
Submitted:
16 April 2025
Posted:
17 April 2025
You are already at the latest version
Abstract
Background/Objectives: We aimed to identify differences in the relationship between patient activation, cancer-related symptoms, and job performance among young adult cancer survivors with low and high workplace support. Methods: Our cross-sectional observational study was conducted using an online survey across Japan in January 2022. The survey was designed to assess demographic and clinical characteristics, patient activation, physical fatigue, depression, cognitive impairments, and job performance. Multiple-group structural equation modeling (SEM) was conducted using data from 202 young adult cancer survivors. Results: Of the 202 participants, 53% were aged 35–39 years, 78% were female, and 67% were permanent workers. Patient activation was positively associated with job performance (β = 0.28, p < 0.01) and negatively related to cancer-related symptoms (β = -0.30, p = 0.01), and cancer-related symptoms were negatively associated with job performance (β = -0.29, p = 0.01), only among young adult cancer survivors with low workplace support. On the other hand, in the high support group, the path coefficients from patient activation to cancer-related symptoms (β = -0.06, p = 0.76), cancer-related symptoms to job performance (β = -0.12, p = 0.37), and patient activation to job performance (β = 0.20, p = 0.21) were not significant. Conclusions: Patient activation plays an important role in improving job performance, especially among young adult cancer survivors who lack workplace support. Even if obtaining workplace support is difficult for young adult cancer survivors, activation of self-management can improve their job performance.
Keywords:
Cancer Survivors
; Long Term Adverse Effects
; Patient Participation
; Social Support
; Work Performance
; Young Adult
1. Introduction
In cancer survivors, the disease, its treatment, and its associated complications would negatively influence their work [1]. Studies showed that although not all cancer survivors were employed, the proportion of overall cancer survivors working post-diagnosis was approximately 70% [2,3]. Maintaining job performance and pursuing employment after cancer diagnosis have been demonstrated to reduce financial burden, enhance self-esteem, and obtain a sense of normality, thereby improving health-related quality of life among cancer survivors [4,5,6]. Some studies found that cancer survivors who were employed were at higher risk of poor job performance than individuals without a cancer history [7,8]. Cancer-related symptoms including physical fatigue, depression, and cognitive impairment were risk factors for impaired job performance after controlling age, gender, educational level, the time since diagnosis, chemotherapy, type of occupation, and job demands [9,10,11,12,13]. A previous study suggested that, among young adult cancer survivors, who are commonly defined as individuals diagnosed with adult-onset cancer and aged 20 to 39 years [14], optimal work outcomes were considered more important than among older adult cancer survivors because young adult cancer survivors were in the formative years of their careers [15,16]. Although there have been studies on work outcomes among older adult cancer survivors, less is known about this population in young adulthood [15]. A further understanding of the work outcomes and these related factors among young adult cancer survivors will be essential for the future development of relevant services and resources for optimal work conditions.
In Japan, the Act for Eliminating Discrimination against Persons with Disabilities states that, "The companies must endeavor to improve the work environment and provide training for the relevant staff in order to appropriately ensure reasonable accommodation to implement the elimination of social barriers" [17]. It mandates that companies provide reasonable accommodation in the workplace for individuals holding a disability certificate. Additionally, under the Act to Facilitate the Employment of Persons with Disabilities [18], individuals with a disability certificate can utilize the employment quota held only for persons with disabilities and receive job support coaching. Although some cancer survivors had a disability certificate due to cancer and its treatment-related complications and were able to utilize these resources, many did not possess a disability certificate [19]. When a cancer survivor does not have a disability certificate, there are few public social resources available for them to utilize. Based on the guidelines for supporting the employment of cancer survivors [20], multidisciplinary teams at hospitals (e.g., healthcare staff, labor and social security attorney, social workers), Hello Work (public employment service center in Japan), and companies provide support to cancer survivors.
Past studies highlighted that workplace support plays an important role in improving job performance among cancer survivors and that the provision of job accommodation had a positive impact on return-to-work experience and job performance in cancer survivors or chronically ill individuals [21,22,23]. Employed cancer survivors often disclosed their cancer history at work and gained workplace support [24,25]. However, some reported workplace discrimination, including bullying and refusing accommodations, as well as constrained opportunities for career development [26]. Japanese young adult cancer survivors are also more likely to experience discrimination and prejudice related to cancer in their workplaces than older cancer survivors [27]. Furthermore, 35% of Japanese cancer survivors quit their jobs because they do not want to be a burden on the workplace, suggesting that it is difficult to request support for themselves from the workplace [28]. This situation indicated that young adult cancer survivors may not always receive workplace support. When obtaining workplace support is difficult and ineffective to improve work outcomes among cancer survivors, interventions targeting individual characteristics should be prioritized [29]. However, few studies have assessed modifiable individual factors, such as one’s problem-solving style (i.e., behavioral and cognitive traits in the face of problems) [29].
