Submitted:
16 June 2025
Posted:
18 June 2025
You are already at the latest version
Abstract
The acoustic environment of dental clinics plays a critical role in shaping patient experience, staff performance, and overall clinical effectiveness. This comprehensive review, supported by systematic search procedures, investigates how soundscapes in dental settings influence psychological, physiological, and operational outcomes. A total of 60 peer-reviewed studies were analyzed across dental, healthcare, architectural, and environmental psychology disciplines. Findings indicate that mechanical noise from dental instruments, ambient reverberation, and inadequate acoustic zoning contribute significantly to patient anxiety and professional fatigue. The review identifies emerging strategies for acoustic optimization, including biophilic and sustainable design principles, sound-masking systems, and adaptive sound environments informed by artificial intelligence. Special attention is given to the integration of lean management and circular economy practices for sustainable dental architecture. A design checklist and practical framework are proposed for use by dental professionals, architects, and healthcare planners. Although limited by the predominance of observational studies and geographic bias in the existing literature, this review offers a comprehensive, interdisciplinary synthesis. It highlights the need for future clinical trials, real-time acoustic assessments, and participatory co-design methods to enhance acoustic quality in dental settings. Overall, the study positions sound design as a foundational element in creating patient-centered, ecologically responsible dental environments.
Keywords:
dental acoustics
; healthcare soundscapes
; biophilic design
; sustainable dentistry
; lean management
; patient-centered care
; environmental psychology
; clinical architecture
1. Introduction
Sound in healthcare environments is increasingly recognized as a critical factor influencing well-being, yet dental clinics remain one of the most overlooked settings for acoustic optimization [1,2]. Characterized by intense, high-pitched mechanical noises and limited auditory insulation, dental soundscapes can generate negative physiological and psychological reactions in patients and practitioners [3]. The dental environment is uniquely vulnerable to acoustic stress due to the proximity of sound sources, the invasive nature of procedures, and often, the lack of noise-absorbing architectural features [2,4].
A growing body of literature has shown that elevated noise levels in dental clinics, often exceeding 80–85 dB, are associated with stress, discomfort, and even temporary hearing disturbances [5]. Studies focusing on patients’ perceptions of sound in the dental setting highlight how auditory exposure is often linked to fear, helplessness, and avoidance behaviors [4]. It was further noted that the sonic environment can compromise quality assurance by hindering communication and concentration, while also intensifying patient anxiety [2]. For dental professionals, prolonged exposure to tonal and high-frequency sounds contributes to fatigue, decreased performance, and reduced job satisfaction [2,6]. These sound-related effects are not merely occupational hazards but are systemic challenges that influence operational efficiency and patient trust [7].
Beyond clinical concerns, the architectural and design aspects of dental clinics play a substantial role in shaping the auditory experience. Traditional dental spaces often prioritize spatial efficiency over acoustic comfort, resulting in high reverberation times and sound leakage between operatories [2,8]. Acoustic interventions, such as sound-absorbing ceiling tiles, zoning layouts, and enclosed operatories, drawn from hospital design, have been shown to enhance patient recovery and satisfaction by reducing stress-inducing stimuli [9,10]. In parallel, the integration of biophilic and salutogenic design principles into healthcare architecture has gained momentum as a method for promoting psychological resilience and environmental sustainability [11]. Exposure to natural materials, plants, and daylight, combined with calming soundscapes such as music or water features, has been shown to improve patient mood and perception of care [12-15]. These approaches extend beyond aesthetics, functioning as therapeutic tools that control sensory overstimulation, including noise-related stress [16,17]. Furthermore, the potential for “plant acoustics”, -the concept that plants respond to and emit sound- represents an emerging frontier in designing responsive and interactive healing spaces [18].
Despite growing interest in healthcare acoustics more broadly, a significant gap persists in the literature concerning dental clinics specifically. While hospital acoustics are increasingly standardized and regulated, dental settings continue to lack clear guidelines or best practices for soundscape design. Moreover, few studies attempt to integrate acoustic optimization with sustainable or biophilic design practices tailored to dental environments [11, 19-21].
This review aims to systematically examine the characteristics and impact of soundscapes in dental environments and to propose integrative design strategies that align with both sustainable development and patient-centered care. Drawing on findings from acoustic engineering, environmental psychology, clinical dentistry, and healthcare architecture, this review addresses the urgent need to reimagine dental spaces as environments of holistic healing, where sound is not an incidental byproduct but a designed and therapeutic component of care.
2. Materials and Methods
2.1. Literature Search Strategy and Eligibility Criteria
This review adopted a comprehensive hybrid approach. While it employed systematic search strategies and structured inclusion criteria, it also integrated conceptual frameworks, narrative insights, and interdisciplinary perspectives, thus adopting a comprehensive review methodology. The aim was to investigate the relationship between soundscapes, user experience, and sustainable acoustic strategies in dental environments, taking into account literature found in healthcare settings. The review included multiple phases of data collection and analysis to ensure thematic relevance, methodological quality, and interdisciplinary depth [22]. The search was conducted across four major academic databases: PubMed, Scopus, Web of Science, and Google Scholar. Keywords used in various Boolean combinations included: “dental acoustics,” “dental clinic noise,” “sound environment in healthcare,” “soundscape in dentistry,” “patient noise perception,” “sustainable architecture dental,” and “biophilic acoustic design.” Additionally, a curated internal dataset in CSV format containing indexed noise-related research was analyzed. To enhance coverage, backward and forward citation tracking was performed, and additional peer-reviewed open-access articles were gathered via Google Scholar. Manual screening ensured that only articles aligned with the acoustic context of dental or healthcare environments were included.
The inclusion criteria were peer-reviewed publications between 2014 and 2025, full-text availability (open access or PMCID), focus on acoustic environments, soundscapes, or noise in dental/healthcare settings, and studies assessing psychological, physiological, architectural, or experiential outcomes related to sound. The exclusion criteria were: Non-healthcare-related acoustic studies, conference abstracts or non-peer-reviewed documents, articles not in English or not available in full text, studies without methodological transparency or sound relevance, and those with inadequate methodological detail or duplicated content.
2.2. Study Selection, Data Extraction, and Thematic Analysis
A total of 83 studies were initially identified through structured searches in four major academic databases: PubMed, Scopus, Web of Science, and Google Scholar, using Boolean combinations of keywords such as “dental acoustics,” “sound environment in healthcare,” and “biophilic acoustic design.” After the removal of 10 duplicate records, 73 studies remained for initial screening. These were assessed based on predefined inclusion and exclusion criteria, resulting in the exclusion of 23 studies due to reasons such as lack of methodological transparency, irrelevance to healthcare soundscapes, non-peer-reviewed format, language restrictions, or lack of full-text availability. Following this, 50 studies met the criteria and were retained for further analysis.
To enrich the dataset and ensure comprehensive thematic coverage, 10 additional articles were sourced through Google Scholar. These additions specifically addressed gaps in areas like biophilic architecture, patient-centered sound design, and perception of acoustic environments in clinical and dental settings. In total, 60 studies were included in the final synthesis and subjected to thematic content analysis based on metadata such as authorship, publication year, study type, methodology, outcomes, and relevance to acoustic optimization in healthcare. In Figure 1, the PRISMA flow chart of the study is presented [23].
All included literature was subjected to thematic content analysis. Key data points, authorship, year, study type, methodology, results, and relevance to acoustic optimization, were extracted and tabulated. Table 1 was used to classify findings and map the diversity of approaches across disciplines. This triangulation ensured comprehensive coverage of clinical, psychological, architectural, and sustainability-related dimensions of healthcare and dental soundscapes. Table 1.
2.3. Assessment of Study Validity
To ensure the methodological strength and internal validity of the included literature, a structured critical appraisal was conducted using validated tools. For primary empirical studies, the Cochrane Risk of Bias 2.0 (RoB 2.0) tool was applied [74]. This tool evaluates risk across five key domains: the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting of results. Each domain is assessed and rated as “low risk,” “some concerns,” or “high risk.” An overall risk of bias score was then derived for each study (Cochrane Methods Bias). This assessment was particularly relevant for the 32 original and empirical studies, many of which employed randomized, quasi-experimental, or observational designs.
For systematic and scoping reviews (a total of 9 studies), the AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews) instrument was basically used. This tool comprises 16 items and assesses the methodological quality of reviews based on criteria such as the comprehensiveness of the literature search, the presence of duplicate screening and data extraction, and whether a risk of bias was considered when interpreting the results. Each review was categorized based on the overall confidence in its findings: “high,” “moderate,” “low,” or “critically low.” [75]. For studies not amenable to these frameworks, such as narrative reviews, conceptual papers, book chapters, and design studies, a qualitative evaluation was performed [76]. These were assessed based on theoretical clarity, citation use, methodological transparency, and relevance to acoustic design in healthcare environments (Table S1).
3. Results
3.1. Distribution of Study Types
Of the 60 studies analyzed, the most prominent category is original and empirical research, comprising 32 studies. These include experimental trials, observational assessments, and mixed-methods investigations conducted in real healthcare environments, such as ICUs, NICUs, dental clinics, and psychotherapy settings. They provide insights into how acoustic interventions affect patient stress, recovery, cognitive focus, and staff well-being. Beyond these, systematic and scoping reviews appear in 9 studies, providing structured syntheses of current evidence. These include Fan & Baharum (2018) on the effects of nature sounds on stress [63], Bergefurt et al. (2023) on how environmental conditions affect mental health [36], Guidolin et al. (2024) on inpatient exposure to nature[15], Raghuwanshi et al. (2024) summarizing hospital noise impacts[31], Verderber et al. (2021) focusing on ICU soundscapes [38], Elf et al. (2024) investigating existing research gaps in the design of inpatient healthcare environments, highlighting the need for more evidence-based, interdisciplinary approaches to architectural features, such as acoustics, lighting, and spatial layout, that directly impact patient outcomes and staff performance [27] and Kumar et al. (2023) reviewing principles of acoustic comfort in smart healthcare environments [35]. Narrative reviews and conceptual papers, represented in 10 studies, offer theoretical perspectives and reflective syntheses. Notable examples include Zhang (2024), who maps the emotional role of acoustics in biophilic design [20], Antoniadou et al. (2022) calling for sustainable acoustic protocols in dental offices [2], and Dabrowska (2020) discussing natural sound as positive distraction [55]. Also, there are 5 studies classified as book chapters or full-length books. These include Engineer et al. (2024), who explore how architectural features impact emotional and pain responses [28], Williams (2017) on the stress-reducing power of auditory nature [65], Jiang (2020) examining soundscapes and views in healing [57]. Mittelmark [64], and Roe & McCay (2021) discussing restorative design in urban health planning [67]. Additionally, 6 studies are literature or applied reviews. These include MacAllister & Zimring (2016) on noise and care satisfaction [68], Al Khatib et al (2024) on environmental comfort elements like biophilic acoustics [33], Zhang & Tzortzopoulos (2016) proposing a health-focused design framework [66], and Tziovara et al. (2024) on thematic sound analysis in dental clinical soundscapes [4]. Lastly, a small but impactful set of design frameworks and evaluation studies (2–3 studies) explores design methods more directly. For example, Zhang and Tzortzopoulos (2016) provide a framework that connects the acoustic environment with occupant health outcomes [66].
