
Submitted:
29 May 2025
Posted:
29 May 2025
You are already at the latest version
Abstract
Reproductive health literacy (RHL) is essential to women’s ability to make informed reproductive health (RH) decisions and is a key determinant of RH outcomes. Resettled refugee women often experience poorer RH outcomes, yet there is limited research on their RHL and its influence on RH decision-making. This scoping review aims to: (1) to evaluate existing methods for measuring RHL among resettled refugee women, and (2) to characterize the relationship between RHL, RH decision-making, behavior, and outcomes among refugee women residing in high-income countries. A search of peer-reviewed literature published in English found limited direct measurement of RHL. Measurement methods were primarily qualitative or based on unvalidated survey instruments, limiting comparability and generalizability. The current methodologies do not adequately capture RH knowledge or RHL proficiency. A range of additional factors were found to influence RH decision-making and behavior, supporting the need for a means to accurately measure RHL. Further quantitative research is needed to clarify the extent to which RHL and knowledge influence RH behavior and outcomes. The development of a culturally relevant, validated RHL instrument that integrates knowledge and contextual influences would support healthcare providers and public health agents in serving and designing effective interventions for refugee women post-resettlement.
Keywords:
refugee
; post-resettlement
; reproductive health literacy
; health behavior
; decision-making
1. Introduction
Health literacy, a predictor of health behavior and health service utilization, is defined as the “knowledge, motivation and competences to access, understand, appraise, and apply health information in order to make judgments and take decisions in everyday life concerning healthcare, disease prevention and health promotion to maintain or improve quality of life during the life course” [1]. Low health literacy is associated with decreased healthcare service utilization, poorer health, and higher mortality [2]. With respect to reproductive health (RH), reproductive health literacy (RHL) greatly influences a woman’s ability to make informed decisions related to contraception, pregnancy, abortion, and other sexual and reproductive health concerns [3]. In studies evaluating the RHL of women in London, higher RHL was associated with the utilization of low-failure contraceptive methods and lower rates of unplanned pregnancy [4]. In contrast, low sexual and reproductive health (SRH) literacy corresponded with a 44% increase in pregnancy prevalence and higher pregnancy frequency [5,6]. These findings suggest a potential influence of RHL, to varying degrees, on individual RH behavior and outcomes.
Comparably, RH knowledge may also function as a predictor of RH behavior. General health knowledge is a precursor to, a component of, and a product of health literacy [7,8]. Together with other determinants of health literacy (such as personal, situational, and societal/environmental determinants as seen in Sørensen’s [1] integrated model of health literacy in Figure 1), health knowledge has a significant influence on health literacy and thereby health-related beliefs and decision-making. This model is also observable in RH domains, where greater RH knowledge is associated with improved oral contraceptive adherence, while limited knowledge is linked to reduced utilization [9,10,11,12].
The degree to which each of these factors influences the health behavior specifically of refugee women residing in their non-native countries is unknown. Given the significant role societal and cultural influences play in forming attitudes, beliefs, and behavior related to RH, women from refugee backgrounds likely experience barriers and facilitators of RH literacy and behavior to different degrees than non-refugee populations, such as limited access to social support and effective, culturally relevant care in their resettled country [13]. Disparities in RH health suggest unaddressed needs in this population. In the U.S., women from refugee backgrounds were reported to have significantly lower prevalence of mammograms, with 86% of refugee women over the age of 40 having never received a mammogram compared to 33% of non-refugee women [14]. A similar pattern is seen with Pap smear testing. When compared to non-refugee migrants in Australia, women from humanitarian source countries were more likely to have late first pregnancy care visits, post term birth, and poor or no pregnancy care attendance than women from non-humanitarian source countries [15]. A review of antenatal and prenatal female refugee outcomes in multiple high-income countries found higher rates of miscarriage, stillbirth, and perinatal mortality, despite lower rates of tobacco and drug usage during pregnancy [16]. Clarifying the role of RH literacy and knowledge in shaping RH outcomes of female refugee communities is critical to developing effective and evidence-based interventions post-resettlement.
There are currently an estimated 43.4 million refugees globally, 49% of whom are women, and 25% of whom are hosted in high-income countries [17]. This population has tripled in the last decade and continues to grow exponentially; however, despite having outpaced the growth of the world’s population, while simultaneously at higher risk for poorer RH outcomes, relatively little investigation has been done to examine the relationship between RHL, knowledge, behavior, and outcomes of refugee women post-resettlement [18]. This scoping review examined the existing literature to evaluate the current capacity to measure the RHL and knowledge of women from refugee backgrounds post-resettlement. It also aims to characterize the relationship between RHL, knowledge, decision-making, and RH outcomes in this population. The findings are intended to guide health care providers (HCPs) and public health agencies in addressing RH disparities in refugee communities and inform future research agendas aimed at better understanding the needs of resettled refugee women.
2. Methods
2.1. Study Design
This review was conducted in accordance with the methodological framework outlined by Arksey and O’Malley [19], and it adheres to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist, provided in the Appendix [20]. A formal review protocol was not developed. Due to the emerging nature of the subject, the heterogeneity of the population, the inclusion of both quantitative and qualitative studies, and the exploratory nature of the research question, a scoping review approach was most appropriate [21].
2.2. Study Aim
To provide a comprehensive picture of RHL with respect to the resettled refugee population, this scoping review aims to (1) identify and summarize the measures, tools, or indicators that have been used to evaluate RHL or knowledge of women from refugee backgrounds residing in high-income countries, and (2) examine any association between RHL or knowledge and RH behavior, decision-making, or outcomes.
2.3. Definitions and Inclusion Criteria
This review included studies that met the following criteria: (1) original, peer-reviewed research employing qualitative, quantitative, or mixed-methods designs published after 2013; (2) studies involving refugee women or mostly refugee women of childbearing age residing in high-income countries; (3) investigations assessing literacy, knowledge, or awareness of RH (or SRH) topics; and (4) publications available in English.
The inclusion criteria were informed based on the World Health Organization’s definition of RH, which encompasses a broad range of topics, including abortion, antenatal care, family planning, gender-based violence, HIV, sexually transmitted infections (STIs), maternal mortality, menstruation and gynecological health, and obstetric care [22]. In addition, studies were included if they examined refugee women’s awareness, knowledge, or literacy regarding any aspect of sexual or RH.
2.4. Data Sources and Search Strategy
The initial search was conducted in December 2023 and updated in September 2024, and May 2025 across three databases: Google Scholar, PUBMED, and Scopus. These databases were selected for their comprehensive coverage of medical, public health, and interdisciplinary literature. Medline, Embase, or Global Health were not included due to institutional access constraints and substantial content overlap with the selected databases.
The search was performed in three iterative rounds to refine search terms and inclusion/exclusion criteria. The final search strategy combined terms to capture relevant studies: (“refugee” OR “refugee women” OR “refugees” OR “resettlement”) AND (“reproductive health” OR “pregnancy” OR “contraception” OR “autonomy” OR “reproductive behavior” OR “reproductive decision”) AND (“health literacy” OR “reproductive literacy” OR “health knowledge” OR “reproductive knowledge”). Although the inclusion criteria encompassed a broad range of RH topics, the search strategy employed a focused set of representative terms to ensure search efficiency and reduce the retrieval of irrelevant records.
2.5. Study Selection
All retrieved titles were merged, and duplicate records were removed. The screening process was then performed in two-steps. In the first phase, titles and abstracts were independently screened by five team members (H.M., A.A., A.C., A.K., and N.S.) using predefined inclusion criteria, then reviewed by the first and last author not involved in the initial screening (K.T. and Z.G.). In the second stage, full-text articles were reviewed by all authors to determine final eligibility. Discrepancies were resolved through group consensus. The initial database search yielded 338 articles. After removing duplicates and conducting the screening process, 42 articles were retained. Of these, 20 articles met all eligibility criteria following full-text review. Citation screening identified 10 additional articles, of which 5 were included in the final analysis. No additional eligible articles were identified during a 2024 search update (performed by H.M.). Two additional articles were identified during a 2025 search update (performed by K.T.). A summary of the search and selection process is presented in Figure 2.
2.6. Data Extraction and Analysis
The first author and the last author (K.T. and Z.G.) identified key variables based on the study aims. These included study design, study population, geographic location, RH domain, measurement of RH knowledge/literacy, tools used to assess RH knowledge/literacy, reported RH behaviors and outcomes, indicators of these RH behavior/outcomes, and any reported association between RH knowledge/literacy and RH behaviors, outcomes, or decision-making.
