Submitted:
03 June 2025
Posted:
04 June 2025
You are already at the latest version
Abstract
Acute pancreatitis (AP) is an inflammatory disorder of the pancreas that can lead to serious systemic complications. Its clinical presentation varies widely, ranging from mild, self-limiting symptoms to severe, life-threatening illness. Currently, there are no specific therapies approved for the treatment of AP, and management primarily relies on supportive care. However, a growing number of clinical trials have evaluated the translational potential of effective therapies derived from experimental models and have identified promising pharmacological agents that may help ameliorate disease severity. Alongside pharmacological approaches, nutritional management of AP has been gaining increasing attention. Evidence supports the use of enteral nutrition over parenteral feeding, as it is associated with a lower risk of necrotic infections, multiple organ dysfunction, mortality, and other associated complications of AP. In this review, we summarize the therapeutic potential of pharmacological and dietary/nutritional interventions for AP in the context of its molecular pathology, with the aim of sup-porting improved clinical decision-making, enhancing patient outcomes, and inform-ing future research directions.
Keywords:
Acute pancreatitis
; Therapeutics
; Pharmacological agents
; Nutrition
; Probiotics
1. Introduction
Acute pancreatitis (AP) is a common and potentially lethal inflammatory condition of the pancreas[1], a vital glandular organ. It presents with varying degrees of severity and is classified accordingly (Table 1) (adapted with slight modifications from reference[2] ). Although regional variation exists[3], the global incidence of AP has alarmingly increased over the past few decades, rising by 59% between 1990 and 2021[4]. Currently, AP affects approximately 35 individuals per 100,000 population annually, equating to nearly 2.75 million people worldwide each year[4]. In the United States alone, AP results in over 255,000 hospitalizations annually, with associated healthcare costs exceeding US$2.5 billion[5]. Moderate to severe AP develops in approximately 20% of patients and carries a mortality rate of 20 to 40%[6,7], further contributing to the economic burden on the health care system. The etiology of AP is multifactorial, with gallstones, trauma, metabolic diseases, and alcohol consumption among the most common causes[8]. Before exploring the various treatment interventions for AP, it is essential to develop a comprehensive understanding of its molecular pathology, as outlined in the following paragraph.
Cellular events such as pathological Ca2+ overload[13,14], premature activation of digestive enzymes (e.g. trypsin) within acinar cells[15,16] and macrophages[17], endoplasmic reticulum stress[18,19], mitochondrial dysfunction[20,21,22], impaired autophagy[23,24,25,26], and gut microbiota dysbiosis[27,28] have all been implicated in the pathogenesis of AP. These processes contribute to a complex pathophysiological cascade that begins with acinar cell injury, activation of the immune system, and progression to systemic pathological responses (Figure 1). One of the early hallmarks is the premature intra-acinar activation of digestive zymogens, such as trypsin, mediated by enterokinase (Figure 1). This aberrant enzyme activation promotes pancreatic auto-digestion, leading to the release of pro-inflammatory mediators, including tumor necrosis-alpha (TNF-α), interleukin-1 beta (IL-1β), and IL-6, which in turn facilitate crosstalk between acinar and immune cells, further amplifying the inflammatory response[29,30,31]. Consequently, these inflammatory mediators disrupt the pancreatic microcirculation, resulting in increased vascular permeability, edema, hemorrhage and tissue necrosis[32,33,34] (Figure 1). Collectively, amplified inflammatory reactions, together with extensive acinar cell injury, contribute to the development of life-threatening systemic inflammatory response syndrome (SIRS)[35,36,37]. SIRS, in turn, leads to distinct organ damage and can progress to multiple organ dysfunction (MOD)[32] (Figure 1), which is ultimately responsible for AP-associated mortality[38].
Although current treatment approaches for AP remain suboptimal, advances in understanding its pathophysiology have driven research toward the development of novel pharmacological and nutritional strategies aimed at restoring organ and tissue homeostasis. Several pharmacological agents[39] have shown promise in targeting key mechanisms of this complex disorder. Alongside pharmacological approaches, the traditional bowl at rest (nothing by mouth) approach has been conventionally employed in the management of AP[2,40]. However, prolonged dietary restriction can exacerbate malnutrition by limiting nutrient intake at a time when the body’s metabolic demands are elevated[41]. This nutritional imbalance may lead to enhanced catabolism, resulting in excessive production of reactive oxygen species and subsequent oxidative stress[42]. These effects can disrupt the gut barrier, promoting bacterial translocation from the gastrointestinal tract to the bloodstream[43], which contributes to infected pancreatic necrosis and increases the risk of mortality[33,44]. Thus, both pharmacological and nutritional approaches such as probiotic and antioxidant therapies are equally crucial in the management of AP. Notably, both recent experimental[45,46] and clinical[47] studies suggest that probiotics could help restore disrupted intestinal homeostasis, potentially reducing bacterial translocation and the risk of secondary infection in AP. The present review summarizes the evidence on the therapeutic potential of pharmacological and nutritional strategies in the clinical management of AP in the hopes of supporting better clinical decision-making and patient outcomes.
2. Pharmaco-Nutritional Management of Clinical AP
Ongoing research into the pathophysiological course of AP has yielded promising evidence supporting both pharmacological and nutritional interventions to manage disease severity. In the following sections, these therapies have been discussed in detail.
3. Pharmacological Approaches
3.1. NSAID Therapy in Clinical AP
Non-steroidal anti-inflammatory drugs (NSAID) possess both analgesic and anti-inflammatory effects and are widely used in the treatment of various inflammatory diseases[48], including AP[49]. Most NSAIDs act as non-selective inhibitors of cyclooxygenase (COX) enzymes[48]. Among these, indomethacin and diclofenac are notable agents that can be conveniently administered as rectal suppositories. Although case reports have linked indomethacin to the development of AP[50], evidence also supports its potential protective role. In a study involving 117 patients undergoing endoscopic retrograde cholangiopancreatography (ERCP), prophylactic administration of indomethacin (100 mg) two hours prior to the procedure significantly reduced the incidence of post-ERCP hyperamylasemia (10.2 % vs. 16.2%) and AP (2.5% vs. 6.8%) compared to placebo[51]. This therapeutic benefit of indomethacin was further confirmed in a larger double blind, randomized trial involving 490 patients, where those who received a 100 mg indomethacin suppository immediately before ERCP experienced a significant reduction in the severity of post-ERCP pancreatitis (PEP)[52]. Moreover, recently, in a randomized clinical trial (ClinicalTrials.gov number, NCT00820612) of 602 patients, rectal indomethacin treatment significantly reduced the incidence of post-ERCP pancreatitis[53]. Pancreatitis developed in 27 of 295 patients (9.2%) in the indomethacin group vs in 52 of 307 patients (16.9%) in the placebo group (P=0.005). Similarly, moderate-to-severe pancreatitis developed in 13 patients (4.4%) in the indomethacin group compared with 27 patients (8.8%) in the placebo group (P=0.03).
The potential protective effects of the NSAID diclofenac have also been investigated. In a study of 220 patients, rectal administration of diclofenac (100 mg) was associated with a significantly lower frequency of PEP compared to placebo (6% vs. 15%; P=0.05)[54]. Additionally, a prospective randomized control trial involving 104 patients investigated the efficacy of a lower dose of diclofenac (50 mg, reduced to 25 mg in patients over 50 kg body weight[55]. This study reported that PEP pain was significantly reduced in the diclofenac group compared to the control group (7.8% vs. 37.7%; P=0.001), suggesting that even low-dose diclofenac may confer protective benefits. Furthermore, intramuscular administration of a single 75 mg dose of diclofenac was assessed in a study of 60 patients and was found to significantly reduce the incidence of PEP (P=0.032)[56]. Additionally, they observed a significant increase in the levels of lipoxin A4, resolvins D1 and E1 in the diclofenac-treated group compared to the control group (P<0.05), suggesting that this may underlie its protective effect. Recently, this therapeutic benefit of diclofenac was further supported by a larger retrospective study of 301 patients[57]. Although this clinical investigation, which utilized a low dose of 25 mg rectal diclofenac, did not observe a reduction in the incidence of PEP in patients with a native papilla and a body weight under 50 kg, it suggested that a higher dose of rectal NSAIDs, such as 100-mg, should be administered regardless of body weight to prevent PEP[57]. Taken together, the results from these trials support the beneficial role of NSAIDs —particularly indomethacin and diclofenac—in the prevention and attenuation of PEP.
3.2. Antibiotics Therapy in Clinical AP
Infected pancreatic necrosis is a major clinical complication that severely worsens prognosis and accounts for approximately 70% of all mortality in AP patients who survive the early phase[58]. The use of antibiotic prophylaxis and therapy in AP has long been debated[59] and current treatment guidelines advocate for minimal and judicious antibiotic usage[60,61]. Concerns against antibiotics arise mainly from the poor quality of underpowered randomized trials and the rising prevalence of multi-resistant organisms and fungal infections, although this is still disputed[62]. A 2004 double-blind, placebo-controlled trial involving 114 patients with AP in combination with a C-reactive protein level exceeding 150 mg/L and/or a CT-verified necrosis, found no significant difference in the incidence of infected pancreatic necrosis between the placebo group and those treated with ciprofloxacin (2 x 400 mg/day) and metronidazole (2 x 500 mg/day)[63].
Nevertheless, antibiotics offer the potential to prevent and/or treat infected necrosis, thereby reducing morbidity and mortality[64,65,66] . The efficacy of antibiotics depends on their ability to penetrate necrotizing pancreatic tissue, which varies among different antibiotic classes[67], and their activity against the specific bacteria commonly implicated in infected pancreatic necrosis. Given that both imipenem and quinolone demonstrate effective penetration into peripancreatic tissue and offer a broad spectrum of activity against probable pathogens, the selection of antibiotics is typically between them[64,68]. A Cochrane meta-analysis of five randomized controlled trials involving 294 AP patients with CT-verified pancreatic necrosis found that antibiotic prophylaxis significantly reduced mortality (odds ratio 0.37; 95% CI: 0.17-0.83), but not the incidence of infected pancreatic necrosis (odds ratio 0.62; 95% CI: 0.35-1.09)[69]. Sub-group analysis by antibiotic regimen showed that beta-lactams significantly reduced both mortality (odds ratio 0.34; 95% CI: 0.13-0.91) and infected pancreatic necrosis (odds ratio 0.41; 95% CI: 0.20-0.85), whereas quinolone plus imidazole combinations did not. Similarly, another Cochrane review of seven randomized studies involving 404 AP patients found no significant benefit of prophylactic antibiotics in reducing infection of pancreatic necrosis or mortality[70]. However, imipenem—a beta-lactam antibiotic—significantly reduced the rate of infected pancreatic necrosis (16.8% vs. 24.2%) without significantly affecting mortality. Furthermore, another study randomized 90 patients with acute necrotizing pancreatitis—defined by CT-confirmed necrosis and C-reactive protein levels >150 mg/L—within 48 hours to receive either imipenem (1.0 g plus cilastatin intravenously 3 times a day) or no antibiotic therapy. Early imipenem treatment significantly reduced the need for surgery and the overall incidence of major organ complications (P=0.0003)[71]. Collectively, these findings suggest that while the overall benefit of prophylactic antibiotics in AP remains inconclusive, beta-lactam antibiotics, particularly imipenem, demonstrate superior efficacy in reducing infected pancreatic necrosis, mortality, and major complications. However, to draw more definitive conclusions and determine the most effective antibiotic regimens, future research should prioritize larger, high-quality randomized clinical trials. Studies on prophylactic use of antibiotics prior to ERCP are limited. Nevertheless, a prospective study by Raty and colleagues[72] involving 321 patients found that administering 2 g of cephtazidime intravenously 30 minutes before ERCP significantly reduced the incidence of PEP compared to the control group (P=0.009). Based on these findings, prophylactic antibiotics may be considered for routine use prior to ERCP. The results also suggest a possible role of bacteria in the pathogenesis of PEP.
3.3. Cytokine and Immunomodulatory Therapy in Clinical AP
IL-10 is produced by regulatory immune cells and acts primarily as an anti-inflammatory cytokine[73,74]. Clinical studies have reported elevated IL-10 levels in patients with severe AP[75,76]. In a randomized study involving 144 patients, human recombinant IL-10 (4 μg/kg or 20 μg/kg) or placebo was administered 30 min prior to ERCP[77]. IL-10 administration significantly reduced the incidence of PEP compared to placebo (P=0.038). As the study controlled for variables such as age, sex, type of treatment, baseline cytokine levels, the authors concluded that IL-10 independently reduces the risk of PEP.
