Submitted:
07 May 2025
Posted:
08 May 2025
You are already at the latest version
Abstract
The study on which this paper is based assessed public knowledge, awareness, and practices regarding air pollution among residents of Hanoi, Vietnam, focusing on its causes, health impacts, and mitigation strategies. It sought to provide evidence-based recommendations for policymaking and public health interventions to address air pol-lution challenges. A cross-sectional survey was conducted with 521 individuals in suburbs around Hanoi. The survey assessed participants' sociodemographic characteristics, knowledge of air pollution, attitudes, and behaviours. Data were analysed statistically using SPSS Statistics for Windows, version 29.0. Nearly all participants (98.3%) were aware of air pollution, with 65.3% attributing it to human activities and 61.2% recognising specific air pollutants as primary contributors. The majority (93.9%) acknowledged health impacts, citing respiratory infections (55.1%) and sinus issues (51.2%) as prevalent con-cerns. Vulnerable groups, such as children under five (82.3%) and adults over 65 years old (77.4%), were identified as disproportionately affected. Social media (68.9%) and television (58.3%) were the dominant sources of information. Despite recognising the importance of air pollution (98.5%), active engagement in environmental organisations was minimal (1.9%), and systemic actions, such as supporting renewable energy markets (1.4%), were underrepresented. Most participants (84.3%) reported personal mitigation efforts, in-cluding energy-saving practices (35.5%) and walking instead of driving a car or bike (35.3%).While awareness of air pollution and its health impacts is high among Hanoi residents, proactive engagement in systemic solutions remains limited. Policymakers should prioritise community-based programs, public-private partnerships, and educa-tional campaigns to bridge gaps between awareness and action. Tailored interventions addressing demographic and cultural factors are essential to foster collective responsibility and long-term change.
Keywords:
Hanoi
; Vietnam
; air pollution
; knowledge
; practice
1. Introduction
Air pollution poses a significant public health challenge in Vietnam, particularly in urban centres like Hanoi, a city of 8.6 million people. The World Health Organization (WHO) attributes over 60,000 deaths annually in Vietnam to air pollution-related diseases, including heart disease, stroke, lung cancer, chronic obstructive pulmonary disease, and pneumonia [1]. This environmental hazard not only shortens life expectancy by approximately 1.4 years but also undermines the country's recent health advancements [2]. The primary contributors to air pollution in Vietnam are rapid urbanisation and industrialisation, leading to increased emissions from transportation, industrial activities, and residential energy use [3]. Hanoi, for instance, experiences elevated levels of fine particulate matter (PM2.5) [4], which can penetrate deep into the lungs and enter the bloodstream, causing respiratory and cardiovascular issues [5,6]. The city's high density of motor vehicles, industrial emissions, and construction activities exacerbate the problem, resulting in air quality that frequently exceeds safe limits [7,8]. In addition, indoor sources of air pollution such as unvented cooking in the home are common to Vietnamese society [9].
Despite the severe health implications, public awareness of air pollution's risks remains limited. Phung et al. highlighted the association between poor air quality and increased hospitalisations for respiratory and cardiovascular conditions in Hanoi and Ho Chi Minh City, underscoring the need for greater public education on this issue [10]. Enhancing community understanding is crucial for fostering behavioural changes and supporting policies aimed at reducing pollution sources. Addressing air pollution effectively requires coordinated efforts from individuals, communities, and government entities [11]. The WHO emphasises the importance of multisectoral collaboration to develop and implement long-term strategies that reduce emissions and promote health [12].
The study on which this paper is based aimed to assess public knowledge, awareness, perceptions, and actions regarding air pollution among residents of Hanoi, Vietnam, focusing on its causes, health impacts, and mitigation strategies. Here, we discuss the findings from the quantitative arm of the study. We also seek to develop evidence-based recommendations for policy development and innovative programs to reduce air pollution and its associated health risks.
2. Materials and Methods
Study Design and Setting
This paper is based on the quantitative arm of the overall study that employed a mixed methods research approach, integrating both quantitative and qualitative data to provide a comprehensive understanding of the research problem. An explanatory sequential design was adopted, where quantitative data collection and analysis were conducted first, followed by qualitative data collection and analysis to elaborate on the quantitative findings [13]. Here, we focus only on the quantitative cross-sectional part of the study.
The study employed a cross-sectional design to obtain quantitative data through a structured questionnaire. The questionnaire included several main sections: knowledge and attitudes about air pollution; risk perception of air pollution and its impact on health; strategies for dealing with air pollution; individuals' prevention and mitigation actions against air pollution; and the need for information and health promotion. The survey was conducted over four consecutive months between September 2022 and January 2023. Prior to data collection, the research team recruited and trained undergraduate students from the College of Health Sciences at VinUniversity for data collection. Each interview lasted approximately 30–45 minutes.
Ethical approval for this study was obtained from the Vinmec International General Hospital Joint Stock Company – VinUniversity Institutional Review Board for Biomedical Research prior to commencement (IRB No.: 95/2022/QD-VMEC; date of approval: 9 September 2022). Written informed consent was obtained from all participants. Data confidentiality and privacy were maintained throughout the study.
Study Participants and Recruitment
The study targeted adult residents of Hanoi, a densely populated urban area heavily impacted by air pollution. Inclusion criteria were residency in Hanoi, willingness to participate, and the ability to complete the survey in Vietnamese. A multistage sampling technique, combining cluster and simple random sampling, was used for participant recruitment. Three central and three suburban districts of Hanoi were randomly selected as clusters. From each district, 250 participants were recruited, aiming for a total sample size of 1,500 participants to allow for a robust analysis. Convenience sampling was then applied within each cluster to actively recruit participants.
A door-to-door approach was employed to identify potential participants, with the first household in each area selected randomly. One individual from each household was invited to participate. As an incentive and gesture of appreciation, participants were offered VND200,000 (US$7.80) for their time and knowledge-sharing.
Survey Development and Data Collection
A structured questionnaire was developed by the research team based on a comprehensive review of relevant literature. The survey was designed to assess knowledge, attitudes, and behaviours related to air pollution, risk perceptions, prevention and mitigation strategies, and sociodemographic factors. The initial version was developed in English and translated into Vietnamese, followed by a back-translation process to ensure accuracy and cultural appropriateness. Content validity was evaluated by a panel of experts from the College of Health Sciences at VinUniversity.
