Submitted:
09 June 2025
Posted:
11 June 2025
You are already at the latest version
Abstract
The gut microbiota has emerged as a key area of biomedical research due to its integral role in maintaining host health and its involvement in the pathogenesis of many systemic diseases. Growing evidence supports the notion that gut dysbiosis contributes significantly to diseases and their progression. An example would be inflammatory bowel disease (IBD), a group of conditions that cause inflammation and swelling of the digestive tract, with the principal types being ulcerative colitis (UC) and Crohn’s disease (CD). Another notable disease with significant association to gut dysbiosis would be colorectal cancer (CRC), a malignancy which typically begins as polyps in the colon or rectum, but has the potential to metastasise to other parts of the body, including the liver and lung amongst others. Concurrently, advances in nanomedicine, an evolving field that applies nanotechnology for disease prevention, diagnosis, and treatment, have opened new avenues for targeted and efficient therapeutic strategies. In this paper, we provide an overview of the gut microbiota and the implications of its dysregulation in human disease. We then review the emerging nanotechnology-based approaches for both therapeutic and diagnostic purposes, with a particular focus on their applications in IBD and CRC.
Keywords:
gut dysbiosis
; inflammatory bowel disease
; colorectal cancer
; nanomedicine
; nanodiagnostics
; nanotherapeutics
; drug delivery systems
1. Introduction
1.1. The Gut Microbiota
The gut microbiome is a complex and dynamic system that originates from vertical transmission from the mother in the uterus, with full-term infants developing extensively colonised gut microbiome [1]. The gut receives a constant stream of microbes, which compete for resources and evade the host immune system to colonise the gut [2]. It is colonised by humongous populations of trillions of microorganisms, of which Bacteroidetes, Firmicutes, Proteobacteria, Fusobacteria, Tenericutes, Actinobacteria, and Verrucomicrobia dominate [3]. The altering gut microbiome has great inter-person variability and undergoes extensive changes with age [4]. Many factors play a role in affecting its composition, including the host’s diet [5], genetics, and immune response [6]. The idea of a healthy gut microbiome is thus hard to define, with possible definitions being one with a stable microbiome community that can resist environmental stresses or a state where important metabolic pathways are preserved [7].
The gut microbiome plays an essential role in maintaining the health of the gastrointestinal tract (GIT). It maintains a thick mucus layer to prevent colonisation of the gut by foreign pathogens [8] and competes for both nutrients and attachment sites on the intestinal walls, preventing pathogen invasion [2,9]. It also promotes the production of antimicrobial molecules [10]. Another key role of the gut microbiome is immunomodulation, as the gut microbiome presents a vast amount of antigens to the immune cells of the mucosa. A fine balance is required to maintain between tolerating the gut microbiome and controlling bacterial microbiome overgrowth [2]. Apart from regulating the local immune response, the gut microbiome also influences the host’s systemic immune responses [10]. The gut is the largest reservoir the immune system actively samples antigens from, and its microbiome is suggested to influence the initiation, progression and severity of autoimmune diseases, including rheumatoid arthritis [11] (Figure 1).
1.2. Gut Dysbiosis
Gut dysbiosis has been described as the disruption of the symbiotic balance between the microbiota and host [12]. It is due to frequent changes to the environment or host related factors [13] that overpowers resistance and protective capabilities of the microbial system in the gut [14]. The host’s diet and antibiotic consumption are 2 major factors that contribute to gut dysbiosis. The gut microbiome is greatly affected by long-term dietary changes, with individuals from different communities having very different gut microbiomes [15]. Different proportions of carbohydrates, proteins, fats, food additives, and cooking methods exert different effects on the gut microbiome [5]. For example, animal-based diets result in a gut microbiome with more bile-tolerant bacteria such as Bacteroides, Alistipes and Biophilia [16,17], but decreases plant polysaccharide-fermenting Firmicutes including Roseburia, Eubacterium rectale, and Ruminococcus bromii [16]. Acute changes in diet can also affect the gut microbiome, with plain plant-based or animal-based diets for 5 days having a significant impact on microbial community structures [16]. Pathogens also trigger gut dysbiosis, where enteric pathogens have the greatest potential to cause microbial dysbiosis in mouse models [18], while foodborne viruses trigger local and systemic inflammation that alters microbial composition [19]. Alteration of the gut microbiome can also promote the growth of unfavourable microbiota that disrupt the intestinal barrier [20], allowing the entrance of hazardous chemicals and promoting systemic inflammation that can cause inflammatory bowel disease (IBD) [21].
The gut microbiome is also severely impacted by the administration of antibiotics, where broad-spectrum antibiotics can affect the abundance of 30% of the bacteria in the gut community, resulting in a marked decrease in taxonomic diversity and richness [22,23]. Antibiotics also alter the gut microbiota’s gene expression, protein activity, and overall metabolism [24,25]. For instance, it has been found that the use of beta-lactams in a host alters carbohydrate degradation and sugar metabolism to mimic that of an obese individual [26]. These antibiotic induced microbiota alterations can remain after long periods of time, ranging from months to years [27]. Notably, another study revealed that mice who were administered antibiotics suffered gut dysbiosis that eventually resulted in cognitive impairment [28]. Other causative factors of gut dysbiosis include host factors such as stress or infections [29].
2. Gut Dysbiosis in Pathogenesis of Diseases
Previous studies have shown that gut dysbiosis has profound implications on health and contributes to the pathogenesis of a range of diseases.
2.1. Gut Dysbiosis in Inflammatory Bowel Disease (IBD)
Gut dysbiosis has been found to play a key role in the pathogenesis of IBD [30], with patients exhibiting a reduced microbial population, functional diversity and microbiome stability [31]. The differing gut microbiota plays a key role in altering the metabolic pathways in the gut– though IBD patients only have a 2% difference in genus level clades, their metabolic pathways have a 12% difference when compared to a healthy individual [32]. Expression of genes related to oxidative stress and sulfate transport were found to be increased in IBD patients [32], and processes including bile acid modification and short chain fatty acid (SCFA) modification also altered in the intestinal microbiome of IBD patients [33,34,35] (Figure 1). These findings support that gut dysbiosis plays a role in the pathogenesis of IBD and is not merely an observed state as a result of the disease.
2.2. Gut Dysbiosis in Colorectal Cancer (CRC)
Changes in the gut microbiome also participate in the development of a substantial number of GIT malignancies [36,37], with links between gut dysbiosis and colorectal cancer (CRC) being found [38,39]. One mechanism involves the gut microbiome inducing genotoxic stress or producing metabolites that promote genetic and epigenetic alterations conducive to carcinogenesis [40]. Another pathway includes modulation of SCFA levels, which can influence global chromatin architecture and subsequently affect gene expression and transcriptional regulation [41]. Butyrate, a SCFA, can modulate the apoptosis, proliferation, and invasion of several cancer cell lines, facilitating aberrant hyperproliferation of colon epithelial cells in mice [42]. Overgrowth of specific bacteria also plays a role in CRC development. Fusobacterium nucleatum directly promotes carcinogenesis when it secretes adhesin FadA that binds to the extracellular domain of E-cadherin on epithelial cells. The adhesin complex is dysfunctional and is unable to bind to beta-catenin, causing beta-catenin to translocate to the nucleus. This upregulates mitogenic signalling, thereby increasing expression of transcription factors and growth stimulation of CRC cells [43]. Bacteroides fragilis secretes the B. fragilis toxin, which cleaves E-cadherin, a tumour suppressor protein. This results in enhanced nuclear Wnt/b-catenin signalling that increases colonic carcinoma cell proliferation and expression of the protooncogene, MYC [44] (Figure 1).
3. Current Therapeutic Strategies
3.1. IBD Treatment
The conventional pharmacological therapy for IBD primarily aims to achieve and sustain remission, as well as alleviate the secondary symptoms of the disease, rather than correct the root pathogenic mechanism [45,46]. Commonly used drugs include corticosteroids, aminosalicylates, and immunosuppressive agents [47], while metronidazole and broad-spectrum antibiotics may be found useful at times [46]. Specific drugs are preferred for various aims; steroids are selected for the short-term control of moderate to severe flare-ups but unsuitable for long-term use due to their many systemic adverse effects and inability to maintain remission. At the same time, immunosuppressants, such as azathioprine, are preferentially employed in long-term therapy due to their delayed onset of therapeutic action [46].
Patients suffering from mild to moderate IBD are first treated with 5-aminosalicylic acid (5-ASA) before being given systemic glucocorticosteroids for more severe disease [48]. Azo-linked prodrugs of 5-ASA include sulfasalazine, olsalazine, and balsalazide, which are designed to deliver 5-ASA (mesalamine) specifically to the colon. These prodrugs remain intact through the upper GIT before being activated in the colon by azoreductase enzymes produced by colonic bacteria, cleaving the azo bond and releasing 5-ASA [46]. 5-ASA exerts its anti-inflammatory effects via the activation of peroxisome proliferator-activated receptor-gamma (PPAR-γ), a nuclear receptor highly expressed in colonic epithelial cells whose signalling is otherwise impaired in IBD [49]. Though 5-ASA is generally well tolerated, the most common adverse effects include diarrhoea, nausea/vomiting, headache, abdominal pain/dyspepsia, rash, fever, fatigue/weakness, arthralgia/myalgia [50].
The preferred corticosteroid therapy for IBD is prednisolone, whose administration can be done orally, rectally or in urgent emergencies, parenterally [46]. Glucocorticoids modulate immune responses by binding to glucocorticoid receptors, regulating pro-inflammatory genes and suppressing immune-controlling transcription factors like nuclear factor κB (NF-κB). They also exert rapid non-genomic effects on cell signalling and ultimately reduce immune cell activation, pro-inflammatory cytokine production and promote apoptosis in dendritic cells and T cells [48]. However, the numerous adverse effects of corticosteroids remain a concern, with long-term use impacting patients’ metabolic and endocrine functions. These include weight gain, change of fat distribution, hyperglycemia leading to diabetes, hypertension, reduced muscle and bone mass leading to osteoporosis and fractures, changes to skin with acne, cataract, glaucoma and depression [51]. There is also a pronounced risk of opportunistic infections when corticosteroids are prescribed concomitantly with other immunosuppressive drugs or biologics [52].
In patients with severe IBD or who are already steroid-resistant or dependent, immunosuppressants such as azathioprine and thiopurine derivative mercaptopurine are being used [53]. Azathioprine is a prodrug that is metabolised into mercaptopurine, which is further converted into 6-thioguanine nucleotides– the primary active compounds that suppress purine synthesis and inhibit cellular proliferation [46]. However, adverse effects are prominent, including allergic reactions consisting of fever or rash, or both, arthritis; leukopenia; pancreatitis; and nausea. In a study, they were severe enough that 27 of 302 patients had to be withdrawn from the trial [53].
Anti-tumor necrosis factor-alpha (TNF-α) monoclonal antibodies such as Infliximab, can induce apoptosis in mucosal T cells [54], macrophages, and monocytes [55]. These antibodies are also able to modulate fibroblast function [56], decrease leukocyte migration [57], and induce mucosal regulatory macrophages [58]. However, the development of tolerance to these drugs [59] and increased frequency of serious infections are the downsides to this treatment [60]. Another antibody used is ustekinumab, a fully humanised antibody that blocks the p40 subunit of interleukin(IL)-12 and IL-23, showing consistent benefit over the placebo group treating CD and UC as both induction and maintenance therapy [61,62]. The rate of antidrug antibodies was found to be low, with the rates of adverse events occurring being similar between the group given ustekinumab and the placebo group [61].
Alternative therapies also include cholestyramine, sodium cromoglycate, bismuth, and arsenical salts, methotrexate and fish oils [46]. Though primarily established as a treatment methodology for recurrent and refractory Clostridium difficile infections, faecal microbiota transplantation (FMT) is also potentially indicated for IBD [63]. It is essentially stool transplantation, where stools from a healthy donor are transferred into another patient’s GIT to directly compensate for the gut dysbiosis present, and FMT via multiple infusions administered via the lower GIT appears very promising for IBD treatment [64].
3.2. CRC Treatment
Pre-cancerous and early-stage CRC can be removed by an endoscope, a safer and less invasive procedure than surgery [65]. For more advanced stages of CRC with liver metastases, surgical resection remains the only cure [66]. Lymph node dissection is also performed in surgery for staging and to determine the patient's prognosis [65]. While surgery is an important first line of defence, surgery has been shown to increase the mortality risk in some cancer patients by metastasis as it disrupts the integrity of the tumour [67]. Chemotherapy is used to treat CRC as well and can be used for neoadjuvant therapy, adjuvant chemotherapy, or chemotherapy for unresectable CRC [65]. Chemotherapeutic agents include cytotoxic drugs, molecular targeted drugs, and immune checkpoint inhibitors [65]. Traditional chemotherapy agents can also cause systemic effects such as nausea, vomiting, diarrhoea, and neuropathy due to their effect on other rapidly dividing cells in the body [67].
Over the past few decades, patients with CRC were treated homogeneously with the same standard chemotherapy drugs administered after surgical resection [68]. Precision medicine is set to change that, where factors including environmental, lifestyle, cancer staging, and biological characteristics will be evaluated, to identify which treatment approach will be most beneficial, improving treatment response and reducing the likelihood of side effects [69]. Drugs such as anti-vascular endothelial growth factor (VEGF) and anti-epidermal growth factor receptor (EGFR) monoclonal antibodies [68] allow for a more targeted treatment with decreased systemic side effects. While the use of such drugs can avoid systemic side effects, they can potentially result in rash appearing in the upper body [67]. Radiotherapy is used too to treat locally advanced rectal cancer, as an adjuvant to therapy, or as palliative care to preserve patient quality of life [65].
4. Nanomedicine
Nanomedicine is an up-and-coming technology, and branch of evolving medicine that uses nanotechnology for disease prevention, monitoring and intervention through new modalities for imaging, diagnosis, treatment, repair and regeneration of biological systems [70]. Nanoparticles have unique chemical and physical properties that make them suitable for optical imaging, allowing for highly sensitive diagnostic tools with reduced degrees of invasiveness [71]. The high surface area to volume ratio of nanoparticles, combined with their ability to have surface modifications, enable them to deliver therapeutic agents to target sites more accurately, reducing unwanted side effects and thereby improving treatment efficacy [71]. Nanomedicine has revealed a promising future, with third-generation nanovectors bearing multi-functionality; externally are recognition units for nanoparticles to interact with target sites, while internally they are drug-loaded to deliver their desired therapeutic effect at the right place and time [72]. With its rapid development, nanomedicine has revealed great potential in becoming an asset to the healthcare industry by being able to overcome the limitations of traditional treatment methods. The different types of nanomedicine available and their uses in treating gut dysbiosis and its associated diseases will be discussed below.
5. Diagnostic Nanomedicine
5.1. Nanomedicine for Measuring Diagnostic Biomarkers
5.1.1. Biomarkers of Gut Dysbiosis
Nanomedicine has proven its usefulness in assisting in the detection of diagnostic biomarkers. Emerging indicators for gut microbiota health and function include indole and its derivatives, including tryptamine and indoxyl sulfate [73]. They carry out key functions in the gut, such as indole acting as an intracellular signalling molecule that enhances epithelial barrier function [74], promoting the growth of beneficial bacteria while inhibiting the growth of harmful bacteria [75]. High indoxyl sulfate levels are associated with reduced bacterial diversity and shifts in bacterial diversity and composition [76]. Due to their functional roles in maintaining a healthy gut, measuring systemic levels of indole and its related metabolites provides insight into the gut microbiota functional status [77]. Currently, indole levels are measured by mass spectrometry or high-performance liquid chromatography coupled with mass spectrometry [78,79,80] However, its potential as a point-of-care test has been limited due to the costly nature and extensive sample preparation required [81]. To combat this, a nanotip array has been proposed [77], which uses electrochemical sensing to provide a relatively low-cost alternative, requiring minimal sample preparation and also bears the potential for miniaturisation. The nanotip array provides a porous surface area for the attachment of selective capture molecules. Modification with silver (Ag) nanoparticles takes advantage of plasmonic effects to amplify electrical signals, allowing specific and sensitive quantification of indole, tryptamine, and indoxyl sulfate via cyclic voltammetry and differential pulse voltammetry. Given the nanotip’s ability to analyse serum and fecal extracts, it has become extremely attractive for point-of-care testing and bears potential for wide usage [77] (Figure 2A) (Table 1).
