Submitted:
15 May 2025
Posted:
16 May 2025
You are already at the latest version
Abstract
Background: Psychoanalytic concepts of destructiveness point to its deep, unconscious roots, related to primal emotional-motivational mechanisms. Traditional, psychiatric models of suicidal risk assessment focus on classic risk factors, limiting diagnostic and interventional options. This study verifies the neuropsychoanalytic basis of destructive tendencies, integrating the mechanisms of sublimation and evolutionary motivational systems, and redefining their role in the process of destruction. Material and methods: 480 illustrations were generated using artificial intelligence, evaluated by judges competent for interpretative accuracy. The final set was used in a projection task conducted online on a sample of 204 respondents, who also completed the sociodemographic part of the survey. Analyses included factorial exploration of the structure of the tool, assessment of psychometric properties (Cronbach α, ROC, AUC), logistic regression and analysis of intergroup differences. Results: Factor analysis identified eight subscales, six of which correspond to Panksepp's emotional systems, suggesting their subcortical basis. The other two – the pursuit of destruction and its sublimation – go beyond natural evolutionary mechanisms. The desire for destruction was best explained by depression and psychological pain (OR=1.385, p<0.001, AUC=0.783), aggression and impulsivity (OR=1.676, p<0.001, AUC=0.715), and anxiety and a sense of threat (OR=1.554, p<0.001, AUC=0.618). Significant predictors of sublimation of destruction were interest and curiosity (OR=3.152, p<0.001, AUC =0.900), closeness and love (OR=3.432, p<0.001, AUC =0.836), and pleasure and fun (OR=3.081, p<0.001, AUC=0.793). Analyses of intergroup differences showed a higher level of destructiveness in people receiving psychological and psychiatric help, with a previous diagnosis and learning compared to working people (p<0.05). Conclusions: The results indicate that the tool is characterized by high reliability (Cronbach's α>0.87) and diagnostic validity (ROC>0.7), which confirms its potential usefulness in the assessment of destructive and sublimation tendencies and in accordance with the neuropsychoanalytic approach to the theory of drives. Subsequent studies will focus on assessing the external validity of the tool and its application in clinical practice.
Keywords:
destructiveness
; psychometrics
; projective scale
; neuropsychoanalysis
; psychological assessment
1. Introduction
Suicide is a multidimensional phenomenon involving various groups of specialists. Clinical understanding of suicidal behavior is based on the analysis of the interaction of psychological, biological, social and environmental factors. According to the World Health Organization, more than 720,000 people take their own lives every year, making suicide the third cause of death in the 15-29 age group (WHO, 2024). In Poland, about 15 people take their own lives every day, and the number of suicide deaths is twice as high as deaths caused by road accidents (KGP, 2024).
From a health care perspective, effective diagnosis of individuals who reveal suicidal risk is critical in the context of efficient identification of at-risk individuals who require preventive or curative interventions (Ajluni & Amarasinghe, 2024; Gupta et al., 2023; Doupnik et al., 2020).
Psychological questionnaire methods support the diagnosis of suicidal risk. Popular diagnostic tools commonly used in clinical practice include the Beck Scale for Suicide Ideation (BSS), Suicide Behavior Questionaire (SBQ-R), Columbia Suicide Severity Rating Scale C-SSRS or Suicidality Scale (SS) (Nowak & Pawelczyk, 2018). New method proposals are also being developed, such as the 'open sourse' Suicidality Scale (Harris et al., 2023).
The available traditional scales designed to assess suicide risk, despite their high psychometric validity, have documented limitations. A diagnostic weakness is exposure to the possibility of intentional falsification of reality by the respondents or too much attention to the results obtained by clinicians who, by focusing on the analysis of the results, may diminish the importance of clinical observations and information from the therapeutic dialogue (Saab et al., 2022).
In order to gain access to more subtle mental processes and deeper unconscious content, the projective method was developed and used in the course of the presented study, enabling the exploration of the unconscious. Within the framework of psychoanalytic theory, the unconscious is a mental area into which unaccepted content is dissociated. Thus, traditional research, which gives access to informed content, is inevitably associated with limitations affecting the quality and reliability of the assessment. The projective form, by assessing the automatic response to a stimulus, makes it possible to project hidden impulses, conflicts, emotions and drives, with minimized resistance from the subject (Lilienfeld et al., 2000; McGrath et al., 2023; Santillo et al., 2025). This form of examination opens up a unique perspective on the diagnosis of suicide risk.
1.1. Unconscious Processes as the Foundation of Projective Diagnostics
Unconscious processes are aspects of the human psyche that remain outside consciousness, but have an impact on psychological functioning in the cognitive, emotional and behavioral dimensions. According to Sigmund Freud's concept, thanks to the mechanism of repression, unaccepted fears, desires and psychological conflicts are repressed to the unconscious, and although they remain inaccessible to conscious reflection, they affect the formation of personality, emotional reactions, decision-making and the way of acting. On the other hand, thanks to the mechanism of projection, what is hidden in the area of the unconscious can be projected onto external objects, without being aware that it comes from the internal psychic world. In this way, the person who first denies and then projects does not expose themselves to the discomfort resulting from identification with unwanted content. It is on this mechanism that psychological projective methods are based (Cramer, 2006; McWilliams, 2011).
1.2. Freud's Death Drive as a Theoretical Basis for Self-Destructiveness
One of the concepts of understanding human intrapsychic life proposed by Sigmund Freud is the dynamic model. According to it, two dominant drives are at the root of thoughts, feelings and behaviors: life and death. The drive for life (libido) serves the survival of the individual and the species. From a biological perspective, it is represented by a sexual drive, and from a psychological perspective, by a desire for tenderness, closeness, adoration, care and respect. On the other hand, the death drive (Thanatos, or destrudo) is focused on destruction and decay, striving for the original form of non-being. Its occurrence can have both positive and negative dimensions. It leads to destruction, disintegration, destruction and domination, but also to separation, healthy competition, self-determination and the struggle for one's own needs. The process of transforming aggressive and destructive impulses into socially acceptable and even desirable actions occurs within the mechanism of sublimation (Freud, 1923; Freud, 1936).
According to Freud, the source of drives are the organs of the body, which experience satisfaction along with their satisfaction. They are the primary scope of mental functioning, and their impact takes place at the level of the unconscious and precedes reflection. Therefore, the presence of the death drive is an integral element of the human psychic world. However, its severity and impact on the ability to function properly and steadily vary depending on a number of factors (Kacperska, 2024). Based on classical psychodynamic theory, Jaccard and Jacoby developed a model to explain the role of the death drive in suicidal behavior. As a result of the loss of the emotional object of love, the ego experiences weakening. Hostile impulses are redirected to the ego itself, and hateful feelings towards the lost object begin to be experienced as their own defect. In the face of additional adverse circumstances, this can push to fantasies of death and even suicide (Jaccard and Jacoby, 2010; Koweszko, 2024).
Projective methods have the potential to stimulate unconscious processes through the use of ambivalent and symbolic stimuli. In this way, thoughts, emotions, desires and conflicts between the drive for life and death can be revealed, which in other circumstances would not be expressed. The human unconscious operates with symbols that, in the form of archetypes, are to a large extent common to the entire population. In this way, images depicting emotionally charged situations can universally evoke a response from people who experience psychological suffering, tension, conflicts, desires or impulses on an unconscious level (Santillo et al., 2025).
1.3. Neurobiological Basis of Unconscious Processes
According to Paul D. MacLean's theory, the human brain can be divided into three systems, developed at different stages of evolution. These structures include the reptilian brain, the limbic brain, and the neocortex. From the perspective of emotional reactions, the oldest primitive reptilian brain is responsible, m.in other things, for feelings of fear and sexual desire. The limbic system is the center of emotions, social relationships, and memory, but also of unconscious processes that are associated with risky behaviors (Institute of Medicine US, 2011). The youngest structure, the neomammalian brain, is responsible for thinking, consciousness, language and planning. These evolutionarily developed structures determine the functioning of man. The environmental situations and circumstances experienced by the individual, as well as the images presented in projective diagnostic methods, cause the activation of mental processes related to the limbic brain. It is the focus on this area that is the subject of our research interest.
1.4. Suicide Risk Factors
In suicide prevention and clinical practice, an important role is played by the efficient diagnosis and identification of clinical risk factors. Diagnostic assessment of the full picture of the phenomenon requires a multidimensional approach, taking into account factors such as depression, aggressiveness, impulsivity, anxiety, psychological pain and suicidal thoughts.
Depression. Depression is a mental disorder that particularly predisposes to suicidal behavior (Cai et al., 2021). Scientific evidence points to a complex etiopathogenesis of suicide in depression. Risk factors include genetic aspects, exogenous and endogenous stressors (interpersonal, occupational, financial), psychiatric disorders, epigenetic alterations, dysfunctions of the hypothalamic-pituitary-adrenal axis, abnormalities in the neurotransmitter system (especially serotonin), lipid profile, neuroimmune biomarkers, and neurotrophic factors and other neuromodulators (Orsolini et al., 2020). The theoretical basis of depression as a driving force for suicide is a cognitive-behavioral model, such as Beck's theory of hopelessness (Beck et al., 1974; Beck et al., 1993; Bolton et al., 2015).
Aggression. Suicide is an act of aggression, a murder committed on oneself. Aggression, along with impulsivity, stressful life events, mental disorders and a sense of hopelessness, are clinical suicidal risk factors. This is described in various theories explaining the process of suicide, such as the Interpersonal Theory of Suicide (Joiner, 2005; Van Orden et al., 2010), the Cry of Pain Model, and the Stress-Diathesis Model (Cummins et al., 2015).
