Submitted:
23 May 2025
Posted:
23 May 2025
You are already at the latest version
Abstract
Background/Objectives: Depression is a significant global public health concern, with working mothers facing unique vulnerabilities due to the intersection of biological, psychological, and social stressors. Biological risk factors (e.g., hormonal fluctuations, genetic predisposition) and psychosocial stressors are well-documented contributors to depression. However, emerging evidence suggests that inner strength—a construct encompassing resilience, emotional regulation, and positive coping—may mediate these relationships. This study addresses critical gaps by examining whether inner strength mediates the pathway from biological risks to depression, offering a potentially modifiable intervention target. Methods: A cross-sectional survey was conducted with 330 Chinese working mothers aged 30 to 45 years. In addition to sociodemographic variables, validated instruments were used, including the Outcome Inventory for Depression, the Inner Strength-Based Inventory, and the Parental Stress Scale. Mediation analysis was performed to assess the indirect effect of inner strength in the relationship between biological risk factors and depression. Results: After controlling for covariates, biological risk factors had both a significant direct effect and an indirect effect (via inner strength) on depressive symptoms. Conclusions: This study underscores the significant role of biological factors in depression while highlighting the protective effect of inner strength in mitigating these risks. To enhance understanding and improve intervention strategies, future research should further explore approaches for strengthening inner resilience.
Keywords:
mental health
; depression
; biological factors
; inner strength
; working mothers
; China
1. Introduction
Based on the Global Burden of Diseases 2019 Study, the global number of individuals living with depression climbed from 172 million in 1990 to 258 million in 2017, demonstrating a 49.86% increase [1]. WHO reports that around 54 million Chinese citizens suffer from depression [2]. Enhancing the mental health status of the Chinese population through public health policies could yield significant benefits worldwide.
Working mothers refer to women with children who are engaged in full-time or part-time employment while simultaneously bearing the primary responsibilities of caregiving and household tasks [3]. In Chinese society, which is deeply influenced by Confucian cultural values, women have traditionally been expected to fulfill family-centered roles [4]. However, with the rising cost of urban living, particularly in housing, education, and healthcare, an increasing number of households rely on dual incomes from both parents to maintain their standard of living [5]. According to a 2020 survey conducted in China, approximately 35% of mothers were employed in full-time jobs, and an additional 8.4% held part-time jobs or operated a secondary business [6]. Meanwhile, Chinese parents have high educational expectations of their children, leading to greater pressure [7]. Especially during a child’s primary school years, mothers are often expected to provide intensive academic and emotional support [8]. Work-family conflict is particularly pronounced for women in the middle years of life [9]. The mental health of working mothers represents an urgent public health concern, especially in rapidly developing societies like China. Addressing the mental health needs of working mothers is critical to promoting social equity, fostering sustainable workforce participation, and strengthening community resilience [10].
Women have an inherent biological vulnerability to depression when encountering stress related to other psychological and environmental factors. Women may have a higher sensitivity to stress-related neurochemical changes, which can affect mood stability [11]. The biological factor includes hormonal fluctuation that can have an impact on women's mental health. Up to 30% of pregnant women experience anxiety, but it is often underdiagnosed [12]. Rapid postpartum drops in estrogen and progesterone are linked to postpartum depression (affecting ~25% of new mothers) [13]. Women undergoing the menopausal transition often experience anxiety and depression symptoms because hormonal changes may influence brain regions like the hypothalamus and hippocampus, affecting neurotransmitter systems such as serotonin and GABA, leading to mood disorders [14]. Notably, another biological risk factor that renders one more likely to develop depression and other psychiatric conditions was highest among those with a family history involving two generations affected by depression [15]. Furthermore, physical diseases that are considered secondary biological factors, such as hypertension, dyslipidemia, and diabetes, are associated with depression, particularly pronounced among females [16]. Moreover, bio-behavioral factors related to lifestyle, such as alcohol consumption and cigarette abuse, are found to be risk factors for depression. Analysis of data from older adults in Ireland revealed that current smokers were significantly more likely to experience symptoms of anxiety and depression compared to non-smokers, indicating a strong association between tobacco use and mental health challenges in later life [17]. These findings are consistent with previous research conducted among Australian adolescents [18]. In addition, individuals with current alcohol dependence exhibited a greater likelihood of persistent depressive disorders over a two-year follow-up period [19].
While risk factors for women have been extensively investigated, protective factors, especially modifiable or psychological factors, are limited. Studies demonstrated that inner strength, an individual's capacity to actively confront and adapt to life’s adversities [20], could be one of them. In the mentioned study, patients with a high level of inner strength are more capable of mobilizing external resources to manage disease progression and treatment, thereby enhancing adherence to therapy and maintaining a better quality of life despite diseases [21]. Another study examining inner strength identified ten positive behavioral traits: truthfulness, perseverance, wisdom, generosity, morality, mindfulness or meditation, patience and endurance, equanimity, determination, and loving-kindness, which found that among Chinese salespersons, inner strength would have a negative correlation with anxiety [22]. According to national health statistics, there were approximately 219,574 community nurses in China in 2020 [23]. A study has demonstrated that even brief sessions of loving-kindness meditation can modulate brain wave activity associated with emotional regulation, particularly in beta and gamma frequencies within the amygdala and hippocampus, which may contribute to reductions in depressive symptoms [24]. The integration of psychological nursing with mindfulness-based stress reduction (MBSR) significantly alleviates depressive symptoms, enhances psychological well-being, and fosters adaptive coping strategies [25]. Community nurses assist patients in identifying and utilizing their inner strengths, such as resilience, hope, coping skills, and social connections, to enhance self-efficacy and resilience [26].
