
Submitted:
28 April 2025
Posted:
29 April 2025
You are already at the latest version
Abstract
The Joint Clinical Assessment (JCA) evaluates the relative effectiveness (RE) of 4 interventions over comparators. While randomized control trials (RCTs) are considered 5 the gold standard, single-arm trials (SATs) require an external control for accurate RE 6 estimation. This study reviewed Health Technology Assessment (HTA) opinions for 7 medicinal products supported by SATs in France, Germany, Poland, and Spain, and 8 simulated the JCA assessment for these products based on evidence submitted in France. 9 Among HTA opinions published in France in 2019-2024, 16% were SAT-driven, and 5.6% 10 of them included external controls. SAT-supported drugs had a high reimbursement 11 approval rate (74%) and showed better HTA outcomes when controls were used. In 12 Germany, 64% of SAT-based opinions indicated no added benefit and 30% - non- 13 quatifiable benefit. In Poland and Spain, 63% and 72% opinions recommending 14 reimbursement, respectively. Despite wide acceptance by Member States, experts 15 determined that 94% of SAT-supported products would not qualify for JCA review due 16 to insufficient evidence. Only 6% would qualify for JCA for a likely limited number of 17 PICOs (Population-Intervention-Comparator-Outcome), but the certainty rating would be 18 low. These findings suggest that SATs, as primary evidence, may not be suitable for JCA, 19 potentially undermining HTA assessments in EU Member States.
Keywords:
Joint Clinical Assessment
; single-arm trial
; health technology assessment
1. Introduction
The implementation of the Joint Clinical Assessment (JCA) in the European Union (EU) [1] represents a significant reform in how new health technologies, particularly medicinal products, are evaluated across Member States (MS). This initiative is part of the broader Health Technology Assessment (HTA) Regulation (EU 2021/2282) [2], which aims to streamline processes and enhance patient access to innovative treatments [1,2].
The HTA Regulation was enacted in January 2022, laying the groundwork for the JCA framework. It aims to standardise assessments across the EU, reducing redundancy and improving access to health technologies [1,3]. Starting from January 12, 2025, the JCA applies to new medicines intended for cancer treatment and advanced therapy medicinal products (ATMPs), expansion to broader inclusion in 2028 to orphan drugs, and all other medicinal products by 2030 is foreseen in the regulation [3,4].
The objective of assessments under JCA is to support national HTA processes with scientific analysis of clinical evidence conducted in a standardized and harmonized manner [3]. The primary output will be a detailed report generated by assessors and co-assessors based on the review of submitted evidence from health technology developers (HTD). This report will summarize clinical evidence, focusing on the relative effectiveness and safety without making judgments about clinical added value or cost-effectiveness [1]. The report is intended to provide MS states with essential data to inform their own national assessments and decision-making processes regarding the adoption of new health technology. MS are required to provide due consideration of these reports but retain the responsibility for making their own conclusions regarding clinical added benefit, value, and reimbursement decisions based on their national HTA framework and health priorities [5].
The JCA utilizes a standardized methodology developed through previous collaborative efforts by EUnetHTA, which concluded its work in September 2023. The assessment is driven by a set of procedural guidance documents, methodological and practical guidelines, and template documents, which have been successively released since March 2024 [6]. The PICO (Population, Intervention, Comparator, Outcomes) framework is adopted to define the scope of the assessment and ensure that the evaluations are relevant to specific patient populations and treatment contexts [5].
The comparator is an essential component of the assessment because JCA focuses on assessing the degree of certainty and the size of the relative effectiveness and safety of a health technology compared to existing treatments or standard care. HTDs are expected to provide robust data demonstrating how their product compares to existing treatments under each defined PICO. Well-designed RCTs with a low risk of bias are considered the "gold standard" for informing estimates of treatment relative effectiveness, and direct comparisons based on adequate RCTs should be applied whenever possible. If RCTs are not feasible, single-arm trials (SATs) may be accepted, especially when combined with an external control arm [7].
The validity of clinical studies used for the JCA is determined by three key dimensions: internal validity, external validity, and statistical precision. A JCA report should explicitly state the study design used and provide a comprehensive assessment of the certainty of the reported relative effectiveness, taking into account all three dimensions [8]. Statistical precision is typically communicated using confidence intervals (CIs), while external validity assessment is more complex and depends on how well the study design resembles the real-life target population and treatment conditions under the various PICOs. To assess the risk of bias associated with the internal validity of RCTs, the Cochrane Risk of Bias (RoB) tool, specifically the RoB version 1, is recommended [8].
In the case of SATs, no formal rules for assessing the risk of bias of the SAT are considered because the lack of a comparator precludes performing direct relative effectiveness assessments. However, when used with an external source of data as a control arm, the certainty of the relative effectiveness is determined by the internal, external validity and statistical precision of the outcome of indirect treatment comparison (ITC), rather than the single-arm trial by itself [8].
Single-arm trials are utilized primarily in specific contexts where traditional RCTs may not be feasible or ethical. Most often, these are rare diseases, including rare cancers, where the patient population is too small to achieve the statistical power required in RCTs. Also, in life-threatening conditions where standard care is not effective, preventing patients in the comparator arm from receiving potentially effective treatment may be considered unethical [9].
SATs are an important tool in clinical research contributing to regulatory decision-making and ultimately improving patient access to innovative therapies [10]. The objective of this research was to review Health Technology Assessments (HTA) opinion in selected MS for products supported by SATs and to simulate the probable JCA outcomes for the same products applying the published procedural guidance documents.
2. Materials and Methods
HTA opinions in France containing SAT were identified in the NaviHTA database (https://www.inovintell.com/). Opinions issued between 2019 and 2024 were included in the analysis. If an HTA report contained two or more subgroups of patients with distinct opinions, they were considered separate HTA opinions. Only opinions, where SAT was the key source of clinical efficacy, were included. If the opinion referred to any direct comparative study, it was excluded from the analysis. The opinions were analysed in terms of the indication, presence of unanchored ITC with external control, the use of a matching-adjusted indirect comparison (MAIC), and the final rating of actual benefit (SMR) and improvement in the actual benefit (ASMR). Based on the HTA reports in France, ITCs with external control and matching-adjusted methodology for the comparisons were identified. Since the ITC could be available only for selected subpopulations within the same HTA report and, ultimately, drive different HTA outcomes, the availability of ITCs was reported for individual HTA opinions. All these data were extracted from the NaviHTA database.
For all identified products having SAT-driven HTA opinions in France, opinions in Germany, Poland, and Spain were searched on the websites of the national HTA agencies (G-BA, AOTMiT and AEMPS). Identified HTA reports were reviewed. Opinions for different patient subgroups were identified and considered. Availability of direct comparative clinical trials not included in the French opinions was an exclusion criterion. Similarly, as in the case of French reports, if the reports contained two or more distinctive opinions, they were considered separate HTA opinions. If the opinions referred to direct comparative clinical trials (including crossover studies), they were excluded from the analysis. For the included opinions, the following data were extracted: indication, opinion date, the final added benefit rating and the resolution statement (in the case of G-BA opinions), reimbursement recommendation, and type of market access pathway (in the case of AOTMiT) or the assessment outcome and the conclusion statement (in the case of AEMPS).
As reimbursement is systematic in Germany, the availability of products on the German market based on information in the global pricing database was extracted and considered as a proxy of reimbursement to allow comparison with other jurisdictions [11].
The orphan status was identified for all products on the European Medicines Agency (EMA) database [12].
Based on data extracted from the NaviHTA database for SAT-driven HTA opinions in France, the JCA assessment simulation was conducted. When no ITC was available, products were considered as not assessable in line with JCA Guidance on Validity of Clinical Studies [8]. When ITC was available, a JCA assessment was performed. Guidance on Validity of Clinical Studies [8] and Methodological Guideline for Quantitative Evidence Synthesis: Direct and Indirect Comparisons [7] were applied independently by 2 experts in the field, and the outcome was reported. In case of disagreement, direct conciliation between the two experts was considered. In case of persistent disagreement, a third expert was appointed to arbitrate between the two initial experts.