Impulsivity. Studies confirm the relationship between impulsivity and the risk of engaging in self-destructive behaviors, including suicidal behavior. From the neurobiological level, emotional dysregulation plays an important role here, which can lead to risky activities, including those of a self-aggressive nature. Impulsivity plays an essential role in sudden, violent, and unplanned suicide attempts (Dougherty et al., 2009).
Anxiety disorders are both an independent risk factor for later suicidal thoughts and behaviors, as well as a predictor of suicide attempts in people with mood disorders (Sareen et al., 2005). Chronic anxiety can significantly increase psychological tension and foster the desire to take one's own life (Franklin et al., 2017). Studies of patients admitted to a general psychiatric ward during the year showed that patients diagnosed with F40–F49 had the highest rate of suicide attempts before admission, compared to patients with other diagnoses (Koweszko et al., 2018).
Mental pain. According to Edwin Shneidman's concept of psychological pain, suicide is the result of unbearable mental suffering resulting from the unmet psychological needs (Shneidman, 1993). Shneidman defined psychological pain as "the experience of anguish, suffering, and negative emotions such as terror, despair, fear, grief, shame, guilt, lack of love, loneliness, and loss" (Chodkiewicz et al., 2017). Suicide, therefore, is not so much a desire to take one's own life, but rather a way to break the stream of unbearable pain (Orbach et al., 2003). Bolger described psychological pain in the context of a traumatic event that destroys an individual's personal identity and affects relationships with other people. The result is emotional distress, causing shattering, wounding, diffusion of identity, disconnectedness, and intensification of negative mental states. Various definitions of psychological suffering boil down to understanding it as a persistent, unbalanced, and unpleasant feeling resulting from a negative evaluation of oneself or the loss experienced (Casanova et al., 2021).
Fantasies about death. Suicidal thoughts can take many forms and intensities, from fleeting thoughts of death to specific plans to take one's own life (Casey et al., 2006). From a clinical perspective, they are a warning signal. Research confirms that suicidal thoughts are a predictor of later suicidal actions. The relationship between suicidal thoughts and suicide is described by theoretical concepts such as Shneidman's theory of psychological pain (Shneidman, 1993), Beck's theory of hopelessness (Beck et al., 1979), and Joiner's interpersonal theory (Joiner, 2005). Integrating the above perspectives, it can be assumed that suicidal thoughts are born out of intense, unbearable suffering, accompanied by a pessimistic perception of reality and disturbed relationships with other people.
1.5. Protective Factors of Suicide
Protective factors serve as a crucial safeguard against suicidal thoughts and behaviors. While they play an important role in mitigating suicide risk, they may not be sufficient to fully counteract severe acute risk factors. Assessing these protective elements is essential in suicide prevention. Posner highlights the significance of social support, access to psychological care, and effective coping mechanisms for managing stress (Posner et al., 2014).
Protective factors can be categorized into internal and external influences, both of which contribute to resilience and suicide prevention. Internal protective factors include an individual's ability to cope with stress, frustration tolerance, religious or spiritual beliefs that discourage self-harm, and fear of death or the act of suicide itself. Additionally, identifying clear reasons for living serves as a strong internal safeguard against suicidal thoughts.
On the other hand, external protective factors encompass broader social, familial, and environmental influences that contribute to suicide prevention. These factors include cultural, spiritual, and moral attitudes opposing suicide, a sense of responsibility for children or loved ones, emotional attachment to beloved pets, a supportive social network of family and friends, and positive therapeutic relationships. Engagement in work or education further strengthens psychological resilience and personal stability (Posner et al., 2011; Fowler, 2012; Stanley et al, 2018). Moreover, research shows that protective factors moderate the effects of stress on depression and suicidal behavior (Breton et al., 2015).
1.6. The Role of Artificial Intelligence in the Diagnostic Process
The current direction of suicide prevention research is the use of technological advances such as machine learning (ML) and artificial intelligence (AI) (Grace et al., 2018). This is consistent with the trend of recent years, where the growing role of artificial intelligence algorithms in medical data analysis is observed (Moini, 2021).
The Stanford Institute for Human-Centered Artificial Intelligence defines artificial intelligence as the ability to learn and apply appropriate techniques to solve problems and achieve goals in a changing and uncertain world. A key pillar of AI is machine learning, which allows computers to improve their operations based on experience or database analysis (SIHCAI, 2023). AI enables the analysis of large data sets with exceptional precision, identifying even subtle factors that may indicate an increased risk of suicide. An example is the use of machine learning methods to analyze the words, actions, and gestures of adolescents, which allowed them to effectively distinguish between people with suicidal thoughts and those who did not (Pestian et al., 2016). Machine learning models based on retrospective data analysis, for example in the case of patients with multiple sclerosis, have shown that creating predictive models for specific groups of patients can improve the accuracy of predictions, providing information even several years before a potential suicide attempt (Barak-Corren et al., 2023). In a study of soldiers using outpatient therapy, the use of machine learning software allowed for the identification of a combination of variables that, when combined, showed greater sensitivity in determining individuals at high risk of suicide than many previous models (Rozek et al., 2020).
Machine learning also enables better personalization of treatments and interventions. For example, in the treatment of Treatment-Resistant Depression (TRD), the use of a machine learning algorithm has generated an efficient model with an accuracy of up to 75% in predicting treatment outcomes, thus exceeding the current predictive capabilities of clinical assessment (Kautzky et al., 2018). In addition, it has been observed that the use of short, automated interventions in digital applications to reduce barriers to access to psychological help can increase the use of this type of support by people in mental crisis – even in the case of people experiencing severe mental stress (Jaroszewski et al., 2019).
The ongoing boom in the emergence of new solutions for the detection of suicide risk includes, for example, activities focused on people using social media based on text data, but also modern solutions based on the analysis of text and vocal pattern (Parsapoor et al., 2023). In a meta-analysis by Ehtemam et al. (2024), the authors confirmed the effectiveness of machine learning algorithms in uncovering hidden connections and providing precise predictions about suicide risk, depending on the appropriate selection of algorithms.
1.7. Aim of the Study
The aim of the presented study is to develop and initially validate a multidimensional scale for suicide risk assessment, which, thanks to its projective nature and simplicity, can be an effective screening tool for early identification of people at risk of suicide who require further intervention and support.
2. Methodology
2.1. Study Design and Setting
This study uses artificial intelligence to generate illustrations using advanced machine learning methods that process input data and create unique images. In this way, symbolic and ambiguous projective stimuli were created, which were aimed at activating unconscious processes in the subjects related to repressed emotional conflicts and assumed risk factors: depression, aggressiveness, impulsivity, anxiety, psychological pain and suicidal thoughts. The use of artificial intelligence to create illustrations allowed for the standardization and replicatability of stimuli, as well as the identification of symbols with which a person in emotional crisis can identify. Using the capabilities of artificial intelligence, the authors of the presented method decided to use illustrations created by AI, which are the key to universal patterns of thinking and the collective unconscious, referring to archetypal images and common human experiences. This makes it possible to reach deep-rooted emotions and thoughts that are not always available at the level of conscious processing. The graphics reflect the common elements of the human psyche, which allows for a more universal and effective approach to suicide risk assessment. Thus, the method aims to enable a more precise and holistic recognition of the risks associated with suicide. In the further part of the publication, the process of construction and initial validation of a multivariate projective scale for the assessment of suicide risk is presented.
The survey was conducted electronically using an algorithm that sent an invitation to participate in the study via social media to people who were interested in the subject of mental health crisis. Participation in the study was voluntary and anonymous, and the subjects did not receive any benefits for participation and could discontinue their participation at any time. At the beginning, the respondents were informed about the form and purpose of the study, and sending the completed questionnaire was equivalent to giving informed consent to participate in the study and the subsequent use by the researchers of the obtained data to prepare a scientific publication describing its course and results. In the first part of the survey, the participants were asked to answer about basic general (sociodemographic) data, use of psychotherapy, previous psychiatric treatment and diagnosis, as well as its impact on current well-being.
In the second part of the survey, respondents were asked to choose any number of displayed illustrations that best described their well-being over the past two weeks.
The scale was given the name Morana Scale. The name comes from the name of the Slavic goddess who was responsible for the death of vegetation in winter and the rebirth of nature in spring. Moran's name derives from the Proto-Indian root mar- or mor-, which means death (Shiyevsky, 2003; Kempiński, 2000).
2.1.1. Competent Judges Procedure
At the initial stage of the construction of the Morana Scale, the researchers created 480 illustrations assigned to 12 theoretical reference frameworks that referred to risk factors and protective factors of suicide. Six clinical risk scales and the same number of opposing protective scales included the following pairs of theoretical factors: fantasies about death - desire for life, impulsivity - reflexivity/balance, depression - vitality/affirmation of life, mental pain - pleasure/relief/bliss, anger/aggression - composure/calmness, and anxiety - sense of security.
480 images were generated using a virtual image creator based on an artificial intelligence (fotor.com) model. In order to limit the number of illustrations and select those that most accurately relate to each category, the images were presented to 15 experts, who took on the role of competent judges. Psychiatrists, clinical psychologists and certified psychotherapists have been invited to this group. The subjects rated each of the illustrations on a 5-point Likert scale in relation to the category they were supposed to represent. After the study, the researchers identified 120 illustrations that were rated the highest (20 for each category). After selecting the illustrations that most accurately represented each category, the researchers prepared an electronic questionnaire to conduct the study. In order to maintain randomness in the order of individual illustrations, a pseudo-random number generator was used when creating the survey.
2.2. Study Population
The study included 204 adults aged 18-66 years (M=30.34). The characteristics of the study group are presented in Table 1.
2.3. Ethical Considerations
The study program and procedure were reported to the Bioethics Committee of the Medical University of Warsaw, which did not raise any objections to the methodology of the study (no. AKBE/322/2024).