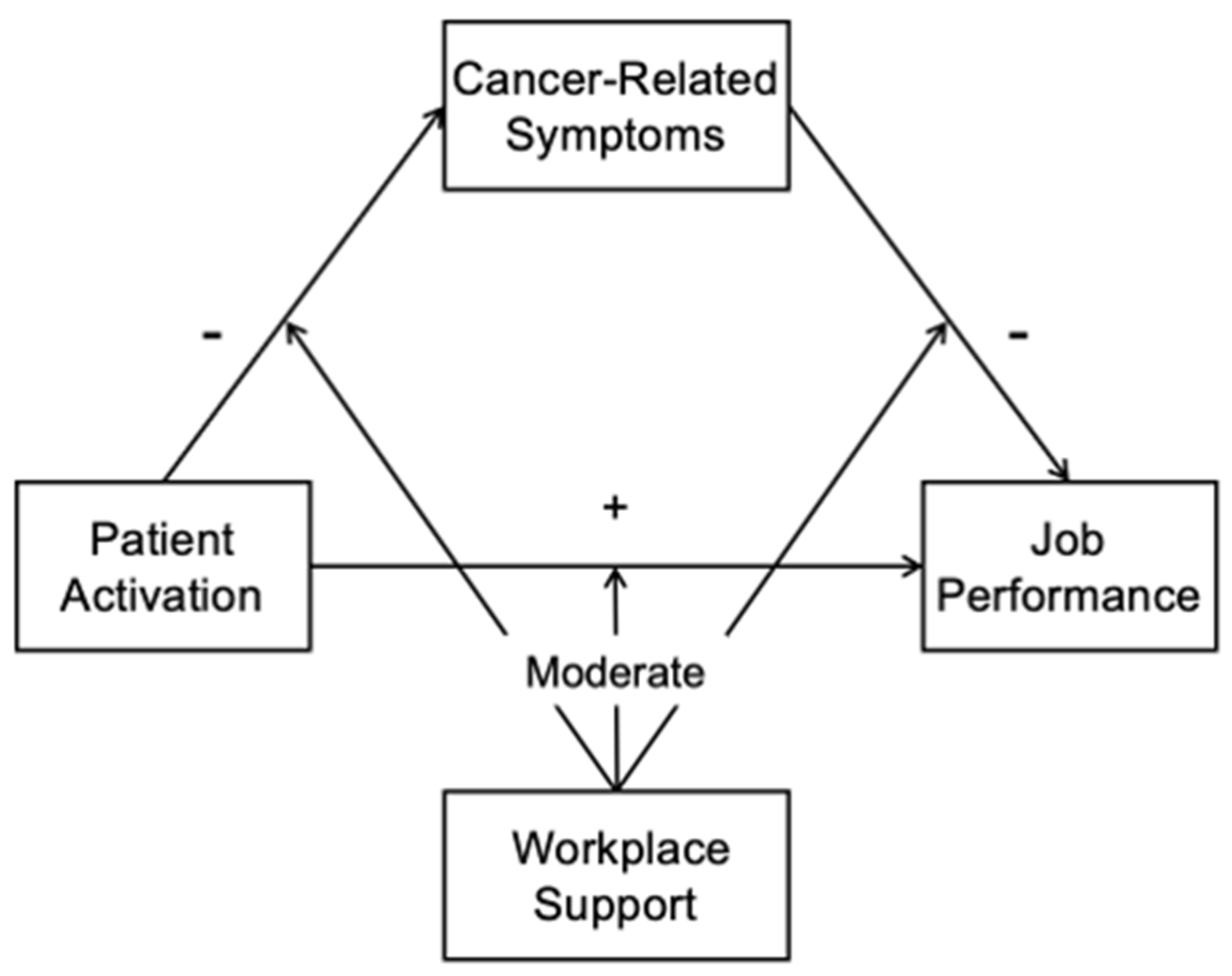
Patient activation is considered an important individual characteristic for improving job performance among cancer survivors. It is defined as an individual’s knowledge, skills, confidence, and behaviors for managing their health [30]. Patient activation relates to the act of making changes in health behaviors and a reduction in symptoms such as fatigue and psychological distress, resulting in better health-related quality of life among individuals with chronic conditions [31,32,33]. A study found that patient activation also improved job performance in terms of working accurately, finishing work on time, and concentrating on the job among cancer survivors [34]. Given that cancer-related symptoms were associated with low job performance [9,10,11,12,13] and high patient activation were associated with a reduction of cancer-related symptoms [31], activation of self-management may be an indirect cause for improved job performance through cancer-related symptoms (Figure 1). However, there was a paucity of empirical evidence on the direct and indirect effects of patient activation on job performance.
