Submitted:
30 April 2025
Posted:
02 May 2025
You are already at the latest version
Abstract
The current meta-analysis modified the Enduring Vulnerability Stress Adaptation model of relationship functioning and the Attachment System Activation model of individual functioning to incorporate various aspects of sexual health. This provided conceptual frameworks for integrating the findings on a wide range of correlates of sexual health into comprehensive models of individual and interpersonal functioning to guide future research. Drawing from the clinical psychology, social psychology, and medical literatures, 3,119 unique records were initially identified, resulting in a final set of 173 records, representing 205 independent (sub)samples and a final combined sample of 160,466 participants. A total of 930 effects were extracted, yielding 44 meta-analytic effects (using random effects modeling). Path analyses of meta-analytic correlation matrices revealed that key dimensions of sexual health (i.e., sexual satisfaction, orgasms, sexual desire, lack of sexual pain, vaginal lubrication) demonstrated unique links to greater health, interpersonal functioning, and individual functioning (i.e., higher psychological well-being, physical health, & relationship satisfaction; lower psychological distress, attachment anxiety, & attachment avoidance). Meta-regression moderation analyses revealed that the effect linking orgasms to higher sexual satisfaction was especially pronounced for women and for individuals in clinical (sub)samples. Moderation analyses also suggested that the link between orgasms and lower distress was especially pronounced for older individuals. The findings were limited by the cross-sectional nature of the vast majority of the findings (96% of the records), leaving the directions of causality unclear. Taken together, these results highlight the central role that sexual health and more specifically orgasms might play in individual and relationship health, supporting the proposed conceptual models and highlighting directions for future research.
Keywords:
orgasm
; well-being
; psychological distress
; physical health
; relationship satisfaction
; sexual health
; meta-analysis
Significance Statement: This meta-analysis highlights the importance of individuals’ sexual health. Sexual satisfaction, orgasms, and sexual desire demonstrated unique links to greater physical health, stronger senses of well-being, lower personal distress, and happier relationships, and were predicted by lower attachment insecurities, underscoring their importance across multiple domains of life.
Sexual behavior has long been discussed as one of the most basic human physical and psychological needs (Maslow, 1943). Consistent with this, previous work has emphasized the importance that sexual health plays in romantic relationships (e.g., Ellsworth & Bailey, 2013; Shaw & Rogge, 2016), as well as in other aspects of life in general (e.g., psychological and physical well-being; e.g., Fabre & Smith, 2012; Levin, 2007). This growing body of work has developed a multidimensional conceptualization of sexual health which includes not only sexual satisfaction, but also orgasmic functioning, sexual desire, vaginal lubrication, lack of sexual pain, and erectile functioning. Given the high value individuals place on orgasms (Opperman et al., 2014), one line of research has focused specifically on links between orgasmic functioning and well-being, underscoring the importance of orgasms for sexual satisfaction, relationship satisfaction, physical health, mental health, and life satisfaction (e.g., Abramov, 1976; Brezsnyak & Whisman, 2004; Brody & Costa, 2009; Ellsworth & Bailey, 2013). The current review sought to synthesize and integrate this growing line of research on the salience of orgasms in the lives of individuals, by examining orgasmic functioning within the broader context of multiple aspects of sexual health, thereby highlighting the unique links between each aspect of sexual health and the well-being correlates examined. Although a broad array of studies spanning both the psychology and medical literatures have examined the correlates of sexual health (and more specifically orgasmic functioning, see Table 1 and Table 2), the vast majority of this work was atheoretical in nature. In addition, the correlates of orgasms and other aspects of sexual health have generally taken a secondary or even tertiary role in the focus of the analyses presented (often appearing only as a handful of undiscussed correlations in a much larger correlation matrix). The current review therefore sought not only to synthesize this vast array of previous studies, but to also develop a theoretical framework to help conceptually integrate previous findings and guide future work in this area.
Conceptualizing Sexual Health
Sexual Health as a Central Process. Defining sexual health is a complex task, as it encompasses physical, emotional, mental, and social well-being (World Health Organization, 2002). As sexual health is not merely the absence of dysfunction, but a holistic experience of well-being, it remains imperative to investigate sexual functioning in its scope beyond dysfunctionality. As such, pleasurable sexual experiences do not focus only on achieving orgasms or other physiological factors such as vaginal lubrication, erectile function, or lack of pain, but also include emotional components such as sexual desire, sexual arousal, and sexual satisfaction. Consistent with this, internationally validated sexual health measurement scales such as the Derogatis Sexual Functioning Inventory (DSFI; Derogatis & Melisaratos, 1979; Derogatis, 1997), Female Sexual Function Index (FSFI; Rosen et al., 2000), or International Index of Erectile Function (IIEF; Rosen et al., 1997) provide the tools for researchers to embrace a more diverse and multivariate conceptualization of sexual health (i.e., including sexual satisfaction, orgasmic functioning, sexual desire, vaginal lubrication, lack of pain, and erectile functioning). Thus, although a large body of work has incidentally examined sexual dysfunctions as secondary symptoms of physical health issues (such as cancer, obesity, or psychiatric diagnoses; e.g., Castellini et al., 2010; Conroy, 2018; Hoyer et al., 2009), the current review applies a novel lens to this literature by examining sexual health as a critical aspect of individual and interpersonal well-being that spans a wide range of populations (both clinical and non-clinical) as well as a wide range of contexts (representing a set of dynamic processes rather than just secondary symptoms).
Orgasms as One Component of Sexual Health. A growing body of work has more specifically focused on orgasmic functioning as a key aspect of sexual health (e.g., Abramov, 1976; Brezsnyak & Whisman, 2004; Brody & Costa, 2009; Ellsworth & Bailey, 2013). In fact, there is evidence suggesting that orgasms are still widely perceived as the ultimate goal of sexual activity (e.g., Opperman et al., 2014), supporting their use as a key marker of sexual health. As a counterpoint to those findings, an emerging area of research has also noted limitations of placing too much weight on orgasms alone, pointing out that: (1) not all orgasms are pleasurable (e.g., Chadwick et al., 2019), (2) sexual pleasure consists of other crucial elements as well (e.g., Chadwick et al., 2019), (3) satiating sexual pleasure can be achieved without orgasming (e.g., Opperman et al., 2014), and (4) some individuals even experience orgasms despite engaging in unpleasurable or coerced sexual activity (e.g., Chadwick et al., 2019). Thus, to integrate these perspectives, when reviewing the literature on how orgasms are linked to physical, mental, and relationship functioning, it is critical to examine orgasmic functioning within the broader multivariate context of sexual health. Thus, the current review examined orgasmic functioning alongside the other key aspects of sexual health, including sexual satisfaction, desire, lack of pain, vaginal lubrication, and erectile function. This allowed us to uncover the unique links between each aspect of sexual health and various aspects of individual functioning.
Modeling Sexual Health. Although scales like the FSFI and IIEF served to operationalize as many as eight distinct facets of sexual health across men and women, those aspects of sexual health are fundamentally interrelated and therefore notably correlated with one another. Thus, in examining the links between components of sexual health and various aspects of well-being, the current review sought to incorporate those interrelations within multivariate path models. Specifically, the current review conceptualized sexual satisfaction as an overarching construct and the other components of sexual health as key contributors to that global evaluation.
Overview of Research on Orgasms
To ground the current review within a broader perspective of the diversity of studies that have examined orgasmic functioning, the following sections provide a brief overview of the broader orgasmic functioning literature. The following overview also allows us to briefly review many of the studies that helped to shape the various fields of research on orgasms but did not meet the criteria to be included in the current meta-analysis. Finally, it allows us to describe some specific studies to provide a deeper sense of the methods commonly used across these studies. Within the literature, experiencing orgasms has been assessed and quantified in three main ways: (1) frequency of orgasms within a recent time frame (e.g., in the last month), (2) consistency of achieving orgasms from sexual activity (e.g., proportion of sexual encounters or activity that results in orgasms), or (3) a group contrast between individuals experiencing orgasms and those not experiencing orgasms (either at a lifetime level or from recent sexual activity). Given these differing operationalizations, we will use the terms “orgasmic functioning,” “orgasms,” and “experiencing orgasms” as umbrella terms to represent all three conceptualizations.
Orgasm Gender Gap. When examining the salience of orgasms in the lives of men and women, the first issue that needs to be acknowledged is that the ability to achieve orgasms is quite different across the sexes. For example, a nationally representative sample of Australians suggested that 95% of men achieved orgasm in their most recent sexual encounter, compared to only 69% of women (Richters et al., 2006). Consistent with this, data from a national probability sample of 3,159 individuals in the United States (the National Health and Social Life Survey) suggested that although 75% of men reported “always” having an orgasm during sexual activity with a partner, only 29% of women reported the same level of consistency (Laumann et al., 2000). These findings were echoed in a sample of 833 college students with 28% of women and only 3% of men reporting never orgasming with partners, and another 23% of women and only 3% of men reporting only “sometimes” orgasming (Wade et al., 2005). In fact, estimates from a national sample of over 52,000 adults suggest that 95% of heterosexual men in the United States are able to experience orgasms from sexual activity compared to only 65% of heterosexual women (Frederick et al., 2018). Women experience orgasms significantly less frequently than men in casual sexual encounters as well as in committed relationships (e.g., Armstrong et al., 2012; Blair et al., 2018; Frederick et al., 2018). Although they have triggered debate within the field (e.g., Brody et al. 2018; Levin, 2007, 2012a, 2012b; Prause, 2012a; Prause, 2012b), a number of studies have even suggested that gender differences might appear most pronounced (and show particularly strong associations) for specific types of orgasms from specific forms of sexual activity (e.g, penile-vaginal intercourse—PVI—without clitoral stimulation; e.g., Blair et al., 2018; Brody & Costa, 2008, 2009; Brody et al., 2010; Costa & Brody, 2007; see Brody, 2006, 2010 for reviews). Despite results suggesting that men and women report comparable levels of overall satisfaction with their sex lives (e.g., Shaw & Rogge, 2016), similar gender differences to those observed with orgasms have emerged for reports of sexual desire (e.g., Regan & Atkins, 2006) and sexual pain (e.g., Rosen, 2000; Stephenson et al., 2011).
Orgasms as Health Correlates. In the medical and treatment literature, the frequency and the ability to achieve orgasms has often been conceptualized as a health correlate. For example, in depression and depression treatment research, difficulty or inability to achieve orgasms has often been studied as a correlate of depressive symptoms (e.g., Chang et al., 2012; Kuffel & Heiman, 2006; Laurent & Simons, 2009), as well as a side effect of antidepressant medication (especially selective serotonin reuptake inhibitors; e.g., Berman et al., 2011; Khazaie et al., 2015; Krishna et al., 2011). Orgasmic functioning has also been examined as a secondary symptom in studies of Parkinson’s disease (e.g., Celikel et al., 2008; Lipe et al., 1990), multiple sclerosis (e.g., Fragla et al., 2014; Sahay et al., 2012), cancer (e.g., Brotto et al., 2008; Flynn et al., 2013), chronic pain (e.g., Aubin et al., 2008; Ciftci et al., 2011), and other medical disorders that may impact sexual functioning (e.g., Atarodi-Kashani et al., 2017; Bouhlel et al., 2017; Caruso et al., 2012; Strizzi et al., 2015). Although not the primary focus of these studies, this has yielded a body of work linking the symptom of orgasmic difficulties to depressive symptoms.
Difficulty with Orgasms as a Disorder. In addition to exploring orgasm difficulties as a secondary dysfunction associated with existing medical disorders, they have also been investigated as primary sexual dysfunctions (e.g., Meston et al., 2004a). The 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013) lists a number of sexual dysfunctions, including those of arousal, drive, and pain. It specifically includes three disorders of orgasm functions: Female Orgasmic Disorder, Delayed Ejaculation, and Premature (Early) Ejaculation (American Psychiatric Association, 2013). While there is some literature exploring the nature, presentation, and etiology of specific sexual dysfunctions (e.g., Brody, 2017; Feldman & Larsen, 2014; Graham, 2014; Hunter & Goodie, 2017; Laan & Rellini, 2012), most research in this area aggregates sexual dysfunctions when examining their correlates (e.g., Du et al., 2016; Galinsky, 2012) rather than examining specific (e.g., orgasmic) sexual dysfunctions separately. That literature has robustly demonstrated the negative correlates of such disorders for individual and interpersonal functioning, highlighting importance of healthy sexual functioning in daily life (e.g., Amicis et al., 1984; Fisher et al., 2005; Jiann et al., 2013).
Orgasms as a Relationship Process. A small but growing body of literature has begun to examine sexual behavior as a key process in romantic relationships. Findings across this body of work suggest that frequency of orgasms is positively linked to other aspects of sexual health (e.g., greater sexual desire and satisfaction, less time needed to achieve sexual arousal; e.g., Brody, 2007; Hurlbert & Whittaker, 1991). Studies have also linked orgasms to greater relationship quality and marital satisfaction (e.g., Brody & Weiss, 2011; Costa & Brody, 2007; Guo et al., 2004; Hurlbert & Whittaker, 1991; Rowland & Kolba, 2019) and to greater relationship investment (e.g., Ellsworth & Bailey, 2013). Although a majority of these studies have focused specifically on the importance of women’s orgasms, a handful of studies have linked higher rates of orgasm consistency and frequency in men to higher levels of sexual satisfaction (e.g., Brody & Costa, 2009; Morokqff & Gilliland, 1993), relationship satisfaction (e.g., Brody & Costa, 2009; Frederick et al., 2018), and even lower mortality (e.g., Abramov, 1976; Persson, 1981).
Orgasms as a Source of Well-Being. A promising vein of research focused primarily on orgasms in the lives of women has begun to examine links between sexual activity and individual well-being. For example, women who reported greater frequency of orgasms reported higher self-esteem (e.g., Hurlbert & Whittaker, 1991), lower subjective stress (e.g., Bodenmann et al., 2010; Pakpour et al., 2015), more effective life coping skills (and lower use of maladaptive coping strategies; e.g., Borissova et al., 2001; Brody et al., 2010). Inability to achieve orgasms on the other hand has been linked to higher attachment anxiety and lower overall satisfaction with life, health, and romantic relationships (e.g., Costa & Brody, 2011). The vast majority of the studies examining these links have been cross-sectional in nature, leaving potential directions of causality unclear. Results from one of the few studies to have employed a longitudinal design suggested that women’s enjoyment of sexual intercourse and men’s frequency of sexual intercourse was linked to greater longevity (i.e., longer life spans; Palmore, 1982).
Sexual Health Correlates
Extending the review of research focused on orgasmic functioning, the remaining aspects of sexual health have demonstrated similar links to physical and mental health as well as interpersonal functioning. For example, due in large part to the widespread adoption of the FSFI and IIEF within the medical literature, sexual satisfaction, sexual desire, a lack of sexual pain, and vaginal lubrication have each demonstrated links to lower psychological distress (e.g., Lew-Starowicz & Rola, 2014; Onem et al., 2008), lower attachment anxiety and attachment avoidance (e.g., Pinsky, 2016; van der Brink et al., 2016), greater well-being (e.g., Artune-Ulkumen et al., 2014; Demir et al., 2013), greater physical health (e.g., Khnaba et al., 2016; Morales et al., 2013), and greater relationship satisfaction (e.g., Stephenson & Meston, 2015; Witting et al., 2008a). This large body of predominantly cross-sectional findings therefore highlights the importance of examining the correlates of orgasms within the broader context of multiple forms of sexual health.
Organizing Conceptual Framework
Much of the work examining orgasms has adopted a more clinical or practical approach, examining the correlates of orgasms to inform the treatment of medical and/or sexual disorders. The bulk of the work in this area has therefore been atheoretical by design. To begin to integrate this growing body of work into a coherent theoretical framework of both individual and relationship functioning, the current review drew upon the Enduring-Vulnerability Stress-Adaptation model of relationship functioning (EVSA; Karney & Bradbury, 1995) as well as the Attachment System Activation model (ASA; Shaver & Mikulincer, 2002). These models therefore informed the selection of correlates to be examined within the meta-analysis.
Enduring-Vulnerability Stress-Adaptation Model. In their EVSA model, Karney and Bradbury (1995) highlight three key sets of processes that interact to shape the course of relationships over time: (1) enduring vulnerabilities (i.e., jagged edges of their personalities that individuals bring with them into relationships such as personality traits and attachment orientations), (2) stressful events (i.e., external events that could impact a relationship such as getting fired, illness, and conflict with family), and (3) adaptive processes (i.e., the adaptive and maladaptive dyadic processes that couples engage in response to life stressors, including constructs such as emotional support, negative conflict, and forgiveness; see Figure 1A for the full EVSA model). Within the EVSA model, enduring vulnerabilities can directly affect how partners interact with one another within the relationship (influencing dyadic adaptive processes), how the partners adapt in stressful situations (potentially interacting with life stress to exacerbate its impact on relationships), and can even serve to generate stressful life events for the couples to navigate. Stressful events are conceptualized as potentiating events that exert pressure on couples, forcing them to engage their emotion regulation and dyadic coping skills in response. Finally, the dyadic adaptive processes are viewed as most proximally linked to relationship quality, with healthy patterns of interaction helping to buffer relationships from the adverse effects of stress and enduring vulnerabilities, whereas maladaptive patterns are posited to exacerbate those negative effects. Notably, within the EVSA model, enduring vulnerabilities and maladaptive dyadic processes are presumed to require triggering by stressful life events to exert their full influence on relationship quality.
Extending this model to focus specifically on sexual functioning (see Figure 1A), enduring vulnerabilities would likely include a diverse array of constructs such as comfort and knowledge of own body, biological difficulty in achieving orgasms, attitudes toward sex, and attachment orientation, as those trait-like qualities could not only influence dyadic behavior (e.g., affecting how individuals approach sexual activity and sexual communication), but could also serve to generate stress within the relationship (e.g., generating tension over differing views and expectations surrounding the sexual component of their relationships, generating disappointing sexual/intimate encounters). In the context of the EVSA model, failure to have an orgasm within a specific sexual encounter could be conceptualized as a stressful event, potentially interacting with enduring vulnerabilities like sexual expectations, and triggering the need for adaptive processes like greater sexual responsiveness, sexual communication, as well as compassion and empathy. The EVSA model would therefore suggest that adaptive processes like strong emotional support and healthy sexual communication would likely buffer relationships from any possible adverse effects of difficulties with orgasms, whereas maladaptive processes (e.g., withdrawal, avoidance, hostile behavior) would likely exacerbate those adverse effects. In fact, within the context of the EVSA model, the ability to consistently achieve orgasms during sexual activity with a partner could also be modeled as another adaptive process, thereby serving to buffer the relationship from stressful events or the jagged edges of both partners’ personalities. As the need for feeling connected to others has been conceptualized as a fundamental human need (Deci & Ryan, 2000), we conceptualized romantic relationship quality as a key marker of this basic need. As a result, we posited that relationship quality would serve as the most proximal factor (and therefore likely the main mechanism) linking sexual relationship processes to individual well-being.
Attachment System Activation Model. To link the current investigation to another robust model in the field of couples research, the current study also conceptualized the ASA (Shaver & Mikulincer, 2002) as a more fine-grained model informed by the EVSA model. The ASA model (Figure 1B) expands upon Bowlby’s (1969/1982, 1973, 1980, 1988) attachment theory by applying it to adult romantic relationships. Specifically, the ASA model highlights three main components: (1) appraisal of a threat (i.e., something causing stress to a relationship or triggering attachment insecurities), (2) individual attachment insecurities (most commonly conceptualized as attachment avoidance and attachment anxiety), and (3) reactive strategies (i.e., behavioral responses to a threat). Thus, within the ASA model, attachment insecurities are not conceptualized as directly impacting relationship quality. Instead, some sort of threat is required to activate the attachment system, triggering specific behavioral reactions involving either deactivating (e.g., withdrawal, emotion suppression) or hyperactivating (e.g., hypervigilance, rumination) strategies. Given this conceptualization, we see clear links between the ASA model and the EVSA model, as the ASA model takes a specific enduring vulnerability of attachment, concentrates on a specific subset of (mal)adaptive processes (i.e., deactivation and hyperactivation strategies), and conceptualizes threats as potentiating the activation of that system in a manner similar to the role of life stress in the EVSA model. Although sexual functioning could be considered an independent system from the attachment system, we assert that the ASA model could be meaningfully applied to sexual functioning. From a sexual functioning perspective, orgasm difficulties and a failure to achieve an orgasm during a sexual encounter with a partner could be conceptualized as a clear threat, activating the attachment system, and thereby promoting deactivation and hyperactivation strategies. Thus, a partner with high levels of attachment avoidance (i.e., feeling uncomfortable with emotional disclosure and intimacy) might withdraw when faced with orgasm difficulties, avoiding communication as well as avoiding further sexual intimacy. Such deactivation strategies would in turn impact relationship quality and eventually individual functioning over time. In contrast, a partner with high levels of attachment anxiety (i.e., a general tendency to feel that partners do not love you as much as you love them leading to excessive preoccupation and worry) might hyper-engage their partner when faced with orgasm difficulties, ruminating over the issue, and possibly becoming demanding and requiring excessive validation. Given this conceptual framework, the current review focused on examining an array of correlates of orgasms spanning the various components of these models (see bolded examples in Figure 1).
Previous Reviews
The current comprehensive literature search (described below) failed to identify any published systematic reviews or meta-analyses focused on examining the correlates of orgasms. However, the current literature search did uncover a number of published narrative and systematic reviews that focused on distinct but related topics. For example, White and Reamy (1982) published a review of 74 articles examining sex during pregnancy, however none of their articles overlapped with the current sample of 173 records. Similarly, narrative reviews of female sexual functioning in old age (Wood et al., 2012; 3 of its 58 articles overlapped with the current review), the health benefits of various sexual activities (Brody, 2010; 9 of its 174 studies overlapped), the psychological and interpersonal correlates of sexual dysfunction (Brotto et al., 2016; 1 of its 364 articles overlapped), and links between sexual activity and both physical and mental health (Levin, 2007; 5 of its 74 articles overlapped) demonstrated similar low levels of overlap with the current review. Finally, although Meston and colleagues (2004b) published a narrative review of 323 articles examining women’s orgasms, the extremely broad scope of that review represented such a distinct focus that none of its articles overlapped with those in the current meta-analysis. Thus, the current review offers a unique quantitative contribution to the current literature, integrating findings across a wide range of disparate fields and then testing novel path models to evaluate unique (i.e., incremental) links from the various aspects of sexual health to the correlates examine. It also represents the first review to systematically examine the correlates of orgasmic functioning within the broader context of a multivariate conceptualization of sexual health, evaluating the unique links between orgasms and both individual and interpersonal functioning after controlling for other key aspects of sexual health.
Present Meta-Analysis
With the aim of integrating and summarizing research across various domains of functioning, the current study draws from literature in social psychology, clinical psychology, and the medical literature to provide a meta-analytic review of associations between orgasms, and individual and relationship functioning. Based on the previous literature, we anticipated that all six of the sexual health dimensions (i.e., sexual satisfaction, orgasms, sexual desire, lack of pain, lubrication, erectile function) would show significant bivariate meta-analytic correlations to lower distress, greater well-being, better physical health, higher relationship satisfaction/quality, lower attachment anxiety, and lower attachment avoidance. To extend that bivariate literature, our hypotheses focused on a set of multivariate path analyses examining unique links between aspects of sexual health and the correlates. Notably, the multivariate question of unique or incremental predictive validity among aspects of sexual health (when examining links to correlates) represents an entirely novel contribution to the field, as it had not been explored across the 1,012 full-text records screened for the current meta-analysis, nor within the 173 records within the current meta-analysis. As seen in Figure 2, we conceptualized the more focused indicators of sexual health (orgasms, sexual desire, lack of pain, lubrication, & erectile function) as individual components feeding into sexual satisfaction. Thus, higher levels of functioning on each of those key components were hypothesized to uniquely promote greater sexual satisfaction (i.e., incrementally contributing to greater positive global evaluations; Hypothesis 1). As seen in Figure 2A, for four of the correlates examined (i.e., distress, well-being, physical health, relationship satisfaction), we hypothesized that sexual satisfaction would demonstrate strong proximal links to those more global forms of functioning. Thus, we hypothesized that even after controlling for the other forms of sexual health, higher sexual satisfaction would predict lower distress (Hypothesis 2A), greater well-being (Hypothesis 2B), better physical health (Hypothesis 2C), and higher relationship satisfaction/quality (Hypothesis 2D). Those hypotheses thereby propose that the more specific indicators of sexual health would be indirectly linked to the individual global functioning correlates via their links with sexual satisfaction (Hypothesis 3). After controlling for those indirect links, we further hypothesized that those more specific components of sexual health (including orgasmic functioning) would show unique predictive links to this set of correlates, further highlighting the central nature of sexual health in the lives of individuals (Hypothesis 4). As attachment avoidance and anxiety reflect more stable characteristics that individuals bring into sexual relationships and encounters (consistent with the EVSA and ASA models), we used a different model to examine associations between those correlates and sexual health. As shown in Figure 2B, we hypothesized that greater attachment insecurities would be linked to lower levels of sexual functioning on the more focused indicators (Hypothesis 5), thereby showing indirect links to lower sexual satisfaction (Hypothesis 6). Even after controlling for those indirect paths involving the more focused aspects of sexual health, we finally hypothesized that greater attachment insecurities would be uniquely linked to lower sexual satisfaction (Hypothesis 7).
Potential Moderators. Drawing from previous research, the current study examined a set of moderators primarily focused on identifying subpopulations more likely to experience difficulties achieving orgasms, hypothesizing that the associations with experiencing orgasms would be stronger in those challenged populations. Given the marked gender disparities already uncovered in this field of research (e.g., Armstrong et al., 2012; Blair et al., 2018), gender of participants was used as the primary moderator, anticipating that the correlations might be stronger in women given their lower rates of achieving orgasms. To allow the analyses to be sensitive to the demographic differences across samples, a number of study-level moderating variables were also extracted and examined. As sex drive and sexual performance vary with age (e.g., Gades et al., 2008; Twenge et al., 2017), orgasms might take on substantively different levels of salience for psychological and relationship health across the lifespan. Consequently, the average age within each sample was tested as a possible moderator, anticipating that orgasms might show stronger associations in older individuals. In addition, given the lower levels of sexual health found among individuals suffering from mental or physical disorders (e.g., Atarodi-Kashani et al., 2017; Chang et al., 2012), the type of population sampled within each study (i.e., clinical or nonclinical) was also examined as a moderator, anticipating that the associations would be stronger within clinical populations. Finally, to directly examine any potential publication bias, the publication status of each study (i.e., published or unpublished research) was examined as a possible moderator. If publication bias was present, we hypothesized that the association biases would therefore be stronger within the published literature.
Method
Selection of Records
A systematic literature search was conducted in accordance with PRISMA guidelines (Moher et al., 2009), using PsychINFO via OVID, PubMed, and Web of Science for records available through the end of February 2020. As the primary goal of the current review was to synthesize the research on orgasmic functioning, we specifically searched for records containing appropriate orgasm variables. As such, keywords representing orgasms included: orgasm, orgasm/ic frequency, orgasm/ic consistency, or orgasm/ic ability. To ensure that broader forms of sexual health were also represented, we also included the keyword of sexual satisfaction. Keywords representing individual functioning included: attachment, depression, distress, life satisfaction, loneliness, positive affect, negative affect, stress, well-being, or vitality. Keywords representing relationship functioning included: maintenance behavior, relationship conflict, relationship longevity, relationship quality, relationship satisfaction, relationship stability, and support. Records were evaluated if they contained at least one of the orgasm terms and at least one of the terms from the other search categories.
Inclusion and Exclusion Criteria
Records were eligible for inclusion in analyses based on the following criteria:
- (1)
- written in English, Spanish, or Polish;
- (2)
- consisted of human participants only;
- (3)
- contained independent samples (i.e., providing effects within a group of participants that have not been previously published in other articles out of that sample);
- (4)
- included a measure of orgasms (i.e., orgasm consistency, difficulty, frequency, or general ability/inability to have an orgasm) resulting from sexual intercourse;
- (5)
- included a measure of individual functioning (i.e., attachment, depression, distress, life satisfaction, loneliness, psychological well-being, negative affect, stress, well-being, vitality) or relationship functioning (i.e., maintenance behavior, relationship conflict, relationship longevity, relationship quality, relationship satisfaction, relationship stability, sexual satisfaction, support);
- (6)
- provided statistical indices of the association between orgasms and individual or relationship functioning within the record (if relevant variables were measured but an effect of their association was not reported, authors of the record were contacted via repeated emails in an attempt to collect the relevant statistic);
- (7)
- reported an effect size specifically either in the form of a Pearson’s r correlation coefficient, a standardized regression coefficient, or other statistical value from which a Pearson’s r correlation coefficient or standardized regression coefficient could be computed (e.g., a 2 by 2 chi-squared, a Cohen’s d; see Method Statistical Analyses for transformation formulas used).
Following these criteria, the initial database searches (of PsychINFO via OVID, PubMed, and Web of Science) yielded a total of 2,464 unique records that were screened for eligibility based on their titles and abstracts (see Figure 3 for a PRISMA diagram). In order to maximize inclusion of unpublished records, Google Scholar was used to conduct a comprehensive reverse citation on some of the most relevant and highly cited articles (included in the current meta-analysis) and on 3 relevant review articles (Brody, 2010; Levin, 2007; Meston et al., 2004b). This yielded another 750 records for a total of 3,119 unique records. Screening of the titles and abstracts of those records yielded 1,012 full-text articles that were screened by both authors, yielding a final set of 173 unique records representing 205 independently analyzed (sub)samples.
