Submitted:
03 June 2025
Posted:
03 June 2025
You are already at the latest version
Abstract
Background: Although improving the patient experience with care is being framed as part of value-based care, the economic and provider well-being impact of interventions for improving the patient experience has not been established. We aim to synthesize the contemporary (2015-2024) empirical literature on the economic (e.g., costs, revenue) and other value-based impacts (e.g., provider well-being) of patient-experience improvement interventions.
Methods: Systematic review using six databases of scientific literature (PubMed, EconLit, CINAHL, PsycINFO, DOAJ, and Scopus) supplemented by journal-specific and snowball searches. Two independent reviewers performed eligibility decisions and quality appraisals of the study methods and economic assessments, when applicable; the latter using the Joanna Briggs Institute’s checklist for economic evaluations.
Results: Out of 1317 unique references, nine were included. Four studies assessed the effectiveness of patient-experience improvement interventions (e.g., provider communication training, discharge or transitional support) coupled with economic evaluations; these found statistically significant positive outcomes for both patient experience and economic dimensions – including reduced costs, improved revenue, or additional costs offset by improved revenue. Three additional studies on provider communication training also found statistically significant positive impacts on provider well-being (i.e., reduced burnout) and patient experience improvements.
Conclusion: These findings shed light on the overall, synergistic value of and business case for investments into developing patient experience improvement programs or activities. However, there is margin for strengthening this body of knowledge in scope, volume, and methods quality, including the need to study the impact on patient experience, provider well-being, health outcomes, and costs (i.e., the quadruple aim) in tandem.
Keywords:
patient experience
; economics
; value
; burnout
Introduction
Patient experience encompasses a spectrum of valuable patient interactions within the healthcare system, such as easy access to information, timely appointments, and effective communication with healthcare providers [1]. A recent systematic review correlated improved patient experiences with better self-reported outcomes and reduced healthcare utilization [2]. Therefore, monitoring and enhancing patient experience, alongside other quality indicators, is crucial for advancing healthcare quality and value.
To facilitate the monitoring of patient experience, the US Agency for Healthcare Research and Quality has established the Consumer Assessment of Healthcare Providers and Systems (CAHPS) program [3]. CAHPS offers standardized patient experience measures, enabling routine monitoring and performance comparisons across providers, influencing consumer choice and encouraging quality improvement. For example, the Centers for Medicare & Medicaid Services (CMS) use CAHPS measures for case-mix adjusted public reporting of patient experience ratings, aligning with other quality indicators [4]. Furthermore, the CMS's Hospital Value-Based Purchasing (VBP) Program, initiated in 2013, incorporates value-based incentives, including CAHPS-measured patient experience performance, to reward providers for key quality indicators [5].
Following value-based incentives and responding to market pressures such as customer loyalty, public reporting of patient experience data, online reviews, and social media accounts [6], health care systems and providers are actively striving to enhance their patient experience performance. To achieve this goal, healthcare organizations have various options. These include investments in patient-experience improvement programs, engaging in quality-improvement activities (e.g., in-service communication training [7]), and implementing new structures like patient experience offices[8] to support these improvement programs.
This review is developed from the standpoint that initiatives for improving the patient experience, when effective, can lead to improved value of care or returns for the investment. For example, improvements may lead to enhanced value-based reimbursements and increased patient volume due to factors such as consumer loyalty, positive word-of-mouth marketing, or favorable online reviews [8,9]. In addition to potential financial returns, initiatives to enhance patient experience can positively impact provider engagement and well-being [10,11].
Viewing healthcare through the lens of relationship-centered care, which recognizes the interdependence of patient-provider interactions [12], suggests that organizations fostering initiatives to improve patient experience may also elevate staff engagement, joy at work, and overall well-being. If so, this contributes to the quadruple aim, which incorporates patient experience, cost, and provider experience alongside population health outcomes among the goals for quality improvement [13,14]. Furthermore, organizational initiatives emphasizing person-centered tenets can promote staff engagement and activation [15], reinforce a climate of compassionate and relational care, and ultimately improve provider well-being and staff retention [16,17].
However, the value of patient-experience improvement activities has not been definitively established or systematically synthesized. For instance, there is a gap in the literature concerning the economic impact of patient-experience improvement activities as well as the impact on their provider well-being or other value-based outcomes. Our review addresses two key questions:
1) What is the economic impact on healthcare organizations of patient-experience improvement interventions?
2) Are there additional value-based impacts, such as improved provider well-being/burnout or reduced healthcare utilization, arising from these interventions?
These findings aim to inform healthcare administrators about the potential supplementary value from investments in patient-experience improvement activities.
Materials and Methods
Design:
This study refers to a systematic review, whose protocol was registered in the PROSPERO database (CRD42022358337). While this systematic review protocol focuses both on the effectiveness and value of health-service interventions targeting improvements in patient experience, the systematic review described in this paper focuses on the value-based component. Reporting follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.[18]
Eligibility criteria:
To answer both review questions, we included empirical studies (e.g., controlled experiments, longitudinal observational studies on the impact of program/ intervention, pre-post test designs) of all activities targeting improvements in patient experience that also reported financial components or other value-based outcomes (e.g., burnout, readmission rates, healthcare utilization). There were no limits placed on health care settings, geography, or health conditions. We excluded improvement or training activities focused exclusively on students or clinicians-in-training (e.g., residents, students in fieldwork placements) and those not using standardized measures or inferential statistics for evaluating the outcomes. Finally, as planned in the protocol, we excluded studies not reported in English or published before 2015, as we looked for contemporary evidence accessible to an international readership.