5.1.2. Biomarkers in CRC
More specific to CRC is a nanosensor array developed using monolayer-capped 5 nm gold nanoparticles (AuNPs), used as a breath sensor. It bears the capability to distinguish between the breaths of healthy and cancerous patients and even differentiate the types of cancers based on their specific volatile organic compounds (VOCs). This breath analysis method had an edge over breath analysis via gas chromatography linked to the mass spectrometry technique (GC-MS) due to its minimal preparation (pre-concentration or de-humidification) needed, quick and simple procedure, and insensitivity to external interrupting factors which could potentially alter the chemical composition of test subject’s breath, making it a technology that could have significant beneficial impact on cancer treatment [82] (Table 1).
5.2. Nanomedicine in Diagnostic Imaging
Nanotechnology has also proven its utility in radiography modalities through aiding in early diagnosis and improving prognosis of specific diseases.
5.2.1. Diagnostic Imaging of IBD
In IBD, the use of macrophages labelled with superparamagnetic iron oxide (SPIO) and indium (111) oxide (In2O3) nanoparticles enhanced magnetic resonance imaging (MRI) quality by visualising areas on the intestinal wall where signal was originally lost. The percentage of normalised enhancement at MRI correlated well with disease activity, revealing the utility and reliability of the incorporation of SPIO nanoparticles (SPIONs) in MRI -based techniques as a way to study and monitor IBD activity [83]. Another developing nanotechnology developed to target IBD is dextran coated cerium oxide nanoparticles (Dex-CeNP). Unlike iodine and barium-based contrast agents used in hospitals today, Dex-CeNP can enhance CT contrast generation and accumulate in inflammation sites, allowing for the localisation of colitis sites in mice models. They also carry the additional benefit of being able to protect cells against oxidative damage in vitro. Dex-CeNPs have shown potential to be transferred to human clinical use, given that 99.9% and 97.6% of nanoparticles were cleared within 24 hours in healthy and colitis mice respectively [84]. Additionally, the more moderate hypoxic state of patients with IBD compared to other diseases has posed a challenge for traditional hypoxia-activatable fluorescence probes. This has prompted the development of hypoxia-activatable and cytoplasmic protein-powered fluorescence cascade amplifiers (HCFA), which were successful in distinguishing the varying degrees of cellular hypoxia sensitively. This has also proven to be an edifying nanotechnology in the precise diagnosis and management of IBD [85] (Figure 2B) (Table 1).
5.2.2. Diagnostic Imaging of CRC
Diagnosing CRC has also been a beneficiary of the developments in nanotechnology. Near-infrared-emitting AuNPs have been found useful in investigating mechano-growth factor (MGF), an insulin-like growth factor (IGF)-1 isoform that is overexpressed in colon cancer tissues. Moreover, when compared to fluorescent dyes, AuNPs show stronger emission intensity and photostability, and are not cytotoxic like semiconductor quantum dots, making them a potential diagnostic agent [86]. Nanoparticles are also promising contrast agents for MRI, with SPIONs coated with a polymer demonstrating such potential [87]. Quantum dots have also been a growing platform for cancer research and can be used as an alternative to organic dyes. Some of their favourable properties include size-modulated absorbance and emission, high photostability, longer lifetime of excited state, and more [88]. Nanotechnology can also be used to detect circulating tumour cells, which are tumour cells shed from the primary tumour that drive cancer relapse. The concentration of such cells is normally in very low concentrations, making them difficult to detect and use to determine patient prognosis and chances of relapse. Poly(amidoamine) (PANAM) dendrimers were conjugated with various purified anti-Slex (aSlex) antibodies and were able to detect HT29 colon cancer cells with a maximum capture efficiency of 77.88% obtained within 1 hour of exposure. The nanoparticles were even able to detect HT29 cells when diluted with other cells commonly found in blood [89] (Figure 2C) (Table 1).
6. Therapeutic Nanomedicine
6.1. Nanomedicine in Drug Delivery
Nanoscale drug delivery systems (DDS) have been gaining much traction recently due to their ability to carry out targeted drug delivery, maximising efficacy while minimising undesired side effects. This can be attributed to the nanoscale of materials allowing for customisation of specific DDS properties, including drug release characteristics, dissolution, solubility, bioavailability and immunogenicity [90]. The utility of nanomedicine in drug delivery in the realm of treating gut dysbiosis and its associated diseases is discussed below.
6.1.1. Drug Delivery for IBD
Patients with IBD are found to have significantly heightened concentrations of reactive oxygen species (ROS) compared to normal mucosa, providing a potential target for DDS [91]. Based on this concept, a new nanoparticle prodrug named Bud-ATK-Tem (B-ATK-T) has been designed, which links budesonide together with tempol via aromatised thioketal. These thioketal bonds break down in the presence of excessive ROS at inflamed areas, allowing drug release from 55-100% based on the level of ROS present. In the mice model with dextran sulfate sodium induced colitis to model IBD, the B-ATK-T nanoparticle also reduced colon inflammation and weight loss, improved disease activity index while not exhibiting any toxicity to major organs [92] (Figure 3) (Table 2).
To overcome the problems of current first line therapy 5-ASA including high pill burden (2-4x dosing daily) and systemic adverse effects [93], a chitosan (Csn) bound ginger nanocarrier has been developed to enhance site-targeted drug delivery to inflamed mucosal linings in IBD. Csn is formed via the deacetylation of chitin, and has been recognised for its non-toxicity, biocompatibility and biodegradability. The drug carrier complex was able to entrap an estimated 50% of drug and was able to release the drug based on pH sensitivity, making itself a possible solution to overcome the current barriers of 5-ASA [94] (Figure 3) (Table 2).
The delivery of corticosteroids via nanoparticle DDS has also helped to reduce its systemic effects of immunosuppression, enabling their use as long term IBD treatment. For instance, the use of pH sensitive Eudragit L100–55 polymer microparticles loaded with prednisolone ensures that it is only released within the colon, and not in the upper GI tract where pH is acidic [95]. Tannic acid, a degradable mucoadhesive polyphenol, together with polymers, were formulated to form polyphenols and polymers self-assembled nanoparticle (PPNP), made to carry out targeted drug delivery to the colon. Esterase, whose levels are elevated in colon inflammation, can hydrolyse the polyphenols and enable drug release. Comparing the levels of dexamethasone released in the colon without and with esterase, its release increased from 30% to 62%, showing that the approach of incorporating polyphenol in corticosteroid therapy can potentially benefit IBD therapy [96] (Figure 3) (Table 2).
6.1.2. Drug Delivery for CRC
Nano-targeted DDS have also gained popularity among research in cancer pharmacology. Nanoparticles can accumulate in tumour cells due to the enhanced permeability and retention (EPR) effect, where the leaky tumour vasculature results in increased permeability to nanoparticles [97]. Cancer cells also rely on glycolysis instead of the Krebs cycle to produce ATP, known as the Warburg effect, causing the tumour environment to be acidic due to the lactic acid formed as the tumour cells undergo anaerobic respiration [97]. These specific tumour environments allow for the drugs to be released in the tumour site, minimising systemic toxicity associated with cancer drugs [98]. Bufadienolides nanocrystals decorated by Csn quaternary ammonium salt could protect bufadienolides from damage in the acidic environment of the stomach, increasing drug delivery the tumour sites in the colon and increasing its therapeutic effect [99].
Nanoparticles can also be modified and functionalised with specific ligands that enhance their ability to target and bind to CRC cells, thereby improving their uptake by these cells. An epidermal growth factor (EGF) modified poly (lactic-co-glycolic acid) (PLGA) nanoparticle was loaded with 5-fluorouracil (5-FU) and perfluorocarbon (PFC) for a targeted treatment for CRC [100]. The presence of EGF allowed the nanoparticles to interact strongly with cancer cells that expressed EGFR, as the cancer cells could take up the cells via EGF receptor-mediated endocytosis. Nanoparticles with EGF had a more pronounced tumour suppression of SW260 colon cancer cell line and also induced apoptosis in more colon cancer cells [100]. Epithelial cell adhesion molecule (EpCAM) is another target for drug delivery, as it is a dominant surface antigen in human colon carcinoma [101]. Polyethylene glycol (PEG) dendrimers with EpCAM aptamer were able to deliver celastrol, an anticancer agent, to induce apoptosis in SW260 colon cancer cells in vitro and in mice [101]. This targeted DDS was able to reduce local and systemic toxicity in xenograft and mice and zebrafish models, providing a promising treatment that can reduce side effects to the patients [101] (Figure 4) (Table 2).
Beyond targeting the cancer cells themselves, scientists have begun looking into treating cancer stem cells (CSCs). CSCs are a subset of cancer cells with increased renewal capacity and ability to recapitulate the heterogeneity found in primary tumours, playing an essential role in the growth and metastasis of tumours [102]. In view of improving targeted chemotherapy to these cells, there has been a development of a biocompatible tumour-cell-exocytosed exosome-biomimetic porous silicon nanoparticle (PSiNPs). These nanoparticles loaded with DOX have exhibited enhanced tumour accumulation, tumour penetration and cross-reactive cellular uptake by both bulk cancer cells and CSC. Notably, killing activity was demonstrated across several tumour models, including subcutaneous transplantation, orthotopic and advanced metastatic tumour models, demonstrating its potential as a drug carrier to improve anticancer therapy [103] (Figure 4) (Table 2).
6.2. Nanomedicine in Targeted Therapies
6.2.1. Hyperthermia Treatment for CRC
Hyperthermia treatment at 43ºC for 60 minutes can inactivate tumour cells [104]. The highest impact on tumour cells is observed when heating and delivering chemotherapeutic drugs are applied simultaneously in the same area [105], with hyperthermia increasing the effectiveness of 5-FU in disrupting DNA synthesis and repair [106]. Csn-coated magnetic nanoparticles (MNPs) with 5-FU were injected into human colon cancer xenograft in mice before the tumour was exposed to an alternating magnetic field. The thermo-chemotherapeutic treatment resulted in distinct tumour regression, much more evident than magnetic hypothermia or 5-FU alone [104]. 5-FU loaded onto PLGA encapsulating iron oxide nanoparticles has also been found to have increased cytotoxic activity on human colon cancer HT-29 cell lines when exposed to hyperthermia. The nanoparticles combined with hyperthermia treatment were found to have a cytotoxicity of 97.3% compared to 75.5% when 5-FU was given alone. As such, this allows for a lower concentration of 5-FU to be given, reducing the effects of systemic toxicity [107] (Figure 4) (Table 2).
6.2.2. Magnetic Drug Targeting for CRC
MNPs have several advantages over nonmagnetic nanoparticles, as drug release can be controlled via specific magnetic field stimulation, thus improving drug stability and bioavailability. They can also be localised and targeted to specific tissues, minimising unwanted side effects on other tissue sites [108]. SPIONs can aggregate to tumour sites upon exposure to a magnetic field, reducing uncontrolled aggregation in other tissue or in the bloodstream. Docetaxel, a drug that is not systemically used due to its hydrophobic nature, was encapsulated into the oil core of polymeric SPIONs. The nanoparticles were found to have an efficient cell-killing effect on the CT26 cell line in the in vitro cytotoxicity study. Only the magnetically targeted groups were found to have significantly smaller tumour volume compared to that of control treatments [109]. SPIONs were also aggregated with mAb198.3, an antibody that is able to stain and recognise CRC samples from surgically resected samples. The SPIONs linked to mAb198.3 significantly reduced tumour growth compared to the control and the nanoparticles without mAb198.3. A similar tumour size was found for the SPIONs linked to mAb198.3 compared to just using free mAb198.3, despite a 300 fold lower concentration used when the antibodies were linked to SPIONs. Erythrocytes too were engineered to contain the SPIONs and tumour reduction was noted at an earlier time than when SPIONs were used without erythrocytes [110] (Figure 4) (Table 2).
EGFR-targeted monoclonal antibodies like cetuximab have improved survival rates in patients, but their effectiveness has been limited by the KRAS activating mutations that confer resistance in approximately 25% of advanced CRC cases [111]. MNPs can induce oxidative stress by depleting glutathione and inducing ROS production [112]. This ROS-dependent apoptosis is found to enhance existing CRC treatment given drug-resistant late-stage cases. Combining Cetuximab and MNPs showed that approximately 31% of SW-480 CRC tumour cells exhibited signs of apoptosis, higher than the 10% observed when Cetuximab was used alone. This synergistic action led to a significant increase in ROS production, suggesting that intracellular ROS production did lead to the cytotoxic effect observed and holds promise of combining Cetuximab and MNPs to treat cancer [111] (Figure 4) (Table 2).
6.2.3. Photothermal Therapy (PTT) for CRC
Photothermal therapy (PTT) is an emerging and promising strategy in cancer treatment. It involves the use of photothermal agents (PTAs) which convert light energy–typically in the near-infrared (NIR) region–into heat energy, inducing localised thermal injury to tumour tissues and ultimately leading to cancer cell death. An advantage of PTT over conventional cancer therapies is its highly effective and noninvasive nature [113], but challenge still lies in the systemic distribution of PTAs in the body which leads to non-precision exposure and damage to normal tissues surrounding the tumours [114]. Nanotechnology has significantly advanced in the field of PTT. Apart from facilitating cancer diagnosis and treatment monitoring through improved imaging capabilities, nanoparticles have also demonstrated strong absorption in the NIR region alongside accurate targeting of cancer cells for improved specificity, making them highly suitable candidates for PTT applications [115]. Commonly used nanoparticles include metal (gold, iron oxide, Ag etc.) nanoparticles, polymer nanoparticles and carbon nanoparticles.
AuNPs are able to convert light energy in the NIR region to heat energy effectively making it suitable for PTT as NIR is able to penetrate tissue optimally [116]. AuNPs have good biocompatibility and can be functionalised with targeting ligands. PEG-ylated nanoshells with gold were able to significantly reduce rapid tumour growth when tumours were irradiated with NIR light in CT26 CRC tumour xenografts in murine models [117]. AuNPs can also be functionalised with an A33 antibody that binds to the surface antigen A33 that is overexpressed in colon cancer, providing a more targeted PTT approach [118]. Gold nanorods were also able to prolong the lifespan of mice bearing CT26 CRC xenografts, and the gold nanorods were found to accumulate mainly in tumours with no confirmed toxicity to other organs [119] (Figure 4) (Table 2)
Carbon nanotubes are also able to convert NIR light energy to heat, making them a suitable candidate to be used for PTT [116]. Carbon nanotubes can be functionalised with nanocomposite polyhedral oligomeric silsesquioxane poly (carbonate-urea) urethane (POSS-PCU) and can reduce the viability of HT29 CRC cells by 95% upon irradiation with NIR light [120]. Carbon nanotubes can also be conjugated with folic acid onto the surface, as the folic acid receptor is overexpressed in CRC. Cell viability was also found to be greatly reduced in HTC116 and RKO CRC cells after irradiation with NIR light [121]. The combination of PTT with immunotherapy has been explored with the development of GNC-Gal@CMaP nanocomposites. They consist of hollow gold nanocages (GNCs) loaded with galunisertib, a transforming growth factor (TGF)-β inhibitor, and surface-functionalized with anti-programmed cell death ligand-1 (PD-L1) antibodies. The study showed that GNC-Gal@CMaP selectively accumulated in tumours, was able to eliminate the primary tumour mass under NIR light irradiation and inhibited distant metastases, demonstrating the abscopal effect [122] (Figure 4) (Table 2).