2.4. Data Analysis
Statistical analyses were carried out using the Statistica 13.3 program enriched with the Plus Set licensed by the Medical University of Warsaw. In the course of the statistical analyses, a number of methods were used to accurately assess the effectiveness and reliability of the developed multidimensional scale for assessing the risk of destructiveness. First, factor analysis with Varimax rotation was carried out, which allowed to identify hidden structures in the data, reduce their dimensionality and simplify the interpretation of the results.
Then, in order to assess the reliability of the scale, Cronbach's alpha tests were used, which made it possible to determine the internal consistency of individual subscales. In addition, Spearman's rho correlations were used to analyze the relationships between variables, which allowed them to study nonlinear relationships in the data.
To assess the differences between the groups, the Mann-Whitney U test was used, which is appropriate for nonparametric comparisons. Finally, logistic regression was performed to analyse the effect of independent variables on the dependent variable, both in univariate and multivariate versions, which made it possible to investigate the interplay between different factors and the risk of destructiveness.
All relationships, correlations and regressions and differences were statistically significant at p≤0.05.
3. Results
3.1. Factor Extraction
In order to extract the subscales, a Varimax factor analysis was performed using the principal axis method. A minimum level of charging factors above the threshold of 0.3 was assumed. In the case of the first factor (depression and mental pain subscale), which was charged by a larger number of items, the threshold was assumed at the level of 0.4. After a factor analysis, the initial assumption of the existence of 12 subscales was modified in the light of the data obtained. As a result, seven factors were initially identified, and the previous assumptions were revised. However, when analyzing the data obtained, it was noticed that factor 4, which referred to death and destruction, had individual items that did not match the others. In order to understand the observed inconsistencies, reference was made to the theoretical foundations of Freud's concept of the death drive (Thanatos). As a result, it was found that the Destruction factor exhibits two properties: the desire for destruction and its sublimation. Therefore, it was decided that two separate subscales would be created to reflect alternative ways of processing the death drive. Items included in these factors were assigned on the basis of factor analysis, but also after a qualitative assessment made by the researchers, based on theoretical assumptions.
The qualitative analysis of the illustrations classified into individual categories, created within the framework of the eight factors, allowed us to give them working names, partly referring to the original theoretical assumptions. The resulting subscales have been predefined as: depression and mental pain subscale, interest and curiosity subscale, aggression and impulsivity subscale, striving for destruction subscale, sublimation of destruction subscale, pleasure and fun subscale, closeness and love subscale, anxiety and sense of threat subscale.
In order to assess reliability, a standardized Cronbach Alpha coefficient with a tetrachoric r correlation matrix (iterative approximation) was determined for each factor. Cronbach's alpha values are shown in Table 2.
3.2. Exploratory Analyses
In the first stage, correlation analyses were carried out, which revealed the relationships between individual scales.

Table 3.
Analysis of Spearman's rho correlation between individual factors and the age and number of children.
Table 3.
Analysis of Spearman's rho correlation between individual factors and the age and number of children.
|
Variable |
Spearman BD rank order correlation removed in pairs Tagged wsp. correlations are significant with p <.05000 | |||||||||
| P1 | P2 | P3 | P4a | P4b | P5 | P6 | P7 | Age | Number of children |
|
| P1 | 1,000000 | -0,058535 | 0,387499 | 0,482755 | 0,088370 | 0,052134 | -0,031750 | 0,309309 | -0,075765 | -0,019890 |
| P2 | -0,058535 | 1,000000 | 0,115889 | -0,064020 | 0,764871 | 0,562732 | 0,649300 | 0,068333 | 0,110310 | -0,012671 |
| P3 | 0,387499 | 0,115889 | 1,000000 | 0,438977 | 0,276512 | 0,066142 | 0,086215 | 0,571672 | -0,048134 | -0,019135 |
| P4a | 0,482755 | -0,064020 | 0,438977 | 1,000000 | 0,051944 | 0,090922 | -0,024448 | 0,246764 | -0,196011 | -0,083470 |
| P4b | 0,088370 | 0,764871 | 0,276512 | 0,051944 | 1,000000 | 0,548530 | 0,602709 | 0,172824 | 0,082679 | -0,005097 |
| P5 | 0,052134 | 0,562732 | 0,066142 | 0,090922 | 0,548530 | 1,000000 | 0,397669 | 0,033504 | -0,016179 | -0,077119 |
| P6 | -0,031750 | 0,649300 | 0,086215 | -0,024448 | 0,602709 | 0,397669 | 1,000000 | 0,051111 | 0,025818 | 0,099400 |
| P7 | 0,309309 | 0,068333 | 0,571672 | 0,246764 | 0,172824 | 0,033504 | 0,051111 | 1,000000 | 0,036608 | 0,029394 |
| Age | -0,075765 | 0,110310 | -0,048134 | -0,196011 | 0,082679 | -0,016179 | 0,025818 | 0,036608 | 1,000000 | 0,595009 |
| Number of children | -0,019890 | -0,012671 | -0,019135 | -0,083470 | -0,005097 | -0,077119 | 0,099400 | 0,029394 | 0,595009 | 1,000000 |
P1=subscale of depression and mental pain, P2=subscale of exploring the world/interest in reality, P3=subscale of aggression and impulsivity, P4a=subscale of striving for destruction, P4b=subscale of sublimation of destruction, P5=subscale of pleasure and fun, P6=subscale of closeness and love, P7=subscale of fear and sense of threat.
Striving for destruction. The subscale of striving for destruction positively correlates with the subscale of depression and mental pain (rho=0.4827), the subscale of aggression and impulsivity (rho=0.4389), the subscale of anxiety and sense of threat (rho=0.2467) and negatively with age (rho=-0.1960). Anxiety is additionally correlated with depression and mental pain (rho=0.3093) and aggression and impulsivity (rho=0.5716). Difficulties in regulating the emotions associated with depression can lead to violent, uncontrollable behavior, and psychological discomfort can exacerbate destructive tendencies. In addition, people experiencing depression often experience an increased sense of threat and fear, which creates a state of increased mental tension and promotes impulsivity. As a result, the above-mentioned mental states can be considered potentially conducive to the pursuit of destruction. The risk of destructiveness appears to decrease with age, which puts younger people at higher risk.
Sublimation of destruction. The subscale of destruction sublimation positively correlates with the interest and curiosity subscale (rho=0.7648), the pleasure and play subscale (rho=0.5485), the closeness and love subscale (rho=0.6027) and the aggression and impulsivity subscale (3) (rho=0.2765) and the anxiety and threat subscale (rho=0.1728). Sublimation of destruction is a mechanism that transforms negative impulses into more constructive actions. There is a clear link between sublimation and curiosity, playfulness, and closeness, which may suggest positive coping strategies. In contrast, weaker correlations with impulsivity and anxiety may indicate some elements of anxiety or emotional reactivity, but not their dominant influence.
Modelling Destructive Tendencies: Statistical Pathways to Risk and Transformation
Logistic regression analyses were conducted to better understand the dynamics of the psychological processes that promote destruction, as well as the mechanism by which destructive impulses are transformed into constructive actions. The division of the results into groups of high and low destructiveness and sublimation of destruction was made on the basis of the limit determined as the mean plus half of the standard deviation. Due to the unequal size of groups with low and high destructiveness and sublimation (tendency to destruction: 48:156; sublimation of destruction: 49:155), statistical weighting was used to increase sample representativeness, adjust the impact of individual observations and improve the comparability of results.
In order to better understand the dynamics of the processes involved in destruction and its sublimation, two types of logistic regression analyses were performed. First, univariate models were applied for each of the dependent variables (striving for destruction and sublimation of destruction), allowing the assessment of the individual impact of individual predictors. Then, multivariate models were created, taking into account the broader context of the interplay of variables. Comparison of the results of both approaches allowed for a more precise interpretation of the mechanisms affecting the risk of destruction and its sublimation strategies. Table 4 presents a comparison of the results obtained for the dependent variables: striving for destruction and sublimation of destruction, respectively.
Comparison of univariate and multivariate models
Striving for destruction
Depression and psychological pain are a strong predictor of destructive tendencies, both as a single variable (OR=1.385) and after adjusting for other factors (OR=1.333. In both models, a large statistically significant effect is observed, although in the multivariate model the OR decreases slightly.
Interest and curiosity are a trait that can reduce the drive to destruction, but only after taking into account other variables. Although in the univariate model the effect is statistically insignificant (OR=0.953), in the multivariate model it becomes moderate (OR=0.748) and has a protective character against destructive tendencies.
Aggression and impulsivity is also a statistically significant variable, although its impact decreases after taking into account other factors. In the univariate model, a large effect is observed (OR=1.676), while in the multivariate model it weakens significantly (OR=1.284).
There is no significant effect indicating a relationship between the sublimation of destruction and the pursuit of destruction.
Pleasure and fun also reveal some connection with destructive tendencies, although it is small. In the univariate model, the effect was very small (OR=1.146), and in the multivariate model it increases slightly, but it still remains small (OR=1.210) and statistically insignificant.
Closeness and love reveals a protective effect against destruction, which is slightly stronger in the multivariate model (OR=0.813), but still remains small and statistically insignificant.
Anxiety and a sense of threat lose their significance in the multivariate model, although in the univariate the effect is large (OR=1.554).
In summary, the drive for destruction is motivated by depression, aggression, and anxiety, and weakened by interest and curiosity, although only in a multivariate model. The strongest predictor of destruction is depression and mental pain. An increase in depression and psychological pain by one point increases the risk of seeking destruction by 38 in the univariate model and 33% in the multivariate model, respectively.
Sublimation of destruction
Depression and psychological pain are not a significant variable in the context of sublimation of destruction. In the univariate model, the effect is small (OR=1.071), and in the multivariate model, it disappears completely (OR=1.026).
