
Submitted:
06 May 2025
Posted:
07 May 2025
You are already at the latest version
Abstract
Background and Clinical Significance: Herein we describe the clinical case of a 17-year-old patient with psychotic disorder due to primary thrombophilia, which was re-lated to protein S deficiency and P.ALA22VAL variant MTHFR gene mutation. Case presentation: A 17-year-old female, with no history of previous illnesses, was admitted to the emergency service due to a psychotic break. Psychiatric evaluation detected disor-ganized thought, euphoria, ideas that were fleeting and loosely associated, psychomotor excitement, and deviant judgment. On the fifth day, an inflammatory process in the pa-rotid gland was detected, pointing out a probable viral meningoencephalitis. An antiviral and antimicrobial treatment was immediately given. One week after antiviral and steroi-dal anti-inflammatory treatments, the symptoms improvement was minimal, leading to a presumptive diagnosis of an encephalopathic syndrome. Given the suspicion of a vascu-lar event, a venous MRI was performed, showing a filling defect in the transverse sinus; consequently, anticoagulation treatment with enoxaparin was initiated. The patient´s be-havior improved, revealing that the encephalopathic symptoms were secondary to thrombosis of the venous sinus. Hematological studies were performed to rule out prima-ry coagulopathy and primary thrombophilia; these studies demonstrated a MTHFR mu-tation variant P.ALA22VAL and a 35% decrease in plasmatic Protein S. Conclusion, this case highlights the feasible relationship between psychiatric and hematological disorders, underlining the importance of the MTHFR mutation and protein S deficiency in the de-velopment and progression of psychotic disorders. Early detection of these factors is es-sential for comprehensive management in patients with onset of atypical psychiatric illnesses.
Keywords:
Bipolar disorder
; primary thrombophilia
; MTHFR
; protein S
1. Introduction
Thrombophilia is a multifactorial blood alteration characterized by a predisposition to develop thrombosis in veins and/or arteries, originated by genetic, environmental and acquired conditions that determine its clinical expression [1]. It has been classified in two types: primary or inherited and secondary. Among the most common causes of primary thrombophilia, mutations in the methylenetetrahydrofolate reductases (MTHFR) enzyme, protein S (PS) and protein C (PC) deficiency, presence of lupus anticoagulant/antiphospholipid syndrome, mutation that increase risk of formation coagulant or Factor V Leiden (FVL) and mutations of the prothrombin gene have been reported [2]. MTHFR deficiency is a rare disorder of the folate and sulfide-containing amino acid metabolism, characterized by low plasma folate levels, hyperhomocysteinemia, hypomethioninemia, and lack of methylmalonic aciduria. Clinically, it occurs during the neonatal period or in childhood, it rarely occurs in adolescence or adulthood and may present neurological symptoms such as encephalopathy, psychomotor retardation, gait disturbances and epilepsy, these symptoms and clinical changes that may be associated with thrombotic events [3]. On the other hand, PS is a multifunctional protein that acts in blood coagulation, inflammation and other cellular processes. Its plasma concentration is about 350 nM, 60% of which is bound to complement protein 4 (C4BP) and the other 40% is free, and both forms perform anticoagulant functions [4]. PS deficiency in the newborn can cause severe thrombosis and alterations in the development of the vascular system with fatal consequences. In this sense, the anticoagulant effects of PC (or PS) are exercised through its qualities as a cofactor of activated PC (APC), cofactor of the tissue factor pathway inhibitor (TFPI) and its inhibition of the factor IXa function [4]. Besides, the mutations in the MTHFR gene and protein S deficiency in cases of severe mental disorders have been reported; these mutations can originate neurometabolic diseases. Conceivably, an alteration in a metabolic process might lead to the deficiency of an essential product or the accumulation of some harmful substance inducing a significant impact on the different systems involved, and this circumstance can manifest itself acutely with a myriad of symptoms, such as digestive and respiratory disorders, neurological deterioration, psychiatric symptoms or behavioral alterations. However, the identification of neuropsychiatric disorders related to a metabolic background, especially in pediatric patients, remains difficult, even though the joint presentation with other alterations can guide the diagnosis [5]. In this sense, a psychotic disorder is characterized by a distorted sense of reality, along with disruptions in thinking, perception, and