
Submitted:
27 May 2025
Posted:
28 May 2025
You are already at the latest version
Abstract
Extreme climate/weather events (ECEs) are a potential source of toxic stress for children when faced with displacement, family separation, poverty, violence, and neglect. Children exposed to displacement, neglect or violence due to ECEs may experience what we term ‘Environmentally driven Adverse Childhood Experiences (E-ACEs)’. Although direct evidence on the neurobiological effects of E-ACEs is limited, evidence on traumatic and adverse childhood experiences (TRACEs) has shown an impact on brain and neural development, impairing cognitive and emotional growth, altering the hypothalamic-pituitary-adrenal (HPA) axis, and leading to long-term stress dysregulation and mental disorders. With the rising number of climate refugees, particularly in low- and middle-income countries (LMICs), ECEs pose an urgent humanitarian challenge in the 21st century, necessitating climate policies that strengthen community resilience and expand mental health services in disaster-prone regions. This perspective explores what E-ACEs are and their health consequences. We argue that ECEs should be recognized as adverse childhood experiences (ACEs) and emphasize that resilience-building strategies could play a role in preventing and mitigating their mental health impacts on children and families.
Keywords:
adverse childhood experiences
; climate change
; extreme weather events
; mental disorders
Main
Between 1990-2023, an average of 364 extreme weather events occurred annually, affecting 400 million people and displacing 26 million globally. [1,2] In 2021, eight of the ten most climate-affected countries globally were low- and middle-income countries (LMICs), including Myanmar, Haiti, the Philippines, Mozambique, Bangladesh, Pakistan, Thailand, and Nepal. [3] Due to ECEs, including storms, cyclones, floods, droughts, heatwaves, and wildfires, many children in these countries face the loss of shelter, disrupted living conditions, family separation, and interruptions to their education every year. [4] These countries often lack the resources to adequately respond to the growing impacts of climate change. [3,5]
We use the term 'extreme climate/weather events (ECEs)' to encompass both extreme weather and climate events, as defined in the glossary (AR5-WG1) of the Intergovernmental Panel on Climate Change (IPCC), including rare, acute weather events (e.g., severe storms, floods, heatwaves) and prolonged climate events (e.g., droughts or heavy seasonal rainfall) that result in extreme averages or cumulative impacts over time. [20] ECEs, exacerbated by climate change, not only cause immediate physical harm but also leave lasting emotional and psychological scars, affecting their development and future health and well-being. The health consequences for affected children include increased risks of infectious diseases, and malnutrition, along with mental health challenges, including post-traumatic stress disorder (PTSD), depression, anxiety, and developmental delays (Table 1). [6,7,8,9,10,11,12,13,14,15,16] Past studies have also explored trauma following ECEs, and its effect on families and children. [6,7,8,9,10,11,12,13,14,15,16,17,18] Extreme weather or climate-related trauma can trigger neurobiological and emotional stress in childhood heightening the risk of mental health conditions such as anxiety, depression, and PTSD, and physical health problems such as cardiovascular diseases in adulthood. [19]
In children, the impacts of ECEs can be similar to the impact of a collection of eight to ten traumatic events in childhood before the age of 18 years, initially defined by Felitti et al. (1998) as adverse childhood experiences (ACEs). [21] These events included: physical, sexual, or emotional abuse; physical or psychological neglect; parental substance abuse or mental illness; parental incarceration; and parental divorce or domestic violence. [21] Approximately 16% of the global population has greater than four ACEs, while in some LMICs, this figure could be as high as 88%. [22] A huge body of evidence exists on detrimental effect of multiple ACEs on physical and mental health during childhood and later in life. [21,23,24] Since 1998, growing evidence on ACEs has led to an expansion of the traditional ACEs model, extending beyond family-centred trauma to include adversities originating from the broader community and socio-economic conditions that affect a child’s physical, mental, and social well-being, with impact that may persists across generations. [25,26]
Emerging evidence suggests that these expanded ACEs include discrimination [27], exposure to community violence [28], bullying [29], economic hardship [30], gun violence [31], war or civil unrest [32], and global health crisis such as COVID-19 [33]. Critiquing the limitations of the traditional ACEs model for excluding certain traumatic experiences, Weems et al. (2021) proposed the Traumatic and Adverse Childhood Experiences (TRACEs) framework to expand the concept of ACEs by incorporating trauma, risk, and protective factors. [34] Many secondary outcomes of ECEs (e.g., poverty, family separation, community violence), are already captured within the TRACEs framework, it still does not explicitly account for upstream environmental stressors that may initiate, intensify, or compound existing adversities. [34] We therefore propose 'environmentally driven ACEs' (E-ACEs) as a conceptual subclass within the TRACEs framework, reflecting the growing significance of extreme weather and climate-related adversities that exert both direct and cascading psychosocial impacts on children. [35] ECEs can be traumatic experiences that may contribute to neurobiological and psychosocial impacts, potentially exacerbating stress responses and increasing vulnerability to long-term health risks. [15,35] This perspective further explores these parallels between TRACEs and E-ACEs in subsequent sections, highlighting shared pathways and intervention strategies.
Framing climate and weather-related adversities within the established models such as ACEs or TRACEs allows us to highlight how environmental adversities, both directly and indirectly, serve as key drivers of childhood mental and physical health outcomes. [34,36] The emerging literature highlights the logical link between TRACEs and mental disorders [36], yet limited research specifically examines the seasonal and repeated ECEs exposure, and its longer-term and cross-generational impacts on children’s physical and mental health in vulnerable communities. [15,18,37,38] Given this, recognizing E-ACEs as a distinct yet interconnected component of the TRACEs framework allows for a more comprehensive understanding of childhood adversity and associated mental disorders in the context of climate change. [34] This approach further enables us to address specific environmental stressors or the compounding nature of climate-induced adversity as key determinants of childhood mental health and well-being.
This perspective discusses what E-ACEs are, their health consequences, and suggests that repeated ECEs should be considered as ACEs and highlights the potential role of resilience-building strategies in preventing and mitigating their impacts on vulnerable populations. We conducted a targeted free-text search in PubMed and Google Scholar to identify empirical evidence on the health impacts of exposure to weather and climate extremes and their association with childhood adversity, and resilience. We included research from diverse geographical regions to highlight the global impact of these stressors, and studies targeting both children as well as the general population to capture broader health impacts relevant to children, especially in contexts where child-specific data are limited (Table 1).