Interest and curiosity strongly influence the sublimation of destruction, both in the univariate (OR=3.152) and multivariate (OR=2.431) models, although in the latter the effect weakens slightly.
Aggression and impulsivity is a variable that creates a stable effect that is moderate, both in the univariate (OR=1.348) and multivariate models.
The pursuit of destruction does not have a significant impact on the sublimation of destruction. In a univariate model, the effect is weak but positive (OR=1.126), while in a multivariate model model, it becomes negative (OR=0.807). This may suggest that the sublimation of destruction does not result from destructive tendencies, but may be an alternative form of dealing with them.
Pleasure and fun are an important factor in the sublimation of destruction. In the univariate model, the effect is large (OR=3.081), although in the multivariate model it weakens slightly (OR=2.072), and in both cases it remains statistically significant.
Closeness and love have a positive effect on the sublimation of destruction, although the effect that is large in the univariate model (OR=3.432) becomes moderate in the multivariate model (OR=1.494).
Anxiety and a sense of threat are a less important variable. In a univariate model, it has a medium impact (OR=1.433), and in a multivariate model, it decreases to a small one (OR=1.340).
In summary, the sublimation of destruction is associated with interest and curiosity, closeness and love, and pleasure and fun. The most stable predictor of sublimation of destruction is interest and curiosity. An increase in this subscale by one point increases the chances of sublimation of destruction by 215% in the univariate model and 107% in the multivariate model.
A multivariate model for the pursuit of destruction and sublimation of destruction for all factors is illustrated in Figure 1.
Age and offspring
Additional regression analyses concerning the effect of age on destructive tendencies indicate that it is a protective factor against the tendency to destructive, although the effect is small and variable is not a key predictor of destructive tendencies. In the multivariate model, after taking into account the number of children, the effect is enhanced. The odds ratio suggests that with each year of life, the risk of seeking destruction decreases by 4.1% in the univariate model and by 5.3% in the multivariate model. The effect of age on sublimation of destruction is minimal and statistically insignificant.
Having children is not a statistically significant variable in the context of sublimation of destruction in any model. The results of logistic regression for the age and number of children in the context of striving for destruction and its sublimation are presented in Table 5.
ROC Curve Analysis
In order to assess the effectiveness of predictive models for individual subscales and to determine optimal cut-off points in the context of striving for destruction and its sublimation, ROC curve analyses were performed. The results are presented in Table 6.
Analysis of the ROC curve for depression and mental pain (AUC= 0.78) indicates that the model has good classification ability. The variable represents a strong predictor of destruction, the cut-off point is 3, indicating that people with higher depression scores have a higher risk of destruction. The parameters of the model indicate a relatively balanced ability to correctly identify people who seek destruction and those who do not.
The ROC curve for aggression and impulsivity (AUC=0.715) indicates moderately good predictive ability. The properties of the model suggest that it is slightly better at correctly excluding people without seeking destruction. The cutoff point for the destruction classification is 1. The model is able to identify people prone to destruction and has a relatively low level of false positives, indicating high classification accuracy.
Anxiety and a sense of threat as a predictor of destruction are characterized by moderate effectiveness (AUC=0.618), weaker than in the case of the previous two factors. The cutoff point for predicting destruction is 2. The model is much better at ruling out the drive for destruction than at correctly identifying it, and some level of false classifications can be expected.
The ROC curve for the interest and curiosity subscale indicates very good predictive ability (AUC=0.900). The parameters of the model indicate very good balance and effectiveness of the model. The cut-off point is 2.
The pleasure and play subscale is characterized by good predictive ability (AUC=0.793). The model shows balanced sensitivity and specificity, and the cut-off point for identifying individuals sublimating destruction is 1.
Analysis of the ROC curve for closeness and love as a predictor of sublimation of destruction indicates a very good predictive ability. The model is characterized by good balance and effectiveness. The factor may allow for effective differentiation of people who are more likely to sublimate destructive impulses. The cut-off point is 1.
Intergroup differences
The last stage of the analysis included the assessment of intergroup differences in the participation of the respondents in psychotherapy, the use of psychiatric treatment, having a psychiatric diagnosis and professional activity.
The subscale of striving for destruction was the only one that differentiated the respondents in terms of participation in psychotherapy (U=3997.500, p<0.03), psychiatric treatment (U=4151.500, p<0.03), psychiatric diagnosis (U=4124.500, p<0.02) and professional activity. Respondents who participated in psychotherapy, psychiatric help and had a psychiatric diagnosis obtained higher results than those who did not use such forms of help. On the other hand, in the context of professional activity, learners showed a higher level of striving for destruction than economically active people (U=3598,000, p<0.01). However, no significant differences were found in the case of students and employed people and the unemployed.
4. Discussion
The study presented the process of construction and initial validation of the psychometric Morana Scale, a projective method for diagnosing the risk of destructiveness created using artificial intelligence. In accordance with the original theoretical assumptions, the initial subscales were based on clinical determinants of suicide, such as depression, aggressiveness, impulsivity, anxiety, psychological pain and fantasies about death. The authors' primary goal was to create a tool for assessing the risk of suicide, but the results obtained in the course of the analyses prompt a certain modification of this idea and the scope of diagnostic usefulness of the scale. The final shape of the subscales indicates that the method is rather intended to differentiate people prone to destruction from those who subject aggressive impulses to sublimation, and thus reduce the risk of threatening activities in favor of developmental activities consistent with social norms.
In the course of our analyses, we noticed that the identified factors, forming the proper subscales, refer to the neural mechanisms of emotions described by Jaak Panksepp, who distinguished seven primary emotional systems located in the subcortical areas (Panksepp & Biven, 2012; Murawiec, 2023). Six of our eight factors reflected the brain's neural systems. Only two of them - striving for destruction and sublimation of destruction - did not fit into the above theoretical framework, which will be discussed and explained below.
Panksepp's emotional systems are universal not only for humans, but for all mammals (Żechowski, 2017). Their original nature confirms our assumptions about the diagnostic tool being created, so that the method allows us to reach preverbal states of mind relating to unconscious content (Davis & Montag, 2019). Therefore, we decided to link the obtained subscales with emotional systems. Thus, we related the subscale (1) of depression and mental pain to the panic/sadness system (PANIC/GRIEF). We considered the subscale (2) of interest and curiosity to be identical with the search system (SEEKING). The subscale (3) of aggression and impulsivity reflects the rage system (RAGE). The subscale (5) of pleasure and play refers to the play system (PLAY). The subscale (6) of closeness and love is the system of care (CARE), and the subscale (7) of fear and sense of threat describes the system of fear (FEAR). The only system from the Panksepp's classification that was not referenced on our scale was the desire system (LUST).
The separate subscales that did not fit into Panksepp's theory were two subscales reflecting complementary mechanisms of processing the death instinct. The first refers to the pursuit of annihilation, while the second describes the mechanism of sublimation, in which destructive impulses are transformed into constructive and socially acceptable activities. The fact that the scale of destruction does not fit into the classification of primary neuronal systems may be due to its non-adaptive dimension for survival. Thus, it does not constitute a permanent representation of the neural system, but rather is characterized by states of pathological experience that interfere with emotional and motivational processes. On the other hand, the scale of death sublimation may reveal mechanisms analogous to those within the desire system (LUST), where primal, raw biological drives are transformed into socially affirmed behaviors related to desire and intimacy, e.g. for the creation of love relationships or starting a family (Montag & Davis, 2018; Davis & Montag, 2019; Fuchshuber et al., 2023).
The presented study revealed a number of connections between the pursuit of destruction and its sublimation, and individual variables representing specific mental states. The observed associations, visible between the subscales of the Morana Scale, are consistent with the current scientific knowledge, which confirms the potential predictive usefulness of the method in diagnosing the risk of suicide. In our analyses, the drive for destruction is most influenced by depression and mental pain, but also by aggression and impulsivity, as well as anxiety and a sense of threat. The literature commonly associates depression with a high risk of suicidal thoughts and behaviours (Eikelenboom et al., 2012), as well asmpulsivity and aggressiveness (Conner et al., 2004; Moore et al., 2022) and anxiety disorders (Busby Grant et al., 2023).
A clinical example illustrating the relationship between these traits and destructiveness is borderline personality disorder. The above range of mental states in this disorder is conducive to an increased risk of suicide. People with borderline disorder often experience intense and unstable feelings, have difficulty regulating emotions, and take impulsive, aggressive actions, including repeated acts of self-harm and suicidal behavior (Chapman et al., 2024).
On the other hand, the sublimation of destruction is a psychological defense mechanism that allows negative impulses to be transformed into constructive actions. The analysis showed a relationship between the sublimation of destruction and openness to new experiences and curiosity, the search for pleasure and fun, as well as closeness and love. Research on the relationship between openness to new experiences and health provides diverse conclusions. This trait can contribute to beneficial effects, but also to negative effects. Bresin and Hunt showed that there is a positive relationship between openness to new experiences and non-suicidal self-harm (Bresin & Hunt, 2023). At the same time, this trait is a protective factor in relation to all-cause mortality (Ferguson & Bibby, 2012). Some researchers assume that a low level of openness to new experiences may promote suicidal behavior due to reduced adaptive abilities due to cognitive rigidity, a limited repertoire of behaviors, and a strongly defined identity (Duberstein, 1995). On the other hand, people with a high level of openness to new experiences are characterized by a greater ability to think divergently, innovative problem-solving strategies, and creative achievement (Abu Raya et al., 2023). This may explain the observation made in our study that interest and curiosity are the strongest predictors of sublimation of destruction.