The first and last authors (K.T. and Z.G.) independently extracted all relevant data using a standardized form designed for this review. The extracted data was then cross-checked and reviewed to ensure completeness and consistency. Preliminary findings were compiled in a data extraction table. A summary of the extracted data is presented in Table 1.
3. Results
3.1. Study Characteristics
From 338 articles, 27 studies met the inclusion criteria. Among these articles, there were 14 qualitative, nine quantitative, and four mixed-method studies. Two articles qualitatively assessed RHL with no formal measurement. Rauf et al. [23] created and validated an RHL scale for Afghan refugees with a focus on cervical cancer care, family planning, and maternal health/postpartum care. All of the remainder of the articles assessed knowledge of specific RH domains, rather than RHL. Family planning knowledge was the most common RH domain addressed, with 13 studies measuring knowledge regarding contraception, birth spacing, and other methods of birth control. Nine articles assessed cervical cancer knowledge, one article assessed gender-based violence, three articles assessed HIV knowledge, two articles assessed maternal care knowledge, one article assessed menstruation and gynecological health knowledge, and five articles assessed knowledge regarding STIs (this domain was always measured in conjunction with others). No studies evaluated knowledge on abortion. From these 27 studies, 15 studies directly assessed the relationship between RH knowledge and decision-making, behavior, or outcomes, of which nine were qualitative, five were quantitative, and one mixed-method. No studies evaluated the relationship between RHL and decision-making/behavior/outcomes.
In regard to geographic distribution, 12 of the studies took place in the U.S., and nine were in Australia. Less common geographical settings included Canada (one), Greece (one), Germany (two), Norway (one), Scotland (one), and Turkey (one).
3.2. RHL and Knowledge: Measurement Methods
3.2.1. RHL
Only one article sought to measure RHL across domains [23]. This study’s objective was specifically to create an RHL measurement tool for refugee women that could be used to assess RHL trainings for Afghan refugees. The primary domains of focus were family planning, maternal health, and cervical cancer prevention. However, the scale also included questions on general health literacy (adapted from HLS-EU-Q6) and digital health literacy (adapted from eHEALS). RH domain specific questions were adapted from the Cervical Cancer Literacy Assessment Tool (C-CLAT) and the Refugee Reproductive Health Network (ReproNet) postpartum literacy scale. These scales were selected due to previous validations for the population addressed in the study.
3.2.2. Cervical Cancer and Screening
Nine articles measured knowledge adequacy of cervical cancer and screening methods. Of the measurement methods, there were five questionnaire-based measures [24,25,26,27,28], four focus groups [27,29,30,31], one semi-structured interview [32], and one in-depth interview [31]. All questionnaires and focus group/interview guides were developed explicitly for their individual studies with the exception of the survey used in Dalla et al. [26] and Rauf et al. [23], which utilized adaptations of the Cervical Cancer Awareness Measure (Cervical CAM) and C-CLAT respectively.
3.2.3. Contraception and Family Planning
A total of 13 studies measured knowledge of topics relating to family planning and contraception. As a means to measure knowledge, three of these studies utilized focus groups [33,34,35], four utilized in-depth interviews [36,37,38,39], two utilized semi-structured interviews [41], and one utilized group concept-mapping [42]. In these articles, all interview guides were designed specifically for each study. Three studies utilized questionnaire-based indicators, of which the tools used in Dean et al. [42] and Napier-Raman et al. [43] were adapted from the National Survey of Australian Secondary Students and Sexual Health. The third questionnaire-based study created their survey specifically for their investigation [44].
3.2.4. HIV
Three articles assessed female refugees’ knowledge of HIV and HIV screening, all of which utilized questionnaires to quantitatively determine participants’ level of knowledge about HIV and screening practices. Two studies utilized indicators adapted from existing validated surveys: Dean et al. [42] used the questionnaire from the National Survey of Australian Secondary Students and Sexual Health (NSASSSH), and Feresu et al. [45] adapted their survey from questionnaires used by WHO, UN Program on HIV/AIDS, CDC, and other similar studies. The remaining article developed a survey specifically for the study by consulting academic experts to produce their questions [46]
3.2.5. Maternal Health and Pregnancy
A total of three studies measured knowledge about maternal care, including ante- and post-natal care and pregnancy. Two studies evaluated knowledge adequacy through interviews [47,48]. In addition to knowledge assessment by interview, Madeira et al. [48] also administered a questionnaire, which was created for a previous similar study, but not based on a validated tool. This is similar to Rauf et al. [23], which assessed knowledge through a previously created postpartum literacy scale.
3.2.6. Other Domains
The remainder of the RH domains—gender-based violence, menstruation/gynecological health and STIs—were never the primary focus of the studies and were consistently measured only alongside other topics. Knowledge of gender-based violence was qualitatively measured using group concept mapping in Napier-Raman et al. [42]. Knowledge in regard to menstruation and STIs was assessed in Metusela et al. [31] via focus groups and in-depth interviews. Other studies evaluating STI knowledge also evaluated family planning knowledge, all of which were qualitative [38,41,42] except for Dean et al. [43].
In total, only three of 25 reviewed studies utilized sets of questions directly or adapted from validated measurement tools. An overview of the indicators and tools used in each study is presented in Table 2.
3.3. RHL and Knowledge: Relation to Behavior, Decision-Making, and Outcomes
3.3.1. Cervical Cancer and Screening
All nine studies examining cervical cancer among refugee women reported limited knowledge of the disease, as well as of appropriate screening and prevention practices. Across multiple studies, reproductive health knowledge was strongly associated with health behaviors such as Pap smear uptake, cervical cancer screening, and HPV vaccination—particularly when combined with enabling factors like full-time employment, marriage, having children, or recent contact with a healthcare provider [24,29,32]. In contrast, low levels of knowledge were consistently linked to low screening rates, as seen in Burmese and Bhutanese refugee communities in the U.S. [30].
Participants across studies identified that both formal and informal health information played a critical role in developing self-efficacy and the confidence to make independent health decisions. Where knowledge was limited, misinformation and emotional barriers often emerged. These included inaccurate beliefs—for example, that HPV vaccines cause cancer or that cervical screening threatens virginity—as well as feelings of fear, embarrassment, and discomfort, particularly when interacting with male healthcare providers [24,30,31,32].
However, increasing awareness alone did not always lead to increased health behavior. In Anaman et al. [24], invitation letters designed to raise awareness of cervical cancer screening failed to improve screening rates. Self-initiated screenings remained nearly ten times lower among refugee women than non-refugees (2.2% vs. 21.0%), reflecting broader gaps in reproductive health literacy. In contrast, Ornelas et al. [28] demonstrated that targeted educational interventions could be more effective. Among Nepali-Bhutanese women, watching educational videos significantly improved awareness of cervical cancer testing (58% to 100%, p<0.001), awareness of the Pap smear (45% to 100%, p<0.001), and intention to screen (40% to 80%, p<0.001). Among Karen-Burmese women, however, results were more limited, with significant improvement observed only in Pap smear awareness (p = 0.008), and no change in screening intention.
3.3.2. Contraception and Family Planning
This review found wide variation in both knowledge of contraception and contraceptive uptake across studies. In general, refugee and asylum-seeking women demonstrated lower levels of knowledge and contraceptive use than native-born populations. In Germany, women who perceived themselves as sexually educated were more likely to use contraception; however, knowledge level did not influence their preference for traditional versus modern methods, suggesting potential gaps in understanding contraceptive efficacy [45]. Similarly, among African Australian teenage mothers in Australia, post-resettlement, awareness increased through informal channels like peers and media, but substantial gaps remained—particularly regarding mechanisms of action—which led to continued belief in myths and misinformation [38]. Similar trends were observed among Afghan refugees in Turkey, who exhibited low awareness of contraceptive options and lacked access to formal family planning education both before and after resettlement [37].
In contrast, Congolese refugee women in the U.S. demonstrated good knowledge of common contraceptive methods such as pills and injections but reported less awareness about long-acting methods like IUDs and implants, particularly regarding side effects [34]. Somali Bantu refugee women in the U.S. were found to have a broad and accurate understanding of birth control options, despite limited formal education or literacy [33]. However, their contraceptive decisions were driven more by sociocultural influences than by knowledge. This was also observed in refugee youth in Australia—despite higher knowledge levels of contraceptives than males, female refugee youth had higher rates of sexual coercion, STIs, and unplanned pregnancy, possibly due to gender norms placing the burden of reproductive responsibility on women [44].
Sociocultural norms and religious beliefs were key factors shaping attitudes and behaviors regarding contraception and family planning. In multiple contexts, stigma, cultural taboos, and traditional gender roles were reported as barriers to seeking RH information and using contraception [40,41]. Among Somali immigrant women in Oslo, religious beliefs and poor access to RH information fostered misconceptions and skepticism about contraceptives [36]. Similarly, Sudanese refugee youth in Australia reported cultural stigma as a major barrier to condom negotiation [43]. Refugee women in Glasgow described how cultural and religious norms limited their openness to discussing reproductive health and seeking care [41].
