Submitted:
12 May 2025
Posted:
13 May 2025
You are already at the latest version
Abstract
Background/Objectives: Physical activity (PA) during pregnancy presents health benefits for mother and child. The World Health Organization recommends at least 150 minutes of moderate-intensity physical activity per week for a healthy pregnancy. The objectives of the study were to describe physical and sedentary activity patterns, estimate the proportion of women meeting PA recommendations and identify associated sociodemographic and obstetric characteristics in a southern European sample of pregnant women. Methods: For this cross-sectional study, a random sample of 385 pregnant women attending their 20th-week scheduled ultrasound at their referral hospital was selected. Inclusion criteria were being between 18 and 22 gestational weeks pregnant and communicating in Spanish. A face-to-face structured interview was used to collect demographic, obstetric and PA data, as well as sedentary patterns. Indexes of weekly PA in various domains were computed. Bivariate analyses were conducted to assess the variability of physical and sedentary activities according to sociodemographic and obstetric variables. Results: 84.4% of participants engaged in some type of PA and 73.7% met PA requirements. Higher leisure PA was associated with higher education and first-time pregnancy. Higher work PA was linked to lower education, being born outside Spain and later pregnancy awareness. Higher sedentary daily time was associated with higher education, speaking Spanish as a child and first-time pregnancy. Conclusions: Most pregnant women in this study met PA recommendations. Correlates of leisure PA differ from those regarding work PA.
Keywords:
physical activity
; sedentary behaviour
; pregnancy
; patterns
; correlates
; guidelines
; Spain
1. Introduction
Engaging in physical activity (PA) during pregnancy is beneficial for the health of mother and offspring [1]. Health advantages for the mother include less risk of developing obesity, cardiovascular diseases, hypertensive disorders and gestational diabetes mellitus [2-7]. Maternal PA also decreases musculoskeletal discomfort [8], prevents excessive gestational weight gain and postpartum weight retention [6,9], and is associated with lower levels of systemic inflammation [10]. As regards mental health, PA during pregnancy improves psychological well-being by reducing anxiety, stress and prenatal depression [11-14] and lowers the risk of postpartum depression [15].
Regarding advantages for the baby, PA during pregnancy does not have negative effects on fetoplacental development and is not associated with neonatal complications [16]. On the contrary, it is linked to advanced neurobehavioral maturation, healthier foetal growth, improved stress tolerance in the baby [2,8] and lowered neonatal adiposity [17]. It also has a positive long-term impact on the body composition and health outcomes of the child [5,16,17]. Engaging in PA during pregnancy positively influences lung development in the foetus, lung functioning in the newborn, and lowers the risk of developing asthma [18].
Besides the health benefits for mother and child, maternal PA lowers the risk of complications at delivery, such as preterm births for women without pregnancy complications [19], c-section births and vulvo-vaginal tears [5,13,20]. Moreover, PA and exercise during pregnancy are also associated with less frequent premature rupture of membranes [21], reduce potential complications for women at risk of preterm delivery [22], and tend to reduce the length of delivery and postpartum recovery [8].
Given the benefits of engaging in PA during pregnancy, various organizations interested in the well-being of women during and after pregnancy as well as the health of the offspring have updated recommendations on this topic. The World Health Organization (WHO) recommends performing at least 150 minutes of moderate-intensity aerobic PA per week for a healthy pregnancy [1]. Similar guidelines have been provided around the world by the United States Department of Health and Human Services (US DHHS) [23], the American College of Obstetricians and Gynecologists (ACOG) [24], the Canadian Society for Exercise Physiology [25], the Royal Australian and New Zealand College of Obstetricians and Gynecologists (RANZCOG) [26], the International Olympic Committee (IOC) [27], the UK Department of Health and Social Care [28], Sports Medicine Australia [29], the Spanish Society of Gynecologists and Obstetricians [30,31] and the Andalusian Health Department [32]. Moreover, the recommendations of international public health guidelines on PA during gestation are similar across organisations [33].
Achieving a global perspective on PA patterns during pregnancy across world regions is not easy, due to the paucity of studies in low-income countries and to the diversity of methods used for measuring PA [34]. Nevertheless, there are indications of relevant differences in this regard among countries. For instance, a Canadian nationwide study concluded that adult pregnant women spent 9.5 hours per day (70% of their time) engaged in sedentary behaviour and 14.9 minutes of moderate-to-vigorous physical activity (MVPA) per day [35]. A study conducted in the United States on recreational PA with women in early pregnancy reported that 61% of women participated in regular PA [36]. In Spain, a study on moderate PA (MPA) among pregnant women concluded that its prevalence was 61% in the second trimester [37].
In terms of meeting the stipulated recommendations of PA during pregnancy, studies have also obtained mixed results. Various researchers have reported high compliance with recommendations for PA during pregnancy. For instance, a study conducted in the city of Donostia-San Sebastian, in the north of Spain [38], collected data on PA related to housework, walking, biking and sports during the first and second trimesters. It concluded that, overall, 80% of pregnant women met recommendations from international guidelines such as the US DHHS and WHO [23,24]. Similarly, a study on leisure time PA in women in early pregnancy in Serbia concluded that about 73% of pregnant women met WHO PA recommendations [39]. In a study carried out in Sweden, almost half of the sample (47.1%) performed the recommended level of PA [40]. In the United States, a study on Hispanic pregnant women and PA related to household chores, caregiving, transport and work found that about 45% of participants in early pregnancy met the recommended levels of PA based on ACOG guidelines [41].
However, low compliance with recommendations has also been observed. For example, a systematic review of PA among Chinese pregnant women estimated the average prevalence of meeting recommended levels of PA at 21% [42]. In a sample of pregnant women in Naples, Italy, only 37% reported performing at least 150 minutes of moderate intensity physical activity per week [43]. In Canada, only 27.5% of pregnant women met the PA levels recommended by the Canadian Physical Activity Guidelines [35]. Similarly, in South Africa, a cross-sectional study in Eastern Cape Province collected data on pregnant women and PA related to household chores, caregiving, occupation and leisure time and found that approximately 26% of pregnant women met the recommended levels of PA based on international guidelines [44]. In addition, a study in Brazil about pregnancy and PA related to domestic and caregiving work, labour and leisure time found very low compliance with international recommended levels of PA during the first (7.2%), second (7.6%) and third (4.7%) trimesters [45].
Furthermore, associations between maternal PA and demographic and obstetric characteristics have been observed. Researchers have found that, among pregnant women, higher education is associated with higher levels of leisure PA [36,39,44, 46-50] as well as meeting PA recommendations for pregnant women [46,50,51]. Nevertheless, the relationship between different domains of PA apart from leisure time PA and educational level among pregnant women has been scarcely studied.
Several studies have explored the relationship between gravidity and PA during pregnancy, with controversial findings. In some studies, multigravidity is associated with more frequent PA during pregnancy [38,41] whereas other studies have found an association between primigravidity and a higher level of PA among pregnant women [36,45,48].
Regarding sedentary behaviour during pregnancy, WHO warns that greater amounts of sedentary behaviour are linked to poor health outcomes, such as higher risk of cardiovascular diseases, cancer or type 2 diabetes. It recommends that pregnant women should limit the amount of time spent being sedentary and replace sedentary behaviour with more time of physical activity of any intensity [1]. Others have observed the following: excessive sitting time during the first and second trimesters of pregnancy can negatively affect placental weight [52]; moreover, sedentary behaviour is associated with an increased risk of preterm births, admissions to the neonatal intensive care unit [53], poor sleep quality [54] and prenatal and postnatal depression [55]. Longitudinal studies addressing sedentary behaviour during pregnancy have found that almost all pregnant women decreased PA levels and increased their sedentary behaviour [17,56]. Lynch et al. [41] highlighted those younger and more educated women decreased their sedentary behaviour compared to older and less educated women. Unfortunately, compared to PA, sedentary behavioural patterns during pregnancy have been scarcely studied [35,57,58].
Exploring the prevalence and understanding the correlates of PA and sedentary behavioural patterns in this population supports the planning and implementation of effective public health strategies, including suitable communication plans, to foster an active and healthy lifestyle during pregnancy.
Considering the current mixed results in the literature on physical and sedentary activity behaviours among pregnant women, the objectives of this study were threefold: 1) to describe physical and sedentary activity patterns of a southern European sample of pregnant women; 2) to estimate the proportion of pregnant women meeting recommended levels of PA according to WHO, and; 3) to assess sociodemographic and obstetric variability regarding physical and sedentary activities of pregnant women.
2. Materials and Methods
Setting and Study Design
A cross-sectional study was conducted with a representative sample of pregnant women in a health district. Participants were attending a scheduled ultrasound in their 20th week of gestation in the outpatient clinics of their referral public (university) hospital in a southern Spanish city (Huelva). After giving signed informed consent, they were interviewed in person by a trained health professional using an anonymous questionnaire.
Participants
A total of 829 women attended the hospital outpatient clinic during the days of data collection (May-August 2021). Due to language barriers (i.e., not being fluent in Spanish) and the lack of availability of interpreters for assisting interviews, 134 of them were not invited to participate in the study. Another 174 women were not invited because the researcher was occupied at the time interviewing another pregnant woman. There was no other reason why these pregnant women were not invited to participate in the study, other than the fortuitous fact that the researcher was interviewing another woman. In this regard, the sample was randomly selected. Finally, a total of 521 women were invited to participate in the study.
Inclusion criteria were being between 18 and 22 gestational weeks pregnant, attending a scheduled scan in the 20th week of gestation at an outpatient clinic of the referral hospital and being able to communicate in Spanish. No criteria for age were established. In pregnant women under 18 years old, informed consent was also provided by the mother, who was present in the interview.
Instrument and Variables for Data Collection
Participants were face-to-face interviewed using an anonymous questionnaire to collect data on demographics, obstetrics, physical activity and sedentary behaviour during pregnancy.
Demographic and obstetric data related to pregnancy were collected using a series of multiple-choice questions included in a questionnaire developed by the research team in a previous study [59,60]. Some questions required verbatim answers, which were categorized after the interview by the research team.
Sociodemographic data included age; educational level, grouped into four categories: no studies, primary education, secondary studies and higher education; currently studying (yes/no); employment status, grouped into four categories: full time, part time, unemployed, or other; population size of the place of residence; relationship status; language spoken at home currently and during childhood; and country of birth.
Obstetric variables included gravidity (including previous miscarriages, abortions and the current pregnancy), number of vaginal and caesarean births (excluding abortions), number of miscarriages, number of abortions, health problems during pregnancies ended in live birth, age at first pregnancy, high-risk pregnancy consultation, pregnancy planning, assisted reproduction pregnancy, trimester of pregnancy awareness (first/second), professional health care during pregnancy, date of initiation of professional control of current pregnancy, date of last menstrual period, and self-reported height and weight to determine body mass index (BMI).
Physical activity was assessed using the Global Physical Activity Questionnaire, Version 2 (GPAQv2) [61]. The GPAQ was tested in nine countries between 2002 and 2005 to collect physical activity information relevant to both developed and developing countries. Its validity and reliability have been demonstrated to be appropriate to measure PA in adult populations [62]. A subsequent study provided low-to-moderate validity and acceptable reliability evidence for the GPAQ [63].
The GPAQ consists of 16 questions regarding physical activity at work, travel to and from places, recreational activities, and sedentary behaviour. To collect physical activity information in these domains, participants are asked about the frequency (i.e., number of days) of the following activities in a typical week and their duration (i.e., amount of time in hours and minutes) on a typical day: 1) vigorous work PA, 2) moderate work PA, 3) active travel to and from places, 4) vigorous recreational PA, 5) moderate recreational PA, and 6) sitting/resting time. The protocol for collecting data using the GPAQ states that PA must be performed for at least 10 minutes continuously to be recorded. In the GPAQ questionnaire, “activity at work” refers to a wide range of possibilities (e.g., paid or unpaid work, study/training, household chores, harvesting food/crops, fishing or hunting for food, seeking employment). Sedentary behaviour was assessed by a single question, namely “How much time do you usually spend sitting or reclining on a typical day?”.
Furthermore, following recommendations of the GPAQ protocol, visual aids were used during the interviews in the form of cards that represented a wide range of vigorous and moderate activities related to the workplace, and recreational and sports activities. These visual aids had been adapted and piloted prior to the beginning of the study to represent activities performed by women in the local context where the study was to be conducted.
Data Collection and Study Procedures
Women were recruited in the waiting room during their 20th-week scheduled ultrasound visit. Any woman waiting for her appointment was invited to participate in the study, except when the interviewer was occupied collecting data from another person. Pregnant women were approached by a trained health professional, received information on the study and were asked for their voluntary participation. If a woman refused, the next woman was invited to participate. Those who agreed were invited to a private space in the outpatient clinic to sign the informed consent form and be interviewed face-to-face using the anonymous questionnaire. Underage participants were asked for parental consent as well. Data collection took place in April-July 2021.
Data Analysis
Physical activity data were cleaned and analysed following the steps from the GPAQ analysis guide [64]. Overall, the number of missing values was less than 1% across all questions.
