
Submitted:
28 May 2025
Posted:
29 May 2025
You are already at the latest version
Abstract
Mitral regurgitation (MR) is a common valvular heart disease associated with significant morbidity and mortality. For patients at high or prohibitive surgical risk, Mitral Transcatheter Edge-to-Edge Repair (M-TEER) offers a less invasive alternative to surgery. This review outlines key aspects of patient selection and procedural planning for M-TEER, with a focus on clinical and echocardiographic criteria essential for success. Comprehensive imaging—especially 2D and 3D transesophageal echocardiography—is critical to assess leaflet anatomy, coaptation geometry, and mitral valve area. Selection criteria differ between primary and secondary MR and are guided by trials such as COAPT and MITRA-FR. Optimal outcomes rely on careful screening, anatomical suitability, and multidisciplinary evaluation. With growing experience and advancing technology, M-TEER has become a transformative option for treating severe MR in non-surgical candidates.
Keywords:
mitral regurgitation
; TEER
; transcatheter interventions
; valvulopathies
; structural heart diseases
; transcatheter edge-to-edge repair
; MitraClip
1. Introduction
Mitral regurgitation (MR) is one of the most common valvular heart diseases worldwide, affecting millions of patients, with its prevalence increasing with age.[1] It represents the second most common indication for cardiac surgery in Europe.[2] Primary/degenerative MR (DMR) represents a disease of the leaflets, resulting from excessive leaflet motion (prolapse or flail, classified as Carpentier type II) or restricted leaflet motion (restriction in systole and diastole, classified as Carpentier type IIIa). In contrast, secondary MR (SMR) results from left ventricular or left atrial pathology, with structurally normal mitral valve (MV) leaflets. The most common mechanism of SMR is left ventricular dysfunction and remodeling (ventricular SMR), that causes displacement of the papillary muscles and leaflet tethering, classified as Carpentier type IIIb. Another clinically significant form of SMR is atrial functional MR (AFMR), classified as Carpentier type I, which occurs in the setting of annular dilatation due to atrial enlargement. Unlike ventricular SMR, AFMR is characterized by preserved left ventricular ejection fraction (LVEF≥50%), absent regional wall motion abnormalities, and significant left atrial remodeling caused by atrial fibrillation or diastolic dysfunction. Patients with AFMR often present with a dilated left atrium (LA volume index ≥40 mL/m²) and normal left ventricular end-diastolic volume (LVEDV).[3] If left untreated, MR can lead to progressive left ventricular dysfunction, heart failure, and increased morbidity and mortality. It can also lead to a restrictive motion of the posterior leaflet with an excentric jet due to the pseudo-prolapse of the anterior leaflet (more complicated to treat) [4,5,6]
Nearly 50% of the patients with MR cannot undergo surgery due to comorbidities, advanced age or reduced ejection fraction.[2] For these patients, transcatheter therapies offer a viable alternative, focusing on leaflet or annulus repair, or valve replacement. The most widely used technique is leaflet approximation (mitral transcatheter edge-to-edge repair/M-TEER) with more than 150,000 implantations worldwide. Two devices are currently available for commercial use, MitraClip (Abbott Vascular) and the PASCAL (Edwards Lifesciences) both targeting leaflet approximation through similar principles, but with distinct technical features. The purpose of this review is to discuss patient selection criteria for M-TEER and to outline the essential imaging and procedural guidance strategies necessary for successful intervention.
2. Echocardiographic Evaluation of MR
The echocardiographic evaluation of mitral regurgitation relies on an integrative approach combining qualitative, quantitative and semiquantitative parameters. The mechanism of MR can be identified through detailed qualitative assessment of mitral valve anatomy and the morphology of subvalvular apparatus.[7]
The spectrum of degenerative (primary) mitral valve disease includes fibroelastic deficiency—characterized by thin leaflets and focal prolapse—and Barlow’s disease, which presents with diffusely thickened leaflets and prolapse involving multiple scallops, as illustrated in Figure 1. Other etiologies of degenerative MR include rheumatic valve disease, papillary muscle rupture in acute MR, leaflet perforation in the context of infective endocarditis, radiation- or drug-induced MR, congenital clefts, and connective tissue disorders. Secondary MR is defined by structurally normal mitral leaflets with impaired coaptation due to leaflet tethering or tenting, typically resulting from left ventricular or left atrial dilation (Figure 2). Eccentric regurgitant jets are commonly observed in primary MR (Figure 1), whereas central jets are more typical of secondary MR. However, in cases of ischemic secondary MR or posterior leaflet tethering, eccentric jets may also occur.
Semiquantitative parameters that support the diagnosis of severe MR include systolic flow reversal in pulmonary vein flow, dominant E-wave in mitral inflow (E-wave > 1.2m/sec) and vena contracta width > 7mm (> 8mm for biplane). Quantification of MR severity is mainly based on PISA method which is valid in central and round orifice jets.[8] Based on the PISA method, the effective regurgitant orifice area (EROA), the regurgitant volume (RVol) and the regurgitant fraction (RF) can be calculated. [9,10,11]
Primary MR is defined as severe when EROA is > 40mm2, RVol > 60ml and RF > 50%. For the definition of severe secondary MR, the same thresholds are proposed in ESC Guidelines 2021 and ACC/AHA guidelines for valvular heart disease.[10,11] Moreover, in ESC Guidelines 2021, lower thresholds (EROA is >30mm2, RVol >45ml) are proposed to be applied for defining severe secondary MR, in cases of elliptical regurgitant orifice area or low-flow conditions.[10] Additionally, increasing EROA, RVol, RF are correlated with increased mortality in SMR patients [12,13]. An important risk-stratification algorithm based on the quantitative assessment of MR has been proposed by Bartko [13] and classifies SMR patients in low risk (EROA<20mm2, RVol<30ml), intermediate risk (EROA=20-29mm2, RVol=30-44ml) and high risk (EROA>30mm2, RVol>45ml). A RF< 50% defined low risk SMR patients, whereas a RF>50% defined high risk SMR patients. [13]
Another important aspect in the evaluation of SMR patients is the dynamic component of SMR [14,15] implying that different loading conditions (exercise, hypertension, volume overload), medical therapy and cardiac resynchronization therapy in cases of LV dyssynchrony, have the potential as well to affect the severity of secondary MR. This dynamic component can be assessed by exercise echocardiography, especially in symptomatic SMR patients with less than severe MR at rest as seen in the clinical example in Figure 3.
3. Indications for Intervention in Mitral Regurgitation
3.1. Indications for Intervention in Primary MR
Surgical mitral valve repair is the preferred treatment for severe primary MR. Indications for surgery in severe primary MR (VC>7mm, RVol>60ml, EROA>0.40cm2, RF>50%) are driven by symptoms, or in asymptomatic patients by LV dysfunction (LVESD>40mm or LVEF<60%), significant LA dilatation (LAVI > 60ml/m2 or diameter > 55mm) and pulmonary hypertension at rest (SPAP > 50mmHg) when performed in a Heart Valve Center and a durable repair is likely.[10,11] However, many patients particularly those with multiple comorbidities or advanced age, are considered of high-risk for surgery. This has led to the emergence of transcatheter mitral valve interventions, with mitral transcatheter edge-to-edge repair (M-TEER) being the most widely adopted percutaneous option. In primary MR, M-TEER is an option for patients deemed inoperable or of high surgical risk (ACC guideline IIa, ESC IIb) [10,11]. (class IIb indication according to ESC guidelines for primary MR in symptomatic patients with appropriate anatomical criteria who are judged inoperable or at high surgical risk by the Heart Team).
3.2. Indications for Intervention in Secondary MR
In patients with severe secondary mitral regurgitation (SMR) undergoing coronary artery bypass grafting (CABG) or other cardiac surgery, concomitant mitral valve intervention is recommended (Class I, Level B, ESC guidelines).[9] However, earlier trials have indicated that surgical repair of SMR is associated with high reoperation rates, leading many surgeons to favor valve replacement over repair.[16] The recently announced MATTERHORN trial [17] compared M-TEER with surgical valve replacement in patients at acceptable surgical risk. It found that M-TEER provided comparable outcomes with fewer complications, supporting a growing trend toward transcatheter intervention as a first-line approach for SMR, even in operable patients.
For patients unsuitable for surgery but requiring revascularization, the Heart Team may consider PCI (and/or TAVI) followed by M-TEER, depending on the patient's clinical profile (Class IIa indication, ESC guidelines). M-TEER is also recommended for selected heart failure (HF) patients who remain symptomatic despite guideline-directed medical therapy (GDMT), including cardiac resynchronization therapy (CRT).
M-TEER offers a minimally invasive alternative to surgery, with evidence from key trials such as COAPT and RESHAPE HF2 showing significant improvement in symptoms, reduced hospitalizations, and lower all-cause mortality compared to medical therapy alone. [18,19] Landmark studies like COAPT and MITRA-FR have defined the role of M-TEER in patients with HF and persistent SMR, despite optimal GDMT or CRT.[18,20]
4. Patient Selection and Screening Criteria
Importantly, optimal M-TEER outcomes depend on careful patient selection and preprocedural echocardiographic screening. A multidisciplinary Heart Team is essential for patients’ evaluation and should include cardiac imaging specialists, interventional cardiologists, cardiac surgeons, HF specialists and electrophysiology specialists as well.
4.1. Selection in Primary Mitral Regurgitation (PMR)
Primary MR results from intrinsic abnormalities of the mitral valve leaflets, including prolapse, flail, perforation, or restriction, classified using the Carpentier system. M-TEER is currently indicated for symptomatic severe PMR in patients at high or prohibitive surgical risk, as determined by clinical scores (STS, EuroSCORE II) and frailty indices.[10,11] In this population, M-TEER has shown consistent safety and effectiveness, particularly in improving symptoms and reducing MR severity, with subsequent reverse remodeling of the left ventricle.
The EVEREST II trial laid the groundwork for PMR treatment with M-TEER, demonstrating non-inferiority to surgery in selected patients with favorable anatomy—central jet origin, adequate leaflet length, and minimal calcification.[21] However, contemporary practice increasingly expands beyond these initial anatomical criteria due to advances in imaging, device design, and operator experience.
Procedural success remains the key determinant of long-term outcome. Therefore, careful anatomical assessment—including segment involvement, leaflet length, mobility, flail gap, and calcification—is essential. Ongoing improvements in TEER systems and the accumulated procedural expertise have enabled treatment of anatomies once deemed unsuitable. Selection should ultimately be guided by a Heart Team, balancing anatomical feasibility with surgical risk and patient preference.
4.2. Selection in Secondary Mitral Regurgitation (SMR)
Clinical and echocardiographic predictors of favorable outcomes were first established by the COAPT trial, which focused specifically on ventricular secondary mitral regurgitation (V-SMR).[18] This trial included heart failure patients with ischemic or non-ischemic cardiomyopathy and reduced left ventricular ejection fraction (LVEF) between 20–50%. Patients with LVEF <20% were excluded due to the limited likelihood of benefit. The left ventricle should not be extremely dilated with an end-systolic diameter <70mm and mitral regurgitation should be clinically significant, defined as moderate-to-severe (>3+) (EROA>30mm2, RVol>45ml) or severe (4+) (EROA>40mm2, RVol>60ml) secondary MR. Eligible patients were symptomatic (NYHA Class II–IV ambulatory), receiving guideline-directed medical therapy (GDMT) and cardiac resynchronization therapy (CRT) when indicated. Other inclusion criteria included at least one HF hospitalization in the prior year, elevated natriuretic peptides, and mitral valve anatomy suitable for M-TEER.
In light of COAPT and MITRA-FR trials, the concept of disproportionate and proportionate MR emerged to explain the contradictory results of these trials.[22] Disproportionate MR refers to a greater degree of MR than expected for the degree of LV dilatation and suggests a higher likelihood of benefit from M-TEER. In contrast, proportionate MR reflects MR severity that aligns with LV size, indicating a preference for optimizing medical therapy rather than intervention.[22]
Disproportionate MR can be quantified by using volumetric ratios, such EROA/LVEDV or RVol/LVEDV.[23] Namazi et al., demonstrated that patients with a high Rvol/EDV>20% ratio had worse survival under medical management, implying that more severe MR with less LV dilatation (disproportionate MR) and a higher ratio RVol/LVEDV was associated with reduced all-cause mortality if this group received MR-correcting therapies.[23] Similarly, Berrill et al. found that disproportionate MR defined by EROA/LVEDV>0.14mm2/ml was associated with worse prognosis in patients with acute heart failure.[24] To guide clinical decision-making, COAPT-eligible vs. ineligible profiles (Table 1) should be systematically considered during patient screening. However, patients should not be excluded solely for not meeting COAPT criteria.
The RESHAPE-HF2 trial expanded the scope of M-TEER by including patients with symptomatic HF and moderate FMR (EROA 25 mm²).[25] Results showed a clear clinical benefit and reduction of hospitalizations and significant decline in the composite rate of hospitalizations and death [19,26]. These findings are consistent with the EXPAND study, which also demonstrated benefit in moderate MR patients treated with TEER, including evidence of reverse LV remodeling—a key therapeutic goal in HF management [27]. Similar reverse remodeling effects were reported in smaller cohort studies [28,29], including strain imaging research by Papadopoulos et al. [30], suggesting TEER's value even in patients with relatively preserved LV function without extensive fibrosis.[31]
Importantly, in patients with severe secondary mitral regurgitation (SMR) and advanced heart failure who do not meet COAPT criteria, M-TEER may still be considered for symptomatic relief or as a bridge to heart transplant (BTT) or left ventricular assist device (LVAD) therapy, as per ESC guidelines (class IIb recommendation). The International MitraBridge Registry demonstrated the safety of MitraClip in this context, showing that two-thirds of patients were free of adverse events at one year, and notably, 23.5% no longer required heart transplantation due to significant clinical improvement.[32] Another group of patients that could benefit is patients in cardiogenic shock and mitral regurgitation. In a multicenter analysis, the authors concluded that transcatheter mitral valve repair may improve short- and long-term mortality in high-risk patients with cardiogenic shock and moderate to severe MR, but further prospective randomized studies are needed to confirm these findings and guide future recommendations. [33]
5. Anatomical Considerations for TEER
Before selecting patients with primary or secondary mitral regurgitation (MR) for transcatheter edge-to-edge repair (TEER), a thorough anatomical evaluation is essential to ensure procedural success. Key echocardiographic parameters should be systematically assessed, including:
- Posterior leaflet length: A minimum of 7 mm (ideally >10mm) is typically required for adequate leaflet grasping.
- Flail gap and flail width: Severe primary MR may demonstrate a flail gap >10 mm and width >15 mm, which traditionally limited eligibility, but can be managed in experienced centers.