Across several studies, family and social networks were central to reproductive health decisions. In Metusela et al. [31], participants described negotiating contraception use with husbands, parents, and in-laws. Among Somali Bantu and Congolese women in the U.S., decision-making was often driven by male partners, regardless of the woman’s knowledge level [33,34]. Similarly, Afghan refugees in Turkey relied heavily on the influence of family and friends for reproductive health information and decisions [37]. In Australia, parental sexual health literacy and attitudes significantly shaped daughters’ knowledge and contraceptive behaviors [39].
In addition to sociocultural and informational barriers, structural challenges also limited contraceptive use. Refugee women in Glasgow reported that low RH knowledge and barriers to information severely constrained their ability to make informed reproductive decisions [41]. For Congolese women in the U.S., meeting basic survival needs—such as securing housing, food, and employment—took priority over seeking reproductive health care, regardless of their awareness or intentions [34]. Among Somali refugees in the U.S., challenges like lack of social support and emotional stress further hindered contraception uptake [35].
3.3.3. HIV
A community of African refugees in U.S. had low levels of HIV knowledge and high levels of stigma. However, higher knowledge was not associated with lower levels of stigma, and testing rates were relatively high at 49.5% of study participants reporting a history of screening [47]. Similarly, among Sudanese Queenslanders, Dean et al. [43] found low and inaccurate knowledge regarding HIV and STIs despite a desire for more information. Low knowledge was also associated with higher rates of sexual risk behavior. In the midwestern U.S., Somali Bantu and Sudanese immigrant women with less than primary school education were more likely to have inaccurate knowledge about the HIV/AIDS test and safe sex practices, but relatively good knowledge regarding HIV transmission (mean score, 10.1/14) [46].
3.3.4. Maternal Health and Pregnancy
In regard to maternal health and pregnancy, knowledge was shown to influence care utilization and care seeking behavior. In Germany, the knowledge level of Arabic speaking refugee women was found to be insufficient to perceive the need for health care in a timely manner during pregnancy and childbirth, resulting in delayed care [48]. An experimental study with Somali refugee and immigrant women showed that a group prenatal care model, Hooyo, increased knowledge of multiple pregnancy and prenatal topics (safe exercise in pregnancy (p=0.02), breastfeeding (p=0.04), hospital experience (p=0.02) and stress management (p=0.03)), and also resulted in increased post-intervention engagement in care [49].
3.3.5. Other Domains
A large qualitative study of migrant and refugee women from Afghanistan, Iraq, Somalia, South Sudan, Sudan, India, Sri Lanka, and South America—resettled in Sydney, Australia and Vancouver, Canada—found widespread self-reported gaps in knowledge across multiple sexual and reproductive health (SRH) domains, including menstruation, fertility, contraception, cervical screening, HPV vaccination, and STIs [31]. Similarly, migrant and refugee youth in Australia reported feeling inadequately educated about RH topics, particularly in areas such as healthy relationships, boundaries, and consent. However, decision-making was not driven by knowledge alone; interpersonal consequences were also cited as major influences on behavior [42].
Low levels of STI knowledge were also reported among Australian refugee youth in another study, which found a link between limited knowledge and increased sexual risk behavior [43].
4. Discussion
4.1. Measurement of RHL and Knowledge
Our ability to measure RHL of refugee women post-resettlement is limited. As such, most studies evaluated RH knowledge and its influence on decision-making and behavior. While RH knowledge influences RHL, they are not synonymous—RHL encompasses other enabling factors such as cognitive, emotional, and practical skills that make it a more comprehensive predictor of RH behavior than RH knowledge alone [2,51]. In addition, the studies included in our review relied predominantly on qualitative methods. While qualitative approaches allow for rich exploration of the many factors shaping RHL and behavior, they limit the ability to quantify and evaluate the strength of associations between RHL, knowledge, behavior, and health outcomes. Only four studies in this review used validated tools to measure RH knowledge, while four others relied on study-specific instruments with limited standardization. Furthermore, only two studies employed experimental designs, reducing the reliability and generalizability of conclusions about the relationship between RH knowledge and RH behaviors.
Most of the validated tools identified in our review—Cervical CAM, NSASSSH, and a WHO questionnaire—were developed for specific RH domains and non-refugee populations, limiting their applicability across broader RH topics or refugee contexts. The only exception to this was the ReproNet RHL scale, which adapted the HLS-EU-Q6 (general health literacy), eHEALS (digital literacy), RHL (C-CLAT), and ReproNet postpartum literacy scale, and was validated for Afghan refugees in the U.S. [23]. This highlights a need for further quantitative research using standardized and validated tools to better assess the links between RHL, knowledge, behavior, and outcomes in resettled refugee populations. Ideally, a comprehensive RHL scale would measure across multiple RH domains and account for the unique cultural, structural, and interpersonal factors influencing RHL and decision-making among refugee women. Existing quantitative RHL tools (e.g., SHELA, SHLS, SRHL-Q for Lao adolescents, and the Reproductive Health Literacy Questionnaire for Chinese Unmarried Youth) have been validated only in specific national contexts [52,53,54,55,56] and remain underutilized in refugee populations post-resettlement. Instead, most research continues to depend on knowledge screenings and qualitative data, resulting in inconsistent and often insufficient measurement of RHL in these communities.
4.2. RH Knowledge’s Influence on Decision-Making, Behavior, and Outcomes
Several studies in this review found that increased RH knowledge was generally associated with improved decision-making, greater engagement with RH services, and more positive health outcomes. Conversely, limited knowledge was linked to lower screening rates and reduced uptake of health-promoting behaviors. In the two experimental studies reviewed [28,49], participants who received RH education—via group prenatal classes or cervical cancer videos—showed increases in healthcare utilization, engagement, and behavioral intention. These findings align with broader evidence linking general health knowledge to positive health behaviors [2].
However, while knowledge played a role, many studies highlighted the importance of other enabling factors that shaped RH decisions and behaviors among refugee women. Several studies found that perceived risk had a stronger influence on behavior than knowledge alone, suggesting that subjective and sociocultural factors significantly impact RH decision-making [24,32,40,42,48].
Key individual and interpersonal factors included predisposing experiences (e.g., trauma, marital status, past healthcare encounters [30,48]), stigma (particularly related to HIV and family planning [27,30,39,40]), and emotional barriers (such as fear, mistrust, and embarrassment [32,35]). Sociocultural influences were also central: religious and gender norms, partner approval, cultural expectations, and reliance on informal sources of information were frequently cited as influential [29,30,31,33,34,35,37,39,40,41,42,44,47,49].
At the structural level, barriers such as transportation difficulties [27,30], lack of RH education during clinical encounters [29,32], limited access to female providers [32], poor continuity of care [27,48], challenges navigating health systems [26,27,30,40], and financial constraints [27,30,34,35,36,38] were frequently reported.
The degree of influence of RH knowledge appears to vary across RH domains. Studies focusing on cervical cancer and screening behaviors were more likely to identify knowledge as a primary factor of service utilization and behavior, possibly due to the presence of structured screening programs and less ingrained social norms, compared to domains like family planning or HIV. This suggests the need for more nuanced, domain-specific research to better understand the how RH knowledge influences RH behavior and outcomes. This is particularly important given that current interventions for resettled refugee women often prioritize knowledge improvement as the primary measurement of success, rather than tangible health outcomes [57]. Future studies should quantitatively assess how RH knowledge influences decision-making and behavior within each RH domain with the objective of creating a model that functions in the context of refugee and migrant communities. Interventions focused on culturally sensitive topics such as family planning, HIV, and maternal health should use a culture-centered framework; consider non-education/awareness-based strategies; and, where appropriate, integrate traditional practices to increase acceptability and effectiveness [37].
4.3. Promoting RHL and Knowledge
Our findings support a high frequency of inadequate RH knowledge and literacy among refugee populations, though as expected, this is not consistent across all RH domains or populations. This aligns with a broader body of research that documents persistent gaps in RHL and knowledge in LMICs and humanitarian settings [58,59,60]. We found two exceptions in our review. Agbemenu et al. [33] found adequate knowledge regarding birth control options among a Somali Bantu refugee community in Buffalo, New York, and [34] observed relatively high levels of knowledge and awareness concerning birth spacing methods among Congolese women in a metropolitan area in the western U.S. Notably, both studies focused specifically on contraception, and both concluded that adequate knowledge did not necessarily translate into behavioral change.