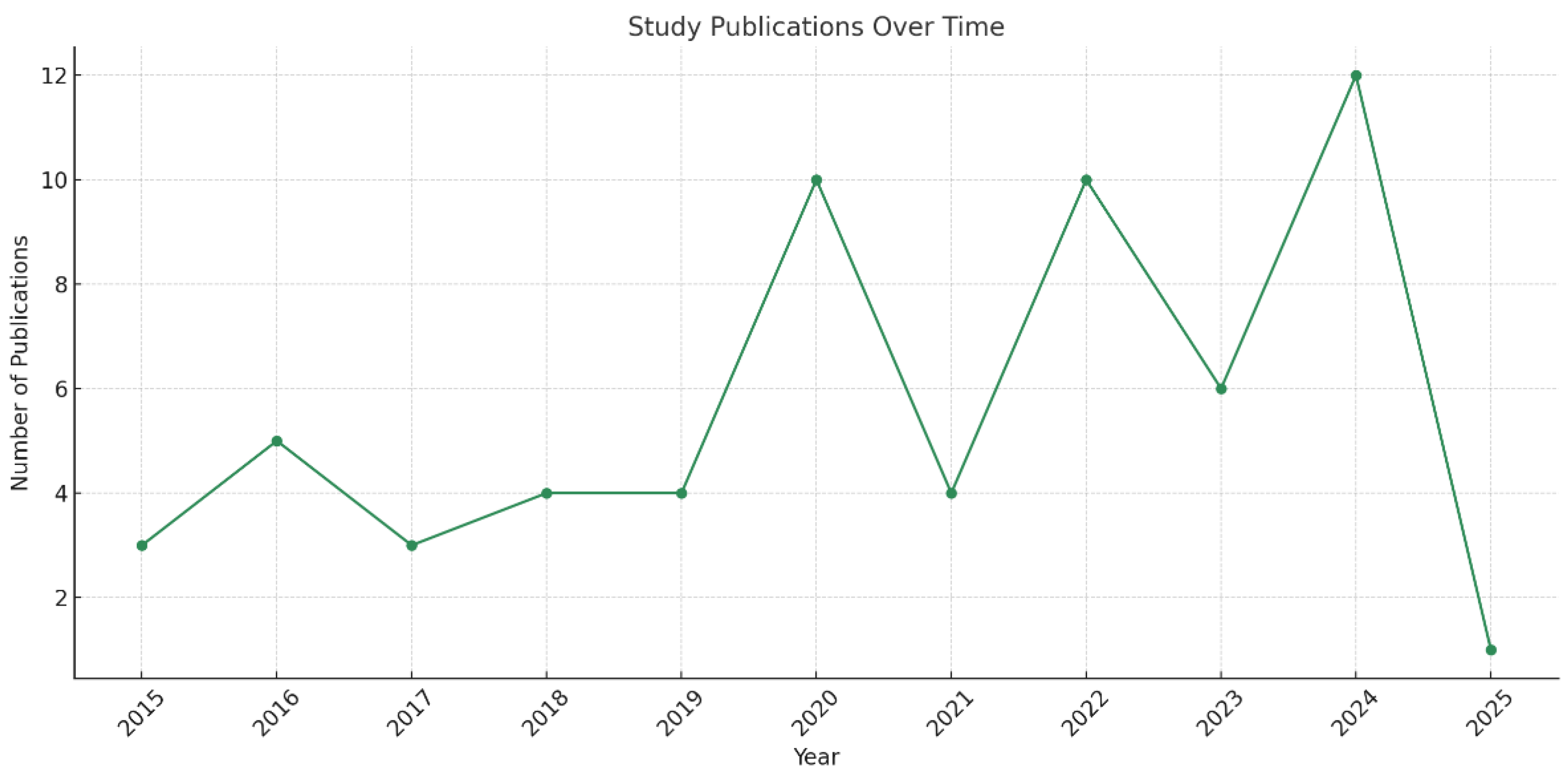
3.2. Publication Trends Over Time
The timeline of publication shows a clear upward trend, particularly from 2020 onwards. This surge likely correlates with heightened awareness around environmental stressors in healthcare, partly catalyzed by the COVID-19 pandemic [77]. The years 2023 and 2024 especially stand out, featuring a concentration of studies exploring biophilic acoustics, nature-based sound interventions, and sensory mapping in both clinical and residential care contexts. These trends suggest a growing recognition of sound not just as a nuisance, but as a powerful therapeutic and architectural element.
3.3. Most Studied Healthcare Settings
When we examine where these studies are set, Intensive Care Units (ICUs) and Neonatal Intensive Care Units (NICUs) emerge as the most researched environments. This is expected, given these spaces' high noise sensitivity and their critical impact on vulnerable patient populations, such as the elderly or pre-term infants. Examples include Tahvili et al. (2025), who documented ICU noise levels reaching 87 dBA[24], Jonescu et al. (2024), who implemented modeling strategies for acoustic optimization [26], Armbruster et al. (2023), who observed noise reduction through lean management interventions [34], and Bringel et al. (2023), who linked NICU noise to staff burnout [37]. Studies like Zhang et al. (2024) and Khowaja et al. (2022) confirmed the physiological impact of noise on preterm infants [19,42], while Benzies et al. (2019) and Souza et al. (2022) highlighted the systemic and architectural challenges in noise control and sleep promotion [61,45]. Dental clinics also represent a significant portion of the studies, demonstrating increasing awareness of acoustics in outpatient environments. Research in this domain often centers around stress reduction through curated music or sound design, such as in Wazzan et al. (2022) and Antoniadou et al. (2023) [44,5]. Other studies, like Tziovara et al. (2024) and Ma et al. (2020), explore patient and practitioner perspectives, highlighting stress, anxiety, and hearing concerns [4,58]. Interventions include real-time monitoring systems and personalized soundscapes to mitigate negative effects. Additionally, general hospital wards, psychotherapy spaces, and healthcare environments such as smart buildings also receive attention. For example, Guidolin et al. (2024) and Lin et al. (2024) propose biophilic soundscapes using natural elements like water or birdsong to improve recovery [15, 25]. Similarly, Meng et al. (2022) and Rodriguez-Nogueiras (2024) examine sound perception in vulnerable groups [40,32], while Elf et al. (2024) offer a meta-perspective on architectural design gaps in inpatient healthcare settings [7]. Deng et al. (2023) and Jiang (2020) illustrate how sensory design, particularly through water features and greenery, can reduce stress and promote healing [9,57]. Overall, these studies emphasize sound’s role in mental health, perceived quality of care, and patient experience in both clinical and transitional care spaces, reinforcing the need for acoustic optimization as part of sustainable and patient-centered design.
3.4. Quality Assessment
The quality assessment of the 60 studies included in this review revealed a diverse methodological landscape with varying degrees of rigor and reliability. The majority of empirical studies, comprising experimental, observational, and mixed-methods research, were judged as suitable for appraisal using the Cochrane RoB 2.0 tool. Most demonstrated low to moderate risk of bias, contributing valuable real-world insights despite occasional limitations in reporting transparency or measurement standardization. For example, Zhang et al. (2024) conducted a meta-analysis on white noise in NICUs [19], while Tahvili et al. (2025) and Armbruster et al. (2023) offered good observational assessments of ICU noise levels [24,34]. Wazzan et al. (2022) used clinical trial methodology to measure stress reduction via music therapy in dental clinics, showcasing strong experimental validity [44]. Further, systematic and scoping reviews, assessed using the AMSTAR 2 tool, generally demonstrated moderate confidence. These included comprehensive literature syntheses, such as Elf et al. (2024), which identified architectural research gaps in inpatient environments [7], and Fan & Baharum (2018), which summarized evidence on natural soundscapes and stress reduction [63]. While structured and insightful, some of these lacked formal risk-of-bias evaluations for included studies, slightly limiting their generalizability. Moreover, narrative reviews, conceptual papers, and book chapters, appraised through qualitative tools, were found to offer strong theoretical contributions, especially in areas like biophilic design and acoustic psychology [40,46,47]. These sources enriched the review by framing the role of sound beyond mere decibel measurements, though their lack of empirical data constrains their direct applicability to clinical design contexts.
In general, the assessment confirms a solid foundation of evidence, with a balanced mix of empirical investigations and theory-driven contributions. This blend affirms the growing maturity and interdisciplinary richness of research in healthcare and dental acoustic environments. In Table S1, the detailed quality appraisal results for each included study are summarized.
3.5. Sources of Sound in Dental Settings
The dental clinic is an acoustically complex environment where various sound sources intersect, often creating high levels of auditory stimulation [2,5]. The soundscape can be categorized into four broad typologies: mechanical, environmental, human, and ambient [78]. Mechanical sounds derive predominantly from dental instruments, including air turbines, ultrasonic scalers, suction devices, and polishing tools [4,5]. Among these, the high-frequency and tonal noise generated by air turbines is the most prominent and has been measured at levels exceeding 85 dB [5]. These instruments contribute significantly to both patient discomfort and occupational hearing risks [5,58]. Also, environmental sounds are often byproducts of the building’s infrastructure, such as HVAC systems, water pipes, and electrical equipment [31,32]. Although less intense than mechanical sounds, their continuous and low-frequency nature raises the general noise floor, affecting background stress and reducing the clarity of verbal communication [34,43]. In addition, human-generated sounds, including patient speech, staff communication, and procedural dialogue, also shape the clinic's acoustic environment. These can become especially disruptive in open-plan or poorly insulated layouts [5,58]. Excessive conversational noise has been found to interfere with staff concentration, reduce team performance, and elevate fatigue [52]. Finally, ambient sound refers to the cumulative reverberations and overlaps of mechanical, environmental, and human noise within the physical space [8,60]. Inadequate use of sound-absorbing materials, reflective surfaces, and poor zoning can result in increased echo and suboptimal auditory ergonomics [19,26]. This has negative consequences on both patient perception and professional effectiveness [4,5]. Together, these sound typologies underline the multifaceted nature of dental acoustics and the pressing need for integrated architectural and technological solutions. According to the reviewed literature, studies consistently emphasize that sound in healthcare environments, including dental settings, is not incidental but central to both environmental quality and care outcomes [27,40,63].
