
Submitted:
03 June 2025
Posted:
04 June 2025
You are already at the latest version
Abstract
With increasing popularity in pickleball (PB) has come an increase in upper extremity (UE) injury. This study examines the relationship between PB-related UE injury and player characteristics, typical weekly playing behavior, grip tightness, and stretching or strengthening exercise. Among the 253 participants, 41% reported at least one UE injury with 10% reporting an acute and 37.5% reporting a chronic UE injury. Chi-square analysis (α = 0.05) was used to determine between group differences. The risk of sustaining a UE injury was 1.51 to 1.53 times higher among individuals who played longer or more frequent sessions, as well as those who played on consecutive days. Acute UE injuries were significantly more likely in players who played > 2 hours at a time, played on consecutive days, or maintained a tight baseline grip—corresponding to relative risks of 2.38, 4.97, and 2.67, respectively. Chronic UE injuries were more common in players with more years of PB experience, higher skill levels, and greater playing volume. No difference in UE injury and sex, strengthening, or stretching was found. These findings may inform evidence-based prevention strategies for reducing UE injury risk among PB players and support tailored recommendations for players, coaches, and healthcare providers.
Keywords:
pickleball
; injury
; upper extremity
; risk
; play volume
; grip
; skill level
1. Introduction
Originating near Seattle, Washington in 1965, pickleball (PB) is now one of the fastest-growing sports in the United States (US) with players spanning all age groups[1]. Though PB shares similarities with tennis, badminton, and paddleball, key differences exist in court dimensions, player positioning, and equipment (racket/paddle and ball/shuttlecock). Additional distinctions include the shorter learning curve to become competitive and the lower physical fitness and agility requirements of players. Initially popular among older adults, the sport’s demographic is shifting. In 2025, adults aged 25-34 constitute the largest segment of PB players, with the average age being 34.8 years[2]. As PB play has surged, so too has the number of injuries[3]. Alarmingly, the rate of PB-related injuries is increasing more rapidly than the rate of participation[3,4]. Because PB is a young sport, there is less published literature on PB-related injury (PBRI) compared to more established racket sports such as tennis and badminton.
Consistent with epidemiological studies of other racket or paddle sports[5,6], playing PB poses a risk for acute UE injury such as strain/sprain, or fracture[7-9],and chronic UE injury, such as epicondyalgia[10,11].Analysis of US emergency department (ED) data indicates PB-related injury to the UE in approximately in 25%-33% of patients, with an increasing number of injuries across the study periods[7,8]. A high number of UE PB-related injuries treated in locations other than the ED have been reported[3,12].
Sex differences in injury patterns have also been noted. In badminton, males are more commonly injured than females, however injury rates were the same when accounting for playing time.[6] In PB, women are more likely to experience fractures[13], particularly of the wrist[3,8]. Age is a well-documented risk factor for racket/paddle-sport-related injuries, with several studies reporting higher injury rates among older players[14-16], though not all studies differentiated between UE and LE injury. Data from the National Electronic Injury Surveillance System (NEISS) confirms that racket/paddle sport-related injury is more common among older individuals[4,7,17]. However, injury risk is not exclusive to older populations. With the increasing participation in PB among younger adults, injury rates in these age groups are also rising[4].
Playing behavior, such as high play volume, poses a higher risk of a chronic UE injury in tennis[18,19]and padel players[20]. In tennis, grip tightness during and following ball contact has been related to higher forces to UE, particularly during off-center impacts [21,22]and during backhand strokes[23].
Stretching and strengthening to facilitate recovery from UE injury is well supported in the literature[24-26]. However, the link between UE injury risk and participation in strength and flexibility is unclear. While some studies find no benefit to these types of training[27], more recent studies indicate that strengthening and stretching can reduce injury rates, especially in overhead sports[14,28].
This study examines the relationship between UE injuries and recreational PB player characteristics, playing behavior, grip tightness, and participation in strengthening and stretching exercises. Findings will help inform both players and healthcare providers regarding evidence-based prevention strategies for upper extremity injuries in PB.
2. Materials and Methods
2.1. Participants
An invitation to participate in an anonymous online survey using the Qualtrics survey platform (Provo, UT) was posted at multiple recreational facilities with PB courts (both indoor and outdoor) and on various PB-related social media group sites across the US. Additionally, PB group social media leaders were asked to share the survey with their internal email lists. The survey could be completed on a computer, tablet, or mobile phone.
To enter the survey, participants had to confirm they were at least 18 years old and had played PB for at least six months. The survey included questions related to sex, age, skill level, number of years playing PB, and typical playing behavior. Participants also reported perceived grip tightness during dinks, volleys, and baseline hits, and whether they engaged in an upper extremity (UE) strengthening program—using free weights, body weight exercises, resistance machines, or other methods—or a stretching program, including yoga (instructor-led or self-guided), general stretching (instructor-led or self-guided), or other forms, at least 1–2 times per week.
