
Submitted:
16 May 2025
Posted:
03 June 2025
You are already at the latest version
Abstract
Colorectal cancer (CRC) is ranked as the third most lethal of all cancers in the USA, following prostate and lung malignancy in men, and breast and lung malignancy in women respectively. The risk factors for developing colorectal cancer fall into 2 categories: modifiable risk factors (obesity and physical inactivity, diet, smoking, alcohol, medications, diabetes, and insulin resistance) and non-modifiable risk factors (race and ethnicity, sex, age, and inflammatory bowel disease). The standard therapeutic approaches to the treatment of colorectal cancer have led to a reduction in the burden of colorectal cancer in the USA, with national statistics revealing a reduction in both the incidence and death rates. At the same time, 5-year survival rates have also greatly improved. However, associated with these standard treatments are complications, which have become a burden (physical and emotional, financial, and economic burdens, and disability-adjusted life years), affecting the quality of life of CRC patients. This paper discusses the standard therapeutic approaches to managing colorectal cancer, the associated complications and their management. In addition, a summary of the newly introduced therapeutic approaches for treating CRC, reported improvement in effectiveness over existing strategies and corresponding reduction in therapeutic complications will be discussed.
Keywords:
colorectal cancer
; therapeutic approaches
; complications
1. Introduction
Colorectal cancers are slowly developing cancers that can start as tumors or tissue growth on the inner linings (glandular or epithelial cells) of the rectum or colon to form polyps [1,2]. The polyp can eventually transform into cancerous by forming a tumor on the walls of the rectum or colon. This transformation occurs when the cells of the epithelium experience genetic mutations that confer a selective advantage on them [3,4]. Subsequently, the tumor then grows into blood vessels or lymph vessels, increasing the chances of metastasis to other anatomical sites [1]. The majority (95%) of the cancers that begin in the colorectal region are classified as adenocarcinomas [1,2]. Adenocarcinoma erupts in the mucus making glands that line the colon and rectum [1,2]. The other types that are less prevalent include carcinoid tumors (erupt from hormone-producing intestinal cells), gastrointestinal stromal tumors (erupt from interstitial cells of Cajal), Lymphomas (cancer of the immune systems forming in the colon or rectum), and sarcomas (normally starts from blood vessels, however, occasionally formed in the colorectal walls) [1,2,5]
Colorectal cancer has been ranked as the third deadliest of all cancers in the USA, following prostate cancer and lung cancer in males, and breast cancer and lung cancer in females (8% of all new cases) [1,6]. CRC is also reecognized as the second most costly cancer to treat, accounting for 12.6% of all cancer treatment costs [7]. The total annual medical cost is estimated at $24.3 billion, with $23.7 billion spent on medical services and $0.6 billion spent on prescription drugs [7]. The risk factors for CRC have been broadly categorized into two: non-modifiable risk factors and modifiable risk factors. The non-modifiable risk factors include race and ethnicity, sex, age, and inflammatory bowel disease (IBD). In the US, CRC is more common among African Americans and Native Americans, and they suffer lower survival among all stages of CRC [3]. Based on sex, males have a higher chance (about 1.5-fold) of developing CRC than females across all ages and nations [3,8]. Age greatly influences the incidence of CRC. In the US, people over 65 years old are about three times more likeely to be diagnosed with CRC than people aged 50-64 and a likelihood of 30 times more to be diagnosed than people aged 25-49 years old [3]. Modifiable risk factors include obesity and physical inactivity, diet, smoking, alcohol, medications, diabetes, and insulin resistance [3].
The standard treatment involves surgery combined with radiotherapy and/or chemotherapy, which is highly dependent on the site of the tumor and the progression of the disease [9]. These therapeutic approaches have led to a reduction in the burden of colorectal cancer in the USA, with national statistics revealing a reduction both in the incidence and death rates. At the same time, 5-year survival rates have greatly improved [1]. However, associated with these standard treatments are complications, which have become a burden that affects the quality of life of CRC patients.
The burden associated with complications CRC treatmeent includes physical and emotional, financial, and economic burdens, and disability-adjusted life years [10,11]. In a meta-synthesis study by Rutherford et al., on the patient-reported outcomes and experiences from the perspective of colorectal cancer survivors, it was shown that stoma problems seen in CRC survivors after treatment impair their physical, social, sexual, and psychological functioning of the patients [11]. Furthermore, according to the work of Regenbogen et al., (2014), Patients who reported complications after surgery had a composite financial burden, which makes them more likely to spend their savings, borrow or take loans, fail to pay their credits, have a reduction in the money spent on food and clothing, decrease recreational activities, get worried about their finances, and took longer time to return to work [10]. Thus, the financial stress associated with CRC complications has significant impact on survivors quality of life.
Therefore, therapeutic complications of CRC treatment and the associated burdens necessitate the need for developing strategies for their management to improve the quality of life of the patient. The ultimate goal iss to develop newer therapeutic approaches with fewer complications and burden that would improve compliance of CRC patients with treatment regimen, increase the survival rates, and enhance the overall quality of life of the patients after treatment. The newer therapeutic approaches to achieving these goals include targeted therapy, immunotherapy, and combination therapies, among many others [12,13]. Thus, this paper discusses the standard therapeutic approaches to managing colorectal cancer, the associated complications, and the strategies for managing the complications. In addition, the newer therapeutic approaches developed towards treating CRC, with an improvement over the conventional treatment approaches in effectivenes, and with reduced complications, will be discused.
2. Research Method
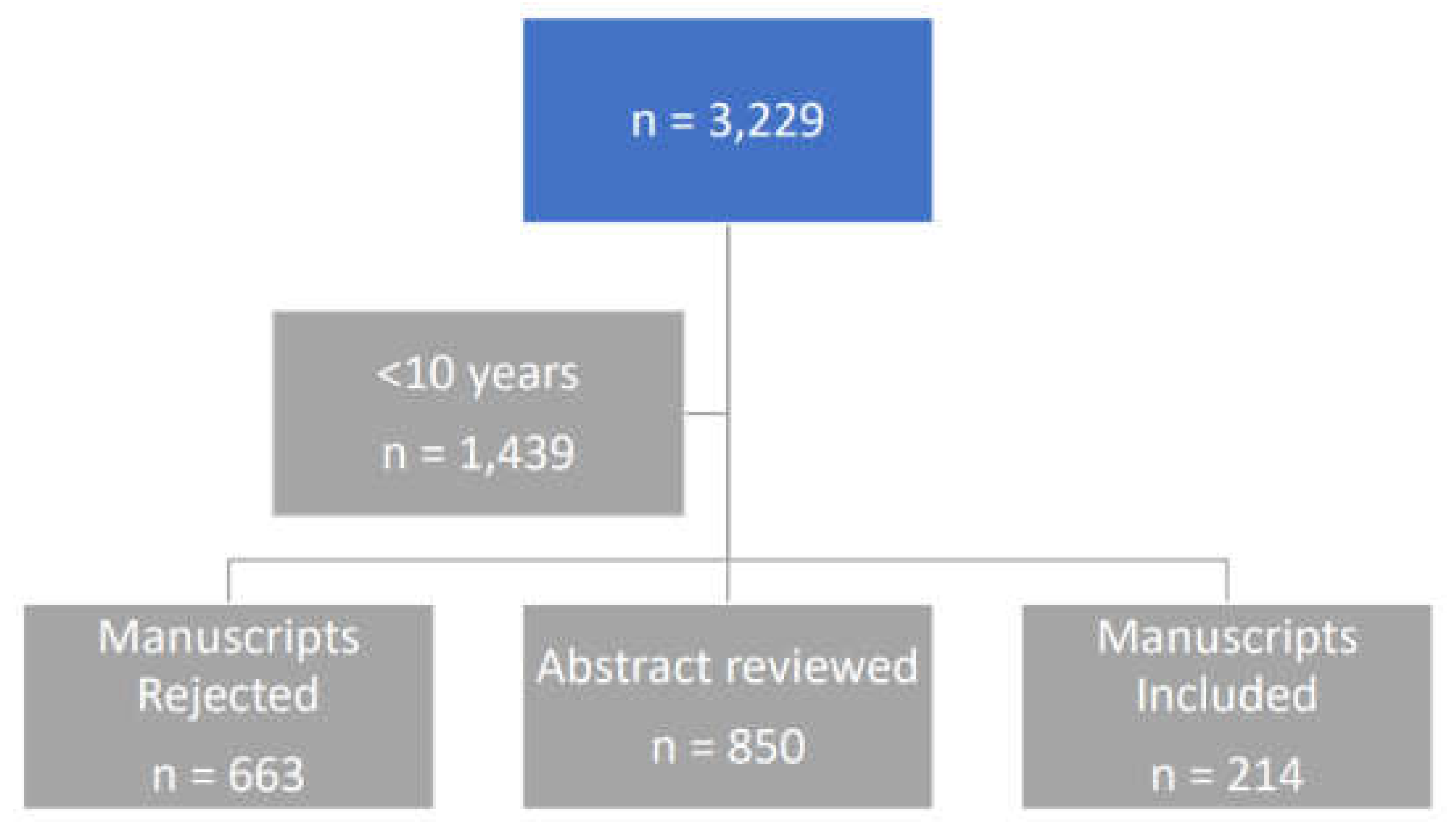
Search strategy: Engine Google Chrome; database: PubMed; search terms: COLORECTAL CANCER, THERAPEUTIC APPROACHES, therapeutic COMPLICATIONS
Returned MESH:
Search: COLORECTAL CANCER, THERAPEUTIC APPROACHES, therapeutic COMPLICATIONS
("colorectal neoplasms OR ("colorectal"[All Fields] AND "neoplasms"[All Fields]) OR "colorectal neoplasms"[All Fields] OR ("colorectal"[All Fields] AND "cancer"[All Fields]) OR "colorectal cancer"[All Fields]) AND ("therapeutical"[All Fields] OR "therapeutically"[All Fields] OR "therapeuticals"[All Fields] OR "therapeutics"[MeSH Terms] OR "therapeutics"[All Fields] OR "therapeutic"[All Fields]) AND ("approach"[All Fields] OR "approach s"[All Fields] OR "approachability"[All Fields] OR "approachable"[All Fields] OR "approache"[All Fields] OR "approached"[All Fields] OR "approaches"[All Fields] OR "approaching"[All Fields] OR "approachs"[All Fields]) AND ("therapeutical"[All Fields] OR "therapeutically"[All Fields] OR "therapeuticals"[All Fields] OR "therapeutics"[MeSH Terms] OR "therapeutics"[All Fields] OR "therapeutic"[All Fields]) AND ("complicances"[All Fields] OR "complicate"[All Fields] OR "complicated"[All Fields] OR "complicates"[All Fields] OR "complicating"[All Fields] OR "complication"[All Fields] OR "complication s"[All Fields] OR "complications"[MeSH Subheading] OR "complications"[All Fields])
Results
THERAPEUTIC APPROACHES IN COLORECTAL CANCER TREATMENT
Table 1 shows therapeutic approaches to colorectal cancer treatment. These include surgical intervention, radiotherapy, chemotherapy, targeted therapy, immunotherapy, and drug combination therapy.
2.1. Surgical Intervention
Surgical intervention is considered to be the most common treatment for CRC patients [14]. Surgical procedure options for CRC are dependent on the site where the tumor is found and the size. The available ones include laparoscopy, radiofrequency ablation, cryoablation, or colostomy [14]. Laparoscopic involves inserting different scopes by making smaller notches into the abdomen [14]. Polypectomy involves the surgical removal of the polyps during colonoscopy [12]. Surgery has been the mainstay curative treatment option in patients with non-metastasized CRC [15]. Surgical removal of the precancerous or cancerous tumor is an effective option and could allow for full recovery of the patient in cases of small, localized cancerous growths [12]. In addition, surgery is for treating solid tumors that have shown resistance to radiation and chemotherapy.
2.2. Radiotherapy
Radiotherapy is one of the mainstay treatment modalities of CRC alongside surgery, chemotherapy, and immunotherapy [16]. It involves the use of ionizing radiation in the management of proliferating tumorous cells [12]. The treatment utilizes ionizing radiation to induce DNA damage by breaking the double-stranded DNA, which leads to cell death [16]. It is used to treat all forms of cancer. However, because of the risk radiation poses to normal tissue, which includes cancers induced by radiation, radiation beams are often aimed at different angles of exposure to ensure the intersection at the tumor. This provides a larger absorbed dose of the radiation directly at the tumor site rather than the regular tissue sites. Different forms of radiation therapy have been reported to be used in the treatment of oligometastasis, which include selective internal radiotherapy (SIRT), trans-arterial chemoembolization (TACE), and radiofrequency ablation (RA) [12].
2.3. Chemotherapy
The treatment of CRC, both at the early stage and at the metastatic stage, is majorly centered on the use of chemotherapy [9]. This method involves destroying the tumor cells through cytotoxicity to the tumor cells which can lead to the suppression of the tumor [12]. The classes of drugs include agents such as alkylating agents, antimetabolites, plant alkaloids, and agents that influence biological responses that could either destroy the tumor cells, suppress the tumor growth, or suppress its cell division [12].
The chemotherapeutic agent that is being used in metastatic cases includes Fluoropyrimidines (5-fluorouracil, 5-FU), oxaliplatin, and irinotecan. Aside from this, treatment also involves the use of multiple agent regimens that combine 5-FU with oxaliplatin (OX), capecitabine (CAP or XELODA or XEL), and irinotecan (IRI) [17]. The core of treatment for advanced CRC involves combining 5-FU and leucovorin with either oxaliplatin or irinotecan. The usage of the chemotherapeutic agent has resulted in a median overall survival ranging from 18 to 20 months [9,17,18].
2.3.1. Fluoropyrimidines
Intravenous Fluorouracil
Fluorouracil (5-FU) is a synthetic fluorinated pyrimidine analog with a general activity through the inhibition of thymidylate synthetase, which is the rate-limiting enzyme in pyrimidine nucleotide synthesis [20,21], thus, inhibiting DNA replication. This has been the mainstay of systemic treatment for colorectal cancer [19]. This is commonly administered with reduced folate, leucovorin, attributed to stabilizing fluorouracil’s interaction with the enzyme [22]. In patients with metastatic cancer, the combination treatment has been shown to reduce the tumor size by 50% or more in about 20% of the patients, and the median survival increased from approximately 6 months to an average of 12 months [23].
Oral Fluoropyrimidines
Oral fluoropyrimidines experience erratic absorption when administered due to the varying concentrations of mucosal catabolic enzyme, dihydropyrimidine dehydrogenase [19]. However, there are two approaches developed to bypass the problem. The first process involves using an absorbable fluorouracil prodrug which is not broken down by the catabolic enzyme, while the second step involves co-administering the drug with a dihydropyrimidine dehydrogenase inhibitor [24]. Examples include Capecitabine, an oral prodrug of fluorouracil that undergoes a 3-conversion step to fluorouracil, while Tegafur Uracil, escapes the erratic intestinal absorption of fluorouracil when they are co-administered with dihydropyrimidine dehydrogenase (Uracil) inhibitor. This permits uniform absorption and bioavailability of the drug.
2.3.2. Topoisomerase Inhibitors (Irinotecan)
Irinotecan is a semisynthetic derivative of a natural alkaloid camptothecin which is often transformed into SN-38 by carboxylesterases [25]. Sn-38 has been reported to cause fragmentation of DNA fragmentation and programmed cell death through the inhibition of topoisomerase I. Topoisomerase I enzyme catalyzes the breaking and rejoining of DNA strands using replication of DNA [19]. It forms a topoisomerase-inhibitor-DNA complex that affects DNA function [21]. Thus, a higher concentration of Topoisomerase I makes the cell more sensitive to Irinotecan [21,26]. Enzymes like Carboxylesterases (CES), β-glucuronidase, uridine diphosphate glucuronosyltransferase (UGT), hepatic cytochrome P-450 enzymes CYP3A, and ATP-binding cassette (ABC) transporter protein play vital roles in the uptake and metabolism of Irinotecan.