It is possible that patient activation is more valuable for maintaining job performance among young adult cancer survivors with low workplace support than among those with high workplace support. In a supportive work environment, cancer survivors can work according to their symptoms by adjusting the job demands, changing their tasks, and using flexible work arrangements, thereby mitigating the negative effects of their symptoms on their job [35,36,37]. Ten percent of Japanese cancer survivors quit their jobs due to difficulties in getting support from their workplace [28]. Additionally, 5–15% of Japanese cancer survivors leave their jobs because they are physically and psychologically unable to work [28], and managing their symptoms is also necessary for young adult cancer survivors to improve work outcomes. When young adult cancer survivors cannot mitigate the negative effects of their symptoms on their work by workplace support, they may need to reduce their negative impact on their work by handling their symptoms on their own; that is, patient activation would be more crucial for young adult cancer survivors without workplace support to maintain job performance than with workplace support. A previous study suggested that Japanese workers who received less support from their supervisors and coworkers were more likely to manage and improve their health on their own than those who received more support from their supervisors and coworkers [38]. In this way, the impact of patient activation on cancer-related symptoms and job performance among young adult cancer survivors may vary depending on workplace support (Figure 1). However, no previous studies have examined this difference due to workplace support among young adult cancer survivors.
Our study thus aimed to identify differences in the relationship between patient activation, cancer-related symptoms, and job performance among young adult cancer survivors with low and high workplace support. We hypothesized that, only among young adult cancer survivors with low workplace support, patient activation would be directly related to job performance, as well as indirectly related to job performance through cancer-related symptoms (Figure 1). We tested this hypothesis to suggest and devise effective interventions that would improve job performance among young adult cancer survivors, considering workplace support. Furthermore, clarifying whether patient activation directly or indirectly affects job performance would help determine whether to prioritize interventions on patient activation or cancer-related symptoms.
Figure 1.
Hypothesis model of this study. Note. The symbol “+” indicates a positive relationship and the symbol “-” indicates a negative relationship. Workplace support moderates the relationship between patient activation and cancer-related symptoms, between patient activation and job performance, and between cancer-related symptoms and job performance.
Figure 1.
Hypothesis model of this study. Note. The symbol “+” indicates a positive relationship and the symbol “-” indicates a negative relationship. Workplace support moderates the relationship between patient activation and cancer-related symptoms, between patient activation and job performance, and between cancer-related symptoms and job performance.
2. Materials and Methods
2.1. Study Participants and Procedures
Our study was a cross-sectional observational design using a web-based survey. Participants were included in this study if they were 20–39 years old; were diagnosed with cancer at an age of 20 years or older; were employed; completed treatment for cancer; and could understand the purpose of this study as well as complete a questionnaire in Japanese.
In January 2022, we invited 6,161 young adult cancer survivors aged 20–39 years who had registered with the commercial cancer panel system of Macromill Inc. (https://group.macromill.com) to participate in this study via email. Macromill Inc. is an internet research company based in Japan. Participants who were interested in this study logged into the online survey system provided by Macromill Inc. on their own devices (tablets, smartphones, etc.). They were informed about this study and gave researchers their consent to participate on the online survey system. They answered the questionnaire only if they gave their consent to participate. This study was approved by the Ethics Committee of the principal investigator’s institution (No. 1029).
2.2. Measures
2.2.1. Demographic and Clinical Characteristics
The following demographic and clinical characteristics were obtained from the participants through the questionnaire: age, gender, educational level, cancer sites, time since diagnosis, treatment, type of employment and occupation, job demands, and workplace support. We used two subscales of the New Brief Job Stress Questionnaire (New BJSQ) to assess job demands and workplace support, and each subscale had six items [39]. Each subscale score is calculated as the sum of item scores divided by the number of items. The missing item scores were imputed with the mean score of other items of the same subscale. If more than half of the items have missing responses, the score is not calculated. The possible response range for each subscale scores is 1 to 4, and a higher score indicates more job demands or workplace support. The Cronbach’s alpha in this study was 0.86 for the subscale on job demands and 0.93 for the subscale on workplace support. The national average score of the workplace support subscale of the New BJSQ was 2.53 points in Japan [39]. Thus, participants who scored less than 2.53 points on the workplace support subscale of the New BJSQ were categorized into the low support group and those who scored 2.53 points or higher were categorized into the high support group. Participants who scored less than 2.53 on the workplace support subscale of the New BJSQ were considered the “low support group” and those who scored 2.53 or higher were considered the “high support group.
2.2.2. Patient Activation
We used the Japanese version of the Patient Activation Measure-13 (PAM13) to assess patient activation [40]. This scale includes 13 items on the respondents’ knowledge, skills, confidence, and behaviors for managing their own health using a four-point Likert scale. The patient activation score is calculated by transforming the sum of all item scores to 0–100. The missing item scores were imputed with the mean score of other items of the PAM13. If more than half of the items are missing, the patient activation score is not calculated. A high score corresponds to a more proactive involvement in self-management. The validity and reliability of the Japanese version of the PAM13, including the internal consistency, test-retest reliability, factorial validity using the Rasch analysis, and concurrent validity against self-efficacy for treatment adherence, were confirmed among patients with mental disorders [40]. The Cronbach’s alpha in this study was 0.87.
