Submitted:
15 May 2025
Posted:
16 May 2025
You are already at the latest version
Abstract
Background: This study aims to explore the relationship between Health literacy (HL), vaccination behaviors and Vaccination unawareness (VU) by trying to understand how HL influences vaccination attitudes and the potential mediation of VU. Methods: Data were collected using HLS-EU-Q16, Vaccination Attitude Scale and Vaccine Unawareness Scale. Results: The results show that 17.3% of the variance in total VAX-I is explained by predictors. Among the significant predictors, low VU and age positively predicts VAX-I, while adequate HL negatively predicts the VAX-I. Analyses for specific dimensions of VAX-I reveal that low VU and age positively predict distrust of benefits, concerns about future effects, concerns about profit, and preference for natural immunity, while adequate HL negatively predicts these dimensions. Mediation analysis showed that low VU significantly mediates the relationship between adequate HL and VAX-I, contributing 44% of total effect in VAX-I and percentages between 35% and 54% in specific dimensions. Conclusions: Results show that lower levels of VU, combined with higher HL, are associated with more positive attitudes toward vaccines. The results suggest that increasing HL levels alone may be necessary but not sufficient to improve vaccination attitudes; therefore, interventions should focus not only on increasing HL levels but also on decreasing VU.
Keywords:
vaccine
; public health
; health literacy
; vaccine unawareness
; vaccine attitudes
1. Introduction
Since their discovery, vaccines have been one of the most effective and cost-efficient tools at the disposal of governments and health authorities to protect the health of the entire population [1,2]. In 2024, the World Health Organization (WHO) estimated that the global immunization initiative has prevented 3.5-5 million deaths per year from infectious diseases such as pertussis, tetanus, influenza, diphtheria, and measles, which has allowed approximately 154 million lives to be saved over the past 50 years [3]. Vaccination is a behavior influenced by several factors; among these, health literacy (HL) seems to have an impact [4,5,6]. A definition of HL is: “Health literacy represents the personal knowledge and competencies that accumulate through daily activities, social interactions and across generations. Personal knowledge and competencies are mediated by the organizational structures and availability of resources that enable people to access, understand, appraise and use information and services in ways that promote and maintain good health and well-being for themselves and those around them.” [7]. Having an adequate level of HL means that an individual is able to access, understand, evaluate, and apply information related to health care, disease prevention, and health prevention, thereby contextualizing their own health, that of their family and community, so as to understand the factors that influence it and take action to resolve them [8,9]. While, on the other hand, an inadequate level of HL is associated with deficits in the understanding of health information, limited knowledge about diseases and their risks, poor utilization of health services, and low adherence to drug prescriptions [4,5,6,7,8,9,10,11,12,13,14], all of which actively contribute to poor health, increased mortality risk [15], hospitalization [16], inadequate use of healthcare and increased costs for the health system [17]. The relationship between HL and vaccination is not clear and needs further investigation: some studies have found that vaccination behaviors can be influenced by HL in association with individual or group contextual determinants [4]; Gusar and colleagues [6] propose that low HL is associated with vaccine refusal, but the authors themselves pointed out that there is no clear correlation between different levels of HL and vaccination choice; Biasio and colleagues [14] argue that a limited HL is associated with poor preventive measures such as immunizations but, given the use of different HL measurement methods in different studies, the association between HL and vaccination was not consistent. Other authors found no association between HL and vaccination adherence; according to the authors part of this result could be interpreted in the light of the fact that the skills and information needed to make a decision on vaccination adherence are different from those needed for other health-related choices [18].
Probably vaccination behavior is the result of a complex and dynamic interaction of cognitive, emotional, social, cultural and experiential factors that are difficult to measure. One of these factors could be vaccination unawareness (VU), defined as the individual’s unawareness of vaccinations received in the past, those that would be recommended at the present time, and when to make a booster for those who remember [19]. This construct refers to a whole set of specific information regarding the subject’s vaccination status, information that, when present, inevitably increases the subject’s level of awareness. According to the transtheoretical model (TTM), awareness is an indispensable condition for implementing behavioral change (e.g., deciding to get vaccinated) as it allows the shift from a pre-contemplation state (where the subject has no intention to plan actions in the foreseeable future) to a contemplation state (where the subject has intention to plan actions in the foreseeable future) [20,21]. In the pre-contemplation phase subjects avoid reading, talking or thinking about their risk behaviors (e.g., not getting vaccinated). In the contemplation phase there is the intention to implement certain healthy behaviors and above all there is an awareness of the advantages and disadvantages of implementing such behaviors [19,20,21]. Awareness when viewed from the perspective of vaccination behaviors translates into awareness of their own vaccination situation and awareness of the behaviors required in the related context, so an active search for information by the individual.
The aim of this study is to try to understand the complicated relationship between vaccination, HL and VU, specifically to examine how HL influences attitudes toward vaccines and how this influence may be mediated by VU.
2. Materials and Methods
Our study takes place within the Transdisciplinary Action Research Against Vaccine Hesitancy (TARAVH) project. The overall goal of the project is to promote vaccine uptake by measuring the magnitude of the determinants of vaccine hesitancy for COVID-19 (short-term impact) or other diseases (medium-term impact); this considering all variables described in the 5C model e decomposing them into sociological, psychological and health competencies, with a public health perspective. In the first part of the research an online survey was administered between June 20, 2023 and January 25, 2024 to a sample of 637 subjects from the Italian population
2.1. Questionnaire and Measures
The socio-demographic characteristics collected are age, gender, region of residence, educational qualification, and annual income. Age was grouped into three categories: 18-35 years, 36-64 years and 65> years. For gender, three categories were identified: “cisgender male”, “cisgender females” and “Other gender” (that include “transgender males”, “transgender females” and “non-binary”). For the purposes of gender categorization, we would like to specify that we recognize the importance of accurate categorization and respectful naming of gender identities in research. While acknowledging the diversity of gender identities and the significance of correctly distinguishing between them, for statistical purposes, the transgender and non-binary population in our study was limited (15 participants). Due to the small sample size, these groups were combined into a single category for analytical reasons. This decision was made solely for statistical necessity and does not intend to minimize or overlook the complexity and validity of transgender and non-binary identities. The educational levels were categorized as: “low education” (that include “elementary school license” and “secondary school license”), “average education” (that include “high school diploma”), “high education” (that include “bachelor’s degree”, “master’s degree” or “old-school degree”, “master’s university” and “Ph.D.” or “specialized school”). For the annual income the categories were: “low income” (<10.000€), “average income” (10.000/36.000€), “high income” (36.000/72.000€, 72.000/120.000€, >120.000€). Finally, the regions of Italy were grouped into “north” (Valle d’Aosta, Piedmont, Liguria, Lombardy, Emilia-Romagna, Veneto, Trentino and Friuli Venezia Giulia), “center” (Tuscany, Umbria, Marche and Lazio) and “south” (Abruzzo, Molise, Campania, Apulia, Basilicata, Calabria, Sicily, Sardinia), according to the Italian legislative classification.
