and repeated implementation of reference BMD testing, which is not always operationally sustainable. That said, alternative confirmation by standard BMD or reference laboratory referral remains essential where UMIC® is not yet available. In these terms, recent multicenter data from Koeth et al. suggests that ComASP® may offer reliable performance for A. baumannii, supporting its use as an alternative to UMIC® for confirmation testing in settings where access is limited [77].
7. Conclusions
To date, real-world evidence has highlighted the role of FDC in treating infections caused by carbapenem-resistant or extensively resistant GN bacteria, particularly in critically ill or immunocompromised patients. Accurate and efficient testing is crucial to ensure that this antimicrobial agent can be utilized effectively in clinical scenarios, where it represents a crucial treatment option. A limitation of our study is the relatively small number of studies currently available for review, positioning our work as a snapshot of the present state of AST for FDC. Recognizing this, we briefly identified the current research gaps and suggested future directions for investigation, as outlined in Box 1. This approach underscores the commitment to advancing the field and supporting the clinical use of cefiderocol as an indispensable option in the antibiotic arsenal.
| Box 1. Gaps in the current research and suggestions for future studies. | ||
| Specific Gaps | Implications | Future Research Suggestions |
| Heterogeneity in Study Design | Diverse methodologies across studies lead to difficulty in comparing and synthesizing results. | Standardize and clearly report frameworks in AST studies to ensure consistency and comparability. |
| Small Sample Sizes | Limited sample sizes reduce the statistical power and generalizability of findings. | Implement multicenter studies to gather larger, more diverse bacterial isolates and enhance the representativeness of results. |
| Use of Standard Reference Strains Only | Reliance solely on ATCC strains might not accurately represent clinical scenarios. | Incorporate clinical isolates with known resistance profiles as controls in testing protocols. |
| Longitudinal Surveillance | Evolving resistance patterns are not adequately monitored over time, affecting the relevance of AST protocols. | Conduct longitudinal surveillance studies to monitor resistance evolution and method efficacy. |
| Variations in ATU | Changes in ATU boundaries may impact susceptibility interpretations, increasing variability in results. | Evaluate the influence of ATU variations on susceptibility testing outcomes and explore strategies to minimize inconsistencies. |
Author Contributions
SS, SS, GR, FA, CV and LP all contributed to conceptualization, methodology, writing, supervision, and finalization of the manuscript.
Funding
Editorial Assistance and advisory board activities were supported by Shionogi Srl.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
Osmosia, Italy, provided medical writing and editorial assistance in preparing this manuscript.
Conflicts of Interest
SS, SS, FA, CV and LP declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. GR declares that has received in the last 3 years support to the laboratory from Shionogi; Biomedical Service (distributor of Merlin). Consulting honoraria from Shionogi and Speakers bureau and manuscript writing from Shionogi.
Abbreviations
The following abbreviations are used in this manuscript:
| FDC | Cefiderocol |
| AST | Antimicrobial susceptibility testing |
| BMD | Broth microdilution |
| ID-CAMHB | Iron-depleted cation-adjusted Mueller-Hinton broth |
| ATUs | Areas of technical uncertainty |
| CRE | Carbapenem-resistant Enterobacterales |
| DD | Disk diffusion |
| S | Susceptible |
| R | Resistant |
| AMR | Antimicrobial resistance |
| GN | Gram-negative |
| ICU | Intensive Care Units |
| CAESAR | Central Asian and European Surveillance of Antimicrobial Resistance |
| EARS-Net | European Antimicrobial Resistance Surveillance Network |
| MBLs | metallo- β -lactamases |
| CR | carbapenemase-resistant |
| CA | Categorical Agreement |
| EA | Essential Agreement |
| VME | Very Major Errors |
| ME | Major Errors |
| mE | minor errors |
| NS-FDC | non-susceptibility to FDC |
| MH | Mueller-Hinton |
| iROMPs | iron-regulated outer membrane proteins |
| ECOFF | epidemiological cut-off |
References
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2023 – 2021 Data. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2023-2021-data (accessed on 5 June 2025).
- Centers for Disease Control and Prevention (U. S.). Antibiotic Resistance Threats in the United States; CDC: Atlanta, GA, USA, 2019; Available online: https://stacks.cdc.gov/view/cdc/82532 (accessed on 5 June 2025).
- Ong'uti, S.; Czech, M.; Robilotti, E.; et al. Cefiderocol: A New Cephalosporin Stratagem Against Multidrug-Resistant Gram-Negative Bacteria. Clin. Infect. Dis. 2022, 74, 1303–1312. [Google Scholar] [CrossRef]
- Sato, T.; Yamawaki, K. Cefiderocol: Discovery, Chemistry, and In Vivo Profiles of a Novel Siderophore Cephalosporin. Clin. Infect. Dis. 2019, 69 (Suppl 7), S538–S543. [Google Scholar] [CrossRef]
- Kaye, K.S.; Naas, T.; Pogue, J.M.; et al. Cefiderocol, a Siderophore Cephalosporin, as a Treatment Option for Infections Caused by Carbapenem-Resistant Enterobacterales. Infect. Dis. Ther. 2023, 12, 777–806. [Google Scholar] [CrossRef]
- Marino, A.; Stracquadanio, S.; Campanella, E.; et al. Intravenous Fosfomycin: A Potential Good Partner for Cefiderocol. Clinical Experience and Considerations. Antibiotics 2022, 12, 49. [Google Scholar] [CrossRef] [PubMed]
- Brauncajs, M.; Bielec, F.; Macieja, A.; et al. Cefiderocol – An effective antimicrobial for MDR infections but a challenge for routine antimicrobial susceptibility testing. Adv. Med. Sci. 2024, 69, 256–263. [Google Scholar] [CrossRef]