Two rounds of pilot testing were conducted with 20 participants from diverse sociodemographic backgrounds to evaluate the reliability and acceptability of the questionnaire. Adjustments were made based on feedback to finalise the survey instrument.
The survey was administered in person by trained undergraduate research assistants. The survey took approximately 30–45 minutes to complete.
Data Analysis
The statistical analysis was performed using the Statistical Package for Social Science (SPSS) Statistics for Windows, version 29.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation (SD) or median with interquartile range (IQR) according to data normality. Categorical data are presented as frequencies with their percentages. A P-value of less than 0.05 was considered statistically significant.
3. Results
A total of 521 participants provided responses for the survey, with a median age of 26 years (IQR: 21–34). Supplementary Table 1 shows the sociodemographic characteristics of the respondents.
3.1. Environmental Health Issues and Exposure to Air Pollution
Participants were asked to select the top environmental health issues that concerned them. The most selected issue was air pollution (86.6%), followed by littering (60.3%), traffic congestion (34.2%), river and ocean pollution (31.9%), and climate change (17.3%). Other issues selected by fewer participants included poor waste management (13.1%) and overpopulation (4.6%), as shown in Figure 1.
The survey results indicate that most respondents (52.8%) have been exposed to particulate matter (PM) in the past five years. This is significantly higher than for any other air pollutant listed in the survey. The second most common pollutant that respondents have been exposed to is carbon monoxide (CO), with 7.3% of respondents indicating exposure (Figure 2).
3.2. Knowledge of Air Pollution
Almost all participants (98.3%) reported being aware of air pollution. When asked about their understanding of air pollution, most identified it as caused by humans (65.3%) and air pollutants (61.2%), with 63.1% recognising its negative impacts on humans and other living beings. Social media (68.9%) and television (58.3%) were the most frequently cited sources of information. Additionally, 14.0% provided other explanations for air pollution, indicating varied and diverse perspectives on the topic (Table 1).
Scientists were the most trusted source of information regarding air pollution, with 63.5% of participants finding them very trustworthy. Environmental organisations were also highly trusted, with 56.2% of participants indicating them as very trustworthy. The government was the third most trusted source, with 67.8% of participants stating it to be very trustworthy. Family members or friends, and media sources, were the least trusted sources, with only 49.7% and 38.4% of participants, respectively, considering them very trustworthy (Supplementary Table 2).
Overall, 81% of respondents indicated that air pollution is "very important" to them, while 17.5% indicated that it is "important." When asked why air pollution is personally important, the most common response was that it affects their health (93.9%). Additionally, as shown in Table 1, a significant number of respondents indicated that air pollution directly affects themselves (67.2%), their daily activities (58%), their personal well-being or mood (44.1%), animals (31.9%), and the environment (44.5%).
3.3. Awareness of and Practices Regarding Air Pollution
Four in every five respondents (80.6%) believed that many transportation options are a major cause of air pollution. Inefficient modes of transportation, such as motor vehicles, were also identified as a significant cause by 51.1% of respondents. Industrial emissions were identified as a cause by 77.7% of respondents. The survey also found that most respondents (79.1%) considered that air pollution has a personal impact on them, with 78.3% indicating that it also impacts their family and friends. In addition, 67.9% of respondents are aware of other effects of air pollution, as shown in Table 2.
Participants identified various groups as being affected by air pollution, with the highest concern shown for infants and children under 5 years old (82.3%), adults over 65 years old (77.4%), and children aged 5 years and above (69.5%). Other perceived vulnerable groups included outdoor workers (66.4%), adults aged 18-64 years old (45.7%), indoor workers (41.1%), animals (43.8%), and plants (38.8%). A smaller proportion of respondents associated air pollution with impacts on vehicle engines (6.7%) and transportation (6.0%), while 12.1% noted other affected entities. Regarding personal well-being, 97.1% of participants perceived air pollution as affecting them, while 1.2% did not, and 1.3% were uncertain.
Among those who felt affected (n = 506), the most reported health impacts included respiratory infections (55.1%), sinus infections (51.2%), and allergies (42.3%). Other frequently mentioned conditions included asthma (33.8%), itchy eyes (33.6%), lung cancer (32.6%), and blurred vision (26.3%), Table 2.
3.4. Actions to Tackle Air Pollution
The majority of participants (82.1%) believed there are ways to tackle air pollution, while 8.8% disagreed, and 7.9% were unsure. Responsibility for addressing air pollution was attributed to individuals (81.6%), national governments (63.9%), and local governments (51.8%), with smaller proportions pointing to businesses (33.2%), local organisations (34.5%), and international bodies (21.1%).
Most participants (84.3%) reported taking action to mitigate air pollution. Among these, common measures included saving energy (35.5%), walking for errands (35.3%), using public transportation (30.3%), and avoiding burning materials (30.5%). Less frequently mentioned actions included reducing emissions through industrial measures (3.6%) and supporting renewable energy (1.4%).
Regarding local air quality, 44.7% of participants rated it as average, while 24.4% and 15.4% considered it poor or very poor, respectively. Only 14.2% rated it as good, and 1.2% as excellent. Personal vehicle usage was reported by 80.2%, with most driving less than 10 km daily (37.0%) or 10–20 km daily (25.1%). A smaller proportion drove over 20 km (17.3%). Additionally, 64.7% of participants had considered improving air quality in their area, while 34.2% had not. These findings highlight a strong individual engagement with air pollution mitigation, alongside concerns about local air quality (Supplementary Table 3).
3.5. Impact of Sociodemographic Factors on Air Pollution Knowledge and Perception
Awareness of air pollution was slightly higher among females (98.6%) compared to males (98.3%; P = 0.043). Females were more likely to attribute air pollution to many forms of transportation (82.6%) compared to males (77.3%; P = 0.011). Females also recognised the role of industrial emissions more frequently than males (79.7% vs. 75.5%; P = 0.019). Females were more likely to indicate that air pollution currently or potentially impacts them personally (82.2%) compared to males (75.1%; P = 0.075). A significantly greater proportion of females than males reported that air pollution affects their overall health (47.7% vs. 33.6%; P = 0.002). Females recognised the potential negative effects of air pollution on agricultural production (14.6% vs. 12.7%;, P = 0.025) and its toxic effects on wildlife (15.7% vs. 17.0%; P = 0.013) at a slightly higher rate than males. Respiratory infections were the most frequently recognised personal impact, significantly higher in females (60.5%) than males (45.0%; P < 0.001). Females also reported itchy eyes (36.7% vs. 27.9%; P = 0.030), blurry vision (27.8% vs. 22.3%; P = 0.008), and allergies (47.7% vs. 33.6%; P = 0.002) as consequences of air pollution compared to males. Additionally, females were more likely to indicate that air pollution had not affected their family or friends (84.7% vs. 70.7%; P = 0.012), whereas males expressed greater uncertainty about its impact (Table 3).