Conceptualising Environmentally Driven Adverse Childhood Experiences (E-ACEs)
E-ACEs refer to the extreme stress children may endure due to direct exposure to ECEs, as well as due to indirect effects, such as displacement, family separation, extreme poverty, or compounding adversities, such as violence and neglect. [35] These events can generate chronic stress responses in children that may have lasting neurobiological and psychosocial consequences. [40]
How does prolonged exposure to ECEs lead to psychological and other health issues in children, with effects persisting into later life? Although there is limited direct evidence on the neurobiological effects of ECEs specifically, extensive research on adversity and trauma demonstrates their direct profound impact on brain development, stress regulation, and immune function. [24,40,41] Given that ECEs may lead to traumatic exposures during childhood, such as displacement, loss of resources, and chronic stress, it is plausible that ECEs may contribute to similar biological alterations, including disrupted brain and neural development, dysregulated hypothalamic-pituitary-adrenal (HPA) axis activity and heightened inflammatory responses (Figure 1). [42,43,44]
Based on current evidence from related fields, we hypothesize that the neurobiological effects of ECEs may include disruptions to brain and neural development due to chronic climate-related stress responses, which can potentially affect brain structure and function, emotional regulation, hinder cognitive development, and the formation of healthy attachment relationships. [24,41] Such chronic stress may also lead to HPA axis dysregulation, leading to altered cortisol levels that result in either hyper-reactivity or hypo-reactivity to stressors, leading to mental disorders later in life. [41]
Another plausible pathway could be immune system dysregulation, persistently elevated inflammatory responses and increased production of pro-inflammatory cytokines, such as Interleukin-6 (IL-6) and Interleukin-2 (IL-2). [40] These cytokines can interfere with normal brain development by altering synaptic pruning, neurogenesis, and the functioning of key neurotransmitter systems, thereby increasing vulnerability to psychological disorders including depression, anxiety, and PTSD. [45] Moreover, chronic inflammation has been linked to the pathogenesis of various non-communicable diseases in adulthood, such as cardiovascular disease, cancer, diabetes mellitus, chronic kidney disease, non-alcoholic fatty liver disease, autoimmune disorders, and neurodegenerative conditions. [46,47,48,49]
While direct causal evidence is still limited, emerging studies suggest that ECEs, through displacement, loss of livelihoods, household instability, food insecurity, and deteriorating living conditions, may contribute to ACEs (Figure 1). [15,22,24,35,50]. Madigan et al. (2023) highlight that children experiencing poverty and deprivations, along with ACEs, face cumulative risks that can impair their development, leading to long-term consequences for mental and physical health. [22] Without adequate support, children facing climate-related stress either from direct threats or deprivations may develop maladaptive coping strategies, such as substance use, aggressive behaviors, or social withdrawal. [24] Additionally, prolonged toxic stress may induce epigenetic changes, such as DNA methylation or histone modifications, which can potentially be passed down to future generations. [46,51]
Despite a growing body of evidence on the impact of ECEs on child mental health, most existing research has focused on short-term exposure or isolated events. [17] However, more recent longitudinal studies from Australia [39] and the United States [15,35,52] have investigated the cumulative and long-term mental health consequences of repeated exposure to climate-related disasters among adolescents and adults. These studies have found that recurrent exposure to events such as floods, storms, and wildfires is associated with elevated risks of psychological distress, depression, anxiety, and post-traumatic stress symptoms, and that a dose–response and cumulative effect of ECEs on mental health outcomes is observed in both adolescent and adults. [15,35,39,52]) Protective factors within the family environment, such as supportive parenting and family cohesion, appear to buffer these effects. [15]
Given that much of this evidence comes from Australia and the US, a critical gap remains in our understanding of how chronic exposure to climate-related trauma affects child development and long-term mental health, particularly in LMICs. Further research is needed to examine these associations in LMICs and to identify the developmental pathways through which repeated climate-related disasters contribute to the onset of mental illness in childhood and later in life.
E-ACEs Representing a Distinct and Growing Subclass Within the TRACEs Framework
The TRACEs framework offers a novel perspective by considering a broader range of traumatic experiences and ACEs, with nearly every component of adversity linked to worse psychiatric symptoms. [34,36] We posit climate-related ACEs as a growingly important subclass of TRACEs, distinct in their role as drivers of both acute and chronic childhood adversity, shaping a child’s developmental, physical, and mental health outcomes (Figure 1). For example, unlike other adversities, ECEs, acutely, elevate the risk of infectious diseases such as dengue [7], malaria [10], and diarrheal infections [6] particularly among children in LMICs (Table 1). Additionally, ECEs contribute to chronic outcomes such as malnutrition [11] and mental health conditions, including PTSD [12], depression [9,13,15], and suicidality [16], as well as long-term cognitive and developmental delays (Table 1). [11]
Within the TRACEs framework, climate-related ACEs extend beyond individual-level trauma to encompass structural and environmental adversities that disrupt family stability, community resources, and access to safe environments. [34] For example, ECEs such as hurricanes, floods, and droughts, compromise water infrastructure, leading to contamination, shortages, and increased reliance on unsafe water sources, [53] heightened the risk of diarrheal infection, vector-borne diseases, and malnutrition. [6,7,10,11] Psychological distress stemming from water scarcity or insecurity and distrust in public water supplies and reliance on alternatives, that are often more expensive or hazardous sources, further exacerbates one’s mental health burden due to cumulative stress. [54,55] ECEs, such as extreme heat events, are also known to cause direct health, as well as economic effects in adults and children leading to socio-economic adversities such as poverty, food insecurity, and inadequate housing potentially leading to lasting mental health effects. [56,57,58] However, the long-term effects of prolonged exposure to ECEs remain largely unexplored. Understanding the long-term impacts and underlying mechanisms of such climate-induced ACEs within the TRACEs framework would provide a clearer case for early intervention and preventive measures aimed at reducing the cumulative impacts of extreme weather on future generations. [34]
E-ACEs as a Humanitarian Crisis
In the aftermath of an extreme weather event such as a cyclone, poor rural families often experience the worst outcomes given their fragile socio-economic conditions. The loss of property and livelihood may force poor families to migrate to cities in search of employment often resulting in significant household instability and family separation, both of which align with traditional ACEs model such as neglect and caregiver absence. [21,59,60] Children left behind by migrating parents may be placed in the care of grandparents or relatives, while those who migrate with their families are often forced to live in overcrowded, impoverished urban slums. The situation in Bangladesh serves as a compelling case study, as Dhaka, the Capital, is home to more than 5,000 slums housing an estimated 4 million people, where access to healthcare, education, and social services are severely limited . [61] These conditions increase children's risk of experiencing neglect, domestic violence, and community violence, adversities that parallel those in the traditional ACE framework. [21]
For children left behind, limited contact with their parents, and the absence of stable caregiving environment can disrupt emotional development, mirroring the effects of household dysfunction and neglect. [21] Likewise, for children living in slums, caregivers’ long working hours often result in extended periods of unsupervised time, increasing vulnerability to exploitation, abuse, and trafficking. [18,62] While extended family or community networks may offer some degree of protection, these informal support systems are frequently overwhelmed. [63]
Due to increasing exposure to ECEs, sea-level rise, desertification, and other environmental changes, ‘climate refugees’ have become a growing phenomenon. [50] Between 2008 and 2023, a total of 402.4 million people were internally displaced globally due to climate related phenomenon, with 383.6 million originated from LMICs (Figure 2). [64,65] According to the Australian Institute for Economics & Peace (2024), 1.3 billion people residing in 50 LMICs face ecological threats, with 70% of them living in nations with low levels of societal resilience, such as Pakistan, Ethiopia, and Iran. [66] The increasing rates of climate refugees presents significant challenges for receiving communities and social services. [50] Without appropriate interventions, displaced children face heightened risks of experiencing adversities, including household dysfunction, exposure to violence, and caregiver separation. It is crucial for informing policies that mitigate the long-term effects of climate-related adversities on child development and mental health. [18,62]
Resilience Against E-ACEs
According to American Psychological Association, resilience is the process and outcome of successfully adapting to difficult or challenging life experiences, especially through mental, emotional, and behavioural flexibility and adjustment to external and internal demands. [67] Building resilience could be a crucial component of humanitarian responses to climate-induced ACEs, as evidence suggests that resilience, both intrinsic (individual-level) and extrinsic (family- and community-level), may help moderate the impact of ECEs on children, reducing their vulnerability to adverse physical and mental health as well as developmental. [63,68,69,70,71]
While developmental psychological theories of resilience emphasize intrinsic characteristics such as learning, problem-solving or self-control, individual resilience alone may not be sufficient for children facing climate-related ACEs, as these environmental traumas are often chronic, severe, and systemic. [71,72] Children coping with post-disaster circumstances depend on a network of social support systems including family, peers, schools, and community structures, which resilience theories describe as essential interdependent social systems for psychological well-being. [72] Therefore, the role of extrinsic characteristics, such as interpersonal relationships, stable family bonds or support networks (e.g., school, and peer groups), are fundamental for building resilience in children faced with prolonged exposure to ECEs. [68,73,74] Contemporary theories of resilience, such as multisystemic resilience, ecological resilience, and resilience portfolio models, highlight the importance of extrinsic factors in fostering resilience against climate-related ACEs. [63] Despite the growing recognition of resilience at multiple levels, research on how individual resilience connects to broader familial and social systems in the context of climate-induced ACEs remains limited, highlighting the need for further investigation.