HL was measured by means of the HLS-EU-Q16, a HL measurement instrument validated in Italian by Lorini and colleagues [5] which is the short form of the 47-items HLS-EU-Q47. The HLS-EU-Q16 is a 16-item self-reported instrument that can be answered with a 4-item Likert scale (“very difficult”-”quite difficult”-”quite easy”-”very easy”). The score is generated by grouping the answers into two categories: “easy” (“quite easy”- “very easy” = 1) and “difficult” (“quite difficult”-”very difficult” = 0); the answer “don’t know” is considered missing. The scale score is calculated as the sum of the scores for each item and has a range from 0 to 16. Participants who answered fewer than 14 items were excluded. Based on the score obtained, three levels of HL are defined: inadequate HL (0-8), problematic HL (9-12) and adequate HL (13-16).
Participants’ explicit attitudes toward vaccines were measured with the Vaccination Attitudes Examination Scale (VAX) developed by Martin & Petrie [25] and later validated in Italian (VAX-I) by Bruno and colleagues [26]. The instrument consists of 12 items with a 6-point Likert scale (1=strongly disagree to 6=strongly agree) with 3 reverse-coded items; high scores on the scale reflect more negative attitudes toward vaccination. The scale is composed by four factors: F1) distrust about vaccine benefits, F2) concerns about un-foreseen future effects, F3) concerns about commercial profit, and F4) preference for natural immunity; each dimension was indicated by 3 items. Regarding the VAX-I scale, the total score was calculated (minimum score of 12 and a maximum score of 72) [22,23,24] as well as the scores for each of its four dimensions (minimum score of 3 and a maximum score of 18) [25,26,27].
VU was measured by Vaccine Unawareness Scale (VUS) consisting of 4 items with a 5-point Likert scale (“strongly disagree” = 1; “disagree” = 2 “neither agree or disagree” = 3 “agree” = 4 “strongly agree” = 5). The items include: 1) I am aware of the diseases from which I am currently covered by vaccination; 2) I am aware of the vaccinations that would be recommended for me by the medical community; 3) I am aware of the duration of coverage of the vaccinations I have received; 4) I have no clear idea of which vaccinations I have received in the past. The score is obtained by calculating the sum of the results of the 4 items (minimum score of 4 and maximum score of 20); item numbers 1, 2 and 3 are reverse-coded items. The higher the scale score, the higher the VU [19].
2.2. Statistical Analysis
The analysis was conducted in three steps. First, we conducted descriptive analyses of HL level, socio-demographic variables, VAX-I scale (for the total scale and for the four dimensions) and VU. To test the associations between variables a chi square test was used for categorical variables while ANOVA for continuous variables. Second, we specified a priori the causal pathways, which consider VU as the mediator of the association between HL and explicit attitudes toward vaccines (Figure 1). A linear regression model was fitted to investigate the association between HL and VU (mediation model). Afterwards linear regression models were used to investigate associations between HL and each explicit attitudes toward vaccines (outcome models, which also includes the mediator as a covariate). All these models were adjusted for each of the socio-demographic variables. Finally, a mediation analysis was conducted to investigate how VU could mediate the effect of HL on attitudes toward vaccines; variables were used to create a mediation model where the total effect of exposure on the outcome is calculated, and this is decomposed into an indirect effect and a direct effect. In terms of interpretation, the indirect effect reflects the magnitude of the effect transmitted through the mediator, while the direct effect takes into account all other possible causal chains. For each analysis, a p-value less than 0.05 was considered significant. All statistical analyses were performed with StataNow 18.5; the analyses were conducted in July 2024
3. Results
The present study considered the data referred to 637 subjects from the population of Italy, between 18 and 70 years old (M = 27.16; SD = 9.94). Our sample had a predominance of females (78.18%), subjects aged between 18 and 35 years (87.28%) and resident in central Italy (57.14%); for the categories related to education there was a low proportion of subjects with low education (1.41%) while for the annual income variable the category of high income had the fewest subjects (13.97%). All results are reported in Table 1.
In our sample, 56.71% of the participants had an adequate HL, 32.43% a problematic HL and 10.87% an inadequate HL. HL levels were not associated with socio-demographic variables. Regarding the explicit attitudes toward vaccines the mean score was M = 32.11; SD = 12.71 for VAX-I total scale, M = 7.14; SD = 3.49 for VAX-I distrust vaccine benefits, M = 10.61; SD = 3. 62 for VAX-I concern for future effects, M = 6.42; SD = 3.84 for VAX-I concern about profits, M = 7.93; SD = 3.83 for VAX-I preference for natural immunity and VU (M = 9.93; SD = 3.38). A significant association has been found between HL and VU (p < 0.001), VAX-I total scale (p < 0.001), VAX-I distrust vaccine benefits (p < 0.001), VAX-I concern for future effects (p= 0.0192), VAX-I concern about profits (p < 0.001), VAX-I preference for natural immunity (p= 0.0016). All results are reported in Table 2.
3.1. Mediator Models
The results of the mediator model show that 10% of the variance in VU scale can be accounted by predictors, collectively, F(12, 576) = 5.27, p < 0.001. The individual contribution of statistically significant predictors variables was: problematic HL (β= -1.95, p= <0.001), adequate HL (β= -2.71, p= <0.001), cisgender females (β= -0.89, p= 0.011), Other gender (β= -1.91, p= 0.038) and age 35-64 (β= –1.28, p= 0.004) negatively predicted the VU. All results are shown in Table 3.
3.2. Outcome Models
Results show that 17.3% of the variance in VAX-I total scale can be accounted for by predictors, collectively, F(13, 575) = 9.29, p < 0.001. Looking at the unique individuals contributions of the statistically significant predictors, the result shows that VU (β= 0.95, p= <0.001), age 35-64 (β= 12.44, p= <0.001) and age 65-70 (β= 9.83, p= 0.015) are positively predict VAX-I total scale while the adequate HL (β= -4.37, p= 0.008) negatively predict VAX-I total scale. The same multiple regression analysis was conducted for all four dimensions of VAX-I. For the dimension of distrust in the benefits of vaccines, the results showed that 14.3% of the variance can be accounted for by predictors, collectively, F(13, 575) = 7.41, p < 0.001. For the individual contributions of the statistically significant predictors: VU (β= 0.28, p= <0.001) and age 35-64 (β= 2.43, p= <0.001) and age 65-70 (β= 2.29, p= 0.015) are positively predict the distrust in vaccines benefits while adequate HL (β= -1.01, p= 0.028) negatively predict the variable. The dimension of concerns for future effects of vaccines shows that 12.4% of the variance can be accounted for by predictors collectively, F(13, 575) = 6.31, p < 0.001. The individual contribution of statistically significant predictors are: VU (β= 0.18, p= <0.001), cisgender females (β= 1.51, p= <0.001,) age 35-64 (β= 3.25, p= <0.001) and age 65-70 (β= 2.40, p= 0.043) and south region (β= 0.92, p= 0.043), positively predicts concern about future effects. The third dimension, concerns about profits, showed that 15.6% of the variance can be accounted for by predictors collectively, F(13, 575) = 6.31, p < 0.001. For the individual contribution of each statistically significant predictors, we can see that VU (β= 0.24, p= <0.001) and age 35.64 (β= 3.58, p= <0.001) positively predicts concern about profit while adequate HL (β= -1.42, p= 0.005) negatively predict this dimensions. Finally, for the dimension of preference for natural immunity, it was found that 12.6% of the variance can be accounted for by predictors collectively, F(13, 575) = 6.39, p < 0.001. The individual contributions of statistically significant predictors, the results show that VU (β= 0.23, p= <0.001), age 35-64 (β= 3.16, p= <0.001) and age 65-70 (β= 2.94, p= 0.019) was positively predicted a preference for natural immunity while adequate HL (β= -1.13, p= 0.027) negatively predicted the variables. All results are shown in Table 3.