First, a univariate analysis was performed for each variable. Next, a series of variables were generated to calculate the Metabolic Equivalent of Task (MET) minutes. These new variables also underwent a univariate analysis. For these calculations, frequency and duration of moderate work-related PA, vigorous work-related PA, active travel to and from places, leisure time moderate PA and leisure time vigorous PA were converted to minutes and added up for each participant to calculate the total minutes per week of each activity domain. Next, totals for moderate PA (work, travel to and from places, and leisure) and totals for vigorous PA (work and leisure) were calculated and converted to MET-minutes to obtain the total PA MET minutes per week.
The GPAQ analysis instructions were followed to transform energy expenditure into METs. When calculating a participant’s overall energy expenditure related to physical activity, 4 METs were assigned to the time spent in moderate activities and 8 METs were assigned to the time spent in vigorous activities [58,59]. Therefore, to convert physical activity time to MET minutes by week, the total time spent performing moderate activities in a typical week was multiplied by 4, and the total time spent in vigorous activities was multiplied by 8. Sedentary behaviour was only measured in minutes on a typical day.
Finally, bivariate analyses to test the relationship between physical activity and sociodemographic and obstetric variables were performed applying the Chi-squared test of independence and the Mann-Whitney and Kruskal-Wallis tests with non-parametric data. Statistical significance was set at P-value <0.05. Data analysis was concluded using the Software Package for Social Sciences (SPSS version 29).
Ethics
The Research Ethics Committee of the Andalusian Health and Families Department reviewed and approved the study protocol. Verbal and written information about the study was given to participants and informed consent forms were signed by all participants before data collection started. All data were anonymous. The 1975 Helsinki declaration and its subsequent amendments were respected.
3. Results
Sociodemographic and Obstetric Characteristics
Of the 521 women who were invited to participate in the study, 117 refused. A total of 404 pregnant women provided signed consent and were subsequently interviewed. The response rate was 77.5%. The mean age of women unwilling to participate (30.0 years) was very similar to that of the final sample (31.8). Yet, as regards educational level, the percentage of women with higher education among those who refused participation (17.9%) was lower than in the sample (30.9%).
After data collection, 19 women were excluded from the analysis because they did not meet the gestational age criterion. A total of 385 women, aged 14 to 48 years with a mean age of 31.8 (SD = 5.99) were included in the final sample. Only 4 women were under 18 years. Approximately 40% of women were over the age of 35. About 46% of the sample had primary education, while 30.9% had higher education. Less than half of the participants worked full time (41%). In addition, two thirds of the sample (67%) lived in towns with a population greater than 20,000 and around 92% of pregnant women had been born in Spain. Almost all women (99.2%) reported being in a current relationship at the time of the interview. Based on the Body Mass Index, nearly half of the sample (48%) was considered within normal weight, about 30% was classified as overweight and 21% lived with obesity (Table 1).
The average number of pregnancies of participants was 2.1 (SD = 1.1) with a mean age of 27.5 years (SD = 6.4) for the first pregnancy. Almost two thirds of women (63.1%) had been pregnant before, and 16.1% of women reported having had problems during previous pregnancies that ended in live birth. Moreover, more than three quarters of women (76.6%) had planned the current pregnancy, 12.7% had used assisted reproduction for their current pregnancies, and 15.6% were receiving high-risk care (Table 2).
Physical and Sedentary Activity Patterns
The mean of total PA (work, travel to and from places, and leisure) was 902.9 min/week (SD = 1,061.3). The mean was 596.3 min/week (SD = 1,037.5) for work-related PA, 97.6 min/week (SD = 211.3) for active travel to and from places, and 212.1 min/week (SD = 262.3) for leisure time PA. On average, women spent 700.3 (SD = 858.6) min/week performing moderate-intensity PA (work, travel to and from places, and leisure) and 202.6 (SD = 681.8) min/week performing vigorous-intensity PA (work and leisure). Finally, the average time spent on sedentary behaviour on a typical day was 234.6 minutes (SD=162.99) (Table 3).
Approximately 84.4% of the pregnant women in this study reported engaging in some type of PA. The proportion of women who reported engaging in PA was 33.5% as part of their work and 36.2% for travel to and from places; however, close to twice as many women (61.7%) engaged in recreational PA. Additionally, only 10.9% of women engaged in vigorous PA (work and leisure) while 81.3% engaged in moderate PA (work, travel to and from places, and leisure) (Table 3).
Proportion of Pregnant Women Meeting the WHO Recommendation
Variability of Compliance with WHO Physical Activity Recommendations for Health According to Sociodemographic and Obstetric Variables
Results yielded significant variability in meeting the WHO recommendation according to one sociodemographic variable: currently studying, and one obstetric variable: gravidity. Compliance with PA recommendations was greater among women who were currently studying (86%), compared to those who were not (71.6%), χ2(1, N=283) = 5.2, p = 0.02, V = 0.12. About 80% of first-time pregnant women reported greater compliance with PA recommendations for health compared to around 70% of multigravida women, χ2(1, N = 283) = 5.04, p = .02, V = 0.11. (Table 4).
Variability of Physical Activity by Domain, MET Minutes/Week and Sedentary Behaviour According to Sociodemographic Variables
A relevant variability in two of the three domains of PA regarding sociodemographic variables was found. First, minutes of leisure time PA varied significantly according to level of education and whether women were currently studying. Leisure time PA and educational level were positively correlated. On average, women with higher levels of education spent more minutes of recreational PA per week compared to those with lower education (Table 5 and Figure 1). Moreover, women who were currently studying engaged in more time of leisure PA per week. Pregnant women who were studying spent an average of 292.5 min/week in leisure PA (SD = 375.), while the mean time for women who were not studying was 198.1 min/week (SD = 235.3) (p<0.05) (Table 5).
Work-related PA also showed variability according to educational level and whether women were currently studying. Women with lower levels of education reported performing more PA as part of their work than women with higher education. Specifically, women with primary education had the highest mean for work-related PA minutes per week (M = 916.4, SD = 1,233.3) (Figure 2 and Table 5). As regards the “currently studying” variable, work-related PA also showed relevant variability. Women who were not currently studying tended to engage in more than twice the amount of weekly time of work-related PA (M = 658.1, SD = 1,085.1) compared to women who were studying (M = 244.2, SD = 602.1; p<0.01). In addition, work-related PA was also significantly related to country of birth. Women who were born in Spain engaged in lower amounts of work-related PA minutes per week (M = 568.8, SD = 1,027.8) compared to women born elsewhere (M = 897.2, SD = 1,110.96; p<0.05) (Figure 3 and Table 5). No significant variability was found between travel to and from places PA and any sociodemographic characteristics (Table 5).
When PA patterns were measured in terms of MET-min/week, a relevant variability was found regarding two sociodemographic variables: educational level and population of the place of residence. Among the four educational level groups, women with lower levels of education performed approximately twice as many MET-min/week than women with higher levels of education. In fact, women with primary education had the highest average MET-min/week (M = 6,294.8, SD = 7,813.6) (Table 5 and Figure 4). As regards the size of the place of residence, the smaller the town, the greater the MET-min/week. Specifically, women who lived in a town with a population greater than 50,000 people spent an average of 3,655.8 MET-min/week (SD = 6,004.3) compared to 5,446.7 MET-min/week (SD = 8,075.1) in those who lived in a town with a population under 5,000 (p<0.05) (Table 5).
Daily time of sedentary behaviour exhibited significant variability in relation to educational level and language spoken at home as a child. Educational level and time spent in sedentary behaviour were positively correlated. Specifically, women with no studies spent an average of 105 min/day in sedentary behaviour (SD = 52.), whereas women with higher education engaged in an average of 281 min/day of sedentary time (SD = 192.1; p<0.01) (Figure 5). As regards language spoken at home as a child, women who spoke Spanish while growing up reported a higher average of daily sedentary time (M = 239.3, SD = 165.) compared to women who spoke another language (M = 189.6, SD = 136.3) (p<0.05) (Table 5).
Physical Activity by Domain, MET-Minutes, and Sedentary Behaviour Variability in Relation to Obstetric Variables
Regarding the relationship between the three physical activity domains and the obstetric variables, results showed significant variability in two domains: leisure time PA according to gravidity, and work-related PA based on trimester of pregnancy awareness. On average, primigravida women spent more min/week (254.3; SD = 242.7) performing leisure time PA than women with previous pregnancies (M =187.3, SD=270.6) (p<0.01) (Table 6). By contrast, a great difference was detected in average time of work PA according to trimester of pregnancy awareness. Women became aware of their pregnancy during the second trimester reported about four times more work-related PA (M =2,124, SD = 741.4) than those who found out during the first trimester (M = 569.9, SD = 1,020.8) (p<0.01) (Table 6).
Regarding MET-min/week, there was no significant variability with obstetric variables except for one: trimester of pregnancy awareness. The earlier women found out about their pregnancy, the fewer MET-min/week they performed. The average METs for women who learned about their pregnancy during the first trimester was 4,273.6 (SD=6,154.5). In women who learnt the news of their pregnancy during the second trimester, the average was 13,836 MET-min/week (SD=6,577.5) (p<0.01) (Table 6).
Finally, a relevant variability in time of sedentary behaviour per day was observed according to gravidity. First-time pregnant women spent more time involved in sedentary behaviours than women who had had more than one pregnancy. Specifically, primigravida women engaged in approximately 252 min/day of sedentary behaviour (SD=160.4) compared to women who had been pregnant before, who spent about 225 min/day being sedentary (SD=163.99) (p<0.05) (Table 6).
4. Discussion
The aim of this study was to describe the physical activity and sedentary activity patterns of pregnant women in a health district in southern Europe, as well as the variability of these behaviour patterns according to sociodemographic and obstetric variables. The research also aimed to estimate the degree of compliance with the WHO recommendation on physical activity during pregnancy.
The physical activity of the pregnant women was assessed in three different domains: work, travel to and from places and leisure time physical activity. If we consider the results globally in terms of the number of minutes per week spent on average in each of these three domains, work PA occupied the most time among the pregnant women in the sample (almost 600 minutes per week on average, out of a total of approximately 900 minutes of PA per week). In this respect, it should not be forgotten that in the GPAQ questionnaire, work is understood in a broad sense, including domestic activities, job search and study, beyond strictly work activities in the usual sense of the term. Moreover, the average weekly PA time spent traveling to and from places was close to 100 minutes (97.6), while the average weekly PA time spent on leisure activities was around 200 minutes (212.1). Logically, the distribution of the average weekly PA time among these three domains, in addition to personal circumstances, was strongly marked by the social and geographical characteristics of this area of southern Europe and may be very different from that found among pregnant women in other parts of the world. For example, in a study of pregnant women in Nepal, leisure time physical activity was reported to be non-existent (only one woman reported doing it) and practically all the PA performed by pregnant women was distributed between work or domestic chores and traveling to and from places [65].
The distribution by PA domains of participants in terms of prevalence yielded a different perspective to results presented in terms of average weekly minutes dedicated to each area of PA. Specifically, a higher percentage of women in the sample reported performing leisure PA (61.7%), while only a third (33.5%) reported performing PA at work or at home and just over a third reported active travel (36.2%).
In this study, time spent weekly on leisure PA appeared to be closely associated with the level of education (the higher the level of education, the greater the time spent). This agrees with the findings of studies in various countries [36,39,40,45, 47-49, 66,67]. Multiple factors may explain this association between educational level and more frequent leisure PA. For example, a higher level of education facilitates access to health information that supports the desirability of maintaining an active lifestyle at any stage of the life cycle. It is also associated with higher income, which makes it easier to live in areas with greater accessibility to parks, gyms or other facilities for PA, and safer areas. It may also facilitate the payment of fees for facilities or programmes, when they are not free [45,48,50,66].
In contrast with the previous finding, weekly time of physical activity at work tended to be inversely related to educational level. In this study, the average weekly minutes of work PA were particularly high among women with only primary education, much higher than among those with higher levels of education. Moreover, PA at work was found to be relatively high among those born outside Spain, among those who spoke a language other than Spanish at home as a child, among the unemployed and among those living in small towns. It is important to note that, in the province of Huelva, in south-western Spain, there are many immigrant women working in the agricultural sector. In addition, as in other geographical areas of the world, women with a lower level of education may be forced to take on more physically demanding work. Yet, regarding unemployed women, the GPAQ questionnaire considers work to include both domestic chores and job search.
Finally, with regard to active travel, no relevant sociodemographic variability was detected in this study. In southern European areas such as that studied, walking or cycling is not necessarily a recreational activity. It can also be a way of going to work, shopping, accompanying children to school, travelling to be with family or friends or accessing health services for pregnant women. It is therefore understandable that no significant social variability in active travel was found, as women from very different social backgrounds may share the habit or need to walk or cycle. In contrast, a study in Ontario, Canada, found that pregnant women with lower educational levels were more likely to walk when travelling [46].
