Submitted:
04 June 2025
Posted:
05 June 2025
You are already at the latest version
Abstract
Antiretroviral Therapy (ART) has significantly improved outcomes in individuals with Human Immunodeficiency Virus (HIV), yet its long-term cardiovascular effects, especially on hypertension risk, remain debated. This pilot study investigated hypertension risk factors in HIV-positive patients undergoing ART. Seventy HIV-infected adults without baseline hypertension were enrolled and followed. Hypertension was defined using the 2017 ACC/AHA guidelines. Data on demographic, anthropometric, metabolic, inflammatory, coagulation, and HIV-related variables were collected. Cox regression analysis identified independent predictors of hypertension. Participants had a median age of 37 years (SD ±10.96), with 84.3% being female. After a median ART exposure of 61.01 months (range: 2–164), 27 individuals (38.6%) developed elevated blood pressure. In multivariable Cox models adjusting for metabolic syndrome and BMI, age ≥35 years was associated with a 2.2-fold higher hypertension risk (Hazard Ratio [HR]: 2.2; 95% Confidence Interval [CI]: 1.04–4.55; p=0.04). Elevated triglycerides significantly increased risk, with a 7.9-fold higher likelihood of hypertension (HR: 7.9; 95% CI: 1.04–59.5; p=0.046). ART regimen type—whether initial or current—did not independently predict hypertension. In conclusion, hypertension is prevalent during ART. Traditional cardiovascular risk factors, notably age ≥35 years and hypertriglyceridemia, were key independent predictors, emphasizing the need for routine cardiovascular risk assessment in HIV management.
Keywords:
ART
; HIV
; age
; triglyceride levels
; hypertension
Introduction
According to the United Nations statistics, Eastern and Southern Africa possessed 20.6 million people living with the human immune-deficiency virus (HIV) in 2018 of which 13.8 million were accessing anti-retroviral therapy (ART) [1]. Sub-Saharan Africa (SSA) bears the greatest load of the HIV crisis, making up approximately 54% of the global HIV burden [2]. The introduction of ART marked a very big improvement in the life expectancy of people living with HIV [3,4,5]. Aging-related diseases including hypertension begin to appear as life expectancy increase [6]. Due to urbanization and westernization, hypertension and other chronic non-communicable diseases (NCDs) are at a rise in SSA [7,8]. Research findings by Nartey et al., 2023 in a study where causal association between ART and hypertension was studied using Propensity score a prevalence of hypertension was significantly greater among individuals exposed to ART (42.4%) compared to individuals who were not exposed to ART (17.0%). Furthermore, systolic (12.0 mm Hg) and diastolic (6.1 mm Hg) blood pressure elevations were linked to ART usage [9]. ART-treated HIV-positive patients exhibit a much greater morbidity rate for cardiovascular disease (CVD) compared to non-ART-treated patients [10].
Studies have shown that there is a higher risk ratio(RR) with people living with hypertension(PWH) in North America and Europe than those living in Africa with increased incidence of hypertension among HIV-positive people receiving antiretroviral therapy in these regions [11]. Reports have shown that there is an association between elevated blood pressure in people with HIV and dolutegravir-based antiretroviral therapy regimens. There is tendency in men using dolutegravir to show an elevated risk of hypertension [12]. The recent increase in CVD morbidity and mortality may be an indicator to HIV infection-related risk factors, ART metabolic effects, and chronic inflammation driven on by the virus [13] Recent regional and global studies present a high and growing incidence of hypertension, with low rates of verification, treatment, and management in Sub-Saharan Africa (SSA) [14] Study by Siddiqui et al.;2022 reported that approximately a third (32%) of the people in a study assessing hypertension a year after receiving ART acquired the condition. A higher risk was linked to the use of stavudine and non-nucleoside reverse transcriptase inhibitors (NNRTIs), especially efavirenz. Additionally, a higher risk of hypertension has been associated with conventional characteristics such advanced age and a higher body mass index (BMI) [15,16]. Prior to the use of ART, hypertension was less prevalent in people with HIV [17,18]. Obesity and older age are increasingly becoming associated with HIV-infection as well [19,20]. A 2024 meta-analysis and systematic review reported that overall prevalence of hypertension remained 21.9%, this study evaluated data from 48 studies comprising 193,843 PLWH. The individuals shows that CD4 counts ≥200, those on antiretroviral medication (ART), and males exhibited higher prevalence rates [21]. Abdela et al.; 2023 investigated the incidence and risk factors of metabolic syndrome (MetS) in people with HIV who were using antiretroviral medication (ART) in Ethiopia between 2022 and 2023. The results of the study revealed that a longer ART duration was linked to a higher risk of metabolic problems. Particularly, the prevalence of MetS was 37.6%, and each participant’s average length of time on combination ART was 10 years. Age over 45, female sex, body mass index (BMI) greater than 25 kg/m2, and usage of lopinavir/ritonavir or efavirenz-based ART regimens have been identified as independent risk factor.[22]. Another study that was conducted in Kenya noted that there is a high prevalence of obesity and hypertension among HIV-positive people. This high prevalence varied between women and men [23]. However, a systematic review conducted in sub-Saharan Africa by Chen et al. 2024 established that the occurrence of lower BP was more prevalent among HIV positive than amongst HIV negative adults [24]. This is supported by a population-based study conducted in South Africa amongst HIV positive individuals, which pointed out that hypertension was not common among HIV positive patients [25].