Another factor that influences the constructive transformation of destructive impulses is pleasure and play. As Davidson et al. writes, such positive experiences can play an important role in the recovery of people with mental disorders (Davidson et al., 2006). The experience of pleasure is a complex neurobiological phenomenon based on reward pathways and limbic activity. It can support cognitive processes, productivity, and health, but at the same time lead to negative behaviors. Moderate pleasurable experiences can increase biological flexibility and health, but seeking out artificial stimulants can be detrimental and lead to addiction (Esch & Stefano, 2004). This duality was also revealed in the analyses of the results presented in our study, where the subscale of pleasure and play was associated not only with the sublimation of destruction, but also with the pursuit of it, as opposed to the protective influence of interest and curiosity as well as closeness and love.
Closeness and love are the last of the three predictors of sublimation of destruction identified in the process of constructing the Morana Scale. Research shows that the health-promoting function of closeness and love, which reduces the risk of destruction, is a decrease in cortisol levels, activation of the reward system, reduction of the risk of depressive and anxiety disorders, increase mental resilience and improve the physical condition of the body (Snir et al., 2020). The importance of this type of experience is crucial from the first moments of life, when the stress axis (HPA) and the oxytocin system are intensively activated. If the first physical contact between mother and baby occurs immediately after birth, the oxytocin system, which has anti-stress potential, becomes more pronounced, which in turn has a long-term impact on the baby's health (Uvnäs-Moberg et al., 2024). From the perspective of psychological processes, later in life, love and closeness can create a safe environment in which the emotional exchange of difficult affects can proceed in a more stable way based on sublimation rather than violent destructive reactions (Shean & Mander, 2020).
The mechanism of sublimation of destruction may be a key protective factor in the context of suicidal risk and other forms of self-harm. The observed associations with health-promoting competences can be related to the Freudian definition of health, described as the ability to work and love (Werbart et al., 2020). The mechanism of sublimation of destruction would be a key aspect in this case in terms of transforming potentially harmful impulses from biological, primary layers of experience into more mature ones conducive to building interpersonal relationships and professional productivity.
With regard to Melanie Klein's concept, it can be assumed that the ability to transform hateful and destructive impulses into constructive forms is related to the quality of the relationship with the original object, usually the mother. It is how the child experiences the mother, both in good and bad aspects, that shapes the ability to cope with his own aggression. According to Klein's assumptions, sublimation is a mental process that allows aggression and hatred to be transformed into creative and prosocial activities, which in turn determines mental health (Iwaszuk, 2021; Glover, 2019; Thieberger, 1991).
Lacan, on the other hand, understood sublimation as the transfer of the drive from its original goal to the space of more symbolic satisfaction. According to his thought, the primordial energy can be transformed into forms for creation and development, e.g. in the form of art, literature or philosophy. Following Lacan's thought, where sublimation finds reference to language and symbols, destruction can be transformed into art and literature that explore the dark aspects of the human mind (Saint-Cyr, 2012; Nobus, 2022).
The last aspect of the analysis included a comparison of the respondents in terms of all subscales in the context of professional activity, the use of psychological and psychiatric help, as well as having a psychiatric diagnosis. The differences were revealed only in the context of striving for destruction. Learners showed stronger inclinations towards destruction than working people. This may be related to age. A large study spanning 90 countries found that young learners show a higher risk of suicide than any other age group (Campisi et al., 2020). Similarly, a study by Yan et al. (2024) indicates that school-aged and college-aged people may be at higher risk of suicidal thoughts than older working people. Although only adults participated in our study, they were still relatively the youngest of the entire study group.
Interestingly, people who received the help of a psychologist or psychiatrist, and those who had a diagnosis, showed a higher level of striving for destruction than those who were not treated. This may be due to the fact that people with stronger destructive impulses are more likely to come into contact with a mental health professional at some point in their lives, e.g. as a result of crisis intervention, hospitalization or other activities related to their risky or threatening behaviour. Research confirms that not all people in mental crisis seek professional help, often delay the decision to seek treatment, and come to psychiatric care not on their own initiative, but rather as a result of contact with health care structures (Larsen et al., 2021).
The presented study made it possible to construct a tool, isolate factors and assess their reliability. From the perspective of theoretical foundations, the method is a kind of bridge between classical psychoanalytic assumptions regarding the death drive and modern knowledge in the field of neurobiological understanding of emotional-motivational processes. The obtained results prove satisfactory psychometric parameters of the method and the predictive value of the identified subscales in relation to the pursuit of destruction and its sublimation.
In the next stage, research is planned to assess the validity of the external scale in relation to indicators of general suicidality risk, specific risk factors consistent with theoretical assumptions, as well as Panksepp's emotional systems associated with scales in the final analyses.
Constraints on Generality
The study has some limitations. Initial validation was performed on a limited sample of subjects, with a significant predominance of female subjects, which may limit the possibility of generalizing the results to a wider clinical population. In addition, limitations in sample size and the use of convenience samples may have affected the stability of the results and the consistency of the factor structure (Boateng et al., 2018). A controversial aspect of the presented study may also be the projective nature of the method being developed, which is based on an interpretative mechanism that is susceptible to the influence of subjective factors on the part of both the researcher and the subject (Clark & Watson, 1995). This type of diagnosis uses ambiguous symbolic stimuli, which makes standardization difficult and raises doubts among some researchers and clinicians (Santillo et al., 2025; Stemplewska-Żakowicz & Paluchowski, 2013). This may be related to the difficulty of unambiguously linking symbolic visual content with specific suicide risk factors. In this respect, the projective formula, although allowing access to more unconscious content, is in itself considered insufficient (DeVellis, 2016).
5. Conclusions
- The satisfactory psychometric properties of the tool indicate that it can provide effective support in clinical diagnosis, especially in the assessment of people at high risk of self-aggressive behaviour.
- The tendency to destroy and the tendency to sublimate it should be diagnosed on the basis of unconscious processes.
- Interest and curiosity, pleasure and fun, and closeness and love support the mechanisms of sublimation of destruction, suggesting the need to develop therapeutic strategies based on positive motivation rather than just reducing risky behaviors.
- The results of the presented research are a point of contact between the psychoanalytic approach and modern neurobiological knowledge, which opens up the possibility of integrative therapeutic methods.
- The next step in the presented study is to assess the external validity of the Morana Scale in order to determine its usefulness in clinical practice, including the assessment of suicidal risk. It is also advisable to investigate the possibility of adapting the tool to different clinical groups in order to improve the effectiveness of interventions in different therapeutic contexts.
References
- Ajluni, V.; Amarasinghe, D. Youth suicide crisis: Identifying at-risk individuals and prevention strategies. Child and Adolescent Psychiatry and Mental Health 2024, 18, 58. [Google Scholar] [CrossRef] [PubMed]
- Barak-Corren, Y.; Castro, V.M.; Javitt, S.; Nock, M.K.; Smoller, J.W.; Reis, B.Y. Improving risk prediction for target subpopulations: Predicting suicidal behaviors among multiple sclerosis patients. PLOS ONE 2023, 18, e0277483. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Ranieri, W.F. Scale for suicide ideation: Psychometric properties of a self-report instrument for measuring suicidal ideation. Journal of Consulting and Clinical Psychology 1979, 47, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quinonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Frontiers in Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Bolton, J.M.; Gunnell, D.; Turecki, G. Suicide risk assessment and intervention in people with mental illness. BMJ 2015, 351, h4978. [Google Scholar] [CrossRef]
- Bresin, K.; Hunt, R.A. The downside of being open-minded: The positive relation between openness to experience and nonsuicidal self-injury. Suicide and Life-Threatening Behavior 2023, 53, 282–288. [Google Scholar] [CrossRef]
- Breton, J.J.; Labelle, R.; Berthiaume, C.; Royer, C.; St-Georges, M.; Ricard, D.; Abadie, P.; Gérardin, P.; Cohen, D. ; Guilé; JM Protective factors against depression and suicidal behaviour in adolescence. Canadian journal of psychiatry. Revue canadienne de psychiatrie 2015, 60(2 Suppl 1), S5–S15. [Google Scholar]
- Busby Grant, J.; Batterham, P.J.; McCallum, S.M.; Werner-Seidler, A.; Calear, A.L. Specific anxiety and depression symptoms are risk factors for the onset of suicidal ideation and suicide attempts in youth. Journal of Affective Disorders 2023, 327, 299–305. [Google Scholar] [CrossRef]
- Cai, H.; Xie, X.M.; Zhang, Q.; Cui, X.; Lin, J.X.; Sim, K.; Ungvari, G.S.; Zhang, L.; Xiang, Y.T. Prevalence of suicidality in major depressive disorder: A systematic review and meta-analysis of comparative studies. Frontiers in Psychiatry 2021, 12, 690130. [Google Scholar] [CrossRef]
- Campisi, S.C.; Carducci, B.; Akseer, N.; et al. Suicidal behaviours among adolescents from 90 countries: A pooled analysis of the global school-based student health survey. BMC Public Health 2020, 20, 1102. [Google Scholar] [CrossRef]
- Casanova, M.P.; Nelson, M.C.; Pickering, M.A.; et al. Measuring psychological pain: Psychometric analysis of the Orbach and Mikulincer Mental Pain Scale. Measurement Instruments for the Social Sciences 2021, 3, 7. [Google Scholar] [CrossRef]
- Casey, P.R.; Dunn, G.; Kelly, B.D.; et al. Factors associated with suicidal ideation in the general population. British Journal of Psychiatry 2006, 189, 410–415. [Google Scholar] [CrossRef]
- Chapman, J.; Jamil, R.T.; Fleisher, C.; Torrico, T.J. (2024). Borderline personality disorder. In StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
- Chodkiewicz, J.; Miniszewska, J.; Strzelczyk, D.; Gąsior, K. Polish adaptation of the Psychache Scale by Ronald Holden and co-workers. Psychiatria Polska 2017, 51, 369–381. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. Psychological Assessment 1995, 7, 309–319. [Google Scholar] [CrossRef]
- Conner, K.R.; Meldrum, S.; Wieczorek, W.F.; et al. The association of irritability and impulsivity with suicidal ideation among 15- to 20-year-old males. Suicide and Life-Threatening Behavior 2004, 34, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Cramer, P. (2006). Protecting the self: Defense mechanisms in action. New York: Guilford Press.