Mediation analysis was performed to assess the mediating role of VU in the relationship between HL and general attitude through vaccines. Regarding VAX-I total scale, problematic HL, compared to inadequate HL revealed a significant total effect (β= -4.18, p= 0.031) and not statistically significant indirect or direct effect; for adequate HL, compared to inadequate HL, results were statistically significant for all three effects, indirect effect (β= -3.07, p= <0.001), direct effect (β= -3.89, p= 0.031) and total effect (β= -6.97, p= <0.001). Thus, the total mediated effect of VU on the VAX-I total scale is 44%. The same analysis was conducted for all 4 dimensions of VAX-I. For the dimension of distrust of vaccine benefits, only the indirect effect (β= -0.96, p= <0.001) and total effect (β= -1.78, p= <0.001) of adequate HL, compared to inadequate HL, was significant; the total mediated effect of VU on the VAX-I distrust vaccine benefits is 54%. Also, for the dimension of concern about future effects, only the indirect effect (β= -0.44, p= 0.034) and total effect (β= -1298, p= 0.006) of adequate HL, compared to inadequate HL, was significant; the total mediated effect of VU on the VAX-I dimension concern about future effects is 35%. The dimension of concern about profits shows a significant total effect (β= -1.23, p= 0.040) and a borderline significance direct effect (β= -1.17, p= 0.051) for problematic HL compared to inadequate HL, while for adequate HL compared to inadequate HL all three effects are statistically significant: indirect effect (β= -0.83, p= <0.001), direct effect (β= -1.28, p= 0.024) and total effect (β= -2.11, p= <0.001). The total mediated effect of VU on the VAX-I dimension concern about profits is 39%. Finally, for the dimension related to the preference of natural immunity, the total effect to borderline significance (β= -1.11, p= 0.056) of problematic HL compared to inadequate HL and the indirect effect (β= -0.83, p= <0.001) and the total effect (β= -1.78, p= <0.001) of adequate HL compared to inadequate HL were significant. The total mediated effect of VU on the VAX-I dimension of preference for natural immunity is 47%. All results are shown in Table 4.
4. Discussion
This study examined the impact of HL on vaccination and its potential mediation by VU. Findings confirm that VU mediates the effect of HL on explicit attitudes toward vaccines.
We found that 10.87% of subjects had inadequate HL, 32.43% a problematic HL and 56.71% an adequate HL, in line with findings from other studies conducted on the Tuscan population [18,19,20,21,22,23,24,25,26,27,28]. For VAX-I level the average levels in the sample were for total scale of M = 32.11 and SD = 12.71, distrust in vaccine benefits of M = 7.14 and SD = 3.49, concern for future effects of M = 10.61 and SD = 3. 62, concerns profits of M = 6.42 and SD = 3.84, and for preference for natural immunity of M = 7.93; SD = 3.83. The results are in line with those presented in other studies, in particular a French study [29] which reported values of M= 30.68 and SD= 11.01 for the VAX total scale, M= 6.89 and SD= 3. 22 for the dimension of distrust in the benefits of vaccines, M= 9.64 and SD= 3.11 for the dimension of concern about future effects, M= 6.42 and SD= 3.47 for the concern about profits and M= 7.72 and SD= 3.39 for the preference for natural immunity. When compared to a study on a South African population [30], our values are lower; in South African population the average values were: M= 43.8 and SD= 14.1 for the VAX total scale, M= 9.3 and SD= 5.0 for the dimension of distrust in the benefits of vaccines, M= 12.9 and SD= 4.0 for the dimension of concern about future effects, M= 10.9 and SD= 4.5 for the concern about profits and M= 10.7 and SD= 4.3 for the preference for natural immunity. This difference could be explained in the light of the proximity, not only geographical but also cultural and social, between Italy and France in relation to South African. There are other studies investigating attitudes towards vaccines via VAX [31,32] but these are difficult to compare due to a large variability within the literature regarding the scoring for each individual domain.
In several studies, it has been observed that VAX is a good predictor of vaccination decisions: higher scores on VAX (more negative attitudes towards vaccines) tend to suggest a possible hesitation or refusal of vaccination [23,24,25,26,27,28,29,30,31,32,33,34,35,36]. In addition to its predictive capacity, its structure, articulated in several separate but interconnected dimensions, allowed us to analyze how the HL may influence the various factors contributing to vaccine decision-making. Indeed, our analysis revealed that some of these dimensions are directly influenced by HL, while others are mediated by VU. This approach allowed us to identify relationships between HL and vaccination behavior that had not been explored in previous studies [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38]. In particular, we hypothesized that VU mediates the effect of HL on VAXI. High levels of VU can be an obstacle for individuals from research and understanding vaccine-related information essential for making informed decisions appropriate to personal health conditions and life circumstances becoming a barrier to vaccination. Even an individual with a good HL might find it difficult to effectively apply health information if the subject is not fully aware of their vaccination status, which could have a negative impact on attitudes towards vaccines. Consequently, VU might limit the effectiveness of HL in improving attitudes towards vaccines by mediating their effect. Our results, indeed, indicate that HL influences VAX-I levels: problematic or inadequate HL correlates with more negative attitudes toward vaccines, while adequate HL correlates with more positive attitudes. Although the effect explained by the regression model is not as strong as might have been expected (R² = 0.173, F (13, 575) = 9.29, p < 0.001), a moderate effect size is present, and it does indeed appear to be mediated by VU.
Based on the TTM conception, we can assume that adequate HL levels are not sufficient to move from the pre-contemplation to the contemplation state. Looking at the data from the mediation analysis, adequate HL, compared to inadequate HL, reduces levels of VU, which in turn reduces negative attitudes towards vaccines, as might be expected. On the other hand, for low HL levels, more negative attitudes towards vaccines are observed mediated by high levels of VU. VU seems to play an important role in attitudes towards vaccines; it has a significant mediating effect, with notable indirect for individuals with adequate HL levels compared to those with inadequate HL levels. One possible explanation for these results could be that the reduction of VU passes from the subject’s active search for information about his vaccination status with a shift from a state of pre-contemplation to a state of contemplation where the desirable behaviors, vaccination, is planned. This search for information will bring the subject into contact, repeatedly, with certain information about vaccines; the improvement in attitudes could be explained by the phenomenon described by Zajonc [39] where the mere repeated exposure of the subject to a certain target stimulus will improve his attitudes towards it. It is conceivable that the effect of VU stems precisely from the fact that individuals with high levels of HL become more actively informed about their vaccination status, reducing their levels of VU. According to the integrated model of HL by Sørensen and colleagues [8], among the four competences that contribute to HL is the ability to ‘access health information’, a competence that is assumed to be possessed by all individuals with adequate levels of HL. Confirming this, individuals with high HL levels tend to use electronic patient records more, trust medical advice, have greater confidence in the healthcare system, and adhere better to treatments [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. This exposure will connect them to specific types of health information, which will inevitably reduce VU and, in turn, contribute to the development of more positive attitudes toward vaccines.