When relevant for enlightening HTA opinion, the rationale and/or the context were reported.
Acceptability was defined in France, Poland, and Spain as achieving reimbursement for a single product for at least one of the indications or subgroups that was filed to HTA bodies. In Germany, products are reimbursed once the price is accepted by HTD. HTA informs the price rather than reimbursement. Therefore, acceptability was defined as market availability and reimbursement.
For JCA, acceptability was defined as reaching a level of certainty for the comparative effectiveness outcome that surpassed the lowest acceptable level. The acceptability derived from the JCA simulation was then compared to the acceptability results from the four countries.
3. Results
3.1. Characteristics of Products with SAT
At the time of the analysis (January 2025), the NaviHTA database contained 883 HTA opinions in France issued between the 1st of January 2019 and the 31st of December 2024. Among those, 141 opinions (16%) were based on an evidence package containing an SAT as the key source of clinical evidence. As a single HTA report could contain more than one HTA opinion, for example, for subgroups, 141 opinions come from 116 HTA reports for 96 different medicinal products.
Nearly half of the products were for oncology indications (44%, 42 products), of which 48% (20 products) were for haematological cancers. According to the EMA database, 33% of products (31) had an orphan drug status, of which half of them (15) were oncology products [13]. The most prevalent oncology indications were lymphomas (10 products) followed by non-small cell lung cancer (7 products) and Multiple Myeloma (6 products). Among non-oncology products, the most frequent indications were: human immunodeficiency virus (HIV) infection (7 products), chronic hepatitis C (4 products), cystic fibrosis and haemophilia A (3 products each). Ten drugs (10%) were classified by the EMA as ATMPs [13].
Out of all 141 HTA opinions driven by SAT, only 8 opinions (6%, 6 products) included any ITC with an external control arm to allow assessment of relative effectiveness. Among those, 4 opinions (3 products) were supported by ITC, which adopted the MAIC approach, and the remaining 4 opinions (3 products) were based on unadjusted methodology.
3.2. Analysis of HTA Opinions in Selected EU Countries
3.1.1. France
Out of all 141 HTA opinions for the total of 96 different products, a significant majority (74%, 104 opinions) was positive, with actual benefit (SMR) ratings ranging from low to important. Positive opinions concerned 82 different products. Over half of the opinions (58%, 82 opinions) indicated an important SMR level (Figure 1).
Eight HTA opinions for 6 products, included an ITC, all indicated an important SMR, except one. However, the negative HTA opinion concerned one subgroup of patients with the Neuromyelitis Optica spectrum disorder treated with Ultomiris® (ravulizumab), while this product received a positive SMR in another subgroup with this indication (patients who failed background immunosuppressive therapy).
Regarding the assessment of improvement in actual benefit (ASMR), 46% of HTA opinions (65 opinions) indicated no improvement (ASMR V) and the frequency of opinions with improved ASMR decreased with the decreasing level of ASMR (16%, 9% and 3% for ASMR IV, III and II, respectively) (Figure 2).
Opinion supported by an ITC obtained higher ratings of ASMR: the rate of opinions with ASMR III was well higher when supported by an ITC compared to the opinions without external control (38% and 8%, respectively). The rate of opinions with ASMR V was similar in both groups (Figure 3). However, the number of opinions with an ITC was low (8 opinions for 6 products).
3.1.2. Germany
The search of HTA opinions for products identified as having SAT in France revealed 123 opinions in Germany for a total of 65 medicinal products. A large majority of the opinions (64%, 79 opinions) were rated as no proof of added benefit. For most of the remaining cases (30%, 37 opinions), opinions were rated non-quantifiable added benefits. In 6% of opinions (7 opinions), despite SAT-derived clinical data, it was possible to quantify the level of added benefit. One opinion indicated a major added benefit, while the 6 remaining were rated as a minor added benefit (Figure 4). Those opinions concerned three products: Brineura® (cerliponase alfa), Libtayo® (cemiplimab) and Sovaldi® (sofosbuvir), where the latter was assessed separately in 5 different subgroups of patients with hepatitis C, which all received an added benefit.
Considering high direct comparative data needs in Germany, 7 opinions, which were based on SAT and included added benefit recognition, were reviewed for justification.
In the justification of the major added benefit rating for Brineura®, the G-BA noted uncertainties associated with the historical comparisons but indicated the rarity of the disease, the paediatric patient population, and the deterministic disease course. The assessment also considered long-term data confirming previous findings of morbidity and mortality advantages [14]. In the opinion of Libtayo®, the minor added benefit assessment was justified based on the lack of relevant effects on clinical response under the comparator therapy of best supportive care, while for the assessed treatment, a hint of advantage in clinical response was found [15]. Justification of minor added benefit assessment of Sovaldi® in all five subgroups of patients with chronic hepatitis C indicated that despite not meeting the highest evidence standards typically required single-arm studies compared to historical controls are acceptable because the disease can cause severe complications, and current interferon-based treatments are lengthy and have serious side effects [16].
Among all 65 medicinal products assessed in Germany, 4 products have been withdrawn, giving an eligibility rate of 94%. HTA opinions for 2 of them indicated no added benefit (Gavreto® and Tabrecta®) while for the other 2 products, non-quantifiable added benefit (Copiktra® and Zynteglo®). Publicly available information confirms that the withdrawal of Tabrecta® was directly associated with negative added benefit assessment [17]. In the case of Zynteglo®, despite the non-quantifiable added benefit, it was withdrawn after failing to reach an agreement with health authorities on the treatment’s price [18]. Gavreto® was withdrawn from the whole EU in January 2025 due to commercial reasons [19]. Copiktra® is still available in the EU, but according to the pricing database, it was withdrawn from Germany a few months before the publication of the G-BA resolution in July 2022.
3.1.3. Poland
Among 96 products identified as having SAT in France, only 40 had HTA opinions in Poland, with 49 HTA opinions available. A majority of the opinions (63%, 31 opinions) were positive and recommended reimbursement of the products, which were evaluated based on SATs (Figure 5).
Since in Poland, different market access pathways could be applied depending on the product profile (a standard pathway, a pathway for drug technologies with a high level of innovation (TLI), and a pathway for drug technologies with high clinical value (TLK)) [20,21], HTA opinions were analysed separately for each pathway. Twenty-two products were assessed using the standard pathway, 18 were assessed using TLI, and 2 using TLK pathways. The analysis (Figure 6) did not reveal significant differences between the pathways, and the rates of positive and negative recommendations were consistent with the overall analysis. The standard pathway and the TLI showed 60% of opinions being positive, concerning 13 and 10 products, respectively. The TLK pathway seems to allow for higher acceptability than other pathways, but since the rate was based only on 4 opinions for 2 products, the trend is highly uncertain (Figure 6).
3.1.4. Spain
Analysis of the AEMPS website revealed 58 HTA opinions for 46 products with SAT. The majority of opinions (72%, 48 opinions) were positive, while the remaining (28%, 16 opinions) were negative (Figure 7).
Many drugs were conditionally accepted based on limited data, pending further research and long-term efficacy and safety results to establish precise positioning. The conclusions of the HTA agency also indicated specific patient populations characterised by the high severity of the disease or lack of alternatives and suggested individual risk/benefit assessments when making treatment decisions.
3.2. Simulation of JCA of Drugs Supported by SATs and Comparison with National HTA Opinions
Analysis of HTA opinions for medicinal products with SAT in countries of scope shows that, despite limitations of the single-arm design, the majority of products have been accepted at the HTA stage (Table 1).
The JCA simulation did not show a discrepancy between experts. Neither conciliation nor arbitration were requested.
All products with no indirect comparative evidence (94%, 90 products) have been classified as non-assessable and excluded from the assessment. For such products, no JCA report would be issued.