SN-38 is metabolized in the liver. It is rendered inactive by a polymorphism in the uridine diphosphate glucuronosyltransferase isoform 1A1 (UGTA1A1) gene through the glucuronidation process and eliminated through the biliary system. The gene causes a reduction in the inactivation of SN-38 followed by a subsequent increase in treatment-related toxicity [27]. The drug is not used in patients having hyperbilirubinemia because of the potential increase in the bilirubin level associated with irinotecan toxicity [19]. Other common toxic effects associated with the drug include diarrhea, myelosuppression, and alopecia.
2.3.3. Platinum Compounds (Oxaliplatin)
Oxaliplatin is a diaminocyclohexane, a 3rd-generation platinum compound that works by forming DNA adducts, leading to the impairment of DNA replication and cellular apoptosis [30] The usage was approved in Europe in 1996, but the USA FDA granted accelerated approval in 2002, and full approval for use in combination with 5-FU granted in 2004 for advanced CRC or mCRC [31]. Although administering singly in patients with mCRC has limited efficacy, however, when administered with fluorouracil and leucovorin, there is significant clinical benefit observed. This has been linked to the possibility of oxaliplatin-induced down-regulation of thymidylate synthetase [19].
Oxaliplatin has a 1,2-diaminocyclohexane ligand (DACH), a unique feature in the structure that differentiates it from other platinum compounds. DACH makes it difficult for DNA repair, thereby improving the tumor cell-killing effect of oxaliplatin [21]. The toxic effect of oxaliplatin is manifested through cumulative sensory neuropathy, with features of paresthesia of the hands and feet.
Clinical studies have shown that adding oxaliplatin to the infusion of fluorouracil and leucovorin (FOLXOX) enhanced the tumor response rate and disease-free survival, having a trend that depicts an increase in overall survival [19].
2.3.4. Antimetabolites (Capecitabine)
This is the earliest oral chemotherapeutic drug that was developed for treating CRC. When metabolized inside the system, it is changed to 5’-deoxy-5-fluorocytidine (5’-OFCR) and 5’-deoxy-5- fluorouridine (5’-DFUR). Thereafter, TP ultimately hydrolyzes 5’-DFUR to 5-FU, exerting its cytotoxic activities. The multinational phase III trial has provided evidence to support the combined therapy containing Capecitabine and irinotecan (XELIRI), with or without Bevacizumab, as a 2nd-line treatment modality in patients having mCRC [21,32,33].
2.4. Targeted Therapy
Targeted therapies are known to work on cancerous cells through the inhibition of cell proliferation, differentiation, and migration. They can also alter the tumor microenvironment, including local blood vessels and immune cells, impeding tumor development and exerting robust surveillance and assault from the immune systems [17]. Smaller molecules have been a major player in targeted therapies. These set of molecules, like monoclonal antibodies, because of their molecular weight (<900Da), have a strong ability to penetrate cancerous cells [17]. They work within the cell to render inactive selected enzymes, which inhibit cancer cell growth and, in addition, prompt apoptosis. The molecular targets include cyclin-dependent kinases, proteasomes, and poly ADP-ribose polymerase [17].
In another way, the targets outside the cell, including receptors on the cell surface or other sites bound on the membrane, can be recognized by monoclonal antibodies or therapeutic antibodies, which bind them to exert direct regulation of the downstream cell cycle progression and cell death. Furthermore, there is a report that certain monoclonal antibodies target other cells different from tumor cells, like immune cells, that can influence the immune system to attack human cancer [17]
The pathways that facilitate initiation, progression, and migration of CRC, like Wnt/β-catenin, Notch, Hedgehog, and TGF-β (transforming growth factor-β)/SMAD, and inclusively, those capable of activating signaling cascades, like phosphatidylinositol 3-kinase (PI3K)/AKT or RAS/rapidly accelerated fibrosarcoma (RAF) are potential sites for cancer targets and druggability [17]
Following chemotherapy, targeted therapies, like monoclonal antibodies and small molecule inhibitors, have been an effective treatment option in CRC patients. Target therapy involves targeting specific genes and proteins, hindering the growth and survival of the cancer cells [14]. Targeting monoclonal antibodies to vascular endothelial growth factors (VEGF) and epidermal growth factor receptor (EGFR), enhanced the overall survival for CRC to 3 years [21]. They are known to exhibit lower side effects as compared to chemotherapy [21].
2.4.1. Angiogenesis inhibitors
Angiogenesis plays a great role in tumor growth and survival [31]. Hypoxia in the tumor microenvironment (TME) is associated with upregulating hypoxia-inducible factor (HIF), followed by the induction of the production of vascular endothelial growth factor (VEGF) [34]. The overexpression of the VEGF gene and the high levels of circulating VEGF protein have been linked with a flawed prognosis in CRC [35]. Angiogenesis involves the establishment of new blood vessels by the cancer to feed the tumor cells with nutrient and oxygen supply. Angiogenesis inhibition has been recognized as a strategy for controlling malignant proliferation and its spread [19]. The current focus in the antiangiogenic strategy involves the inhibition of vascular endothelial growth factor (VEGF) [19]. VEGF is a soluble protein that promotes blood vessel proliferation.
Bevacizumab is an antiangiogenic drug in this class, and the first to precisely target VEGF, leading to the reduction in tumor growth. It is a humanized monoclonal antibody used against VEGF, combined with chemotherapy in patients with advanced CRC [19]. Bevacizumab works through the reduction of the formation of new blood vessels needed by growing tumors for continuous development [31]. Though Bevacizumab is well tolerated, it has a mild toxic effect of reversible hypertension and proteinuria. Rare cases of toxicity include bowel perforation, serious bleeding events, risk of arterial embolic events, and reversible posterior leukoencephalopathy syndrome [36,37,38]. Clinical studies show improvement in tumor response rate and progression-free survival when Bevacizumab is administered with Fluorouracil and Leucovorin in patients with metastatic colorectal cancer. In addition, adding Bevacizumab to FOLFIRI or FOLFOX in patients having untreated, mCRC has established an enhanced rate of response and progression-free survival times [39].
2.4.2. Epidermal Growth Factor Receptor (EGFR) Inhibitors
To inhibit the function of EGFR receptor, scientists have developed several antibodies targeted to the extracellular domain of EGFR coupled with small molecular inhibitors of the intracellular tyrosine kinase domain, with only anti-EGFR monoclonal antibodies, cetuximab, and panitumumab displaying efficacy in the treatment of CRC [40]. As a chimeric immunoglobulin G (IgG), Cetuximab works by inducing internalization of EGFR and inducing degradation after it has bound to the external domain of EGFR. Binding to the external domain of the EGFR prevents ligand binding, which in the end, prevents cell growth and survival [31]. The binding brings about receptor internalization and degradation without activation or phosphorylation [31,41]. In addition, it has also been established that the binding of cetuximab to the receptor induces antibody-mediated cytotoxicity, progressing to tumoral cell death [31,42]. Furthermore, a study shows that cetuximab down-regulated VEGF expression, therefore, lowering tumor angiogenesis [43]. With its great potential, Cetuximab has been shown to improve progression-free survival (PFS) in patients which has shown a reduction in their response to singular-agent irinotecan therapy in metastatic cancer [17].
Studies involving patients having disease progression while on fluoropyrimidine, irinotecan, and oxaliplatin, with weekly administration of cetuximab had shown an improvement in progression-free and overall survival when compared to those with supportive care treatment alone [19]. In a further study with patients with irinotecan-refectory metastatic cancer, the use of cetuximab alone gave a tumor response rate of 10%, while a response of 20% was reported when used with irinotecan [44]. This established Cetuximab’s ability to overcome tumor cells with irinotecan resistance. Other studies also indicated there is a prolonged overall survival (OS) and PFS when Cetuximab is used in patients with CRCs that have either experience failure with treatment using Fluoropyrimidin (IRI and OX) or where it is contraindicated [17]
Panitumumab is a humanized monoclonal antibody also used in the targeting of EGFR but with biweekly dosing, but with similar activity to cetuximab in mCRC [40]. There was a positive tumor response in patients (9%) who had earlier been treated with fluorouracil combined with either oxaliplatin or irinotecan, after treating with panitumumab [45]. Due to the type of patients who respond to the use of cetuximab and panitumumab, molecular markers have been used to predict tumor response when investigated. This can be used to define patients’ subsets who can have great benefits if treated with EGFR inhibitors [19]. Two tumor characteristics are presently in use for this purpose: EGFR copy number (as established using fluorescence in situ hybridization) and K-ras gene mutation stage [19]. A high EGFR copy number using fluorescence in situ hybridization has a link with an increasing rate of tumor response and prolongation of disease-free and overall survival. On the other way around, patients having a mutation in K-ras have developed resistance when treated with cetuximab or panitumumab [46], with reduced response rates and poorer survival.
2.5. Immunotherapy (Immune Checkpoint Inhibitors)
Immunotherapy has been considered to be the fourth treatment modality in CRC treatment, based on advances in molecular biology, cell biology, and immunology [12]. Immunotherapy involves the use of immune checkpoint inhibitors (ICIs) to enhance the patient’s immune system’s capability to adequately identify and overcome cancer cells [47]. This strategy involves interrupting immunosuppressive signals within the TME and reactivating the antitumor immunity through the targeting of the molecular immune checkpoints [48]. Tumors create microenvironments that are immunosuppressive, which allows them to escape immune system surveillance. This is achieved with the presence of immunosuppressive tumor-associated macrophages, myeloid-derived suppressor cells, and regulatory T cells residing within the tumor. The products of these results in a microenvironment that disrupts the activation of the immune system activation and any attack [12,49]. The ICIs modulate the interaction of T cells, antigen-presenting cells (APCs), and tumor cells aiding the activation of the suppressed immune responses [50]. This has been found effective for patients with mCRC that is mismatch-repair-deficient (dMMR) or microsatellite instability-high (MSI-H) [50]. The clinical study of programmed cell death receptor (PD)-1 mAb in patients having mCRC revealed promising effects. The progression-free survival rates of 78% and 11% were exhibited in mismatch-repair-deficient (dMMR) and mismatch-repair-proficient (pMMR) tumors, respectively [51; 52].
The dMMR tumors have a high mutational burden, tumor-infiltrating lymphocytes (TILs) enrichment, and upregulated PD-L1 expression within the TME [53]. These features enable the CRC in this category to have better responses to immune checkpoint immunotherapies [48,52]. In 2017, the US Food and Drug Administration (FDA) approved pembrolizumab (anti-PD-1) usage for advanced/metastatic solid malignancies with dMMR or MSI, including use in CRCs [48]. In addition, nivolumab (with or without Ipilimumab) was also approved to serve the same purpose [50].
However, it is imperative to note that dMMR or microsatellite unstable (MSI) CRC tumors is just 14% of all CRCs, which is a smaller percentage [48,51]. The mCRC is categorized by inadequate mutated tumor antigens. This portends a great challenge in immunotherapy providing benefits for a lot of mCRC patients who have mismatch-repair-proficient (pMMR) or microsatellite-stable (MSS) or low microsatellite instability (MSI-L) (termed pMMR/ MSS/MSI-L mCRC [50]. To date, the only predictor biomarker for response to checkpoint inhibitors is the presence of dMMR in the cancer tumor.
2.6. Combination therapies approach for colorectal cancer treatment
Combining two or more therapeutic treatments to specifically target cancer-inducing or cell-sustaining pathways is a fundamental strategy in cancer therapy [54,55]. While monotherapy remains a commonly employed approach for various types of cancer, it is generally regarded as less effective compared to combination therapy. Traditional monotherapeutic methods indiscriminately attack rapidly dividing cells, leading to the destruction of both healthy and cancerous cells [56]. Chemotherapy, a frequently used monotherapy, can cause significant toxicity, with numerous side effects and risks. It often weakens the immune system by damaging bone marrow cells, thereby increasing vulnerability to infections and other diseases [57,58].
Although combination therapy involving chemotherapeutic agents may also present toxicity risks, these are typically reduced because multiple pathways are targeted. This synergistic or additive effect allows for lower therapeutic doses of each drug [59]. Furthermore, combination therapy has the potential to minimize toxic effects on healthy cells while maintaining cytotoxic efficacy against cancer cells. This is possible when one drug in the regimen antagonizes the cytotoxic effects of another drug on normal cells, effectively shielding healthy cells while still attacking cancerous ones [60].
2.6.1. FOLFIRI
FOLFIRI is one of the most widely used standard chemotherapy regimens for colorectal cancer (CRC) and consists of three drugs: irinotecan, 5-fluorouracil (5-FU), and leucovorin. 5-FU acts as a pyrimidine antagonist. Its activation begins with its conversion by orotate phosphoribosyltransferase (OPRT) and uridine phosphorylase (UP) into fluorouridine monophosphate (FUMP) and fluorouridine (FUR). FUR is subsequently converted to FUMP via uridine kinase (UK), which is then phosphorylated into fluorouridine diphosphate (FUDP) and further into the active metabolites fluorouridine triphosphate (FUTP) or fluorodeoxyuridine diphosphate (FdUDP) through ribonucleotide reductase (RNR) FUTP, a fluorinated RNA nucleotide analog, can be mistakenly incorporated into tumor cell RNA, causing RNA damage. Meanwhile, FdUDP can be phosphorylated or dephosphorylated to produce active metabolites such as fluorodeoxyuridine triphosphate (FdUTP) and fluorodeoxyuridine monophosphate (FdUMP) [61].
The FOLFIRI regimen is typically administered every two weeks across multiple treatment cycles. However, patients often develop congenital or acquired resistance to 5-FU, which limits its efficacy as a monotherapy and poses a significant challenge to effective clinical treatment [62]. To address this, 5-FU is usually administered with leucovorin, which enhances the drug’s binding affinity to thymidylate synthase (TS), thereby improving its efficacy [63]. A meta-analysis confirmed these findings, showing that combining 5-FU with leucovorin increases response rates (RR) and overall survival (OS) compared to 5-FU alone [64].
The addition of irinotecan to the regimen further enhances its effectiveness. Compared to 5-FU and leucovorin alone, the FOLFIRI regimen demonstrates significant improvements in progression-free survival (PFS), OS, and RR, while effectively delaying cancer progression [65]. Importantly, irinotecan does not exhibit cross-resistance with 5-FU/leucovorin therapy, making it a valuable component of combination therapy for CRC.
2.6.2. FOLFOXIRI
The FOLFOXIRI regimen, combining irinotecan, oxaliplatin, and 5-FU/leucovorin, is a high-intensity chemotherapy protocol used for colorectal cancer (CRC). Oxaliplatin, one of the cytotoxic agents in this regimen, primarily targets DNA, although its exact mechanism of action remains incompletely understood. Studies indicate that oxaliplatin induces cytotoxicity mainly through DNA damage. Upon entering tumor cells, oxaliplatin forms platinum-DNA adducts, disrupting DNA transcription and replication, ultimately leading to tumor cell death [66,67]. The antitumor process of oxaliplatin involves four key phases: drug uptake, activation through hydration, DNA platinization, and intracellular processing.
The FOLFOXIRI regimen has demonstrated significant efficacy in improving objective response rates (RR), progression-free survival (PFS), and overall survival (OS), with manageable and well-tolerated side effects. It is now recommended by the Chinese Society of Clinical Oncology (CSCO), the European Society for Medical Oncology (ESMO), and the National Comprehensive Cancer Network (NCCN) for treating advanced CRC. Early clinical evidence supported the feasibility and effectiveness of combining irinotecan and oxaliplatin for CRC [68,69]. FOLFOXIRI’s safety and efficacy as a first-line treatment for metastatic CRC (mCRC) were first reported in 2002 [70].