A multifunctional endoscope-based interventional system has also been developed, consisting of both bioelectronics and nanoparticles. These nanoparticles are engineered to carry both phototherapeutic and chemotherapeutic agents, which can be precisely delivered and locally activated via light stimulation. This system offers optical fluorescence-based mapping, radio frequency-based ablation and site-specific photo/chemotherapy, forming the basis of a minimally invasive treatment strategy for CRC [123] (Table 2).
6.3. Nanotechnology and the Gut Microbiota
Nanoformulations of probiotics, prebiotics and synbiotics are emerging as powerful tools for optimising gut health treatments [124].
6.3.1. Nano-Prebiotics
Prebiotics are non-digestible food ingredients that selectively stimulate activity of beneficial bacteria in the colon. Prebiotics can be used as a vehicle for improved delivery of nanomedicine. Pectin (Pcn) is a biocompatible polysaccharide that is reputed for its biodegradability, biocompatibility and non-toxicity [125]. Csn is also a biopolymer that has received attention due to its biocompatibility, antimicrobial [126], mucoadhesive and absorption-enhancing properties [127]. Together, they were both used as a prebiotic shell around a PLGA core loaded with sulfasalazine. This design exhibited pH-responsive characteristics for protecting anti-inflammatory drugs in the upper GIT, and also demonstrated a specific colonic delivery property triggered by pectinase which degraded the Pcn/Csn shell, whose enzymatic product revealed notable prebiotic properties [128]. High molecular weight insulin nanoparticles were also shown to improve drug delivery, with no toxicity detected in peripheral blood mononuclear cells at concentrations < 200 μg/mL [129] (Table 2). Other nano-prebiotics such as phthalyl dextran nanoparticles have also shown antimicrobial effects [130] (Figure 5). Altogether, nano-prebiotics offer a promising solution for targeted therapy and microbial modulation in the gut.
6.3.2. Nano-Probiotics
Probiotics are live microorganisms (eg. bacteria, yeast) that offer health benefits to the gut microbiome when consumed. Nanotechnology has contributed to the development of strategies to preserve probiotic viability and functionality in food systems. A recent study developed modified poly(L-glutamic acid) (PG) films incorporating varying levels of poly(L-lysine) (PL), resulting in a dual-function active packaging material, capable of acting as a microbioreactor which enabled continued gamma-aminobutyric acid (GABA) production by the probiotic during the shelf life of the packaged food and also bearing antimicrobial activity, preventing the growth of foodborne pathogenic bacteria [131] (Figure 5) (Table 2).
Nano-probiotics have demonstrated utility in their anticancer properties. Synthesized Ag/Lactobacillus rhamnosus GG nanoparticles (Ag-LNPs) were assessed against CRC cell lines and significantly decreased the viability of these cell lines from 7.8-1000 μg/ml, possibly due to the activation of ROS which led to cell damage and death [132]. Probiotic bacteria Lactobacillus casei was also used to synthesize copper oxide nanoparticles (CuONPs) which exerted cytotoxic effects by suppressing growth, increasing oxidative stress and inducing apoptosis on cancer cells, alongside antimicrobial effects on gram positive and negative bacteria [133] (Table 2). Other nanotechnologies that have shown anti-cancer properties include selenium nanoparticles synthesised by Lactobacillus casei [134,135], dead nano-sized Lactobacillus plantarum (LP) [136] and AuNPs synthesised by novel probiotic Lactobacillus kimchicus [137] (Figure 5). These findings highlight how nano-probiotics can go beyond conventional supplementation into potent bioactive agents for gut health intervention by maintaining microbial viability, enhancing therapeutic properties and even offer anticancer properties in the gut.
6.3.4. Nano-Synbiotics
Synbiotics are combinations of probiotics and prebiotics that work synergistically to improve host health. Nano prebiotics [eg. phthalyl pullulan nanoparticles (PPNs)] has been developed to enhance the antimicrobial action of probiotics (LP), and together, were tested as synbiotics for their therapeutic effect on dysbiosis-induced models. Results demonstrated that antimicrobial activity of the PPN-internalised LP was significantly higher than that of untreated LP or pullulan alone, and groups that underwent synbiotic treatment also had the greatest gain in body weight and longest colons [138]. This suggests weight gain as part of recovery with little to no supplement, and ability to reverse colon shortening, an occurrence due to intestinal inflammation. Additionally, synbiotic treatment also lowered endotoxin and permeability levels, reduced coliform bacteria while boosting lactic acid bacteria, and restored microbiome diversity to a more balanced state [138] (Figure 5) (Table 2).
Nano emulsion systems have also been developed to enhance the bioavailability and maintain the viability of probiotics. One example is the formulation of a synbiotic nanoemulsion incorporating whey protein concentrate, inulin, Gum Arabic, and Enterococcus faecium in the aqueous phase, with coconut oil as the oil phase. The study showed that the droplet size increased up to 500 nm after 60 days of storage, while the viability of the probiotic organism remained promising [139] (Figure 5) (Table 2).
Encapsulation technologies have also been explored to enhance the tolerance and stability of probiotic bacteria. A study developed an oral synbiotic supplement using alginate beads incorporated with varying concentrations of inulin to protect three probiotic strains: Pediococcus acidilactici, Lactobacillus reuteri, and Lactobacillus salivarius. Notably, encapsulation did not affect the antimicrobial or probiotic properties of the strains. Inulin-enhanced beads improved bacterial survival in acidic conditions, while beads containing 5% inulin offered the greatest protection against bile salts [140]. This study highlights the potential of emerging nanotechnologies in improving the delivery and efficacy of probiotics in the gut (Figure 5) (Table 2). These studies collectively point to nano-synbiotics as a powerful therapeutic approach to combat gut dysbiosis through enhanced delivery, viability and functional outcomes.
6.3.5. Nanoparticles with Antioxidant and Anti-Inflammatory Effects (IBD)
Tantalum (Ta), a medical metal element known for its superb physicochemical properties, has been used for the treatment of many diseases, but yet to be explored deeply in IBD. Modification with chondroitin sulfate has resulted in the formation of TACS (Ta2C modified with chondroitin sulfate), evaluated to be a highly targeted therapy nanomedicine for IBD. Its main mechanism of action is mitochondrial protection, oxidative stress elimination, inhibition of macrophage M1 polarisation, among others [141] (Figure 6) (Table 2).
Another therapeutic strategy being explored is a nanomedicine that treats IBD by targeting multiple proinflammatory factors that contribute to its pathogenesis. Specific to this study, researchers reasoned that the neutralisation of cell-free DNA (cfDNA) could modulate the imbalanced immune response in IBD [142]. This is because cfDNA released by damaged cells activated toll like receptor (TLR)-9 mediated proinflammatory signalling in immune cells and contributed to the extent and timespan of inflammation [143]. A nanoparticulate, polyethylenimine-mesoporous organosilica nanoparticles (MON-PEI), was developed via conjugating DNA binding polyethylenimine to antioxidative diselenide-bridged mesoporous organosilica nanoparticles (MON), which bears cfDNA-scavenging, antioxidative and anti-inflammatory properties. It also effectively decreased cfDNA-induced TLR9-MyD88-NF-κB signaling and proinflammatory macrophage activation in treating inflammation, and has an additional benefit of lower dose frequency with better safety profile compared to mesalazine due to its preferential accumulation in diseased areas [142] (Figure 6) (Table 2).
Another approach is capitalising on physiological anti-inflammatory molecules, an example being the gut hormone glucagon like peptide-1 (GLP-1). In order to overcome its limitation of a short half-life due to degradation by enzymes such as dipeptidyl peptidase IV (DPP-4), GLP-1 in sterically stabilised phospholipid micelles (GLP-1-SSM) was developed. GLP-1-SSM treatment was able to lessen colonic inflammation and associated diarrhoea in mouse colitis models via decreasing the expression IL-1β, a pro-inflammatory cytokine, increasing goblet cells and preserving the architecture of the intestinal epithelium [144] (Figure 6) (Table 2). These results show the potential of GLP-1 nanomedicine in acting as IBD treatment.
Mimicking the body’s natural enzymes can also be a way to combat ROS. In this system, the free radical scavenger tempol, which acts as a superoxide dismutase (SOD) mimic, is loaded into a β-cyclodextrin-derived material (OxbCD) that also mimics catalase activity. These components were then assembled into stable nanoparticles with 1,2-distearoyl-sn-glycero-3-phosphoethanolamine (DSPE)-PEG. Upon entering inflamed areas with high levels of ROS, nanoparticles release tempol, reducing both inflammatory cytokines and disease index. It is significant to note that this nanoparticle treatment performed more effectively than free tempol and tempol-loaded PLGA nanoparticles [92] (Figure 6) (Table 2).
6.3.6. Nanomedicine for Microbiome Modulation
- In IBD
Traditional approaches to treating IBD focus mainly on suppressing the immune response via immunosuppressant drugs. However, such a strategy causes systemic side effects and is unable to treat the disrupted intestinal barriers or restore the underlying gut dysbiosis. The development of hyaluronic acid-bilirubin nanomedicine (HABN) aims to improve this by accumulating in the inflamed colon and restoring the epithelium barriers in murine models of acute colitis [145]. HABN was also able to regulate gut microbiomes, increasing their diversity and richness. This is due to hyaluronic acid’s ability to regulate macrophages and induce antimicrobial peptides and CD4 T regulatory cells. Bilirubin has strong ROS scavenging, anti-oxidant, and cytoprotective properties that allow HABN to aggregate to colon inflammation. Mice undergoing HABN treatment were able to achieve full body weight recovery, maintain colon length, reduce colon damage, and increase beneficial bacteria in IBD such as Akkermansia muciniphila, Clostridium and Lactobacillus [145] (Figure 6) (Table 2).
Ag nanoparticles conjugated with a selective wall-binding domain targeting Fusobacteriaceae were found to eliminate these bacteria– known to be overabundant in IBD patients– and thereby reduce intestinal inflammation [146]. Zinc oxide nanoparticles have also been found to reduce the population of Lactobacillus and alter their production of SCFA, a key process that is implicated in the pathogenesis of IBD [146] (Figure 6) (Table 2).
- In CRC
Traditional methods to modulate the gut microbiome have shown promise in enhancing cancer treatment but damage the commensal gut microbiome [147]. The ability to modify the surface of nanoparticles allows them to target specific bacteria, resulting in a controlled killing of cancer-causing microbes with minimal effect on the rest of the gut microbiome [147]. A bacteriophage was found to eliminate a cancer-causing bacterium, F. nucleatum. The bacteriophage was functionalised to nanoparticles and was able to reduce F. nucleatum load with minimal inhibition to other bacteria strains, preserving strains such as Clostridium butycirum, that are useful in suppressing the growth of colon cancer [147] (Figure 7) (Table 2).
Figure 7.
Nanotherapeutics in colorectal cancer include microbiome modulation.
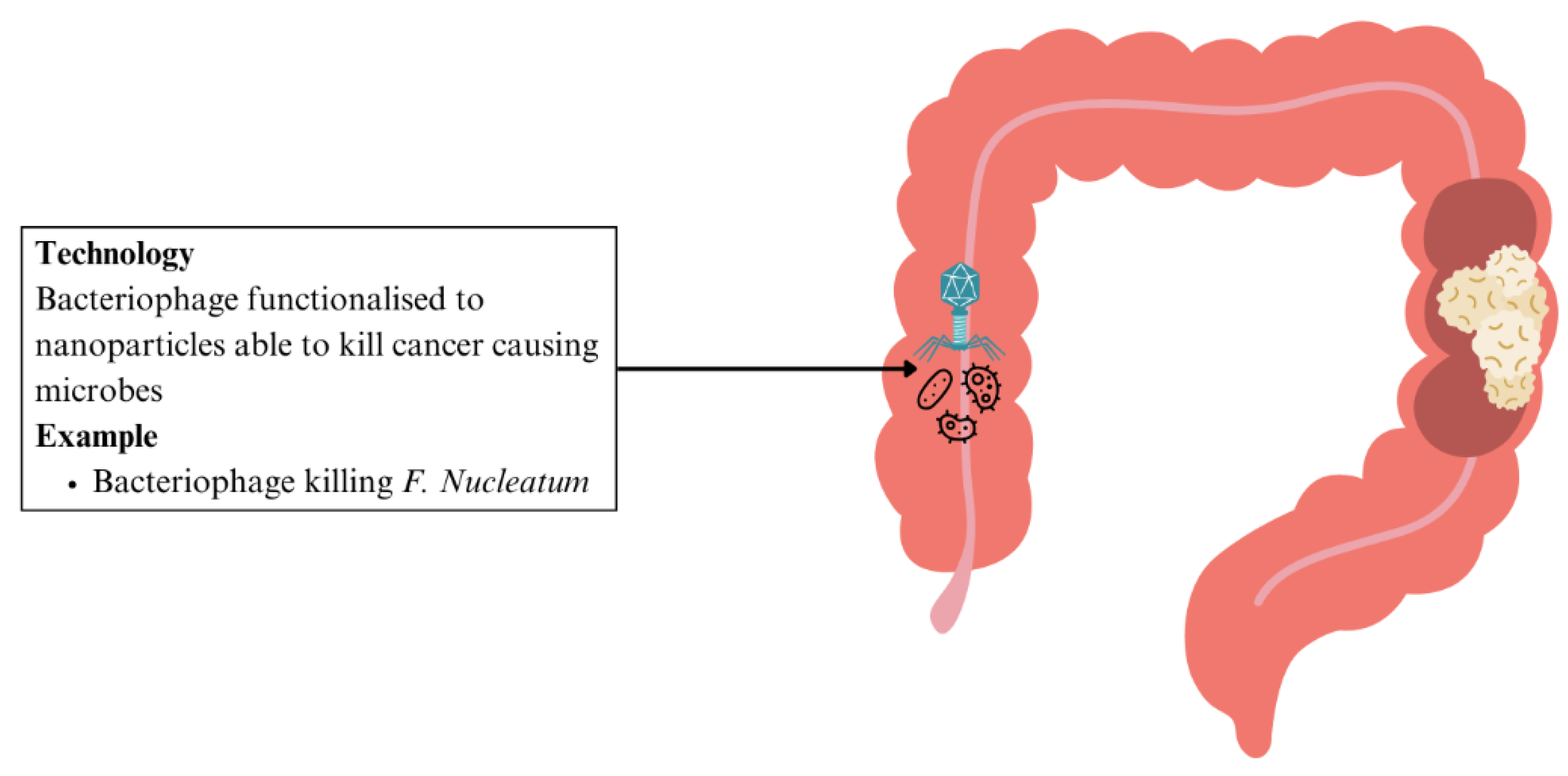

Table 2.