The direct effect of adequate HL, compared to inadequate HL, is only observable in the total VAX-I scale and in the concerns about profits dimension. Even in other studies, the factor ‘concern about profits’ retained a small degree of specificity compared to the other three dimensions of VAX scale [27]. One possible explanation is that concerns about commercial profit extend beyond vaccines to a broader ‘profit over people’ bias, which frames pharmaceutical profits as conflicting with public health and fuels a complex medical-political-economic debate [43,44]. This topic relates less to individual engagement in verifying vaccination status and more to general HL and knowledge of drug production and distribution. This attitude seems to be poorly predictive of vaccination; generally, the greatest attitudinal barriers to receiving vaccines are mistrust of the benefits of vaccines and concern about their safety and future effects [33].
Conversely, HL has no direct effect on vaccine benefit perception, concerns about vaccine effects, or preference for natural immunity. Knowledge about vaccines is highly specific, which is why Vaccine Literacy (VL) has been proposed as a distinct construct. VL is defined as: “It entails people’s and communities’ knowledge, motivation, and competencies to access, understand, and critically appraise and apply information about immunization, vaccines, vaccination programmes, and organizational processes to access vaccination and to navigate the health system, in order to make informed decisions about vaccines for themselves, the members of their family, and the community, and to appreciate the larger global impact of vaccines with respect to population health. A vaccine literate community is able to mobilize collective resources, and to advocate for structural changes to make it easier to access vaccination” [45, p.4-5]. The relationship between HL and VL is not clear; apparently, not necessarily those with a high HL level have a high VL level and moreover, these two literacies only partly overlap [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47]. It is therefore possible to think that HL does not directly influence these dimensions because there is not enough specific knowledge to deal directly with immunization and vaccination issues [18]. Adequate HL provides sufficient general health knowledge for individuals to seek vaccination information actively, thereby reducing VU levels.
Interestingly, vaccination behavior in individuals with problematic HL, compared to inadequate HL, never appears to be mediated by VU. This may be because the knowledge and competence levels in problematic HL are not sufficient to significantly impact VU—i.e., individuals do not actively seek information about their vaccination status or develop attitudes toward vaccines comparable to those with adequate HL. However, they are not low enough to foster strongly negative attitudes toward vaccines and their use.
5. Limitation and Future Direction
The main limitations of this study include the use of convenience sampling, which limits generalizability, and a cross-sectional design that prevents causal inference. Additionally, vaccine acceptance was not directly measured; instead, attitudes toward vaccines were used as a proxy, given their critical role in acceptance or refusal [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48]. Several studies have also linked negative vaccine attitudes to refusal [33,34,35,36]. Further research is needed, and a larger, representative study is currently underway to strengthen these findings.
6. Conclusions
Studying HL and its positive effects is crucial to counteract issues like vaccination refusal, which harm individual and community health. However, we believe it’s important to broaden the analysis by including other constructs, such as VU, to clarify the complex relationship between HL and health behaviors like vaccination. In our study, VU demonstrated a mediating effect between HL and VAX-I by showing how low levels of VU combined with high levels of HL mediated more positive attitudes towards vaccines. The presence of negative attitudes towards vaccines seems to be positively correlated with possible vaccine rejection, which is why it is important to improve the population’s attitudes towards vaccines. Reducing VU seems to be a good way to improve subjects’ attitudes towards vaccination. In practice, interventions to improve vaccination levels could be directed in two directions: on the one hand, an increase in general literacy interventions that would improve people’s ability to take action to find the correct health information and to increase their level of trust in the health system so as to achieve greater compliance with medical advice; on the other hand, it seems to be necessary to provide tools that simplify the procedures for citizens to access information on vaccines and their vaccination status and to increase the amount of information that becomes available; this would allow a decrease in VU as the increase in HL alone seems a necessary but not sufficient cause to promote vaccination behavior. Further studies on VU are needed to improve this construct, which could prove to be a useful tool to understand the relationship between HL and vaccination to improve vaccination levels in the population.
Author Contributions
Conceptualization, P.Z. and V.S..; methodology, P.Z.; formal analysis, V.S.; investigation V.S. and P.Z.; resources, G.C. and M.D.R.; data curation, M.D., M.B., G.C., N.G., N.D.M., A.G., E.M., L.M.; writing—original draft preparation, V.S. and P.Z.; writing—review and editing, M.D., M.B., G.C., N.G., M.D.R., N.D.M., A.G., E.M., L.M..; project administration, L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Ethical Committee of the University of Florence on 23 January 2024 (Ref. No. 0016853).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
The data presented in this study are available on request from the corresponding authors.
Acknowledgments
We thank the Transdisciplinary Action Research Against Vaccine Hesitancy (TARAVH) and the ADVerse reactions to drugs and vaccines, perinatal heAlth and womeN’s soCial wEllbeing - (ADVANCE) projects for supporting and promoting this work.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HL | Health Literacy |
| VU | Vaccine unawareness |
| VAX-I | Vaccination Attitudes Examination scale (-Italian Version) |
| TTM | Transtheoretical model |
| VL | Vaccine Literacy |
References
- Antona, D. (2022). [Vaccination, a public health tool]. Revue de l’infirmiere, 71(279), 16–18. [CrossRef]
- Zhang, E., Dai, Z., Wang, S., Wang, X., Zhang, X., & Fang, Q. (2023). Vaccine Literacy and Vaccination: A Systematic Review. International Journal of Public Health, 68. [CrossRef]
- World Health Organization (WHO). (2024, April 24). Global immunization efforts have saved at least 154 million lives over the past 50 years. Https://Www.Who.Int/News/Item/24-04-2024-Global-Immunization-Efforts-Have-Saved-at-Least-154-Million-Lives-over-the-Past-50-Years.
- Lorini, C., Santomauro, F., Donzellini, M., Capecchi, L., Bechini, A., Boccalini, S., Bonanni, P., & Bonaccorsi, G. (2018). Health literacy and vaccination: A systematic review. Human Vaccines & Immunotherapeutics, 14(2), 478–488. [CrossRef]
- Lorini, C., Lastrucci, V., Mantwill, S., Vettori, V., Bonaccorsi, G., & Florence Health Literacy Research Group. (2019). Measuring health literacy in Italy: a validation study of the HLS-EU-Q16 and of the HLS-EU-Q6 in Italian language, conducted in Florence and its surroundings. Annali Dell’Istituto Superiore Di Sanita, 55(1), 10–18. [CrossRef]
- Gusar, I., Konjevoda, S., Babić, G., Hnatešen, D., Čebohin, M., Orlandini, R., & Dželalija, B. (2021). Pre-Vaccination COVID-19 Vaccine Literacy in a Croatian Adult Population: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(13), 7073. [CrossRef]
- World Health Organization (WHO). (2021). Health promotion glossary of terms 2021 (Inis Communication, Ed.).
- Sørensen, K., van den Broucke, S., Fullam, J., Doyle, G., Pelikan, J., Slonska, Z., & Brand, H. (2012). Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health, 12(1), 80. [CrossRef]
- Council of Europe. (2023, January). Guide to health literacy. Contributing to trust building and equitable access to healthcare . Https://Rm.Coe.Int/Inf-2022-17-Guide-Health-Literacy/1680a9cb75.
- Berkman, N. D., Sheridan, S. L., Donahue, K. E., Halpern, D. J., Viera, A., Crotty, K., Holland, A., Brasure, M., Lohr, K. N., Harden, E., Tant, E., Wallace, I., & Viswanathan, M. (2011). Health literacy interventions and outcomes: an updated systematic review. Evidence Report/Technology Assessment, 199, 1–941.