- Cummins, N.; Scherer, S.; Krajewski, J.; Schnieder, S.; Epps, J.; Quatieri, T.F. A review of depression and suicide risk assessment using speech analysis. Speech Communication 2015, 71, 10–49. [Google Scholar] [CrossRef]
- Davidson, L.; Shahar, G.; Lawless, M.S.; Sells, D.; Tondora, J. Play, pleasure, and other positive life events: "Non-specific" factors in recovery from mental illness? Psychiatry 2006, 69, 151–163. [Google Scholar] [CrossRef]
- Davis, K.L.; Montag, C. Selected principles of Pankseppian affective neuroscience. Frontiers in Neuroscience 2019, 12, 1025. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale development: Theory and applications, 4th ed.; Sage Publications: Thousand Oaks, CA, 2016. [Google Scholar]
- Dougherty, D.M.; Mathias, C.W.; Marsh-Richard, D.M.; Prevette, K.N.; Dawes, M.A.; Hatzis, E.S.; Palmes, G.; Nouvion, S.O. Impulsivity and clinical symptoms among adolescents with non-suicidal self-injury with or without attempted suicide. Psychiatry Research 2009, 169, 22–27. [Google Scholar] [CrossRef]
- Doupnik, S.K.; Rudd, B.; Schmutte, T.; Worsley, D.; Bowden, C.F.; McCarthy, E.; Eggan, E.; Bridge, J.A.; Marcus, S.C. Association of suicide prevention interventions with subsequent suicide attempts, linkage to follow-up care, and depression symptoms for acute care settings: A systematic review and meta-analysis. JAMA Psychiatry 2020, 77, 1021–1030. [Google Scholar] [CrossRef]
- Duberstein, P.R. Openness to experience and completed suicide across the second half of life. International Psychogeriatrics 1995, 7, 183–198. [Google Scholar] [CrossRef]
- Ehtemam, H.; Sadeghi Esfahlani, S.; Sanaei, A.; Ghaemi, M.M.; Hajesmaeel-Gohari, S.; Rahimisadegh, R.; Bahaadinbeigy, K.; Ghasemian, F.; Shirvani, H. Role of machine learning algorithms in suicide risk prediction: A systematic review-meta analysis of clinical studies. BMC Medical Informatics and Decision Making 2024, 24, 138. [Google Scholar] [CrossRef]
- Eikelenboom, M.; Smit, J.H.; Beekman, A.T.; Penninx, B.W. Do depression and anxiety converge or diverge in their association with suicidality? Journal of Psychiatric Research 2012, 46, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Esch, T.; Stefano, G.B. The neurobiology of pleasure, reward processes, addiction and their health implications. Neuro Endocrinology Letters 2004, 25, 235–251. [Google Scholar] [PubMed]
- Ferguson, E.; Bibby, P.A. Openness to experience and all-cause mortality: A meta-analysis and r(equivalent) from risk ratios and odds ratios. British Journal of Health Psychology 2012, 17, 85–102. [Google Scholar] [CrossRef] [PubMed]
- Fowler, J.C. Suicide risk assessment in clinical practice: pragmatic guidelines for imperfect assessments. Psychotherapy (Chicago Ill.) 2012, 49, 81–90. [Google Scholar] [CrossRef]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; et al. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin 2017, 143, 187–232. [Google Scholar] [CrossRef]
- Freud, A. (2007). The ego and the mechanisms of defense. International Universities Press.
- Freud, S. (2018). The ego and the id. W. W. Norton & Company.
- Fuchshuber, J.; Prandstätter, T.; Andres, D.; Roithmeier, L.; Schmautz, B.; Freund, A.; Schwerdtfeger, A.; Unterrainer, H.F. The German version of the brief affective neuroscience personality scales including a LUST scale (BANPS-GL). Frontiers in Human Neuroscience 2023, 17, 1213156. [Google Scholar] [CrossRef]
- Glover, E. Sublimation, substitution and social anxiety. Essaim 2019, 36, 7–14. [Google Scholar] [CrossRef]
- Grace, K.; Salvatier, J.; Dafoe, A.; Zhang, B.; Evans, O. When will AI exceed human performance? Evidence from AI experts. Journal of Artificial Intelligence Research 2018, 62, 729–754. [Google Scholar] [CrossRef]
- Gupta, M.; Esang, M.; Moll, J.; Gupta, N. Inpatient suicide: Epidemiology, risks, and evidence-based strategies. CNS Spectrums 2023, 28, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.M.; Wang, L.; Mu, G.M.; et al. Measuring the suicidal mind: The ‘open source’ Suicidality Scale, for adolescents and adults. PLOS ONE 2023, 18, e0282009. [Google Scholar] [CrossRef]
- Institute of Medicine (US) and National Research Council (US) Committee on the Science of Adolescence. (2011). The science of adolescent risk-taking: Workshop report. Washington, DC: National Academies Press. Available from: https://www.ncbi.nlm.nih.gov/books/NBK53414/.
- Iwaszuk, M. Between thought and action: Symbolization in depressive position and its external expressions. Journal of Education Culture and Society 2021, 12, 13–25. [Google Scholar] [CrossRef]
- Jaccard, J.; Jacoby, J. (2010). Theory construction and model-building skills: A practical guide for social scientists. New York: Guilford Press.
- Jaroszewski, A.C.; Morris, R.R.; Nock, M.K. Randomized controlled trial of an online machine learning-driven risk assessment and intervention platform for increasing the use of crisis services. Journal of Consulting and Clinical Psychology 2019, 87, 370–379. [Google Scholar] [CrossRef]
- Kautzky, A.; Dold, M.; Bartova, L.; Spies, M.; Vanicek, T.; Souery, D.; Montgomery, S.; Mendlewicz, J.; Zohar, J.; Fabbri, C.; Serretti, A.; Lanzenberger, R.; Kasper, S. Refining prediction in treatment-resistant depression: Results of machine learning analyses in the TRD III sample. The Journal of Clinical Psychiatry 2018, 79, 16m11385. [Google Scholar] [CrossRef]
- Kempiński, A.M. (2000). Encyklopedia mitologii ludów indoeuropejskich (in Polish). Warszawa: Iskry.
- Komenda Główna Policji (2024) Statystyki zamachów samobójczych i wypadków drogowych. Warszawa: KGP Available from: https://statystyka.policja.pl/st/wybrane-statystyki/zamachy-samobojcze; https://statystyka.policja.pl/st/ruch-drogowy/76562,Wypadki-drogowe-raporty-roczne.html.
- Larsen, A.; Tele, A.; Kumar, M. Mental health service preferences of patients and providers: A scoping review of conjoint analysis and discrete choice experiments from global public health literature over the last 20 years (1999–2019). BMC Health Services Research 2021, 21, 589. [Google Scholar] [CrossRef]
- Lilienfeld, S.O.; Wood, J.M.; Garb, H.N. The scientific status of projective techniques. Psychological Science in the Public Interest 2000, 1, 27–66. [Google Scholar] [CrossRef] [PubMed]
- McGrath, R.E.; Twibell, A.; Carroll, E.J. (2023). The current status of “projective” tests. In H. Cooper, M.N. Coutanche, L.M. McMullen, A.T. Panter, D. Rindskopf, & K. J. Sher (Eds.), APA handbook of research methods in psychology: Foundations, planning, measures, and psychometrics (2nd ed., pp. 433–450). Washington, DC: American Psychological Association. [CrossRef]
- McWilliams, N. (2011). Psychoanalytic diagnosis: Understanding personality structure in the clinical process (2nd ed.). New York: Guilford Press.
- Moini, J.; Avgeropoulos, N.; Samsam, M. (2021). Epidemiology of brain and spinal tumors (1st ed.). Academic Press.
- Montag, C.; Davis, K.L. Affective neuroscience theory and personality: An update. Personal Neuroscience 2018, 1, e12. [Google Scholar] [CrossRef] [PubMed]
- Moore, F.R.; Doughty, H.; Neumann, T.; McClelland, H.; Allott, C.; O'Connor, R.C. Impulsivity, aggression, and suicidality relationship in adults: A systematic review and meta-analysis. EClinicalMedicine. 2022. [Google Scholar] [CrossRef]
- Murawiec, S. The primary-process emotional brain systems, according to Jaak Panksepp’s conceptualization, can serve as a component enabling the understanding of psychiatric pharmacotherapy. Psychiatria Spersonalizowana 2023, 2, 46–54. [Google Scholar] [CrossRef]
- Nobus, D. (2022). Lacan’s clinical artistry: On sublimation, sublation and the sublime. In Critique of Psychoanalytic Reason (1st ed., pp. 25–54). Routledge.