3.6. Patients’ perceptions of dental soundscapes
Patients’ perceptions of dental soundscapes are shaped by more than just volume; they are deeply influenced by associations with pain, anxiety, and prior traumatic experiences [2,5]. High-frequency sounds from dental drills and suction devices are consistently reported as among the most distressing elements in the clinical environment [5]. These sounds have been directly linked to anticipatory fear, particularly among those with previous negative dental experiences or high auditory sensitivity [52]. Importantly, perceptual responses to sound are not uniform. Certain populations, including children, elderly patients, and individuals with neurodevelopmental conditions such as autism spectrum disorder, exhibit heightened reactivity to unpredictable or high-pitched stimuli [27,40]. This can result in increased distress, avoidance behaviors, or non-compliance during treatment. Such findings support the need for inclusive acoustic design, tailored to accommodate diverse sensory thresholds [39,51].
The psychophysiological impact of dental noise is also measurable. Exposure to sharp or sudden clinical sounds can activate the sympathetic nervous system, leading to elevated heart rate, blood pressure, and cortisol levels, as seen in both patient and staff populations [5,37,44]. In this context, non-invasive interventions such as music therapy have gained clinical attention. Wazzan et al. (2022) demonstrated that customized music sessions not only reduced subjective anxiety but also lowered objective stress markers in patients undergoing dental treatment [44]. Moreover, carefully curated background music has been shown to mask aversive clinical sounds, creating a more calming and supportive environment [2,4]. This strategy aligns with broader healing environment design principles, which emphasize multisensory comfort as a pillar of care quality [31,63]. Together, these findings affirm that dental soundscapes are not merely a technical concern but a central element of the patient’s experience. Perception of sound operates as a complex interplay of physical stimuli, emotional interpretation, and environmental context, one that can and should be actively shaped through architectural, technological, and psychological design strategies [5,19,27].
3.7. Designing for Acoustic Wellness
Designing for acoustic wellness in dental settings requires adapting proven strategies from broader healthcare environments to address the unique psychological and spatial dynamics of outpatient dentistry. Hospital-based research shows that poor acoustic environments contribute to sleep disruption, physiological stress, and delayed recovery, supporting the need to extend similar design principles to dental clinics [8,19,62]. To be more specific, dental clinics often evoke anticipatory anxiety, making sound control not only a matter of comfort but of clinical importance. Tziovara et al. (2024) found that chaotic soundscapes in clinics intensify stress-related responses [4], while Antoniadou et al. (2023) quantitatively recorded noise levels surpassing comfort thresholds, urging the application of sound-absorbing ceiling tiles, wall panels, and spatial zoning [5]. Similarly, Dzhambov et al. (2021) linked poor acoustic design to decreased well-being in healthcare learning spaces, reinforcing its importance in academic and pediatric clinics [51].
Furthermore, strategic spatial zoning is essential: high-noise areas such as sterilization rooms should be acoustically separated from quiet zones like recovery or consultation rooms [29,39]. In open-plan clinics, sound-dampening dividers and directional barriers can reduce sound spillover, though private operatories offer the greatest control over the auditory environment [26,43].
Emerging research also supports biomedical acoustics, a concept that uses evidence-based layout planning and sound modulation to enhance healing [10]. These principles align with biophilic strategies, where natural acoustic stimuli, like water sounds or birdsong, create calming environments [25,57,63]. These can be particularly effective in waiting or reception areas, where patients experience peak anticipatory anxiety [19].
Best practices include specifying materials with high NRC and CAC ratings, using insulated doors, noise-controlling HVAC, and rubber flooring in non-clinical areas [27, 50,68]. Real-time noise monitoring can further optimize these spaces dynamically [10,58]. Additionally, incorporating feedback from dental professionals is key to ensuring both functionality and sensory comfort [28]. Guidelines from industry sources discuss early-stage acoustic planning to minimize retrofitting costs and disruptions. Ultimately, as dentistry transitions toward a more holistic, preventive model, acoustic wellness must be considered a core design parameter, benefiting not only patient experience but also staff retention, workflow efficiency, and environmental sustainability [2,13,36].
3.8. Sustainability and Biophilic Integration
The integration of sustainability and biophilic design in dental settings reflects a growing shift toward holistic and patient-centered care that acknowledges both environmental responsibility and psychological well-being [78]. Biophilic design, defined as the incorporation of nature-inspired elements into architectural planning, has demonstrated measurable impacts on patient outcomes [79]. Research has shown that incorporating biophilic elements such as green walls, indoor plants, natural wood finishes, and organic textures can significantly reduce patient anxiety in healthcare environments [15]. These design features have also been associated with higher levels of user satisfaction and enhanced physiological comfort, supporting both psychological restoration and sensory well-being [79]. Evidence indicates that even modest plant-based interventions, such as dish gardens, can lead to measurable improvements in neuropsychological outcomes among pediatric patients and patients in psychotherapy offices, supporting their integration into dental operatories and waiting rooms too [53]. In addition to visual biophilia, natural soundscapes, such as birdsong or flowing water, can mask mechanical noise and reduce physiological stress. Studies by Fan & Baharum (2018), Jiang (2020), and Dabrowska (2020) confirm the anxiolytic effects of these sounds in healthcare settings, promoting calmness and enhancing cognitive clarity [55,57,63]. These findings justify the integration of nature-inspired audio environments in reception and treatment zones of dental clinics.
Furthermore, designing for sustainability extends beyond aesthetics. Environmentally friendly material choices, such as bamboo wall panels, low-VOC (volatile organic compound) paints, and rubber flooring, enhance indoor air quality and support compliance with LEED and WELL building standards [13,27]. Fenestration strategies that maximize daylight also reduce energy consumption while contributing to mood regulation and circadian alignment [65,66,80]. Research highlights that transitional areas such as corridors and lobbies are critical zones where patient stress often peaks, underlining the importance of targeted design interventions in these spaces [8,81]. Here, biophilic elements serve not only as visual reprieve but as sensory anchors that aid orientation and reduce anxiety, especially for neurodivergent individuals. Incorporating acoustic panels made from recycled fibers, green wall systems, and multisensory zoning strengthens the link between comfort and sustainability [10,65,66,80]. Importantly, as highlighted in the Routledge Handbook of High-Performance Workplaces (2023) and supported by Antoniadou (2024), acoustic performance and environmental sustainability are not competing priorities but are synergistic goals [82]. Acoustic comfort reduces cognitive load and fosters well-being, while sustainable materials and design layouts improve long-term health and operational efficiency [26,81,82].
In this study and based on the WELL Building Standard (v1 with May 2016 Addenda, https://standard.wellcertified.com/well), we present a list of relevant WELL features that intersect with our themes of soundscapes, patient well-being, environmental sustainability, and dental settings.

Table 2.
WELL, Building Standard checklist for dental spaces.
| WELL Concept | Feature Name | Article Relevance |
|---|---|---|
| Air | VOC Reduction (Feature 4) | Use of low-emission materials in green dentistry clinics. |
| Air Quality Standards (Feature 1) | Sustainable ventilation impacts perceived environmental quality. | |
| Water | Fundamental Water Quality (Feature 30) | Indirect relevance, biophilic use of water elements as calming features. |
| Nourishment | N/A | Not applicable. |
| Light | Circadian Lighting Design (Feature 54) | Integration of lighting systems to reduce stress in dental clinics. |
| Fitness | Active Furnishings (Feature 71) | Less directly relevant but could tie into ergonomic design in staff areas. |
| Comfort | Acoustic Comfort (Feature 80) | Central to the article, acoustic design in dental settings, noise mitigation, and stress relief. |
| Sound Masking (Feature 81) | Use of music therapy and nature soundscapes. | |
| Individual Thermal Comfort (Feature 76) | Peripheral relevance; supports holistic sensory environments. | |
| Mind | Biophilic Design I & II (Features 88, 100) | Directly addressed through green elements, natural soundscapes, and visual comfort. |
| Stress Support (Feature 84) | Interventions like music therapy reduce dental anxiety. | |
| Adaptable Spaces (Feature 89) | Encourages responsive, user-centered design in dental clinics. | |
| Beauty and Design (Feature 87) | Aesthetic and multisensory enhancements are covered in patient journey mapping. | |
| Innovation | Custom Features | Adaptive AI-driven soundscapes and plant acoustics meet innovation criteria. |
In summary, the convergence of biophilic and sustainable architectural strategies in dental settings contributes not only to reduced stress and better care experiences but also supports broader goals of resource efficiency, equity, and environmental responsibility [78, 82-84]. These innovations redefine the dental office as a healing space, actively designed to promote calm, resilience, and ecological stewardship.
4. Emerging Research and Novel Ideas
As acoustic awareness continues to evolve within healthcare design, novel interdisciplinary innovations are beginning to shape the future of soundscapes in dental spaces. One of the most intriguing developments is the exploration of plant acoustics, the notion that plants not only react to sound but may also emit sound frequencies in response to stress or environmental changes [65,66,81,82]. Hussain et al. (2023) explored this concept in “Plants Can Talk,” suggesting that integrating responsive greenery in healthcare settings could open pathways to dynamic, biofeedback-driven environments that are more attuned to natural rhythms and patient needs [85].
Beyond biological responses, advancements in artificial intelligence (AI) and adaptive sound technologies are paving the way for personalized sound environments. AI-enabled systems can monitor noise patterns in real time and adjust ambient soundscapes, accordingly, lowering volume during periods of peak stress or tailoring auditory stimuli based on patient profiles [86]. This concept has been trialed in dementia care and neonatal units [38], showing promise in modulating agitation and enhancing therapeutic outcomes [38,39,46,47,56]. Such adaptive technologies could be seamlessly integrated into dental settings to create individualized sound profiles. For instance, neurodivergent patients or those with PTSD could benefit from pre-set calming sound environments, while pediatric dental spaces might use gamified auditory cues to reduce procedural fear. Personalized acoustic zoning could also be employed through smart headphones or directional speakers embedded in dental chairs, too [4]. These approaches do not sound like a fixed background condition, but as an active therapeutic modality, programmable, customizable, and aligned with the user’s sensory and emotional state [19,20]. As acoustic science intersects with biomimicry, data-driven systems, and sensory design, the potential for acoustic innovation in dental care is substantial [87].
5. Discussion
The growing convergence of acoustics, healthcare design, and sustainability reflects a marked shift from function-driven to experience-driven clinical environments, signaling a more human-centered approach to care. This transformation is particularly salient in dental settings where patients are conscious during procedures and highly sensitive to environmental stimuli [4,5]. As discussed by multiple studies, dental clinics must no longer be viewed solely as procedural spaces but as sensory landscapes that influence trust, compliance, and health outcomes [2,4,5,58].