- Simner, P.J.; Patel, R. Cefiderocol Antimicrobial Susceptibility Testing Considerations: The Achilles' Heel of the Trojan Horse? J. Clin. Microbiol. 2020, 59, e00951–20. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Rousaki, M.; Vassilopoulou, L.; et al. Global prevalence of cefiderocol non-susceptibility in Enterobacterales, Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia: a systematic review and meta-analysis. Clin. Microbiol. Infect. 2024, 30, 178–188. [Google Scholar] [CrossRef]
- Yamano, Y.; Ishibashi, N.; Kuroiwa, M.; et al. Characterisation of cefiderocol-non-susceptible Acinetobacter baumannii isolates from Taiwan. J. Glob. Antimicrob. Resist. 2022, 28, 120–124. [Google Scholar] [CrossRef]
- Poirel, L.; Sadek, M.; Nordmann, P. Contribution of PER-Type and NDM-Type β-Lactamases to Cefiderocol Resistance in Acinetobacter baumannii. Antimicrob. Agents Chemother. 2021, 65, e00877-21. [Google Scholar] [CrossRef]
- Poirel, L.; Ortiz de la Rosa, J.M.; Sakaoglu, Z.; et al. NDM-35-Producing ST167 Escherichia coli Highly Resistant to β-Lactams Including Cefiderocol. Antimicrob. Agents Chemother. 2022, 66, e00311-22. [Google Scholar] [CrossRef] [PubMed]
- Nurjadi, D.; Kocer, K.; Chanthalangsy, Q.; et al. New Delhi Metallo-Beta-Lactamase Facilitates the Emergence of Cefiderocol Resistance in Enterobacter cloacae. Antimicrob. Agents Chemother. 2022, 66, e02011-21. [Google Scholar] [CrossRef]
- Ito, A.; Sato, T.; Ota, M.; et al. In Vitro Antibacterial Properties of Cefiderocol, a Novel Siderophore Cephalosporin, Against Gram-Negative Bacteria. Antimicrob. Agents Chemother. 2017, 62, e01454-17. [Google Scholar] [CrossRef] [PubMed]
- Poirel, L.; Sadek, M.; Kusaksizoglu, A.; et al. co-resistance to ceftazidime-avibactam and cefiderocol in clinical isolates producing KPC Variants. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 677–680. [Google Scholar] [CrossRef] [PubMed]
- Poirel, L.; Ortiz de la Rosa, J.M.; Sadek, M.; et al. Impact of Acquired Broad-Spectrum β-Lactamases on Susceptibility to Cefiderocol and Newly Developed β-Lactam/β-Lactamase Inhibitor Combinations in Escherichia coli and Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2022, 66, e00039-22. [Google Scholar] [CrossRef]
- Coppi, M.; Antonelli, A.; Niccolai, C.; et al. Nosocomial outbreak by NDM-1-producing Klebsiella pneumoniae highly resistant to cefiderocol, Florence, Italy, August 2021 to June 2022. Euro Surveill. 2022, 27, 2200795. [Google Scholar] [CrossRef]
- Liu, X.; Lei, T.; Yang, Y.; et al. Structural Basis of PER-1-Mediated Cefiderocol Resistance and Synergistic Inhibition of PER-1 by Cefiderocol in Combination with Avibactam or Durlobactam in Acinetobacter baumannii. Antimicrob. Agents Chemother. 2022, 66, e00828-22. [Google Scholar] [CrossRef] [PubMed]
- Karakonstantis, S.; Rousaki, M.; Kritsotakis, E.I. Cefiderocol: Systematic Review of Mechanisms of Resistance, Heteroresistance and In Vivo Emergence of Resistance. Antibiotics 2022, 11, 723. [Google Scholar] [CrossRef]
- Abdul-Mutakabbir, J.C.; Nguyen, L.; Maassen, P.T.; et al. In Vitro Antibacterial Activity of Cefiderocol Against Multidrug-Resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2021, 65, e02646-20. [Google Scholar] [CrossRef]
- Simner, P.J.; Mostafa, H.H.; Bergman, Y.; et al. Progressive Development of Cefiderocol Resistance in Escherichia coli During Therapy Is Associated with an Increase in blaNDM-5 Copy Number and Gene Expression. Clin. Infect. Dis. 2022, 75, 47–54. [Google Scholar] [CrossRef]
- Hobson, C.A.; Cointe, A.; Jacquier, H.; et al. Cross-resistance to cefiderocol and ceftazidime-avibactam in KPC β-Lactamase mutants and the inoculum effect. Clin. Microbiol. Infect. 2021, 27, 1172.e7–1172.e10. [Google Scholar] [CrossRef]
- Shields, R.K.; Iovleva, A.; Kline, E.G.; et al. Clinical Evolution of AmpC-Mediated Ceftazidime-Avibactam and Cefiderocol Resistance in Enterobacter cloacae Complex Following Exposure to Cefepime. Clin. Infect. Dis. 2020, 71, 2713–2716. [Google Scholar] [CrossRef] [PubMed]
- Kawai, A.; McElheny, C.L.; Iovleva, A.; et al. Structural Basis of Reduced Susceptibility to Ceftazidime-Avibactam and Cefiderocol in Enterobacter cloacae Due to AmpC R2 Loop Deletion. Antimicrob. Agents Chemother. 2020, 64, e00198-20. [Google Scholar] [CrossRef]
- Vuillemin, X.; Da Silva, M.; Bour, M.; et al. Cefiderocol activity is compromised by acquired extended-spectrum oxacillinases in Pseudomonas aeruginosa. Int. J. Antimicrob. Agents 2023, 62, 106917. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Ito, A.; Ishioka, Y.; et al. Escherichia coli strains possessing a four amino acid yrin insertion in PBP3 identified as part of the SIDERO-WT-2014 surveillance study. JAC Antimicrob. Resist. 2020, 2, dlaa081. [Google Scholar] [CrossRef]
- Nordmann, P.; Shields, R.K.; Doi, Y.; et al. Mechanisms of Reduced Susceptibility to Cefiderocol Among Isolates from the CREDIBLE-CR and APEKS-NP Clinical Trials. Microb. Drug Resist. 2022, 28, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Takemura, M.; Yamano, Y.; Matsunaga, Y.; et al. Characterization of Shifts in Minimum Inhibitory Concentrations During Treatment with Cefiderocol or Comparators in the Phase 3 CREDIBLE-CR and APEKS-NP Studies. Open Forum Infect. Dis. 2020, 7 (Suppl 1), S649–S650. [Google Scholar] [CrossRef]
- Kocer, K.; Boudour-Halil, D.; Chanthalangsy, Q.; et al. Genomic Modification of TonB and Emergence of Small-Colony Phenotype in VIM- and NDM-Producing Escherichia coli Following Cefiderocol Exposure In Vitro. Antimicrob. Agents Chemother. 2023, 67, e00118-23. [Google Scholar] [CrossRef]
- Klein, S.; Boutin, S.; Kocer, K.; et al. Rapid Development of Cefiderocol Resistance in Carbapenem-Resistant Enterobacter cloacae During Therapy Is Associated with Heterogeneous Mutations in the Catecholate Siderophore Receptor cirA. Clin. Infect. Dis. 2022, 74, 905–908. [Google Scholar] [CrossRef]