All other studies in our review reported low levels of knowledge or misinformation, particularly in relation to HIV, cervical cancer, and maternal health. The comparatively higher levels of contraception knowledge may reflect the longstanding prioritization of family planning in global RH funding, which has often framed contraception as a tool for economic development and health equity in low-or middle-income countries (LMICs) [61,62]. Family planning also remains a central focus of RH interventions in humanitarian settings [59,63]. Future research should examine how global RH education initiatives are distributed across RH domains—both within and beyond humanitarian contexts—and how that distribution affects knowledge and behavior following resettlement. Programs pursuing global reproductive justice should expand their educational scope beyond contraception to address broader RH concerns within resettled refugee communities.
Several studies in this review identified actionable opportunities to promote RH knowledge directly within refugee populations. Some participants demonstrated a strong desire for more RH information and took initiative to seek it out, often through internet sources [41,42,43,48]. Participants also cited web-based multimedia (including videos and digital reading materials) as helpful resources. Peer educators, particularly those who share the same cultural and religious backgrounds, and group care models for pre- and postnatal care were also reported as acceptable and effective strategies for increasing RH knowledge [31,49]. While promising, these strategies require further evaluation, especially in resettled refugee contexts. Additionally, expanding RH education to include digital health tools such as mHealth and mobile learning could be impactful, as both have demonstrated effectiveness in delivering health education to refugee populations in other domains [64,65].
HCPs were consistently identified as trusted sources of RH information—sometimes preferred even over family or community leaders [29,41,43]. This positions HCPs as key actors in reducing RH knowledge gaps and promoting RHL. Strategies to support this role include: conducting comprehensive patient histories to uncover migration- and trauma-related experiences; adopting a culture-centered approach to education; promoting shared goals in patient-provider relationships; integrating education into routine care; and improving cultural competence through provider training. Additionally, HCPs may benefit from using whole-family approaches to education and decision-making when appropriate. Structural interventions can also enhance RH knowledge acquisition—such as diversifying the healthcare workforce and ensuring financial coverage for professional medical interpreters, who play a crucial role in patient comprehension and communication [29,41,48].
4.4. Limitations
This review is subject to several limitations that affect the generalizability and interpretability of its findings. First, the lack of uniformity in how RHL and knowledge are measured across studies presents a challenge for this review. The absence of a validated, standardized RHL measurement tool limits the comparability of study results and hinders our ability to draw strong conclusions about the relationship between RHL, RH knowledge, and health behaviors across different populations and contexts. The diverse and inconsistent methods used to assess knowledge and literacy—ranging from study-specific survey instruments to qualitative interviews—make it difficult to evaluate the strength of associations or aggregate findings across studies.
Second, generalizability is also affected by the wide heterogeneity of refugee populations included in the reviewed studies. Differences in cultural background, language, migration experiences, and host country health systems reduce the extent to which findings can be applied to refugee populations more broadly. While this diversity provides important insight into the varying contexts of RH decision-making, it also complicates synthesis and limits the ability to give focused recommendations. Additionally, because our search was limited to studies that explicitly identified participants as refugees or migrants, relevant studies that assessed RH literacy or knowledge among refugee populations but categorized them more broadly under general immigrant groups were excluded [66]. However, given the unique experiences of migration and resettlement that often differ significantly from the experience of non-refugee populations, narrowing the scope of our review may strengthen the relevance and specificity of our findings to the refugee experience.
Third, this review may be influenced by publication bias. Only peer-reviewed literature was included; therefore, relevant findings from gray literature, unpublished reports, or community-level evaluations may have been omitted. Although comprehensive search strategies were used—including multiple database queries and reference mining—some eligible studies may still have been missed. Furthermore, the review was limited to studies published in English, which may have excluded relevant research conducted in non-English-speaking countries, particularly those hosting large refugee populations.
Finally, as a scoping review focused on thematic synthesis, this review does not include a formal quality appraisal of included studies. While this approach allows for the mapping of broad themes and gaps in the literature, it limits the ability to comment on the rigor or methodological quality of the individual studies reviewed.
5. Conclusions
This review aimed to provide a comprehensive overview of our current ability to measure the RHL and knowledge of refugee women in high-income countries, and to identify gaps in understanding the relationship between RHL, knowledge, behavior, decision-making, and outcomes. Our findings reveal that the current literature is limited in its use of validated, standardized tools to measure RHL, with most studies focusing instead on RH knowledge, mostly using inconsistent and study-specific instruments. While RH knowledge is an important component of RHL, our analysis suggests that independently, it is an insufficient predictor of RH behaviors or outcomes, particularly in populations facing complex sociocultural, interpersonal, and structural barriers.
To strengthen future research and improve RH outcomes, there is a critical need for validated, culturally relevant tools that measure RHL across multiple RH domains. Such tools would support providers and policymakers in assessing needs, tailoring interventions, and evaluating impact. Future interventions should not only address knowledge gaps but also focus on facilitating communication, foster trust in healthcare systems, and improve access to culturally and linguistically appropriate resources. Addressing the broader determinants of RH behavior in refugee populations will require integrated, equity-focused strategies that go beyond addressing RH knowledge through traditional health education models.
Author Contributions
Conceptualization, K.T. and Z.G.; methodology, Z.G.; software, K.T.; validation, K.T. and Z.G.; formal analysis, K.T.; resources, Z.G.; investigation, A.A., A.C., A.K., H.M., N.S., K.T.; data curation, K.T.; writing—original draft preparation, A.A., A.C., A.K., H.M., N.S., K.T., and Z.G.; writing—review and editing, K.T. and Z.G.; visualization, K.T.; supervision, Z.G.; project administration, K.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HCP | Health care provider |
| LMIC | low-or middle-income country |
| RH | Reproductive health |
| RHL | Reproductive health literacy |
| SRH | Sexual and reproductive health |
Appendix A
Appendix A.1

Table A1.
PRISMA-ScR checklist.
| Section | Item | PRISMA-ScR Checklist Item | Reported on page # |
|---|---|---|---|
| Title | 1 | Identify the report as a scoping review. | 1 |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1 |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 1-3 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 3 |
| Methods | 3 | ||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | 3 |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 3 |
| Information sources* | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 3 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | 3-4 |
| Selection of sources of evidence† | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 4 |
| Data charting process‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 4 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 5, Table 1, Table 2 |
| Critical appraisal of individual sources of evidence§ | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | NA |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 4 |
| Results | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 8 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | Table 1, Table 2 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | NA |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | Table 1, Table 2 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 9-12 |
| Discussion | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 12-15 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 15 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 15-16 |
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 18 |
JBI = Joanna Briggs Institute; PRISMA-ScR = Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. * Where sources of evidence (see second footnote) are compiled from, such as bibliographic databases, social media platforms, and Web sites. † A more inclusive/heterogeneous term used to account for the different types of evidence or data sources (e.g., quantitative and/or qualitative research, expert opinion, and policy documents) that may be eligible in a scoping review as opposed to only studies. This is not to be confused with information sources (see first footnote). ‡ The frameworks by Arksey and O’Malley (6) and Levac and colleagues (7) and the JBI guidance (4, 5) refer to the process of data extraction in a scoping review as data charting. § The process of systematically examining research evidence to assess its validity, results, and relevance before using it to inform a decision. This term is used for items 12 and 19 instead of “risk of bias” (which is more applicable to systematic reviews of interventions) to include and acknowledge the various sources of evidence that may be used in a scoping review (e.g., quantitative and/or qualitative research, expert opinion, and policy document).