2.2.3. Cancer-Related Symptoms
The Physical Fatigue subscale of the Cancer Fatigue Scale (CFS) was used to measure the participants’ physical fatigue [41]. The CFS includes three symptom domains including physical, affective, and cognitive fatigue. The Physical Fatigue subscale was used in the present study because the other subscales measure psychological and cognitive dimensions of fatigue. The Physical Fatigue subscale consists of seven items and uses a five-point Likert scale. The subscale score is calculated as the sum of the scores of all items. The missing item scores were imputed with the mean score of other items of the same subscale. If more than half of the items have missing responses, the score is not calculated. The score ranges from 0 to 28 for this subscale, and a higher score indicates more severe physical fatigue. The Cronbach’s alpha in this study was 0.94.
The Kessler-6 (K6) was used to measure depressive symptoms among participants [42]. It includes six items using a five-point Likert scale. The K6 score is calculated as the sum of the scores of all items. The missing item scores were imputed with the mean score of other items of the K6. If more than half of the items have missing responses, the K6 score is not computed. The score ranges from 0 to 24, and a higher score indicates more severe depressive symptoms. The Cronbach’s alpha in this study was 0.94.
The Cognitive Functioning subscale of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) was used to measure the participants’ cognitive impairments [43]. This subscale includes two items and uses a four-point Likert scale. The subscale score is calculated by transforming the average score for each item answered between 0–100. The missing item scores were imputed with the mean score of other items of the same subscale. If all the items have missing responses, the score is not calculated. A higher score indicates better cognitive functioning. This subscale has been used in numerous studies to assess the cognitive impairment of cancer survivors [44]. The Cronbach’s alpha in this study was 0.79.
2.2.4. Job Performance
We used the short form of the World Health Organization Health and Performance Questionnaire (WHO-HPQ) to assess job performance [45]. The WHO-HPQ measures the respondents’ actual performance using one numerical rating item from 0 to 10. This score is calculated as the item score multiplied by 10, and ranges from 0 (total lack of job performance) to 100 (no lack of job performance). If the single-item of WHO-HPQ is not responded to, the score is not calculated. A higher score on the respondents’ actual performance indicates better job performance.
2.3. Statistical Analysis
Frequencies, percentages, means, or standard deviations (SD) of demographic and clinical characteristics, patient activation, cancer-related symptoms, and job performance were calculated, and these variables were compared between the low and high support groups using the chi-squared test and Welch’s t-test. Furthermore, for the WHO-HPQ, correlation ratios (η2) with categorical variables and Spearman’s rank correlation coefficients (r) with continuous variables were calculated to explore the demographic and clinical characteristics that potentially confounded the association of job performance with patient activation and cancer-related symptoms.
Multiple-group structural equation modeling (SEM) was performed to examine differences in the relationship between patient activation, cancer-related symptoms, and job performance between young adult cancer survivors with low and high workplace support. First, we developed the model without any path constraints on the relationship between patient activation, cancer-related symptoms, and job performance. Cancer-related symptoms were set as a latent variable consisting of physical fatigue, depression, and cognitive impairments. Second, the model fit indicators were compared between the model without any path constraints and the models with equality constraints of each path and all paths to assess whether each relationship between the main variables was moderated depending on workplace support. Significant changes of chi-squared statistics in the constrained model indicated that path coefficients could be different between the low and high support groups. Insignificant changes of chi-squared statistics in the constrained model indicated that path coefficients could be equal. A good model fit was indicated by chi-square statistics divided by degrees of freedom (CMIN/df) < 2, comparative fit index (CFI) > 0.97, goodness-of-fit index (GFI) > 0.95, adjusted goodness-of-fit index (AGFI) > 0.90, and root mean square error of approximation (RMSEA) < 0.05 [46]. No demographic and clinical characteristics significantly correlated with job performance (WHO-HPQ) in the analysis of correlation ratios and Spearman’s rank correlation analysis. We therefore used the multiple-group SEM model, including only cancer-related symptoms, patient activation, and job performance, in further analyses. Standardized path coefficients (β) with 95% confidence intervals (CIs) were estimated using a bootstrap analysis with 2,000 iterations and were tested by the bias-corrected bootstrap test.
All analyses were performed using IBM SPSS and Amos software version 24 (SPSS, Inc., Chicago, IL, USA), and the significance level was set at 0.05 (two-tailed).
3. Results
Of 6,161 young adult cancer survivors, 693 returned the online questionnaires (response rate, 11.3%). This response rate was similar to that in a previous study [47]. Participants who were diagnosed with cancer at less than 20 years of age (n = 138), were unemployed (n = 120), did not complete treatment (n = 216), and did not complete the WHO-HPQ (n = 17) were excluded. Finally, we analyzed data from 202 young adult cancer survivors.
The low and high support groups consisted of 97 (48%) and 105 (52%) participants, respectively (Table 1). Of the participants, 107 (53%) were aged 35–39 years, 157 (78%) were female, and 135 (67%) were permanent workers. The most common diagnosis was female genital cancer (n = 85, 42%), including uterine (n = 76, 38%) and ovarian cancer (n = 9, 4%). A total of 122 participants (60%) received surgery. Overall, 72 (36%) of the participants were diagnosed more than five years ago. The high support group had a higher percentage of permanent workers (p = 0.01), a lower percentage of female genital cancer (p = 0.04), and a shorter time since diagnosis (p = 0.02) than did the low support group. No correlation coefficients between characteristics and job performance were significant. The mean scores of PAM13 and WHO-HPQ were 55.0 (SD = 14.7) and 63.9 (SD = 17.4), respectively (Table 2). The high support group reported a higher score on the WHO-HPQ than did the low support group (p < 0.01).
