
Submitted:
25 April 2025
Posted:
28 April 2025
You are already at the latest version
Abstract
Background: Vasculonecrotic reactions in leprosy are often present in the context of a type 2 leprosy reaction. Differentiation between necrotizing ery-thema nodosum leprosum (nENL) and Lucio's phenomenon (LP) can be dif-ficult, and cases of overlapping reactions have been reported. Mycobacterum lepromatosis, a relatively new species causing leprosy, has been sporadically reported to cause LP. Type 1 leprosy reaction occurs more commonly in HIV-coinfected individuals, and only sporadic cases of LP and ENL have been reported in the context of unmasked or paradoxical immune reconstitu-tion inflammatory syndrome (IRIS). Methods: We present a case of a vascu-lonecrotic reaction in an antiretroviral-naive leprosy/HIV-coinfected indi-vidual caused by M. lepromatosis. Results: The patient had a 2-month course of papules and nodules that evolved into painful necrotic ulcers accompanied by systemic symptoms. The lesions were consistent with nENL; however, the histopathological findings were more consistent with LP. The patient rapidly progressed to sepsis and died. Conclusions: Vasculonecrotic reactions are considered a life-threatening medical emergency, and sepsis is a common complication. To our knowledge, this is the first reported case of a leprous vasculonecrotic reaction in an HIV-infected individual not associated with IRIS caused by M. lepromatosis. Leprosy vasculonecrotic reactions may not be easily recognized in HIV-infected individuals, particularly those with severe immunosuppression, where opportunistic infections, especially fungal infec-tions, malignant syphilis, and other mycobacteriosis, may present similar findings. Delayed diagnosis can lead to severe complications and risk of death.
Keywords:
Vasculonecrotic reaction
; Leprosy
; HIV infection
; Mycobacterium lepromatosis
; necrotizing erythema nodosum leprosum
; Lucio's phenomenon
; Leprosy reactions
1. Introduction
Leprosy is a chronic granulomatous infection caused by Mycobacterium leprae or Mycobacterium lepromatosis. Both species are closely related with 13% genetic difference in nucleotide sequence [1] and have a common ancestor with a divergence of 13.9 million years ago [2].
Leprosy reactions (LR) are immunological episodes that can occur before, during or after leprosy treatment and these can be stimulated by M. leprae antigens such as phenolic-glycolipid-I (PGL-I) or by co-infections [3].
Leprosy reactions are classified as type 1 leprosy reaction (T1R), a cell-mediated reversal reaction characterized by the development of new lesions, exacerbation of those already present, thickening and tenderness of peripheral nerves occurring in people with tuberculoid leprosy (TL), borderline tuberculoid (BT), borderline (BB). In the other hand, type 2 leprosy reaction (T2R) or erythema nodosum leprosum (ENL) is associated with the formation of immune complexes in the blood that are deposited inside tissues, especially skin, kidneys and joints [3]. T2R occurs usually as an immunological complication of the clinical forms of borderline lepromatous (BL) and lepromatous leprosy (LL) [3]. Borderline forms are immunologically unstable and more predisposed to developing LR [4].
Vasculonecrotic reactions in leprosy occur as part of a type 2 leprosy reaction (T2R) including a severe form of necrotizing erythema nodosum leprosum (nENL) that occurs in BL or LL cases [5,6] and Lucio's phenomenon (LP) a leprosy reaction which occurs in an untreated anergic form of the disease, named diffuse lepromatous leprosy (DLL), although it can also be presented in LL and BL forms[5]. These two reactions can be difficult to differentiate [7,8].
We present a case of a fatal vasculonecrotic reaction in a HIV/leprosy coinfected patient caused by M. lepromatosis Infection.
2. Case Presentation
A 33-year-old male with a recent diagnosis of HIV infection, originally from Jalisco and resident from Aguascalientes, Mexico. He started 2 months before his hospital admission with violaceous papules and nodules that evolved into painful necrotic ulcers, which began on the trunk and later appeared on the limbs and face, associated with malaise, weight loss, fever and nocturnal diaphoresis. Fifteen days prior to his hospitalization, he had loss of vision in his right eye. The physical examination revealed deep, punched-out ulcers of variable size, ranging from 5 to 20 mm, round and ovoid in shape with regular edges (Figure 1). The ophthalmological evaluation showed blindness in the right eye, retinal detachment with hemorrhagic and fibrotic lesions compatible with cytomegalovirus chorioretinitis, accordingly ganciclovir was started. The HIV-1 RNA was 301,000 copies/µL and CD4+ T cells count 4 cells/mm3. Significant laboratory findings included Hb 9.4g/dL, leukocytes 3.76 103/µL, GGT 176 IU/L, albumin 2.4g/dL, ALT 199 U/L, AST 331 IU/L, alkaline phosphatase 215 IU/L, lactate dehydrogenase 486 U/L, VDRL positive, title 1:1. Abdominal US showed hepatomegaly with steatosis.