Unlike men, women have more biological vulnerability to depression than men due to hormonal instability that influences low mood. Despite extensive research on the biological vulnerability of women to depression, such as hormonal fluctuations, genetic predisposition, and neurochemical differences, less is known about how inner strengths, such as loving-kindness, mindfulness, perseverance, ethical living, and generosity, may mediate this vulnerability and serve as protective factors. Understanding this mediation effect is crucial, as it offers a holistic approach to mental health that integrates biological, psychological, and spiritual resilience mechanisms. By identifying whether and how these inner strengths mitigate depression risk, this study can contribute to targeted interventions, promoting non-pharmacological, strength-based mental health strategies for women from healthcare providers such as nurses. This study is essential for developing preventive frameworks that empower women to cultivate inner strengths as a buffer against biological stressors and depressive symptoms. Based on this rationale, the researchers hypothesize that inner strengths would significantly mediate the relationship between biological vulnerability and depression in women. Specifically, higher engagement in these strengths will be associated with reduced depressive symptoms, regardless of biological predisposition.
To examine the underlying mechanism linking biological factors and depressive symptoms, inner strength was included as a mediating variable in the structural equation model, as illustrated in Figure 1.
2. Materials and Methods
2.1. Study Design
This study employed a cross-sectional survey administered online in mainland China. The research received approval from the Research Ethics Committee of the Faculty of Medicine at Chiang Mai University. All participants provided informed consent prior to participation. The sample size (n) was calculated based on previous literature data using the formula: n = z² × p × (1−p) / e². Where: z = 1.96 for a 95% confidence level (α), p = 0.3 for the proportion (expressed as a decimal), e = 0.05 for the margin of error, and n = 1.96² × 0.3 × (1-0.3) / 0.05², which approximates 323. Finally, 330 questionnaires were collected.
2.2. Participants
The participants consisted of working mothers from various urban cities and regional areas in China. The inclusion criteria were (1) women aged between 30-45 years, (2) had one or more children aged from 6-11 who were primary school students, (3) had a full-time or part-time job, (4) women during pregnancy, premenopausal or perimenopausal period, (5) had computers or smartphones with good internet. The exclusion criteria were (1) employed but on long-term leave, (2) living in rural areas as recorded in the Chinese household registration book.
2.3. Procedure
Each participant received a detailed explanation of the research, including a Participant Information Sheet (PIS) and an Informed Consent Form (ICF). The questionnaire was designed exclusively for research purposes, and participants were asked to complete self-evaluation items to determine eligibility based on the inclusion and exclusion criteria. A total of 369 individuals were invited to participate through an online platform, and 330 completed questionnaires met the eligibility requirements. To acknowledge their participation, each respondent received CNY 5 via Alipay Red Envelopes. The first author downloaded the data daily to an offline database accessible to the research team. Data collection was conducted from October 17 to November 21, 2024.
2.4. Measurements
2.4.1. Demographic and Socioeconomic Factors
Sociodemographic and socioeconomic characteristics were assessed using a self-administered questionnaire, including participants’ age, marital status, weekly working hours, educational level, and annual income.
2.4.2. Outcome Inventory 21 (OI-21)
The Outcome Inventory-21 (OI-21) employs a 21-point Likert scale [27]. The self-rating process evaluated four distinct areas: depression, anxiety, somatization, and interpersonal difficulty. The ratings on this scale span from 0, which represents "never," to 4, signifying "almost always." The overall scores for the OI-21 can range from 0 to 84. A higher score shows the presence of a greater number of symptoms. In terms of the approach for ascertaining the prevalence, it was drawn on previous research regarding the development of anxiety and depression symptoms with a cut-off score of 7 [27]. The Cronbach’s alpha of OI-21 of anxiety, depression, interpersonal difficulty, and somatization scales among all participants were 0.934, 0.934, 0.899, and 0.922, respectively.
2.4.3. Inner-Strength-Based Inventory (I-SBI)
The Inner Strength-Based Inventory (I-SBI) [28] assesses ten positive behavioral traits, which were truthfulness, perseverance, wisdom, generosity, morality, mindfulness or meditation, patience and endurance, equanimity, determination, and loving-kindness. They are derived from the ten perfections that are integral to the Buddhist doctrine. One strength was assessed using a single multiple-choice question on a 5-point scale. Higher scores on a scale of 10 to 50 correspond to more inner strength. The Chinese version [22] of the SBI demonstrated a good reliability coefficient of 0.86 in the reliability test. In this research, the tool has Cronbach’s α = 0.878.
2.4.4. Parental Stress Scale (PSS)
Authors Berry and Jones (1995) [29] developed the Parental Stress Scale, which was subsequently translated into Chinese by Cheung (2000) [30]. The positive and negative aspects of parenthood are represented among its 18 items, ranging from Strongly Disagree to Agree, on a five-point scale Strongly. Parental stress increases in proportion to the score. The Chinese version of the scale exhibits satisfactory levels of validity and reliability. The alpha value of 0.89 was obtained in this group [30].
2.5. Statistical Analysis
Descriptive analysis techniques were employed to characterize the demographic information, mental health results, and levels of depression. These were presented in terms of the mean value and standard deviation. Sociodemographic variables were either nominal or ordinal and were summarized by presenting the relevant counts and percentages. Analysis of Variance (ANOVA) was utilized to investigate the differences existing among multiple groups. Pearson’s and Spearman's Rank correlations were applied to determine the relationship between variables. Multiple regression is a method used to understand the relationship between one outcome (the dependent variable) and two or more factors that might influence it (independent variables). It helps you see how each factor affects the outcome when all the factors are considered simultaneously.