- Rowlands, G., Khazaezadeh, N., Oteng-Ntim, E., Seed, P., Barr, S., & Weiss, B. D. (2013). Development and validation of a measure of health literacy in the UK: the newest vital sign. BMC Public Health, 13(1), 116. [CrossRef]
- Liu, C., Wang, D., Liu, C., Jiang, J., Wang, X., Chen, H., Ju, X., & Zhang, X. (2020). What is the meaning of health literacy? A systematic review and qualitative synthesis. Family Medicine and Community Health, 8(2), e000351. [CrossRef]
- Sundell, E., Wångdahl, J., & Grauman, Å. (2022). Health literacy and digital health information-seeking behavior - a cross-sectional study among highly educated Swedes. BMC Public Health, 22(1), 2278. [CrossRef]
- Biasio, L. R., Zanobini, P., Lorini, C., Monaci, P., Fanfani, A., Gallinoro, V., Cerini, G., Albora, G., del Riccio, M., Pecorelli, S., & Bonaccorsi, G. (2023). COVID-19 vaccine literacy: A scoping review. Human Vaccines & Immunotherapeutics, 19(1). [CrossRef]
- Bostock, S., & Steptoe, A. (2012). Association between low functional health literacy and mortality in older adults: longitudinal cohort study. BMJ, 344(mar15 3), e1602–e1602. [CrossRef]
- Baker, D. W., Gazmararian, J. A., Williams, M. v, Scott, T., Parker, R. M., Green, D., Ren, J., & Peel, J. (2002). Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. American Journal of Public Health, 92(8), 1278–1283. [CrossRef]
- Weiss, B. D., & Palmer, R. (2004). Relationship between health care costs and very low literacy skills in a medically needy and indigent Medicaid population. The Journal of the American Board of Family Practice, 17(1), 44–47. [CrossRef]
- Zanobini, P., Lorini, C., Caini, S., Lastrucci, V., Masocco, M., Minardi, V., Possenti, V., Mereu, G., Cecconi, R., & Bonaccorsi, G. (2022). Health Literacy, Socioeconomic Status and Vaccination Uptake: A Study on Influenza Vaccination in a Population-Based Sample. International Journal of Environmental Research and Public Health, 19(11). [CrossRef]
- Duradoni, M., Baroni, M., Colombini, G., Gori, N., Della Maggiora, N., Saviozzi, V., Macrì, E., Zanobini, P., Materassi, L., Guazzini, A. (2025) Development and Validation of the Vaccine Unawareness Scale (VUS): A New Measure for Vaccine Unawareness – in review.
- Prochaska, J. O., & Velicer, W. F. (1997). The Transtheoretical Model of Health Behavior Change. American Journal of Health Promotion, 12(1), 38–48. [CrossRef]
- Prochaska, J. O., Redding, C. A., & Evers, K. E. (2015). The transtheoretical model and stages of change. (In K. Glanz, B. K. Rimer, & K. “V.” Viswanath). Health Behavior: Theory, Research, and Practice, 125–148.
- Manoharan, B., Stennett, R., de Souza, R. J., Bangdiwala, S. I., Desai, D., Kandasamy, S., Khan, F., Khan, Z., Lear, S. A., Loh, L., Nocos, R., Schulze, K. M., Wahi, G., & Anand, S. S. (2024). Sociodemographic factors associated with vaccine hesitancy in the South Asian community in Canada. Canadian Journal of Public Health = Revue Canadienne de Sante Publique. [CrossRef]
- Wood, L., Smith, M., Miller, C. B., & O’Carroll, R. E. (2019). The Internal Consistency and Validity of the Vaccination Attitudes Examination Scale: A Replication Study. Annals of Behavioral Medicine : A Publication of the Society of Behavioral Medicine, 53(1), 109–114. [CrossRef]
- Keisala, J., Jarva, E., Comparcini, D., Simonetti, V., Cicolini, G., Unsworth, J., Tomietto, M., & Mikkonen, K. (2024). Factors influencing nurses and nursing students’ attitudes towards vaccinations: A cross-sectional study. International journal of nursing studies, 162, 104963. Advance online publication. [CrossRef]
- Martin, L. R., & Petrie, K. J. (2017). Understanding the Dimensions of Anti-Vaccination Attitudes: the Vaccination Attitudes Examination (VAX) Scale. Annals of Behavioral Medicine : A Publication of the Society of Behavioral Medicine, 51(5), 652–660. [CrossRef]
- Bruno, F., Laganà, V., Pistininzi, R., Tarantino, F., Martin, L., & Servidio, R. (2023). Validation and psychometric properties of the Italian Vaccination Attitudes Examination (VAX-I) scale. Current Psychology, 42(25), 21287–21297. [CrossRef]
- Jovanović, V., & Lazić, M. (2023). Vaccination Attitudes Examination (VAX) Scale: a Bifactor-ESEM approach in a youth sample (15-24 years). BMC Psychology, 11(1), 351. [CrossRef]
- Zanobini, P., Bonaccorsi, G., Giusti, M., Minardi, V., Possenti, V., Masocco, M., Garofalo, G., Mereu, G., Cecconi, R., & Lorini, C. (2023). Health literacy and breast cancer screening adherence: results from the population of Tuscany, Italy. Health Promotion International, 38(6). [CrossRef]
- Eisenblaetter, M., Madiouni, C., Laraki, Y., Capdevielle, D., & Raffard, S. (2023). Adaptation and Validation of a French Version of the Vaccination Attitudes Examination (VAX) Scale. Vaccines, 11(5), 1001. [CrossRef]
- Padmanabhanunni, A., Pretorius, T. B., & Isaacs, S. A. (2023). Validation of the vaccination attitudes examination scale in a South African context in relation to the COVID-19 vaccine: quantifying dimensionality with bifactor indices. BMC Public Health, 23(1), 1872. [CrossRef]
- Paredes, B., Cárdaba, M. Á., Cuesta, U., & Martinez, L. (2021). Validity of the Spanish Version of the Vaccination Attitudes Examination Scale. Vaccines, 9(11). [CrossRef]
- Espejo, B., Martín-Carbonell, M., Romero-Acosta, K. C., Fernández-Daza, M., & Paternina, Y. (2022). Evidence of Validity and Measurement Invariance by Gender of the Vaccination Attitudes Examination (VAX) Scale in Colombian University Students. Journal of Clinical Medicine, 11(16), 4682. [CrossRef]
- Raffard, S., Bayard, S., Eisenblaetter, M., Attal, J., Andrieu, C., Chereau, I., Fond, G., Leignier, S., Mallet, J., Tattard, P., Urbach, M., Misdrahi, D., Laraki, Y., & Capdevielle, D. (2022). Attitudes towards Vaccines, Intent to Vaccinate and the Relationship with COVID-19 Vaccination Rates in Individuals with Schizophrenia. Vaccines, 10(8), 1228. [CrossRef]
- Ye, X., Lee, H.-H., Hui, K.-H., Xin, M., & Mo, P. K. H. (2023). Effects of Negative Attitudes towards Vaccination in General and Trust in Government on Uptake of a Booster Dose of COVID-19 Vaccine and the Moderating Role of Psychological Reactance: An Observational Prospective Cohort Study in Hong Kong. Vaccines, 11(2), 393. [CrossRef]
- Paul, E., Steptoe, A., & Fancourt, D. (2021). Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. The Lancet Regional Health. Europe, 1, 100012. [CrossRef]
- Biella, M., Orrù, G., Ciacchini, R., Conversano, C., Marazziti, D., & Gemignani, A. (2023). Anti-Vaccination Attitude and Vaccination Intentions Against Covid-19: A Retrospective Cross-Sectional Study Investigating the Role of Media Consumption. Clinical Neuropsychiatry, 20(4), 252–263. [CrossRef]
- Siena, L. M., Isonne, C., Sciurti, A., de Blasiis, M. R., Migliara, G., Marzuillo, C., de Vito, C., Villari, P., & Baccolini, V. (2022). The Association of Health Literacy with Intention to Vaccinate and Vaccination Status: A Systematic Review. Vaccines, 10(11). [CrossRef]
- Biasio, L. R. (2019). Vaccine literacy is undervalued. Human Vaccines & Immunotherapeutics, 15(11), 2552–2553. [CrossRef]
- Zajonc, R. B. (1968). Attitudinal effects of mere exposure. Journal of Personality and Social Psychology, 9(2, Pt.2), 1–27. [CrossRef]
- Sarkar, U., Karter, A. J., Liu, J. Y., Adler, N. E., Nguyen, R., López, A., & Schillinger, D. (2010). The Literacy Divide: Health Literacy and the Use of an Internet-Based Patient Portal in an Integrated Health System—Results from the Diabetes Study of Northern California (DISTANCE). Journal of Health Communication, 15(sup2), 183–196. [CrossRef]
- Tsai, T.-I., Yu, W.-R., & Lee, S.-Y. D. (2018). Is health literacy associated with greater medical care trust? International Journal for Quality in Health Care, 30(7), 514–519. [CrossRef]
- Miller, T. A. (2016). Health literacy and adherence to medical treatment in chronic and acute illness: A meta-analysis. Patient Education and Counseling, 99(7), 1079–1086. [CrossRef]
- Brezis M. (2008) Big Pharma and health care: Unsolvable conflict of interests between private enterprise and public health. The Israel Journal of Psychiatry and Related Sciences 45(2): 83–89. [PubMed] [Google Scholar].