- Price, T.K.; Davar, K.; Contreras, D.; et al. Case Report and Genomic Analysis of Cefiderocol-Resistant Escherichia coli Clinical Isolates. Am. J. Clin. Pathol. 2022, 157, 257–265. [Google Scholar] [CrossRef]
- Hall, C.M.; Somprasong, N.; Hagen, J.P.; et al. Exploring Cefiderocol Resistance Mechanisms in Burkholderia pseudomallei. Antimicrob. Agents Chemother. 2023, 67, e00171–23. [Google Scholar] [CrossRef]
- McElheny, C.L.; Fowler, E.L.; Iovleva, A.; et al. In Vitro Evolution of Cefiderocol Resistance in an NDM-Producing Klebsiella pneumoniae Due to Functional Loss of CirA. Microbiol. Spectr. 2021, 9, e01779-21. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Landman, D.; Quale, J. Relationship of TonB-Dependent Receptors with Susceptibility to Cefiderocol in Clinical Isolates of Pseudomonas aeruginosa. J. Antimicrob. Chemother. 2022, 77, 1282–1285. [Google Scholar] [CrossRef]
- Daoud, L.; Al-Marzooq, F.; Moubareck, C.A.; et al. Elucidating the Effect of Iron Acquisition Systems in Klebsiella pneumoniae on Susceptibility to the Novel Siderophore-Cephalosporin Cefiderocol. PLoS One 2022, 17, e0277946. [Google Scholar] [CrossRef] [PubMed]
- Stracquadanio, S.; Nicolosi, A.; Privitera, G.F.; et al. Role of Transcriptomic and Genomic Analyses in Improving the Comprehension of Cefiderocol Activity in Acinetobacter baumannii. mSphere 2024, 9, e00617-23. [Google Scholar] [CrossRef]
- Galdino, A.C.M.; Vaillancourt, M.; Celedonio, D.; et al. Siderophores Promote Cooperative Interspecies and Intraspecies Cross-Protection Against Antibiotics In Vitro. Nat. Microbiol. 2024, 9, 631–646. [Google Scholar] [CrossRef]
- Teran, N.; Egge, S.L.; Phe, K.; et al. The Emergence of Cefiderocol Resistance in Pseudomonas aeruginosa from a Heteroresistant Isolate During Prolonged Therapy. Antimicrob. Agents Chemother. 2024, 68, e01009-23. [Google Scholar] [CrossRef] [PubMed]
- Smoke, S.M.; Brophy, A.; Reveron, S.; et al. Evolution and Transmission of Cefiderocol-Resistant Acinetobacter baumannii During an Outbreak in the Burn Intensive Care Unit. Clin. Infect. Dis. 2023, 76, e1261–e1265. [Google Scholar] [CrossRef]
- Tascini, C.; Coppi, M.; Antonelli, A.; et al. In Vivo Evolution to High-Level Cefiderocol Resistance of NDM-1-Producing Klebsiella pneumoniae, Followed by Intra-Hospital Cross-Transmission. Clin. Microbiol. Infect. 2024, 30, 398–400. [Google Scholar] [CrossRef]
- Sadek, M.; Le Guern, R.; Kipnis, E.; et al. Progressive In Vivo Development of Resistance to Cefiderocol in Pseudomonas aeruginosa. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 61–66. [Google Scholar] [CrossRef]
- He, Y.; Wang, Y.; Ma, X.; et al. Resistance to Cefiderocol Involved Expression of PER-1 β-Lactamase and Downregulation of Iron Transporter System in Carbapenem-Resistant Acinetobacter baumannii. Infect. Drug Resist. 2022, 15, 7177–7187. [Google Scholar] [CrossRef]
- Simner, P.J.; Beisken, S.; Bergman, Y.; Posch, A.E.; Cosgrove, S.E.; Tamma, P.D. Cefiderocol Activity Against Clinical Pseudomonas aeruginosa Isolates Exhibiting Ceftolozane-Tazobactam Resistance. Open Forum Infect. Dis. 2021, 8, ofab311. [Google Scholar] [CrossRef]
- Simner, P.J.; Bergman, Y.; Conzemius, R.; et al. An NDM-Producing Escherichia coli Clinical Isolate Exhibiting Resistance to Cefiderocol and the Combination of Ceftazidime-Avibactam and Aztreonam: Another Step Toward Pan-β-Lactam Resistance. Open Forum Infect. Dis. 2023, 10, ofad276. [Google Scholar] [CrossRef] [PubMed]
- Domingues, S.; Lima, T.; Saavedra, M.J.; et al. An Overview of Cefiderocol’s Therapeutic Potential and Underlying Resistance Mechanisms. Life (Basel) 2023, 13, 1427. [Google Scholar] [CrossRef]
- Yamano, Y. In Vitro Activity of Cefiderocol Against a Broad Range of Clinically Important Gram-Negative Bacteria. Clin. Infect. Dis. 2019, 69 (Suppl 7), S544–S551. [Google Scholar] [CrossRef]
- Simner, P.J.; Palavecino, E.L.; Satlin, M.J.; et al. Potential of Inaccurate Cefiderocol Susceptibility Results: A CLSI AST Subcommittee Advisory. J. Clin. Microbiol. 2023, 61, e01600-22. [Google Scholar] [CrossRef] [PubMed]
- Stracquadanio, S.; Nicolosi, A.; Marino, A.; et al. Issues with Cefiderocol Testing: Comparing Commercial Methods to Broth Microdilution in Iron-Depleted Medium—Analyses of the Performances, ATU, and Trailing Effect According to EUCAST Initial and Revised Interpretation Criteria. Diagnostics (Basel) 2024, 14, 2318. [Google Scholar] [CrossRef] [PubMed]
- Uskudar-Guclu, A.; Danyildiz, S.; Mirza, H.C.; et al. In Vitro Activity of Cefiderocol Against Carbapenem-Resistant Acinetobacter baumannii Carrying Various β-Lactamase-Encoding Genes. Eur. J. Clin. Microbiol. Infect. Dis. 2024, 43, 1171–1179. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing—Thirty-Fourth Edition: M100. CLSI 2024.
- Stracquadanio, S.; Bonomo, C.; Marino, A.; et al. Acinetobacter baumannii and Cefiderocol, Between Cidality and Adaptability. Microbiol. Spectr. 2022, 10, e02347–22. [Google Scholar] [CrossRef]
- Leonildi, A. In Vitro Susceptibility Test to Cefiderocol of NDM-Producing K. pneumoniae from Bloodstream Isolates: A Comparison of Commercial Methods and the Reference Method. In Proceedings of the Congress of the European Society of Clinical Microbiology and Infectious Diseases Global, Barcelona, Spain, 2024; Abstract P1641.
- EUCAST. EUCAST Warnings Concerning Antimicrobial Susceptibility Testing Products or Procedures. EUCAST 2024. Available online: https://www.eucast.org/ast-of-bacteria/warnings (accessed on 5 June 2025).
- Critchley, I.A.; Basker, M.J. Conventional Laboratory Agar Media Provide an Iron-Limited Environment for Bacterial Growth. FEMS Microbiol. Lett. 1988, 50, 35–39. [Google Scholar] [CrossRef]
- EUCAST. EUCAST Breakpoint Table 14.0 (2024) Available for Consultation (5–19 December, 2023). EUCAST 2023. Available online: https://www.eucast.org/eucast_news/news_singleview?tx_ttnews%5Btt_news%5D=566&cHash=db55f3a8829726044512a1fe74cce41b (accessed on 5 June 2025).