The multiple-group SEM showed a good model fit: CMIN/df = 0.39, CFI = 1.00, GFI = 0.99, AGFI = 0.98, and RMSEA = 0.00 (Figure 2). In the model of the low support group, the path coefficients from patient activation to cancer-related symptoms (β = -0.30, 95% CI -0.46 to -0.05, p = 0.01), cancer-related symptoms to job performance (β = -0.29, 95% CI -0.54 to -0.06, p = 0.01), and patient activation to job performance (β = 0.28, 95% CI 0.08 to 0.48, p < 0.01) were significant. On the other hand, in the model of the high support group, the path coefficients from patient activation to cancer-related symptoms (β = -0.06, 95% CI -0.31 to 0.26, p = 0.76), cancer-related symptoms to job performance (β = -0.12, 95% CI -0.42 to 0.15, p = 0.37), and patient activation to job performance (β = 0.20, 95% CI -0.08 to 0.43, p = 0.21) were not significant.
The comparisons of the model fit indicators between the model without any path constraints and the models with equality constraints of each path and all paths showed that the significance of the change of the chi-square statistics between the model without any path constraints and the other models were not statistically significant (Table 3). However, the model fit indicators of the model without any path constraints showed an overall tendency to be a better fit according to the absolute indicators (e.g., GFI and AGFI), than that of the model with the constraints each path and all paths.
4. Discussion
This study demonstrated that, only among young adult cancer survivors with low workplace support, patient activation was directly related to job performance, and indirectly related to job performance through cancer-related symptoms, which supported our hypothesis. Furthermore, the differences on path coefficients between patient activation, cancer-related symptoms, and job performance between low and high support groups would be supported by the changes of the model fit index (e.g., GFI, and AGFI), while there was no significant difference on path coefficients between the low and high support group. However, it may be premature to conclude the moderating effect of workplace support in the relationship between patient activation, cancer-related symptoms, and job performance. Even if employed cancer survivors often disclosed their cancer history at work [24,25], some reported workplace discriminations as well as low workplace support [26]. Of Japanese adult cancer survivors, 10% reported that it was difficult for them to receive enough support from their workplace [28]. Our findings on the differences of the impact of patient activation on cancer-related symptoms and job performance depending on workplace support should be considered because of the practical importance of the role of patient activation among Japanese young adult cancer survivors lacking workplace support.
Our study demonstrated that the direct and positive relationship between patient activation and job performance was observed only for young adult cancer survivors with low workplace support. In a previous study, cancer survivors with high patient activation were less likely to feel stressed at their job, which led to working accurately and finishing their job with concentration [34]. Patient activation reflects the sense of control in not only the health-related aspect, but also other life domains such as work [34,48]. Employees’ inability to control physical and psychological burdens in a job leads to lower productivity, increased sickness absence, and poor health and well-being [49]. Young adult cancer survivors with high patient activation may have the sense of controlling physical and psychological burden at their job, which results in improved job performance.
On the contrary, our study found that patient activation had no significant impact on job performance among young adult cancer survivors with high workplace support. The characteristics of any job are divided into job demands and resources [50]. Job resources stimulate employee initiatives to complete work goals [51]. Past studies showed that workplace support as a job resource resulted in shared values and attitudes of trust and reciprocity, as well as practices of collective action in a workplace, such as assisting other employees in completing work-related duties, which increased job performance [50,52]. This supportive work environment would enable young adult cancer survivors to maintain job performance, regardless of patient activation.
Previous studies did not find the mediating role of health conditions for the relationship between patient activation and work outcomes, including participation in paid work and work-related problems [34]. Our finding that patient activation was indirectly associated with job performance through cancer-related symptoms among young adult cancer survivors with low workplace support, was notable. In addition, although numerous previous studies reported modifiable workplace factors (e.g., physical and psychological job demands) that were relevant to job performance, few studies identified modifiable individual factors [29]. Our result highlights the importance of patient activation as an individual factor for improving job performance in a situation where workplace support and accommodation are less available.
On the other hand, our study did not indicate an indirect relationship between patient activation and job performance among young adult cancer survivors with high workplace support. Furthermore, this result suggests that workplace support reduces the adverse effect of cancer-related symptoms on job performance. One possible reason for this is that a supportive work environment does not require young adult cancer survivors to handle cancer-related symptoms and maintain job performance themselves through self-management. Among cancer survivors who received enough workplace support, supervisors and coworkers adjusted survivors’ burdens and tasks at the job according to their symptoms, and promoted their utilization of remote work and flexible timings [36,37]. Cancer survivors who availed themselves of a flexible work arrangement also maintained a balance between working and taking breaks, depending on their condition, without hesitation to coworkers and supervisors [35]. This workplace accommodation would enable young adult cancer survivors to work depending on their cancer-related symptoms, reducing their adverse effect on job performance and maintaining job performance, regardless of their self-management.