Summary of nanomedicine based therapeutic approaches for IBD and CRC.
| Application | Disease | Nanotechnology Used | Mechanism | Advantages | Stage | Reference |
|---|---|---|---|---|---|---|
| Drug delivery | IBD | B-ATK-T nanoparticle prodrug linked with budesonide | Thioketal bonds that link budesonide with tempol break down in areas where there is excessive ROS | Precise delivery of higher drug dosage to affected areas, less systemic side effects, reduced colon inflammation and weight loss | Preclinical | [92] |
| Csn bound ginger nanocarrier linked with 5-ASA | Drug carrier complex that releases drug in colon based on pH sensitivity | Enhanced site-targeted drug delivery, decreased pill burden and systemic side effects | [94] | |||
| Eudragit polymer microparticles containing prednisolone | Drug carrier complex that releases drug in colon based on pH sensitivity | Higher drug dosage to diseased areas, reduced systemic immunosuppressive effects | [95] | |||
| PPNP loaded with dexamethasone | The inflamed colon's higher esterase levels hydrolyse phenols allowing targeted drug release | Higher drug dosage to diseased areas, reduced systemic immunosuppressive effects | [96] | |||
| CRC | EGF modified PLGA nanoparticles loaded with 5-FU and PFC | Nanoparticles interact directly with cancer cells that express EGFR | More effective tumour suppression, more induced apoptosis for cancer cell death | [100] | ||
| PEG dendrimer nanoparticles with EpCAM aptamer loaded with Celastrol | EpCAM aptamer on nanoparticles target cancer cells | Reduced local and systemic toxicity, improving precision | [101] | |||
| PSiNPs loaded with DOX | Enhanced tumour accumulation and penetration in cancer cells and CSCs | Improved chemotherapy efficacy | [103] | |||
| Hyperthermia treatment | CRC | Csn-coated MNPs with 5-FU | Hyperthermia combined with chemotherapy increased tumour regression | Improved chemotherapy efficacy | [104] | |
| 5-FU loaded onto PLGA encapsulating iron oxide nanoparticles | Increased cytotoxic activity on human colon cancer cells | Decreased dosage required allowing reduced systemic toxicity | [107] | |||
| Magnetic drug targeting |
CRC | Docetaxel encapsulated with oil core polymeric SPIONs | Local magnetic field promotes nanoparticle aggregation in tumour site to deliver chemotherapeutics | Efficient cell-killing effect, precise delivery, decreased systemic side effects | [109] | |
| SPIONs aggregated with mAb198.3 | mAb198.3 is able to stain and recognise CRC samples | Significant reduction in tumour growth | [110] | |||
| MNPs combined with Cetuximab | MNPs can induce oxidative stress, overcoming cancer cells resistant to Cetuximab | Promising treatment to overcome Cetuximab resistant CRC | [111,112] | |||
| PTT |
CRC | AuNPs functionalised with A33 antibody | Act as PTAs that absorb NIR region light to promote cancer cell death, A33 antibody functionalised to target CRC cells, good accumulation in tumours | More targeted PTT with no toxicity to other organs | [117,118,119] | |
| Carbon nanotubes functionalised with nanocomposite POSS-PCU | Functionalisation allows carbon nanotubes to aggregate in CRC tumours, allowing for effective decreases in CRC cell lines | More targeted PTT approach due to functionalising with antibodies | [120,121] | |||
| GNC-Gal@CMaP nanocomposites loaded with galunisertib, surface-functionalized with anti-PD-L1 antibodies | Accumulates in tumour cells selectively, improving PTT efficacy | More targeted PTT approach due to functionalising with antibodies, could eliminate primary tumour while inhibiting metastases | [122] | |||
| Multifunctional endoscope-based interventional system | Fluorescence-based mapping, radio frequency-based ablation and site-specific photo/chemotherapy | Novel minimally invasive treatment strategy for CRC | [123] | |||
| Nanoprebiotics | IBD | Pcn and Csn prebiotic shell surrounding PLGA core loaded with sulfasalazine | pH-responsive prebiotic shell to protect drug from acidic environment for enhanced drug delivery, prebiotic properties | Improved drug concentration in target sites | [128] | |
| High molecular weight insulin nanoparticles | Improved drug delivery | No toxicity detected in peripheries | [129] | |||
| Nanoprobiotics | General dysbiosis | Modified PG films incorporating varying levels of PL | Active packaging material, continues GABA production by probiotic, antimicrobial properties | Preserves probiotic viability and functionality during shelf-life | [131] | |
| CRC | Ag-LNPs | Activation of ROS in CRC cell lines causing cell death | Decreased viability of CRC cell lines | [132] | ||
| CuONPs synthesised with Lactobacillus casei | Suppresses growth of cancer cells, increases oxidative stress and induces apoptosis in cancer cells, antimicrobial effects | Cytotoxic effects on CRC cell lines | [133] | |||
| Nanosynbiotics | IBD | PPNs and LP | Enhances probiotic function, lowers endotoxin and permeability levels, restores microbiome diversity and balance | Enhanced antimicrobial action, decreased dysbiosis | [138] | |
| Nanoemulsion incorporating whey protein concentrate, inulin, Gum Arabic, and Enterococcus faecium, coconut oil | Enhance bioavailability and maintain viability of probiotics | Increased efficacy of probiotics | [139] | |||
| Alginate beads incorporated with inulin to protect probiotic strains Pediococcus acidilactici, Lactobacillus reuteri, and Lactobacillus salivarius | Improved probiotic survival, maintained antimicrobial and probiotic properties | Improved probiotic efficacy in the gut | [140] | |||
| Anti-oxidant and anti-inflammatory nanoparticles |
IBD | TACS | Mitochondrial protection, oxidative stress elimination, inhibition of macrophage M1 polarisation | Reduction of IBD inflammation | [141] | |
| MON-PEI | Has cfDNA-scavenging, antioxidative, anti-inflammatory peroerties, targets multiple proinflammatory factors | Has lower dose frequency, better safety profile than mesalazine | [144] | |||
| GLP-1-SSM | Decreases expression of IL-1β, increases goblet cells and preserves intestinal epithelium architecture | Able to lessen colonic inflammation and associated diarrhoea | [145] | |||
| DSPE-PEG assembled with tempol and OxbCD | Releases tempol in areas with high levels of ROS, reducing inflammatory cytokines and disease index | Enhanced anti-inflammatory activity compared to free tempol and tempol-loaded PLGA nanoparticles | [92] | |||
| Microbiome Modulation |
IBD | HABN | Accumulates in inflamed colon, restore epithelium barriers in colitis, regulates gut microbiome | Directly targets underlying gut dysbiosis and restores disrupted intestinal barriers | [145] | |
| Ag nanoparticles targeting Fusobacteriaceae | Selective wall binding domain to target Fusobacteriaceae directly | Addresses underlying dysbiosis that underlies pathology of IBD | [146] | |||
| Zinc oxide nanoparticles | Reduce population of Lactobacillus and alter production of SCFA | Minimises processes implicated in IBD pathogenesis | [146] | |||
| CRC | Bacteriophage targeting F. nucleatum functionalised to nanoparticles | Eliminates cancer-causing F. nucleatum, while preserving other strains that suppress CRC growth | Controlled killing of cancer-causing microbes with minimal effect on other gut microbiome | [147] |
7. Challenges and Future Directions
While nanotechnology has shown much promise in animal models with its unique and useful physical and chemical properties, current clinical trials and regulations prove to be major obstacles to translate this technology into clinical practice. Some of the major challenges include difficulties with reproducible manufacturing and scale-up, inadequate characterisation tools, instability in vivo, safety concerns and a limited understanding of disease variability and patient selection [148]. Moreover, regulatory agencies such as the US Food and Drug Administration and European Medicines Agency require extensive safety and efficacy evaluations for nanotechnology, yet there is a lack of standardised protocol to determine the safety of nanomaterials [149]. Concerns have also been expressed over the potential long-term toxicity of nanoparticles, due to their tendency to accumulate in organs such as the liver and spleen [149]. Furthermore, the GIT’s complex environment characterised by fluctuating pH, enzymatic activity and mucus layers, have also posed significant barriers for effective drug delivery [149], further complicating the transition of nanomedicine from lab research to clinical application. In essence, more extensive research, clinical trials and standardised protocols are necessary to accelerate the integration of nanomedicine into routine clinical practice (Figure 8).
8. Conclusion
It is evident that gut dysbiosis plays a key role in the pathogenesis of IBD and CRC and should be treated to prevent implications in both the gut and other parts of the body. In this regard, nanomedicine has emerged as a transformative frontier. By enabling targeted drug delivery with controlled release, nanotechnological approaches offer the potential to overcome current limitations of conventional therapies to improve patient outcomes. The ongoing advancements in nanomedicine across many treatment modalities hold much promise for future clinical application.
Acknowledgments
Dr. Tarini Dinesh is currently a junior resident in the Department of Anesthesiology at Tagore Medical College and Hospital, affiliated with The Tamil Nadu Dr. M.G.R. Medical University, Chennai, India.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Abbreviation
| 5-ASA | 5-aminosalicylic acid |
| 5-FU | 5-fluorouracil |
| Ag | silver |
| Ag-LNP | silver/Lactobacillus rhamnosus GG nanoparticle |
| aSlex | anti-Slex |
| AuNP | gold nanoparticle |
| B-ATK-T | Bud-ATK-Tem |
| CD | Crohn’s disease |
| cfDNA | cell-free DNA |
| CRC | colorectal cancer |
| CuONP | copper oxide nanoparticle |
| CSC | cancer stem cell |
| Csn | chitosan |
| DDS | drug delivery system |
| Dex-CeNP | dextran coated cerium oxide nanoparticle |
| DPP-4 | dipeptidyl peptidase IV |
| DSPE | 1,2-distearoyl-sn-glycero-3-phosphoethanolamine |
| EGF | epidermal growth factor |
| EGFR | epidermal growth factor receptor |
| EpCAM | epithelial cell adhesion molecule |
| EPR | enhanced permeability and retention |
| FMT | faecal microbiota transplantation |
| GABA | gamma-aminobutyric acid |
| GC-MS | gas chromatography linked to the mass spectrometry technique |
| GIT | gastrointestinal tract |
| GLP-1 | glucagon like peptide-1 |
| GLP-1-SSM | GLP-1 in sterically stabilised phospholipid micelles |
| GNC | gold nanocages |
| HABN | hyaluronic acid-bilirubin nanomedicine |
| HCFA | hypoxia-activatable and cytoplasmic protein-powered fluorescence cascade amplifier |
| IBD | inflammatory bowel disease |
| IGF | insulin-like growth factor |
| IL | interleukin |
| In2O3 | indium (111) oxide |
| LP | Lactobacillus plantarum |
| MGF | mechano-growth factor |
| MNP | magnetic nanoparticle |
| MON | mesoporous organosilica nanoparticles |
| MON-PEI | polyethylenimine-mesoporous organosilica |
| MRI | magnetic resonance imaging |
| NF-κB | nuclear factor κB |
| NIR | near-infrared |
| OxbCD | β-cyclodextrin-derived material |
| PANAM | poly(amidoamine) |
| Pcn | pectin |
| PD-L1 | programmed cell death ligand-1 |
| PEG | polyethylene glycol |
| PG | poly(L-glutamic acid) |
| PL | poly(L-lysine) |
| PLGA | poly (lactic-co-glycolic acid) |
| PFC | perfluorocarbon |
| POSS-PCU | polyhedral oligomeric silsesquioxane poly (carbonate-urea) urethane |
| PPAR-γ | peroxisome proliferator-activated receptor-gamma |
| PPN | phthalyl pullulan nanoparticle |
| PPNP | polyphenols and polymers self-assembled nanoparticle |
| PSiNP | porous silicon nanoparticle |
| PTA | photothermal agent |
| PTT | photothermal therapy |
| ROS | reactive oxygen species |
| SCFA | short chain fatty acid |
| SPIO | superparamagnetic iron oxide |
| SPION | superparamagnetic iron oxide nanoparticle |
| Ta | Tantalum |
| TACS | Ta2C modified with chondroitin sulfate |
| TGF | transforming growth factor |
| TLR | toll-like receptor |
| TNF-α | tumour necrosis factor-alpha |
| UC | ulcerative colitis |
| VEGF | vascular endothelial growth factor |
| VOC | volatile organic compounds |
References
- Gritz EC, Bhandari V. The human neonatal gut microbiome: a brief review. Front Pediatr. 2015;3:17. [CrossRef]
- Sekirov I, Russell SL, Antunes LC, Finlay BB. Gut microbiota in health and disease. Physiol Rev. 2010;90(3):859–904. [CrossRef]
- Gomaa EZ. Human gut microbiota/microbiome in health and diseases: a review. Antonie Van Leeuwenhoek. 2020;113(12):2019–2040. [CrossRef]
- Badal VD, Vaccariello ED, Murray ER, Yu KE, Knight R, Jeste DV, et al. The gut microbiome, aging, and longevity: a systematic review. Nutrients. 2020;12(12):3759. [CrossRef]
- Su Q, Liu Q. Factors affecting gut microbiome in daily diet. Front Nutr. 2021;8:644138. [CrossRef]
- Kumbhare SV, Patangia DVV, Patil RH, Shouche YS, Patil NP. Factors influencing the gut microbiome in children: from infancy to childhood. J Biosci. 2019;44(2):49.