Regarding the impact of age, participants aged 35–44 years were significantly more likely to recognise air pollution as caused by air pollutants (80.0%) compared to those aged 18–34 years (62.4%) and ≥ 45 years (65.7%; P = 0.042). Those aged ≥ 45 years were most likely to attribute air pollution to human activities (80.0%) compared to other age groups (P = 0.033). Social media was the most reported source of knowledge among those aged 18–34 years (79.5%), but this decreased significantly with age (37.1% among those ≥ 45 years; P < 0.001). Conversely, reliance on radio and newspapers as sources increased with age, with participants ≥ 45 years reporting the highest use of radio (48.6%; P = 0.002) and newspapers (65.7%; P < 0.001). Construction and demolition works were identified as a cause of air pollution more frequently by participants aged 35–44 years (49.1%) than by younger and older groups (P = 0.025). The perception of air pollution reducing the quality of life was significantly more common among participants ≥ 45 years (65.7%) compared to those aged 18–34 years (41.3%; P = 0.008). Finally, lung cancer was reported as a way air pollution affects individuals significantly more among participants ≥ 45 years (60.0%) compared to younger groups (P = 0.005) (Supplementary Table 4).
Participants educated to university undergraduate or postgraduate level were significantly more likely to have heard about air pollution compared to those with up to high school education (100% vs. 95.9%; P = 0.003). Recognising air pollution as damaging to the climate or materials was more common among undergraduate and postgraduate participants (39.8% and 39.3%, respectively) compared to those with up to high school education (23.8%; P = 0.001). University level participants were also more likely to identify the negative impacts of air pollution on humans and other living beings (69.3% and 75.0%, respectively) compared to high school-educated participants (54.4%, P = 0.002). Regarding causes, university participants were more likely to attribute air pollution to inefficient transportation (57.5% vs. 42.5%; P = 0.006) and industrial emissions (80.3% vs. 71.0%; P = 0.019) compared to high school participants. Postgraduate participants were most likely to cite construction and demolition works as a cause (57.1%; P < 0.001). Awareness of other effects of air pollution was higher among university participants (72.0% vs. 60.6%; P = 0.026). For personal impacts, respiratory infections (62.2% vs. 40.4%; P < 0.001), asthma (40.9% vs. 19.7%; P < 0.001), sinus infections (58.3% vs. 34.7%; P < 0.001), and allergies (50.0% vs. 28.0%, P < 0.001) were more frequently reported by university participants compared to those with up to high school education (Supplementary Table 5).
4. Discussion
This Hanoi, Vietnam-based study revealed exceptionally high levels of awareness about air pollution, with 98.3% of respondents acknowledging familiarity with the issue. This aligns with findings from Jeddah, Saudi Arabia [14] and Muscat, Oman [15], where awareness levels were similarly high, reflecting significant public concern about air pollution's health impacts. In contrast, lower awareness levels in regions such as Ireland [16], where only 66% of respondents recognised air pollution's national effects, highlight regional disparities in information dissemination. Similarly, in Malaysia [17], many respondents underestimated the severity of local air pollution, further underscoring the importance of context-specific educational campaigns to address these gaps effectively.
This study revealed that air pollution is overwhelmingly perceived as a critical issue, with 98.5% of participants rating it as "very important" or "important." This strong concern reflects the city's direct and prolonged exposure to urban, industrial, and vehicular emissions. However, this heightened perception of importance has not translated into significant proactive engagement, as evidenced by the low membership of environmental organisations. Similar patterns were observed in Muscat [15], where respondents recognised the criticality of air pollution but showed limited engagement in mitigation efforts. In Jeddah, younger and more educated individuals were more likely to prioritise air pollution, reflecting demographic variations in perceptions of importance [14]. In Malaysia, while air pollution was acknowledged as important during episodic haze events, the general perception of air quality as "good" or "satisfactory" indicated a disconnect between actual pollution levels and public perception [17]. In Ghana, perceptions of air pollution's importance were closely tied to direct exposure and its impacts on health and economic conditions [18], similar to the patterns seen in Hanoi.
Our findings demonstrated high levels of awareness regarding the causes and impacts of air pollution. Most participants identified human activities as the main contributors, while 61.2% directly linked pollution to specific air pollutants. Awareness of health-related consequences was particularly robust, with 93.9% recognising adverse effects and 97.1% reporting personal impacts such as respiratory infections (55.1%), sinus issues (51.2%), and allergies (42.3%). Moreover, participants highlighted the effects on vulnerable populations, including children under five and adults over 65 years. Broader environmental impacts, such as damage to plants and animals, were acknowledged less frequently, reflecting a stronger focus on human health over ecological concerns.
When compared to other studies, a similar awareness of the causes of air pollution was observed in Jeddah [14] and Muscat [15] , where respondents primarily attributed it to vehicular emissions and industrial activities. However, these studies placed less emphasis on family-level impacts or vulnerable groups, adopting a more individualistic perspective. In Malaysia, while episodic events like haze heightened public concern, there was less sustained awareness of family or personal impacts compared to Hanoi [17]. The findings from Ghana align closely with those in Hanoi, as respondents in both regions demonstrated significant concern for the health impacts on family and vulnerable groups [18]. The study by Kim et al. further reinforces that local exposure raises awareness of air pollution causes, although in both Vietnam and Ghana, environmental effects beyond human health received limited attention [19]. These patterns underscore the importance of broadening public discourse to address not only personal and family health impacts but also the broader ecological consequences of air pollution.