Six products with an ITC have been assessed under JCA guidance, which represents 6% of all products evaluated in France based on SAT. Those products were considered qualifying for JCA for a likely limited number of PICOs (Population-Intervention-Comparator-Outcome). However, in line with the JCA guidance documents, all of them received the lowest degree of certainty because of unanchored ITC.
The comparison between JCA and countries in scope is reported in Table 1.
4. Discussion
This study aimed to assess the proportion of SAT-supported products that gain reimbursement or market access (availability) in France, Germany, Spain, and Poland. These countries primarily rely on direct comparative evidence for granting availability as defined in the methodology section. Availability was compared between these four countries, and JCA outcomes obtained by simulation performed by two experts in the field. This study confirms that SAT-supported products have a high availability rate in the 4 countries of scope, despite not meeting HTA requirements (direct comparative evidence). In contrast, JCA-related availability was zero. Although the JCA report does not recommend reimbursement per se, MS are required to consider the JCA report and document how they did it in the appraisal process. This study highlights the disparity between the current availability of SAT-supported products and the potential outcomes of JCA. The implications of that disparity are discussed later in this section.
SATs remain important tools for drug development. However, a reflection paper of the EMA outlines several trial aspects which should be taken into account when assessing the efficacy of medicines based on SATs. These include selection of outcomes that cannot occur without the treatment and can be objectively measured, e.g., specific biological measures, cure or survival beyond time, which would be expected based on the natural course of the disease. In the case of continuous endpoints, a cut-off value should be predefined, which cannot be achieved without treatment. The trial population should be well-defined, and its characteristics should reflect the assumptions on the natural course of the disease. If there is knowledge about prognostic or predictive biomarkers, they should also be reflected in the SAT sample [10].
4.1. SAT-Supported Products Enjoy a Fair Recognition
Several MS HTA frameworks require direct comparative evidence and do have a low appetite for indirect comparative evidence (France and Germany), therefore, it is notable to observe a high rate of product acceptability [22]. The rates are 85% for France, 76% for Spain, 90% for Poland, and 94% for Germany.
France has strict comparative evidence requirements for reimbursement. Despite this, many drugs receive favourable recommendations, even though parliament mandates direct comparative evidence as well as HAS doctrine [23]. Notably, some medicines achieved ASMR II and III classifications with just single-arm trials. In France, ITCs are considered supportive [24].
As per AMNOG regulations, the actual patient-relevant benefit of a new drug is required to be demonstrated through a comparison with an established drug or treatment strategy. In the absence of direct comparisons, indirect comparative data may be used, however, non-adjusted indirect comparisons are considered unacceptable [25].
In Germany, all orphan-designated medicinal products are legally entitled to receive an additional benefit [26]. For orphan-designated medicinal products supported by SAT, the GBA is required by law to grant an additional benefit, often it is unquantifiable, even in the absence of comparative evidence [27]. This may increase the number of SAT-supported medicinal products reported as having a positive additional benefit. However, G-BA assessments indicate that SATs with a non-quantifiable additional benefit represent 30% in our sample. Without this regulation, they would not qualify for additional benefit. Despite the stringent requirement for relative effectiveness evidence, seven SAT-based opinions were granted a quantifiable additional benefit, with one receiving a major additional benefit.
In Poland, while many medicinal products are reimbursed with an SAT, only 40 out of 96 have been assessed. Even if non-assessed products are considered to have negative opinions, the reimbursement rate would remain high, especially given Poland’s lower GDP per inhabitant in the EU and the usual high price of such products.
In Spain, similarly to Poland, only part of the products assessed based on SAT (46 out of 96) underwent evaluation by the HTA agency. However, the rate of positive options is even higher than in Poland, indicating the significant acceptability of SAT-based products despite the associated uncertainties.
Our results regarding reimbursement and availability align with several published studies using various methodologies and scopes. This trend extends beyond France. Analyses of HTA recommendations in multiple countries (including Germany, the United Kingdom, Sweden, the Netherlands, Canada, and Australia) have demonstrated that SAT-based evidence for medicinal products does not necessarily result in negative outcomes. In those studies, many products supported by SATs received positive HTA recommendations at a rate comparable to those based on randomized data [28].
Recent research on HTA opinions in France and Germany for products with SATs between January 2020 and May 2022 confirms high success rates. In France, 55% of reports (11 of 20) had positive outcomes, while in Germany, 85% (23 of 27) were considered positive [29].
In Portugal, 8 out of 9 HTA processes for products with SAT from January 2017 to April 2022 received positive reimbursement decisions with non-quantifiable additional benefits [30].
4.2. The Low Value of JCA for SAT-Supported Products Justifies Their Exemption from JCA
The guidance document on the validity of clinical studies stakes a definitive position regarding SAT. SATs are not suitable for assessing relative effectiveness and, without an indirect comparison, will be classified as not assessable and not assessed [8]. This classification applies to the majority of products, 90 out of 96 in our sample.
In ITC, methodologies are inherently unanchored for SAT, resulting in the lowest degree of certainty of relative effectiveness [22]. Moreover, as indicated in the JCA guidelines on quantitative evidence synthesis, unanchored indirect comparisons break randomisation and require the assumption of "conditional constancy of absolute effects" [7]. This assumption means that the absolute outcome in treatment arms is constant at any given level of prognostic variables and effect modifiers. This assumption is usually unjustifiable in practice, making the ITC without a common comparator highly unreliable [7,31]. Based on that, it is highly probable that even if an ITC is available for some products, such evidence would be classified as highly confounded. This would only lead to a conclusion of the lowest degree of certainty of the relative effectiveness, severely impacting their assessability by the MS.
This raises several questions:
While most medicinal products supported by SAT get reimbursed, what impact will a “negative” JCA assessment have? As MS HTA bodies must document the due consideration of JCA reports, this could complicate reimbursement and additional benefit assessments, including major benefits or ASMR II or III.
Given that JCAs for SAT-supported products are inconclusive with known outcomes before filing, their utility is limited.
The JCA is a long-term process lasting more than a year and is very resource-intensive. Running such a process while the outcome is known beforehand may be considered questionable. The JCA is decontextualized, whereas MS HTA bodies’ assessment is contextualized, integrating various constraints and a face-value benefit appreciation that can influence the appraisal. For instance, the high level of unmet needs and the burden of these conditions is part of the assessment in France, Spain, and Poland. Given this context, the added value of JCA is debatable.
Exempting such medicinal products from JCA might be beneficial and would:
- Prevent potential restrictions on access to important interventions;
- Align with current HTA practices that often favour SAT-supported products;
- Reduce workload for already stretched Member State Coordination Group on Health Technology Assessment (HTACG) resources.
Medicinal products supported by JCA and eligible for JCA between 2025 and 2028 are already developed or in late clinical stages. Thus, JCA guidelines (available since 2024) have come too late for consideration in their development. Exempting these products from JCA and reconsidering them in 2028 seems reasonable.
Concerns that HTD may avoid JCA by engaging more in SAT are mitigated by the fact that 25% or more of such products do not get reimbursement, and the rate will inevitably increase. HTA and payers will penalize inappropriate decisions to engage deliberately and inappropriately in SAT if they consider the only rationale for engaging in a SAT development was to avoid JCA. No HTD will take the risk to engage in a SAT development just to avoid the JCA process given the expected impact of the inappropriate use of SAT. Additionally, this decision should be endorsed by regulators. Though they may be perceived as less strict than HTA on this matter, they are careful in approving SAT. Up to 90% of SAT-supported medicinal products receive positive reimbursement recommendations from HTA, indicating a fair alignment between HTAs and regulators. Exempting SAT from JCA is unlikely to encourage more SAT adoption for development. The EU-HTA regulation’s likely modest impact does not warrant risking the development strategy by avoiding direct comparative evidence development to the benefit of SAT.