A skin biopsy of a lesion revealed ulceration and necrosis of the epidermis with acute inflammatory infiltrate at the expense of polymorphonuclear cells, the dermis exhibited extensive chronic histiocytic inflammatory infiltrate of neurotropic behavior, besides, a panniculitis pattern of inflammation of the subcutaneous cellular tissue, leukocytoclastic vasculitis and thrombosis was observed. A CD68 immunohistochemistry revealed macrophages located perineurally. A Fite-Faraco stain resulted positive to abundant acid-fast bacillus (AFB) Based on the histopathological findings a lepromatous leprosy with Lucio's phenomenon was diagnosed (Figure 2).
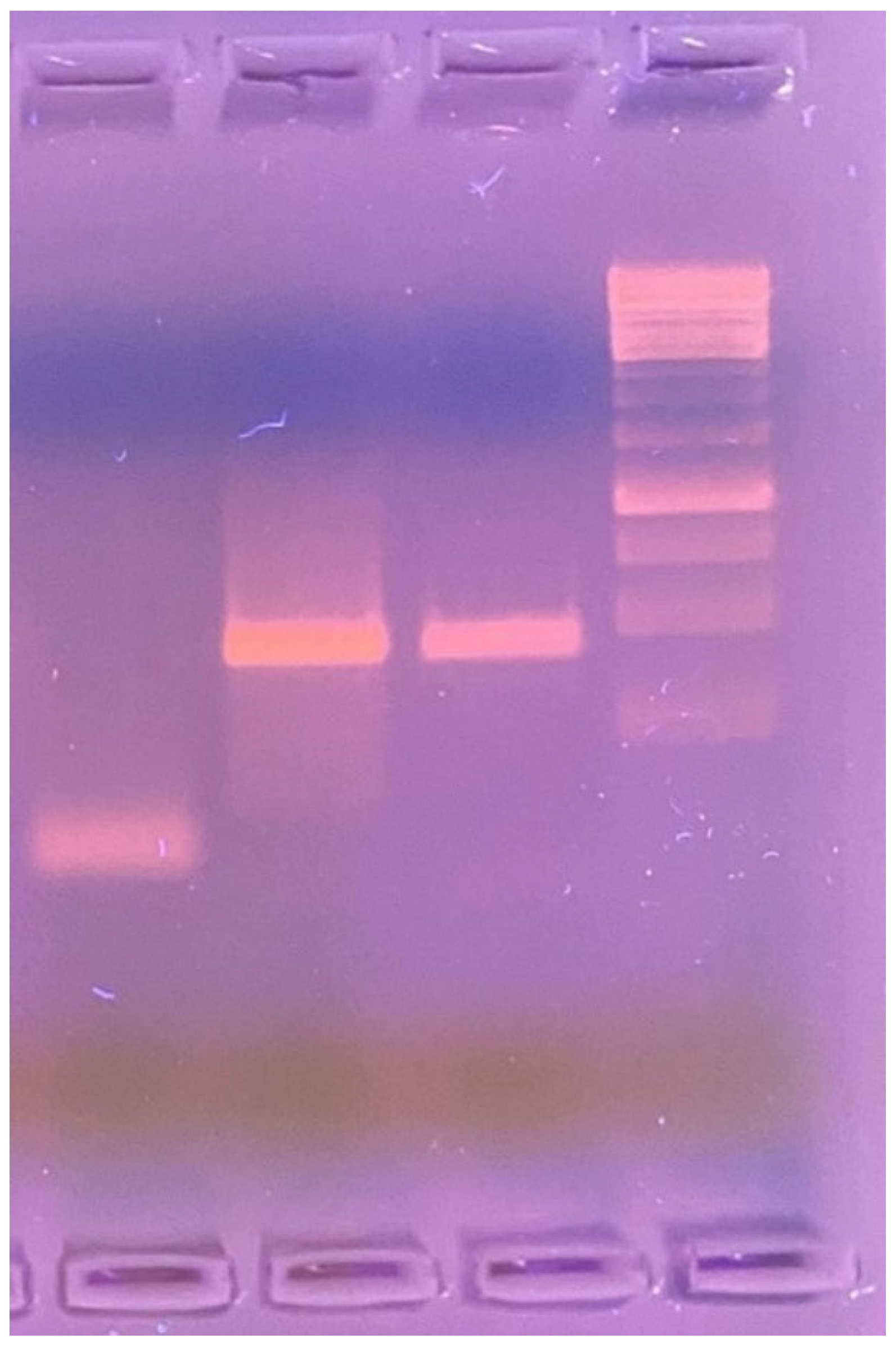
A PCR from the skin tissue was obtained to identify the microorganism. Using a 1% agarose gel, we carry out a PCR with the LPMF-244 Primers, a hemN gene region specific to Mycobacterium lepromatosis (absent in other known mycobacteria) (Figure 3)
During hospitalization, the patient developed septic shock treated with antibiotics (vancomycin and meropenem) and vasopressors, but he did not respond to the treatment and finally died from septic shock.