Participants in Hanoi have experienced prolonged exposure to pollution driven by rapid urbanisation, industrialisation, and heavy reliance on fossil fuels. The city's significant vehicular density, with over five million registered vehicles, along with coal combustion and industrial emissions, has created persistent air quality challenges [20]. This continuous exposure is reflected in health concerns raised by respondents, including respiratory infections, sinus problems, and allergies. Vulnerable populations, particularly children and the elderly, were acknowledged as disproportionately affected, highlighting the far-reaching health impacts of chronic air pollution exposure. Comparisons with other studies reveal differences in the nature and perception of pollution exposure. In Muscat [15] and Malaysia [17], pollution is episodic, often linked to specific events like construction activities or transboundary haze episodes, which prompt immediate public attention but do not foster sustained concern. Conversely, Jeddah [14] and Ghana [18] face continuous exposure due to urban and industrial activities, contributing to sustained health risks. Unlike Hanoi, where vehicular emissions dominate, Ghana's pollution sources are more varied, including biomass burning and waste disposal practices [18]. Despite prolonged exposure in Hanoi and Vietnam as a whole, as noted by Kim et al. [19], this has yet to translate into strong opposition to systemic causes such as reliance on coal-fired power plants, underscoring the challenges in converting awareness into advocacy.
Our study revealed that while most participants believe in actionable ways to tackle air pollution (82.1%) and reported personal mitigation efforts (84.3%), these actions were predominantly individualistic, such as saving energy, walking, or using public transportation. Systemic measures, such as advocating for renewable energy or industrial emission reductions, were far less common, with limited emphasis placed on the role of businesses and international organisations. Similar trends were observed in other studies, including Jeddah [14], Muscat [15], and Malaysia [17], where personal actions outweighed collective or institutional efforts. However, Ghana presented a notable exception, demonstrating greater engagement with community-based and institutional initiatives, indicating the importance of cultural and systemic support for collective action [18].
The present study reveals significant differences in air pollution awareness, perceptions, and reported impacts across gender, age, and educational levels. For instance, female participants exhibited slightly higher awareness of air pollution than males. Similarly, in Jeddah, Muscat, and California, USA, females exhibited higher awareness levels than males, suggesting the influence of gender in shaping perceptions [14,15,21]. Females were more likely to attribute air pollution to transportation and industrial emissions, reflecting greater recognition of major urban pollution sources. Tailored public health campaigns should address these gender-specific perceptions and vulnerabilities, focusing on reducing exposure and improving access to healthcare for pollution-related conditions.
Our findings also demonstrate age-related differences in the attribution of causes and the recognition of the health impacts of air pollution. Participants aged 35–44 years were more likely to associate air pollution with specific pollutants, while those ≥ 45 years attributed it to human activities, potentially reflecting cumulative life experience and awareness of anthropogenic environmental damage. Younger participants predominantly used social media for information, while reliance on traditional media such as radio and newspapers increased with age. These insights suggest that age-targeted communication strategies are essential. For instance, younger audiences may benefit from digital campaigns, while older populations may prefer traditional media outlets.
Our results also noted that educational attainment significantly influenced air pollution awareness and perceived impacts. Participants with higher education levels were more likely to identify specific causes, such as inefficient transportation and industrial emissions, and to recognise their broader effects on the climate and health. Other studies reported that individuals in higher-skilled occupations exhibited significantly more positive attitudes towards environmental concerns compared to those in lower-skilled roles [22,23,24]. It was also noted that a country's income level and the willingness of individuals to pay to save the environment are strongly correlated with awareness of air pollution [22,25]. These variations point to the need for tailored educational interventions that consider cultural and demographic contexts.
The present study has some limitations that should be considered. It relied on self-reported data, which may introduce bias as participants might overestimate their awareness or actions due to social desirability effects. Additionally, the cross-sectional nature of the study limits the ability to establish causal relationships between awareness, actions, and policy effectiveness. The focus on urban residents in Hanoi may not fully capture perceptions and behaviours in rural areas or other regions in Vietnam. Furthermore, while individual and community actions were well-documented, the study did not investigate deeply the structural and institutional barriers that limit systemic engagement.
Future research should focus on conducting longitudinal studies to evaluate the long-term effectiveness of public health campaigns and policy interventions in changing awareness, attitudes, and behaviours. Expanding research to include comparative studies between rural and urban populations in Vietnam and across similar socio-economic contexts globally would provide a broader understanding of regional differences. Investigating behavioural barriers to systemic engagement and designing interventions to encourage collective action, particularly in areas with low participation rates, would address critical gaps identified in this study.
5. Conclusions
This study highlights high levels of awareness and concern about air pollution among Hanoi residents, coupled with significant gaps in proactive engagement and systemic action. While personal measures to mitigate air pollution are prevalent, broader participation in institutional and community-level initiatives remains limited. These findings underscore the urgent need for tailored policies, robust public education, and enhanced community engagement to address the multifaceted challenges of air pollution. Policymakers, in collaboration with stakeholders, must prioritise integrated strategies that align individual, community, and institutional efforts to combat air pollution effectively. Future research should focus on overcoming barriers to systemic action, leveraging technological innovations, and developing holistic solutions to protect public health and the environment.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary Tables S1–S5.
Author Contributions
Conceptualisation, Data curation, Formal analysis, Validation: LV, AE, DK PL, AWT-R; Funding acquisition, Methodology, Project administration, Resources, Supervision: PL, AWT-R, LV, OTKN; Data collection: KVNH, HXH, MPH, MGT, PHN, TNHP; Writing – original draft: LV, AE, DK, PL, AWT-R; Writing – review & editing: LV, PL, AWT-R. All authors reviewed and approved the final draft before submission.
Funding
This study was supported by a VinUniversity research seed grant ‘Air Hanoi Project: public knowledge, awareness and perceptions of air pollution in Vietnam’s capital city – a mixed methods study’.
Institutional Review Board Statement
All study’s procedures run in line with the principles of the latest version of the Declaration of Helsinki and applicable local laws. Ethical approval for this study was obtained from the Vinmec International General Hospital Joint Stock Company – VinUniversity Institutional Review Board for Biomedical Research prior to commencement (IRB No.: 95/2022/QD-VMEC; date of approval: 9 September 2022). Informed consent was obtained from all participants. Data confidentiality and privacy were maintained throughout the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all participants in this study.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- World Health Organization. More than 60 000 deaths in Viet Nam each year linked to air pollution. 2018.Available: Available online: https://www.who.int/vietnam/news/detail/02-05-2018-more-than-60-000-deaths-in-viet-nam-each-year-linked-to-air-pollution#:~:text=New data from the World Health Organization %28WHO%29,a basic requirement for human health and well-being.
- United Nations Children’s Fund. Viet Nam’s heavy air pollution needs stronger action. 2024.Available: https://www.undp.org/vietnam/blog/viet-nams-heavy-air-pollution-needs-stronger-action.