Data Extraction and Coding Procedure
A coding procedure was developed to extract relevant information from each study, including record level- and sample level-characteristics. Record level-characteristics included: record authors, year of publication, record title, journal, and record type (i.e., published and peer-reviewed article, dissertation, thesis, or book chapter). Sample level-characteristics included: sample size for each specific effect extracted, mean age of participants, percentage of male participants, percentage of Caucasian participants, percentage of married participants, country of sample population, and whether the sample was clinical or community based. Effects representing bi-variate associations among the six dimensions of sexual health were extracted whenever possible, as were bi-variate associations between the dimensions of sexual health and the six correlates (psychological distress, psychological well-being, physical health, relationship satisfaction, attachment avoidance, and attachment anxiety). Given the possibility that gender might moderate the associations between aspects of sexual health and well-being, we extracted separate effects for men and women whenever possible, thereby treating male and female respondents as distinct subsamples within the records presenting results by gender. Similarly, as the links between sexual health and individual functioning might differ within clinical and nonclinical populations, we extracted separate effects for those two populations whenever possible. We therefore use the term (sub)samples to refer to the resulting 205 distinct samples identified within the 173 records as some of those represent the full sample of a record and others represent subsamples. For a comprehensive overview of (sub)sample characteristics, see Table 1.
All extracted effects were evaluated for directionality to ensure that they were coded in appropriate directions. In the two records that offered similar correlational effects for two separate orgasm dimensions (orgasm consistency and frequency; Hurlbert et al., 1993; Klapilova et al., 2015), the two effects were averaged to prevent overrepresentation of those samples in the resulting meta-analyzed effects. The data extraction process was conducted and checked independently by both authors. Discrepancies were rare (< 1%) and were resolved through discussion until a consensus could be reached. A total of 930 relevant effects were extracted from the 205 (sub)samples.
Classification of Variable Domains
Classification of Sexual Health. Sexual health dimensions consisted of sexual satisfaction, orgasms, sexual desire, lack of pain, lubrication, and erectile function, and were most commonly measured using (1) the Female Sexual Function Index (FSFI-S; Rosen et al., 2000; used in 40% of the records), (2) single items developed for each study (used in 23% of the records), or (3) the International Index of Erectile Function (IIEF; Rosen et al., 1997; used in 8% of the records) with the remaining 29% of studies using a method of assessment unique to each study.
Sexual satisfaction was defined as a general satisfaction with sexual activity and overall sexual life (e.g., “How satisfied have you been with your sexual relationship with your partner?”). Orgasms were operationalized as a general ability to experience orgasms (i.e., group contrast between people who have had at least one orgasm from people who have not; e.g., “Within the past 12 months, have you been unable to achieve orgasms?”), consistency of orgasms (i.e., percentage or proportion of sexual encounters resulting in orgasms; e.g., “When you had sexual stimulation or intercourse, how often did you reach orgasm (climax)?”), or orgasm frequency (i.e., count of orgasms experienced during sexual encounters over a specific time frame; e.g., “On how many days in the last month did you orgasm during sexual activity?”). Sexual desire was conceptualized as a desire or interest in sexual activity (e.g., “How would you rate your level / degree of sexual desire or interest?”). Lack of pain was defined as lack of discomfort or pain during or following vaginal penetration (e.g., “How would you rate your level / degree of discomfort or pain during or following vaginal penetration”). Lubrication was defined as the ease and ability to become lubricated or maintain lubrication during sexual activity or intercourse (e.g., “How difficult was it to become lubricated (“wet”) during sexual activity or intercourse?”). Erectile function was conceptualized as the ability to become erect or maintain an erection during sexual activity or intercourse (e.g., “How often were you able to get an erection during sexual activity?”).
Classification of Correlates. As represented in Figure 1, the current literature review aimed to extract correlates representing key components of the EVSA and ASA models. Although we attempted to assess a broader range of correlates (including the relationship factors of negative conflict, social/emotional support, and relationship stability), only seven distinct correlate domains emerged as having been examined within the previous literature: (1) psychological distress, (2) psychological well-being, (3) physical health, (4) attachment anxiety, (5) attachment avoidance, (6) relationship satisfaction, and (7) sexual satisfaction. Although a majority of the (sub)samples used well-validated measures (see the most commonly used measures listed below), 26% of the (sub)samples used single items to assess these correlates.
Relationship Satisfaction. Relationship satisfaction was defined as a general satisfaction or happiness within a romantic relationship, reflecting its overall quality. This domain included a variety of variables fitting this definition, including relationship satisfaction, marital satisfaction, relationship quality, marital adjustment, and dyadic adjustment. Despite the range of construct names, these scales contained extremely similar item content (e.g., “How satisfied are you with your relationship?” “How rewarding was your relationship?” “How warm and comfortable was your relationship?”). The most common measure used to assess relationship satisfaction was the Relationship Assessment Scale (RAS; Hendrick et al., 1998).
Psychological Distress. Psychological distress was defined as a difficult or negative psychological experience. This domain therefore included the more specific constructs of: depressive symptoms (e.g., the Beck Depression Inventory; BDI; Beck, et al., 1996), psychological distress (e.g., the Mood and Anxiety Symptom Questionnaire; MASQ; Watson & Clark, 1991), anxiety (e.g., Hospital Anxiety and Depression Scale; HADS; Zigmond & Snaith, 1983), negative affect (e.g., the Positive and Negative Affect Schedule; PANAS; Watson et al., 1988), and stress (e.g., the Perceived Stress Scale; PSS; Cohen et al., 1983).
Psychological Well-Being. Psychological well-being was defined as an adaptive or positive psychological experience and therefore included the constructs of: vitality (e.g., the Short-Form Health Survey; SF-36; Ware & Sherbourne, 1992), positive affect (e.g., the PANAS; Watson et al., 1988), well-being or mental adjustment (e.g., Martin et al., 1995), quality of life (e.g., the Quality of Life scale; QOL; Heinrichs et al., 1984), and life satisfaction (e.g., the Satisfaction With Life Scale; SWLS; Diener et al., 1985).
Physical Health. Physical health was defined as the perceived overall quality of physical health (e.g., “My health is excellent”). Eight of the nine records reporting physical health as an orgasm correlate used the Short-Form Health Survey (6 records used the SF-36; Ware & Sherbourne, 1992; 2 records used the SF-12; Ware et al., 1996). The remaining records used the World Health Organization Quality of Life Assessment (WHOQoL; WHOQoL Group, 1998).
Attachment Anxiety and Avoidance. All records reporting attachment anxiety and avoidance as orgasm correlates used the Experiences in Close Relationships Questionnaire—Revised (ECR; Fraley et al., 2000).
Statistical Analyses
Transforming Effects. A majority of the records presented effects as correlations (75%). When both the orgasm experience and correlates were converted into group contrasts (creating an effect in the form of a chi-squared, 7% of effects), that effect was first converted into a 2x2 chi-squared with one degree of freedom (collapsing groups if necessary). That allowed the use of the following formula to transform those values into Pearson’s r correlations (see Rosenberg, 2010 for the k correction to the typical formula): r = sqrt(c2/nk), in which χ2 represents the chi-squared value, n represents the total number of participants used in the analysis, and k represents the ratio of proportions between groups (i.e., individuals able to achieve orgasms vs. individuals unable to achieve orgasms). When an odds ratio value was provided (4% of effects), the following formula was used to transform this value to a standardized regression coefficient: b = ln(OR). All effects presented as regression coefficients (11%) were transformed into correlations: rxy = bx*(SDx/SDy). When group means, standard deviations, and numbers of participants were provided (3% of effects), we computed a Cohen’s d and then transformed that into a Pearson’s r correlation coefficient: r = d/(d2 + a) where a = (n1 + n2)2/(n1n2).
Meta-Analytic Effect Analyses. Analyses were conducted using Rstudio v.1.1.453 (R Core Team, 2018) using the foreign and metafor packages (R Core Team, 2017; Viechtbauer, 2010). Given the wide variety of sample populations, sample sizes, measurement instruments, and study designs, we used random-effects models to estimate our meta-analytic effects (Borenstein et al., 2009; Cooper et al., 2009). I2 estimates were used to estimate levels of heterogeneity among effect sizes. Cochran’s Q estimates were used to quantify each sample’s weighted contribution to the meta-analysis (Cochran, 1954). All extracted effects in their forms as correlations were transformed to Fisher’s Z values and weighted by sample size before analysis. These effects were then meta-analyzed, and the results were subsequently transformed back into correlations for ease of interpretation (Lipsey & Wilson, 2001). Meta-analytic effects were interpreted using Cohen’s (1992) correlational effect size guidelines, with r = .10 indicating a small effect, r = .30 indicating a moderate effect, and r = .50 indicating a large effect. The presence of potential outliers was assessed using the influence.measures function, which calculates outlier diagnostics (e.g., studentized residuals, Cook’s distances, covariance ratios), and identifies individual effects that are disproportionally influential to the overall effect. These analyses identified a handful of outlying effects. However, as results from analyses with and without the outliers remined relatively unchanged and excluding outliers could introduce additional biases, all reported results were from analyses conducted including that handful of outlying effects.
Publication Bias.Funnel plot asymmetry tests were conducted to evaluate the possibility of publication bias in this set of records. Funnel plots were visually inspected for asymmetrical distribution of effects around the funnel plot. This distribution was further tested using Egger’s regression tests (Egger et al., 1997). If asymmetry was present, Duval and Tweedie’s trim and fill analyses were conducted to estimate the effect sizes that might have emerged without that bias (Duval & Tweedie, 2000). Publication bias was further examined using selection method analyses conducted in Rstudio with functions developed and validated by McShane and colleagues (2016). These analyses estimate the relative probability of a contradictory finding (i.e., non-significant or in the opposite direction) being included in the analysis in comparison to the probability of a consistent and significant finding being included. Thus, relative probabilities close to a value of 1.0 would suggest the presence of very little publication bias within the current sample, whereas relative probabilities much lower than 1.0 would suggest publication bias.
Incremental Prediction Analyses. To examine the unique links between the various aspects of sexual health and each correlate, path analyses were run on meta-analytic correlation matrices within Mplus 7.11. Although we had planned on including erectile function as a dimension of sexual health in these analyses, there were insufficient studies providing correlations with erectile functioning to create the necessary meta-analytic correlation matrices. This restricted our path analyses to sexual satisfaction and the four remaining sexual health components (orgasms, desire, lack of pain, and lubrication). Sexual satisfaction was typically assessed as a global positive evaluation of individuals’ sex lives, and therefore represents an overarching construct to which the other aspects of sexual health contribute. To recognize this within our path models, we allowed the other dimensions of sexual health to predict levels of sexual satisfaction (Figure 2). The correlates representing global functioning (distress, well-being, physical health, and relationship satisfaction) were then modeled as outcomes (Figure 2A), treating global sexual satisfaction as a mechanism linking the more specific components of sexual health to each correlate). The four more specific aspects of sexual health were also allowed to directly predict levels of the correlate, after controlling for: (1) their links to sexual satisfaction, (2) the link between sexual satisfaction and the correlate being examined, (3) the associations among those four more specific indices of sexual health, and (4) the unique predictive links of each of those four indices to the outcome. This allowed our models to estimate the unique predictive associations of each of those indices of sexual health. In contrast, the correlates of attachment anxiety and attachment avoidance were treated as predictors of both the four more focused aspects of sexual health as well as sexual satisfaction (which served as the outcome; Figure 2B). As the path models tested were fully saturated, they yielded perfect fit.
Moderator Analyses. Meta-regression (using mixed effects models to accommodate the heterogeneity of the records) was used to assess the degree to which participant gender, participant age, (sub)sample population (i.e., clinical vs. nonclinical), and publication type moderated the associations between aspects of sexual health and the individual and relationship functioning correlates examined. More specifically, we focused our moderation on associations between aspects of sexual health and the correlates with sufficient numbers of (sub)samples to support the analyses: (1) sexual satisfaction (to examine moderation of the contribution of more specific sexual health factors to overall evaluations of sexual well-being; k = 118), (2) psychological distress (k = 84), (3) psychological well-being (k = 20), and (4) relationship satisfaction (k = 51). The moderators were entered into the meta-regressions simultaneously, thereby serving as controls for one another so that the analysis evaluated their unique moderation of the meta-analytic effects.
Results
Overview of Records
Table 1 presents an overarching summary of the 205 (sub)samples yielding the effects for this meta-analysis. Table 2 then presents details on each of the 173 records yielding those (sub)samples to ground the systematic review.
Participant Characteristics. Given the orgasm gender gap (e.g., Frederick et al., 2018; Lomann et al., 2000), 70% (121) of the records and 65% (134) of the resulting (sub)samples were focused exclusively on examining sexual functioning within women (Table 1). This general trend was balanced by some large-scale records collecting data from both genders or exclusively from men, yielding data from 46,535 men (29% of the comprehensive sample of 160,466 unique respondents) for the current meta-analysis. The 205 (sub)samples included in the current meta-analysis were notably international in their scope as the (sub)samples represented 36 different countries (e.g., China, Italy, Poland, Portugal, Turkey). Thus, likely due to the international adoption of scales like the FSFI and the IIEF, the meta-analytic sample is reasonably globally representative, allowing the results to potentially generalize beyond just the United States and Western Europe. The sample was also reasonably diverse with 64% of respondents (within the 89% of the (sub)samples reporting ethnicity) identifying as Caucasian. Sample average ages ranged from 18 to 74 years old with a weighted average age of 38.9, suggesting that a majority of the respondents were in their 20s, 30s, 40s and 50s. Although 26 of the (sub)samples (13%) collected data from college students, the vast majority of the (sub)samples were drawn from community adults or clinical populations. Consistent with this, 75% of participants were cohabiting or married (within the 95 records reporting these statistics) and the sample average relationship lengths ranged from 1.4 to 34.1 years with a weighted mean of 13.8 years (within the 40 records reporting). Taken together, these results highlight a diverse international sample made up largely of young and middle-aged adults typically in long-term romantic relationships.
Record/Manuscript Characteristics. Although the 173 records primarily included articles published in peer-reviewed journals (k = 158, 91%), the comprehensive literature search also uncovered relevant unpublished doctoral dissertations (k = 11) and unpublished master’s theses (k = 4), which were included in the current meta-analyses to help defray the impact of possible publication bias (Table 2). Those records yielded 187 distinct (sub)samples from peer-reviewed articles and 18 (sub)samples from unpublished dissertations and theses (Table 1). In addition, for a majority of the records identified (80%), the correlations between orgasm constructs and well-being were incidental to the main focus of the papers, with the relevant correlations simply showing up in a study-wide correlation matrix without any associated results narrative. In fact, only 45 records (26%) had the words orgasm or sexual satisfaction in the title. Thus, for the vast majority of the records in this meta-analytic sample, the significance of the relevant correlations would likely have had little impact on the publication of those manuscripts.
The (sub)samples had been published across a 49-year span, with a majority of the (sub)samples (69%) having been published in the last 10 years (Table 1). The (sub)samples were a fairly even mix of community adults and adults within specific clinical populations. As seen in Table 1, the clinical (sub)samples represented a large variety of different clinical diagnoses (i.e., 33 distinct diagnoses, including: depression or anxiety, sexual dysfunction, cancer, menopause, and pregnancy). Most of the records included in this meta-analysis were cross-sectional in design (96%; see Table 2), and although eight records contained longitudinal designs, only two reported longitudinal effects between orgasms and relevant correlates such as sexual satisfaction or positive affect (i.e., Burleson et al., 2007; Gunst et al., 2017). Similarly, only five records collected data from both partners within a romantic relationship, and only three of those records (Gewirtz-Meydan & Finzi-Dottan, 2018; Jones et al., 2014; Klapilova, et al., 2015) analyzed the partner data dyadically with approaches like actor-partner interdependence modeling (APIM; e.g., Cook & Kenny, 2005).
Data Characteristics. A total of 930 distinct effects were extracted from the 205 (sub)samples, yielding large numbers of effects (ranging from 110 to 280) for the correlates of psychological distress and relationship satisfaction, and smaller numbers of effects (ranging from 25 to 66) for the correlates of well-being, physical health, attachment anxiety and avoidance (Table 1). Although the comprehensive search screened for the relationship processes of negative conflict behavior and social support as possible orgasm correlates, the searches failed to uncover any records having examined those associations. Given the lower rate of studies examining men’s sexual health, the literature search only uncovered 9 records demonstrating links between erectile functioning and the correlates examined. Finally, a majority of the subsamples (73%) operationalized orgasm experiences as orgasm consistency (e.g., proportion of times that sexual activity with a partner resulted in achieving an orgasm) due in large part to the widespread use of the FSFI and the IIEF across these literatures.
Meta-Analytic Correlations
The dimensions of sexual health (i.e., sexual satisfaction, orgasms, sexual desire, lack of pain, lubrication, erectile function) were positively associated with one another (r = .246 to .551, k = 8 to 115; see bottom of Table 3 for full results). As anticipated, higher levels on each of the dimensions of sexual health were associated with lower levels of psychological distress (r = -.248 to -.135, k = 9 to 84), higher psychological well-being (r = .212 to .376, k = 10 to 20), higher physical health (r = .269 to .370, k = 2 to 9), lower levels of attachment anxiety (r = -.242 to -.145, k = 2 to 9), lower levels of attachment avoidance (r = -.351 to -.124, k = 2 to 9), and higher relationship satisfaction. (r = .141 to .529, k = 10 to 51).
Meta-Analytic Path Analyses
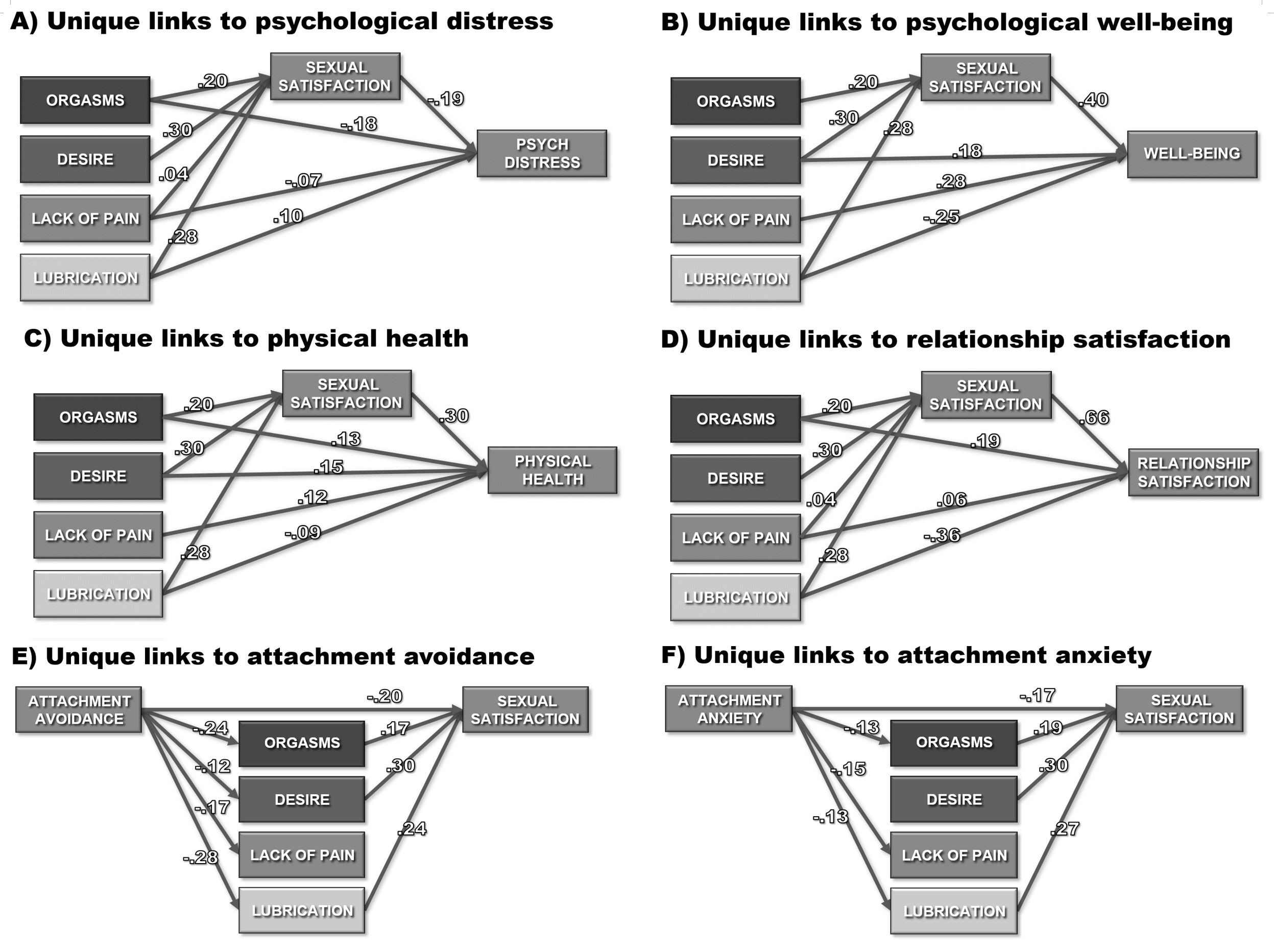
The meta-analytic estimates of the bivariate associations among the constructs being examined (from Table 3) were submitted as correlation matrices to Mplus to evaluate the unique predictive links between each aspect of sexual health and the individual and interpersonal correlates examined. Table 4 and Figure 4 present the standardized path coefficients generated by these models for each of the correlates. Offering partial support for Hypothesis 1, orgasms, sexual desire, and vaginal lubrication were each uniquely predictive of greater sexual satisfaction (Figure 4A-D) after controlling for their associations with one another. In contrast, lack of sexual pain yielded only a very weak and often non-significant association with sexual satisfaction after controlling for the other dimensions of sexual health. Consistent with Hypothesis 2, sexual satisfaction in turn, uniquely predicted lower psychological distress (Hypothesis 2A, Figure 4A), greater well-being (Hypothesis 2B, Figure 4B), better physical health (Hypothesis 2C, Figure 4C), and higher relationship satisfaction (Hypothesis 2D, Figure 4D), suggesting proximal associations with those indices of global functioning. Asymmetric confidence interval tests suggested significant indirect paths linking more focused components of sexual health to the correlates via higher sexual satisfaction (see Table 4), thereby offering partial support for Hypothesis 3. Thus, greater orgasms, sexual desire, and vaginal lubrication were indirectly linked to better functioning (lower distress and greater well-being, physical health, & relationship satisfaction) through their links to greater sexual satisfaction.
After controlling for those indirect associations, three of the specific aspects of sexual health (orgasms, desire, and lack of pain) demonstrated additional direct links to individual and relationship functioning in the expected directions, offering partial support for Hypothesis 4. Thus, even after controlling for sexual satisfaction and the other aspects of sexual health, greater orgasmic functioning was uniquely linked to three of those four correlates (lower psychological distress, greater physical health, and greater relationship satisfaction) further augmenting its indirect links to those outcomes via higher sexual satisfaction. Similarly, a lack of sexual pain was uniquely linked to slightly lower psychological distress, greater well-being, greater physical health, and slightly higher relationship satisfaction. Finally, sexual desire was uniquely linked to greater well-being and physical health. After controlling for the other aspects of sexual health as well as indirect links to functioning via sexual satisfaction, multivariate suppressor effects emerged for vaginal lubrication. Thus, higher levels of the residual aspects of vaginal lubrication that were completely independent of levels of orgasms, desire, and sexual satisfaction were linked to slightly greater psychological distress, and to slightly lower well-being, physical health, and relationship satisfaction.
Turning to the path models examining attachment insecurities as predictors of sexual health, attachment avoidance was linked to lower levels of all four specific aspects of sexual health (Figure 4E) and attachment anxiety was linked to lower orgasms, greater sexual pain, and lower vaginal lubrication (Figure 4F), offering partial support for Hypothesis 5. As seen in Table 4, asymmetric confidence interval tests revealed significant indirect links between attachment insecurities and lower sexual satisfaction via their links to lower levels of the more specific aspects of sexual health, offering partial support for Hypothesis 6. Even after controlling for those indirect links through specific aspects of sexual health, both attachment avoidance (Figure 4E) and attachment anxiety (Figure 4F) demonstrated additional direct links to lower sexual satisfaction, supporting Hypothesis 7. Taken as a set, these path analysis findings highlight the unique roles that various aspects of sexual health play in the lives of individuals.
Moderation Effects
Moderation analyses were conducted to estimate the moderating effects of gender, (sub)sample population (i.e., clinical vs. nonclinical), age, and publication type on the bivariate associations between specific aspects of sexual health and the three correlates to which sexual health was linked across at least 20 studies (offering sufficient numbers of effects to support these analyses): psychological distress, well-being, and relationship satisfaction. As the specific components of sexual health were conceptualized as contributing to overall sexual satisfaction, moderation analyses were also conducted on those predictive links. Given the broad range of samples, methods, and measures employed across the 205 (sub)samples, the Q statistics for the effects examined were significant, suggesting meaningful amounts of heterogeneity to support moderation analyses. Weighted random-effects meta-regression models were run using the metafor package in Rstudio to simultaneously test the unique effects of these four moderators on the links between orgasms and each of the outcomes. As shown in Table 5, when tested simultaneously, only a handful of significant moderation effects emerged from these analyses, thereby suggesting that a majority of the meta-analytic effects generalized across these moderators.
Moderation by Gender. Despite notable gender differences on orgasmic functioning and sexual desire between the primary genders, gender largely failed to emerge as a significant moderator for all but one of the effects tested. Gender only emerged as a unique moderator of links between orgasms and sexual satisfaction (b = -.172, p = .001). Thus, although orgasms are linked to higher satisfaction across both primary genders, this effect was predicted to be significantly stronger in women (b = .444) than in men (b = .444 − .172 = .272), suggesting that orgasmic functioning might be more salient for sexual satisfaction in women.
Moderation by Age. After controlling for the other moderators, average sample age emerged as a significant moderator of the links between orgasms and psychological distress (b = -.006, p = .007). As that predictor was centered at 38.9 years (the weighted mean across all samples), these results predict only a nominal association for samples with average ages of 18.9 (b = -.138 + (-20)*(-.006) = -.018) but a notably stronger association for samples with average ages of 58.9 (b = -.138 + (20)*(-.006) = -.258). Similarly, age significantly intensified the positive links between sexual desire and sexual satisfaction (b = .007, p = .040) as well as the positive links between lack of pain during sex and relationship satisfaction (b = .009, p = .010).
Moderation by Clinical vs. Non-Clinical Population. Population type emerged as a unique moderator of the links between orgasms and sexual satisfaction (b = .145, p = .001), such that the association was significantly stronger in samples drawn from clinical populations (b = .444 + .145 = .589) than from nonclinical populations (b = .444). This suggests that orgasmic functioning might take on particular salience for well-being in clinical populations. Population type also moderated the positive link between lack of pain during sex and well-being (b = -.344, p = .011), markedly reducing that positive association within a clinical population (b = .524 + -.344 = .180) in comparison to the effect in a non-clinical population (b = .524). This suggests that lack of pain during sex might be less directly related to well-being in a clinical population (potentially struggling with pain due to other medical conditions).
Publication Bias
As seen in Table 5, after controlling for the other moderators, publication status failed to emerge as a significant moderator of the links between specific aspects of sexual health and the constructs with sufficient numbers of effects to support meta-analytic regressions. This suggests that the 9 effects tested (for which publication status could be tested as a moderator) did not significantly differ between published peer-reviewed and unpublished research (sub)samples. Consistent with this, Egger’s regression tests only identified significant funnel plot asymmetry for 18 of the 44 effects (see Table 3) and the resulting shifts in meta-analytic effect sizes from trim and fill analyses were largely minimal. In fact, the trim and fill analyses yielded unchanged estimates for 3 of those 18 effects and stronger estimates for 14 of them. This is likely a consequence of 8.8% of the (sub)samples being drawn from unpublished sources. It is also likely due in part to the fact that in roughly 80% of the records, the relevant effects being extracted were incidental to the main focus of those manuscripts (typically appearing within a study-wide correlation matrix without ever being discussed). As a result, the significance of those effects would have had no effect on the publishing decisions for those articles. Taken together, these findings converge to suggest that minimal levels of publication bias were present in the meta-analyzed effects.
In contrast, the relative probabilities estimated by selection method analyses (e.g., McShane et al., 2016) provide a note of caution to those broader publication bias findings. The relative probability of a contradictory finding (e.g., non-significant or in the opposite direction) being included in the current review was roughly equivalent (if not greater) than the probability of a consistent finding being included for the correlates of psychological distress, attachment anxiety, and attachment avoidance (i.e., relative probabilities close to 1 or greater). However, the probabilities of contradictory findings being included for the remaining correlates were occasionally lower, suggesting that current meta-analytic effect estimates might have been slightly inflated by the publication (or inclusion) biases.
Discussion
As research studies from diverse fields have explored the potential benefits of experiencing orgasms and sexual health on physical, emotional, and interpersonal well-being across the last 49 years (often incidentally to the primary foci of those studies), this meta-analysis drew from clinical psychology, social psychology, and medical literatures to integrate that vast body of work. Thus, the current literature review resulted in a set of 173 records, yielding 205 (sub)samples and 930 effects, representing a combined total sample of 160,466 participants. Given the importance that individuals continue to place on orgasms (e.g., Opperman et al., 2014), our primary focus was to examine the links between orgasmic functioning and various indices of well-being. However, given the multivariate perspective on sexual functioning that has developed within the literature (e.g., Rosen et al., 2000), we took a broad perspective and examined orgasmic functioning as one component within the greater context of sexual health. Consistent with our modified EVSA and ASA models, the meta-analytic findings and subsequent path analyses revealed unique links from the various aspects of sexual health (i.e., sexual satisfaction, orgasms, sexual desire, lack of pain, vaginal lubrication, erectile function) to physical health, individual well-being and relationship well-being. Meta-analytic moderation results further revealed stronger links between orgasms and specific forms of well-being for: (1) women, (2) individuals from clinical populations, and (3) older individuals. As the first published meta-analysis in this area, the review sought to integrate findings from diverse fields of study within the EVSA and ASA conceptual frameworks, providing a clear focus to the review and frameworks to guide future work. The current study further offered a quantitative synthesis of the correlates of orgasms, which enabled us to markedly advance the literature by quantifying the unique associations of various aspects of sexual health with a range of individual and interpersonal correlates.