- Coaptation depth and coaptation length: Excessive coaptation depth (>11 mm) or reduced coaptation length (<2 mm) may pose procedural difficulty in secondary MR.
- Mitral valve area (MVA) and pressure gradient (PG): MVA <4.0 cm² may raise concern for post-procedural mitral stenosis, especially in patients requiring multiple devices. Cut-off values of 3.0cm2 for MVA and 4mmHg for mean PG are used to consider a patient ineligible for this method.
- Mitral annular and leaflet calcification: These may hinder adequate device deployment and leaflet grasping.
- Mitral annulus dimensions: Small dimensions of annulus (annulus area, anterior-posterior and medial-lateral diameters) should also be considered in the screening process.
Multiplanar reconstruction (MPR) and 3D transesophageal echocardiography (3DTOE) are indispensable tools in accurately measuring these parameters and ensuring favorable anatomy and procedural outcomes. Anatomical criteria are presented in Table 2.
6. Implications for Clinical Practice
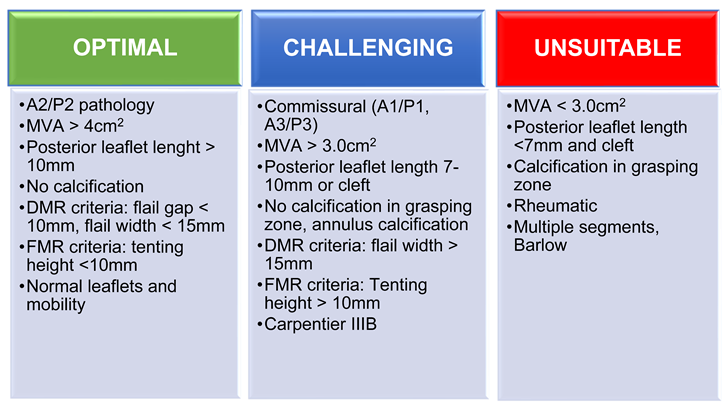
Low-volume centers should begin with central jets, located to the A2/P2 segments, with mitral valve area (MVA) above 4cm2, with posterior leaflet length above 10mm and no calcification in the grasping zone [34]. For degenerative MR, flail gap should be below 10mm and for secondary MR the tenting height should not exceed 10mm for beginners’ cases. Commissural jets (A1/P1, A3/P3) represent more challenging anatomies, as well as MVA 3.0-4.0cm2, posterior leaflet length 7-10mm or cleft and presence of annulus calcification. High-volume centers and experienced teams should treat complex cases such as patients with MVA < 3.0cm2, posterior leaflet length <7mm and cleft, calcification in grasping zone, Carpentier IIIb and Barlow disease with multiple segments prolapsing after case by case analysis by an experienced Heart Team [34]. However, there are some limitations of the method even for experienced centers: red-unsuitable cases might need transcatheter annuloplasty or even transcatheter MV replacement.
7. Preprocedural Echocardiographic Assessment
Comprehensive echocardiographic assessment is the cornerstone of transcatheter edge-to-edge repair (TEER) planning. In both primary mitral regurgitation (PMR) and secondary mitral regurgitation (SMR), accurate anatomical characterization informs feasibility and procedural strategy. Preprocedural imaging should systematically evaluate leaflet anatomy, valve area, and coaptation geometry. This section focuses on essential 2D and 3D transesophageal echocardiography (TEE) views, with emphasis on reproducible measurements relevant to patient selection and procedural success.
7.1. Mitral Valve Anatomy
The mid-esophageal commissural TOE view allows for precise segmentation of mitral valve anatomy and identification of different scallops. The use of biplane imaging and scanning from lateral to medial commissure, allows localization of mitral valve pathology between different scallops of the anterior and posterior leaflet. Additionally, the 3D “en face” render view provides a “surgeon’s view” for intuitive localization of A1–P1, A2–P2, and A3–P3 scallops, as seen in Figure 4. For correct orientation into the dataset, two landmarks are used for biplane and 3D evaluation of MV; the aortic valve and the left atrial appendage (LAA). In biplane imaging, the lateral part of the valve is close to the left atrial appendage while the medial part is on the other side. 3D “Surgeon’s” view requires an aortic valve position at 12 o’ clock and LAA at the left side of the screen in an atrial perspective of the valve. That way we can easily distinguish what is lateral-medial, anterior and posterior.
7.2. Posterior Leaflet Length
7.3. Mitral Valve Area and Gradient
Planimetric MVA should exceed 4.0 cm² to avoid post-procedural mitral stenosis since TEER in general reduces the MVA by 50% (Figure 6A). The mean gradient should also be recorded at baseline (Figure 6B) with a cut-off value >4mmHg to be considered as a predictor for post-operative stenosis. Valve area between 3.0–4.0 cm² is considered acceptable but requires caution, while <3.0 cm² is considered as unsuitable for M-TEER. [35]
7.4. Flail Gap and Width (PMR)
7.5. Tenting Height and Coaptation Length (SMR)
Coaptation depth or tenting height, coaptation length and coaptation gap are additional parameters that have to be evaluated in secondary MR (Figure 8). These reflect leaflet tethering from LV remodeling. A tenting height <10 mm and coaptation length > 2mm predict better leaflet approximation by M-TEER.
8. Anatomical Challenges
-
Posterior Leaflet Cleft-like IndentationThe posterior leaflet normally has two indentations that differentiate the scallops. A cleft-like indentation is defined as having a depth of at least 50% of the adjacent scallops [37,38] and 3D imaging is the best option to recognize such abnormalities (Figure 9). This feature makes grasping challenging and may lead to residual mitral regurgitation (MR).
-
Leaflet and Annular Calcification
-
Adequate but Tethered LeafletsPosterior leaflet length may be sufficient, but severe tethering reduces coaptation and grasping success (Figure 11).
9. Intraprocedural Guidance
9.1. Transseptal Puncture
The transseptal puncture is an essential step in the M-TEER procedure (Figure 12). When done correctly, it facilitates access and alignment for device delivery, streamlining the procedure. However, if not performed accurately, it can induce challenges that complicate the procedure. Precision at this stage is key to ensuring procedural success.
Different mitral valve pathologies and target segments necessitate specific transseptal puncture locations to optimize access and alignment. A superior and posterior puncture at approximately 4 cm serves as the default strategy.[40] (Figure 12 and Figure 13).
However, adjustments are required based on the targeted segment (Figure 14):
- Lateral commissure: A superior and lower puncture height, approximately 3.5 cm, is preferred to facilitate access.[40]
- Medial commissure: A more inferior puncture, closer to the inferior vena cava (IVC), with a higher height of 4.5–5 cm is recommended for better alignment. [41]
- Ventricular functional MR: The puncture height should be set 1 cm lower than the usual height to match the coaptation depth.[40]
9.2. Navigating the Device
Echocardiographic guidance of the device towards the mitral valve requires simultaneous use of commissural and long-axis TOE views in order to target the anterior-posterior and medial-lateral part of the valve. Biplane imaging or live 3D guidance with MPR can provide all the necessary information for this step of the procedure. (Figure 15). The device is advanced towards the mitral valve that way and this approach optimizes alignment and minimizes the risk of injury of neighboring structures.
9.3. Device Alignment and Implantation
Visualizing both device arms in the long-axis view (mid-esophageal 135°) is not a definitive confirmation but can serve as a rough predictor of good alignment. Device alignment is more accurately assessed using 3D imaging, which provides a clear perspective of the device’s orientation in relation to the coaptation line. Proper alignment should be perpendicular to the coaptation line (Figure 16). Before advancing the device into the left ventricle (LV), it is essential to test the functionality of the grippers to ensure they are working properly and to understand which knob operates each gripper (Figure 17). Device perpendicularity is reevaluated after crossing mitral valve, as seen in (Figure 18).
9.4. Leaflet Grasping
Inadequate leaflet grasping can result in leaflet detachment, posing significant challenges. During M-TEER procedures, simultaneous grasping is the standard method used to capture both leaflets concurrently. If the initial capture is suboptimal, leaflet optimization is performed by reopening the gripper on the affected side to recapture the compromised leaflet. It is crucial to maintain the clip's orientation during these adjustments, as even minor twisting can create excessive tension and increase the risk of leaflet injury or tear. Although independent grasping, where each leaflet is captured individually, is available, it is rarely used due to the risk of clip twisting and the associated complications. [42] Precise adjustments are critical to achieving optimal outcomes while minimizing the likelihood of complications (Figure 19)
9.5. Device Deployment and Release
Prior to releasing the device, it is critical to assess both the severity and location of any residual mitral regurgitation (MR). Identifying whether the residual jet is medial or lateral helps understand if an additional device is needed and where it should be implanted. Equally important is confirming that the mitral mean gradient remains within acceptable limits, as significant iatrogenic mitral stenosis might occur. This is generally defined by a mitral valve area (MVA) ≥1.5 cm² and a mean transmitral gradient < 5 mmHg (Figure 20).[43]
In degenerative MR (DMR), special attention should be given to the underlying leaflet pathology, such as flail or prolapse. Regardless of the residual MR severity, correcting the primary anatomical defect is essential in order to stabilize the valve structure and minimize the risk of future device detachment. Thus, device placement should be guided by anatomical leaflet correction, rather than residual jet severity alone (Figure 21).
Following device deployment, a successful outcome is typically defined by a reduction in MR severity to trace or mild levels. According to the Mitral Valve Academic Research Consortium (MVARC) criteria, an optimal result corresponds to post-procedural MR of none or trace, while an acceptable result involves at least a one-grade reduction from baseline MR severity (e.g., from severe to moderate).[43] Doppler measurements, including mitral gradient and valve area, should be interpreted within the context of the patient’s hemodynamic status, as systemic hypotension can underestimate MR severity by reducing driving force across the regurgitant orifice and suppressing the color Doppler jet appearance.
Additional echocardiographic findings provide further confirmation of successful MR reduction. The resolution of systolic flow reversal in the pulmonary veins suggests effective decompression of left atrial pressure [44], while the presence of spontaneous echo contrast (SEC) in the left atrium after clip placement indicates flow stagnation and confirms significant MR reduction. [45]
Before the procedure is considered complete, the device's stability must be confirmed. If rocking or malposition is noted, additional device implantation may be necessary[46], provided the mitral valve area, gradient, and leaflet quality are still suitable for further intervention. A stable device not only ensures immediate success, but also reduces the risk of complications such as subacute device detachment. [46]
10. Conclusions
Mitral Transcatheter Edge-to-Edge Repair (M-TEER) has significantly advanced the treatment of mitral regurgitation (MR), combining theoretical insights with clinical application. Its success depends on both precise procedural execution and careful patient selection. Echocardiography plays a central role by evaluating valve anatomy and ventricular remodeling, ensuring durable outcomes. By aligning imaging, patient characteristics, and technique, M-TEER transforms complex valve disease into a treatable condition, offering lasting improvement in patient care.
Author Contributions
“Conceptualization, K.P., A. Z., E.D.; writing—original draft preparation, K.P., A.Z., P.R., G.L., E.D.; writing—review and editing, K.P., I.I., A.Z., P.R., G.L, E.D.; supervision, K.P., I.I., E.D.; All authors have read and agreed to the published version of the manuscript.”.
Funding
“This research received no external funding”.
Data Availability Statement
All data supporting this article are available upon reasonable request.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
Abbreviations
The following abbreviations are used in this manuscript:
| AFMR | atrial functional MR |
| BTT | bridge-to-transplant |
| CRT | cardiac resynchronization therapy |
| DMR | degenerative mitral regurgitation |
| EROA | effective regurgitant orifice area |
| GDMT | guideline-directed medical therapy |
| HF | heart failure |
| IVC | inferior vena cava |
| LA | left atrium |
| LAVI | left atrial volume index |
| LV | left ventricle |
| LVAD | left ventricular assist device |
| LVEDV | left ventricular end-diastolic volume |
| LVEF | left ventricular ejection fraction |
| LVESD | left ventricular end-systolic diameter |
| MPR | multiplanar reconstruction |
| MR | mitral regurgitation |
| M-TEER | mitral transcatheter edge-to-edge repair |
| MV | mitral valve |
| MVA | mitral valve area |
| NYHA | New York Heart Association Class |
| PCI | percutaneous coronary intervention |
| PMR | primary mitral regurgitation |
| RF | regurgitant fraction |
| RVol | regurgitant volume |
| SMR | secondary mitral regurgitation |
| SPAP | systolic pulmonary artery pressure |
| TAVI | transcatheter aortic valve implantation |
| TEE/TOE | transesophageal echocardiography |
| TR | tricuspid regurgitation |
| VC | vena contracta |
References
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. The Lancet. 2006;368(9540):1005-11. [CrossRef]
- Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Bärwolf C, Levang OW, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. European Heart Journal. 2003;24(13):1231-43.
- Zoghbi William A, Levine Robert A, Flachskampf F, Grayburn P, Gillam L, Leipsic J, et al. Atrial Functional Mitral Regurgitation. JACC: Cardiovascular Imaging. 2022;15(11):1870-82.
- Prakash R, Horsfall M, Markwick A, Pumar M, Lee L, Sinhal A, et al. Prognostic impact of moderate or severe mitral regurgitation (MR) irrespective of concomitant comorbidities: a retrospective matched cohort study. BMJ Open. 2014;4(7):e004984. [CrossRef]
- Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet. 2009;373(9672):1382-94.
- Sannino A, Smith RL, 2nd, Schiattarella GG, Trimarco B, Esposito G, Grayburn PA. Survival and Cardiovascular Outcomes of Patients With Secondary Mitral Regurgitation: A Systematic Review and Meta-analysis. JAMA Cardiol. 2017;2(10):1130-9.
- Zoghbi WA, Adams D, Bonow RO, Enriquez-Sarano M, Foster E, Grayburn PA, et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. Journal of the American Society of Echocardiography. 2017;30(4):303-71.
- Grayburn PA. How to measure severity of mitral regurgitation: valvular heart disease. Heart. 2008;94(3):376-83.
- Lancellotti P, Pibarot P, Chambers J, La Canna G, Pepi M, Dulgheru R, et al. Multi-modality imaging assessment of native valvular regurgitation: an EACVI and ESC council of valvular heart disease position paper. Eur Heart J Cardiovasc Imaging. 2022;23(5):e171-e232. [CrossRef]
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal. 2021;43(7):561-632. [CrossRef]
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021;77(4):e25-e197.
- Enriquez-Sarano M, Avierinos JF, Messika-Zeitoun D, Detaint D, Capps M, Nkomo V, et al. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N Engl J Med. 2005;352(9):875-83. [CrossRef]
- Bartko PE, Arfsten H, Heitzinger G, Pavo N, Toma A, Strunk G, et al. A Unifying Concept for the Quantitative Assessment of Secondary Mitral Regurgitation. J Am Coll Cardiol. 2019;73(20):2506-17.