- Vo DH, Ho CM, Vo AT. Do Urbanization and Industrialization Deteriorate Environmental Quality? Empirical Evidence from Vietnam. Sage Open. 2024;14(2). [CrossRef]
- Dominutti PA, Mari X, Jaffrezo J-L, Dinh VTN, Chifflet S, Guigue C, et al. Disentangling fine particles (PM2.5) composition in Hanoi, Vietnam: Emission sources and oxidative potential. Sci Total Environ. 2024;923:171466. [CrossRef]
- Chen J, Rodopoulou S, de Hoogh K, Strak M, Andersen ZJ, Atkinson R, et al. Long-Term Exposure to Fine Particle Elemental Components and Natural and Cause-Specific Mortality—a Pooled Analysis of Eight European Cohorts within the ELAPSE Project. Environ Health Perspect. 2021;129. [CrossRef]
- Chen J, Hoek G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environ Int. 2020;143:105974. [CrossRef]
- Hien PD, Men NT, Tan PM, Hangartner M. Impact of urban expansion on the air pollution landscape: A case study of Hanoi, Vietnam. Sci Total Environ. 2020;702:134635. [CrossRef]
- Ly B-T, Matsumi Y, Nakayama T, Sakamoto Y, Kajii Y, Nghiem T-D. Characterizing PM2.5 in Hanoi with New High Temporal Resolution Sensor. Aerosol Air Qual Res. 2018;18:2487–97. [CrossRef]
- World Health Organization. 2025. Air pollution in Viet Nam. Available: https://www.who.int/vietnam/health-topics/air-pollution.
- Phung D, Hien TT, Linh HN, Luong LMT, Morawska L, Chu C, et al. Air pollution and risk of respiratory and cardiovascular hospitalizations in the most populous city in Vietnam. Sci Total Environ. 2016;557–558:322–30. [CrossRef]
- Ward F, Lowther-Payne HJ, Halliday EC, Dooley K, Joseph N, Livesey R, et al. Engaging communities in addressing air quality: a scoping review. Environ Health. 2022;21:89. [CrossRef]
- World Health Organization. Working together for equity and healthier populations: sustainable multisectoral collaboration based on health in all policies approaches. 2023. Available: https://www.who.int/publications/i/item/9789240067530.
- Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research. Organizational Research Methods. 2018. Available: https://login.proxy.libraries.rutgers.edu/login?url=http://search.ebscohost.com.proxy.libraries.rutgers.edu/login.aspx?direct=true&db=buh&AN=44386156&site=ehost-live.
- Alahmadi NA, Alzahrani R, Bshnaq AG, Alkhathlan MA, Alyasi AA, Alahmadi AM, et al. General Public Knowledge, Attitude, and Practice Regarding the Impact of Air Pollution and Cardiopulmonary Diseases in Jeddah, Saudi Arabia. Cureus. 2023;15(11):e48976. [CrossRef]
- Al-Shidi HK, Ambusaidi AK, Sulaiman H. Public awareness, perceptions and attitudes on air pollution and its health effects in Muscat, Oman. J Air Waste Manage Assoc. 2021;71:1159–74. [CrossRef]
- Quintyne KI, Kelly C. Knowledge, attitudes, and perception of air pollution in Ireland. Public Heal Pract. 2023;6:100406. [CrossRef]
- Chin YSJ, De Pretto L, Thuppil V, Ashfold MJ. Public awareness and support for environmental protection-A focus on air pollution in peninsular Malaysia. PLoS One. 2019;14:1–21. [CrossRef]
- Odonkor ST, Mahami T. Knowledge, Attitudes, and Perceptions of Air Pollution in Accra, Ghana: A Critical Survey. J Environ Public Health. 2020;2020. [CrossRef]
- Kim SE, Harish SP, Kennedy R, Jin X, Urpelainen J. Environmental Degradation and Public Opinion: The Case of Air Pollution in Vietnam. J Environ Dev. 2020;29:196–222. [CrossRef]
- General Statistics Office of Vietnam. Statistical Yearbook of Vietnam 2023. Statistical Publishing House Hanoi, Vietnam; 2024.Available: https://www.gso.gov.vn/en/default/2024/07/statistical-yearbook-of-2023/.
- Cisneros R, Brown P, Cameron L, Gaab E, Gonzalez M, Ramondt S, et al. Understanding public views about air quality and air pollution sources in the San Joaquin Valley, California. J Environ Public Health. 2017;2017:4535142. [CrossRef]
- Pampel FC. The Varied Influence of SES on Environmental Concern. Soc Sci Q. 2014;95:57–75. [CrossRef]
- Manstead ASR. The psychology of social class: How socioeconomic status impacts thought, feelings, and behaviour. Br J Soc Psychol. 2018;57:267–91. [CrossRef]
- Unni B, Tang N, Cheng YM, Gan D, Aik J. Community knowledge, attitude and behaviour towards indoor air quality: A national cross-sectional study in Singapore. Environ Sci Policy. 2022;136:348–56. [CrossRef]
- Lin Y, Wijedasa LS, Chisholm RA. Singapore’s willingness to pay for mitigation of transboundary forest-fire haze from Indonesia. Environ Res Lett. 2017;12:24017. [CrossRef]
Figure 1.
Top environmental health issues of participants.