- Bäckhed F, Fraser CM, Ringel Y, Sanders ME, Sartor RB, Sherman PM, et al. Defining a healthy human gut microbiome: current concepts, future directions, and clinical applications. Cell Host Microbe. 2012;12(5):611–622. [CrossRef]
- Petersson J, Schreiber O, Hansson GC, Gendler SJ, Velcich A, Lundberg JO, et al. Importance and regulation of the colonic mucus barrier in a mouse model of colitis. Am J Physiol Gastrointest Liver Physiol. 2011;300(2):G327–G333. [CrossRef]
- Bäumler AJ, Sperandio V. Interactions between the microbiota and pathogenic bacteria in the gut. Nature. 2016;535(7610):85–93. [CrossRef]
- Cénit MC, Matzaraki V, Tigchelaar EF, Zhernakova A. Rapidly expanding knowledge on the role of the gut microbiome in health and disease. Biochim Biophys Acta. 2014;1842(10):1981–1992. [CrossRef]
- Brusca SB, Abramson SB, Scher JU. Microbiome and mucosal inflammation as extra-articular triggers for rheumatoid arthritis and autoimmunity. Curr Opin Rheumatol. 2014;26(1):101–107. [CrossRef]
- Dahiya D, Nigam PS. Antibiotic-therapy-induced gut dysbiosis affecting gut microbiota-brain axis and cognition: restoration by intake of probiotics and synbiotics. Int J Mol Sci. 2023;24(4):3074. [CrossRef]
- Zmora N, Suez J, Elinav E. You are what you eat: diet, health and the gut microbiota. Nat Rev Gastroenterol Hepatol. 2019;16(1):35–56. [CrossRef]
- Levy M, Kolodziejczyk AA, Thaiss CA, Elinav E. Dysbiosis and the immune system. Nat Rev Immunol. 2017;17(4):219–232. [CrossRef]
- Chandel N, Maile A, Shrivastava S, Verma AK, Thakur V. Establishment and perturbation of human gut microbiome: common trends and variations between Indian and global populations. Gut Microbiome. 2024;5:e8. [CrossRef]
- David LA, Maurice CF, Carmody RN, Gootenberg DB, Button JE, Wolfe BE, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. 2014;505(7484):559–563. [CrossRef]
- Pareek S, Kurakawa T, Das B, Motooka D, Nakaya S, Rongsen-Chandola T, et al. Comparison of Japanese and Indian intestinal microbiota shows diet-dependent interaction between bacteria and fungi. NPJ Biofilms Microbiomes. 2019;5(1):37. [CrossRef]
- Carding S, Verbeke K, Vipond DT, Corfe BM, Owen LJ. Dysbiosis of the gut microbiota in disease. Microb Ecol Health Dis. 2015;26:26191. [CrossRef]
- Kamada N, Seo SU, Chen GY, Núñez G. Role of the gut microbiota in immunity and inflammatory disease. Nat Rev Immunol. 2013;13(5):321–335. [CrossRef]
- Van der Sluis M, De Koning BA, De Bruijn AC, Velcich A, Meijerink JP, Van Goudoever JB, et al. Muc2-deficient mice spontaneously develop colitis, indicating that MUC2 is critical for colonic protection. Gastroenterology. 2006;131(1):117–129. [CrossRef]
- Rohr MW, Narasimhulu CA, Rudeski-Rohr TA, Parthasarathy S. Negative effects of a high-fat diet on intestinal permeability: a review. Adv Nutr. 2020;11(1):77–91. [CrossRef]
- Dethlefsen L, Relman DA. Incomplete recovery and individualized responses of the human distal gut microbiota to repeated antibiotic perturbation. Proc Natl Acad Sci U S A. 2011;108(Suppl 1):4554–4561. [CrossRef]
- Dethlefsen L, Huse S, Sogin ML, Relman DA. The pervasive effects of an antibiotic on the human gut microbiota, as revealed by deep 16S rRNA sequencing. PLoS Biol. 2008;6(11):e280. [CrossRef]
- Pérez-Cobas AE, Gosalbes MJ, Friedrichs A, Knecht H, Artacho A, Eismann K, et al. Gut microbiota disturbance during antibiotic therapy: a multi-omic approach. Gut. 2013;62(11):1591–1601. [CrossRef]
- Maurice CF, Haiser HJ, Turnbaugh PJ. Xenobiotics shape the physiology and gene expression of the active human gut microbiome. Cell. 2013;152(1-2):39–50. [CrossRef]
- Hernández E, Bargiela R, Diez MS, Friedrichs A, Pérez-Cobas AE, Gosalbes MJ, et al. Functional consequences of microbial shifts in the human gastrointestinal tract linked to antibiotic treatment and obesity. Gut Microbes. 2013;4(4):306–315. [CrossRef]
- Francino MP. Antibiotics and the human gut microbiome: dysbioses and accumulation of resistances. Front Microbiol. 2016;6:1543. [CrossRef]
- Fröhlich EE, Farzi A, Mayerhofer R, Reichmann F, Jačan A, Wagner B, et al. Cognitive impairment by antibiotic-induced gut dysbiosis: analysis of gut microbiota-brain communication. Brain Behav Immun. 2016;56:140–155. [CrossRef]
- Belizário JE, Faintuch J. Microbiome and gut dysbiosis. In: Faintuch J, Faintuch S, editors. Precision Medicine for Investigators, Practitioners and Providers. Experientia Supplementum. Cham: Springer; 2018. p. 459–476. [CrossRef]
- Baumgart DC, Carding SR. Inflammatory bowel disease: cause and immunobiology. Lancet. 2007;369(9573):1627–1640. [CrossRef]
- Hansen J, Gulati A, Sartor RB. The role of mucosal immunity and host genetics in defining intestinal commensal bacteria. Curr Opin Gastroenterol. 2010;26(6):564–71. [CrossRef]
- Morgan XC, Tickle TL, Sokol H, Gevers D, Devaney KL, Ward DV, et al. Dysfunction of the intestinal microbiome in inflammatory bowel disease and treatment. Genome Biol. 2012;13(9):R79. [CrossRef]
- Ogilvie LA, Jones BV. Dysbiosis modulates capacity for bile acid modification in the gut microbiomes of patients with inflammatory bowel disease: a mechanism and marker of disease? Gut. 2012;61(11):1642–3. [CrossRef]
- Duboc H, Rajca S, Rainteau D, Benarous D, Maubert MA, Quervain E, et al. Connecting dysbiosis, bile-acid dysmetabolism and gut inflammation in inflammatory bowel diseases. Gut. 2013;62(4):531–9. [CrossRef]
- Smith PM, Howitt MR, Panikov N, Michaud M, Gallini CA, Bohlooly-Y M, et al. The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science. 2013;341(6145):569–73. [CrossRef]
- Ahn J, Sinha R, Pei Z, Dominianni C, Wu J, Shi J, et al. Human gut microbiome and risk for colorectal cancer. J Natl Cancer Inst. 2013;105(24):1907–11. [CrossRef]
- Yu YN, Fang JY. Gut Microbiota and Colorectal Cancer. Gastrointest Tumors. 2015;2(1):26–32. [CrossRef]
- Chen CC, Lin WC, Kong MS, Shi HN, Walker WA, Lin CY, et al. Oral inoculation of probiotics Lactobacillus acidophilus NCFM suppresses tumour growth both in segmental orthotopic colon cancer and extra-intestinal tissue. Br J Nutr. 2012;107(11):1623–34. [CrossRef]
- Gagnière J, Raisch J, Veziant J, Barnich N, Bonnet R, Buc E, et al. Gut microbiota imbalance and colorectal cancer. World J Gastroenterol. 2016;22(2):501–18. [CrossRef]
- Belcheva A, Irrazabal T, Martin A. Gut microbial metabolism and colon cancer: can manipulations of the microbiota be useful in the management of gastrointestinal health? BioEssays. 2015;37(4):403–12. [CrossRef]
- Krautkramer KA, Kreznar JH, Romano KA, Vivas EI, Barrett-Wilt GA, Rabaglia ME, et al. Diet-Microbiota Interactions Mediate Global Epigenetic Programming in Multiple Host Tissues. Mol Cell. 2016;64(5):982–92. [CrossRef]
- Belcheva A, Irrazabal T, Robertson SJ, Streutker C, Maughan H, Rubino S, et al. Gut microbial metabolism drives transformation of MSH2-deficient colon epithelial cells. Cell. 2014;158(2):288–99. [CrossRef]
- Raskov H, Burcharth J, Pommergaard HC. Linking Gut Microbiota to Colorectal Cancer. J Cancer. 2017;8(17):3378–95. [CrossRef]
- Sears CL, Garrett WS. Microbes, microbiota, and colon cancer. Cell Host Microbe. 2014;15(3):317–28. [CrossRef]
- Damião AOMC, de Azevedo MFC, Carlos AS, Wada MY, Silva TVM, Feitosa FC. Conventional therapy for moderate to severe inflammatory bowel disease: A systematic literature review. World J Gastroenterol. 2019;25(9):1142–57. [CrossRef]
- Pithadia AB, Jain S. Treatment of inflammatory bowel disease (IBD). Pharmacol Rep. 2011;63(3):629–42. [CrossRef]
- Hanauer SB, Baert F. Medical therapy of inflammatory bowel disease. Med Clin North Am. 1994;78(6):1413–26. [CrossRef]
- Hvas CL, Bendix M, Dige A, Dahlerup JF, Agnholt J. Current, experimental, and future treatments in inflammatory bowel disease: a clinical review. Immunopharmacol Immunotoxicol. 2018;40(6):446–60. [CrossRef]
- Desreumaux P, Ghosh S. Review article: mode of action and delivery of 5-aminosalicylic acid - new evidence. Aliment Pharmacol Ther. 2006;24 Suppl 1:2–9. [CrossRef]
- Loftus EV Jr, Kane SV, Bjorkman D. Systematic review: short-term adverse effects of 5-aminosalicylic acid agents in the treatment of ulcerative colitis. Aliment Pharmacol Ther. 2004;19(2):179–89. [CrossRef]
- Troncone E, Monteleone G. The safety of non-biological treatments in Ulcerative Colitis. Expert Opin Drug Saf. 2017;16(7):779–89. [CrossRef]
- Toruner M, Loftus EV Jr, Harmsen WS, Zinsmeister AR, Orenstein R, Sandborn WJ, Colombel JF, Egan LJ. Risk factors for opportunistic infections in patients with inflammatory bowel disease. Gastroenterology. 2008;134(4):929–36. [CrossRef]
- Pearson DC, May GR, Fick GH, Sutherland LR. Azathioprine and 6-mercaptopurine in Crohn disease. A meta-analysis. Ann Intern Med. 1995;123(2):132–42. [CrossRef]
- Van den Brande JM, Braat H, van den Brink GR, Versteeg HH, Bauer CA, Hoedemaeker I, van Montfrans C, Hommes DW, Peppelenbosch MP, van Deventer SJ. Infliximab but not etanercept induces apoptosis in lamina propria T-lymphocytes from patients with Crohn's disease. Gastroenterology. 2003;124(7):1774–85. [CrossRef]
- Lügering A, Schmidt M, Lügering N, Pauels HG, Domschke W, Kucharzik T. Infliximab induces apoptosis in monocytes from patients with chronic active Crohn's disease by using a caspase-dependent pathway. Gastroenterology. 2001;121(5):1145–57. [CrossRef]
- Di Sabatino A, Pender SL, Jackson CL, Prothero JD, Gordon JN, Picariello L, Rovedatti L, Docena G, Monteleone G, Rampton DS, Tonelli F, Corazza GR, MacDonald TT. Functional modulation of Crohn's disease myofibroblasts by anti-tumor necrosis factor antibodies. Gastroenterology. 2007;133(1):137–49. [CrossRef]
- Arijs I, De Hertogh G, Machiels K, Van Steen K, Lemaire K, Schraenen A, Van Lommel L, Quintens R, Van Assche G, Vermeire S, Schuit F, Rutgeerts P. Mucosal gene expression of cell adhesion molecules, chemokines, and chemokine receptors in patients with inflammatory bowel disease before and after infliximab treatment. Am J Gastroenterol. 2011;106(4):748–61. [CrossRef]
- Vos AC, Wildenberg ME, Arijs I, Duijvestein M, Verhaar AP, de Hertogh G, Vermeire S, Rutgeerts P, van den Brink GR, Hommes DW. Regulatory macrophages induced by infliximab are involved in healing in vivo and in vitro. Inflamm Bowel Dis. 2012;18(3):401–8. [CrossRef]
- Ainsworth MA, Bendtzen K, Brynskov J. Tumor necrosis factor-alpha binding capacity and anti-infliximab antibodies measured by fluid-phase radioimmunoassays as predictors of clinical efficacy of infliximab in Crohn's disease. Am J Gastroenterol. 2008;103(4):944–8. [CrossRef]
- Nyboe Andersen N, Pasternak B, Friis-Møller N, Andersson M, Jess T. Association between tumour necrosis factor-α inhibitors and risk of serious infections in people with inflammatory bowel disease: nationwide Danish cohort study. BMJ. 2015;350:h2809. [CrossRef]
- Feagan BG, Sandborn WJ, Gasink C, Jacobstein D, Lang Y, Friedman JR, et al.; UNITI–IM-UNITI Study Group. Ustekinumab as induction and maintenance therapy for Crohn's disease. N Engl J Med. 2016;375(20):1946–60. [CrossRef]
- Sands BE, Sandborn WJ, Panaccione R, O'Brien CD, Zhang H, Johanns J, et al.; UNIFI Study Group. Ustekinumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2019;381(13):1201–14. [CrossRef]
- Wang JW, Kuo CH, Kuo FC, Wang YK, Hsu WH, Yu FJ, et al. Fecal microbiota transplantation: Review and update. J Formos Med Assoc. 2019;118 Suppl 1:S23–31. [CrossRef]
- Na SY, Moon W. Perspectives on current and novel treatments for inflammatory bowel disease. Gut Liver. 2019;13(6):604–16. [CrossRef]
- Shinji S, Yamada T, Matsuda A, Sonoda H, Ohta R, Iwai T, et al. Recent advances in the treatment of colorectal cancer: A review. J Nippon Med Sch. 2022;89(3):246–54. [CrossRef]
- Poston GJ, Figueras J, Giuliante F, Nuzzo G, Sobrero AF, Gigot JF, et al. Urgent need for a new staging system in advanced colorectal cancer. J Clin Oncol. 2008;26(29):4828–33. [CrossRef]
- Viswanath B, Kim S, Lee K. Recent insights into nanotechnology development for detection and treatment of colorectal cancer. Int J Nanomedicine. 2016;11:2491–504. [CrossRef]
- Yau TO. Precision treatment in colorectal cancer: Now and the future. JGH Open. 2019;3(5):361–9. [CrossRef]
- Verma M. Personalized medicine and cancer. J Pers Med. 2012;2(1):1–14.
- Liz-Marzán LM, Nel AE, Brinker CJ, Chan WC, Chen C, Chen X, et al. What do we mean when we say nanomedicine? ACS Nano. 2022;16(9):13257–9.
- Bansal M, Kumar A, Malinee M, Sharma TK. Nanomedicine: Diagnosis, treatment, and potential prospects. Nanoscience in Medicine. 2020;1:297–331.
- Riehemann K, Schneider SW, Luger TA, Godin B, Ferrari M, Fuchs H. Nanomedicine—challenge and perspectives. Angew Chem Int Ed Engl. 2009;48(5):872–97. [CrossRef]
- Brydges CR, Fiehn O, Mayberg HS, Schreiber H, Dehkordi SM, Bhattacharyya S, et al.; Mood Disorders Precision Medicine Consortium. Indoxyl sulfate, a gut microbiome-derived uremic toxin, is associated with psychic anxiety and its functional magnetic resonance imaging-based neurologic signature. Sci Rep. 2021;11(1):21011. [CrossRef]
- Takayama K, Maehara S, Tabuchi N, Okamura N. Anthraquinone-containing compound in rhubarb prevents indole production via functional changes in gut microbiota. J Nat Med. 2021;75(1):116–28. [CrossRef]
- Gao J, Xu K, Liu H, Liu G, Bai M, Peng C, et al. Impact of the gut microbiota on intestinal immunity mediated by tryptophan metabolism. Front Cell Infect Microbiol. 2018;8:13. [CrossRef]
- Yang CY, Tarng DC. Diet, gut microbiome and indoxyl sulphate in chronic kidney disease patients. Nephrology (Carlton). 2018;23 Suppl 4:16–20. [CrossRef]
- Wang X, Shi S, Zhang F, Li S, Tan J, Su B, et al. Application of a nanotip array-based electrochemical sensing platform for detection of indole derivatives as key indicators of gut microbiota health. Alexandria Eng J. 2023;85:294–9.
- Reiter S, Dunkel A, Metwaly A, Panes J, Salas A, Haller D, et al. Development of a highly sensitive ultra-high-performance liquid chromatography coupled to electrospray ionization tandem mass spectrometry quantitation method for fecal bile acids and application on Crohn's disease studies. J Agric Food Chem. 2021;69(17):5238–51. [CrossRef]
- Chen L, Sun X, Khalsa AS, Bailey MT, Kelleher K, Spees C, et al. Accurate and reliable quantitation of short chain fatty acids from human feces by ultra high-performance liquid chromatography-high resolution mass spectrometry (UPLC-HRMS). J Pharm Biomed Anal. 2021;200:114066. [CrossRef]
- Salihović S, Dickens AM, Schoultz I, Fart F, Sinisalu L, Lindeman T, et al. Simultaneous determination of perfluoroalkyl substances and bile acids in human serum using ultra-high-performance liquid chromatography-tandem mass spectrometry. Anal Bioanal Chem. 2020;412(10):2251–9. [CrossRef]
- Luo Z, Lv T, Zhu K, Li Y, Wang L, Gooding JJ, et al. Paper-based ratiometric fluorescence analytical devices towards point-of-care testing of human serum albumin. Angew Chem Int Ed Engl. 2020;59(8):3131–6. [CrossRef]
- Peng G, Hakim M, Broza YY, Billan S, Abdah-Bortnyak R, Kuten A, et al. Detection of lung, breast, colorectal, and prostate cancers from exhaled breath using a single array of nanosensors. Br J Cancer. 2010;103(4):542–51. [CrossRef]
- Wu Y, Briley-Saebo K, Xie J, Zhang R, Wang Z, He C, et al. Inflammatory bowel disease: MR- and SPECT/CT-based macrophage imaging for monitoring and evaluating disease activity in experimental mouse model—pilot study. Radiology. 2014;271(2):400–7. [CrossRef]
- Naha PC, Hsu JC, Kim J, Shah S, Bouché M, Si-Mohamed S, et al. Dextran-coated cerium oxide nanoparticles: A computed tomography contrast agent for imaging the gastrointestinal tract and inflammatory bowel disease. ACS Nano. 2020;14(8):10187–97. [CrossRef]
- Zhou Y, Yang S, Guo J, Dong H, Yin K, Huang WT, et al. In vivo imaging of hypoxia associated with inflammatory bowel disease by a cytoplasmic protein-powered fluorescence cascade amplifier. Anal Chem. 2020;92(8):5787–94. [CrossRef]
- Alagaratnam S, Yang SY, Loizidou M, Fuller B, Ramesh B. Mechano-growth factor expression in colorectal cancer investigated with fluorescent gold nanoparticles. Anticancer Res. 2019;39(4):1705–10. [CrossRef]
- Perumal K, Ahmad S, Mohd-Zahid MH, Wan Hanaffi WN, ZA I, Six JL, et al. Nanoparticles and gut microbiota in colorectal cancer. Front Nanotechnol. 2021;3:681760.