Search process:
Six scientific literature databases (PubMed/Medline, EconLit, CINAHL, PsycINFO, DOAJ, and Scopus) were searched using a combination of free-text words with indexed terms. We used terms for patient experience or related to methods to collect or improve those experiences (e.g., experience-based codesign, experience rounding). These keywords were combined with a broad set of keywords on health services management and improvement approaches. No restriction was applied to country or health service type. The most recent search was updated until December 2024. Supplementary Table 1 provides details about the complete search.
The databases searches were complemented by targeted searches within specific peer-reviewed journals with a track record of publishing on patient experience activities. These journals include the Patient Experience Journal, Journal of Patient Experience, Medical Care, and Health Expectations. NEJM Catalyst Innovations in Care Delivery was also searched for publications since January 2020, when the journal became peer-reviewed. Finally, we applied snowball strategies (e.g., author-tracking, citation-tracking) using the final included articles and any related systematic or scoping reviews, including those identified through the initial searches.
Selection of papers and data extraction:
Two independent reviewers were used for title-and-abstracts screening and full-text selection; two rounds of discussion among the reviewers were sufficient to achieve agreement. The research team constructed a tailored data extraction table, which included data on a) study characteristics (e.g., study design, objective, country, settings, measures used, analytic approaches), b) interventions used and their impact on patient experience scores, c) any economic analyses and their findings (i.e., on financial variables or indicators assessed, sources of these data, economic analysis type and methods used, and the results of these analyses), d) any additional analyses and findings on provider well-being / burnout or quality-of-care outcomes. Data extraction was performed by the lead author and then fully verified by another author for accuracy and completeness.
Quality assessment (risk-of-bias assessment):
We used a two-level quality assessment. First, we assessed the methodological quality of the overall study design, according to design type. For controlled experiments, we used the Cochrane-suggested risk-of-bias criteria for Effective Practice and Organization of Care reviews. In turn, for pre-post and observational studies we used quality assessment tools from National Institutes of Health. Finally, for the studies that also contain economic assessments, we additionally used the Joanna Briggs Institute’s critical appraisal checklist for economic evaluations. Two independent reviewers performed each assessment, with a third reviewer involved in resolving any conflicts.
Data synthesis:
The study methods, indicators, and quantitative findings, with a focus on the economic and other value-based assessments, were then tabulated and narratively synthesized to address each review question. Due to the heterogeneity of contexts and study designs, meta-analysis was not possible.
Results
Figure 1 provides the PRISMA flowchart of this review. Out of 1317 unique references, 144 full texts were assessed, and nine were included - all from the USA. Of the nine studies on patient experience that also assessed other value-based impacts, five focused on economic impact, three on provider well-being / burnout, and four on healthcare utilization. Two studies that assessed readmission rates also assessed economic impacts, i.e., fit in both categories.
The methodological quality of the economic impact evaluations ranged from a few methodological concerns such as the use of estimated versus actual reimbursement [19] to a paper with no details about how the financial results were obtained [20]. Supplementary Table 2 and Supplementary Table 3, respectively, provide a synthesis of the methodological quality assessment of each study (for both the underlying study design and economic evaluation component, where applicable), based on the respective quality assessment
checklists. The key methodological features of each paper provide the context to the synthesized findings below for each review question.
Economic Impact of the Patient-Experience Improvement Interventions
Table 1 provides synthesized details of the four studies on the improvement of patient experience that also assessed the economic impact - on costs, revenue, operating margin or combinations of these. All these studies showed significant changes in at least in some of its dimensions (e.g., in five of 11 assessed items [19]).
Below, we synthesize the economic findings and methods, organized by intervention type.
Discharge Support
Two studies focused on this intervention type (Table 1). A controlled before-and-after study with historical controls and adjustment for price changes found that a telephone-based transitional support cost an additional $430 per patient compared to usual care. The increased cost was statistically significant, in both the univariate and multivariate models (p<.01 and p=.03, respectively). But the same models showed no significant changes for hospital margin (p=.25 and p=.23, respectively) [19], suggesting that improved revenues were offsetting the increased cost of the intervention.
intervention type (Table 1). The study found that communication training for the surgeons (n= 56) of a children’s hospital increased hospital revenue (payments by 25% and charges by 21%), after adjusting for yearly price changes. In the same study, a small, controlled subgroup analysis (surgeons; n= 8) showed that payments and charges increased further (by 71% and 113%, respectively) for the plastic surgeons who received communication training, while revenue decreased for surgeons who did not receive the training [7].
Patient Experience Office
Finally, we included a secondary analysis (i.e., observational, retrospective, comparative study) of the financial impact of operating a patient experience office in a national sample of 132 hospitals [8]. Years of the office’s operation were negatively yet weakly associated with the operating costs (b= -0.18, p< 0.10). These results support a 1.4% reduction in operating costs for each added year of the office’s operation which, according to supplementary key-informant interviews, are likely a result of efficiencies in communication trainings, improved outcomes, greater patient volumes, and better value-based reimbursements [8].