The Long-term use of ART on HIV infected patients include obesity, immune complications and have drug toxicity, hence suffer from hypertension [26]. Although there have been recent studies that investigated the prevalence of hypertension and its associated risk factors in HIV-infected people on ART in SSA, there is an urgent need for further research focusing on how HIV and hypertension combine in Sub-Saharan Africa, given the region’s high prevalence of both diseases [27]. We conducted this study to evaluate the prevalence of hypertension and its risk factors in a cohort of HIV-positive clinic attendees on ART in a rural area of the Eastern Cape province in South Africa, considering the scarcity of data on CVD risk factors in the context of HIV in our setting.
2. Materials and Methods
We conducted a pilot study among 70 HIV infected patients receiving ART attending Ngangelizwe community health centre (NCHC), a government healthcare facility , located at King Sabata Dalindyebo (KSD) local municipality in the South Africa’s rural Eastern Cape province between 1st February and 28th February 2019. A written informed consent, patients were consecutively enrolled into the study if they were aged 18 years and above, diagnosed with HIV infection but free from hypertension at the initiation of ART. World Health Organization (WHO) STEPwise instrument for data collection and measurement of non-communicable diseases (NCD) risk factors was used [28,29]. Demographic data, medical history (including history of Type 2 Diabetes Mellitus (T2DM), hypertension, tobacco smoking and alcohol use), and physical examination findings were recorded using WHO STEPwise tool. Systolic blood pressure (SBP) and diastolic blood pressure (DBP), weight, and height were measured. Body mass index (BMI) was defined as underweight (BMI<18.5 kg/m2), normal (BMI: 18.5 to 24.9 kg/m2), overweight (BMI: 25.0 to 29.9 kg/m2), and obese (BMI ≥30 kg/m2). The presence of metabolic syndrome (MetS) among the study participants was ascertained using criteria developed by the International Diabetes Federation (IDF) and the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III [26,27]. According to IDF criteria, MS was characterized by the presence of central obesity (waist circumference ≥94 cm for men or ≥80 cm for women) together with two of the following diagnostic criteria: (1) elevated triglyceride levels (≥150 mg/dl or ≥1.7 mmol/L); (2) low HDL cholesterol (<40 mg/dl or <1.04 mmol/L in men and <50 mg/dl or <1.29 mmol/L in women); (3) hypertension (BP ≥130/≥85 mmHg); (4) fasting hyperglycemia (glucose level ≥5.6 mmol/L or ≥100 mg/dL) or previous diagnosis of diabetes. The waist circumference was measured at the belly button using a tailor’s tape. Random blood glucose, glycated hemoglobin (HbA1c), lipid profiles including total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, D-dimmer and C-reactive protein (CRP) were measured on the Cobas 6000 (Roche, Germany). CD4+ T-cell counts were measured using Partec CyFlow Counter (Cyflow SL, Partec, Munster, Germany), whereas HIV and Hepatitis B measurements were performed using the Multiplex HIV, HCV & HBV nucleic acid test for use on the Cobas® 6800/8800 Systems (Roche, Germany) [30,31,32]. For HIV testing, at the clinic, a serial algorithm with Determine Rapid HIV-1/2 antibody (Abbott Laboratories, Abbott Park, Illinois, USA) followed by Unigold Rapid HIV Test (Trinity Biotech, PLC, IDA Business Park, Bray, County Wicklow, Ireland) was used. Cobas m511 integrated hematology analyzer (Roche, Basel, Switzerland) automatically prepared blood samples for immediate testing of platelet counts, erythrocyte sedimentation rate (ESR), and white cell counts. Continuous data were summarized as median (±SD) whilst categorical data were presented as proportions (%). The Chi-square test was used for testing relationships between variables of interest. If the outcome was a continuous variable, we used linear regression. Since the study outcome was ‘time to event’, we used Cox proportional hazard models with a p-value <0.05 being significant. IBM SPSS v.23 (IL, Chicago) was used for statistical data analysis.
3. Results
Of the 70 HIV infected patients, 27 (38.6%) developed abnormal BP: 13/27 (48.10%) within the initial 5 years of ART exposure; 10 (37.04%) between 5 and 10 years of ART exposure; and the remaining 4 (14.81%) developed abnormal BP after 10 years of ART exposure.

Table 1.
Characteristics of the study participants and univariate/bivariate analysis of factors associated with the occurrence of abnormal blood pressure among the HIV positive clinic attendees. The table reveal the link between age and body weight (BMI) to high blood pressure in the study.
Table 1.
Characteristics of the study participants and univariate/bivariate analysis of factors associated with the occurrence of abnormal blood pressure among the HIV positive clinic attendees. The table reveal the link between age and body weight (BMI) to high blood pressure in the study.