When PA was estimated in terms of energy expenditure equivalent (MET min/week), sociodemographic variability was detected in only two aspects: educational level and size of place of residence. Pregnant women with lower educational levels reported much higher MET min/week (approximately twice as high) than those with higher educational levels, which could be related to a greater involvement in physical work or domestic activities or to a lower use of private cars as a means of transport, among other factors. With regard to the size of the place of residence, a higher energy expenditure in physical activity was detected among pregnant women living in small towns. In the geographical area studied, it is precisely in small towns where it is more common for women to work in agriculture or for women to live and travel to larger towns to work as domestic servants. It is also relatively easy to walk to the shops or to the health centre, to go on walks in rural trails, or to use the municipal public sports facilities in these smaller towns. All these activities, among others, may involve higher energy expenditure than is typical among pregnant women living in large cities. However, as the relationship between physical activity in pregnant women and size of place of residence has been scarcely studied, future studies should address this to better understand this relationship.
As regards differences in the practice of PA in the three domains explored considering obstetric variables, they were only detected in the number of pregnancies of participants and the trimester of pregnancy awareness. In this study, primigravidae reported spending more time per week performing leisure PA than those who had had previous pregnancies. This is consistent with other studies, where pregnant women in their first pregnancy or without children have reported higher levels of physical exercise or leisure physical activity than those with children [36,45,48, 68-70]. In contrast, in a study conducted in the city of Donostia-San Sebastián, in northern Spain, pregnant women with living children spent more weekly time doing light or moderate PA, measured objectively and with self-reported instruments [38]. Similarly, a study of Hispanic women in the United States found that having children was associated with a higher level of PA, including housework and caregiving.
Both types of results (i.e., higher frequency of PA in primigravidae and higher frequency of PA in multigravidae or multiparous women) could be reasonably explained, although with different arguments. On the one hand, in a social context where social support for parenting is scarce, it seems logical that women who are pregnant for the first time have more free time for recreational PA than those who already have children. On the other hand, if they already have children, this may imply, in addition to more housework, having to leave the house frequently to accompany them (e.g., to school or the park). Yet, in certain social groups, having children may denote a higher level of income than that of childless women, which in turn facilitates having free time or being able to pay fees of gyms and the like. Of course, this depends on the geographical area, the type of urban planning in the cities, the social policies of the country and the socioeconomic characteristics of the population. Hence, the results of studies in different social contexts may be divergent.
As regards the trimester of pregnancy awareness, very marked differences were detected between women who became aware in the first trimester and those who did in the second trimester. Those who became aware in the second trimester (only 5 cases, 1.3% of the sample) had significantly higher levels of work-related PA as well as energy expenditure (MET-min/week). To correctly interpret this results, it would be necessary to further explore the specific characteristics of these five individuals, according to the anonymous data collected in the questionnaire. However, this was beyond the scope of this study as it was a marginal percentage of pregnant women in the sample.
Regarding compliance with the WHO recommendation to practice at least 150 minutes a week of moderate PA, the prevalence detected in this study (73.7%) was somewhat lower than that estimated among pregnant women in the city of Donostia-San Sebastián, (85%) [38]. Yet, it was higher than that estimated in the city of Malaga (50.8%) [13], which, like the area studied in this study (the province of Huelva), is in southern Spain. Several studies have found even lower prevalences of compliance with this recommendation among pregnant women. Some examples are a study conducted in Italy (37%) [43], one in South Africa (25%) [44] and one in Brazil (10%) [45], as well as the average prevalence estimated from various studies carried out in China (21%) [42]. However, it should be noted that in our study, as in most of these other studies, the PA of pregnant women was self-reported and was not assessed by pedometers, accelerometers or other objective measuring techniques [71]. The assessment of PA with questionnaires allows large samples to be studied or to be integrated into clinical practice. However, it may lead to biases associated with social desirability or poor recall, or with transient or stable cognitive impairments that prevent an accurate perception of the subject's own lifestyle. Interestingly, a Canadian study found that adult pregnant women reported a mean of 34.3 daily minutes of PA, whereas time measured objectively was 14.9 minutes [35].
Overall, in our study we found low variability in the prevalence of adherence to the WHO recommendation. Slightly higher compliance was found among participants who were currently studying compared to those who were not. The percentage was somewhat higher among primigravidae than among those who had previously had more pregnancies. This is consistent with the results of other studies [36,48]. In this study, no relevant variability was detected in the weekly time spent performing PA by pregnant women according to BMI. By contrast, a study in Sweden estimated a higher compliance rate among pregnant women with lower BMI [40].
As regards time spent daily in sedentary activities, participants reported an average of 3.9 hours per day, significantly lower than in other studies. According to a review published in 2017, the average daily time spent by pregnant women in sedentary activities, measured objectively, ranged from 7.07 hours in a study in the USA to 18.3 hours in a study in Ethiopia. Yet, participants in a study in Singapore reported an average of 8.6 hours of sedentary activities per day [58]. More recent studies also show considerable disparity in average daily sedentary activity figures: 5.9 hours in a study in Japan [59] and 9.3 hours in a study in Sweden [53]. Moreover, a study in Pittsburgh, USA, found that during the COVID years, PA time of pregnant women decreased and sedentary activity increased compared to previous years [72].
There has been little research on sociodemographic or obstetric correlates of the time spent in sedentary activities by pregnant women. In our study, marked differences were found according to the educational level of participants (the higher the educational level, the more time spent in sedentary activities per day). This seems to agree with a study in Japan, which showed that time spent in sedentary activities correlated with the income level of the pregnant women [59]. In our study sample, it was also correlated with the language spoken at home as a child (i.e., higher among those who spoke Spanish as a child) and to gravidity (more time spent in sedentary activities per day among primigravidae).
The potential risks of excessive sedentary activity for the pregnant woman, for childbirth and for child development are highly relevant [52-55]. Hence, it would be desirable to expand research in this field, addressing the prevailing sedentary activity patterns among pregnant women per se and their predictors and correlates, and to further explore their consequences. This could contribute to improving public health policies and to inform sound professional practice in terms of health advice to pregnant women on physical and sedentary activities. Several studies have confirmed that there tends to be a reduction in physical activity and an increase in sedentary activity during pregnancy [17,56]. Yet, Canadian researchers note that this may now be exacerbated by increasing social pressure for sedentary activities [35].
Moreover, previous studies have shown that there tends to be a continuity between the pre-pregnancy lifestyle and the lifestyle of pregnant women, also in terms of physical activity [34,37,41,48,73]. Women who had an active lifestyle before pregnancy tend to engage in higher levels of PA during pregnancy. This is logical but implies an important challenge in promoting PA among pregnant women, as it highlights the need to promote an active lifestyle among adolescents and women of childbearing age in general. In a global context of increasing physical inactivity among adolescent girls [74], it is key to address the many barriers already identified in many countries that prevent adolescent girls from adopting an active lifestyle [75]. Reducing these barriers necessarily involves cross-sectoral action, not only by the health system or from sport and exercise-related agencies, and interdisciplinary collaboration across multiple domains.
Some studies have specifically investigated the barriers encountered by pregnant women when practising PA. One of those most frequently cited is not having received suitable health advice recommending PA, or having received contradictory information on the subject [44,45,76]. At the same time, other types of research on the determinants of health professionals' practice when recommending PA to pregnant women have found that their professional practice in this respect is often influenced by relevant limitations and that they have little support to perform their work in this area [77]. One of the barriers identified in such studies is a lack of undergraduate or postgraduate training. For example, in the United States, only 8% of medical students report having received specific training in physical activity [78]. This may suggest that curricula in medical and other health studies should be reviewed in appropriate areas to allow greater training in the promotion of healthy lifestyles in pregnant women and in the population as a whole [79,80]. The results of these studies also suggest that changes may also be needed in the organisation of health care services. Such changes should enable professionals to provide lifestyle advice to pregnant women with more time in consultations, to have greater institutional support in this role, and to benefit from multidisciplinary collaboration when needed [81].
For obvious reasons, pregnant women with obesity are one of the groups of pregnant women who would require the most support from health professionals in adopting an active lifestyle. Yet, one study suggests that they are the least likely to receive health advice in this regard [82]. This may be linked to the widespread problem of social stigmatisation of obesity, which may also be affecting the health care received by pregnant women living with obesity [83]. Such social stigma has been identified as reducing access to health services for pregnant women with excess weight and leading to mental health problems, with potential counterproductive side-effects on the course of obesity itself [84].
Strengths and Limitations
This study has some strengths. The sample selection process was governed by the criterion of obtaining a representative sample of the population of pregnant women who were being attended at their reference public hospital for regular pregnancy monitoring (specifically, at the 20th-week ultrasound scan). An internationally validated questionnaire (i.e., the GPAQ) was used to collect information on different domains of physical activity (at work, in leisure time and during travel). Data were collected in face-to-face interviews by a trained health professional, in a quiet space in the hospital, using an anonymous questionnaire. Information cards with locally adapted pictures were used to illustrate different types of moderate or vigorous physical activity, both at work and in leisure time. The omission rate for all questions in the questionnaire was very low (generally less than 1%). Among other aspects, the correlates of sedentary activity in pregnant women, which is a relatively little studied field, were investigated.
However, the study also has some limitations. Its design was cross-sectional, which excludes the possibility of inferring causal relationships between the variables studied. It was not possible to interview foreign pregnant women who were not fluent in Spanish, due to the lack of support from interpreters in the various languages. Although the response rate was relatively high (77.5%), the percentage of women with a university degree among those who agreed to be interviewed was higher than among those who refused to participate. Data were self-reported, as they were collected by means of a questionnaire, which does not exclude different types of bias (mainly social desirability or recall bias). In addition, the GPAQ measures sedentary activities by means of a single item, which could be a limitation of this instrument [85,86].
5. Conclusions
The estimated prevalence of compliance with the WHO recommendation for physical activity in pregnancy (i.e., a minimum of 150 minutes of moderate PA per week) was relatively high among the participants in the sample (approximately 74%). However, this indicates that a quarter of pregnant women have a rather inactive lifestyle, which may lead to considerable problems for themselves and for child development.
There was little sociodemographic variability in compliance with the WHO recommendation. The average weekly time spent on physical activity at work was three times higher than that of leisure time PA in the sample as a whole. Work-related PA was performed by approximately one third of the sample, while leisure time PA was practised by approximately two thirds.
The sociodemographic correlates of leisure time PA differed substantially from those of work-related PA, mainly in terms of educational level. Work-related PA was the area of PA with the greatest sociodemographic variability. PA linked to travel did not exhibit any relevant sociodemographic variability.
As for the time spent by pregnant women on sedentary activities, marked differences were detected according to educational level, to the language spoken at home during childhood and to gravidity.
Most pregnant women of this study met international PA recommendations for pregnancy. However, the correlates of leisure PA are different from those regarding work PA. Therefore, planning and implementation of effective public health strategies to foster an active and healthy lifestyle during pregnancy may require different approaches and communication plans, depending on PA literacy and socioeconomic factors.
Author Contributions
Conceptualization, R.M.-B. and R.S.-R.; methodology, R.M.-B., R.S.-R., D.G.-B. and K.M.C.; investigation, R.M.-B., E.F.-M., D.G.-B., A.J.G., M.M.-R., S.R.-B and R.S.-R; resources, R.M.-B. and S.R.-B.; data curation, R.M.-B.; writing—original draft preparation, K.M.C. and R.M.-B.; writing—review and editing, R.M.-B., R.S.-R., D.G.-B., A.J.G., M.M.-R., E.F.-M. and S.R.-B.; supervision, R.M.-B., D.G.-B. and R.S.-R.; project administration, R.M.-B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Research Ethics Committee of the Andalusian Health and Family Department, Spain, reviewed and approved the study protocol (code 0626-N-20). Date of approval: 20 July 2020.