Other Value-Based Impacts of Patient-Experience Improvement Interventions
Seven studies on the improvement of patient experience with care also assessed other value-based impacts such as provider well-being / burnout (n= 3) and readmission rates (n= 4). Of note, two of the latter [19,20] also assessed economic impacts and, therefore, have some components described in Table 1.
Provider Well-Being/Burnout Outcomes
Table 2. summarizes the three studies assessing the impact of patient experience improvement interventions with provider well-being or burnout, all using a pre-post design and employing physician communication training interventions. well-being. Two pre-post studies were relatively large (physicians trained= 104 [21] and 947 [11]), and the smaller study (physicians trained = 30) was part of a randomized controlled trial (RCT) – i.e., pre-post study for the burnout outcomes and RCT for the patient experience outcomes [10].
All three studies found positive impacts on the patient experience of care, although the smaller only for patient experience scores (i.e., not on percentile ranks, among peer-providers) [10]. All three also found improvements in provider well-being or burnout. The smaller study found significant improvements in two of the subscales of the Maslach Burnout Inventory [10], while the largest found gains for all three subscales, with improvements on two subscales sustained after three months [11]. Finally, the remaining study found statistically significant positive impacts on three out of five burnout subscales measured with the Professional Fulfillment Index (Table 3), although not if Bonferroni corrections were applied (supplementary table 2) [21].
Healthcare Utilization (e.g., Readmission Rates, Emergency Room Visits)
Table 3 describes four studies on improving the patient experience with post-discharge support or transitional care that also assessed the intervention’s impact on readmission rates.
One study found statistically significant impacts on health care utilization in the planned analyses. In a pragmatic randomized controlled trial of transitional care, no significant between-group differences in healthcare utilization (outpatient visit, hospitalization, emergency room visits) were found within 60 days [22]. In a controlled before-and-after study of telephone-based post-discharge support, no significant between-group difference was found for 90-day readmissions (p= .21) [19]. In the pre-pre-post study of discharge support, no significant differences in readmission rates were found [20]. Finally, a casecontrol study found no effects on readmission outcomes from a pharmacist-led, pre- and post-discharge education and medication reconciliation intervention; only in an unplanned subgroup analysis (for the post-discharge component) did the study find pre-post reductions on 30-day readmission rates: 17.3%–12.4% (p=.007) [23].
Discussion
This review synthesizes recent peer-reviewed literature spanning 2015-2024, focusing on the synergistic value-based assessments of patient-experience improvement interventions. Emphasis was placed on economic impacts, provider well-being, and healthcare utilization outcomes. The synthesized interventions focused on provider-communication training or post-discharge and transitional support. These interventions showed effectiveness in improving selected dimensions of patient experience and were coupled with either fiscal neutrality (e.g., costs offset by improved revenue [19]) or positive financial returns such as improved revenue [7]). Reduced healthcare utilization was not found in the target outcomes of studies on discharge and transitional care processes [19,20,22,23]. Nonetheless, these processes resulted in economic benefits [20] or neutrality [19]. These results align with secondary correlational studies, demonstrating positive associations of patient experience scores with health organizations’ financial performance [20,24,25].
From a broader value-based perspective, interventions targeting provider communication have been shown to yield gains in provider well-being and reduce burnout [10,11,21]. Through the lens of relationship-centered care, it is hypothesized that improving patient-provider communication can positively impact patient as well as provider experiences, which are viewed as dynamically interconnected [12]. The improvement mechanism may involve fostering staff engagement with compassionate and relational care, contrasting with instrumental organizational climates that can negatively affect provider well-being and sense of accomplishment [15,16,17,26].
Initiatives for improving patient-provider communication may have high synergistic potential and even potentially contribute to all four components of a value-based perspective focused on the quadruple aim: population health, cost, patient experience, and provider wellbeing [13,14]. Here we found that these initiatives can have positive financial, patient experience, and provider wellbeing impacts, and synergistically so. In turn, in the broader literature, better patient experience scores have been correlated with improved self-reported patient health outcomes [2], including through enhanced shared decision-making [27]. Therefore, an enhanced value proposition may apply to organizational activities that aim to improve patient-provider communication.
Additionally, enhancing provider well-being can offer significant value to healthcare organizations grappling with challenges in recruiting, retaining, and maintaining an engaged and productive staff. High vacancy and turnover rates entail various costs, including recruitment and retention expenses, continual retraining of new staff, the inability to meet heightened demands due to staff shortages, and potential risks to reliability resulting from uncoordinated team processes [13,28]. Notably, the potential benefits of these factors were not assessed or quantified in the reviewed literature and may be further avenues for research.
Similarly, the literature did not explore the potential reduction in litigation costs, despite the plausibility of such benefits. Improved communication practices, a frequent determinant of litigation, could lead to diminished legal costs or malpractice premiums [29]. Lastly, there were no included studies on patient-experience improvement activities beyond provider communication or post-discharge support (e.g., real-time patient experience feedback[30,31]). Exploring these avenues could provide further opportunities to investigate the synergistic value of activities aimed at enhancing patient experience.