| Variables of interest |
Total N (%) |
Blood pressure | Chi-square | p-value | |
| Normal | High | ||||
| Non-modifiable risk factors: | |||||
| Age, years <35 ≥35 |
32 (45.71%) 38 (54.29%) |
24 /32 (/75%) 19/38 (50%) |
8 /32(25%) 19/38 (70.4%) |
4.58 |
0.032 |
| Gender Male Female |
11 (15.70%) 59 (84.30%) |
9/11 (81.8%) 34/59 (57.6%) |
2/11 (18.2%) 25/59 (42.4%) |
2.29 |
0.130 |
| Modifiable risk factors: | |||||
| Alcohol consumption Yes No |
26 (37.1%) 44 (62.9%) |
15/26(57.7%) 28/44 (63.6%) |
11/26 (42.3%) 16/44 (36.%) |
0.24 |
0.621 |
| Cigarette smoking Yes No |
13 (18.6%) 57 (81.4%) |
9/13(20.9%) 34/57 (59.1%) |
4/13 (30.8%) 23/57 (40.4%) |
0.41 |
0.521 |
| History of type 2 Diabetes mellitus Yes No |
4 (6.2%) 61 (93.8%) |
3/4 (75.0%) 39/61 (63.9%) |
1/4 (25.0%) 22/61 (36.1%) |
0.16 |
0.686 |
| Body mass index Normal Overweight Obesity |
29 (41.4%) 20 (28.6%) 21 (30%) |
24/29 (82.8%) 10/20(50.0%) 9/21(42.9%) |
5/29 (17.2%) 10/20 (50%) 12/21 (57.1%) |
9.74 |
0.008 |
Table 2.
Univariate/bivariate analysis of lipid profiles, blood glucose tests, coagulation disorders and inflammatory disorders associated with the occurrence of high BP among the HIV positive clinic attendees.
Table 2.
Univariate/bivariate analysis of lipid profiles, blood glucose tests, coagulation disorders and inflammatory disorders associated with the occurrence of high BP among the HIV positive clinic attendees.
| Variables of interest |
Total N (%) |
Blood pressure | Chi-square | p-value | |
| Normal | High | ||||
| Lipid profile: | |||||
| Total cholesterol, mmol/L Desirable High |
60 (93.8%) 4 (6.3%) |
38/60 (63.3%) 1/4 (25.0%) |
22/60 (36.7%) 3 /4 (75%) |
2.32 |
0.128 |
| LDL, mmol/L Desirable High |
45 (97.8%) 1 (2.2%) |
28/45 (62.2%) 0/1 (0%) |
17/45 (37.8)% 1/1 (100%) |
1.60 |
0.205 |
| HDL, mmol/L Desirable Low |
45 (70.3%) 19 (29.7%) |
26/45 (57.8%) 14/19 (35%) |
19/45 (42.2%) 5/19 (20.8%) |
1.44 |
0.230 |
| Triglyceride, mmol/L Desirable High |
46 (82.1%) 10 (17.9%) |
33/46 (77.1%) 1/10(10.0%) |
13/46 (28.3%) 9/10 (90.0%) |
13.15 |
0.0002 |
| Ratio total cholesterol/HDL <4 4-6 >6 |
56 (88.9%) 6 (9.5%) 1/1 (1.6%) |
36/56 (64.3%) 2/6(33.3%) 1/1(100%) |
20/56 (83.3%) 4/6(66.7%) 0 /1 (0%) |
2.83 |
0.024 |
| Blood glucose tests | |||||
| Random blood glucose, mmol/L Normal Abnormal |
69 (98.6%) 1 (1.4%) |
42/69 (60.9%) 1/1 (100%) |
27/69 (39.1%) 0 /1(0%) |
0.64 |
0.424 |
| Glycated Hb, mmol/L Normal Abnormal |
48 (68.6%) 22 (31.4%) |
26/48 (60.5%) 17/22 (77.3%) |
22/48 (81.5%) 5/22 (22.72%) |
3.40 |
0.065 |
| Coagulation disorders | |||||
| D-dimmer Positive Negative |
30 (46.2%) 35 (53.8%) |
16/30 (53.3%) 24/35 (68.5%) |
14/30 (46.6%) 11/35 (31.4%) |
1.58 |
0.208 |
Table 3.
Univariate/bivariate analysis of the presence of metabolic syndrome (MS), HIV related parameters and ART regiments associated the occurrence of high BP among the HIV positive clinic attendees.
Table 3.
Univariate/bivariate analysis of the presence of metabolic syndrome (MS), HIV related parameters and ART regiments associated the occurrence of high BP among the HIV positive clinic attendees.
| Variables of interest |
Total N (%) |
Blood pressure | Chi-square | p-value | |
| Normal | High | ||||
| Metabolic syndrome | |||||
| MS by NCEP Present Absent |
31 (44.3%) 39 (55.7%) |
15/31 (48.4%) 28/39 (71.7%) |
16/31 (51.6%) 11/39 (28.2%) |
3.07 |
0.080 |
| MS by IDF Present Absent |
31 (44.3%) 39 (55.7%) |
16/31 (51.6%) 27/39 (69.2%) |
15/31 (48.4%) 12 /39(30.8%) |
1.58 |
0.209 |
| HIV associated risk factors | |||||
| WHO staging at ART initiation Stage 1 Stage 2 Stage 3 Stage 4 |
34 (49.3%) 15 (21.7%) 18 (26.1%) 2 (2.9%) |
20/34 (58.8%) 8 /15(53.3%) 12/18 (66.7%) 2/2 (100%) |
14 /34(41.2%) 7/15 (46.7%) 6 /18(33.3%) 0 /2(0%) |
1.96 |
0.58 |
| Current HIV viral load, copies/mL Detectable Undetectable |
39 (58.2%) 28 (41.8%) |
22/39 (56.4%) 20/28 (71.4%) |
17/39 (43.6%) 8 /28(28.6%) |
1.00 |
0.32 |
| Level of immunosuppression Severe Advanced Mild Normal |
4 (6%) 10 (14.9%) 7 (10.4%) 46 (68.7%) |
3 /4(75.0%) 6/10 (60.0%) 4 /7(57.1%) 29 /46(63.0%) |
1/4 (25.0%) 4/10 (40.0%) 3 /7(42.8%) 17 /46(36.9%) |
0.38 |
0.943 |
| ART associated risk factors | |||||
| Initial ART regiments** 1T3E 1TFE 1S3E 1S3N 1T3N |
25 (35.7%) 33 (47.1%) 3 (4.3%) 5 (7.1%) 4 (5.7%) |
15/25 (60.0%) 20/33 (60.9%) 3/3 (100%) 3/5(60.0%) 2 /4(50.0%) |
10/25 (40.0%) 13/33(39.4%) 0/3 (0%) 2/5 (40.0%) 2/4 (50.0%) |
2.14 |
0.71 |
| Current ART regiments 1T3E 1TFE 1S3E 1S3N 1T3N |
16 (23.2%) 48 (69.6%) 2 (2.9%) 1 (1.4%) 2 (2.9%) |
10/16 (62.5%) 30/48 (62.5%) 2 /2(100.0%) 0/1 (0%) 0/2 (0%) |
6/16 (37.5%) 18/48 (37.5%) 0/2 (0%) 1 /1(100.0%) 2/2 (100%) |
6.02 |
0.019 |
| ART duration, years <5 years 5-10 years >10 years |
36 (51.4%) 24 (34.3%) 10 (14.3%) |
23/36 (63.5%) 14/24(58.3%) 6/10 (60.0%) |
13 /36(36.1%) 10/24 (41.7%) 4/10 (40.0%) |
0.20 |
0.91 |
Table 4.