Skill level definitions, as published by the USA Pickleball Organization[29], were provided within the survey. Participants reported whether they had experienced an acute UE injury, a chronic UE injury, and which anatomical region (shoulder, elbow, wrist/hand) had been injured. The survey remained open for six months. This study was approved by the Institutional Review Board of the University of Tennessee at Chattanooga.
2.2. Statistical Analysis
Survey results were imported into SPSS version 29.0.2. Unanswered questions were coded as missing and excluded from the analysis. A descriptive analysis was performed to obtain information regarding the
number of times the categories of each study variable occurred (frequency and percentage). The chi-squared test of independence (α = 0.05) was used to determine differences in the report of at least one acute or chronic UE injury and the following variables: sex, age, skill levels of play, and playing behavior (number and length of sessions per week), consecutive days of play, and overall play volume). Additional analyzed variables included perceived grip tightness measured on a 5-point Likert scale during dinks, volleys and baseline play; as well as engagement in upper extremity (UE) strengthening or stretching exercises at least once or twice a week. The association between skill leval and playing behavior was calculated. Effect sizes were determined for all significant differences using phi for dichotomous variables and Cramér’s V for non-dichotomous variables. The magnitude of effect for both phi and Cramér’s V was classified as small (0.1), moderate (0.3), or large (0.5)[30].
For significant associations involving three categories, post-hoc tests were performed using the Bonferroni correction to control for the risk of type I errors. The adjusted p-value for post-hoc testing was calculated as .05/3 = .0167. Due to sample size considerations, dichotomous categories were created for all variables except age. Age was grouped into three categories to allow comparisons of younger adults (18–34 years old), middle-aged adults (35–64 years old), and older adults (≥65 years old). Cut points for non-dichotomous variables (years of play, session length, and play volume) were based on mean responses approximating a 50% split. While the average number of times played per week reported in this sample was 3.7, a cutoff of 3 (i.e., <3 vs. ≥4) was chosen because those playing 4 days per week must play on consecutive days while those who play 3 times per week may not, thus potentially differentiating between these two groups. Skill level was collapsed into two categories (<3.5 vs. >3.5) to reflect differences in consistency, strategy, shot selection, and control that mark the transition to the 4.0 skill level. Because a firmer grip may be linked to injury, perceived grip strength was grouped into two categories: sufficient and tight.
3. Results
3.1. Survey Participation and Demographics
A total of 269 participants began the survey and 253 participants (94%) completed it. Data from the 253 participants were included in the final analysis. See Table 1 for frequency data of the sample. One hundred and four participants reported a total of 152 UE injuries. There were 30 acute injuries: 16 strain/sprains (14 shoulder, 2 wrist/hand), 10 fractures (4 elbow, 6 wrist/hand) and 4 unspecified (3 shoulder, 1 elbow). There were 122 chronic injuries. Three participants reported more than one acute injury, while 18 participants report more than one chronic UE injury.
Figure 1 provides details on acute and chronic injury location. Of the 61 reported chronic elbow injuries, 38 were lateral, 13 were medial, and 10 were both lateral and medial. Among participants who reported engaging in strengthening exercises, 97 utilized free weights, 79 performed body weight resistance exercises, and 49 used resistance machines. Of participants reported engaging in stretching activities, 114 performed general stretching and 29 performed yoga.
3.2. Overall Upper Extremity Injury
Overall UE injury was not significantly different based on sex. Therefore, data from both sexes were pooled for analyses. The average age of participants was 52.8 years (SD = 16.7; range: 19 – 83 years). Differences between participants reporting an injury and not reporting an injury are reported in Table 2. There were significant differences with small effect in reported UE injury based on age, session length, play frequency, and playing on consecutive days. Post-hoc analysis of age indicated the middle age group is significantly different than the younger or older age groups. In participants with UE injury there was an association of small to moderate effect between skill level and the play behaviors of sessions played per week [Χ²(1)=11.947, p=.0005, phi=.219], play volume per week [Χ²(1)=13.014, p=.0003, phi=.229], and playing on consecutive days [Χ²(1)=13.014, p=.0003, phi=.229] and no association between skill level and session length [Χ²(1)=3.352, p=.067].
3.3. Acute Upper Extremity Injury
Acute UE injury was not significantly different based on sex, so data from both sexes were pooled for subsequent analyses. Between groups difference in reported acute injury are in Table 3. There were significant differences with small effect in reported acute UE injury based on session length, playing on consecutive days, and perceived grip tightness during baseline shots. No significant between group differences were found for demographic factors, other playing characteristics, or grip tightness during dinks or volleys.