For instance, families vary in resilience depending on internal challenges, such as domestic violence, caregiver mental illnesses, or substance abuse, as well as external conditions including poverty, community violence, or repeated climate shocks. When family support systems are compromised, alternative social structures, such as support networks, neighbourhood bonds, and religious and cultural affiliations, mass media, non-governmental organizations (NGOs), and government-led interventions (e.g., child protection services, foster care, and mental health support), may play a critical role in mitigating the impact of climate-related ACEs. [63,68,72,73] Given that ECEs disrupting functioning across multiple levels of socio-cultural systems, children’s recovery from E-ACEs may reflect larger community recovery processes, which often depend on available resources and social infrastructure. However, due to increasing frequency and severity of climate crises, many communities are struggling to maintain and mobilize these resources effectively. [68]
In humanitarian responses, resilience-building interventons can help communities prepare for, withstand, and recover from climate crises by strengthening psychological, social, and economic support systems that buffer against the negative effects of ECEs. [75] For example, post-disaster interventions that integrate mental health services, economic recovery programs, and community-driven rebuilding efforts have shown promise in reducing trauma-related outcomes in affected populations. [75] Moving beyond the traditional idea of resilience, which often focuses on bouncing back to a previous state, transformational resilience, in the context of climatic disasters, refers to the capacity of individuals, communities, or systems to undergo deep, adaptive changes that allow them not only to recover from a disaster but also to emerge stronger and better equipped to cope with future environmental challenges. [70]
Given that the most harmful impacts of ECEs are caused not only by immediate consequences but also by persistent, overwhelming toxic stress [32], there are gaps in resilience-building frameworks, as most existing frameworks are designed for short-term post-disaster responses rather than specifically addressing the compounded effects of ACEs and ECEs on children. [63,72] Resilience program models, therefore, need to incorporate three key responses: stress resistance (e.g., fostering supportive environments and enhancing adaptive coping skills to prevent long-term harm), recovery (e.g., promoting emotional regulation and rebuilding caregiver-child relationships after a crisis), and positive transformation (e.g., strengthening long-term social supports to better manage future stressors). [72] Such resilience models might have a transformational effect if they incorporate strategies at the population level, as well as targeted interventions addressing specific stressors (e.g., neglect, abuse, parental separation), to meet the diverse needs of different societal (individual, family, community), geographic (urban, rural), and temporal (short-term, long-term) contexts. [70] These strategies may also reduce neurobiological disruptions (e.g., HPA axis dysfunction, inflammation) and long-term mental health risks associated with ACEs and E-ACEs.
One emerging framework is the Composite of Post-Event Well-Being (COPEWELL), a resilience model initially developed to assess and improve long-term community resilience in the United States. [75] COPEWELL integrates multiple resilience domains, including health system capacity, social capital, economic stability, and emergency response coordination, to help communities recover from ECEs and prevent long-term adverse outcomes. [75] However, the applicability, scalability, and effectiveness of COPEWELL in preventing E-ACEs, particularly in LMICs, remain untested and require further adaptation for a local context. Many LMICs still lack practical tools and resources for implementing community resilience measures, creating a need for localized, evidence-based interventions. [75,76]
Potential Interventions for E-ACEs
Potential interventions to strengthen resilience and reduce the impact of ECEs emphasize may benefit from multi-sectoral collaboration and coordinated efforts across policy, community and individual levels, considering evidence-based policies and culturally responsive approaches (Table 2) [66,72,75,77]. Policymakers may consider prioritizing investments in adaptive infrastructure, economic stability, and emergency preparedness to reduce the impact of climate-related disruptions on vulnerable families. [76] For example, strengthening adaptive infrastructure (such as climate-resilient housing, sustainable water management, and green spaces) could reduce climate stressors on children and families by creating safer living environments and help mitigate displacement risks. [78] Urban or rural settlements designed to ensure access to basic health services, integration of displaced children into schools and communities, and long-term mental health support may play a crucial role in helping children cope with post-traumatic stress. [76]
Investing in social safety nets, including microfinancing, vocational training, income diversification, and sustainable agriculture could reduce economic stressors that exacerbate childhood adversity by enhancing financial inclusion and climate-resilient livelihoods. [79] Community capacity building initiatives, such as training and information dissemination, fostering solidarity, and positive parenting interventions may strengthen resilience in the face of climate-related stressors. [66,72,75,77] Agroecological systems (e.g., indigenous crop varieties, conservation agriculture) could potentially reduce displacement risks for poor rural families. [80] Schools may contribute to building resilience by integrating climate stress education, importance of social connections, social-emotional learning programs, and trauma-informed care into curricula, fostering psychological resilience among children. [73]
Integrated, trauma-informed, community-based mental health care could help address both immediate psychological needs and broader structural determinants, thus improving long-term adaptation and well-being. [19,68,77,81,82] In South Asia, community-based initiatives, such as peer-led models and digital mental health support, have been effective enhancing coping with extreme weather events, and reducing post-traumatic stress, though more comprehensive research is needed to assess their long-term effectiveness. [83,84,85,86,87,88,89,90,91,92,93,94]
India’s National Institute of Mental Health and Neurosciences (NIMHANS) (Figure 3) program integrates psychosocial assessment, psychological first aid, professional-led therapies, and peer-led support (Figure 3), and evaluations suggest it has been effective in reducing stress symptoms and enhancing resilience among adults and children. [87,88,89,90,91,92,93,94] It’s effectiveness may be due to its community-led approach, which mobilizes local community and spiritual leaders, community health workers, and lay volunteers, while also integrating layered, trauma-informed strategies, utilising both face-to-face and digital tools, and supporting the development of local mental health task forces and guidelines in low-resource, disaster-prone regions. [87,88,89,90,91,92,93,94] By leveraging local knowledge and building local capacity, the model enhances accessibility, cultural relevance, and community ownership of psychosocial care. [87,88,89,90,91,92,93,94]
The NIMHANS psychosocial care model serves as a promising practice for regions facing similar socio-economic and climate-related challenges, demonstrating how community-led, scalable, and cost-effective interventions can improve mental health outcomes in vulnerable communities. Yet, there are few areas for improvements. For example, only a limited number of activities within psychosocial care model specifically targeted children, and most efforts served as immediate disaster response rather than structured, long-term resilience-building initiatives. Thus, it remains unclear whether the benefits of these community-based approaches can translate into sustained resilience against future climate-related adversities. Several challenges may hinder their long-term effectiveness including funding limitations, the absence of targeted policies and guidelines for children affected by climate-induced trauma, limited reach in remote or underserved areas, insufficient community resources and capacities, and an emphasis on rebuilding physical infrastructure and economic support over addressing the psychological aspects of recovery. [66]
Addressing these gaps requires stronger partnerships between government agencies, non-governmental organizations, and local communities to generate sustainable funding for children's mental health and resilience-building initiatives. Integrating mental health services with climate change anticipatory actions within national disaster risk management and public health systems may be essential for both preventing and addressing the long-term consequences of climate-related adversities. [75] While the evaluations of these psychosocial model suggests that early intervention may reduce the mental health burden among climate affected populations, further research is needed to determine which specific components of these programs are most effective and scalable.
Despite increasing awareness about mental health implications of climate change, research on its impact on children in LMICs remains scarce. Gaps remain in the evidence regarding which specific exposures have been linked to various long-term health outcomes for children chronically exposed to climate-induced adversities, as well as the most effective components of resilience-building programs across diverse contexts, and the economic burden of climate-related ACEs on national health systems. Future research should focus on understanding how socio-economic factors, cultural norms, and policy environments influence children’s resilience to ACEs and ECEs and evaluate the effectiveness of community-led interventions in mitigating the long-term consequences of childhood adversity in climate-vulnerable regions. National governments in LMICs should consider shifting their investments toward research, preparedness, and prevention of ACEs in climate-affected areas. More developed nations must take responsibility for addressing climate-related threats, recognizing their disproportionate impact on children in LMICs.