The HORG study, which included 283 patients, reported higher incidences of alopecia, diarrhea, and neurotoxicity in the FOLFOXIRI group compared to FOLFIRI. While OS improved in the FOLFOXIRI group (21.5 vs. 19.5 months), the difference was not statistically significant (p = 0.337) [71]. Additionally, the tolerability of FOLFOXIRI is poorer among Asian populations compared to Europeans, leading to modifications in its application in China. For example, the irinotecan dosage in FOLFOXIRI was reduced from 180 mg/m² to 150–165 mg/m² to suit Chinese patients, although further studies are required to confirm the efficacy and safety of this modified regimen [72].
Despite these challenges, FOLFOXIRI has shown promising results, including a PFS of 13.37 ± 9 months and an overall response rate of 79.4%, while maintaining side effects within an acceptable range for mCRC first-line therapy [73].
2.6.3. XELIRI
The XELIRI regimen, which combines irinotecan with capecitabine, offers a more convenient chemotherapy option, requiring only 2–3 hours of infusion every three weeks. A phase II single-arm study demonstrated favorable efficacy and safety in patients with metastatic colorectal cancer (mCRC) [74]. Capecitabine, an oral fluorouracil prodrug with nearly 100% bioavailability, is notable for its convenience, safety, and significant antitumor activity [74]. After oral administration, capecitabine is absorbed through the intestinal mucosa and metabolized in the liver by carboxylesterase (CES) into 5′-deoxy-5-fluorocytidine (5′-DFCR) [75]. It is then converted into 5′-deoxy-fluorouracil (5′-DFUR) by cytidine deaminase (CD), which is abundant in both liver and tumor tissues [76]. The final step occurs predominantly in tumor tissues, where thymidine phosphorylase (TP) converts 5′-DFUR into 5-FU, enhancing antitumor effects while minimizing systemic toxicity due to low TP activity in normal tissues.
A meta-analysis comparing XELIRI and FOLFIRI regimens for first-line mCRC therapy found no significant differences in overall survival (OS), response rates, or progression-free survival (PFS), and their safety profiles were comparable [77]. However, the XELIRI regimen offers greater convenience due to capecitabine’s oral administration, reducing the need for prolonged infusions and central venous access required by FOLFIRI [78].
Despite these advantages, XELIRI is associated with increased gastrointestinal toxicity compared to FOLFIRI [79,80]. To address this, the AXEPT trial, a large multicenter randomized phase III study, evaluated a modified XELIRI (mXELIRI) regimen. The study demonstrated that mXELIRI, with or without bevacizumab, is a viable alternative to FOLFIRI as a second-line treatment for mCRC, with comparable OS (16.8 vs. 15.4 months, p < 0.0001) and a significantly lower incidence of grade 3–4 neutropenia (17% vs. 43%) [81].
From a cost-benefit perspective, mXELIRI has been found to be a cost-effective alternative for second-line mCRC treatment and it is also a more tolerable and convenient option than FOLFIRI [82].
3. Complications Associated with the Therapeutic Approaches and their Management
3.1. Complications Associated with Surgery, and Management
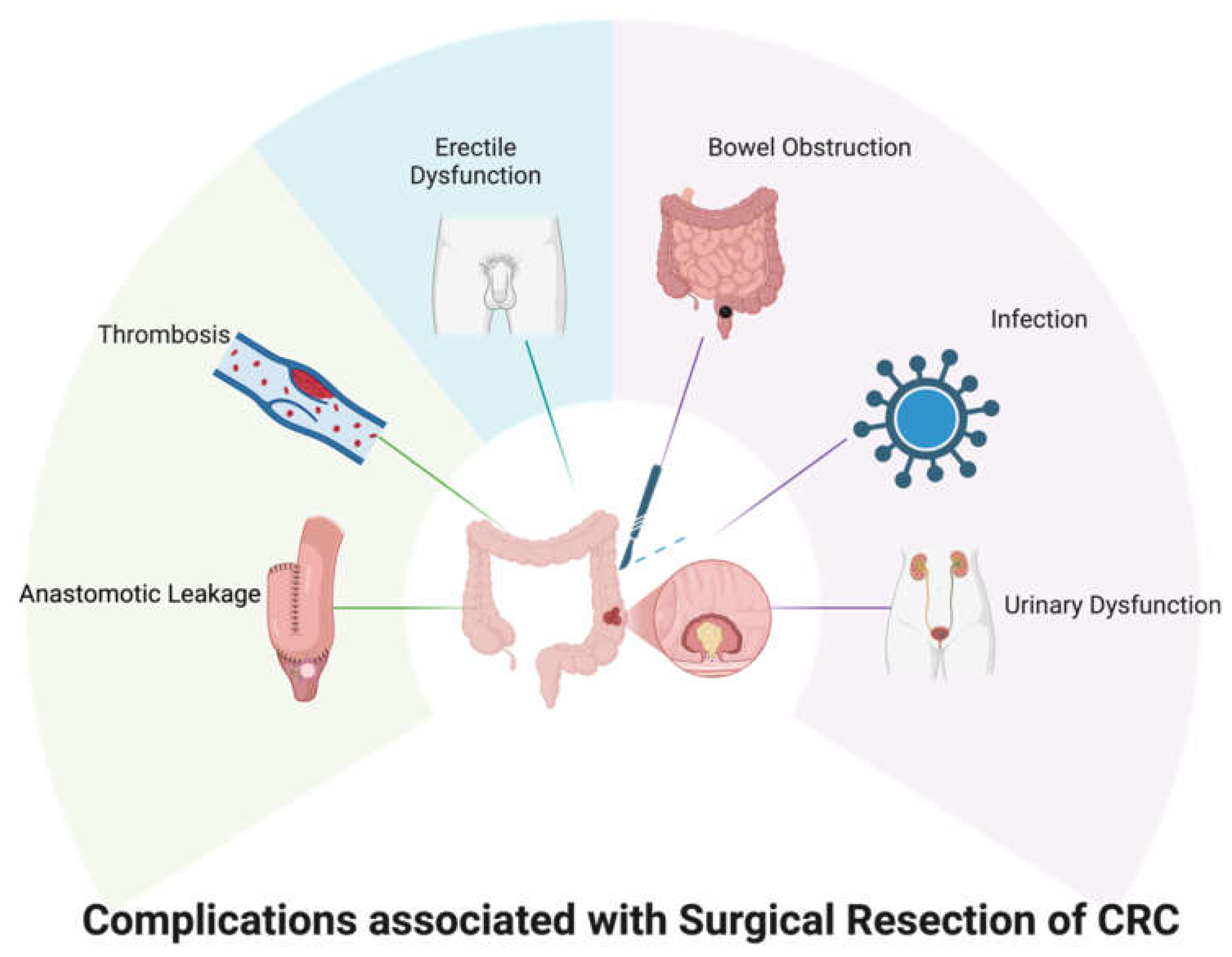
Due to the complexities associated with colorectal cancer surgery, several complications have been reported in the literature. These complications include adhesion and small bowel obstructions (SBO), thrombosis, infections, and urogenital dysfunction (Figure 1) [83,84,85]. Other complications associated with colorectal cancer surgery include port site metastases commonly seen in minimal resection of colorectal surgery [86], anastomotic leakage, and ileus that cause nausea/vomiting and pain [83,87], and colonic ischemia (ischemic colitis) [83].
Figure 1.
Search terms and articles found in PubMed search.
3.1.1. Adhesion and small bowel obstructions (SBO)
Adhesions, based on reports, is a complication frequently linked with laparoscopy, with occurrence in about 95% of cases, and often the lead origin of small bowel obstruction [83]. It has been reported that about 10% of colorectal surgery, postoperatively, leads to SBO together with peritoneal adhesions [83], with a study showing that laparoscopic and open surgery have an equal association in the development of SBO [88]. The adhesive SBO recurrence leads to a reduction in the survival rate, thus, necessitating timely surgical management to suppress the recurrence [89]. Management of SBO includes non-surgical management and laparoscopic adhesiolysis [83]. Non-surgical management is achieved first by bowel decompression, nonetheless, the majority of patients need surgery [83]. On the other hand, laparoscopic adhesiolysis has been reported to achieve lower mortality and faster recovery [90], though with a report of a higher recurrence rate [91]. The preventive measures for SBO include the use of carboxymethyl cellulose and hyaluronic acid, and the use of Poly (L-lactide-co-D, L-lactide) adhesion barrier to prevent the formation of peristomal adhesion [86,87,92].
3.1.2. Thrombosis
The occurrence of thromboembolic events in CRC surgery has been associated with 2.5% of the cases [83]. There is a higher risk of this event in patients with the use of steroids, preoperative sepsis, weight loss history, extended surgical duration, and postoperative chemotherapy [84,94]. Both laparoscopic and open colorectal surgery have been associated with this event [95]. Preoperative screening has been reported to reduce intra and postoperative complications [96]. In addition, the use of anti-thrombotic drugs for prophylaxis has been suggested to prevent thrombosis, for example, using low molecular weight heparin (LMWH) [97,98]. Furthermore, extended thromboprophylaxis perioperative, for a period of 30 days, has also been reported to cause reduction in thromboembolic events, contrary to 10 days of standard LMWH therapy [99].
3.1.3. Infections
Postoperative infections have been reported to contribute to morbidity and mortality associated with colorectal cancer surgery [84]. Advanced age, perioperative complications, types of surgical wounds, and surgeries for neoplasms have been recognized as the major factors leading to the incidence of infections, while other factors include diabetes mellitus, chemotherapy, and the use of steroids [84]. Recommendations for preventing infections include mechanical bowel preparations (MBP) to clear the bowel in order to prevent sepsis, and MBP in combination with antibiotics [94,100].
3.1.4. Urogenital Dysfunction
Urogenital dysfunction remains a frequent challenge occurring after colorectal cancer treatment, with surgery, radiation, or chemotherapy [85,88]. It has been reported that about a higher than half of patients who have undergone colorectal cancer treatment experience a decline in sexual function [101]. In males, sexual dysfunction after colorectal cancer includes ejaculatory dysfunction and impotence, and for women, the common being vaginal dryness and dyspareunia [102]. It has been reported that about 63% of men develop ejaculation dysfunction and about 63% have difficulty ejaculating after rectal cancer treatment [103,104]. It is also reported that urinary dysfunction arises in one-third of patients who have undergone treatment for rectal cancer [101]. Urinary and sexual dysfunction in colorectal cancer treatment has been linked to surgical nerve damage in low rectal cancer and abdominoperineal resection, while radiotherapy was linked to the progression of sexual dysfunction without necessarily affecting urinary function [102]. Surgical treatment could affect the parasympathetic and sympathetic nerves that are involved in erection and ejaculation [105], while radiation could impact nerves and blood vessels involved in erection [102].
In a work done by Perry et al. on sexual dysfunction resulting from surgery for rectal cancer based on a single-institution experience, it was reported that out of 147 patients examined, the overall sexual dysfunction rate was found to be 70% at a 38-month median time from surgery [106]. 62% of men and 87% of women report an overall score that fell below one standard deviation of the population mean. The study showed a high rate of the occurrence of sexual dysfunction after rectal cancer surgery, with more risk peculiar to female patients. In another study by Mannaerts et al., it was reported that of 73 men who had undergone both radiation and surgery as treatments for rectal cancer, about 10% could experience ‘quality erection’ and only about 10% could ejaculate postoperatively [104]. Sexual dysfunction could impact the quality of health experienced by colorectal cancer patients after treatment. Men who experience sexual dysfunction could experience depression, distress, and other psychological events that could impair their intimacy in relationships [107,108].
The management of sexual dysfunction involves the use of phosphodiesterase-5 inhibitors (PDE5i), intracavernosal injections [109]. The mechanism of PDE5i revolves around increasing intracellular cGMP levels that allow for prolonged erection [110]. The PDE5i drugs approved by the FDA for erectile dysfunction include sildenafil, tadalafil, avanafil, and vardenafil [110,111,112]. PDE5i both stimulates libido and may result in better erectile discovery [113]. Intracavernosal injections have also been used in the treatment of erectile dysfunction in males [109]. The most common of these is intracavernosal alprostadil which is a synthetic analog of prostaglandin E1 (PGE1). Alprostadil binds to G-coupled PGE1 receptors available on the surface of smooth muscle cells [114]. It is, however, important that the physician inquires from, and consider alternatives for patients who might have a fear of penile injections [109]. PDE5i and intracavernosal injections have been found to be efficacious and well-endured among patients [115]. The other option for males is the use of an inflatable penile prosthesis, however, it is faced with issues regarding reservoir placement.
The challenge with ejaculatory function, retrograde ejaculation has been managed with electroejaculation and alkalization of urinary pH to preserve sperm viability [116,117]. Anejaculation, a condition where a male finds it difficult to ejaculate any semen during the course of sexual activity associated with nerve damage, pharmaceutical side effects, or previous surgery, can be addressed using penile vibratory stimulation (PVS), though not the best option for sensate patients [118]. Electroejaculation is preferred in sensate patients [109]. In addition to this, dopaminergic drugs like oxytocin and clomiphene citrate, are other alternatives that have been used to enhance ejaculatory nerve sensitivity or semen production [119] Even though several treatments for erectile dysfunction have been postulated, only about 50-80% of men comply with the medical interventions and only about 38% of such men found such treatment helpful in mending their sex lives [85,120].
3.2. Complications Associated with Radiotherapy and Management.
Every year, several thousands of patients receive radiotherapy as part of their colorectal cancer treatment plan. While there have been some successes recorded with the use of radiotherapy, several patients have come down with mild-severe complications due to chemotherapy [121,122]. Jairam et al 2019 conducted a retrospective cohort study between January 2006 and December 2015, they found that about 1.5 million patients developed one or more complications associated with radiotherapy treatment [123]. The reported complications include but are not limited to neutropenia, sepsis, anemia, pneumonia, and acute kidney injury (Figure 2).
Figure 2.
Summary of surgical and therapeutic interventions with colorectal cancer. FOLFIRI contains Irinotecan, 5-FU, and Leucovorin; FOLFOXIRI contains Irinotecan, Oxaliplatin, and 5-FU/Leucovorin; XELIRI contains Irinotecan and Capecitabine.
Figure 2.
Summary of surgical and therapeutic interventions with colorectal cancer. FOLFIRI contains Irinotecan, 5-FU, and Leucovorin; FOLFOXIRI contains Irinotecan, Oxaliplatin, and 5-FU/Leucovorin; XELIRI contains Irinotecan and Capecitabine.