One of the most compelling innovations explored across recent literature is the multisensory optimization of clinical settings through biophilic design. Exposure to natural stimuli, such as daylight, vegetation, and nature-inspired acoustics, has been shown to reduce stress, improve mood, and enhance overall patient experience [15,79-87]. These effects are not only physiologically significant, lowering heart rate, anxiety, and cortisol, but also contribute to a positive emotional climate in the clinic. Importantly, the presence of biophilic elements can offer patients a subconscious signal of care and safety even before the clinical encounter begins [57,58,84]. Additionally, plant-based design interventions have been linked to improvements in spatial legibility and user comfort, supporting psychological orientation and well-being in both pediatric and general dental settings [54]. Water features, used strategically, have also demonstrated calming effects, particularly in high-stimulus zones like waiting areas and corridors, and are especially effective for neurodivergent individuals or those with heightened sensory sensitivities [25,40]. Mapped against the dental patient journey, from arrival to procedure and post-treatment recovery, these principles contribute to what Devetziadou & Antoniadou (2021) describe as the “environmental scaffolding” of emotional resilience [88]. The infusion of greenery, scent, and tailored soundscapes at critical touchpoints supports the so-called “wow effect,” which strengthens perception of care quality and long-term loyalty [88].
Moreover, the use of curated auditory environments, such as music therapy, ambient soundscapes, and nature-based acoustic masking, has emerged as a non-invasive, patient-centered strategy for emotional regulation in dental and pediatric clinics. These interventions have been shown to lower anxiety, modulate physiological stress responses, and enhance perceived quality of care [10,13,44,45,60]. Integrating such auditory tools into clinical workflows supports a more calming and predictable sensory experience, particularly beneficial for vulnerable populations, including children, neurodivergent patients, and individuals with prior dental trauma [40,51]. As patients transition into treatment zones, the focus increases to green dentistry, a growing field that fuses environmental responsibility with architectural innovation. Research highlights that elements such as energy-efficient lighting systems, low-VOC (volatile organic compound) materials, and the use of recycled acoustic panels are not only ecologically sound but also elevate the professional image of dental practices [89]. This alignment with green building standards is becoming a differentiating factor in dental clinic branding, influencing patient choice and contributing to long-term cost efficiency [90,91]. In tandem, quieter dental equipment, including low-noise air turbines and ultrasonic scalers, are recommended to reduce background stress, improve communication clarity, and protect the auditory health of staff and patients alike [2,5]. Additionally, spatial zoning, strategically separating high-noise procedures from quieter consultative or recovery areas, has emerged as a key intervention to manage cumulative sound exposure and optimize workflow within eco-conscious clinic layouts [58].
Crucially, the emerging frontier in healthcare and dental design lies in adaptive and personalized soundscapes [92]. Recent research highlights how AI-integrated acoustic systems can dynamically adjust the auditory environment in response to patient-specific needs, reducing sensory overload for neurodivergent individuals, providing calming background tones for anxious adults, or incorporating gamified, interactive cues to ease pediatric procedures [85,93]. These intelligent sound environments not only enhance patient comfort but also improve communication, reduce staff fatigue, and support procedural efficiency. They align with broader biomimetic and responsive design movements that draw inspiration from nature’s feedback systems, aiming to create “healing ecosystems” where architecture, sound, light, and user behavior are in continuous dialogue. Such innovations represent a paradigm shift from static clinical settings to dynamic, emotionally attuned environments that actively support health and well-being [38,71,85,93].
At the systems level, interdisciplinarity is not merely encouraged; it is essential. Collaboration among architects, clinicians, environmental psychologists, and engineers must guide both the design of new dental facilities and the retrofitting of existing ones to meet contemporary standards of sensory and psychological care [19,27]. Such collaborative efforts ensure that acoustic strategies are not treated as afterthoughts but are integrated from the earliest planning stages. Furthermore, design frameworks must evolve to treat acoustic quality as a core determinant of health, aligning with hygiene, lighting, and ergonomic principles [43,68]. These perspectives reinforce the need for regulatory bodies and institutional stakeholders to adopt acoustic benchmarks in dental and healthcare facility guidelines, thereby institutionalizing sound as an element of therapeutic infrastructure.
Overall, the dental clinic is evolving from a space of sterile procedural function into an experiential care hub, capable of supporting emotional health, staff performance, and environmental responsibility. Acoustic wellness is no longer an optional amenity; it is integral to therapeutic outcomes and patient trust. As this field matures, it must continue to push boundaries through research, design innovation, and policy advocacy to redefine what dental care environments can be.
Ultimately, this review proposes a critical redefinition: the dental clinic is no longer a neutral shell for technical delivery, but a carefully orchestrated sensorial environment that amplifies healing, professionalism, and sustainability. Through evidence-based design and visionary collaboration, acoustic and biophilic excellence can become signature hallmarks of 21st-century dental care. Future dental environments may feature intelligent ecosystems where walls adapt to noise, plants interact acoustically, and soundscapes are personalized in real time, ushering in a new era of responsive, human-centered, and ecologically informed clinic design.
6. Limitations and Strengths of the Study
This review presents several limitations. Most notably, there is a scarcity of randomized controlled trials specifically evaluating acoustic interventions in dental settings. Much of the evidence is extrapolated from broader healthcare environments like ICUs, NICUs, and inpatient wards (e.g., [15,24,27]), which, while relevant, limits direct applicability to dentistry. Additionally, the geographic focus of the included studies skews toward high-income regions, underrepresenting dental environments in low- and middle-income countries [41,58]. Another constraint is the emerging nature of innovations like AI-driven soundscapes and plant acoustics, which are still largely conceptual [85,93]. This makes it difficult to assess their real-world effectiveness in clinical dental settings.
Despite these limitations, the review’s strength lies in its interdisciplinary synthesis. It is among the first to systematically link sustainable acoustics, lean practice, and patient-centered care in dentistry, drawing from 60 screened studies across environmental psychology, healthcare design, and clinical acoustics [94-96]. Practical tools, such as tables, checklists, and a multi-sensory patient journey map, enhance their translational value for clinicians, designers, and policymakers [97-99]. Importantly, this review reframes acoustics as a core component of dental care quality and sustainability. Integrating sound design with the principles of green dentistry and the circular economy promotes the transformation of dental clinics from purely utilitarian settings into spaces that actively support healing, emotional well-being, and sustainable operations [96]. Future research should prioritize participatory design methods, especially engaging vulnerable populations such as children and neurodivergent individuals, to ensure inclusive and adaptive dental environments. Empirical trials should evaluate the impact of real-time sound modulation, acoustic zoning, and biophilic design strategies tailored to clinical dentistry. Additionally, alignment with frameworks such as the WELL Building Standard, particularly its provisions on Comfort (Feature 80: Sound Reducing Surfaces), Mind (Feature 89: Adaptable Spaces), and Nourishment of Sensory Health, can guide the development of acoustically resilient, psychologically supportive, and environmentally responsive dental care spaces [82, 99-101].
7. Conclusions
Acoustic design is a fundamental element of effective, empathetic, and sustainable dental care, not a secondary concern. This review has shown that soundscapes profoundly affect emotional regulation, physiological stress responses, communication, and clinical performance. Given that dental patients remain conscious and psychologically engaged throughout treatment, managing acoustic conditions becomes critical for both therapeutic outcomes and overall patient experience. Overall, the complexity of dental acoustics calls for a truly interdisciplinary approach. Collaboration between dental professionals, architects, acoustic engineers, and behavioral scientists is essential to develop environments that are not only technically proficient but also psychologically supportive and environmentally responsible. Finally, this review proposes the integration of acoustic benchmarks within dental facility guidelines and regulatory standards. It also underlines the need for future empirical studies, particularly randomized trials, real-time soundscape monitoring, and participatory co-design, to validate and refine current design strategies.
As dentistry evolves toward more person-centered, digitally enhanced, and ecologically conscious models, acoustics must be embraced as a core design principle. Doing so will transform dental clinics from purely clinical spaces into restorative, intelligent environments that support the well-being of patients, staff, and the planet alike.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, M.A.; methodology, M.A.; software, M.A., E.I.T., and C.A.; validation, M.A.; formal analysis, M.A., E.I.T., and C.A.; investigation, M.A., E.I.T., and C.A.; resources, M.A.; data curation, M.A., E.I.T., and C.A.; writing—original draft preparation, M.A., E.I.T., and C.A.; writing—review and editing, M.A., E.I.T., and C.A.; visualization, M.A.; supervision, M.A.; project administration, M.A.; funding acquisition, M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
Intensive Care Units (ICUs), Neonatal Intensive Care Units (NICUs), Leadership in energy and environmental design (LEED), Performance-based system for measuring, certifying, and monitoring features of the built environment that impact human health and well-being, through air, water, nourishment, light, fitness, comfort and mind (WELL).