3. Discussion
In this report, we describe the case of a vasculonecrotic reaction with systemic symptoms caused by M. lepromatosis in a HIV-infected subject who was unaware of having leprosy, with severe immunosuppression, naive to antiretroviral treatment, who rapidly progressed to sepsis with fatal outcome.
Vasculonecrotic lesions in leprosy occur on T2R and most frequently are presented as a complication of the anergic form of diffuse lepromatous leprosy[8,9]. Differentiation between nENL and LP can sometimes be difficult and there are reported cases of overlapping of both reactions [5,7,8,10]. Clinical and histopathological findings are essential for diagnosis [11].
Clinically, nENL is characterized by nodular lesions that develop necrosis and painful ulcers, it is accompanied by systemic symptoms including fever, myalgia, arthralgia, malaise, lymphadenopathy, iritis, episcleritis, hepatitis, neuritis, and orchitis, which usually appears after treatment has started [7]. In contrast, LP presents multiple and extensive purpuric areas with net-like pattern and superficial ulceration over areas of infiltrated skin[5]; polygonal with angled margins and jagged-edges ulcers eventually evolve to necrosis, which commonly affect extremities, it is accompanied by a burning sensation, leaving stellar atrophic scars; systemic symptoms and visceral involvement are usually absent; the lesions appear in untreated or inadequately treated non-nodular lepromatous leprosy and other forms of LL [7] and frequently presents as the debut of the disease without a previous leprosy diagnosis [11]. Our patient did not have a previous diagnosis of leprosy. A systematic review found that 42/49 (85.7%) of patients diagnosed with LP had no prior diagnosis of leprosy [12].
Histological nENL shows histiocytes in the dermis with infiltration of neutrophils in the deeper layer of the dermis, vasculitis and panniculitis with few bacilli present [12]. On the other hand, LP is characterized by many AFB aggregates in the vascular endothelium, leukocytoclastic vasculitis, endothelial cell proliferation[8], ischemic epidermal necrosis [12], necrotizing vasculitis on superficial and medium-sized vessels [13], and presence of fibrin thrombi [7].
The pathogenesis of LP is attributed to massive bacillary invasion into the vascular endothelium that leads to narrowing and subsequent occlusion of the lumen of the small vessels that progresses to thrombosis and skin necrosis, with a further secondary inflammatory response and deposition of immune complex [10]; immunofluorescence tests in LP often exhibit immune complexes of IgM, IgG, C3, and C1q in the walls of dermal blood vessels [14]. Differential diagnosis of LP includes cryoglobulinemia, leukocytoclastic vasculitis, pyoderma gangrenosum, antiphospholipid syndrome, and disseminated intravascular coagulation [15,16]. In contrast, in ENL the triggering event is an immunological process with the deposition of immune complexes [10].
Because of the high bacillary load in LP, treatment with multidrug therapy (MDT) is a priority accompanied by steroids, antibiotic, anticoagulants, surgical debridement and skin grafting for the wounds [17,18]. In contrast, the treatment of nENL is based on steroids and thalidomide [5].
M. lepromatosis was recognized in 2008 as a new species causing a fatal DLL in 2 Mexican patients [19]. Although M. lepromatosis is endemic in Mexico, it has also been identified less frequently in other regions in the Americas and sporadic cases in Asia [20,21,22]. The clinical presentation of M. lepromatosis infection is most frequently as DLL, a form of endemic leprosy in Mexico characterized by diffuse non-nodular cutaneous infiltration[22] described by Lucio and Alvarado in 1852 [23] and later recognized by Latapí and Chevez-Zamora in 1948 [24].
Han et al. found that of 87 species-confirmed cases of leprosy in Mexico, 63.2% were caused by M. lepromatosis, 20.7% by M. leprae and both species were identified in 16.1% of cases. In the M. lepromatosis group, 34/55 (61.8%) were diagnosed with LL, and the total of 13 cases of DLL (23.6% of 55 cases) were caused by M. lepromatosis [25]. These results differ from the findings of a study, which found that of 7 specimens positive for M. lepromatosis from Brazilian patients, all presented as tuberculoid leprosy (TL) suggesting that ethnicity could play an important role in clinical forms [26].
Both M. leprae and M. lepromatosis have been found by PCR of tissue in LP, which shows that both species can trigger this immunological reaction suggesting a host component, rather than the species of Mycobacterium would be responsible for this reaction [27]. Reported cases of LP associated to M. lepromatosis have been mostly from subjects originating from Mexico or the Caribbean [12,28,29,30].
HIV infection has altered the epidemiology of several mycobacterial infections particularly M. tuberculosis and Mycobacterium avium intracellulare complex infection, which have increased their prevalence and severity in these population [31], however the number of leprosy cases has not increased due to HIV infection and HIV seroprevalence among cases newly diagnosed with leprosy have not shown significant difference between case and control groups [32].