One may consider that SAT-supported medicinal products should undergo JCA, and the potential negative impact of the JCA report on market access may prompt HTD to evaluate carefully whether to proceed with an SAT development program as a last resort. This obligation to undergo JCA with a likely negative outcome may reduce the number of SAT-supported products. However, it is unlikely for several reasons. The decision to engage in SAT is primarily made at regulatory bodies’ level, such as the FDA and EMA. Once the decision is made, experience shows that HTA carries little weight in this decision, especially since it is predominantly an EU process and all cost-effectiveness analysis driven HTA bodies accept unanchored ITC. In the United States, the largest pharmaceutical market, HTA has minimal impact. Furthermore, HTA bodies, especially ICER in the US, accept unanchored indirect evidence.
HTD may contend that it is impossible to develop evidence at the expected level of the JCA subgroup and may submit a dossier that is classified as not assessable. This approach could mitigate the potential negative impact of the JCA report.
If the JCA targets SAT and contributes to restriction of access to SAT-supported products, it would counteract its primary strategic objective: expanding access to innovative medicinal products in the EU. This action will be monitored by the European Parliament and deemed unacceptable.
Furthermore, the actual influence of JCA on MS HTA opinions remains unproven. Mandating all SAT products to undergo JCA and subsequently receive poor assessments conclusion is unlikely to gain support from EU citizens or the European Parliament.
The argument that increasing JCA for SAT will encourage HTD to reduce the number of SAT-developed medicinal products is unlikely to effectively decrease SAT-supported products.
4.3. Study Limitations
Choosing France as the reference country may introduce some limitations to this study. However, since HAS reviews all products that have been granted marketing authorisation and for which a submission occurs [24], a set of products identified as having SAT as the key evidence is likely one of the broadest obtainable through the HTA database analysis. It makes France a reasonable reference for a comprehensive review of SAT-driven submissions in Europe.
In Germany, all medicinal products receive reimbursement upon marketing authorization, so HTA outcomes do not affect reimbursement. After assessing the added benefit, pharmaceutical companies must negotiate prices with GKV, which depends on the GBA’s assessment [32,33]. An unfavourable assessment could result in an unviable price and prevent the product’s launch in Germany or withdrawal after HTA or after pricing negotiation. Therefore, availability can be considered a proxy for the HTA reimbursement decision.
Using the JCA degree of certainty as a proxy for acceptability may be considered as excessive. However, because MS HTA bodies have to provide due consideration to the JCA report, it may, in these specific cases, be considered as a potential influencer of the HTA opinion.
JCA may stimulate performing indirect evidence generation. However, such evidence will always be unanchored. Therefore, according to JCA guidance documents, it will systematically lead to the lowest level of certainty of relative effectiveness. This will rather be a disincentive to submit such evidence.
It remains to be seen if JCA will enhance the number of direct comparative evidence submissions and reduce the number of SAT-supported products. It is very unlikely as so far regulatory agencies continue to accept SAT and obviously, the reimbursement rate and availability on the market are high for such products.
5. Conclusions
The proportion of SAT-supported medicinal products enjoys a very high availability, up to 90% in our study countries’ scope. This happens despite a strong requirement for direct comparative evidence. Most products developed with SAT will not be eligible for JCA review, assuming they are filed with current evidence. Even if more will be reviewed by the JCA subgroup, for a limited number of PICOs, because of HTD performing more ITC, they receive the lowest degree certainty ratings. This study and the discussing points bring some useful learning points:
- Contextualisation and deliberative processes are critical for SAT and, by essence, overlooked in JCA.
- If JCA express a negative opinion for SAT-supported products and this opinion impacts negatively availability at MS level, it will contradict the primary strategic objective of EU-HTA regulation.
- If JCA express a negative opinion for SAT-supported products and this opinion does not affect the decision of MS to grant a high rate of availability, this would evidence low impact of JCA.
- The JCA process is unlikely to impact the decision of HTD to engage in SAT development.
- Exempting SAT from JCA is unlikely to increase the number of SAT-supported medicinal products.
Therefore, it is questionable whether SAT-based products should be considered for JCA, as they may not effectively inform MS HTA assessments.
Author Contributions
Conceptualization, M.T. and K.K.; methodology, M.T. and K.K.; formal analysis, all authors; investigation, K.K., E.Ł., M.K. and I.T.-C.; resources, K.K.; data curation, K.K., M.K, I.T.-C.; writing—original draft preparation, all authors; writing—review and editing, all authors; visualization, K.K., E.Ł., M.K. and I.T.-C.; supervision, M.T. and K.K.; project administration, K.K. and E.Ł. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were generated during the study.
Acknowledgments
During the preparation of this manuscript, the authors used the NaviHTA database (https://www.inovintell.com/) for the purposes of identification of HTA opinions in France. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ASMR | Improvement in the actual benefit |
| ATMP | Advanced therapy medicinal products |
| EMA | European Medicine Agency |
| EU | European Union |
| HTA | Health Technology Assessment |
| HTD | Health Technology Developers |
| ITC | Indirect treatment comparison |
| JCA | Joint Clinical Assessment |
| MAIC | Matching-adjusted indirect comparison |
| MS | Member States |
| PICO | Population, Intervention, Comparator, Outcomes |
| RCT | Randomized control trials |
| RE | Relative effectiveness |
| SATs | Single-arm trials |
| SMR | Rating of actual benefit |
References
- European Commission. Commission Implementing Regulation (EU) 2024/1381 of 23 May 2024 laying down, pursuant to Regulation (EU) 2021/2282 on health technology assessment, procedural rules for the interaction during, exchange of information on, and participation in, the preparation and update of joint clinical assessments of medicinal products for human use at Union level, as well as templates for those joint clinical assessments. 23 May 2024. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ:L_202401381 (accessed on 21 January 2025).
- European Parliament and Council of the EU. Regulation (EU) 2021/2282 of the European Parliament and of the Council of 15 December 2021 on health technology assessment and amending Directive 2011/24/EU (Text with EEA relevance). 15 December 2021. Available online: https://eur-lex.europa.eu/eli/reg/2021/2282 (accessed on 21 January 2025).
- European Commission. Joint Clinical Assessments. 2025. Available online: https://health.ec.europa.eu/health-technology-assessment/implementation-regulation-health-technology-assessment/joint-clinical-assessments_en (accessed on 21 January 2025).
- Gentilini, A.; Parvanova, I. Managing experts’ conflicts of interest in the EU Joint Clinical Assessment. BMJ Open 2024, 14(11), e091777. [Google Scholar] [CrossRef] [PubMed]
- HTA Coordination Group. Guidance on outcomes for joint clinical assessments. 10 June 2024. Available online: https://health.ec.europa.eu/document/download/a70a62c7-325c-401e-ba42-66174b656ab8_en?filename=hta_outcomes_jca_guidance_en.pdf (accessed on 21 January 2025).
- European Commission. Implementation Rolling Plan. 10 January 2025. Available online: https://health.ec.europa.eu/document/download/397b2a2e-1793-48fd-b9f5-7b8f0b05c7dd_en?filename=hta_htar_rolling-plan_en.pdf.
- HTA Coordination Group. Methodological Guideline for Quantitative Evidence Synthesis: Direct and Indirect Comparisons. 8 March 2024. Available online: https://health.ec.europa.eu/document/download/4ec8288e-6d15-49c5-a490-d8ad7748578f_en?filename=hta_methodological-guideline_direct-indirect-comparisons_en.pdf&prefLang=el#:~:text=The%20objective%20of%20this%20document%20is%20to%20describe,comparisons%2C%2 (accessed on 21 January 2025).
- HTA Coordination Group. Guidance on Validity of Clinical Studies. 04 July 2024. Available online: https://health.ec.europa.eu/document/download/9f9dbfe4-078b-4959-9a07-df9167258772_en?filename=hta_clinical-studies-validity_guidance_en.pdf (accessed on 21 January 2025).
- Wang, M.; et al. Single-arm clinical trials: design, ethics, principles. BMJ Support Palliat Care 2024, 15(1), 46–54. [Google Scholar] [CrossRef] [PubMed]
- EMA. Single-arm trials as pivotal evidence for the authorisation of medicines in the EU. 21 April 2023. Available online: https://www.ema.europa.eu/en/news/single-arm-trials-pivotal-evidence-authorisation-medicines-eu (accessed on 21 January 2025).