Multivariate Cox-regression analysis displaying independent risk factors for the development of hypertension over the duration of ART exposure.
Table 4.
Multivariate Cox-regression analysis displaying independent risk factors for the development of hypertension over the duration of ART exposure.
| Risk factors |
Hazard Ratio (HR) (95% CI for HR) |
B-coefficient | SE | Wald chi-square | p-value | |
| Age, years |
2.169 (1.035–4.546) |
0.774 |
0.378 |
4.206 |
0.040* |
|
| Triglyceride, mmol/L | 7.855 (1.037–59.469) |
2.061 | 1.033 | 3.982 |
0.046* |
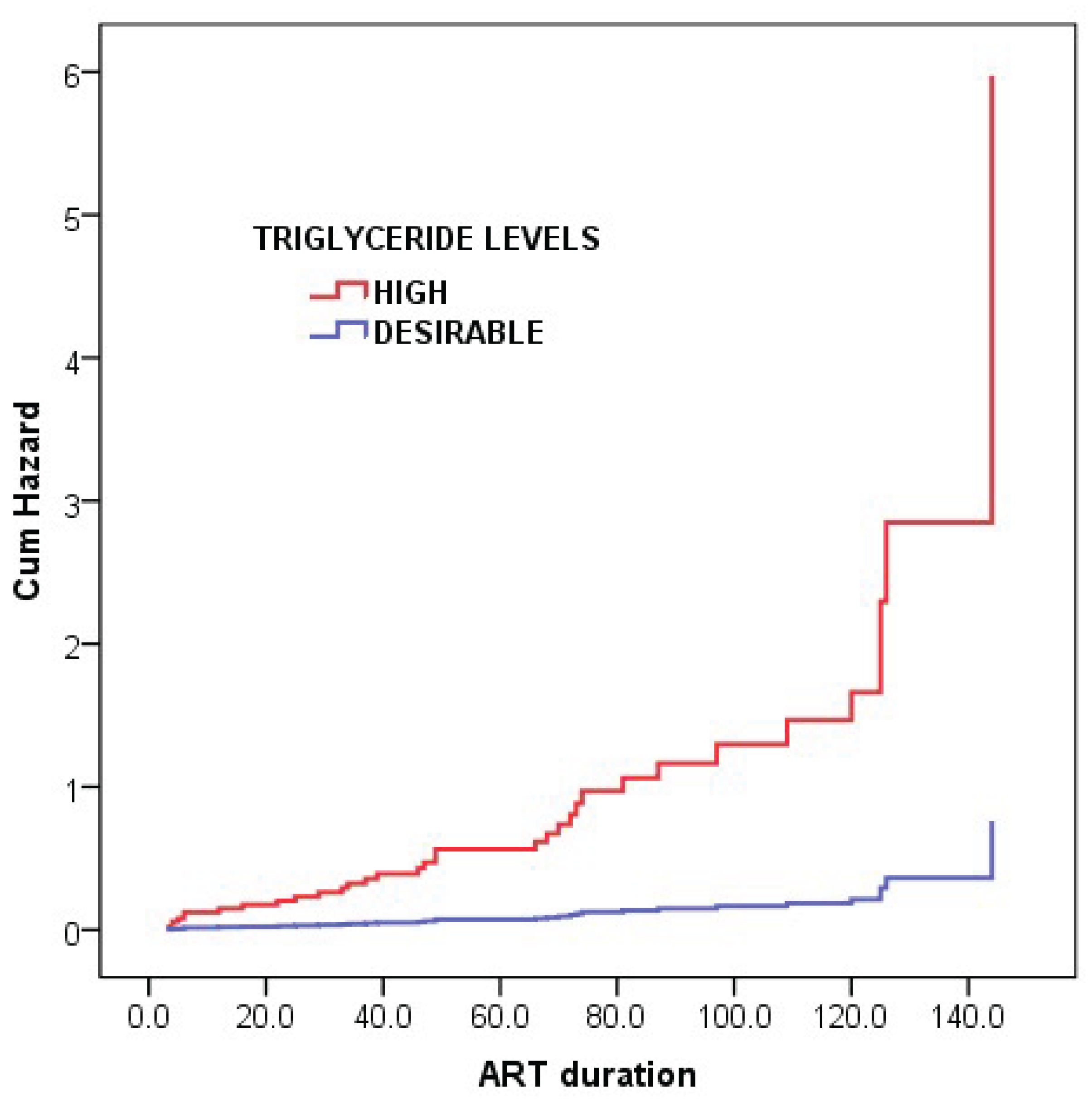
Figure 1 shows the presence of metabolic syndrome and BMI, patients aged 35 years and above and those displaying blood levels of triglyceride above the desirable.