behavior, and/or hallucinations that occur in various neuropsychiatric and medical conditions [6,7]. It has been reported that expression of MTHFR gene polymorphisms may be a risk factor for psychotic disorder, bipolar disorder and schizophrenia, particularly the C/T transition at nucleotide 677 in the exon 4, which produces the amino acid substitution from alanine to valine (Al222Val). In homozygotes with the C677T polymorphism, only 30% of the MTHFR enzymatic activity remains, while in heterozygotes, 65% of its activity is retained [6,8]. Moreover, the MTHFR gene is linked with other at-risk genes, such as the Val66Met mutation of the brain derived neurotrophic factor (BDNF), that can interact in patients with a first psychotic episode, as seen in the effects of the hippocampal volume [9]. On the other hand, PS deficiency has been also found in patients with psychiatric disorders. A study comparing 70 schizophrenic patients against 98 controls, showed a deficiency of free protein S in 22% of the patients, but was not detected in any control [8]. Furthermore, free PS deficiency is associated with a 145-fold increase in the risk of having a first-degree relative with schizophrenia [8]. The present paper seeks to illustrate how genetic mutations linked to primary thrombophilia and decreased plasma PS concentrations may contribute to the development of psychotic disorder in a 17-year-old patient, in order to identify specific therapeutic targets for a more precise approach and to broaden the knowledge about metabolic-related psychiatric illnesses.
2. Case Presentation
The Materials ad A 17-year-old female was admitted to the emergency room due to a psychotic outbreak less than 48 hours after onset. She had had no previous psychiatric events, was conscious but disoriented, showed nonsensical speech, had fleeting and megalomaniacal ideas, loose associations due to consonance, divagated judgment and psychomotor agitation. Laboratory blood studies were normal, and cytochemical and cytological analysis of cerebrospinal fluid (CSF), magnetic resonance imaging with gadolinium contrast of the brain, and an electroencephalogram were requested. The initial diagnosis was psychosis with suspected autoimmune encephalitis. Lorazepam 2 mg IV every 6 hours and olanzapine 10 mg/day IM were the initial treatment. The patient was evaluated by the personnel of the psychiatry and neurology departments, and, on the fifth day, she continued with the same psychotic pattern, without showing signs of a systemic inflammatory response, but with notable inflammation in the left parotid gland (Figure 1); a viral panel was requested, and a positive cytomegalovirus result was obtained (Table 1).
Antiviral treatment was started with ganciclovir 5 mg/kg IV every 12 hours, dexamethasone IV, 8 mg every 8 hours; dexmedetomidine in 0.9% saline titrate 0.5 to 1 mcg/kg/hour IV and, in case of agitation, olanzapine 5 mg every 12 hours IV. The cytological and cytochemical CSF studies were within normal limits, while the electroencephalogram (EEG) showed neuronal activity related with encephalopathy without epileptic activity. One week after treatment initiation, the patient did not show significant improvement. A venous magnetic resonance imaging (MRI) was requested, and a filling defect in the transverse sinus was revealed, suggesting venous thrombosis of the transverse sinus (Figure 1), so anticoagulant therapy was started with enoxaparin 1 mg/kg/IV (60 mg). At this time, a history of a maternal grandmother with coagulopathy was documented. On the ninth day of admission, an improvement in behavior and neuropsychiatric symptoms secondary to the treatment of venous sinus thrombosis of undetermined origin began to be observed. On physical examination, confusion, disinhibition, and inattention persisted, with no signs of psychomotor excitement or catatonia, although with fluctuations in alertness.
Hematological studies were requested to rule out primary thrombophilia, as well as a panel of mutations, quantification of anticoagulant proteins (protein C, protein S and anti-thrombin), mutation 677c7 of the MTHFR gene, mutation of the prothrombin gene 20210a and factor V Leiden mutation. The anticoagulant treatment was changed, and rivaroxaban 20 mg/day, orally, was given.
Finally psychotic disorder and primary thrombophilia due to MTHFR and PS deficiency were diagnosed (Table 2 and Table 3). Laboratory findings revealed the presence of the MTHFR variant P.ALA222VAL mutation without reference value, as well as a decrease levels in PS to 35% its normal value (Reference Value, 54.0 – 103.0%). Taken together, these findings supported the diagnosis: psychotic disorder attributed to venous thrombosis of the transverse sinus secondary to primary thrombophilia due to PS deficiency.