While the literature primarily focuses on the United States, this trend may stem from a combination of factors. The CMS Value-Based Purchasing program offers incentives to U.S. health providers based on quality and patient experience metrics, potentially motivating health organizations in the U.S. to invest in and study patient-experience improvement activities. However, caution must be taken regarding the generalizability of the results from this review to other contexts, where the same incentives and returns may not apply. Additionally, the U.S. operates under a consumer-based healthcare delivery system, where consumers' choices for providers are influenced by lived patient experiences, word-of-mouth recommendations, online reviews, and comparison websites [6]. This dynamic places the financial strength of healthcare organizations at risk based on their performance in patient experience. Consequently, these incentives are likely drivers for increasing organizational investments in patient-experience improvement structures and activities in the U.S. [8], fostering an enhanced interest in studying the business case for such investments.
Limitations:
These results should be taken with caution, apart from the generalizability for outside of the US context. First, the volume of the literature was not large, and controlled study designs were rare. We only covered English-language peer-reviewed literature, while many economic analyses of patient-experience improvement activities may be in the grey literature or even non-published, internal analyses. Many health-sector contexts, such as primary care settings and safety-net hospitals, were not adequately represented in the reviewed literature. Furthermore, the economic analyses exhibited a spectrum of methodological rigor, ranging from no substantive risks of bias to a complete underreporting of methods, resulting in significant variability. Collectively, these methodological weaknesses and variations in study designs pose challenges to the robustness of the body of knowledge derived from this review.
Conclusions
The findings of this review, based on literature from the U.S. context, underscore the potential financial and employee well-being benefits associated with investments in activities targeting and effectively achieving improvements in patient experiences with care. These results contribute to the value-based argument for healthcare administrators to prioritize investments in patient-experience improvement activities, with a particular emphasis on enhancing patient-provider communication.
However, it is essential to approach these findings with caution, considering the substantive potential for strengthening this body of knowledge in terms of scope, volume, and methodological quality. Opportunities exist for incorporating additional economic variables, such as malpractice litigation costs and factors secondary to employee engagement and retention. Additionally, further research could explore the impact on the quadruple aim, encompassing patient experience, provider well-being, clinical effectiveness, and costs, particularly when examined in tandem.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Acknowledgments
Not applicable.
References
- Agency for Healthcare Research and Quality. What Is Patient Experience? Rockville, MD [December 2022]. Available from: https://www.ahrq.gov/cahps/about-cahps/patient-experience/index.html.
- Navarro S, Ochoa CY, Chan E, Du S, Farias AJ. Will Improvements in Patient Experience With Care Impact Clinical and Quality of Care Outcomes?: A Systematic Review. Medical care. 2021;59(9):843-56. Epub 2021/06/25. [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. The CAHPS Program Rockville, MD [December 22]. Available from: https://www.ahrq.gov/cahps/about-cahps/cahps-program/index.html.
- Medicare.gov. Find & compare providers near you 2022 [cited 2022 December 21].
- Elliott MN, Beckett MK, Lehrman WG, Cleary P, Cohea CW, Giordano LA, et al. Understanding The Role Played By Medicare’s Patient Experience Points System In Hospital Reimbursement. Health Affairs. 2016;35(9):1673-80. [CrossRef]
- Adams C, Walpola R, Schembri AM, Harrison R. The ultimate question? Evaluating the use of Net Promoter Score in healthcare: A systematic review. Health expectations : an international journal of public participation in health care and health policy. 2022. Epub 2022/08/20. [CrossRef] [PubMed]
- Abu-Ghname A, Davis MJ, Shook JE, Reece EM, Hollier LH, Jr. Press Ganey: Patient-Centered Communication Drives Provider and Hospital Revenue. Plastic and reconstructive surgery. 2021;147(2):526-35. Epub 2021/02/11. [CrossRef] [PubMed]
- Sharma L, Chandrasekaran A, Bendoly E. Does the Office of Patient Experience Matter in Improving Delivery of Care? Production and Operations Management. 2020;29(4):833-55. [PubMed]
- Boissy A. Getting to Patient-Centered Care in a Post–Covid-19 Digital World: A Proposal for Novel Surveys, Methodology, and Patient Experience Maturity Assessment. NEJM Catalyst. 2020. [CrossRef]