In addition to IL-10, the immunomodulatory monoclonal anti-TNF-α antibody infliximab, which neutralizes the effects of secreted TNF-α, has been investigated as a potential therapeutic agent in experimental AP[78,79]. TNF-α, produced by resident macrophages in the pancreas, is known to be elevated in the serum during AP[80,81]. In experimental models, blocking TNF-α mediated inflammation with anti-TNF-α antibodies or agents like pentoxifylline has shown beneficial effects on histological score and mortality[78,79,82]. However, clinical data are extremely limited. To date, only two case reports have described the use of infliximab in patients with AP. A recent case report involving a 48-year-old man with the extremely rare co-occurrence of colitis and AP investigated the therapeutic use of infliximab, administered at 5 mg/kg in three biweekly doses[83]. Treatment led to immediate clinical improvement, including resolution of diarrhea and hematochezia, normalization of pancreatic enzyme levels, and no recurrence of either condition. Similarly, an earlier case described a male patient with segmental Crohn’s disease presenting with severe bloody diarrhea who also developed interstitial AP[84]. Following a single infusion of infliximab, the patient experienced clinical improvement and normalization of serum amylase levels without complications. These reports highlight the potential of cytokine-targeting therapies, such as infliximab, in the treatment of AP. However, to validate these beneficial effects and determine efficacy and safety in broader patient populations, more well-designed clinical trials are urgently needed. Encouragingly, a randomized trial investigating infliximab for AP (study ID: NCT03684278) is currently underway in the UK[85].
Platelet activated factor (PAF) is a phosphoglyceride produced by endothelial cells, macrophages, neutrophils, and platelets[86] (Figure 1). It induces a broad range of physiological effects, including platelet aggregation, increased vascular permeability, leukocyte infiltration, edema, and tissue injury[87]. Alongside pro-inflammatory cytokines (IL-1β, IL-6, IL-8, TNF-α) and anti-inflammatory cytokines (IL-2, IL-10), PAF plays a key role in the pathogenesis of AP[88]. In experimental models, PAF antagonists have been shown to ameliorate the severity of AP[89,90,91].Based on these promising preclinical results, numerous clinical studies have been conducted to evaluate the effect of PAF inhibition in AP[92].
Lexipafant is one of the most potent PAF antagonists and has been shown to reduce both local and systemic inflammation associated with AP[89]. Clinical findings suggest that lexipafant could significantly reduce the incidence of pseudocysts, systemic sepsis and deaths when administered within the first 48 hours of AP symptom onset[93]. The first clinical trial to assess the effi cacy of lexipafant was a randomized, double-blind study involving 83 AP patients who received either placebo or lexipafant at a dose of 60 mg/day intravenously for three days[94]. The inflammatory response over days 1-5 was assessed by measuring IL-8, IL-6, E-selectin, C-reactive protein, and polymorphonuclear elastase-α (1)-antitrypsin. The lexipafant group showed a greater reduction in organ failure (P=0.041), IL-8 (P=0.038), and IL-6 levels. These effects were further confirmed in another clinical trial in which patients received lexipafant (100 mg/day) or placebo for 5-7 days. A significant reduction in OFS was observed in the treatment group (P=0.003), along with trends toward fewer systemic complications and reduced mortality[95]. However, despite these early promising results, a larger, more definitive multicenter phase III trial failed to demonstrate any benefit of lexipafant in reducing organ failure or mortality in patients with severe AP, suggesting it is unlikely to be effective as a standalone therapy for severe AP[96].
Drotrecogin alfa (Xigris) is a 55 kDa glyco protein analog of endogenous activated protein C[97,98]. Endogenous protein C is a vitamin K-de pendent glycoprotein synthesized by the liver that inhibits thrombin formation and facilitates thrombolysis[99]. Low levels of activated protein C are associated with a higher risk of mortality in AP and are thought to influence disease progression by modulating immune and inflammatory responses[100]. Proposed mechanisms of action include regulation of leukocyte-endothelial interactions and mitogen-activated kinases, improvement of intestinal microcirculation, and reduction of bacterial translocation through mesenteric lymph nodes[101]. Several experimental models of AP treated with activat ed protein C have demonstrated improved pancreatic histology, decreased infection rates, and lower systemic in flammatory markers[102,103,104]. In clinical settings, drotrecogin alfa has shown potential benefits in the treatment of severe AP and its associated septic complications. The first clinical evaluation in 2004 involved two patients who developed severe sepsis during AP, with treatment resulting in interruption of the severe sepsis cascade and improved organ function[105]. In contrast, a randomized, double-blind study involving 32 patients with severe AP found that intravenous administration of activated protein C (24 µg/kg/h for 96 h) did not result in a significant difference in MOD compared to placebo[100]. Moreover, due to concerns about the potential risk of pancreatic hemorrhage in this population, a prospective safety study was conducted in 166 consecutively admitted patients, of whom 43 met screening criteria and 19 were recruited[106]. In this study, intravenous administration of Drotrecogin alfa (24 µg/kg/h for 24 h) appeared to be safe. Separately, a large randomized, double-blind, placebo-controlled multicenter phase III trial involving 1690 patients with severe sepsis found that Drotrecogin alfa significantly reduced the relative mortality risk by 19.4% (95% CI, 6.6 – 30.5), and the absolute risk by 6.1% (P=0.005), although it was associated with a trend toward increased bleeding compared to placebo (P=0.06)[107]. Collectively, these mixed findings underscore the urgent need for larger, well-designed clinical trials to further evaluate the safety, efficacy, and therapeutic potential of Drotrecogin alfa in patients with severe AP.
4. Nutritional Approaches
4.1. Nutrition Therapy in Clinical AP
Historically, AP patients were managed by a nothing by mouth (NBM) strategy to rest the pancreas[108]. Most clinical guidelines recommended withholding oral intake until resolution of abdominal pain, while some also suggested waiting for normalization of pancreatic enzyme levels[109,110,111]. This long-held assumption—that pancreatic rest through fasting promotes recovery in AP—has been increasingly challenged by both experimental and clinical evidence[112,113]. Indeed, in AP, intestinal barrier dysfunction—combined with bacterial overgrowth due to impaired gut motility and systemic immunosuppression—promotes bacterial translocation, leading to pancreatic tissue necrosis and infection, and the development of MODS[33,43,44,114]. Maintaining gut barrier integrity is a central therapeutic goal in the management of AP[27,115,116]. For this reason, in AP, nutritional support has been proposed to help prevent morphological deterioration of the intestinal lining and restore gut function[2,117]. The metabolic response in AP[118,119] closely resembles that seen in severe sepsis or trauma[120,121], characterized by increased protein catabolism, persistent gluconeogenesis despite exogenous glucose administration, elevated energy expenditure, insulin resistance, and increased dependence on fatty acid oxidation for energy. These metabolic alterations, combined with the dynamic clinical course of AP, mean that energy and nutrient requirements vary depending on disease severity, stage, patient comorbidities, and complications[122]. Thus, nutritional support is essential. Table 2 summarizes the various forms of nutritional therapy and their protective roles across the clinical spectrum of AP, as well as the effectiveness of the two main forms of nutrient delivery: enteral nutrition, which involves the delivery of nutrients directly to the gastrointestinal tract, and parenteral nutrition, which provides nutrients intravenously, bypassing the gastrointestinal tract. Total enteral nutrition is able to attenuate the acute-phase response—as evidenced by reductions in serum C-reactive protein, IgM anti-endotoxin antibodies, and improvements in total antioxidant capacity—and to improve clinical outcomes by mitigating disease severity[123]. Enteral feeding could also maintain the gut mucosal barrier and hinder bacterial translocation, thereby limiting the risk of infection in pancreatic necrosis[124,125]. Multiple studies (as summarized in Table 2) have demonstrated that early oral feeding during the course of AP is associated with shorter hospital stays, decreased infectious complications, and lower morbidity and mortality. In contrast, while a small percentage of AP patients will still need a parenteral nutrition, total parenteral nutrition is not recommended for patients with either mild or severe AP[125], as numerous randomized controlled trials have linked total parenteral nutrition to increased risks of infection and other closely related complications.
To optimize nutritional support, several studies have also explored the use of immune-enhanced nutritional formulations, such as those enriched with omega-3 fatty acids, which have shown improved outcomes compared to traditional nutritional regimens[126,127]. Within this context, a meta-analysis of randomized controlled trials[128] concluded that, when use as part of parenteral nutrition, ω-3 FA is beneficial in reducing the risk of mortality, infectious complications, and length of hospital stay.

Table 2.
Nutritional therapeutic management of clinical AP.
| Nutrition | Study design | N | Protective role(s) in clinical AP | Conclusion |
| EEN vs. ODN[129] |
RCT | 208 | ■ infection (25% vs. 26%), ↓ death (11% vs. 7%) | EEN showed no significant advantage over ODN in ↓ infection and mortality rates |
| EEN vs. DEN[130] |
PCT, RCT | 60 | ■ IAP, ↓ IAH, beneficial for patients with an IAP <15 mmHg, ■ mortality | EEN prevents IAH and ↓ the severity of severe AP compared with DEN |
| SD vs. CLD[131] |
RIT | 60 | (*)↓ hospitalization stay, (*)↓ post-refeeding length of hospitalization | A SD as the initial meal in patients with mild AP is well tolerated and ↓ length of hospitalization |
| EEN vs. DEN[132] |
HCS | 197 | ↓ pancreatic necrosis (4 vs.18), ↓ respiratory failure and transfer to intensive care unit occurred (5 vs. 15), ↓ (9 vs. 16), ↓ surgery (7 vs. 11), (*)↓ mortality (0 vs. 9) | EEN started within 48 hrs of admission improves clinical outcomes via reducing complications |
| TEN vs. TPN[133] |
RCT | 107 | (*) ↓ MOF (21% vs. 80%), (*)↓ surgery (22% vs. 80%), (*)↓ pancreatic septic necrosis (23% vs. 72%), (*)↓ mortality (11% vs. 43%). | TEN is better than TPN in preventing pancreatic necrotic infection |
| EN vs. TPN[134] |
PCT, RCT | 50 | (*) ↓ serum CRP, (*) ↑ serum albumin, (*) ↑transferrin value, ■ surgery (56% vs. 60%), ■ infective complications (64% vs. 60%), ■ hospital stay, ■ mortality (20% vs. 16%) |
EN is comparable to PNT in terms of hospital stay, need for surgical intervention, infections and mortality |
| EIN vs. TPN[135] |
HCS | 76 | ↓ severity, ↑ intestinal permeability, ↑ clinical outcomes | Improved clinical outcomes with EIN compared to TPN |
| TEN vs. TPN[136] |
PRT | 22 | ■ APACHE II score, CRP, TNF-a, IL-6, pre-albumin and albumin levels, ↓ severe complications, ■ surgery, ■ hospital stay | TEN tends to be associated with a better outcome compared to TPN |
| TEN vs. TPN[137] |
RCT | 466 | (*)↓pancreatic infectious complications (7 vs. 16), ↓ MOF (7 vs. 17), (*)↓overall mortality 2 vs.12) | Early TEN could be used as prophylactic therapy for infected pancreatic necrosis |
| TEN +Abx vs. TPN+Abx[138] | PNR | 87 | ↓ MOF (31% vs.79%), ↓ surgery (25% vs. 88%), ↓ pancreatic necrosis infection (20% vs. 74%), (*) ↓ death rate (5% vs. 35%) | TEN could be used as a prophylactic therapy for infected pancreatic necrosis |
| EN vs. PN[139] |
RCT | 728 | ↓ CRP, ■ cholecystokinin levels, ↓ mortality, ↓ infected pancreatic necrosis, ↓ cost | EN tends to be associated with fewer septic complications, quicker inflammation reduction, and greater cost-effectiveness compared to PN |
| EN+PN vs. TPN[140] | RCT | 96 | ↑ body weight and prealbumin, ↓ APACHE II, ↓TNF-a, ↓ IL-6, ↓ serum CRP, ■ albumin, ■ pancreatic lesions, ■ endotoxin and lactulose/manicol of urine, (*)↑ CD4:CD8 T-cells and IgG | Combined therapy of EN and PN may be better than TPN as it improves nutrition status, moderates inflammation, and protects the gut integrity and immunity more effectively |
| TEN vs. TPN[141] |
RCT | 17 | ↓ fatigue, ■ oxidative stress, ■ plasma glutamine, ↓ respiratory failure, ↓ hospital stay, ↓ cost |
TEN is as safe and as efficacious as TPN |
| TEN vs. TPN[142] |
RCT | 156 | ↓ feeding duration, ↓nutrition costs, (*) ↓ nutritional requirements, (*) ↓ metabolic and septic complications | TEN seems to be safer and less expensive than TPN |
| TEN vs. TPN[143] |
RCT | 89 | (*) ↓ septic complications, ↓ MOF, ↓ mortality | EEN in combination with abx prophylaxis may prevent MOF |
■, no effect; *results are significant; ↑, increase/higher; ↓, decrease/lower; TEN, total enteral nutrition; TPN, total parenteral nutrition; EEN, early enteral nutrition; DEN, delayed enteral nutrition; EIN, eco immune nutrition; SD, solid diet; CLD, clear liquid diet; ODN, on demand nutrition; FA, Fatty acids; Abx, antibiotics; Ctl, control; vs., comparison; RCT, randomized control trial; PCT, pilot/prospective clinical trial; HCS, hospital conducted study; PRT, prospective randomized trial; PNR, prospective non-randomized; RIT, randomized interventional trial; MOF, multiple organ failure; IAP, intra-abdominal pressure; IAH, intra-abdominal hypertension; CRP, C-reactive protein; APACHE II, Acute physiology and chronic health evaluation II; sTNFRI, soluble tumour necrosis factor receptor I.