- Bertrand PB, Schwammenthal E, Levine RA, Vandervoort PM. Exercise Dynamics in Secondary Mitral Regurgitation: Pathophysiology and Therapeutic Implications. Circulation. 2017;135(3):297-314.
- Onishi H, Izumo M, Naganuma T, Nakamura S, Akashi YJ. Dynamic Secondary Mitral Regurgitation: Current Evidence and Challenges for the Future. Front Cardiovasc Med. 2022;9:883450. [CrossRef]
- Goldstein D, Moskowitz Aj Fau - Gelijns AC, Gelijns Ac Fau - Ailawadi G, Ailawadi G Fau - Parides MK, Parides Mk Fau - Perrault LP, Perrault Lp Fau - Hung JW, et al. Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation. (1533-4406 (Electronic)).
- Baldus S, Doenst T, Pfister R, Gummert J, Kessler M, Boekstegers P, et al. Transcatheter Repair versus Mitral-Valve Surgery for Secondary Mitral Regurgitation. New England Journal of Medicine. 2024;391(19):1787-98. [CrossRef]
- Mack MJ, Abraham WT, Lindenfeld J, Bolling SF, Feldman TE, Grayburn PA, et al. Cardiovascular Outcomes Assessment of the MitraClip in Patients with Heart Failure and Secondary Mitral Regurgitation: Design and rationale of the COAPT trial. American Heart Journal. 2018;205:1-11. [CrossRef]
- Ponikowski P, Friede T, von Bardeleben RS, Butler J, Shahzeb Khan M, Diek M, et al. Hospitalization of Symptomatic Patients With Heart Failure and Moderate to Severe Functional Mitral Regurgitation Treated With MitraClip: Insights From RESHAPE-HF2. J Am Coll Cardiol. 2024;84(24):2347-63.
- Obadia J-F, Messika-Zeitoun D, Leurent G, Iung B, Bonnet G, Piriou N, et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. New England Journal of Medicine. 2018;379(24):2297-306. [CrossRef]
- Feldman T, Foster E, Glower DD, Kar S, Rinaldi MJ, Fail PS, et al. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med. 2011;364(15):1395-406.
- Grayburn PA, Sannino A, Packer M. Proportionate and Disproportionate Functional Mitral Regurgitation: A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials. JACC Cardiovasc Imaging. 2019;12(2):353-62.
- Namazi F, van der Bijl P, Fortuni F, Mertens BJA, Kamperidis V, van Wijngaarden SE, et al. Regurgitant Volume/Left Ventricular End-Diastolic Volume Ratio: Prognostic Value in Patients With Secondary Mitral Regurgitation. JACC Cardiovasc Imaging. 2021;14(4):730-9.
- Berrill M, Beeton I, Fluck D, John I, Lazariashvili O, Stewart J, et al. Disproportionate Mitral Regurgitation Determines Survival in Acute Heart Failure. Front Cardiovasc Med. 2021;8:742224. [CrossRef]
- Anker SD, Friede T, von Bardeleben RS, Butler J, Khan MS, Diek M, et al. Percutaneous repair of moderate-to-severe or severe functional mitral regurgitation in patients with symptomatic heart failure: Baseline characteristics of patients in the RESHAPE-HF2 trial and comparison to COAPT and MITRA-FR trials. (1879-0844 (Electronic)).
- Anker SD, Friede T, von Bardeleben RS, Butler J, Khan MS, Diek M, et al. Transcatheter Valve Repair in Heart Failure with Moderate to Severe Mitral Regurgitation. N Engl J Med. 2024;391(19):1799-809. [CrossRef]
- Asgar AW, Tang GHL, Rogers JH, Rottbauer W, Morse MA, Denti P, et al. Evaluating Mitral TEER in the Management of Moderate Secondary Mitral Regurgitation Among Heart Failure Patients. (2213-1787 (Electronic)).
- Giannini C, Petronio As Fau - De Carlo M, De Carlo M Fau - Guarracino F, Guarracino F Fau - Conte L, Conte L Fau - Fiorelli F, Fiorelli F Fau - Pieroni A, et al. Integrated reverse left and right ventricular remodelling after MitraClip implantation in functional mitral regurgitation: an echocardiographic study. (2047-2412 (Electronic)).
- Scandura S, Ussia Gp Fau - Capranzano P, Capranzano P Fau - Caggegi A, Caggegi A Fau - Sarkar K, Sarkar K Fau - Cammalleri V, Cammalleri V Fau - Mangiafico S, et al. Left cardiac chambers reverse remodeling after percutaneous mitral valve repair with the MitraClip system. (1097-6795 (Electronic)).
- Papadopoulos K, Ikonomidis I, Chrissoheris M, Chalapas A, Kourkoveli P, Parissis J, et al. MitraClip and left ventricular reverse remodelling: a strain imaging study. (2055-5822 (Electronic)).
- Citro R, Baldi C, Lancellotti P, Silverio A, Provenza G, Bellino M, et al. Global longitudinal strain predicts outcome after MitraClip implantation for secondary mitral regurgitation. Journal of Cardiovascular Medicine. 2017;18(9). [CrossRef]
- Godino C, Munafò A, Scotti A, Estévez-Loureiro R, Portolés Hernández A, Arzamendi D, et al. MitraClip in secondary mitral regurgitation as a bridge to heart transplantation: 1-year outcomes from the International MitraBridge Registry. J Heart Lung Transplant. 2020;39(12):1353-62. [CrossRef]
- Jung RG, Simard T, Kovach C, Flint K, Don C, Di Santo P, et al. Transcatheter Mitral Valve Repair in Cardiogenic Shock and Mitral Regurgitation: A Patient-Level, Multicenter Analysis. JACC Cardiovasc Interv. 2021;14(1):1-11.
- Gavazzoni M, Taramasso M, Zuber M, Russo G, Pozzoli A, Miura M, et al. Conceiving MitraClip as a tool: percutaneous edge-to-edge repair in complex mitral valve anatomies. Eur Heart J Cardiovasc Imaging. 2020;21(10):1059-67. [CrossRef]
- Boekstegers P, Hausleiter J, Baldus S, von Bardeleben RS, Beucher H, Butter C, et al. Percutaneous interventional mitral regurgitation treatment using the Mitra-Clip system. Clin Res Cardiol. 2014;103(2):85-96. [CrossRef]
- Adamo M, Chiari E, Curello S, Maiandi C, Chizzola G, Fiorina C, et al. Mitraclip therapy in patients with functional mitral regurgitation and missing leaflet coaptation: is it still an exclusion criterion? Eur J Heart Fail. 2016;18(10):1278-86.
- Ring L, Rana BS, Ho SY, Wells FC. The prevalence and impact of deep clefts in the mitral leaflets in mitral valve prolapse. Eur Heart J Cardiovasc Imaging. 2013;14(6):595-602. [CrossRef]
- La Canna G, Arendar I, Maisano F, Monaco F, Collu E, Benussi S, et al. Real-time three-dimensional transesophageal echocardiography for assessment of mitral valve functional anatomy in patients with prolapse-related regurgitation. Am J Cardiol. 2011;107(9):1365-74. [CrossRef]
- Praz F, Braun D, Unterhuber M, Spirito A, Orban M, Brugger N, et al. Edge-to-Edge Mitral Valve Repair With Extended Clip Arms: Early Experience From a Multicenter Observational Study. JACC Cardiovasc Interv. 2019;12(14):1356-65.
- Radinovic A, Mazzone P, Landoni G, Agricola E, Regazzoli D, Della-Bella P. Different transseptal puncture for different procedures: Optimization of left atrial catheterization guided by transesophageal echocardiography. Ann Card Anaesth. 2016;19(4):589-93. [CrossRef]
- Harb SC, Cohen JA, Krishnaswamy A, Kapadia SR, Miyasaka RL. Targeting the Future: Three-Dimensional Imaging for Precise Guidance of the Transseptal Puncture. Struct Heart. 2025;9(1):100340. [CrossRef]
- Hausleiter J, Stocker TJ, Adamo M, Karam N, Swaans MJ, Praz F. Mitral valve transcatheter edge-to-edge repair. EuroIntervention. 2023;18(12):957-76. [CrossRef]
- Stone GW, Adams DH, Abraham WT, Kappetein AP, Généreux P, Vranckx P, et al. Clinical Trial Design Principles and Endpoint Definitions for Transcatheter Mitral Valve Repair and Replacement: Part 2: Endpoint Definitions: A Consensus Document From the Mitral Valve Academic Research Consortium. J Am Coll Cardiol. 2015;66(3):308-21.
- El Shaer A, Chavez Ponce AA, Ali MT, Oguz D, Pislaru SV, Nkomo VT, et al. Pulmonary Vein Flow Morphology After Transcatheter Mitral Valve Edge-to-Edge Repair as Predictor of Survival. J Am Soc Echocardiogr. 2024;37(5):530-7.
- Sato H, Cavalcante JL, Enriquez-Sarano M, Bae R, Fukui M, Bapat VN, et al. Significance of Spontaneous Echocardiographic Contrast in Transcatheter Edge-to-Edge Repair for Mitral Regurgitation. J Am Soc Echocardiogr. 2023;36(1):87-95. [CrossRef]
- Maisano F, Franzen O, Baldus S, Schäfer U, Hausleiter J, Butter C, et al. Percutaneous mitral valve interventions in the real world: early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J Am Coll Cardiol. 2013;62(12):1052-61.
Figure 1.
(A, B, C): Primary MR with multiscallop prolapse and diffusely thickened leaflets (Barlow disease). (D, E, F): Primary MR with P3 prolapse, thin leaflets and chordal rupture (Fibroelastic deficiency).
Figure 1.
(A, B, C): Primary MR with multiscallop prolapse and diffusely thickened leaflets (Barlow disease). (D, E, F): Primary MR with P3 prolapse, thin leaflets and chordal rupture (Fibroelastic deficiency).
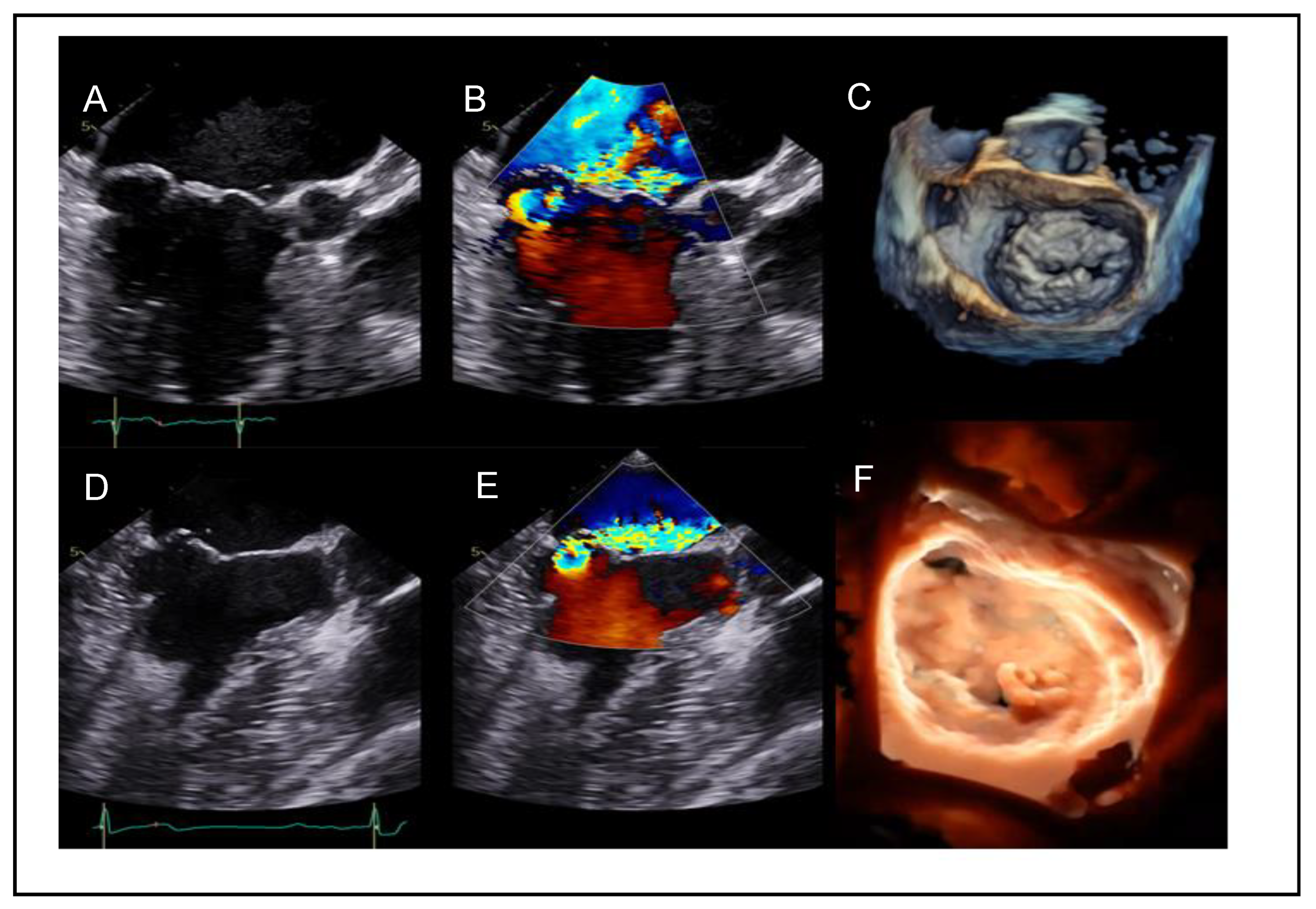
Figure 2.
Severe secondary ventricular MR in a patient with ischemic cardiomyopathy due to akinesia of the inferolateral and lateral wall.
Figure 2.
Severe secondary ventricular MR in a patient with ischemic cardiomyopathy due to akinesia of the inferolateral and lateral wall.