References
- Sørensen, K.; Van Den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium Health Literacy Project European. Health Literacy and Public Health: A Systematic Review and Integration of Definitions and Models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N. D.; Sheridan, S. L.; Donahue, K. E.; Halpern, D. J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann Intern Med 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Corneliess, C.; Gray, K.; Kidwell Drake, J.; Namagembe, A.; Stout, A.; Cover, J. Education as an Enabler, Not a Requirement: Ensuring Access to Self-Care Options for All. Sexual and Reproductive Health Matters 2022, 29, 2040776. [Google Scholar] [CrossRef] [PubMed]
- Ghavami, B.; Sohrabi, Z.; RaisiDehkordi, Z.; Mohammadi, F. Relationship between Reproductive Health Literacy and Components of Healthy Fertility in Women of the Reproductive Age. Journal of Education and Health Promotion 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Dongarwar, D.; Salihu, H. M. Influence of Sexual and Reproductive Health Literacy on Single and Recurrent Adolescent Pregnancy in Latin America. Journal of Pediatric and Adolescent Gynecology 2019, 32, 506–513. [Google Scholar] [CrossRef]
- Bahrampour, B.; Shahali, S.; Lamyian, M.; Rasekhi, A. Sexual Health Literacy among Rural Women in Southern Iran. Sci Rep 2024, 14, 17377. [Google Scholar] [CrossRef]
- Von Wagner, C.; Steptoe, A.; Wolf, M. S.; Wardle, J. Health Literacy and Health Actions: A Review and a Framework From Health Psychology. Health Educ Behav 2009, 36, 860–877. [Google Scholar] [CrossRef]
- Freedman, D. A.; Bess, K. D.; Tucker, H. A.; Boyd, D. L.; Tuchman, A. M.; Wallston, K. A. Public Health Literacy Defined. American Journal of Preventive Medicine 2009, 36, 446–451. [Google Scholar] [CrossRef]
- Alomair, N.; Alageel, S.; Davies, N.; Bailey, J. V. Factors Influencing Sexual and Reproductive Health of Muslim Women: A Systematic Review. Reprod Health 2020, 17, 33. [Google Scholar] [CrossRef]
- Hall, K. S.; Castaño, P. M.; Westhoff, C. L. The Influence of Oral Contraceptive Knowledge on Oral Contraceptive Continuation Among Young Women. Journal of Women’s Health 2014, 23, 596–601. [Google Scholar] [CrossRef]
- Kilfoyle, K. A.; Vitko, M.; O’Conor, R.; Bailey, S. C. Health Literacy and Women’s Reproductive Health: A Systematic Review. Journal of Women’s Health 2016, 25, 1237–1255. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, D.; Aronson, B. D.; Kading, M.; Morisky, D. Relationship between Self-Efficacy and Patient Knowledge on Adherence to Oral Contraceptives Using the Morisky Medication Adherence Scale (MMAS-8). Reprod Health 2017, 14, 110. [Google Scholar] [CrossRef] [PubMed]
- Morris, M. D.; Popper, S. T.; Rodwell, T. C.; Brodine, S. K.; Brouwer, K. C. Healthcare Barriers of Refugees Post-Resettlement. J Community Health 2009, 34, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Barnes, D. M.; Harrison, C. L. Refugee Women’s Reproductive Health in Early Resettlement. Journal of Obstetric, Gynecologic & Neonatal Nursing 2004, 33, 723–728. [Google Scholar] [CrossRef]
- Gibson-Helm, M. E.; Teede, H. J.; Cheng, I.; Block, A. A.; Knight, M.; East, C. E.; Wallace, E. M.; Boyle, J. A. Maternal Health and Pregnancy Outcomes Comparing Migrant Women Born in Humanitarian and Nonhumanitarian Source Countries: A Retrospective, Observational Study. Birth 2015, 42, 116–124. [Google Scholar] [CrossRef]
- Sturrock, S.; Williams, E.; Greenough, A. Antenatal and Perinatal Outcomes of Refugees in High Income Countries. Journal of Perinatal Medicine 2021, 49, 80–93. [Google Scholar] [CrossRef]
- Global Trends: Forced Displacement in 2023; United Nations High Commissioner for Refugees, 2024. https://www.unhcr.org/global-trends-report-2023.
- Davidson, N.; Hammarberg, K.; Romero, L.; Fisher, J. Access to Preventive Sexual and Reproductive Health Care for Women from Refugee-like Backgrounds: A Systematic Review. BMC Public Health 2022, 22, 403. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. International Journal of Social Research Methodology 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O’Brien, K. K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M. D. J.; Horsley, T.; Weeks, L.; Hempel, S.; Akl, E. A.; Chang, C.; McGowan, J.; Stewart, L.; Hartling, L.; Aldcroft, A.; Wilson, M. G.; Garritty, C.; Lewin, S.; Godfrey, C. M.; Macdonald, M. T.; Langlois, E. V.; Soares-Weiser, K.; Moriarty, J.; Clifford, T.; Tunçalp, Ö.; Straus, S. E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M. D. J.; Marnie, C.; Tricco, A. C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C. M.; Khalil, H. Updated Methodological Guidance for the Conduct of Scoping Reviews. JBI Evidence Synthesis 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Rauf, M.; Goliaei, Z.; Machta, L.; Chang, J.; Thiel De Bocanegra, H. Reproductive Health Literacy Scale: A Tool to Measure the Effectiveness of Health Literacy Training. Reprod Health 2025, 22, 12. [Google Scholar] [CrossRef]
- Reproductive Health Indicators: Guidelines for Their Generation, Interpretation and Analysis for Global Monitoring; World Health Organization, 2006. https://iris.who.int/bitstream/handle/10665/43185/924156315X_eng.pdf.
- Anaman, J. A.; Correa-Velez, I.; King, J. A Survey of Cervical Screening among Refugee and Non-refugee African Immigrant Women in Brisbane, Australia. Health Prom J of Aust 2017, 28, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Anaman, J. A.; Correa-Velez, I.; King, J. Knowledge Adequacy on Cervical Cancer Among African Refugee and Non-Refugee Women in Brisbane, Australia. J Canc Educ 2018, 33, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Dalla, V.; Panagiotopoulou, E.-K.; Deltsidou, A.; Kalogeropoulou, M.; Kostagiolas, P.; Niakas, D.; Labiris, G. Level of Awareness Regarding Cervical Cancer Among Female Syrian Refugees in Greece. J Canc Educ 2022, 37, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Haworth, R. J.; Margalit, R.; Ross, C.; Nepal, T.; Soliman, A. S. Knowledge, Attitudes, and Practices for Cervical Cancer Screening Among the Bhutanese Refugee Community in Omaha, Nebraska. J Community Health 2014, 39, 872–878. [Google Scholar] [CrossRef]
- Ornelas, I. J.; Ho, K.; Jackson, J. C.; Moo-Young, J.; Le, A.; Do, H. H.; Lor, B.; Magarati, M.; Zhang, Y.; Taylor, V. M. Results From a Pilot Video Intervention to Increase Cervical Cancer Screening in Refugee Women. Health Educ Behav 2018, 45, 559–568. [Google Scholar] [CrossRef]
- Allen, E. M.; Lee, H. Y.; Pratt, R.; Vang, H.; Desai, J. R.; Dube, A.; Lightfoot, E. Facilitators and Barriers of Cervical Cancer Screening and Human Papilloma Virus Vaccination Among Somali Refugee Women in the United States: A Qualitative Analysis. J Transcult Nurs 2019, 30, 55–63. [Google Scholar] [CrossRef]
- Lor, B.; Ornelas, I. J.; Magarati, M.; Do, H. H.; Zhang, Y.; Jackson, J. C.; Taylor, V. M. We Should Know Ourselves: Burmese and Bhutanese Refugee Women’s Perspectives on Cervical Cancer Screening. Journal of Health Care for the Poor and Underserved 2018, 29, 881–897. [Google Scholar] [CrossRef]
- Metusela, C.; Ussher, J.; Perz, J.; Hawkey, A.; Morrow, M.; Narchal, R.; Estoesta, J.; Monteiro, M. “In My Culture, We Don’t Know Anything About That”: Sexual and Reproductive Health of Migrant and Refugee Women. Int.J. Behav. Med. 2017, 24, 836–845. [Google Scholar] [CrossRef]
- Anaman-Torgbor, J. A.; King, J.; Correa-Velez, I. Barriers and Facilitators of Cervical Cancer Screening Practices among African Immigrant Women Living in Brisbane, Australia. European Journal of Oncology Nursing 2017, 31, 22–29. [Google Scholar] [CrossRef]
- Agbemenu, K.; Volpe, E. M.; Dyer, E. Reproductive Health Decision-making among US -dwelling Somali Bantu Refugee Women: A Qualitative Study. Journal of Clinical Nursing 2018, 27, 3355–3362. [Google Scholar] [CrossRef] [PubMed]