The results of this study suggested that workplace support reduced the adverse effects of cancer-related symptoms on job performance, though workplace support reduced the relationship between patient activation and job performance. A previous study and a guideline indicated that collaboration between healthcare staff and workplaces were important while making workplace accommodations for young adult cancer survivors [20,28]. Firstly, wherein nurses and other healthcare staff collect information from young adult cancer survivors about their job, and upon receiving survivors’ consent, healthcare staff and workplaces (i.e., employers, supervisors, coworkers, occupational physicians, or occupational health nurses) need to share their cancer diagnosis, treatment modalities, possible or existing cancer-related complications which negatively affect job performance, job tasks they are required to complete, and accommodations needed in their workplaces. Labor and social security attorneys or social workers may need to advise workplaces about laws and social welfare systems regarding workplace support and accommodations for young adult cancer survivors. The Basic Plan to Promote Cancer Control Programs in Japan prescribes that employers should support cancer survivors in balancing treatment and follow-up with working, promoting their understanding at the workplace, and forming a work climate that is suitable for them [53]. When healthcare staff share the information about young adult cancer survivors with their workplace, they would be more likely to receive workplace support. Even if young adult cancer survivors do not want to disclose such information to then receive enough support from their workplace, our findings suggested that nurses and other healthcare staff need to assess the existing symptoms of each young adult cancer survivor and provide them with tailored advice on symptom management and lifestyle change using relevant materials and websites, in order to enhance their patient activation. Healthcare staff should also assess whether young adult cancer survivors are confident in managing their symptoms and successfully implement these management strategies after advising them on symptom management. Some previous studies showed that a web-based intervention related to patient activation had a positive effect on patient activation in young adult cancer survivors than in older cancer survivors [54,55]. A similar web-based intervention may be more accessible and valuable for young adult cancer survivors, who are familiar with tablets and smartphones; this may help promote patient activation and manage their health conditions, thereby improving job performance.
Our study had certain limitations. First, the response rate of our study was low, and our study participation may be biased toward younger adult cancer survivors in better health condition, who are able to complete the questionnaire. In addition, our study participants included a high proportion of female genital and breast cancer survivors, reflecting the proportion of cancer types among young adults in Japan [56]. Thus, our findings had limited generalizability. Second, the participants had a higher educational level, considering that 54% graduated from university or graduate school, compared to the general Japanese population [57]. Previous studies reported that educational level was positively related to patient activation and job performance among cancer survivors [29,30]. Our study may overestimate the relationship between patient activation and job performance. Third, while the WHO-HPQ is a scale with sufficient validity and reliability, this scale is a single-item scale and may not adequately measure job performance. Further research should use a multidimensional measure of job performance, such as the Work Limitations Questionnaire [58], to verify our findings. Fourth, this study supported our hypothesis by the multiple-group SEM indicating a good model fit, but it had a cross-sectional observational design. Thus, causal relationships between patient activation, cancer-related symptoms, and job performance should be interpreted with caution. Further study using a longitudinal design is needed to identify this causal association. Finally, our study did not clarify the detailed workplace support that young adult cancer survivors received. Previous studies reported that cancer survivors received various types of workplace support, such as remote work and flextime [35,36,37]. Future research should inspect the differences in our findings by type of workplace support in effectively maintaining job performance.
5. Conclusions
The results indicated that patient activation would be directly related to job performance and be indirectly related to it through cancer-related symptoms only among young adult cancer survivors with low workplace support. Our findings suggest the importance of workplace support for young adult cancer survivors and patient activation for those with low workplace support in maintaining job performance. However, this study did not confirm the causal relationship between patient activation, cancer-related symptoms, and job performance due to a cross-sectional observational design. Given the limitation of the present study design, our findings require further research.
Author Contributions
Conceptualization, T.S., M.K., and M.T.; methodology, T.S., M.K., and M.T.; formal analysis, T.S.; investigation, T.S., M.K., and M.T.; writing—original draft preparation, T.S.; writing—review and editing, T.S., M.K., and M.T.; funding acquisition, T.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the grant from the Japan Society for the Promotion of Science (JSPS KAKENHI Grant-in-Aid for Young Scientists), grant number 19K19639.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Biological Research Involving Human Subjects established by the Ministry of Health, Labor, and Welfare of Japan, and approved by the Ethics Committee of the Graduate School of Health Sciences, Kobe University (August 31, 2021, No. 1029).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available because the authors did not receive approval from the Ethics Committee of the principal investigator’s institution to share the collected data publicly. Inquiries for data access may be addressed to the corresponding author (Takafumi Soejima, soejimat@people.kobe-u.ac.jp).