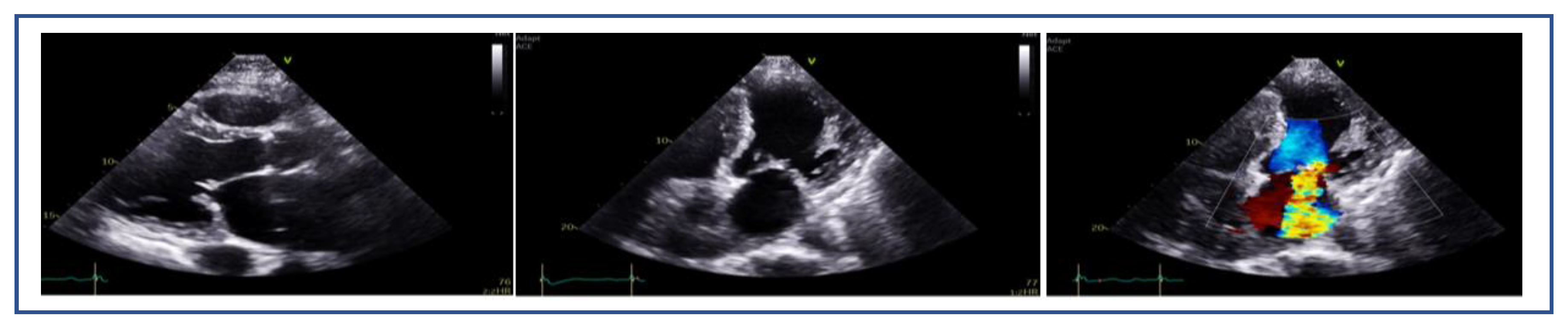
Figure 3.
Ischemic dynamic MR unmasked by exercise echocardiography in a 66-y.o. patient with ischemic cardiomyopathy (LVEF=25%) due to anterior infarct and exertional dyspnea NYHA III. (A): At rest, MR is mild, (B): whereas at 75 Watts the patient develops dyspnea upon aggravation of MR (EROA=0.41cm2, RVol=39ml) with significant elevation of pulmonary pressures (TR Vmax=4.0m/sec, TR PeakPG=65mmHg, estimated SPAP=70mmHg).
Figure 3.
Ischemic dynamic MR unmasked by exercise echocardiography in a 66-y.o. patient with ischemic cardiomyopathy (LVEF=25%) due to anterior infarct and exertional dyspnea NYHA III. (A): At rest, MR is mild, (B): whereas at 75 Watts the patient develops dyspnea upon aggravation of MR (EROA=0.41cm2, RVol=39ml) with significant elevation of pulmonary pressures (TR Vmax=4.0m/sec, TR PeakPG=65mmHg, estimated SPAP=70mmHg).
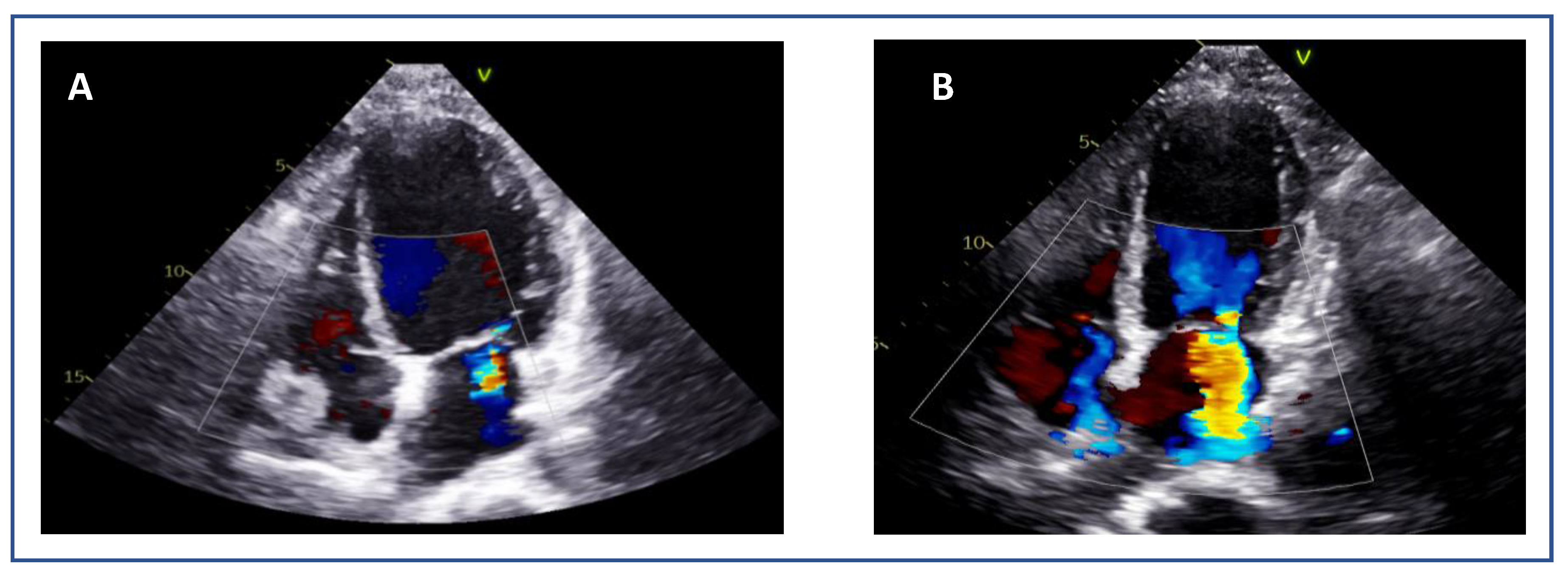
Figure 4.
Segmental assessment of the mitral valve. (A): Mid-esophageal commissural view with biplane imaging allows systematic segmentation from the lateral commissure (noted by the left atrial appendage). (B–D): Biplane cuts demonstrate sequential leaflet scallops: A1–P1 (red line, B), A2–P2 (yellow line, C), and A3–P3 (green line, D). (E): Three-dimensional “en face” view of the mitral valve from the left atrial perspective provides comprehensive anatomical context and spatial orientation of scallops.
Figure 4.
Segmental assessment of the mitral valve. (A): Mid-esophageal commissural view with biplane imaging allows systematic segmentation from the lateral commissure (noted by the left atrial appendage). (B–D): Biplane cuts demonstrate sequential leaflet scallops: A1–P1 (red line, B), A2–P2 (yellow line, C), and A3–P3 (green line, D). (E): Three-dimensional “en face” view of the mitral valve from the left atrial perspective provides comprehensive anatomical context and spatial orientation of scallops.
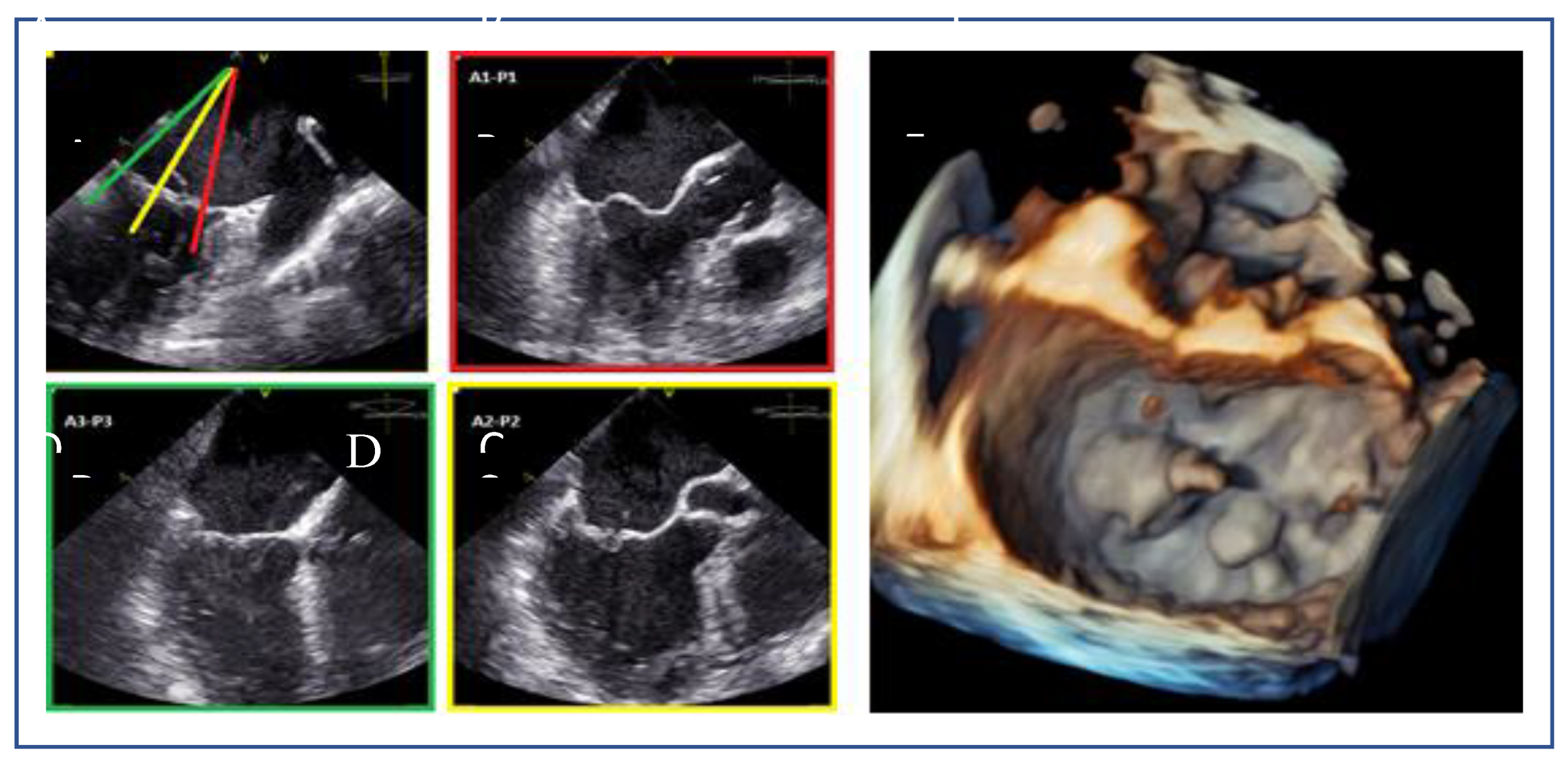
Figure 5.
(A): Posterior leaflet length measurement using 2D and (B): Multiplanar reconstruction (MPR) at grasping zone.
Figure 5.
(A): Posterior leaflet length measurement using 2D and (B): Multiplanar reconstruction (MPR) at grasping zone.
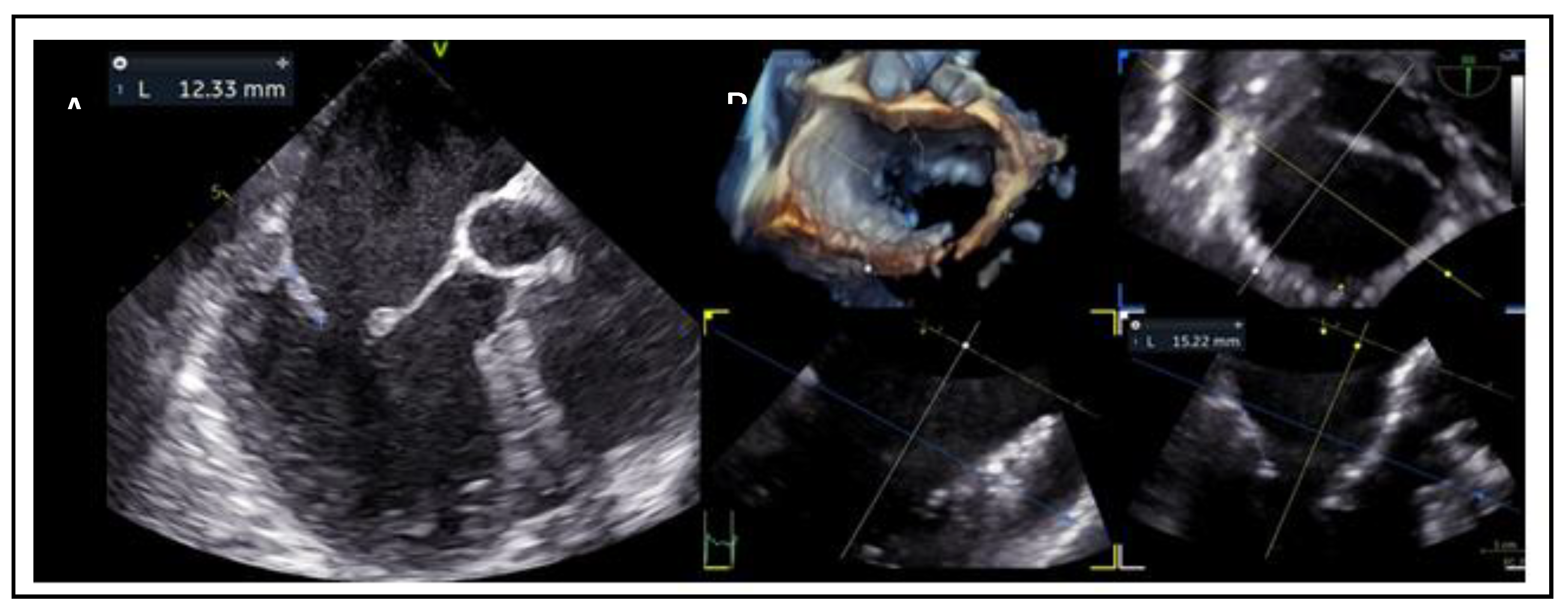
Figure 6.
(A): Mitral valve area measurement using MPR. (B): Baseline mean mitral valve gradient using CW Doppler.
Figure 6.
(A): Mitral valve area measurement using MPR. (B): Baseline mean mitral valve gradient using CW Doppler.
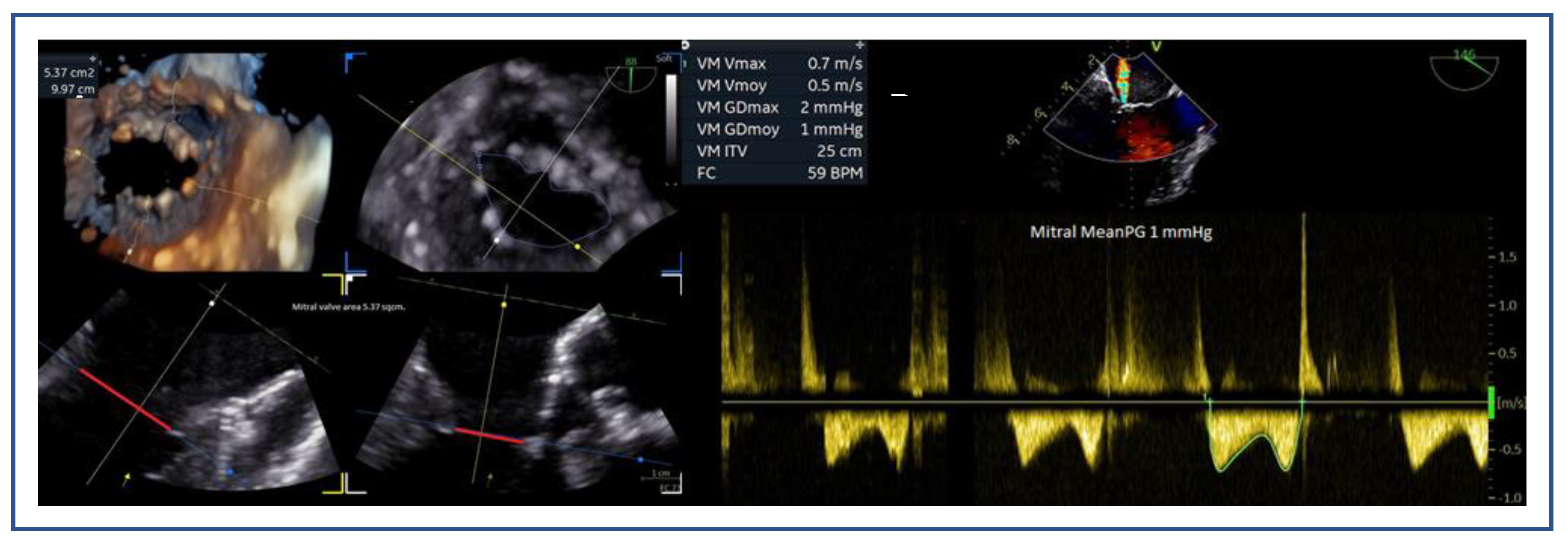
Figure 7.