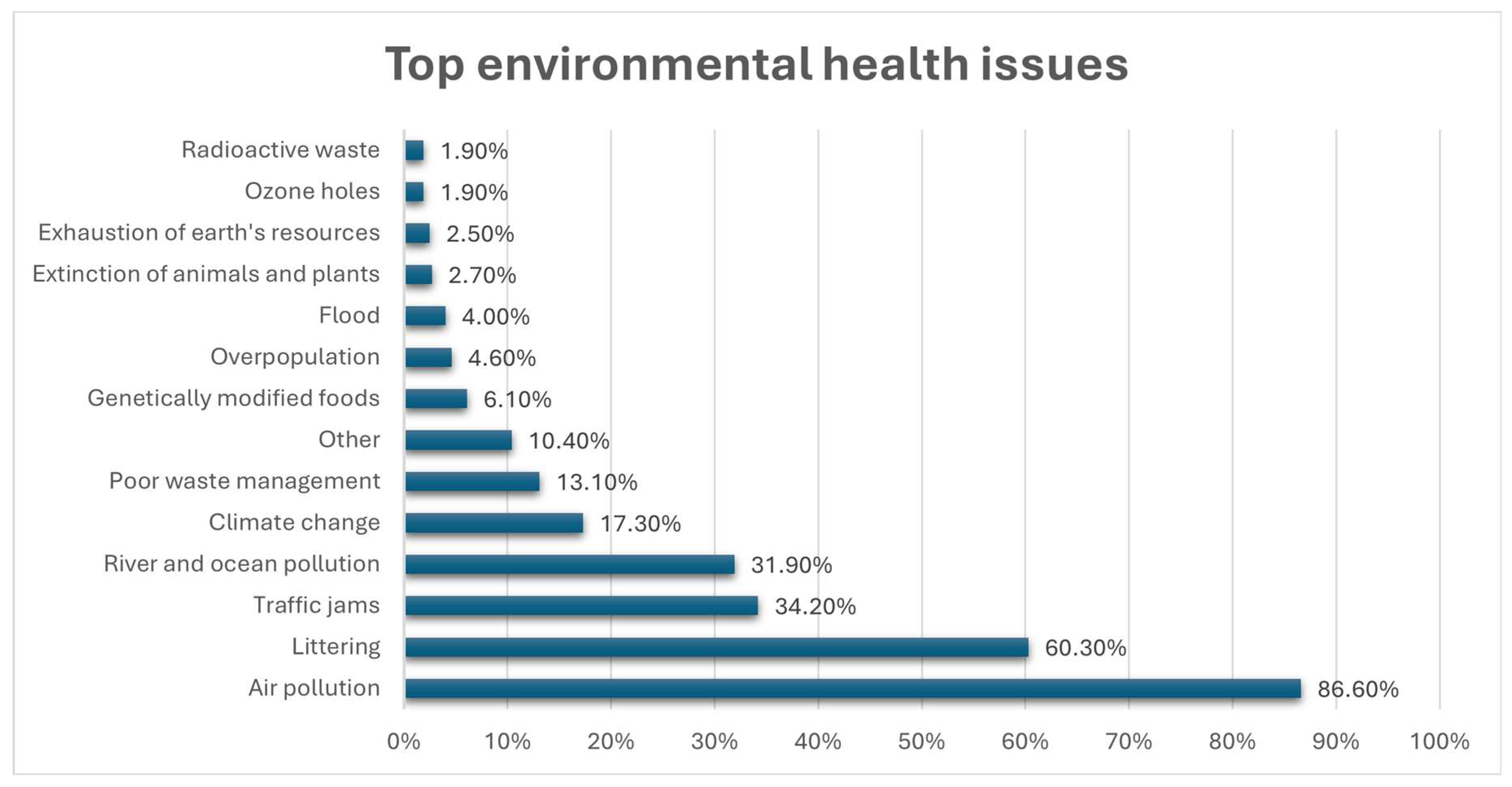
Figure 2.
History of exposure to air pollution among participants.
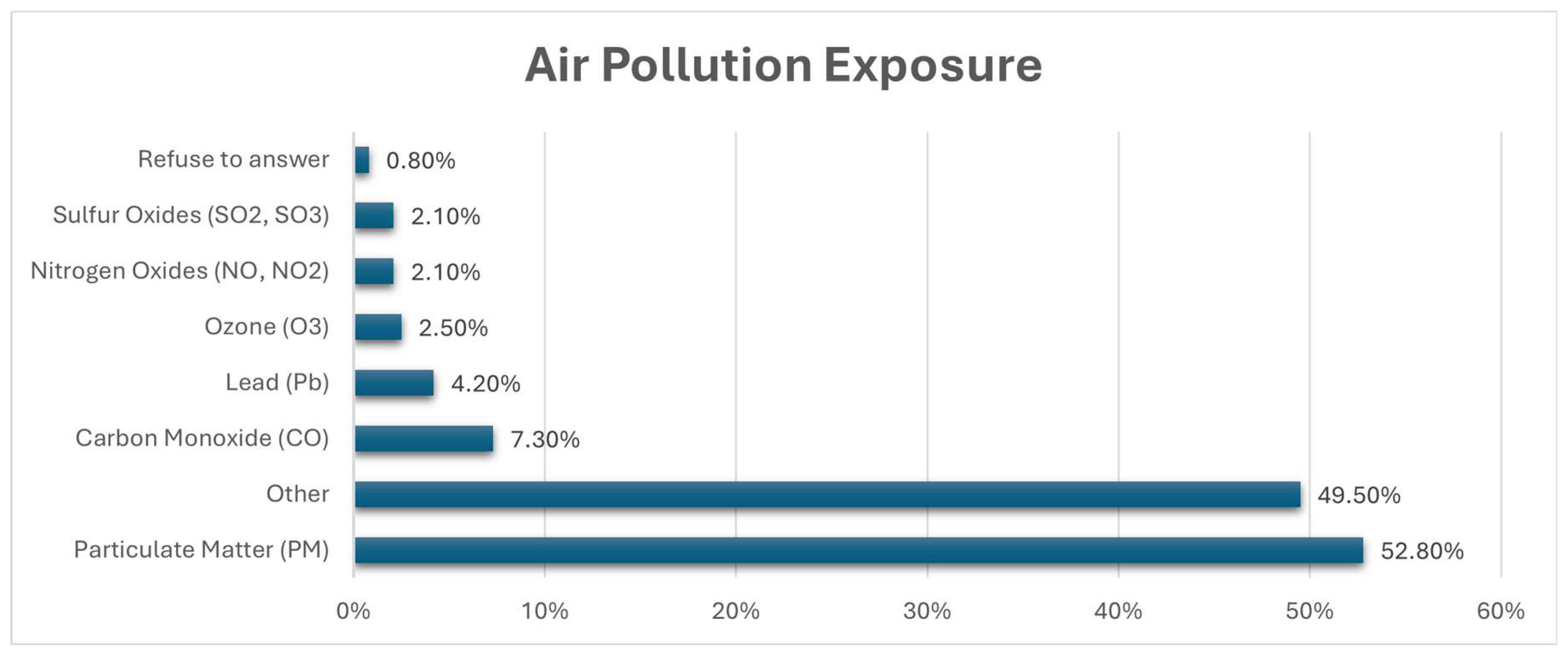

Table 1.