- Congiusta S, Ascher EM, Ahn S, Nash IS. The Use of Online Physician Training Can Improve Patient Experience and Physician Burnout. Am J Med Qual. 2020;35(3):258-64. [CrossRef]
- Boissy A, Windover AK, Bokar D, Karafa M, Neuendorf K, Frankel RM, et al. Communication Skills Training for Physicians Improves Patient Satisfaction. Journal of general internal medicine. 2016;31(7):755-61. Epub 2016/02/28. [CrossRef] [PubMed] [PubMed Central]
- Beach MC, Inui T. Relationship-centered care. A constructive reframing. Journal of general internal medicine. 2006;21 Suppl 1(Suppl 1):S3-8. [CrossRef] [PubMed] [PubMed Central]
- Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573-6. Epub 2014/11/12. [CrossRef] [PubMed] [PubMed Central]
- Fitzpatrick B, Bloore K, Blake N. Joy in Work and Reducing Nurse Burnout: From Triple Aim to Quadruple Aim. AACN Adv Crit Care. 2019;30(2):185-8. [CrossRef] [PubMed]
- Howell TG, Mylod DE, Lee TH, Shanafelt T, Prissel P. Physician Burnout, Resilience, and Patient Experience in a Community Practice: Correlations and the Central Role of Activation. Journal of Patient Experience. 2019;7(6):1491-500. [CrossRef]
- Porter TH, Rathert C, Ishqaidef G, Simmons DR. System justification theory as a foundation for understanding relations among toxic health care workplaces, bullying, and psychological safety. Health Care Manage Rev. 2024;49(1):59-67. [CrossRef] [PubMed]
- Rathert C, Vogus T, Hearld LR. Psychological work climates and health care worker well-being. Health Care Manage Rev. 2024;49(2):85. [CrossRef] [PubMed]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. 2021;372:n71. Epub 20210329. [CrossRef] [PubMed] [PubMed Central]
- Schreiter NA, Fisher A, Barrett JR, Acher A, Sell L, Edwards D, et al. A telephone-based surgical transitional care program with improved patient satisfaction scores and fiscal neutrality. Surgery. 2021;169(2):347-55. Epub 2020/10/24. [CrossRef] [PubMed]
- Thum A, Ackermann L, Edger MB, Riggio J. Improving the Discharge Experience of Hospital Patients Through Standard Tools and Methods of Education. Journal for Healthcare Quality: Promoting Excellence in Healthcare. 2022;44(2):113-21. Language: English. Entry Date: 20220419. Revision Date: 20220419. Publication Type: Article. [CrossRef] [PubMed]
- Altamirano J, Kline M, Schwartz R, Fassiotto M, Maldonado Y, Weimer-Elder B. The effect of a relationship-centered communication program on patient experience and provider wellness. Patient education and counseling. 2022;105(7):1988-95. Epub 2021/11/14. [CrossRef] [PubMed]
- LaBedz SL, Prieto-Centurion V, Mutso A, Basu S, Bracken NE, Calhoun EA, et al. Pragmatic Clinical Trial to Improve Patient Experience Among Adults During Transitions from Hospital to Home: the PArTNER study. Journal of general internal medicine. 2022;37(16):4103-11. Epub 20220308. [CrossRef] [PubMed] [PubMed Central]
- March KL, Peters MJ, Finch CK, Roberts LA, McLean KM, Covert AM, et al. Pharmacist Transition-of-Care Services Improve Patient Satisfaction and Decrease Hospital Readmissions. Journal of pharmacy practice. 2022;35(1):86-93. Epub 2020/09/19. [CrossRef] [PubMed]
- Akinleye DD, McNutt LA, Lazariu V, McLaughlin CC. Correlation between hospital finances and quality and safety of patient care. PloS one. 2019;14(8):e0219124. Epub 2019/08/17. [CrossRef] [PubMed] [PubMed Central]
- Richter JP, Muhlestein DB. Patient experience and hospital profitability: Is there a link? Health care management review. 2017;42(3):247-57. Epub 2016/04/07. [CrossRef] [PubMed]
- Jesus TS, Stern BZ, Struhar J, Deutsch A, Heinemann AW. The use of patient experience feedback in rehabilitation quality improvement and codesign activities: Scoping review of the literature. Clin Rehabil. 2023;37(2):261-76. Epub 20220916. [CrossRef] [PubMed]
- Elwyn G, Frosch DL, Kobrin S. Implementing shared decision-making: consider all the consequences. Implementation science : IS. 2016;11:114. Epub 2016/08/10. [CrossRef] [PubMed] [PubMed Central]
- Coulmont M, Roy C, Dumas L. Does the Planetree patient-centered approach to care pay off?: a cost-benefit analysis. The health care manager. 2013;32(1):87-95. Epub 2013/02/01. [CrossRef] [PubMed]
- Lee VS, Miller T, Daniels C, Paine M, Gresh B, Betz AL. Creating the Exceptional Patient Experience in One Academic Health System. Acad Med. 2016;91(3):338-44. [CrossRef] [PubMed] [PubMed Central]
- Jesus TS, Struhar J, Zhang M, Lee D, Stern BZ, Heinemann AW, et al. Near real-time patient experience feedback with data relay to providers: a systematic review of its effectiveness. Int J Qual Health Care. 2024;36(2). [CrossRef] [PubMed]
- Khanbhai M, Flott K, Darzi A, Mayer E. Evaluating Digital Maturity and Patient Acceptability of Real-Time Patient Experience Feedback Systems: Systematic Review. J Med Internet Res. 2019;21(1):e9076. Epub 20190114. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
PRISMA flowchart of the review .