To ensure the suitability of the data for mediation analysis, multiple regression analyses were conducted across the variables. These analyses confirmed that standard error distribution and homoscedasticity assumptions were met for all regressions, supporting the validity of the mediation approach. To examine the mediation models, we first assessed the magnitude of relationships among biological factors (where all biological determinants were aggregated), the inner strength score, and depression scores using zero-order correlations. For mediation analysis, we investigated the effect of biological factors (X) on depression (Y), mediated by inner strength (M) (Figure 1). Mediation analysis was conducted using the PROCESS macro, a computational tool designed to estimate mediation models. It facilitates the assessment of indirect effects through bootstrapping methods, enabling researchers to examine whether another variable mediates the impact of an independent variable on a dependent variable. The data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) Version 27. For all the data analyzed, a p-value of less than 0.05, 0.01, or 0.001 was considered significant.
3. Results
3.1. Sociodemographic and Socioeconomic Characteristics
Table 1 summarizes the sociodemographic and socioeconomic characteristics of the 330 Chinese mothers, including group comparisons and corresponding percentages. Among the participants, 83.6% were married or cohabiting, and 42.7% (n = 141) reported having two or more children. Over half of the respondents held at least a bachelor’s degree, indicating a relatively high educational attainment. The majority of employed mothers (n = 205) were engaged in full-time employment, typically working 40 hours or more per week. In terms of household income, approximately 75% of the participants reported an annual income of less than CNY 150,000, indicating a predominantly lower- to middle-income population.
3.2. Table 2: Biological Characteristics
Table 2 summarizes the biological characteristics of the 330 participants. Core biological factors—namely, hormone fluctuations and a family history of psychiatric disorders—were observed in 17.6% of the sample. Bio-behavioral factors, defined as cigarette and alcohol use, were present in 20.3% of participants. Secondary biological factors, represented by existing physical illnesses, were reported by 22.7% of the cohort. When considering composite biological variables (i.e., the presence of any of the above factors), 37.3% of participants exhibited at least one.

Table 2.
Biological characteristics (n = 330).
| Variables | Categories | n | % | |
|---|---|---|---|---|
| Core-biological | No | 272 | 82.4 | |
| Yes | 58 | 17.6 | ||
| Bio-behavioral | No | 263 | 79.7 | |
| Yes | 67 | 20.3 | ||
| Secondary biological | No | 255 | 77.3 | |
| Yes | 75 | 22.7 | ||
| Composite biological | 0 | 207 | 62.7 | |
| 1 | 78 | 23.6 | ||
| 2 | 31 | 9.4 | ||
| 3 | 8 | 2.4 | ||
| 4 | 6 | 1.8 | ||
| Mean ± SD, min-max | 0.57 ± 0.8, 0-4 | |||
| Median, interquartile range | 0,1 | |||
3.3. Test Differences Between Associated Factors and Depression
The results indicated that participants who were single, divorced, widowed, or separated reported significantly higher levels of depression compared to those who were married or cohabiting. Mothers with three or more children exhibited the highest levels of depression. Lower educational attainment was also associated with increased depressive symptoms; notably, participants with less than a high school education reported the highest depression scores. Furthermore, participants working more than 54 hours per week demonstrated significantly higher levels of depression, suggesting a potential association between long working hours and adverse mental health outcomes.
The findings also indicated that participants experiencing hormonal fluctuations—during pregnancy, within one year postpartum, or during perimenopause/menopause—reported significantly higher levels of depressive symptoms. Additionally, mothers who reported cigarette or alcohol use had elevated depression scores. A higher level of depressive symptoms was also observed among participants with a family history of psychiatric disorders. Furthermore, those diagnosed with physical conditions such as cardiovascular disease, hypertension, or other chronic illnesses exhibited significantly higher levels of depression (See Table 3).
3.4. Pearson’s Correlation among Variables
Table 4 presents the correlation coefficients among four key variables: Composite Biological, I-SBI, OI-Depression, and PSS. Composite Biological is negatively correlated with I-SBI (-0.347**) but positively correlated with OI-Depression (0.429**) and PSS (0.371**), suggesting that biological factors may contribute to depression and parental stress but inversely relate to inner strengths. I-SBI shows strong negative correlations with both OI-Depression (-0.708**) and PSS (-0.705**), indicating that inner strengths significantly buffer against depression and stress. OI-Depression and PSS have a high positive correlation (0.837**), reinforcing the close link between depression and parental stress in this sample.
3.5. Tests of Moderation
Table 5 presents the results from a multiple regression model and a Mediation model (Model 4) that examine the relationships between biological factors, demographics, psychological variables, and depressive symptoms. In the multiple regression model, “Composite biological” significantly positively correlated with depressive symptoms (B = 1.599, p < 0.001), as did several demographic factors. The model accounted for 67.1% of variance (R² = 0.671, F = 37.744, p < 0.0001). In Model 4, “Composite biological” (B = 0.5838, p < 0.001), inner strength (I-SBI, B = -0.1432, p < 0.001), and parental stress (PSS, B = 0.1916, p < 0.001) had significant associations. Other variables were non-significant. This model explained 75.1% of variance (R² = 0.751, F = 106.954, p < 0.001), illuminating the complex relationships underlying depressive symptoms.