Since HIV primarily affects the host cell-mediated immune response, it was expected that there would be an increase in lepromatous leprosy in co-infected individuals; however, the clinical spectrum of leprosy has not been modified in HIV-infected patients[33].
The histopathological findings have not been modified by HIV infection either. A study compared the histological findings in patients co-infected with leprosy and HIV infection vs patients infected with leprosy alone and did not find histopathological differences between both groups. Typical histological lesions were found in co-infected patients with a granulomatous-type immune response [34]. Granuloma formation in leprosy has not been affected in co-infected subjects with HIV even with low CD4+ T-cell counts [36].
Nevertheless, an increased incidence of leprosy was observed within the first 3 months following initiation of antiretroviral (ARV) therapy because of immune reconstitution, although no significant difference was found in patients treated for more than 3 months [36]. Some cases of paradoxical immune reconstitution inflammatory syndrome (IRIS) after starting ARV therapy have been reported [37,38] principally manifested with leprosy T1R after improving cell-mediated immunity by increasing the CD4+ T lymphocyte count usually within the first six months of ARV therapy, mostly in borderline forms predominantly BT form [39].
Although an increase in leprosy reactions has been reported in people co-infected with HIV/leprosy[40,41], a cohort study of 40 patients co-infected vs 107 patients non-HIV-infected followed for 2 years found no increase in frequency of leprosy reactions, 86.7% of the reactions in the co-infected group were T1R, 53.3% as a manifestation of IRIS and 93.3% of the patients were in AIDS stage, showing that several factors may influence the immune behavior of both diseases. The co-infected group did not present clinical or histological differences in the leprosy reactions presented vs the leprosy alone group [42].
The largest cohort of HIV/leprosy coinfected patients reported in Brazil found that of 92 coinfected subjects, 33 (36%) patients had a leprosy reaction at the time of diagnosis, of which 32 (97%) had T1R and the use of ARV therapy was the only factor associated with T1R [43]. Although T1R is clearly more common in co-infected patients, sporadic cases of LP and ENL have been reported in the context of unmasking or paradoxical IRIS [44,45,46].
LP is considered a life-threatening medical emergency [47] and sepsis is a frequent complication in subjects with LP due to bacterial superinfection of the lesions with fatal results [48]. Systemic antibiotics for sepsis were used in 15/49 (30.6%) of subjects with LP presenting a high mortality [12]. In the present case, the patient died from sepsis.
The clinical characteristics of the lesions presented in our case showed nodular lesions that evolved into deep painful necrotic ulcers with systemic symptoms (fever, malaise) consistent with nENL, while the histological characteristics corresponded to LP with skin necrosis, vasculitis and thrombosis with a high AFB load in an untreated patient with DLL. We consider that the severe lack of cell-mediated immune response in this HIV-infected patient with very low CD4+ T cells count led to a high bacillary load as revealed in the histopathological findings that triggered the known pathophysiological mechanisms of this reaction.
4. Conclusions
Vasculonecrotic reactions are considered a life-threatening medical condition. To our knowledge, this is the first case reported of leprosy vasculonecrotic reaction in HIV-infected subjects not associated with IRIS caused by M. lepromatosis. Leprosy vasculonecrotic reactions may not be easily recognized in HIV-infected individuals, where also atypical severe presentations of various infections may occur, including cutaneous cryptococcosis, disseminated sporotrichosis, malignant syphilis, cutaneous mycobacterial infections among others, hence the diagnosis is challenging. Delay in recognition of the disease can lead to untimely start of appropriate treatment with poor outcomes including devastating cutaneous damage, sepsis and high risk of death.
Author Contributions
Conceptualization, F.A.-L. and J.L.M.-G.; methodology, F.J.B.-R. and J.L.M.-G.; software, X.X.; validation, F.J.B.-R. and J.L.M.-G.; formal analysis, F.A.-L. F.J.B.-R. and J.L.M.-G; investigation, F.A.-L.; resources, L.A.G.-H.; data curation, P.M.-A.; writing—original draft preparation, P.M.-A.; writing—review and editing, F.A.-L. and J.L.M.-G.; visualization, L.A.G.-H. and J.F.A.-V.; supervision, F.A.-L.; project administration, J.F.A.-V..; funding acquisition, L.A.G.-H.
Funding
This research received no external funding.
Institutional Review Board Statement
This is a case report, and no IRB approval is necessary. Case reports are exempt from IRB according to Hospital Civil de Guadalajara policy.
Informed Consent Statement
Informed consent for publication was obtained from the patient for the case report and imaging.