Informed Consent Statement
Verbal and written information about the study was given to participants. Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Acknowledgments
The corresponding author was supported by Polytechnic University of Santarém and SPRINT - Sport Physical Activity and Health Research & Innovation Center [UID/06185/2023], by national funds through FCT – Fundação para a Ciência e Tecnologia, the Portuguese Foundation for Science and Technology, within the scope of the Active Pregnancy project [2023.14896.PEX]. PI: Rita Santos-Rocha. DOI: 10.54499/2023.14896.PEX. Website: https://sprint-sci.com/en/research-innovation/research-projects-external/active-pregnancy-202314896pex. YouTube Channel: @GravidezAtiva-ActivePregnancy.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ACOG | American College of Obstetricians and Gynaecologists. |
| ESDRM | Sport Sciences School of Rio Maior – Santarém Polytechnic University, Portugal |
| GPAQ | Global Physical Activity Questionnaire. |
| IOC | International Olympic Committee. |
| MET | Metabolic Equivalents of Task. |
| MVPA | Moderate-to-vigorous physical activity. |
| PA | Physical activity. |
| RANZCOG | Royal Australian and New Zealand College of Obstetricians and Gynaecologist. |
| SPRINT | Sport Physical Activity and Health Research & Innovation Center, Portugal. |
| US DHHS | United States Department of Health and Human Services. |
| WHO | World Health Organization. |
References
- World Health Organization. WHO guidelines on physical activity and sedentary behavior. 2020;3(2):115-118. doi:10.1016/j.smhs.2021.05.001. [CrossRef]
- Dipietro L, Evenson KR, Bloodgood B, et al. Benefits of Physical Activity during Pregnancy and Postpartum: An Umbrella Review. Med Sci Sports Exerc. 2019;51(6):1292-1302. doi:10.1249/MSS.0000000000001941. [CrossRef]
- Pereira MA, Rifas-Shiman SL, Kleinman KP, et al. Predictors of change in physical activity during and after pregnancy: Project Viva. Am J Prev Med. 2007;32(4):312-319. doi:10.1016/j.amepre.2006.12.017. [CrossRef]
- Okely AD, Kontsevaya A, Ng J, Abdeta C. 2020 WHO guidelines on physical activity and sedentary behavior. Sports Med Health Sci. 2021;3(2):115-118. doi:10.1016/j.smhs.2021.05.001. [CrossRef]
- Mudd LM, Owe KM, Mottola MF, Pivarnik JM. Health benefits of physical activity during pregnancy: an international perspective. Med Sci Sports Exerc. 2013;45(2):268-277. doi:10.1249/MSS.0b013e31826cebcb. [CrossRef]
- Ferrari N, Joisten C. Impact of physical activity on course and outcome of pregnancy from pre- to postnatal. Eur J Clin Nutr. 2021;75(12):1698-1709. doi:10.1038/s41430-021-00904-7. [CrossRef]
- Xie W, Zhang L, Cheng J, et al. Physical activity during pregnancy and the risk of gestational diabetes mellitus: a systematic review and dose-response meta-analysis. BMC Public Health. 2024;24(1):594. doi:10.1186/s12889-024-18131-7. [CrossRef]
- Melzer K, Schutz Y, Boulvain M, Kayser B. Physical activity and pregnancy: cardiovascular adaptations, recommendations and pregnancy outcomes. Sports Med. 2010;40(6):493-507. doi:10.2165/11532290-000000000-00000. [CrossRef]
- Grau A, Sánchez Del Pino A, Amezcua-Prieto C, et al. An umbrella review of systematic reviews on interventions of physical activity before pregnancy, during pregnancy, and postpartum to control and/or reduce weight gain. Int J Gynaecol Obstet. 2024;166(3):915-931. doi:10.1002/ijgo.15453. [CrossRef]
- Dhar P, Sominsky L, O'Hely M, et al. Physical activity and circulating inflammatory markers and cytokines during pregnancy: A population-based cohort study. Acta Obstet Gynecol Scand. 2024;103(9):1808-1819. doi:10.1111/aogs.14870. [CrossRef]
- Cai C, Busch S, Wang R, Sivak A, Davenport MH. Physical activity before and during pregnancy and maternal mental health: A systematic review and meta-analysis of observational studies. J Affect Disord. 2022;309:393-403. doi:10.1016/j.jad.2022.04.143. [CrossRef]
- Davenport MH, McCurdy AP, Mottola MF, et al. Impact of prenatal exercise on both prenatal and postnatal anxiety and depressive symptoms: a systematic review and meta-analysis. Br J Sports Med. 2018;52(21):1376-1385. doi:10.1136/bjsports-2018-099697. [CrossRef]
- González-Cazorla E, Brenes-Romero AP, Sánchez-Gómez MJ, et al. Physical Activity in Work and Leisure Time during Pregnancy, and Its Influence on Maternal Health and Perinatal Outcomes. J Clin Med. 2024;13(3):723. doi:10.3390/jcm13030723. [CrossRef]
- Wu D, Chen S, Zhong X, et al. Prevalence and factors associated with antenatal depressive symptoms across trimesters: a study of 110,584 pregnant women covered by a mobile app-based screening programme in Shenzhen, China. BMC Pregnancy Childbirth. 2024;24(1):480. doi:10.1186/s12884-024-06680-z. [CrossRef]
- Ekelöf K, Andersson O, Holmén A, et al. Depressive symptoms postpartum is associated with physical activity level the year prior to giving birth - A retrospective observational study. Sex Reprod Healthc. 2021;29:100645. doi:10.1016/j.srhc.2021.100645. [CrossRef]
- Menke BR, Duchette C, Tinius RA, et al. Physical Activity during Pregnancy and Newborn Body Composition: A Systematic Review. Int J Environ Res Public Health. 2022;19(12):7127. doi:10.3390/ijerph19127127. [CrossRef]
- Dieberger AM, Obermayer-Pietsch B, Harreiter J, et al; DALI Core Investigator group. Physical activity and sedentary time across pregnancy and associations with neonatal weight, adiposity and cord blood parameters: a secondary analysis of the DALI study. Int J Obes. 2023;47(9):873-881. doi:10.1038/s41366-023-01347-9. [CrossRef]
- Musakka ER, Ylilauri MP, Jalanka J, et al. Maternal exercise during pregnancy is associated with reduced risk of asthma in the child: A prospective birth cohort study. Med. 2025;6(2):100514. doi:10.1016/j.medj.2024.09.003. [CrossRef]
- Zhang J, Xiao Y, Bai S, et al. The Association Between Exercise During Pregnancy and the Risk of Preterm Birth. Int J Womens Health. 2024;16:219-228. doi:10.2147/IJWH.S447270. [CrossRef]
- Weng YM, Green J, Yu JJ, et al. The relationship between incidence of cesarean section and physical activity during pregnancy among pregnant women of diverse age groups: Dose-response meta-analysis. Int J Gynaecol Obstet. 2024;164(2):504-515. doi:10.1002/ijgo.14915. [CrossRef]
- Lv C, Lu Q, Zhang C, et al. Relationship between first trimester physical activity and premature rupture of membranes: a birth cohort study in Chinese women. BMC Public Health. 2024;24(1):1736. doi:10.1186/s12889-024-18791-5. [CrossRef]
- Claiborne A, Wisseman B, Kern K, et al. Exercise during pregnancy Dose: Influence on preterm birth outcomes. Eur J Obstet Gynecol Reprod Biol. 2024;300:190-195. doi:10.1016/j.ejogrb.2024.07.017. [CrossRef]
- US Department of Health and Human Services. Physical activity guidelines for Americans. Oklahoma Nurse. 2018;53(4):25. doi:10.1249/fit.0000000000000472. [CrossRef]
- ACOG CO. Physical Activity and Exercise During Pregnancy and the Postpartum Period. Obstet Gynecol. 2020;135(4):178–188. doi:10.1097/AOG.0000000000004267. [CrossRef]
- Mottola MF, Davenport MH, Ruchat SM, et al. No. 367-2019 Canadian Guideline for Physical Activity throughout Pregnancy [published correction appears in J Obstet Gynaecol Can. 2019;41(7):1067. doi:10.1016/j.jogc.2019.05.001.]. J Obstet Gynaecol Can. 2018;40(11):1528-1537. doi:10.1016/j.jogc.2018.07.001. [CrossRef]
- The Royal Australian New Zealand College of Obstetricians and Gynecologists (RANZCOG). Exercise during Pregnancy. 2016. https://ranzcog.edu.au/womens-health/patient-informationresources/exercise-during-pregnancy.
- Bø K, Artal R, Barakat R, et al. Exercise and pregnancy in recreational and elite athletes: 2016/2017 evidence summary from the IOC expert group meeting, Lausanne. Part 5. Recommendations for health professionals and active women. Br J Sports Med. 2018;52(17):1080-1085. doi:10.1136/bjsports-2018-099351. [CrossRef]
- Department of Health & Social Care. UK Chief Medical Officer’s physical activity guidelines. 2019. https://assets.publishing.service.gov.uk/media/5d839543ed915d52428dc134/uk-chief-medical-officers-physical-activity-guidelines.pdf.
- Sport Medicine Australia. SMA statement the benefits and risks of exercise during pregnancy. J Sci Med Sport. 2002;5(1):11-19. doi:10.1016/s1440-2440(02)80293-6. [CrossRef]
- Barakat R, et al. Guía de práctica clínica sobre la actividad física durante el embarazo [Spanish]. Universidad Politécnica de Madrid. 2023. https://portal.guiasalud.es/gpc/actividad-fisica-embarazo/.
- Goya M, Miserachs M, SuyA, et al. Documento de consenso de la Sociedad Española de Obstetricia y Ginecologia (SEGO) y el Comité Español Interdisciplinario para la Prevención Vascular (CEIPV). Ventana de oportunidad: prevención del riesgo vascular en la mujer. Resultados adversos del embarazo y riesgo de enfermedad vascular [Consensus document of the Spanish Society of Obstetrics and Gynaecology (SEGO) and the Spanish Interdisciplinary Committee for Vascular Prevention (CEIPV). Window of opportunity: prevention of vascular risk in women]. 2023;97:e202310084.
- Muñoz J, Delgado M. (coord.) Guía de recomendaciones para la promoción de actividad física [Guide of recommendations for promoting physical activity]. Junta de Andalucía, Consejería de Salud. 2010. https://acortar.link/3EniXS.
- Hayman M, Brown WJ, Brinson A, et al. Public health guidelines for physical activity during pregnancy from around the world: a scoping review. Br J Sports Med. 2023;57(14):940-947. doi:10.1136/bjsports-2022-105777. [CrossRef]
- Silva-Jose C, Mottola MF, Palacio M, et al. Impact of Physical Activity Interventions on High-Risk Pregnancies: A Systematic Review and Meta-Analysis. J Pers Med. 2023;14(1):14. doi:10.3390/jpm14010014. [CrossRef]
- Srugo SA, Fernandes da Silva D, Menard LM, et al. Recent Patterns of Physical Activity and Sedentary Behaviour Among Pregnant Adults in Canada. J Obstet Gynaecol Can. 2023;45(2):141-149. doi:10.1016/j.jogc.2022.11.011. [CrossRef]
- Ning Y, Williams MA, Dempsey JC, et al. Correlates of recreational physical activity in early pregnancy. J Matern Fetal Neonatal Med. 2003;13(6):385-393. doi:10.1080/jmf.13.6.385.393. [CrossRef]
- Román-Gálvez MR, Amezcua-Prieto C, Salcedo-Bellido I, et al. Physical activity before and during pregnancy: A cohort study. Int J Gynaecol Obstet. 2021;152:374-381.
- Mendinueta A, Esnal H, Arrieta H, et al. What Accounts for Physical Activity during Pregnancy? A Study on the Sociodemographic Predictors of Self-Reported and Objectively Assessed Physical Activity during the 1st and 2nd Trimesters of Pregnancy. Int J Environ Res Public Health. 2020;17(7):2517. doi:10.3390/ijerph17072517. [CrossRef]
- Todorovic J, Terzic-Supic Z, Bjegovic-Mikanovic V, et al. Factors Associated with the Leisure-Time Physical Activity (LTPA) during the First Trimester of the Pregnancy: The Cross-Sectional Study among Pregnant Women in Serbia. Int J Environ Res Public Health. 2020;17(4):1366. doi:10.3390/ijerph17041366. [CrossRef]
- Lindqvist M, Lindkvist M, Eurenius E, et al. Leisure time physical activity among pregnant women and its associations with maternal characteristics and pregnancy outcomes. Sex Reprod Health. 2016;9:14-20.