Implications
Promising Conceptual Frameworks. The focus of the current review was conceptually grounded in the EVSA and ASA models (i.e., seeking model-consistent correlates). Although the meta-analytic path models tested fell short of truly testing those more complex models, the current findings demonstrated robust links between sexual health and key constructs from those two models. Thus, the current findings offer a compelling foundation to support using the EVSA and ASA models as conceptual frameworks to guide future work in this area. For example, future studies of romantic relationships would likely benefit from modeling aspects of sexual health as adaptive processes, chronic sexual difficulties as enduring vulnerabilities, and/or failure to achieve orgasm as a stressor within the context of the EVSA model. Similarly, studies focused on the role of adult attachment insecurities could potentially benefit from modeling sexual health difficulties as possible threats that could trigger the activation of the attachment system within the context of the ASA model.
Sexual Health Benefits Relationships. Consistent with previous literature, current findings demonstrate that sexual health is linked to overall relationship quality (e.g., Brezsnyak & Whisman, 2004; Costa & Brody, 2007; Ellsworth & Bailey, 2013; Peixoto & Nobre, 2015; Therrien & Brotto, 2016; Witting et al., 2008), highlighting the potential importance of sexual health within romantic relationships for both men and women. Although these findings provide a solid foundation for examining sexual health as a distinct relationship process that could influence relationship quality over time, given the cross-sectional nature of the vast majority of the studies reviewed, future work is needed to explore the direction of those associations. In fact, the EVSA and ASA models highlight a myriad of more specific relationship processes that have yet to be examined and modeled with sexual health (e.g., sexual communication, relationship conflict, partner responsiveness, social support, attributions for partner behavior, mindfulness, psychological flexibility, gratitude, demand-withdrawal, and hypervigilance). Although those relationship processes have yet to be examined in the context of sexual health, they are likely to interact with sexual health to shape the course of relationships. Thus, the conceptual frameworks organizing this review further highlight an array of promising directions for future work.
Sexual Health Benefits Individuals. Although sexual behavior is often a dyadic experience, current findings and previous literature suggest that the benefits of sexual health extend far beyond relationship functioning (e.g., Levin, 2007). For both men and women, sexual health appears to have important implications for individual functioning, (e.g., Brody, 2007; Costa & Brody, 2012; Fabre & Smith, 2012; Mernone el al., 2019; Stephenson and Meston, 2015). The current findings suggest that all six dimensions of sexual health are linked to lower psychological distress, higher psychological well-being, and greater physical health. In the case of the correlates of orgasmic functioning, this could be explained in part by findings that sexual activities, and orgasms even more so, release prolactin and oxytocin (e.g., Carmichael et al., 1987; Krüger et al., 2002; Leeners et al., 2013; Magon & Kalra, 2011; Meston et al., 2004a), hormones which have been shown to demonstrate calming satiation and stress relieving features in both men and women (e.g., Kikusui et al., 2006; Krüger et al., 2005; Levin, 2007; Smith & Wang, 2014; Uynas-Mober, 1998), Thus, it may be interesting and useful to explore the potential stress-buffering benefits of orgasms and other sexual health dimensions in future studies. In the context of the ASA model, healthy sexual functioning, as well as consistent and high-quality experiences of orgasms might also serve as buffers to prevent perceived threats from triggering the attachment system, thereby lowering the stress experienced by individuals with attachment anxieties. Similarly, within the EVSA model, pleasurable sexual experiences might actually serve as an adaptive relationship process that buffers relationships from the jagged edges of individuals’ personalities and from the adverse impact of stressful events, thereby promoting individual well-being by bolstering relationship quality. Future work could explore these various mechanisms linking sexual health and experiences of orgasms to greater individual health.
Orgasms Matter—Particularly to Women. Although positive links to orgasms are found for both men and women, it appears that they are especially salient for women. As existing literature highlights, women experience orgasms at notably lower rates than do men (e.g., Armstrong et al., 2012; Blair et al., 2018; Frederick et al., 2018; Wade, 2015; Wade et al., 2005). Furthermore, although both men and women experience orgasm sexual dysfunctions, men more typically experience premature or delayed orgasms, in contrast to the complete absence of orgasms that many women experience (e.g., Delavierre, 2008; Jannini & Lenzi, 2005). Such findings, in combination with the results of the current meta-analysis, suggest that as women experience less frequent orgasms, the links between orgasms and positive correlates might become especially crucial for them. Although not a focus of the current review, a related line of study has demonstrated that greater frequency of women’s orgasms is linked to pleasure focused sexual education received in childhood or adolescence (e.g., Brody & Weiss, 2010), highlighting possible points of intervention. Thus, future work could examine the more developmental predictors of both women and men developing the skills to have consistent and high-quality experiences of orgasms from pleasurable sexual activity.
Understanding Vaginal Lubrication. Consistent with our hypotheses, vaginal lubrication demonstrated: (1) positive bi-variate associations with the other aspects of sexual health, (2) adaptive bi-variate associations with the correlates (e.g., greater well-being, lower distress), (3) unique positive links to sexual satisfaction in the path models, and (3) corresponding indirect associations with lower distress, and with greater well-being, physical health, and relationship satisfaction in those same path models. However, after controlling for those indirect links, suppressor effects (see Maassen & Bakker, 2001) emerged in the remaining direct links from vaginal lubrication to those four correlates in the path models. Thus, the aspects of vaginal lubrication that were completely unrelated to orgasms, sexual desire, lack of pain during sex, and sexual satisfaction were associated with greater psychological distress, lower well-being, lower physical health, and lower relationship satisfaction. As these suppressor effects are based on residual variance, they should be interpreted with caution as they tend to be less stable and might not continue to emerge with a slightly different set of covariates (see Maassen & Bakker, 2001 for a discussion of suppressor effects). Having said that, these results suggest that being able to lubricate in the absence of sexual satisfaction or desire might serve as a marker for less traditional sexual attitudes (possibly reflecting a greater comfort and proclivity toward causal sex). Although links between vaginal lubrication and sociosexual orientation are yet to be investigated, having an unrestricted sociosexual orientation (i.e., being more embracing of casual sex) has been linked to lower relationship satisfaction and quality (e.g., Lamela et al., 2020; Urganci et al., 2021) whereas it has been linked to greater psychological well-being and lower psychological distress after engaging in casual sex (Vrangalova & Ong, 2014). Given that most effects were drawn from samples of individuals in romantic relationships, it may be possible that having unrestricted sociosexual orientation might have a negative effect on individual and relationship functioning as those individuals found themselves constrained by what were likely to be predominantly monogamous relationships. Thus, future research could explore this phenomenon and examine potential links between vaginal lubrication (and other aspects of sexual health) and sociosexual orientation.
Future Directions
While the current systematic review has unified findings from a diverse set of literature, it has also uncovered a number of areas for future work that have yet to be explored.
Theoretically Grounded Studies. Despite a large body of work supporting the current meta-analytic findings, much of that work was more pragmatic in nature (i.e., examining sexual functioning as a secondary outcome in studies of physical illness) than conceptually focused. Thus, the effects extracted from those studies were typically tangential or completely unrelated to the primary focus of the manuscripts and were often not even discussed within the results narratives. As a result, the current findings offer an important first step toward developing a theoretically grounded program of research in this area, highlighting the EVSA and ASA as potential conceptual frameworks for future studies and therefore suggesting a number of directions to be explored in future studies.
Examining Mediators.The mechanisms linking sexual health to relationship quality remain unclear. The EVSA model (see Figure 1A) suggests a host of potential adaptive processes that could be examined as possible mechanisms in future studies (e.g., sexual communication, relationship conflict, demand-withdraw behaviors, partner responsiveness, social support, attributions for partner behavior, mindfulness, and psychological flexibility). Given the atheoretical nature of the vast majority of the research on sexual health, the links between sexual health and these relevant relationship processes have yet to be examined, much less treated as possible mechanisms within larger models of relationship functioning. Future studies could therefore conceptually extend this work by examining models and specific constructs or processes informed by the EVSA or ASA models. For example, positive, consistent, and high-quality sexual experiences might strengthen romantic relationship quality by promoting more compassion, responsiveness, and emotional support within those relationships. Of course, such experiences could even be modeled as a mechanism. For example, a future study could examine how an enduring vulnerability like negative body image might adversely impact romantic relationship quality by lowering the quality and consistency of pleasurable sexual experiences. The EVSA model therefore provides a framework for integrating the correlational findings on orgasms into a variety of conceptual models to be tested.
Biological Mechanisms.Although somewhat outside of the scope of the current review, a growing body of work has uncovered possible neurochemical mechanisms linking orgasms to emotional bonding. Thus, studies have shown that around the time of orgasm, there is a cascade of changes in cerebral blood flow in the brain including deactivation in left prefrontal cortex and left temporal lobe (e.g., Gerorgiadis et al., 2009; Georgiadis & Kringelbach, 2012; Holstege & Huynh, 2011; Levin, 2014), as well as activation in the cerebellum (Gerorgiadis et al., 2009; Holstege & Huynh, 2011; Meston et al., 2004a; Levin, 2014), right prefrontal cortex (Holstege & Huynh, 2011; Tiihonen et al., 1994), and hypothalamus (Komisaruk & Whipple, 2005; Meston et al., 2004a; Meston et al., 2004b). Specifically, activation in the hypothalamus results in the release of oxytocin, referred to as the “feel good hormone” which facilitates social bonding in both men and women (e.g., Carmichael et al., 1987; Carter, 1992; Murphy et al., 1990; Murphy et al., 1987; Ogawa et al., 1980; Pickering, 2003; Uvnas-Mober, 1998). Since evidence suggests that oxytocin is fundamental in bonding, this could help explain how couples who have orgasms together feel closer. Thus, in addition to process-oriented models examining psychological and interpersonal processes as mechanisms, future work could extend the current findings by also clarifying and quantifying the biological links between sexual health and well-being.
Examining Moderation. Another conceptual possibility suggested by both the EVSA and ASA models is that sexual health might function as a moderator within models of relationship and individual functioning. For example, drawing from the EVSA model (Figure 1A), a future study could examine how experiencing consistent and high-quality orgasms or pleasurable sexual activity (as a dynamic state-like process) might serve as an adaptive relationship process, buffering those relationships from the adverse effects of enduring vulnerabilities and stressful life events. Of course, more pervasive sexual health difficulties (e.g., chronic sexual pain, chronic difficulties with lubrication/erection, or being completely anorgasmic at the more stable trait-level) could be conceptualized as an enduring vulnerability that could create stress within the relationship and could shape the tone of other dyadic processes (i.e., moderating the impact of conflict and support behaviors). Drawing from the ASA model (Figure 1B), future studies might examine how experiencing consistent and high-quality orgasms, or pleasurable sexual activity, might buffer individuals from perceived threats triggering or activating their attachment systems, thereby ameliorating the impact of attachment insecurities on relationship and individual functioning. Within that same framework, chronic and pervasive difficulties with sexual health could be expected to potentially make individuals more reactive to perceived threats, lowering the threshold for attachment system activation and prompting greater levels of deactivating (e.g., withdrawal, avoidance, denial) and/or hyperactivating (e.g., demand, rumination, hypervigilance) behaviors, particularly for individuals with greater levels of attachment insecurities. At more of a dynamic state or event level, having negative sexual experiences or sexual health difficulties during a specific intimate encounter could serve as a threat to the relationship within the ASA framework, triggering hyperactivating and/or deactivating behaviors by activating an individual’s attachment insecurities. Extending that logic back to the EVSA framework, future studies could even explore how the quality of sexual health and/or consistency of pleasurable sexual experiences might interact with other relationship processes (e.g., conflict, support, responsiveness) to help shape the course of romantic relationships over time.
Examining Predictors of Sexual Health. Finally, the EVSA model sheds light on how more stable and enduring aspects of individuals can be incorporated into comprehensive models of functioning in future studies. Although the current review focused on attachment insecurities as the only enduring vulnerability examined, previous work has examined a variety of predictors of sexual health including enduring traits like sexual education (e.g., Farnam et al., 2008; Brody & Weiss, 2010), negative body image (e.g., Dosch et al., 2016; Quinn-Nilas et al., 2016), knowledge of own body (e.g., Wade et al., 2005), and sexual attitudes like erotophilia (e.g., Hangen & Rogge, 2021; Hurlbert et al., 1993), sociosexual orientation (e.g., Stern et al., 2020; Velten & Margraf, 2017; Wongsomboon et al., 2019), and sexual sensation seeking (e.g., Burri, 2017). The EVSA conceptual framework therefore offers researchers a method of integrating those predictive links to sexual health into broader models of individual and relationship functioning. Future studies could therefore build on the current findings and the broader predictive findings within the sexual health literature by expanding beyond just running analyses to sexual health. Specifically, future studies could examine how a broad array of enduring vulnerabilities might not only (1) predict the quality of sexual health and consistency of pleasurable sex or orgasms, but also (2) might generate stressful events for couples to navigate, and (3) interact with stressful life events to influence both sexual health and other relationship processes to shape the course of relationships over time.
Tracking the Impact of Sexual Health Over Time. While much research has been conducted on sexual health dimensions and its correlates, the vast majority of this work (96% of the records) has been cross-sectional (with none of the records predicting residual change to ensure that baseline associations would not inflate prediction) leaving the directions of causality unclear. Longitudinal research would greatly inform this field of study. Specifically, analyses in multi-wave longitudinal designs could clarify directions of associations. These designs could include short-term intensive studies such as daily diaries or ecological momentary assessments to examine immediate and daily effects of sexual health dimensions. Previous findings within a daily diary study of 96 couples have suggested that sexual activity leaves a lingering “afterglow” of positive effect on sexual and marital satisfaction for roughly 48 hours (Meltzer et al., 2017). In one of the few records to examine orgasms on daily basis, Burleson and colleagues (2007) collected 36 weeks of daily diary assessments from 58 women. Their lagged analyses supported reciprocal links between orgasming and positive mood even after controlling for rates of intercourse and physical affection, thereby providing initial evidence of bi-directional causality for those two constructs. Future work could examine the daily correlates of sexual health dimensions with the full range of correlates examined in this meta-analysis as most of those links remain largely unexamined. Future work could also extend the timeframe of diary assessments by using weekly diaries, potentially capturing slightly more lasting effects on relationship and individual functioning. In addition to tracking daily or weekly correlates of sexual health dimensions, long term designs (e.g., spanning months or years) could also prove informative for examining how this aspect of a couple’s sexual relationship might interact with other relationship processes over the broader course of romantic relationships. For example, it would be interesting to track sexual behavior and orgasms along with other common relationship processes (e.g., social support, negative conflict behavior, forgiveness, aggression) in newlywed couples over the first few years of marriage. As a small but growing body of studies have demonstrated that sexual activity and orgasms offer unique predictive variance (e.g., Costa & Brody, 2007), it is likely that they could play unique roles across the early years of marriage. Thus, a newlywed couple engaging in high levels of sexual activity in which one of the partners experiences a low rate of sexual satisfaction, desire, or orgasms could very well have a very different trajectory of marital functioning than a couple engaging in lower levels of activity but with a far higher satisfaction, desire, or orgasm rate as a result of those activities. This example highlights how orgasms and other aspects of sexual health might serve to moderate or interact with other relationship processes like sexual activity, physical affection, emotional support and even conflict behavior. As a result, such studies would help clarify the impact of possible sexual health gaps on relationship functioning during that high-risk stage of early marriage.
Examining Orgasm Specificity. A series of studies (e.g., Brody, 2010; Brody & Costa, 2009) has focused on emphasizing the distinct differences between types of orgasms (i.e., vaginal orgasms without clitoral stimulation compared to orgasms with clitoral stimulation) and their sources (i.e., through penile-vaginal intercourse (PVI), partnered masturbation, or solitary masturbation). For example, some findings have suggested that PVI frequency may be a stronger predictor of greater sexual satisfaction, relationship satisfaction, mental health, and life satisfaction (e.g., Body and Costa, 2009). Similarly, orgasms from PVI without clitoral stimulation have shown strong links to greater positive affect (e.g., Tavares et al., 2017). However, these studies have been criticized for potential deficits in: scientific rigor, theoretical grounding, and replication by independent researchers (Levin, 2007, 2012a; Prause, 2012a, 2012b; Therrien & Brotto, 2016). The emphasis on distinguishing between type of orgasms has also been criticized as lacking utility given that the clitoral structure envelops the vaginal opening, and is therefore not only stimulated via PVI regardless of direct stimulation of the clitoral glans, but also the resulting orgasms are largely indistinguishable for most women (e.g., Levin, 2007, 2012b; Prause, 2012). The exclusive focus on PVI within this line of work also excludes the study of sexual health in sexual and gender minority groups. Given these concerns, the vast majority of the research in this area has yet to fully explore this specificity. Consequently, there were too few published results to support the estimation of meta-analytic effects for specific types or sources of orgasms. Future research could continue to explore the potential specificity of benefits from various types of orgasms from various forms of sexual activity. However, given the critiques of the early work in this area, future studies should seek to use more rigorous methods (e.g., more comprehensively assessing sexual health), seek more diverse populations (e.g., expanding to include sexual and gender minorities), and ground those studies within larger conceptual frameworks.
Studying Sexual Health as a Dyadic Relationship Process. Most of the records reviewed examined sexual health within individuals, collecting data from just one individual from each relationship for the individuals in relationships. When records do include partner data, analyses are typically examined for actor (i.e., within-person) effects, rather than examining how one partner’s experiences may affect the other partner’s experiences (i.e., partner effects). This primarily conceptualizes sexual health as a predominantly individual experience. However, as sexual health dimensions are often part of sexual activity with another person, and much of that sexual activity occurs within the context of romantic relationships, it is reasonable to propose that having satisfying and painless sex or orgasms (or unsatisfying or painful sex without orgasms) within a sexual coupling could very likely have a meaningful impact on the romantic or sexual partner in that couple. In fact, sexual activity with another person can be an emotionally charged experience (e.g., Fahs & Plante, 2017; Salamon et al., 2005), laden with expectations from both partners (e.g., Aubrey et al., 2003) and offering the possibility of intense intimacy (e.g., Gewirtz-Meydan & Finzi-Dottan, 2018). Any failures to meet those expectations or achieve fulfilling pleasure could therefore be troubling to one or both partners in that sexual coupling. Thus, by conceptualizing sexual health as a dyadic relationship process, relationship research could capture the dynamics of what can be an extremely intense experience within models of relationship functioning. It will also allow researchers to explore links between sexual health and other relationship processes, such as support, conflict, or even intimate partner violence.
One of the meta-analyzed records moved the examination of orgasms closer to a dyadic level by demonstrating links between simultaneous orgasms and relationship quality for both men and women (Brody & Weiss, 2010). Similarly, another recent survey of 38,747 heterosexual men and women in 3+ year relationships from the United States shifted the focus toward the dyadic nature of orgasms by showing positive ties between an individual’s reports of their partner’s orgasm consistency and that individual’s own sexual satisfaction (Frederick et al., 2017). Notably, those pseudo-partner effects (pseudo, as they are still only reported by a single individual) remained significant even after controlling for sexual activity and sexual communication. Although both of those records take important steps toward recognizing the dyadic nature of orgasms during sexual activity with a sexual/romantic partner, they were both limited by collecting data from only one individual in each relationship.
Within the current systematic review, only five records examined the links between sexual health dimensions and relationship functions by specifically collecting data from both romantic partners (Frederick et al., 2017; Gewirtz-Meydan & Finzi-Dottan, 2018; Guo et al., 2004; Jones et al., 2014; Klapilova et al., 2015). However, of these five records, only three (Gewirtz-Meydan & Finzi-Dottan, 2018; Jones et al., 2014; Klapilova, et al., 2015) analyzed the partner data dyadically (i.e., actor-partner interdependence modeling, APIM; e.g., Cook & Kenny, 2005). For example, analyses in a sample of 128 Israeli heterosexual couples, Gewirtz-Meydan and Finzi-Dottan (2018) demonstrated that individuals’ orgasmic consistencies were linked to higher sexual satisfaction (and lower attachment insecurities) for those individuals and their partners. Future work could advance our understanding of the salience of sexual health in the lives of couples by taking a similarly dyadic approach to studying it.
Investigating Sexual Health as a Developmental Process. Given the cross-sectional and largely incidental nature of the research linking sexual health to well-being, this work has been fairly atheoretical in its approach, often focusing on practical questions within clinical populations (e.g., to what extent is chronic pelvic pain linked to depressive symptoms and reduced orgasms; Aubin et al., 2008) rather than developing testable theories. However, given the central role that sexual activity and sexual health can play in peoples’ lives and in their relationships, the current findings begin to suggest that various aspects of sexual health (i.e., learning about and growing comfortable with our bodies, embracing our sexual desires, exploring intimate activity, learning to communicate sexual needs, and developing the ability to have orgasms) could be conceptualized as a fundamental skills to be obtained as individuals become sexually active. Many records included in the current meta-analysis have measured orgasms as an ability/inability to have orgasms (e.g., Barrientos & Páez, 2006; Davidson & Hoffman, 1986; Haavio-Mannila & Kontula, 1997; Zhang et al., 2015). Records like these have identified a population of women in their 40’s, 50’s, and 60’s who have never experienced orgasms despite engaging in sexual activity (e.g., Fabre et al., 2013; Zhang et al., 2015), illustrating that some women have not and may never experience orgasms. Although biological issues might prevent some women from being able to experience orgasms or even pleasurable sex in general, for many women, sexual health difficulties could simply arise from a lack of knowledge of and comfort with their own bodies, and the associated skills needed to embrace sexual desire, communicate sexual needs, or achieve orgasms (either alone or during sexual activity with a partner). Thus, while many women are able to quickly learn those skills across their early sexual experiences, for many others, these skills might take years or decades after a sexual debut to acquire, delaying their abilities to achieve consistent, reliable, and satisfying sexual pleasure. Given the findings that childhood and adolescent sexual education can influence the achievement of these skills (e.g., Brody & Weiss, 2010), it is possible that sexual health functioning could be considered a developmental process beginning in adolescence and extending through young adulthood and beyond. This process would not only include the physical development and sexual maturation of individuals’ bodies, but also the cognitive and emotional development of those individuals as they develop and embrace their own sexual identities, grow to know their own bodies, develop comfort and understanding of their own sexual interests and needs, establish their own sexual attitudes, and develop schemas and scripts for how sex fits into their lives and into their relationships. Although researchers have briefly commented on these ideas in previous work (e.g., Chatterji et al., 2017; Giordano & Rush, 2010; Laan & Rellini, 2011), this remains a largely unexamined area of research on sexual health, and especially orgasms. We would posit that these developmental factors will influence the quality of an individual’s sexual health both within and outside of committed relationships, most likely serving as enduring vulnerabilities and adaptive processes within the EVSA model. Thus, future work could take a more developmental and holistic perspective by assessing these various developmental processes over time appropriate developmental timeframes (e.g., during those formative years in adolescence) to place an individual’s current experience of sexual health functioning within a larger socio-emotional developmental context. Models based on such a developmental approach would likely offer novel insights to individual functioning across the lifespan.
Linking Sexual and Physical Health. The comprehensive review uncovered 9 previous studies linking orgasms to improved physical health. For example, analyses in a sample of 117 Turkish women linked sexual satisfaction, desire, lack of pain, vaginal lubrication, and consistency of orgasms to greater physical health on the SF-36 (Artune-Ulkumen et al., 2014). Similarly, analyses in 76 Dutch women with a history of vulvar cancer and radiotherapy, the same sexual health dimensions were linked to greater physical health (Hazewinkel et al., 2012). Another study has linked men’s sexual intercourse frequency to greater longevity (Palmore, 1982). Extending these studies, analyses in 143 Scottish men and women demonstrated a link between orgasms and greater resting heart rate variability, an indicator which is indicative of not only better mental health and emotion regulation, but also greater physical health and longevity (Costa & Brody, 2012), thereby highlighting a possible mechanism for the current findings. Although the path models tested in the current review conceptualized sexual health predicting physical health, it is likely that those forms of health are reciprocally related. In fact, in the case of chronic illness, it is more likely that physical health might function as the causal factor reducing the quality of sexual health and functioning over time. Future work could therefore extend the current findings by examining links between physical and sexual health in multi-wave longitudinal studies, thereby allowing those reciprocal directions of causality to be modeled. Future work could further extend the current body of work by examining the links between sexual health dimensions and other more concrete daily health outcomes, such as the number of colds, visits to a physician, and missed days at work, thereby extending these findings to nonclinical populations.
Embracing Relationship and Sexual Orientation Diversity. As most records in the current meta-analysis have only looked at heterosexual respondents, and presume monogamous relationship structures, it is difficult to ascertain whether these findings are applicable to sexual minorities or to those in non-monogamous relationships. Although each of sexual health components are likely to be important for individuals of all sexual orientations and in all forms of relationships, we would posit that it is also possible that these findings may vary across those groups. Given findings highlighting possible differences in the frequencies of sexual activity and orgasms across gay and lesbian relationships (e.g., Frederick et al., 2018; Spitalnick & McNair, 2005), it is also possible that the salience of sexual activity and orgasms might take on unique meanings within specific populations. Consistent with this, another body of work on relationship diversity has explored the characteristics of individuals in fundamental classes of monogamous and nonmonogamous relationships (Hangen et al., 2019). Findings in a diverse sample of 1,658 adult men and women suggested that although certain forms of nonmonogamy demonstrated comparable levels of individual and relationship functioning to monogamous relationships, the individuals in nonmonogamous relationships reported markedly different sexual attitudes from individuals in more traditional monogamous relationships, reporting higher socio-sexual orientations (i.e., comfort with and interest in casual sex) and higher sexual sensation seeking. Thus, it is likely that each of the sexual health components might take on different salience in nonmonogamous relationships. To extend the current findings, future work would therefore benefit from seeking greater diversity in the populations sampled and examining the correlates of sexual health components in non-heterosexual individuals and within nonmonogamous relationships.
Examining Correlates of Exaggerating Sexual Pleasure. The sexual health gender gap continues to be well documented in the United States (e.g., Armstrong et al., 2012; Blair et al., 2018; Frederick et al., 2018; Regan & Atkins, 2006; Stephenson et al., 2011), suggesting that women generally experience orgasms and sexual desire at notably lower rates than men, as well as sexual pain at higher rates than men. Given the intense expectations that can surround partnered sexual activity, orgasm difficulties (particularly those in women) likely exert pressure on individuals to exaggerate their own pleasure or even fake their orgasms. This is most commonly done in an effort to protect the feelings of a sexual partner (e.g., Fahs, 2014; Muehlenhard & Shippee, 2010; Salisbury & Fisher, 2014), especially since greater amounts of sexual activity has been linked to lower relationship satisfaction for men whose female partners orgasm at low rates (Muehlenhard & Shippee, 2010). The phenomenon of exaggerating pleasure fell beyond the scope of the current meta-analysis, but it remains a closely related process to orgasm difficulties and a growing body of studies have investigated this phenomenon. Although both men and women have reported having exaggerated pleasure or faked orgasms during intercourse, this appears to be much more prevalent in women than in men (e.g., Muehlenhard & Shippee, 2010). In one of the first published records to link faking orgasms to relationship functioning, Ellsworth and Bailey (2013) found that greater frequency of women’s faking orgasms was linked to lower relationship satisfaction, fewer self-reported orgasms, and greater reports of past infidelity in current relationships, highlighting the potential risks of faking orgasms. Extending this work, a number of labs have developed scales to assess common reasons for faking orgasms (e.g., Cooper et al., 2014; Goodman et al., 2017; Seguin et al., 2015), as well as examining predictors of faking orgasms (e.g., Kaighobadi et al., 2012; Mialon, 2011), and the possible impacts of faking orgasms on romantic relationships (e.g., Denes et al., 2019). As the current meta-analytic findings highlight the correlates of orgasms across multiple domains of functioning, the current findings could be extended meaningfully in future studies by examining the associated phenomenon of faking orgasms and the motives underlying such behavior.
Conclusion
The current meta-analytic review was the first of its kind to quantitatively integrate 49 years of research examining the correlates of sexual health across a wide range of literatures. As the vast majority of that work was pragmatic rather than theoretically driven, the current review also sought to develop conceptual frameworks to theoretically integrate disparate lines of research into more comprehensive models of individual and relationship functioning. The meta-analytic results demonstrated links between sexual health components and physical, emotional, and relationship health and well-being, laying a foundation of support for the proposed models. The review also revealed a number of promising directions for future research: (1) examining mechanisms linking sexual health to individual and relationship functioning, (2) examining sexual health components as possible mediators and moderators with the EVSA and ASA models, (3) integrating predictors of sexual health as enduring traits within the EVSA model, (4) examining possible directions of casual influence using multi-wave longitudinal studies, (5) examining the specificity of various types and sources of orgasms, (6) collecting dyadic data to fully model sexual pleasure as a dyadic interpersonal process, (7) modeling sexual health and more specifically the ability to achieve orgasms as developmental processes involving a discrete set of skills and stages, (8) deepening our understanding of links between sexual and physical health, (9) embracing diversity in relationship commitment structures and sexual orientations, and (10) extending work on exaggerating pleasure or faking orgasms to hide orgasmic difficulties from a romantic or sexual partner. Thus, the current meta-analytic review not only synthesizes quantitative findings, but also offers concrete guidelines for extending the past 49 years of research on the correlates of sexual health in a theoretically grounded manner.
Data Availability Statement
The data used in the current analyses will be made available upon request via the osf.io platform.