- Royer, P. A.; Olson, L. M.; Jackson, B.; Weber, L. S.; Gawron, L.; Sanders, J. N.; Turok, D. K. Family Planning Knowledge, Attitudes, and Practices Among Somali and Congolese Refugee Women After Resettlement to the United States. Qual Health Res 2020, 30, 391–408. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; McCoy, E. E.; Scego, R.; Phillips, W.; Godfrey, E. A Qualitative Exploration of Somali Refugee Women’s Experiences with Family Planning in the U.S. J Immigrant Minority Health 2020, 22, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Gele, A. A.; Musse, F. K.; Shrestha, M.; Qureshi, S. Barriers and Facilitators to Contraceptive Use among Somali Immigrant Women in Oslo: A Qualitative Study. PLoS ONE 2020, 15, e0229916. [Google Scholar] [CrossRef]
- Kuru Alici, N.; Ogüncer, A. Knowledge, Beliefs, and Cultural Practices of Sexual and Reproductive Health Among Afghan Refugee Women in Türkiye. J Transcult Nurs 2024, 35, 30–40. [Google Scholar] [CrossRef]
- Ngum Chi Watts, M. C.; Liamputtong, P.; Carolan, M. Contraception Knowledge and Attitudes: Truths and Myths among African Australian Teenage Mothers in Greater Melbourne, Australia. Journal of Clinical Nursing, 2131. [Google Scholar] [CrossRef]
- Ngum Chi Watts, M. C.; McMichael, C.; Liamputtong, P. Factors Influencing Contraception Awareness and Use: The Experiences of Young African Australian Mothers. Journal of Refugee Studies 2015, 28, 368–387. [Google Scholar] [CrossRef]
- Dhar, C. P.; Kaflay, D.; Dowshen, N.; Miller, V. A.; Ginsburg, K. R.; Barg, F. K.; Yun, K. Attitudes and Beliefs Pertaining to Sexual and Reproductive Health Among Unmarried, Female Bhutanese Refugee Youth in Philadelphia. Journal of Adolescent Health 2017, 61, 791–794. [Google Scholar] [CrossRef]
- Kaneoka, M.; Spence, W. The Cultural Context of Sexual and Reproductive Health Support: An Exploration of Sexual and Reproductive Health Literacy among Female Asylum Seekers and Refugees in Glasgow. IJMHSC 2019, 16, 46–64. [Google Scholar] [CrossRef]
- Napier-Raman, S.; Hossain, S. Z.; Mpofu, E.; Lee, M.-J.; Liamputtong, P.; Dune, T. Sexual and Reproductive Health and Rights Decision-Making among Australian Migrant and Refugee Youth: A Group Concept Mapping Study. Culture, Health & Sexuality 2024, 26, 979–996. [Google Scholar] [CrossRef]
- Dean, J.; Mitchell, M.; Stewart, D.; Debattista, J. Sexual Health Knowledge and Behaviour of Young Sudanese Queenslanders: A Cross-Sectional Study. Sex. Health 2017, 14, 254. [Google Scholar] [CrossRef]
- Napier-Raman, S.; Bidewell, J.; Hossain, S. Z.; Mpofu, E.; Lee, M.-J.; Liamputtong, P.; Dune, T. Migrant and Refugee Youth’s Sexual and Reproductive Health and Rights: A Gender Comparison of Knowledge, Behaviour, and Experiences. Sexuality & Culture 2025, 29, 734–760. [Google Scholar] [CrossRef]
- Inci, M. G.; Kutschke, N.; Nasser, S.; Alavi, S.; Abels, I.; Kurmeyer, C.; Sehouli, J. Unmet Family Planning Needs among Female Refugees and Asylum Seekers in Germany – Is Free Access to Family Planning Services Enough? Results of a Cross-Sectional Study. Reprod Health 2020, 17, 115. [Google Scholar] [CrossRef] [PubMed]
- Feresu, S.; Smith, L. Knowledge, Attitudes, and Beliefs about HIV/AIDS of Sudanese and Bantu Somali Immigrant Women Living in Omaha, Nebraska. OJPM 2013, 03, 84–98. [Google Scholar] [CrossRef]
- Agbemenu, K.; Aidoo-Frimpong, G.; Auerbach, S.; Jafri, A. HIV Attitudes and Beliefs in U.S.-Based African Refugee Women. Ethnicity & Health 2022, 27, 499–508. [Google Scholar] [CrossRef]
- Henry, J.; Beruf, C.; Fischer, T. Access to Health Care for Pregnant Arabic-Speaking Refugee Women and Mothers in Germany. Qual Health Res 2020, 30, 437–447. [Google Scholar] [CrossRef]
- Madeira, A. D.; Rangen, C. M.; Avery, M. D. Design and Implementation of a Group Prenatal Care Model for Somali Women at a Low-Resource Health Clinic. Nursing for Women’s Health 2019, 23, 224–233. [Google Scholar] [CrossRef]
- Napier-Raman, S.; Hossain, S. Z.; Mpofu, E.; Lee, M.-J.; Liamputtong, P.; Dune, T. Sexual and Reproductive Health and Rights Decision-Making among Australian Migrant and Refugee Youth: A Group Concept Mapping Study. Culture, Health & Sexuality 2024, 26, 979–996. [Google Scholar] [CrossRef]
- Alhussaini, N. W. Z.; Elshaikh, U.; Abdulrashid, K.; Elashie, S.; Hamad, N. A.; Al-Jayyousi, G. F. Sexual and Reproductive Health Literacy of Higher Education Students: A Scoping Review of Determinants, Screening Tools, and Effective Interventions. Global Health Action 2025, 18, 2480417. [Google Scholar] [CrossRef]
- Ma, X.; Yang, Y.; Wei, Q.; Jiang, H.; Shi, H. Development and Validation of the Reproductive Health Literacy Questionnaire for Chinese Unmarried Youth. Reprod Health 2021, 18, 226. [Google Scholar] [CrossRef]
- Maasoumi, R.; Tavousi, M.; Zarei, F. Development and Psychometric Properties of Sexual Health Literacy for Adults (SHELA) Questionnaire. Hayat, Journal of School of Nursing and Midwifery 25, 56–59.
- Panahi, R.; Dehghankar, L.; Amjadian, M. Investigating the Structural Validity and Reliability of the Sexual Health Literacy for Adults (SHELA) Questionnaire among a Sample of Women in Qazvin, Iran. BMC Women’s Health 2022, 22, 524. [Google Scholar] [CrossRef]
- Rashidi, K.; Watson, P.; Farahani, H.; Chesli, R. R.; Abiri, F. A. Developing and Validating the Sexual Health Literacy Scale in an Iranian Adult Sample. Humanit Soc Sci Commun 2023, 10, 180. [Google Scholar] [CrossRef] [PubMed]
- Vongxay, V.; Thongmixay, S.; Stoltenborg, L.; Inthapanyo, A.; Sychareun, V.; Chaleunvong, K.; Rombout Essink, D. Validation of the Questionnaire on Sexual and Reproductive Health Literacy for Adolescents Age 15 to 19 Years in Lao People’s Democratic Republic. HLRP: Health Literacy Research and Practice. [CrossRef]
- Bitterfeld, L.; Ozkaynak, M.; Denton, A. H.; Normeshie, C. A.; Valdez, R. S.; Sharif, N.; Caldwell, P. A.; Hauck, F. R. Interventions to Improve Health Among Refugees in the United States: A Systematic Review. J Community Health 2025, 50, 130–151. [Google Scholar] [CrossRef] [PubMed]
- Amanu, A.; Birhanu, Z.; Godesso, A. Sexual and Reproductive Health Literacy among Young People in Sub-Saharan Africa: Evidence Synthesis and Implications. Global Health Action 2023, 16, 2279841. [Google Scholar] [CrossRef] [PubMed]
- Desrosiers, A.; Betancourt, T.; Kergoat, Y.; Servilli, C.; Say, L.; Kobeissi, L. A Systematic Review of Sexual and Reproductive Health Interventions for Young People in Humanitarian and Lower-and-Middle-Income Country Settings. BMC Public Health 2020, 20, 666. [Google Scholar] [CrossRef]
- Soeiro, R. E.; De Siqueira Guida, J. P.; da-Costa-Santos, J.; Costa, M. L. Sexual and Reproductive Health (SRH) Needs for Forcibly Displaced Adolescent Girls and Young Women (10–24 Years Old) in Humanitarian Settings: A Mixed-Methods Systematic Review. Reprod Health 2023, 20, 174. [Google Scholar] [CrossRef]
- Nandagiri, R. What’s so Troubling about ‘Voluntary’ Family Planning Anyway? A Feminist Perspective. Population Studies 2021, 75, 221–234. [Google Scholar] [CrossRef]
- Senderowicz, L.; Valley, T. Fertility Has Been Framed: Why Family Planning Is Not a Silver Bullet for Sustainable Development. St Comp Int Dev 2023. [CrossRef]
- Jennings, L.; George, A. S.; Jacobs, T.; Blanchet, K.; Singh, N. S. A Forgotten Group during Humanitarian Crises: A Systematic Review of Sexual and Reproductive Health Interventions for Young People Including Adolescents in Humanitarian Settings. Confl Health 2019, 13, 57. [Google Scholar] [CrossRef]
- El-Haj-Mohamad, R.; Nohr, L.; Niemeyer, H.; Böttche, M.; Knaevelsrud, C. Smartphone-Delivered Mental Health Care Interventions for Refugees: A Systematic Review of the Literature. Camb. prisms Glob. ment. health 2023, 10, e6. [Google Scholar] [CrossRef]
- Meyer, C. L.; Surmeli, A.; Hoeflin Hana, C.; Narla, N. P. Perceptions on a Mobile Health Intervention to Improve Maternal Child Health for Syrian Refugees in Turkey: Opportunities and Challenges for End-User Acceptability. Front. Public Health 2022, 10, 1025675. [Google Scholar] [CrossRef]
- Vazquez Corona, M.; Hazfiarini, A.; Vaughan, C.; Block, K.; Bohren, M. A. Participatory Health Research With Women From Refugee, Asylum-Seeker, and Migrant Backgrounds Living in High-Income Countries: A Scoping Review. International Journal of Qualitative Methods 2024, 23, 16094069231225371. [Google Scholar] [CrossRef]
Figure 1.