(A, B): Measurement of flail width in Primary MR. (C, D): Measurement of flail gap.
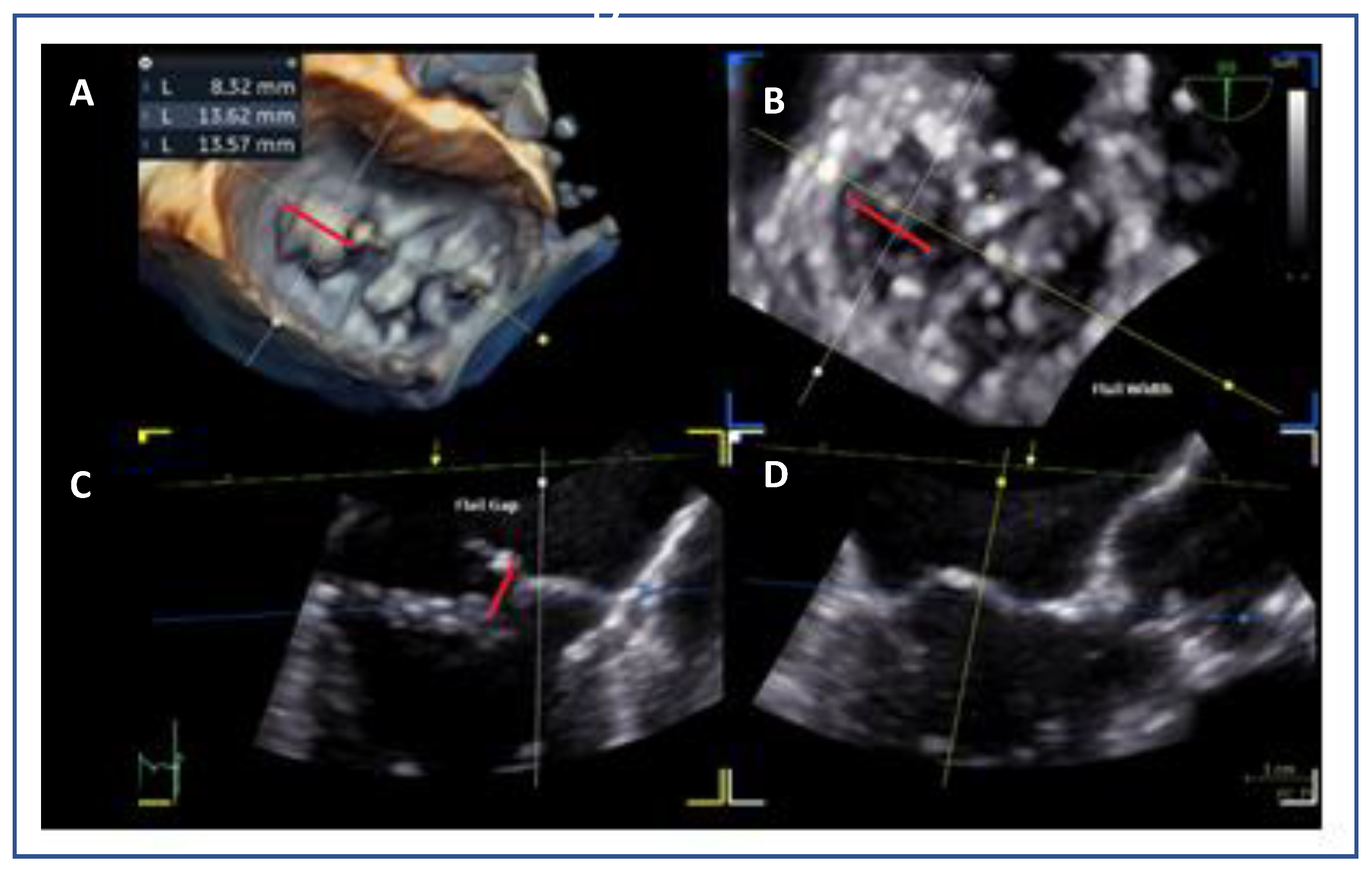
Figure 8.
(A): Measurement of coaptation depth (or tenting height) in secondary MR. (B): Measurement of coaptation length. (C): Measurement of coaptation gap.
Figure 8.
(A): Measurement of coaptation depth (or tenting height) in secondary MR. (B): Measurement of coaptation length. (C): Measurement of coaptation gap.
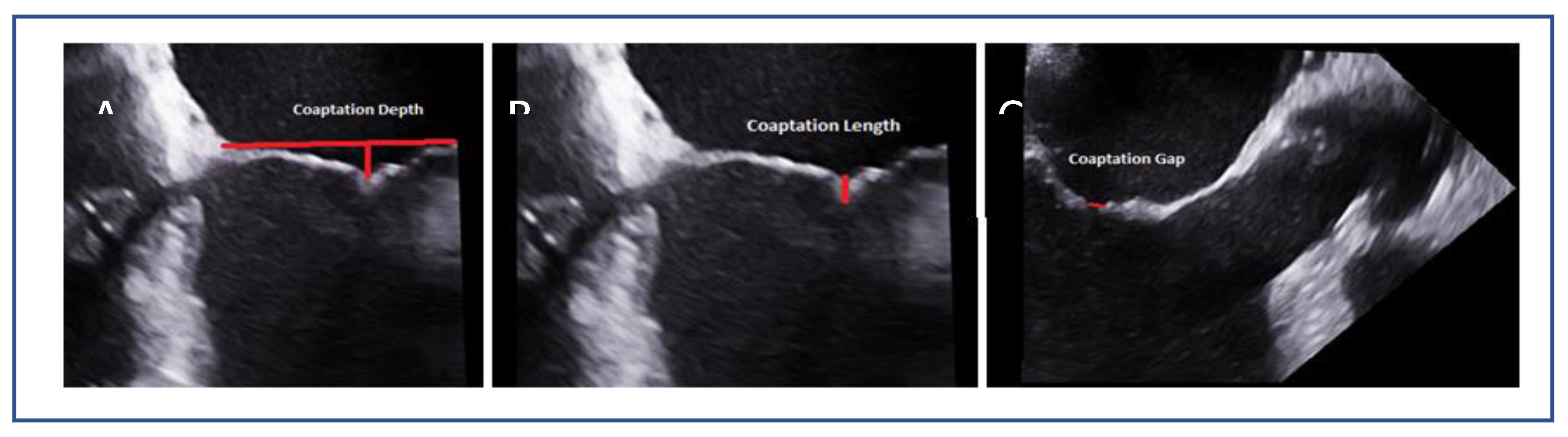
Figure 9.
3D “en face” mitral valve shows cleft-like indentation at the junction of the P2 and the P3 segment (A): atrial view or surgeon’s view and (B): ventricular view.
Figure 9.
3D “en face” mitral valve shows cleft-like indentation at the junction of the P2 and the P3 segment (A): atrial view or surgeon’s view and (B): ventricular view.
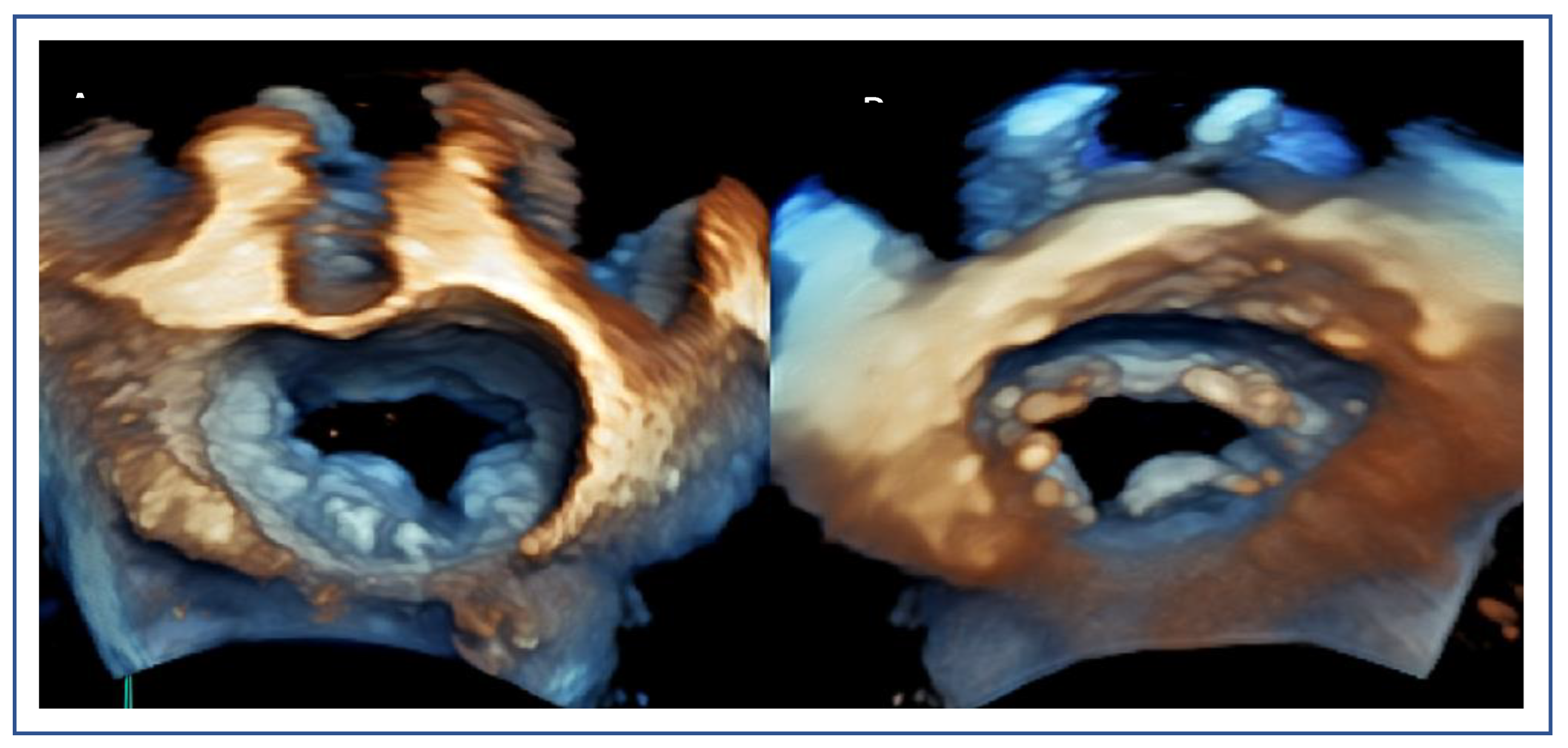
Figure 10.
(A): The posterior annulus is calcified and extended into the posterior leaflet, resulting in a shorter effective posterior leaflet for grasping in 2D image and (B): in 3D with multiplanar reconstruction.
Figure 10.
(A): The posterior annulus is calcified and extended into the posterior leaflet, resulting in a shorter effective posterior leaflet for grasping in 2D image and (B): in 3D with multiplanar reconstruction.
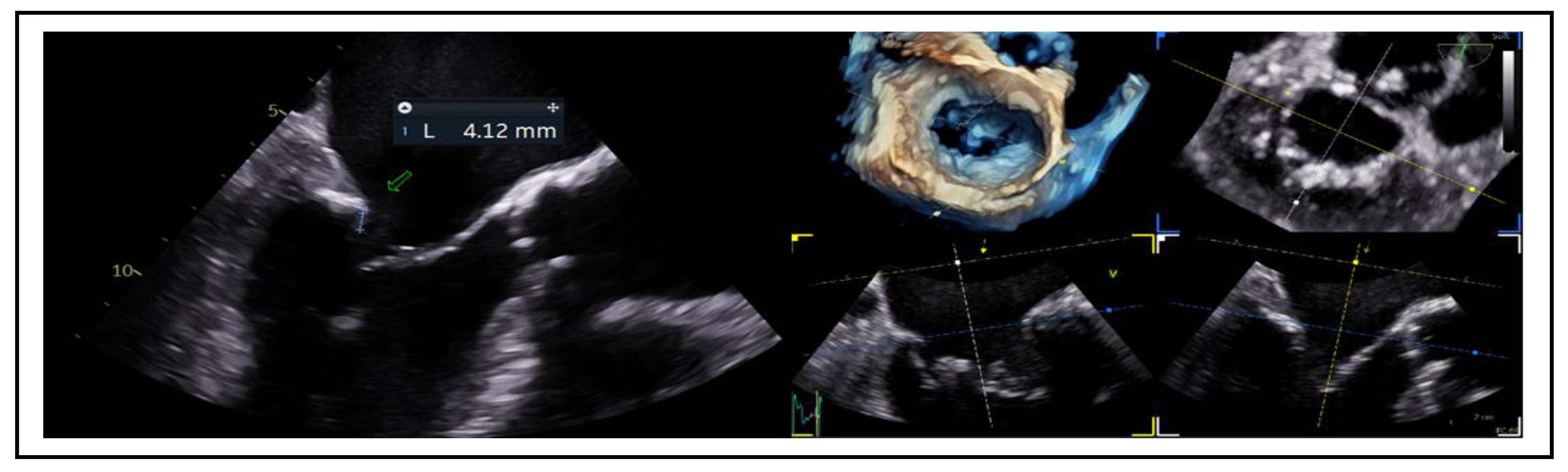
Figure 11.
Comparative assessment of posterior leaflet motion in (A): Systolic and (B): Diastolic phases. The posterior leaflet, indicated by a red arrow in both images, demonstrates a complete lack of movement throughout the cardiac cycle.