4.2. Antioxidant Therapy in Clinical AP
Oxidative stress plays a significant pathological role in AP, closely linked to the systemic inflammatory response[144]. Hypo-oxygenated pancreatic tissues and polymorphonuclear leukocytes generate ROS, which can further infiltrate and damage the inflamed pancreas[145]. Clinical studies have demonstrated that blood levels of antioxidants are depleted during AP, with lower levels correlating with increased disease severity[146,147]. Antioxidants such as n-acetylcysteine (NAC), methionine, beta-carotene, selenium, ascorbic acid, and α-tocopherol form a heterogeneous group of agents that modulate the inflammatory response and may help mitigate oxidative tissue damage in inflammatory diseases[148,149,150]. Clinical trials assessing these agents support the role of ROS in pancreatic cellular injury and highlight the therapeutic potential of antioxidant supplementation in AP. One randomized clinical trial evaluated the combined protective effects of NAC (200 mg every 8 hours), vitamin C (500 mg every 8 hours), and antoxyl forte (1 capsule every hour) in AP[151]. The intervention led to a significant reduction in oxidative stress markers (thiobarbituric acid reactive substances and superoxide dismutase), alongside a marked increase in serum antioxidant levels and total antioxidant capacity. The authors further hypothesized that antioxidant supplementation may decrease the hospital stay duration and complication rates in AP patients. Further research is warranted to explore the role of antioxidant therapy as a potential therapeutic target in this context.
Moreover, glutamine, a potent antioxidant, is an important constituent of both intra- and extracellular amino acid pools and plays an essential role in the development and function of immune cells[152,153]. Its depletion has been demon strated in critically ill patients[154]. A meta-analysis of 12 randomized controlled trials of glutamine supplementation in AP showed a mortality benefit and a significant reduction in infectious complications, although no significant difference was observed in length of hospital stay[155]. These findings are supported by another meta-analysis conducted by Jeurnink and colleagues[156], which concluded that glutamine treatment may offer potential benefits for AP patients. Furthermore, early administration (initiated on the day of admission) of alanyl-glutamine dipep tide in cases of severe AP has been associated with statistically significant improvements in key clinical outcomes, including duration of hospitalization, rate of infection, organ dysfunction, need for surgery and mortality, when compared to delayed treatment initiated five days after admission[157]. Collectively, these studies indicate that glutamine may represent a promising adjunctive therapy in the management of AP.
4.3. Probiotic Therapy in Clinical AP
Changes in intestinal motility, microbiome composition[43], immune response[29], and mucosal barrier function[114] contribute to bacterial translocation[158]—primarily involving Gram-negative strains— which can lead to pancreatic necrosis infection. The exact pathomechanisms and specific routes of this translocation, though remain incompletely understood, are actively being investigated[159,160]. Definitive evidence is also lacking regarding whether bacteria predominantly originate from the colon or the small bowel. Nevertheless, the recognized role of bacterial translocation in the progression of AP has prompted several studies to explore the therapeutic potential of probiotics in reducing necrotic infection. Oral probiotics are living microorganisms that confer health benefits beyond basic nutrition by restoring gut integrity, modulating immune responses to invading pathogens, and inhibiting the proliferation of harmful bacteria[161,162].
A recent review of experimental studies suggests that probiotics and/or probiotic food may plausibly diminish bacterial translocation and thereby decrease the risk of infectious complications in AP[163]. These findings have been further supported by clinical evidence. For example, a prospective randomized trial involving 66 patients with severe AP compared standard EN (N=32) to EN combined with Bifidobacterium quadruplex live bacterial tablets (N=34)[164]. Probiotic supplementation was associated with significant reductions in inflammatory markers such as IL-6, TNF-α, and C-reactive protein (P<0.05 for all inflammatory markers), as well as clinical improvements including relief of abdominal pain, alleviation of pancreatic edema, and shorter hospital stays (P<0.05 for all outcomes)[164]. In another placebo-controlled, double-blind clinical study of 64 AP patients, a combination of Bacillus subtilis and Enterococcus faecium was evaluated[47]. Although no difference in recurrent abdominal pain was observed between the probiotic and control groups, the probiotic-treated group showed a statistically significant reduction in the time to abdominal relief (P<0.01), time to successful oral feeding (P<0.01), and length of hospital stay (5.36 ± 0.15 v.s 6.02 ± 0.17 d, P<0.05). A prior randomized clinical trial involving 22 patients with AP demonstrated that Leuconostoc plantarum 299, administered at a dose of 1×109 organisms twice daily for one week alongside oat fibre, significantly reduced pancreatic sepsis and the number of surgical interventions related to pancreatic damage[165]. Additionally, a placebo-controlled double-blind study of 62 patients with severe AP also evaluated a combination of four probiotic strains (L. mesenteroides, L. plantarum, L. paracasei, Pediococcus pentosaceus) at a dose of 1×1010 colony forming units administered once daily for one week along with prebiotics containing four bioactive fibers (inulin, beta-glucan, resistant starch and pectin)[166]. This intervention resulted in a statistically significant reduction in SIRS and multiple organ failure (MOF) compared to the control group receiving only prebiotic feeding (P<0.05), suggesting a protective role of probiotics against organ dysfunction in severe AP. Moreover, Ecologic 641, a multispecies probiotic preparation containing L. casei, L. salivarius, L. acidophilus, L. lactis, B. bifidum, and B. lactis, was shown to significantly increase levels of the anti-inflammatory cytokine IL-10 and decrease levels of the pro-inflammatory cytokine IL-2, compared to its individual components[167]. These findings further suggest that probiotics may help modulate inflammation in AP. Furthermore, the administration of synbiotics (L. mesenteroides, L. plantarum, L. paracasei, P. pentosaceus at a dose of 1×1010 organisms combined with dietary fibers) in 90 patients with severe AP significantly reduced the rate of pancreatic necrosis infection, the need for surgical interventions, and the length of hospital stay, suggesting that early, low-volume enteral oral synbiotic supplementation could potentially be incorporated into routine treatment protocols for AP[168]. Thus, the current data support the therapeutic potential of probiotic administration in patients with AP.
5. Conclusions
The global incidence of AP continues to rise, posing a significant healthcare burden. Recent advances in understanding the cellular and molecular mechanisms of AP in animal models have led to the identification of promising pharmacological agents, some of which have shown beneficial effects in clinical settings. These pharmacological interventions aim to prevent or treat pancreatic necrosis, multiple organ dysfunction syndrome, and infection of necrotic pancreatic tissue. In parallel, nutritional support has emerged as a key component in the management of AP. Evidence consistently supports the use of enteral nutrition over parenteral nutrition, as it is associated with reduced mortality, fewer infectious complications, and a lower incidence of MOF. Importantly, the first 24–48 hours after symptom onset represent a critical interventional window during which inflammatory processes can be effectively targeted, potentially improving clinical outcomes. Nonetheless, it is essential to recognize that pharmacological and nutritional therapies are only components of a comprehensive, multimodal treatment approach. As summarized in this review, several therapeutic agents under investigation may provide a foundation for future treatments. Looking ahead, it is essential to conduct further studies and to establish international observational registries involving AP patients. Such a globally coordinated effort would offer a robust platform for evaluating emerging therapies and improving care for this complex and often life-threatening condition.
Author Contributions
M.S.; conceptualization, literature search, writing—original draft preparation, writing—review and editing, and artwork; S.A.; literature search, writing—review and editing, and artwork; S.N.; literature search, artwork; P.N.S.; supervision, and writing—review and editing; R.W.L.; funding acquisition, supervision, and writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
“This research received no external funding”.
Institutional Review Board Statement
This study did not require ethical approval.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
Abbreviations
The following abbreviations are used in this manuscript:
AP, Acute pancreatitis
TOF, transient organ failure
POF, persistent organ failure
EPC, exacerbation of pre-exiting comorbidity
N/A, not applicable
SOFA, sepsis-related organ failure assessment
TNF-α, tumor necrosis-alpha
IL, interleukin
SIRS, systemic inflammatory response syndrome
MOD, multiple organ dysfunction
Iκ, I kappa
NF-κB, nuclear factor kappa B
PAF, platelet-activating factor
Neut., neutrophils
Baso., basophils
Dendt., dendritic cell
Mon., monocytes
Macr., macrophages
Plt., platelet
Mast., mast cell
REL, proto-oncogne
P, phosphorylation
Ub, ubiquitination
NSAID, non-steroidal anti-inflammatory drugs
ERCP, endoscopic retrograde cholangiopancreatography (ERCP)
PEP, post-ERCP pancreatitis
NBP, nothing by mouth
TEN, total enteral nutrition
TPN, total parenteral nutrition
EEN, early enteral nutrition
DEN, delayed enteral nutrition
EIN, eco immune nutrition
SD, solid diet
CLD, clear liquid diet
ODN, on demand nutrition
FA, Fatty acids
Abx, antibiotics
Ctl, control
vs., comparison
RCT, randomized control trial
PCT, pilot/prospective clinical trial
HCS, hospital conducted study
PRT, prospective randomized trial
PNR, prospective non-randomized
RIT, randomized interventional trial
MOF, multiple organ failure
IAP, intra-abdominal pressure
IAH, intra-abdominal hypertension
CRP, C-reactive protein
APACHE II, Acute physiology and chronic health evaluation II
sTNFRI, soluble tumour necrosis factor receptor I.