Sørensen’s Integrated Model of Health Literacy. Reproduced from Sørensen et al. (2012), BMC Public Health, 12(1), 80. Licensed under CC BY 2.0.
Figure 1.
Sørensen’s Integrated Model of Health Literacy. Reproduced from Sørensen et al. (2012), BMC Public Health, 12(1), 80. Licensed under CC BY 2.0.
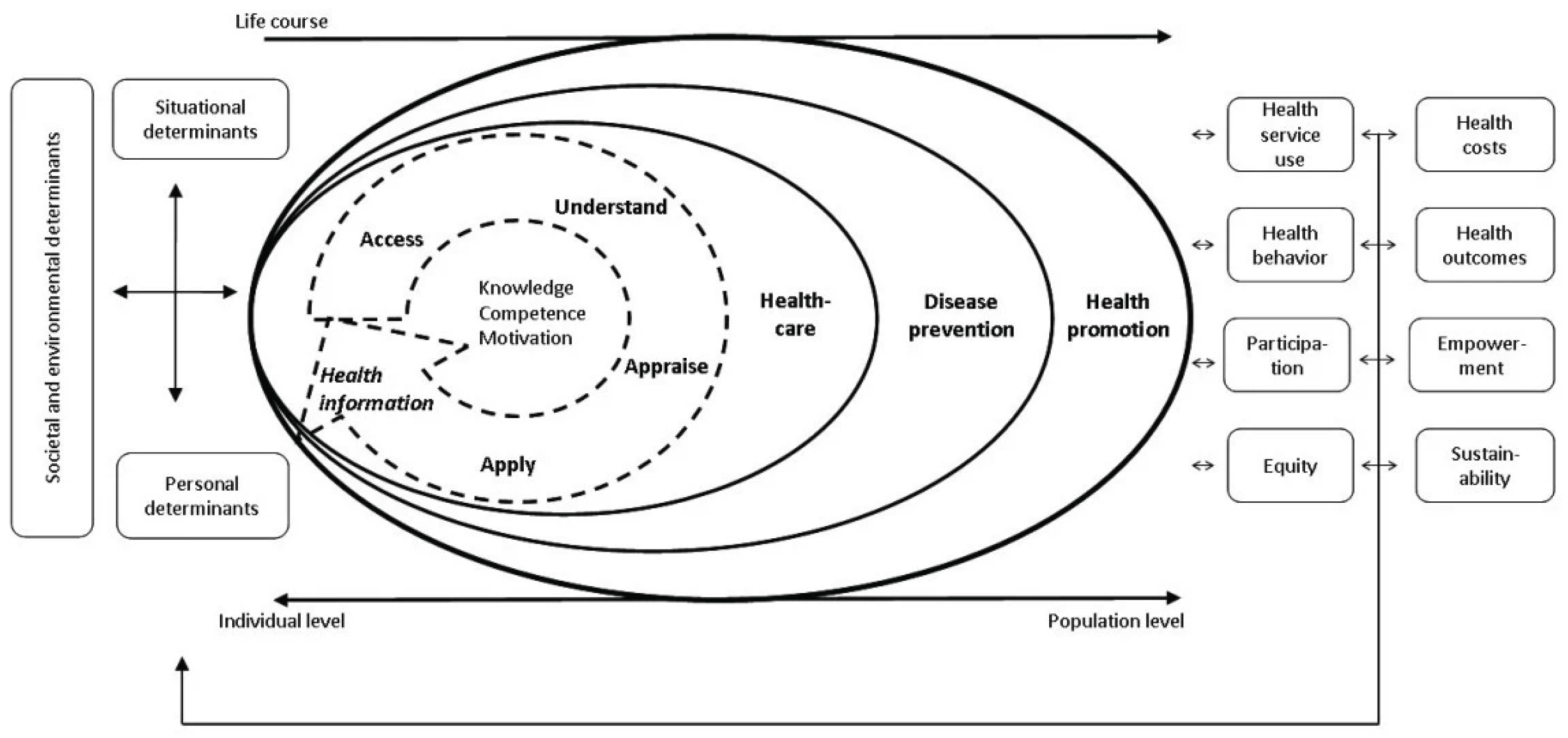
Figure 2.
PRISMA Flow Diagram.
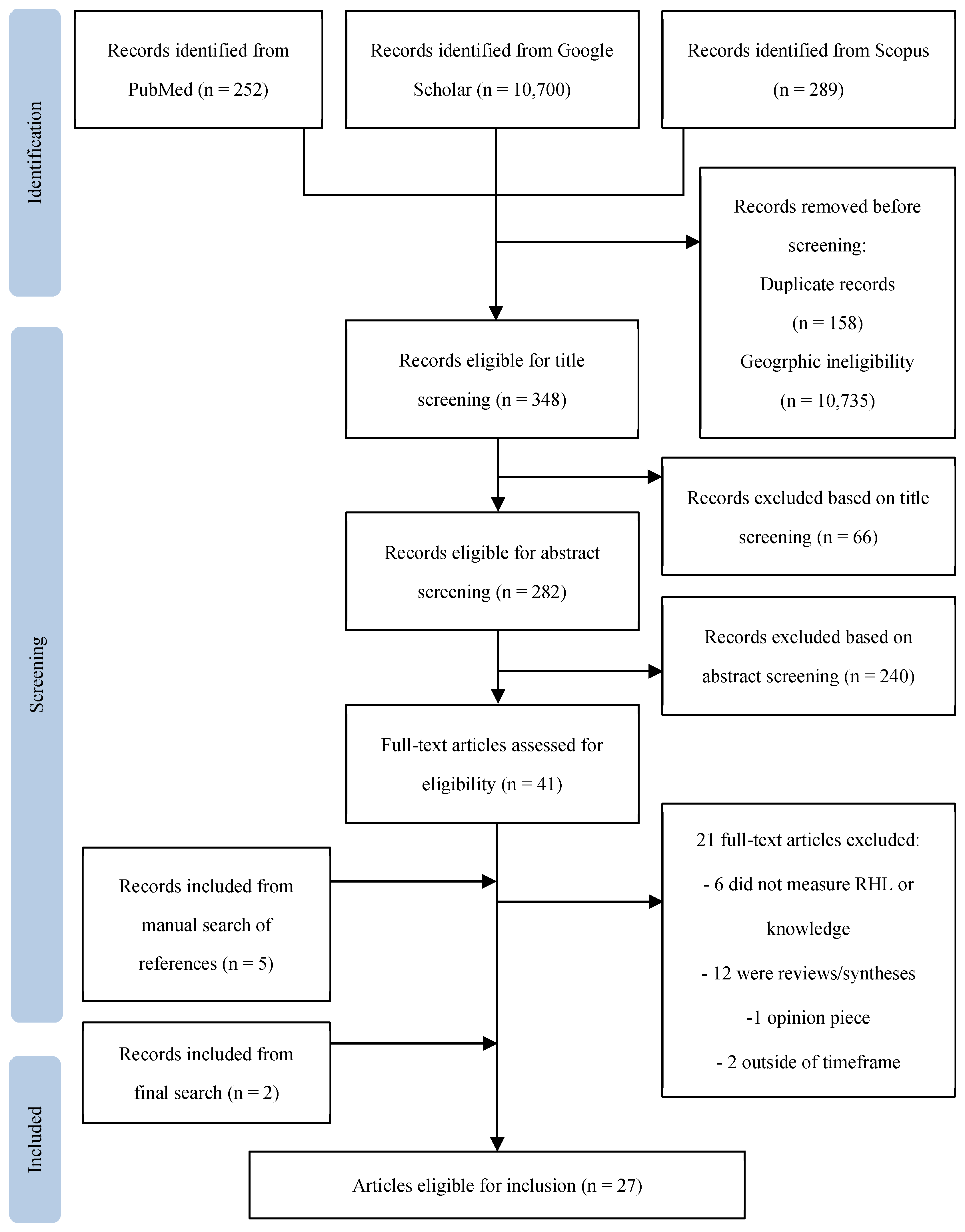
Table 1.