References
- Liu Y, Chen X. A study on the influence of dominant sound sources on users’ emotional perception in a pediatric dentistry clinic. Front. Psychol., 2024, 15. [CrossRef]
- Antoniadou M, Tziovara P, Antoniadou C. The Effect of Sound in the Dental Office: Practices and Recommendations for Quality Assurance-A Narrative Review. Dent J (Basel). 2022 Dec 5;10(12):228. [CrossRef]
- Erfanian M, Mitchell AJ, Kang J, Aletta F. The Psychophysiological Implications of Soundscape: A Systematic Review of Empirical Literature and a Research Agenda. Int J Environ Res Public Health. 2019 Sep 21;16(19):3533. [CrossRef]
- Tziovara, P.; Antoniadou, C.; Antoniadou, M. Patients’ Perceptions of Sound and Noise Dimensions in the Dental Clinic Soundscape. Appl. Sci. 2024, 14, 2587. [Google Scholar] [CrossRef]
- Antoniadou, M.; Tziovara, P.; Konstantopoulou, S. Evaluation of Noise Levels in a University Dental Clinic. Appl. Sci. 2023, 13, 10869. [Google Scholar] [CrossRef]
- Hartland JC, Tejada G, Riedel EJ, Chen AH, Mascarenhas O, Kroon J. Systematic review of hearing loss in dental professionals. Occup Med (Lond). 2023 Oct 20;73(7):391-397. [CrossRef]
- Williamson, S.M.; Prybutok, V. Balancing Privacy and Progress: A Review of Privacy Challenges, Systemic Oversight, and Patient Perceptions in AI-Driven Healthcare. Appl. Sci. 2024, 14, 675. [Google Scholar] [CrossRef]
- Zhou T, Wu Y, Meng Q and Kang J (2020) Influence of the Acoustic Environment in Hospital Wards on Patient Physiological and Psychological Indices. Front. Psychol. 11:1600. [CrossRef]
- Deng L., Hui Rising H, Gu C., Bimal A. The Mitigating Effects of Water Sound Attributes on Stress Responses to Traffic Noise. Environment and Behavior. (accessed on 14 June from https://www.ivysci.com/en/articles/3430467__The_Mitigating_Effects_of_Water_Sound_Attributes_on_Stress_Responses_to_Traffic_Noise. [CrossRef]
- Torresin, S.; Aletta, F.; Babich, F.; Bourdeau, E.; Harvie-Clark, J.; Kang, J.; Lavia, L.; Radicchi, A.; Albatici, R. Acoustics for Supportive and Healthy Buildings: Emerging Themes on Indoor Soundscape Research. Sustainability 2020, 12, 6054. [Google Scholar] [CrossRef]
- Zhao Y, Zhan Q, Xu T. Biophilic Design as an Important Bridge for Sustainable Interaction between Humans and the Environment: Based on Practice in Chinese Healthcare Space. Comput Math Methods Med. 2022 Jul 6;2022:8184534. [CrossRef]
- Drahota A, Ward D, Mackenzie H, Stores R, Higgins B, Gal D, Dean TP. Sensory environment on health-related outcomes of hospital patients. Cochrane Database Syst Rev. 2012 Mar 14;2012(3):CD005315. [CrossRef]
- Khan SH, Xu C, Purpura R, Durrani S, Lindroth H, Wang S, Gao S, Heiderscheit A, Chlan L, Boustani M, Khan BA. Decreasing Delirium Through Music: A Randomized Pilot Trial. Am J Crit Care. 2020 Mar 1;29(2):e31-e38. [CrossRef]
- Cerwén, G.; Pedersen, E.; Pálsdóttir, A.-M. The Role of Soundscape in Nature-Based Rehabilitation: A Patient Perspective. Int. J. Environ. Res. Public Health 2016, 13, 1229. [Google Scholar] [CrossRef] [PubMed]
- Guidolin K, Jung F, Hunter S, et al. The Influence of Exposure to Nature on Inpatient Hospital Stays: A Scoping Review. HERD: Health Environments Research & Design Journal. 2024;17(2):360-375. [CrossRef]
- Finnigan, K.A. Sensory Responsive Environments: A Qualitative Study on Perceived Relationships between Outdoor Built Environments and Sensory Sensitivities. Land 2024, 13, 636. [Google Scholar] [CrossRef]
- Alotaibi, H.M.; Alduais, A.; Qasem, F.; Alasmari, M. Sensory Processing Measure and Sensory Integration Theory: A Scientometric and Narrative Synthesis. Behav. Sci. 2025, 15, 395. [Google Scholar] [CrossRef] [PubMed]
- Pagano, M.; Del Prete, S. Symphonies of Growth: Unveiling the Impact of Sound Waves on Plant Physiology and Productivity. Biology 2024, 13, 326. [Google Scholar] [CrossRef] [PubMed]
- Zhang Q, Huo Q, Chen P, Yao W, Ni Z.Effects of white noise on preterm infants in the neonatal intensive care unit: A meta-analysis of randomised controlled trials. Nurs Open. 2024 Jan;11(1):e2094. [CrossRef]
- Zhang, Z. Linking architecture and emotions: sensory dynamics and methodological innovations. Tesi doctoral, UPC, Departament de Representació Arquitectònica, 2024. Accessed on 14 June from : http://hdl.handle.net/2117/410676. [CrossRef]
- Asojo, A.; Hazazi, F. Biophilic Design Strategies and Indoor Environmental Quality: A Case Study. Sustainability 2025, 17, 1816. [Google Scholar] [CrossRef]
- Sutton J, Austin Z. Qualitative Research: Data Collection, Analysis, and Management. Can J Hosp Pharm. 2015 May-Jun;68(3):226-31. [CrossRef]
- Page MJ, et al. BMJ 2021;372:n71. [CrossRef]
- Tahvili A, Waite A, Hampton T, Welters I, Lee PJ.Noise and sound in the intensive care unit: a cohort study. Sci Rep. 2025 Mar 29;15(1):10858. [CrossRef]
- Lin CY, Shepley MM, Ong A. Blue Space: Extracting the Sensory Characteristics of Waterscapes as a Potential Tool for Anxiety Mitigation. HERD. 2024 Oct;17(4):110-131. Epub 2024 Sep 16. [CrossRef]
- Jonescu EE, Farrel B, Ramanayaka CE, White C, Costanzo G, Delaney L, Hahn R, Ferrier J, Litton E.Mitigating Intensive Care Unit Noise: Design-Led Modeling Solutions, Calculated Acoustic Outcomes, and Cost Implications. HERD. 2024 Jul;17(3):220-238. Epub 2024 Mar 21. [CrossRef]
- Elf M, Lipson-Smith R, Kylén M, Saa JP, Sturge J, Miedema E, Nordin S, Bernhardt J, Anåker A. A Systematic Review of Research Gaps in the Built Environment of Inpatient Healthcare Settings. HERD. 2024 Jul;17(3):372-394. Epub 2024 May 28. [CrossRef]
- Engineer, A., Ida, A., Jung, W., Sternberg, E.M. Measuring the Impact of the Built Environment on Health, Wellbeing, and Performance: Techniques, Methods, and Implications for Design Research (1st ed.). Routledge. 2024. [CrossRef]
- Tronstad O, Zangerl B, Patterson S, Flaws D, Yerkovich S, Szollosi I, White N, Garcia-Hansen V, Leonard FR, Weger BD, Gachon F, Brain D, Lavana J, Hodgson C, Fraser JF.The effect of an improved ICU physical environment on outcomes and post-ICU recovery-a protocol. Trials. 2024 Jun 11;25(1):376. [CrossRef]
- Kurniawati ND, Dewi YS, Wahyuni ED, Arifin H, Poddar S, AlFaruq MF, Febriyanti RD. Overview of ICU Nurses' Knowledge and Need Assessment for Instrument to Detect Sick Building Syndrome. SAGE Open Nurs. 2024 Dec 12;10:23779608241288716. eCollection 2024 Jan-Dec. [CrossRef]
- Raghuwanshi NK, Yadav SK, Jayaswal P, Parey A. Noise effects, analysis and control in hospitals - A review. Noise & Vibration Worldwide. 2024;55(3):123-134. [CrossRef]
- Rodríguez-Nogueiras, (2024), Factors Related to The Perception of Hospital Noise in A Neuroscience Unit, J Clinical Cardiology and Cardiovascular Interventions, 7(14). [CrossRef]
- Al Khatib I. Samara F., Ndiaye M. A systematic review of the impact of therapeutical biophilic design on health and wellbeing of patients and care providers in healthcare services settings. Front. Built Environ., 2024, 10 – 2024. anti gia Rodhe. [CrossRef]
- Armbruster C, Walzer S, Witek S, Ziegler S, Farin-Glattacker E.Noise exposure among staff in intensive care units and the effects of unit-based noise management: a monocentric prospective longitudinal study. BMC Nurs. 2023 Dec 6;22(1):460. [CrossRef]
- Kumar S., Underwood SH., Masters JL. Manley NA., Konstantzos J. Ten questions concerning smart and healthy built environments for older adults. Building and Environment. 2023, 244, 110720. [CrossRef]
- Bergefurt L, Appel-Meulenbroek R, Arentze T. How physical home workspace characteristics affect mental health: A systematic scoping review. Work. 2023;76(2):489-506. [CrossRef]
- Bringel JMA, Abreu I, Muniz MMC, de Almeida PC, Silva MG. Excessive Noise in Neonatal Units and the Occupational Stress Experienced by Healthcare Professionals: An Assessment of Burnout and Measurement of Cortisol Levels. Healthcare (Basel). 2023 Jul 12;11(14):2002. [CrossRef]
- Verderber S, Koyabashi U, Cruz CD, Sadat A, Anderson DC. Residential Environments for Older Persons: A Comprehensive Literature Review (2005–2022). HERD: Health Environments Research & Design Journal. 2023;16(3):291-337. [CrossRef]
- Nicoletta S, Eletta N, Cardinali P, Migliorini L.A Broad Study to Develop Maternity Units Design Knowledge Combining Spatial Analysis and Mothers' and Midwives' Perception of the Birth Environment. HERD. 2022 Oct;15(4):204-232. Epub 2022 Jul 10. [CrossRef]
- Meng Q, Lee PJ and Ma H (2022) Editorial: Sound Perception and the Well-Being of Vulnerable Groups. Front. Psychol. 13:836946. [CrossRef]
- Lo Castro, F.; Iarossi, S.; Brambilla, G.; Mariconte, R.; Diano, M.; Bruzzaniti, V.; Strigari, L.; Raffaele, G.; Giliberti, C. Surveys on Noise in Some Hospital Wards and Self-Reported Reactions from Staff: A Case Study. Buildings 2022, 12, 2077. [Google Scholar] [CrossRef]
- Khowaja S, Ariff S, Ladak L, Manan Z, Ali T. Measurement of sound levels in a neonatal intensive care unit of a tertiary care hospital, Karachi, Pakistan. Pediatr Neonatol. 2022 Nov;63(6):618-624. Epub 2022 Jul 31. [CrossRef]
- Ruettgers N, Naef AC, Rossier M, Knobel SEJ, Jeitziner MM, Grosse Holtforth M, Zante B, Schefold JC, Nef T, Gerber SM.Perceived sounds and their reported level of disturbance in intensive care units: A multinational survey among healthcare professionals. PLoS One. 2022 Dec 30;17(12):e0279603. eCollection 2022. [CrossRef]
- Wazzan M, Estaitia M, Habrawi S, Mansour D, Jalal Z, Ahmed H, Hasan HA, Al Kawas S. The Effect of Music Therapy in Reducing Dental Anxiety and Lowering Physiological Stressors. Acta Biomed. 2022 Jan 19;92(6):e2021393. [CrossRef]
- Souza RCDS, Calache ALSC, Oliveira EG, Nascimento JCD, Silva NDD, Poveda VB. Noise reduction in the ICU: a best practice implementation project. JBI Evid Implement. 2022 Dec 1;20(4):385-393. [CrossRef]
- Seyffert, S., Moiz, S., Coghlan, M. et al. Decreasing delirium through music listening (DDM) in critically ill, mechanically ventilated older adults in the intensive care unit: a two-arm, parallel-group, randomized clinical trial. Trials 23, 576 (2022). [CrossRef]
- Huntsman DD, Bulaj G. Healthy Dwelling: Design of Biophilic Interior Environments Fostering Self-Care Practices for People Living with Migraines, Chronic Pain, and Depression. Int J Environ Res Public Health. 2022 Feb 16;19(4):2248. [CrossRef]
- Torresin S, Albatici R, Aletta F, Babich F, Oberman T, Kang J. Associations between indoor soundscapes, building services and window opening behaviour during the COVID-19 lockdown. Building Services Engineering Research & Technology. 2021;43(2):225-240. [CrossRef]
- de Lima Andrade E, da Cunha E Silva DC, de Lima EA, de Oliveira RA, Zannin PHT, Martins ACG.Environmental noise in hospitals: a systematic review. Environ Sci Pollut Res Int. 2021 Apr;28(16):19629-19642. Epub 2021 Mar 5. [CrossRef]
- Patil J. Perception of Patient and Visitors on Noise Pollution in Hospitals and Need of the Real Time Noise Monitoring System. J Health Edu Res Dev, 2021, 9:4.