NAC, n-acetylcysteine
ROS, reactive oxygen species
References
- Lee, P.J.; Papachristou, G.I. New Insights into Acute Pancreatitis. Nat Rev Gastroenterol Hepatol 2019, 16, 479–496. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.-L.; Li, J.; Shamoon, M.; Bhatia, M.; Sun, J. Recent Advances on Nutrition in Treatment of Acute Pancreatitis. Front. Immunol. 2017, 8, 762. [Google Scholar] [CrossRef] [PubMed]
- Iannuzzi, J.P.; King, J.A.; Leong, J.H.; Quan, J.; Windsor, J.W.; Tanyingoh, D.; Coward, S.; Forbes, N.; Heitman, S.J.; Shaheen, A.-A.; et al. Global Incidence of Acute Pancreatitis Is Increasing Over Time: A Systematic Review and Meta-Analysis. Gastroenterology 2022, 162, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Qin, C.; Zhao, B.; Li, Z.; Zhao, Y.; Lin, C.; Wang, W. Global and Regional Burden of Pancreatitis: Epidemiological Trends, Risk Factors, and Projections to 2050 from the Global Burden of Disease Study 2021. BMC Gastroenterology 2024, 24, 398. [Google Scholar] [CrossRef]
- Peery, A.F.; Murphy, C.C.; Anderson, C.; Jensen, E.T.; Deutsch-Link, S.; Egberg, M.D.; Lund, J.L.; Subramaniam, D.; Dellon, E.S.; Sperber, A.D.; et al. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: Update 2024. Gastroenterology 2025, 168, 1000–1024. [Google Scholar] [CrossRef]
- Schepers, N.J.; Bakker, O.J.; Besselink, M.G.; Ahmed Ali, U.; Bollen, T.L.; Gooszen, H.G.; van Santvoort, H.C.; Bruno, M.J. Dutch Pancreatitis Study Group Impact of Characteristics of Organ Failure and Infected Necrosis on Mortality in Necrotising Pancreatitis. Gut 2019, 68, 1044–1051. [Google Scholar] [CrossRef]
- Bang, J.Y.; Wilcox, C.M.; Arnoletti, J.P.; Varadarajulu, S. Superiority of Endoscopic Interventions over Minimally Invasive Surgery for Infected Necrotizing Pancreatitis: Meta-analysis of Randomized Trials. Digestive Endoscopy 2020, 32, 298–308. [Google Scholar] [CrossRef]
- Weiss, F.U.; Laemmerhirt, F.; Lerch, M.M. Etiology and Risk Factors of Acute and Chronic Pancreatitis. Visc Med 2019, 35, 73–81. [Google Scholar] [CrossRef]
- Bradley, E.L. A Clinically Based Classification System for Acute Pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993, 128, 586–590. [Google Scholar] [CrossRef]
- Colvin, S.D.; Smith, E.N.; Morgan, D.E.; Porter, K.K. Acute Pancreatitis: An Update on the Revised Atlanta Classification. Abdom Radiol (NY) 2020, 45, 1222–1231. [Google Scholar] [CrossRef]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Acute Pancreatitis Classification Working Group Classification of Acute Pancreatitis--2012: Revision of the Atlanta Classification and Definitions by International Consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, E.P.; Forsmark, C.E.; Layer, P.; Lévy, P.; Maraví-Poma, E.; Petrov, M.S.; Shimosegawa, T.; Siriwardena, A.K.; Uomo, G.; Whitcomb, D.C.; et al. Determinant-Based Classification of Acute Pancreatitis Severity: An International Multidisciplinary Consultation. Ann Surg 2012, 256, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Liu, G.; Shi, N.; Tang, D.; Ferdek, P.E.; Jakubowska, M.A.; Liu, S.; Zhu, X.; Zhang, J.; Yao, L.; et al. A microRNA Checkpoint for Ca2+ Signaling and Overload in Acute Pancreatitis. Molecular Therapy 2022, 30, 1754–1774. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.; Voronina, S.; Javed, M.A.; Awais, M.; Szatmary, P.; Latawiec, D.; Chvanov, M.; Collier, D.; Huang, W.; Barrett, J.; et al. Inhibitors of ORAI1 Prevent Cytosolic Calcium-Associated Injury of Human Pancreatic Acinar Cells and Acute Pancreatitis in 3 Mouse Models. Gastroenterology 2015, 149, 481–492.e7. [Google Scholar] [CrossRef]
- Geisz, A.; Sahin-Tóth, M. A Preclinical Model of Chronic Pancreatitis Driven by Trypsinogen Autoactivation. Nat Commun 2018, 9, 5033. [Google Scholar] [CrossRef]
- Modenbach, J.M.; Möller, C.; Asgarbeik, S.; Geist, N.; Rimkus, N.; Dörr, M.; Wolfgramm, H.; Steil, L.; Susemihl, A.; Graf, L.; et al. Biochemical Analyses of Cystatin-C Dimers and Cathepsin-B Reveals a Trypsin-Driven Feedback Mechanism in Acute Pancreatitis. Nat Commun 2025, 16, 1702. [Google Scholar] [CrossRef]
- Sendler, M.; Weiss, F.-U.; Golchert, J.; Homuth, G.; Van Den Brandt, C.; Mahajan, U.M.; Partecke, L.-I.; Döring, P.; Gukovsky, I.; Gukovskaya, A.S.; et al. Cathepsin B-Mediated Activation of Trypsinogen in Endocytosing Macrophages Increases Severity of Pancreatitis in Mice. Gastroenterology 2018, 154, 704–718.e10. [Google Scholar] [CrossRef]
- Yan, C.; Ma, Y.; Li, H.; Cui, J.; Guo, X.; Wang, G.; Ji, L. Endoplasmic Reticulum Stress Promotes Caspase-1-Dependent Acinar Cell Pyroptosis through the PERK Pathway to Aggravate Acute Pancreatitis. International Immunopharmacology 2023, 120, 110293. [Google Scholar] [CrossRef]
- Zhang, X.; Xu, C.; Ji, L.; Zhang, H. Endoplasmic Reticulum Stress in Acute Pancreatitis: Exploring the Molecular Mechanisms and Therapeutic Targets. Cell Stress Chaperones 2025, 30, 119–129. [Google Scholar] [CrossRef]
- Mukherjee, R.; Mareninova, O.A.; Odinokova, I.V.; Huang, W.; Murphy, J.; Chvanov, M.; Javed, M.A.; Wen, L.; Booth, D.M.; Cane, M.C.; et al. Mechanism of Mitochondrial Permeability Transition Pore Induction and Damage in the Pancreas: Inhibition Prevents Acute Pancreatitis by Protecting Production of ATP. Gut 2016, 65, 1333–1346. [Google Scholar] [CrossRef]
- Javed, M.A.; Wen, L.; Awais, M.; Latawiec, D.; Huang, W.; Chvanov, M.; Schaller, S.; Bordet, T.; Michaud, M.; Pruss, R.; et al. TRO40303 Ameliorates Alcohol-Induced Pancreatitis Through Reduction of Fatty Acid Ethyl Ester-Induced Mitochondrial Injury and Necrotic Cell Death. Pancreas 2018, 47, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Ren, Y.; Wang, T.; Wang, M.; Xu, Y.; Zhang, J.; Bi, J.; Wu, Z.; Zhang, Y.; Wu, R. Blocking CIRP Protects against Acute Pancreatitis by Improving Mitochondrial Function and Suppressing Pyroptosis in Acinar Cells. Cell Death Discov. 2024, 10, 156. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhang, T.; Ergashev, A.; Bo, Z.; Wang, J.; Shi, F.; Pan, Z.; Xie, H.; Chen, G.; Ma, F.; et al. CIP2A Inhibitors TD52 and Ethoxysanguinarine Promote Macrophage Autophagy and Alleviates Acute Pancreatitis by Modulating the AKT-mTOR Pathway. Phytomedicine 2025, 136, 156263. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.C.C.; Koike, M.K.; Barbeiro, D.F.; Soriano, F.G. Fasting-Induced Autophagy Reduces the Severity of Acute Pancreatitis in a Rodent Model. Journal of Gastrointestinal Surgery 2024, 28, 2116–2117. [Google Scholar] [CrossRef]
- Kong, L.; Deng, J.; Zhou, X.; Cai, B.; Zhang, B.; Chen, X.; Chen, Z.; Wang, W. Sitagliptin Activates the P62–Keap1–Nrf2 Signalling Pathway to Alleviate Oxidative Stress and Excessive Autophagy in Severe Acute Pancreatitis-Related Acute Lung Injury. Cell Death Dis 2021, 12, 928. [Google Scholar] [CrossRef]
- Ji, L.; Wang, Z.; Zhang, Y.; Zhou, Y.; Tang, D.; Yan, C.; Ma, J.; Fang, K.; Gao, L.; Ren, N.; et al. ATG7-Enhanced Impaired Autophagy Exacerbates Acute Pancreatitis by Promoting Regulated Necrosis via the miR-30b-5p/CAMKII Pathway. Cell Death Dis 2022, 13, 211. [Google Scholar] [CrossRef]
- Chen, X.; Chen, X.; Yan, D.; Zhang, N.; Fu, W.; Wu, M.; Ge, F.; Wang, J.; Li, X.; Geng, M.; et al. GV-971 Prevents Severe Acute Pancreatitis by Remodeling the Microbiota-Metabolic-Immune Axis. Nat Commun 2024, 15, 8278. [Google Scholar] [CrossRef]
- Liu, J.; Yan, Q.; Li, S.; Jiao, J.; Hao, Y.; Zhang, G.; Zhang, Q.; Luo, F.; Zhang, Y.; Lv, Q.; et al. Integrative Metagenomic and Metabolomic Analyses Reveal the Potential of Gut Microbiota to Exacerbate Acute Pancreatitis. npj Biofilms Microbiomes 2024, 10, 29. [Google Scholar] [CrossRef]
- Shamoon, M.; Deng, Y.; Chen, Y.Q.; Bhatia, M.; Sun, J. Therapeutic Implications of Innate Immune System in Acute Pancreatitis. Expert Opinion on Therapeutic Targets 2016, 20, 73–87. [Google Scholar] [CrossRef]
- Watanabe, T.; Kudo, M.; Strober, W. Immunopathogenesis of Pancreatitis. Mucosal Immunology 2017, 10, 283–298. [Google Scholar] [CrossRef]
- Liu, R.; Wang, K.; Guo, X.; Wang, Q.; Zhang, X.; Peng, K.; Lu, W.; Chen, Z.; Cao, F.; Wang, Z.; et al. A Causal Relationship between Distinct Immune Features and Acute or Chronic Pancreatitis: Results from a Mendelian Randomization Analysis. Pancreatology 2024, 24, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Mahapatra, S.J.; Garg, P.K. Organ Failure and Prediction of Severity in Acute Pancreatitis. Gastroenterology Clinics of North America 2025, 54, 1–19. [Google Scholar] [CrossRef]
- Liu, W.; Wu, D.H.; Wang, T.; Wang, M.; Xu, Y.; Ren, Y.; Lyu, Y.; Wu, R. CIRP Contributes to Multiple Organ Damage in Acute Pancreatitis by Increasing Endothelial Permeability. Commun Biol 2025, 8, 403. [Google Scholar] [CrossRef] [PubMed]
- Mofidi, R.; Duff, M.D.; Wigmore, S.J.; Madhavan, K.K.; Garden, O.J.; Parks, R.W. Association between Early Systemic Inflammatory Response, Severity of Multiorgan Dysfunction and Death in Acute Pancreatitis. British Journal of Surgery 2006, 93, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Liang, F.; Chen, C.; Lin, J.; Wu, Y.; Hou, Z.; Huang, H.; Fang, H.; Pan, Y. Annexin A1 Regulates Inflammatory-Immune Response and Reduces Pancreatic and Extra- Pancreatic Injury during Severe Acute Pancreatitis. Genes Immun 2025, 26, 124–136. [Google Scholar] [CrossRef]
- Zhang, R.; Zhu, S.; Shi, L.; Zhang, H.; Xu, X.; Xiang, B.; Wang, M. Automated Machine Learning for Early Prediction of Systemic Inflammatory Response Syndrome in Acute Pancreatitis. BMC Med Inform Decis Mak 2025, 25, 167. [Google Scholar] [CrossRef]
- Bhatia, M. Acute Pancreatitis as a Model of SIRS. Front Biosci (Landmark Ed) 2009, 14, 2042–2050. [Google Scholar] [CrossRef]
- Machicado, J.D.; Gougol, A.; Tan, X.; Gao, X.; Paragomi, P.; Pothoulakis, I.; Talukdar, R.; Kochhar, R.; Goenka, M.K.; Gulla, A.; et al. Mortality in Acute Pancreatitis with Persistent Organ Failure Is Determined by the Number, Type, and Sequence of Organ Systems Affected. United European Gastroenterol J 2021, 9, 139–149. [Google Scholar] [CrossRef]
- Ding, L.; Jian, L.; Xu, J.; He, Q.; Wang, Y.; Sun, C.; Wang, W.; Sun, X. Pharmacological Interventions for Acute Pancreatitis in Adults: An Overview of Systematic Reviews. J Evid Based Med 2025, 18, e70007. [Google Scholar] [CrossRef]
- Marik, P.E. What Is the Best Way to Feed Patients with Pancreatitis? Curr Opin Crit Care 2009, 15, 131–138. [Google Scholar] [CrossRef]
- Carnevale, S.; Vitale, A.; Razzi, M.; Onori, C.; Cornacchia, G.; Grispo, O.; Corsinovi, E.; Rossl, L.; Spinetti, E.; Tosi, M.; et al. Non-Evidence-Based Dietary Restrictions in Hospital Nutrition and Their Impact on Malnutrition: A Narrative Review of International and National Guidelines. Dietetics 2024, 3, 568–587. [Google Scholar] [CrossRef]