Characteristics of studies included in the review.
| N | Author | Year | Country | Population (n) | Design | Findings |
|---|---|---|---|---|---|---|
| 1 | Agbemenu et al. | 2018 | U.S.A. | Somali Bantu refugee women (30) | Qualitative | Accurate and high levels of knowledge on birth control options did not increase contraceptive uptake. |
| 2 | Agbemenu et al. | 2022 | U.S.A. | African refugee women (101) | Quantitative | Study population had overall low levels of knowledge. Accurate knowledge did not override stigma. |
| 3 | Allen et al. | 2018 | U.S.A. | Somali Bantu refugee women with >1 child (31) | Qualitative | Low knowledge about HPV was associated with low HPV vaccination rates. |
| 4 | Anaman et al. | 2017 | Australia | African refugee (144) and non-refugee (110) women | Quantitative | Low health literacy and low levels of knowledge regarding cervical cancer and screening were associated with low Pap smear uptake. |
| 5 | Anaman et al. | 2018 | Australia | African refugee (144) and non-refugee (110) women | Quantitative | Refugees in the study population had significantly lower levels of knowledge about cervical cancer and Pap smear screening. |
| 6 | Anaman-Torgbor et al. | 2017 | Australia | African refugee (10) and non-refugee (9) women | Qualitative | Low knowledge was identified as a barrier to cervical cancer screening participation. |
| 7 | Dalla et al. | 2022 | Greece | Syrian refugee women (176) | Quantitative | Study population had extreme low levels of knowledge regarding cervical cancer, screening methods, and HPV vaccination, assessed using Cervical CAM. |
| 8 | Dean et al. | 2017 | Australia | Sudanese refugee-background youth, age 16-24 (80 female and 149 male) | Quantitative | Low levels of STI and HIV knowledge were associated with higher sexual risk behavior. Knowledge was measured using NSASSSH. |
| 9 | Dhar et al. | 2017 | U.S.A. | Bhutanese refugee female youth (14) | Qualitative | Study population had low levels of knowledge across RH domains |
| 10 | Feresu et al. | 2013 | U.S.A. | Sudanese (86) and Somali Bantu (14) immigrant women from predominantly refugee community | Mixed methods | Knowledge on different aspects of HIV (transmission, protection, testing, etc.) was generally low and associated with low rate of condom usage. |
| 11 | Gele et al. | 2020 | Norway | Somali immigrant women (21) | Qualitative | Low levels of knowledge regarding contraceptives was associated with non-usage. |
| 12 | Haworth et al. | 2014 | U.S.A. | Bhutanese refugee women (69) | Mixed methods | Limited knowledge was identified as a barrier to Pap test utilization. History of Pap smear was associated with increased knowledge. |
| 13 | Henry et al. | 2020 | Germany | Iraqi, Syrian, and Palestinian refugee women (12) | Qualitative | Low health literacy and knowledge regarding maternal care was associated with delays in seeking care. |
| 14 | Inci et al. | 2020 | Germany | Refugee women from various countries (307) | Quantitative | History of sexual education was associated with contraceptive usage, but not associated with preference for more effective contraceptive methods. |
| 15 | Kaneoka et al. | 2020 | Scotland | Asylum seeking and refugee women from various countries (14) | Qualitative | RH literacy was in the study population was low, which was identified as a barrier to RH decision-making. |
| 16 | Kuru Alici and Ogüncer | 2024 | Turkey | Afghan refugee women (20) | Qualitative | Low and inaccurate knowledge was not associated with nonuse of contraceptives. |
| 17 | Lor et al. | 2018 | U.S.A. | Burmese (31) and Bhutanese (27) refugee women | Qualitative | Low cervical cancer knowledge was associated with low rates of screening. Health information was identified as a facilitator of health behavior and independent health decision-making |
| 18 | Madeira et al. | 2019 | U.S.A. | Somali women from a predominantly refugee community (21) | Mixed methods | Participation in group prenatal care was associated with increased knowledge. Increased knowledge was associated with increased engagement in prenatal care. |
| 19 | Metusela et al. | 2017 | Australia, Canada | Migrant and refugee women from Afghanistan (35), Iraq (27), Somalia (38), South Sudan (11), Sudan (20), India (9), Sri Lanka (12), and South America (17) | Qualitative | Study population had inadequate knowledge across multiple RH domains. Inaccurate knowledge was a barrier to RH behavior. |
| 20 | Napier-Raman et al. | 2023 | Australia | Migrant and refugee youth, age 16-26 (42 female and 13 male) from various countries (68) | Mixed methods | Study participants had lack of RH knowledge and education. Relational factors were more influential in the decision-making process than knowledge. |
| 21 | Napier-Raman et al. | 2025 | Australia | Migrant and refugee youth, age 16-26 (74 female and 32 male) from various countries (107) | Quantitative | Females had greater knowledge and awareness of contraceptive than males, but misconceptions persisted in both genders. Contraceptive utilization was not different between genders. Women had higher rates of sexual coercion, STIs, and unplanned pregnancy. |
| 22 | Ngum Chi Watts et al. | 2014 | Australia | Refugee teenagers and women from Sudan (10), Liberia (3), Ethiopia (1), Burundi (1), and Sierra Leone (1) with h/o teenage pregnancy (16) | Qualitative | Low knowledge surrounding contraceptives was identified as a deterrent to contraceptive uptake. |
| 23 | Ngum Chi Watts et al. | 2015 | Australia | Refugee teenagers and women from Sudan (10), Liberia (3), Ethiopia (1), Burundi (1), and Sierra Leone (1) with h/o teenage pregnancy (16) | Qualitative | Low and inaccurate knowledge was associated with nonuse of contraceptives. |
| 24 | Ornelas et al. | 2017 | U.S.A. | Karen-Burmese (20) and Nepali-Bhutanese (20) refugee women | Quantitative | Increased knowledge after watching cervical cancer educational videos was not consistently associated with increased intention to pursue Pap screening. |
| 25 | Rauf et al. | 2025 | U.S.A. | Afghan refugees (184), specifically Dari (67), Arabic (53), and Pashto (64) speakers | Quantitative | Reproductive health literacy scale made of HLS-EU-Q6, eHEALS, C-CLAT, and SHELA showed good inter-item reliability for this population |
| 26 | Royer et al. | 2019 | U.S.A. | Somali (41) and Congolese (25) refugee women | Qualitative | High levels of knowledge regarding available methods of contraception was not associated with contraceptive usage. |
| 27 | Zhang et al. | 2020 | U.S.A. | Somali refugee women of reproductive age (53) | Qualitative | Inaccurate knowledge was a barrier to contraceptive uptake. |
Table 2.
Indicators of knowledge/literacy of RH domains. Specific tools listed if used.
| Agbemenu et al., 2018 | Agbemenu et al., 2022 | Allen et al., 2018 | Anaman et al., 2017 | Anaman et al., 2018 | Anaman-Torgbor et al., 2017 | Dalla et al., 2022 | Dean et al., 2017 | Dhar et al., 2017 | Feresu et al., 2013 | Gele et al., 2020 | Haworth et al., 2014 | Henry et al., 2020 | Inci et al., 2020 | Kaneoka et al., 2020 | Kuru Alici & Ogüncer, 2024 | Lor et al., 2018 | Madeira et al., 2019 | Metusela et al., 2017 | Napier-Raman et al., 2023 | Napier-Raman et al., 2025 | Ngum Chi Watts et al., 2014 | Ngum Chi Watts et al., 2015 | Ornelas et al., 2017 | Rauf et al., 2025 | Royer et al., 2019 | Zhang et al., 2020 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Domain | Abortion | |||||||||||||||||||||||||||
| Cervical Cancer | X | X | X | X | CAM | X | X | X | X | ReproNet** | ||||||||||||||||||
| Family Planning | X | NSASSSH | X | X | X | X | X | X | X | NSASSSH | X | X | ReproNet** | X | ||||||||||||||
| Gender-Based Violence | X | |||||||||||||||||||||||||||
| HIV | X | X | WHO* | |||||||||||||||||||||||||
| Maternal Health and Obstetric Care | X | X | ReproNet** | |||||||||||||||||||||||||
| Menstruation and Gynecological Health | X | |||||||||||||||||||||||||||
| STIs | X | X | X | X | X |
* Tool not specified. ** ReproNet RHL scale: adaptation of HLS-EU-Q6 (general health literacy), eHEALS (digital literacy), RHL (C-CLAT), and ReproNet postpartum literacy scale.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