Conclusions
Due to the increasing frequency and severity of ECEs, there is growing concern that they can be a significant source of ACEs, with potential implications for the health and development of afflicted children. It has been hypothesized that prolonged exposure to ECEs and the resulting ACEs could disrupt brain and neural development, potentially impairing cognitive and emotional functioning. Additionally, alterations to the HPA axis may lead to long-term stress dysregulation and an increased risk of mental disorders. Further, chronic exposure to climate stress has been suggested to contribute to immune system dysregulation and heightened inflammatory responses, which could influence long-term mental and physical health outcomes in adulthood. In the developing world, rising rates of ECEs may be contributing to the displacement of rural populations, forcing many into large urban slums where ACEs could emerge due to increased socioeconomic instability. However, research suggests that communities and children with stronger social bonds, family support, and access to resources may be more likely to demonstrate psychosocial resilience against the impacts of climate change. Given this, it is critical to explore whether investing in interventions that enhance community resilience and expand mental health services can help mitigate the impact of future E-ACEs. Building resilience requires coordinated efforts across individual, community, policy, and global public health levels. It is important for higher-income countries to acknowledge their capacity and opportunity to support global efforts in addressing climate-related threats, particularly given the disproportionate impacts on children in LMICs. Climate-induced ACEs represent a pressing issue, and further research is needed to understand their full scope and to develop effective interventions.
References
- Ritchie, H.; Rosado, P. Natural Disasters Our World in Data; 2024. Available online: https://ourworldindata.org/natural-disasters.
- (IDMC) TIDMC. Annual Report 2022 Geneva, Switzerland: The Internal Displacement Monitoring Centre (IDMC); 2022. Available online: https://api.internal-displacement.org/sites/default/files/publications/documents/IDMC_Annual_Report_2022.pdf.
- Garschagen, M.; Doshi, D.; Reith, J.; Hagenlocher, M. Global patterns of disaster and climate risk—an analysis of the consistency of leading index-based assessments and their results. Climatic Change. 2021, 169, 11. [Google Scholar] [CrossRef]
- Louise, S.; Elizabeth, G. 1328 Climate change, children’s development and the Griffiths III community. Archives of Disease in Childhood. 2022, 107 (Suppl 2), A317. [Google Scholar]
- Nashwan, A.J.; Ahmed, S.H.; Shaikh, T.G.; Waseem, S. Impact of natural disasters on health disparities in low- to middle-income countries. Discover Health Systems. 2023, 2, 23. [Google Scholar] [CrossRef]
- Dimitrova, A.; McElroy, S.; Levy, M.; Gershunov, A.; Benmarhnia, T. Precipitation variability and risk of infectious disease in children under 5 years for 32 countries: a global analysis using Demographic and Health Survey data. Lancet Planet Health. 2022, 6, e147–e55. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wei, Y.; Li, K.; Jiang, X.; Li, C.; Yue, Q.; et al. Impact of extreme weather on dengue fever infection in four Asian countries: A modelling analysis. Environment International. 2022, 169, 107518. [Google Scholar] [CrossRef]
- Kessler, R.C.; Galea, S.; Gruber, M.J.; Sampson, N.A.; Ursano, R.J.; Wessely, S. Trends in mental illness and suicidality after Hurricane Katrina. Mol Psychiatry. 2008, 13, 374–384. [Google Scholar] [CrossRef]
- Tang, B.; Liu, X.; Liu, Y.; Xue, C.; Zhang, L. A meta-analysis of risk factors for depression in adults and children after natural disasters. BMC Public Health. 2014, 14, 623. [Google Scholar] [CrossRef]
- Boyce, R.; Reyes, R.; Matte, M.; Ntaro, M.; Mulogo, E.; Metlay, J.P.; et al. Severe Flooding and Malaria Transmission in the Western Ugandan Highlands: Implications for Disease Control in an Era of Global Climate Change. The Journal of Infectious Diseases. 2016, 214, 1403–1410. [Google Scholar] [CrossRef]
- Aguilar, A.; Vicarelli, M. El Niño and children: Medium-term effects of early-life weather shocks on cognitive and health outcomes. World Development. 2022, 150, 105690. [Google Scholar] [CrossRef]
- Lai, B.S.; Kelley, M.L.; Harrison, K.M.; Thompson, J.E.; Self-Brown, S. Posttraumatic stress, anxiety, and depression symptoms among children after Hurricane Katrina: A latent profile analysis. Journal of child and family studies. 2015, 24, 1262–1270. [Google Scholar] [CrossRef]
- Kar, N.; Sharma, P.; Murali, N.; Mehrotra, S. Mental health consequences of the trauma of super-cyclone 1999 in Orissa. Indian journal of psychiatry. 2004, 46, 228–237. [Google Scholar] [PubMed]
- McFarlane, A.C.; Van Hooff, M. Impact of childhood exposure to a natural disaster on adult mental health: 20-year longitudinal follow-up study. British Journal of Psychiatry. 2009, 195, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, G.Y.; Zacher, M.; Merdjanoff, A.A.; Do, M.P.; Pham, N.K.; Abramson, D.M. The effects of cumulative natural disaster exposure on adolescent psychological distress. J Appl Res Child. 2021, 12. [Google Scholar] [CrossRef]
- Kar, N. Suicidality following a natural disaster. American journal of disaster medicine. 2010, 5, 361–368. [Google Scholar] [PubMed]
- Burke, S.E.L.; Sanson, A.V.; Van Hoorn, J. The Psychological Effects of Climate Change on Children. Curr Psychiatry Rep. 2018, 20, 35. [Google Scholar] [CrossRef]
- Ojala, M. How do children cope with global climate change? Coping strategies, engagement, and well-being. Journal of Environmental Psychology. 2012, 32, 225–233. [Google Scholar]
- Hayes, K.; Blashki, G.; Wiseman, J.; Burke, S.; Reifels, L. Climate change and mental health: risks, impacts and priority actions. International Journal of Mental Health Systems. 2018, 12, 28. [Google Scholar] [CrossRef]
- Change, I.P.O.C. Climate change 2013: The physical science basis. Contribution of Working Group I to the fifth assessment report of the Intergovernmental Panel on Climate Change Cambridge, United Kingdom and New York, NY, USA: Cambridge University Press; 2013. Available online: https://www.ipcc.ch/report/ar5/wg1/.
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Madigan, S.; Deneault, A.A.; Racine, N.; Park, J.; Thiemann, R.; Zhu, J.; et al. Adverse childhood experiences: a meta-analysis of prevalence and moderators among half a million adults in 206 studies. World Psychiatry. 2023, 22, 463–471. [Google Scholar] [CrossRef]
- Dube, S.R.; Anda, R.F.; Felitti, V.J.; Chapman, D.P.; Williamson, D.F.; Giles, W.H. Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: findings from the Adverse Childhood Experiences Study. JAMA. 2001, 286, 3089–3096. [Google Scholar] [CrossRef]
- Sheridan, M.A.; McLaughlin, K.A. Dimensions of early experience and neural development: deprivation and threat. Trends in Cognitive Sciences. 2014, 18, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Finkelhor, D.; Shattuck, A.; Turner, H.; Hamby, S. Improving the Adverse Childhood Experiences Study Scale. JAMA Pediatrics. 2013, 167, 70–75. [Google Scholar] [CrossRef]
- Fujiwara, T. Impact of adverse childhood experience on physical and mental health: A life-course epidemiology perspective. Psychiatry and Clinical Neurosciences. 2022, 76, 544–551. [Google Scholar] [CrossRef]
- Helton, J.J.; Davis, J.P.; Lee, D.S.; Pakdaman, S. Expanding adverse child experiences to inequality and racial discrimination. Preventive Medicine. 2022, 157, 107016. [Google Scholar] [CrossRef]
- Lee, H.; Kim, Y.; Terry, J. Adverse childhood experiences (ACEs) on mental disorders in young adulthood: Latent classes and community violence exposure. Preventive Medicine. 2020, 134, 106039. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Wu, D.; He, X.; Ma, Q.; Peng, J.; Mao, G.; et al. Meta-analysis of the relationship between bullying and depressive symptoms in children and adolescents. BMC Psychiatry. 2023, 23, 215. [Google Scholar] [CrossRef]
- Lee, H.; Slack, K.S.; Berger, L.M.; Mather, R.S.; Murray, R.K. Childhood Poverty, Adverse Childhood Experiences, and Adult Health Outcomes. Health & Social Work. 2021, 46, 159–170. [Google Scholar]
- Holloway, K.; Cahill, G.; Tieu, T.; Njoroge, W. Reviewing the Literature on the Impact of Gun Violence on Early Childhood Development. Curr Psychiatry Rep. 2023, 25, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Muthanna, S.; Sara, H.; Panos, V.; Basel, E.-K.; Nader, A.-D. Children’s prolonged exposure to the toxic stress of war trauma in the Middle East. BMJ. 2020, 371, m3155. [Google Scholar]
- Sanders, L.M. Is COVID-19 an adverse childhood experience (ACE): Implications for screening for primary care. The Journal of Pediatrics. 2020, 222, 4–6. [Google Scholar] [CrossRef]
- Weems, C.F.; Russell, J.D.; Herringa, R.J.; Carrion, V.G. Translating the neuroscience of adverse childhood experiences to inform policy and foster population-level resilience. Am Psychol. 2021, 76, 188–202. [Google Scholar] [CrossRef] [PubMed]
- Auchincloss, A.H.; Ruggiero, D.A.; Donnelly, M.T.; Chernak, E.D.; Kephart, J.L. Adolescent mental distress in the wake of climate disasters. Preventive Medicine Reports. 2024, 39, 102651. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.D.; Heyn, S.A.; Peverill, M.; DiMaio, S.; Herringa, R.J. Traumatic and Adverse Childhood Experiences and Developmental Differences in Psychiatric Risk. JAMA Psychiatry. 2025, 82, 66–74. [Google Scholar] [CrossRef]
- UNICEF Children displaced by a changing climate: preparing for a future already underway.: UNICEF; 2023. Available online: https://www.unicefusa.org/sites/default/files/2023-10/ClimateDisplacementReport.pdf.