- Dzhambov AM, Lercher P, Stoyanov D, Petrova N, Novakov S, Dimitrova DD. University Students' Self-Rated Health in Relation to Perceived Acoustic Environment during the COVID-19 Home Quarantine. Int J Environ Res Public Health. 2021 Mar 4;18(5):2538. [CrossRef]
- Fu VX ; Oomens, P.; Merkus, N., Jeekel J.The Perception and Attitude Toward Noise and Music in the Operation Room: A Systematic Review. United States. The Journal of surgical research, 2021, 263, 193.
- Allahyar M., Kazemi F. Effect of landscape design elements on promoting neuropsychological health of children. Urban Forestry & Urban Greening. 2021, 65, 127333. [CrossRef]
- Noble, L. The Design of Psychotherapy Waiting Rooms" Psychology Honors Papers. 2020, 79. https://digitalcommons.conncoll.edu/psychhp/79.
- Dabrowska MA. The Role of Positive Distraction in the Patient’s Experience in Healthcare Setting:A Literature Review of the Impacts of Representation of Nature, Sound, Visual Art, and Light A Thesis Presented to The Academic Faculty By Maria Anna D ! browska In Partial Fulfillment Of the Requirements for the Degree Master of Science in Architecture: Health and Design School of Architecture Georgia Institute of Technology December 2020 (accessed on 14 June from https://www.scribd.com/document/743506359/Dabrowska-Thesis-2020).
- Schmidt N, Gerber SM, Zante B, Gawliczek T, Chesham A, Gutbrod K, Müri RM, Nef T, Schefold JC, Jeitziner MM.Effects of intensive care unit ambient sounds on healthcare professionals: results of an online survey and noise exposure in an experimental setting. Intensive Care Med Exp. 2020 Jul 23;8(1):34. [CrossRef]
- Jiang, S. (2022). Nature through a Hospital Window: The Therapeutic Benefits of Landscape in Architectural Design (1st ed.). Routledge. [CrossRef]
- Ma KW, Wong HM, Mak CM. Dental Environmental Noise Evaluation and Health Risk Model Construction to Dental Professionals. Int J Environ Res Public Health. 2017 Sep 19;14(9):1084. [CrossRef]
- Mohammed, H.M.EH.S., Badawy, S.S.I., Hussien, A.I.H. et al. Assessment of noise pollution and its effect on patients undergoing surgeries under regional anesthesia, is it time to incorporate noise monitoring to anesthesia monitors: an observational cohort study. Ain-Shams J Anesthesiol 12, 20 (2020). [CrossRef]
- Zijlstra E, Hagedoorn M, Krijnen WP, van der Schans CP, Mobach MP (2019) The effect of a non-talking rule on the sound level and perception of patients in an outpatient infusion center. PLoS ONE 14(2): e0212804. [CrossRef]
- Benzies KM, Shah V, Aziz K, Lodha A, Misfeldt R.The health care system is making 'too much noise' to provide family-centred care in neonatal intensive care units: Perspectives of health care providers and hospital administrators. Intensive Crit Care Nurs. 2019 Feb;50:44-53. Epub 2018 May 11. [CrossRef]
- Johansson L, Lindahl B, Knutsson S, Ögren M, Persson Waye K, Ringdal M.Evaluation of a sound environment intervention in an ICU: A feasibility study. Aust Crit Care. 2018 Mar;31(2):59-70. Epub 2017 May 12. [CrossRef]
- Fan L, Baharum MR. The effect of exposure to natural sounds on stress reduction: a systematic review and meta-analysis. Stress. 2024 Jan;27(1):2402519. Epub 2024 Sep 17. [CrossRef]
- Mittelmark M. B., Sagy S., Eriksson M., Bauer G. F., Pelikan J. M., Lindström B., Espnes G. A. (Eds.). (2017). The handbook of salutogenesis. Springer.
- Williams, F. The Nature Fix: Why Nature Makes Us Happier, Healthier, and More Creative. W. W. Norton & Company, 2017.
- Zhang, Y., Tzortzopoulos, P., & Kagioglou, M. (2018). Healing built-environment effects on health outcomes: environment–occupant–health framework. Building Research & Information, 47(6), 747–766. [CrossRef]
- Roe, J., McCay LRestorative Cities. urban design for mental health and wellbeing, Bloomsbury Publishing 2016.
- MacAllister L, Zimring C, Ryherd E. Environmental Variables That Influence Patient Satisfaction: A Review of the Literature. HERD: Health Environments Research & Design Journal. 2016;10(1):155-169. [CrossRef]
- Fecht D, Hansell AL, Morley D, Dajnak D, Vienneau D, Beevers S, Toledano MB, Kelly FJ, Anderson HR, Gulliver J.Spatial and temporal associations of road traffic noise and air pollution in London: Implications for epidemiological studies. Environ Int. 2016 Mar;88:235-242. Epub 2016 Jan 11. [CrossRef]
- Kaur H, Rohlik GM, Nemergut ME, Tripathi S.Comparison of staff and family perceptions of causes of noise pollution in the Pediatric Intensive Care Unit and suggested intervention strategies. Noise Health. 2016 Mar-Apr;18(81):78-84. [CrossRef]
- Iyendo, TO. Exploring the effect of sound and music on health in hospital settings: A narrative review. Int J Nurs Stud. 2016 Nov;63:82-100. Epub 2016 Aug 20. [CrossRef]
- Nieto-Sanjuanero A, Quero-Jiménez J, Cantú-Moreno D, Rodríguez-Balderrama I, Montes-Tapia F, Rubio-Pérez N, Treviño-Garza C, de la O-Cavazos M.Evaluation of strategies aimed at reducing the level of noise in different areas of neonatal care in a tertiary hospital].Gac Med Mex. 2015 Nov-Dec;151(6):741-8.
- Mazer, S. Music as Environmental Design. Accessed on 14 June from file:///E:/%CE%9D%CE%AD%CE%B5%CF%82%20%CE%B4%CE%B7%CE%BC%CE%BF%CF%83%CE%B9%CE%B5%CF%8D%CF%83%CE%B5%CE%B9%CF%82%20%CE%B3%CE%B9%CE%B1%20coaching%202/sound%20in%20dentistry/mdpi_acoustics%20in%20dental%20spacies/Music_as_Environmental_Design.pdf.
- Cochrane Methods Bias. RoB 2: A revised Cochrane risk-of-bias tool for randomized trials. Accessed on 25 april from https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials.
- Li L, Asemota I, Liu B, Gomez-Valencia J, Lin L, Arif AW, Siddiqi TJ, Usman MS. AMSTAR 2 appraisal of systematic reviews and meta-analyses in the field of heart failure from high-impact journals. Syst Rev. 2022 Jul 23;11(1):147. [CrossRef]
- Sukhera, J. Narrative Reviews: Flexible, Rigorous, and Practical. J Grad Med Educ. 2022 Aug;14(4):414-417. [CrossRef]
- Antoniadou M, Tzoutzas I, Tzermpos F, Panis V, Maltezou CH, et al. (2020) Infection Control during COVID-19 Outbreak in a University Dental School. J Oral Hyg Health 8: 264.
- Antoniadou, M. Integrating Lean Management and Circular Economy for Sustainable Dentistry. Sustainability 2024, 16, 10047. [Google Scholar] [CrossRef]
- Zhong W., SchröderT., Bekkering J. Biophilic design in architecture and its contributions to health, well-being, and sustainability: A critical review.Frontiers of Architectural Research 2022, 11, 114-141. [CrossRef]
- Heikkilä M, Verma I, Nenonen S. Toward Restorative Hospital Environment: Nature and Art in Finnish Hospitals. HERD: Health Environments Research & Design Journal. 2024;17(3):239-250. [CrossRef]
- Fei, X.; Wu, Y.; Dong, J.; Kong, D. The Effects of Soundscape Interactions on the Restorative Potential of Urban Green Spaces. Sustainability 2025, 17, 2674. [Google Scholar] [CrossRef]
- Bhandawat A., Jayaswall K. Biological relevance of sound in plants.Environmental and Experimental Botany 2022, 200, 104919. [CrossRef]
- Candido C., Durakovic I., Marzban S. Routledge Handbook of High-Performance Workplaces.1st Edition, 2024.
- Yin J, Yuan J, Arfaei N, Catalano PJ, Allen JG, Spengler JD. Effects of biophilic indoor environment on stress and anxiety recovery: A between-subjects experiment in virtual reality. Environ Int. 2020 Mar;136:105427. Epub 2019 Dec 24. [CrossRef] [PubMed]
- Hussain M., Rahman MK., Mishra RC., Van Der Straeten D. Plants can talk: a new era in plant acoustics. Trends in Plant Sci. 2023, 28, 987-990. [CrossRef]
- Napier T., Ahn E. Allen-Ankins S., Lin Schwarzkopf L., Lee I. Advancements in preprocessing, detection and classification techniques for ecoacoustic data: A comprehensive review for large-scale Passive Acoustic Monitoring. Expert Systems with Applications 2024, 252, Part B. [CrossRef]
- Zaffaroni-Caorsi, V.; Azzimonti, O.; Potenza, A.; Angelini, F.; Grecchi, I.; Brambilla, G.; Guagliumi, G.; Daconto, L.; Benocci, R.; Zambon, G. Exploring the Soundscape in a University Campus: Students’ Perceptions and Eco-Acoustic Indices. Sustainability 2025, 17, 3526. [Google Scholar] [CrossRef]
- Devetziadou M., Antoniadou M. Dental patients’ journey map: Introduction to patients’ touchpoints. On J Dent & Oral Health 2021, 4(4). OJDOH.MS.ID.000593.