- Nordmann, P.; Bouvier, M.; Poirel, L.; et al. Rapid Cefiderocol NP Test for Detection of Cefiderocol Susceptibility/Resistance in Enterobacterales. J. Antimicrob. Chemother. 2022, 77, 3456–3461. [Google Scholar] [CrossRef]
- Raro, O.H.F.; Bouvier, M.; Kerbol, A.; et al. Rapid Detection of Cefiderocol Susceptibility/Resistance in Acinetobacter baumannii. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 1511–1518. [Google Scholar] [CrossRef]
- Jeannot, K.; Gaillot, S.; Triponney, P.; et al. Performance of the Disc Diffusion Method, MTS Gradient Tests and Two Commercially Available Microdilution Tests for the Determination of Cefiderocol Susceptibility in Acinetobacter spp. Microorganisms 2023, 11, 1971. Microorganisms 2023, 11, 1971. [Google Scholar] [CrossRef] [PubMed]
- Kolesnik-Goldmann, N.; Seth-Smith, H.M.B.; Haldimann, K.; et al. Comparison of Disk Diffusion, E-Test, and Broth Microdilution Methods for Testing In Vitro Activity of Cefiderocol in Acinetobacter baumannii. Antibiotics (Basel) 2023, 12, 1212. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, R.A.; Emeraud, C.; Jousset, A.B.; et al. Comparison of Disk Diffusion, MIC Test Strip and Broth Microdilution Methods for Cefiderocol Susceptibility Testing on Carbapenem-Resistant Enterobacterales. Clin. Microbiol. Infect. 2022, 28, 1156.e1–1156.e5. [Google Scholar] [CrossRef] [PubMed]
- Albano, M.; Karau, M.J.; Schuetz, A.N.; et al. Comparison of Agar Dilution to Broth Microdilution for Testing In Vitro Activity of Cefiderocol Against Gram-Negative Bacilli. J. Clin. Microbiol. 2020, 59, e00966-20. [Google Scholar] [CrossRef]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-Negative Bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef]
- Ibrahim, A.; Bouvier, M.; Sadek, M.; et al. A Selective Culture Medium for Screening Cefiderocol Resistance in Enterobacterales, Pseudomonas aeruginosa, and Acinetobacter baumannii. J. Clin. Microbiol. 2023, 61, e01883-22. [Google Scholar] [CrossRef]
- McCreary, E.K.; Heil, E.L.; Tamma, P.D. New Perspectives on Antimicrobial Agents: Cefiderocol. Antimicrob. Agents Chemother. 2021, 65, e02171–20. [Google Scholar] [CrossRef]
- Jena, J.; Behera, B.; Nayak, G.; et al. In Vitro Susceptibility of Burkholderia pseudomallei Isolates to Cefiderocol and Ceftazidime/Avibactam from Odisha, India. J. Lab. Physicians 2023, 15, 573–577. [Google Scholar] [CrossRef]
- Matuschek, E.; Longshaw, C.; Takemura, M.; et al. Cefiderocol: EUCAST Criteria for Disc Diffusion and Broth Microdilution for Antimicrobial Susceptibility Testing. J. Antimicrob. Chemother. 2022, 77, 1662–1669. [Google Scholar] [CrossRef]
- Morris, C.P.; Bergman, Y.; Tekle, T.; et al. Cefiderocol Antimicrobial Susceptibility Testing Against Multidrug-Resistant Gram-Negative Bacilli: A Comparison of Disk Diffusion to Broth Microdilution. J. Clin. Microbiol. 2020, 59, e01649-20. [Google Scholar] [CrossRef] [PubMed]
- Emeraud, C.; Gonzalez, C.; Dortet, L. Comparison of ComASP® and UMIC® Methods with the Reference Method for Cefiderocol Susceptibility Testing on Carbapenem-Resistant Enterobacterales. J. Antimicrob. Chemother. 2023, 78, 1800–1801. [Google Scholar] [CrossRef] [PubMed]
- Bianco, G.; Boattini, M.; Comini, S.; et al. Disc Diffusion and ComASP® Cefiderocol Microdilution Panel to Overcome the Challenge of Cefiderocol Susceptibility Testing in Clinical Laboratory Routine. Antibiotics (Basel) 2023, 12, 604. [Google Scholar] [CrossRef]
- Bianco, G.; Boattini, M.; Comini, S.; et al. Performance Evaluation of Bruker UMIC® Microdilution Panel and Disc Diffusion to Determine Cefiderocol Susceptibility in Enterobacterales, Acinetobacter baumannii, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, Achromobacter xylosoxidans and Burkholderia Species. Eur. J. Clin. Microbiol. Infect. Dis. 2024, 43, 559–566. [Google Scholar]
- Bovo, F.; Lazzarotto, T.; Ambretti, S.; et al. Comparison of Broth Microdilution, Disk Diffusion and Strip Test Methods for Cefiderocol Antimicrobial Susceptibility Testing on KPC-Producing Klebsiella pneumoniae. Antibiotics (Basel) 2023, 12, 614. [Google Scholar] [CrossRef] [PubMed]
- Dortet, L.; Niccolai, C.; Pfennigwerth, N.; et al. Performance Evaluation of the UMIC® Cefiderocol to Determine MIC in Gram-Negative Bacteria. J. Antimicrob. Chemother. 2023, 78, 1672–1676. [Google Scholar] [CrossRef]
- Devoos, L.; Biguenet, A.; Rousselot, J.; et al. Performance of discs, Sensititre EUMDROXF microplates and mts gradient strips for the determination of the susceptibility of multidrug-resistant Pseudomonas aeruginosa to Cefiderocol. Clin. Microbiol. Infect. 2023, 29, 652.e1–652.e8. [Google Scholar] [CrossRef]
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 15.0. EUCAST 2025.
- Liu, Y.; Ding, L.; Han, R.; et al. Assessment of Cefiderocol Disk Diffusion Versus Broth Microdilution Results When Tested Against Acinetobacter baumannii Complex Clinical Isolates. Microbiol. Spectr. 2023, 11, e05355-22. [Google Scholar] [CrossRef]
- Russo, C.; Humphries, R. Approaches to Testing Novel β-Lactam and β-Lactam Combination Agents in the Clinical Laboratory. Antibiotics (Basel) 2023, 12, 1700. [Google Scholar] [CrossRef]
- Koeth, L.M.; DiFranco-Fisher, J.M.; Palavecino, E.; et al. A Multicenter Performance Evaluation of Cefiderocol MIC Results: ComASP in Comparison to CLSI Broth Microdilution. J. Clin. Microbiol. 2024, 63, e00926-24. [Google Scholar] [CrossRef]
Figure 1.