Data Availability Statement
All data are included within the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Han, X.Y.; Mistry, N.A.; Thompson, E.J.; Tang, H.L.; Khanna, K.; Zhang, L. Draft Genome Sequence of New Leprosy Agent Mycobacterium lepromatosis. Genome Announc. 2015, 3. [Google Scholar] [CrossRef]
- Singh, P.; Benjak, A.; Schuenemann, V.J.; Herbig, A.; Avanzi, C.; Busso, P.; et al. Insight into the evolution and origin of leprosy bacilli from the genome sequence of Mycobacterium lepromatosis. Proceedings of the National Academy of Sciences. 2015, 112, 4459–4464. [Google Scholar] [CrossRef]
- Antunes, D.E.; Santos, D.F.; Lima, M.I.S.; Caixeta, L.P.; Correa, M.B.C.; Moraes ECdos, S.; et al. Clinical, epidemiological, and laboratory prognostic factors in patients with leprosy reactions: A 10-year retrospective cohort study. Front Med (Lausanne). 2022, 9. [Google Scholar] [CrossRef]
- Luo, Y.; Kiriya, M.; Tanigawa, K.; Kawashima, A.; Nakamura, Y.; Ishii, N.; et al. Host-Related Laboratory Parameters for Leprosy Reactions. Front Med (Lausanne). 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Góes, L.D.M.; Morais PMde Rebello, P.F.B.; Schettini, A.PM. Necrotic erythema nodosum reaction associated with histological alterations of Lucio’s phenomenon. An Bras Dermatol. 2022, 97, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Tourlaki, A.; Marzano, A.V.; Gianotti, R.; Fiallo, P.; Nunzi, E.; Alessi, E. Necrotic Erythema Nodosum Leprosum as the First Manifestation of Borderline Lepromatous Leprosy. Arch Dermatol. 2008, 144. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, R.; Singh, N.; Chatterjee, D.; Saikia, U.N.; Narang, T.; Dogra, S. Lucio phenomenon or necrotic erythema nodosum leprosum: walking the thin line. Int J Dermatol. 2020, 59. [Google Scholar] [CrossRef]
- Chandrashekar, L.; Kumari, R.; Thappa, D.; Badhe, B.; Ranugha, P. Is it lucio phenomenon or necrotic erythema nodosum leprosum? Indian J Dermatol. 2013, 58, 160. [Google Scholar] [CrossRef]
- Fogagnolo, L.; Souza EMde Cintra, M.L.; Velho, P.E.N.F. Vasculonecrotic reactions in leprosy. Brazilian Journal of Infectious Diseases. 2007, 11, 378–382. [Google Scholar] [CrossRef]
- Benard, G.; Sakai-Valente, N.Y.; Bianconcini Trindade, T.r.i.n.d.a.d.e. MA. Concomitant Lucio Phenomenon and Erythema Nodosum in a Leprosy Patient: Clues for Their Distinct Pathogeneses. Am J Dermatopathol. 2009, 31, 288–292. [Google Scholar] [CrossRef]
- Barreto Spandonari, C.; Villagra, D.J.; Flor, L.; Agüero Zaputovich, F.; Di Martino, B.; Aldama, A. Lucio´s phenomenon. About a case. Anales de la Facultad de Ciencias Médicas (Asunción). 2022, 55, 88–91. [Google Scholar] [CrossRef]
- Frade, M.A.C.; Coltro, P.S.; Filho, F.B.; Horácio, G.S.; Neto, A.A.; da Silva, V.Z.; et al. Lucio’s phenomenon: A systematic literature review of definition, clinical features, histopathogenesis and management. Indian J Dermatol Venereol Leprol. 2021, 88, 464. [Google Scholar] [CrossRef] [PubMed]
- Velarde-Félix, J.S.; Alvarado-Villa, G.; Vera-Cabrera, L. “Lucio’s Phenomenon” Associated with Mycobacterium lepromatosis. Am J Trop Med Hyg. 2016, 94, 483–484. [Google Scholar] [CrossRef]
- Ang, P.; Tay, Y.K.; Ng, S.K.; Seow, C.S. Fatal Lucio’s phenomenon in 2 patients with previously undiagnosed leprosy. J Am Acad Dermatol. 2003, 48, 958–961. [Google Scholar] [CrossRef]
- Aldama, A.; Wattiez, V.; Mendoza, G. Fenómeno de Lucio. Comunicación de 14 casos. Piel. 2018, 33, 81–85. [Google Scholar] [CrossRef]
- Curi, P.F.; Villaroel, J.S.; Migliore, N.; Albertengo, A.; Aquino, M.L.; Ceccato, F.; et al. Lucio’s phenomenon: report of five cases. Clin Rheumatol. 2016, 35, 1397–1401. [Google Scholar] [CrossRef]
- Yang, H.M.; Liu, S.W.; Li, Y.F.; Wang, Y.C. Lucio’s phenomenon. Journal of Microbiology, Immunology and Infection. 2023, 56, 647–648. [Google Scholar] [CrossRef]
- Dilipbhai Bodar, P.; Kailashbhai Patel, J.; Subramonia Pillai, D.; Vipul, V.o.r.a.R. Lucio phenomenon; A case report. Indian J Dermatol Venereol Leprol. 2023, 0, 1. [Google Scholar] [CrossRef]
- Han, X.Y.; Seo, Y.H.; Sizer, K.C.; Schoberle, T.; May, G.S.; Spencer, J.S.; et al. A New Mycobacterium Species Causing Diffuse Lepromatous Leprosy. Am J Clin Pathol. 2008, 130, 856–864. [Google Scholar] [CrossRef]
- Han, X.Y.; Quintanilla, M. Diffuse Lepromatous Leprosy Due to Mycobacterium lepromatosis in Quintana Roo, Mexico. J Clin Microbiol. 2015, 53, 3695–3698. [Google Scholar] [CrossRef]
- Sharma, G.; Sharma, V.D. Mycobacterium lepromatosis Lepromatous Leprosy in US Citizen Who Traveled to Disease-Endemic Areas. Emerg Infect Dis. 2019, 25, 389–390. [Google Scholar] [CrossRef]
- Collin, S.M.; Lima, A.; Heringer, S.; Sanders, V.; Pessotti, H.A.; Deps, P. Systematic Review of Hansen Disease Attributed to Mycobacterium lepromatosis. Emerg Infect Dis. 2023, 29. [Google Scholar] [CrossRef] [PubMed]
- Lucio, R.; Alvarado, I.; Francis, A. Opúsculo sobre el mal de San Làzaro, ó, Elefanciasis de los Griegos / escrito por los professores de medicina y cirugía Rafael Lucio e Ygnacio Alvarado.