References
- *Abdel-Hamid, I. A. , & Saleh, E. S. (2011). Primary lifelong delayed ejaculation: Characteristics and response to bupropion. Journal of Sexual Medicine. [CrossRef]
- *Abedi, P. , Afrazeh, M., Javadifar, N., & Saki, A. (2015). The relation between stress and sexual function and satisfaction in reproductive-age women in Iran: A cross-sectional study. Journal of Sex & Marital Therapy. [CrossRef]
- Abramov, L. A. (1976). Sexual life and sexual frigidity among women developing acute myocardial infarction. Psychosomatic Medicine, 38. [CrossRef]
- *Aerts, L. , Enzlin, P., Verhaeghe, J., Poppe, W., Vergote, I., & Amant, F. (2015). Sexual functioning in women after surgical treatment for endometrial cancer: A prospective controlled study. Journal of Sexual Medicine. [CrossRef]
- *Adam, F. , De Sutter, P., Day, J., & Grimm, E. (2020). A randomized study comparing video-based mindfulness-based cognitive therapy with video-based traditional cognitive behavioral therapy in a sample of women struggling to achieve orgasm. The Journal of Sexual Medicine. [CrossRef]
- *Alvisi, S., Baldassarre, M., Lambertini, M., Martelli, V., Berra, M., Moscatiello, S., Marchesini, G., Venturoli, S., & Meriggiola, M. C. (2014). Sexuality and psychopathological aspects in premenopausal women with metabolic syndrome. Journal of Sexual Medicine, 11, 2020–2028. [CrossRef]
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (5th ed.). American Psychiatric Association.
- Amicis, L. A. De, Goldberg, D. C., Lopiccolo, J., & Davies, L. (1984). Three-year follow-up of couples evaluated for sexual dysfunction. Journal of Sex & Marital Therapy. [CrossRef]
- *Appa, A. A. , Creasman, J., Brown, J. S., Van Den Eeden, S. K., Thom, D. H., Subak, L. L., & Huang, A. J. (2014). The impact of multimorbidity on sexual function in middle-aged and older women: Beyond the single disease perspective. Journal of Sexual Medicine. [CrossRef]
- Armstrong, E. A. , England, P., & Fogarty, A. C. K. (2012). Accounting for women’s orgasm and sexual enjoyment in college hookups and relationships. American Sociological Review. [CrossRef]
- *Artune-Ulkumen, B. , Erkan, M. M., Pala, H. G., & Bulbul, Y. B. (2014). Sexual dysfunction in Turkish women with dyspareunia and its impact on the quality of life. Clinical and Experimental Obstetrics & Gynecology. [CrossRef]
- *Asselmann, E. , Hoyer, J., Wittchen, H. U., & Martini, J. (2016). Sexual problems during pregnancy and after delivery among women with and without anxiety and depressive disorders prior to pregnancy: A prospective-longitudinal study. Journal of Sexual Medicine. [CrossRef]
- *Assimakopoulos, K. , Panayiotopoulos, S., Iconomou, G., Karaivazoglou, K., Matzaroglou, C., Vagenas, K., & Kalfarentzos, F. (2006). Assessing sexual function in obese women preparing for bariatric surgery. Obesity Surgery. [CrossRef]
- Atarodi-Kashani, Z. , Kariman, N., Ebadi, A., Majd, H. A., & Beladi-Moghadam, N. (2017). Sexual function and related factors in Iranian woman with epilepsy. Seizure: European Journal of Epilepsy. [CrossRef]
- *Atis, G. , Dalkilinc, A., Altuntas, Y., Atis, A., Gurbuz, C., Ofluoglu, Y., Cil, E., & Caskurlu, T. (2011). Hyperthyroidism: A risk factor for female sexual dysfunction. Journal of Sexual Medicine. [CrossRef]
- *Aubin, S., Berger, R., Heiman, J. R., & Ciol, M. (2008). The association between sexual function, pain, and psychological adaptation of men diagnosed with chronic pelvic pain syndrome type III. Journal of Sexual Medicine, 5, 657–667. [CrossRef]
- Aubrey, J. S. , Harrison, K., Kramer, L., & Yellin, J. (2003). Variety versus timing: Gender differences in college students’ sexual expectations as predicted by exposure to sexually oriented television. Communication Research. [CrossRef]
- *Bakhtiari, A., Basirat, Z., & Nasiri-Amiri, F. (2016). Sexual dysfunction in women undergoing fertility treatment in Iran: prevalence and associated risk factors. Journal of Reproduction & Infertility, 17, 26. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4769852/.
- *Barbara, G. , Pifarotti, P., Facchin, F., Cortinovis, I., Dridi, D., Ronchetti, C., Calzolari, L., & Vercellini, P. (2016). Impact of mode of delivery on female postpartum sexual functioning: Spontaneous vaginal delivery and operative vaginal delivery vs cesarean section. The Journal of Sexual Medicine. [CrossRef]
- *Barrientos, J. E. , & Páez, D. (2006). Psychosocial variables of sexual satisfaction in Chile. Journal of Sex & Marital Therapy. [CrossRef]
- *Battaglia, C., Battaglia, B., Mancini, F., Nappi, R. E., Paradisi, R., & Venturoli, S. (2011). Moderate alcohol intake, genital vascularization, and sexuality in young, healthy, eumenorrheic women. A pilot study. Journal of Sexual Medicine, 8, 2334–2343. [CrossRef]
- *Beaber, T. E., & Werner, P. D. (2009). The relationship between anxiety and sexual functioning in lesbians and heterosexual women. Journal of Homosexuality, 56, 639–654. [CrossRef]
- Beck, A.T. , Steer, R.A., & Brown, G.K. (1996). Manual for the Beck Depression Inventory-II. Psychological Corporation.
- *Berenguer, C. , Rebôlo, C., & Costa, R. M. (2019). Interoceptive awareness, alexithymia, and sexual function. Journal of Sex & Marital Therapy. [CrossRef]
- Berman, J. R. , Berman, L. A., Lin, H., Flaherty, E., Lahey, N., & Cantey-Kiser, J. (2011). Effect of sildenafil on subjective and physiologic parameters of the female sexual response in women with sexual arousal disorder. Journal of Sex & Marital Therapy. [CrossRef]
- *Blair, K. L. , Cappell, J., & Pukall, C. F. (2018). Not all orgasms were created equal: Differences in frequency and satisfaction of orgasm experiences by sexual activity in same-sex versus mixed-sex relationships. Journal of Sex Research. [CrossRef]
- Bodenmann, G., Atkins, D. C., Schär, M., & Poffet, V. (2010). The association between daily stress and sexual activity. Journal of Family Psychology, 24, 271–279. [CrossRef]
- Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to Meta-Analysis. John Wiley & Sons Ltd.
- *Borissova, A. M. , Kovatcheva, R., Shinkov, A., & Vukov, M. (2001). A study of the psychological status and sexuality in middle-aged Bulgarian women: Significance of the hormone replacement therapy (HRT). Maturitas. [CrossRef]
- Bouhlel, S. , Derbel, C. H., Nakhli, J., Bellazreg, F., Meriem, H. Ben, Omezzine, A., & Hadj, B. Ben. (2017). Sexual dysfunction in Tunisian patients living with HIV. Sexologies 26, e11–e16. [CrossRef]
- Bowlby, J. (1969/1982). Attachment and loss: Vol. 1. Attachment (2nd ed.). Basic Books.
- Bowlby, J. (1973). Attachment and loss: Vol. 2. Separation: Anxiety and anger. Basic Books.
- Bowlby, J. (1980). Attachment and loss: Vol. 3. Sadness and depression. Basic Books.
- Bowlby, J. (1988). A secure base: Clinical applications of attachment theory. Routledge.
- Brezsnyak, M. , & Whisman, M. A. (2004). Sexual desire and relationship functioning: The effects of marital satisfaction and power. Journal of Sex & Marital Therapy. [CrossRef]
- Brody, S. (2006). Penile—vaginal intercourse is better: Evidence trumps ideology. Sexual and Relationship Therapy. [CrossRef]
- Brody, S. (2007). Vaginal orgasm is associated with better psychological function. Sexual and Relationship Therapy. [CrossRef]
- Brody, S. (2010). The relative health benefits of different sexual activities. Journal of Sexual Medicine. [CrossRef]
- Brody, S. (2017). Evaluation of female orgasmic disorder. In W. W. Ishak (Ed.), Textbook of Clinical Sexual Medicine (pp. 203–218). Springer, Cham.
- Brody, S., & Costa, R. M. (2008). Vaginal orgasm is associated with less use of immature psychological defense mechanisms. Journal of Sexual Medicine, 5, 1167–1176. [CrossRef]
- Brody, S. , & Costa, R. M. (2009). Satisfaction (sexual, life, relationship, and mental health) is associated directly with penile-vaginal intercourse, but inversely with other sexual behavior frequencies. Journal of Sexual Medicine. [CrossRef]
- Brody, S. , Costa, R. M., Klapilová, K., & Weiss, P. (2018). Specifically penile-vaginal intercourse frequency is associated with better relationship satisfaction: A commentary on Hicks, McNulty, Meltzer, and Olson (2016). Psychological science. [CrossRef]
- Brody, S. , Houde, S., & Hess, U. (2010). Greater tactile sensitivity and less use of immature psychological defense mechanisms predict women’s penile-vaginal intercourse orgasm. Journal of Sexual Medicine. [CrossRef]
- Brody, S., & Weiss, P. (2010). Vaginal orgasm is associated with vaginal (not clitoral) sex education, focusing mental attention on vaginal sensations, intercourse duration, and a preference for a longer penis. Journal of Sexual Medicine, 7, 2774–2781. [CrossRef]
- *Brody, S. , & Weiss, P. (2011). Simultaneous penile-vaginal intercourse orgasm is associated with satisfaction (sexual, life, partnership, and mental health). Journal of Sexual Medicine. [CrossRef]
- Brotto, L. , Atallah, S., Johnson-Agbakwu, C., Rosenbaum, T., Abdo, C., Byers, E. S., Graham, C., Nobe, P., & Wylie, K. (2016). Psychological and interpersonal dimensions of sexual function and dysfunction. The journal of sexual medicine.
- Brotto, L. A., Heiman, J. R., Goff, B., Greer, B., Lentz, G. M., Swisher, E., Tamimi, H., & Van Blaricom, A. (2008). A Psychoeducational Intervention for Sexual Dysfunction in Women with Gynecologic Cancer. Archives of Sexual Behavior, 37, 317–329. [CrossRef]
- *Burleson, M. H. , Trevathan, W. R., & Todd, M. (2007). In the mood for love or vice versa? Exploring the relations among sexual activity, physical affection, affect, and stress in the daily lives of mid-aged women. Archives of Sexual Behavior. [CrossRef]
- Burri, A. (2017). Sexual sensation seeking, sexual compulsivity, and gender identity and its relationship with sexual functioning in a population sample of men and women. The Journal of Sexual Medicine.
- *Burri, A. , Hilpert, P., & Spector, T. (2015). Longitudinal evaluation of sexual function in a cohort of pre- and postmenopausal women. Journal of Sexual Medicine. [CrossRef]
- *Burri, A., Spector, T., & Rahman, Q. (2013). A discordant monozygotic twin approach to testing environmental influences on sexual dysfunction in women. Archives of Sexual Behavior, 42, 961–972. [CrossRef]
- *Cagnacci, A., Venier, M., Xholli, A., Paglietti, C., & Caruso, S. (2020). Female sexuality and vaginal health across the menopausal age. Menopause, 27, 14-19. [CrossRef]
- *Canat, M., Canat, L., Öztürk, F. Y., Eroğlu, H., Atalay, H. A., & Altuntaş, Y. (2016). Vitamin D 3 deficiency is associated with female sexual dysfunction in premenopausal women. International Urology and Nephrology, 48, 1789-1795. [CrossRef]
- *Carmen, R. A. (2014). Untangling the complexities of female sexuality: A mixed approach (Master’s thesis, State University of New York at New Paltz, New Paltz, New York). http://hdl.handle.net/1951/63469.
- Carmichael, M. S. , Humbert, R., Dixen, J., Palmisano, G., Greenleaf, W., & Davidson, J. M. (1987). Plasma oxytocin increases in the human sexual response. The Journal of Clinical Endocrinology & Metabolism. [CrossRef]
- *Carrobles, J. A., Guadix, M. G., & Almendros, C. (2011). Funcionamiento sexual, satisfacción sexual y bienestar psicológico y subjetivo en una muestra de mujeres españolas. Anales de Psicología/Annals of Psychology, 27, 27-34. https://revistas.um.es/analesps/article/view/113441.
- Carter, C. S. (1992). Oxytocin and sexual behavior. Neuroscience & Biobehavioral Reviews. [CrossRef]
- Caruso, S., Cicero, C., Romano, M., Presti, L. Lo, Ventura, B., & Malandrino, C. (2012). Tadalafil 5 mg daily treatment for type 1 diabetic premenopausal women affected by sexual genital arousal disorder. Journal of Sexual Medicine, 9, 2057–2065. [CrossRef]
- *Castellini, G., Mannucci, E., Mazzei, C., Lo Sauro, C., Faravelli, C., Rotella, C. M., Maggi, M., & Ricca, V. (2010). Sexual function in obese women with and without binge eating disorder. Journal of Sexual Medicine, 7, 3969–3978. [CrossRef]
- Celikel, E. , Ozel-kizil, E. T., Akbostanci, M. C., & Cevik, A. (2008). Assessment of sexual dysfunction in patients with Parkinson’s disease: A case–control study. European Journal of Neurology. [CrossRef]
- *Ceyhan, O. , Ozen, B., Simsek, N., & Dogan, A. (2019). Sexuality and marital adjustment in women with hypertension in Turkey: how culture affects sex. Journal of Human Hypertension. [CrossRef]
- Chadwick, S. B. , Francisco, M., & van Anders, S. M. (2019). When orgasms do not equal pleasure: Accounts of “bad” orgasm experiences during consensual sexual encounters. Archives of Sexual Behavior. [CrossRef]
- *Chang, S., Ho, H., Chen, K., Shyu, M., Huang, L., & Lin, W. (2012). Depressive symptoms as a predictor of sexual function during pregnancy. Journal of Sexual Medicine, 9, 2582–2589. [CrossRef]
- *Chang, S. R. , Yang, C. F., & Chen, K. H. (2019). Relationships between body image, sexual dysfunction, and health-related quality of life among middle-aged women: A cross-sectional study. Maturitas. [CrossRef]
- Chatterji, S. , Bay-Cheng, L. Y., Schick, V., Dodge, B., Baldwin, A., Van Der Pol, B., & Fortenberry, J. D. (2017). The year’s best: Interpersonal elements of bisexual women’s most satisfying sexual experiences in the past year. The Journal of Sex Research. [CrossRef]
- *Cheng, J. Y. W., Ng, E. M. L., & Ko, J. S. N. (2007). Depressive symptomatology and male sexual functions in late life. Journal of Affective Disorders, 104, 225–229. [CrossRef]
- *Chivers, M. L. , Pittini, R., Grigoriadis, S., Villegas, L., & Ross, L. E. (2011). The relationship between sexual functioning and depressive symptomatology in postpartum women: A pilot study. Journal of Sexual Medicine. [CrossRef]
- Ciftci, H., Savas, M., Gulum, M., Yeni, E., Verit, A., & Topal, U. (2011). Evaluation of sexual function in men with orchialgia. Archives of Sexual Behavior, 40, 631–634. [CrossRef]
- *Cohen, D. L. , & Belsky, J. (2008). Avoidant romantic attachment and female orgasm: Testing an emotion-regulation hypothesis. Attachment and Human Development. [CrossRef]
- Cohen, J. (1992). A Power Primer. Psychological Bulletin. [CrossRef]
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385-396. [CrossRef]
- Cochran, W. G. (1954). The combination of estimates from different experiments. Biometrics. [CrossRef]
- *Conroy, K. (2018). The relationship between sexual activity and sexual function in breast and gynecologic cancer patients during adjuvant chemotherapy (Master’s thesis, Ohio State University, Columbus, Ohio). http://hdl.handle.net/1811/84805.
- *Constantine, S. (2017). Women’s sexual fantasies in context: The emotional content of sexual fantasies, psychological and interpersonal distress, and satisfaction in romantic relationships (Doctoral dissertation, City University of New York, New York City, New York). https://academicworks.cuny.edu/gc_etds/2162.
- Cook, W. L., & Kenny, D. A. (2005). The actor–partner interdependence model: A model of bidirectional effects in developmental studies. International Journal of Behavioral Development, 29, 101-109. [CrossRef]
- Cooper, E. B. , Fenigstein, A., & Fauber, R. L. (2014). The faking orgasm scale for women: Psychometric properties. Archives of Sexual Behavior. [CrossRef]
- Cooper, H., Hedges, L. V., & Valentine, J. C. (2009). The handbook of research synthesis and meta-analysis (2nd ed). Russell Sage Foundation.
- *Costa, R. M. , & Brody, S. (2007). Women’s relationship quality is associated with specifically penile-vaginal intercourse orgasm and frequency. Journal of Sex & Marital Therapy. [CrossRef]
- *Costa, R. M., & Brody, S. (2011). Anxious and avoidant attachment, vibrator use, anal sex, and impaired vaginal orgasm. Journal of Sexual Medicine, 8, 2493–2500. [CrossRef]
- Costa, R. M. , & Brody, S. (2012a). Greater resting heart rate variability is associated with orgasms through penile–vaginal intercourse, but not with orgasms from other sources. The Journal of Sexual Medicine. [CrossRef]
- *Costa, R. M., Pestana, J., Costa, D., & Wittmann, M. (2016). Altered states of consciousness are related to higher sexual responsiveness. Consciousness and Cognition, 42, 135–141. [CrossRef]
- *Dashti, S., Latiff, L. A., Hamid, H. A., Sani, S. M., Akhtari-Zavare, M., Bakar, A., Sabiri, N. A., Ismail, M., & Esfehani, A. J. (2016). Sexual dysfunction in patients with polycystic ovary syndrome in Malaysia. Asian Pacific Journal of Cancer Prevention, 17, 3747-3751. http://journal.waocp.org/article_33048.html.
- *Davidson, J. K. , & Hoffman, L. E. (1986). Sexual fantasies and sexual satisfaction: An empirical analysis of erotic thought. The Journal of Sex Research. [CrossRef]
- Deci, E. L. , & Ryan, R. M. (2000). The ‘‘what’’ and ‘‘why’’ of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry, 11. [CrossRef]
- *de Jong, D. C. (2016). Validation of a measure of implicit sexual desire for romantic partners (Doctoral dissertation, University of Rochester, Rochester, New York). https://search.proquest.com/docview/1823257882?pq-origsite=gscholar.
- *de Lucena, B. B. , & Abdo, C. H. N. (2014). Personal factors that contribute to or impair women’s ability to achieve orgasm. International Journal of Impotence Research. [CrossRef]
- *de Oliveira Ferro, J. K. , Lemos, A., da Silva, C. P., de Paiva Lima, C. R. O., Raposo, M. C. F., de Aguiar Cavalcanti, G., & de Oliveira, D. A. (2019). Predictive Factors of Male Sexual Dysfunction After Traumatic Spinal Cord Injury. Spine. [CrossRef]
- Delavierre, D. (2008). Diagnosis of male anorgasmia. Progres en urologie: journal de l’Association francaise d’urologie et de la Societe francaise d’urologie, 18, F8-10. https://europepmc.org/article/med/18773846.
- *Demir, S. E., Rezvani, A., & Ok, S. (2013). Assessment of sexual functions in female patients with ankylosing spondylitis compared with healthy controls. Rheumatology International, 33, 57-63. [CrossRef]
- *Denes, A. (2012). Pillow talk: Exploring disclosures after sexual activity. Western Journal of Communication. [CrossRef]
- *Denes, A. (2018). Toward a post-sex disclosures model: Exploring the associations among orgasm, self-disclosure, and relationship satisfaction. Communication Research. [CrossRef]
- Denes, A. , Horan, S. M., & Bennett, M. (2019). “Faking it” and affectionate communication: Exploring the authenticity of orgasm and relational quality indicators. Personality and Individual Differences. [CrossRef]
- Derogatis, L. R. (1997). The Derogatis Interview for Sexual Functioning (DISF/DISF-SR): An introductory report. Journal of Sex & Marital Therapy, 23. [CrossRef]
- Derogatis, L. R. , & Melisaratos, N. (1979). The DSFI: A multidimensional measure of sexual functioning. Journal of Sex & Marital Therapy, 5. [CrossRef]
- *Dèttore, D. , Pucciarelli, M., & Santarnecchi, E. (2013). Anxiety and female sexual functioning: An empirical study. Journal of Sex & Marital Therapy. [CrossRef]
- Diener, E. D., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71-75. [CrossRef]
- *Dissiz, M. (2018). The effect of heroin use disorder on the sexual functions of women. Journal of Psychiatry and Neurological Sciences. [CrossRef]
- *Dogan, V. B., Dagdeviren, H., Dirican, A., Dirican, A. C., Tutar, N. K., Yayla, V. A., & Cengiz, H. (2017). Hormonal effect on the relationship between migraine and female sexual dysfunction. Neurological Sciences, 38, 1651–1655. [CrossRef]
- Dosch, A. , Ghisletta, P., & Van der Linden, M. (2016). Body image in dyadic and solitary sexual desire: The role of encoding style and distracting thoughts. The Journal of Sex Research. [CrossRef]
- Du, J. , Ruan, X., Gu, M., Bitzer, J., & Mueck, A. O. (2016). Prevalence of and risk factors for sexual dysfunction in young Chinese women according to the Female Sexual Function Index: An internet-based survey. European Journal of Contraception & Reproductive Health Care. [CrossRef]
- *Duits, A. , Van Oirschot, N., Van Oostenbrugge, R. J., & Van Lankveld, J. (2009). The relevance of sexual responsiveness to sexual function in male stroke patients. The Journal of Sexual Medicine. [CrossRef]
- *Dunkley, C. R. , Dang, S. S., Chang, S. C. H., & Gorzalka, B. B. (2016). Sexual functioning in young women and men: Role of attachment orientation. Journal of Sex and Marital Therapy. [CrossRef]
- *Dunn, K. M. , Croft, P. R., & Hackett, G. I. (1999). Association of sexual problems with social, psychological, and physical problems in men and women: a cross sectional population survey. Journal of Epidemiology & Community Health. [CrossRef]
- Duval, S. , & Tweedie, R. (2000). Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics. [CrossRef]
- *Dyar, C., Newcomb, M. E., Mustanski, B., & Whitton, S. W. (2019). A structural equation model of sexual satisfaction and relationship functioning among sexual and gender minority individuals assigned female at birth in diverse relationships. Archives of Sexual Behavior, online first, 1-18. [CrossRef]
- *Eaton, L., Kueck, A., Maksut, J., Gordon, L., Metersky, K., Miga, A., Brewer, M., Siembida, E., & Bradley, A. (2017). Sexual health, mental health, and beliefs about cancer treatments among women attending a gynecologic oncology clinic. Sexual Medicine, 5, e175-e183. [CrossRef]
- Egger, M. , Davey Smith, G., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. British Medical Journal. [CrossRef]
- *Eichel, E. W. , De Simone Eichel, J., & Kule, S. (1988). The technique of coital alignment and its relation to female orgasmic response and simultaneous orgasm. Journal of Sex and Marital Therapy. [CrossRef]
- *Ellero, J. (2019). Altered states of consciousness, absorption, and sexual responsiveness (Master’s thesis, ISPA—Instituto Universitário, Lisbon, Portugal). http://hdl.handle.net/10400.12/7173.
- *Ellsworth, R. M. , & Bailey, D. H. (2013). Human female orgasm as evolved signal: A test of two hypotheses. Archives of Sexual Behavior. [CrossRef]
- *Fabre, L. F. , Clayton, A. H., Smith, L. C., Goldstein, I. M., & Derogatis, L. R. (2013). Association of major depression with sexual dysfunction in men. Journal of Neuropsychiatry and Clinical Neurosciences 25, 308–318. [CrossRef]
- *Fabre, L. F. , & Smith, L. C. (2012). The effect of major depression on sexual function in women. Journal of Sexual Medicine 9, 231–239. [CrossRef]
- Fahs, B. (2014). Coming to power: Women’s fake orgasms and best orgasm experiences illuminate the failures of (hetero) sex and the pleasures of connection. Culture, Health & Sexuality. [CrossRef]
- Fahs, B. , & Plante, R. (2017). On ‘good sex’ and other dangerous ideas: women narrate their joyous and happy sexual encounters. Journal of Gender Studies. [CrossRef]
- *Fan, X. , Henderson, D. C., Chiang, E., Briggs, L. B. N., Freudenreich, O., Evins, A. E., Cather, C., & Goff, D. C. (2007). Sexual functioning, psychopathology and quality of life in patients with schizophrenia. Schizophrenia Research. [CrossRef]
- Farnam, F. , Pakgohar, M., Mirmohamadali, M., & Mahmoodi, M. (2008). Effect of sexual education on sexual health in Iran. Sex Education. [CrossRef]
- Feldman, J. , & Larsen, K. (2014). Sexual Dysfunction. In S. Richards & M. W. O’Hara (Eds.), Oxford Handbook of Depression and Comorbidity (pp. 218–235). Oxford University Press, Incorporated.
- Fisher, W. A. , Rosen, R. C., Eardley, I., Sand, M., & Goldstein, I. (2005). Sexual experience of female partners of men with erectile dysfunction: The female experience of men’s attitudes to life events and sexuality (FEMALES) study. Journal of Sexual Medicine. [CrossRef]
- Flynn, K. E. , Lin, L., Cyranowski, J. M., Reeve, B. B., Reese, J. B., Jeffery, D. D., Smith, A. W., Porter, L. S., Dombeck, C. B., Burner, D. W., Keefe, F. J., & Weinfurt, K. P. (2013). Development of the NIH PROMIS® sexual function and satisfaction measures in patients with cancer. Journal of Sexual Medicine. [CrossRef]
- *Forbes, M. K. , Baillie, A. J., & Schniering, C. A. (2016). Should sexual problems be included in the internalizing spectrum? A comparison of dimensional and categorical models. Journal of Sex & Marital Therapy. [CrossRef]
- Fragla, E. , Privitera, S., Giardina, R., Di Rosa, A., Russo, G. I., Favilla, V., Caramma, A., Patti, F., Cimino, S., & Morgia, G. (2014). Determinants of sexual impairment in multiple sclerosis in male and female patients with lower urinary tract dysfunction: Results from an Italian cross-sectional study. Journal of Sexual Medicine. [CrossRef]
- Fraley, R. C. , Waller, N. G., & Brennan, K. A. (2000). An item response theory analysis of self-report measures of adult attachment. Journal of Personality and Social Psychology. [CrossRef]
- *Frederick, D. A. , Lever, J., Gillespie, B. J., & Garcia, J. R. (2017). What keeps passion alive? Sexual satisfaction is associated with sexual communication, mood setting, sexual variety, oral sex, orgasm, and sex frequency in a national U.S. study. Journal of Sex Research. [CrossRef]
- Frederick, D. A. John, H. K. S., Garcia, J. R., & Lloyd, E. A. (2018). Differences in orgasm frequency among gay, lesbian, bisexual, and heterosexual men and women in a U.S. national sample. Archives of Sexual Behavior 47, 273–288. [CrossRef]
- Gades, N. M., Jacobson, D. J., McGree, M. E., Sauver, J. L. S., Lieber, M. M., Nehra, A., Girman, C. J., Klee, G. G., & Jacobsen, S. J. (2008). The associations between serum sex hormones, erectile function, and sex drive: the Olmsted County Study of Urinary Symptoms and Health Status among Men. The Journal of Sexual Medicine, 5, 2209-2220.
- Galinsky, A. M. (2012). Sexual touching and difficulties with sexual arousal and orgasm among U.S. older adults. Archives of Sexual Behavior. [CrossRef]
- *Gallup, G. G. , Ampel, B. C., Wedberg, N., & Pogosjan, A. (2014). Do orgasms give women feedback about mate choice? Evolutionary Psychology. [CrossRef]
- *Gracia, C. R. , Freeman, E. W., Sammel, M. D., Lin, H., & Mogul, M. (2007). Hormones and sexuality during transition to menopause. Obstetrics & Gynecology. [CrossRef]
- Georgiadis, J. R. , & Kringelbach, M. L. (2012). The human sexual response cycle: Brain imaging evidence linking sex to other pleasures. Progress in Neurobiology. [CrossRef]
- Georgiadis, J. R. , Reinders, A. S., Paans, A. M., Renken, R., & Kortekaas, R. (2009). Men versus women on sexual brain function: prominent differences during tactile genital stimulation, but not during orgasm. Human Brain Mapping. [CrossRef]
- *Gewirtz-Meydan, A. (2017). Why do narcissistic individuals engage in sex? Exploring sexual motives as a mediator for sexual satisfaction and function. Personality and Individual Differences. [CrossRef]
- *Gewirtz-Meydan, A. , & Finzi-Dottan, R. (2018). Sexual satisfaction among couples: The role of attachment orientation and sexual motives. The Journal of Sex Research. [CrossRef]
- Giordano, F. G. , & Rush, C. L. (2010). Self-esteem and sexuality: An exploration of differentiation and attachment. Self-esteem across the lifespan: Issues and interventions.
- *Gomes, A. L. Q. , & Nobre, P. (2012). The International Index of Erectile Function (IIEF-15): Psychometric properties of the Portuguese version. Journal of Sexual Medicine. [CrossRef]
- *Goodman, D. L. (2011). Associations of attachment style and reasons to pretend orgasm; development and validation of reasons to pretend orgasm measure in a relational context (Doctoral dissertation, University of Kansas, Lawrence, Kansas). http://hdl.handle.net/1808/13008.
- Goodman, D. L. , Gillath, O., & Haj-Mohamadi, P. (2017). Development and validation of the pretending orgasm reasons measure. Archives of Sexual Behavior 46, 1973–1991.
- Graham, C. A. (2014). Orgasm Disorders in Women. In Y. M. Binik & K. S. K. Hall (Eds.), Principles and Practice of Sex Therapy (5th ed., pp. 89–111). The Guildford Press.
- *Granata, A. , Tirabassi, G., Pugni, V., Arnaldi, G., Boscaro, M., Carani, C., & Balercia, G. (2013). Sexual dysfunctions in men affected by autoimmune Addison’s disease before and after short-term gluco-and mineralocorticoid replacement therapy. The Journal of Sexual Medicine. [CrossRef]
- *Grose, R. G. (2016). Critical consciousness and sexual pleasure: Evidence for a sexual empowerment process for heterosexual and sexual minority women (Doctoral dissertation, University of California, Santa Cruz, Santa Cruz, California). https://escholarship.org/uc/item/61r1d1sm.