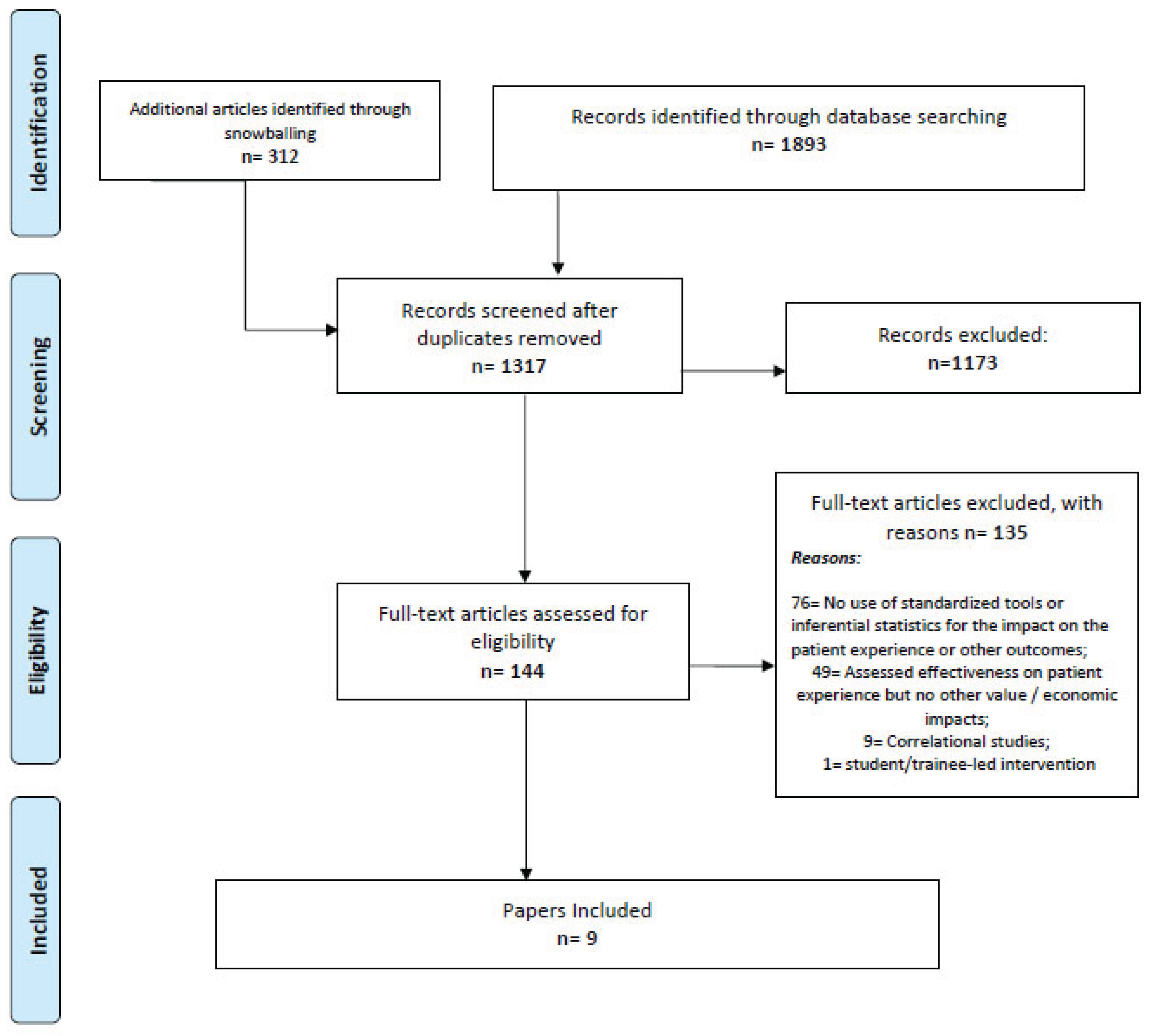

Table 1.
The costs and benefit of interventions aimed at improving the patient experience of care, ordered by date of publication.
Table 1.
The costs and benefit of interventions aimed at improving the patient experience of care, ordered by date of publication.