- GlobalData. Pharmaceutical Prices (POLI) Database . Available online: https://www.globaldata.com/marketplace/pharmaceuticals/pharmaceutical-prices-poli-database/ (accessed on 21 January 2025).
- EMA. Download medicine data. Orphan designations . 2025. Available online: https://www.ema.europa.eu/en/medicines/download-medicine-data#orphan-designations-69050 (accessed on 21 January 2025).
- EMA. Download medicine data . Available online: https://www.ema.europa.eu/en/medicines/download-medicine-data (accessed on 7 February 2025).
- G-BA. Benefit Assessment of Medicinal Products with New Active Ingredients according to Section 35a SGB V Cer-liponase Alfa (reassessment after the deadline (type 2 neuronal ceroid lipofuscinosis)) . 2022. Available online: https://www.g-ba.de/downloads/40-1465-9111/2022-12-15_AM-RL-XII_Cerliponase-Alfa_D-849_TrG_EN.pdf (accessed on 21 January 2025).
- G-BA. Benefit Assessment of Medicinal Products with New Active Ingredients according to Section 35a SGB V Cemiplimab (new therapeutic indication: basal cell carcinoma, locally advanced or metastatic) . 2022. Available online: https://www.g-ba.de/downloads/40-1465-8181/2022-01-20_AM-RL-XII_Cemiplimab_D-706_TrG_EN.pdf (accessed on 23 January 2025).
- G-BA. Beschlüsse über die Nutzenbewertung von Arzneimitteln mit neuen Wirkstoffen nach § 35a SGB V - Sofosbuvir . 2014. Available online: https://www.g-ba.de/downloads/40-268-2899/2014-07-17_AM-RL-XII_Sofosbuvir_2014-02-01-D-091_TrG.pdf (accessed on 21 January 2025).
- Navlin. Novartis Withdraws Tabrecta in Germany . 2023. Available online: https://www.navlindaily.com/article/18714/novartis-withdraws-tabrecta-in-germany (accessed on 21 January 2025).
- Ned, P. Bluebird to withdraw gene therapy from Germany after dispute over price. 20 April 2021. Available online: https://www.biopharmadive.com/news/bluebird-withdraw-zynteglo-germany-price/598689/ (accessed on 21 January 2025).
- EMA. Gavreto (pralsetinib) - Withdrawal of the marketing authorisation in the European Union. 17 January 2025. Available online: https://www.ema.europa.eu/en/documents/public-statement/public-statement-gavreto-withdrawal-marketing-authorisation-european-union_en.pdf (accessed on 23 January 2025).
- AOTMiT. Assessment of reimbursement applications. June 2024. Available online: https://www.aotm.gov.pl/en/medicines/assessment-of-reimbursement-applications/ (accessed on 23 January 2025).
- Ministry of Health. Fundusz Medyczny. D Subfundusz Terapeutyczno_Innowacyjny (STI) . 2025. Available online: https://www.gov.pl/web/zdrowie/d-subfundusz-terapeutyczno-innowacyjny-sti (accessed on 23 January 2025).
- Macabeo, B.; et al. The Acceptance of Indirect Treatment Comparison Methods in Oncology by Health Technology Assessment Agencies in England, France, Germany, Italy, and Spain. Pharmacoecon Open 2024, 8(1), 5–18. [Google Scholar] [CrossRef] [PubMed]
- Remuzat, C.; Toumi, M.; Falissard, B. New drug regulations in France: what are the impacts on market access? Part 1 - Overview of new drug regulations in France. J Mark Access Health Policy 2013, 1. [Google Scholar] [CrossRef] [PubMed]
- HAS. Transparency Committee doctrine. 02 December 2020. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2019-07/doctrine_de_la_commission_de_la_transparence_-_version_anglaise.pdf (accessed on 21 January 2025).
- Ivandic, V. Requirements for benefit assessment in Germany and England - overview and comparison. Health Econ Rev 2014, 4(1), 12. [Google Scholar] [CrossRef] [PubMed]
- Kranz, P.; et al. Results of health technology assessments of orphan drugs in Germany-lack of added benefit, evidence gaps, and persisting unmet medical needs. Int J Technol Assess Health Care 2024, 40(1), e68. [Google Scholar] [CrossRef] [PubMed]
- Schulz, S.; et al. The Evaluation of Orphan Drugs by the German Joint Federal Committee-An Eight-Year Review. Dtsch Arztebl Int 2020, 117(50), 868–869. [Google Scholar] [CrossRef] [PubMed]
- IQVIA. HTA Uncovered. July 2016. Available online: https://www.iqvia.com/-/media/library/white-papers/hta-uncovered-july-2016.pdf (accessed on 23 January 2025).
- Heidbrede, T.; et al. Health technology assessments of single-arm clinical trials in Germany and France; ISPOR Poster 121937, 2022. [Google Scholar]
- Cardoso, A.; Santos, S. Use of single arms studies for Health Technology Assessment in Portugal; ISPOR Poster, 2022. [Google Scholar]
- HTA Coordination Group. Practical Guideline for Quantitative Evidence Synthesis: Direct and Indirect Comparisons . 2024. Available online: https://health.ec.europa.eu/document/download/1f6b8a70-5ce0-404e-9066-120dc9a8df75_en?filename=hta_practical-guideline_direct-and-indirect-comparisons_en.pdf (accessed on 21 January 2025).
- G-BA. Benefit Assessment of Medicinal Products . 2025. Available online: https://www.g-ba.de/english/benefitassessment/ (accessed on 21 January 2025).
- Blümel, M.; et al. Germany. Health System Review. Health Systems in Transition 2020, 22(6), i-273. [Google Scholar]
Figure 1.
Actual benefit (SMR) ratings in the HTA opinions based on SAT in France.
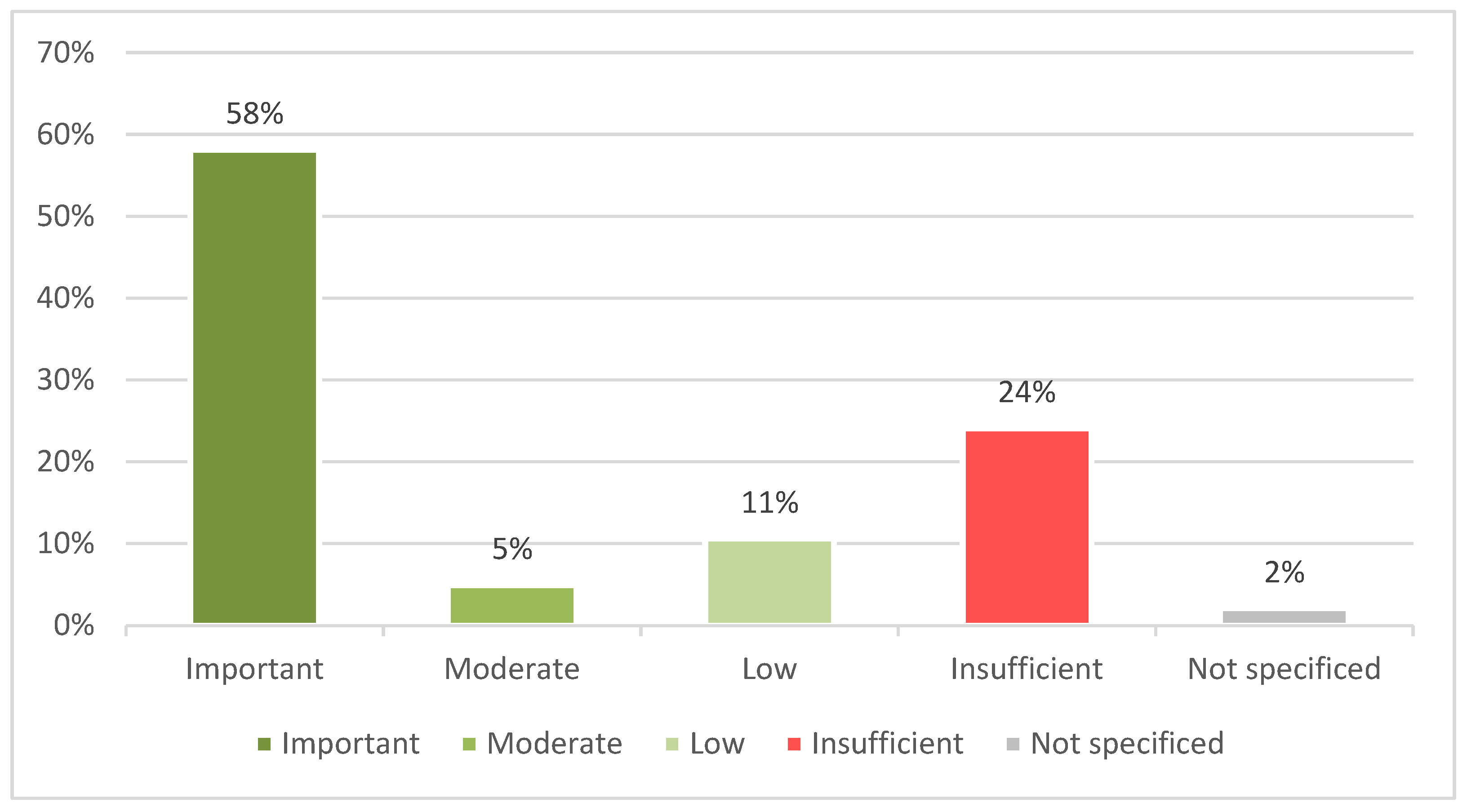
Figure 2.