- Dănescu, T., & Popa, M. A. (2020). Public health and corporate social responsibility: exploratory study on pharmaceutical companies in an emerging market. Globalization and health, 16(1), 117. [CrossRef]
- Lorini, C., del Riccio, M., Zanobini, P., Biasio, R. L., Bonanni, P., Giorgetti, D., Ferro, V. A., Guazzini, A., Maghrebi, O., Lastrucci, V., Rigon, L., Okan, O., Sørensen, K., & Bonaccorsi, G. (2023). Vaccination as a social practice: towards a definition of personal, community, population, and organizational vaccine literacy. BMC Public Health, 23(1), 1501. [CrossRef]
- Biasio, Luigi & Zanobini, Patrizio & Lorini, Chiara & Bonaccorsi, Guglielmo. (2024). Perspectives in the Development of Tools to Assess Vaccine Literacy. Vaccines. 12. 422. [CrossRef]
- Isonne, C., Iera, J., Sciurti, A., Renzi, E., De Blasiis, M. R., Marzuillo, C., Villari, P., & Baccolini, V. (2024). How well does vaccine literacy predict intention to vaccinate and vaccination status? A systematic review and meta-analysis. Human vaccines & immunotherapeutics, 20(1), 2300848. [CrossRef]
- Brun, C., Akinyemi, A., Houtin, L., Zerhouni, O., Monvoisin, R., & Pinsault, N. (2022). Intolerance of Uncertainty and Attitudes towards Vaccination Impact Vaccinal Decision While Perceived Uncertainty Does Not. Vaccines, 10(10). [CrossRef]
Figure 1.
Mediation model.
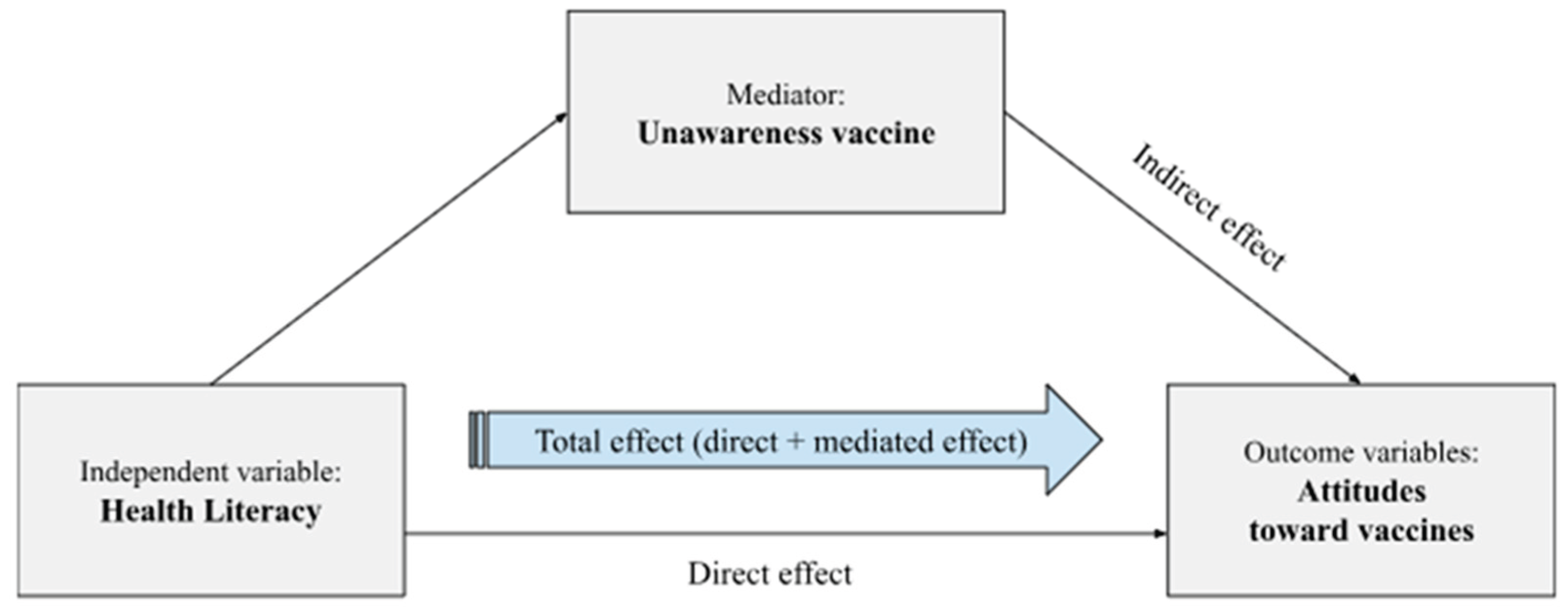

Table 1.
F1 = distrust vaccine benefits; F2= concern for future effects; F3 = concern about profits; F4 = preference for natural immunity; VU = vaccine unawareness, HL = health literacy.
Table 1.