Decision Framework for Cefiderocol Susceptibility Testing in Enterobacterales and P. aeruginosa. Abbreviations: DD, disk diffusion, BMD, Broth Microdilution; ATU, Area of Technical Uncertainty.
Figure 1.
Decision Framework for Cefiderocol Susceptibility Testing in Enterobacterales and P. aeruginosa. Abbreviations: DD, disk diffusion, BMD, Broth Microdilution; ATU, Area of Technical Uncertainty.
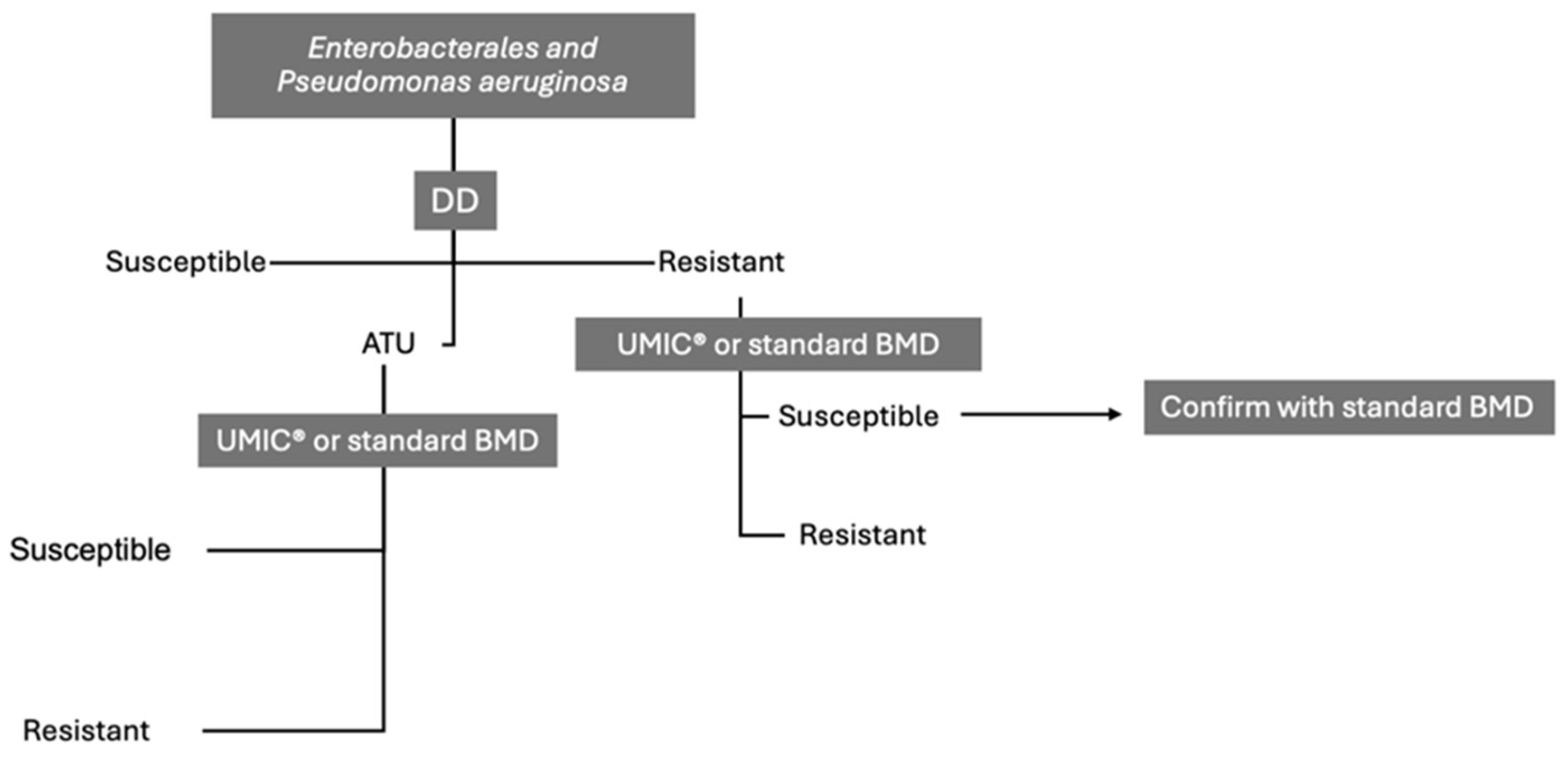
Figure 2.
Decision Framework for Cefiderocol Susceptibility Testing in A. baumaniii complex. Abbreviations: DD, disk diffusion, BMD, Broth Microdilution. *could be reported in a note as a MIC ≤ 2; **very preliminary information: possible change from 18 (ECOFFS) to 19 (breakpoint).
Figure 2.
Decision Framework for Cefiderocol Susceptibility Testing in A. baumaniii complex. Abbreviations: DD, disk diffusion, BMD, Broth Microdilution. *could be reported in a note as a MIC ≤ 2; **very preliminary information: possible change from 18 (ECOFFS) to 19 (breakpoint).