| Patient Experience Component | Economic Component | |||||
|---|---|---|---|---|---|---|
| Design & Context | Intervention (synthesis) | Patient Experience Outcomes (synthesis) | Economic Indicator(s) & Data | Economic Analysis & Methods | Economic outcomes | |
| (Thum, Ackermann et al. 2022) | Pre-post test, 12 months each. Academic hospital and its community hospital affiliate. | Discharge support: Nurses were trained in teach back; workflow was redesigned. A new discharge summary was created, linked to a hard stop in the electronic health record. | Improved top box %s: Care Transitions, 52.4–54.5% (p< .001); Discharge Information, 87.4–90.1% (p< .001). Improved percentile rank: 45.2–74.3 (p= .020) for Discharge Information. | Revenue; Unspecified internal organizational data | Hospital Revenue impact analysis, pre- and post-intervention Unspecified methods. | The intervention had a positive impact on the value-based purchasing program, with an estimated savings of $75,000 compared to the pre-intervention expectations due to better patient experience scores: Care Transitions and Discharge Information domains. |
| (Schreiter, Fisher et al. 2021) | Controlled before-and-after, historical cohort of controls. Academic hospital. | Post-discharge support: Telephone follow-up delivered by nurses after hospital discharge for patient education, medication reconciliation, or remediation care (e.g., same-day clinic appointment) if required. | Intervention got greater %s of top-box scores in 5 of 11 items: asking about having the needed help (100% vs. 93%, p<.01), educational materials (68% vs. 55% p< .01), understanding of responsibilities (69% vs. 59%, p= .02), instructions on whom to call with post discharge questions (76% vs. 69%; p= .04), and global experience (57% vs. 46%, p= .02). | Costs: Total hospital costs and transitional care expenses (new nurses’ salaries and fringe; infrastructure investments negligible). Margin: Estimated payer reimbursements subtracting the total hospital costs. | Hospital Costs & Margin Impact. Fiscal data converted to 2017 US dollars using Consumer Price Index. Wilcoxon rank-sum test to compare groups’ fiscal data. Predictive multivariable models of cost and margin for index admission, 90-day readmission, and aggregate. Covariates were those with statistical and clinical relevance (e.g., age). | The intervention cost +$430 per patient; the rank-sum comparison for aggregate 90-day admissions showed between-group differences for the hospital cost ($25,827 vs $22,814, p<.01) but not the margin: $4.698 (95% CI: -2.85–21,100) vs $7.027 (-1.36–20,734), p=.25. The multivariable model showed similarly significant results (cost differences: p=.03; margin differences; p=.23). |
| (Abu-Ghname, Davis et al. 2021) | Pre-post test, retrospective, one site; controlled subgroup analysis for plastic surgeons. Children's hospital. | Communication training: 5.5h course led by two volunteer practicing clinicians trained in-house (in facilitation in a model of relationship-centered care). The course featured role-playing of the communication skills. | Improvements in the scope of provider recommendation (90.7-94.1; p<.001), language (90.9-94.0; p=.007), concern (91.4-94.1; p=.007), decision sharing (91.8-94.3; p=.001), and information (94.0-95.4; p=.031). | Revenue, in charges (the amount billed by the hospital) and in payments (the amount of reimbursements received). Internal organizational data adjusted for price increases. | Hospital Revenue, pre-post impact: total charges and overall payments (plus # of distinct patients and encounters). To control for price changes, revenue was compared after controlling for calendar year 2016 per-unit charges (Current Procedural Terminology). | Payments increased by 25%, and charges increased by 21% - clinical encounters increased by 26%, and the number of patients increased by 26%. Specifically for the subgroup of plastic surgeons, participants reported 113% increases in charges and 71% increases in payments, whereas controls had decreases of 10% in charges and 4% in payments. |
| (Sharma, Chandrasekaran et al. 2020) | Retrospective comparative study. National sample of hospitals. Key informant interviews (1 hospital). | Office of Patient Experience (OPX): Patient experience office as a new administrative structure with its own budget and staff and a head who is an executive board member (versus hospital without that structure). | A 1.95% increase was found in experiential quality per year of operation (p<.05), more so for hospitals with high vs low patient complexity (6.5% vs -0.3%, p< .05). | Operating Costs. Any expenses incurred in every aspect of a hospital’s operations, including salaries, supplies, and administrative expenses. CMS Cost Reports | Hospital Operating Costs impact: proxy for the cost of setting up & running an OPX. Once computed from the CMS Cost Reports, operating costs were divided by the # of beds to normalize it for size. A natural log of cost per bed was used to reduce the impact of outliers. Fixed effects instrumental variable regression with years of OPX operation as the predictor. | Years of operation were weakly associated with reduced operating costs (b= -0.18, p< 0.10). It translates into a 1.4% operating-costs reduction per added year of operation. Interviews suggest efficiencies in trainings, improved outcomes due to better provider communication, greater patient volumes due to satisfaction and word of mouth, and better value-based reimbursement. |
Table 2.
Wellbeing outcomes from interventions aimed at improving the patient experience of care, ordered by date of publication.
Table 2.
Wellbeing outcomes from interventions aimed at improving the patient experience of care, ordered by date of publication.