The patient was discharged with the following therapeutic regimen: haloperidol 10 mg/day, magnesium valproate 200 mg every 8 hours, rivaroxaban 20 mg/day, biperiden 2 mg every 8 hours, esomeprazole 40 mg/day; the whole medication had to be orally administered.
3. Discussion
Authors The present study reports for the first time a clinical case of the possible association between psychotic disorders and primary thrombophilia due to MTHFR and PS deficiency. In this sense, bipolar disorder with early onset during childhood or adolescence has been associated with a worse prognosis compared to cases with a later onset during adulthood and, in most cases, is linked to a genetic component [10]. Psychotic disorders are clinically characterized by hallucinations, delusions, and disorganized thinking and behavior, as observed in schizophrenia, although they can also occur in other psychiatric and medical conditions. Many children and adolescents report psychotic-like experiences, which may be related to other forms of psychopathology and personal history, such as trauma, substance use, or suicidal behavior [7]. The origin may be involved in heredity, changes in the levels of some neurotransmitters and maladaptation of psychological factors. On the other hand, neuropsychiatric disorders with metabolic origin are difficult to identify, although the early signs and their association with extra-neurological manifestations such as hematological, gastrointestinal or respiratory symptoms may also suggest a genetic component [5,7]. In the present case, the concomitant development of neuropsychiatric symptoms and thrombophilia suggested a neurometabolic alteration. Some of the signs that might guide clinical evaluation towards a neurometabolic disease are: 1) Resistance, refractory or paradoxical response to antipsychotics, 2) Serious neurological adverse effects after the administration of antipsychotics, 3) Abrupt development of psychiatric disorders in patients with seizures or developmental delays, 4) Early onset of psychiatric symptoms along with mental retardation or progressive cognitive impairment in children with prior normal development and 5) Presence of catatonia associated with atypical elements [5].
Mutations in MTHFR and expression of PS have been widely documented in primary thrombophilia [1,2]. In this regard, major psychiatric disorders such as major depression and schizophrenia development have been associated with an increase in thrombotic risk [8]. Feasibly, healthy blood tissues ensure brain homeostasis and any disturbance in them could unchain serious neuropsychiatric conditions. In this clinical case, acute steroid management and dosage cannot acutely generate bipolar disorder or changes associated with blood coagulation. Using drugs to reduce hypercoagulability significantly improved the patient's behavior in the short term: neuronal metabolism (oxygenation, temperature, ATP levels and neurochemistry) gradually recovered as flow and perfusion were restored, especially in the brain.
Besides its role in primary thrombophilia, MTHFR gene mutations have also been related to bipolar disorder and schizophrenia [6,7,8,9,10,11,12,13,14,15,16,17]. Likewise, free PS deficiency has been reported in patients with schizophrenia [8], although an association with bipolar disorder has not been established. The coexistence of neurological symptoms, such as epilepsy, along with thrombosis due to MTHFR deficiency has already been described in two brothers [3]. However, a case of bipolar disorder associated with thrombophilia in the same patient has not been reported yet.
In conclusion, the present case highlights the importance of ruling out neurometabolic and hematological alterations in patients with psychiatric disorders, especially those with early symptoms onset or when they coincide with atypical signs. A prompt and accurate diagnosis could offer a better quality of life to the patients, since their symptoms correspond to treatable psychiatric disorders. The relationship between MTHFR mutation, PS deficiency and psychotic disorder still requires more research but, hopefully, this paper will contribute breakthrough insights to grant accurate diagnosis and suitable treatments.
Author Contributions
Conceptualization, DMP and ADSM.; methodology, DMP, ADSM AND MEME .; validation, JCG and EC; formal analysis, DMP, ADSM, JCG and EC, investigation, DMP, ADSM, JCG and EC.; data curation, BS, MEME, HSC and AAG.; writing—original draft preparation EFS, BSRM and RJ,.; writing—review and editing, LMM, BS, RJ and EFS.; visualization, HSC and AAG.; supervision, LMM, BSRM and EFS.; funding acquisition, RJ and EFS. All authors have read and agreed to the published version of the manuscript.