- *Gunst, A. , Ventus, D., Kärnä, A., Salo, P., & Jern, P. (2017). Female sexual function varies over time and is dependent on partner-specific factors: A population-based longitudinal analysis of six sexual function domains. Psychological Medicine. [CrossRef]
- *Guo, Y. N. , Ng, E. M. L., & Chan, K. (2004). Foreplay, orgasm, and after-play among Shanghai couple and its integrative relation with their marital satisfaction. Sexual and Relationship Therapy. [CrossRef]
- *Gutsche, M. , & Burri, A. (2017). What women want—An explorative study on women’s attitudes toward sexuality boosting medication in a sample of Swiss women. Journal of Sexual Medicine. [CrossRef]
- *Haavio-Mannila, E. , & Kontula, O. (1997). Correlates of increased sexual satisfaction. Archives of Sexual Behavior 26, 399–419. [CrossRef]
- Hangen, F. , Crasta, D., & Rogge, R. D. (2019). Delineating the boundaries between nonmonogamy and infidelity: Bringing consent back into definitions of consensual nonmonogamy with latent profile analysis. The Journal of Sex Research. [CrossRef]
- Hangen, F. , & Rogge, R. D. (2021). Focusing the Conceptualization of Erotophilia and Erotophobia on Global Attitudes Toward Sex: Development and Validation of the Sex Positivity-Negativity Scale. Archives of Sexual Behavior. [CrossRef]
- *Harte, C. B. , & Meston, C. M. (2012). Recreational use of erectile dysfunction medications and its adverse effects on erectile function in young healthy men: the mediating role of confidence in erectile ability. The Journal of Sexual Medicine. [CrossRef]
- *Hassan, A. , El-Hadidy, M., El-Deeck, B. S., & Mostafa, T. (2008). Couple satisfaction to different therapeutic modalities for organic erectile dysfunction. The Journal of Sexual Medicine 5, 2381–2391. [CrossRef]
- *Hazewinkel, M. H. , Laan, E. T., Sprangers, M. A., Fons, G., Burger, M. P., & Roovers, J. P. W. (2012). Long-term sexual function in survivors of vulvar cancer: a cross-sectional study. Gynecologic Oncology. [CrossRef]
- Heinrichs, D. W. , Hanlon, T. E., & Carpenter Jr, W. T. (1984). The Quality of Life Scale: an instrument for rating the schizophrenic deficit syndrome. Schizophrenia Bulletin. [CrossRef]
- Hendrick, S. S. , Dicke, A., & Hendrick, C. (1998). The relationship assessment scale. Journal of Social and Personal Relationships 15, 137–142. [CrossRef]
- *Hevesi, K. , Gergely Hevesi, B., Kolba, T. N., & Rowland, D. L. (2019). Self-reported reasons for having difficulty reaching orgasm during partnered sex: relation to orgasmic pleasure. Journal of Psychosomatic Obstetrics & Gynecology. [CrossRef]
- *Hevesi, K. , Mészáros, V., Kövi, Z., Márki, G., & Szabó, M. (2017). Different characteristics of the Female Sexual Function Index in a sample of sexually active and inactive women. The Journal of Sexual Medicine 14, 1133–1141. [CrossRef]
- Holstege, G. , & Huynh, H. K. (2011). Brain circuits for mating behavior in cats and brain activations and de-activations during sexual stimulation and ejaculation and orgasm in humans. Hormones and Behavior. [CrossRef]
- *Horton, D. J. (1982). Sex-role orientation, sexual behavior and sexual satisfaction in women (Doctoral dissertation, George Washington University, Washington, District of Columbia). https://www.elibrary.ru/item.asp?id=7351884.
- *Hoyer, J. , Uhmann, S., Rambow, J., & Jacobi, F. (2009). Reduction of sexual dysfunction: By-product of cognitive-behavioural therapy for psychological disorders? Sexual and Relationship Therapy. [CrossRef]
- Hunter, C. L., & Goodie, J. L. (2017). Sexual Problems. American Psychiatric Association.
- *Hurlbert, D. F. , Apt, C., & Rabehl, S. M. (1993). Key variables to understanding female sexual satisfaction: An examination of women in nondistressed marriages. Journal of Sex and Marital Therapy. [CrossRef]
- Hurlbert, D. F. , & Whittaker, K. E. (1991). The role of masturbation in marital and sexual satisfaction: A comparative study of female masturbators and nonmasturbators. Journal of Sex Education and Therapy. [CrossRef]
- *Hwang, U. J. , Lee, M. S., Jung, S. H., Ahn, S. H., & Kwon, O. Y. (2019). Pelvic Floor Muscle Parameters Affect Sexual Function After 8 Weeks of Transcutaneous Electrical Stimulation in Women with Stress Urinary Incontinence. Sexual Medicine 7, 505–513. [CrossRef]
- Jannini, E. A. , & Lenzi, A. (2005). Ejaculatory disorders: epidemiology and current approaches to definition, classification and subtyping. World Journal of Urology. [CrossRef]
- *Jensen, P. T. , Klee, M. C., Tharanov, I., & Groenvold, M. (2004). Validation of a questionnaire for self-assesment of sexual function and vaginal changes after gynaecological cancer. Psycho-Oncology. [CrossRef]
- Jiann, B. , Su, C., & Tsai, J. (2013). Is female sexual function related to the male partners’ erectile function? Journal of Sexual Medicine. [CrossRef]
- *Jones, A. C. , Robinson, W. D., & Seedall, R. B. (2018). The role of sexual communication in couples’ sexual outcomes: A dyadic path analysis. Journal of Marital and Family Therapy. [CrossRef]
- *Kahn, A. S. (2001). Entitlement and sexuality: An exploration of the relationship between entitlement level and female sexual attitudes, behaviors, and satisfaction (Doctoral dissertation, Adelphi University, Garden City, New York). https://www.elibrary.ru/item.asp?id=5346342.
- Kaighobadi, F., Shackelford, T. K., & Weekes-Shackelford, V. A. (2012). Do women pretend orgasm to retain a mate? Archives of Sexual Behavior, 41, 1121-1125.
- *Kalmbach, D. A. , Arnedt, J. T., Pillai, V., & Ciesla, J. A. (2015). The impact of sleep on female sexual response and behavior: A pilot study. Journal of Sexual Medicine. [CrossRef]
- *Kalmbach, D. A. , Ciesla, J. A., Janata, J. W., & Kingsberg, S. A. (2012). Specificity of anhedonic depression and anxious arousal with sexual problems among sexually healthy young adults. Journal of Sexual Medicine 9, 505–513. [CrossRef]
- *Kalmbach, D. A. , Kingsberg, S. A., Roth, T., Cheng, P., Fellman-Couture, C., & Drake, C. L. (2019). Sexual function and distress in postmenopausal women with chronic insomnia: exploring the role of stress dysregulation. Nature and Science of Sleep. [CrossRef]
- *Kalmbach, D. A. , & Pillai, V. (2014). Daily affect and female sexual function. Journal of Sexual Medicine 11, 2938–2954. [CrossRef]
- *Karabulutlu, E. Y., Okanli, A., & Sivrikaya, S. K. (2011). Sexual dysfunction and depression in Turkish female hemodialysis patients. Pakistan Journal of Medical Sciences, 27, 842-846. http://dspace.balikesir.edu.tr/xmlui/handle/20.500.12462/7148#sthash.4HofFX3Y.dpbs.
- Karney, B. R. , & Bradbury, T. N. (1995). The longitudinal course of marital quality and stability: A review of theory, methods, and research. Psychological Bulletin. [CrossRef]
- *Kelley, E. L. , & Gidycz, C. A. (2017). Mediators of the relationship between sexual assault and sexual behaviors in college women. Journal of Interpersonal Violence 7, 574–582. [CrossRef]
- *Keskin, G. , Babacan Gümüş, A., & Taşdemir Yiğitoğlu, G. (2019). Sexual dysfunctions and related variables with sexual function in patients who undergo dialysis for chronic renal failure. Journal of Clinical Nursing 28, 257–269. [CrossRef]
- *Khajehei, M. , Doherty, M., Tilley, P. J. M., & Sauer, K. (2015). Prevalence and risk factors of sexual dysfunction in postpartum Australian women. Journal of Sexual Medicine 12, 1415–1426. [CrossRef]
- Khazaie, H. , Rezaie, L., Payam, N. R., & Najafi, F. (2015). Antidepressant-induced sexual dysfunction during treatment with fluoxetine, sertraline and trazodone: A randomized controlled trial. General Hospital Psychiatry. [CrossRef]
- *Khnaba, D. , Rostom, S., Lahlou, R., Bahiri, R., Abouqal, R., & Hajjaj-Hassouni, N. (2016). Sexual dysfunction and its determinants in Moroccan women with rheumatoid arthritis. Pan African Medical Journal 24, 1–13. [CrossRef]
- Kikusui, T. , Winslow, J. T., & Mori, Y. (2006). Social buffering: relief from stress and anxiety. Philosophical Transactions of the Royal Society B: Biological Sciences. [CrossRef]
- *Klapilová, K. , Brody, S., Krejčová, L., Husárová, B., & Binter, J. (2015). Sexual satisfaction, sexual compatibility, and relationship adjustment in couples: The role of sexual behaviors, orgasm, and men’s discernment of women’s intercourse orgasm. Journal of Sexual Medicine. [CrossRef]
- Komisaruk, B. R. , & Whipple, B. (2005). Functional MRI of the brain during orgasm in women. Annual Review of Sex Research 16, 62–86. [CrossRef]
- *Kračun, I. , Tul, N., Blickstein, I., & Velikonja, V. G. (2019). Quantitative and qualitative assessment of maternal sexuality during pregnancy. Journal of Perinatal Medicine 47, 335–340. [CrossRef]
- *Kreuter, M. , Dahllöf, A. G., Gudjonsson, G., Sullivan, M., & Siösteen, A. (1998). Sexual adjustment and its predictors after traumatic brain injury. Brain Injury 12, 349–368. [CrossRef]
- Krüger, T. H. , Haake, P., Hartmann, U., Schedlowski, M., & Exton, M. S. (2002). Orgasm-induced prolactin secretion: feedback control of sexual drive? Neuroscience & Biobehavioral Reviews. [CrossRef]
- Krüger, T. H. , Hartmann, U., & Schedlowski, M. (2005). Prolactinergic and dopaminergic mechanisms underlying sexual arousal and orgasm in humans. World Journal of Urology 23(2), 130–138. [CrossRef]
- Krishna, K. , Avasthi, A., & Grover, S. (2011). Prevalence and psychological impact of antidepressant-associated sexual dysfunction: A study from North India. Journal of Clinical Psychopharmacology. [CrossRef]
- Kuffel, S. W. , & Heiman, J. R. (2006). Effects of depressive symptoms and experimentally adopted schemas on sexual arousal and affect in sexually healthy women. Archives of Sexual Behavior 35, 163–177. [CrossRef]
- Laan, E. , & Rellini, A. H. (2012). Can we treat anorgasmia in women? The challenge to experiencing pleasure. Sexual and Relationship Therapy. [CrossRef]
- Lamela, D. , Figueiredo, B., Jongenelen, I., Morais, A., & Simpson, J. A. (2020). Coparenting and relationship satisfaction in mothers: The moderating role of sociosexuality. Archives of Sexual Behavior. [CrossRef]
- Laumann, E. O., Gagnon, J. H., Michael, R. T., & Michaels, S. (2000). The social organization of sexuality: Sexual practices in the United States. University of Chicago press.
- Laurent, S. M. , & Simons, A. D. (2009). Sexual dysfunction in depression and anxiety: Conceptualizing sexual dysfunction as part of an internalizing dimension. Clinical Psychology Review. [CrossRef]
- *Leeners, B. , Hengartner, M. P., Rössler, W., Ajdacic-Gross, V., & Angst, J. (2014). The role of psychopathological and personality covariates in orgasmic difficulties: A prospective longitudinal evaluation in a cohort of women from age 30 to 50. Journal of Sexual Medicine. [CrossRef]
- Leeners, B. , Kruger, T. H., Brody, S., Schmidlin, S., Naegeli, E., & Egli, M. (2013). The quality of sexual experience in women correlates with post-orgasmic prolactin surges: Results from an experimental prototype study. The Journal of Sexual Medicine. [CrossRef]
- *Leonhardt, N. D. , Willoughby, B. J., Busby, D. M., Yorgason, J. B., & Holmes, E. K. (2018). The significance of the female orgasm: A nationally representative, dyadic study of newlyweds’ orgasm experience. The Journal of Sexual Medicine. [CrossRef]
- Levin, R. J. (2007). Sexual activity, health and well-being—The beneficial roles of coitus and masturbation. Sexual and Relationship Therapy. [CrossRef]
- Levin, R. J. (2012a). The ever continuing life of that ‘little death’–the human orgasm.
- Levin, R. J. (2012b). The human female orgasm: A critical evaluation of its proposed reproductive functions. Sexual and Relationship Therapy. [CrossRef]
- Levin, R. J. (2014). The pharmacology of the human female orgasm—Its biological and physiological backgrounds. Pharmacology Biochemistry and Behavior. [CrossRef]
- *Lew-Starowicz, M. , & Rola, R. (2014). Correlates of sexual function in male and female patients with multiple sclerosis. Journal of Sexual Medicine 11, 2172–2180. [CrossRef]
- Lipe, H. , Longstreth, W. T., Bird, T. D., & Linde, M. (1990). Sexual function in married men with Parkinson’s disease compared to married men with arthritis. Neurology. [CrossRef]
- Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis. Sage Publications, Inc.
- *Llaneza, P. , Fernández-Iñarrea, J. M., Arnott, B., García-Portilla, M. P., Chedraui, P., & Pérez-López, F. R. (2011). Sexual function assessment in postmenopausal women with the 14-item Changes in Sexual Functioning Questionnaire. Journal of Sexual Medicine. [CrossRef]
- Madewell, A. N. (2013). Knowing thyself: Constructing women’s sexual identity theory with sexual anatomy knowledge, vulva genital awareness, and sociopolitical ideations (Doctoral dissertation, Oklahoma State University, Stillwater, Oklahoma). https://hdl.handle.net/11244/10973.
- Maes, C. A. (2017). A descriptive analysis of perceived stress and sexual function among community-dwelling older adult males (Doctoral dissertation, University of Arizona, Tucson, Arizona). https://repository.arizona.edu/handle/10150/625647.
- Magon, N., & Kalra, S. (2011). The orgasmic history of oxytocin: Love, lust, and labor. Indian Journal of Endocrinology and Metabolism, 15, S156-S161.
- Martin, L. R. , Friedman, H. S., Tucker, J. S., Schwartz, J. E., Criqui, M. H., Wingard, D. L., & Tomlinson-Keasey, C. (1995). An archival prospective study of mental health and longevity. Health Psychology 14(5), 381.
- Maslow, A. H. (1943). A Theory of Human Motivation. Psycholgical Review. [CrossRef]
- *Masmoudi, R. , Aissi, M., Halouani, N., Fathallah, S., Louribi, I., Aloulou, J., Amami, O., & Frih, M. (2018). Female sexual dysfunction and multiple sclerosis: A case-control study. Progres en urologie: Journal de l’Association francaise d’urologie et de la Societe francaise d’urologie. [CrossRef]
- Maassen, G. H., & Bakker, A. B. (2001). Suppressor variables in path models: Definitions and interpretations. Sociological Methods & Research, 30(2), 241-270.
- *McNicoll, G. , Corsini-Munt, S., O. Rosen, N., McDuff, P., & Bergeron, S. (2017). Sexual assertiveness mediates the associations between partner facilitative responses and sexual outcomes in women with provoked Vestibulodynia. Journal of Sex & Marital Therapy. [CrossRef]
- McShane, B. B. , Bockenholt, U., & Hansen, K. T. (2016). Adjusting for publication bias in meta-analysis: An evaluation of selection methods and some cautionary notes. Perspectives on Psychological Science, 11. [CrossRef]
- Meadow, R. M. (1982). Factors contributing to the sexual satisfaction of married women: A multiple regression analysis (Doctoral dissertation, Arizona State University, Tempe, Arizona). https://www.elibrary.ru/item.asp?id=7354749.
- Meltzer, A. L. , Makhanova, A., Hicks, L. L., French, J. E., McNulty, J. K., & Bradbury, T. N. (2017). Quantifying the sexual afterglow: The lingering benefits of sex and their implications for pair-bonded relationships. Psychological Science. [CrossRef]
- *Mendes, A. K. , Cardoso, F. L., & Savall, A. C. R. (2008). Sexual satisfaction in people with spinal cord injury. Sexuality and Disability 26, 137–147. [CrossRef]
- *Mernone, L. , Fiacco, S., & Ehlert, U. (2019). Psychobiological factors of sexual health in aging women-findings from the Women 40+ Healthy Aging Study. Frontiers in Psychology. [CrossRef]
- Meston, C. M. , Hull, E., Levin, R. J., & Sipski, M. (2004a). Disorders of orgasm in women. Journal of Sexual Medicine 1, 66–68. [CrossRef]
- Meston, C. M. , Levin, R. J., Sipski, M. L., Hull, E. M., & Heiman, J. R. (2004b). Women’s orgasm. Annual review of sex research. [CrossRef]
- Mialon, H. M. (2012). The economics of faking ecstasy. Economic Inquiry. [CrossRef]
- Moher, D. , Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Annals of Internal Medicine. [CrossRef]
- *Monga, T. N. , Tan, G., Ostermann, H. J., Monga, U., & Grabois, M. (1998). Sexuality and sexual adjustment of patients with chronic pain. Disability and Rehabilitation 20, 317–329. [CrossRef]
- *Morales, M. G. , Rubio, J. C., Peralta-Ramirez, M. I., Romero, L. H., Fernández, R. R., García, M. C., Navarrete, N. N., & Centeno, N. O. (2013). Impaired sexual function in women with systemic lupus erythematosus: a cross-sectional study. Lupus. [CrossRef]
- Morokqff, P. J. , & Gillilland, R. (1993). Stress, sexual functioning, and marital satisfaction. Journal of Sex Research 30, 43–53. [CrossRef]
- *Moshfeghy, Z. , Tahari, S., Janghorban, R., Najib, F. S., Mani, A., & Sayadi, M. Original Investigation Association of sexual function and psychological symptoms (depression, anxiety and stress) in women with recurrent vulvovaginal candidiasis. Unpublished manuscript. [CrossRef]
- Muehlenhard, C. L. , & Shippee, S. K. (2010). Men’s and women’s reports of pretending orgasm. Journal of Sex Research. [CrossRef]
- Murphy, M. R. , Checkley, S. A., Seckl, J. R., & Lightman, S. L. (1990). Naloxone inhibits oxytocin release at orgasm in man. The Journal of Clinical Endocrinology & Metabolism. [CrossRef]
- Murphy, M. R. , Seckl, J. R., Burton, S., Checkley, S. A., & Lightman, S. L. (1987). Changes in oxytocin and vasopressin secretion during sexual activity in men. The Journal of Clinical Endocrinology & Metabolism. [CrossRef]
- *Najafabady, M. T. , Salmani, Z., & Abedi, P. (2011). Prevalence and related factors for anorgasmia among reproductive aged women in Hesarak, Iran. Clinics 66, 83–86. [CrossRef]
- *Nascimento, E. R. , Maia, A. C. O., Nardi, A. E., & Silva, A. C. (2015). Sexual dysfunction in arterial hypertension women: The role of depression and anxiety. Journal of Affective Disorders. [CrossRef]
- *Norhayati, M. N. , & Azman Yacob, M. (2017). Long-term postpartum effect of severe maternal morbidity on sexual function. The International Journal of Psychiatry in Medicine. [CrossRef]
- Ogawa, S. , Kudo, S., Kitsunai, Y., & Fukuchi, S. (1980). Increase in oxytocin secretion at ejaculation in male. Clinical endocrinology 13, 95–97. [CrossRef]
- *Onem, K. , Erol, B., Sanli, O., Kadioglu, P., Yalin, A. S., Canik, U., Cuhadaroglu, C., & Kadioglu, A. (2008). Is sexual dysfunction in women with obstructive sleep apnea-hypopnea syndrome associated with the severity of the disease? A pilot study. Journal of Sexual Medicine. [CrossRef]
- *Opperman, E. A. , Benson, L. E., & Milhausen, R. R. (2013). Confirmatory factor analysis of the Female Sexual Function Index. Journal of Sex Research 50, 29–36. [CrossRef]
- Opperman, E., Braun, V., Clarke, V., & Rogers, C. (2014). “It feels so good it almost hurts”: Young adults’ experiences of orgasm and sexual pleasure. The Journal of Sex Research, 51(5), 503-515.
- *Özcan, T. , Benli, E., Demir, E. Y., Özer, F., Kaya, Y., & Haytan, C. E. (2014). The relation of sexual dysfunction to depression and anxiety in patients with Parkinson’s disease. Acta Neuropsychiatrica. [CrossRef]
- *Özdemir, C. , Eryılmaz, M., Yurtman, F., & Karaman, T. (2007). Sexual functioning after renal transplantation. Transplantation Proceedings 39, 1451–1454.
- *Pakpour, A. H. , Yekaninejad, M. S., Pallich, G., & Burri, A. (2015). Using ecological momentary assessment to investigate short-term variations in sexual functioning in a sample of peri-menopausal women from Iran. PLoS ONE. [CrossRef]
- Palmore, E. B. (1982). Predictors of the longevity difference: A 25-year follow-up. The Gerontologist. [CrossRef]
- *Papini, M. N. , Fioravanti, G., Talamba, G., Benni, L., Pracucci, C., Godini, L., Lazzeretti, L., Casale, S., & Faravelli, C. (2013). Female sexual functioning: the role of psychopathology. Rivista di Psichiatria. [CrossRef]
- *Parish, W. L. , Luo, Y., Stolzenberg, R., Laumann, E. O., Farrer, G., & Pan, S. (2007). Sexual practices and sexual satisfaction: A population based study of Chinese urban adults. Archives of Sexual Behavior. [CrossRef]
- *Pascoal, P. M. , Byers, E. S., Alvarez, M. J., Santos-Iglesias, P., Nobre, P. J., Pereira, C. R., & Laan, E. (2018). A dyadic approach to understanding the link between sexual functioning and sexual satisfaction in heterosexual couples. The Journal of Sex Research. [CrossRef]
- *Peixoto, C. , Carrilho, C. G., Ribeiro, T. T. D. S. B., da Silva, L. M., Gonçalves, E. A., Fernandes, L., Nardi, A. E., Cardoso, A., & Veras, A. B. (2019). Relationship between sexual hormones, quality of life and postmenopausal sexual function. Trends in Psychiatry and Psychotherapy. [CrossRef]
- Peixoto, M. M., & Nobre, P. (2015). Prevalence and sociodemographic predictors of sexual problems in Portugal: a population-based study with women aged 18 to 79 years. Journal of Sex & Marital Therapy, 41(2), 169-180.
- Persson, G. (1981). Five-year mortality in a 70-year-old urban population in relation to psychiatric diagnosis, personality, sexuality and early parental death. Acta Psychiatrica Scandinavica. [CrossRef]
- *Philippsohn, S. , & Hartmann, U. (2009). Determinants of sexual satisfaction in a sample of German women. Journal of Sexual Medicine 6, 1001–1010. [CrossRef]
- Pickering, T. G. (2003). Men are from Mars, women are from Venus: Stress, pets, and oxytocin. The Journal of Clinical Hypertension. [CrossRef]
- *Pinney, E. M. , Gerrard, M., & Denney, N. W. (1987). The Pinney Sexual Satisfaction Inventory. Journal of Sex Research 23, 233–251. [CrossRef]
- *Pinsky, I. S. (2016). Attachment quality and sexual satisfaction and sexual functioning in romantic relationships for combat veterans. [CrossRef]
- Powers, C. R. (2012). Female orgasm from intercourse: Importance, partner characteristics, and health (Doctoral dissertation, University of North Texas, Denton, Texas). https://www.semanticscholar.org/paper/Female-Orgasm-From-Intercourse%3A-Importance%2C-Partner-Powers/af8da4739c7dd49aadebf0042a99b0a4b534658f.
- Prause, N. (2012a). The human female orgasm: Critical evaluations of proposed psychological sequelae. Sexual and Relationship Therapy. [CrossRef]
- Prause, N. (2012b). A response to Brody, Costa and Hess (2012): theoretical, statistical and construct problems perpetuated in the study of female orgasm. Sexual and Relationship Therapy. [CrossRef]
- Quinn-Nilas, C. , Benson, L., Milhausen, R. R., Buchholz, A. C., & Goncalves, M. (2016). The relationship between body image and domains of sexual functioning among heterosexual, emerging adult women. Sexual Medicine 4(3), e182–e189.
- R Core Team (2017). foreign: Read data stored by SPSS, R package version 0.8-70. R Core Team.
- R Core Team (2018). R: A language and environment for statistical computing. (n.d.). R Foundation for Statistical Computing.
- Randolph, M. E. (2002). The role of depression, relationship support, and child sexual abuse in predicting the impact of chronic pelvic pain on women’s sexual functioning (Doctoral dissertation, University of Wisconsin—Milwaukee, Milwaukee, Wisconsin). https://www.elibrary.ru/item.asp?id=5439148.
- Regan, P. C., & Atkins, L. (2006). Sex differences and similarities in frequency and intensity of sexual desire. Social Behavior and Personality: An international journal, 34(1), 95-102.
- Richters, J. , de Visser, R., Rissel, C., & Smith, A. (2006). Sexual practices at last heterosexual encounter and occurrence of orgasm in a national survey. Journal of Sex Research 43, 217–226. [CrossRef]
- *Rosen, N. O. , Dubé, J. P., Corsini-Munt, S., & Muise, A. (2019). Partners experience consequences, too: A comparison of the sexual, relational, and psychological adjustment of women with Sexual Interest/Arousal Disorder and their partners to control couples. The Journal of Sexual Medicine. [CrossRef]
- *Rosen, R. , Brown, C., Heiman, J., Leiblum, S., Meston, C., Shabsigh, R., Ferguson, D., & D’Agostino, R. (2000). The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. Journal of Sex and Marital Therapy. [CrossRef]
- Rosen, R. C. , Riley, A., Wagner, G., Osterloh, I. H., Kirkpatrick, J., & Mishra, A. (1997). The International Index of Erectile Function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology. [CrossRef]
- Rosenberg, M. S. (2010). A generalized formula for converting chi-square tests to effect sizes for meta-analysis. PloS one. [CrossRef]
- *Rottmann, N. , Gilså Hansen, D., dePont Christensen, R., Hagedoorn, M., Frisch, M., Nicolaisen, A., Kroman, N., Flyger, H., & Johansen, C. (2017). Satisfaction with sex life in sexually active heterosexual couples dealing with breast cancer: a nationwide longitudinal study. Acta Oncologica. [CrossRef]
- *Rowland, D. L. , & Kolba, T. N. (2019). Relationship of Specific Sexual Activities to Orgasmic Latency, Pleasure, and Difficulty During Partnered Sex. The Journal of Sexual Medicine 16, 559–568. [CrossRef]
- *Rowland, D. L. , Sullivan, S. L., Hevesi, K., & Hevesi, B. (2018). Orgasmic latency and related parameters in women during partnered and masturbatory sex. The Journal of Sexual Medicine 15, 1463–1471. [CrossRef]
- Sahay, R. D. , Haynes, E. N., Rao, M. B., & Pirko, I. (2012). Assessment of sexual satisfaction in relation to potential sexual problems in women with multiple sclerosis: A pilot study. Sexuality and Disability. [CrossRef]
- *Sakinci, M. , Ercan, C. M., Olgan, S., Coksuer, H., Karasahin, K. E., & Kuru, O. (2016). Comparative analysis of copper intrauterine device impact on female sexual dysfunction subtypes. Taiwanese Journal of Obstetrics and Gynecology 55, 30–34. [CrossRef]
- Salisbury, C. M. A. , & Fisher, W. A. (2014). “Did you come?” A qualitative exploration of gender differences in beliefs, experiences, and concerns regarding female orgasm occurrence during heterosexual sexual interactions. The Journal of Sex Research. [CrossRef]
- Salamon, E. , Esch, T., & Stefano, G. B. (2005). Role of amygdala in mediating sexual and emotional behavior via coupled nitric oxide release. Acta Pharmacologica Sinica 26, 389–395. [CrossRef]
- *Sariyildiz, M. A. , Batmaz, I., Dilek, B., İnanir, A., Bez, Y., Tahtasiz, M., Em, S., & Çevik, R. (2013). Relationship of the sexual functions with the clinical parameters, radiological scores and the quality of life in male patients with ankylosing spondylitis. Rheumatology International 33, 623–629. [CrossRef]
- *Sarti, C. D. , Graziottin, A., Mincigrucci, M., Ricci, E., Chiaffarino, F., Bonaca, S., Becorpi, A., & Parazzini, F. (2010). Correlates of sexual functioning in Italian menopausal women. Climacteric 13, 447–456. [CrossRef]
- *Scott, S. B. , Ritchie, L., Knopp, K., Rhoades, G. K., & Markman, H. J. (2018). Sexuality within female same-gender couples: Definitions of sex, sexual frequency norms, and factors associated with sexual satisfaction. Archives of Sexual Behavior. [CrossRef]
- Seguin, L. J. , Milhausen, R. R., & Kukkonen, T. (2015). The development and validation of the motives for feigning orgasms scale. The Canadian Journal of Human Sexuality 24, 31–48.