| Patient Experience Component | Wellness outcomes | ||||
| Study Design & Context | Intervention (synthesis) | Patient Experience Outcomes (synthesis) |
Outcome(s) type and Measure | Outcomes | |
| (Altamirano, Kline et al. 2022) | Pre-post test, 3 months post intervention, four sites. Academic hospital - four sites, multi- department. | Communication training: training (8h) in workshops (n= 48; 14 seats each), led by trained peer physicians. After nomination by department chairs, a board selected instructors on 6 criteria: e.g., patient experience scores, thought leader for communication. Instructors had training toward certification. Trainees applied the skills to cases elicited during the workshop followed by small group feedback. Continuing education credits were provided. | Top-box scores increased from 82.8% to 84.5% (p<.0001). The odds of receiving a top-box score 6 months after the program vs prior (1.11, p= .01) and >6 months (1.15, p< .0001) also increased. Gains persisted in a propensity score weighted analysis (1.09, p= .04; 1.14, p< .0001). When stratified by site, two of four had significant improvements. | Burnout/Wellness, Professional Fulfillment Index subscales: burnout, compassionate self-improvement, professional fulfillment, emotional exhaustion, and interpersonal disengagement. | Burnout decreased significantly from 35% to 26% (p< .039). In addition, compassionate self-improvement and professional fulfillment increased from 37% to 50% (p< .020) and from 41% to 51% (p< .034). Scores for emotional exhaustion and interpersonal disengagement decreased, but the changes were not statistically significant. |
| (Congiusta, Ascher et al. 2020) | Pre-post test (burnout outcomes) within a RCT (patient experience outcomes), Medical practices. | Communication training: Online provider training weekly for 24 weeks and biweekly conference calls led by top-performing physicians trained in the model and facilitation. Trainees needed to "learn", "do", and "share" the successes in conference calls or a web tool. Team-based breakfast for the best-performers and graduation celebration. | The intervention group had a greater improvement in scores compared to controls (median [Q1, Q3]= 1.6 [0.4, 2.4] vs 0.6 [−1.3, 1.9], p< .039), but no significant difference in the percentile ranks (median [Q1, Q3]= 4.0 [-27.0, 13.0] vs -13.0 [-36.0, 12.0], p < .346). | Burnout: Maslach Burnout Inventory and its three subscales: emotional exhaustion, burnout, depersonalization, and personal achievement | Two of the subscales had significant changes. The depersonalization score was significantly lower than baseline – mean difference (SD) -2.43 (5.30), p< .023), and the personal achievement score increased (mean difference 3.10 (3.62); p = .0007). The decrease in the burnout, total score, nearly reached statistical significance (p= .0504). |
| (Boissy, Windover et al. 2016) | Pre-, post-, and 3-months post study within a controlled, before- and-after study; hospital & clinician group. | Communication training: 8h provider training. Each course (<12 physicians each) was facilitated by two clinicians trained in the communication model, adult learning, performance assessment, and group facilitation. Didactic presentations, live or video-based skill demonstrations, and small-group skills practice sessions were followed by skills practice on communication challenge from trainees’ practices. | Clinicians Group: Adjusted communication scores were greater for the intervention group vs controls (92.09 vs 91.09, p< .03). Hospital: Adjusted respect scores were greater in the intervention vs controls (91.08 vs 88.79, p=.02), but differences were non-significant for the adjusted communication scores (83.95 vs 82.73, p=0.2). | Burnout: Maslach Burnout Inventory and its three subscales: emotional exhaustion, burnout, depersonalization, and personal achievement | Following the course, lower burnout was significantly found on all three subscales (emotional exhaustion: p< .001; depersonalization: p= .003, and personal achievement: p= .04). Improvements in all measures except emotional exhaustion were sustained at 3 months. |
Table 3.
Healthcare utilization outcomes from interventions aimed at improving the patient experience of care, ordered by date of publication.
Table 3.
Healthcare utilization outcomes from interventions aimed at improving the patient experience of care, ordered by date of publication.
| Patient Experience Component | Healthcare utilization outcomes | ||||
| Study Design & Context | Intervention (synthesis) | Patient Experience Outcomes (synthesis) |
Outcome(s) type and Measure | Outcomes | |
| (LaBedz, Prieto-Centurion et al. 2022) | Pragmatic RCT, patient-level randomization. Multivariable linear regression models, with a Bonferroni correction for the co-primary outcomes | Transitional care: The intervention group received an intervention during the index hospitalization and for 60 days post-discharge, which included 1) in-hospital visits by a community health worker to assess barriers to health/healthcare and to develop a personalized Discharge Patient Education Tool (DPET); 2) a post-discharge home visit by a community health worker to review the DPET; and 3) telephone-based peer coaching. | No significant between-group differences in the 30-day change in informational support (adjusted difference: −0.01, 97.5% CI −2.0 to 1.9, p=0.99), or any secondary outcomes such as emotional support [−0.12, 95% CI −1.5, 1.2, p=0.86] or instrumental support [−0.43, 95% CI −1.7, 0.93, p=0.53]. An exploratory subgroup analysis showed greater improvements in 30-day informational support for navigator group participants without health insurance (+11.9, 95% CI 2.3 to 21.4). | Utilization: 14-day outpatient visit, 30-day and 60-day hospitalization or emergency room visits | No significant between-group differences in healthcare utilization (outpatient visit, hospitalization, emergency room visits). |
| (March, Peters et al. 2022) | Observational, case control comparison with retrospective review, single-center, pilot program, hospital-based pharmacy | Patient education and discharge support: Pharmacist-led medication reconciliation and education, sensitive to health literacy levels, prior and post discharge following alerts from the electronic medical record system. | Significant improvement in the top-box scores (52.6% vs. 67.3%; p= <.001) in the composite of medication-related HCAHPS results and its specific items: “tell you what the medicine was for” (67.7% vs. 81.9%; p= .018), “describe possible medicine side effects” (37.7% vs. 58.9%; p= 0.004), and "understood the purpose of taking medications" (52.3% vs. 63.7%; p= .035). | Readmissions: 30-day readmissions. | Non-significant difference in 30-day readmissions for the complete intervention vs non-intervention (16.4% vs 13.3%; p= .133); an unplanned subgroup analysis for the discharge phone calls (with or without discharge education) showed a significant reduction in 30-day readmission rates: 17.3% vs 12.4% (p= .007). |
| (Thum, Ackermann et al. 2022), described in Table 1 | Readmissions: 30-day readmissions | No significant difference pre- to post-intervention (p=.69). | |||
| (Schreiter, Fisher et al. 2021), described in Table 1 | Readmissions: 90-days readmissions | No significant difference between groups (p= .21) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