3.4. Chronic Upper Extremity Injury
There was no difference in chronic UE injury and sex; therefore, data from both sexes were pooled in the analysis. Chronic UE between group differences are reported in Table 4. The report of a chronic UE injury was significantly associated with age, with middle-aged individuals more often reporting a chronic UE injury than the younger or older participants, with all differences of small effect. Those who have played for more years, had higher skill level, played longer or more frequent sessions, played greater volume, or played on consecutive days were significantly more likely to report a chronic UE injury. No significant differences were found between the report of a chronic UE injury and perceived grip tightness, or participation in stretching or strengthening programs.
3.5. Relative Risk for Injury
The relative risk for a UE injury (overall, acute, and chronic) is reported for each significant variable in Table 5.
4. Discussion
4.1. General Overview
Playing PB poses a risk of UE injury. In the present study, 41% of participants self-reported a UE injury which is comparable to the 39% found by Myers and Hanks[10] and the 36.5% in recreational padel players (36.5%) found by Thomas et al.[20]. In contrast, data from ED databases show lower rates of UE injury, ranging from 26%[7] to 31%[3]. This discrepancy may be due to an underreporting in ED data, given that individuals with less severe injuries are less likely to seek urgent care.
In this study, an acute UE injury was 2.38 times more likely for those playing 2 hours or more hours per session and nearly 5 times more likely for those playing on consecutive days. The fatigue associated with playing longer sessions and on consecutive days may contribute to an acute injury. Using a tight grip during baseline shots resulted in a nearly 3-fold increase in acute injury. In tennis players, differences in muscle activation during the various phases of the two-handed volley and groundstrokes are reported, with more wrist stabilization required during the volley than groundstroke.[31] These finding should not immediately be generalized to PB, due to differences in the tennis racket and PB. The present study did not differentiate a one versus two handed shot. While it is possible that, in PB, a tight grip on baseline shots requires greater muscle activation than required and thus elevates the risk of acute injury, more research is needed to explain the injury risk related to grip tightness.
This study found 37.5% of participants reported a chronic UE injury, a finding consistent with the 39% found in a separate study of recreational PB players[32], but lower than the 63.2% reported among club tennis players[5]. The lighter pickleball, shorter paddle, and shorter shot distance might explain these differences.
4.2. Sex and Age
Sex was not different between those reporting or not reporting a UE injury. This is similar to studies in tennis[33,34]and badminton[6]. Middle-aged participants were more likely report a UE injury, in general, and a chronic UE injury, in particular. Using ED data, Changstrom[17] found a mean age of 37 years for non-PB racket/paddle-related injuries, while Forrester reported a mean age of 63 years for PB-related injuries[7]. However, neither study differentiated UE injuries by age. Among club tennis players, the prevalence of lateral epicondylagia was higher among middle-aged players than younger players and leveled off among older players[18]. It is possible that older PB players are more likely to stop play or reduce play frequency.
4.3. Skill Level and Play Behavior
In this study, a chronic UE injury was more common in the more highly skilled PB players. While Jørgensen[6] found no difference in overall injury rates between elite and recreational players, overuse injuries—particularly to the upper extremity—were significantly more common in elite players. There appears to be an interaction between skill level and play behaviors. Higher-skilled players were significantly more likely to play more frequently each week, spend over six hours playing, and participate on consecutive days compared to players with lower skill levels. These findings align with injury and play behavior in other racket/paddle sports, with studies of tennis players reporting higher injury rates among those who play longer sessions[18]. In padel players, a higher UE injury risk occurred among those who had higher playing volume[20]. Intuitively, one might expect that advanced players use superior techniques, which would reduce their injury risk. Indeed, studies of tennis players have demonstrated that advanced players utilized techniques that reduced joint upper extremity forces[23,35]. While increased playtime may foster skill development, it is also associated with a higher risk of chronic UE injury[18]. Therefore, it is plausible that volume of play, rather than skill level alone, plays a more critical role in the development of chronic UE injury among pickleball players. Further research is warranted to better understand the interplay between skill level, play volume, and injury risk.
4.4. Stretching and Strengthening
Over half (52.6%) of participants reported engagement in UE strengthening or stretching exercises at least 1–2 times per week, but no difference was found between participation and the report of UE injury. In this study, the most common UE strengthening and stretching exercises was free weights and general stretching, respectively. Reduced muscle length and joint range of motion (ROM) is associated with a greater injury risk[36]. Strengthening exercise should be tailored to meet sport-specific requirements[37]. While strengthening and stretching exercises are commonly recommended as part of training programs for racket/paddle sports players[38], the specific type and volume of strengthening and stretching exercise required for UE injury reduction has not been specified for PB.ften use
4.5. Grip and Injury
The association of a tight baseline grip with acute UE injury was not surprising, but the lack of association with chronic injury was surprising. Previous work has linked grip tightness with chronic injury in other racquet sports[21]. It is possible that the mechanics of pickleball, with its lighter ball and shorter racket, creates less UE tissue stress than tennis. Perhaps in PB, factors other than grip tightness, such as spin and grip pattern, influence UE injury. Future studies should investigate these variables.