- Liu, H.; Wang, S.; Wang, J.; Guo, X.; Song, Y.; Fu, K.; Gao, Z.; Liu, D.; He, W.; Yang, L.-L. Energy Metabolism in Health and Diseases. Sig Transduct Target Ther 2025, 10, 1–71. [Google Scholar] [CrossRef]
- Li, X.-Y.; He, C.; Zhu, Y.; Lu, N.-H. Role of Gut Microbiota on Intestinal Barrier Function in Acute Pancreatitis. World J Gastroenterol 2020, 26, 2187–2193. [Google Scholar] [CrossRef] [PubMed]
- Ge, P.; Luo, Y.; Okoye, C.S.; Chen, H.; Liu, J.; Zhang, G.; Xu, C.; Chen, H. Intestinal Barrier Damage, Systemic Inflammatory Response Syndrome, and Acute Lung Injury: A Troublesome Trio for Acute Pancreatitis. Biomedicine & Pharmacotherapy 2020, 132, 110770. [Google Scholar] [CrossRef]
- Du, B.; Yan, R.; Hu, X.; Lou, J.; Zhu, Y.; Shao, Y.; Jiang, H.; Hao, Y.; Lv, L. Role of Bifidobacterium Animalis Subsp. Lactis BB-12 in Mice with Acute Pancreatitis. AMB Express 2025, 15, 62. [Google Scholar] [CrossRef]
- Werawatganon, D.; Vivatvakin, S.; Somanawat, K.; Tumwasorn, S.; Klaikeaw, N.; Siriviriyakul, P.; Chayanupatkul, M. Effects of Probiotics on Pancreatic Inflammation and Intestinal Integrity in Mice with Acute Pancreatitis. BMC Complement Med Ther 2023, 23, 166. [Google Scholar] [CrossRef]
- Wan, Y.-D.; Zhu, R.-X.; Bian, Z.-Z.; Sun, T.-W. Effect of Probiotics on Length of Hospitalization in Mild Acute Pancreatitis: A Randomized, Double-Blind, Placebo-Controlled Trial. World J Gastroenterol 2021, 27, 224–232. [Google Scholar] [CrossRef]
- Sohail, R.; Mathew, M.; Patel, K.K.; Reddy, S.A.; Haider, Z.; Naria, M.; Habib, A.; Abdin, Z.U.; Razzaq Chaudhry, W.; Akbar, A. Effects of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and Gastroprotective NSAIDs on the Gastrointestinal Tract: A Narrative Review. Cureus 2023, 15, e37080. [Google Scholar] [CrossRef]
- Huang, Z.; Ma, X.; Jia, X.; Wang, R.; Liu, L.; Zhang, M.; Wan, X.; Tang, C.; Huang, L. Prevention of Severe Acute Pancreatitis With Cyclooxygenase-2 Inhibitors: A Randomized Controlled Clinical Trial. Am J Gastroenterol 2020, 115, 473–480. [Google Scholar] [CrossRef]
- Memis, D.; Akalin, E.; Yücel, T. Indomethacin-Induced Pancreatitis: A Case Report. JOP 2005, 6, 344–347. [Google Scholar]
- Montaño Loza, A.; García Correa, J.; González Ojeda, A.; Fuentes Orozco, C.; Dávalos Cobián, C.; Rodríguez Lomelí, X. Prevention of hyperamilasemia and pancreatitis after endoscopic retrograde cholangiopancreatography with rectal administration of indomethacin. Rev Gastroenterol Mex 2006, 71, 262–268. [Google Scholar] [PubMed]
- Sotoudehmanesh, R.; Khatibian, M.; Kolahdoozan, S.; Ainechi, S.; Malboosbaf, R.; Nouraie, M. Indomethacin May Reduce the Incidence and Severity of Acute Pancreatitis after ERCP. Am J Gastroenterol 2007, 102, 978–983. [Google Scholar] [CrossRef] [PubMed]
- Elmunzer, B.J.; Scheiman, J.M.; Lehman, G.A.; Chak, A.; Mosler, P.; Higgins, P.D.R.; Hayward, R.A.; Romagnuolo, J.; Elta, G.H.; Sherman, S.; et al. A Randomized Trial of Rectal Indomethacin to Prevent Post-ERCP Pancreatitis. N Engl J Med 2012, 366, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Murray, B.; Carter, R.; Imrie, C.; Evans, S.; O’Suilleabhain, C. Diclofenac Reduces the Incidence of Acute Pancreatitis after Endoscopic Retrograde Cholangiopancreatography. Gastroenterology 2003, 124, 1786–1791. [Google Scholar] [CrossRef]
- Otsuka, T.; Kawazoe, S.; Nakashita, S.; Kamachi, S.; Oeda, S.; Sumida, C.; Akiyama, T.; Ario, K.; Fujimoto, M.; Tabuchi, M.; et al. Low-Dose Rectal Diclofenac for Prevention of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis: A Randomized Controlled Trial. J Gastroenterol 2012, 47, 912–917. [Google Scholar] [CrossRef]
- Zhao, X.; Bao, J.; Hu, C.; Ding, H.; Liu, X.; Mei, Q.; Xu, J. Effect of Diclofenac on the Levels of Lipoxin A4 and Resolvin D1 and E1 in the Post-ERCP Pancreatitis. Dig Dis Sci 2014, 59, 2992–2996. [Google Scholar] [CrossRef]
- Tomoda, T.; Kato, H.; Miyamoto, K.; Matsumi, A.; Ueta, E.; Fujii, Y.; Saragai, Y.; Yamazaki, T.; Uchida, D.; Matsumoto, K.; et al. Efficacy of Low Dose Rectal Diclofenac for Preventing Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis: Propensity Score-Matched Analysis. Dig Endosc 2021, 33, 656–662. [Google Scholar] [CrossRef]
- Werge, M.; Novovic, S.; Schmidt, P.N.; Gluud, L.L. Infection Increases Mortality in Necrotizing Pancreatitis: A Systematic Review and Meta-Analysis. Pancreatology 2016, 16, 698–707. [Google Scholar] [CrossRef]
- De Campos, T.; Assef, J.C.; Rasslan, S. Questions about the Use of Antibiotics in Acute Pancreatitis. World J Emerg Surg 2006, 1, 20. [Google Scholar] [CrossRef]
- Sun, E.; Tharakan, M.; Kapoor, S.; Chakravarty, R.; Salhab, A.; Buscaglia, J.M.; Nagula, S. Poor Compliance with ACG Guidelines for Nutrition and Antibiotics in the Management of Acute Pancreatitis: A North American Survey of Gastrointestinal Specialists and Primary Care Physicians. JOP 2013, 14, 221–227. [Google Scholar] [CrossRef]
- Vlada, A.C.; Schmit, B.; Perry, A.; Trevino, J.G.; Behrns, K.E.; Hughes, S.J. Failure to Follow Evidence-Based Best Practice Guidelines in the Treatment of Severe Acute Pancreatitis. HPB (Oxford) 2013, 15, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Raraty, M.G.T.; Connor, S.; Criddle, D.N.; Sutton, R.; Neoptolemos, J.P. Acute Pancreatitis and Organ Failure: Pathophysiology, Natural History, and Management Strategies. Curr Gastroenterol Rep 2004, 6, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Isenmann, R.; Rünzi, M.; Kron, M.; Kahl, S.; Kraus, D.; Jung, N.; Maier, L.; Malfertheiner, P.; Goebell, H.; Beger, H.G.; et al. Prophylactic Antibiotic Treatment in Patients with Predicted Severe Acute Pancreatitis: A Placebo-Controlled, Double-Blind Trial. Gastroenterology 2004, 126, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Xu, L.; Zhang, D.; Sun, W.; Che, Z.; Zhao, B.; Chen, Y.; Yang, Z.; Chen, E.; Ni, T.; et al. Effect of Early Antibiotic Treatment Strategy on Prognosis of Acute Pancreatitis. BMC Gastroenterol 2023, 23, 431. [Google Scholar] [CrossRef]
- Guo, D.; Dai, W.; Shen, J.; Zhang, M.; Shi, Y.; Jiang, K.; Guo, L. Assessment of Prophylactic Carbapenem Antibiotics Administration for Severe Acute Pancreatitis: An Updated Systematic Review and Meta-Analysis. Digestion 2022, 103, 183–191. [Google Scholar] [CrossRef]
- de-Madaria, E.; Buxbaum, J.L. Advances in the Management of Acute Pancreatitis. Nat Rev Gastroenterol Hepatol 2023, 20, 691–692. [Google Scholar] [CrossRef]
- Bassi, C.; Falconi, C.; Casetti, L.; Valerio, A.; Caldiron, E.; Butturini, G.; Pederzoli, P. Antibiotics in Severe Pancreatitis: The Current Status. HPB 1999, 1, 57–60. [Google Scholar] [CrossRef]
- Røkke, O.; Bache Harbitz, T.; Liljedal, J.; Pettersen, T.; Fetvedt, T.; Øystein Heen, L.; Skreden, K.; Viste, A. Early Treatment of Severe Pancreatitis with Imipenem: A Prospective Randomized Clinical Trial. Scandinavian Journal of Gastroenterology 2007, 42, 771–776. [Google Scholar] [CrossRef]
- Villatoro, E.; Bassi, C.; Larvin, M. Antibiotic Therapy for Prophylaxis against Infection of Pancreatic Necrosis in Acute Pancreatitis. Cochrane Database Syst Rev 2006, CD002941. [Google Scholar] [CrossRef]
- Villatoro, E.; Mulla, M.; Larvin, M. Antibiotic Therapy for Prophylaxis against Infection of Pancreatic Necrosis in Acute Pancreatitis. Cochrane Database Syst Rev 2010, 2010, CD002941. [Google Scholar] [CrossRef]
- Nordback, I.; Sand, J.; Saaristo, R.; Paajanen, H. Early Treatment with Antibiotics Reduces the Need for Surgery in Acute Necrotizing Pancreatitis--a Single-Center Randomized Study. J Gastrointest Surg 2001, 5, 113–118; discussion 118-120. [Google Scholar] [CrossRef] [PubMed]
- Räty, S.; Sand, J.; Pulkkinen, M.; Matikainen, M.; Nordback, I. Post-ERCP Pancreatitis: Reduction by Routine Antibiotics. J Gastrointest Surg 2001, 5, 339–345; discussion 345. [Google Scholar] [CrossRef] [PubMed]
- Mishra, B.; Bachu, M.; Yuan, R.; Wingert, C.; Chaudhary, V.; Brauner, C.; Bell, R.; Ivashkiv, L.B. IL-10 Targets IRF Transcription Factors to Suppress IFN and Inflammatory Response Genes by Epigenetic Mechanisms. Nat Immunol 2025, 26, 748–759. [Google Scholar] [CrossRef]
- Saraiva, M.; O’Garra, A. The Regulation of IL-10 Production by Immune Cells. Nat Rev Immunol 2010, 10, 170–181. [Google Scholar] [CrossRef]
- Berney, T.; Gasche, Y.; Robert, J.; Jenny, A.; Mensi, N.; Grau, G.; Vermeulen, B.; Morel, P. Serum Profiles of Interleukin-6, Interleukin-8, and Interleukin-10 in Patients with Severe and Mild Acute Pancreatitis. Pancreas 1999, 18, 371–377. [Google Scholar] [CrossRef]
- Pezzilli, R.; Billi, P.; Miniero, R.; Barakat, B. Serum Interleukin-10 in Human Acute Pancreatitis. Dig Dis Sci 1997, 42, 1469–1472. [Google Scholar] [CrossRef]
- Devière, J.; Le Moine, O.; Van Laethem, J.L.; Eisendrath, P.; Ghilain, A.; Severs, N.; Cohard, M. Interleukin 10 Reduces the Incidence of Pancreatitis after Therapeutic Endoscopic Retrograde Cholangiopancreatography. Gastroenterology 2001, 120, 498–505. [Google Scholar] [CrossRef]
- Oruc, N.; Ozutemiz, A.O.; Yukselen, V.; Nart, D.; Celik, H.A.; Yuce, G.; Batur, Y. Infliximab: A New Therapeutic Agent in Acute Pancreatitis? Pancreas 2004, 28, e1–8. [Google Scholar] [CrossRef]
- Tekin, S.O.; Teksoz, S.; Terzioglu, D.; Arikan, A.E.; Ozcevik, H.; Uslu, E. Use of Infliximab in Treatment of Acute Pancreatitis. Bratisl Lek Listy 2015, 116, 167–172. [Google Scholar] [CrossRef]
- Bishehsari, F.; Sharma, A.; Stello, K.; Toth, C.; O’Connell, M.R.; Evans, A.C.; LaRusch, J.; Muddana, V.; Papachristou, G.I.; Whitcomb, D.C. TNF-Alpha Gene (TNFA) Variants Increase Risk for Multi-Organ Dysfunction Syndrome (MODS) in Acute Pancreatitis. Pancreatology 2012, 12, 113–118. [Google Scholar] [CrossRef]
- Malleo, G.; Mazzon, E.; Siriwardena, A.K.; Cuzzocrea, S. Role of Tumor Necrosis Factor-Alpha in Acute Pancreatitis: From Biological Basis to Clinical Evidence. Shock 2007, 28, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Malleo, G.; Mazzon, E.; Genovese, T.; Di Paola, R.; Muià, C.; Centorrino, T.; Siriwardena, A.K.; Cuzzocrea, S. Etanercept Attenuates the Development of Cerulein-Induced Acute Pancreatitis in Mice: A Comparison with TNF-Alpha Genetic Deletion. Shock 2007, 27, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Ohwada, S.; Ishigami, K.; Yokoyama, Y.; Kazama, T.; Masaki, Y.; Takahashi, M.; Yoshii, S.; Yamano, H.; Chiba, H.; Nakase, H. Immune-Related Colitis and Pancreatitis Treated with Infliximab. Clin J Gastroenterol 2023, 16, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Triantafillidis, J.K.; Cheracakis, P.; Hereti, I.A.; Argyros, N.; Karra, E. Acute Idiopathic Pancreatitis Complicating Active Crohn’s Disease: Favorable Response to Infliximab Treatment. Am J Gastroenterol 2000, 95, 3334–3336. [Google Scholar] [CrossRef]
- Randomised Treatment of Acute Pancreatitis With Infliximab: Double-Blind, Placebo-Controlled, Multi-Centre Trial (RAPID-I). Available online: https://www.centerwatch.com (accessed on 18 May 2025).