- Lynch KE, Landsbaugh JR, Whitcomb BW, et al. Physical activity of pregnant Hispanic women. Am J Prev Med. 2012;43(4):434-439. doi:10.1016/j.amepre.2012.06.020. [CrossRef]
- Zhang W, Zhang L, Xu P, et al. Physical activity levels and influencing factors among pregnant women in China: A systematic review and meta-analysis. Int J Nurs Stud. 2024;158:104841. doi:10.1016/j.ijnurstu.2024.104841. [CrossRef]
- Sarno L, Borrelli P, Mennitti C, et al. Adherence to physical activity among pregnant women in Southern Italy: results of a cross-sectional survey. Midwifery. 2024;137:104102. doi:10.1016/j.midw.2024.104102. [CrossRef]
- Okafor UB, Goon DT. Physical Activity Level during Pregnancy in South Africa: A Facility-Based Cross-Sectional Study. Int J Environ Res Public Health. 2020;17(21):7928. doi:10.3390/ijerph17217928. [CrossRef]
- Nascimento SL, Surita FG, Godoy AC, et al. Physical Activity Patterns and Factors Related to Exercise during Pregnancy: A Cross Sectional Study [publication correction: appears in PLoS One. 2015;10(7):e0133564.10.1371/journal.pone.0133564.]. PLoS One. 2015;10(6):e0128953. doi:10.1371/journal.pone.0128953. [CrossRef]
- Gaston A, Vamos CA. Leisure-time physical activity patterns and correlates among pregnant women in Ontario, Canada. Matern Child Health J. 2013;17(3):477-484. doi:10.1007/s10995-012-1021-z. [CrossRef]
- Amezcua-Prieto C, Olmedo-Requena R, Jiménez-Mejías E, et al. Factors associated with changes in leisure time physical activity during early pregnancy. Int J Gynaecol Obstet. 2013;121(2):127-131. doi:10.1016/j.ijgo.2012.11.021. [CrossRef]
- Gaston A, Cramp A. Exercise during pregnancy: a review of patterns and determinants. J Sci Med Sport. 2011;14(4):299-305. doi:10.1016/j.jsams.2011.02.006. [CrossRef]
- Evenson KR, Savitz DA, Huston SL. Leisure-time physical activity among pregnant women in the US. Paediatr Perinat Epidemiol. 2004;18(6):400-407. doi:10.1111/j.1365-3016.2004.00595.x. [CrossRef]
- Rinaldi AEM, Paula JA, Almeida MA, et al. Trend in physical activity patterns of pregnant women living in Brazilian capitals. Rev Saude Publica. 2022;56:42. doi:10.11606/s1518-8787.2022056003300. [CrossRef]
- Petersen AM, Leet TL, Brownson RC. Correlates of physical activity among pregnant women in the United States. Med Sci Sports Exerc. 2005;37(10):1748-1753. doi:10.1249/01.mss.0000181302.97948.90. [CrossRef]
- Kubler JM, Edwards C, Cavanagh E, et al. Maternal physical activity and sitting time and its association with placental morphology and blood flow during gestation: Findings from the Queensland Family Cohort study. J Sci Med Sport. 2024;27(7):480-485. doi:10.1016/j.jsams.2024.02.011. [CrossRef]
- Lindberger E, Ahlsson F, Johansson H, et al. Associations of maternal sedentary behavior and physical activity levels in early to mid-pregnancy with infant outcomes: A cohort study. Acta Obstet Gynecol Scand. 2024;103(12):2522-2531. doi:10.1111/aogs.14983. [CrossRef]
- Khojah N, Gibbs BB, Alghamdi SA, et al. Associations Between Domains and Patterns of Sedentary Behavior with Sleep Quality and Duration in Pregnant Women. Healthcare (Basel). 2025;13(3):348. doi:10.3390/healthcare13030348. [CrossRef]
- Osumi A, Kanejima Y, Ishihara K, et al. Effects of Sedentary Behavior on the 556 Complications Experienced by Pregnant Women: A Systematic Review. Reprod Sci. 2024;31(2):352-365. doi:10.1007/s43032-023-01321-w. [CrossRef]
- Evenson KR, Wen F. Prevalence and correlates of objectively measured physical activity and sedentary behavior among US pregnant women. Prev Med. 2011;53(1-2):39-43. doi:10.1016/j.ypmed.2011.04.014. [CrossRef]
- Fazzi C, Saunders DH, Linton K, et al. Sedentary behaviours during pregnancy: a systematic review. Int J BehavNutr Phys Act. 2017;14(1):32. doi:10.1186/s12966-017-0485-z. [CrossRef]
- Nagai M, Tsuchida A, Matsumura K, et al; Japan Environment and Children’s Study Group. Factors related to sedentary behavior of pregnant women during the second/third trimester: prospective results from the large-scale Japan Environment and Children's Study. BMC Public Health. 2024;24(1):3182. doi:10.1186/s12889-024-20574-x. [CrossRef]
- Corrales-Gutierrez I, Mendoza R, Gomez-Baya D, Leon-Larios F. Understanding the Relationship between Predictors of Alcohol Consumption in Pregnancy: Towards Effective Prevention of FASD. Int J Environ Res Public Health. 2020;17(4):1388. doi:10.3390/ijerph17041388. [CrossRef]
- Mendoza R, Morales-Marente E, Palacios MS, et al. Health advice on alcohol consumption in pregnant women in Seville (Spain). Gac Sanit. 2020;34(5):449-458. doi:10.1016/j.gaceta.2018.11.008. [CrossRef]
- Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health. 2006;14:66-70. doi:10.1007/s10389-006-0024-x. [CrossRef]
- Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire (GPAQ): nine country reliability and validity study. J Phys Act Health. 2009;6(6):790-804. doi:10.1123/jpah.6.6.790. [CrossRef]
- Herrmann SD, Heumann KJ, Der Ananian CA, Ainsworth BE. Validity and Reliability of the Global Physical Activity Questionnaire (GPAQ). Measurement Physical Edu Exercise Sci. 2013;17(3):221-235. doi:10.1080/1091367X.2013.805139. [CrossRef]
- World Health Organization. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. Surveillance and Population-Based Prevention, Prevention of Noncommunicable Diseases Department, World Health Organization. https://www.who.int/docs/default-source/ncds/ncd-surveillance/gpaq-analysis-guide.pdf.
- Algallai N, Martin K, Shah K, et al. Reliability and validity of a Global Physical Activity Questionnaire adapted for use among pregnant women in Nepal. Archives Public Health.2023;81(1):1–9. doi:10.1186/s13690-023-01032-3. [CrossRef]
- Meander L, Lindqvist M, Mogren I, et al. Physical activity and sedentary time during pregnancy and associations with maternal and fetal health outcomes: an epidemiological study. BMC Pregnancy Childbirth. 2021;21(1):166. doi:10.1186/s12884-021-03627-6. [CrossRef]
- Rial-Vázquez J, Vila-Farinas A, Varela-Lema L, et al. Actividad física en el embarazo y puerperio: prevalencia y recomendaciones de los profesionales sanitarios [Physical activity during pregnancy and postpartum: prevalence and healthcare professional recommendations]. Aten Primaria. 2023;55(5):102607. doi:10.1016/j.aprim.2023.102607. [CrossRef]
- Garland M, Wilbur JE, Semanik P, Fogg L. Correlates of Physical Activity During Pregnancy: A Systematic Review with Implications for Evidence-based Practice. Worldviews Evidence-Based Nursing. 2019;16(4):310–318. doi:10.1111/wvn.12391. [CrossRef]
- Fell DB, Joseph KS, Armson BA, Dodds L. The impact of pregnancy on physical activity level. Maternal Child Health J. 2009;13(5):597–603. doi:10.1007/s10995-008-0404-7. [CrossRef]
- Mok KC, Liu M, Wang X. The physical activity and sedentary behavior among pregnant women in Macao: A cross-sectional study. PLoS One. 2025;20(1):e0318352. doi:10.1371/journal.pone.0318352. [CrossRef]
- Aparicio-Ugarriza R, Mielgo-Ayuso J, Benito PJ, et al.; EXERNET Study Group. Physical activity assessment in the general population; instrumental methods and new technologies. Nutr Hosp. 2015;31Suppl 3:219-26. doi:10.3305/nh.2015.31.sup3.8769. [CrossRef]
- Kozai AC, Jones MA, Borrowman JD, et al. Patterns of physical activity, sedentary behavior, and sleep across pregnancy before and during two COVID pandemic years. Midwifery. 2025;141:104268. doi:10.1016/j.midw.2024.104268. [CrossRef]
- Yimer A, Endris S, Wossen A, Abate M. Pregnant women's knowledge, attitude, and practice toward physical exercise during pregnancy and its associated factors at Dessie town health institutions, Ethiopia. AJOG Glob Rep. 2024;4(4):100391. doi:10.1016/j.xagr.2024.100391. [CrossRef]
- Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. The Lancet. Child Ado Health. 2020;4(1):23-35. doi:10.1016/S2352-4642(19)30323-2. [CrossRef]
- Duffey K, Barbosa A, Whiting S, et al. Barriers and Facilitators of Physical Activity Participation in Adolescent Girls: A Systematic Review of Systematic Reviews. Front Public Health. 2021;9:743935.10.3389/fpubh.2021.743935.
- Gonçalves H, Soares ALG, Domingues MR, et al. Why are pregnant women physically inactive? A qualitative study on the beliefs and perceptions about physical activity during pregnancy. Cad Saude Publica. 2024;40(1):e00097323. doi:10.1590/0102-311XEN097323. [CrossRef]
- Heslehurst N, Newham J, Maniatopoulos G, et al. Implementation of pregnancy weight management and obesity guidelines: a meta-synthesis of healthcare professionals' barriers and facilitators using the Theoretical Domains Framework. Obes Rev. 2014;15(6):462-486.10.1111/obr.12160.
- Panton ZA, Smith S, Duggan M, et al. The Significance of Physical Activity Education: A Survey of Medical Students. Am J Lifestyle Med. 2023;18(6):832-842. doi:10.1177/15598276231187838. [CrossRef]
- Corfe BM, Smith T, Heslehurst N, et al. Long overdue: undergraduate nutrition education for medical students. Br J Nutr. 2022;129(6):1-2. doi:10.1017/S0007114522001647. [CrossRef]
- Jones G, Macaninch E, Mellor DD, et al. Putting nutrition education on the table: development of a curriculum to meet future doctors' needs. Br J Nutr. 2022;129(6):1-9. doi:10.1017/S0007114522001635. [CrossRef]
- Dilworth S, Doherty E, Mallise C, et al. Barriers and enablers to addressing smoking, nutrition, alcohol consumption, physical activity and gestational weight gain (SNAP-W) as part of antenatal care: A mixed methods systematic review. Implement Sci Commun. 2024;5(1):112. doi:10.1186/s43058-024-00655-z. [CrossRef]
- Santo EC, Forbes PW, Oken E, Belfort MB. Determinants of physical activity frequency and provider advice during pregnancy. BMC Pregnancy Childbirth. 2017;17(1):286. doi:10.1186/s12884-017-1460-z. [CrossRef]
- Tomiyama AJ, Carr D, Granberg EM, et al. How and why weight stigma drives the obesity 'epidemic' and harms health. BMCMed. 2018;16(1):123. doi:10.1186/s12916-018-1116-5. [CrossRef]
- Hill B, Azzari A, Botting KJ, et al. The Challenge of Weight Stigma for Women in the Preconception Period: Workshop Recommendations for Action from the 5th European Conference on Preconception Health and Care. Int J Environ Res Public Health. 2023;20(22):7034. doi:10.3390/ijerph20227034. [CrossRef]
- Laeremans M, Dons E, Avila-Palencia I, et al. Physical activity and sedentary behaviour in daily life: A comparative analysis of the Global Physical Activity Questionnaire (GPAQ) and the Sense Wear armband. PLoS One. 2017;12(5):e0177765. doi:10.1371/journal.pone.0177765. [CrossRef]
- Meh K, Jurak G, Sorić M, et al. Validity and Reliability of IPAQ-SF and GPAQ for Assessing Sedentary Behaviour in Adults in the European Union: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2021;18(9):4602. doi:10.3390/ijerph18094602. [CrossRef]
Figure 1.
Average number of weekly minutes of physical activity in leisure time according to educational level.
Figure 1.
Average number of weekly minutes of physical activity in leisure time according to educational level.
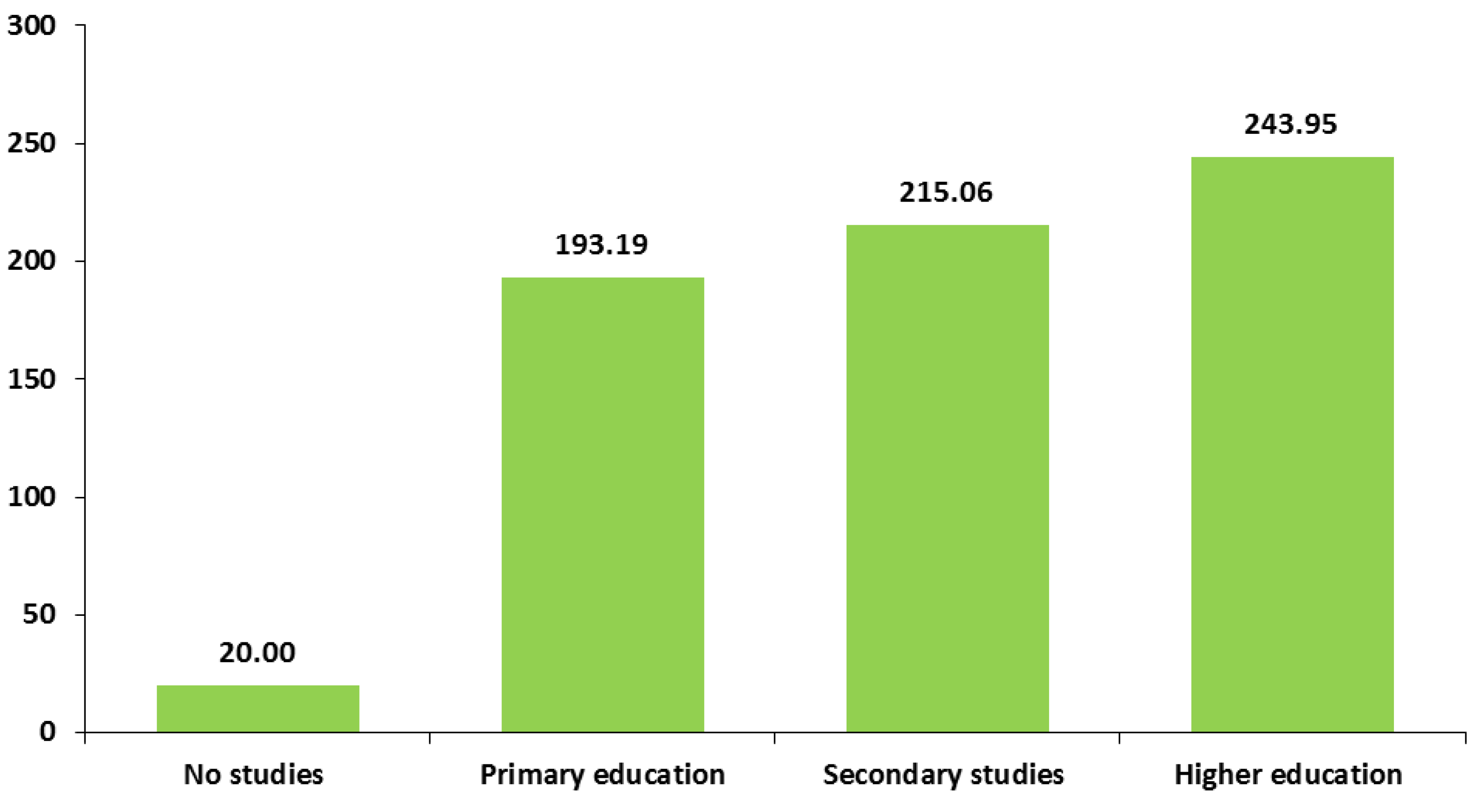
Figure 2.