Figure 11.
Comparative assessment of posterior leaflet motion in (A): Systolic and (B): Diastolic phases. The posterior leaflet, indicated by a red arrow in both images, demonstrates a complete lack of movement throughout the cardiac cycle.
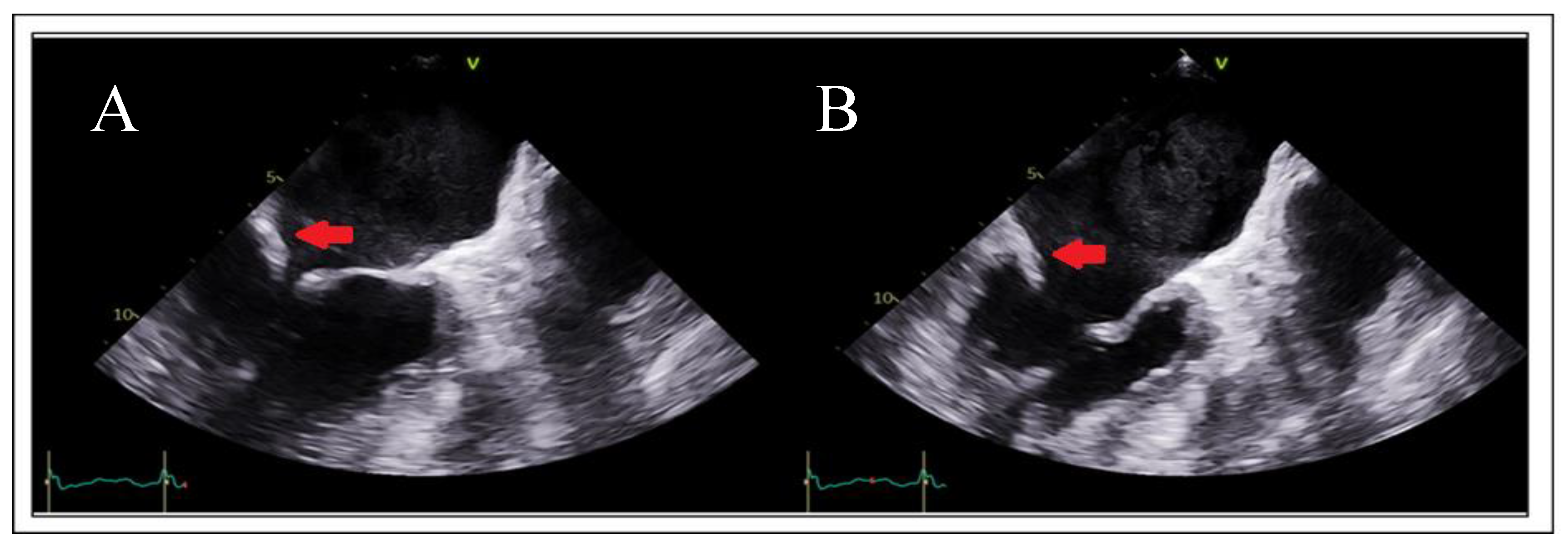
Figure 12.
(A): The circle represents optimal transseptal puncture site (superior and posterior) (B): Short axis view guides anterior (towards the aorta) or posterior position, (C): Bicaval view guides superior or inferior position, (D): 4-chamber view for measurement of puncture height from the level of annulus and (E): When the puncture site is positioned more superiorly than typically expected and the four-chamber view fails to adequately delineate both the puncture site and the annulus, a modified 135°–150° view is employed to optimize alignment, thereby enabling precise visualization and measurement.
Figure 12.
(A): The circle represents optimal transseptal puncture site (superior and posterior) (B): Short axis view guides anterior (towards the aorta) or posterior position, (C): Bicaval view guides superior or inferior position, (D): 4-chamber view for measurement of puncture height from the level of annulus and (E): When the puncture site is positioned more superiorly than typically expected and the four-chamber view fails to adequately delineate both the puncture site and the annulus, a modified 135°–150° view is employed to optimize alignment, thereby enabling precise visualization and measurement.
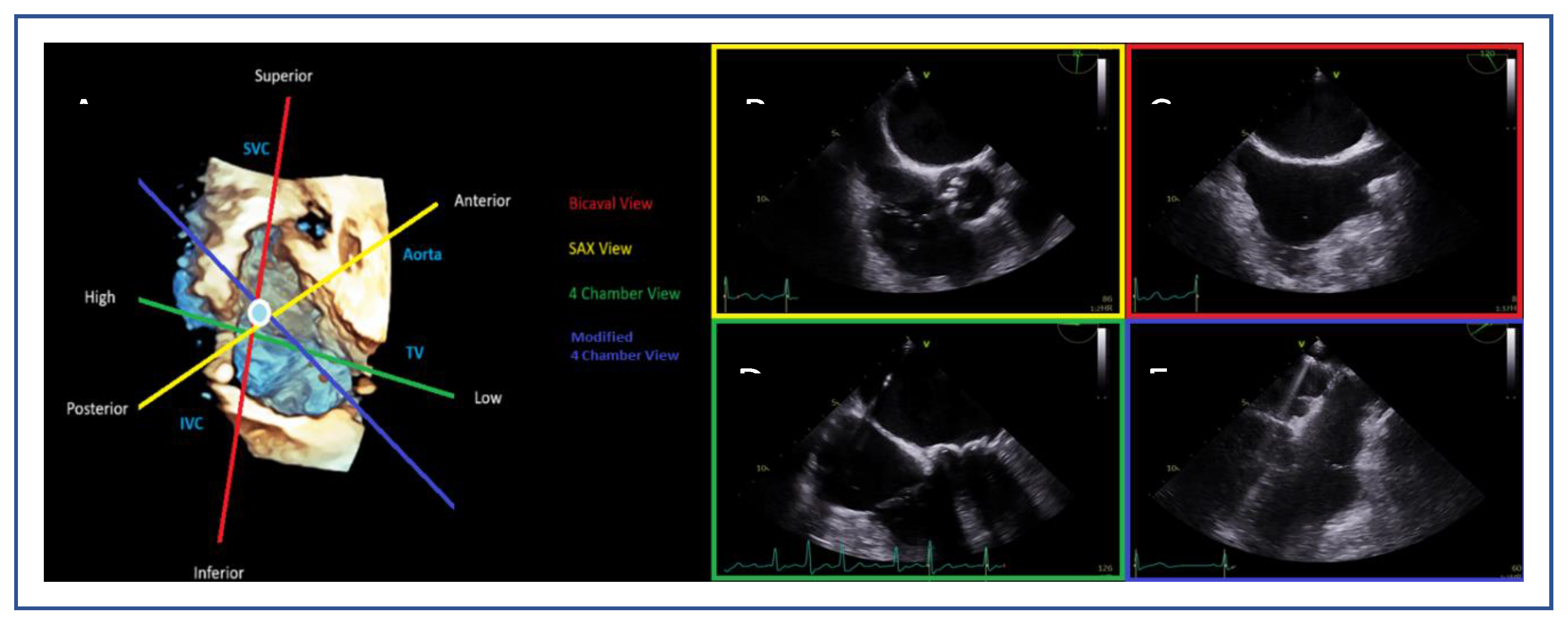
Figure 13.
Measurement of the height of transseptal puncture from the level of annulus.
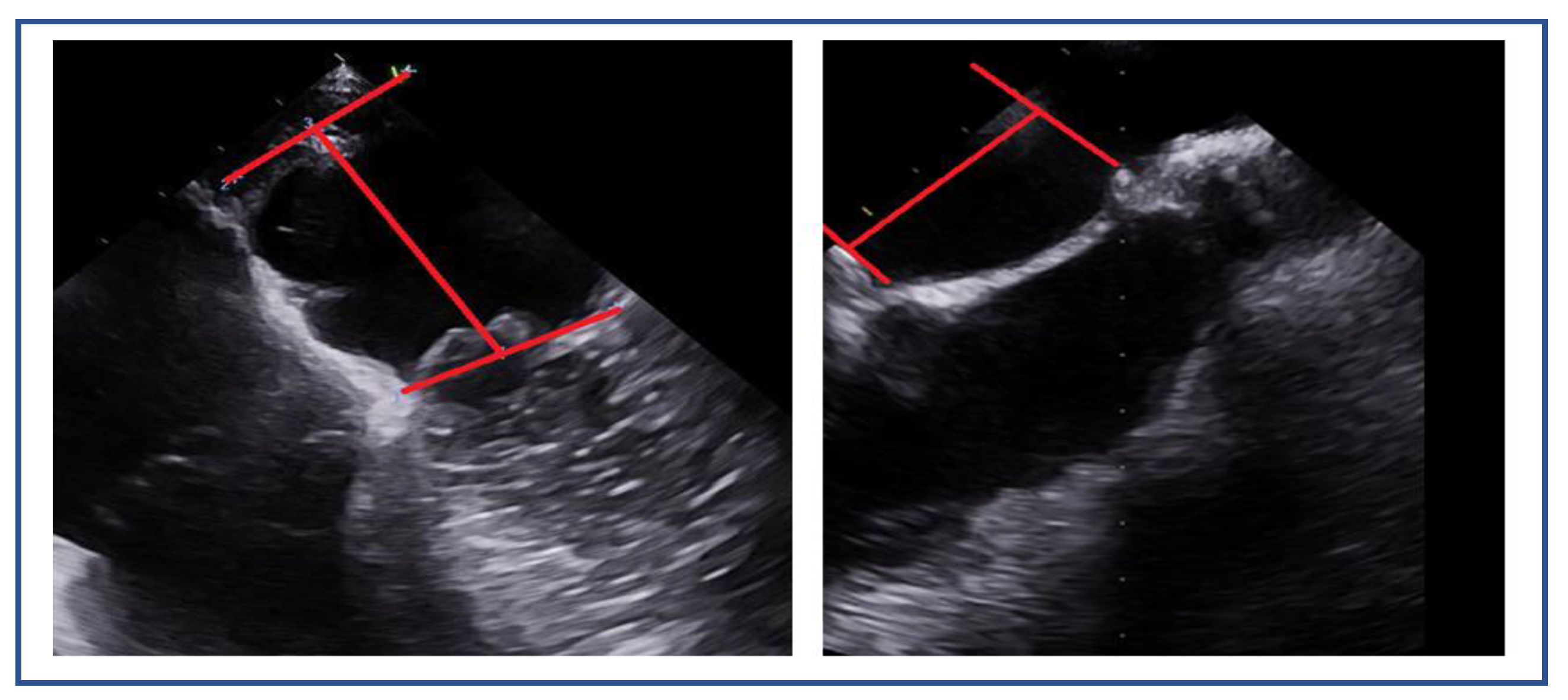
Figure 14.
Superior puncture position offers better alignment to the lateral commissure, whereas inferior puncture position offers better alignment to the medial commissure. These adjustments are crucial to tailoring the procedure based on the targeted segment and ensuring optimal outcomes.
Figure 14.
Superior puncture position offers better alignment to the lateral commissure, whereas inferior puncture position offers better alignment to the medial commissure. These adjustments are crucial to tailoring the procedure based on the targeted segment and ensuring optimal outcomes.
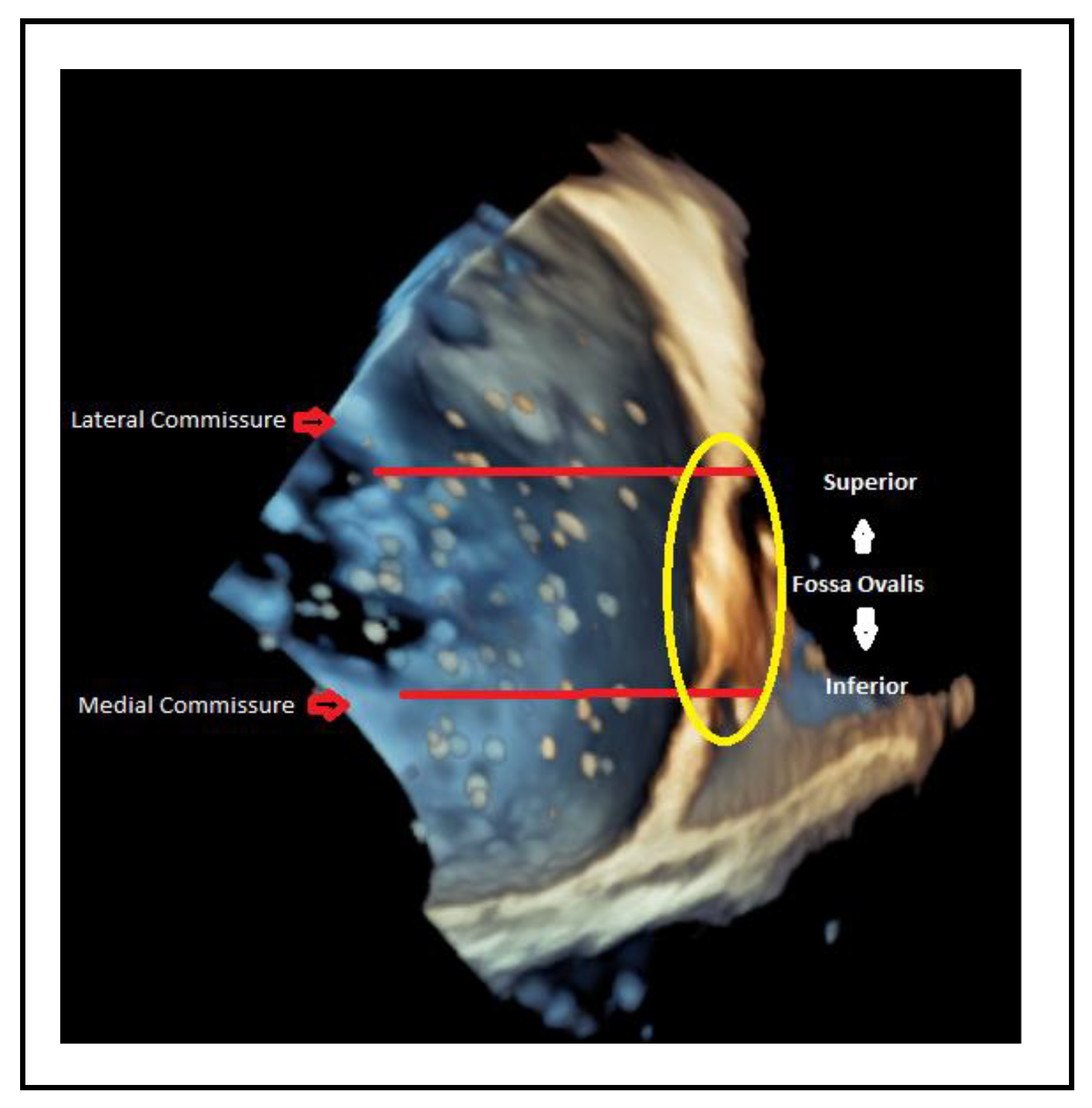
Figure 15.