- Nowak, M.P.; Pawelczyk, T. Skale oceny ryzyka samobójstwa dorosłych w praktyce psychologa klinicznego i psychiatry: Przegląd dostępnych narzędzi. Psychiatria Psychologii Klinicznej 2018, 18, 180–187. [Google Scholar] [CrossRef]
- Orbach, I.; Mikulincer, M.; Gilboa-Schechtman, E.; Sirota, P. Mental pain and its relationship to suicidality and life meaning. Suicide and Life-Threatening Behavior 2003, 33, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Orsolini, L.; Latini, R.; Pompili, M.; Serafini, G.; Volpe, U.; Vellante, F.; Fornaro, M.; Valchera, A.; Tomasetti, C.; Fraticelli, S.; Alessandrini, M.; La Rovere, R.; Trotta, S.; Martinotti, G.; Di Giannantonio, M.; De Berardis, D. Understanding the complex of suicide in depression: From research to clinics. Psychiatry Investigation 2020, 17, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Pestian, J.P.; Grupp-Phelan, J.; Bretonnel Cohen, K.; Meyers, G.; Richey, L.A.; Matykiewicz, P.; Sorter, M.T. A controlled trial using natural language processing to examine the language of suicidal adolescents in the emergency department. Suicide & Life-Threatening Behavior 2016, 46, 154–159. [Google Scholar] [CrossRef]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; Mann, J.J. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. The American journal of psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef]
- Posner, K.; Subramany, R.; Amira, L.; Mann, J.J. (2014). From uniform definitions to prediction of risk: The Columbia Suicide Severity Rating Scale approach to suicide risk assessment. In K. Cannon & T. Hudzik (Eds.), Suicide: Phenomenology and Neurobiology (pp. 59–84). Springer, Cham. [CrossRef]
- Rozek, D.C.; Andres, W.C.; Smith, N.B.; Leifker, F.R.; Arne, K.; Jennings, G.; Dartnell, N.; Bryan, C.J.; Rudd, M.D. Using machine learning to predict suicide attempts in military personnel. Psychiatry Research 2020, 294, 113515. [Google Scholar] [CrossRef] [PubMed]
- Saint-Cyr, V.M. Creating a void or sublimation in Lacan. Recherches en psychanalyse 2012, 13, 15–21. [Google Scholar] [CrossRef]
- Santillo, G.; Morra, R.C.; Esposito, D.; Romani, M. Projective in time: A systematic review on the use of construction projective techniques in the digital era—beyond inkblots. Children 2025, 12, 406. [Google Scholar] [CrossRef]
- Sareen, J.; Cox, B.J.; Afifi, T.O.; et, al. Anxiety disorders and risk for suicidal ideation and suicide attempts: A population-based longitudinal study of adults. Archives of General Psychiatry 2005, 62, 1249–1257. [Google Scholar] [CrossRef]
- Shean, M.; Mander, D. (2020). Building emotional safety for students in school environments: Challenges and opportunities. In R. Midford, G. Nutton, B. Hyndman, & S. Silburn (Eds.), Health and education interdependence. Springer. [CrossRef]
- Shneidman, E.S. (1993). The suicidal process. In M. Golden (Ed.), The suicidal crisis. New York: Free Press.
- Snir, S.; Gavron, T.; Maor, Y.; Haim, N.; Sharabany, R. Friends' closeness and intimacy from adolescence to adulthood: Art captures implicit relational representations in joint drawing: A longitudinal study. Frontiers in Psychology 2020, 11, 2842. [Google Scholar] [CrossRef]
- Stanford Institute for Human-Centered Artificial Intelligence. (2023). AI key terms glossary & definition [Internet]. Stanford University. Available from: https://hai.stanford.edu/sites/default/files/2023-03/AI-Key-Terms-Glossary-Definition.pdf.
- Stanley, B.; Brown, G.K.; Brenner, L.A.; Galfalvy, H.C.; Currier, G.W.; Knox, K.L.; Chaudhury, S.R.; Bush, A.L.; Green, K.L. Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department. JAMA psychiatry 2018, 75, 894–900. [Google Scholar] [CrossRef]
- Stemplewska-Żakowicz, K.; Paluchowski, W.J. The reliability of projective techniques as tools of psychological assessment. Part 1: Why it is unjustified to describe some of them as projective? Problems of Forensic Sciences 2013, 93, 421–437. [Google Scholar]
- Szyjewski, A. (2003). Religia Słowian [Religion of the Slavs] (in Polish). Kraków: Wydawnictwo WAM.
- Thieberger, J. The concept of reparation in Melanie Klein's writing. Melanie Klein & Object Relations 1991, 9, 56–71. [Google Scholar]
- Uvnäs-Moberg, K.; Gross, M.M.; Calleja-Agius, J.; Turner, J.D. The yin and yang of the oxytocin and stress systems: Opposites, yet interdependent and intertwined determinants of lifelong health trajectories. Frontiers in Endocrinology (Lausanne) 2024, 15, 1272270. [Google Scholar] [CrossRef] [PubMed]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E. Jr. The interpersonal theory of suicide. Psychological Review 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed]
- Werbart, A.; Bergstedt, A.; Levander, S. Love, work, and striving for the self in balance: Anaclitic and introjective patients' experiences of change in psychoanalysis. Frontiers in Psychology 2020, 11, 144. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. (2024). Suicide prevention. Geneva: WHO Available from: https://www.who.int/health-topics/suicide.
- Yan, N.; Luo, Y.; Mackay, L.E.; et al. Global patterns and trends of suicide mortality and years of life lost among adolescents and young adults from 1990 to 2021: A systematic analysis for the Global Burden of Disease Study 2021. Epidemiology and Psychiatric Sciences 2024, 33, e52. [Google Scholar] [CrossRef]
- Żechowski, C. Theory of drives and emotions - from Sigmund Freud to Jaak Panksepp. Psychiatria Polska 2017, 51, 1181–1189. [Google Scholar] [CrossRef]
Figure 1.
Flow Diagram of Sankey depicting relationships between independent variables and destructive drive and destruction sublimation in a multivariate model.
Figure 1.
Flow Diagram of Sankey depicting relationships between independent variables and destructive drive and destruction sublimation in a multivariate model.
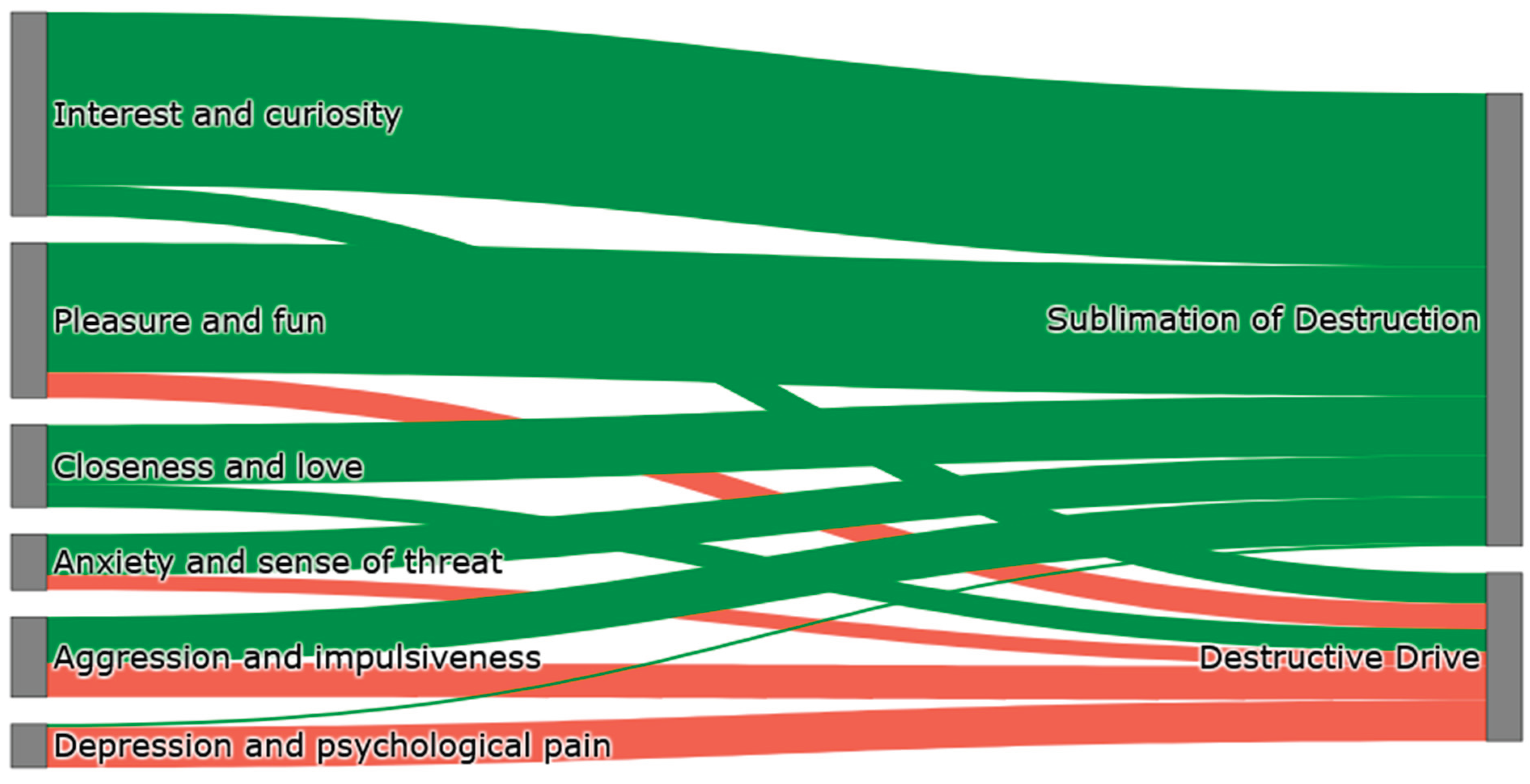
Table 1.