Improvement in actual benefit (ASMR) ratings in the HTA opinions based on SAT in France. *ASMR was not assessed due to insufficient SMR or not specified.
Figure 2.
Improvement in actual benefit (ASMR) ratings in the HTA opinions based on SAT in France. *ASMR was not assessed due to insufficient SMR or not specified.
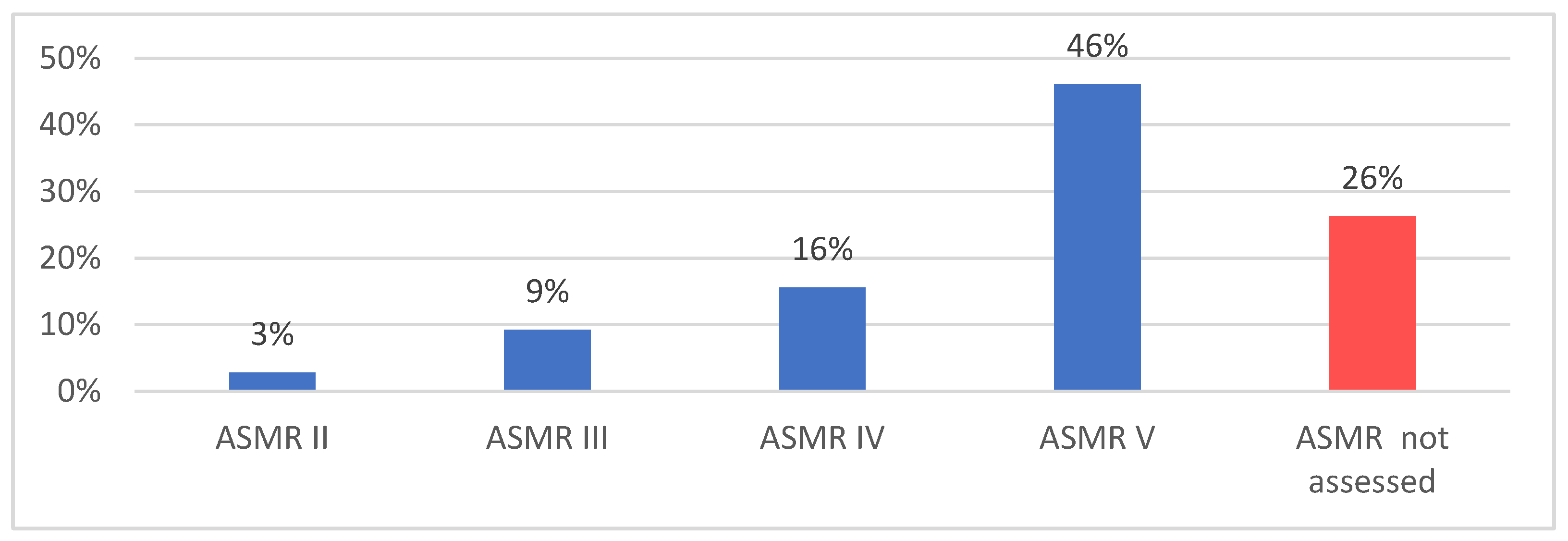
Figure 3.
Improvement in actual benefit (ASMR) ratings in the HTA opinions depending on the use of an ITC.
Figure 3.
Improvement in actual benefit (ASMR) ratings in the HTA opinions depending on the use of an ITC.
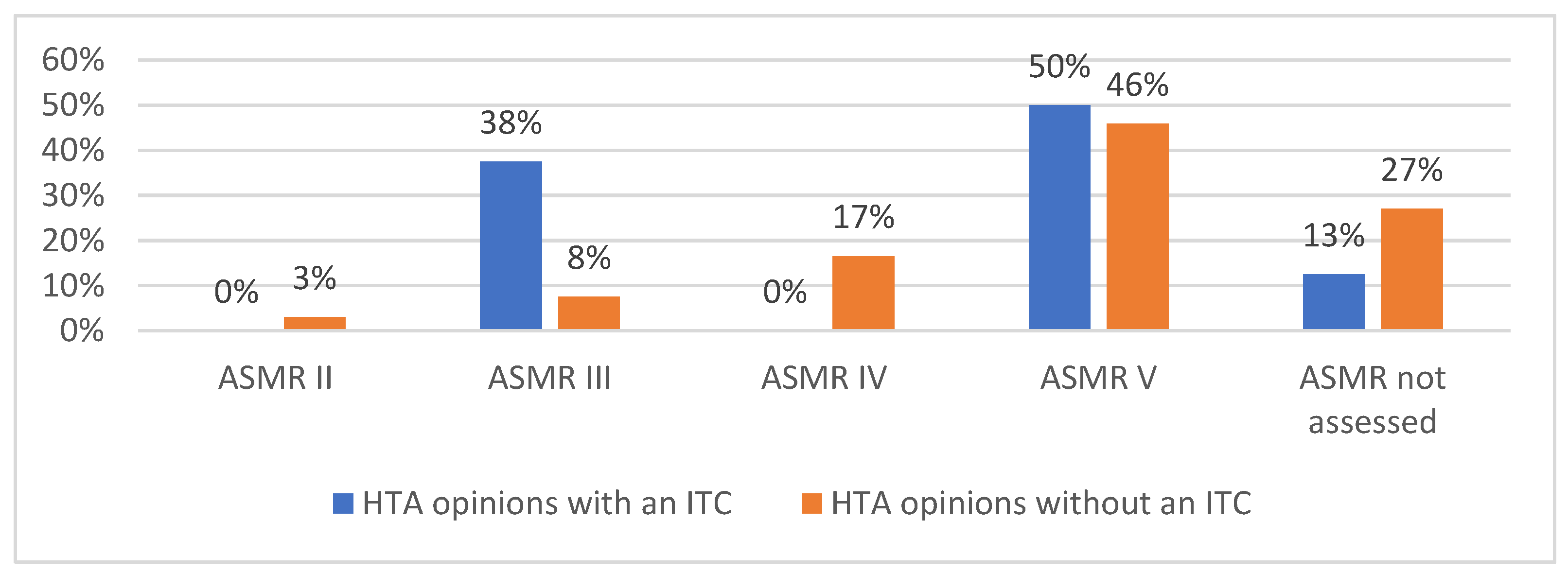
Figure 4.
Added benefit ratings in the HTA opinions in Germany.