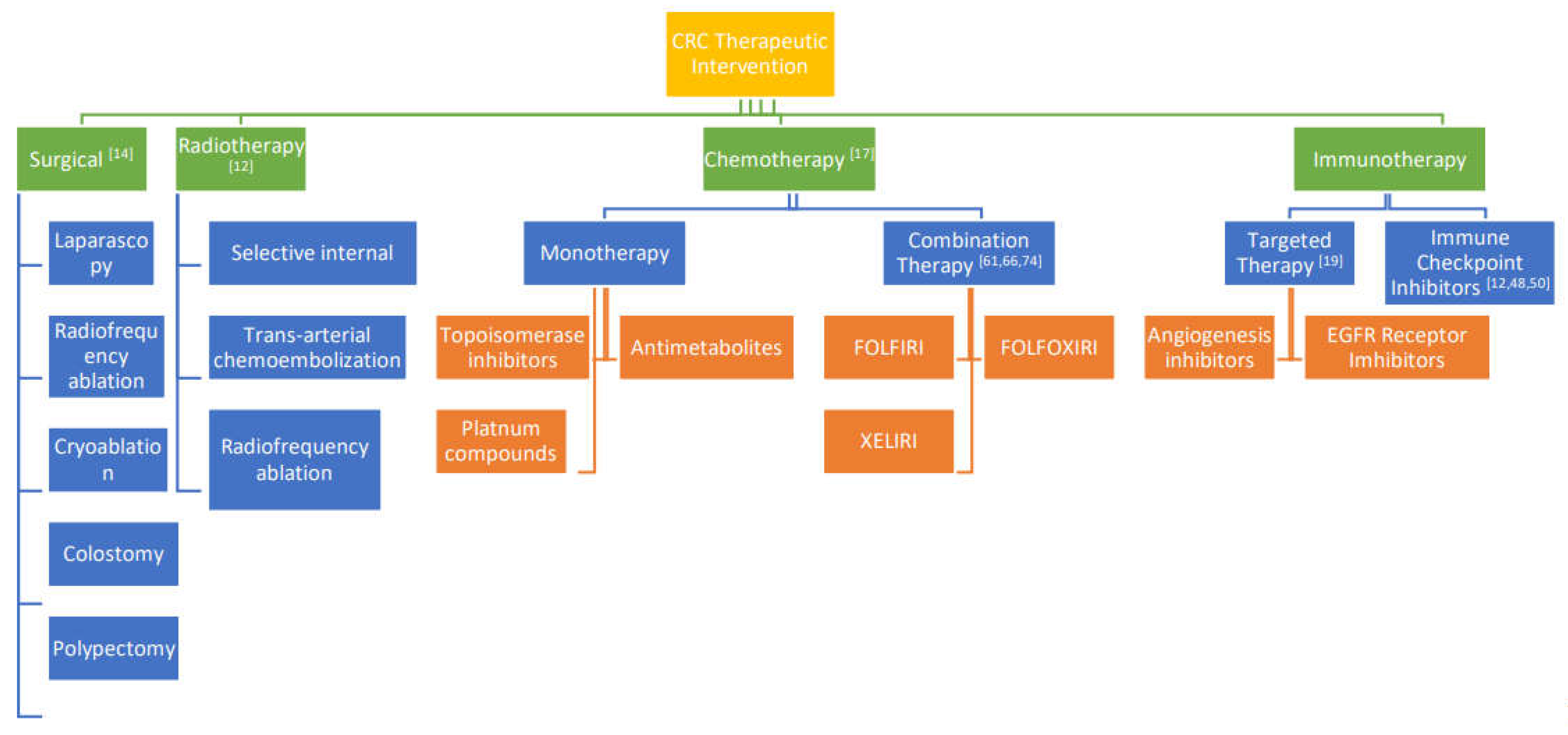
Figure 3.
Complications associated with surgical intervention in CRC treatment.
Intraoperative radiation therapy (IORT) has been shown to improve disease outcomes in advanced and recurrent CRC. It is however associated with several short-term complications such as abscess Fistulae, wound, and anastomotic leakage; and long-term complications including Ureteric obstruction and sacral necrosis [124]. Most side effects gradually go away in the weeks or months after treatment. However, some side effects can continue and might be noticed months or years later.
Figure 4.
Complications associated with radiotherapy interventions in CRC treatment.

Chronic enteritis caused by radiation is usually managed as the symptoms arise. Diet modification is usually considered first, and it might take a period of time for a perfect dietary plan to be developed. For complications that present as diarrhea and urgency, patients are usually advised to avoid foods that are high in fiber [125,126]. Limiting lactose and dairy intake has also been found to be helpful. With the emerging interest in the involvement of gut microbiome in colorectal cancer, the use of probiotics in managing complications has also been considered. A meta-analysis of recent trials has suggested that probiotics either in the pill or drink form are effective in managing radiation-induced diarrhea [127,128].
Another important complication that has attracted a lot of discussion is radiation-induced fertility and sexual toxicity. This increasingly becoming important to consider because of the increase in the number of young people being diagnosed with CRC. In female patients unfortunately, the ovaries have been shown to be highly sensitive to radiotherapy, and the doses at which radiation is used for peri-operative or definitive purposes can result in infertility [129,130,131]. Due to this, women are usually advised to harvest their eggs prior to the start of radiotherapy. In the case of men receiving radiotherapy, the risk of infertility of approximately 20%. Therefore, sperm banking is recommended to maximize the probability of having biologic children [132,133]. Conversely, for those who do not wish to have more children, contraception is advised during and after radiation therapy.
3.3. Complications Associated with Chemotherapy and Management
The chemotherapeutic drugs used in the adjuvant treatment of colorectal cancer are known to produce undesirable neurological and gastrointestinal side effects [134]. Most often, the chronic side effects lead to dose limitations, while in severe cases, there is a need to stop the chemotherapy treatment because of the inability of the patient to tolerate the adverse effects, thus impeding the efficient treatment of CRC using chemotherapeutic agents [134,135]. Approximately 40% of patients placed on standard and high-dose chemotherapy experience pain, bloating, ulceration, vomiting, and diarrhea [136]
3.3.1. Chemotherapy-Induced Diarrhea (CID)
Chemotherapy-induced diarrhea (CID) is one of the frequent dose-limiting side effects associated with chemotherapeutic drugs which affects about 80% of patients placed on chemotherapy for colorectal cancer and other gastrointestinal cancers [138,139]. It has been reported, in addition, that about 5% of early deaths experienced from chemotherapeutic combination treatment stem from CID.
CID in colorectal cancer patients is linked with the use of 5-FU, irinotecan, capecitabine, and oxaliplatin [140,141]. However, the incidence and the severity of CID differ depending on the chemotherapeutic drug and the combination, with the 5-FU and irinotecan combination having a high rate of about 87% [139,142]. The occurrence and persistence of CID in patients on combination therapy often led to malnutrition and dehydration, causing other secondary effects like weight loss, renal failure, fatigue, and hemorrhoids [143,144]. In addition, CID could cause severe inflammation and bowel wall thickening ulceration [134,145]. Thus, CID has played a key contributor to the disruption of clinical outcomes and treatment alteration. About 60% of treatment alterations arise from CID, having about 22% of patients having dose reductions, 28% of patients ending up with dose delays, and 15% of patients having treatment cessation due to severe diarrhea during CRC treatment [146,147].
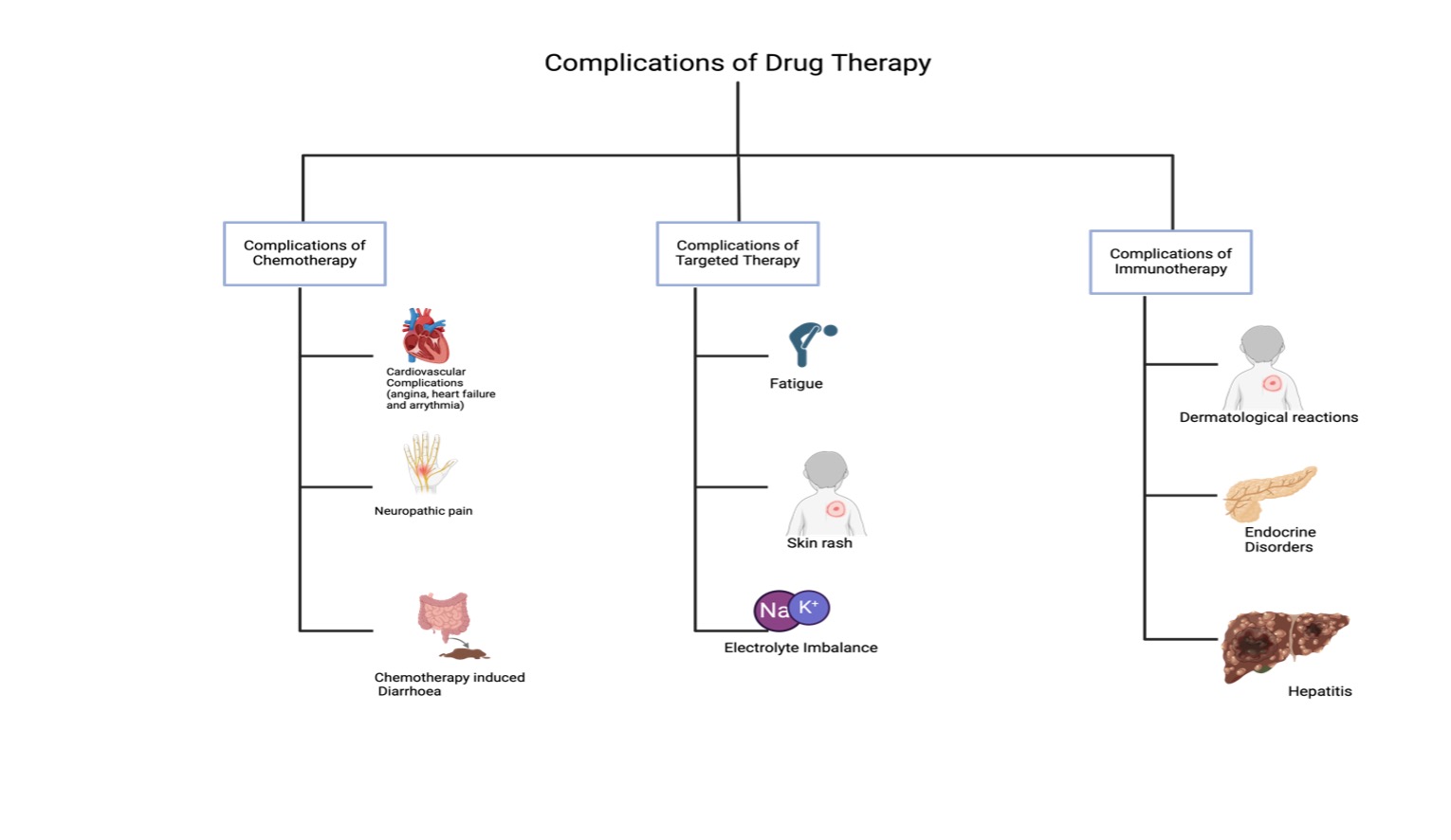
Figure 5.
Complications associated with drug interventions in Colorectal Cancer Treatment.
The mechanisms underlying CID are not well understood. The most notable explanation in literature is that it is a form of mucositis or its by-product [136]. Mucositis is an inflammation and ulceration of the mucous membrane of the gastrointestinal tract. GIT mucositis arises from the disruption of the intestinal microflora and mucin secretion, which stimulates the development of CID [136]. The toxicity of the chemotherapeutic agent affects the rapidly dividing crypt cells of the intestinal epithelium, and in addition to depletion of enzymes, leads to decreased absorption and an increase in fluid retention, which is often seen in CID [134,137]. The villi and mature cells of the intestinal wall are directly harmed, leading to a higher proportion of the immature secretory cells. The increase in fluid retention and decrease in the absorptive capacity of the villi cause an alteration in the osmotic gradient within the GIT that leads to the onset of diarrhea [134,148]. In addition to this mechanism, alteration of the GIT microflora induced by chemotherapeutic agents causes an increase in solutes and chloride ions in the intestinal tracts [148].
The presence of chloride ions triggers a shift in the osmotic gradient, causing water to be retained in the canal, and causing osmotic diarrhea [137,149]. However, it is unclear whether all CID from chemotherapeutic agents is a result of alteration in the epithelial surface of the intestines [134]. Attribution has also been made to the enteric nervous damage made by the chemotherapeutic agent which might be responsible for gastrointestinal secretory and motility disturbances associated with the pathophysiology of CID [134,150,151]. The recommendation by the consensus conference on the management of CID for the management of uncomplicated CID is through modification of diet and the use of standard doses of medication like loperamide, octreotide, and tincture of opium in outpatient patients. Nonetheless, complicated diarrhea might require an aggressive approach and hospitalization, involving patients placed on anti-diarrhea medications and intravenous fluids [142,149].
3.3.2. Cardiovascular Complications
Cardiovascular complications in colorectal cancer often develop perioperatively or during chemotherapy [152]. Out of the 90% of adverse effects experienced by the patients during the first cycle of treatment, 39% have been reported to be cardiovascular (CV) events [152]. This CV includes hypertension, myocardial infarction, angina, arrhythmias, thrombotic events, heart failure, and in extreme cases, death [152].
5-FU has been reported to have 1.2% to 18% cardiotoxic events [153], with the most significant cardiotoxic presentation being angina [153], followed by other manifestations like dyspnea, palpitations, and hypotension [154]. A four-step approach has been proposed for managing 5-FU cardiotoxicity. (i) Immediately discontinuing the 5-FU; (ii) practical symptomatic treatment (iii) confirming that the symptoms are related to 5-FU (iv) rechallenging with pharmacological prophylaxis or determining a different chemotherapeutic regimen [152]. Initiation using calcium channel blockers or nitrates is the lone proposed treatment by the European Society of Cardiology in treating the fatal cardiotoxic consequences of 5-FU [155].
Capecitabine, an oral pro-drug of 5-FU, produces cardiotoxic events like angina-like chest pain, acute ischemic events [156], arrhythmias, heart failures [157], ventricular fibrillation [158], and sudden cardiac death linked to coronary vasospasm [159]. The topmost cardiotoxic events with capecitabine occur when in combination with oxaliplatin, and bevacizumab [159]. Treatment of this is often symptomatic [160].
Bevacizumab has been associated with hypersensitivity adverse reactions with dyspnea, hypotension, hypoxia, and fever resulting from the massive release of cytokines [152]. Another class effect associated with Bevacizumab is hypertension and heart failure [161]. Hypertension is a reversible occurrence that is dependent on the duration of the drug use and the dose [162]. Thus, regular monitoring of hypertension is needed during administration of the dose [163]. The treatment proposed includes angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs) [163]. Of great interest is that the induction of hypertension in patients using bevacizumab has been used as a predicting factor for antitumor efficacy and better survival [164]. Finally, bevacizumab also induced venous thrombotic events [165] but can be treated using oral anticoagulants [166].
Cetuximab produces complications like urticaria and bronchospasm that come with hypotension and in extreme cases angina, myocardial infarction, heart failure, shock, and sudden death [167]. Venous thromboembolism is also associated with cetuximab, with limited data [168]. Panitumumab, on the other hand, has cardiotoxic effects like hypotension, hypertension, and venous thromboembolic events. The cardiotoxic effects requiring attention in the two drugs are palpitation, chest pain, arrhythmias, and dyspnea [169,170].
3.3.3. Neuropathic Complications
Chemotherapy-induced peripheral neuropathy (CIPN) is a frequent dose-limiting complication suffered by colorectal patients on chemotherapy. It is reported that about 30-40% of patients undergoing chemotherapy may develop CIPN and the severity is variable between patients [171]. The classes of drugs causing neurotoxicity include platinum, vinca alkaloids, and taxanes [171]. Symptoms associated with CIPN often begin during the first two months of treatment [171] and can stabilize soon after the completion of treatment. However, acute neurotoxicity may present with paclitaxel and oxaliplatin or a coasting effect associated with the discontinuation of cisplatin [171]. The manifestation of CIPN is an implication for a dose decrease or in some instances, stopping the chemotherapeutic drug [171]. Discontinuing the chemotherapeutic drug may hold back treatment [171,172].