Figure 2 above present over the course of ART 2 times (Hazard Ratio: 2.2; 95% CI: 1.04–4.55; p= 0.04) and 8-times (Hazard Ratio: 7.9; 95% CI: 1.04–59.5; p=0.046) high likely to develop hypertension, respectively. Variables in the Cox proportional-hazards model are displayed.
4. Discussion
Studies have shown that high levels of triglyceride contribute to the thickening of the artery walls (arteriosclerosis), resulting in increased risk of hypertension, stroke, heart attack and other cardiovascular diseases [33,34]. Most patients in this study were either obese or overweight. Losing weight is strongly advised because it would lower excessive calories, which could be converted to triglycerides. Furthermore, most of the patients in this study who had high blood pressure were drinking alcohol, however this was not statistically significant. The latter is high in calories and sugar, and previous studies have demonstrated that regular consumption of alcohol had a potent effect on levels of triglycerides [35,36]. It is evident from this study that traditional risk factors (not HIV and ART related factors) were key players in the development of hypertension among HIV infected patients on chronic medication therefore policies on healthy eating habits should be promoted. The use of healthier fats such as fat found in plants, vegetables and fish, which are high in omega-3 should be recommended. Regular exercise along with reducing sugar and processed carbohydrates are additional healthy lifestyle choices that patients can make to prevent elevated blood triglyceride levels [37].
Study has established a link between age and triglyceride levels. Triglyceride levels in men’s blood have been found to progressively rise until the age of fifty, at which point it begins to lightly decrease. Nonetheless, as women age, their triglyceride levels continue to rise, mild hypertriglyceridemia are reported in women from the age of 60 years and 30 years in men [38,39]. Although age influences blood levels of triglycerides, it has been previously reported as being an independent risk factor for hypertension [39]. Prior statistics show that older age groups have a substantially greater mean blood pressure. These studies suggested that the age-related rise of blood pressure is not inevitable in all patients, irrespective of their HIV status and ART regimens [40].
Our findings in this study reports traditional risk factor such as being older than 35 and having an elevated triglyceride which suggest significant, independent and highly associated risk factor in hypertension, the incidence of hypertension is also high among HIV-infected patients receiving chronic ART medication in this study.
5. Conclusions
One of the limitations in this study is that the pilot study was conducted in one community health centre only. There is a need for a robust and expanded study throughout the province with comparable data among various settings so as establish the findings from this study. However, the study shares light about the increasing prevalence of hypertension and its associated risk factors within the context of a rural setting where the HIV epidemic has been continuously growing, with majority of these HIV infected patients receiving ART.
Author Contributions
T.A,U.T and O.OA methodology, T.A and U.T and O.OA, validation, T.A, U.T and O.O.A and formal analysis U.T and T.A investigation, T.A, U.T and O.O.A resources; T.A, U.T, data curation,T.A, writing—original draft preparation; T.A, U.T and O.O.A visualization, T.A, U.T and O.O.A project administration T.A and U.T..
Funding
The study was financed by the South African Medical Research Council (SAMRC) with grant number MRC-RFA-CC-01-2024
Institutional Review Board Statement
The study was approved by the Research Ethics and Biosafety Committee of the Faculty of Health Sciences in Walter Sisulu University, bearing the protocol number 073/15. Permissions to conduct the study were obtained from the Eastern Cape Department of Health and the health district office. Written informed consents were obtained from all study participants, and confidentiality was observed throughout the study. To protect privacy and confidentiality of patients, no names were recorded and instead, a personalized research number was used for each patient and only investigators had access to the collected data..
Acknowledgments
The work reported herein was made possible through funding by the South African Medical Research Council (SAMRC) through its Division of Research Capacity Development under the SAMRC Research Strengthening & Capacity Development Initiative (RCDI) Programme. The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the SAMRC.”
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of to study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ACC | American College of Cardiology |
| AHA | American Heart Association |
| ART | Anti-retroviral therapy |
| ANOVA | Analysis of variance |
| BMI | Body mass index |
| CD4 | Cluster of differentiation 4 |
| CI | Confidence interval |
| CRP | C-reactive protein |
| DBP | Diastolic blood pressure |
| HDL | High-density lipoprotein |
| HIV | Human immunodeficiency virus |
| LDL | Low-density lipoprotein |
| NCD | Non-communicable diseases |
| NHLS | National Health Laboratory Services |
| SBP | Systolic blood pressure |
| SD | Standard deviation |
| SSA | Sub-Saharan Africa |
| TC | Total cholesterol |
| WHO | World Health Organization |
References
- UNAIDS. FACT SHEET—WORLD AIDS DAY 2019 Geneva: GLOBAL HIV STATISTICS; 2019: Accessed online 28 May 2025 https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf.