Average weekly minutes of physical activity at work according to educational level.
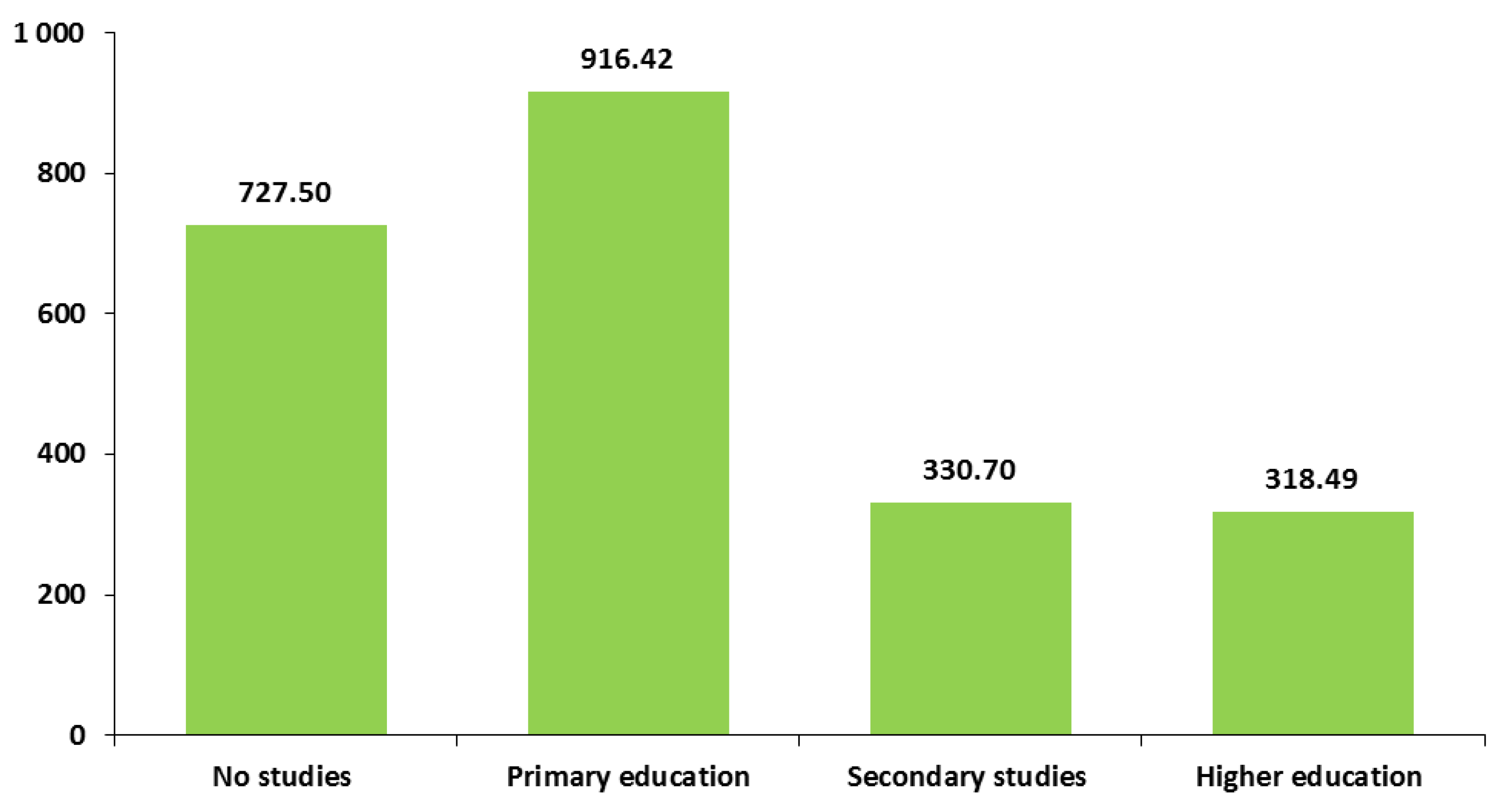
Figure 3.
Average weekly minutes of physical activity at work according to country of birth.
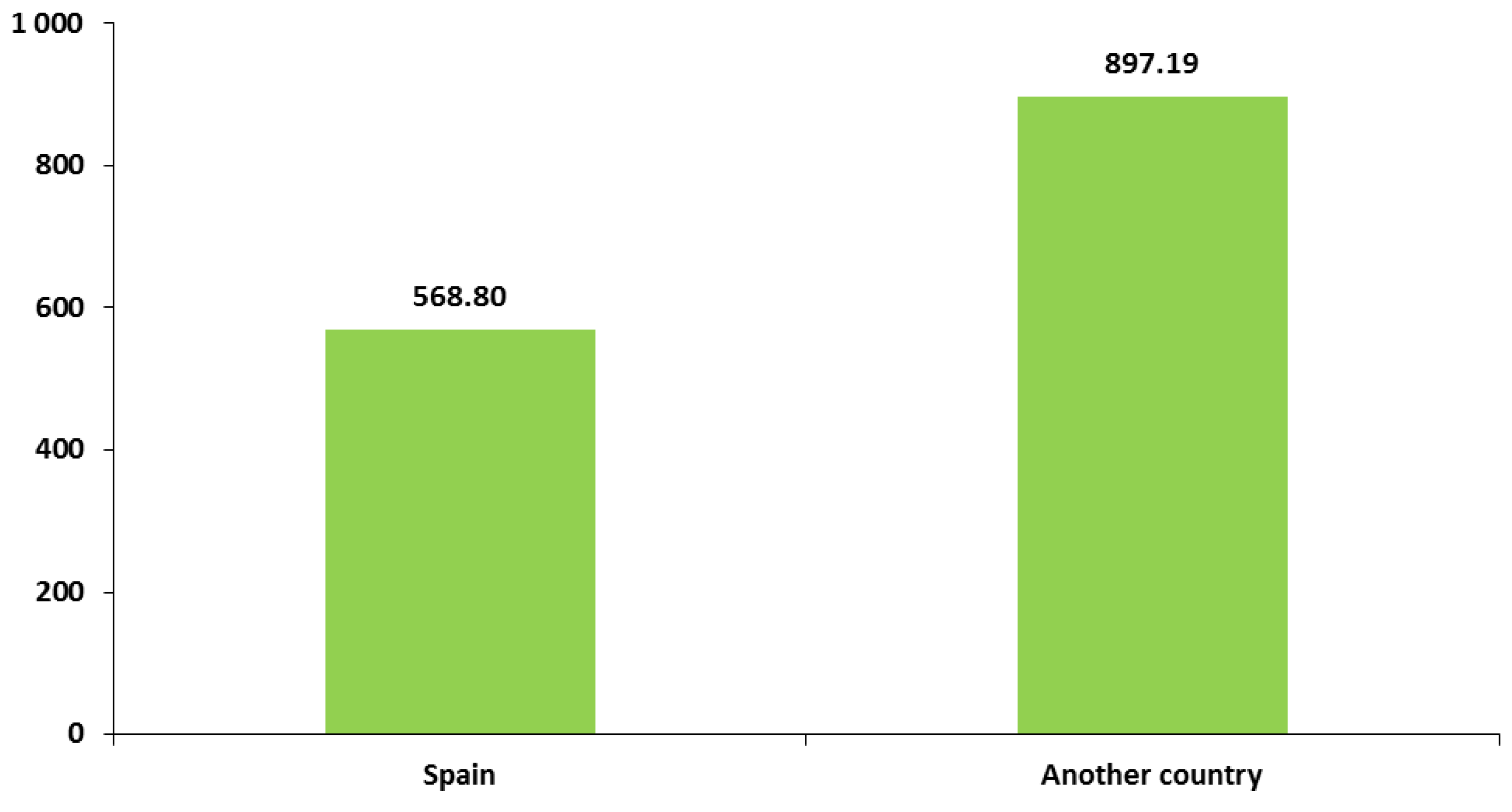
Figure 4.
Average MET-minutes per week according to educational level.
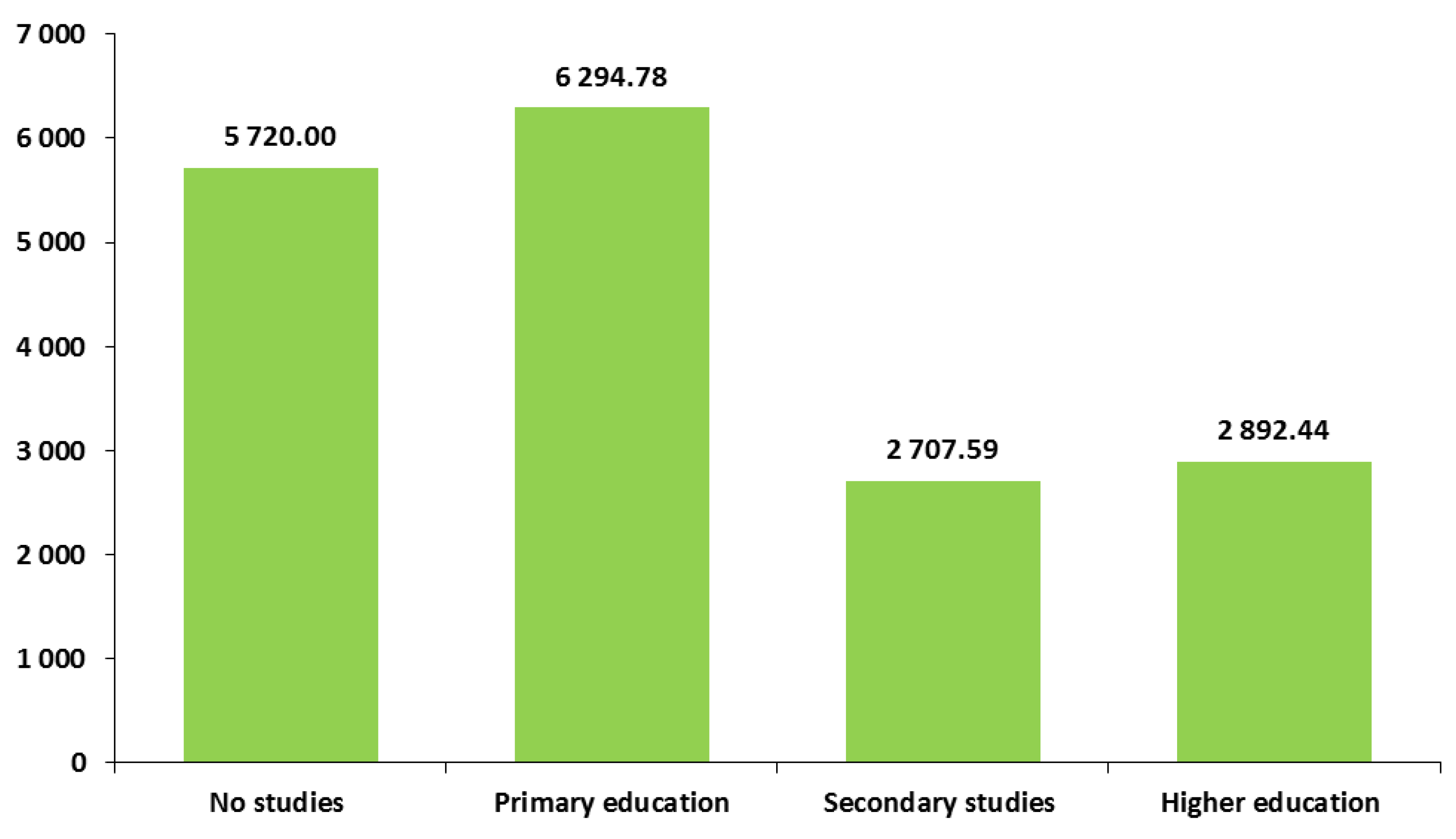
Figure 5.
Average daily minutes of sedentary behaviour according to educational level.