- *Seldin, D. R. , Friedman, H. S., & Martin, L. R. (2002). Sexual activity as a predictor of life-span mortality risk. Personality and Individual Differences. [CrossRef]
- Shaver, P. R. , & Mikulincer, M. (2002). Attachment-related psychodynamics. Attachment & Human Development. [CrossRef]
- Shaw, A. M. , & Rogge, R. D. (2016). Evaluating and refining the construct of sexual quality with item response Theory: Development of the Quality of Sex Inventory. Archives of Sexual Behavior. [CrossRef]
- *Shifren, J. L. , Monz, B. U., Russo, P. A., Segreti, A., & Johannes, C. B. (2008). Sexual problems and distress in United States women: prevalence and correlates. Obstetrics & Gynecology. [CrossRef]
- *Skoczyński, S. , Nowosielski, K., Minarowski, Ł., Brożek, G., Oraczewska, A., Glinka, K., Ficek, K., Kotulska, B., Tobiczyk, E., Skomoro, R., Mróz, R., & Barczyk, A. (2019). May Dyspnea Sensation Influence the Sexual Function in Men With Obstructive Sleep Apnea Syndrome? A Prospective Control Study. Sexual Medicine. [CrossRef]
- Smith, A. S. , & Wang, Z. (2014). Hypothalamic oxytocin mediates social buffering of the stress response. Biological Psychiatry 76, 281–288. [CrossRef]
- *Speer, J. J. , Hillenberg, B., Sugrue, D. P., Blacker, C., Kresge, C. L., Decker, V. B., Zakalik, D., & Decker, D. A. (2005). Study of sexual functioning determinants in breast cancer survivors. The Breast Journal 11, 440–447. [CrossRef]
- Spitalnick, J. S. , & McNair, L. D. (2005). Couples therapy with gay and lesbian clients: An analysis of important clinical issues. Journal of Sex & Marital Therapy. [CrossRef]
- Stephenson, K. R., Ahrold, T. K., & Meston, C. M. (2011). The association between sexual motives and sexual satisfaction: Gender differences and categorical comparisons. Archives of Sexual Behavior, 40(3), 607-618.
- *Stephenson, K. R. , Hughan, C. P., & Meston, C. M. (2012). Childhood sexual abuse moderates the association between sexual functioning and sexual distress in women. Child Abuse and Neglect 36, 180–189. [CrossRef]
- *Stephenson, K. R. , & Meston, C. M. (2010). Differentiating components of sexual well-being in women: Are sexual satisfaction and sexual distress independent constructs? The Journal of Sexual Medicine. [CrossRef]
- Stephenson, K. R., & Meston, C. M. (2015). The conditional importance of sex: Exploring the association between sexual well-being and life satisfaction. Journal of Sex & Marital Therapy, 41(1), 25-38.
- Stern, J. , Karastoyanova, K., Kandrik, M., Torrance, J., Hahn, A. C., Holzleitner, I., DeBruine, L. M., & Jones, B. C. (2020). Are sexual desire and sociosexual orientation related to men’s salivary steroid hormones? Adaptive Human Behavior and Physiology. [CrossRef]
- Strizzi, J. , Landa, L. O., Pappadis, M., Olivera, S. L., Tangarife, E. R. V., Agis, I. F., Perrin, P. B., Arango-Lasprilla, J. C. (2015). Sexual functioning, desire, and satisfaction in women with TBI and healthy controls. Behavioural Neurology. [CrossRef]
- *Stoeber, J. , & Harvey, L. N. (2016). Multidimensional sexual perfectionism and female sexual function: A longitudinal investigation. Archives of Sexual Behavior. [CrossRef]
- *Takahashi, M. , Inokuchi, T., Watanabe, C., Saito, T., & Kai, I. (2011). The Female Sexual Function Index (FSFI): Development of a Japanese version. Journal of Sexual Medicine. [CrossRef]
- *Tao, P. , & Brody, S. (2011). Sexual behavior predictors of satisfaction in a Chinese sample. Journal of Sexual Medicine 8, 455–460. [CrossRef]
- *Tavares, I. M. , Laan, E. T. M., & Nobre, P. J. (2017). Cognitive-affective dimensions of female orgasm: The role of automatic thoughts and affect during sexual activity. Journal of Sexual Medicine. [CrossRef]
- *Thakurdesai, A. , & Sawant, N. (2018). A prospective study on sexual dysfunctions in depressed males and the response to treatment. Indian Journal of Psychiatry 60, 472. [CrossRef] [PubMed]
- *Therrien, S. , & Brotto, L. A. (2016). A critical examination of the relationship between vaginal orgasm consistency and measures of psychological and sexual functioning and sexual concordance in women with sexual dysfunction. Canadian Journal of Human Sexuality 25, 109–118. [CrossRef]
- Tiihonen, J. , Kuikka, J., Kupila, J., Partanen, K., Vainio, P., Airaksinen, J., Eronen, M., Hallikainen, T., Paanila, J., Kinnunen, I., & Huttunen, J. (1994). Increase in cerebral blood flow of right prefrontal cortex in man during orgasm. Neuroscience letters 170, 241–243. [CrossRef] [PubMed]
- *Tracy, J. K. , & Junginger, J. (2007). Correlates of lesbian sexual functioning. Journal of Women’s Health. [CrossRef]
- *Træen, B. (2007). Sexual dissatisfaction among men and women with congenital and acquired heart disease. Sexual and Relationship Therapy. [CrossRef]
- *Tuinman, M. A. , Hoekstra, H. J., Vidrine, D. J., Gritz, E. R., Sleijfer, D. T., Fleer, J., & Hoekstra-Weebers, J. E. H. M. (2010). Sexual function, depressive symptoms and marital status in nonseminoma testicular cancer patients: A longitudinal study. Psycho-Oncology. [CrossRef]
- *Tutino, J. S. , Ouimet, A. J., & Shaughnessy, K. (2017). How do psychological risk factors predict sexual outcomes? A comparison of four models of young women’s sexual outcomes. The Journal of Sexual Medicine. [CrossRef]
- Twenge, J. M., Sherman, R. A., & Wells, B. E. (2017). Declines in sexual frequency among American adults, 1989–2014. Archives of Sexual Behavior, 46, 2389-2401.
- *Uddenberg, N. (1974). Psychological aspects of sexual inadequacy in women. Journal of Psychosomatic Research. [CrossRef]
- Urganci, B. , Sevi, B., & Sakman, E. (2021). Better relationships shut the wandering eye: Sociosexual orientation mediates the association between relationship quality and infidelity intentions. Journal of Social and Personal Relationships. [CrossRef]
- Uvnas-Moberg, K. (1998). Antistress pattern induced by oxytocin. Physiology. [CrossRef]
- *van den Brink, F. , Smeets, M. A. M., Hessen, D. J., & Woertman, L. (2016). Positive body image and sexual functioning in Dutch female university students: The role of adult romantic attachment. Archives of Sexual Behavior. [CrossRef]
- *van Nimwegen, J. F. , Arends, S., van Zuiden, G. S., Vissink, A., Kroese, F. G., & Bootsma, H. (2015). The impact of primary Sjögren’s syndrome on female sexual function. Rheumatology. [CrossRef]
- Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software. [CrossRef]
- Villeda Sandoval, C. I. V., Calao-Pérez, M., Enríquez González, A. B., Gonzalez-Cuenca, E., Ibarra-Saavedra, R., Sotomayor, M., & Castillejos Molina, R. A. (2014). Orgasmic Dysfunction: Prevalence and Risk Factors from a Cohort of Young Females in Mexico. The Journal of Sexual Medicine, 11, 1505-1511. [CrossRef]
- Vrangalova, Z. , & Ong, A. D. (2014). Who benefits from casual sex? The moderating role of sociosexuality. Social Psychological and Personality Science. [CrossRef]
- Velten, J., & Margraf, J. (2017). Satisfaction guaranteed? How individual, partner, and relationship factors impact sexual satisfaction within partnerships. PloS one, 12(2), e0172855.
- Wade, L. (2015). Are women bad at orgasms? Understanding the gender gap. In Tarrant, S. (Ed.), Gender, sex, and politics: In the streets and between the sheets in the 21st century (pp. 227-237). Routledge.
- Wade, L. , Kremer, E. C., & Brown, J. (2005). The incidental orgasm: The presence of clitoral knowledge and the absence of orgasm for women. Women & Health. [CrossRef]
- *Waite, L. J. , & Joyner, K. (2001). Emotional satisfaction and physical pleasure in sexual unions: Time horizon, sexual behavior, and sexual exclusivity. Journal of Marriage and Family. [CrossRef]
- *Wallace, D. H. , & Barbach, L. G. (1974). Preorgasmic group treatment. Journal of Sex & Marital Therapy, 1. [CrossRef]
- Ware, J. E. & Sherbourne, C.D. (1992). A 36-item short-form health survey (SF-36), I: conceptual framework and item selection. Medical Care. [CrossRef]
- Ware, J. E. , Kosinski, M., & Keller, S. D. (1996). A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Medical Care, 34. [CrossRef]
- Watson, D. , & Clark, A. L. (1991). The Mood and Anxiety Symptom Questionnaire (MASQ). Unpublished manuscript. [CrossRef]
- Watson, D. , Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of Personality and Social Psychology. [CrossRef]
- *Weiss, P. , & Brody, S. (2011). International Index of Erectile Function (IIEF) scores generated by men or female partners correlate equally well with own satisfaction (sexual, partnership, life, and mental health). The Journal of Sexual Medicine 8, 1404–1410. [CrossRef]
- White, S. E., & Reamy, K. (1982). Sexuality and pregnancy: A review. Archives of Sexual Behavior, 11(5), 429-444.
- WHOQoL Group. (1998). Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological medicine, 28. [CrossRef]
- *Witting, K. , Santtila, P., Alanko, K., Harlaar, N., Jern, P., Johansson, A., Von Der Pahlen, B., Varjonen, M., Algars, M., & Sandnabba, N. K. (2008a). Female sexual function and its associations with number of children, pregnancy, and relationship satisfaction. Journal of Sex & Marital Therapy. [CrossRef]
- *Witting, K. , Santtila, P., Jern, P., Varjonen, M., Wager, I., Höglund, M., Johansson, A., Vikstrom, N., & Sandnabba, N. K. (2008b). Evaluation of the Female Sexual Function Index in a population based sample from Finland. Archives of Sexual Behavior 37, 912–924. [CrossRef]
- *Wongsomboon, V. , Burleson, M. H., & Webster, G. D. (2019). Women’s orgasm and sexual satisfaction in committed sex and casual sex: Relationship between sociosexuality and sexual outcomes in different sexual contexts. The Journal of Sex Research. [CrossRef]
- Wood, A. , Runciman, R., Wylie, K. R., & McManus, R. (2012). An update on female sexual function and dysfunction in old age and its relevance to old age psychiatry. Aging and Disease 3(5), 373.
- World Health Organization. (2002). Sexual and reproductive health: Gender and human rights. https://www.who.int/reproductivehealth/topics/gender_rights/sexual_health/en/.
- *Yangin, H. B. , Sözer, G. A., Şengün, N., & Kukulu, K. (2008). The relationship between depression and sexual function in menopause period. Maturitas 61, 233–237. [CrossRef]
- *Yanikkerem, E. , Goker, A., Ustgorul, S., & Karakus, A. (2016). Evaluation of sexual functions and marital adjustment of pregnant women in Turkey. International Journal of Impotence Research 28, 176–183. [CrossRef]
- *Yela, D. A. , Soares, P. M., & Benetti-Pinto, C. L. (2018). Influence of sexual function on the social relations and quality of life of women with premature ovarian insufficiency. Revista Brasileira de Ginecologia e Obstetrícia/RBGO Gynecology and Obstetrics. [CrossRef]
- *Yeoh, S. H. , Razali, R., Sidi, H., Razi, Z. R. M., Midin, M., Jaafar, N. R. N., & Das, S. (2014). The relationship between sexual functioning among couples undergoing infertility treatment: A pair of perfect gloves. Comprehensive Psychiatry. [CrossRef]
- Young, M., Denny, G., Luquis, R., & Young, T. (1998). Correlates of sexual satisfaction in marriage. Canadian Journal of Human Sexuality, 7, 115-128. https://www.researchgate.net/profile/Raffy_Luquis/publication/281691542_Correlates_of_sexual_satisfaction_in_marriage/links/5693e45d08ae3ad8e33b3f5d/Correlates-of-sexual-satisfaction-in-marriage.pdf.
- Zigmond, A. S. & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavia 67, 361–370. [CrossRef]
- *Zhang, H. , Fan, S., & Yip, P. S. F. (2015). Sexual dysfunction among reproductive-aged chinese married women in hong kong: Prevalence, risk factors, and associated consequences. Journal of Sexual Medicine. [CrossRef]
- *Zhou, M. (1993). A survey of sexual states of married, healthy, reproductive age women. Journal of Psychology & Human Sexuality. [CrossRef]
Figure 1.
Conceptual Models Integrating Sexual Health into Models of Relationship and Individual Functioning. Note. Bolded constructs in panel A correspond to search terms used to identify potential correlates.
Figure 1.
Conceptual Models Integrating Sexual Health into Models of Relationship and Individual Functioning. Note. Bolded constructs in panel A correspond to search terms used to identify potential correlates.
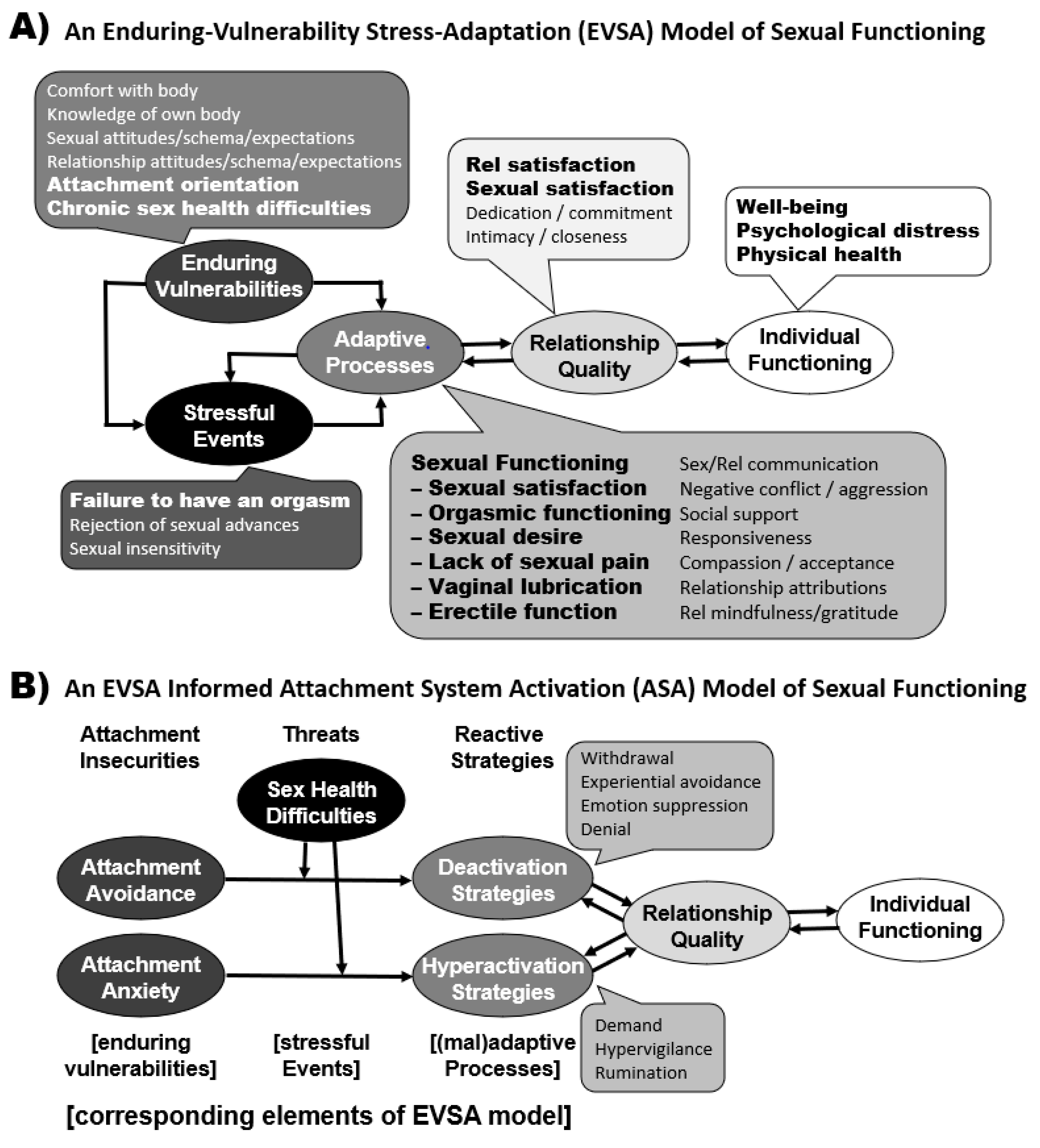
Figure 2.
Hypotheses to be Tested in Path Models.
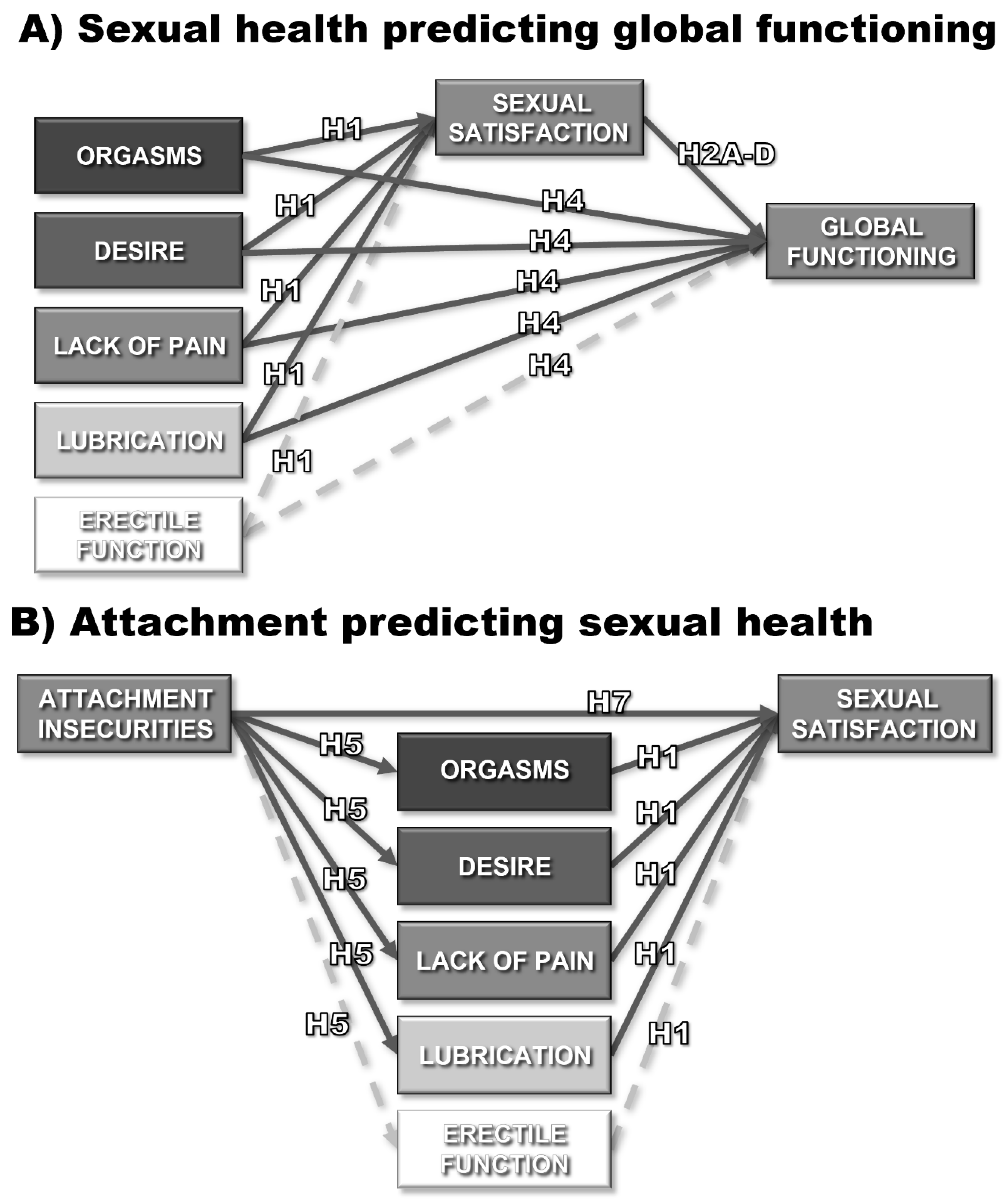
Figure 3.
Flowchart detailing record search, record screening, data inclusions, and data exclusions. Note. The PsycINFO search was set up to automatically remove duplicate records.
Figure 3.
Flowchart detailing record search, record screening, data inclusions, and data exclusions. Note. The PsycINFO search was set up to automatically remove duplicate records.
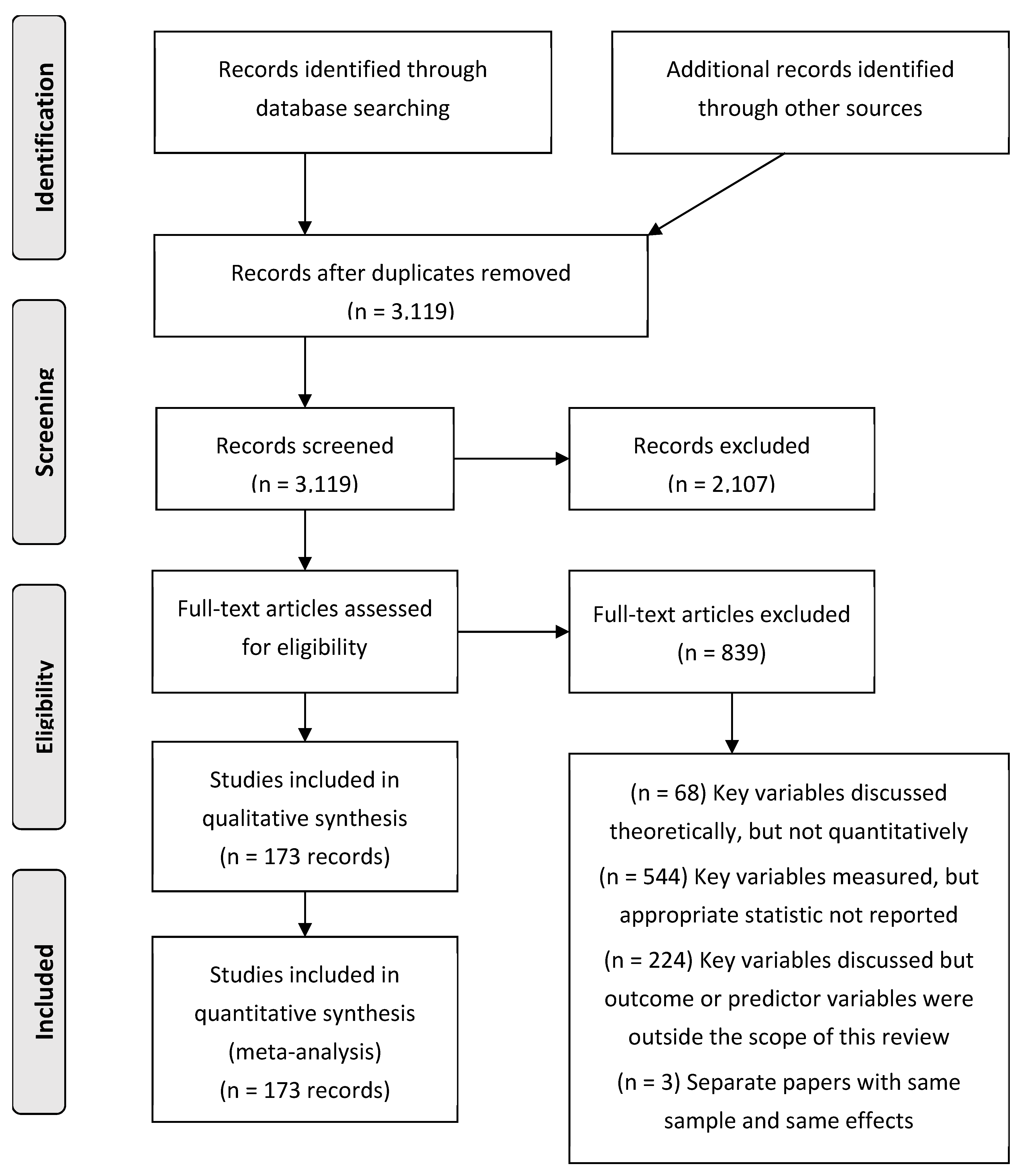
Figure 4.
Results of Path Models Examining the Unique Predictive Links of the Dimensions of Sexual Health. Note. Only paths significant at p < .01 are shown.
Figure 4.
Results of Path Models Examining the Unique Predictive Links of the Dimensions of Sexual Health. Note. Only paths significant at p < .01 are shown.
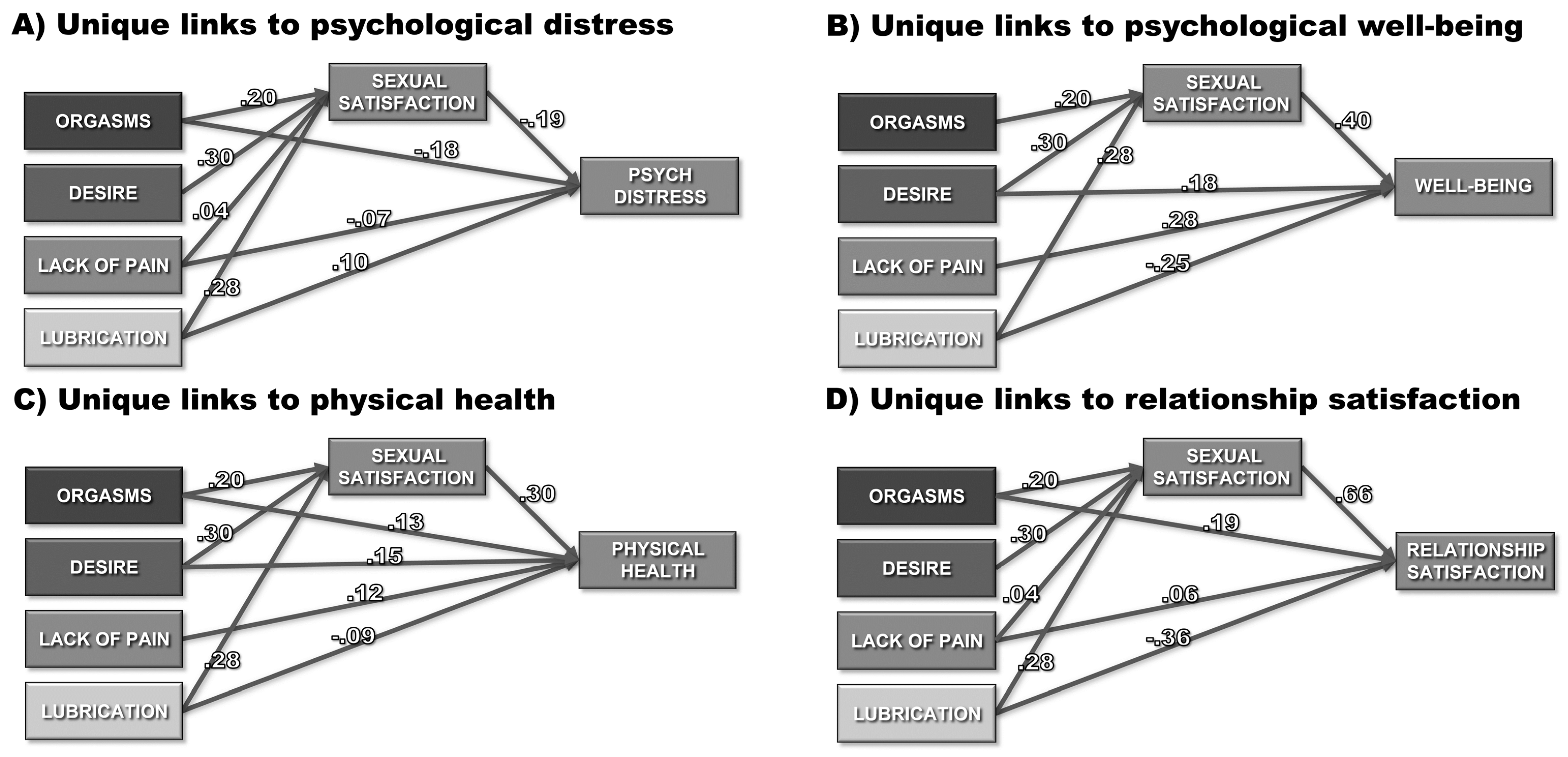
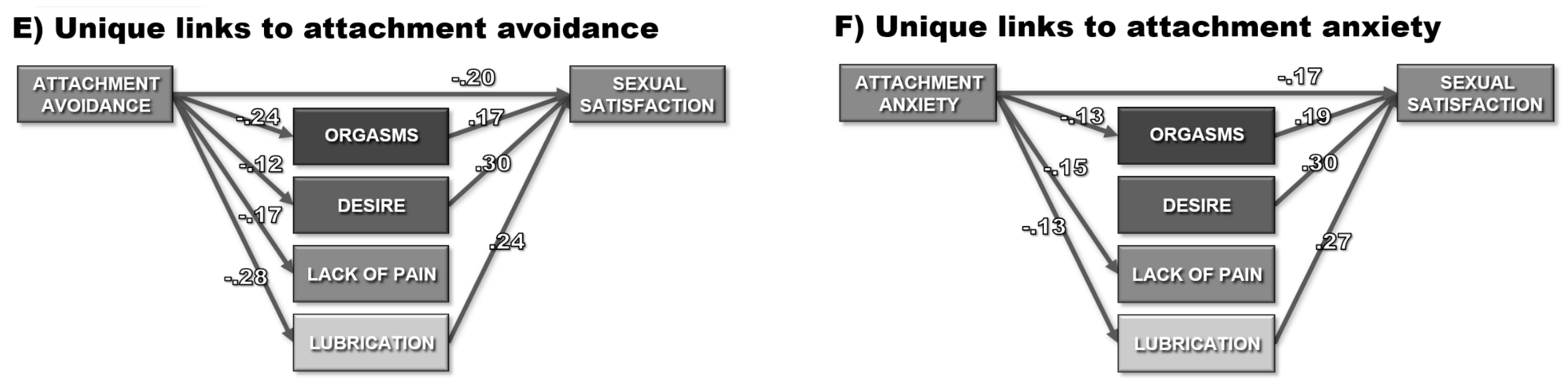

Table 1.