- The Global HIV/AIDS Epidemic. The Global HIV/AIDS Epidemic USA: KFF; 2019 updated Sep 9. Accessed online May 28, 2025, from: https://www.kff.org/global-health-policy/fact-sheet/the-global-hivaids-epidemic.
- Kooij, K.W.; Zhang, W.; Trigg, J.; Cunningham, N.; O Budu, M.; E Marziali, M.; Lima, V.D.; A Salters, K.; Barrios, R.; Montaner, J.S.G.; et al. Life expectancy and mortality among males and females with HIV in British Columbia in 1996–2020: a population-based cohort study. Lancet Public Heal. 2025, 10, e228–e236. [Google Scholar] [CrossRef]
- Appiedu-Addo, S.N.A.; Appeaning, M.; Magomere, E.; Ansa, G.A.; Bonney, E.Y.; Quashie, P.K. The urgent need for newer drugs in routine HIV treatment in Africa: the case of Ghana. Front. Epidemiology 2025, 5, 1523109. [Google Scholar] [CrossRef] [PubMed]
- Moyo, R.C.; Sigwadhi, L.N.; Carries, S.; Mkhwanazi, Z.; Bhana, A.; Bruno, D.; Davids, E.L.; Van Hout, M.-C.; Govindasamy, D. Health-related quality of life among people living with HIV in the era of universal test and treat: results from a cross-sectional study in KwaZulu-Natal, South Africa. HIV Clin. Trials 2024, 25, 2298094. [Google Scholar] [CrossRef] [PubMed]
- Okyere, J.; Ayebeng, C.; Owusu, B.A.; Dickson, K.S. Prevalence and factors associated with hypertension among older people living with HIV in South Africa. BMC Public Heal. 2022, 22, 1–9. [Google Scholar] [CrossRef]
- Gafane-Matemane, L.F.; Craig, A.; Kruger, R.; Alaofin, O.S.; Ware, L.J.; Jones, E.S.W.; Kengne, A.P. Hypertension in sub-Saharan Africa: the current profile, recent advances, gaps, and priorities. J. Hum. Hypertens. 2024, 39, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef]
- Nartey, E.T.; A Tetteh, R.; Anto, F.; Sarfo, B.; Kudzi, W.; Adanu, R.M. Risk of hypertension in adult patients on antiretroviral therapy: a propensity score matching analysis. 2023. [CrossRef]
- Ghandakly, E.; Moudgil, R.; Holman, K. Cardiovascular disease in people living with HIV: Risk assessment and management. Clevel. Clin. J. Med. 2025, 92, 159–167. [Google Scholar] [CrossRef]
- management. Cleveland Clinic journal of medicine, 92(3), 159-167.
- Davis, K.; Perez-Guzman, P.; Hoyer, A.; Brinks, R.; Gregg, E.; Althoff, K.N.; Justice, A.C.; Reiss, P.; Gregson, S.; Smit, M. Association between HIV infection and hypertension: a global systematic review and meta-analysis of cross-sectional studies. BMC Med. 2021, 19, 1–16. [Google Scholar] [CrossRef]
- Hirigo, A.T.; Yilma, D.; Astatkie, A.; Debebe, Z. The association between dolutegravir-based antiretrovirals and high blood pressure among adults with HIV in southern Ethiopia: a cross-sectional study. Ther. Adv. Infect. Dis. 2024, 11. [Google Scholar] [CrossRef]
- Mugisha, N. , Ghanem, L., Komi, O. A., Noureddine, R., Shariff, S., Wojtara, M.,... & Uwishema, O. (2025). Addressing Cardiometabolic Challenges in HIV: Insights, Impact, and Best Practices for Optimal Management—A Narrative Review. Health Science Reports, 8(4), e70727.
- Derick, K.I.; Khan, Z. Prevalence, Awareness, Treatment, Control of Hypertension, and Availability of Hypertension Services for Patients Living With Human Immunodeficiency Virus (HIV) in Sub-Saharan Africa (SSA): A Systematic Review and Meta-analysis. Cureus 2023, 15. [Google Scholar] [CrossRef]
- Siddiqui, M.; Moore, T.; Long, D.M.; Burkholder, G.A.; Willig, A.; Wyatt, C.; Heath, S.; Muntner, P.; Overton, E.T. Risk Factors for Incident Hypertension Within 1 Year of Initiating Antiretroviral Therapy Among People with HIV. AIDS Res. Hum. Retroviruses 2022, 38, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Tsuro, U.; Oladimeji, K.E.; Pulido-Estrada, G.-A.; Apalata, T.R. Risk Factors Attributable to Hypertension among HIV-Infected Patients on Antiretroviral Therapy in Selected Rural Districts of the Eastern Cape Province, South Africa. Int. J. Environ. Res. Public Heal. 2022, 19, 11196. [Google Scholar] [CrossRef] [PubMed]
- Mivumbi, J. P. , & Gbadamosi, M. A. (2025). Hypertension Prevalence and Associated Factors in HIV Positive Women at Kicukiro, Kigali, Rwanda: A Cross-Sectional Analysis. medRxiv, 2025-03.
- Siddiqui, M.; Moore, T.; Long, D.M.; Burkholder, G.A.; Willig, A.; Wyatt, C.; Heath, S.; Muntner, P.; Overton, E.T. Risk Factors for Incident Hypertension Within 1 Year of Initiating Antiretroviral Therapy Among People with HIV. AIDS Res. Hum. Retroviruses 2022, 38, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Bailin, S.S.; Koethe, J.R.; Rebeiro, P.F. The pathogenesis of obesity in people living with HIV. Curr. Opin. HIV AIDS 2023, 19, 6–13. [Google Scholar] [CrossRef]
- Fanfair, R. , Cheever, L., & Mermin, J. is National HIV/AIDS and Aging Awareness Day CDC encourages people aged 50 or older to get tested for HIV At a glance. 18 September.