A limitation in this study is self-reporting bias with the potential for participants to under- or over-report injury. While the definitions of acute and chronic UE injury were provided in the survey, participants may have misclassified their injury. While the survey method of data collection is common in racket/paddle sport-related injury studies, no medical provider confirmed the presence or absence of injury. The small sample size limits immediate generalization of results. However, the number of participants in this study is consistent with, or larger than other racket/paddle sport-related injury survey-based studies.
5. Conclusions
Among recreational PB players, the risk of UE injury is higher for those who play longer and more frequent sessions, and play on consecutive days. Additionally acute UE injuries are more likely when using a tight grip for baseline shots while chronic UE injuries are more common in individuals who have been playing for two or more years, play at a higher skill level, and play over six hours per week.
Author Contributions
June Hanks: Conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing – original draft, writing- review & editing, visualization, supervision, project administration. Betsy Myers: Validation, formal analysis, writing- original draft; writing-review & editing, visualization.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of The Unversity of Tennessee at Chattanooga (IRB #24-042, 3 July 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
The authors wish to acknowledge the valuable contributions by those who participated in this study. The authors thank Gabriel Aranda, Taylor Carroll, Chris Carter, Eli Fields, Emilie Guigou, Lilliana Hatch, Cristina Northcutt, Jensen Overbay, and Lainey Persinger for their assistance with this project.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Players, A.o.P. APP Pickleball Participation Report: Part Two; 2023 March; pp. 1-5.
- Pickleheads. Pickleball-Statistics. Available online: https://www.pickleheads.com/blog/pickleball-statistics (accessed on 24 May 2025).
- Herzberg, S.D.; Bowman, E.N.; Hill, K.L. Evaluation of Pickleball-Related Injuries at a Single Institution From 2017 to 2022. Orthop J Sports Med. 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Hannon, M.; Dorian, J.; Norwood, T. 424 Emergency Department Visits for Pickleball Injuries From 2017-2022. Ann Emerg Med. 2024, 84, S190. [Google Scholar] [CrossRef]
- Krueckel, J.; Dominik, S.; Julia, L.; Julian, F.; Johannes, W.; Leonard, A.; Rainer, M.; Volker, A.; and Fehske, K. Tennis Injuries Among German League Players: Investigating Patterns and Epidemiology of Acute and Chronic Injuries. J Sports Med. 2024, 15, 67–75. [Google Scholar] [CrossRef]
- Jørgensen, U.; Winge, S. Epidemiology of Badminton Injuries. Int J Sports Med. 1987, 8, 379–382. [Google Scholar] [CrossRef]
- Forrester, M.B. Pickleball-Related Injuries Treated in Emergency Departments. J Emerg Med.. 2020, 58, 275–279. [Google Scholar] [CrossRef]
- Weiss, H.; Dougherty, J.; DiMaggio, C. Non-fatal senior pickleball and tennis-related injuries treated in United States emergency departments, 2010-2019. Inj Epidemiol. 2021, 8, 34. [Google Scholar] [CrossRef]
- Ghattas, Y.S.; Zeblisky, P.; Cassinat, J.; Aceto, M.; Spindler, K.P.; Cannada, L.K. Pickleball-Related Fractures in the United States From 2002 to 2022: An Analysis Using the NEISS Database. Orthop J Sports Med. 2024, 12, 23259671241255674. [Google Scholar] [CrossRef]
- Myers, B.; Hanks, J. Overuse Injuries and Epicondylalgia in Recreational Pickleball Players. Int. J Racket Sports Sci. 2023, 5, 32–40. [Google Scholar] [CrossRef]
- Myers, B.A.; Hanks, J. Positive clinical tests for medial epicondylalgia are more common than tests for lateral epicondylalgia in recreational pickleball players: A cross-sectional study. J Hand Ther. 2025. [Google Scholar] [CrossRef]
- Kasper, A.A.; Gibbons, J.L.; Abboudi, J.; Aita, D.; Takei, T.R.; Fletcher, D.; Gallant, G.G.; Kwok, M.; Beredjiklian, P. Pickleball- and Paddleball-Related Injuries to the Upper Extremity. Cureus. 2023, 15, e39831. [Google Scholar] [CrossRef]
- Boroumand, S.; Nancy, P.; Beatrice, K.; Emily, Q.; Mackenzie, N.; Peter, J.; Fortunay, D.; Olivier, N.; Jay, M.; and Jimenez, A. The perils of pickleball: A two decade analysis of upper and lower extremity injuries from America’s fastest growing sport. J Sports Sci. 2025, 1–8. [Google Scholar] [CrossRef]
- Vitale, K.; Liu, S. Pickleball: Review and Clinical Recommendations for this Fast-growing Sport. Curr Sports Med Rep. 2020, 19, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, S.D.; Bowman, E.N.; Hill, K.L. Evaluation of Pickleball-Related Injuries at a Single Institution From 2017 to 2022. Orthop J Sports Med. 2025, 13, 23259671251316997. [Google Scholar] [CrossRef] [PubMed]