(A, B): Navigating the guiding catheter and the device towards mitral valve. (C): Medial-lateral orientation (blue=lateral, green=medial). (D): Anterior-posterior orientation (red=anterior, yellow=posterior).
Figure 15.
(A, B): Navigating the guiding catheter and the device towards mitral valve. (C): Medial-lateral orientation (blue=lateral, green=medial). (D): Anterior-posterior orientation (red=anterior, yellow=posterior).
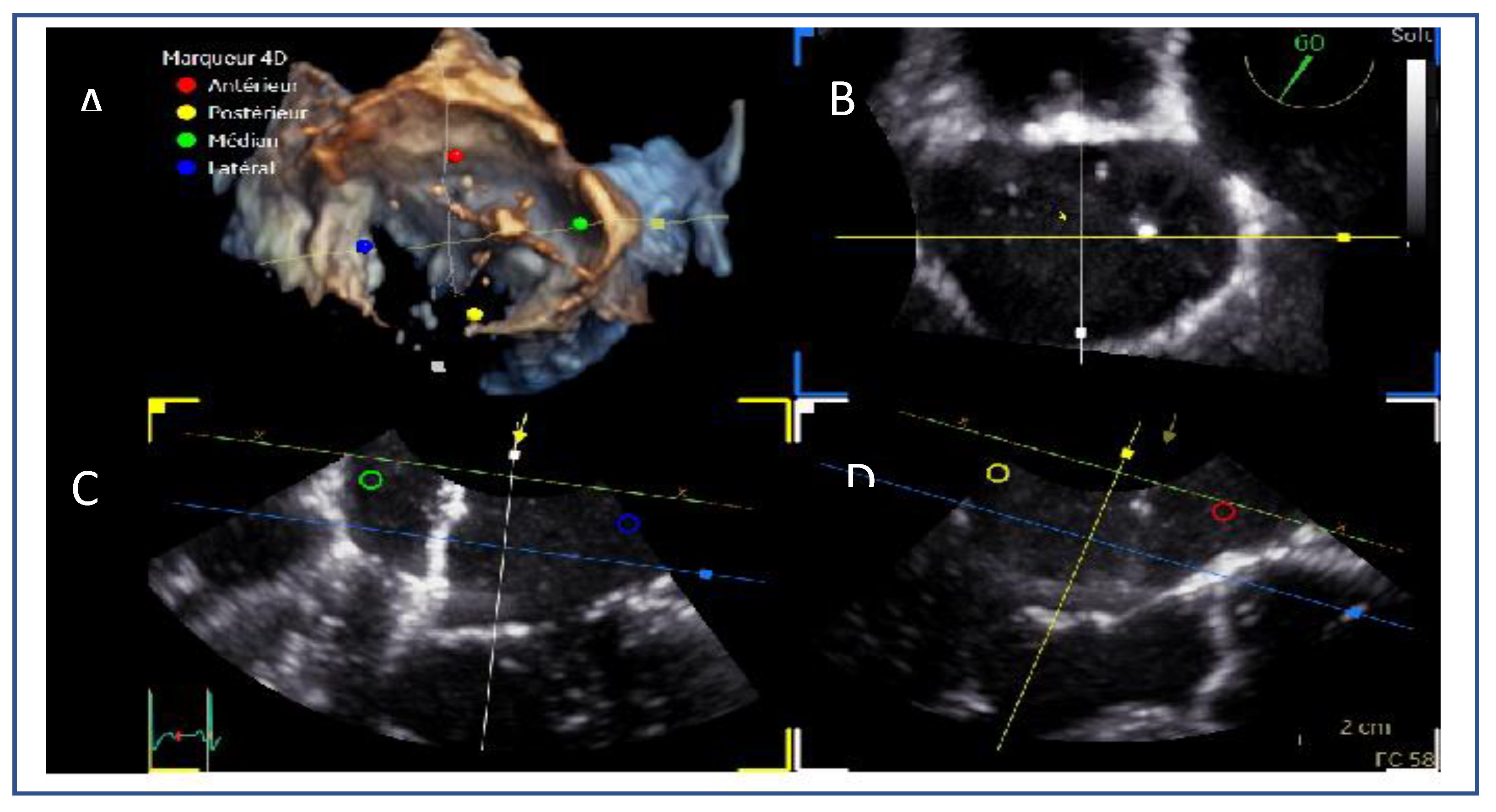
Figure 16.
Three-dimensional en face view of the mitral valve demonstrating device orientation. Perpendicular alignment is assessed prior to valve crossing to ensure optimal trajectory.
Figure 16.
Three-dimensional en face view of the mitral valve demonstrating device orientation. Perpendicular alignment is assessed prior to valve crossing to ensure optimal trajectory.
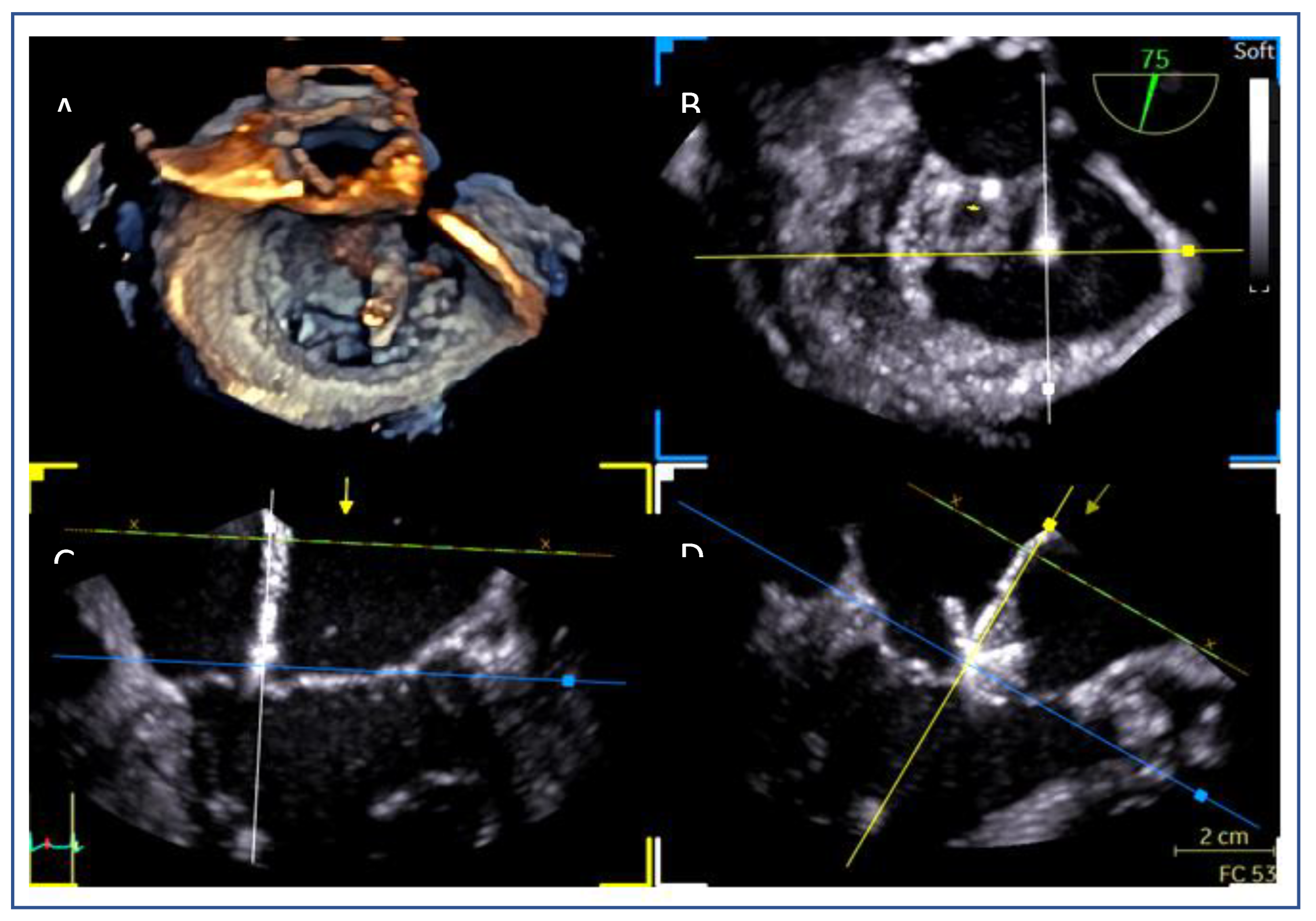
Figure 17.
Testing the grippers (indicated by red arrow) to ensure proper function.
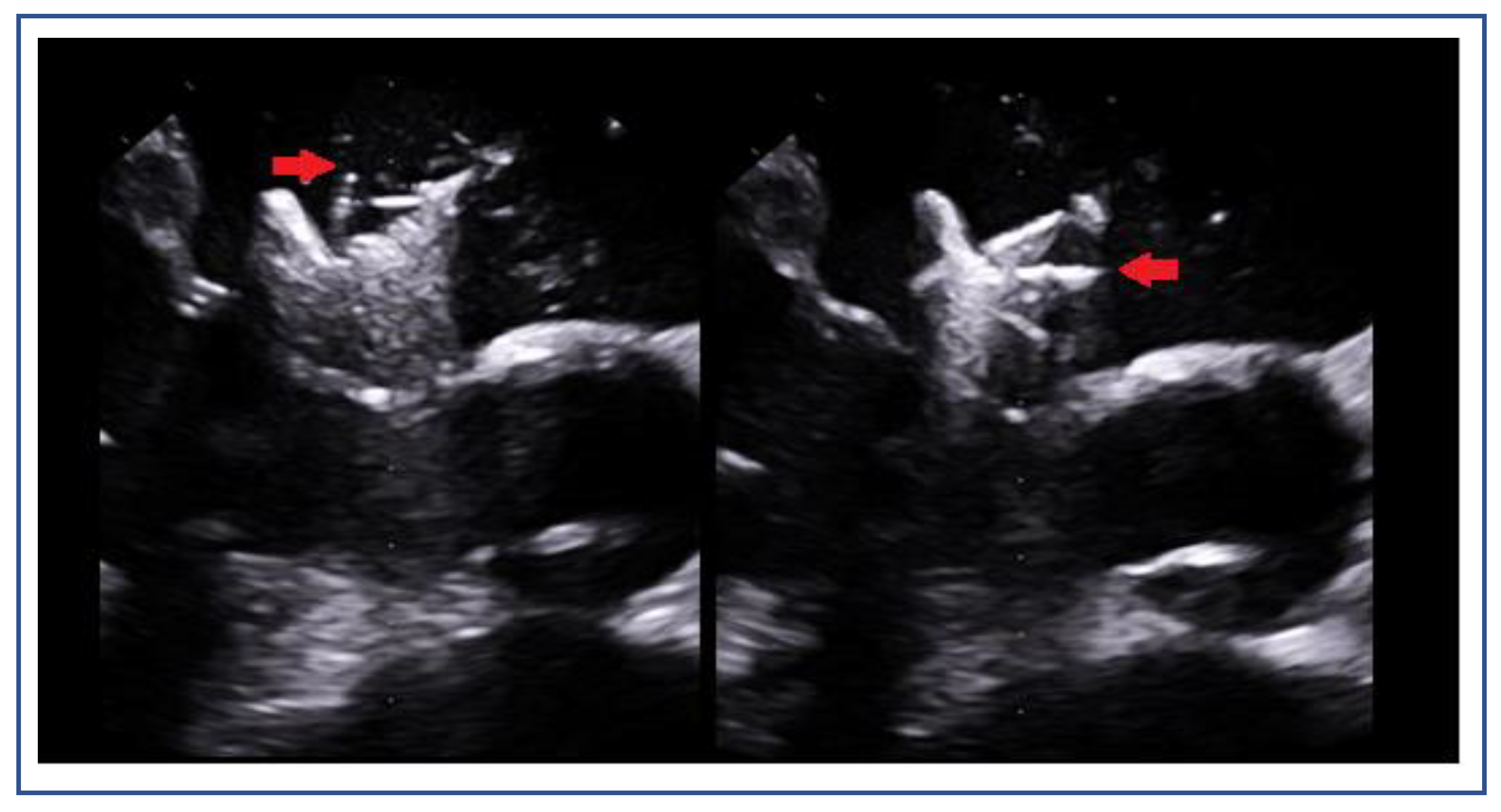
Figure 18.
3D mitral valve shows device orientation (A): Perpendicularity control after crossing mitral valve to check optimal orientation. (B): After the device is advanced into the left ventricle (LV), its orientation can be assessed using 3D echocardiography. Reducing the gain during imaging enhances the clarity of the clip and its position, allowing for more precise visualization of its alignment in relation to the coaptation line.
Figure 18.
3D mitral valve shows device orientation (A): Perpendicularity control after crossing mitral valve to check optimal orientation. (B): After the device is advanced into the left ventricle (LV), its orientation can be assessed using 3D echocardiography. Reducing the gain during imaging enhances the clarity of the clip and its position, allowing for more precise visualization of its alignment in relation to the coaptation line.