- Latapi, F.; Chevez-Zamora, A. The “spotted” leprosy of Lucio: an introduction to its clinical and histological study. Int J Lepr. 1948, 16, 421–423. [Google Scholar]
- Han, X.Y.; Sizer, K.C.; Velarde-Félix, J.S.; Frias-Castro, L.O.; Vargas-Ocampo, F. The leprosy agents Mycobacterium lepromatosis and Mycobacterium leprae in Mexico. Int J Dermatol. 2012, 51, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Han, X.Y.; Aung, F.M.; Choon, S.E.; Werner, B. Analysis of the Leprosy Agents Mycobacterium leprae and Mycobacterium lepromatosis in Four Countries. Am J Clin Pathol. 2014, 142, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Singh, P.; McCoy, R.C.; Lenz, S.M.; Donovan, K.; Ochoa, M.T.; et al. Isolation of Mycobacterium lepromatosis and Development of Molecular Diagnostic Assays to Distinguish Mycobacterium leprae and M. lepromatosis. Clinical Infectious Diseases. 2020, 71, e262–e269. [Google Scholar] [CrossRef]
- Trave, I.; Barabino, G.; Cavalchini, A.; Parodi, A. Long-term ulcerations caused by Mycobacterium lepromatosis. Int J Mycobacteriol. 2020, 9, 223. [Google Scholar] [CrossRef]
- Han, X.Y.; Jessurun, J. Severe Leprosy Reactions Due to Mycobacterium lepromatosis. Am J Med Sci. 2013, 345, 65–69. [Google Scholar] [CrossRef]
- Vera-Cabrera, L.; Escalante-Fuentes, W.G.; Gomez-Flores, M.; Ocampo-Candiani, J.; Busso, P.; Singh, P.; et al. Case of Diffuse Lepromatous Leprosy Associated with “Mycobacterium lepromatosis”. J Clin Microbiol. 2011, 49, 4366–4368. [Google Scholar] [CrossRef]
- Massone, C.; Talhari, C.; Ribeiro-Rodrigues, R.; Sindeaux, R.H.M.; Mira, M.T.; Talhari, S.; et al. Leprosy and HIV coinfection: a critical approach. Expert Rev Anti Infect Ther. 2011, 9, 701–710. [Google Scholar] [CrossRef]
- Ustianowski, A.P.; Lawn, S.D.; Lockwood, D.N. Interactions between HIV infection and leprosy: a paradox. Lancet Infect Dis. 2006, 6, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Deps, P.; Lucas, S.; Porro, A.M.; Maeda, S.M.; Tomimori, J.; Guidella, C.; et al. Clinical and histological features of leprosy and human immunodeficiency virus co-infection in Brazil. Clin Exp Dermatol. 2013, 38, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Pires, C.A.A.; Miranda MFRde Bittencourt Mde, J.S.; Brito ACde, X.a.v.i.e.r. MB. Comparison between histopathologic features of leprosy in reaction lesions in HIV coinfected and non-coinfected patients*. An Bras Dermatol. 2015, 90, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, E.P.; Caneshi, J.R.; Nery, J.A.; Duppre, N.C.; Pereira, G.M.; Vieira, L.M.; et al. Cellular immune response to Mycobacterium leprae infection in human immunodeficiency virus-infected individuals. Infect Immun. 1995, 63, 1848–1854. [Google Scholar] [CrossRef]
- Couppié, P.; Domergue, V.; Clyti, E.; Guedj MEl Vaz, T.; Sainte-Marie, D.; et al. Increased incidence of leprosy following HAART initiation: a manifestation of the immune reconstitution disease. AIDS. 2009, 23, 1599–1600. [Google Scholar] [CrossRef]
- George, A.; Vidyadharan, S. Hansen’s disease in association with immune reconstitution inflammatory syndrome. Indian Dermatol Online J. 2016, 7, 29. [Google Scholar] [CrossRef]
- Viard, J.P.; Caux, F.; Bille, E.; Lévy, A.; Charlier, C.; Lortholary, O.; et al. Unmasking Leprosy: An Unusual Immune Reconstitution Inflammatory Syndrome in a Patient Infected with Human Immunodeficiency Virus. Am J Trop Med Hyg. 2010, 83, 13–14. [Google Scholar]