- Martin N. Sheppard M., Gorasia GP., Arora P., Cooper M., Mulligan S.Awareness and barriers to sustainability in dentistry: A scoping review. Journal of Dentistry 2021, 112, 103735. [CrossRef]
- Antoniadou, M.; Chrysochoou, G.; Tzanetopoulos, R.; Riza, E. Green Dental Environmentalism among Students and Dentists in Greece. Sustainability 2023, 15, 9508. [Google Scholar] [CrossRef]
- Speroni, S.; Polizzi, E. Green Dentistry: State of the Art and Possible Development Proposals. Dent. J. 2025, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Glista D, Schnittker JA, Brice S. The Modern Hearing Care Landscape: Toward the Provision of Personalized, Dynamic, and Adaptive Care. Semin Hear. 2023 Jun 6;44(3):261-273. [CrossRef]
- Almadhoob A, Ohlsson A. Sound reduction management in the neonatal intensive care unit for preterm or very low birth weight infants. Cochrane Database Syst Rev. 2020 Jan 27;1(1):CD010333. Update in: Cochrane Database Syst Rev. 2024 May 30;5:CD010333. 10.1002/14651858.CD010333.pub4. [CrossRef]
- Shannon MM, Nordin S, Bernhardt J, Elf M. Application of Theory in Studies of Healthcare Built Environment Research. HERD. 2020 Jul;13(3):154-170. Epub 2020 Jan 29. [CrossRef] [PubMed]
- Bernhardt J, Lipson-Smith R, Davis A, White M, Zeeman H, Pitt N, Shannon M, Crotty M, Churilov L, Elf M. Why hospital design matters: A narrative review of built environments research relevant to stroke care. Int J Stroke. 2022 Apr;17(4):370-377. Epub 2021 Oct 5. [CrossRef]
- Antoniadou, M. Integrating Lean Management and Circular Economy for Sustainable Dentistry. Sustainability 2024, 16, 10047. [Google Scholar] [CrossRef]
- Nenningsland TS, Alfheim HB, Asadi-Azarbaijani B, Mattsson J, Mikkelsen G, Hansen EH.Nurses' perceptions of the layout and environment of the paediatric intensive care unit in terms of sleep promotion. Nurs Crit Care. 2025 May;30(3):e70016. [CrossRef]
- Zhang, Z. Linking architecture and emotions: sensory dynamics and methodological innovations. Tesi doctoral, UPC, De-partament de Representació Arquitectònica, 2024. Available at: http://hdl.handle.net/2117/410676. [CrossRef]
- Noble L, Devlin AS. Perceptions of Psychotherapy Waiting Rooms: Design Recommendations. HERD. 2021 Jul;14(3):140-154. Epub 2021 Apr 12. [CrossRef]
- Tronstad O, Flaws D, Patterson S, Holdsworth R, Fraser JF.Creating the ICU of the future: patient-centred design to optimise recovery. Crit Care. 2023 Oct 21;27(1):402. [CrossRef]
- WELL Building Standard v1, 2016. Accessed 14 June 2025 from https://standard.wellcertified.com/well].
Figure 1.
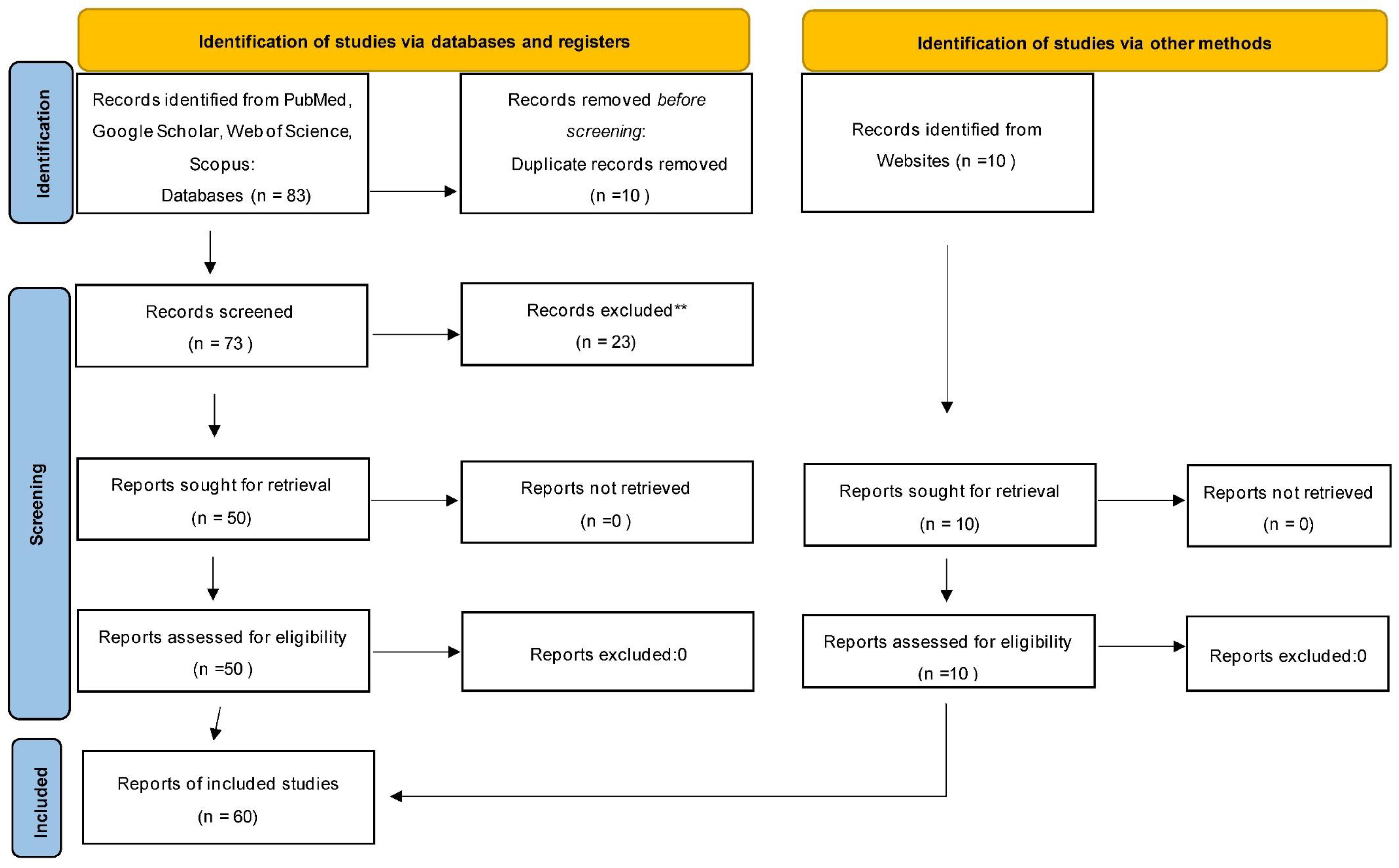
Table 1.
Multidisciplinary Evidence on Acoustic Environments in Dental and Healthcare Settings.
| No | Study (Authors, Year) | Study Type | Setting | Methodology | Outcomes | Suggested Architectural Intervention |
|---|---|---|---|---|---|---|
| 1 | Tahvili et al. (2025)[24]. | Cohort Study | ICU | Measured ICU noise at 87 dBA | Confirmed excessive noise, often over threshold | General Environmental Improvement |
| 2 | Zhang et al. (2024)[19]. | Meta-analysis | NICU | Review of RCTs assessing effects of white noise on preterm infants | White noise reduced pain and improved weight gain and vital signs | General Environmental Improvement |
| 3 | Guidolin et al. (2024)[15]. | Scoping Review | Hospital | Comparative studies of inpatient nature exposure | Nature soundscapes aid stress recovery and satisfaction | Biophilic and Acoustic Comfort Design |
| 4 | Lin et al. (2024)[25]. | Empirical Study | Healthcare | Sensory mapping and soundscape assessment | Water and greenery reduce anxiety | Biophilic and Acoustic Comfort Design |
| 5 | Zhang (2024)[20]. | Conceptual Paper | Healthcare | Design review & emotional mapping | Biophilic design enhances perception through acoustics | Biophilic and Acoustic Comfort Design |
| 6 | Jonescu et al. (2024)[26]. | Modeling Study | ICU | Design-led acoustic modeling intervention | Reduced noise transmission and improved acoustic outcomes | Architectural Redesign (e.g., sound-absorbing materials, spatial layout changes) |
| 7 | Elf, et al . (2024)[27]. | Systematic Review | Inpatient Healthcare Settings | Comprehensive literature review of peer-reviewed studies on built environments in inpatient care | Identified major research gaps including the lack of evidence on spatial design and environmental factors (like acoustics) affecting outcomes | Call for interdisciplinary research; emphasized patient-centered architectural design, incorporating flexible, adaptable, and sensory-sensitive spaces |
| 8 | Engineer et al. (2024)[28]. | Book Chapter | Healthcare | Review and applied examples | Built environment influences pain perception and emotional state | Healing Environment Design (e.g., sleep-supportive design, family zones) |
| 9 | Tronstad et al. (2024)[29]. | Protocol | ICU | Study protocol for improved ICU environment | Focus on the environment (noise, light) to optimize recovery | Architectural Redesign (e.g., sound-absorbing materials, spatial layout changes) |
| 10 | Kurniawati et al. (2024)[30]. | Survey | ICU | Nurses' knowledge and needs for detecting Sick Building Syndrome | Knowledge gaps found; suggested educational programs | General Environmental Improvement |
| 11 | Raghuwanshi et al. (2024)[31]. | Review | Hospital | Review of noise effects and control strategies in hospitals | Summarized impacts and control methods | General Environmental Improvement |
| 12 | Rodriguez-Nogueiras (2024)[32]. | Observational Study | Neuroscience Unit | Perception of hospital noise | Highlighted high perceived noise among patients | General Environmental Improvement |
| 13 | Tziovara et al. (2024)[4]. | Survey | Dental Clinic | Patients' perceptions of dental clinic soundscape | Described sound as potentially stressful | General Environmental Improvement |
| 14 | Al Khatib et al (2024)[33]. | Review | Healthcare | Environmental comfort synthesis | Comfort includes biophilic sounds and views | Biophilic and Acoustic Comfort Design |
| 15 | Armbruster et al. (2023)[34]. | Longitudinal Study | ICU | Prospective study of noise levels and noise management | Interventions reduced noise, but levels remained above WHO limits | General Environmental Improvement |
| 16 | Antoniadou et al. (2023)[5]. | Observational Study | Dental Clinic | Noise level evaluation at the university dental clinic | Documented excessive noise levels and suggested solutions | General Environmental Improvement |
| 17 | Deng et al. (2023)[9]. | Experimental Study | Healthcare | Water sound interventions | Calming water sounds reduce physiological stress, improve comfort | Healing Environment Design (e.g., sleep-supportive design, family zones) |
| 18 | Kumar et al. (2023)[35]. | Perspective/Review | Smart Buildings | Ten principles review | Acoustic comfort is essential in smart healthcare environments | Multi-Sensory and Comfort-Oriented Design |
| 19 | Bergefurt et al. (2023)[36]. | Systematic Review | Workspaces | Mental health metrics | Noise, privacy, and green views affect mental health | Healing Environment Design (e.g., sleep-supportive design, family zones) |
| 20 | Bringel et al. (2023)[37]. | Observational Study | NICU | Assessed noise and staff cortisol levels | Identified link between noise and staff burnout | General Environmental Improvement |
| 21 | Verderber et al. (2023)[38]. | Comprehensive Literature Review | Residential Environments for Older Adults | Reviewed 17 years of interdisciplinary literature (2005–2022) on residential design for older populations | Identified key environmental factors influencing physical health, emotional well-being, and social engagement in aging | Design of age-friendly, sensory-sensitive spaces with biophilic elements, acoustic zoning, and adaptable layouts |
| 22 | Nicoletta et al. (2022)[39]. | Mixed Methods Study | Maternity Unit | Combined spatial analysis and user perception | Contributed to design knowledge for maternity care | Architectural Redesign (e.g., sound-absorbing materials, spatial layout changes) |
| 23 | Antoniadou et al. (2022)[2]. | Narrative Review | Dental Clinic | Sound impact in dental clinics | Outlined practices and recommendations for sound control | General Environmental Improvement |
| 24 | Meng et al. (2022)[40]. | Editorial | Vulnerable Groups | Overview on sound perception | Emphasized its role in well-being | Healing Environment Design (e.g., sleep-supportive design, family zones) |
| 25 | Lo Castro et al. (2022)[41]. | Survey | Hospital | Measured noise in wards; staff reactions | Revealed stress and annoyance among healthcare workers | General Environmental Improvement |
| 26 | Khowaja et al. (2022)[42]. | Observational Study | NICU | Sound level measurements in NICU, Karachi | Increased noise is linked to more procedures and staff presence | Real-time Noise Monitoring Systems |