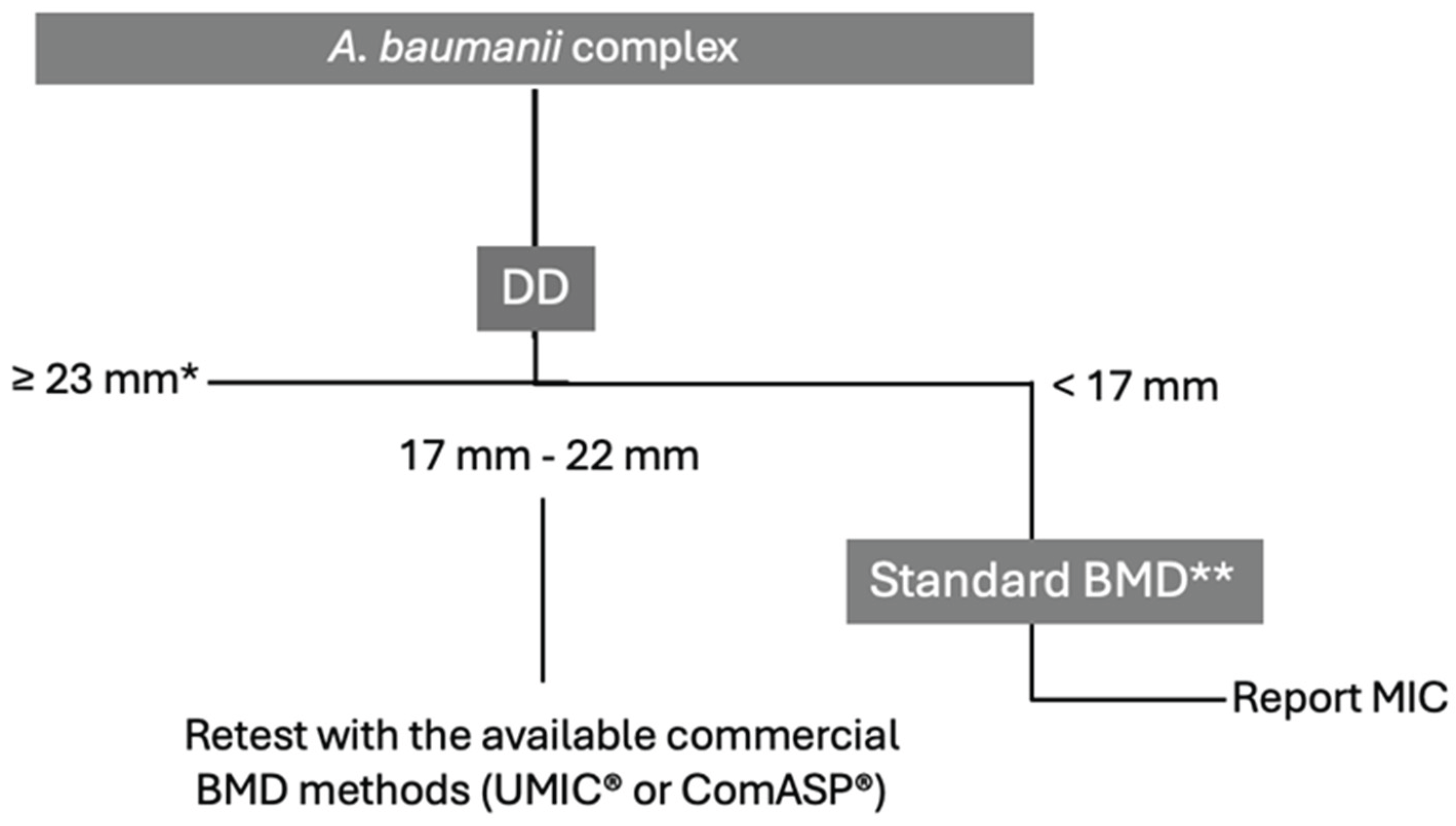

Table 1.
CLSI, EUCAST and FDA cefiderocol breakpoints.
| MIC Breakpoint (mg/L) | Disk Zone Diameter Breakpoint (mm) | ||||||
|---|---|---|---|---|---|---|---|
| Organism | CLSI | EUCAST | FDA | CLSI | EUCAST | ATU (EUCAST) | FDA |
| Enterobacterales | ≤4 (S), 8 (I), ≥16 (R) | ≤2 (S), >2 (R) | M-100 standard is recognized | ≥16 (S), 9-15 (I), ≤8 (R) | ≥23 (S), <23 (R) | 21-23 | M-100 standard is recognized§ |
| Pseudomonas aeruginosa | ≤4 (S), 8 (I), ≥16 (R) | ≤2 (S), >2 (R) | ≤1 (S), 2 (I), ≥4 (R) | ≥18 (S), 13-17 (I), ≤12 (R) | ≥22 (S), <22 (R) | 20-21 | ≥22 (S), 13-21 (I), ≤12 (R) |
| Acinetobacter baumannii complex | ≤4 (S), 8 (I), ≥16 (R) | IE | ≤1 (S), 2 (I), ≥4 (R) | ≥15 (S)** | Note* | ≥19 (S), 12-18 (I), ≤11 (R) | |
| Stenotrophomonas maltophilia | ≤4 (S), 8 (I), ≥16 (R) | IE | Not specified | ≥15 (S) | Note° | ≥17 (S) | |
*Zone diameters of ≥17 mm for the cefiderocol 30 µg disk correspond to MIC values below the PK-PD breakpoint of S ≤ 2 mg/L. IE: Insufficient evidence exists that the organism is a good target for therapy with the agent. ATU, Area of technical Uncertainty **DD ≤ 14 mm should not be interpreted or reported because it occurs with resistant, intermediate, and susceptible isolates. For these, do not report without performing a MIC test.° Zone diameters of ≥20 mm for the cefiderocol 30 µg disk correspond to MIC values below the PK-PD breakpoint of S ≤ 2 mg/L. §Clinical efficacy was shown for Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, and Enterobacter cloacae complex in patients with complicated urinary tract infections (cUTI) and for Escherichia coli, Klebsiella pneumoniae, Enterobacter cloacae complex, and Serratia marcescens in patients with hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia (HABP/VABP).
Table 2.
Comparative Analysis of AST Methods for Enterobacterales. Data are referred to EUCAST breakpoints where not otherwise indicated. BMD, brothmicrodilution; DD, disk diffusion; EA, Essential Agreement; CA, Categorical Agreement; VME, Very major error; ME, Major error; ATU, Areas of Technical Uncertainty; NA, not available; ID-CAMHB, Iron-Depleted Cation-Adjusted Mueller-Hinton Broth.
Table 2.
Comparative Analysis of AST Methods for Enterobacterales. Data are referred to EUCAST breakpoints where not otherwise indicated. BMD, brothmicrodilution; DD, disk diffusion; EA, Essential Agreement; CA, Categorical Agreement; VME, Very major error; ME, Major error; ATU, Areas of Technical Uncertainty; NA, not available; ID-CAMHB, Iron-Depleted Cation-Adjusted Mueller-Hinton Broth.