Summary of (Sub)samples in Analysis.
| Category | # subsamples | Category | # subsamples | Category/code | # subsamples | |||
| Subset (# reporting) | (# of effects) | Subset | ||||||
| Summary | Clinical population2 | Country | ||||||
| Distinct samples | 205 | Addison's disease | 1 | Australia | 2 | |||
| Unique subjects | 160,466 | Ankylosing spondylitis | 2 | Belgium | 2 | |||
| Distinct effects | 930 | Brain or spinal cord injury | 3 | Brazil | 7 | |||
| Publication type | Cancer | 3 | Bulgaria | 1 | ||||
| Peer-reviewed article | 187 | Chronic pain | 3 | Canada | 10 | |||
| Thesis/dissertation | 18 | Depression &/or anxiety | 9 | Chile | 2 | |||
| Publication year | Dialysis | 2 | China | 8 | ||||
| 1971-1990 | 7 | Fertility treatment | 3 | Czech Republic | 5 | |||
| 1991-2000 | 10 | Gynecological disorders | 11 | Denmark | 2 | |||
| 2001-2010 | 47 | Heart disease / hypertension | 3 | Egypt | 1 | |||
| 2011-2020 | 141 | Heroin use | 1 | Finland | 5 | |||
| Sex Health1 | Hyperthyroidism | 1 | Germany | 4 | ||||
| Sexual Satisfaction | 152 (322) | Incontinence | 1 | Greece | 1 | |||
| Orgasm | 205 (398) | Lupus | 1 | Hungary | 1 | |||
| Desire | 96 (227) | Metabolic syndrome | 1 | India | 1 | |||
| Lack of pain | 60 (154) | Migraines | 1 | International | 5 | |||
| Lubrication | 58 (167) | Multiple sclerosis | 4 | Iran | 5 | |||
| Erectile function | 18 (38) | Nonspecific medical3 | 2 | Israel | 5 | |||
| Correlate | Obesity &/or eating disorder | 3 | Italy | 12 | ||||
| Psychological distress | 88 (280) | Parkinson's disease | 1 | Japan | 1 | |||
| Psychological well-being | 22 (66) | Pre-, post-, &/or menopausal | 8 | Malaysia | 5 | |||
| Physical health | 9 (38) | Pregnant &/or postpartum | 9 | Mexico | 1 | |||
| Attachment anxiety | 9 (25) | PTSD | 1 | Morocco | 1 | |||
| Attachment avoidance | 9 (25) | Renal transplant | 1 | Netherlands | 5 | |||
| Relationship satisfaction | 54 (110) | Rheumatoid arthritis | 1 | Norway | 1 | |||
| Type of population2 | Schizophrenia | 2 | Poland | 3 | ||||
| College students | 26 | Sexual abuse | 2 | Portugal | 7 | |||
| Community | 87 | Sexual dysfunction | 12 | Scotland | 1 | |||
| Clinical | 97 | Sjogren’s syndrome | 1 | South Korea | 1 | |||
| Gender | Sleep apnea | 2 | Spain | 3 | ||||
| Female only study | 152 | Stroke | 1 | Sweden | 2 | |||
| Male only study | 40 | Vitamin D3 deficiency | 1 | Switzerland | 3 | |||
| Both genders | 13 | Average age (k=199) | Taiwan | 2 | ||||
| Weighted percent female | 71% | Lowest | 18.8 | Tunisia | 1 | |||
| Relationship length (k=41) | Highest | 73.5 | Turkey | 17 | ||||
| Lowest | 1.4 | Weighted mean | 38.9 | UK | 5 | |||
| Highest | 34.1 | Married / Cohabiting (k=96) | US | 67 | ||||
| Weighted mean | 13.8 | Weighted % | 75.2 | Caucasian (k=182) | ||||
| Weighted % | 64.4 | |||||||
Note. The 205 unique subsamples presented in this table were drawn from the 173 unique records presented in the following table. 1These numbers represent the number of subsamples providing at least one effect involving the construct listed. 2These numbers sum to more than 205 as these are not mutually exclusive categories (e.g., some samples were made up of both students and people from the community). 3These two studies were not focused on a specific clinical population but instead included samples of elderly individuals with a wide range of medical diagnoses.
Table 2.
Characteristics of Individual Study Subsamples in Analysis.
| Author (Year) | Record Type | N | Country | Subsample | Mean Age | Percent White | Sex Health Dimension(s) | Sex Health Scale(s) | Correlate Dimension | Correlate Scale | # effects |
| Abdel-Hamid & Saleh (2011) | PR | 38 | Egypt | Muslim males w/ lifelong delayed ejaculation | 30.8 | 0 | O | IIEF | depressive sxs | SRADM | 1 |
| Abedi et al. (2015) | PR | 228 | Iran | Women w/ & w/out abnormal sexual function | 30.4 | 0 | SODPL | FSFI | perceived stress | PSS | 5 |
| Adam et al. (2020) | PR | 65 | Belgium | Women aged 18-58 w/ orgasm difficulties | 32.7 | 100 | SO | FSFI | only sex health* | 1 | |
| Aerts et al. (2015) | PR | 84 | Belgium | Women w/ endometrial cancer | 63.0 | 100 | O | SSFS | relationship sat | DAS | 1 |
| Alvisi et al. (2014) | PR | 204 | Italy | Women w/ & w/out metabolic syndrome | 40.0 | 100 | O | FSFI | depressive sxs | MHQ | 2 |
| Appa et al. (2014) | PR | 1997 | US | Middle-aged women w/ multiple medical diagnoses | 60.2 | 36 | SODPL | 1 item | depression diagnosis | medical diagnosis | 5 |
| Artune-Ulkumen et al. (2014) | PR | 177 | Turkey | Women in sexual relationships w/ & w/o sexual dysfunction | 32.3 | 0 | SODPL | FSFI | mental health, vitality, physical health | SF-36 | 15 |
| Asselmann et al. (2016) | PR | 149 | Germany | Pregnant women w/ & w/o depression | 28.9 | 100 | SODL | MGH | depression diagnosis | CIDI | 4 |
| Assimakopoulos et al. (2006) | PR | 110 | Greece | Healthy women & obese women preparing for bariatric surgery | 34.4 | 100 | SODPL | FSFI | depressive sxs | BDI | 5 |
| Atis et al. (2011) | PR | 80 | Turkey | Women w/ & w/o hyperthyroidism | 36.8 | 0 | SODPL | FSFI | depressive sxs | BDI | 5 |
| Aubin et al. (2008) | PR | 72 | US | Men w/chronic pelvic pain syndrome | 40.8 | 66 | O | BSFQ | depressive sxs | CESD | 1 |
| Bakjtiari et al. (2016) | PR | 236 | Iran | Women in fertility treatment | 26.4 | 0 | SOD | DSM-IV | relationship sat | 1 item | 4 |
| Barbara et al. (2016) | PR | 269 | Italy | Women who have given birth 6mo ago | 34.4 | 100 | SO | FSFI | only sex health* | 1 | |
| Barrientos & Páez (2006) | PR | 4339 | Chile | Women & men aged 18-69 | 39.7 | 0 | SO | 1 item | only sex health* | 2 | |
| Battaglia et al. (2011) | PR | 87 | Italy | Menstruating women | 28.7 | 100 | O | 1 item | depressive sxs | BDI | 1 |
| Beaber & Werner (2009) | PR | 120 | US | Women in heterosexual & lesbian relationships | 29.4 | 77 | SODPL | FSFI | only sex health* | 16 | |
| Berenguer et al. (2019) | PR | 149 | Portugal | Adult women | 25.0 | 0 | SO | FSFI | only sex health* | 1 | |
| Blair et al. (2018) | PR | 750 | Canada | Women & men in same or opposite sex relationships | 30.0 | 0 | SO | IIEF | only sex health* | 2 | |
| Borissova et al. (2001) | PR | 627 | Bulgaria | Middle-aged pre- & post-menopausal women w/ & w/o hormone replacement therapy | 48.0 | 100 | O | 1 item | coping with life | 1 item | 1 |
| Brody & Weiss (2011) | PR | 1570 | Czech Republic | Women & men aged 35-65 in relationships | 48.8 | 100 | SO | 1 item | life sat, relationship sat | LiSat | 6 |
| Burleson et al. (2007) | PR | 58 | US | Middle-aged women | 47.6 | 0 | O | 1 item | Depressive sxs, positive affect | 1 item, 7 items | 2 |
| Burri et al. (2015) | PR | 507 | UK | Pre- & post-menopausal twin women | 56.3 | 100 | SODPL | FSFI | relationship sat | 1 item | 14 |
| Burri et al. (2013) | PR | 866 | UK | Monozygotic twin women discordant for sexual dysfunction | 55.0 | 100 | SODPL | FSFI | relationship sat | 1 item | 5 |
| Cagnacci et al. (2019) | PR | 518 | Italy | Sexually active women aged 40-55 at gynecological clinics | 49.4 | 100 | SO | FSFI | only sex health* | 1 | |
| Canat et al. (2016) | PR | 108 | Turkey | Women aged 22-51 w/ vitamin D3 deficiency | 34.9 | 0 | SODPL | FSFI | depressive sxs | BDI | 5 |
| Carmen (2014) | MT | 145 | US | Adult women | 25.8 | 0 | SODPL | FSFI | only sex health* | 10 | |
| Carrobles et al. (2011) | PR | 157 | Spain | College women aged 20-45 | 22.8 | 0 | SO | 3 items | mental health | WHO-5 | 3 |
| Castellini et al. (2010) | PR | 309 | Italy | Obese & not obese women w/ & w/o Binge ED | 39.1 | 100 | SODPL | FSFI | depressive sxs | BDI | 15 |
| Ceyhan et al. (2019) | PR | 102 | Turkey | Married women in treatment for hypertension | 55.1 | 0 | SOD | ASEX | relationship sat | MAT | 3 |
| Chang et al. (2012) | PR | 555 | Taiwan | Pregnant women | 33.0 | 0 | SODPL | FSFI | depressive sxs | CESD | 5 |
| Chang et al. (2019) | PR | 1026 | Taiwan | Women aged 40-65 | 48.5 | 0 | SODPL | FSFI | mental health, physical health | SF-12, SF-12 | 10 |
| Cheng et al. (2007) | PR | 160 | China | Sexually active men aged 50+ from a primary care treatment center | 55.0 | 0 | SOE | IIEF | depressive sxs | GDS | 3 |
| Chivers et al. (2011) | PR | 57 | Canada | Post-partum women w/ & w/o depression | 0.0 | 0 | SODPL | FSFI | depressive sxs | EPDS | 5 |
| Cohen & Belsky (2008) | PR | 323 | UK | Adult women | 24.4 | 70 | O | 4 items | attachment | ECR | 2 |
| Conroy (2018) | MT | 158 | US | Women w/ gynecologic or breast cancer | 57.7 | 92 | SO | DSFI; 1 item | depressive sxs, relationship sat | CESD, single item? | 3 |
| Constantine (2017) | DD | 531 | US | Adult women | 27.0 | 78 | SO | ISS, 1 item | psychological sxs, attachment, relationship sat | ?, ECR, RAS | 7 |
| Costa & Brody (2007) | PR | 30 | Portugal | Women currently in sexual relationships | 25.8 | 0 | SO | 1 item | relationship sat | PRQC | 2 |
| Costa & Brody (2011) | PR | 70 | Scotland | College sexually experienced women | 25.7 | 100 | O | 1 item | attachment | ECR | 2 |
| Costa et al. (2016) | PR | 116 | Portugal | Adult women & men | 24.9 | 0 | SO | 1 item | only sex health* | 2 | |
| Dashti et al. (2016) | PR | 16 | Malaysia | Women aged 28-48 w/ PCOS | 33.4 | 0 | SODPL | FSFI | depressive sxs | DASS-21 | 5 |
| Davidson & Hoffman (1986) | PR | 206 | US | Married undergrad & graduate women | 28.1 | 0 | SO | 1 item | only sex health* | 1 | |
| de Jong (2016) | DD | 220 | US & Canada | Couples w/o current sexual, medical, or psychiatric diagnoses or treatments | 26.5 | 86 | SO | 2 items | only sex health* | 1 | |
| de Lucena & Abdo (2014) | PR | 96 | Brazil | Women attending routine gynecology checkup | 38.5 | 0 | SOD | FSQ | anxiety sxs | BAI | 3 |
| de Olivera Ferro et al. (2019) | PR | 46 | Brazil | Men aged 18-60 w/ spinal cord injury | 34.0 | 0 | SO | IIEF | only sex health* | 2 | |
| Demir et al. (2013) | PR | 23 | Turkey | Women w/ ankylosing spondylitis | 39.3 | 0 | SODPL | FSFI | depressive sxs, vitality, physical health | BDI, SF-36, SF-36 | 15 |
| Denes (2012) | PR | 200 | US | Undergrad women & men from U of California, Santa Barbara | 19.6 | 59 | O | 1 item | relationship sat | MOQ | 1 |
| Denes (2018) | PR | 206 | US | Female & male college students | 19.3 | 68 | O | 1 item | relationship sat | MOQ | 2 |
| Dettore et al. (2013) | PR | 130 | Italy | Women w/ & w/out anxiety diagnoses | 29.5 | 100 | SODPL | FSFI | anxiety sxs | STAI | 10 |
| Dissiz (2018) | PR | 57 | Turkey | Women heroin users | 26.2 | 0 | SODPL | FSFI | depressive sxs | BDI | 7 |
| Dogan et al. (2017) | PR | 142 | Turkey | Women w/ & w/o migraines | 34.0 | 0 | OL | FSFI | depressive sxs | BDI | 2 |
| Duits et al. (2009) | PR | 19 | Netherlands | Men w/ history of strokes | 58.8 | 100 | SODE | IIEF | depressive sxs | SCL | 4 |
| Dunkley et al. (2016) | PR | 576 | Canada | Undergrad women from U of British Columbia | 20.8 | 37 | SODPL | FSFI | attachment | ECR | 10 |
| Dunn et al. (1999) | PR | 613 | UK | Women aged 18-75 | 50.0 | 0 | OL | ? | depressive sxs, marital difficulties | BDI, ? | 4 |
| Dyar et al. (2018) | PR | 279 | US | Young adult sexual & gender minorities assigned female at birth | 21.2 | 19 | SO | 3 items, 2 items | relationship sat | RAS | 3 |
| Eaton et al. (2017) | PR | 70 | US | Women w/ gynecologic cancer | 53.0 | 80 | OP | WSIDI | depressive sxs | PHQ | 2 |
| Eichel et al. (1988) | PR | 86 | US | Men & women who had or had not learned & practiced the coital alignment technique | 41.1 | 0 | SO | 1 item | only sex health* | 1 | |
| Ellero (2019) | MT | 330 | International | Portuguese or English speaking, sexually active women & men | 28.4 | 0 | SOD | 1 item | only sex health* | 4 | |
| Ellsworth & Bailey (2013) | PR | 112 | US | Female undergraduate students in relationships | 18.8 | 0 | O | 1 item | relationship sat | RAS | 1 |
| Fabre & Smith (2012) | PR | 281 | US | Women w/ depression | 38.3 | 88 | OD | CSFQ | depressive sxs | HAMD | 2 |
| Fabre et al. (2013) | PR | 326 | US | Men w/ major or atypical depression | 39.5 | 80 | OD | DISF | depressive sxs | HAMD | 2 |
| Fan et al. (2007) | PR | 64 | US | Women & men w/ schizophrenia in outpatient treatment | 43.5 | 70 | SOD | CSFQ | depressive sxs, quality of life | HAMD, QOL | 12 |
| Forbes et al. (2016) | PR | 336 | Australia | Sexually active women aged 19-65 | 29.5 | 100 | SO | FSFI | depressive sxs, | DASS | 2 |
| Frederick et al. (2017) | PR | 38747 | US | Heterosexual women & men in a relationship for at least 3 years | 39.4 | 87 | SO | 1 item | only sex health* | 4 | |
| Gallup et al. (2014) | PR | 54 | US | Heterosexual undergrad women in sexual relationships | 19.0 | 0 | SO | 1 item | only sex health* | 1 | |
| Garcia et al. (2007) | PR | 311 | US | Women enrolled in the Penn Ovarian Aging Study | 48.0 | 51 | SODL | FSFI | anxiety sxs | ZAI | 4 |
| Gewirtz-Meydan (2017) | PR | 256 | Israel | Heterosexual couples (dyads) | 34.4 | 87 | SOD | ISS, ISBI | only sex health* | 6 | |
| Gewirtz-Meydan & Finzi-Dottan (2018) | PR | 256 | Israel | Married or cohabitating couples, together 3+y & co-parenting 1+ children (dyads) | 34.4 | 0 | SOD | ISS, 3 items | attachment | ECR | 18 |
| Gomes & Nobre (2012) | PR | 1363 | Portugal | Sexually active men w/ & w/o erectile dysfunction | 37.7 | 0 | SODE | IIEF | only sex health* | 6 | |
| Goodman (2011) | DD | 1576 | US | Adult women & men collected online | 32.0 | 79 | O | 1 item | attachment, relationship sat | ECR, PRQC | 3 |
| Granata et al. (2013) | PR | 12 | Italy | Men aged 21-59 w/ Addison's disease | 40.5 | 100 | SOD | IIEF | only sex health* | 2 | |
| Grose (2016) | DD | 430 | US | Heterosexual undergrad women w/ a sex partner in the last year | 19.9 | 38 | SO | MSSCQ-S, FSFI | only sex health* | 2 | |
| Gunst et al. (2017) | PR | 2173 | Finland | Twin women | 25.5 | 100 | SODPL | FSFI | only sex health* | 10 | |
| Guo et al. (2004) | PR | 13498 | China | Newlywed women & men in Shanghai (dyads) | 27.8 | 0 | SO | 1 item | relationship sat | 1 item | 4 |
| Gutsche & Burri (2017) | PR | 159 | Switzerland | Adult women | 31.8 | 100 | SODPL | FSFI | relationship sat, | RAS | 15 |
| Haavio-Mannila & Kontula (1997) | PR | 2250 | Finland | Women & men aged 18-74 | 42.2 | 100 | SO | 2 items | only sex health* | 2 | |
| Harte & Meston (2012) | PR | 1207 | US | Undergrad sexually active men using & not using ED meds | 21.9 | 73 | SODE | IIEF | only sex health* | 6 | |
| Hassan et al. (2008) | PR | 354 | Turkey | Men w/ erectile dysfunction | 37.9 | 0 | SO | IIEF | only sex health* | 1 | |
| Havesi et al. (2017) | PR | 508 | Hungary | Undergrad women & patients w/ endometriosis or PCOS | 27.9 | 100 | SODPL | FSFI | only sex health* | 10 | |
| Hazewinkel et al. (2012) | PR | 76 | Netherlands | Women w/ history of vulvar cancer & radiotherapy | 68.0 | 100 | SOD | FSFI | physical health | SF-36 | 3 |
| Hevesi et al. (2019) | PR | 1843 | US & Hungary | Adult women | 28.8 | 0 | SO | 1 item | relationship sat | 1 item | 2 |
| Horton (1982) | DD | 99 | US | Women in relationships | 27.5 | 97 | SO | SII 1 item | only sex health* | 1 | |
| Hoyer et al. (2009) | PR | 451 | Germany | CBT outpatients w/ anxiety or depression diagnosis | 36.0 | 100 | SODLE | MGH | only sex health* | 9 | |
| Hoyer et al. (2009) | PR | 451 | Germany | Women & men at an outpatient mental health clinic | 36.0 | 100 | SODLE | MGH | only sex health* | 9 | |
| Hurlbert et al. (1993) | PR | 98 | US | Fort Hood, TX military wives | 26.7 | 68 | SOD | ISS, 1 item | only sex health* | 3 | |
| Hwang et al. (2019) | PR | 32 | South Korea | Women w/ & w/o stress urinary incontinence | 41.7 | 0 | SO | FSFI | only sex health* | 1 | |
| Jensen et al. (2004) | PR | 75 | Denmark | Gynecological cancer patients (cervical, endometrial, ovarian) aged 28-77 | 58.0 | 100 | SOL | SVQ | only sex health* | 2 | |
| Jones et al. (2017) | PR | 284 | US | Heterosexual couples (dyads) | 32.4 | 90 | SO | NSSS-S, 1 item | only sex health* | 2 | |
| Kahn (2001) | DD | 104 | US | Married women aged 25-40 | 31.7 | 0 | SO | ISS, 1 item | only sex health* | 1 | |
| Kalambach & Pillai (2014) | PR | 136 | US | Adult women | 20.7 | 82 | OP | FSDS-R | depressive sxs | CESD | 2 |
| Kalambach et al. (2012) | PR | 1258 | US | Undergrad women & men from Kent State U w/ depression &/or anxiety | 19.6 | 0 | SODPLE | FSFI/ MSFI, PFSF | general distress | MASQ | 3 |
| Kalambach et al. (2015) | PR | 171 | US | College women free of antidepressants | 20.1 | 81 | ODL | FSFI | depressive sxs | CESD | 22 |
| Kalmbach et al. (2019) | PR | 150 | US | Postmenopausal women w/ chronic insomnia | 56.4 | 52 | SODPL | FSFI | depressive sxs | BDI | 5 |
| Karabulitlu et al. (2011) | PR | 33 | Turkey | Women getting hemodialysis | 41.0 | 0 | SODPL | FSFI | depressive sxs | BDI | 5 |
| Kelley & Gidycz (2017) | PR | 501 | US | Undergrad women from Ohio U w/ & w/o history of sexual assault | 18.9 | 88 | ODPL | FSFI | depressive sxs | TSC-D | 10 |
| Keskin et al. (2019) | PR | 225 | Turkey | Dialysis patients | 43.0 | 0 | SOE | GRISS | depressive sxs | BSI | 3 |
| Khajehei et al. (2015) | PR | 295 | Australia | Postpartum women | 29.7 | 0 | SO | FSFI | depressive sxs, relationship sat | PHQ, RAS | 3 |
| Khnaba et al. (2016) | PR | 60 | Morocco | Women w/ rheumatoid arthritis | 45.2 | 0 | SODPL | FSFI | depressive sxs, vitality, physical health | HADS-D, SF-36, SF-36 | 15 |
| Klapilova et al. (2015) | PR | 170 | Czech Republic | Heterosexual couples (dyads) | 27.1 | 100 | SO | 1 item | relationship sat | DAS | 4 |
| Kracun et al. (2018) | PR | 200 | Israel | Women aged 21-44 attending antenatal classes | 30.5 | 0 | SODPL | FSFI | relationship sat | EMS | 10 |
| Kreuter et al. (1998) | PR | 84 | Sweden | Women & men post traumatic brain injury | 40.0 | 100 | SO | SIS, 1 item | only sex health* | 4 | |
| Leeners et al. (2014) | PR | 299 | Switzerland | Adult women | 50.0 | 100 | O | 1 item | depressive sxs | SCL | 1 |
| Leonhardt et al. (2018) | PR | 3366 | US | Heterosexual newlywed couples (dyads) | 28.6 | 62 | SO | GRISS, 1 item | relationship sat | CSI | 4 |
| Lew-Starowicz & Rola (2014) | PR | 204 | Poland | Women & men w/ multiple sclerosis | 50.3 | 100 | SODPLE | SFQ | depressive sxs | BDI | 9 |
| Llaneza et al. (2011) | PR | 117 | Spain | Post-menopausal women | 57.0 | 0 | OD | CSFQ | depressive sxs | CESD | 2 |
| Madewell (2013) | DD | 243 | US | Undergrad women from Oklahoma State U | 19.6 | 69 | SODP | GSF | only sex health* | 6 | |
| Maes (2017) | DD | 92 | US | Men enrolled in Osher Lifelong Learning Institute at U of Nevada, Las Vegas | 73.5 | 89 | SOE | MSHQ | perceived stress | PSSI | 3 |
| Masmoudi et al. (2018) | PR | 52 | Tunisia | Women aged 27-57 w/ & w/out multiple sclerosis | 37.7 | 0 | SODPL | FSFI | depressive sxs | BDI | 5 |
| McNicoll et al. (2017) | PR | 137 | Canada | Women reporting pain during sex | 32.2 | 0 | SO | FSFI | only sex health* | 1 | |
| Meadow (1982) | DD | 95 | US | Arizona married female community college students | 38.5 | 0 | SO | SIS | relationship sat | MAT | 3 |
| Mendes et al. (2008) | PR | 90 | Brazil | Men w/ spinal cord injury - retroactive pre-injury report | 33.5 | 0 | SODE | 1 item | only sex health* | 3 | |
| Mernone et al. (2019) | PR | 93 | Switzerland | Women aged 40-73 | 52.5 | 100 | SODPL | FSFI | life sat, relationship sat | SWLS, RAS | 10 |
| Monga et al. (1998) | PR | 82 | US | Women &men aged 29-74 in treatment for chronic pain | 49.9 | 67 | O | DISF | depressive sxs | CESD | 1 |
| Morales et al. (2013) | PR | 65 | Spain | Women w/ lupus | 39.0 | 0 | SODPL | FSFI | depressive sxs, vitality, physical health | SCL, SF-36, SF-36 | 15 |
| Moshfeghy et al. (2019) | PR | 100 | Iran | Sexually active married women w/ & w/out recurrent vulvovaginal candidiasis | 31.5 | 0 | SODPL | FSFI | depressive sxs | DASS-21 | 5 |
| Najafabady et al. (2011) | PR | 1200 | Iran | Reproductive aged women | 29.9 | 0 | SO | FSFI | anxiety | ? | 2 |
| Nascimento et al. (2015) | PR | 157 | Brazil | Hypertensive women | 56.4 | 0 | SODPL | FSFI | depressive sxs | HADS-D | 15 |
| Norhayati & Yacob (2017) | PR | 321 | Malaysia | Women w/ & w/out severe delivery complications | 30.2 | 0 | SO | FSFI | only sex health* | 1 | |
| Onem et al. (2008) | PR | 26 | Turkey | Patients w/ obstructive sleep apnea-hypopnea | 45.8 | 0 | SODPL | FSFI | depressive sxs | BDI | 5 |
| Opperman et al. (2013) | PR | 85 | Canada | Undergrad women in relationship | 20.8 | 100 | SODPL | FSFI | only sex health* | 10 | |
| Ozcan et al. (2015) | PR | 89 | Turkey | Adults w/ Parkinson's disease | 67.7 | 0 | ODLE | ASEX | depressive sxs | HAMD | 4 |
| Ozdemir et al. (2007) | PR | 98 | Turkey | Women & men w/ renal transplants | 36.1 | 0 | OD | ASEX | depressive sxs | BDI | 3 |
| Pakpour et al. (2015) | PR | 131 | Iran | Peri-menopausal women at a health center | 55.8 | 0 | SODPL | FSFI | stress, relationship sat | ?, ? | 20 |
| Papini et al. (2013) | PR | 44 | Italy | College women aged 21-47 | 26.1 | 100 | SODPL | FSFI | depressive sxs | SCL | 5 |
| Parish et al. (2007) | PR | 2411 | China | Sexually active women & men aged 20-64yo in long-term relationships | 40.4 | 0 | SO | 1 item | only sex health* | 2 | |
| Pascoal (2018) | PR | 248 | Portugal | Women & men in heterosexual couples | 29.5 | 0 | SODLE | GMSEX, FSFI | only sex health* | 12 | |
| Peixoto et al. (2019) | PR | 36 | Brazil | Postmenopausal women aged 45-65 at a climacteric clinic | 55.4 | 0 | SODPL | FSFI | mental health, vitality, physical health | SF-36 | 15 |
| Philippsohn & Hartmann (2009) | PR | 102 | Germany | Adult women | 36.7 | 100 | SO | 4 items, 1 item | only sex health* | 1 | |
| Pinney et al. (1987) | PR | 275 | US | College aged sexually active heterosexual women | 20.5 | 97 | SO | PSSI, 1 item | only sex health* | 1 | |
| Pinsky (2016) | MT | 248 | US | Male combat veterans w/ PTSD aged over 18y | 0.0 | 85 | SODE | IIEF | attachment | ECR | 19 |
| Powers (2012) | DD | 835 | US | Undergrad sexually active women from U of North Texas | 21.2 | 60 | O | 1 item | depressive sxs | QIDS | 1 |
| Randolph (2002) | DD | 63 | US | Women w/ endometriosis & suffering from chronic pelvic pain | 33.3 | 87 | OD | DISF | depressive sxs | CESD | 3 |
| Rosen et al. (2000) | PR | 259 | US | Women w/ & w/o sexual arousal disorder | 40.1 | 76 | SODPL | FSFI | only sex health* | 20 | |
| Rosen et al. (2019) | PR | 193 | Canada | Women w/ sexual arousal disorder & their male partners (dyads) | 31.2 | 86 | SO | FSFI | depressive sxs, relationship sat | BDI, CSI | 10 |
| Rottman et al. (2017) | PR | 574 | Denmark | Heterosexual, sexually active couples dealing w/ breast cancer (dyads) | 55.8 | 100 | SO | PROMIS | only sex health* | 2 | |
| Rowland & Kolba (2019) | PR | 2068 | US & Hungary | Adult women | 29.1 | 0 | O | 1 item | relationship sat | 1 item | 1 |
| Rowland et al (2018) | PR | 2304 | US & Hungary | Adult women | 28.8 | 0 | SO | 1 item | depression diagnosis; relationship sat | 1 item each | 3 |
| Sakinci et al. (2016) | PR | 159 | Turkey | Sexually active women at routine gynecology visits | 33.7 | 0 | SODPL | FSFI | depressive sxs | BDI | 15 |
| Sariyildiz et al. (2012) | PR | 70 | Turkey | Men aged 20-50 w/ ankylosing spondylitis | 36.4 | 0 | SODE | IIEF | depressive sxs | HADS-D | 4 |
| Sarti et al. (2010) | PR | 2087 | Italy | Women at menopausal clinics | 54.0 | 100 | O | 1 item | mental health, physical health | SF-12 | 2 |
| Scott et al. (2018) | PR | 206 | US | Women in lesbian couples | 33.7 | 73 | SO | 1 item | only sex health* | 1 | |
| Seldin et al. (2001) | PR | 493 | US | Adult women | 0.0 | 0 | O | 1 item | mental adjustment | 1 item | 1 |
| Shifren et al. (2008) | PR | 31581 | US | Women from a nationally representative sample | 49.5 | 81 | O | 3 items | depressive sxs | CSFQ | 1 |