CIPN is initiated by the neurotoxic effects of chemotherapeutic drugs on neurons, and the associated sensory symptoms are higher compared to motor or autonomic [171]. In the majority of patients, there is dose-dependent development of CIPN after several cycles of administration of the chemotherapeutic drugs [171]. The signs and symptoms associated with CIPN often arise due to the damaging effect of chemotherapeutic drugs on the dorsal root ganglion neurons or their axons [171]. This leads to “acral pain, sensory loss, and sometimes, sensory ataxia” [171]. Platinum compounds, including oxaliplatin which is widely used in colorectal cancer, cause sensory neuropathy [171. This effect is attributed to the penetrability of the blood-nerve barrier at the point of the dorsal root ganglion [171]. The platinum-based compounds triggered harm to the dorsal root ganglia neurons through the formation of adducts with nuclear and mitochondria DNA.
Thus, all platinum agents are known to cause long-term peripheral sensory damage attributed to neuropathy [173]. This phenomenon is seen in 30-40% of patients receiving oxaliplatin and cisplatin treatment [174]. Furthermore, Oxaliplatin is associated with acute neuropathic pain, which contains cold-induced dysesthesia that is significant in the hands, face, and oral cavity. Intense pain, may, therefore, be induced by cold conditions like cold winds or cold drinks [171]. The ‘coasting’ phenomenon is a worsened CIPN for several months after the discontinuation of platinum chemotherapy (cisplatin and oxaliplatin) [171]. The mechanism for oxaliplatin-induced peripheral neurotoxicity (OIPN) is linked to ‘DNA damage, dysfunction of voltage-gated ion channels, neuroinflammation, transporters, oxidative stress, and mitochondrial dysfunction [172].
Presently, it has been difficult to develop CIPN-preventing agents because of the complications that surround such agents decreasing the efficacy of the chemotherapeutic agent.
Another approach embraced is identifying patient-specific risk factors that can translate to planning chemotherapy strategies for each patient [171]. These factors include dose, delivery route, concurrent medication usage, age, pre-existing neuropathy, and pre-existing conditions like diabetes [175]. The further approach involves identifying individual patient-specific mechanisms [176]. The only pharmacological treatment recommendation by the American Society of Clinical Oncology (ASCO) in treating CIPN is duloxetine [177]. Duloxetine is a serotonin-norepinephrine reuptake inhibitor (SNRI) that shows a substantial enhancement in pain management.
Other intervention modalities include the use of acupuncture, cryotherapy and compression therapy, surgical treatment, exercise, and diets [177]. The emerging therapy includes the use of botulinum toxin injections, ganglioside-monosialic acid, mitochondria enzyme, and immunomodulation [177,178,179,180,181]. For OIPN, the strategies for management include the use of ‘chemoprotectants (e.g. glutathione, Ca/Mg, ibudilast, etc.), dose reduction, chronomodulated infusion, reintroduction of oxaliplatin and topical administration, pressurized intraperitoneal aerosol chemotherapy (PIPAC), and hyperthermic intraperitoneal chemotherapy (HIPEC)’ [172].
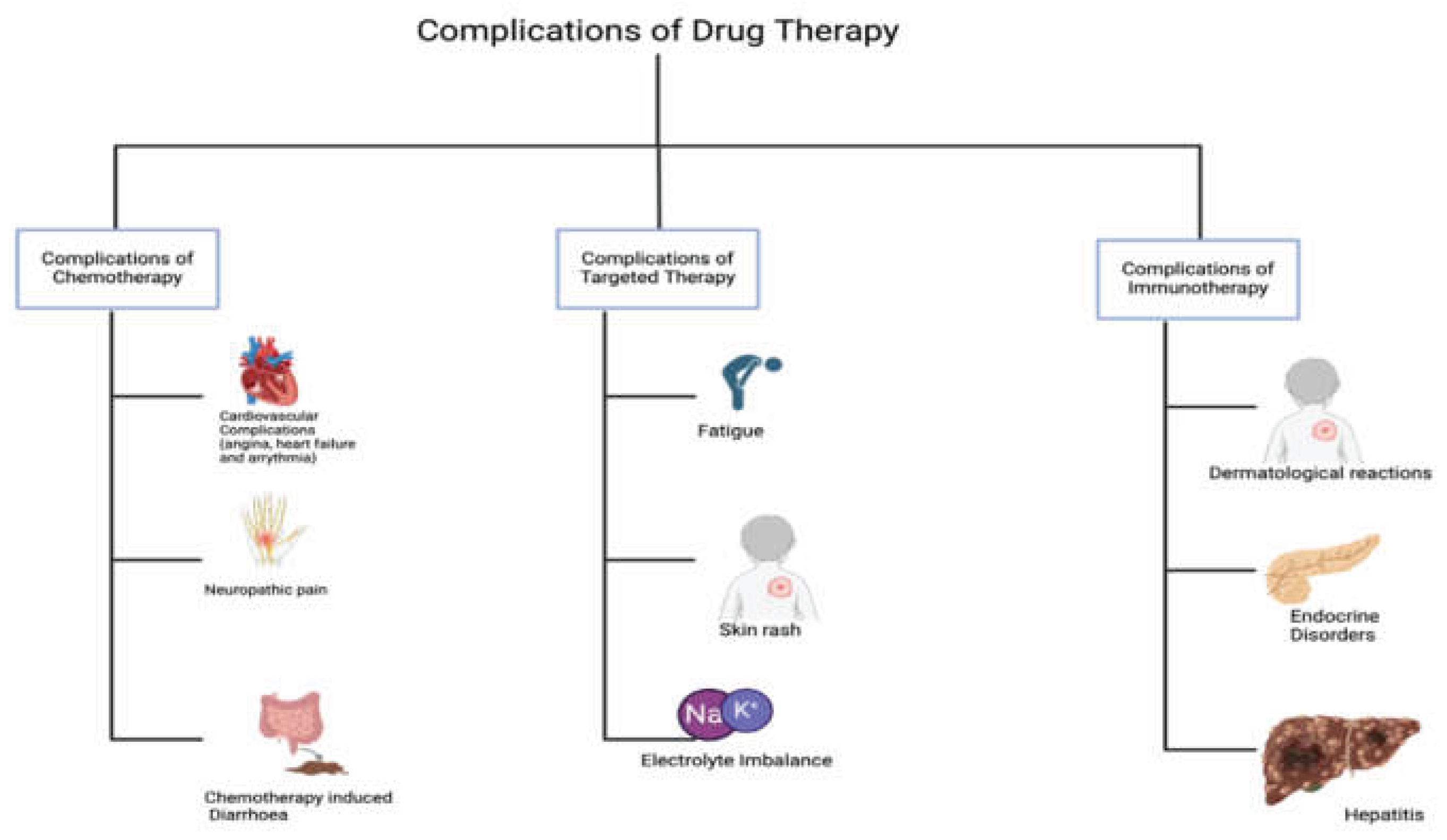
3.4. Complications Associated with Targeted Therapy and Management
This class of therapeutics has delivered on the promise of target selectivity. However, they have also been associated with several toxicities that are not typically seen with traditional cytotoxic agents. The mechanisms underlying these novel toxicities have not yet been fully elucidated (Jin et al., 2023).
While small molecule inhibitors targeting the intracellular EGFR TK domain have demonstrated activity in other malignancies, only antibodies directed at the ligand-binding domain have shown efficacy in colorectal cancer. Currently, cetuximab is the only EGFR monoclonal antibody approved by the Food and Drug Administration (FDA) for the treatment of colorectal cancer, with others, such as panitumumab and matuzumab, undergoing clinical development.
Cetuximab is an IgG1 chimeric version of the murine monoclonal antibody M225 [183]. Phase I study identified skin rash as the primary toxicity and reported saturable clearance consistent with receptor binding. Overall, cetuximab treatment is generally well tolerated. Common side effects include fatigue and dermatologic reactions, while less frequent adverse effects, such as allergic reactions and electrolyte imbalances, have also been reported [184]. Typical management includes corticosteroids, epinephrine, oxygen, and antihistamines. Severe reactions, such as angioedema, require discontinuation of cetuximab and are best managed with epinephrine and supportive care [185].
The adverse event profile of panitumumab is similar to that of cetuximab. However, as panitumumab is a fully human antibody without a murine component, allergic reactions are uncommon (with only one possible hypersensitivity reaction reported). Additionally, cutaneous toxicity is almost universal in patients receiving panitumumab, which may be attributed to its higher affinity for the receptor [186,187]. The addition of bevacizumab, an antibody targeting VEGF, to chemotherapy, has significantly improved survival in patients with metastatic colon cancer [188]. While generally well tolerated, bevacizumab has a unique side effect profile associated with vascular disturbances. Vascular development plays a crucial role in both cancer biology and normal physiological processes [189].
The toxicities associated with bevacizumab have been extensively documented across multiple trials. The most common side effects include hypertension and proteinuria. Less frequent but more severe complications, such as bowel perforation, arterial thrombotic events, and bleeding, have also been observed. These adverse effects do not appear to be strongly dose-dependent, as both 5 mg/kg and 10 mg/kg doses have been used in colorectal cancer trials. Most of these adverse effects can be managed symptomatically [188,190].
3.5. Complications Associated with Immunotherapy and Management
While immunotherapeutic agents are relatively well tolerated, their uses have been linked to a range of toxicities and adverse effects which may be easily contained in most cases or severe and fatal in rare cases and may ultimately lead to therapy discontinuation [191; 192]. The most common immunotherapy-related adverse effects are dermatological, gastrointestinal, hepatic and endocrine toxicities [193]. PD-1 inhibitors, including nivolumab and pembrolizumab, exhibit a reduced occurrence of side effects compared to CTLA-4 blockers like ipilimumab [194]. The concomitant use of two or more Immunotherapeutics or combination with other treatment modalities such as chemotherapy and radiotherapy may increase the incidence, severity, and onset of these unwanted adverse effects. For example, a higher incidence of immune-related adverse drug events was observed on combination of nivolumab and ipilimumab. In contrast to 20% of patients treated with nivolumab alone, over 30% of patients who received combination therapy experienced grade 3–4 treatment-related adverse events [194,195].
Skin rash and pruritus are very common among patients receiving immunotherapy and the management varies depending on the severity. Grade 1 and 2 can be managed with topical corticosteroid creams while grade 3 and 4 require a more serious measure like high-dose steroids or discontinuation of therapy [196]. About 1 in 3 colorectal cancer patients receiving immune checkpoint inhibitor ipilimumab have diarrhea [197]. The incidence rate rises by over 10 % when combined with nivolumab. Having ruled out other potential causes of diarrhea, treatment options range from antidiarrheal medications to systemic corticosteroids such as methylprednisolone and budesonide, and withdrawing the therapeutic agents causing the toxicity, depending on the severity of the condition [197]. Infliximab, a tumor necrosis factor-alpha inhibitor, and vedolizumab, an integrin receptor antagonist are other safe and efficient alternatives used in severe diarrhea and colitis [197,198]. The use of steroids and immunosuppressive therapy to mitigate adverse toxicities has the propensity to diminish the anticancer effect of Immunotherapeutics. As a result, the dosage and timing of these agents should be carefully considered. Steroid use soon after immunotherapy is discouraged whenever possible, and low-dose steroids are advised.
Hypothyroidism, hyperthyroidism, type 1 diabetes mellitus, and hypophysitis (pituitary inflammation)) are some of the immunotherapy-related adverse effects of the endocrine [191,199] Although less common, they are serious and life-threatening adverse effects. Hypothyroidism is often managed with beta-blockers to relieve presented symptoms or by hormonal replacement (levothyroxine) depending on the severity of the side effects [199]. Other less common adverse effects are hepatitis, pneumonitis, infusion reaction, anemia myocarditis, amongst others [191,194].
4. Conclusions
There is a rapid evolution of colorectal cancer treatment. The present focus is tilting towards personalized medicine, robot-assisted surgery, and laparoscopic procedures for minimal invasion during surgery, discoveries in immunotherapy and targeted therapies, and the use of combination therapeutic approaches. These approaches hold great promise for a more effective approach to CRC treatment, nevertheless, complications arising from available treatment approaches remain crucial. While efforts are being garnered toward developing innovative approaches to CRC, the management of the complications associated with the present approaches remains a major concern. An interdisciplinary approach towards improving outcomes, reducing treatment complications and enhancing quality of life in CRC patients should be the goal of emerging treatment options.
Author Contributions
Conceptualization, AA, & ASA; methodology, ASA, AA, OO & KA.; software, ASA, AA, OO & KA; validation, ASA, AA, SKA, KA.; formal analysis, ASA, KA, SKA.; investigation, AA, ASA, and KA.; resources, ASA, SKA, AA & KA.; data curation, AA, ASA, OO & KA.; writing—original draft preparation, AA, OO and ASA.; writing—review and editing, ASA, SKA.; visualization, AA, KA, ASA; supervision, ASA and SKA; project administration, ASA and AA; funding acquisition, ASA. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the American Cancer Society Diversity in Cancer Research Institutional Development Grant No DICRIDG-21-074-01-DICRIDG at Howard University and the Georgetown Howard Universities Center for Clinical and Translational Science (GHUCCTS)-Pilot Translational and Clinical Studies, Grant No: GRT000558.
Institutional Review Board Statement
The Colorectal Cancer research project was approved by the IBC-2023-0016: Sequential passive-active targeted delivery of niosomal combination drugs for colorectal cancer treatment.
Informed Consent Statement
“Not applicable.”
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to related studies that are ongoing and pending patent applications.
Acknowledgments
Nil
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Andry R Marley, Hongemei Nan, 2016. Review Article: Epidemiology of colorectal cancer. Int J Mol Epidemiol Genet 2016;7(3):105-114. www.ijmeg.org /ISSN:1948-1756/IJMEG0036410.
- What is colorectal cancer? [Internet]. Cancer. org; 2016 [17 May 2016]. Available from: http: //www.cancer.org/cancer/colonandrectumcancer/detailedguide/colorectal-cancer-what-is-colorectal-cancer.
- Prashanth Rawla, Tagore Sunkara, Adam Barsouk. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Gastroenterology Rev 2019; 14 (2): 89–103. [CrossRef]
- Ewing I, Hurley JJ, Josephides E, Millar A. The molecular genetics of colorectal cancer. Frontline Gastroenterol 2014; 5: 26-3.
- Cancer Facts & Figures 2016 [Internet]. Cancer.org; 2016 [17 May 2016]. Available from: http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-04-7079.pdf.
- Colorectal Cancer: Overview [Internet]. Cancer. net; 2015 [19 October 2015]. Available from: /www.cancer.net/cancer-types/colorectal-cancer/overview.
- U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2021 submission data (1999-2019): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; https://www.cdc.gov/cancer/dataviz, released in November 2022.
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68: 394-424.
- Cerrito, M.G.; Grassilli, E. Identifying Novel Actionable Targets in Colon Cancer. Biomedicines 2021, 9, 579. [CrossRef]
- Regenbogen, S. E., Veenstra, C. M., Hawley, S. T., Banerjee, M., Ward, K. C., Kato, I., & Morris, A. M. . The personal financial burden of complications after colorectal cancer surgery. Cancer. 2014; 120(19), 3074–3081. [CrossRef]
- Rutherford, C., Müller, F., Faiz, N., King, M. T., & White, K.. Patient-reported outcomes and experiences from the perspective of colorectal cancer survivors: Meta-synthesis of qualitative studies. Journal of Patient-Reported Outcomes. 2020; 4(1), 1-19. [CrossRef]
- Jayshree Mishra, Joseph Drummond, Sohel H. Quazi , Satya Sridhar Karanki, J.J. Shaw, Ben Chen, Narendra Kumar. Prospective of colon cancer treatments and scope for combinatorial approach to enhanced cancer cell apoptosis. Critical Reviews in Oncology/Hematology. 2016; 86: 232–250.