Table 6 presents the total, direct, and indirect effects of biological factors on depressive symptoms. The results indicate a significant total effect of biological factors on depressive symptoms (β = 1.600, p < 0.001). The direct effect was also significant (β = 0.977, p < 0.001), as was the indirect effect (β = 0.623, 95% CI [0.294, 0.962]). Notably, the indirect effect accounted for 38.94% of the total effect, while the direct effect accounted for 61.06%. These findings suggest that inner strength plays a moderating role in the relationship between biological factors and depressive symptoms.
4. Discussion
This study aimed to investigate the prevalence of depression symptoms as well as the mediating effect of inner strengths on the biological factor and depressive symptoms. It found that the prevalence was 38.2% for depression symptoms, according to self-reported screening measurement of Outcome Inventory-21. These rates are notably higher than those reported in previous research among Chinese women aged 40–60 years, where 19.5% experienced depressive symptoms [31]. One possible reason is that the previous study focused only on women, without specifically targeting the subgroup of working mothers. Another reason may be attributed to the different measurement methods used in the studies. Although clinicians should make a definitive diagnosis to find the accurate prevalence of the disorders, these prevalence rates give us concern about the mental health status of Chinese working women.
In this research, the mediating role of inner strength between biological factors and depression was confirmed. Inner strength, often defined as an individual's ability to maintain emotional stability, resilience, and a positive mindset, has been associated with reduced depression symptoms. Consistent with Sripunya and colleagues’ study, the inner strength served as a protective factor against negative mental health among individuals with feelings of emptiness [32], an inner strength acted as a protective variable for major depression, anxiety, and somatic symptoms among Chinese sales workers [22], and among patient with Spinocerebellar ataxia [33]. The fact that inner strength seems to be a potent factor may be because it encompasses many values, including truthfulness, perseverance, wisdom, generosity, morality, mindfulness or meditation, patience and endurance, equanimity, determination, and loving kindness. These virtues, although derived from Buddhism, are universal, positive attributes that can be cultivated in non-Buddhist contexts.
It is expected that parental stress and working hours are closely associated with the occurrence of depressive symptoms. A recent study reported that 57% of parents are experiencing parenting burnout, with maternal stress being particularly pronounced. Parenting burnout is strongly linked to internal and external expectations, such as striving to meet the ideal image of a “good parent”, perceived social judgment, and the amount of time devoted to interacting with children. Excessive parenting stress is a known precipitant of maternal depression [34]. Women who work more than 55 hours per week exhibit 7.3% more depressive symptoms compared to those who work 35 - 40 hours per week, and they are more likely to feel a sense of powerlessness [35].
Overall, men and women show no difference in the risk of depression associated with a family history of psychiatric disorders, related physical illnesses, or substance use (alcohol and cigarettes). However, women experience natural hormonal fluctuations, compounded by psychosocial factors such as excessive working hours, which collectively contribute to prenatal stress and, ultimately, depression. This study, however, suggests that individuals with strong inner strengths possess a protective factor against the development of depression.
4.1. Implications
The strengths of this study are that the findings of this study offer a more comprehensive understanding of mental health challenges among Chinese working mothers, helping both individual treatment. Community nurses play an indispensable role in primary care through routine screening, enabling early detection of mental distress during home visits or checks. Nurses can leverage their health education expertise to conduct training on stress-coping methods, integrating knowledge of psychological well-being to equip mothers with practical skills. They can also provide interventions that foster inner strength to enhance mothers' resilience. The result can also inform public health policymaking, such as giving mothers with more extended maternity leave, flexible working hours, and access to high-quality childcare services.
4.2. Limitations and Recommendations for Further Research
This study has several limitations that should be acknowledged. First, the sample was restricted to urban and regional areas in mainland China. Further research should broaden the inclusion criteria to rural settings. Second, increasing the sample size and incorporating additional relevant variables would also enhance the robustness of future studies. Third, the use of a cross-sectional design precludes the establishment of causal relationships between the identified predictors and depression outcomes. Longitudinal studies and the application of random sampling methods are recommended to strengthen causal inference. Ultimately, a mixed-methods approach can address the limitations inherent in quantitative data by providing deeper contextual insights and enhancing the validity and reliability of the findings [36].
5. Conclusions
This study highlights the significant role of biological factors in depression, as well as the protective effect of inner strength in mitigating the impact of biological risk factors. The findings suggest that regular training, screening, and early intervention—alongside efforts to cultivate inner strength—may help reduce the risk of depression in this population. To enhance understanding and improve intervention strategies, future studies should further explore approaches for training inner strengths.
Author Contributions
Conceptualization, J.J., T.W., R.J., S.W., S.B. and B.H.; methodology, J.J., T.W. and R.J.; software, J.J. and T.W.; validation, J.J., T.W., R.J., S.W. and S.B.; formal analysis, J.J., T.W. and R.J.; investigation, J.J. and S.B.; resources, J.J., T.W., R.J., S.B., and S.W.; data curation, J.J. and T.W.; writing—original draft preparation, J.J.; writing—review and editing, J.J., T.W., R.J., S.W. and S.B.; visualization, J.J. and T.W.; supervision, J.J., T.W., R.J., S.W., S.B. and B.H.; project administration, T.W. and R.J.; funding acquisition, J.J. and T.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not obtain any external funding.
Institutional Review Board Statement
This study received endorsement from the research ethics committee of the Faculty of Medicine, Chiang Mai University (protocol code: PSY-2567-0513), with certification number 380/2024, effective October 1, 2025.