Acknowledgments
The authors would like to give special thanks to the young adult cancer survivors for participating in this study. We would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AGFI | Adjusted Goodness-of-Fit Index |
| CFI | Comparative Fit Index |
| CFS | Cancer Fatigue Scale |
| CMIN | Chi-Square Statistic |
| df | Degrees of Freedom |
| EORTC QLQ-C30 |
European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 |
| GFI | Goodness-of-Fit Index |
| K6 | Kessler-6 |
| New BJSQ | New Brief Job Stress Questionnaire |
| PAM-13 | 13-item version of Patient Activation Measure |
| RMSEA | Root Mean Square Error of Approximation |
| SD | Standard Deviation |
| SEM | Structural Equation Modeling |
| WHO-HPQ | World Health Organization Health and Performance Questionnaire |
References
- de Boer A.G.; Taskila T.;, Ojajärvi A.; van Dijk F.J.; Verbeek J.H. Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA 2009, 301, 753–762. [CrossRef]
- Jeon S.H. The long-term effects of cancer on employment and earnings. Health Econ 2017, 26, 671–684. [CrossRef]
- Tison A.; Sagaon-Teyssier L.; Sansonetti C.; Blatier J.F.; Paraponaris A.; VICAN group. Transitions in the labor market after cancer: a comparison of self-employed workers and salaried staff. Support Care Cancer 2016, 24, 4879–4886. [CrossRef]
- Torp S.; Paraponaris A.; Van Hoof E.; Lindbohm M.L.; Tamminga S.J.; Alleaume C.; Campenhout N.V.; Sharp L.; de Boer A.G. Work-related outcomes in self-employed cancer survivors: a European multi-country study. J Occup Rehabil 2019, 29, 361–374. [CrossRef]
- Bradley C.J.; Brown K.L.; Haan M.; Glasgow R.E.; Newman L.S.; Rabin B.; Ritzwoller D.P.; Tenney L. Cancer survivorship and employment: intersection of oral agents, changing workforce dynamics, and employers’ perspectives. J Natl Cancer Inst 2018, 110, 1292–1299. [CrossRef]
- Desiron H.A.; Crutzen R.; Godderis L.; Van Hoof E.; de Rijk A. Bridging health care and the workplace: formulation of a return-to-work intervention for breast cancer patients using an intervention mapping approach. J Occup Rehabil 2016, 26, 350–365. [CrossRef]
- Todd B.L.; Feuerstein E.L.; Feuerstein M. When breast cancer survivors report cognitive problems at work. Int J Psychiatry Med 2011, 42, 279–294. [CrossRef]
- Calvio L.; Peugeot M.; Bruns G.L.; Todd B.L.; Feuerstein M. Measures of cognitive function and work in occupationally active breast cancer survivors. J Occup Environ Med 2010, 52, 219–227. [CrossRef]
- Kim S.Y.; Kissane D.W.; Richardson G.; Senior J.; Morgan J.; Gregory P.; Birks S.; Ooi C.; Lipton L.; Antill Y.; Vereker M.; Michael N.; Bobevski I. The role of depression and other psychological factors in work ability among breast cancer survivors in Australia. Psychooncology 2022, 31, 167–175. [CrossRef]
- Dahl A.A.; Fosså S.D.; Lie H.C.; Loge J.H.; Reinertsen K.V.; Ruud E.; Kiserud C.E. Employment status and work ability in long-term young adult cancer survivors. J Adolesc Young Adult Oncol 2019, 8, 304–311. [CrossRef]
- Dorland H.F.; Abma F.I.; Van Zon S.K.R.; Stewart R.E.; Amick B.C.; Ranchor A.V.; Roelen C.A.M.; Bültmann U. Fatigue and depressive symptoms improve but remain negatively related to work functioning over 18 months after return to work in cancer patients. J Cancer Surviv 2018, 12, 371–378. [CrossRef]
- Von Ah D.; Storey S.; Crouch A. Relationship between self-reported cognitive function and work-related outcomes in breast cancer survivors. J Cancer Surviv 2018, 12, 246–255. [CrossRef]
- van Muijen P.; Duijts S.F.A.; Bonefaas-Groenewoud K.; van der Beek A.J.; Anema J.R. Predictors of fatigue and work ability in cancer survivors. Occup Med 2017, 67, 703–711. [CrossRef]
- Hydeman J.A.; Uwazurike O.C.; Adeyemi E.I.; Beaupin L.K.. Survivorship needs of adolescent and young adult cancer survivors: a concept mapping analysis. J Cancer Surviv 2019, 13, 34–42. [CrossRef]
- Stone D.S.; Ganz P.A.; Pavlish C.; Robbins W.A. Young adult cancer survivors and work: a systematic review. J Cancer Surviv 2017, 11, 765–81. [CrossRef]
- Braun I.; Friedrich M.; Morgenstern L.; Sender A.; Geue K.; Mehnert-Theuerkauf A.; Leuteritz K. Changes, challenges and support in work, education and finances of adolescent and young adult (AYA) cancer survivors: a qualitative study. Eur J Oncol Nurs 2023, 64, 102329. [CrossRef]
- Act for eliminating discrimination against persons with disabilities. Available online: https://www.japaneselawtranslation.go.jp/ja/laws/view/3052 (accessed on 25 May 2024).