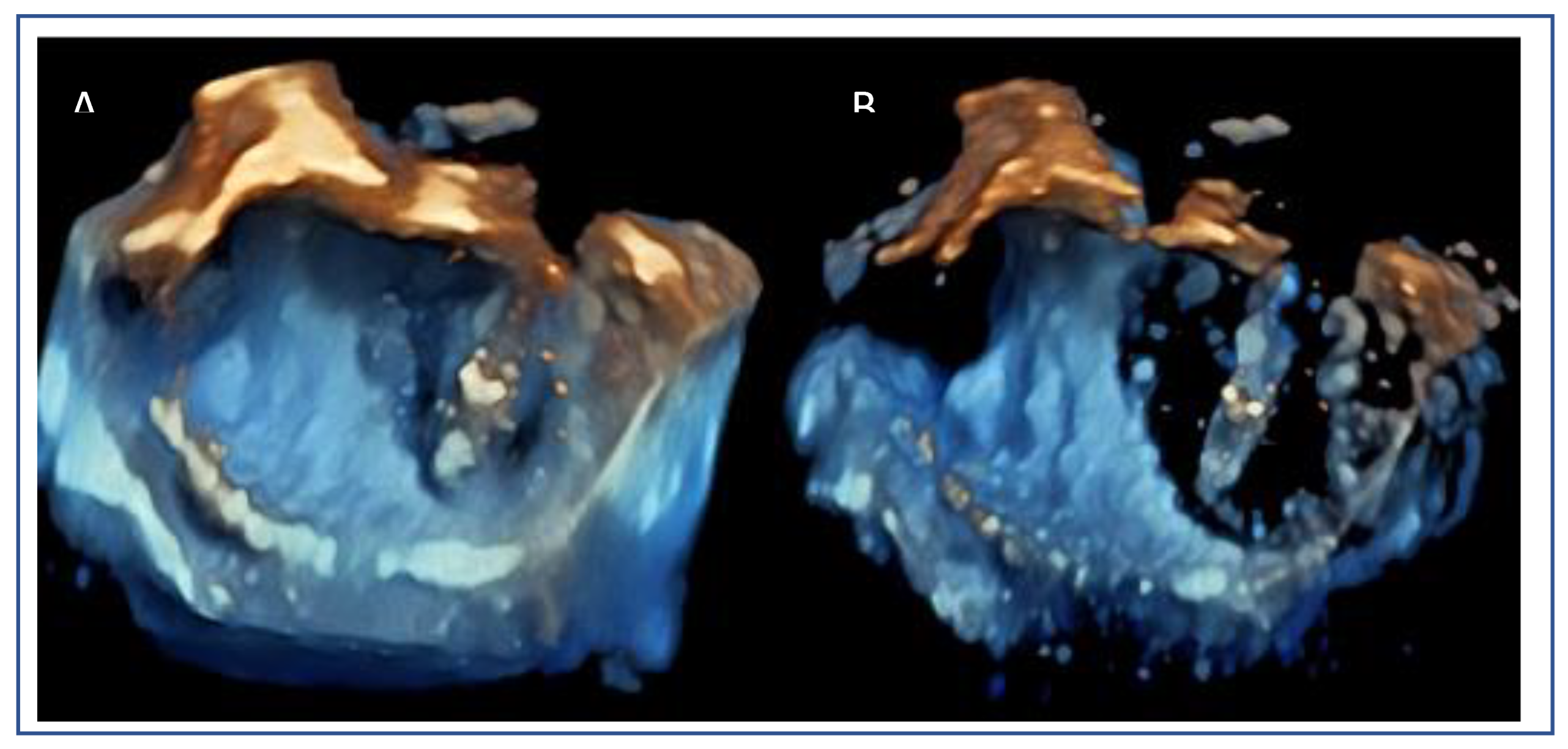
Figure 19.
(A): Failure to grasp anterior leaflet (indicated by red arrow), (B): partial capture of anterior leaflet (red arrow), (C): complete capture for both leaflets.
Figure 19.
(A): Failure to grasp anterior leaflet (indicated by red arrow), (B): partial capture of anterior leaflet (red arrow), (C): complete capture for both leaflets.
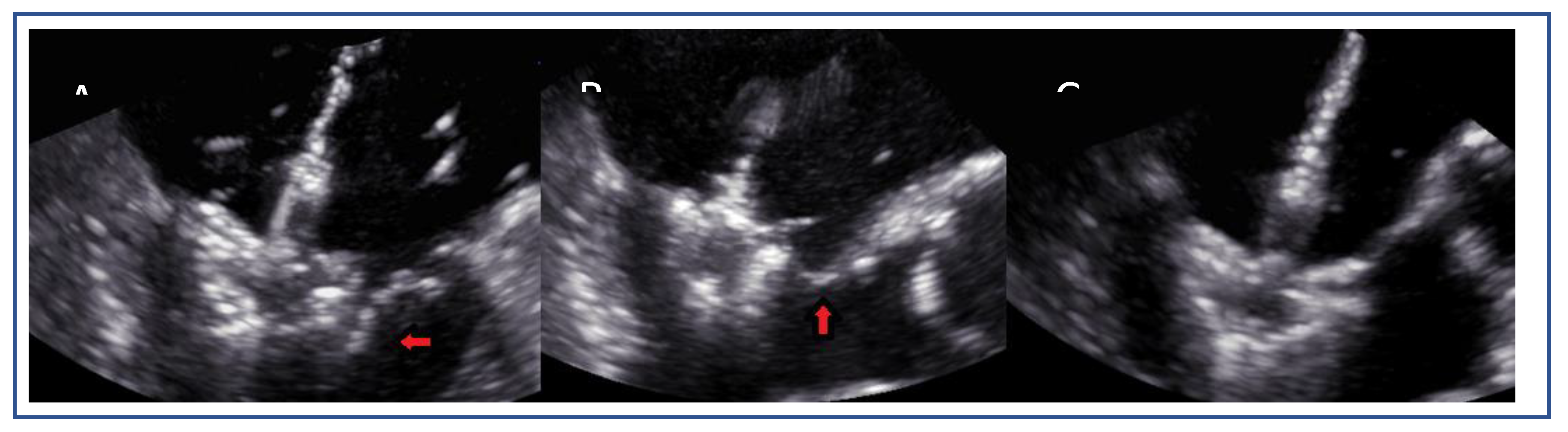
Figure 20.
Post-device deployment echocardiographic assessment. (A): Color Doppler imaging reveals trace residual mitral regurgitation, indicating minimal leakage after device deployment. (B): Continuous-wave Doppler evaluation demonstrates a mean trans-mitral gradient of <5 mmHg, indicating the absence of significant iatrogenic mitral stenosis. (C): 3D multi-planar reconstruction confirms an adequate mitral valve area (MVA ≥1.5 cm²). (D):3D image after device implantation demonstrates good tissue bridging.
Figure 20.
Post-device deployment echocardiographic assessment. (A): Color Doppler imaging reveals trace residual mitral regurgitation, indicating minimal leakage after device deployment. (B): Continuous-wave Doppler evaluation demonstrates a mean trans-mitral gradient of <5 mmHg, indicating the absence of significant iatrogenic mitral stenosis. (C): 3D multi-planar reconstruction confirms an adequate mitral valve area (MVA ≥1.5 cm²). (D):3D image after device implantation demonstrates good tissue bridging.
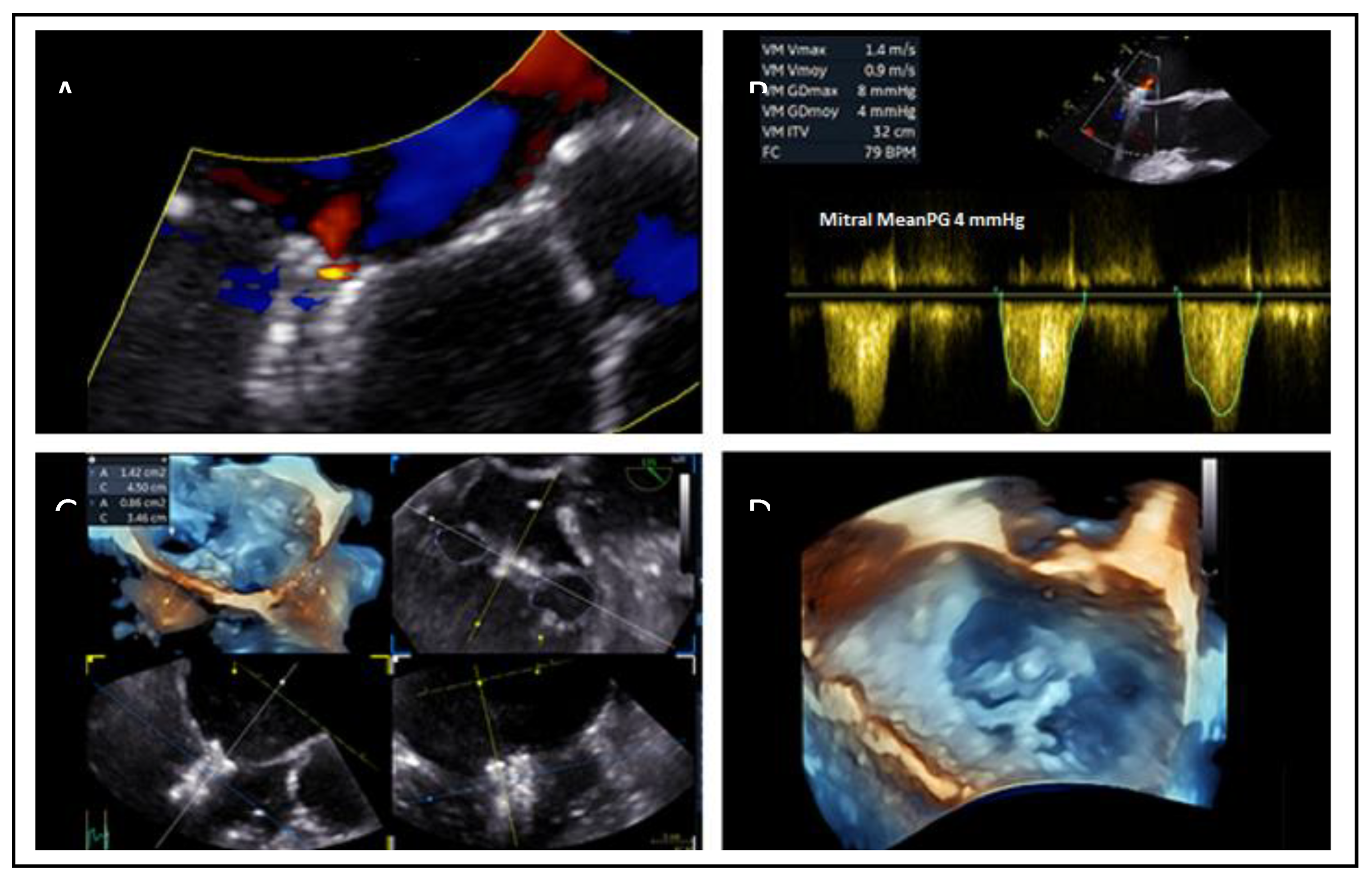
Figure 21.
Residual leaflet prolapse after the deployment of the first device and subsequent correction with an additional device implanted medially to the first one. (A): A 2D echocardiographic view demonstrates persistent leaflet prolapse, medially to the initial device. (B): The corresponding color Doppler image reveals a regurgitant jet at the medial aspect, indicating residual mild MR. (C): A 2D echocardiographic view, similar to (A), shows no residual prolapse after the placement of a second device, confirming optimal anatomical correction. (D): The corresponding color Doppler image, similar to (B), demonstrates non-significant residual MR.
Figure 21.
Residual leaflet prolapse after the deployment of the first device and subsequent correction with an additional device implanted medially to the first one. (A): A 2D echocardiographic view demonstrates persistent leaflet prolapse, medially to the initial device. (B): The corresponding color Doppler image reveals a regurgitant jet at the medial aspect, indicating residual mild MR. (C): A 2D echocardiographic view, similar to (A), shows no residual prolapse after the placement of a second device, confirming optimal anatomical correction. (D): The corresponding color Doppler image, similar to (B), demonstrates non-significant residual MR.
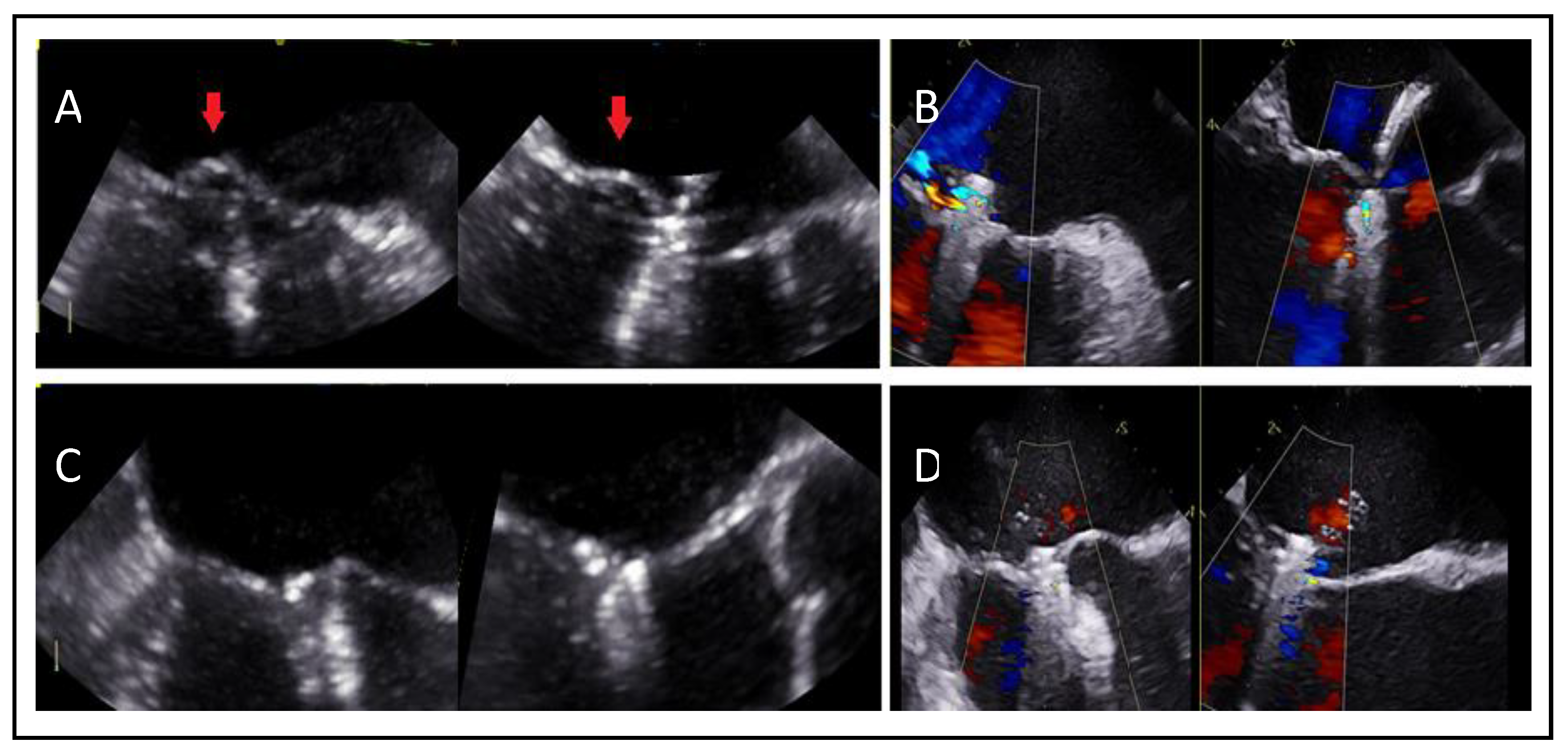

Table 1.
Clinical criteria for optimal patient selection for M-TEER.
| COAPT-eligible characteristics | COAPT-ineligible characteristics |
|---|---|
|
|
Table 2.
Anatomical selection criteria for M-TEER.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