Informed Consent Statement
All participants gave informed consent for the study through the online platform.
Data Availability Statement
According to the policy implemented during this study, the ethics committee does not permit the authors to share the data with other entities. The data sets used and/or analyzed for the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors express their gratitude to all working mothers who participated in this research.
Conflicts of Interest
The authors assert that they have no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| OI-21 | Outcome Inventory 21 |
| I-SBI | Inner-Strength-Based Inventory |
| ANOVA | Analysis of Variance |
References
- Liu, Q.; He, H.; Yang, J.; Feng, X.; Zhao, F.; Lyu, J. Changes in the global burden of depression from 1990 to 2017: Findings from the Global Burden of Disease study. J Psychiatr Res 2020, 126, 134–140. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health in China. Available online: https://www.who.int/china/health-topics/mental-health (accessed on 10 March 2025).
- Lin, W.; Wang, H.; Gong, L, Lai, G. ; Zhao, X.; Ding, H.; Wang, Y. Work stress, family stress, and suicide ideation: A cross-sectional survey among working women in Shenzhen, China. J Affect Disord 2020, 277, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Raymo, J.M.; Park, H.; Xie, Y.; Yeung, W. J. Marriage and Family in East Asia: Continuity and Change. Annu Rev Sociol 2015, 41, 471–92. [Google Scholar] [CrossRef]
- Guo, X.; Zhong, S.; Li, L.; Luo, M. How housing burden damages residents’ health: Evidence from Chinese cities. Front Public Health 2024, 12, 1345775. [Google Scholar] [CrossRef]
- Textor, C.; Population in China from 2014 to 2024, by gender. Statista. Available online: https://www.statista.com/statistics/1225146/china-employment-situation-of-mothers/ (accessed on 17 January 2025).
- Chen, G.; Oubibi, M.; Liang, A.; Zhou, Y. Parents' Educational Anxiety Under the "Double Reduction" Policy Based on the Family and Students' Personal Factors. Psychol Res Behav Manag 2022, 15, 2067–2082. [Google Scholar] [CrossRef]
- Sun, J.; Liu, T.; Gao, Y.; Li, H.; Chen, Y.; Diao, H.; Zhang, G.; Shen, H.; Chang, R.; Yu, Z.; Lu, J.; Liang, L.; Zhang, L. Questionnaire development on measuring parents' anxiety about their children's education: Empirical evidence of parental perceived anxiety data for primary and secondary school students in China. Front Psychol 2022, 13, 1018313. [Google Scholar] [CrossRef]
- Chai, H.; Fu, R.; Coyte, P.C. How Do Middle-Aged Chinese Men and Women Balance Caregiving and Employment Income? Healthcare 2021, 9, 415. [Google Scholar] [CrossRef]
- He, L.; Mai, Z.; Guan, X.; Cai, P.; Li, X.; Feng, J.; Hung, S. The Moderating Role of Social Capital Between Parenting Stress and Mental Health and Well-Being Among Working Mothers in China. Healthcare 2025, 2, 117. [Google Scholar] [CrossRef]
- Mengelkoch, S.; Slavich, G.M. Sex differences in stress susceptibility as a key mechanism underlying depression risk. Curr Psychiatry Rep 2024, 26, 157–165. [Google Scholar] [CrossRef]
- Parents. Treating anxiety during pregnancy. https://www.parents.com/treating-anxiety-during-pregnancy-117267252. (accessed on 17 March 2024).
- Meltzer-Brody, S.; Miller, L. J. Postpartum hormonal changes and maternal mental health: A narrative review. J Womens Health 2021, 30, 4–13. [Google Scholar]
- Alblooshi, S.; Taylor, M.; Gill, N. Does menopause elevate the risk for developing depression and anxiety? Results from a systematic review. Australas Psychiatry 2023, 31, 345–352. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, M.T.; Murphy, E.; Posner, J.E.; Talati, A.; Weissman, M.M. Association of multigenerational family history of depression with lifetime depressive and other psychiatric disorders in children: Results from the Adolescent Brain Cognitive Development (ABCD) Study. JAMA Psychiatry 2021, 78, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Osborne, M.T.; Zureigat, H.; Abohashem, S.; Mezue, K.; Gharios, C.; Grewal, S.; Cardeiro, A.; Naddaf, N.; Civieri, G.; Abbasi, T.; Radfar, A.; Aldosoky, W.; Seligowski, A.V.; Wasfy, M.M.; Guseh, J.S.; Churchill, T.W.; Rosovsky, R.P.; Fayad, Z.; Rosenzweig, A.; Baggish, A.; Pitman, R.K.; Choi, K.W.; Smoller, J.; Shin, L.M.; Tawakol, A. Anxiety and depression associated with increased cardiovascular disease risk through accelerated development of risk factors. JACC: Advances 2024, 3, 101208. [Google Scholar]
- Monroe, D.C.; McDowell, C.P.; Kenny, R.A.; Herring, M.P. Dynamic associations between anxiety, depression, and tobacco use in older adults: Results from The Irish Longitudinal Study on Ageing. J Psychiatr Res 2021, 139, 99–105. [Google Scholar] [CrossRef]
- Lawrence, D.; Johnson, S.E.; Mitrou, F.; Lawn, S.; Sawyer, M. Tobacco smoking and mental disorders in Australian adolescents. Aust N Z J Psychiatry 2022, 56, 58–68. [Google Scholar] [CrossRef]
- Boschloo, L.; Vogelzangs, N.; Smit, J.H.; van den Brink, W.; Veltman, D.J.; Beekman, A.T.F.; Penninx, B.W.J.H. Alcohol use disorders and the course of depressive and anxiety disorders. Br J Psychiatry 2012, 200, 476–484. [Google Scholar] [CrossRef]
- Wongpakaran, T.; Yang, T.; Varnado, P.; Siriai, Y.; Mirnics, Z.; Kövi, Z.; Wongpakaran, N. The development and validation of a new resilience inventory based on inner strength. Sci Rep 2023, 13, 2506. [Google Scholar] [CrossRef]
- XIE, Ying. The relationship among internal strength, self-efficacy and quality of life in patients with chronic liver disease [D]. Yanji: Yanbian University.