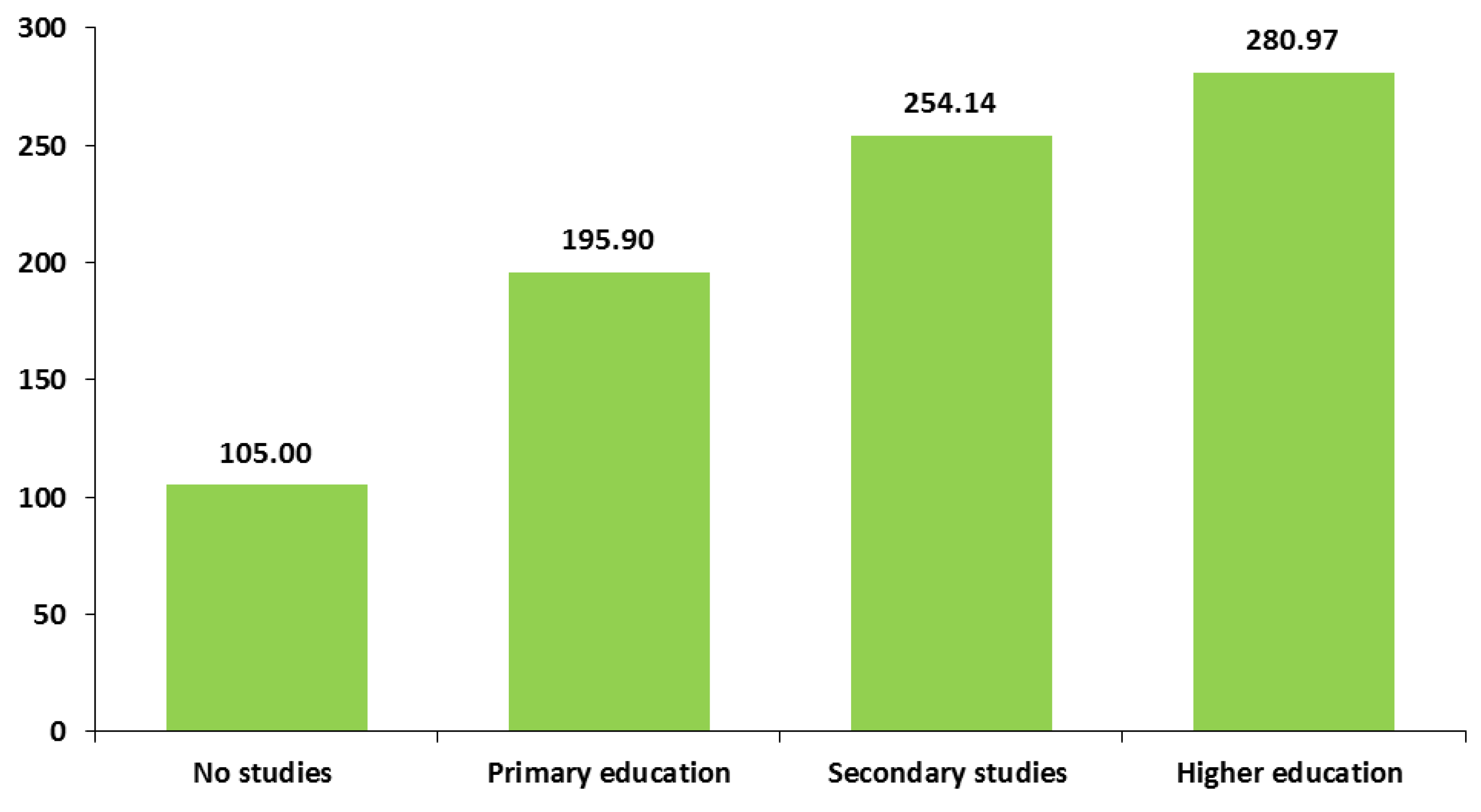

Table 1.
Sample description of sociodemographic and somatometric characteristics.
| Variables | N | Mean | Standard deviation | |
|---|---|---|---|---|
| Age (years) | 385 | 31.84 | 5.99 | |
| Approximate weight (kg) | 383 | 70.04 | 14.21 | |
| Approximate height (cm) | 383 | 163.30 | 6.12 | |
| Body Mass Index (Kg/height2) | 382 | 26.26 | 5.15 | |
| Variables | Categories | N | % | |
| Age | Less than 30 years | 119 | 30.9 | |
| 30 to 35 years | 110 | 28.6 | ||
| More than 35 years | 156 | 40.5 | ||
| Educational level | No studies | 4 | 1.0 | |
| Primary education | 175 | 45.5 | ||
| Secondary studies | 87 | 22.6 | ||
| Higher education | 119 | 30.9 | ||
| Currently studying | No | 328 | 85.2 | |
| Yes | 57 | 14.8 | ||
| Employment status | Full time | 157 | 41.1 | |
| Part time | 82 | 21.5 | ||
| Unemployed | 68 | 17.8 | ||
| Other | 75 | 18.6 | ||
| Size of place of residence | Up to 5,000 inhabitants | 45 | 11.7 | |
| From 5,001 to 20,000 inhabitants | 82 | 21.3 | ||
| From 20,001 to 50,000 inhabitants | 137 | 35.6 | ||
| More than 50,000 inhabitants | 121 | 31.4 | ||
| In a relationship | Yes | 382 | 99.2 | |
| No | 3 | 0.8 | ||
| Current language spoken at home |
Spanish | 347 | 90.1 | |
| Other (including bilinguals) | 38 | 9.9 | ||
| Language spoken at home as a child |
Spanish | 349 | 90.6 | |
| Other (including bilingual) | 36 | 9.4 | ||
| Country of birth | Spain | 353 | 91.7 | |
| Another country | 32 | 8.3 | ||
| Body Mass Index | Underweight | 5 | 1.3 | |
| Normal weight | 182 | 47.6 | ||
| Overweight | 116 | 30.4 | ||
| Obesity | 79 | 20.7 | ||
| Total sample size: 385 | ||||
Table 2.
Sample description of obstetric characteristics.
| Variables | N | Mean | Standard deviation | |
|---|---|---|---|---|
| Number of pregnancies including the current one | 385 | 2.06 | 1.11 | |
| Number of vaginal births | 385 | 0.48 | 0.74 | |
| Number of cesarean births | 385 | 0.12 | 0.34 | |
| Number of miscarriages | 385 | 0.37 | 0.72 | |
| Number of abortions | 385 | 0.10 | 0.35 | |
| Number of health problems during pregnancies ended in live birth | 190 | 0.25 | 0.63 | |
| Age at first pregnancy (years) | 383 | 27.50 | 6.35 | |
| Date of initiation of health care (in gestational weeks) | 380 | 6.42 | 2.40 | |
| Number of weeks since last menstrual period | 382 | 20.23 | 0.69 | |
| Variables | Categories | N | % | |
| Gravidity (number of pregnancies including the current one) | Primigravida | 142 | 36.9 | |
| Multigravida | 243 | 63.1 | ||
| Health problems during pregnancies ended in live birth | No | 159 | 83.7 | |
| Yes | 31 | 16.3 | ||
| Pregnancy planning | No | 90 | 23.4 | |
| Yes | 294 | 76.6 | ||
| Assisted reproduction pregnancy | No | 254 | 87.3 | |
| Yes | 37 | 12.7 | ||
| High-risk pregnancy care | No | 325 | 84.4 | |
| Yes | 60 | 15.6 | ||
| Trimester of pregnancy awareness | First trimester | 379 | 98.7 | |
| Second trimester | 5 | 1.3 | ||
| Professional health careduring pregnancy | No | 2 | 0.5 | |
| Yes | 383 | 99.5 | ||
Table 3.
Frequency of physical and sedentary activity patterns by domains, METs and totals.
| Variables | N | Mean | Standard deviation | |
|---|---|---|---|---|
| Total PA (work, travel to and from places, and leisure) (min/week) | 384 | 902.85 | 1,061.31 | |
| Total work PA (min/week) | 382 | 596.31 | 1,037.52 | |
| Vigorous work PA (min/week) | 382 | 201.28 | 683.26 | |
| Moderate work PA (min/week) | 380 | 397.11 | 818.45 | |
| Total active travel to and from places (min/week) | 384 | 97.57 | 211.28 | |
| Total leisure PA (min/week) | 384 | 212.07 | 262.34 | |
| Vigorous leisure PA (min/week) | 384 | 2.34 | 34.20 | |
| Moderate leisure PA (min/week) | 384 | 209.73 | 261.99 | |
| Total vigorous PA (work and leisure) (min/week) | 384 | 202.58 | 681.80 | |
| Total moderate PA (work, travel to and from places, and leisure) (min/week) | 384 | 700.27 | 858.64 | |
| Total % moderate PA (min/week) | 339 | 90.46 | 26.66 | |
| Number of MET-min/week | 384 | 4,421.70 | 6,254.84 | |
| Sedentary behaviour (min/day) | 383 | 234.61 | 162.99 | |
| Variables | Categories | N | % | |
| Engaged in PA at work | Yes | 128 | 33.5 | |
| No | 254 | 66.5 | ||
| Engaged in PA for travel to and from places | Yes | 139 | 36.2 | |
| No | 245 | 63.8 | ||
| Engaged in PA for leisure | Yes | 237 | 61.7 | |
| No | 147 | 38.3 | ||
| Engaged in some type of PA | Yes | 324 | 84.4 | |
| No | 60 | 15.6 | ||
| Engaged in vigorous PA | Yes | 42 | 10.9 | |
| No | 342 | 89.1 | ||
| Engaged in moderate PA | Yes | 312 | 81.3 | |
| No | 72 | 18.8 | ||
| Engaged in at least 150 minutes of moderate intensity PA per week. Met WHO requirement of PA during pregnancy | Yes | 283 | 73.7 | |
| No | 101 | 26.3 | ||
Notes. PA: Physical activity; MET: Metabolic Equivalents of Task.
Table 4.
Variability of compliance with the WHO recommendation of at least 150 minutes of moderate PA per week according to sociodemographic and obstetric characteristics.
Table 4.
Variability of compliance with the WHO recommendation of at least 150 minutes of moderate PA per week according to sociodemographic and obstetric characteristics.
| Variables / Categories | Yes | N | Statistical parameters |
|---|---|---|---|
| Age | N=283 % |
N=101 % |
Chi2 (2) = 2.56; p = 0.28;Cramer’s V = 0.08 |
| Less than 30 years | 70.6 | 29.4 | |
| From 30 to 35 years | 70.9 | 29.1 | |
| More than 35 years | 78.1 | 21.9 | |
| Educational level | N=283 % |
N=101 % |
Chi2 (3) = 5.44; p = 0.14;Cramer’s V = 0.12 |
| No studies | 25.0 | 75.0 | |
| Primary education | 73.0 | 27.0 | |
| Secondary studies | 77.0 | 23.0 | |
| Higher education | 73.9 | 26.1 | |
| Currently studying | N=283 % |
N=101 % |
Chi2 (1) = 5.2; p = 0.02;Cramer’s V = 0.12 |
| No | 71.6 | 28.4 | |
| Yes | 86.0 | 14.0 | |
| Employment status | N=280 % |
N=101 % |
Chi2 (3) = 1.27; p = 0.74;Cramer’s V = 0.06 |
| Full time | 73.1 | 26.9 | |
| Part time | 78.0 | 22.0 | |
| Unemployed | 70.6 | 29.4 | |
| Other | 72.0 | 28.0 | |
| Size of place of residence | N=283 % |
N=101 % |
Chi2 (3) = 4.52; p = 0.21;Cramer’s V = 0.11 |
| Up to 5,000 inhabitants | 77.8 | 22.2 | |
| From 5,001 to 20,000 inhabitants | 81.7 | 18.3 | |
| From 20,001 to 50,000 inhabitants | 70.6 | 29.4 | |
| More than 50,000 inhabitants | 70.2 | 29.8 | |
| In a relationship | N=283 % |
N=101 % |
Chi2 (1) = 0.08; p = 0.78;Cramer’s V = 0.01 |
| Yes | 73.8 | 26.2 | |
| No | 66.7 | 33.3 | |
| Current language spoken at home | N=283 % |
N=101 % |
Chi2 (1) = 0.15; p = 0.7;Cramer’s V = 0.02 |
| Spanish | 74.0 | 26.0 | |
| Other (including bilinguals) | 71.1 | 28.9 | |
| Language spoken at home as a child | N=283 % |
N=101 % |
Chi2 (1) = 0.96; p = 0.33;Cramer’s V = 0.05 |
| Spanish | 73.0 | 27.0 | |
| Other (including bilinguals) | 80.6 | 19.4 | |
| Country of birth | N=283 % |
N=101 % |
Chi2 (1) = 0.03; p = 0.86;Cramer’s V = 0.01 |
| Spain | 73.6 | 26.4 | |
| Another country | 75.0 | 25.0 | |
| Body Mass Index (BMI) | N=280 % |
N=101 % |
Chi2 (3) = 1.42; p = 0.7;Cramer’s V = 0.06 |
| Underweight | 80.0 | 20.0 | |
| Normal weight | 74.2 | 25.8 | |
| Overweight | 69.8 | 30.2 | |
| Obesity | 76.9 | 23.1 | |
| Gravidity (Number of pregnancies including the current one) | N=283 % |
N=101 % |
Chi2 (1) = 5.04; p = 0.02;Cramer’s V = 0.11 |
| Primigravida | 80.3 | 19.7 | |
| Multigravida | 69.8 | 30.2 | |
| Health problems during pregnancies ended in live birth | N=130 % |
N=59 % |
Chi2 (1) = 0.07; p = 0.79;Cramer’s V = 0.02 |
| No | 69.2 | 30.8 | |
| Yes | 66.7 | 33.3 | |
| Pregnancy planning | N=217 % |
N=73 % |
Chi2 (1) = 1.36; p = 0.24;Cramer’s V = 0.06 |
| No | 68.9 | 31.1 | |
| Yes | 75.1 | 24.9 | |
| Assisted reproduction pregnancy | N=283 % |
N=101 % |
Chi2 (1) = 0; p = 0.98;Cramer’s V = 0 |
| No | 74.8 | 25.2 | |
| Yes | 75.0 | 25.0 | |
| High-risk pregnancy care | N=283 % |
N=101 % |
Chi2 (1) = 0.5; p = 0.48;Cramer’s V = 0.04 |
| No | 74.4 | 25.6 | |
| Yes | 70.0 | 30.0 | |
| Trimester of pregnancy awareness | N=282 % |
N=101 % |
Chi2 (1) = 0.48; p = 0.49;Cramer’s V = 0.04 |
| First trimester | 73.8 | 26.2 | |
| Second trimester | 60.0 | 40.0 | |
| Professional health care during pregnancy | N=283 % |
N=101 % |
Chi2 (1) = 0.58; p = 0.45;Cramer’s V = 0.04 |
| No | 50.0 | 50.0 | |
| Yes | 73.8 | 26.2 |
Table 5.