- Ashraf, M.A.; Nookala, V. Biochemistry of Platelet Activating Factor. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Stafforini, D.M.; McIntyre, T.M.; Zimmerman, G.A.; Prescott, S.M. Platelet-Activating Factor, a Pleiotrophic Mediator of Physiological and Pathological Processes. Crit Rev Clin Lab Sci 2003, 40, 643–672. [Google Scholar] [CrossRef]
- Chen, C.; Xia, S.-H.; Chen, H.; Li, X.-H. Therapy for Acute Pancreatitis with Platelet-Activating Factor Receptor Antagonists. World J Gastroenterol 2008, 14, 4735–4738. [Google Scholar] [CrossRef]
- Konturek, S.J.; Dembinski, A.; Konturek, P.J.; Warzecha, Z.; Jaworek, J.; Gustaw, P.; Tomaszewska, R.; Stachura, J. Role of Platelet Activating Factor in Pathogenesis of Acute Pancreatitis in Rats. Gut 1992, 33, 1268–1274. [Google Scholar] [CrossRef]
- Emanuelli, G.; Montrucchio, G.; Dughera, L.; Gaia, E.; Lupia, E.; Battaglia, E.; De Martino, A.; De Giuli, P.; Gubetta, L.; Camussi, G. Role of Platelet Activating Factor in Acute Pancreatitis Induced by Lipopolysaccharides in Rabbits. European Journal of Pharmacology 1994, 261, 265–272. [Google Scholar] [CrossRef]
- Lane, J.S.; Todd, K.E.; Gloor, B.; Chandler, C.F.; Kau, A.W.; Ashley, S.W.; Reber, H.A.; McFadden, D.W. Platelet Activating Factor Antagonism Reduces the Systemic Inflammatory Response in a Murine Model of Acute Pancreatitis. Journal of Surgical Research 2001, 99, 365–370. [Google Scholar] [CrossRef]
- Abu-Zidan, F.M.; Windsor, J.A. Lexipafant and Acute Pancreatitis: A Critical Appraisal of the Clinical Trials. The European Journal of Surgery 2002, 168, 215–219. [Google Scholar] [CrossRef]
- Johnson, C.D. Platelet-Activating Factor and Platelet-Activating Factor Antagonists in Acute Pancreatitis. Dig Surg 1999, 16, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Kingsnorth, A.N.; Galloway, S.W.; Formela, L.J. Randomized, Double-Blind Phase II Trial of Lexipafant, a Platelet-Activating Factor Antagonist, in Human Acute Pancreatitis. Journal of British Surgery 1995, 82, 1414–1420. [Google Scholar] [CrossRef] [PubMed]
- McKay, C.J.; Curran, F.; Sharples, C.; Baxter, J.N.; Imrie, C.W. Prospective Placebo-Controlled Randomized Trial of Lexipafant in Predicted Severe Acute Pancreatitis. Br J Surg 1997, 84, 1239–1243. [Google Scholar] [PubMed]
- Johnson, C.D. Double Blind, Randomised, Placebo Controlled Study of a Platelet Activating Factor Antagonist, Lexipafant, in the Treatment and Prevention of Organ Failure in Predicted Severe Acute. Gut 2001, 48, 62–69. [Google Scholar] [CrossRef]
- McCoy, C.; Matthews, S.J. Drotrecogin Alfa (Recombinant Human Activated Protein C) for the Treatment of Severe Sepsis. Clinical Therapeutics 2003, 25, 396–421. [Google Scholar] [CrossRef]
- Raggio, M.J.; Morris, P.E. Drotrecogin Alfa. Drugs of Today 2004, 40, 517. [Google Scholar] [CrossRef]
- Xu, J.; Ji, Y.; Zhang, X.; Drake, M.; Esmon, C.T. Endogenous Activated Protein C Signaling Is Critical to Protection of Mice from Lipopolysaccaride-Induced Septic Shock. J Thromb Haemost 2009, 7, 851–856. [Google Scholar] [CrossRef]
- Lindstrom, O.; Kylanpaa, L.; Mentula, P.; Puolakkainen, P.; Kemppainen, E.; Haapiainen, R.; Fernandez, J.A.; Griffin, J.H.; Repo, H.; Petaja, J. Upregulated but Insufficient Generation of Activated Protein C Is Associated with Development of Multiorgan Failure in Severe Acute Pancreatitis. Crit Care 2006, 10, R16. [Google Scholar] [CrossRef]
- Chen, P.; Zhang, Y.; Qiao, M.; Yuan, Y. Activated Protein C, an Anticoagulant Polypeptide, Ameliorates Severe Acute Pancreatitis via Regulation of Mitogen-Activated Protein Kinases. J Gastroenterol 2007, 42, 887–896. [Google Scholar] [CrossRef]
- Jamdar, S.; Babu, B.I.; Nirmalan, M.; Jeziorska, M.; McMahon, R.F.; Siriwardena, K. Activated Protein c in L-Arginine-Induced Experimental Acute Pancreatitis. Pancreas 2008, 37, 476. [Google Scholar] [CrossRef]
- Alsfasser, G. Decreased Inflammation and Improved Survival With Recombinant Human Activated Protein C Treatment in Experimental Acute Pancreatitis. Arch Surg 2006, 141, 670. [Google Scholar] [CrossRef] [PubMed]
- Yamanel, L.; Mas, M.R.; Comert, B.; Isik, A.T.; Aydin, S.; Mas, N.; Deveci, S.; Ozyurt, M.; Tasci, I.; Unal, T. The Effect of Activated Protein C on Experimental Acute Necrotizing Pancreatitis. Crit Care 2005, 9, R184–190. [Google Scholar] [CrossRef] [PubMed]
- Machała, W.; Wachowicz, N.; Komorowska, A.; Gaszyński, W. The Use of Drotrecogin Alfa (Activated) in Severe Sepsis during Acute Pancreatitis - Two Case Studies. Med Sci Monit 2004, 10, CS31–36. [Google Scholar] [PubMed]
- Miranda, C.J.; Mason, J.M.; Babu, B.I.; Sheen, A.J.; Eddleston, J.M.; Parker, M.J.; Pemberton, P.; Siriwardena, A.K. Twenty-Four Hour Infusion of Human Recombinant Activated Protein C (Xigris) Early in Severe Acute Pancreatitis: The XIG-AP 1 Trial. Pancreatology 2015, 15, 635–641. [Google Scholar] [CrossRef]
- Bernard, G.R.; Vincent, J.-L.; Laterre, P.-F.; LaRosa, S.P.; Dhainaut, J.-F.; Lopez-Rodriguez, A.; Steingrub, J.S.; Garber, G.E.; Helterbrand, J.D.; Ely, E.W.; et al. Efficacy and Safety of Recombinant Human Activated Protein C for Severe Sepsis. N Engl J Med 2001, 344, 699–709. [Google Scholar] [CrossRef]
- Steinberg, W.; Tenner, S. Acute Pancreatitis. N Engl J Med 1994, 330, 1198–1210. [Google Scholar] [CrossRef]
- Leppäniemi, A.; Tolonen, M.; Tarasconi, A.; Segovia-Lohse, H.; Gamberini, E.; Kirkpatrick, A.W.; Ball, C.G.; Parry, N.; Sartelli, M.; Wolbrink, D.; et al. 2019 WSES Guidelines for the Management of Severe Acute Pancreatitis. World J Emerg Surg 2019, 14, 27. [Google Scholar] [CrossRef]
- Crockett, S.D.; Wani, S.; Gardner, T.B.; Falck-Ytter, Y.; Barkun, A.N.; Crockett, S.; Falck-Ytter, Y.; Feuerstein, J.; Flamm, S.; Gellad, Z.; et al. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology 2018, 154, 1096–1101. [Google Scholar] [CrossRef]
- Tenner, S.; Vege, S.S.; Sheth, S.G.; Sauer, B.; Yang, A.; Conwell, D.L.; Yadlapati, R.H.; Gardner, T.B. American College of Gastroenterology Guidelines: Management of Acute Pancreatitis. Am J Gastroenterol 2024, 119, 419–437. [Google Scholar] [CrossRef]
- De Lucia, S.S.; Candelli, M.; Polito, G.; Maresca, R.; Mezza, T.; Schepis, T.; Pellegrino, A.; Zileri Dal Verme, L.; Nicoletti, A.; Franceschi, F.; et al. Nutrition in Acute Pancreatitis: From the Old Paradigm to the New Evidence. Nutrients 2023, 15, 1939. [Google Scholar] [CrossRef]
- Petrov, M.S. Moving beyond the “pancreatic Rest” in Severe and Critical Acute Pancreatitis. Crit Care 2013, 17, 161. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Goswami, P.; Poudel, S.; Gunjan, D.; Singh, N.; Yadav, R.; Kumar, U.; Pandey, G.; Saraya, A. Acute Pancreatitis Is Characterized by Generalized Intestinal Barrier Dysfunction in Early Stage. Pancreatology 2023, 23, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, H.-X.; Bai, C.; Zhou, X.-Y. Blockade of High-Mobility Group Box 1 Attenuates Intestinal Mucosal Barrier Dysfunction in Experimental Acute Pancreatitis. Sci Rep 2017, 7, 6799. [Google Scholar] [CrossRef] [PubMed]
- Mei, Q.; Hu, J.; Huang, Z.; Fan, J.; Huang, C.; Lu, Y.; Wang, X.; Zeng, Y. Pretreatment with Chitosan Oligosaccharides Attenuate Experimental Severe Acute Pancreatitis via Inhibiting Oxidative Stress and Modulating Intestinal Homeostasis. Acta Pharmacol Sin 2021, 42, 942–953. [Google Scholar] [CrossRef]
- Lakananurak, N.; Gramlich, L. Nutrition Management in Acute Pancreatitis: Clinical Practice Consideration. World J Clin Cases 2020, 8, 1561–1573. [Google Scholar] [CrossRef]
- Dancu, G.; Tarta, C.; Socaciu, C.; Bende, F.; Danila, M.; Sirli, R.; Sporea, I.; Miutescu, B.; Popescu, A. Unraveling the Metabolic Changes in Acute Pancreatitis: A Metabolomics-Based Approach for Etiological Differentiation and Acute Biomarker Discovery. Biomolecules 2023, 13, 1558. [Google Scholar] [CrossRef]
- Mahajan, U.M.; Weiss, F.U.; Lerch, M.M.; Mayerle, J. Molecular, Biochemical, and Metabolic Abnormalities of Acute Pancreatitis. In The Pancreas; Beger, H.G., Büchler, M.W., Hruban, R.H., Mayerle, J., Neoptolemos, J.P., Shimosegawa, T., Warshaw, A.L., Whitcomb, D.C., Zhao, Y., Groß, C., Eds.; Wiley, 2023; pp. 155–163 ISBN 978-1-119-87597-0.