- Mao, B.; Kanjanarat, P.; Wongpakaran, T.; Permsuwan, U.; O’Donnell, R. Factors Associated with Depression, Anxiety and Somatic Symptoms Among International Salespeople in the Medical Device Industry: A Cross-sectional Study in China. Healthcare 2023, 11, 2174. [Google Scholar] [CrossRef]
- Wu, X.; Luo, Q.; Ma, W.; Xie, C. Status and development of community nursing in China: Challenges and opportunities. Front Public Health 2024, 12, 1083091. [Google Scholar]
- Maher, C.; Tortolero, L.; Jun, S.; Cummins, D. D.; Saad, A.; Young, J.; Nunez Martinez, L.; Schulman, Z.; Marcuse, L.; Waters, A.; Mayberg, H.S.; Davidson, R.J.; Panov, F.; Saez, I. Intracranial substrates of meditation-induced neuromodulation in the amygdala and hippocampus. Proc Natl Acad Sci U S A 2025, 122, e2409423122. [Google Scholar] [CrossRef]
- Wang, P.; Pang, Z.; Li, G. The intervention effect of mindfulness-based stress reduction therapy on patients with depression. Psychol Mon 2024, 19, 121–123. [Google Scholar]
- Russell, N.G.; Rodney, T.; Peterson, J.K.; Baker, A.; Francis, L. Nurse-Led Mental Health Interventions for College Students: A Systematic Review. Prev Chronic Dis 2025, 22, E17. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran; T. ; Kövi, Z. Development and validation of 21-item outcome inventory (OI-21). Heliyon 2022, 8, e09682. [Google Scholar] [CrossRef]
- Wongpakaran, T.; Yang, T.; Varnado, P.; Siriai, Y.; Mirnics, Z.; Kövi, Z.; Wongpakaran, N. The development and validation of a new resilience inventory based on inner strength. Sci Rep 2023, 13, 2506. [Google Scholar] [CrossRef]
- Berry, J.O.; Jones, W.H. The parental stress scale: initial psychometric evidence. J Soc Pers Relat 1995, 12, 463–72. [Google Scholar] [CrossRef]
- Cheung, S.K. Psychometric properties of the Chinese version of the parental stress scale. Psychologia 2000, 43, 253–261. [Google Scholar]
- Wang, X.; Zhao, G.; Di, J.; Wang, L.; Zhang, X. Prevalence and risk factors for depressive and anxiety symptoms in middle-aged Chinese women: a community-based cross-sectional study. BMC Womens Health 2022, 22, 319. [Google Scholar] [CrossRef]
- Sripunya, P.; Wongpakaran, T.; Wongpakaran, N. The relationship between feelings of emptiness and self-harm among Thai patients exhibiting borderline personality disorder symptoms: The mediating role of the inner strengths. Medicina 2024, 60, 1776. [Google Scholar] [CrossRef]
- Jekpoo, K.; Wongpakaran, T.; Wongpakaran, N.; Siriai, Y. Inner strength and its association with mental health outcomes in patients with spinocerebellar ataxia: A cross-sectional study. J Neurol Sci 2023, 430, 120056. [Google Scholar]
- Gawlik, K.; Melnyk, B. Pandemic Parenting: Examining the Epidemic of Working Parental Burnout and Strategies to Help. [Report]. Ohio State University. 2024. [Google Scholar]
- Weston, G.; Carvalho, L.A.; Stafford, M.; Kivimäki, M. Association of working hours with depressive symptoms: a longitudinal study of UK employees. J Epidemiol Community Health 2019, 73, 448–454. [Google Scholar]
- Wasti, S.P.; Simkhada, P.; van Teijlingen, E.R.; Sathian, B.; Banerjee, I. The Growing Importance of Mixed-Methods Research in Health. Nepal J Epidemiol 2022, 12, 1175–1178. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mediation effect of inner strengths on the biological factors and depressive symptoms.