Knowledge of air pollution among participants.
| Variable, No. (%)# | Response (n = 521) |
|---|---|
| Have you heard of air pollution? | |
| Yes | 512 (98.3%) |
| No | 9 (1.7%) |
| What do you know about air pollution? | |
| Natural phenomenon | 56 (10.7%) |
| Relevant to the environment | 169 (32.4%) |
| Not a big problem | 6 (1.2%) |
| Caused by air pollutants | 319 (61.2%) |
| Caused by animals | 25 (4.8%) |
| Caused by humans | 340 (65.3%) |
| Benefits the climate and/or environment | 6 (1.2%) |
| Damages the climate and/or environment | 165 (31.7%) |
| Has positive impacts on humans and other living beings | 10 (1.9%) |
| Has negative impacts on humans and other living beings | 329 (63.1%) |
| Other | 73 (14.0%) |
| Source of knowledge | |
| Government agency information | 37 (7.1%) |
| Local government internet | 53 (10.2%) |
| Social media | 359 (68.9%) |
| Television | 304 (58.3%) |
| Radio | 151 (29.0%) |
| Newspaper(s) | 254 (48.8%) |
| Specialised/academic magazine(s), school/college/university | 39 (7.5%) |
| Public library | 12 (2.3%) |
| Environmental group(s) | 19 (3.6%) |
| Energy provider | 3 (0.6%) |
| Friends/family | 50 (9.6%) |
| Other | 60 (11.5%) |
| How important is the issue of air pollution to you personally? | |
| Not important at all | 1 (0.2%) |
| Not very important | 6 (1.2%) |
| Important | 91 (17.5%) |
| Very important | 422 (81.0%) |
| Refuse to answer | 1 (0.2%) |
| Why is air pollution important to you?# | |
| Directly affects you personally (e.g., work, lifestyle) | 350 (67.2%) |
| Affects health | 489 (93.9%) |
| Affects daily activities | 302 (58.0%) |
| Affects personal well-being/mood | 230 (44.1%) |
| Affects animals | 166 (31.9%) |
| Affects the environment | 232 (44.5%) |
| Other | 18 (3.5%) |
#participants may select more than one answer to each question.
Table 2.
Awareness and practice of air pollution among participants.
| Variable, No. (%)# | Response (n = 521) |
|---|---|
| Causes of air pollution | |
| Many modes of transportation | 420 (80.6%) |
| Inefficient modes of transportation (motor vehicles) | 266 (51.1%) |
| Inefficient burning of fuel by households for cooking, lighting, and heating | 84 (16.1%) |
| Outdoor burning of fossil fuels | 60 (11.5%) |
| Industrial emissions | 405 (77.7%) |
| Indoor air pollution (use of toxic products: incense, cooking by wood) | 73 (14.0%) |
| Wildfires | 103 (19.8%) |
| Open burning of garbage waste | 293 (56.2%) |
| Construction and demolition work | 155 (29.8%) |
| Agriculture activities | 69 (13.2%) |
| Use of chemical and synthetic products | 83 (15.9%) |
| Other | 83 (15.9%) |
| Personal impact of air pollution | |
| Yes | 412 (79.1%) |
| No | 76 (14.6%) |
| Do not know | 33 (6.3%) |
| Refuse to answer | 0 (0.0%) |
| Impact on family/friends | |
| Yes | 408 (78.3%) |
| No | 73 (14.0%) |
| Do not know | 38 (7.3%) |
| Refuse to answer | 2 (0.4%) |
| Awareness of other effects of air pollution | |
| Yes | 354 (67.9%) |
| No | 63 (12.1%) |
| Do not know | 99 (19.0%) |
| Refuse to answer | 5 (1.0%) |
| Other effects of air pollution (if aware) | (n = 354) |
| Reduced agricultural production | 72 (20.3%) |
| Toxic to wildlife | 83 (23.4%) |
| Toxic to livestock/domesticated animals | 87 (24.6%) |
| Birth defects | 43 (12.1%) |
| Vulnerability to stresses | 118 (33.3%) |
| Vulnerability to diseases | 178 (50.3%) |
| Reduced quality of life | 237 (66.9%) |
| Affected by air pollution | |
| Infants/children under 5 years old | 429 (82.3%) |
| Children 5 years old and above | 362 (69.5%) |
| Adults (18 – 64 years old) | 238 (45.7%) |
| Adults over 65 years old | 403 (77.4%) |
| Outdoor workers | 346 (66.4%) |
| Indoor workers | 214 (41.1%) |
| Animals | 228 (43.8%) |
| Plants | 202 (38.8%) |
| Industrial Engines | 35 (6.7%) |
| Transportation | 31 (6.0%) |
| Other | 63 (12.1%) |
| Refuse to answer | 1 (0.2%) |
| Perception of air pollution's effects on yourself | |
| Yes | 506 (97.1%) |
| No | 6 (1.2%) |
| Do not know | 7 (1.3%) |
| Refuse to answer | 2 (0.4%) |
| Ways air pollution affects yourself | (n = 506) |
| Itchy eyes | 170 (33.6%) |
| Blurred vision | 133 (26.3%) |
| Respiratory infections | 279 (55.1%) |
| Emphysema | 67 (13.2%) |
| Asthma | 171 (33.8%) |
| Chronic obstructive pulmonary disease | 89 (17.6%) |
| Heart disease | 41 (8.1%) |
| Lung cancer | 165 (32.6%) |
| Sinus infections | 259 (51.2%) |
| Allergies | 214 (42.3%) |
| Other | 91 (18.0%) |
#participants may select more than one answer to each question.
Table 3.
Impact of gender on knowledge and perception of air pollution.