- Chen, A.; Chan, Y.-K.; Mocumbi, A.O.; Ojji, D.B.; Waite, L.; Beilby, J.; Codde, J.; Dobe, I.; Nkeh-Chungag, B.N.; Damasceno, A.; et al. Hypertension among people living with human immunodeficiency virus in sub-Saharan Africa: a systematic review and meta-analysis. Sci. Rep. 2024, 14, 1–11. [Google Scholar] [CrossRef]
- Abdela, A.A.; Yifter, H.; Reja, A.; Shewaamare, A.; Ofotokun, I.; Degu, W.A. Prevalence and risk factors of metabolic syndrome in Ethiopia: describing an emerging outbreak in HIV clinics of the sub-Saharan Africa – a cross-sectional study. BMJ Open 2023, 13, e069637. [Google Scholar] [CrossRef]
- Saito, A.; Karama, M.; Kamiya, Y. HIV infection, and overweight and hypertension: a cross-sectional study of HIV-infected adults in Western Kenya. Trop. Med. Heal. 2020, 48, 1–12. [Google Scholar] [CrossRef]
- Chen, A.; Chan, Y.-K.; Mocumbi, A.O.; Ojji, D.B.; Waite, L.; Beilby, J.; Codde, J.; Dobe, I.; Nkeh-Chungag, B.N.; Damasceno, A.; et al. Hypertension among people living with human immunodeficiency virus in sub-Saharan Africa: a systematic review and meta-analysis. Sci. Rep. 2024, 14, 1–11. [Google Scholar] [CrossRef]
- Galaviz, K.I.; Patel, S.A.; Siedner, M.J.; Goss, C.W.; Gumede, S.B.; Johnson, L.C.; Ordóñez, C.E.; Laxy, M.; Klipstein-Grobusch, K.; Heine, M.; et al. Integrating hypertension detection and management in HIV care in South Africa: protocol for a stepped-wedged cluster randomized effectiveness-implementation hybrid trial. Implement. Sci. Commun. 2024, 5, 1–11. [Google Scholar] [CrossRef]
- Spach, D. H. Spach, D. H. . National HIV Curriculum. Adverse Effects of Antiretroviral Medications(2025). Accessed online May 29,2025:https://www.hiv.uw.edu/go/antiretroviral-therapy/adverse-effects/core-concept/all?utm_source.
- Denu, M.K.I.; Revoori, R.; Buadu, M.A.E.; Oladele, O.; Berko, K.P. Hypertension among persons living with HIV/AIDS and its association with HIV-related health factors. AIDS Res. Ther. 2024, 21, 1–6. [Google Scholar] [CrossRef]
- World Health Statistics 2023. Accessed online May 29, 2025. https://cdn.who.int/media/docs/default-source/gho-documents/world-health-statistic-reports/2023/world-health-statistics-2023_20230519_.pd.
- Fryar, C. D. , Kit, B., Carroll, M. D., & Afful, J. (2024). Hypertension Prevalence, Awareness, Treatment, and Control among Adults Ages 18 and Older: United States, August 2021—August 2023.
- Demissie, B.M.; Girmaw, F.; Amena, N.; Ashagrie, G. Prevalence of metabolic syndrome and associated factors among patient with type 2 diabetes mellitus in Ethiopia, 2023: asystematic review and meta analysis. BMC Public Heal. 2024, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ayoobi, F.; Jalali, Z.; Bidaki, R.; Lotfi, M.A.; Esmaeili-Nadimi, A.; Khalili, P. Metabolic syndrome: a population-based study of prevalence and risk factors. Sci. Rep. 2024, 14, 1–11. [Google Scholar] [CrossRef]
- WHO. Global HIV Programme. Accessed online May 29, 2025. https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/treatment/advanced-hiv-disease. 3.
- Ren, Q.-W.; Teng, T.-H.K.; Ouwerkerk, W.; Tse, Y.-K.; Tsang, C.T.W.; Wu, M.-Z.; Tse, H.-F.; Voors, A.A.; Tromp, J.; Lam, C.S.P.; et al. Triglyceride levels and its association with all-cause mortality and cardiovascular outcomes among patients with heart failure. Nat. Commun. 2025, 16, 1–11. [Google Scholar] [CrossRef]
- Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; Johnson, H.M.; et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2023, 148, E9–E119. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Sun, L.; Mu, Z. Effects of different weight loss dietary interventions on body mass index and glucose and lipid metabolism in obese patients. Medicine 2023, 102, e33254. [Google Scholar] [CrossRef]
- Fuentes, J.B.; Beara, I.; Torović, L. Regulatory Compliance of Health Claims on Omega-3 Fatty Acid Food Supplements. Foods 2024, 14, 67. [Google Scholar] [CrossRef]
- Suzuki, T.; Fukui, S.; Shinozaki, T.; Asano, T.; Yoshida, T.; Aoki, J.; Mizuno, A. Lipid Profiles After Changes in Alcohol Consumption Among Adults Undergoing Annual Checkups. JAMA Netw. Open 2025, 8, e250583. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, M. , Wilsgaard, T., Grimsgaard, S., Hopstock, L. A., & Hansson, P. (2023). Associations between postprandial triglyceride concentrations and sex, age, and body mass index: cross-sectional analyses from the Tromsø study 2015–2016. Frontiers in Nutrition, 10, 1158383.