- Touhey, D.C.; Bozorgmehr, C.K.; Tartibi, D.S.; Smith, M.V.; Knapik, D.M.; Smith, M.; Knapik, D. Pickleball Injuries in the Aging Athlete: A Critical Analysis Review. Cureus. 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Changstrom, B.; McBride, A.; Khodaee, M. Epidemiology of racket and paddle sports-related injuries treated in the United States emergency departments, 2007-2016. Phys Sportsmed. 2022, 50, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Kitai, E.; Itay, S.; Ruder, A.; Engel, J.; Modan, M. An epidemiological study of lateral epicondylitis (tennis elbow) in amateur male players. Ann Chir Main. 1986, 5, 113–121. [Google Scholar] [CrossRef]
- Gruchow, H.W.; Pelletier, D. An epidemiologic study of tennis elbow. Incidence, recurrence, and effectiveness of prevention strategies. Am J Sports Med. 1979, 7, 234–238. [Google Scholar] [CrossRef]
- Thomas, E.; Giustino, V.; Ferrisi, E.; Patti, A.; Cassarino, M.; Drid, P.; Bianco, A. Incidence of injuries and associated risk factors in a sample of Italian recreational padel players. J Sports Med Phys Fitness. 2023, 63, 1324–1330. [Google Scholar] [CrossRef]
- King, M.A.; Kentel, B.B.; Mitchell, S.R. The effects of ball impact location and grip tightness on the arm, racquet and ball for one-handed tennis backhand groundstrokes. J Biomech. 2012, 45, 1048–1052. [Google Scholar] [CrossRef]
- Elliott, B.C. Tennis: the influence of grip tightness on reaction impulse and rebound velocity. Med Sci Sports Exerc. 1982, 14, 348–352. [Google Scholar] [CrossRef]
- Wei, S.-H.; Chiang, J.-Y.; Shiang, T.-Y.; Chang, H.-Y. Comparison of Shock Transmission and Forearm Electromyography Between Experienced and Recreational Tennis Players During Backhand Strokes. Clin J Sport Med. 2006, 16, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Jaggi, A.; Lambert, S. Rehabilitation for shoulder instability. Br J Sports Med 2010, 44, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Abrams, G.D.; Safran, M.R. Diagnosis and management of superior labrum anterior posterior lesions in overhead athletes. Br J Sports Med. 2010, 44, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Dines, J.S.; Bedi, A.; Williams, P.N.; Dodson, C.C.; Ellenbecker, T.S.; Altchek, D.W.; Windler, G.; Dines, D.M. Tennis injuries: epidemiology, pathophysiology, and treatment. J Am Acad Orthop Surg. 2015, 23, 181–189. [Google Scholar] [CrossRef]
- Hjelm, N.; Werner, S.; Renstrom, P. Injury risk factors in junior tennis players: a prospective 2-year study. Scand J Med Sci Sports 2012, 22, 40–48. [Google Scholar] [CrossRef]
- Liaghat, B.; Pedersen, J.R.; Husted, R.S.; Pedersen, L.L.; Thorborg, K.; Juhl, C.B. Diagnosis, prevention and treatment of common shoulder injuries in sport: grading the evidence - a statement paper commissioned by the Danish Society of Sports Physical Therapy (DSSF). Br J Sports Med. 2023, 57, 408–416. [Google Scholar] [CrossRef]
- Pickleball, U. Definitions of Player Skill Ratings. Available online: https://usapickleball.org/player-skill-rating-definitions/ (accessed on 3 March 2024).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences., 2nd ed.; Psychology Press: New York, 1988. [Google Scholar]
- Mu-Lin, T.; Chun-Ju, Y.; Wen-Tzu, T.; Elliott, B.; Kai-Lung, C. Upper Extremity Muscle Activation during Drive Volley and Groundstroke for Two-Handed Backhand of Female Tennis Players. J Sports Sci Med. 2022, 21, 586–594. [Google Scholar] [CrossRef]
- Myers, B.A.; Hanks, J. Overuse injuries and epicondylalgia in recreational pickleball players. Int. J Racket Sports Sci 2023, 5, 32–40. [Google Scholar] [CrossRef]
- Sallis, R.E.; Jones, K.; Sunshine, S.; Smith, G.; Simon, L. Comparing sports injuries in men and women. Int J Sports Med. 2001, 22, 420–423. [Google Scholar] [CrossRef]
- Winge, S.; Jorgensen, U.; Lassenm Nielsen, A. Epidemiology of injuries in Danish championship tennis. 1989, 10, 368-371. Int J Sports Med. 1989, 10, 368–371. [Google Scholar] [CrossRef]
- Lo, K.C.; Hsieh, Y.C. Comparison of Ball-And-Racket Impact Force in Two-Handed Backhand Stroke Stances for Different-Skill-Level Tennis Players. J Sports Sci Med. 2016, 15, 301–307. [Google Scholar] [PubMed]
- Small, K.; Mc Naughton, L.; Matthews, M. A Systematic Review into the Efficacy of Static Stretching as Part of a Warm-Up for the Prevention of Exercise-Related Injury. Res Sports Med. 2008, 16, 213–231. [Google Scholar] [CrossRef] [PubMed]
- Reilly, T.; Morris, T.; Whyte, G. The specificity of training prescription and physiological assessment: a review. J Sports Sci. 2009, 27, 575–589. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, M.S. Applied physiology of tennis performance. Brit J S Med. 2006, 40, 381–385. [Google Scholar] [CrossRef]
Figure 1.