- Seehusen, D.A.; Bowman, M.A.; Britz, J.; Ledford, C.J.W. A Focus on Climate Change and How It Impacts Family Medicine. J Am Board Fam Med. 2024, 37, 1–3. [Google Scholar] [CrossRef]
- Mitchell, A.; Maheen, H.; Bowen, K. Mental health impacts from repeated climate disasters: an Australian longitudinal analysis. The Lancet Regional Health – Western Pacific. 2024, 47, 101087. [Google Scholar] [CrossRef]
- Danese, A.; Baldwin, J.R. Hidden Wounds? Inflammatory Links Between Childhood Trauma and Psychopathology. Annu Rev Psychol. 2017, 68, 517–544. [Google Scholar]
- Nelson, C.A.; Bhutta, Z.A.; Burke Harris, N.; Danese, A.; Samara, M. Adversity in childhood is linked to mental and physical health throughout life. BMJ. 2020, 371, m3048. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.; Rogosch, F.A. The impact of child maltreatment and psychopathology on neuroendocrine functioning. Dev Psychopathol. 2001, 13, 783–804. [Google Scholar] [CrossRef]
- Gunnar, M.R.; Vazquez, D. Stress neurobiology and developmental psychopathology. Developmental Psychopathology: Volume Two: Developmental Neuroscience. 2015:533-77.
- Miller, G.E.; Cole, S.W. Clustering of depression and inflammation in adolescents previously exposed to childhood adversity. Biol Psychiatry. 2012, 72, 34–40. [Google Scholar] [CrossRef]
- Miller, A.H.; Maletic, V.; Raison, C.L. Inflammation and Its Discontents: The Role of Cytokines in the Pathophysiology of Major Depression. Biological Psychiatry. 2009, 65, 732–741. [Google Scholar] [CrossRef]
- Abdelzaher, H.; Tawfik, S.M.; Nour, A.; Abdelkader, S.; Elbalkiny, S.T.; Abdelkader, M.; et al. Climate change, human health, and the exposome: Utilizing OMIC technologies to navigate an era of uncertainty. Front Public Health. 2022, 10, 973000. [Google Scholar] [CrossRef] [PubMed]
- Zagaria, A.; Fiori, V.; Vacca, M.; Lombardo, C.; Pariante, C.M.; Ballesio, A. Inflammation as a mediator between adverse childhood experiences and adult depression: A meta-analytic structural equation model. J Affect Disord. 2024, 357, 85–96. [Google Scholar] [CrossRef]
- Di, N.; He, W.; Zhang, K.; Cui, J.; Chen, J.; Cheng, J.; et al. Association of short-term air pollution with systemic inflammatory biomarkers in routine blood test: A longitudinal study. Environmental Research Letters. 2021, 16(3).
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; et al. Chronic inflammation in the etiology of disease across the life span. Nature Medicine. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, S.; Popescu, C.; Panu Napodano, C.M.; Fiamma, M.; Cegolon, L. Global health, climate change and migration: The need for recognition of "climate refugees". J Glob Health. 2023, 13, 03011. [Google Scholar] [CrossRef] [PubMed]
- Kellermann, N.P. Epigenetic transmission of Holocaust trauma: can nightmares be inherited? Isr J Psychiatry Relat Sci. 2013, 50, 33–39. [Google Scholar]
- Harville, E.W.; Shankar, A.; Dunkel Schetter, C.; Lichtveld, M. Cumulative effects of the Gulf oil spill and other disasters on mental health among reproductive-aged women: The Gulf Resilience on Women’s Health study. Psychological Trauma: Theory, Research, Practice, and Policy. 2018, 10, 533. [Google Scholar] [CrossRef]
- Weems, C.F.; Poleacovschi, C.; Ikuma, K. A perspective for identifying intersections among the social, engineering, and geosciences to address water crises. Frontiers in Water. 2023, 5. [Google Scholar] [CrossRef]
- Weems, C.F.; Watts, S.E.; Marsee, M.A.; Taylor, L.K.; Costa, N.M.; Cannon, M.F.; et al. The psychosocial impact of Hurricane Katrina: contextual differences in psychological symptoms, social support, and discrimination. Behav Res Ther. 2007, 45, 2295–2306. [Google Scholar] [CrossRef]
- Nelson, T.; Poleacovschi, C.; Ikuma, K.; Garcia, I.; Weems, C.; Rehmann, C.; et al. Knowledge–Behavior Gap in Tap Water Consumption in Puerto Rico: Implications for Water Utilities. ASCE OPEN Multidisciplinary Journal of Civil Engineering. 2023, 1. [Google Scholar] [CrossRef]
- Liu, J.; Varghese, B.M.; Hansen, A.; Xiang, J.; Zhang, Y.; Dear, K.; et al. Is there an association between hot weather and poor mental health outcomes? A systematic review and meta-analysis. Environ Int. 2021, 153:106533.
- Hunt, A.P.; Brearley, M.; Hall, A.; Pope, R. Climate Change Effects on the Predicted Heat Strain and Labour Capacity of Outdoor Workers in Australia. Int J Environ Res Public Health. 2023, 20(9).
- Vergunst, F.; Berry, H.L. Climate Change and Children's Mental Health: A Developmental Perspective. Clin Psychol Sci. 2022, 10, 767–785. [Google Scholar] [CrossRef]
- Ahmed, M. Health and Well-Being of Climate Migrants in Slum Areas of Dhaka. In: Leal Filho W, Wall T, Azul AM, Brandli L, Özuyar PG, editors. Good Health and Well-Being. Encyclopedia of the UN Sustainable Development Goals. Cham: Springer International Publishing; 2020. p. 277-93.
- Rana, M.M.P.; Ilina, I.N. Climate change and migration impacts on cities: Lessons from Bangladesh. Environmental Challenges. 2021, 5, 100242. [Google Scholar] [CrossRef]
- (BBS), B.B.o.S. Census of slum areas and floating population 2014 Dhaka, Bangladesh: Bangladesh Bureau of Statistics 2015 [Available from: https://dataspace.princeton.edu/bitstream/88435/dsp01wm117r42q/1.