| Type of ID-CAMHB |
Disk Diffusion | ComASP® | UMIC® | Sensititre™ | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ATU% | CA% | VME% | ME% | CA% | EA% | Bias% | VME% | ME% | CA% | EA% | Bias% | VME% | ME% | CA% | EA% | Bias% | VME% | ME% | |||||||||||||
| Collection characteristics | Aggregated data on strain collection not available | ||||||||||||||||||||||||||||||
| Frozen panels | |||||||||||||||||||||||||||||||
|
Dortet 2023 (n=180) [72] |
87.8 | 91.7 | -25.0 | 2.7 | 0.5 | ||||||||||||||||||||||||||
| Collection characteristics | Beta-lactamases producers (3), KPCs (34), NDM producers (22), VIM producers (10), OXA producers (7), CTX-M producers (11), SHV and TEM producers (3) | ||||||||||||||||||||||||||||||
| Bruker Daltonics | Oxoid, Liofilchem, and Mast Diagnostics on MHA | ||||||||||||||||||||||||||||||
|
Bianco 2024 (n=90) [70] |
37.8 | 98.2 (Mast group) - 100 (others) | 0 | 0 (others) - 1 (Mast group) | 81.1 | 91.1 | +26.7 | 1.1 | 7.7 | ||||||||||||||||||||||
| Collection characteristics | 44% CRE i.e., KPC (21), NDM and OXA-181 (3), OXA-181 (1), and (SME) (1) | ||||||||||||||||||||||||||||||
| Sensititre™ (Thermo Fisher) | Mast Diagnostics disks and HardyDisks on MHA (Becton Dickinson) |
||||||||||||||||||||||||||||||
|
Morris 2021 (n=58)* [67] |
NA | 88 (CLSI)-90 Mast 88-91(CLSI)-Hardy |
0-0 Mast 0-0 Hardy |
NA(CLSI)-14 Mast 0 (CLSI)-17 Hardy |
|||||||||||||||||||||||||||
| Collection characteristics | KPC producers (114), ceftazidime/avibactam resistant (44), NDM producers (19), VIM-producers (31), OXA-48-like producers and KPC/VIM co-producers (10) | ||||||||||||||||||||||||||||||
| ID-CAMHB BMD | Oxoid disks and CA-MH agar (Becton-Dickinson) | ||||||||||||||||||||||||||||||
|
Bianco 2023 (n=178) [69] |
21.4 | 92.1 | NA | NA | 2.6 | 5.3 | |||||||||||||||||||||||||
| Collection characteristics | Carbapenemase of Ambler’s class A, B, D, multiple carbapenemases and non carbapenemase-producers | ||||||||||||||||||||||||||||||
| Frozen panels | Liofilchem disks on MHA (Biorad, Marnes la Coquette, France) | ||||||||||||||||||||||||||||||
|
Bonnin 2022 (n=100) [60] |
21.3 | 77 | 35.9 | 1.6 | 95 | 87 | NA | 2.8 | 1.6 | ||||||||||||||||||||||
| Collection characteristics | CRE (21 OXA-48 like, 15 NDM, 4 VIM, 2 KPC, 2 IMP, 1 FRI-1, 1 GIM-1, 1 GES-5, 1 NmcA, 1 OXA-372, 4 double-producing OXA-48 like and NDM, 1 NDM + KPC and 1 NDM + VIM) and 5 strains with high-level expression of EBSL or AmpC associated with decreased permeability of the outer membrane | ||||||||||||||||||||||||||||||
| Sensititre™ (Thermo Fisher) | |||||||||||||||||||||||||||||||
|
Emeraud 2023 (n=60) [68] |
83.3 | 76.7 | -6.7 | 34.5 (17.2 out of EA) | 0 |
83 | 91.7 | -10 | 24.1 (6.9 out of EA) | 0 | |||||||||||||||||||||
| Collection characteristics | KPC-producing K. pneumoniae, 42.6% resistant to CAZ-AVI and/or MER-VAB and/or IMIREL. 46.9% of the CAZ-AVI R strains carried blaKPC3, 50% mutated blaKPC3 and 3.1% blaKPC2 | ||||||||||||||||||||||||||||||
| ID-CAMHB BMD | Liofilchem disks on regular non-supplemented MHA (Liofilchem) | ||||||||||||||||||||||||||||||
|
Bovo 2023 (n=75) [71] |
NA | 92 (98.6**) | 0 | 16.7 (2.8 **) |
|||||||||||||||||||||||||||
| Collection characteristics | NDM- K. pneumoniae isolates from bloodstream infections with MICs ranging between 0.5-2 µg/mL | ||||||||||||||||||||||||||||||
| ID-CAMHB BMD | Liofilchem disks on MHA plates (Biolife) | ||||||||||||||||||||||||||||||
|
Leonildi Poster 1641 ESCMID 2024 (n=30) [52] |
74 | NA | NA | NA | NA | 100 | NA | NA | NA | NA | 100 | NA | NA | NA | |||||||||||||||||
*minor error (mE)% 12 (CLSI) Mast and 9 (CLSI) Hardy; **Excluding the discordant strains within the ATU.
Table 3.
Comparative Analysis of AST Methods for Pseudomonas aeruginosa. Data are referred to EUCAST breakpoints where not otherwise indicated. BMD, brothmicrodilution; DD, disk diffusion; EA, Essential Agreement; CA, Categorical Agreement; VME, Very major error; ME, Major error; ATU, Areas of Technical Uncertainty; NA, not available; ID-CAMHB, Iron-Depleted Cation-Adjusted Mueller-Hinton Broth.
Table 3.
Comparative Analysis of AST Methods for Pseudomonas aeruginosa. Data are referred to EUCAST breakpoints where not otherwise indicated. BMD, brothmicrodilution; DD, disk diffusion; EA, Essential Agreement; CA, Categorical Agreement; VME, Very major error; ME, Major error; ATU, Areas of Technical Uncertainty; NA, not available; ID-CAMHB, Iron-Depleted Cation-Adjusted Mueller-Hinton Broth.
| Type of BMD ID- CAMHB |
Disk Diffusion | ComASP® | UMIC® | Sensititre™ | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ATU% | CA% | VME% | ME% | CA% | EA% | Bias% | VME% | ME% | CA% | EA% | Bias% | VME% | ME% | CA% | EA% | Bias% | VME% | ME% | ||
| Collection characteristics | Carbapenem-resistant P. aeruginosa | |||||||||||||||||||
| Sensititre™ (ThermoFisher) | Mast Diagnostics disks and HardyDisks on MHA (Becton Dickinson) |
|||||||||||||||||||
|
Morris 2021 (n=14)* [67] |
NA | 86-86 (CLSI) Mast 79-93(CLSI) Hardy |
0 (CLSI) – 25 Mast 0 (CLSI) – 25 Hardy |
0 (CLSI) – 10 Mast 0 (CLSI) – 14 Hardy |
||||||||||||||||
| Collection characteristics | Carbapenem-resistant P. aeruginosa. 10 harbored blaVIM | |||||||||||||||||||
| ID-CAMHB BMD | Oxoid disks and CA-MH agar (Becton-Dickinson) | |||||||||||||||||||
|
Bianco et al. 2023 (n=42) [69] |
11.9 | NA | NA | NA | 100 | NA | NA | 0 | 0 |
|||||||||||
| Aggregated data on strain collection not available | ||||||||||||||||||||
| Frozen panels | ||||||||||||||||||||
|
Dortet 2023 (n=49) [72] |
98 | 93.9 | +12.2 | 0 | 2.04 | |||||||||||||||
| Collection characteristics | 13 strains no carbapenemase, 6 strains VIM-related carbapenemase, 5 strains IMP-related carbapenemase, 7 strains KPC or TEM-related carbapenemase, 5 strains NDM-related carbapenemase, the other mixed OXA-related carbapenemase | |||||||||||||||||||
| Bruker Daltonics | Oxoid, Liofilchem, and Mast Diagnostics on MHA | |||||||||||||||||||
|
Bianco 2024 (n=21) [70] |
40 | 95.8-100 | 2.5 | 0 | 90 | 92.5 | <30 | 0 | 8 | |||||||||||
| Collection characteristics | 40 producing ESBL, 52 producing carbapenemases (including 11 VIM-2), and 15 producing both types of enzymes. | |||||||||||||||||||
| ID-CAMHB BMD | Mast Diagnostic, Liofilchem, and Oxoid disks on MHA plates from 6 manufacturers** |
|||||||||||||||||||
|
Devoos 2023 (n=150) [73] |
NA | 78-89.3 (overall 84) |
18.7-84.3 | low° | 86.7 | 69.3 | -9.3 - +77.5 | 2.7 | 8 |
|||||||||||
*minor error (mE)% 14(CLSI) Mast and 7 (CLSI) Hardy; ** Oxoid, Thermofisher scientific; Mast Diagnostic, Amiens; Becton Dickinson; I2a diagnostics,Montpellier, France; Bio-Rad, Marnes-la-Coquette, France and bioM erieux, Marcy-L'Etoile,France); °the exact value was not reported.