Number and Location of Injuries by Type.
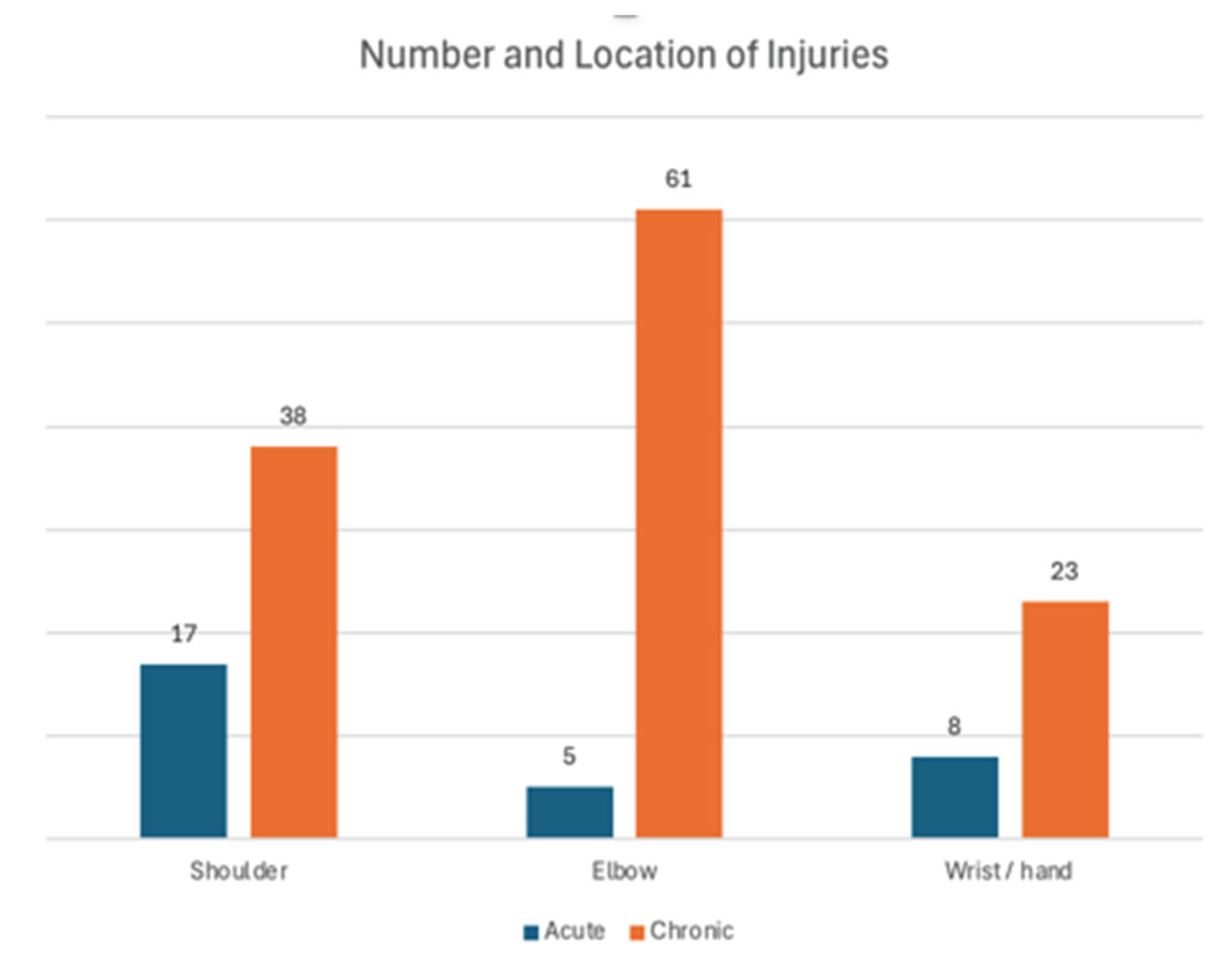

Table 1.