F1 = distrust vaccine benefits; F2= concern for future effects; F3 = concern about profits; F4 = preference for natural immunity; VU = vaccine unawareness, HL = health literacy.
| Gender | Age | Region | Educational qualification | Annual Income | HL | ||||||||||||||
| [M±SD] | Male | Female | Other | 18-35 | 36-64 | 65-70 | North | center | south | low | average | high | low | average | high | inadequate | problematic | adequate | |
| VAX-I | (N=124) | (N=498) | (N=15) | (N=556) | (N=71) | (N=10) | (N=170) | (N=364) | (N=103) | (N=9) | (N=328) | (N=300) | (N=283) | (N=265) | (N=89) | (N=64) | (N=191) | (N=334) | |
| total scale | 32.11±12.71 | 32.41±14.68 | 31.99±12.10 | 33.33±15.53 | 30.70±11.09 | 41.80±17.41 | 41.6±22.52 | 32.35±14.17 | 31.53±11.79 | 33.72±13.26 | 34.11±16.55 | 31.87±12.68 | 32.31±12.65 | 31.33±12.06 | 32.31±12.86 | 33.95±14.12 | 37.31±14.30 | 33.01±12.15 | 30.31±12.28 |
| F1 | 7.14±3.49 | 7.20±4.09 | 7.11±3.33 | 7.66±3.69 | 6.86±3.09 | 9±5.01 | 9.6±6.36 | 7.45±4.02 | 6.89±3.23 | 7.52±3.41 | 8.22±4.26 | 7.14±3.46 | 7.12±3.52 | 7.12±3.45 | 7.03±3.45 | 7.55±3.74 | 8.46±4.33 | 7.41±3.47 | 6.70±3.21 |
| F2 | 10.61±3.62 | 10.02±3.87 | 10.75±3.55 | 10.6±3.69 | 10.29±3.43 | 12.87±4.01 | 12.3±5.45 | 10.31±3.8 | 10.62±3.58 | 11.06±3.45 | 11±4.03 | 10.63±3.73 | 10.57±3.51 | 10.44±3.63 | 10.71±3.52 | 10.83±3.91 | 11.57±3.64 | 10.73±3.54 | 10.25±3.64 |
| F3 | 6.42±3.84 | 6.79±4.34 | 6.30±3.69 | 7.06±4.51 | 5.99±3.35 | 9.43±5.33 | 8.8±6.52 | 6.59±4.06 | 6.22±3.53 | 6.82±4.49 | 7±4.63 | 6.27±3.80 | 6.56±3.87 | 6.05±3.44 | 6.58±3.96 | 7.07±4.56 | 8±4.35 | 6.73±3.79 | 5.88±3.64 |
| F4 | 7.93±3.83 | 8.38±4.33 | 7.81±3.66 | 8±4.82 | 7.55±3.50 | 10.49±4.92 | 10.9±5.02 | 8±4.22 | 7.79±3.61 | 8.31±3.93 | 7.88±4.78 | 7.82±3.73 | 8.05±3.92 | 7.71±3.61 | 7.97±3.89 | 8.49±4.28 | 9.26±4.20 | 8.13±3.69 | 7.48±3.78 |
| V.U. | 9.93±3.38 | 10.64±3.45 | 9.78±3.36 | 8.8±2.21 | 10.06±3.33 | 8.85±3.43 | 10.3±4.47 | 9.70±3.58 | 9.85±3.23 | 10.58±3.49 | 9.33±3.31 | 10.07±3.34 | 9.79±3.42 | 10.39±3.27 | 9.58±3.47 | 9.48±3.26 | 11.95±4.01 | 10.07±3.24 | 9.29±3.13 |
| N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | N(%) | |||||
| (HL) inadequate | - | 10 (9.01%) | 52 (11.21%) | 2 (14.29%) | 56 (10.89%) | 8 (12.12%) | 0 (0.00%) | 18 (11.46%) | 36 (10.62%) | 10 (10.75%) | 0 (0.00%) | 30 (9.97%) | 34 (12.19%) | 29 (11.46%) | 25 (10.00%) | 10 (11.63%) | - | - | - |
| (HL) problematic | - | 41 (36.94%) | 148 (31.90%) | 2 (14.29%) | 166 (32.30%) | 24 (36.36%) | 1 (11.11%) | 46 (29.30%) | 120 (35.40%) | 25 (26.88%) | 4 (44.44%) | 107 (35.55%) | 80 (28.67%) | 86 (33.99%) | 79 (31.60%) | 26 (30.23%) | - | - | - |
| (HL) adequate | - | 60 (54.05%) | 264 (56.90%) | 10 (71.43%) | 292 (56.81%) | 34 (51.52%) | 8 (88.89%) | 93 (59.24%) | 183 (53.98%) | 58 (62.37%) | 5 (55.56%) | 164 (54.49%) | 165 (59.14%) | 138 (54.55%) | 146 (58.40%) | 50 (28.14%) | - | - | - |
Table 2.
Means (M) and standard deviation (SD) value for VU and VAX-I (total scale, F1 = distrust vaccine benefits, F2= concern for future effects, F3 = concern about profits, F4 = preference for natural immunity).
Table 2.
Means (M) and standard deviation (SD) value for VU and VAX-I (total scale, F1 = distrust vaccine benefits, F2= concern for future effects, F3 = concern about profits, F4 = preference for natural immunity).
| HL | |||||||
| HL inadequate | HL problematic | HL adequate | F | p | R² | ||
| VAX-I | [M±SD] | (N=64) | (N=191) | (N=334) | |||
| total scale | [32.11±12.71] | [37.31±14.30] | [33.01±12.15] | [30.31±12.28] | 9.48 | 0.0001 | 0.0313 |
| F1 | [7.14±3.49] | [8.46±4.33] | [7.41±3.47] | [6.70±3.21] | 8.15 | 0.0003 | 0.0271 |
| F2 | [10.61±3.62] | [11.57±3.64] | [10.73±3.54] | [10.25±3.64] | 3.98 | 0.0192 | 0.0134 |
| F3 | [6.42±3.84] | [8±4.35] | [6.73±3.79] | [5.88±3.64] | 9.64 | 0.0001 | 0.0319 |
| F4 | [7.93±3.83] | [9.26±4.20] | [8.13±3.69] | [7.48±3.78] | 6.50 | 0.0016 | 0.0217 |
| V.U. | [9.93±3.38] | [11.95±4.01] | [10.07±3.24] | [9.29±3.13] | 18.46 | 0.0001 | 0.0593 |
Table 3.
1Health Literacy levels; 2Gender; 3Age; 4Region; 5Education; 6Income; F1 = distrust vaccine benefits, F2= concern for future effects, F3 = concern about profits, F4 = preference for natural immunity.
Table 3.
1Health Literacy levels; 2Gender; 3Age; 4Region; 5Education; 6Income; F1 = distrust vaccine benefits, F2= concern for future effects, F3 = concern about profits, F4 = preference for natural immunity.