| Skoczynski et al. (2019) | PR | 129 | Poland | Men aged 31-76 w/ & w/out obstructive sleep apnea | 57.9 | 100 | SO | IIEF | depressive sxs, relationship sat | HADS-D, ? | 5 |
| Speer et al. (2005) | PR | 55 | US | Women aged 41-69 surviving breast cancer | 53.4 | 100 | SOD | FSFI | relationship distress | MSI-R | 5 |
| Stephenson & Meston (2010) | PR | 319 | US | Women in sexually active heterosexual relationships w/ & w/o sexual arousal disorder | 22.8 | 63 | SODPL | FSFI | relationship sat | DAS | 28 |
| Stephenson et al. (2012) | PR | 176 | US | Women w/ & w/out history of childhood sexual abuse | 33.3 | 71 | SODPL | SSS-W, FSFI | only sex health* | 10 | |
| Stoeber & Harvey (2016) | PR | 289 | UK | College women & internet users aged 17-69 | 23.5 | 73 | SO | FSFI | only sex health* | 1 | |
| Takahashi et al. (2011) | PR | 126 | Japan | Women in partnered relationships | 38.1 | 0 | SODPL | FSFI | only sex health* | 10 | |
| Tao & Brody (2011) | PR | 158 | China | Women & men industrial workers | 40.2 | 0 | SO | MSQ, 1 item | only sex health* | 1 | |
| Tavares et al. (2017) | PR | 926 | Portugal | Sexually active heterosexual premenopausal women | 25.2 | 0 | O | 1 item | depressive sxs, positive affect, relationship sat | ?, PANAS, ? | 3 |
| Thakurdesai & Sawant (2018) | PR | 116 | India | Men w/ & w/o depression | 32.4 | 0 | SODE | IIEF | depressive sxs | BDI | 4 |
| Therrien & Brotto (2016) | PR | 255 | Canada | Women w/ sexual dysfunction | 0.0 | 82 | O | FSFI | depressive sxs, relationship sat | BDI, ? | 2 |
| Tracy & Junginger (2007) | PR | 350 | US | Lesbian women | 35.5 | 86 | SODPL | FSFI | psychological sxs, relationship sat | BSI, DAS | 20 |
| Træen (2007) | PR | 42 | Norway | Heart disease patients | 58.8 | 0 | SOD | 1 item | only sex health* | 3 | |
| Tuinman et al. (2010) | PR | 93 | Netherlands | Testicular cancer patients | 29.4 | 100 | OE | IIEF | depressive sxs | CESD | 2 |
| Tutino et al. (2017) | PR | 311 | Canada | College women aged 17-38 | 19.2 | 81 | ODPL | FSFI | depressive sxs | DASS | 10 |
| Uddenberg (1974) | PR | 94 | Sweden | Pregnant women & their mothers | 0.0 | 100 | SO | 1 item | only sex health* | 1 | |
| van der Brink et al. (2016) | PR | 399 | Netherlands | Undergrad women | 21.7 | 100 | SODPL | FSFI | attachment | ECR | 13 |
| van Nimwegen et al. (2015) | PR | 85 | Netherlands | Women w/ & w/out Sjogren's syndrome | 45.4 | 100 | SO | FSFI | depressive sxs | HADS-D | 2 |
| Villeda Sandoval et al. (2014) | PR | 200 | Mexico | Young adult women from Mexico City | 26.3 | 0 | O | FSFI | depression diagnosis | 1 item | 1 |
| Waite & Joyner (2001) | PR | 2195 | US | Women & men in national sample | 36.8 | 87 | SO | 1 item | relationship sat | 2 items | 4 |
| Wallace & Barbach (1974) | PR | 15 | US | Treatment of preorgasmic women | 27.5 | 88 | SO | 1 item | only sex health* | 1 | |
| Weiss & Brody (2011) | PR | 720 | Czech Republic | Women in relationships aged 35-65 | 47.6 | 100 | SO | 1 item | life sat, relationship sat | 1 item each | 3 |
| Witting et al. (2008) | PR | 2081 | Finland | Women aged 33-43 | 37.5 | 100 | SODPL | FSFI | only sex health* | 10 | |
| Witting et al. (2008) | PR | 2081 | Finland | Pregnant women, & women w/ children | 37.5 | 100 | SOD | FSFI | relationship sat | PRQC | 5 |
| Wongsomboon et al. (2019) | PR | 1315 | US | Women reporting committed or casual sex | 23.7 | 0 | SO | SSS-W, FSFI | only sex health* | 2 | |
| Yangin et al. (2008) | PR | 300 | Turkey | Menopausal women | 53.6 | 100 | SODPL | FSFI | depressive sxs | BDI | 5 |
| Yanikkerem et al. (2016) | PR | 298 | Turkey | Pregnant married women | 27.5 | 0 | SO | GRISS | relationship sat | MAS | 3 |
| Yela et al. (2018) | PR | 80 | Brazil | Women w/ premature ovarian insufficiency | 38.4 | 0 | SODPL | FSFI | mental health, physical health | WHOQoL | 10 |
| Yeoh et al. (2014) | PR | 269 | Malaysia | Married heterosexual couples in fertility treatments (dyads) | 33.2 | 0 | SODPLE | FSFI | only sex health* | 16 | |
| Young et al. (1998) | PR | 797 | US | Married women | 0.0 | 0 | SO | 3 items, 1 item | relationship sat | 1 item | 3 |
| Zhang et al. (2015) | PR | 1518 | China | Married women | 38.9 | 0 | SODPL | 1 item | life sat, relationship sat | 1 item each | 11 |
| Zhou (1993) | PR | 1789 | China | Adult women | 37.2 | 0 | SO | 1 item | only sex health* | 1 item | 1 |
Note. PR = peer reviewed article; DD = doctoral dissertation; MT = master's thesis; sxs = symptoms; sat = satisfaction; S = sexual satisfaction; O = orgasm; D = sexual desire; P = lack of pain; L = vaginal lubrication; E = erectile function. Sexual health scales: ASEX = Arizona Sexual Experience Scale; BSFQ = Brief Sexual Functioning Questionnaire; CSFQ = Changes in Sexual Functioning Questionnaire; DISF = Derogatis Interview for Sexual Functioning; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders – 4th edition; FSDS-R = Female Sexual Distress Scale – Revised; FSFI = Female Sexual Function Index; FSQ = Female Sexual Quotient; GMSEX = Global Measure of Sexual Satisfaction; GRISS = Golombok-Rust Inventory of Sexual Satisfaction; GSF = Global Sexual Functioning; IIEF = International Index of Erectile Function; ISBI = Israeli Sexual Behaviour Inventory; ISS = Index of Sexual Satisfaction; MGH = Massachusetts General Hospital Sexual Functioning; MSFI = Male Sexual Function Index; MSHQ = Male Sexual Health Questionnaire; MSQ = Multidimensional Sexuality Questionnaire; MSSCQ-S = Multidimensional Sexual Self-Concept Questionnaire – Sexual Satisfaction; NSSS-S = New Sexual Satisfaction Scale – Short; PFSF = Profile of Female Sexual Function; PROMIS = Patient-Reported Outcomes Measurement Information System; PSSI = Pinnes Sexual Satisfaction Inventory; SFQ = Female Sexual Function Questionnaire; SII = Sexual Interaction Inventory; SIS = Sexual Interest and Satisfaction; SSFS = Short Sexual Functioning Scale; SSS-W = Sexual Satisfaction Scale for Women; SVQ = Sexual function-Vaginal changes Questionnaire – Sexual Functioning; WSIDI = Women's Sexual Interest Diagnostic Interview. Correlate scales: BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; BSI = Brief Symptom Inventory; CESD = Center for Epidemiologic Studies Depression Scale; CIDI = World Health Organization’s Composite International Diagnostic Interview; CSI = Couples Satisfaction Index; DAS = Dyadic Adjustment Scale; DASS = Depression Anxiety Stress Scales; DASS-21 = 21-item Depression Anxiety Stress Scales; ECR = Experiences in Close Relationships; EMS = ENRICH Marital Satisfaction Scale; EPDS = Edinburgh Postnatal Depression Scale; GDS = Geriatric Depression Scale; GHQ = General Health Questionnaire; GMREL = Global Measure of Relationship Satisfaction; HADS-D = Hospital Anxiety and Depression Scale; HAMD = Hamilton Rating Scale for Depression;; LiSat = Life Satisfaction – life, relationship, & sexual satisfaction items; MAS = Marital Adjustment Scale; MASQ = Mood and Anxiety Symptom Questionnaire; MAT = Marital Adjustment Test; MHQ = Middlesex Hospital Questionnaire; MOQ = Marital Opinion Questionnaire; MSI-R = Marital Satisfaction Inventory – Revised; PANAS = Positive and Negative Affect Schedule; PHQ = Patient Health Questionnaire; PROMIS = Patient-Reported Outcomes Measurement Information System; PRQC = Perceived Relationship Quality Components – Global Relationship Quality; PRQC-S = Perceived Relationship Quality Components – Satisfaction; PSS = Perceived Stress Scale; QOL = Heinrichs Quality of Life Scale; RAS = Relationship Adjustment Scale; SCL = 90-item Symptom Check List; SF-12 = 12-item Short-Form Health Survey; SF-36 = 36-item Short-Form Health Survey; SRADM = Shaheen-Rakhawy Anxiety & Depression Measure; STAI = State and Trait Anxiety Inventory; = Satisfaction with Life Scale; TSC-D = Trauma Symptom Checklist – Depression; WHO-5 = The World Health Organization-Five Well-Being Index; WHOQoL = The World Health Organization Quality of Life; ZAI = Zung Anxiety Index.
Table 3.
Associations between Sexual Health and both Individual and Relationship Functioning Correlates.
Table 3.
Associations between Sexual Health and both Individual and Relationship Functioning Correlates.
| Category of Results | SMRel-Prob | Funnel Plot AsymZ | Trim and Fill adj. est. | ||||||||||
| Correlate variable | |||||||||||||
| Sexual health variables | k | N | r | SE | 95% CI | Q | I2 | r | k | ||||
| Sexual health links to correlates | |||||||||||||
| Psychological distress | |||||||||||||
| Sexual satisfaction | 53 | 9851 | -.248**** | .021 | [-.290, -.207] | 246.59**** | 76.19 | 0.98 | 0.74 | ||||
| Orgasms | 84 | 51914 | -.244**** | .024 | [-.292, -.197] | 10453.85**** | 97.11 | 2.26 | 0.89 | ||||
| Desire | 54 | 9875 | -.135**** | .034 | [-.201, -.069] | 976.01**** | 91.41 | 1.18 | -0.95 | ||||
| Lack of pain | 38 | 7651 | -.153** | .047 | [-.245, -.061] | 1355.70**** | 94.73 | 4.22 | -0.63 | ||||
| Lubrication | 42 | 8920 | -.143** | .046 | [-.233, -.053] | 2897.01**** | 96.26 | 1.90 | -0.48 | ||||
| Erectile function | 9 | 1087 | -.226* | .096 | [-.412, -.037] | 204.26**** | 92.42 | 0.91 | 0.28 | ||||
| Psychological well-being | |||||||||||||
| Sexual satisfaction | 14 | 2141 | .376**** | .056 | [.266, .486] | 283.96**** | 86.84 | 0.11 | -2.17* | .464**** | 19 | ||
| Orgasms | 20 | 9260 | .258**** | .040 | [.179, .337] | 577.42**** | 93.68 | 0.33 | -0.75 | ||||
| Desire | 12 | 3342 | .333**** | .083 | [.170, .496] | 318.07**** | 98.00 | 2.10 | -2.35* | .353**** | 13 | ||
| Lack of pain | 10 | 3278 | .282**** | .074 | [.138, .427] | 193.68**** | 95.20 | 27.33 | -2.65*** | .332**** | 12 | ||
| Lubrication | 10 | 3278 | .212** | .066 | [.083, .341] | 248.39**** | 91.32 | 4.65 | -0.23 | ||||
| Erectile function | 0 | 0 | |||||||||||
| Physical health | |||||||||||||
| Sexual satisfaction | 7 | 1467 | .370** | .121 | [.133, .608] | 223.23**** | 93.96 | 0.56 | -2.24* | .428*** | 8 | ||
| Orgasms | 9 | 3630 | .323*** | .083 | [.160, .486] | 625.69**** | 96.34 | 0.03 | -1.02 | ||||
| Desire | 8 | 1543 | .336*** | .098 | [.144, .529] | 194.70**** | 91.31 | 1.35 | -1.57 | ||||
| Lack of pain | 7 | 1467 | .261*** | .086 | [.093, .430] | 74.01**** | 84.45 | 43.83 | -1.72 | ||||
| Lubrication | 7 | 1467 | .269*** | .104 | [.065, .473] | 112.49**** | 90.29 | 4.76 | -1.36 | ||||
| Erectile function | 0 | 0 | |||||||||||
| Attachment anxiety | |||||||||||||
| Sexual satisfaction | 6 | 1536 | -.242**** | .035 | [-.310, -.174] | 11.74* | 59.36 | 0.88 | -0.15 | ||||
| Orgasms | 9 | 3979 | -.149**** | .022 | [-.193, -.105] | 10.43* | 64.31 | 0.91 | -2.58** | -.127**** | 12 | ||
| Desire | 5 | 1479 | -.043 | .046 | [-.133, .048] | 9.43 | 59.61 | 0.86 | -1.90 | ||||
| Lack of pain | 2 | 975 | -.145**** | .031 | [-.207, -.083] | 0.89 | 0.00 | 0.75 | |||||
| Lubrication | 2 | 975 | -.128**** | .032 | [-.190, -.067] | 0.22 | 0.00 | 0.75 | |||||
| Erectile function | 1 | 248 | |||||||||||
| Attachment avoidance | |||||||||||||
| Sexual satisfaction | 6 | 1536 | -.351**** | .064 | [-.477, -.225] | 40.76**** | 90.69 | 0.89 | 2.25**** | -.351**** | 6 | ||
| Orgasms | 9 | 3979 | -.241**** | .029 | [-.270, -.158] | 24.02** | 63.99 | 0.91 | -0.19 | ||||
| Desire | 5 | 1479 | -.124** | .046 | [-.213, -.034] | 9.71* | 64.27 | 0.86 | 2.03* | -.124* | 5 | ||
| Lack of pain | 2 | 975 | -.165**** | .040 | [-.243, -.088] | 1.58 | 36.82 | 0.75 | |||||
| Lubrication | 2 | 975 | -.279**** | .070 | [-.416, -.142] | 5.56* | 82.02 | 0.75 | |||||
| Erectile function | 1 | 248 | |||||||||||
| Relationship satisfaction | |||||||||||||
| Sexual satisfaction | 22 | 45945 | .529**** | .042 | [.447, .611] | 6393.69**** | 99.31 | 0.04 | -2.96** | .589**** | 27 | ||
| Orgasms | 51 | 41547 | .271**** | .033 | [.207, .335] | 25110.64**** | 99.14 | 0.25 | -2.02* | .338**** | 64 | ||
| Desire | 14 | 6810 | .225* | .059 | [.110, .339] | 907.31**** | 96.64 | 3.68 | -2.21* | .285**** | 17 | ||
| Lack of pain | 10 | 3895 | .163** | .057 | [.052, .273] | 53.01**** | 89.54 | 1.38 | 0.12 | ||||
| Lubrication | 12 | 6026 | .141*** | .038 | [.066, .216] | 69.20**** | 85.83 | 1.43 | -0.01 | ||||
| Erectile function | 1 | 248 | |||||||||||
| Links among sexual health dimensions | |||||||||||||
| Sexual satisfaction correlating with | |||||||||||||
| Orgasms | 118 | 103,458 | .416**** | 0.021 | [.376, .456] | 62950.63**** | 99.36 | 0.11 | -2.38** | .482**** | 140 | ||
| Desire | 41 | 15974 | .418**** | .033 | [.353, .4831] | 3243.58**** | 97.74 | 4.61 | -2.34* | .493**** | 50 | ||
| Lack of pain | 21 | 9950 | .349**** | .057 | [.237, .461] | 1095.71**** | 98.13 | 0.65 | -2.98*** | .349**** | 21 | ||
| Lubrication | 24 | 10852 | .459**** | .044 | [.372, .549] | 937.17**** | 97.79 | 0.13 | -4.24**** | .532**** | 30 | ||
| Erectile function | 10 | 4605 | .461**** | .040 | [.383, .538] | 93.79**** | 89.65 | 0.36 | 0.45 | ||||
| Orgasms correlating with | |||||||||||||
| Desire | 44 | 15557 | .335**** | .027 | [.282, .387] | 791.52**** | 92.94 | 0.32 | -2.32* | .381**** | 52 | ||
| Lack of pain | 22 | 9244 | .372*** | .048 | [.277, .467] | 1233.55**** | 97.14 | 0.13 | -2.11* | .396**** | 24 | ||
| Lubrication | 24 | 10071 | .551**** | .047 | [.460, .643] | 1872.90**** | 99.09 | 0.04 | -5.58**** | .563**** | 25 | ||
| Erectile function | 8 | 4473 | .537**** | .039 | [.461, .613] | 105.00**** | 91.80 | 0.10 | -1.36 | ||||
| Desire correlating with | |||||||||||||
| Lack of pain | 22 | 9244 | .246**** | .030 | [.186, .305] | 142.90**** | 87.74 | 1.00 | 0.70 | ||||
| Lubrication | 24 | 10071 | .408**** | .028 | [.354, .462] | 245.57**** | 90.12 | 0.04 | -1.50 | ||||
| Erectile function | 8 | 4473 | .423**** | .076 | [.273, .570] | 268.43**** | 97.58 | 0.10 | -1.166 | ||||
| Lack of pain correlating with | |||||||||||||
| Lubrication | 20 | 8538 | .533**** | .041 | [.452, .614] | 962.50**** | 97.41 | 0.05 | -3.11** | .572**** | 23 | ||
| Erectile function | 0 | ||||||||||||
| Lubrication correlating with | |||||||||||||
| Erectile function | 0 | ||||||||||||
Note. SM Rel-Prob = the relative probability of finding a contradictory finding (i.e., non-significant or in the opposite direction to a majority of the other effects for that pair of variables) compared to finding a consistent finding (estimated using the selection method analyses of McShane et al., 2016). Numbers close to 1 suggest no publication bias and numbers over 1 suggest a greater relative likelihood of non-significant or counter-intuitive findings getting published. Funnel Plot Asym Z = Eggers test of funnel plot asymmetry, another test of possible publication bias. Trim and fill methods were used to adjust the estimates of effects showing significant asymmetry. Significant effects have been bolded for ease of interpretation. N/A = These correlations are between constructs measured only in women or men but not in both genders (i.e., unique to either the FSFI or the IIEF but not common to both). **** p < .0001, *** p < .001, ** p < .01, * p < .05.
Table 4.
Results of Path Models on Meta-Analytic Correlation Matrices.
| MODEL | 99% Cis | MODEL | 99% Cis | |||||||||||
| Correlate being predicted | Correlate being predicted | |||||||||||||
| Predictors | b | p | LL | UL | Predictors | b | p | LL | UL | |||||
| PSYCH DISTRESS MODEL | WELL-BEING MODEL | |||||||||||||
| SexH → psychological distress | SexH → well-being | |||||||||||||
| Sexual satisfaction | -.191 | <.001 | -.227 | -.155 | Sexual satisfaction | .396 | <.001 | .336 | .457 | |||||
| Orgasms | -.182 | <.001 | -.217 | -.146 | Orgasms | .027 | .242 | -.032 | .086 | |||||
| Desire | .005 | .678 | -.028 | .039 | Desire | .179 | <.001 | .124 | .235 | |||||
| Lack of pain | -.073 | <.001 | -.108 | -.039 | Lack of pain | .281 | <.001 | .223 | .338 | |||||
| Lubrication | .101 | <.001 | .060 | .141 | Lubrication | -.248 | <.001 | -.315 | -.180 | |||||
| SexH → sex satisfaction | SexH → sex satisfaction | |||||||||||||
| Orgasms | .198 | <.001 | .169 | .226 | Orgasms | .198 | <.001 | .144 | .251 | |||||
| Desire | .295 | <.001 | .269 | .320 | Desire | .295 | <.001 | .246 | .343 | |||||
| Lack of pain | .039 | <.001 | .011 | .067 | Lack of pain | .039 | .056 | -.014 | .092 | |||||
| Lubrication | .278 | <.001 | .246 | .310 | Lubrication | .278 | <.001 | .218 | .338 | |||||
| Indirect paths | Indirect paths | |||||||||||||
| Orgasm à SexSat à Distress | -.038 | -.047 | -.029 | Orgasm à SexSat à Well-being | .078 | .054 | .103 | |||||||
| Desire à SexSat à Distress | -.056 | -.068 | -.045 | Desire à SexSat à Well-being | .117 | .091 | .143 | |||||||
| L-pain à SexSat à Distress | -.007 | -.013 | -.002 | L-pain à SexSat à Well-being | .016 | -.006 | .037 | |||||||
| Lube à SexSat à Distress | -.053 | -.065 | -.041 | Lube à SexSat à Well-being | .110 | .081 | .139 | |||||||
| PHYSICAL HEALTH MODEL | REL SATISFACTION MODEL | |||||||||||||
| SexH → perceived health | SexH → rel satisfaction | |||||||||||||
| Sexual satisfaction | .301 | <.001 | .225 | .378 | Sexual satisfaction | .657 | <.001 | .616 | .697 | |||||
| Orgasms | .125 | <.001 | .050 | .200 | Orgasms | .193 | <.001 | .153 | .233 | |||||
| Desire | .147 | <.001 | .077 | .217 | Desire | .020 | .174 | -.018 | .057 | |||||
| Lack of pain | .123 | <.001 | .050 | .195 | Lack of pain | .057 | <.001 | .019 | .096 | |||||
| Lubrication | -.092 | .006 | -.177 | -.006 | Lubrication | -.358 | <.001 | -.403 | -.312 | |||||
| SexH → sex satisfaction | SexH → sex satisfaction | |||||||||||||
| Orgasms | .198 | <.001 | .133 | .262 | Orgasms | .198 | <.001 | .158 | .237 | |||||
| Desire | .295 | <.001 | .236 | .353 | Desire | .295 | <.001 | .259 | .330 | |||||
| Lack of pain | .039 | .114 | -.025 | .103 | Lack of pain | .039 | .010 | .000 | .078 | |||||
| Lubrication | .278 | <.001 | .205 | .351 | Lubrication | .278 | <.001 | .233 | .323 | |||||
| Indirect paths | Indirect paths | |||||||||||||
| Orgasm à SexSat à Health | .060 | .035 | .084 | Orgasm à SexSat à RelSat | .130 | .103 | .157 | |||||||
| Desire à SexSat à Health | .089 | .060 | .117 | Desire à SexSat à RelSat | .193 | .167 | .220 | |||||||
| L-pain à SexSat à Health | .012 | -.008 | .031 | L-pain à SexSat à RelSat | .026 | .000 | .051 | |||||||
| Lube à SexSat à Health | .084 | .053 | .114 | Lube à SexSat à RelSat | .183 | .151 | .214 | |||||||
| ATTCH AVOIDANCE MODEL | ATTCH ANXIETY MODEL | |||||||||||||
| Attch avoidance → SexH | Attch anxiety → SexH | |||||||||||||
| Sexual satisfaction | -.200 | <.001 | -.265 | -.136 | Sexual satisfaction | -.168 | <.001 | -.231 | -.104 | |||||
| Orgasms | -.241 | <.001 | -.321 | -.161 | Orgasms | -.127 | <.001 | .107 | .263 | |||||
| Desire | -.124 | <.001 | -.206 | -.042 | Desire | -.043 | .179 | -.125 | .039 | |||||
| Lack of pain | -.165 | <.001 | -.246 | -.084 | Lack of pain | -.145 | <.001 | -.227 | -.063 | |||||
| Lubrication | -.279 | <.001 | -.358 | -.200 | Lubrication | -.128 | <.001 | -.210 | -.046 | |||||
| SexH → sex satisfaction | SexH → sex satisfaction | |||||||||||||
| Orgasms | .172 | <.001 | .095 | .250 | Orgasms | .185 | <.001 | .107 | .263 | |||||
| Desire | .297 | <.001 | .228 | .366 | Desire | .299 | <.001 | .229 | .369 | |||||
| Lack of pain | .040 | .171 | -.036 | .116 | Lack of pain | .023 | .448 | -.054 | .099 | |||||
| Lubrication | .235 | <.001 | .147 | .322 | Lubrication | .271 | <.001 | .184 | .359 | |||||
| Indirect paths | Indirect paths | |||||||||||||
| Avoid à Orgasm à SexSat | -.042 | -.065 | -.018 | Anxiety à Orgasm à SexSat | -.023 | -.042 | -.005 | |||||||
| Avoid à Desire à SexSat | -.037 | -.063 | -.011 | Anxiety à Desire à SexSat | -.013 | -.038 | .012 | |||||||
| Avoid à L-pain à SexSat | -.007 | -.020 | .006 | Anxiety à L-pain à SexSat | -.003 | -.015 | .008 | |||||||
| Avoid à Lube à SexSat | -.066 | -.096 | -.035 | Anxiety à Lube à SexSat | -.035 | -.060 | -.010 | |||||||
Note: Consistent with the EVSA and ASA conceptual models, sexual health was treated as a predictor for the correlates of psychological distress, well-being, physical health, and relationship satisfaction whereas attachment avoidance and anxiety were treated as predictors of sexual health. SexH = sexual health; SexSat = sexual satisfaction; L-pain = lack of pain; RelSat = relationship satisfaction; Attch = attachment; Avoid = attachment avoidance; Anxiety = attachment anxiety. All path models were run on correlation matrices of meta-analytic estimates using Mplus 7.11. The models were fully saturated and therefore gave perfect fit. Path coefficients significant at p < .01 have been bolded for ease of interpretation.
Table 5.
Examining Moderation of Links between Orgasms and Correlates.
| Sexual Health Indicator | ||||||||||||||||
| Correlate being predicted | Sexual Satisfaction | Orgasms | Desire | Lack of Pain | Lubrication | |||||||||||
| Moderators tested | estimate | p | estimate | p | estimate | p | estimate | p | estimate | p | ||||||
| Predicting sexual satisfaction | ||||||||||||||||
| intercept | --- | --- | .444 | <.0001 | .340 | .009 | .580 | .004 | .829 | <.0001 | ||||||
| Male contrast | --- | --- | -.172 | .000 | -.046 | .548 | --- | --- | --- | --- | ||||||
| Age (centered at 38.9yrs) | --- | --- | .001 | .701 | .007 | .040 | .010 | .071 | .004 | .383 | ||||||
| Clinical population contrast | --- | --- | .145 | .001 | .036 | .595 | .043 | .726 | .064 | .505 | ||||||
| Peer-reviewed contrast | --- | --- | -.025 | .670 | .131 | .293 | -.224 | .275 | -.404 | .068 | ||||||
| Predicting psychological distress | ||||||||||||||||
| intercept | -.345 | .001 | -.138 | .151 | -.207 | .439 | -.229 | .030 | -.089 | .338 | ||||||
| Male contrast | .037 | .520 | .064 | .314 | .119 | .233 | --- | --- | --- | --- | ||||||
| Age (centered at 38.9yrs) | -.001 | .783 | -.006 | .006 | .002 | .487 | .003 | .511 | -.003 | .573 | ||||||
| Clinical population contrast | .020 | .744 | -.018 | .732 | -.172 | .065 | .101 | .415 | -.088 | .426 | ||||||
| Peer-reviewed contrast | .077 | .509 | -.115 | .247 | .196 | .438 | --- | --- | --- | --- | ||||||
| Predicting psychological well-being | ||||||||||||||||
| intercept | .501 | <.0001 | .291 | <.0001 | .513 | .003 | .524 | <.0001 | .129 | .366 | ||||||
| Male contrast | -.307 | .073 | -.153 | .291 | -.244 | .436 | --- | --- | --- | --- | ||||||
| Age (centered at 38.9yrs) | .007 | .075 | -.001 | .766 | .004 | .747 | -.006 | .492 | .005 | .637 | ||||||
| Clinical population contrast | -.152 | .150 | -.026 | .764 | -.241 | .219 | -.344 | .011 | .106 | .527 | ||||||
| Predicting relationship satisfaction | ||||||||||||||||
| intercept | .742 | <.0001 | .276 | .015 | .229 | .027 | .125 | .074 | .079 | .080 | ||||||
| Male contrast | -.030 | .781 | -.106 | .203 | -.056 | .816 | --- | --- | --- | --- | ||||||
| Age (centered at 38.9yrs) | .005 | .303 | .001 | .808 | .007 | .196 | .009 | .010 | .003 | .380 | ||||||
| Clinical population contrast | -.040 | .665 | .010 | .890 | -.013 | .925 | .047 | .615 | .123 | .066 | ||||||
| Peer-reviewed contrast | -.224 | .074 | .018 | .870 | --- | --- | --- | --- | --- | --- | ||||||
Note. Weighted mixed-effects linear meta-regression models were run with the rma function of the metafor package in Rstudio to simultaneously test the unique contributions of the potential moderators in predicting links between orgasms and each of the 4 outcome variables with sufficient numbers of studies to support these analyses. Significant effects have been bolded for ease of interpretation. --- indicates effects not possible to estimate (i.e., sexual satisfaction predicting sexual satisfaction or male gender moderating lack of vaginal pain or vaginal lubrication) or effects with too few studies to estimate (which was often the case for the peer-reviewed moderator).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