- Gou, Y.; Lv, B.-H.; Zhang, J.-F.; Li, S.-M.; Hei, X.-P.; Liu, J.-J.; Li, L.; Yang, J.-Z.; Feng, K. Identifying Early Predictive and Diagnostic Biomarkers and Exploring Metabolic Pathways for Sepsis after Trauma Based on an Untargeted Metabolomics Approach. Sci Rep 2025, 15, 12068. [Google Scholar] [CrossRef]
- Wasyluk, W.; Zwolak, A. Metabolic Alterations in Sepsis. J Clin Med 2021, 10, 2412. [Google Scholar] [CrossRef]
- Gianotti, L.; Meier, R.; Lobo, D.N.; Bassi, C.; Dejong, C.H.C.; Ockenga, J.; Irtun, O.; MacFie, J. ESPEN ESPEN Guidelines on Parenteral Nutrition: Pancreas. Clin Nutr 2009, 28, 428–435. [Google Scholar] [CrossRef]
- Windsor, A.C.; Kanwar, S.; Li, A.G.; Barnes, E.; Guthrie, J.A.; Spark, J.I.; Welsh, F.; Guillou, P.J.; Reynolds, J.V. Compared with Parenteral Nutrition, Enteral Feeding Attenuates the Acute Phase Response and Improves Disease Severity in Acute Pancreatitis. Gut 1998, 42, 431–435. [Google Scholar] [CrossRef]
- Feng, P.; He, C.; Liao, G.; Chen, Y. Early Enteral Nutrition versus Delayed Enteral Nutrition in Acute Pancreatitis: A PRISMA-Compliant Systematic Review and Meta-Analysis. Medicine (Baltimore) 2017, 96, e8648. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, M.; Aadam, A.A. Nutrition Management in Acute Pancreatitis. Nut in Clin Prac 2019, 34. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, R.L.; Gaudet, D.; Davidson, M.; Rensfeldt, M.; Yang, H.; Nilsson, C.; Kvarnström, M.; Oscarsson, J. Omega-3 Fatty Acid Exposure with a Low-Fat Diet in Patients with Past Hypertriglyceridemia-Induced Acute Pancreatitis; an Exploratory, Randomized, Open-Label Crossover Study. Lipids Health Dis 2020, 19, 117. [Google Scholar] [CrossRef]
- Al-Leswas, D.; Eltweri, A.M.; Chung, W.-Y.; Arshad, A.; Stephenson, J.A.; Al-Taan, O.; Pollard, C.; Fisk, H.L.; Calder, P.C.; Garcea, G.; et al. Intravenous Omega-3 Fatty Acids Are Associated with Better Clinical Outcome and Less Inflammation in Patients with Predicted Severe Acute Pancreatitis: A Randomised Double Blind Controlled Trial. Clinical Nutrition 2020, 39, 2711–2719. [Google Scholar] [CrossRef]
- Lei, Q.C.; Wang, X.Y.; Xia, X.F.; Zheng, H.Z.; Bi, J.C.; Tian, F.; Li, N. The Role of Omega-3 Fatty Acids in Acute Pancreatitis: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2015, 7, 2261–2273. [Google Scholar] [CrossRef]
- Bakker, O.J.; Van Brunschot, S.; Van Santvoort, H.C.; Besselink, M.G.; Bollen, T.L.; Boermeester, M.A.; Dejong, C.H.; Van Goor, H.; Bosscha, K.; Ali, U.A.; et al. Early versus On-Demand Nasoenteric Tube Feeding in Acute Pancreatitis. N Engl J Med 2014, 371, 1983–1993. [Google Scholar] [CrossRef]
- Sun, J.; Li, W.; Ke, L.; Tong, Z.; Ni, H.; Li, G.; Zhang, L.; Nie, Y.; Wang, X.; Ye, X.; et al. Early Enteral Nutrition Prevents Intra-abdominal Hypertension and Reduces the Severity of Severe Acute Pancreatitis Compared with Delayed Enteral Nutrition: A Prospective Pilot Study. World j. surg. 2013, 37, 2053–2060. [Google Scholar] [CrossRef]
- Rajkumar, N.; Karthikeyan, V.S.; Ali, S.M.; Sistla, S.C.; Kate, V. Clear Liquid Diet vs Soft Diet as the Initial Meal in Patients With Mild Acute Pancreatitis: A Randomized Interventional Trial. Nut in Clin Prac 2013, 28, 365–370. [Google Scholar] [CrossRef]
- Wereszczynska-Siemiatkowska, U.; Swidnicka-Siergiejko, A.; Siemiatkowski, A.; Dabrowski, A. Early Enteral Nutrition Is Superior to Delayed Enteral Nutrition for the Prevention of Infected Necrosis and Mortality in Acute Pancreatitis. Pancreas 2013, 42, 640–646. [Google Scholar] [CrossRef]
- Wu, X.-M.; Ji, K.-Q.; Wang, H.-Y.; Li, G.-F.; Zang, B.; Chen, W.-M. Total Enteral Nutrition in Prevention of Pancreatic Necrotic Infection in Severe Acute Pancreatitis. Pancreas 2010, 39, 248–251. [Google Scholar] [CrossRef]
- Doley, R.P.; Yadav, T.D.; Wig, J.D.; Kochhar, R.; Singh, G.; Bharathy, K.G.S.; Kudari, A.; Gupta, R.; Gupta, V.; Poornachandra, K.S.; et al. Enteral Nutrition in Severe Acute Pancreatitis. JOP 2009, 10, 157–162. [Google Scholar] [PubMed]
- Qin, H.-L.; Zheng, J.-J.; Tong, D.-N.; Chen, W.-X.; Fan, X.-B.; Hang, X.-M.; Jiang, Y.-Q. Effect of Lactobacillus Plantarum Enteral Feeding on the Gut Permeability and Septic Complications in the Patients with Acute Pancreatitis. Eur J Clin Nutr 2008, 62, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Casas, M.; Mora, J.; Fort, E.; Aracil, C.; Busquets, D.; Galter, S.; Jáuregui, C.E.; Ayala, E.; Cardona, D.; Gich, I.; et al. Total enteral nutrition vs. total parenteral nutrition in patients with severe acute pancreatitis. Rev Esp Enferm Dig 2007, 99, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S.; Kukosh, M.V.; Emelyanov, N.V. A Randomized Controlled Trial of Enteral versus Parenteral Feeding in Patients with Predicted Severe Acute Pancreatitis Shows a Significant Reduction in Mortality and in Infected Pancreatic Complications with Total Enteral Nutrition. Dig Surg 2006, 23, 336–344; discussion 344-345. [Google Scholar] [CrossRef]
- Targarona Modena, J.; Barreda Cevasco, L.; Arroyo Basto, C.; Orellana Vicuna, A.; Portanova Ramirez, M. Total Enteral Nutrition as Prophylactic Therapy for Pancreatic Necrosis Infection in Severe Acute Pancreatitis. Pancreatology 2006, 6, 58–64. [Google Scholar] [CrossRef]
- Louie, B.E.; Noseworthy, T.; Hailey, D.; Gramlich, L.M.; Jacobs, P.; Warnock, G.L. 2004 MacLean-Mueller Prize Enteral or Parenteral Nutrition for Severe Pancreatitis: A Randomized Controlled Trial and Health Technology Assessment. Can J Surg 2005, 48, 298–306. [Google Scholar]
- Zhao, G.; Wang, C.-Y.; Wang, F.; Xiong, J.-X. Clinical Study on Nutrition Support in Patients with Severe Acute Pancreatitis. World J Gastroenterol 2003, 9, 2105–2108. [Google Scholar] [CrossRef]
- Gupta, R.; Patel, K.; Calder, P.C.; Yaqoob, P.; Primrose, J.N.; Johnson, C.D. A Randomised Clinical Trial to Assess the Effect of Total Enteral and Total Parenteral Nutritional Support on Metabolic, Inflammatory and Oxidative Markers in Patients with Predicted Severe Acute Pancreatitis (APACHE II > or =6). Pancreatology 2003, 3, 406–413. [Google Scholar] [CrossRef]
- Abou-Assi, S.; Craig, K.; O’Keefe, S.J.D. Hypocaloric Jejunal Feeding Is Better than Total Parenteral Nutrition in Acute Pancreatitis: Results of a Randomized Comparative Study. Am J Gastroenterol 2002, 97, 2255–2262. [Google Scholar] [CrossRef]
- Oláh, A.; Pardavi, G.; Belágyi, T.; Nagy, A.; Issekutz, A.; Mohamed, G.E. Early Nasojejunal Feeding in Acute Pancreatitis Is Associated with a Lower Complication Rate. Nutrition 2002, 18, 259–262. [Google Scholar] [CrossRef]
- Robles, L.; Vaziri, N.D.; Ichii, H. Role of Oxidative Stress in the Pathogenesis of Pancreatitis: Effect of Antioxidant Therapy. Pancreat Disord Ther 2013, 3, 112. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.-C.; Chen, H.-T.; Deng, H.; Huang, Y.-T.; Xu, G.-Q. Reactive Oxygen Species and Oxidative Stress in Acute Pancreatitis: Pathogenesis and New Therapeutic Interventions. World J Gastroenterol 2024, 30, 4771–4780. [Google Scholar] [CrossRef] [PubMed]
- Curran, F.J.; Sattar, N.; Talwar, D.; Baxter, J.N.; Imrie, C.W. Relationship of Carotenoid and Vitamins A and E with the Acute Inflammatory Response in Acute Pancreatitis. Br J Surg 2000, 87, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Morris-Stiff, G.J.; Bowrey, D.J.; Oleesky, D.; Davies, M.; Clark, G.W.B.; Puntis, M.C.A. The Antioxidant Profiles of Patients with Recurrent Acute and Chronic Pancreatitis. The American Journal of Gastroenterology 1999, 94, 2135–2140. [Google Scholar] [CrossRef]
- Firdous, S.M.; Pal, S.; Mandal, S.; Sindhu, R.K. Antioxidants in Inflammatory Diseases. In Antioxidants; John Wiley & Sons, Ltd, 2025; pp. 83–126 ISBN 978-1-394-27057-6.