Funding
Edgar Flores-Soto and Ruth Jaimez were supported by the División de Investigación, Facultad de Medicina, Universidad Nacional Autónoma de México. EFS (FM/DI/123/2024) RJ (FM/DI/022/2024).
Institutional Review Board Statement
Ethical approval is not required for this case report in accordance with local or national guidelines. Consent to publish statement: Written informed consent was obtained from the patient and legal gardian for publication of the details of the medical case and any accompanying images.
Informed Consent Statement
Informed consent was obtained from the patient and legal gardian involved in the study. Written informed consent has been obtained from the patient and legal gardian to publish this paper.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on reasonable request.
Acknowledgments
The authors would also like to thank Ms Dora Nely Martinez Aguirre for administrative and technical support (National Autonomous University of Mexico, Mexico City 04510).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MTHFR | methylenetetrahydrofolate reductases |
| PS | protein S |
| PC | protein C |
| FVL | Factor V Leiden |
| C4BP | complement protein 4 |
| APC | activated PC |
| TFPI | tissue factor pathway inhibitor |
| Al222Val | alanine to valine |
| BDNF | brain derived neurotrophic factor |
| CSF | cerebrospinal fluid |
| EEG | electroencephalogram |
| MRI | magnetic resonance imaging |
| ATP | Adenosin triphosphate |
References
- Méndez-López, M.; Salazar-Sánchez, L.; Porras, P. J. Trombofilia Primaria: Mejorando el Diagnóstico Basado en Evidencia. Rev. Costarric. cardiol. 2013, 15(2), 25–30. [Google Scholar]
- Castro Quismondo, N.; Rodríguez Rodríguez, M.; Zafra Torres, D.; Martínez-López, J. Trombofilia y trombosis. Medicine. 2020, 13(22), 1259–66. [Google Scholar] [CrossRef]
- Gales, A.; Masingue, M.; Millecamps, S.; Giraudier, S.; Grosliere, L.; Adam, C.; et al. Adolescence/adult onset MTHFR deficiency may manifest as isolated and treatable distinct neuro-psychiatric syndromes. Orphanet. J. Rare. Dis. 2018, 13(29). [Google Scholar] [CrossRef] [PubMed]
- Majumder, R.; Nguyen, T. Protein S: function, regulation, and clinical perspectives. Curr. Opin. Hematol. 2021, 28(5), 339–44. [Google Scholar] [CrossRef] [PubMed]
- Herrera, P.M.; Vélez Van Meerbeke, A.; Bonnot, O. Trastornos psiquiátricos secundarios a enfermedades neurometabólicas. Rev. Colomb. Psiquiatr. 2018, 47(4), 244–51. [Google Scholar] [CrossRef] [PubMed]