Frequency Data.
| Parameter | Category | N | % |
|---|---|---|---|
| Sex | Female Male Prefer not to say |
137 116 0 |
54.2 45.8 0 |
| Age | 18-34 35-64 >65 |
57 128 68 |
22.5 50.6 26.9 |
| Participants with at least one upper extremity injury | No Yes |
149 104 |
58.9 41.1 |
| Participants with at least one upper extremity acute upper extremity injury | No Yes |
226 27 |
89.3 10.7 |
| Participants with at least one chronic upper extremity injury | No Yes |
158 95 |
62.5 37.5 |
| Years of play |
<2 ≥2 |
113 140 |
44.7 55.3 |
| Skill level |
1.0 – 2.0 2.5-3.5 ≥4 Don’t know |
0 186 63 4 |
0 73 24.9 1.6 |
| Sessions/week |
≤3 ≥4 |
160 93 |
63.2 36.8 |
| Session length | ≤2hours >2 hours |
166 87 |
65.6 34.4 |
| Play volume/week |
≤6 hours ≥7 hours |
127 126 |
50.2 49.8 |
| Play on consecutive days | No Yes |
97 156 |
38 61.7 |
| Dink grip |
Sufficient Tight |
222 31 |
87.7 12 |
| Volley grip |
Sufficient Tight |
148 103 |
58.4 40.7 |
| Baseline grip | Sufficient Tight |
134 119 |
20.9 18.5 |
| Strengthening |
No Yes |
120 133 |
47.4 52.6 |
| Stretching |
No Yes |
120 133 |
47.4 52.6 |
Table 2.
Reported upper extremity injury: Between group differences.
| Variable | Category | No Injury | Injury | Statistic |
|---|---|---|---|---|
| Sex | Female Male |
85 64 |
52 52 |
Χ²(1)=1.225, p=.268 |
| Age | 18-34 35-64 ≥65 |
43 60 46 |
14 68 22 |
Χ²(2)=16.235, p=.0003* Cramer’s V=.253† |
| Years of play | <2 ≥2 |
74 75 |
39 65 |
Χ²(1)=3.667, p=.055 |
| Skill Level | ≤3.5 ≥4 |
115 31 |
71 32 |
Χ²(1)=3091, p=.079 |
| Session length | ≤2hours >2 hours |
108 41 |
58 46 |
Χ²(1)=7.584, p=.006*, phi=.173 |
| Sessions/week | ≥3 ≥4 |
105 44 |
55 49 |
Χ²(1)=8.148, p=.004*, phi=.179 |
| Play volume | ≤6 >6 |
82 67 |
45 59 |
Χ²(1)=3.391, p=.066 |
| Play on consecutive days | No Yes |
67 82 |
30 74 |
Χ²(1)=6.733, p=.009*, phi=.163 |
| Dink grip | Mod Tight |
124 22 |
95 8 |
Χ²(1)=3.038, p=.081 |
| Volley grip | Mod Tight |
91 55 |
55 48 |
Χ²(1)=1.986, p=.159 |
| Baseline grip | Mod Tight |
83 63 |
47 56 |
Χ²(1)=3.046 p=.081 |
| Strengthening | No Yes |
66 83 |
54 50 |
Χ²(1)=1.429, p=.232 |
| Stretching | No Yes |
72 77 |
48 56 |
Χ²(1)=.155, p=.734 |
†Pairwise comparisons of age groups: 18-34 years vs. 35-64 years, [x2(1)=13.039, p=.0003, phi=.265, adjusted residual 3.6 for mid, -3.6 for young]; 35-64 years vs. > 65 years [x2(1)=7.716, p=.005, phi=.198, AR for mid=2.8, older=-2.8]; and 18-34 years vs. > 65 years [x2(1)=.918, p=.338].
Table 3.