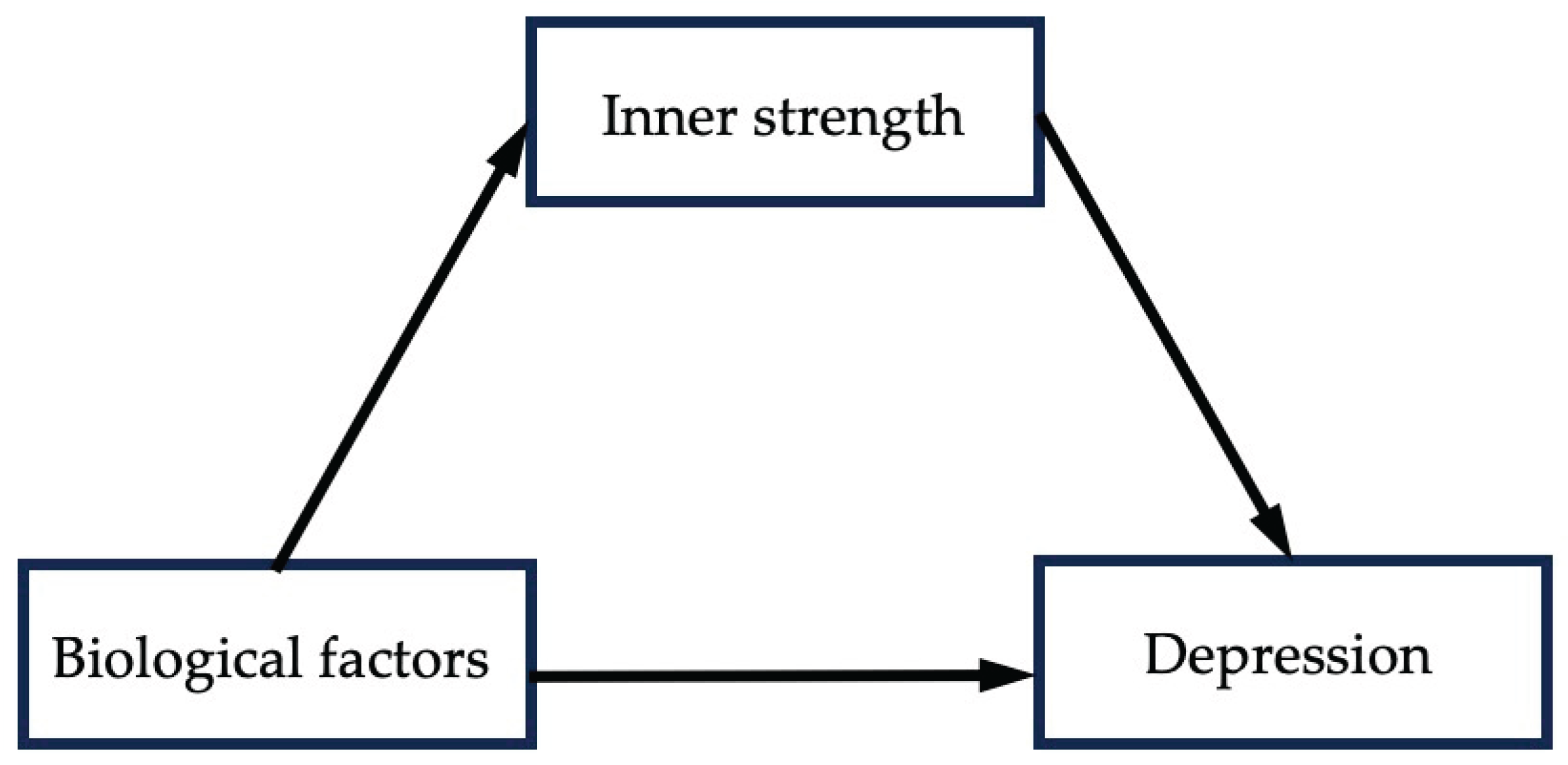
Table 1.
Sociodemographic and socioeconomic characteristics (n = 330).
| Variables | Categories | n | % |
|---|---|---|---|
|
Age |
30-35 | 94 | 28.5 |
| 36-40 | 141 | 42.7 | |
| 41-45 | 95 | 28.8 | |
|
Marital status |
Married/ cohabiting | 276 | 83.6 |
| Single | 9 | 2.7 | |
| Divorced/ widowed/ separated | 45 | 13.6 | |
| Children number |
1 | 189 | 57.3 |
| 2 | 111 | 33.6 | |
| ≥3 | 30 | 9.1 | |
| Educational level |
High school and below | 81 | 24.6 |
| High vocational school | 69 | 20.9 | |
| Bachelor’s degree and above | 180 | 54.5 | |
| 1-20 | 48 | 14.6 | |
| Weekly working hours |
21-39 | 77 | 23.3 |
| 40-54 | 147 | 44.5 | |
| ≥55 | 58 | 17.6 | |
|
Annual income (CNY) |
0-60,000 | 78 | 23.6 |
| 61,000-10,000 | 88 | 26.7 | |
| 101,000-150,000 | 81 | 24.5 | |
| >151,001 | 83 | 25.2 |
CNY = Chinese yuan (7.30 CNY=1 U.S. Dollar).
Table 3.
Depression symptoms based on the participants’ characteristics (n=330).