- Joshi, R.; Andersen, P.T.; Thapa, S.; Aro, A.R. Sex trafficking, prostitution, and increased HIV risk among women during and after the 2015 Nepal earthquake. SAGE Open Med. 2020, 8, 2050312120938287. [Google Scholar] [CrossRef]
- Hamby, S.; Guerra, C.; Toro, E.; Pinto-Cortez, C. Advancing the science of adverse childhood experiences and resilience: A case for global and ecological perspectives. Child Protection and Practice. 2024, 3:100060.
- Bilak, A.; Cardona-Fox, G.; Ginnetti, J.; Rushing, E.J.; Scherer, I.; Swain, M.; et al. Global Report on Internal Displacement Geneva, Switzerland: Internal Displacement Monitorring Center (IDMC); 2016. Available online: https://api.internal-displacement.org/sites/default/files/publications/documents/2016-global-report-internal-displacement-IDMC.pdf.
- Internal Displacement Monitoring Centre. IDMC Data Portal 2024. Available online: https://www.internal-displacement.org/database/displacement-data/.
- (IEP), I.f.E.P. Ecological threat report 2024: Analysing ecological threats, resilience & peace Sydney, Australia: Institute for Economics & Peace (IEP); 2024. Available online: https://www.economicsandpeace.org/wp-content/uploads/2024/10/ETR-2024-web.pdf.
- Association, A.P. Association, A.P. APA Dictionary of Psychology: Resilience Washington, DC 20002-4242: American Psychological Association; 2025. Available online: https://dictionary.apa.org/resilience.
- Beese, S.; Drumm, K.; Wells-Yoakum, K.; Postma, J.; Graves, J.M. Flexible Resources Key to Neighborhood Resilience for Children: A Scoping Review. Children (Basel). 2023, 10(11).
- DiClemente, C.M.; Rice, C.M.; Quimby, D.; Richards, M.H.; Grimes, C.T.; Morency, M.M.; et al. Resilience in Urban African American Adolescents: The Protective Enhancing Effects of Neighborhood, Family, and School Cohesion Following Violence Exposure. The Journal of Early Adolescence. 2018, 38, 1286–1321. [Google Scholar] [CrossRef]
- Doppelt, B. Transformational resilience: How building human resilience to climate disruption can safeguard society and increase wellbeing: Routledge; 2017.
- Masten, A.S.; Best, K.M.; Garmezy, N. Resilience and development: Contributions from the study of children who overcome adversity. Development and Psychopathology. 1990, 2, 425–444. [Google Scholar] [CrossRef]
- Masten, A.; Obradović, J. Disaster Preparation and Recovery: Lessons from Research on Resilience in Human Development. Ecology and Society. 2008, 13(1).
- Nijs, L.; Nicolaou, G. Flourishing in Resonance: Joint Resilience Building Through Music and Motion. Front Psychol. 2021, 12:666702.
- Yule, K.; Houston, J.; Grych, J. Resilience in Children Exposed to Violence: A Meta-analysis of Protective Factors Across Ecological Contexts. Clin Child Fam Psychol Rev. 2019, 22, 406–431. [Google Scholar] [CrossRef] [PubMed]
- Slemp, C.C.; Sisco, S.; Jean, M.C.; Ahmed, M.S.; Kanarek, N.F.; Erös-Sarnyai, M.; et al. Applying an Innovative Model of Disaster Resilience at the Neighborhood Level:The COPEWELL New York City Experience. Public Health Reports. 2020, 135, 565–570. [Google Scholar] [CrossRef]
- Walter, T.G.; Bricknell, L.K.; Preston, R.G.; Crawford, E.G.C. Climate Change Adaptation Methods for Public Health Prevention in Australia: an Integrative Review. Current Environmental Health Reports. 2024, 11, 71–87. [Google Scholar] [CrossRef] [PubMed]
- Links, J.M.; Schwartz, B.S.; Lin, S.; Kanarek, N.; Mitrani-Reiser, J.; Sell, T.K.; et al. COPEWELL: A Conceptual Framework and System Dynamics Model for Predicting Community Functioning and Resilience After Disasters. Disaster Med Public Health Prep. 2018, 12, 127–137. [Google Scholar] [CrossRef]
- Ahdoot, S.; Baum, C.R.; Cataletto, M.B.; Hogan, P.; Wu, C.B.; Bernstein, A.; et al. Climate change and children’s health: building a healthy future for every child. Pediatrics. 2024, 153(3).
- Bhalla, G.; Knowles, M.; Dahlet, G.; Poudel, M. Scoping review on the role of social protection in facilitating climate change adaptation and mitigation for economic inclusion among rural populations. 2024.
- Zenda, M.; Rudolph, M. A Systematic Review of Agroecology Strategies for Adapting to Climate Change Impacts on Smallholder Crop Farmers’ Livelihoods in South Africa. Climate. 2024, 12, 33. [Google Scholar] [CrossRef]
- Von Peter, G.; Von Dahlen, S.; Saxena, S.C. Unmitigated disasters? New evidence on the macroeconomic cost of natural catastrophes. 2012.
- Reduction, U.U.N.O.f.D.R. Disaster displacement: How to reduce risks, address impacts, and strengthen resilience 2024. Available online: https://www.undrr.org/words-into-action/disaster-displacement-how-reduce-risk-address-impacts-and-strengthen-resilience.
- Kar, N. Psychosocial issues following a natural disaster in a developing country: a qualitative longitudinal observational study. International Journal of Disaster Medicine. 2006, 4, 169–176. [Google Scholar] [CrossRef]
- Paul, S.K.; Routray, J.K. Household response to cyclone and induced surge in coastal Bangladesh: coping strategies and explanatory variables. Natural Hazards. 2011, 57, 477–499. [Google Scholar] [CrossRef]
- Wickrama, T.; Wickrama, K.; Banford, A.; Lambert, J. PTSD symptoms among tsunami exposed mothers in Sri Lanka: the role of disaster exposure, culturally specific coping strategies, and recovery efforts. Anxiety, Stress, & Coping. 2017, 30, 415–427. [Google Scholar]
- Senarath, S.K. Well-being of students affected by disaster: A case study of 2004 tsunami in Sri Lanka. International Journal of Disaster Management. 2021, 3, 58–70. [Google Scholar] [CrossRef]
- Becker, S.M. Psychosocial care for adult and child survivors of the 2004 tsunami disaster in India. Am J Public Health. 2006, 96, 1397–1398. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.M. Psychosocial care for women survivors of the tsunami disaster in India. American journal of public health. 2009, 99, 654–658. [Google Scholar] [CrossRef]
- Telles, S.; Singh, N.; Joshi, M.; Balkrishna, A. Post traumatic stress symptoms and heart rate variability in Bihar flood survivors following yoga: a randomized controlled study. BMC psychiatry. 2010, 10:1-10.
- Satapathy, S. Mental health impacts of disasters in India: ex-ante and ex-post analysis. Economic and welfare impacts of disasters in East Asia and policy responses ERIA research project report. 2011, 8:425-61.
- Bhadra, S. Psychosocial support for the children affected by communal violence in Gujarat, India. International Journal of Applied Psychoanalytic Studies. 2012, 9, 212–232. [Google Scholar] [CrossRef]
- Kuttichira, P.; Kallivayalil, R.A.; James, A.; Thomas, C.; Rahiman, A. Immediate Mental Health Response to Kerala Floods 2018 Victims. World Social Psychiatry. 2020, 2, 210–216. [Google Scholar] [CrossRef]
- Kola, L.; Kohrt, B.A.; Hanlon, C.; Naslund, J.A.; Sikander, S.; Balaji, M.; et al. COVID-19 mental health impact and responses in low-income and middle-income countries: reimagining global mental health. The Lancet Psychiatry. 2021, 8, 535–550. [Google Scholar] [CrossRef]
- Channaveerachari, N.K.; Raj, A.; Joshi, S.; Paramita, P.; Somanathan, R.; Chandran, D.; et al. Psychiatric and medical disorders in the after math of the uttarakhand disaster: Assessment, approach, and future challenges. Indian journal of psychological medicine. 2015, 37, 138–143. [Google Scholar] [CrossRef]
Figure 1.