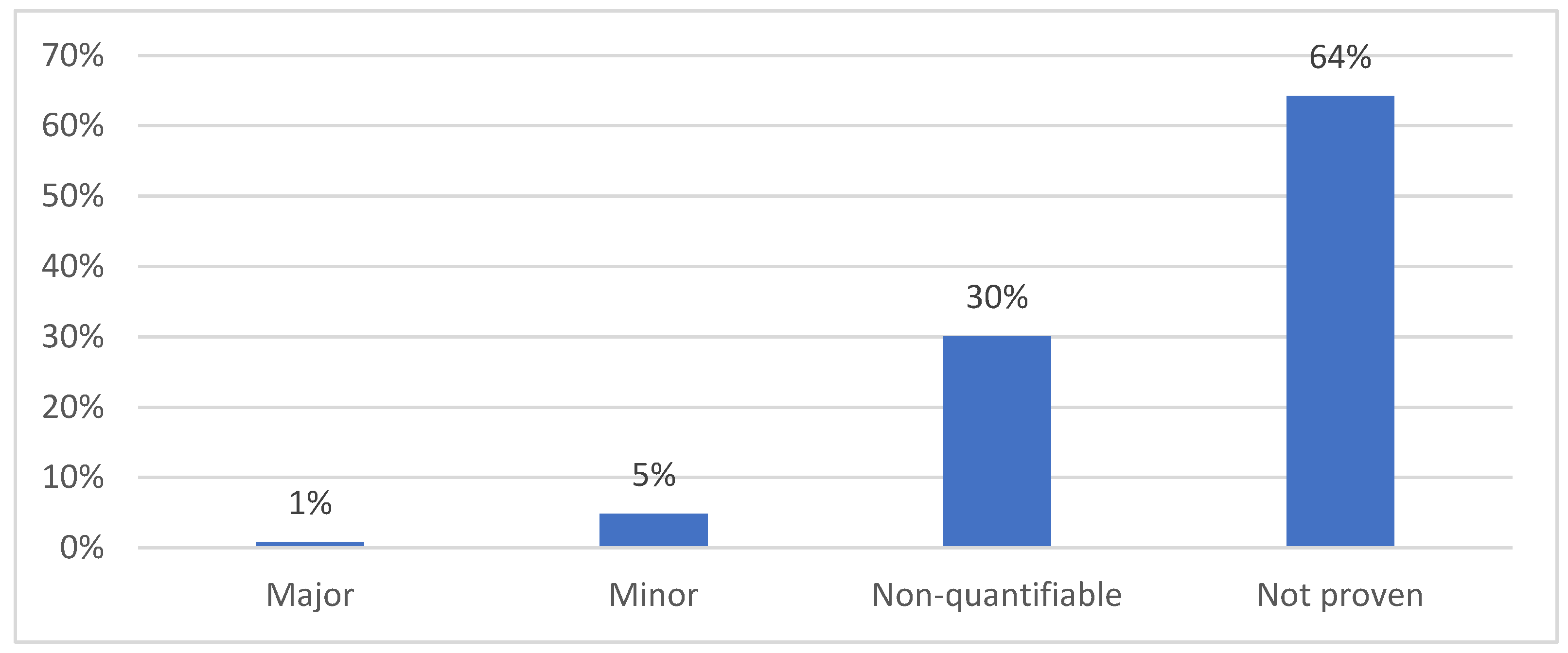
Figure 5.
Reimbursement recommendations in the HTA opinions in Poland.
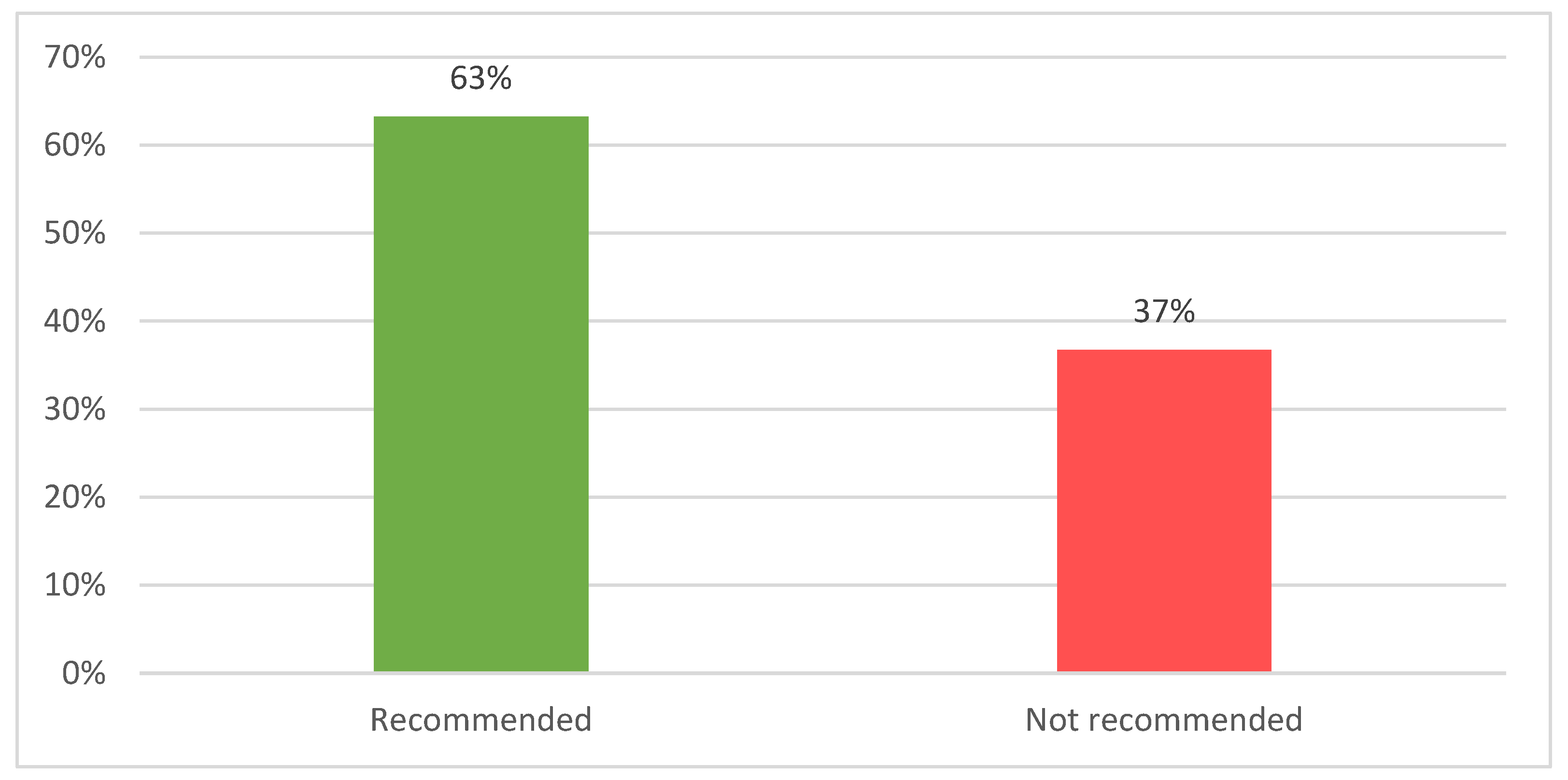
Figure 6.
Reimbursement recommendations in the HTA opinions in Poland depending on the market access pathway.
Figure 6.
Reimbursement recommendations in the HTA opinions in Poland depending on the market access pathway.