- Bhol, N.K.; Bhanjadeo, M.M.; Singh, A.K.; Dash, U.C.; Ojha, R.R.; Majhi, S.; Duttaroy, A.K.; Jena, A.B. The Interplay between Cytokines, Inflammation, and Antioxidants: Mechanistic Insights and Therapeutic Potentials of Various Antioxidants and Anti-Cytokine Compounds. Biomedicine & Pharmacotherapy 2024, 178, 117177. [Google Scholar] [CrossRef]
- Blagov, A.V.; Summerhill, V.I.; Sukhorukov, V.N.; Zhigmitova, E.B.; Postnov, A.Y.; Orekhov, A.N. Potential Use of Antioxidants for the Treatment of Chronic Inflammatory Diseases. Front. Pharmacol. 2024, 15. [Google Scholar] [CrossRef]
- Sateesh, J.; Bhardwaj, P.; Singh, N.; Saraya, A. Effect of Antioxidant Therapy on Hospital Stay and Complications in Patients with Early Acute Pancreatitis: A Randomised Controlled Trial. Trop Gastroenterol 2009, 30, 201–206. [Google Scholar]
- Antunes, D.; Gonçalves, S.M.; Matzaraki, V.; Rodrigues, C.S.; Gonçales, R.A.; Rocha, J.; Sáiz, J.; Marques, A.; Torrado, E.; Silvestre, R.; et al. Glutamine Metabolism Supports the Functional Activity of Immune Cells against Aspergillus Fumigatus. Microbiol Spectr 2023, 11, e02256–22. [Google Scholar] [CrossRef]
- Guo, C.; You, Z.; Shi, H.; Sun, Y.; Du, X.; Palacios, G.; Guy, C.; Yuan, S.; Chapman, N.M.; Lim, S.A.; et al. SLC38A2 and Glutamine Signalling in cDC1s Dictate Anti-Tumour Immunity. Nature 2023, 620, 200–208. [Google Scholar] [CrossRef]
- Stehle, P.; Kuhn, K.S. Glutamine: An Obligatory Parenteral Nutrition Substrate in Critical Care Therapy. BioMed Research International 2015, 2015, 1–7. [Google Scholar] [CrossRef]
- Asrani, V.; Chang, W.K.; Dong, Z.; Hardy, G.; Windsor, J.A.; Petrov, M.S. Glutamine Supplementation in Acute Pancreatitis: A Meta-Analysis of Randomized Controlled Trials. Pancreatology 2013, 13, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Jeurnink, S.M.; Nijs, M.M.; Prins, H. a. B.; Greving, J.P.; Siersema, P.D. Antioxidants as a Treatment for Acute Pancreatitis: A Meta-Analysis. Pancreatology 2015, 15, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Xue, P.; Deng, L.-H.; Xia, Q.; Zhang, Z.-D.; Hu, W.-M.; Yang, X.-N.; Song, B.; Huang, Z.-W. Impact of Alanyl-Glutamine Dipeptide on Severe Acute Pancreatitis in Early Stage. World J Gastroenterol 2008, 14, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Huang, L.; Luo, M.; Xia, X. Bacterial Translocation in Acute Pancreatitis. Crit Rev Microbiol 2019, 45, 539–547. [Google Scholar] [CrossRef]
- Glaubitz, J.; Wilden, A.; Frost, F.; Ameling, S.; Homuth, G.; Mazloum, H.; Rühlemann, M.C.; Bang, C.; Aghdassi, A.A.; Budde, C.; et al. Activated Regulatory T-Cells Promote Duodenal Bacterial Translocation into Necrotic Areas in Severe Acute Pancreatitis. Gut 2023, 72, 1355–1369. [Google Scholar] [CrossRef]
- Zhang, C.; Chen ,Shiyin; Wang ,Zhien; Zhang ,Jian; Yu ,Wenqiao; Wang ,Yanshuai; Si ,Weiwei; Zhang ,Yuwei; Zhang ,Yun; and Liang, T. Exploring the Mechanism of Intestinal Bacterial Translocation after Severe Acute Pancreatitis: The Role of Toll-like Receptor 5. Gut Microbes 2025, 17, 2489768. [CrossRef]
- Sanders, M.E.; Merenstein, D.J.; Reid, G.; Gibson, G.R.; Rastall, R.A. Probiotics and Prebiotics in Intestinal Health and Disease: From Biology to the Clinic. Nat Rev Gastroenterol Hepatol 2019, 16, 605–616. [Google Scholar] [CrossRef]
- Suez, J.; Zmora, N.; Segal, E.; Elinav, E. The Pros, Cons, and Many Unknowns of Probiotics. Nat Med 2019, 25, 716–729. [Google Scholar] [CrossRef]
- Qin, W.; Wang, G.; Xia, Y.; Song, X.; Xiong, Z.; Huang, C.; Gong, C.; Zeng, Y.; Ai, L. The Role of Probiotic Foods in Acute Pancreatitis: Current Status and Future Directions. Current Opinion in Food Science 2024, 60, 101231. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, R.; Wang, S.; Yang, C.; Wang, Y.; Fan, H.; Yang, M. Observation on the Therapeutic Effect of Probiotics on Early Oral Feeding in the Treatment of Severe Acute Pancreatitis. Front. Med. 2024, 11. [Google Scholar] [CrossRef]
- Oláh, A.; Belágyi, T.; Issekutz, A.; Gamal, M.E.; Bengmark, S. Randomized Clinical Trial of Specific Lactobacillus and Fibre Supplement to Early Enteral Nutrition in Patients with Acute Pancreatitis. Br J Surg 2002, 89, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Oláh, A.; Belágyi, T.; Pótó, L.; Romics, L.; Bengmark, S. Synbiotic Control of Inflammation and Infection in Severe Acute Pancreatitis: A Prospective, Randomized, Double Blind Study. Hepatogastroenterology 2007, 54, 590–594. [Google Scholar] [PubMed]
- Timmerman, H.M.; Niers, L.E.M.; Ridwan, B.U.; Koning, C.J.M.; Mulder, L.; Akkermans, L.M.A.; Rombouts, F.M.; Rijkers, G.T. Design of a Multispecies Probiotic Mixture to Prevent Infectious Complications in Critically Ill Patients. Clin Nutr 2007, 26, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Plaudis, H.; Pupelis, G.; Zeiza, K.; Boka, V. Early Low Volume Oral Synbiotic/Prebiotic Supplemented Enteral Stimulation of the Gut in Patients with Severe Acute Pancreatitis: A Prospective Feasibility Study. Acta Chir Belg 2012, 112, 131–138. [Google Scholar] [CrossRef]
Figure 1.
Cellular mechanisms and inflammatory pathways involved in the pathophysiological course of AP. In a healthy pancreas, digestive enzymes are secreted in an inactive form and activated only upon reaching the small intestine. In AP, etiological stress triggers pancreatic injury and premature activation of digestive zymogens. This initiates an inflammatory cascade characterized by immune system activation and the release of various pro-inflammatory mediators. Activated leukocytes further amplify inflammation by increasing the expression of adhesion molecules, promoting leukocyte aggregation and infiltration into pancreatic microcirculation, and releasing additional cytokines and inflammatory mediators. At the cellular signaling level, inflammatory stimuli activate the I kappa B (IκB) kinase complex, which phosphorylates IκBα, leading to its degradation. This process frees nuclear factor-kappa B (NF-κB) to translocate into the nucleus, where it enhances the transcription of inflammatory genes. The resulting upregulation of inflammatory mediators promotes further recruitment of inflammatory cells and sustains the activation of IκB kinase, creating a feedback loop. Meanwhile, platelet-activating factor (PAF) increases the vascular permeability and facilitates the extravasation of inflammatory cells. These combined responses lead to tissue oedema, microvascular dysfunction, hypoxia, cellular injury, multiple organ dysfunction (MOD), and ultimately, death. Baso., basophils; Dendt., dendritic cell; IKK, Ikappa kinase; Inflam., inflammatory; Macr., macrophages; Mast., mast cell; Mon., monocytes; Neut., neutrophils; NF-κB, nuclear factor kappa B; P, phosphorylation; Plt., platelet; REL, proto-oncogne; Ub, ubiquitination. Image created with BioRender (www.biorender.com) (created in BioRender. Soleimanpour, S. (2025) https://BioRender.com/ob8rd34).
Figure 1.
Cellular mechanisms and inflammatory pathways involved in the pathophysiological course of AP. In a healthy pancreas, digestive enzymes are secreted in an inactive form and activated only upon reaching the small intestine. In AP, etiological stress triggers pancreatic injury and premature activation of digestive zymogens. This initiates an inflammatory cascade characterized by immune system activation and the release of various pro-inflammatory mediators. Activated leukocytes further amplify inflammation by increasing the expression of adhesion molecules, promoting leukocyte aggregation and infiltration into pancreatic microcirculation, and releasing additional cytokines and inflammatory mediators. At the cellular signaling level, inflammatory stimuli activate the I kappa B (IκB) kinase complex, which phosphorylates IκBα, leading to its degradation. This process frees nuclear factor-kappa B (NF-κB) to translocate into the nucleus, where it enhances the transcription of inflammatory genes. The resulting upregulation of inflammatory mediators promotes further recruitment of inflammatory cells and sustains the activation of IκB kinase, creating a feedback loop. Meanwhile, platelet-activating factor (PAF) increases the vascular permeability and facilitates the extravasation of inflammatory cells. These combined responses lead to tissue oedema, microvascular dysfunction, hypoxia, cellular injury, multiple organ dysfunction (MOD), and ultimately, death. Baso., basophils; Dendt., dendritic cell; IKK, Ikappa kinase; Inflam., inflammatory; Macr., macrophages; Mast., mast cell; Mon., monocytes; Neut., neutrophils; NF-κB, nuclear factor kappa B; P, phosphorylation; Plt., platelet; REL, proto-oncogne; Ub, ubiquitination. Image created with BioRender (www.biorender.com) (created in BioRender. Soleimanpour, S. (2025) https://BioRender.com/ob8rd34).
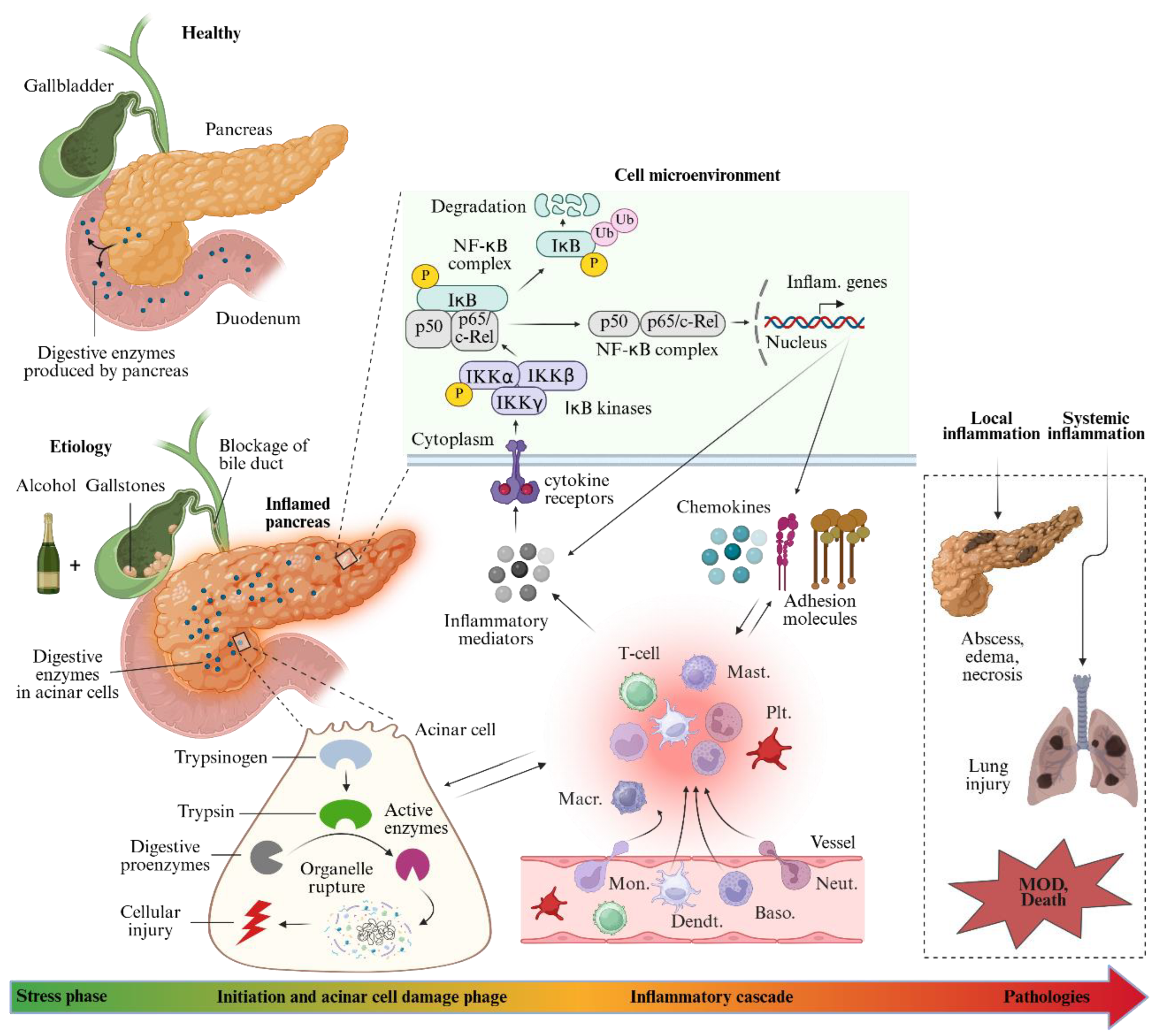
Table 1.
Classification of acute pancreatitis.
| AP classification | Degree of severity | Complications | |||
| Local | Systemic | ||||
| TOF | POF | EPC | |||
| Atlanta 1992[9] | Mild | × | × | × | N/A |
| Severe | √ | √ | √ | N/A | |
| *Revised Atlanta 2012[10,11] | Mild | × | × | × | × |
| Moderate | √ | √ | × | √ | |
| Severe | √ | × | √ | √ or × | |
| #Determinant-based[12] | Mild | × | × | × | N/A |
| Moderate | Sterile | √ | × | N/A | |
| Severe | Infected | √ | √ | N/A | |
| Critical | Infected | × | √ | N/A | |
TOF, transient organ failure; POF, persistent organ failure; EPC, exacerbation of pre-exiting comorbidity; √, Yes; ×, No; N/A, not applicable; *According to the revised Atlanta classification (2012), local complications are subcategorized into interstitial oedematous, necrotizing pancreatitis, infected necrotizing pancreatitis, and other local complications. Systemic complications are defined as TOF, POF, or an EPC. POF is defined as a Marshall score of 2 or more in any one of the three organ systems —renal, respiratory, cardiovascular —persisting for more than 48 hours. #The sepsis-related organ failure assessment (SOFA) scoring system is also used to define organ failure. For a diagnosis of severe pancreatitis, either POF or infected pancreatic necrosis is required.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