| Variable, No. (%)# | Female (n = 281) | Male (n = 229) | P-value |
|---|---|---|---|
| Have you heard about air pollution? | |||
| Yes | 277 (98.6%) | 225 (98.3%) | 0.043 |
| No | 4 (1.4%) | 4 (1.7%) | |
| What do you know about air pollution? | |||
| Natural phenomenon | 27 (9.6%) | 27 (11.8%) | 0.218 |
| Relevant to the environment | 101 (35.9%) | 66 (28.8%) | 0.264 |
| Not a big problem | 5 (1.8%) | 1 (0.4%) | 0.546 |
| Caused by air pollutants | 168 (59.8%) | 146 (63.8%) | 0.546 |
| Caused by animals | 14 (5.0%) | 11 (4.8%) | 0.902 |
| Caused by humans | 190 (67.6%) | 145 (63.3%) | 0.133 |
| Benefit to the climate and/or materials | 6 (2.1%) | 0 (0.0%) | 0.159 |
| Damage to the climate or to materials | 87 (31.0%) | 74 (32.3%) | 0.460 |
| Has positive impacts on humans and other beings | 7 (2.5%) | 3 (1.3%) | 0.764 |
| Has negative impacts on humans and other beings | 178 (63.3%) | 144 (62.9%) | 0.785 |
| Other | 32 (11.4%) | 39 (17.0%) | 0.111 |
| Source of knowledge | |||
| Government agency/information | 13 (4.6%) | 23 (10.0%) | 0.078 |
| Local government Internet | 23 (8.2%) | 29 (12.7%) | 0.306 |
| Social media | 196 (69.8%) | 157 (68.6%) | 0.268 |
| Television | 162 (57.7%) | 135 (58.9%) | 0.747 |
| Radio | 76 (27.0%) | 73 (31.9%) | 0.555 |
| Newspaper | 141 (50.2%) | 111 (48.5%) | 0.225 |
| Specialized/academic magazines, school/college/university | 19 (6.8%) | 19 (8.3%) | 0.563 |
| Public library | 8 (2.8%) | 4 (1.7%) | 0.815 |
| Environmental groups | 11 (3.9%) | 7 (3.1%) | 0.338 |
| Energy providers | 0 (0.0%) | 3 (1.3%) | 0.278 |
| Family/friends/ | 28 (10.0%) | 21 (9.2%) | 0.809 |
| Other | 34 (12.1%) | 25 (10.9%) | 0.806 |
| How important is the issue of air pollution to you personally? | |||
| Important | 44 (15.7%) | 46 (20.1%) | 0.963 |
| Very important | 231 (82.2%) | 181 (79.0%) | |
| Why is air pollution important to you? | |||
| Directly affects you personally | 189 (67.3%) | 152 (66.4%) | 0.473 |
| Affects health | 264 (94.0%) | 215 (93.9%) | 0.559 |
| Affects daily activities | 162 (57.7%) | 132 (57.6%) | 0.284 |
| Affects personal well-being/mood | 136 (48.4%) | 90 (39.3%) | 0.086 |
| Affects animals | 90 (32.0%) | 74 (32.3%) | 0.804 |
| Affects the environment | 128 (45.6%) | 100 (43.7%) | 0.911 |
| Other | 9 (3.2%) | 9 (3.9%) | 0.896 |
| Causes of air pollution | |||
| Many transportations | 232 (82.6%) | 177 (77.3%) | 0.176 |
| Inefficient modes of transportation | 146 (51.9%) | 114 (49.8%) | 0.940 |
| Inefficient burning of fuel in households | 43 (15.3%) | 39 (17.0%) | 0.953 |
| Burning of fossil fuels | 29 (10.3%) | 30 (13.1%) | 0.623 |
| Industrial emission | 224 (79.7%) | 173 (75.5%) | 0.515 |
| Indoor air pollution | 45 (16.0%) | 27 (11.8%) | 0.436 |
| Wildfires | 51 (18.1%) | 51 (22.3%) | 0.451 |
| Open burning of garbage waste | 168 (59.8%) | 118 (51.5%) | 0.192 |
| Construction and demolition works | 80 (28.5%) | 72 (31.4%) | 0.735 |
| Agriculture activities | 38 (13.5%) | 30 (13.1%) | 0.838 |
| Use of chemical and synthetic products | 47 (16.7%) | 34 (14.8%) | 0.451 |
| Other | 40 (14.2%) | 39 (17.0%) | 0.228 |
| Personal impact of air pollution | |||
| Yes | 231 (82.2%) | 172 (75.1%) | 0.075 |
| No | 40 (14.2%) | 36 (15.7%) | |
| Do not know | 10 (3.6%) | 21 (9.2%) | |
| Impact on family/friends | |||
| Yes | 1 (0.4%) | 0 (0.0%) | 0.012 |
| No | 238 (84.7%) | 162 (70.7%) | |
| Do not know | 27 (9.6%) | 46 (20.1%) | |
| Awareness of other effects of air pollution | |||
| Yes | 192 (68.3%) | 153 (66.8%) | 0.980 |
| No | 33 (11.7%) | 29 (12.7%) | |
| Do not know | 52 (18.5%) | 46 (20.1%) | |
| Other effects of air pollution (if aware) | (n = 354) | ||
| Reduce agricultural production | 41 (14.6%) | 29 (12.7%) | 0.237 |
| Toxic to wildlife | 44 (15.7%) | 39 (17.0%) | 0.511 |
| Toxic to livestock/domesticated animals | 46 (16.4%) | 41 (17.9%) | 0.481 |
| Birth defects | 23 (8.2%) | 20 (8.7%) | 0.786 |
| Vulnerability to stresses | 71 (25.3%) | 47 (20.5%) | 0.178 |
| Vulnerability to diseases | 94 (33.5%) | 82 (35.8%) | 0.659 |
| Reduce the quality of life | 130 (46.3%) | 101 (44.1%) | 0.391 |
| Other | 48 (17.1%) | 39 (17.0%) | 0.135 |
| Perception of air pollution's effects on self | |||
| Yes | 0 (0.0%) | 1 (0.4%) | 0.795 |
| No | 277 (98.6%) | 218 (95.2%) | |
| Do not know | 3 (1.1%) | 3 (1.3%) | |
| Ways air pollution affects self | (n = 506) | ||
| Itchy eyes | 103 (36.7%) | 64 (27.9%) | 0.030 |
| Blurry vision | 78 (27.8%) | 51 (22.3%) | 0.008 |
| Respiratory infections | 170 (60.5%) | 103 (45.0%) | <0.001 |
| Emphysema | 41 (14.6%) | 25 (10.9%) | 0.451 |
| Asthma | 89 (31.7%) | 78 (34.1%) | 0.438 |
| Chronic obstructive pulmonary disease (COPD) | 51 (18.1%) | 36 (15.7%) | 0.906 |
| Heart disease | 23 (8.2%) | 17 (7.4%) | 0.653 |
| Lung cancer | 94 (33.5%) | 68 (29.7%) | 0.657 |
| Sinus infections | 147 (52.3%) | 109 (47.6%) | 0.063 |
| Allergies | 134 (47.7%) | 77 (33.6%) | 0.002 |
| Other | 48 (17.1%) | 41 (17.9%) | 0.53 |
#participants may select more than one response to each question.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