- Mouchard, A.; Blaizot, R.; Graille, J.; Couppié, P.; Bertin, C. Leprosy as immune reconstitution inflammatory syndrome in patients living with HIV: Description of French Guiana’s cases over 20 years and systematic review of the literature. PLoS Negl Trop Dis. 2022, 16, e0010239. [Google Scholar] [CrossRef]
- Lockwood, D.N.J.; Lambert, S.M. Human Immunodeficiency Virus and Leprosy: An Update. Dermatol Clin. 2011, 29, 125–128. [Google Scholar] [CrossRef]
- Batista, M.D.; Porro, A.M.; Maeda, S.M.; Gomes, E.E.; Yoshioka, M.C.N.; Enokihara, M.M.S.S.; et al. Leprosy Reversal Reaction as Immune Reconstitution Inflammatory Syndrome in Patients with AIDS. Clinical Infectious Diseases. 2008, 46, e56–60. [Google Scholar] [CrossRef]
- Pires, C.A.A.; Jucá Neto, F.O.M.; de Albuquerque, N.C.; Macedo, G.M.M.; Batista Kde, N.M.; Xavier, M.B. Leprosy Reactions in Patients Coinfected with HIV: Clinical Aspects and Outcomes in Two Comparative Cohorts in the Amazon Region, Brazil. PLoS Negl Trop Dis. 2015, 9, e0003818. [Google Scholar] [CrossRef] [PubMed]
- Menezes, V.M.; Nery, J.A.C.; Sales, A.M.; Miranda, A.; Galhardo, M.C.G.; Bastos, F.I.; et al. Epidemiological and clinical patterns of 92 patients co-infected with HIV and Mycobacterium leprae from Rio de Janeiro State, Brazil. Trans R Soc Trop Med Hyg. 2014, 108, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Arakkal, G.; Damarla, S.; Chanda, G. Immune reconstitution inflammatory syndrome unmasking erythema nodosum leprosum: A rare case report. Indian J Dermatol. 2015, 60, 106. [Google Scholar] [CrossRef]
- Serrano-Coll, H.A.; Beltrán-Alzate, J.C.; Buitrago, S.M.; Cardona-Castro, N. Lepromatous leprosy and human immunodeficiency virus co-infection associated with phenomenon of Lucio versus immune reconstitution inflammatory syndrome. Infectio. 2016, 20, 272–275. [Google Scholar] [CrossRef]
- Cusini, A.; Gunthard, H.F.; Weber, R.; Huber, M.; Kamarashev, J.; Bertisch, B.; et al. Lepromatous leprosy with erythema nodosum leprosum as immune reconstitution inflammatory syndrome in an HIV-1 infected patient after initiation of antiretroviral therapy. Case Reports. 2009, 2009, bcr0520091904–bcr0520091904. [Google Scholar] [CrossRef] [PubMed]
- Bernardes Filho, F.; Pess, D.; Akabane, A.L.; Foss, N.T.; Frade, M.A.C. Lucio’s phenomenon: A life-threatening medical emergency. International Journal of Infectious Diseases. 2018, 69, 94–95. [Google Scholar] [CrossRef]
- Kumari, R.; Thappa, D.M.; Basu, D. A fatal case of Lucio phenomenon from India. Dermatol Online J. 2008, 14. [Google Scholar] [CrossRef]
Figure 1.
(a, b) Multiple deep, punched-out ulcers, well-demarcated, covered by necrotic eschars. Some papules and nodules are evolving into necrotic ulcers on the face. (c) Ulcers on the back have an erythematous halo and (d) ulcers on extremities are in a later stage.
Figure 1.
(a, b) Multiple deep, punched-out ulcers, well-demarcated, covered by necrotic eschars. Some papules and nodules are evolving into necrotic ulcers on the face. (c) Ulcers on the back have an erythematous halo and (d) ulcers on extremities are in a later stage.

Figure 2.
Histopathology of a skin biopsy showing: (a) Epidermis with reactive changes, ulceration and necrosis of the epithelium, with acute inflammatory infiltrate at the expense of polymorphonuclear neutrophils (H&E, X5). (b) leukocytoclastic vasculitis (H&E, X40). (c) CD68 immunohistochemistry, positive immunostaining of perineurally located macrophages (X40). (d) Multiple acid-fast bacillary structures inside and outside the macrophages (Fite-Faraco stain, X40).
Figure 2.