Hypothetical pathways between exposure to extreme climate/weather events (ECEs) and health outcomes in children. (The green arow suggests protective effects. The health outcomes presented are examples. HPA axis =hypothalamic pituitary adrenal axis).
Figure 1.
Hypothetical pathways between exposure to extreme climate/weather events (ECEs) and health outcomes in children. (The green arow suggests protective effects. The health outcomes presented are examples. HPA axis =hypothalamic pituitary adrenal axis).
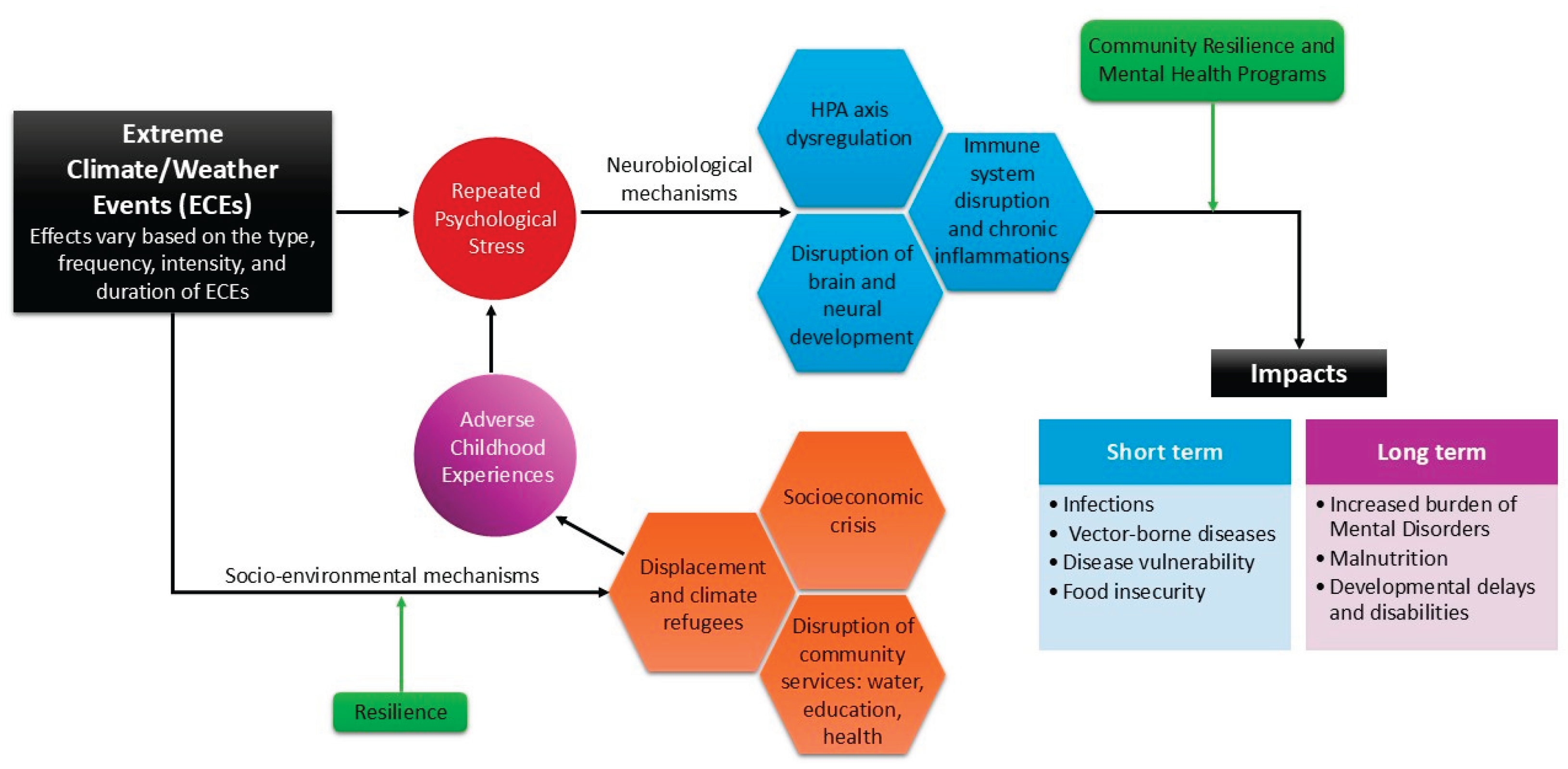
Figure 2.
Number of people internally displaced due to natural disasters (2008 –2023). Scale for total population displaced by extreme climate/weather events to the left. (Source: Internal Displacement Monitoring Centre) [65].
Figure 2.
Number of people internally displaced due to natural disasters (2008 –2023). Scale for total population displaced by extreme climate/weather events to the left. (Source: Internal Displacement Monitoring Centre) [65].
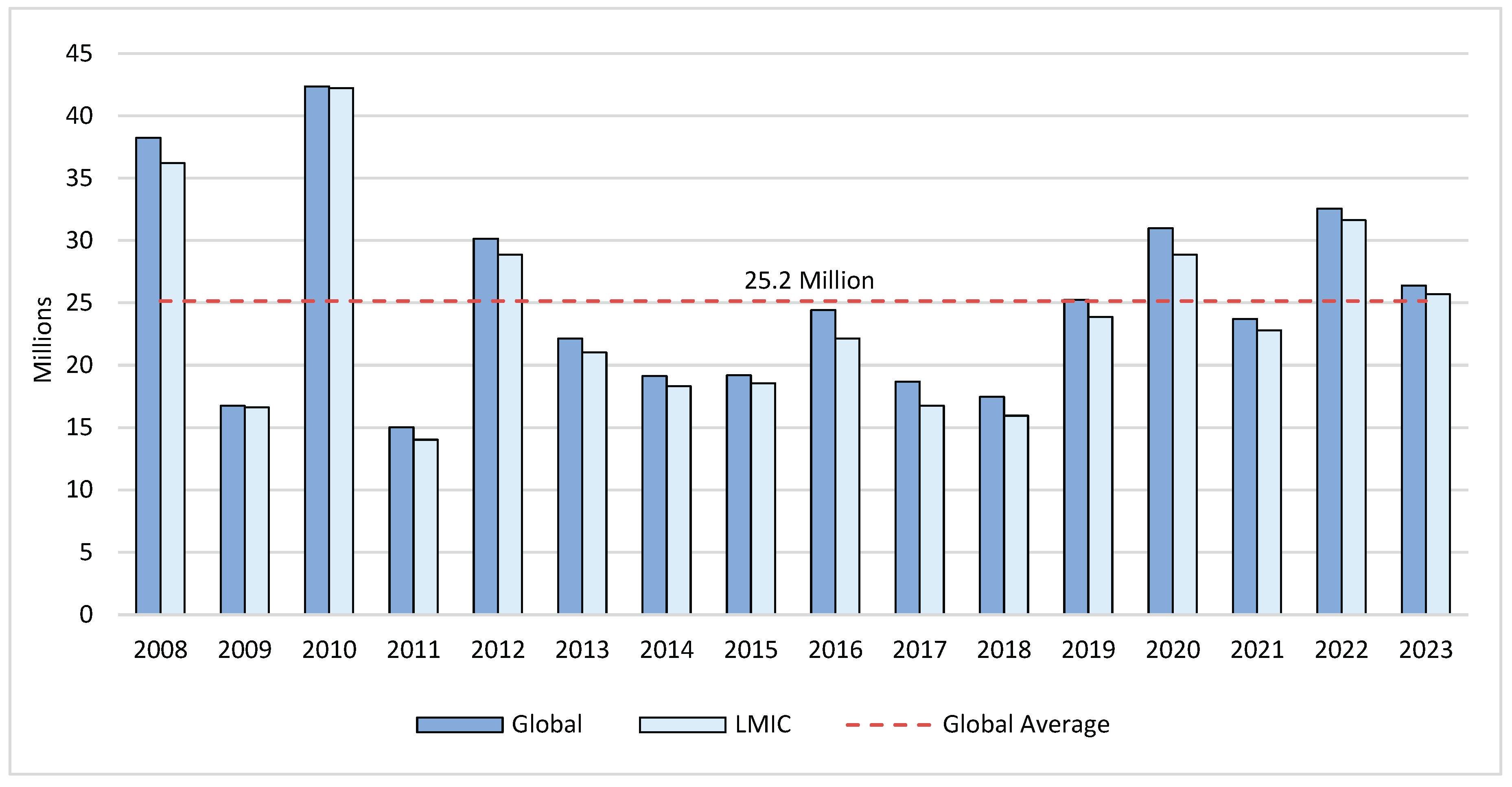
Figure 3.