Table 4.
Comparative Analysis of AST Methods for A. baumannii complex. Data are referred to EUCAST breakpoints where not otherwise indicated. BMD, brothmicrodilution; DD, disk diffusion; EA, Essential Agreement; CA, Categorical Agreement; VME, Very major error; ME, Major error; ATU, Areas of Technical Uncertainty; NA, not available; ID-CAMHB, Iron-Depleted Cation-Adjusted Mueller-Hinton Broth; ID-CAMH, Iron-Depleted Cation-Adjusted Mueller-Hinton.
Table 4.
Comparative Analysis of AST Methods for A. baumannii complex. Data are referred to EUCAST breakpoints where not otherwise indicated. BMD, brothmicrodilution; DD, disk diffusion; EA, Essential Agreement; CA, Categorical Agreement; VME, Very major error; ME, Major error; ATU, Areas of Technical Uncertainty; NA, not available; ID-CAMHB, Iron-Depleted Cation-Adjusted Mueller-Hinton Broth; ID-CAMH, Iron-Depleted Cation-Adjusted Mueller-Hinton.
| Type of BMD ID- CAMHB |
Disk Diffusion | ComASP® | UMIC® | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ATU % | CA % | VME % | ME % | CA% | EA% | Bias% | VME% | ME% | CA% | EA% | Bias% | VME% | ME% | ||
| Collection characteristics | Carbapenem-resistant A. baumannii complex | ||||||||||||||
| Sensititre™ (ThermoFisher) | MASTDISCS (Mast Group) disks and HardyDisks (Hardy Diagnostics, Santa Maria, CA) on MH agar (Becton Dickinson |
||||||||||||||
|
Morris 2021* (n=14) [67] |
NA | 71-86 (CLSI) Mast 64-61 (CLSI) Hardy |
0 (CLSI) – 11 Mast 0 (CLSI) – 33 Hardy |
0 (CLSI) – 20 Mast 25 (CLSI) – 20 Hardy |
|||||||||||
| Collection characteristics | Carbapenem-resistant A. baumannii. 46 OXA-23 carbapenemase and 2 OXA-23/NDM co-producers | ||||||||||||||
| ID-CAMHB BMD | Oxoid disks and CA-MH agar (Becton-Dickinson) | ||||||||||||||
|
Bianco 2023 (n=48) [69] |
14.5 | 97.9 | 0 | 2.1 | 85.7 | NA | NA | 0 | 0 |
||||||
| Collection characteristics | Aggregated data on strain collection not available | ||||||||||||||
| Frozen panels | |||||||||||||||
|
Dortet 2023 (n=44) [72] |
90.9 | 84.1 | -11.4 | 6.81 | 2.27 |
||||||||||
| Collection characteristics | 29/39 blaOXA-23-positive alone or in combination with other mechanism, other (i.e., NDM-1; OXA-66, ADC-30, OXA-58) | ||||||||||||||
| Bruker Daltonics | Oxoid, Liofilchem, and Mast Diagnostics on MHA | ||||||||||||||
|
Bianco 2024 (n=39) [70] |
NA | 94.9 | 3 | 3 | 97.4 | 89.7 | NA | NA | NA | ||||||
| Collection characteristics | Plasmid-borne carbapenemases in 94/100 isolates. OXA-23 (63%), OXA-72 (14%), OXA-58 (3%), and OXA-40 (1%) | ||||||||||||||
| ID-CAMHB BMD | Liofilchem disk on ID-CAMH, Biomerieux and Liofilchem CAMH-agar plates | ||||||||||||||
|
Kolesnik-Goldmann 2023 (n=100) [59] |
NA | 86 ID-CAMH, 87 Biomerieux, 84 Liofilchem 95.1 ID-CAMH (CLSI), 91.1 Biomerieux (CLSI), 89.2 Liofilchem (CLSI) |
7 ID-CAMH, 11 Biomerieux, 16 Liofilchem 1.2 ID-CAMH (CLSI), 11 Biomerieux (CLSI), 6.4 Liofilchem (CLSI) |
7 ID-CAMH, 2 Biomerieux, 0 Liofilchem 3.7 ID-CAMH (CLSI), 4.4 Biomerieux (CLSI), 4.3 Liofilchem (CLSI) |
88 -86 (CLSI) | 76- 76 (CLSI) | NA | 7-6 (CLSI) | 5-0 (CLSI) | 89 – 86 (CLSI) | 76- 76 (CLSI) | NA | 9-3 (CLSI) | 2-1 (CLSI) |
|
| Collection characteristics | 70 carbapenemase producers (OXA-type 58 strains, NDM-type in 11 strains, IMP-type enzyme in 1strain), 22 with two carbapenemase-encoding genes. ESBL in 17 strains. 1 strain GES-11 ESBL | ||||||||||||||
| ID-CAMHB BMD | Oxoid, Liofilchem and MAST disks on MH agar (Becton-Dickinson) | ||||||||||||||
|
Jeannot 2023 (n=97) [58] |
NA | 72.2 (Oxoid)-78.4 (Liofilchem) 81.4 (MAST) | 42.9 (Oxoid)- 50 (Liofilchem) 64.3 (MAST) | 0 | 95.9 | 81.4 | - 36.1 | NA | NA | 93.8 | 78.4 | -42.3 | NA | NA | |
| Collection characteristics | 104 carbapenem-susceptible A. baumannii complex and 364 carbapenem-resistant A. baumannii complex | ||||||||||||||
| ID-CAMHB BMD | Mast disks and MHA Oxoid | ||||||||||||||
|
Liu et al., 2023 (n=468) [75] |
NA | 98.1 (CLSI) - 97.0 | 0.9 (CLSI) -1.9 | NA | |||||||||||
*minor error (mE)% 28CLSI) Mast and 14 (CLSI) Hardy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