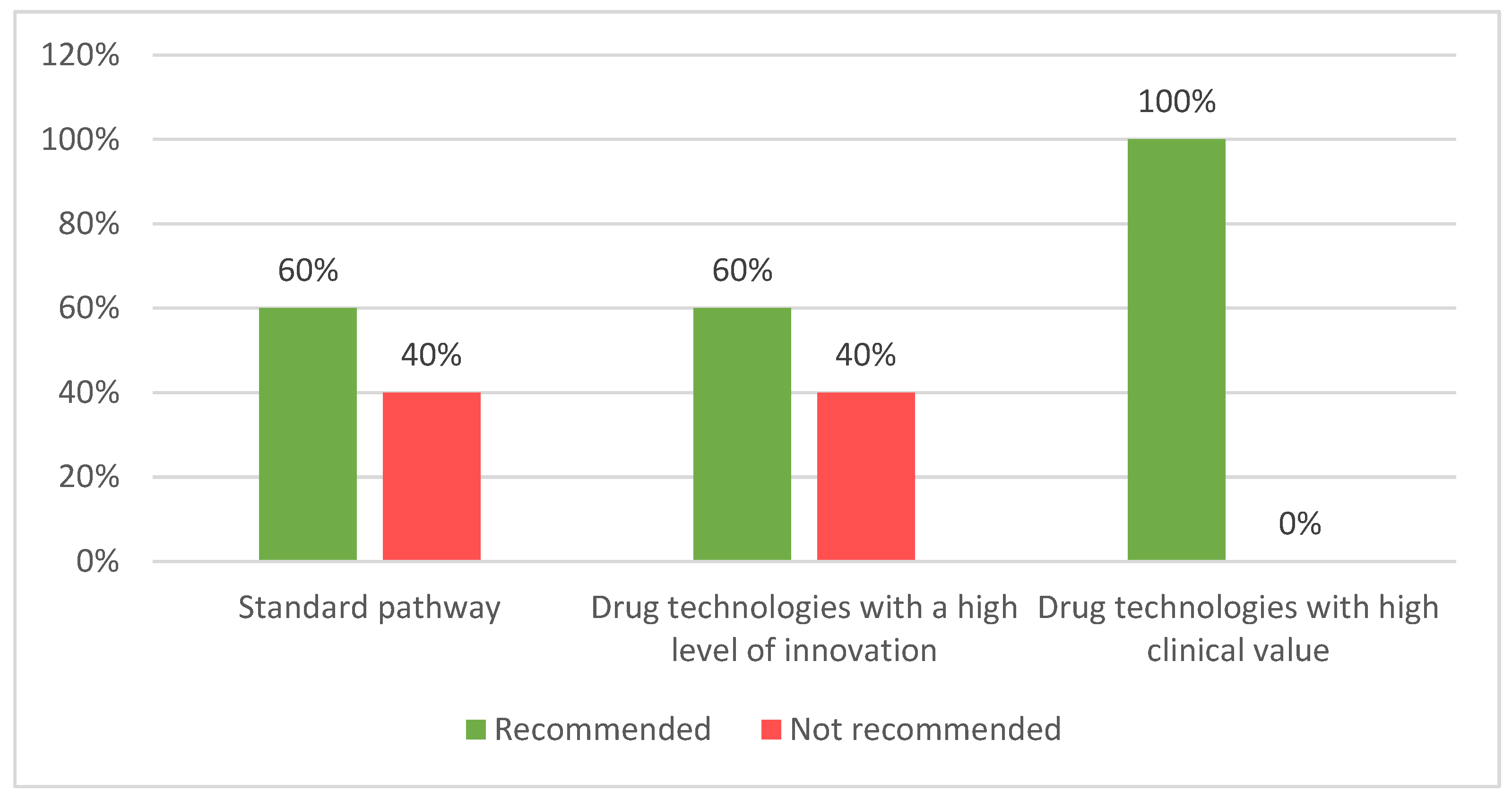
Figure 7.
HTA opinions in Spain.
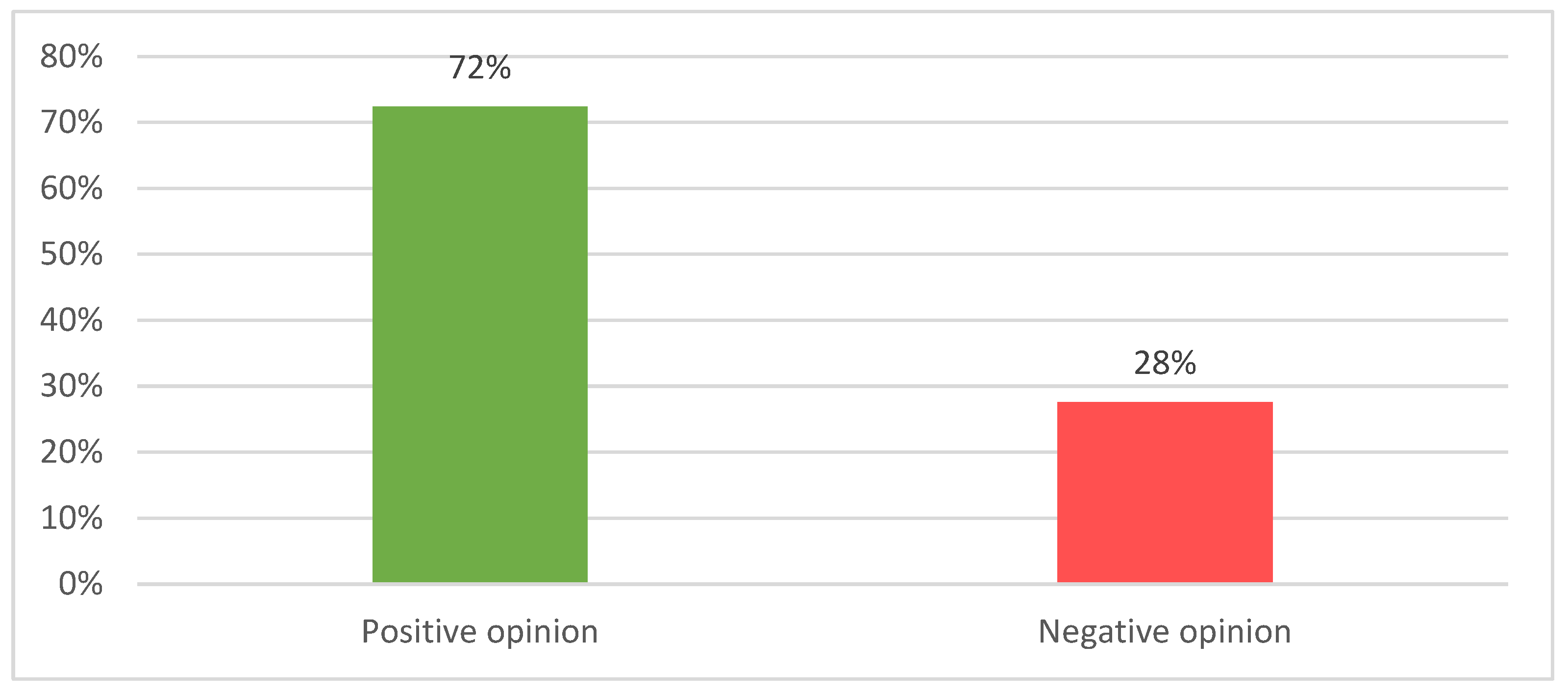

Table 1.
Assessment of the assessability and acceptability of products with SAT under different HTA frameworks.
Table 1.
Assessment of the assessability and acceptability of products with SAT under different HTA frameworks.
| HTA framework | Number of products with SAT | Number of products assessed | Number of products accepted 1 | Acceptability rate |
|---|---|---|---|---|
| France | 96 | 96 | 82 | 85% |
| Germany | 65 | 61 | 94% | |
| Poland | 40 | 36 | 90% | |
| Spain | 46 | 35 | 76% | |
| JCA | 6 2 | 0 3 | 0% |
1 Products accepted for reimbursement based on SAT at the HTA stage at least in one subgroup of patients (except in Germany, where all products are accepted by default; unaccepted are products withdrawn from the market due to HTA-driven pricing not acceptable for the company). 2 Anticipated number of assessable products with the availability of data for MAIC or non-adjusted ITC against external control, based on the information included in the French HTA opinions. 3 Anticipated number of acceptable products based on the degree of certainty of the relative effectiveness assessment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