- Kuipers EJ, Grady WM, Lieberman D, et al. Colorectal cancer. Nat Rev Dis Primers. 2015;1:15065. [CrossRef]
- Purnima Gogoi, Geetika Kaur, Nikhlesh K Singh. Nanotechnology for colorectal cancer detection and treatment. World J Gastroenterol 2022 December 14; 28(46): 6497-6511. [CrossRef]
- Matsuda T, Yamashita K, Hasegawa H, et al. Recent updates in the surgical treatment of colorectal cancer. Ann Gastroenterol Surg. 2018;2(2):129–36. [CrossRef]
- Sadia Islam Kana, Karim Essani. ImmunoOncolytic Viruses: Emerging Options in the Treatment of Colorectal Cancer. Molecular Diagnosis & Therapy. 2021; 25:301–313. [CrossRef]
- Yuan-Hong Xie, Ying-Xuan Chen and Jing-Yuan Fang. Comprehensive review of targeted therapy for colorectal cancer. Signal Transduction and Targeted Therapy 2020; 5:22. [CrossRef]
- Cremolini, C.; Schirripa, M.; Antoniotti, C.; Moretto, R.; Salvatore, L.; Masi, G.; Falcone, A.; Loupakis, F. First-line chemotherapy for mCRC—a review and evidence-based algorithm. Nat. Rev. Clin. Oncol. 2015, 12, 607.
- Brian M. Wolpin And Robert J. Mayer. Systemic Treatment of Colorectal Cancer. Gastroenterology 2008;134:1296 –131.
- Sobrero A, Guglielmi A, Grossi F, et al. Mechanism of action of fluoropyrimidines: relevance to the new developments in colorectal cancer chemotherapy. Semin Oncol 2000;27:72–77.
- Kevin Van der Jeught, Han-Chen Xu, Yu-Jing Li, Xiong-Bin Lu, Guang Ji. Drug resistance and new therapies in colorectal cancer. World J Gastroenterol 2018 September 14; 24(34): 3834-3848. [CrossRef]
- Zhang ZG, Harstrick A, Rustum YM. Modulation of fluoropyrimidines: role of dose and schedule of leucovorin administration. Semin Oncol 1992;19:10–15.
- Thirion P, Michiels S, Pignon JP, et al. Modulation of fluorouracil by leucovorin in patients with advanced colorectal cancer: an updated meta-analysis. J Clin Oncol 2004;22:3766–3775.
- Meropol NJ. Oral fluoropyrimidines in the treatment of colorectal cancer. Eur J Cancer 1998;34:1509–1513.
- Mathijssen RH, van Alphen RJ, Verweij J, et al. Clinical pharmacokinetics and metabolism of irinotecan (CPT-11). Clin Cancer Res 2001;7:2182–2194.
- Palshof JA, Høgdall EV, Poulsen TS, Linnemann D, Jensen BV, Pfeiffer P, Tarpgaard LS, Brünner N, Stenvang J, Yilmaz M, Nielsen DL. Topoisomerase Ⅰ copy number alterations as biomarker for irinotecan efficacy in metastatic colorectal cancer. BMC Cancer 2017; 17: 48. [CrossRef] [PubMed]
- Ando M, Hasegawa Y, Ando Y. Pharmacogenetics of irinotecan: a promoter polymorphism of UGT1A1 gene and severe adverse reactions to irinotecan. Invest New Drugs 2005;23:539–545.
- Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluorouracil alone as firstline treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet 2000;355:1041–1047.
- Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med 2000; 343:905–914.
- Raymond E, Chaney SG, Taamma A, et al. Oxaliplatin: a review of preclinical and clinical studies. Ann Oncol 1998;9:1053–1071.
- William A. Hammond, Abhisek Swaika and Kabir Mody. Pharmacologic resistance in colorectal cancer: a review. Ther Adv Med Oncol 2016, Vol. 8(1) 57–84. [CrossRef]
- Hu J, Li J, Yue X, Wang J, Liu J, Sun L, Kong D. Expression of the cancer stem cell markers ABCG2 and OCT-4 in right-sided colon cancer predicts recurrence and poor outcomes. Oncotarget 2017; 8: 28463-28470. [CrossRef] [PubMed]
- de Sousa E Melo F, Colak S, Buikhuisen J, Koster J, Cameron K, de Jong JH, Tuynman JB, Prasetyanti PR, Fessler E, van den Bergh SP, Rodermond H, Dekker E, van der Loos CM, Pals ST, van de Vijver MJ, Versteeg R, Richel DJ, Vermeulen L, Medema JP. Methylation of cancer-stem-cell-associated Wnt target genes predicts poor prognosis in colorectal cancer patients. Cell Stem Cell 2011; 9: 476-485. [CrossRef] [PubMed]
- Maxwell, P., Dachs, G., Gleadle, J., Nicholls, L., Harris, A., Stratford, I. et al. Hypoxia-inducible factor-1 modulates gene expression in solid tumors and influences both angiogenesis and tumor growth. Proc Natl Acad Sci U S A. 1997; 94: 8104–8109.
- Jurgensmeier, J., Schmoll, H., Robertson, J., Brooks, L., Taboada, M., Morgan, S. et al. (2013) Prognostic and predictive value of VEGF, SVEGFR-2 and CEA in mCRC studies comparing cediranib, bevacizumab and chemotherapy. Br J Cancer 108: 1316–1323.
- Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335–2342.
- Hurwitz HI, Fehrenbacher L, Hainsworth JD, et al. Bevacizumab in combination with fluorouracil and leucovorin: an active regimen for first-line metastatic colorectal cancer. J Clin Oncol 2005; 23:3502–3508.
- Glusker P, Recht L, Lane B. Reversible posterior leukoencephalopathy syndrome and bevacizumab. N Engl J Med 2006;354:980– 982.
- Fuchs CS, Marshall J, Mitchell E, et al. Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C study. J Clin Oncol 2007;25:4779–4786.
- Messersmith WA, Hidalgo M. Panitumumab, a monoclonal anti epidermal growth factor receptor antibody in colorectal cancer: another one or the one? Clin Cancer Res 2007;13:4664–4666.
- Tabernero, J. The role of VEGF and EGFR inhibition: implications for combining anti-VEGF and anti-EGFR agents. Mol Cancer Res. 2007; 5: 203–220.
- Ciardiello, F. and Tortora, G. EGFR antagonists in cancer treatment. N Engl J Med. 2008; 358: 1160–1174.
- Ciardiello, F., Bianco, R., Damiano, V., Fontanini, G., Caputo, R., Pomatico, G. et al. Antiangiogenic and antitumor activity of antiepidermal growth factor receptor C225 monoclonal antibody in combination with vascular endothelial growth factor antisense oligonucleotide in human GEO colon cancer cells. Clin Cancer Res. 2000; 6: 3739–3747.
- Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 2004;351:337–345.
- Jonker DJ, O’Callaghan CJ, Karapetis CS, et al. Cetuximab for the treatment of colorectal cancer. N Engl J Med 2007;357:2040– 2048.
- Finocchiaro G, Cappuzzo F, Janne PA, et al. EGFR, HER2, Kras as predictive factors for cetuximab sensitivity in colorectal cancer (abstr). J Clin Oncol 2007;25:18S.
- Krasteva, N.; Georgieva, M. Promising Therapeutic Strategies for Colorectal Cancer Treatment Based on Nanomaterials. Pharmaceutics 2022, 14, 1213. [CrossRef]
- Mai F. Tolba. Revolutionizing the landscape of colorectal cancer treatment: The potential role of immune checkpoint inhibitors. Int. J. Cancer. 2020;147:2996–3006. [CrossRef]
- Halama N, Zoernig I, Jager D. Immunotherapy for cancer – modern immunologic strategiesin oncology. DeutscheMedizinischeWochenschrift 2008;133:2105–8.
- Ahui Fan, Boda Wang, Xin Wang, Yongzhan Nie, Daiming Fan, Xiaodi Zhao and Yuanyuan Lu. Immunotherapy in colorectal cancer: current achievements and future perspective. International Journal of Biological Sciences 2021; 17(14): 3837-3849. [CrossRef]
- Le DT UJN, Wang H, Bartlett BR, et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med. 2015;372:2509-2520.
- Boland PM, Ma WW. Immunotherapy for colorectal cancer. Cancer. 2017;9:50.
- Germano G, Lamba S, Rospo G, et al. Inactivation of DNA repair triggers neoantigen generation and impairs tumour growth. Nature. 2017;552:116-120.
- Mokhtari, R. B., Homayouni, T. S., Baluch, N., Morgatskaya, E., Kumar, S., Das, B., & Yeger, H.. Combination therapy in combating cancer. Oncotarget,2017; 8(23), 38022.
- Guo, Y. Combination Therapy to Enhance Cancer Treatment. University of California, Merced (2020).
- Cidón, E. U. The challenge of metastatic colorectal cancer. Clinical Medicine Insights: Oncology, 2101; 4, CMO-S5214.
- Grothey, A., Van Cutsem, E., Sobrero, A., Siena, S., Falcone, A., Ychou, M., ... & Laurent, D. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. The Lancet,2013; 381(9863), 303-312.
- Tonini, G., Vincenzi, B., Santini, D., Olzi, D., Lambiase, A., & Bonini, S. Ocular toxicity related to cetuximab monotherapy in an advanced colorectal cancer patient. Journal of the National Cancer Institute,2005; 97(8), 606-607.
- Albain, K. S., Nag, S. M., Calderillo-Ruiz, G., Jordaan, J. P., Llombart, A. C., Pluzanska, A., ... & O’Shaughnessy, J. Gemcitabine plus paclitaxel versus paclitaxel monotherapy in patients with metastatic breast cancer and prior anthracycline treatment. Journal of Clinical Oncology, 2008; 26(24), 3950-3957.
- Jang, B., Kwon, H., Katila, P., Lee, S. J., & Lee, H. Dual delivery of biological therapeutics for multimodal and synergistic cancer therapies. Advanced drug delivery reviews, 2016; 98, 113-133.
- Sethy, C., & Kundu, C. N. 5-Fluorouracil (5-FU) resistance and the new strategy to enhance the sensitivity against cancer: Implication of DNA repair inhibition. Biomedicine & Pharmacotherapy, 2021; 137, 111285.
- Longley, D. B., Harkin, D. P., & Johnston, P. G. 5-fluorouracil: mechanisms of action and clinical strategies. Nature reviews cancer, 2002; 3(5), 330-338.
- Benson III, A. B., & Goldberg, R. M. Optimal use of the combination of irinotecan and 5-fluorouracil. In Seminars in oncology 2003; (Vol. 30, No. 3, pp. 68-77). WB Saundv.
- Thirion, P., Michiels, S., Pignon, J. P., Buyse, M., Braud, A. C., Carlson, R. W., ... & Piedbois, P. Modulation of fluorouracil by leucovorin in patients with advanced colorectal cancer: an updated meta-analysis. Journal of clinical oncology: official journal of the American Society of Clinical Oncology, 2004; 22(18), 3766-3775.
- Saltz, L. B., Cox, J. V., Blanke, C., Rosen, L. S., Fehrenbacher, L., Moore, M. J., ... & Miller, L. L. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. New England Journal of Medicine, 2000; 343(13), 905-914.
- Szefler, B., & Czeleń, P. Will the interactions of some platinum (II)-Based drugs with B-vitamins reduce their therapeutic effect in cancer patients? Comparison of chemotherapeutic agents such as cisplatin, carboplatin and oxaliplatin—a review. International Journal of Molecular Sciences, 2023; 24(2), 1548.
- O’Dowd, P. D., Sutcliffe, D. F., & Griffith, D. M. Oxaliplatin and its derivatives–An overview. Coordination Chemistry Reviews, 2023; 497, 215439.
- Yoshino, T., Arnold, D., Taniguchi, H., Pentheroudakis, G., Yamazaki, K., Xu, R. H., ... & Douillard, J. Y. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: a JSMO–ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Annals of Oncology, 2018; 29(1), 44-70.
- Rosati, Gerardo, Giuseppe Aprile, Alfredo Colombo, Stefano Cordio, Marianna Giampaglia, Alessandro Cappetta, Concetta Maria Porretto, Alfonso De Stefano, Domenico Bilancia, and Antonio Avallone. "Colorectal cancer heterogeneity and the impact on precision medicine and therapy efficacy." Biomedicines 10, no. 5 (2022): 1035.
- Falcone, A., Masi, G., Allegrini, G., Danesi, R., Pfanner, E., Brunetti, I. M., ... & Conte, P. Biweekly chemotherapy with oxaliplatin, irinotecan, infusional fluorouracil, and leucovorin: a pilot study in patients with metastatic colorectal cancer. Journal of clinical oncology, 2002; 20(19), 4006-4014.
- Souglakos, J., Ziras, N., Kakolyris, S., Boukovinas, I., Kentepozidis, N., Makrantonakis, P., ... & Polyzos, A. Randomised phase-II trial of CAPIRI (capecitabine, irinotecan) plus bevacizumab vs FOLFIRI (folinic acid, 5-fluorouracil, irinotecan) plus bevacizumab as first-line treatment of patients with unresectable/metastatic colorectal cancer (mCRC). British journal of cancer, 2012; 106(3), 453-459.
- Cai, Y., Deng, R., Hu, H., Zhang, J., Ling, J., Wu, Z., ... & Deng, Y. Analysis on safety and preliminary efficacy of dose-modified regimen of 5-fluorouracil plus oxaliplatin and irinotecan (FOLFOXIRI) in advanced colorectal cancer. Zhonghua wei Chang wai ke za zhi= Chinese Journal of Gastrointestinal Surgery, 2018; 21(9), 1045-1050.
- Le Huy, T., Bui, M. H., Dinh, T. C., & Xuyen, H. T. H. Efficacy and toxicity of folfoxiri for patients with metastatic colorectal cancer. Open access Macedonian journal of medical sciences, 2019; 7(24), 4244.
- García-Alfonso, P., Muñoz Martín, A. J., Ortega Morán, L., Soto Alsar, J., Torres Perez-Solero, G., Blanco Codesido, M., ... & Grasso Cicala, S. Oral drugs in the treatment of metastatic colorectal cancer. Therapeutic Advances in Medical Oncology, 2021; 13, 17588359211009001.
- Walko, C. M., & Lindley, C. Capecitabine: a review. Clinical therapeutics, 2005; 27(1), 23-44.
- Alzahrani, S. M., Al Doghaither, H. A., Al-Ghafari, A. B., & Pushparaj, P. N. 5-Fluorouracil and capecitabine therapies for the treatment of colorectal cancer. Oncology Reports,2023; 50(4), 175.
- Guo, Y., Shi, M., Shen, X., Yang, C., Yang, L., & Zhang, J. Capecitabine plus irinotecan versus 5-FU/leucovorin plus irinotecan in the treatment of colorectal cancer: a meta-analysis. Clinical colorectal cancer, 2014; 13(2), 110-118.
- Montagnani, F., Chiriatti, A., Licitra, S., Aliberti, C., & Fiorentini, G. Differences in efficacy and safety between capecitabine and infusional 5-fluorouracil when combined with irinotecan for the treatment of metastatic colorectal cancer. Clinical Colorectal Cancer, 2010; 9(4), 243-247.
- Haller, D. G., J. Cassidy, S. Clarke, D. Cunningham, E. Van Cutsem, P. Hoff, M. Rothenberg, L. Saltz, H. J. Schmoll, and C. Twelves. "Tolerability of fluoropyrimidines appears to differ by region." Journal of Clinical Oncology 24, no. 18_suppl (2006): 3514-3514.
- Fuchs, C. S., Marshall, J., Mitchell, E., Wierzbicki, R., Ganju, V., Jeffery, M., ... & Barrueco, J. Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C Study. Journal of Clinical Oncology, 2007; 25(30), 4779-4786.