| 27 | Ruettgers et al. (2022)[43]. | Survey | ICU | Online survey of ICU professionals about noise disturbances | Perceived noise negatively impacted well-being | Healing Environment Design (e.g., sleep-supportive design, family zones) |
| 28 | Wazzan et al. (2022)[44]. | Clinical Trial | Dental Clinic | Music therapy intervention with stress measures | Music therapy significantly reduces stress and heart rate in dental patients | Healing Environment Design (e.g., sleep-supportive design, family zones) |
| 29 | Souza et al. (2022)[45]. | Implementation Project | ICU | Best practice implementation for noise control | Successful noise reduction and sleep improvement | Soundproofing and Noise Mitigation (e.g., insulation, barriers, quiet zones) |
| 30 | Seyffert et al. (2022)[46]. | Randomized Clinical Trial | ICU (Intensive Care Unit), Older Adults | Two-arm, parallel-group RCT testing individualized music listening in mechanically ventilated patients | Music listening significantly reduced incidence and duration of delirium in ICU patients | Integration of music delivery systems in patient rooms; sound-zoned ICU design for non-pharmacological interventions |
| 31 | Huntsman & Bulaj (2022)[47]. | Conceptual/Design Study | Residential and clinical interiors | Proposed a framework combining biophilic design with self-care strategies for individuals with chronic conditions | Biophilic interiors promote relaxation, reduce pain perception, and support emotional well-being in chronic patients | Integration of natural elements (plants, natural light, textures, sensory zones) into care-oriented interiors |
| 32 | Torresin et al. (2021)[48]. | Survey + Acoustic Assessment | Residential/Urban | Building soundscape perceptions during lockdown | Access to natural sounds improved well-being and acoustic comfort | Biophilic and Acoustic Comfort Design |
| 33 | de Lima Andrade et al. (2021)[49]. | Systematic Review | Hospital | Reviewed noise levels in hospital settings | Noise impacts both patients' health and staff performance | General Environmental Improvement |
| 34 | Patil (2021)[50]. | Survey | Hospital | Patients and visitors' perceptions of noise | Identified the need for real-time noise monitoring | Real-time Noise Monitoring Systems |
| 35 | Dzhambov et al. (2021)[51]. | Cross-sectional Study | Educational | Student survey on acoustic discomfort | Mental health moderated by perception of indoor soundscapes | Multi-Sensory and Comfort-Oriented Design |
| 36 | Fu et al. (2021)[52]. | Systematic Review | Operating Room | Review of attitudes toward noise/music in OR | Mixed attitudes on the effects of music and noise on performance | General Environmental Improvement |
| 37 | Allahyar & Kazemi (2021)[53]. | Experimental Study | Urban healthcare and educational settings | Evaluated the psychological and neurophysiological effects of different landscape design elements on children through structured observation and assessment tools | Found that natural landscape features such as vegetation, sensory gardens, and organic materials positively influenced neuropsychological well-being, attention, and stress reduction in children | Integration of green zones, sensory gardens, and nature-based play or waiting areas into dental and pediatric clinic architecture |
| 38 | Noble (2020)[54]. | Qualitative Study | Psychotherapy | Psychotherapy waiting room evaluation | Sound and lighting influence the perception of care | Healing Environment Design (e.g., sleep-supportive design, family zones) |
| 39 | Dabrowska (2020)[55]. | Literature Review | Healthcare | Design stimuli (art, sound, nature) | Nature sounds support healing as a positive distraction | Biophilic and Acoustic Comfort Design |
| 40 | Schmidt et al. (2020)[56]. | Survey and Experiment | ICU | Survey and experimental exposure to ICU noise | Identified noise as a stressor for healthcare professionals | General Environmental Improvement |
| 41 | Jiang (2020)[57]. | Qualitative Study | Hospital | User perspectives on hospital design | Biophilic design, including nature sounds, enhances recovery | Biophilic and Acoustic Comfort Design |
| 42 | Ma KW et al. (2020)[58]. | Observational Study | Dental Clinic | Practitioners surveyed about noise effects | Noise is linked to fatigue, impaired focus, and long-term hearing risks | Real-time Noise Monitoring Systems |
| 43 | Khan et al. (2020)[13]. | Randomized Pilot Trial | ICU | Delirium reduction via personalized music in ICU | Music reduced delirium severity, promising for stress environments like dental offices | Healing Environment Design (e.g., sleep-supportive design, familyes) |
| 44 | Mohammed et al. (2020)[59]. | Observational Study | Surgical Suite | Noise exposure in surgeries under regional anesthesia | Proposed real-time noise monitoring during anesthesia | Real-time Noise Monitoring Systems |
| 45 | Zhou et al. (2020)[8]. | Experimental Study | Hospital Ward | Studied acoustic impact on physiological/psychological indices | Reported significant influence of acoustic environment | Architectural Redesign (e.g., sound-absorbing materials, spatial layout changes) |
| 46 | Zijlstra et al. (2019)[60]. | Experimental Study | Outpatient | Tested non-talking rule for sound level impact | Reduced sound and improved patient experience | General Environmental Improvement |
| 47 | Benzies et al. (2019)[61]. | Qualitative Study | NICU | Interviews with healthcare providers and administrators | Highlighted barriers to family-centered care due to noise | General Environmental Improvement |
| 48 | Johansson et al. (2018)[62]. | Feasibility Study | ICU | Intervention to improve ICU sound environment | Design changes were feasible and reduced noise levels | Architectural Redesign (e.g., sound-absorbing materials, spatial layout changes) |
| 49 | Fan & Baharum (2018)[63]. | Systematic Review | Healthcare | Meta-analysis of nature sound exposure | Natural acoustic stimuli reduce stress more than mechanical soundscapes | Biophilic and Acoustic Comfort Design |
| 50 | Lin et al. (2017)[25]. | Mixed-Methods Study | Healthcare | Waterscape preferences for anxiety | Water and greenscape elements significantly reduced anxiety | Biophilic and Acoustic Comfort Design |
| 51 | Mittelmark et al. (2017)[64]. | Book | Healthcare | Focus groups on design elements | Green materials and natural lighting are perceived as most healing | Biophilic and Acoustic Comfort Design |
| 52 | Williams (2017)[65]. | Book | General | Science communication | Auditory connection to nature reduces stress | Biophilic and Acoustic Comfort Design |
| 53 | Zhang & Tzortzopoulos (2016)[66]. | Framework Analysis | Healthcare | Environment and occupants’ health linkage | Multi-sensory comfort is critical to healthcare performance | Multi-Sensory and Comfort-Oriented Design |
| 54 | Roe & McCay (2016)[67]. | Urban Design Theory | Urban | Cross-disciplinary city planning insights | Biophilic city elements improve mental health and reduce stress | Biophilic and Acoustic Comfort Design |
| 55 | MacAllister & Zimring (2016)[68]. | Literature Review | Healthcare | Environmental psychology in design | Noise directly impacts satisfaction and perceived quality of care | Architectural Redesign (e.g., sound-absorbing materials, spatial layout changes) |
| 56 | Fecht et al. (2016)[69]. | Observational Study | Urban | Analyzed noise and air pollution correlations in London | Found spatial-temporal patterns affecting epidemiological results | Architectural Redesign (e.g., sound-absorbing materials, spatial layout changes) |
| 57 | Kaur et al. (2016)[70]. | Survey | PICU | Staff and family survey on noise sources and strategies | Identified key sources of noise and suggested interventions | General Environmental Improvement |
| 58 | Iyendo (2016)[71]. | Narrative Review | Hospital Environments | Synthesized evidence from interdisciplinary studies on the impact of music and sound in hospitals | Sound and music reduce patient anxiety, improve mood, aid healing, and enhance satisfaction | Incorporation of curated soundscapes and therapeutic music zones in hospital design |
| 59 | Nieto-Sanjuanero et al. (2015)[72]. | Observational Study | Neonatal Care | Noise measurement and strategy evaluation | Proposed effective noise-reduction strategies | Real-time Noise Monitoring Systems |
| 60 | Mazer (2014)[73]. | Conceptual/Theoretical Paper | Healthcare Environments | Narrative exploration integrating environmental psychology, music therapy, and person-environment theory | Demonstrated how music, when used as part of environmental design, reduces anxiety, masks unpleasant noise, improves patient experience, and enhances healing. Emphasizes music’s role as a positive auditory stimulus in therapeutic contexts | Integration of curated music into ambient design; use of person-environment auditory alignment; incorporation of music therapy as part of spatial and sensory planning in hospitals and clinics |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