- Li, C.; Zhao, S.; Li, Y.; He, S.; Jian, W.; Liu, Y.; Cheng, Z.; Peng, H. Triglyceride-glucose index predicts adverse cardiovascular events in patients with H-type hypertension combined with coronary heart disease: a retrospective cohort study. Cardiovasc. Diabetol. 2025, 24, 1–16. [Google Scholar] [CrossRef]
- Chen, A.; Chan, Y.-K.; Mocumbi, A.O.; Ojji, D.B.; Waite, L.; Beilby, J.; Codde, J.; Dobe, I.; Nkeh-Chungag, B.N.; Damasceno, A.; et al. Hypertension among people living with human immunodeficiency virus in sub-Saharan Africa: a systematic review and meta-analysis. Sci. Rep. 2024, 14, 1–11. [Google Scholar] [CrossRef]
Figure 1.
Age (≥35 years) as an independent risk factor for the development of abnormal BP over the course of ART in HIV infected patients (n = 70).
Figure 1.
Age (≥35 years) as an independent risk factor for the development of abnormal BP over the course of ART in HIV infected patients (n = 70).
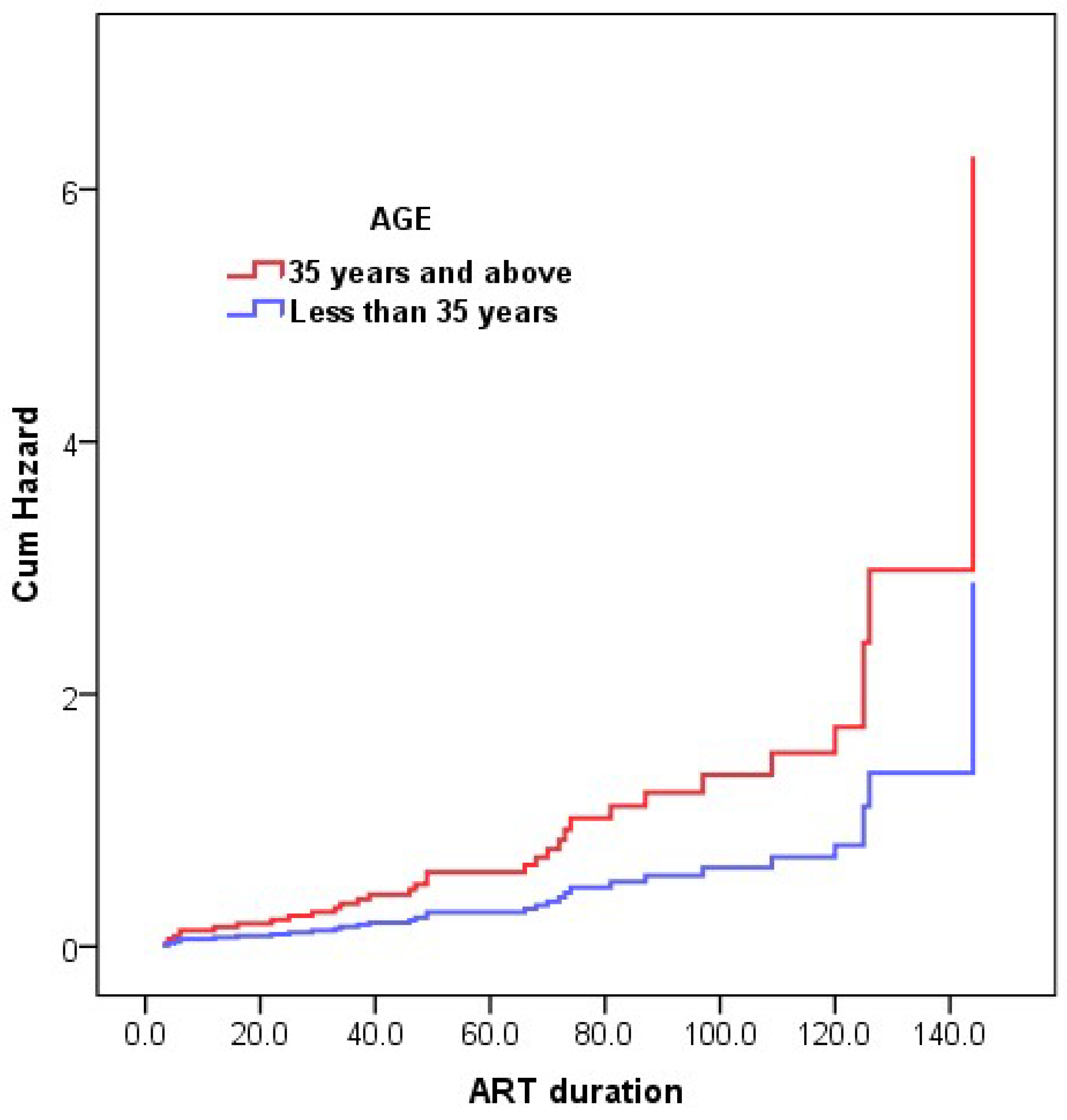
Figure 2.
Hypertriglyceridemia as an independent risk factor for the development of abnormal BP over the course ART in HIV infected patients (n = 70).
Figure 2.
Hypertriglyceridemia as an independent risk factor for the development of abnormal BP over the course ART in HIV infected patients (n = 70).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