Histopathology of a skin biopsy showing: (a) Epidermis with reactive changes, ulceration and necrosis of the epithelium, with acute inflammatory infiltrate at the expense of polymorphonuclear neutrophils (H&E, X5). (b) leukocytoclastic vasculitis (H&E, X40). (c) CD68 immunohistochemistry, positive immunostaining of perineurally located macrophages (X40). (d) Multiple acid-fast bacillary structures inside and outside the macrophages (Fite-Faraco stain, X40).
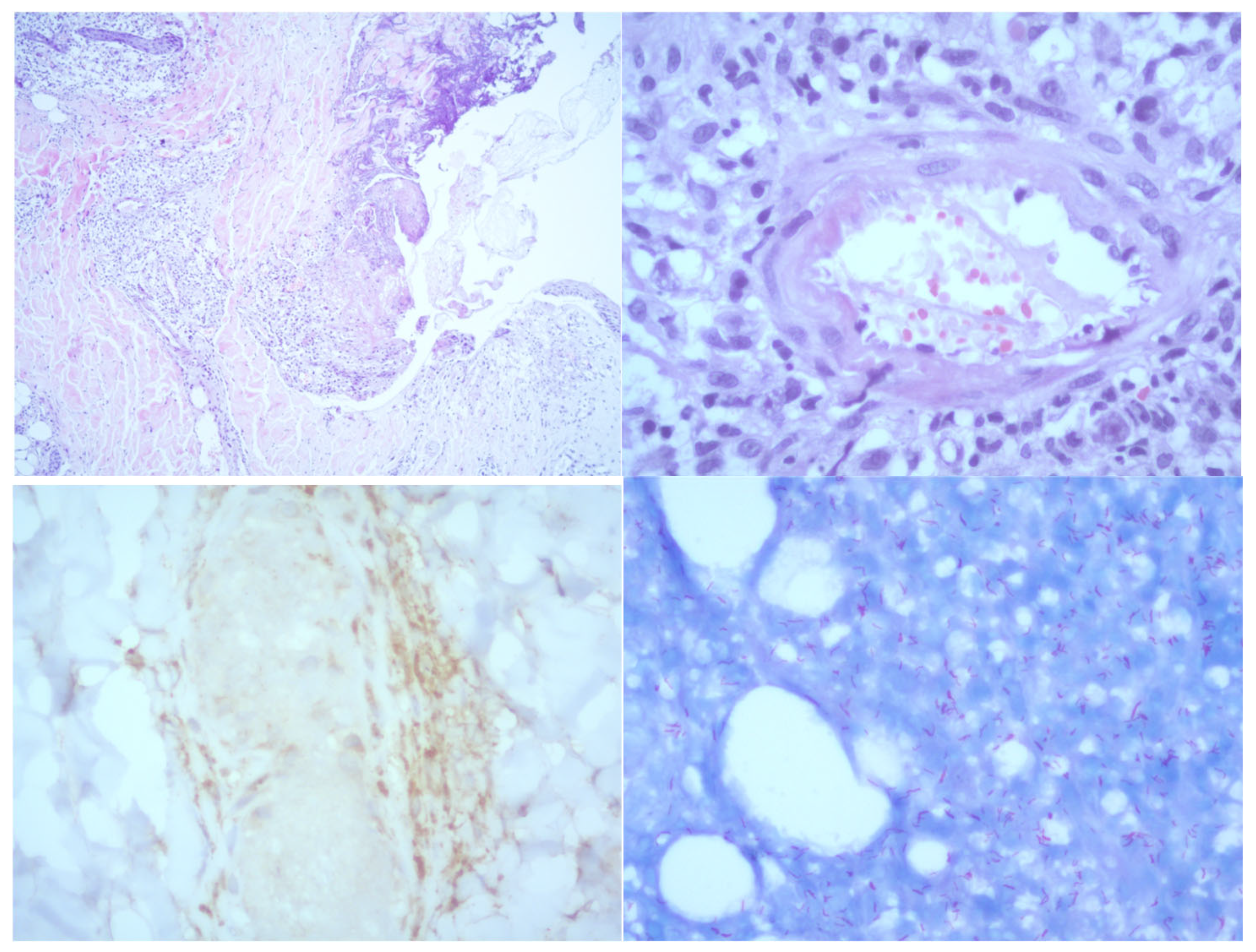
Figure 3.
1% agarose gel (left to right): Negative control: Sterile saline solution. Positive control: Sample from a patient with confirmed M. lepromatosis infection. Test sample: Amplified with LPMF-244 primers targeting a hemN gene region specific to Mycobacterium lepromatosis (absent in other known mycobacteria) 100 bp.
Figure 3.
1% agarose gel (left to right): Negative control: Sterile saline solution. Positive control: Sample from a patient with confirmed M. lepromatosis infection. Test sample: Amplified with LPMF-244 primers targeting a hemN gene region specific to Mycobacterium lepromatosis (absent in other known mycobacteria) 100 bp.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