Characteristics of the study group.
| Variable | Category | N | % |
|---|---|---|---|
| Sex | Woman Man |
156 48 |
23,52 76,47 |
| Age | 18-66 | ||
| Marital status | Free Marriage Divorce Widowhood |
136 55 11 2 |
66,66 26,96 5,39 0,98 |
| Number of children | 0 1 2 3 More |
157 16 23 7 1 |
76,96 7,84 11,27 3,43 0,49 |
| Education | Basic Grammar school Essential professional Average Higher |
1 1 3 76 123 |
0,49 0,49 1,47 37,25 60,29 |
| Domicile | Village A city below 100 thousand City 100-500 thousand City over 500 thousand |
34 33 18 119 |
16,66 16,17 8,82 58,33 |
| Professional activity | Education Professional career Unemployment |
80 116 8 |
39,21 56,86 3,92 |
| Psychiatric treatment currently or in the past | No Yes |
82 122 |
40,19 59,80 |
| Psychotherapy now or in the past | No Yes |
74 130 |
36,27 63,72 |
| Psychiatric diagnosis | No How: Psychotic disorders F20-F29 Affective Disorder F30-F39 Anxiety Disorders F40-F49 Personality Disorders F60-F69 |
83 121 3 98 16 4 |
40,68 59,32 1,47 48,03 7,84 1,96 |
| The impact of the diagnosis on current well-being | Not applicable No Yes |
74 30 100 |
36,27 14,70 49,01 |
Table 2.
Internal consistency (Cronbach's Alpha) and item count for subscales.
| Podskala | Number of items | Alf Cronbach |
|---|---|---|
| (1) depression and mental pain | 18 | 0,9346 |
| (2) Interests and Curiosity | 15 | 0,9569 |
| (3) aggression and impulsivity | 14 | 0,9409 |
| (4a) Destructive Strivings | 8 | 0,8900 |
| (4b) sublimation of destruction | 11 | 0,8774 |
| (5) Enjoyment and Fun | 14 | 0,9397 |
| (6) closeness and love | 7 | 0,8770 |
| (7) anxiety and a sense of danger | 9 | 0,8985 |
Table 4.
Comparison of univariate and multivariate models for the pursuit of destruction and sublimation of destruction.
Table 4.
Comparison of univariate and multivariate models for the pursuit of destruction and sublimation of destruction.
| Striving for Destruction | ||||
| Factor | Single-variate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size | Multivariate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size |
| Depression and mental pain | B=0.326, SE=0.047, Wald χ²=47.569, p=0.000, OR=1.385, CI=[1.262–1.520] | Big impact | B=0.288, SE=0.050, Forest χ²=32.770, p=0.000, OR=1.333, CI=[1.208–1.472] | Big impact |
| Interest and curiosity | B=-0.048, SE=0.047, Forest χ²=1.022, p=0.312, OR=0.953, CI=[0.869–1.046] | Lack | B=-0.291, SE=0.137, Wald χ²=4.473, p=0.034, OR=0.748, CI=[0.571–0.980] | Medium (protective) effect |
| Aggression and impulsivity | B=0.516, SE=0.106, Wald χ²=23.808, p=0.000, OR=1.676, CI=[1.361–2.063] | Big impact | B=0.250, SE=0.136, Wald χ²=3.360, p=0.067, OR=1.284, CI=[0.982–1.679] | Small effect |
| Sublimation of destruction | B=0.101, SE=0.066, forest χ²=2.350, p=0.125, OR=1.106, CI=[0.972–1.259] | Lack | B=0.132, SE=0.131, Wald χ²=1.015, p=0.314, OR=1.142, CI=[0.881–1.479] | Lack |
| Fun and enjoyment | B=0.136, SE=0.071, Wald χ²=3.672, p=0.055, OR=1.146, CI=[0.996–1.317] | Lack | B=0.191, SE=0.131, Wald χ²=2.138, p=0.144, OR=1.210, CI=[0.936–1.565] | Small effect |
| Closeness and love | B=-0.114, SE=0.099, Wald χ²=1.323, p=0.250, OR=0.892, CI=[0.734–1.084] | Low (protective) effect | B=-0.207, SE=0.144, Forest χ²=2.073, p=0.150, OR=0.813, CI=[0.612–1.079] | Low (protective) effect |
| Anxiety and a sense of threat | B=0.441, SE=0.104, Wald χ²=18.066, p=0.000, OR=1.554, CI=[1.267–1.906] | Big impact | B=0.114, SE=0.142, Wald χ²=0.648, p=0.421, OR=1.121, CI=[0.848–1.481] | No effect |
| Sublimation of destruction | ||||
| Factor | Single-variate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size | Multivariate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size |
| Depression and mental pain | B=0.069, SE=0.032, Forest χ²=4.739, p=0.029, OR=1.071, CI=[1.007–1.140] | Lack | B=0.026, SE=0.067, forest χ²=0.143, p=0.705, OR=1.026, CI=[0.898–1.171] | Lack |
| Interest and curiosity | B=1.148, SE=0.132, Wald χ²=75.974, p=0.000, OR=3.152, CI=[2.432–4.085] | Big impact | B=0.888, SE=0.154, Wald χ²=33.242, p=0.000, OR=2.431, CI=[1.795–3.291] | Big impact |
| Aggression and impulsivity | B=0.299, SE=0.080, Wald χ²=13.865, p=0.000, OR=1.348, CI=[1.151–1.579] | Medium effect | B=0.322, SE=0.157, Wald χ²=4.195, p=0.041, OR=1.380, CI=[1.013–1.882] | Medium effect |
| Striving for destruction | B=0.118, SE=0.068, Forest χ²=3.061, p=0.080, OR=1.126, CI=[0.985–1.286] | Lack | B=-0.214, SE=0.164, Forest χ²=1.710, p=0.191, OR=0.807, CI=[0.585–1.114] | Small effect |
| Fun and enjoyment | B=1.125, SE=0.157, Wald χ²=51.543, p=0.000, OR=3.081, CI=[2.263–4.195] | Big impact | B=0.728, SE=0.199, Forest χ²=13.411, p=0.000, OR=2.072, CI=[1.401–3.064] | Big impact |
| Closeness and love | B=1.233, SE=0.166, Wald χ²=55.317, p=0.000, OR=3.432, CI=[2.476–4.755] | Big impact | B=0.402, SE=0.191, Wald χ²=4.414, p=0.036, OR=1.494, CI=[1.026–2.177] | Medium effect |
| Anxiety and a sense of threat | B=0.360, SE=0.094, Wald χ²=14.655, p=0.000, OR=1.433, CI=[1.191–1.725] | Medium effect | B=0.293, SE=0.203, Forest χ²=2.081, p=0.149, OR=1.340, CI=[0.899–1.998] | Small effect |
* Statistically significant effect.
Table 5.
Analysis of univariate and multivariate logistic regression for dependent variables: striving for destruction and sublimation of destruction in relation to independent variables: age and number of children.
Table 5.
Analysis of univariate and multivariate logistic regression for dependent variables: striving for destruction and sublimation of destruction in relation to independent variables: age and number of children.
| Striving for destruction | ||||
| Variable | Single-variate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size | Multivariate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size |
| Age | B=-0.042, SE=0.012, Forest χ²=11.860, p=0.000, OR=0.959, CI=[0.937–0.982] | Poor | B=-0.054, SE=0.015, Forest χ²=13.680, p=0.000, OR=0.947, CI=[0.921–0.975] | Poor |
| Number of children | B=0.007, SE=0.100, Forest χ²=0.005, p=0.943, OR=1.007, CI=[0.827–1.227] | Lack | B=0.244, SE=0.152, Forest χ²=2.581, p=0.108, OR=1.277, CI=[0.947–1.722] | Lack |
| Sublimation of destruction | ||||
| Variable | Single-variate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size | Multivariate model (B, SE, Wald χ², p, OR, 95% CI) | Effect size |
| Age | B=0.011, SE=0.010, Forest χ²=1.101, p=0.294, OR=1.011, CI=[0.990–1.032] | Lack | B=0.007, SE=0.012, Forest χ²=0.375, p=0.540, OR=1.007, CI=[0.984–1.030] | Lack |
| Number of children | B=0.119, SE=0.104, Wald χ²=1.322, p=0.251, OR=1.127, CI=[0.918–1.383] | Lack | B=0.090, SE=0.112, Forest χ²=0.643, p=0.423, OR=1.094, CI=[0.878–1.363] | Lack |
Table 6.
Summary of ROC analysis results for individual subscales.
| Striving for destruction | |||||||||||
| Variables | AUC | SE | Cl 95% | Cut-off point | Sensitivity | Specificity | Accuracy | Positive predictive value | Negative predictive value | Youden Index | |
| Depression and mental pain | 0,783* | 0,036 | [0,712; 0,855] | 3 | 0,750 | 0,647 | 0,672 | 0,396 | 0,894 | 0,397 | |
| Aggression and impulsivity | 0,715* | 0,44 | [0,629; 0,802] | 1 | 0,688 | 0,724 | 0,716 | 0,434 | 0,883 | 0,41 | |
| Anxiety and a sense of threat | 0,618** | 0,051 | [0,519; 0,717] | 2 | 0,396 | 0,904 | 0,784 | 0,559 | 0,829 | 0,30 | |
| Sublimation of destruction | |||||||||||
| Variables | AUC | HERSELF | Cl 95% | Cut-off point | Sensitivity | Specificity | Accuracy | Positive predictive value | Negative predictive value | Youden Index | |
| Interest and curiosity | 0,900* | 0,026 | [0,848; 0,951] | 2 | 0,837 | 0,871 | 0,863 | 0,672 | 0,944 | 0,71 | |
| Fun and enjoyment | 0,793* | 0,041 | [0,713; 0,873] | 1 | 0,755 | 0,761 | 0,760 | 0,500 | 0,908 | 0,52 | |
| Closeness and love | 0,836* | 0,035 | [0,767; 0,905] | 1 | 0,837 | 0,800 | 0,809 | 0,569 | 0,939 | 0,64 | |
* p<0.00001; ** p<0.02.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