|
Variables |
OI-Depression Score (Mean ±SD) |
Test Difference |
p-value |
|---|---|---|---|
| Age | |||
| 30-35 | 6.67±5.7 | F (2, 327) = 4.572 | p < 0.05 |
| 36-40 | 4.73±4.3 | ||
| 41-45 | 5.31±4.6 | ||
| Marital status | |||
| Married/ cohabiting | 4.87±4.5 |
F (2, 327) = 12.878 |
|
| Single | 7.78±7.3 | p < 0.001 | |
| Divorced/ widowed/ separated | 8.56±5.4 | ||
| Children number | |||
| 1 | 4.03±4.2 | F (2, 327) = 36.693 | p < 0.001 |
| 2 | 6.32±5.0 | ||
| ≥3 | 11.17±3.8 | ||
| Educational level | |||
| High school and below | 9.74±5.0 | F (2, 327) = 55.364 | p < 0.001 |
| High vocational school | 4.52±3.8 | ||
| Bachelor’s degree and above | 3.87±4.1 | ||
| Weekly working hours | |||
| 1-20 | 5.15±4.9 |
F (3, 326) = 16.181 |
|
| 21-40 | 3.53±4.2 | p < 0.001 | |
| 41-54 | 5.16±4.5 | ||
| ≥55 | 8.98±5.0 | ||
| Table 3. Cont | |||
| Annual income | |||
| 0-60,000 | 6.96±5.6 |
F (4, 325) = 10.995 |
|
| 61,000-10,000 | 6.74±4.7 | p < 0.001 | |
| 101,000-150,000 | 5.36±4.2 | ||
| >151,001 | 2.80±3.9 | ||
| Hormonal fluctuations | |||
| No | 5.03±4.9 |
F (3, 326) = 4.708 |
|
| Pregnancy | 7.00±4.9 | ||
| Within 1 year after delivery | 8.11±4.7 | p < 0.01 | |
| Perimenopause or menopause | 7.94±4.4 | ||
| Smoking | |||
| No | 5.11±4.7 | F (1, 328) = 26.329 | p < 0.001 |
| Yes | 10.70±4.4 | ||
| Alcohol use | |||
| No | 4.96±4.7 | F (1, 328) = 31.888 | p < 0.001 |
| Yes | 9.82±5.0 | ||
| Family psychiatric history |
|||
| No | 5.25±4.8 | F (1, 328) = 18.229 | p < 0.001 |
| Yes | 11.80±4.8 | ||
| Psychical disease(s) | |||
| No | 4.65±4.7 |
F (5, 324) = 8.234 |
|
| Arthritis | 6.11±4.4 | ||
| Cardiovascular disease | 7.90±5.6 | p < 0.001 | |
| Hypertension | 8.85±4.7 | ||
| Diabetes | 5.83±4.8 | ||
| Others | 9.71±4.4 | ||
OI = Outcome Inventory.
Table 4.
Correlation coefficients among variables (n=330).
| Items | Composite biological | I-SBI | OI-Depression | PSS |
|---|---|---|---|---|
| Composite biological | - | |||
| I-SBI | -0.347** | - | ||
| OI-Depression | 0.429** | -0.708** | - | |
| PSS | 0.371** | -0.705** | 0.837** | - |
I-SBI = inner-strength based inventory; OI = Outcome Inventory; PSS = Parental Stress Scale, * p < 0.05, ** p < 0.01.
Table 5.
Mediation effect of inner strengths on the Biological factor and Depressive symptoms.
| B Coefficient | SE | t | p-value | LLCI | ULCI | |
|---|---|---|---|---|---|---|
| Multiple Regression Model | ||||||
| Constant | 2.517 | 1.501 | 1.677 | 0.950 | ||
| Composite biological | 1.599 | 0.241 | 6.623 | < 0.001 | ||
| Age | -0.310 | 0.280 | -1.107 | 0.269 | ||
| Weekly working hours | 0.499 | 0.206 | 2.429 | 0.016 | ||
| Marital status | 1.069 | 0.533 | 2.006 | 0.046 | ||
| Educational level | -0.973 | 0.215 | -4.536 | < 0.001 | ||
| Number of children | 2.010 | 0.317 | 6.335 | < 0.001 | ||
| Annual income (CNY) | -0.432 | 0.175 | -2.477 | 0.014 | ||
| R2 | 0.671 (F=37.744, Df1=5, Df2=322, P<0.0001) | |||||
| Mediation model (Model 4) | ||||||
| Constant | -0.3095 | 1.5675 | -0.1974 | 0.8436 | -3.3934 | 2.7745 |
| Composite biological | 0.5838 | 0.1714 | 3.4059 | 0.0007 | 0.2466 | 0.9211 |
| I-SBI | -0.1432 | 0.0244 | -5.8629 | 0.0000 | -0.1912 | -0.0951 |
| PSS | 0.1916 | 0.0145 | 13.2075 | 0.0000 | -0.1631 | 0.2201 |
| Age | -0.1035 | 0.1894 | -0.5465 | 0.5851 | -0.4761 | 0.2691 |
| Weekly working hours | 0.2412 | 0.1396 | 1.7273 | 0.0851 | -0.0335 | 0.5159 |
| Marital status | 0.6675 | 0.3622 | 1.8428 | 0.0663 | -0.0451 | 1.3801 |
| Educational level | -0.2192 | 0.1516 | -1.4463 | 0.1491 | -0.5175 | 0.0790 |
| Number of children | -0.4798 | 0.2505 | -1.9155 | 0.0563 | -0.9725 | 0.0130 |
| Annual Income (CNY) | 0.2340 | 0.1244 | 1.8806 | 0.0609 | -0.0108 | 0.4788 |
| R2 | 0.751 (F= 106.954, df1=9, Df2= 320, p<0.001) | |||||
β = standardized coefficient, SE = standard error, LLCI = Lower-level confidence interval, ULCI = Upper-level confidence interval, Df = degree of freedom, I-SBI = inner-strength based inventory; PSS = Parental Stress Scale, CNY = Chinese yuan (7.30 CNY=1 U.S. Dollar).
Table 6.
Direct and indirect effects of biological factors on depressive symptoms.
| β | S.E. | LLCI | ULCI | p-value | Effective size | |
|---|---|---|---|---|---|---|
| Total effect | 1.600 | 0.2415 | 1.1242 | 2.0744 | 0.000 | |
| Direct effect | 0.977 | 0.210 | 0.564 | 1.389 | 0.000 | 61.06% |
| Indirect effect | 0.623 | 0.170 | 0.294 | 0.962 | 38.94% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