- Xu, R. H., Muro, K., Morita, S., Iwasa, S., Han, S. W., Wang, W., ... & Kim, T. W. Modified XELIRI (capecitabine plus irinotecan) versus FOLFIRI (leucovorin, fluorouracil, and irinotecan), both either with or without bevacizumab, as second-line therapy for metastatic colorectal cancer (AXEPT): a multicentre, open-label, randomised, non-inferiority, phase 3 trial. The Lancet Oncology, 2018; 19(5), 660-671.
- Wu, Q., Zhang, P., Wang, X., Zhang, M., Liao, W., & Li, Q. Cost-effectiveness of capecitabine+ irinotecan versus leucovorin+ fluorouracil+ irinotecan in the second-line treatment of metastatic colorectal cancer in China. Clinical Therapeutics, 2020; 42(11), 2148-2158.
- Pak, H., Maghsoudi, L. H., Soltanian, A., & Gholami, F. Surgical complications in colorectal cancer patients. Annals of Medicine and Surgery. 2020; 55, 13-18. [CrossRef]
- M. Gachabayov, A.J. Senagore, S.K. Abbas, S.B. Yelika, K. You, R. Bergamaschi, Perioperative hyperglycemia: an unmet need within a surgical site infection bundle, Tech. Coloproctol. 2018; 22 (3): 201–207.
- Schover, L. R., Van der Kaaij, M., Van Dorst, E., Creutzberg, C., Huyghe, E., & Kiserud, C. E. Sexual dysfunction and infertility as late effects of cancer treatment. European Journal of Cancer Supplements. 2014; 12(1), 41-53. [CrossRef]
- W.K. Lee, Y.H. Park, S. Choi, W.S. Lee, Is liquid-based hyaluronic acid equivalent to sodium hyaluronate-based bioresorbable membrane to reduce small bowel obstruction in patients undergoing colorectal surgery, Asian J. Surg. 2019; 42 (2): 443–449.
- M. Fesharakizadeh, D. Taheri, S. Dolatkhah, S.D. Wexner, Postoperative ileus in colorectal surgery: is there any difference between laparoscopic and open surgery? Gastroenterology report. 2013; 1 (2): 138–143.
- S. Smolarek, M. Shalaby, G. Paolo Angelucci, G. Missori, I. Capuano, L. Franceschilli, et al., Small-bowel obstruction secondary to adhesions after open or laparoscopic colorectal surgery, J. Soc. Laparoendosc. Surg. : J. Soc. Laparoendosc. Surg. 2016; 20 (4): e201600073.
- K.M. Yang, C.S. Yu, J.L. Lee, C.W. Kim, Y.S. Yoon, I.J. Park, et al., The long-term outcomes of recurrent adhesive small bowel obstruction after colorectal cancer surgery favor surgical management. 2017; 96 (43) e8316.
- V. Sallinen, S. Di Saverio, E. Haukijärvi, R. Juusela, H. Wikström, V. Koivukangas, et al., Laparoscopic versus open adhesiolysis for adhesive small bowel obstruction (LASSO): an international, multicentre, randomized, open-label trial, Lancet.Gastroenterol. Hepatol. 2019; 4 (4): 278–286.
- S. Yao, E. Tanaka, Y. Matsui, A. Ikeda, T. Murakami, T. Okumoto, et al., Does laparoscopic adhesiolysis decrease the risk of recurrent symptoms in small bowel obstruction? A propensity score-matched analysis, Surg. Endosc. 2017; 31 (12): 5348–5355.
- S. Fujii, M. Tsukamoto, R. Shimada, K. Okamoto, T. Hayama, T. Tsuchiya, et al., Absorptive anti-adhesion barrier for the prevention of bowel obstruction after laparoscopic colorectal cancer surgery. 2018; 2 (1): 1–8.
- C.-W. Hsu, M.-C. Chang, J.-H. Wang, C.-C. Wu, Y-HJIJoCD. Chen, Placement of SurgiWrap® adhesion barrier film around the protective loop stoma after laparoscopic colorectal cancer surgery may reduce the peristomal adhesion severity and facilitate the closure. 2019; 34 (3): 513–518.
- M. Elia-Guedea, E. Cordoba-Diaz de Laspra, E. Echazarreta-Gallego, M.I. Valero Lazaro, J.M. Ramirez-Rodriguez, V. Aguilella-Diago, Colorectal surgery and surgical site infection: is a change of attitude necessary? Int. J. Colorectal Dis. 2017; 32 (7): 967–974.
- Y.Z. Xie, K. Fang, W.L. Ma, Z.H. Shi, X.Q. Ren, Risk of postoperative deep venous thrombosis in patients with colorectal cancer treated with open or laparoscopic colorectal surgery: a meta-analysis, Indian J. Canc. 2015; 51 (Suppl 2): e42–e44.
- E. Sebastian, R. Courtier, F. Macia, L. Grande, M. Pera, The impact of screening on short-term outcome after surgery for colorectal cancer, Rev. Esp. Enferm. Dig. : organo oficial de la Sociedad Espanola de Patologia Digestiva. 2017; 109 (7): 485–490.
- K.N. Zaghiyan, H.C. Sax, E. Miraflor, D. Cossman, W. Wagner, J. Mirocha, et al., Timing of chemical thromboprophylaxis and deep vein thrombosis in major colorectal surgery: a randomized clinical trial, Ann. Surg. 2016; 264 (4): 632–639.
- A. Holwell, J.L. McKenzie, M. Holmes, R. Woods, H. Nandurkar, C.S. Tam, et al., Venous thromboembolism prevention in patients undergoing colorectal surgery for cancer, ANZ J. Surg. 2014; 84 (4): 284–288.
- M. Carrier, A.D. Altman, N. Blais, A. Diamantouros, D. McLeod, U. Moodley, et al., Extended thromboprophylaxis with low-molecular weight heparin (LMWH) following abdominopelvic cancer surgery, Am. J. Surg. (2018).
- A.K. Saha, F. Chowdhury, A.K. Jha, S. Chatterjee, A. Das, P. Banu, Mechanical bowel preparation versus no preparation before colorectal surgery: a randomized prospective trial in a tertiary care institute, J. Nat. Sci. Biol. Med. 2014; 5 (2): 421–424.
- Lange MM, van de Velde CJ. Urinary and sexual dysfunction after rectal cancer treatment. Nat Rev Urol. 2011 Jan;8(1):51-7. Epub 2010 Dec 7. [CrossRef] [PubMed]
- Ball, M., Nelson, C.J., Shuk, E. et al. Men’s Experience with Sexual Dysfunction Post-rectal Cancer Treatment: A Qualitative Study. J Canc Educ. 2013; 28, 494–502. [CrossRef]
- Hendren SK, O'Connor BI, Liu M, et al. Prevalence of male and female sexual dysfunction is high following surgery for rectal cancer. Ann Surg. 2005; 242:212–23. [PubMed: 16041212].
- Mannaerts G, Schijven MP, Hendrikx A, Martijn H, Rutten HJ, Wiggers T. Urologic and sexual morbidity following multimodality treatment for locally advanced primary and locally recurrent rectal cancer. Eur J Surg Oncol. 2001; 27:265–72. [PubMed: 11373103].
- Ho VP, Lee Y, Stein SL, Temple LK. Sexual function after treatment for rectal cancer: a review. Diseases of the Colon & Rectum. 2011; 54:113–25. [PubMed: 21160322].
- Perry WRG, Abd El Aziz MA, Duchalais E, Grass F, Behm KT, Mathis KL, Kelley SR. Sexual dysfunction following surgery for rectal cancer: a single-institution experience. Updates Surg. 2021 Dec;73(6):2155-2159. Epub 2021 Jul 8. [CrossRef] [PubMed]
- Andersen BL, Cyranowski JM, Espindle D. Men's sexual self-schema. J Pers Soc Psychol. 1999; 76:645–61. [PubMed: 10234850].
- Nelson CJ, Deveci S, Stasi J, Scardino PT, Mulhall JP. Sexual bother following radical prostatectomy. J Sex Med. 2010; 7:129–35. [PubMed: 20104671].
- Ghomeshi, A., Zizzo, J., Reddy, R., White, J., Swayze, A., Swain, S., & Ramasamy, R. The erectile and ejaculatory implications of the surgical management of rectal cancer. International Journal of Urology. 2023; 30(10), 827-837. [CrossRef]
- Dhaliwal A, Gupta M (2022). PDE5 inhibitors. StatPearls Publishing LLC: Treasure Island (FL).
- Hor M, Baradeiya AM, Qasim H, Nasr M, Mohammad A. Non-Arteritic anterior ischemic optic neuropathy associated with the use of phosphodiesterase type 5 inhibitors: a literature review. Cureus. 2022; 14(8):e27642.
- Değer MD, Madendere S. Erectile dysfunction treatment with Phosphodiesterase-5 inhibitors: Google trends analysis of last 10 years and COVID-19 pandemic. Arch Ital Urol Androl. 2021; 93(3): 361–5.
- Chen Y, Chang HC, Huang WJ, Wang CJ, Hwang TIS, Liao CH, et al., Consensus of experts on the treatment of sexual dysfunction after surgery for prostate cancer in Taiwan. J Clin Med. 2023; 12(3): 740.
- Cuzin B. Alprostadil cream in the treatment of erectile dysfunction: clinical evidence and experience. Ther Adv Urol. 2016; 8(4): 249–56.
- Hatzimouratidis K, Salonia A, Adaikan G, Buvat J, Carrier S, el-Meliegy A, et al.,. Pharmacotherapy for erectile dysfunction: recommendations from the fourth international consultation for sexual medicine (ICSM 2015). J Sex Med. 2016; 13(4): 465–88.
- Das S, Dodd S, Soni BM, Sharma SD, Gazvani R, Lewis-Jones DI. Does repeated electro-ejaculation improve sperm quality in spinal cord injured men? Spinal Cord. 2006; 44(12): 753–6.
- Gupta S, Sharma R, Agarwal A, Parekh N, Finelli R, Shah R, et al. A comprehensive guide to sperm recovery in infertile men with retrograde ejaculation. World J Mens Health. 2022; 40(2): 208–16.
- Cong R, Zhang Q, Wang Y, Meng X, Wang Z, Song N. Two cases of psychogenic anejaculation patients got normal ejaculation ability after penile vibratory stimulation or electroejaculation. Transl Androl Urol. 2019; 8(6): 758–61.
- Surbone A, Vaucher L, Primi MP, Leyvraz C, Pitteloud N, Ballabeni P, et al.,. Clomiphene citrate effect on testosterone level and semen parameters in 18 infertile men with low testosterone level and normal/low gonadotropines level. Eur J Obstet Gynecol Reprod Biol. 2019; 238: 104–9.
- Canada AL, Neese LE, Sui D, Schover LR. Pilot Intervention to Enhance Sexual Rehabilitation for Couples after Treatment for Localized Prostate Carcinoma. Cancer. 2006.
- Fadlallah, H., El Masri, J., Fakhereddine, H., Youssef, J., Chemaly, C., Doughan, S., & Abou-Kheir, W. Colorectal cancer: recent advances in management and treatment. World Journal of Clinical Oncology, 2024; 15(9), 1136.
- Horesh, N., Emile, S. H., Garoufalia, Z., Gefen, R., Zhou, P., & Wexner, S. D. Trends in management and outcomes of colon cancer in the United States over 15 years: Analysis of the National Cancer Database. International Journal of Cancer, 2024; 155(1), 139-148.
- Jairam, V., Lee, V., Park, H. S., Thomas, C. R., Melnick, E. R., Gross, C. P., ... & James, B. Y. Treatment-related complications of systemic therapy and radiotherapy. JAMA oncology, 2019; 5(7), 1028-1035.
- Kumar AR, Sanford NN. Toxicity Management in the Era of Changing Treatment Paradigms for Locally Advanced Rectal Cancer. Curr Colorectal Cancer Rep. 2022;18(5):55-59Epub 2022 Nov 7. [CrossRef] [PubMed] [PubMed Central]
- Jian, Y., Zhang, D., Liu, M., Wang, Y., & Xu, Z. X. The impact of gut microbiota on radiation-induced enteritis. Frontiers in cellular and infection microbiology, 2021; 11, 586392.
- Long, L., Zhang, Y., Zang, J., Liu, P., Liu, W., Sun, C., ... & Xiao, J. Investigating the relationship between postoperative radiotherapy and intestinal flora in rectal cancer patients: a study on efficacy and radiation enteritis. Frontiers in Oncology, 2024; 14, 1408436.
- Liu, M. M., Li, S. T., Shu, Y., & Zhan, H. Q. Probiotics for prevention of radiation-induced diarrhea: A meta-analysis of randomized controlled trials. PloS one, 2017; 12(6), e0178870.
- Garczyk, A., Kaliciak, I., Drogowski, K., Horwat, P., Kopeć, S., Staręga, Z., and Mardas, M. Influence of probiotics in prevention and treatment of patients who undergo chemotherapy or/and radiotherapy and suffer from mucositis, diarrhoea, constipation, nausea and vomiting. Journal of Clinical Medicine, 2022; 11(12), 3412.
- Meirow, D., Biederman, H., Anderson, R. A., & Wallace, W. H. B. Toxicity of chemotherapy and radiation on female reproduction. Clinical obstetrics and gynecology, 2010; 53(4), 727-739.
- Skrzypek, M., Wdowiak, A., Panasiuk, L., Stec, M., Szczygieł, K., Zybała, M., & Filip, M. Effect of ionizing radiation on the female reproductive system. Annals of Agricultural and Environmental Medicine, 2019; 26(4), 606-616.
- Aldoury, R. S. M. A Review Article: Effect of Radiation on Infertility. International Journal for Research in Applied Sciences and Biotechnology, 2022; 9(1), 45-65.
- Kesari, K. K., Agarwal, A., & Henkel, R. Radiations and male fertility. Reproductive Biology and Endocrinology, 2018; 16(1), 118.
- Fukunaga, H., Yokoya, A., & Prise, K. M. A brief overview of radiation-induced effects on spermatogenesis and oncofertility. Cancers, 2022; 14(3), 805.
- McQuade, R. , Bornstein, J. and Nurgali, K. Anti-Colorectal Cancer Chemotherapy-Induced Diarrhoea: Current Treatments and Side-Effects. International Journal of Clinical Medicine. 2014; 5, 393-406. [CrossRef]
- Baek, K.L., Lee, J., Park, S.H., Park, J.O., Park, Y.S., Lim, H.Y., Kiang, W.K., Cho, Y.B., Yun, S.H., Kim, H.C., Lee, Y.W. and Chun, H.K. Oxaliplatin-Induced Chronic Peripheral Neurotocixity: A Prospective Analysis in Patients with Colorectal Cancer. Cancer Research and Treatment. 2010; 45, 185-190. [CrossRef]
- Stringer, A.M., Gibson, R.J., Logan, R.M., Bowen, J.M. and Yeoh, A.S. Chemotherapy-Induced Diarrhoea Is Associated with Changes in the Luminal Environment in the DA Rat. Experimental Biology & Medicine. 2007; 232, 96-106.
- Stringer, A.M., Gibson, R.J., Bowen, J.M., Logan, R.M., Ashton, K., Yeoh, A.S.J., Al-Dasooqi, N. and Keefe, D.M.K. Irinotecan-Induced Mucositis Manifesting as Diarrhoea Corresponds with Amended Intestinal Flora and Mucin Profile. International Journal of Experimental Pathology. 2009; 90: 489-499. [CrossRef]
- Verstappen, C.C.P., Heimans, J.J., Hoekman, K. and Postma, T.J. Nuerotoxic Complocations of Chemotherapy in Patients with Cancer, Clinical Signs and Optimal Management. Therapy in Practice. 2003; 63: 1549-1563.