- Gil HM, Price TW, Chelani K, Bouillard JG, Calaminus SDJ, Stasiuk GJ. NIR-quantum dots in biomedical imaging and their future. iScience. 2021;24(3):102189. [CrossRef]
- Xie J, Wang J, Chen H, Shen W, Sinko PJ, Dong H, et al. Multivalent conjugation of antibody to dendrimers for the enhanced capture and regulation on colon cancer cells. Sci Rep. 2015;5:9445. [CrossRef]
- Chandrakala V, Aruna V, Angajala G. Review on metal nanoparticles as nanocarriers: current challenges and perspectives in drug delivery systems. Emerg Mater. 2022;5(6):1593–615. [CrossRef]
- Sedghi S, Fields JZ, Klamut M, Urban G, Durkin M, Winship D, et al. Increased production of luminol enhanced chemiluminescence by the inflamed colonic mucosa in patients with ulcerative colitis. Gut. 1993;34(9):1191–7. [CrossRef]
- Abed OA, Attlassy Y, Xu J, Han K, Moon JJ. Emerging Nanotechnologies and Microbiome Engineering for the Treatment of Inflammatory Bowel Disease. Mol Pharm. 2022;19(12):4393–410. [CrossRef]
- Sonu I, Lin MV, Blonski W, Lichtenstein GR. Clinical pharmacology of 5-ASA compounds in inflammatory bowel disease. Gastroenterol Clin North Am. 2010;39(3):559–99. [CrossRef]
- Markam R, Bajpai AK. Functionalization of ginger derived nanoparticles with chitosan to design drug delivery system for controlled release of 5-amino salicylic acid (5-ASA) in treatment of inflammatory bowel diseases: An in vitro study. React Funct Polym. 2020;149:104520.
- Shams T, Illangakoon UE, Parhizkar M, Harker AH, Edirisinghe S, Orlu M, Edirisinghe M. Electrosprayed microparticles for intestinal delivery of prednisolone. J R Soc Interface. 2018;15(145):20180491. [CrossRef]
- Wang X, Yan JJ, Wang L, Pan D, Yang R, Xu Y, et al. Rational design of polyphenol-poloxamer nanovesicles for targeting inflammatory bowel disease therapy. Chem Mater. 2018;30(12):4073–80.
- Linton SS, Sherwood SG, Drews KC, Kester M. Targeting cancer cells in the tumor microenvironment: opportunities and challenges in combinatorial nanomedicine. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2016;8(2):208–22. [CrossRef]
- Liu J, Huang Y, Kumar A, Tan A, Jin S, Mozhi A, Liang XJ. pH-sensitive nano-systems for drug delivery in cancer therapy. Biotechnol Adv. 2014;32(4):693–710. [CrossRef]
- Tian Z, Wu X, Peng L, Yu N, Gou G, Zuo W, Yang J. pH-responsive bufadienolides nanocrystals decorated by chitosan quaternary ammonium salt for treating colon cancer. Int J Biol Macromol. 2023;242(Pt 2):124819. [CrossRef]
- Wu P, Zhou Q, Zhu H, Zhuang Y, Bao J. Enhanced antitumor efficacy in colon cancer using EGF functionalized PLGA nanoparticles loaded with 5-Fluorouracil and perfluorocarbon. BMC Cancer. 2020;20(1):354. [CrossRef]
- Ge P, Niu B, Wu Y, Xu W, Li M, Sun H, et al. Enhanced cancer therapy of celastrol in vitro and in vivo by smart dendrimers delivery with specificity and biosafety. Chem Eng J. 2020;383:123228.
- Nassar D, Blanpain C. Cancer Stem Cells: Basic Concepts and Therapeutic Implications. Annu Rev Pathol. 2016;11:47–76. [CrossRef]
- Yong T, Zhang X, Bie N, Zhang H, Zhang X, Li F, et al. Tumor exosome-based nanoparticles are efficient drug carriers for chemotherapy. Nat Commun. 2019;10(1):3838. [CrossRef]
- Dabaghi M, Rasa SMM, Cirri E, Ori A, Neri F, Quaas R, Hilger I. Iron Oxide Nanoparticles Carrying 5-Fluorouracil in Combination with Magnetic Hyperthermia Induce Thrombogenic Collagen Fibers, Cellular Stress, and Immune Responses in Heterotopic Human Colon Cancer in Mice. Pharmaceutics. 2021;13(10):1625. [CrossRef]
- Hildebrandt B, Wust P, Ahlers O, Dieing A, Sreenivasa G, Kerner T, et al. The cellular and molecular basis of hyperthermia. Crit Rev Oncol Hematol. 2002;43(1):33–56. [CrossRef]
- Mini E, Dombrowski J, Moroson BA, Bertino JR. Cytotoxic effects of hyperthermia, 5-fluorouracil and their combination on a human leukemia T-lymphoblast cell line, CCRF-CEM. Eur J Cancer Clin Oncol. 1986;22(8):927–34. [CrossRef]
- Eynali S, Khoei S, Khoee S, Esmaelbeygi E. Evaluation of the cytotoxic effects of hyperthermia and 5-fluorouracil-loaded magnetic nanoparticles on human colon cancer cell line HT-29. Int J Hyperthermia. 2017;33(3):327–35. [CrossRef]
- Wang N, Chen L, Huang W, Gao Z, Jin M. Current Advances of Nanomaterial-Based Oral Drug Delivery for Colorectal Cancer Treatment. Nanomaterials (Basel). 2024;14(7):557. [CrossRef]
- Al-Jamal KT, Bai J, Wang JT, Protti A, Southern P, Bogart L, et al. Magnetic Drug Targeting: Preclinical in Vivo Studies, Mathematical Modeling, and Extrapolation to Humans. Nano Lett. 2016;16(9):5652–60. [CrossRef]
- Grifantini R, Taranta M, Gherardini L, Naldi I, Parri M, Grandi A, et al. Magnetically driven drug delivery systems improving targeted immunotherapy for colon-rectal cancer. J Control Release. 2018;280:76–86. [CrossRef]
- Yousefi M, Farzi-Khajeh H, Akbarzadeh-Khiavi M, Safary A, Adibkia K. Improved Biological Impacts of anti-EGFR Monoclonal Antibody in KRAS-Mutant Colorectal Cancer Cells by Silica-Coated Magnetic Nanoparticle Conjugation. Pharm Sci. 2024;30(4):444–55.
- Ahamed M, Alhadlaq HA, Alam J, Khan MA, Ali D, Alarafi S. Iron oxide nanoparticle-induced oxidative stress and genotoxicity in human skin epithelial and lung epithelial cell lines. Curr Pharm Des. 2013;19(37):6681–90. [CrossRef]
- Zhao L, Zhang X, Wang X, Guan X, Zhang W, Ma J. Recent advances in selective photothermal therapy of tumor. J Nanobiotechnol. 2021;19(1):335. [CrossRef]
- Liu Y, Bhattarai P, Dai Z, Chen X. Photothermal therapy and photoacoustic imaging via nanotheranostics in fighting cancer. Chem Soc Rev. 2019;48(7):2053–108. [CrossRef]
- Wei W, Zhang X, Zhang S, Wei G, Su Z. Biomedical and bioactive engineered nanomaterials for targeted tumor photothermal therapy: A review. Mater Sci Eng C Mater Biol Appl. 2019;104:109891. [CrossRef]
- Khot MI, Andrew H, Svavarsdottir HS, Armstrong G, Quyn AJ, Jayne DG. A Review on the Scope of Photothermal Therapy-Based Nanomedicines in Preclinical Models of Colorectal Cancer. Clin Colorectal Cancer. 2019;18(2):e200–9. [CrossRef]
- O’Neal DP, Hirsch LR, Halas NJ, Payne JD, West JL. Photo-thermal tumor ablation in mice using near infrared-absorbing nanoparticles. Cancer Lett. 2004;209(2):171–6. [CrossRef]
- Kirui DK, Krishnan S, Strickland AD, Batt CA. PAA-derived gold nanorods for cellular targeting and photothermal therapy. Macromol Biosci. 2011;11(6):779–88. [CrossRef]
- Goodrich GP, Bao L, Gill-Sharp K, Sang KL, Wang J, Payne JD. Photothermal therapy in a murine colon cancer model using near-infrared absorbing gold nanorods. J Biomed Opt. 2010;15(1):018001. [CrossRef]
- Tan A, Madani SY, Rajadas J, Pastorin G, Seifalian AM. Synergistic photothermal ablative effects of functionalizing carbon nanotubes with a POSS-PCU nanocomposite polymer. J Nanobiotechnol. 2012;10:34. [CrossRef]
- Graham EG, MacNeill CM, Levi-Polyachenko NH. Quantifying folic acid-functionalized multi-walled carbon nanotubes bound to colorectal cancer cells for improved photothermal ablation. J Nanopart Res. 2013;15:1–12.
- Wang S, Song Y, Cao K, Zhang L, Fang X, Chen F, Feng S, Yan F. Photothermal therapy mediated by gold nanocages composed of anti-PDL1 and galunisertib for improved synergistic immunotherapy in colorectal cancer. Acta Biomater. 2021;134:621–32. [CrossRef]
- Lee H, Lee Y, Song C, Cho HR, Ghaffari R, Choi TK, et al. An endoscope with integrated transparent bioelectronics and theranostic nanoparticles for colon cancer treatment. Nat Commun. 2015;6:10059. [CrossRef]
- Durazzo A, Nazhand A, Lucarini M, Atanasov AG, Souto EB, Novellino E, Capasso R, Santini A. An Updated Overview on Nanonutraceuticals: Focus on Nanoprebiotics and Nanoprobiotics. Int J Mol Sci. 2020;21(7):2285. [CrossRef]
- Kedir WM, Deresa EM, Diriba TF. Pharmaceutical and drug delivery applications of pectin and its modified nanocomposites. Heliyon. 2022;8(9):e10654. [CrossRef]
- Ładniak A, Jurak M, Palusińska-Szysz M, Wiącek AE. The Influence of Polysaccharides/TiO2 on the Model Membranes of Dipalmitoylphosphatidylglycerol and Bacterial Lipids. Molecules. 2022;27(2):343. [CrossRef]
- Jafernik K, Ładniak A, Blicharska E, Czarnek K, Ekiert H, Wiącek AE, Szopa A. Chitosan-Based Nanoparticles as Effective Drug Delivery Systems-A review. Molecules. 2023;28(4):1963. [CrossRef]
- Li H, Cheng Y, Cui L, Yang Z, Wang J, Zhang Z, et al. Combining Gut Microbiota Modulation and Enzymatic-Triggered Colonic Delivery by Prebiotic Nanoparticles Improves Mouse Colitis Therapy. Biomater Res. 2024;28:0062. [CrossRef]
- Jiménez-Sánchez M, Pérez-Morales R, Goycoolea FM, Mueller M, Praznik W, Loeppert R, et al. Self-assembled high molecular weight inulin nanoparticles: Enzymatic synthesis, physicochemical and biological properties. Carbohydr Polym. 2019;215:160–9. [CrossRef]
- Kim WS, Han GG, Hong L, Kang SK, Shokouhimehr M, Choi YJ, Cho CS. Novel production of natural bacteriocin via internalization of dextran nanoparticles into probiotics. Biomaterials. 2019;218:119360. [CrossRef]
- Karimi M, Yazdi FT, Mortazavi SA, Shahabi-Ghahfarrokhi I, Chamani J. Development of active antimicrobial poly (l-glutamic) acid-poly (l-lysine) packaging material to protect probiotic bacterium. Polym Test. 2020;83:106338.
- Aziz Mousavi SMA, Mirhosseini SA, Rastegar Shariat Panahi M, Mahmoodzadeh Hosseini H. Characterization of Biosynthesized Silver Nanoparticles Using Lactobacillus rhamnosus GG and its In Vitro Assessment Against Colorectal Cancer Cells. Probiotics Antimicrob Proteins. 2020;12(2):740–6. [CrossRef]
- Kouhkan M, Ahangar P, Babaganjeh LA, Allahyari-Devin M. Biosynthesis of copper oxide nanoparticles using Lactobacillus casei subsp. casei and its anticancer and antibacterial activities. Curr Nanoscience. 2020;16(1):101–11.
- Xu C, Qiao L, Guo Y, Ma L, Cheng Y. Preparation, characteristics and antioxidant activity of polysaccharides and proteins-capped selenium nanoparticles synthesized by Lactobacillus casei ATCC 393. Carbohydr Polym. 2018;195:576–85. [CrossRef]
- Xu C, Guo Y, Qiao L, Ma L, Cheng Y, Roman A. Biogenic Synthesis of Novel Functionalized Selenium Nanoparticles by Lactobacillus casei ATCC 393 and Its Protective Effects on Intestinal Barrier Dysfunction Caused by Enterotoxigenic Escherichia coli K88. Front Microbiol. 2018;9:1129. [CrossRef]
- Lee HA, Kim H, Lee KW, Park KY. Dead Nano-Sized Lactobacillus plantarum Inhibits Azoxymethane/Dextran Sulfate Sodium-Induced Colon Cancer in Balb/c Mice. J Med Food. 2015;18(12):1400–5. [CrossRef]
- Markus J, Mathiyalagan R, Kim YJ, Abbai R, Singh P, Ahn S, et al. Intracellular synthesis of gold nanoparticles with antioxidant activity by probiotic Lactobacillus kimchicus DCY51T isolated from Korean kimchi. Enzyme Microb Technol. 2016;95:85–93. [CrossRef]
- Hong L, Lee SM, Kim WS, Choi YJ, Oh SH, Li YL, et al. Synbiotics Containing Nanoprebiotics: A Novel Therapeutic Strategy to Restore Gut Dysbiosis. Front Microbiol. 2021;12:715241. [CrossRef]
- Krithika B, Preetha R. Formulation of protein based inulin incorporated synbiotic nanoemulsion for enhanced stability of probiotic. Mater Res Express. 2019;6(11):114003.
- Atia A, Gomaa A, Fliss I, Beyssac E, Garrait G, Subirade M. A prebiotic matrix for encapsulation of probiotics: physicochemical and microbiological study. J Microencapsul. 2016;33(1):89–101. [CrossRef]
- Song X, Huang Q, Yang Y, Ma L, Liu W, Ou C, Chen Q, Zhao T, Xiao Z, Wang M, Jiang Y, Yang Y, Zhang J, Nan Y, Wu W, Ai K. Efficient therapy of inflammatory bowel disease (IBD) with highly specific and durable targeted Ta2C modified with chondroitin sulfate (TACS). Adv Mater. 2023;35(36):e2301585. [CrossRef]
- Shi C, Dawulieti J, Shi F, Yang C, Qin Q, Shi T, Wang L, Hu H, Sun M, Ren L, Chen F, Zhao Y, Liu F, Li M, Mu L, Liu D, Shao D, Leong KW, She J. A nanoparticulate dual scavenger for targeted therapy of inflammatory bowel disease. Sci Adv. 2022;8(4):eabj2372. [CrossRef]
- Latz E, Schoenemeyer A, Visintin A, Fitzgerald KA, Monks BG, Knetter CF, Lien E, Nilsen NJ, Espevik T, Golenbock DT. TLR9 signals after translocating from the ER to CpG DNA in the lysosome. Nat Immunol. 2004;5(2):190–8. [CrossRef]
- Anbazhagan AN, Thaqi M, Priyamvada S, Jayawardena D, Kumar A, Gujral T, Chatterjee I, Mugarza E, Saksena S, Onyuksel H, Dudeja PK. GLP-1 nanomedicine alleviates gut inflammation. Nanomedicine. 2017;13(2):659–65. [CrossRef]
- Lee Y, Sugihara K, Gillilland MG 3rd, Jon S, Kamada N, Moon JJ. Hyaluronic acid-bilirubin nanomedicine for targeted modulation of dysregulated intestinal barrier, microbiome and immune responses in colitis. Nat Mater. 2020;19(1):118–26. [CrossRef]
- Long D, Merlin D. Micro- and nanotechnological delivery platforms for treatment of dysbiosis-related inflammatory bowel disease. Nanomedicine (Lond). 2021;16(20):1741–5. [CrossRef]
- Song W, Anselmo AC, Huang L. Nanotechnology intervention of the microbiome for cancer therapy. Nat Nanotechnol. 2019;14(12):1093–103. [CrossRef]
- Agrahari V, Agrahari V. Facilitating the translation of nanomedicines to a clinical product: challenges and opportunities. Drug Discov Today. 2018;23(5):974–91. [CrossRef]
- Zheng G, Zhang B, Yu H, et al. Therapeutic applications and potential biological barriers of nano-delivery systems in common gastrointestinal disorders: a comprehensive review. Adv Compos Hybrid Mater. 2025;8:227. [CrossRef]
Figure 1.