- El-Hadidy, M.A.; Abdeen, H.M.; Abd El-Aziz, S.M.; Al-Harrass, M. MTHFR Gene Polymorphism and Age of Onset of Schizophrenia and Bipolar Disorder. Biomed. Res. Int. 2014, 2014, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sunshine, A.; Mcclellan, J. Practitioner Review: Psychosis in children and adolescents. J. Child. Psychol. Psychiatry. 2023, 64, 980–8. [Google Scholar] [CrossRef] [PubMed]
- Hoirisch-Clapauch, S.; Nardi, A.E.; Gris, J.C.; Brenner, B. Coagulation and Mental Disorders. Rambam. Maimonides. Med. J. 2014, 5(4), e0036. [Google Scholar] [CrossRef] [PubMed]
- Pujol, N.; Mané, A.; Bergé, D.; Mezquida, G.; Amoretti, S.; Pérez, L.; et al. Influence of BDNF and MTHFR polymorphisms on hippocampal volume in first-episode psychosis. Schizophr. Res. 2020, 223, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, K.P.; Cullen, K.R.; Deyoung, C.G. Klimes-Dougan B. The genetics of early-onset bipolar disorder: A systematic review. J. Affect. Disord. 2015, 184, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.Y.; Qian, Z.Z.; Gong, F.F.; Lu, S.S.; Feng, F.; Wu, Y.L.; et al. Methylenetetrahydrofolate reductase (MTHFR) polymorphism susceptibility to schizophrenia and bipolar disorder: an updated meta-analysis. J. Neural. Transm. 2015, 122(2), 307–20. [Google Scholar] [CrossRef] [PubMed]
- Peerbooms, O.L.; van Os, J.; Drukker, M.; Kenis, G.; Hoogveld, L.; Group MiP.; et al. Meta-analysis of MTHFR gene variants in schizophrenia, bipolar disorder and unipolar depressive disorder: evidence for a common genetic vulnerability? Brain. Behav. Immun. 2011, 25(8), 1530–43. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Lee, S.Y.; Chen, S.L.; Chang, Y.H.; Chen, P.S.; Huang, S.Y.; et al. A potential interaction between COMT and MTHFR genetic variants in Han Chinese patients with bipolar II disorder. Sci. Rep. 2015, 5(1), 8813. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Zheng, J.L.; Sun, M.L.; Lai, H.Y.; Wang, B.J.; Yao, J.; et al. Association between MTHFR (677C>T and 1298A>C) polymorphisms and psychiatric disorder: A meta-analysis. PLoS One. 2022, 17(7), e0271170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.X.; Yang, L.P.; Gai, C.; Cheng, C.C.; Guo, Z.Y.; Sun, H.M.; et al. Association between variants of MTHFR genes and psychiatric disorders: A meta-analysis. Front. Psychiatry. 2022, 13, 976428. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.; Li, Y.; Zhang, Z.; Sun, Z.; He, Y.; Li, R. Methylenetetrahydrofolate reductase and psychiatric diseases. Translational. Psychiatry. 2018, 8, 242. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Naeem, A.; Fritts, A.; Cummins, M.; Kayes, C.; Fang, W. Discovery of Methylenetetrahydrofolate Reductase (MTHFR) Deficiency in Individuals With Common Psychiatric Comorbidities: A Retrospective Case Review. Cureus. 2024, 16(4), e58122. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Contrast-enhanced magnetic resonance imaging of the brain. A) Image showing left parotid gland enlargement. B) Venoresonance with filling defect of the transverse sinus and hyperintensity at the confluence of the sinuses can be appreciated. C) Venoresonance post-treatment without filling defect.
Figure 1.
Contrast-enhanced magnetic resonance imaging of the brain. A) Image showing left parotid gland enlargement. B) Venoresonance with filling defect of the transverse sinus and hyperintensity at the confluence of the sinuses can be appreciated. C) Venoresonance post-treatment without filling defect.
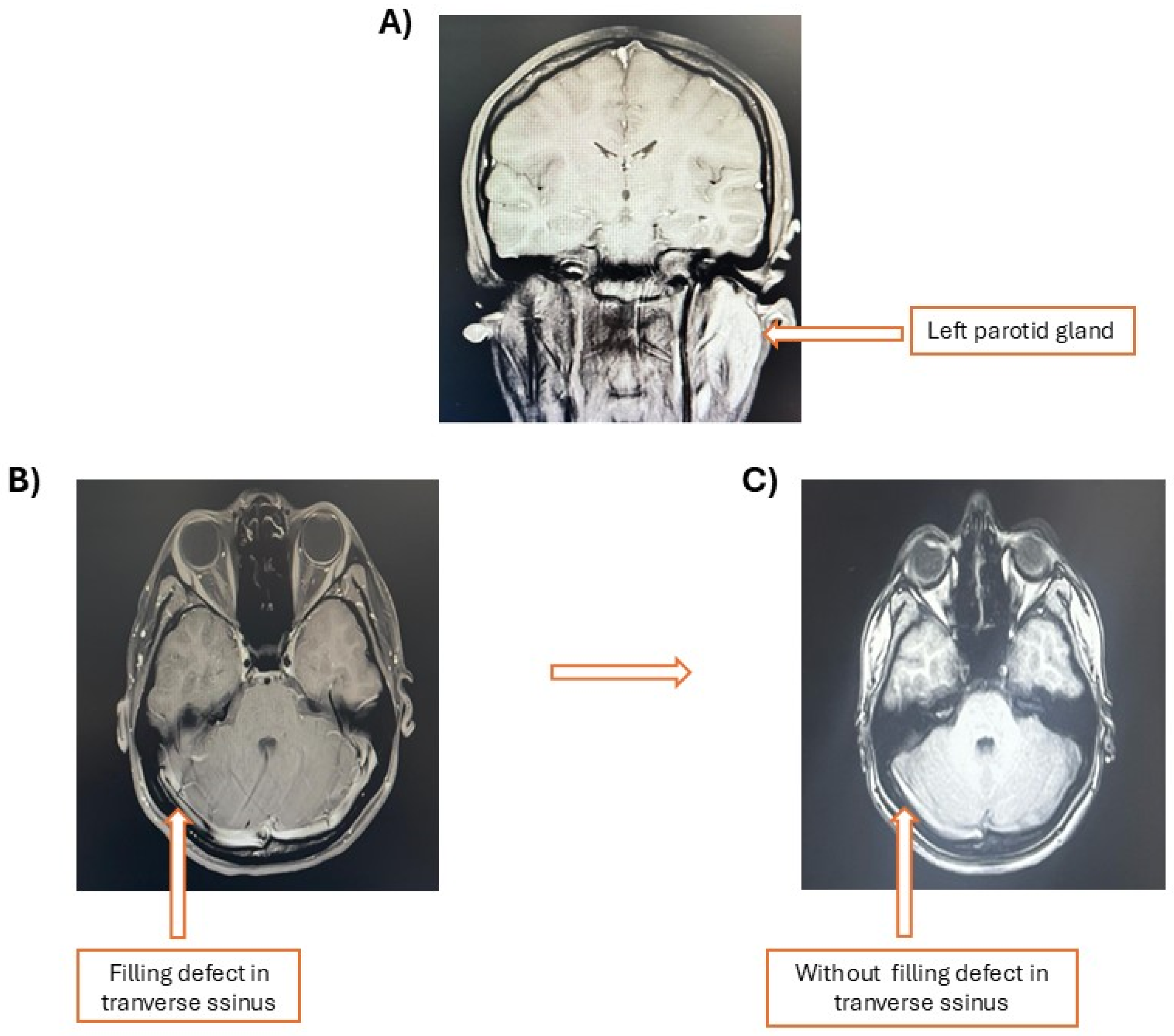

Table 1.
TORCH profile.
| Study | Outcome | Reference Value |
|---|---|---|
| Toxo IgG | < 5 UI/mL | Non-reactive |
| Toxo IgM | 0.02 l/mL | Non-reactive |
| Rubella IgM | 0.16 IC | Non-reactive |
| Cytomegalovirus IgG | 2.42 IC | Reactive >1.1 |
| Cytomegalovirus IgM | 0.2 IC | Non-reactive |
| Herpes I and II IgG | 0.63 IC | Non-reactive |
Table 2.
Thrombophilic and Autoimmune Profile. Analysis of Genetic and Coagulation Factors.
| Study | Outcome | Reference Value |
|---|---|---|
| Factor II mutation 20210 genotype | Not detected | Not detected |
| Mutation factor V (Leiden mutation) | Not detected | Not detected |
| MTHFR variant P.ALA22VAL | Detected | Not detected |
| C3 complement | 119.620 | 90-180 |
| C4 complement | 26.835 | 10-40 |
| ANTI-SSB Antibodies (LA) | 3.3 | <20 |
| Anti-NATIVE DNA antibodies (IFI) | Negative | Negative |
| Antineutrophil cytoplasmic antibodies (ANCA P) | Negative | Negative |
| Perinuclear neutrophil antibodies | Negative | Negative |
| Myeloperoxidase | Negative | Negative |
| Anti SSA antibodies (RO) | 4.9 | < 20 |
| Anti-beta 2 glycoprotein IGG antibodies | 6.4 | < 20 |
| Anti-beta 2 glycoprotein IGM antibodies | 2.1 | < 20 |
| Lupus anticoagulant | 1.14 | < 1.16 |
| Anticardiolipin IGG antibodies | 4.0 | < 20 |
| Anticardiolipin antibodies IGM | 2.1 | < 20 |
| Coagulation protein C | 77.0 | 65-130 |
| Coagulation protein S | 35.0 | 54.0-103.0 |
| Coagulation factor XII | 65.9 | 36.0-159.0 |
| Prothrombin time | 11.8 sec | 11-13 sec |
| International normalized ratio (INR) | 1 | 0.8-1.2 |
| Activated partial thromboplastin time | 23.2 sec | 25-45 sec |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