Variability of physical and sedentary activities during pregnancy according to sociodemographic and somatometric characteristics.
Table 5.
Variability of physical and sedentary activities during pregnancy according to sociodemographic and somatometric characteristics.
| Variables / Categories | Leisure PA min/week | Work PA min/week | Travel to and from places PA min/week | MET minutes/week | Sedentary minutes/day | ||||||||||
| Mean | SD | Sign. | Mean | SD | Sign. | Mean | SD | Sign. | Mean | SD | Sign. | Mean | SD | Sign. | |
| Age | p=0.06 | p=0.17 | p=0.6 | p=0.18 | p=0.29 | ||||||||||
| Less than 30 years | 182.86 | 221.12 | 770.08 | 1,193.63 | 108.28 | 233.72 | 5,316.81 | 7,536.17 | 215.80 | 126.82 | |||||
| 30 to 35 years | 176.68 | 197.66 | 528.91 | 934.35 | 86.62 | 215.12 | 3,677.20 | 5,254.22 | 267.86 | 193.74 | |||||
| More than 35 years | 259.61 | 319.71 | 509.61 | 965.19 | 97.13 | 190.35 | 4,262.84 | 5,762.11 | 225.39 | 161.33 | |||||
| Educational level | p<0.05 | p<0.01 | p=0.28 | p<0.01 | p<0.01 | ||||||||||
| No studiesa | 20.00 | 40.00 | c, d | 727.50 | 1,337.69 | 0.00 | 0.00 | 5,720.00 | 10,750.70 | 105.00 | 51.96 | c, d | |||
| Primary education b | 193.19 | 255.03 | d | 916.42 | 1,233.32 | c, d | 100.56 | 239.02 | 6,294.78 | 7,813.60 | c, d | 195.90 | 127.05 | c, d | |
| Secondary studiesc | 215.06 | 198.56 | a | 330.70 | 758.30 | b | 92.53 | 178.85 | 2,707.59 | 3,448.23 | b | 254.14 | 166.90 | a, b | |
| Higher education d | 243.95 | 310.54 | a, b | 318.49 | 720.22 | b | 100.17 | 193.53 | 2,892.44 | 4,014.44 | b | 280.97 | 192.05 | a, b | |
| Currently studying | p<0.05 | p<0.01 | p=0.12 | p=0.73 | p=0.19 | ||||||||||
| No | 198.06 | 235.31 | 658.06 | 1,085.14 | 95.99 | 215.94 | 4,687.38 | 6,570.30 | 230.67 | 162.83 | |||||
| Yes | 292.46 | 375.01 | 244.21 | 602.12 | 106.67 | 183.74 | 2,897.54 | 3,673.28 | 257.11 | 163.52 | |||||
| Employment situation | p=0.87 | p<0.05 | p=0.27 | p=0.12 | p=0.38 | ||||||||||
| Full time e | 212.44 | 240.42 | 592.18 | 1,068.96 | g | 76.28 | 192.99 | 4,132.05 | 5,797.18 | 268.74 | 201.44 | ||||
| Part time f | 228.66 | 331.38 | 654.51 | 1,010.48 | g | 102.20 | 204.62 | 4,869.27 | 6,872.31 | 209.09 | 129.92 | ||||
| Unemployed g | 195.66 | 211.93 | 354.55 | 937.02 | e, f, h | 130.41 | 248.83 | 3,180.18 | 5,285.89 | 225.00 | 127.12 | ||||
| Other h | 203.93 | 263.30 | 777.87 | 1,075.26 | g | 106.13 | 218.88 | 5,767.73 | 7,150.25 | 194.07 | 115.87 | ||||
| Size of place of residence | p=0.51 | p<0.05 | p=0.66 | p<0.05 | p=0.13 | ||||||||||
| Up to 5,000 inhabitants i | 225.11 | 227.89 | 688.89 | 1,178.00 | 139.00 | 351.39 | 5,446,67 | 8,075.07 | 196.33 | 129.03 | |||||
| 5,001 to 20,000 inhabitants j | 256.71 | 352.68 | 764.63 | 998.78 | l | 93.35 | 166.48 | 5,278.29 | 5,911.79 | k, l | 199.76 | 125.89 | |||
| 20,001 to 50,000 inhabitants k | 191.25 | 227.36 | 583.90 | 1,000.03 | 73.42 | 156.57 | 4,247.50 | 5,947.52 | i | 246.21 | 169.26 | ||||
| More than 50,000 inhabitants l | 200.37 | 237.57 | 459.50 | 1,042.73 | i | 112.17 | 222.22 | 3,655.80 | 6,004.34 | i | 259.63 | 183.45 | |||
| In a relationship | p=0.92 | p=0.75 | p=0.21 | p=0.8 | p=0.37 | ||||||||||
| Yes | 212.44 | 263.09 | 593.27 | 1,033.72 | 98.34 | 211.93 | 4,389.59 | 6,197.47 | 234.41 | 163.48 | |||||
| No | 165.00 | 158.03 | 980.00 | 1,697.41 | 0.00 | 0.00 | 8,500.00 | 13,010.50 | 260.00 | 91.65 | |||||
| Current language spoken at home | p=0.78 | p=0.85 | p=0.56 | p=0.87 | p=0.53 | ||||||||||
| Spanish | 211.03 | 263.36 | 599.30 | 1,040.26 | 99.78 | 218.91 | 4,460.32 | 6,319.26 | 236.10 | 164.38 | |||||
| Other (Including bilinguals) | 221.58 | 256.06 | 569.21 | 1,025.60 | 77.50 | 121.57 | 4,070.00 | 5,699.70 | 221.05 | 151.12 | |||||
| Language spoken at home as a child | p=0.45 | p<0.05 | p=0.2 | p=0.07 | p<0.05 | ||||||||||
| Spanish | 211.32 | 266.63 | 564.62 | 1,025.29 | 102.82 | 219.05 | 4,314.52 | 6,283.85 | 239.28 | 164.97 | |||||
| Other (including bilinguals) | 219.31 | 219.62 | 900.83 | 1,118.29 | 46.81 | 99.13 | 5,457.78 | 5,951.16 | 189.58 | 136.31 | |||||
| Country of birth | p=0.84 | p<0.05 | p=0.74 | p=0.08 | p=0.38 | ||||||||||
| Spain | 213.78 | 268.38 | 568.80 | 1,027.84 | 99.88 | 216.43 | 4,309.52 | 6,243.45 | 235.83 | 162.32 | |||||
| Another country | 193.28 | 185.23 | 897.19 | 1,110.96 | 72.19 | 142.81 | 5,655.63 | 6,346.92 | 221.25 | 172.21 | |||||
| Body Mass Index (BMI) | p=0.29 | p=0.75 | p=0.08 | p=0.67 | p=0.15 | ||||||||||
| Underweight | 192.00 | 245.19 | 546.00 | 1,220.89 | 462.00 | 558.68 | 6,984.00 | 10,340.35 | 222.00 | 162.39 | |||||
| Normal weight | 237.91 | 290.53 | 536.35 | 976.92 | 85.21 | 187.09 | 3,923.91 | 5,552.11 | 240.82 | 165.78 | |||||
| Overweight | 188.06 | 234.35 | 598.17 | 1,036.30 | 99.61 | 237.23 | 4,607.93 | 6,479.77 | 245.78 | 165.90 | |||||
| Obesity | 184.10 | 233.09 | 743.46 | 1,176.17 | 99.49 | 173.46 | 5,182.05 | 7,209.59 | 208.46 | 153.80 | |||||
Table 6.
Variability of physical and sedentary behaviour during pregnancy according to obstetric characteristics.
Table 6.
Variability of physical and sedentary behaviour during pregnancy according to obstetric characteristics.
| Variables / Categories | Leisure PA min/week | Work PA min/week | Travel to and from places PA min/week | MET – min/week | Sedentary min./day | ||||||||||
| Mean | SD | Sign. | Mean | SD | Sign. | Mean | SD | Sign. | Mean | SD | Sign. | Mean | SD | Sign. | |
| Gravidity (number of pregnancies including the current one) | p<0.01 | p=0.07 | p=0.64 | p=0.64 | p<0.05 | ||||||||||
| Primigravida | 254.33 | 242.74 | 470.85 | 939.63 | 98.23 | 222.17 | 3,863.18 | 5,482.26 | 251.91 | 160.35 | |||||
| Multigravida | 187.27 | 270.61 | 670.54 | 1,086.39 | 97.19 | 205.09 | 4,749.42 | 6,655.75 | 224.52 | 163.99 | |||||
| Health problems during pregnancies ended in live birth | p=0.13 | p=0.9 | p=0.97 | p=0.43 | p=0.96 | ||||||||||
| No | 199.37 | 300.35 | 621.20 | 1,035.87 | 103.36 | 227.58 | 4,647.42 | 6,571.48 | 227.83 | 170.32 | |||||
| Yes | 123.17 | 198.20 | 580.34 | 997.64 | 96.33 | 197.37 | 3,506.00 | 5,120.43 | 205.50 | 129.04 | |||||
| Pregnancy planning | p=0.34 | p=0.28 | p=0.51 | p=0.51 | p=0.6 | ||||||||||
| No | 195.67 | 243.24 | 646.52 | 1,002.53 | 121.92 | 274.21 | 4,806.36 | 6,271.93 | 213.03 | 125.34 | |||||
| Yes | 217.83 | 268.26 | 580.58 | 1,050.89 | 90.43 | 188.06 | 4,308.81 | 6,265.72 | 241.76 | 172.40 | |||||
| Assisted reproduction pregnancy | p=0.44 | p=0.12 | p=0.77 | p=0.25 | p=0.15 | ||||||||||
| No | 216.10 | 271.69 | 623.72 | 1,098.43 | 88.25 | 186.58 | 4,580.71 | 6,615.44 | 238.72 | 173.25 | |||||
| Yes | 243.19 | 251.74 | 267.50 | 571.08 | 66.67 | 134.27 | 2,309.44 | 2,367.26 | 270.83 | 170.84 | |||||
| High-risk pregnancy consultation | p=0.36 | p=0.68 | p=0.37 | p=0.9 | p=0.42 | ||||||||||
| No | 217.13 | 268.96 | 585.37 | 1,043.02 | 98.13 | 208.48 | 4,378.80 | 6,292.21 | 231.08 | 159.00 | |||||
| Yes | 184.75 | 223.20 | 655.00 | 1,014.05 | 94.58 | 227.66 | 4,653.33 | 6,095.47 | 253.58 | 183.25 | |||||
| Trimester of pregnancy awareness | p=0.47 | p<0.01 | p=0.94 | p<0.01 | p=0.48 | ||||||||||
| First trimester | 212.09 | 262.55 | 569.92 | 1,020.82 | 97.49 | 211.10 | 4,273.58 | 6,154.53 | 235.24 | 163.21 | |||||
| Second trimester | 162.00 | 272.98 | 2,124.00 | 741.37 | 123.00 | 266.73 | 13,836.00 | 6,577.54 | 198.00 | 174.41 | |||||
| Professional health care during pregnancy | p=0.73 | p=0.62 | p=0.39 | p=0.93 | p=0.96 | ||||||||||
| No | 315.00 | 445.48 | 940.00 | 1,329.36 | 420.00 | 593.97 | 10,300.00 | 14,566.40 | 210.00 | 127.28 | |||||
| Yes | 211.53 | 261.92 | 594.50 | 1,037.71 | 95.88 | 208.33 | 4,390.92 | 6,212.02 | 234.74 | 163.28 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