In healthy individuals, a balanced microbiota prevents pathogen colonisation and has antimicrobial and immunomodulation properties. Conversely, gut dysbiosis contributes to the pathogenesis of inflammatory bowel disease and colorectal cancer. In dysbiosis, pathogenic shifts lead to alterations of physiologic processes, increased expression of harmful genes and decreased microbiome diversity. Abbreviations: IBD: inflammatory bowel disease; SCFA: short chain fatty acid; CRC: colorectal cancer.
Figure 1.
In healthy individuals, a balanced microbiota prevents pathogen colonisation and has antimicrobial and immunomodulation properties. Conversely, gut dysbiosis contributes to the pathogenesis of inflammatory bowel disease and colorectal cancer. In dysbiosis, pathogenic shifts lead to alterations of physiologic processes, increased expression of harmful genes and decreased microbiome diversity. Abbreviations: IBD: inflammatory bowel disease; SCFA: short chain fatty acid; CRC: colorectal cancer.
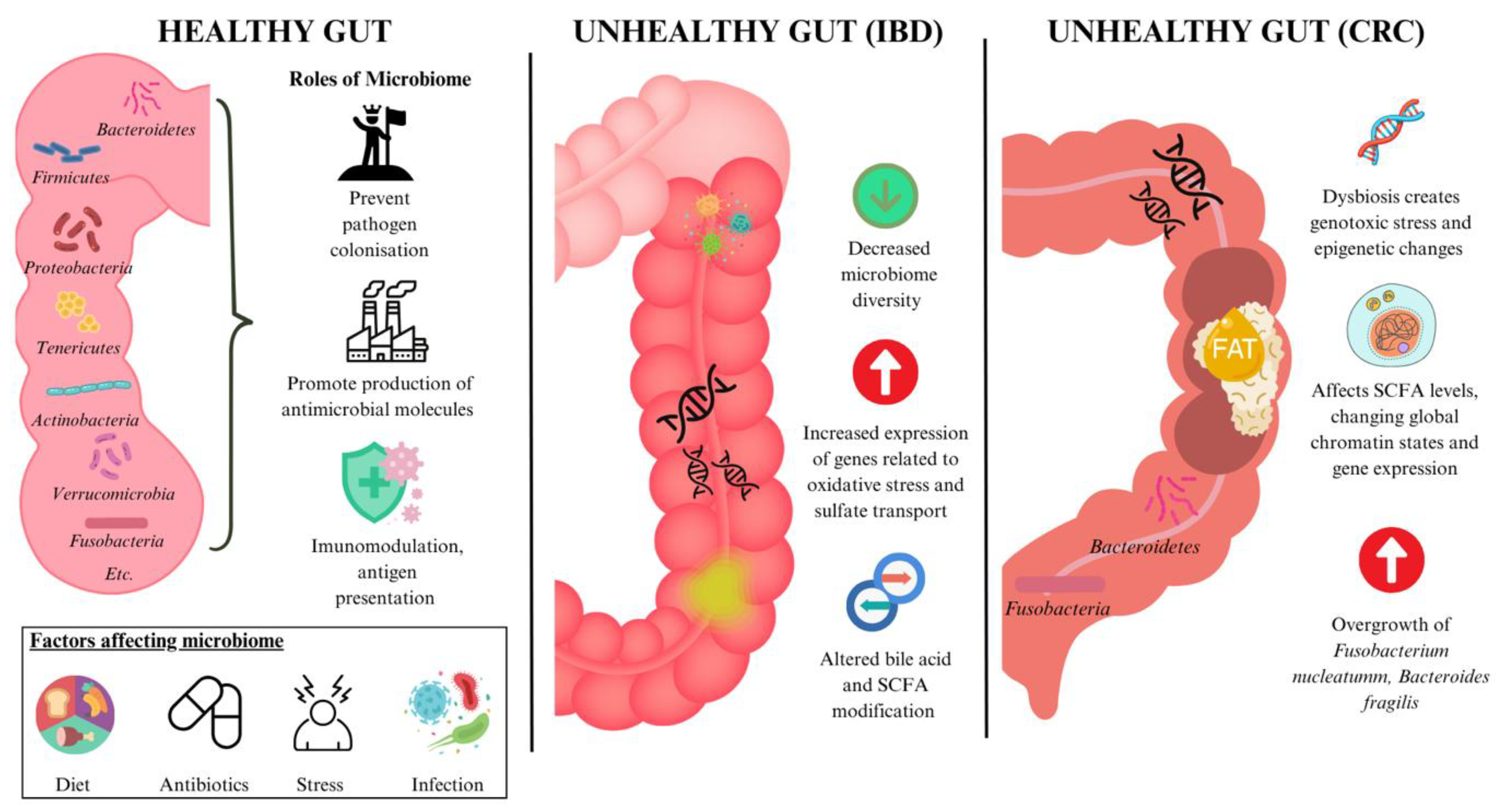
Figure 2.
A-C. Nanomedicine-enabled diagnostics for general dysbiosis (A), inflammatory bowel disease (B) and colorectal cancer (C) include biosensors for biomarker detection and nanoparticle-based imaging techniques, enabling early, sensitive, and non-invasive disease monitoring. Ag: silver; IBD: inflammatory bowel disease; HCFA: hypoxia-activatable and cytoplasmic protein-powered fluorescence cascade amplifier; Dex-CeNP: dextran coated cerium oxide nanoparticle; SPION: superparamagnetic iron oxide nanoparticle; In2O3: indium (111) oxide; CRC: colorectal cancer; AuNP: gold nanoparticle; MGF: mechano-growth factor; PANAM: poly(amidoamine); aSlex: anti-Slex.
Figure 2.
A-C. Nanomedicine-enabled diagnostics for general dysbiosis (A), inflammatory bowel disease (B) and colorectal cancer (C) include biosensors for biomarker detection and nanoparticle-based imaging techniques, enabling early, sensitive, and non-invasive disease monitoring. Ag: silver; IBD: inflammatory bowel disease; HCFA: hypoxia-activatable and cytoplasmic protein-powered fluorescence cascade amplifier; Dex-CeNP: dextran coated cerium oxide nanoparticle; SPION: superparamagnetic iron oxide nanoparticle; In2O3: indium (111) oxide; CRC: colorectal cancer; AuNP: gold nanoparticle; MGF: mechano-growth factor; PANAM: poly(amidoamine); aSlex: anti-Slex.

Figure 3.
Targeted drug delivery systems are a form of nanotherapeutics for inflammatory bowel disease. Abbreviations: IBD: inflammatory bowel disease; B-ATK-T: Bud-ATK-Tem; Csn: chitosan; 5-ASA: 5-aminosalicylic acid; PPNP: polyphenols and polymers self-assembled nanoparticle.
Figure 3.
Targeted drug delivery systems are a form of nanotherapeutics for inflammatory bowel disease. Abbreviations: IBD: inflammatory bowel disease; B-ATK-T: Bud-ATK-Tem; Csn: chitosan; 5-ASA: 5-aminosalicylic acid; PPNP: polyphenols and polymers self-assembled nanoparticle.
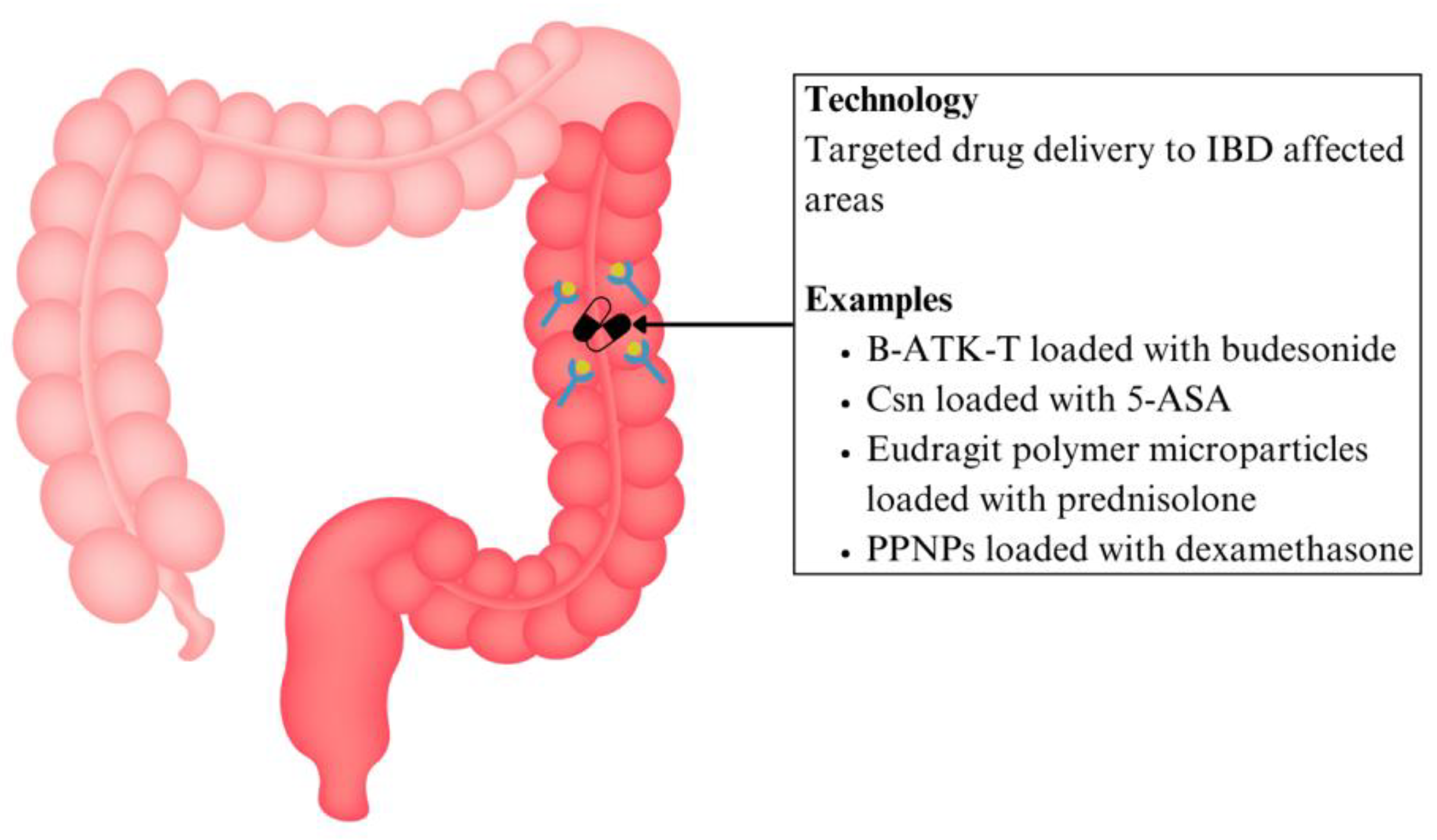
Figure 4.
Nanotherapeutics for colorectal cancer include targeted drug delivery systems, magnetic drug targeting, hyperthermia treatment, and photothermal therapy. Abbreviations: CRC: colorectal cancer; EGF: epidermal growth factor; PLGA: poly (lactic-co-glycolic acid); 5-FU: 5-fluorouracil; PFC: perfluorocarbon; EpCAM: epithelial cell adhesion molecule; PEG: polyethylene glycol; PSiNP: porous silicon nanoparticle; PTT: photothermal therapy; AuNP: gold nanoparticle; GNC: gold nanocages; MNP: magnetic nanoparticle; SPION: superparamagnetic iron oxide nanoparticle; Csn: chitosan.
Figure 4.
Nanotherapeutics for colorectal cancer include targeted drug delivery systems, magnetic drug targeting, hyperthermia treatment, and photothermal therapy. Abbreviations: CRC: colorectal cancer; EGF: epidermal growth factor; PLGA: poly (lactic-co-glycolic acid); 5-FU: 5-fluorouracil; PFC: perfluorocarbon; EpCAM: epithelial cell adhesion molecule; PEG: polyethylene glycol; PSiNP: porous silicon nanoparticle; PTT: photothermal therapy; AuNP: gold nanoparticle; GNC: gold nanocages; MNP: magnetic nanoparticle; SPION: superparamagnetic iron oxide nanoparticle; Csn: chitosan.
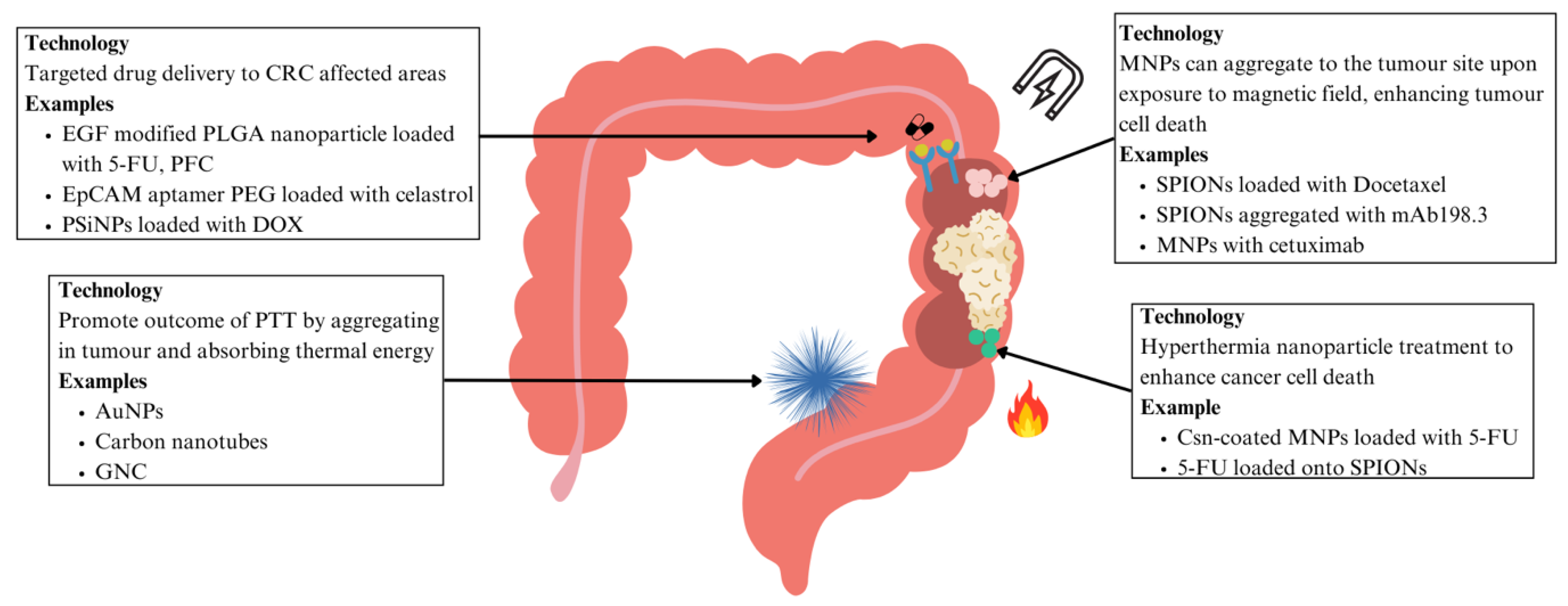
Figure 5.