Timeline of the development of the psychosocial model for post-disaster support by India’s National Institute of Mental Health and Neurosciences (NIMHANS) [83,87,88,89,90,91,92,93,94].
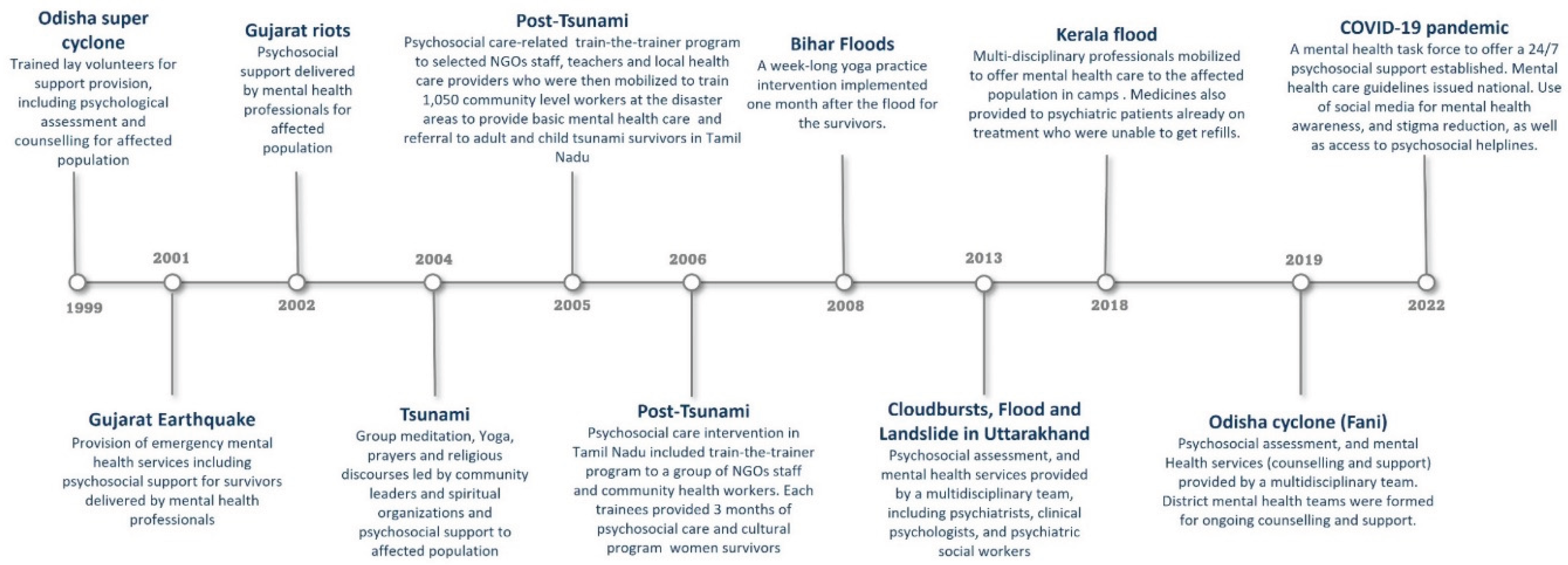

Table 1.
Physical, mental and development health impacts of exposure to ECEs in children and general population.
Table 1.
Physical, mental and development health impacts of exposure to ECEs in children and general population.
| Health Impacts | Climate/weather event | Effect size |
Target population |
|---|---|---|---|
| Physical Health impacts | |||
| Infectious diseases | Precipitation variability | OR=1.81 (95% CI: 1.20–2.71) [6] | Children<5 years across 32 LMICs |
| Dengue | Extremely high temperatures | RR=1.07 (95% CI: 1.02–1.13) within 1-3 weeks following extreme temperature rises [7] | General population in Singapore, Sri Lanka, Malaysia, and Thailand |
| Malaria | Severe Flooding | Increased risk by approx. 30% of having positive malaria diagnostic among flood exposed compared to those living away from the river [10] | General population in the Western Ugandan highlands |
| Malnutrition | Extreme precipitation levels | 8.3% points higher likelihood of being stunted among ECEs exposed [11] | Children aged 2–6 years in Rural Mexico |
| Mental health impacts | |||
| PTS symptoms/PTSD | Hurricane | OR=3.45 (95% CI: 1.49–8.03) [12] | Children aged 8–15 years in Louisiana, USA |
| Cyclone | Prevalence=44.3% in ECEs exposed [13] | General population in Orissa, India | |
| Bushfire | Lifetime RR=1.8 (95% CI: 1.11-2.93) [14] | General population in Australia | |
| Psychological distress | Multiple Hurricanes | OR=1.41 (95% CI: 1.05–1.88) [15] | Children aged 10–17 years in Louisiana, Mississippi, and New Orleans, USA |
| Storms, snowstorms, floods, droughts, wildfire | High disaster exposure was linked to 25% and 20% higher odds of major depression over 2- and 5-year periods, respectively [35] | 12-19 years in the USA | |
| Depression | Tsunami and earthquake | Prevalence=7.5% to 44.8% among ECEs exposed [9] | Children aged 7–18 years in Armenia, China, Turkey, and Thailand |
| Cyclone | Prevalence=52.7% among ECEs exposed [13] | General population in Orissa, India | |
| Flood, bushfire, cyclone | Multiple disaster exposure was linked to a −1.8-point decline in MHI-5 scores (95% CI: −3.4 to −0.3) from baseline [39] | General population in Australia | |
| Anxiety | Bushfire | Lifetime RR=1.37 (95% CI: 1.05–1.78) [14] | General population in Australia |
| Cyclone | Prevalence=57.5% of ECEs exposed [13] | General population in Orissa, India | |
| Suicidality | Hurricane | Suicidal ideation increased from 2.8% to 6.8% post-ECEs [8] | General population in Alabama, Mississippi, and Louisiana, USA) |
| Cyclone | Prevalence=12.6% suicidal attempts, 18.3% with suicidal plans and 38% with suicidal ideas among ECEs exposed [16] | General population (Orissa, India) | |
| Cognitive- developmental impacts | |||
| Developmental delays | Extreme precipitation | Cognitive test scores in language, memory and visual-spatial thinking 0.19, 0.17 and 0.15 SDs lower than children unexposed to ECEs [11] | Children aged 2–6 years in Rural Mexico |
* OR and RR compare individuals who are exposed to ECEs with those are not; CI: Confidence interval; ECEs: Extreme climate/weather events; LMICs: Low- and middle-income countries; MHI: Mental Health Inventory–5; OR: Odds Ratio; RR: Risk Ratio; PTS: Posttraumatic stress, PTSD: Posttraumatic stress disorder; SD: Standard deviation.
Table 2.
Key recommendations for preventing and mitigating the mental health outcomes of environmentally driven adverse childhood experiences (E-ACEs).
Table 2.
Key recommendations for preventing and mitigating the mental health outcomes of environmentally driven adverse childhood experiences (E-ACEs).
| Socio-structural level |
|---|
Building resilient environments, and resilient economies
|
Develop trauma-informed climate policies
|
Develop targeted policies for displaced children
|
Improve data systems and expand research in low- and middle-income countries (LMICs)
|
| Community level |
Implement community-based resilience programs
|
Leverage local knowledge and resources
|
Scale-up digital mental health solutions
|
| Individual level |
Enhance early intervention strategies for at-risk children
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