- Benson III, A.B., Ajani, J.A., Catalano, R.B., Engelking, C., Kornlau, S.M., Martenson Jr., J.A., McCallum, R., Mit chell, E.P., O’Dorsio, T.M., Vokes, E.E. and Wadler, S. (2004) Recommended Guidelines for the Treatment of Cancer Treatment- Induced Diarrhea. Journal of Clinical Oncolog. 2004; 22: 2918-2926. [CrossRef]
- Stein, A., Voigt, W. and Jordan, K. Review: Chemotherapy-Induced Diarrhea: Pathophysiology, Frequency and Guideline Based Management. Therapeutic Advances in Medical Oncology. 2010; 2: 51-63. [CrossRef]
- Keefe, D.M., Schubert, M.M., Elting, L.S., Sonis, S.T., Epstein, J.B., Raber-Durlacher, J.E., Migliorati, C.A., McQuire, D.B., Hutchins, R.D. and Peterson, D.E. Updates Clinical Practice Guidelines for the Prevention and Treatment of Mucositis. Cancer. 2007; 109: 820-832. [CrossRef]
- Richardson, G.G. and Dobish, R.R. Chemotherapy-Induced Diarrhea. Journal of Oncology Pharmacy Practice. 2007; 13: 181-198. [CrossRef]
- Mitchell, E.P. Gastrointestinal Toxicity of Chemotherapeutic Agents. Seminars in Oncology. 2006; 33, 106-120. [CrossRef]
- Shafi, M.A. and Bresalier, R.S. The Gastrointestinal Complications of Oncologic Therapy. Gastroenterology Clinics of North America. 2010; 39, 629-647. [CrossRef]
- Kuebler, J.P., Colengalo, L., O’Connell, M.J., Smith, R.E., Yothers, G., Begovic, M., Robinson, B., Seay, T.E. and Wol- mark, N. Severe Enteropathy among Patients with Stage II/III Colon Cancer Treated on a Randomized Trial of Bolus 5-FU/Leucovorin Plus or Minus Oxaliplatin. Cancer. 2007; 110: 1945-1950. [CrossRef]
- Dranitsaris, G., Maroun, J. and Shah, A. Estimating the Cost of Illness in Colorectal Cancer Patients Who Were Hospitalized for Severe Chemotherapy-Induced Diarrhea. Canadian Journal of Gastroenterology. 2005; 19: 83-87.
- Arbuckle, R.B., Huber, S.L. and Zacker, C. The Consequences of Diarrhea Occurring during Chemotherapy for Colorectal Cancer: A Retrospective Study. The Oncologist. 2000; 5: 250-259. [CrossRef]
- Castro-Rodriguez, J.A., Salazar-Lindo, E. and Leon-Barua, R. (1997) Differentiation of Osmotic and Secretory Diar- rhoea by Stool Carbohydrate and Osmolar Gap Measurements. Archives of Disease in Childhood. 1997; 77: 201-205. [CrossRef]
- Ferrell, B.R. and Coyle, N. (2005) Textbook of Palliative Nursing. Oxford University Press, Oxford.
- Vera, G., Castillo, M., Cabezos, P.A., Chairlone, A., Martin, M.I., Gori, A., Paquinelli, G., Barbara, G., Staghelleni, V., Corinaldesi, R., De Giorgio, R. and Abalo, R. Enteric Neuropathy Evoked by Repeated Cisplatin in the Rat. Neurogastroenterology & Motility. 2011; 23: 370-e162. [CrossRef]
- Wafai, L., Taher, M., Jovanovska, V., Bornstein, J.C., Dass, C.R. and Nurgali, K. Effects of Oxaliplatin on Mouse Myenteric Neurons and Colonic Motility. Frontiers in Neuroscience. 2013; 7, 1-8. [CrossRef]
- Kalliopi Keramida Georgios Charalampopoulos, Dimitrios Filippiadis, Elias Tsougos, Dimitrios Farmakisi. Cardiovascular complications of metastatic colorectal cancer treatment. J Gastrointest Oncol 2019;10(4):797-806. [CrossRef]
- Becker K, Erckenbrecht JF, Haussinger D, et al. Cardiotoxicity of the antiproliferative compound fluorouracil. Drugs 1999;57:475-84.
- Polk A, Vaage-Nilsen M, Vistisen K, et al. Cardiotoxicity in cancer patients treated with 5-fluorouracil or capecitabine: a systematic review of incidence, manifestations and predisposing factors. Cancer Treat Rev 2013;39:974-84.
- Zamorano JL, Lancellotti P, Rodriguez Munoz D, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J 2016;37:2768-801.
- McKendrick J, Coutsouvelis J. Capecitabine: effective oral fluoropyrimidine chemotherapy. Expert Opin Pharmacother 2005;6:1231-9.
- Leicher LW, de Graaf JC, Coers W, et al. Tolerability of Capecitabine Monotherapy in Metastatic Colorectal Cancer: A Real-World Study. Drugs R D 2017;17:117-24.
- Shah NR, Shah A, Rather A. Ventricular fibrillation as a likely consequence of capecitabine-induced coronary vasospasm. J Oncol Pharm Pract 2012;18:132-5.
- Kwakman JJ, Simkens LH, Mol L, et al. Incidence of capecitabine-related cardiotoxicity in different treatment schedules of metastatic colorectal cancer: A retrospective analysis of the CAIRO studies of the Dutch Colorectal Cancer Group. Eur J Cancer 2017;76:93-9.
- Saif MW, Shah MM, Shah AR. Fluoropyrimidine associated cardiotoxicity: revisited. Expert Opin Drug Saf 2009;8:191-202.
- Di Lorenzo G, Autorino R, Bruni G, et al. Cardiovascular toxicity following sunitinib therapy in metastatic renal cell carcinoma: a multicenter analysis. Ann Oncol 2009;20:1535-42.
- Zhu X, Wu S, Dahut WL, et al. Risks of proteinuria and hypertension with bevacizumab, an antibody against vascular endothelial growth factor: systematic review and meta-analysis. Am J Kidney Dis 2007;49:186-93.
- Brinda BJ, Viganego F, Vo T, et al. Anti-VEGF-Induced Hypertension: a Review of Pathophysiology and Treatment Options. Curr Treat Options Cardiovasc Med 2016;18:33.
- Cai J, Ma H, Huang F, et al. Correlation of bevacizumab induced hypertension and outcomes of metastatic colorectal cancer patients treated with bevacizumab: a systematic review and meta-analysis. World J Surg Oncol 2013;11:306.
- Totzeck M, Mincu RI, Rassaf T. Cardiovascular Adverse Events in Patients With Cancer Treated With Bevacizumab: A Meta-Analysis of More Than 20 000 Patients. J Am Heart Assoc 2017;6.
- Hurwitz HI, Saltz LB, Van Cutsem E, et al. Venous thromboembolic events with chemotherapy plus bevacizumab: a pooled analysis of patients in randomized phase II and III studies. J Clin Oncol 2011; 29:1757-64.
- Baron Esquivias G, Asteggiano R. Cardiac Management of Oncology Patients: Clinical Handbook for Cardio-Oncology. New York: Springer International Publishing; 2015.
- Petrelli F, Cabiddu M, Borgonovo K, et al. Risk of venous and arterial thromboembolic events associated with anti EGFR agents: a meta-analysis of randomized clinical trials. Ann Oncol 2012;23:1672-9.
- Tang XM, Chen H, Liu Y, et al. The cardiotoxicity of cetuximab as single therapy in Chinese chemotherapy-refractory metastatic colorectal cancer patients. Medicine (Baltimore) 2017; 96:e5946.
- Tang XM, Chen H, Li Q, et al. Assessment of the cardiac safety between cetuximab and panitumumab as single therapy in Chinese chemotherapy-refractory mCRC. Onco Targets Ther 2017; 11:123-9.
- Staff NP, Grisold A, Grisold W, Windebank AJ. Chemotherapy-induced peripheral neuropathy: A current review. Ann Neurol. 2017 Jun;81(6):772-781. Epub 2017 Jun 5. [CrossRef] [PubMed] [PubMed Central]
- Cheng F, Zhang R, Sun C, Ran Q, Zhang C, Shen C, Yao Z, Wang M, Song L and Peng C. Oxaliplatin-induced peripheral neurotoxicity in colorectal cancer patients: mechanisms, pharmacokinetics and strategies. Front. Pharmacol. 2023; 14:1231401. [CrossRef]
- Krarup-Hansen A, Rietz B, Krarup C, Heydorn K, Rorth M, Schmalbruch H. Histology and platinum content of sensory ganglia and sural nerves in patients treated with cisplatin and carboplatin: an autopsy study. Neuropathol Appl Neurobiol. 1999 Feb; 25(1):29–40. [PubMed: 10194773].
- Bentzen AG, Balteskard L, Wanderas EH, et al. Impaired health-related quality of life after chemoradiotherapy for anal cancer: late effects in a national cohort of 128 survivors. Acta Oncol. 2013 May; 52(4):736–44. [PubMed: 23438358].
- Johnson C, Pankratz VS, Velazquez AI, et al. Candidate pathway-based genetic association study of platinum and platinum-taxane related toxicity in a cohort of primary lung cancer patients. J Neurol Sci. 2015 Feb 15; 349(1-2):124–8. [PubMed: 25586538].
- Chambers SM, Qi Y, Mica Y, et al. Combined small-molecule inhibition accelerates developmental timing and converts human pluripotent stem cells into nociceptors. Nat Biotechnol. 2012 Jul; 30(7):715–20. [PubMed: 22750882].
- Mezzanotte, Jessica & Grimm, Michael & Shinde, Namrata & Nolan, Timiya & Worthen-Chaudhari, Lise & Williams, Nicole & Lustberg, Maryam. Updates in the Treatment of Chemotherapy-Induced Peripheral Neuropathy. Current Treatment Options in Oncology. 2022; 23. [CrossRef]
- Mustafa G, et al. , Anti-nociceptive effect of a conjugate of substance P and light chain of botulinum neurotoxin type A. Pain, 2013. 154(11): p. 2547–2553. [PubMed: 23933181].
- Zhu Y, et al. , Ganglioside-monosialic acid (GM1) prevents oxaliplatin-induced peripheral neurotoxicity in patients with gastrointestinal tumors. World J Surg Oncol, 2013. 11: p. 19. [PubMed: 23351188].
- Glimelius B, et al. , Persistent prevention of oxaliplatin-induced peripheral neuropathy using calmangafodipir (PledOx(¬¨√Ü)): a placebo-controlled randomised phase II study (PLIANT). Acta Oncol, 2018. 57(3): p. 393–402. [PubMed: 29140155].
- Szepanowski F, et al., Fingolimod promotes peripheral nerve regeneration via modulation of lysophospholipid signaling. J Neuroinflammation, 2016. 13(1): p. 143. [PubMed: 27283020].
- Jin, H., Wang, L., & Bernards, R. Rational combinations of targeted cancer therapies: background, advances and challenges. Nature Reviews Drug Discovery, 2023; 22(3), 213-234.
- Mohapatra, L., Tripathi, A. S., Mishra, D., Parida, S. K., Yasir, M., Maurya, R. K., & Prajapati, B. G. Current drug therapy for colorectal cancer. In Colorectal Cancer 2024; (pp. 115-148). Academic Press.
- Wu, J., Wang, Z., Jin, C., Ren, H., Hu, Y., Yang, B., & Hu, Y. Effect of cetuximab combined with chemotherapy in treating metastatic colorectal cancer and its prognostic analysis. J BUON, 2021; 26(1), 101-108.
- Kasi, P. M., Afable, M. G., Herting, C., Lukanowski, M., & Jin, Z. Anti-EGFR antibodies in the management of advanced colorectal cancer. The Oncologist, 2023; 28(12), 1034-1048.
- Liu, T., Jiang, S., Teng, X., Zhong, L., Liu, M., Jin, Y., & Dong, M. A comparison of panitumumab and cetuximab in the treatment of KRAS wild-type metastatic colorectal cancer: a systematic review and meta-analysis. Immunopharmacology and Immunotoxicology, 2023; 45(1), 1-9.
- Watanabe, J., Muro, K., Shitara, K., Yamazaki, K., Shiozawa, M., Ohori, H., ... & Yoshino, T. Panitumumab vs bevacizumab added to standard first-line chemotherapy and overall survival among patients with RAS wild-type, left-sided metastatic colorectal cancer: a randomized clinical trial. Jama, 2023; 329(15), 1271-1282.
- Chibani, H., El Bairi, K., Al Jarroudi, O., & Afqir, S. Bevacizumab in metastatic colorectal cancer in a real-life setting–toxicity profile, survival outcomes, and impact of tumor sidedness. Contemporary Oncology/Współczesna Onkologia, 2022; 26(1), 32-39.
- Moisuc, D. C., Marinca, M. V., Matei, A. M., Popovici, L., & Cianga, P. The Impact of Bevacizumab and Chemotherapy on Quality of Life in Metastatic Colorectal Cancer Patients. In Healthcare 2023; (Vol. 11, No. 4, p. 591). MDPI.
- Wei, Y., Jin, R., Xue, H., Zhou, R., & Chen, Z. Clinical Efficacy and Adverse Effects of Bevacizumab in Combination with Chemotherapy for Metastatic Colorectal Cancer. Alternative Therapies in Health and Medicine, 2024; AT10143-AT10143.
- Manz, S. M., Losa, M., Fritsch, R., & Scharl, M. Efficacy and side effects of immune checkpoint inhibitors in the treatment of colorectal cancer. Therapeutic advances in gastroenterology, 2021; 14, 17562848211002018. [CrossRef]
- Goodman, R. S., Johnson, D. B., & Balko, J. M. Corticosteroids and Cancer Immunotherapy. Clinical cancer research: an official journal of the American Association for Cancer Research, 2023; 29(14), 2580–2587. [CrossRef]
- Nasca, V., Barretta, F., Corti, F., Lonardi, S., Niger, M., Elez, M. E., ... & Pietrantonio, F. Association of immune-related adverse events with the outcomes of immune checkpoint inhibitors in patients with dMMR/MSI-H metastatic colorectal cancer. Journal for immunotherapy of cancer, 2023; 11(1).
- Friedman, C. F., Proverbs-Singh, T. A., & Postow, M. A. Treatment of the immune-related adverse effects of immune checkpoint inhibitors: a review. JAMA oncology, 2016; 2(10), 1346-1353.
- Ganesh, K., Stadler, Z. K., Cercek, A., Mendelsohn, R. B., Shia, J., Segal, N. H., & Diaz Jr, L. A. Immunotherapy in colorectal cancer: rationale, challenges and potential. Nature reviews Gastroenterology & hepatology, 2019; 16(6), 361-375.
- Golshani, G., & Zhang, Y. Advances in immunotherapy for colorectal cancer: a review. Therapeutic advances in gastroenterology, 2020; 13, 1756284820917527. [CrossRef]
- Collins, M., Soularue, E., Marthey, L., & Carbonnel, F. Management of patients with immune checkpoint inhibitor-induced enterocolitis: a systematic review. Clinical gastroenterology and hepatology, 2020; 18(6), 1393-1403.
- Abu-Sbeih, H., Ali, F. S., Wang, X., Mallepally, N., Chen, E., Altan, M., ... & Wang, Y. Early introduction of selective immunosuppressive therapy associated with favorable clinical outcomes in patients with immune checkpoint inhibitor-induced colitis. Journal for immunotherapy of cancer, 2019; 7, 1-11.
- Martins, F., Sofiya, L., Sykiotis, G. P., Lamine, F., Maillard, M., Fraga, M., ... & Obeid, M. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. Nature reviews Clinical oncology, 2019; 16(9), 563-580.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