Reported acute injury: Between group differences.
| Parameter | Category | No Injury | Injury | Statistics |
|---|---|---|---|---|
| Age (in years) | 18-34 35-64 ≥65 |
53 110 63 |
4 18 5 |
Χ²(1)=3.128, p=.209 |
| Sex | Female Male |
120 106 |
17 10 |
Χ²(1)=.946, p=.331 |
| Years of PB play | <2 ≥2 |
102 124 |
11 16 |
Χ²(1)=.118, p=.664 |
| Skill Level | ≤3.5 ≥4 |
166 56 |
20 7 |
Χ²(1)=.006, p=.937 |
| Session Length | ≤2hours >2 hours |
154 72 |
12 15 |
Χ²(1)=6.003, p=.014, phi=.154 |
| Sessions/week | ≥3 ≥4 |
147 79 |
13 14 |
Χ²(1)=2.962, p=.085 |
| Play Volume | ≤6 >6 |
117 109 |
10 17 |
Χ²(1)=2.094, p=.148 |
| Play on Consecutive Days | No Yes |
94 132 |
3 24 |
Χ²(1)=9.479, p=.002, phi=.194 |
| Dink Grip |
Sufficient Tight |
197 29 |
25 2 |
Χ²(1)=.660, p=.417 |
| Volley Grip | Sufficient Tight |
136 90 |
17 13 |
Χ²(1)=.963, p=.405 |
| Baseline Grip | Sufficient Tight |
126 100 |
8 19 |
Χ²(1)=6.607, p=.010 phi=.162 |
| Strengthening | ≤2 >2 |
105 121 |
15 12 |
Χ²(1)=.800, p=.371 |
| Stretching | ≤2 >2 |
106 120 |
14 13 |
Χ²(1)=.237, p=.626 |
Table 4.
Chronic Upper Extremity Injury.
| Parameter | Category | No | Yes | Statistic |
|---|---|---|---|---|
| Sex | Female Male |
92 66 |
45 50 |
Χ²(1)=2.818, p=.093 |
| Age | 18-34 35-64 ≥65 |
45 65 48 |
12 | Χ²(2)=15.968, p=.0003 * Cramer’s V=.251† |
| Years of Play | <2 ≥2 |
102 79 |
34 61 |
Χ²(1)=4.847, p=.028*, phi=.138 |
| Skill level | ≤3.5 ≥4 |
123 32 |
63 31 |
Χ²(1)=4.710, p=.030*, phi=.138 |
| Session length | ≤2hours >2 hours |
113 45 |
53 42 |
Χ²(1)=6.506, p=.011*, phi=.160 |
| Sessions/week | ≥3 ≥4 |
112 46 |
48 47 |
Χ²(1)=10.579, p=.001*, phi=.204 |
| Play volume | ≤6 >6 |
88 70 |
39 56 |
Χ²(1)=5.089, p=.024*, phi=.142 |
| Play on consecutive days |
No Yes |
70 88 |
27 68 |
Χ²(1)=6.331, p=.012*, phi=.158 |
| Dink grip | Mod Tight |
136 22 |
86 9 |
Χ²(1)=1.093, p=.296 |
| Volley grip | Mod Tight |
100 58 |
50 45 |
Χ²(1)=2.793, p=.095 |
| Baseline grip | Mod Tight |
88 70 |
46 49 |
Χ²(1)=1.260 p=.262 |
| Strengthening | No Yes |
87 78 |
46 42 |
Χ²(1)=1.050, p=.306 |
| Stretching | No Yes |
78 80 |
42 53 |
Χ²(1)=.633, p=.426 |
* Significant difference, †Pairwise comparisons of age groups: 18-34 years vs. 35-64 years, [χ²(1)=12.979,p=.0003, phi=.265]; 35-64 years vs. ≥ 65 years [χ²(1)=7.136., p=.008, phi=.191]; and 18-34 years vs. ≥65 years [χ²(1)=1.138, p=.286].
Table 5.
Relative Risk for Injury.
| Variable | Relative Risk | Confidence Interval (95%) | |
|---|---|---|---|
| Upper extremity injury | Session length (≤2 vs. >2hours) | 1.51 | 1.136-2.017 |
| Sessions/week (≤3 vs. ≥4) | 1.53 | 1.149-2.044 | |
| Consecutive days | 1.53 | 1.091-2.155 | |
| Acute upper extremity injury | Session length (≤2 vs. >2hours) | 2.38 | 1.169 – 4.8677 |
| Consecutive days | 4.97 | 1.539-16.08 | |
| Baseline grip (Sufficient vs. Tight ) | 2.67 | 1.116- 5.0882 | |
| Chronic upper extremity injury | Years of Play (<2 vs. ≥2) | 1.45 | 1.0323 – 2.031 |
| Skill level (≤3.5 vs. ≥4) | 1.45 | 1.0535 – 2.0033 | |
| Session length (≤2 vs. >2 hours) | 1.55 | 1.111-2.169 | |
| Sessions/week (≤3 vs. ≥4) | 1.68 | 1.234-2.298 | |
| Play volume (≤ vs. >6 hours) | 1.45 | 1.045-2.005 | |
| Consecutive days | 1.57 | 1.085-2.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