| Vaccine Unawareness | VAX-I | F1 | F2 | F3 | F4 | |||||||||||||
| β | p | 95% CI | β | p | 95% CI | β | P | 95% CI | β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | |
| constant | 13.22 | <0.001 | [-10.752 15.705] | 17.78 | <0.001 | [8.053 27.511] | 4.46 | 0.001 | [1.743 7.182] | 6.05 | <0.001 | [3.182 8.925] | 3.01 | 0.047 | [0.041 5.992] | 4.24 | 0.006 | [1.215 7.280] |
| vaccine unawareness | - | - | - | 0.95 | <0.001 | [0.656 1.246] | 0.28 | <0.001 | [0.200 0.365] | 0.18 | <0.001 | [-0.094 0.268] | 0.24 | <0.001 | [0.159 0.339] | 0.23 | <0.001 | [0.145 0.329] |
| problematic1 | -1.95 | <0.001 | [-2.878 -1.035] | -2.29 | 0.180 | [-5.666 1.068] | -0.46 | 0.327 | [-1.411 0.471] | -0.44 | 0.380 | [-1.438 0.549] | -0.74 | 0.158 | [-1.771 0.288] | -0.64 | 0.229 | [-1.692 0 .406] |
| adequate1 | -2.71 | <0.001 | [-3.580 -1.841] | -4.37 | 0.008 | [-7.603 -1.142] | -1.01 | 0.028 | [-1.914 -0.108] | -0.79 | 0.101 | [-1.749 0.157] | -1.42 | 0.005 | [-2.414 -0.438] | -1.13 | 0.027 | [-2.144 -0.131] |
| cis. Females2 | -0.89 | 0.011 | [-1.572 -0.207] | 2.04 | 0.104 | [-0.421 4.518] | 0.42 | 0.232 | [-0.270 1.110] | 1.51 | <0.001 | [0.781 2.239] | 0.15 | 0.692 | [-0.603 0.907] | -0.03 | 0.929 | [-0.805 0.734] |
| other2 | -1.91 | 0.038 | [-3.727 -0.102] | 5.38 | 0.107 | [-1.164 11.931] | 1.42 | 0.128 | [-0.408 3.252] | 1.81 | 0.065 | [-0.114 3.750] | 1.40 | 0.167 | [-0.593 3.412] | 0.733 | 0.480 | [-1.307 2.774] |
| 35-643 | -1.28 | 0.004 | [-2.168 -0.401] | 12.44 | <0.001 | [9.238 15.642] | 2.43 | <0.001 | [1.536 3.327] | 3.25 | <0.001 | [2.305 4.195] | 3.58 | <0.001 | [2.609 4.568] | 3.16 | <0.001 | [2.17 4.166] |
| 65-703 | -0.047 | 0.966 | [-2.24 2.14] | 9.83 | 0.015 | [1.937 17.730] | 2.29 | 0.041 | [0.092 4.506] | 2.40 | 0.043 | [0.077 4.738] | 2.18 | 0.076 | [-0.232 4.598] | 2.94 | 0.019 | [0.48 5.404] |
| center4 | 0.19 | 0.554 | [-0.443 0.826] | -0.77 | 0.508 | [-3.058 1.516] | -0.59 | 0.068 | [-1.233 0.045] | 0.374 | 0.276 | [-0.300 1.050] | -0.26 | 0.456 | [-0.965 0.433] | -0.28 | 0.431 | [-0.999 0.426] |
| south4 | 0.74 | 0.082 | [-0.095 1.579] | 1.60 | 0.296 | [-1.413 4.631] | 0.12 | 0.780 | [-0.724 0.965] | 0.92 | 0.043 | [0.030 1.814] | 0.29 | 0.531 | [-0.629 1.219] | 0.27 | 0.572 | [-0.670 1.213] |
| average5 | -0.30 | 0.793 | [-2.54 1.94] | 5.27 | 0.201 | [-2.810 13.352] | 0.482 | 0.675 | [-1.777 2.741] | 1.52 | 0.211 | [-0.864 3.905] | 1.36 | 0.279 | [-1.109 3.834] | 1.90 | 0.138 | [-0.614 4.424] |
| high5 | -0.32 | 0.773 | [-2.55 1.90] | 3.84 | 0.348 | [-4.194 11.876] | 0.04 | 0.972 | [-2.205 2.286] | 1.03 | 0.390 | [-1.333 3.409] | 1.10 | 0.377 | [-1.350 3.564] | 1.65 | 0.195 | [-0.849 4.160] |
| average6 | -0.39 | 0.183 | [-.988 0.189] | 0.25 | 0.817 | [-1.871 2.373] | -0.18 | 0.539 | [-0.778 0.407] | 0.034 | 0.913 | [-0.591 0.661] | 0.31 | 0.334 | [-.329 0.968] | 0.08 | 0.808 | [-0.579 0.743] |
| high6 | -0.54 | 0.189 | [-1.36 0.268] | 2.18 | 0.144 | [-0.747 5.126] | 0.49 | 0.241 | [-0.330 1.311] | 0.18 | 0.674 | [-0.681 1.052] | 0.85 | 0.062 | [-0.042 1.753] | 0.65 | 0.158 | [-0.257 1.573] |
| R²= 0.098 | R²= 0.173 | R²= 0.143 | R²= 0.124 | R²= 0.156 | R²= 0.126 | |||||||||||||
| F(12, 576)= 5.27 | F(13, 575)= 9.29 | F(13, 575)= 7.41 | F(13, 575)= 6.31 | F(13, 575)= 8.23 | F(13, 575)= 6.39 | |||||||||||||
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | |||||||||||||
Table 4.
Mediation model: NIE = indirect effect; NDE = direct effect; TE = total effect; VAX-I = total scale, F1 = distrust vaccine benefits, F2= concern for future effects, F3 = concern about profits, F4 = preference for natural immunity.
Table 4.
Mediation model: NIE = indirect effect; NDE = direct effect; TE = total effect; VAX-I = total scale, F1 = distrust vaccine benefits, F2= concern for future effects, F3 = concern about profits, F4 = preference for natural immunity.
| VAX-I | F1 | F2 | F3 | F4 | ||||||||||||
| β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | ||
| [problematic vs inadequate] | NIE | -0.56 | 0.294 | [-1.633 0.493] | -0.06 | 0.692 | [-.359 0.238] | -0.31 | 0.081 | [-0.668 0.039] | -0.06 | 0.699 | [-0.392 0.263] | -0.129 | 0.424 | [-0.447 0.188] |
| NDE | -3.61 | 0.061 | [-7.395 0.161] | -0.97 | 0.096 | [-2.117 0.173] | -0.48 | 0.326 | [-1.463 0.486] | -1.17 | 0.051 | [-2.354 0.005] | -0.98 | 0.096 | [-2.137 0.173] | |
| TE | -4.18 | 0.031 | [-7.986 -0.387] | -1.03 | 0.076 | [-2.174 0.108] | -0.80 | 0.107 | [-1.779 0.172] | -1.23 | 0.040 | [-2.421 -0.056 | -1.11 | 0.056 | [-2.252 0.029] | |
| [adequate vs inadequate] | NIE | -3.07 | <0.001 | [-4.739 -1.406] | -0.96 | <0.001 | [-1.439 -0.48] | -0.44 | 0.034 | [-0.862 -0.0.34] | -0.83 | <0.001 | [-1.307 -0.353] | -0.83 | <0.001 | [-1.298 -0.367] |
| NDE | -3.89 | 0.031 | [-7.445 -0.352] | -0.82 | 0.120 | [-1.862 0.214] | -0.84 | 0.089 | [-1.816 0.127] | -1.28 | 0.024 | [-2.392 -0.168] | -0.94 | 0.092 | [-2.053 0.154] | |
| TE | -6.97 | <0.001 | [-10.579 -3.363] | -1.78 | 0.001 | [-2.868 -0.702] | -1.29 | 0.006 | [-2.212 -0.373] | -2.11 | <0.001 | [-3.223 -0.998] | -1.78 | <0.001 | [-2.872 -0.693] | |
| [Outcome: VAX-I total scale, mediator: V.U., predictor: HL] | [Outcome: F1, mediator: V.U., predictor: HL] | [Outcome: F2, mediator: V.U., predictor: HL] | [Outcome: F3, mediator: V.U., predictor: HL] | [Outcome: F4, mediator: V.U., predictor: HL] | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