Nanotechnology-based microbiome modulators, including nano-prebiotics, -probiotics, and -synbiotics, enhance gut microbial balance and immune modulation, offering novel therapeutic avenues in inflammatory bowel disease and colorectal cancer. Abbreviations: Pcn: pectin; Csn: chitosan; PLGA: poly (lactic-co-glycolic acid); PG: poly(L-glutamic acid); PL: poly(L-lysine); Ag-LNP: silver/Lactobacillus rhamnosus GG nanoparticle; CRC: colorectal cancer; CuONP: copper oxide nanoparticle; AuNP: gold nanoparticle; PPN: phthalyl pullulan nanoparticle; LP: lactobacillus plantarum.
Figure 5.
Nanotechnology-based microbiome modulators, including nano-prebiotics, -probiotics, and -synbiotics, enhance gut microbial balance and immune modulation, offering novel therapeutic avenues in inflammatory bowel disease and colorectal cancer. Abbreviations: Pcn: pectin; Csn: chitosan; PLGA: poly (lactic-co-glycolic acid); PG: poly(L-glutamic acid); PL: poly(L-lysine); Ag-LNP: silver/Lactobacillus rhamnosus GG nanoparticle; CRC: colorectal cancer; CuONP: copper oxide nanoparticle; AuNP: gold nanoparticle; PPN: phthalyl pullulan nanoparticle; LP: lactobacillus plantarum.
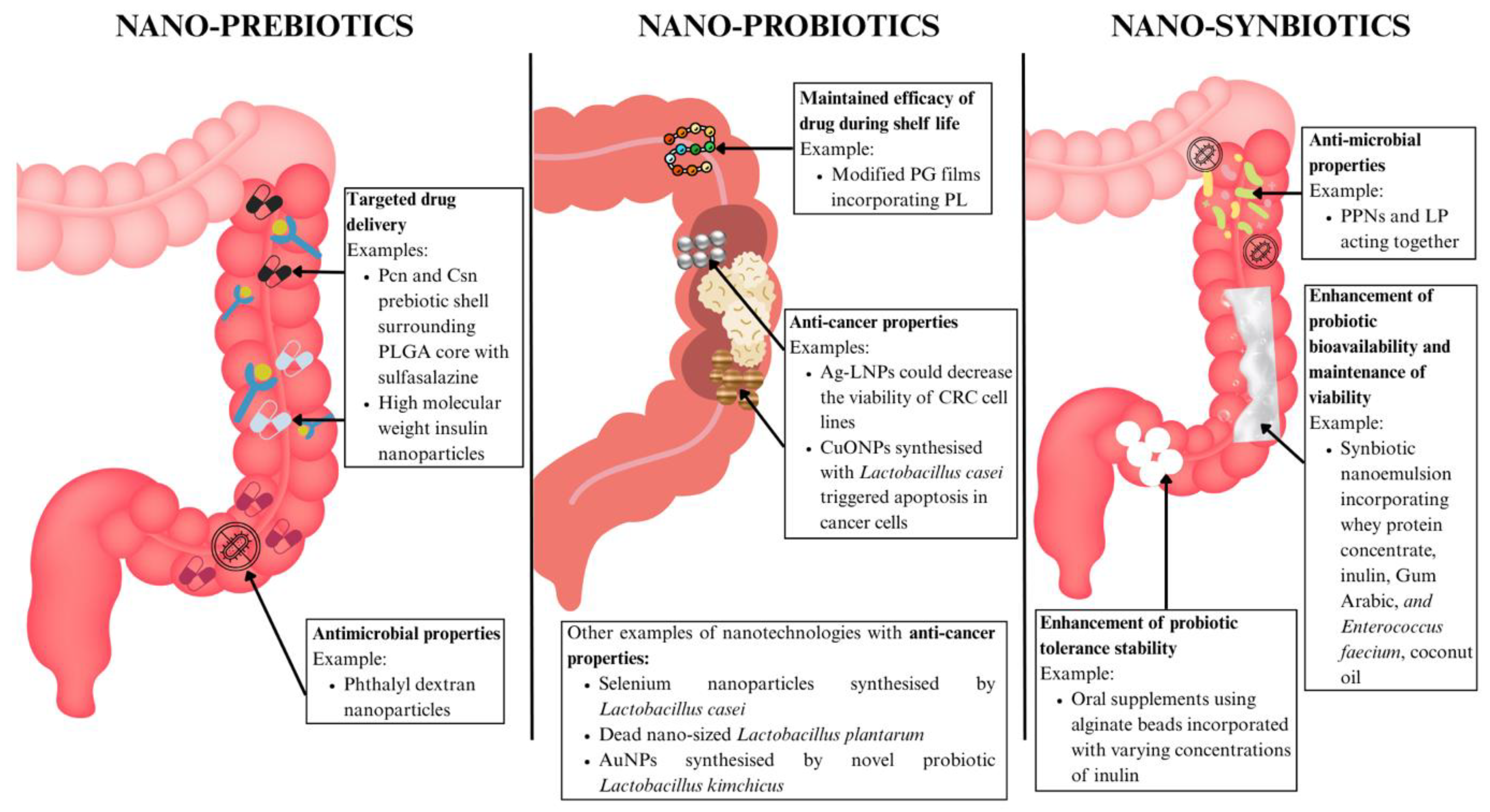
Figure 6.
Nanotherapeutics in inflammatory bowel disease include nanoparticles with anti-inflammatory and anti-oxidant properties and microbiome modulation. Abbreviations: HABN: hyaluronic acid-bilirubin nanomedicine; Ag: silver; TACS: Ta2C modified with chondroitin sulfate; MON-PEI: polyethylenimine-mesoporous organosilica; GLP-1-SSM: GLP-1 in sterically stabilised phospholipid micelles; DSPE: 1,2-distearoyl-sn-glycero-3-phosphoethanolamine; PEG: polyethylene glycol; OxbCD: β-cyclodextrin-derived material.
Figure 6.
Nanotherapeutics in inflammatory bowel disease include nanoparticles with anti-inflammatory and anti-oxidant properties and microbiome modulation. Abbreviations: HABN: hyaluronic acid-bilirubin nanomedicine; Ag: silver; TACS: Ta2C modified with chondroitin sulfate; MON-PEI: polyethylenimine-mesoporous organosilica; GLP-1-SSM: GLP-1 in sterically stabilised phospholipid micelles; DSPE: 1,2-distearoyl-sn-glycero-3-phosphoethanolamine; PEG: polyethylene glycol; OxbCD: β-cyclodextrin-derived material.
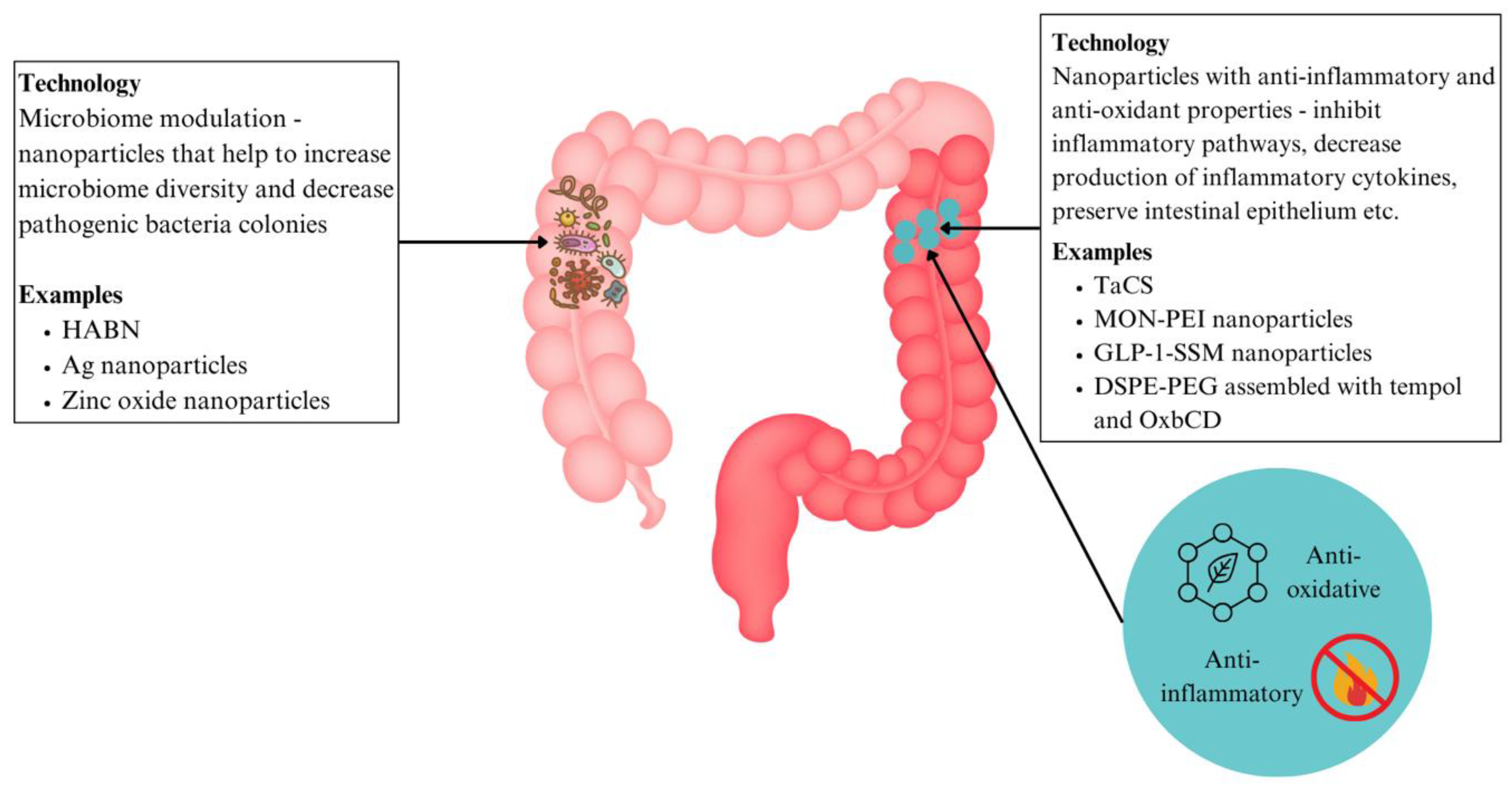
Figure 8.
Roadmap for clinical translation of nanomedicine in inflammatory bowel disease and colorectal cancer highlights current progress, existing challenges, and emerging future directions.
Figure 8.
Roadmap for clinical translation of nanomedicine in inflammatory bowel disease and colorectal cancer highlights current progress, existing challenges, and emerging future directions.
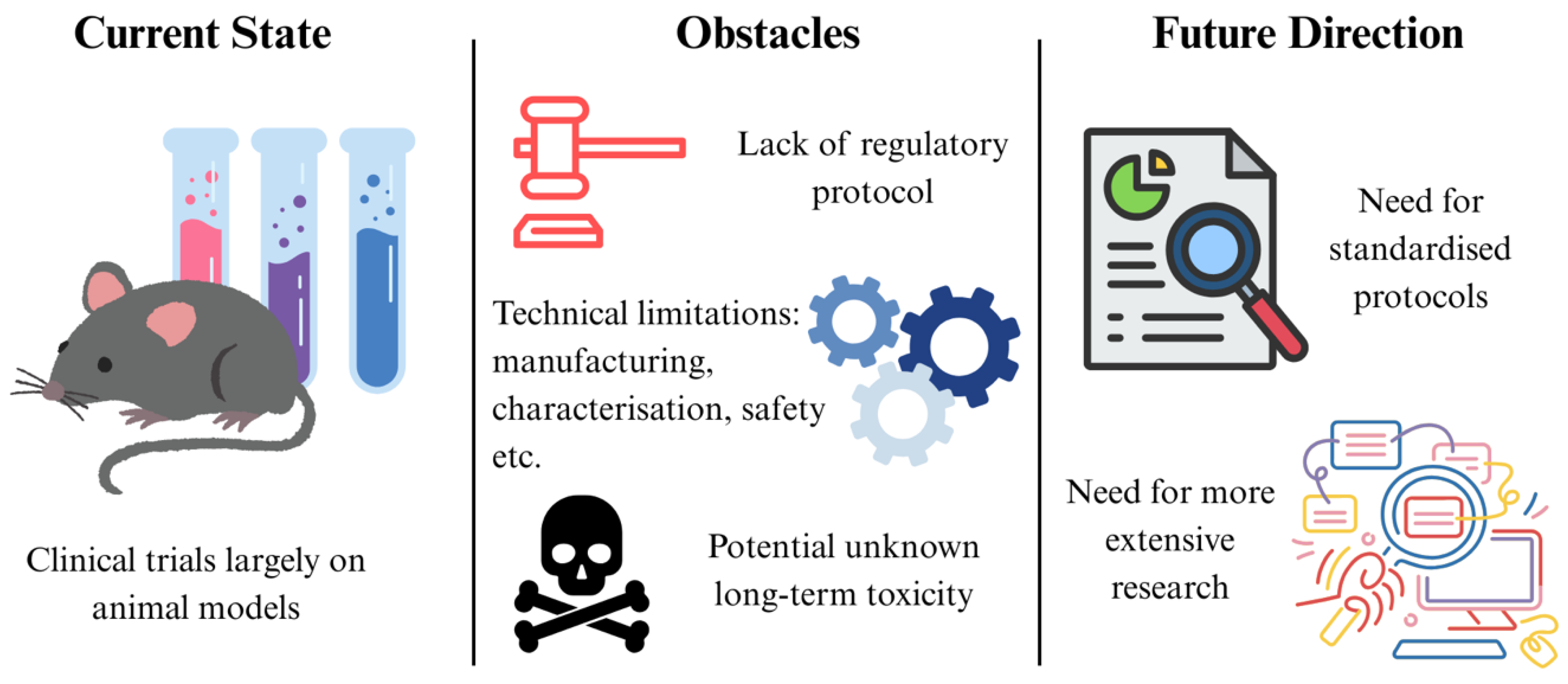
Table 1.
Summary of nanomedicine based diagnostic approaches for inflammatory bowel disease and colorectal cancer.
Table 1.
Summary of nanomedicine based diagnostic approaches for inflammatory bowel disease and colorectal cancer.
| Application | Disease | Nanotechnology Used | Mechanism | Advantages | Stage | Reference |
|---|---|---|---|---|---|---|
| Biomarker Detection |
General dysbiosis | Ag nanoparticles nanotip array | Electrochemical sensing | Low cost, easy sample preparation | Preclinical | [77] |
| CRC | Monolayer capped AuNPs | Electrochemical sensing | Minimal preparation, quick and simple procedure, insensitivity to external disturbances | [82] | ||
| Diagnostic Imaging | IBD | SPIONs and In2O3 particles | MRI | Enhances MRI imaging, correlates well with disease activity | [83] | |
| Dex-CeNP | CT imaging | Localises to diseased areas and enhances CT contrast generation | [84] | |||
| HCFA | Hypoxia-activatable fluorescence probes | Able to distinguish varying degrees of cellular hypoxia for precise treatment | [85] | |||
| CRC | AuNPs | Detect MGF in CRC tissues | Aids in determination of cancerous tissues, stronger emission intensity and photostability than fluorescent dyes | [86] | ||
| SPIONs | MRI contrast agent | Enhances MRI imaging | [87] | |||
| Quantum dots | Contrast agent for fluorescence imaging | Size-modulated absorbance and emission, high photostability, longer excited state etc. | [88] | |||
| PANAM dendrimers conjugated with various aSlex antibodies | Detects circulating tumour cells | High capture efficiency, good sensitivity, non-invasive prognostic tool | [89] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