- Act to Facilitate the Employment of Persons with Disabilities. Available online: https://www.japaneselawtranslation.go.jp/ja/laws/view/3845 (accessed on 25 May 2024).
- Ishida Y.; Hayashi M.; Inoue F.; Ozawa M. Recent employment trend of childhood cancer survivors in Japan: a cross-sectional survey. Int J Clin Oncol 2014, 19, 973-981. [CrossRef]
- Jigyojyo ni okeru chiryo to shigoto no ryoritsu shien no tame no gaidorain [Guidelines for supporting the balance of treatment and work in the workplace]. Available online: https://chiryoutoshigoto.mhlw.go.jp/dl/download/guideline.pdf (accessed on 10 Jun 2021).
- Hammond A.; O’Brien R.; Woodbridge S.; Bradshaw L.; Prior Y.; Radford K.; Culley J.; Whitham D.; Pulikottil-Jacob R. Job retention vocational rehabilitation for employed people with inflammatory arthritis (WORK-IA): a feasibility randomized controlled trial. BMC Musculoskelet Disord 2017, 18, 315. [CrossRef]
- van Vilsteren M.; Boot C.R.; Twisk J.W.; van Schaardenburg D.; Steenbeek R.; Voskuyl A.E.; Anema J.R. Effectiveness of an integrated care intervention on supervisor support and work functioning of workers with rheumatoid arthritis. Disabil Rehabil 2017, 39, 354–362. [CrossRef]
- Tamminga S.J.; Verbeek J.H.; Bos M.M.; Fons G.; Kitzen J.J.E.M.; Plaisier P.W.; Frings-Dresen M.H.W.; de Boer A.G. Effectiveness of a hospital-based work support intervention for female cancer patients - a multi-centre randomised controlled trial. PLoS One 2013, 8, e63271. [CrossRef]
- Rabin C. Cancer-related self-disclosure in the workplace/school by adolescent and young adult cancer survivors. J Adolesc Young Adult Oncol 2020, 9, 528–533. [CrossRef]
- Stergiou-Kita M.; Pritlove C.; van Eerd D.; Holness L.D.; Kirsh B.; Duncan A.; Jones J. The provision of workplace accommodations following cancer: survivor, provider, and employer perspectives. J Cancer Surviv 2016, 10, 489–504. [CrossRef]
- Stergiou-Kita M.; Pritlove C.; Kirsh B. The "Big C"-stigma, cancer, and workplace discrimination. J Cancer Surviv 2016, 10, 1035–1050. [CrossRef]
- Fujisawa D.; Umezawa S.; Fujimori M.; Miyashita M. Prevalence and associated factors of perceived cancer-related stigma in Japanese cancer survivors. Jpn J Clin Oncol 2020, 50, 1325–1329. [CrossRef]
- Takahashi M.; Tsuchiya M.; Horio Y.; Funazaki H.; Aogi K.; Miyauchi K.; Arai Y. Job resignation after cancer diagnosis among working survivors in Japan: timing, reasons and change of information needs over time. Jpn J Clin Oncol 2018, 48, 43–51. [CrossRef]
- Soejima T.; Kamibeppu K. Are cancer survivors well-performing workers? A systematic review. Asia Pac J Clin Oncol 2016, 12, e383–97. [CrossRef]
- Hibbard J.H.; Mahoney E.R.; Stockard J.; Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res 2005, 40, 1918–1930. [CrossRef]
- Hibbard J.H.; Mahoney E.; Sonet E. Does patient activation level affect the cancer patient journey? Patient Educ Couns 2017, 100, 1276–1279. [CrossRef]
- Rijken M.; Heijmans M.; Jansen D.; Rademakers J. Developments in patient activation of people with chronic illness and the impact of changes in self-reported health: results of a nationwide longitudinal study in The Netherlands. Patient Educ Couns 2014, 97, 383–390. [CrossRef]
- Greene J.; Hibbard J.H. Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. J Gen Intern Med 2012, 27, 520–526. [CrossRef]
- van Maarschalkerweerd P.; Rademakers J.; Rijken M. Cancer survivors’ activation to self-management and its relationship with participation in paid work and work-related problems. Psychooncology 2017, 26, 1881–1887. [CrossRef]
- Hallgren E.; Ayers B.L.; Moore R.; Purvis R.S.; McElfish P.A.; Maraboyina S.; Bryant-Smith G. Facilitators and barriers to employment for rural women cancer survivors. J Cancer Surviv 2023, 17, 1338-1346. [CrossRef]
- Kollerup A.; Ladenburg J.; Heinesen E.; Kolodziejczyk C. The importance of workplace accommodation for cancer survivors - The role of flexible work schedules and psychological help in returning to work. Econ Hum Biol 2021, 43, 101057. [CrossRef]
- Alleaume C.; Paraponaris A.; Bendiane M.K.; Peretti-Watel P.; Bouhnik A.D. The positive effect of workplace accommodations on the continued employment of cancer survivors five years after diagnosis. Support Care Cancer 2020, 28, 4435–4443. [CrossRef]
- Bochimoto H.; Ishimaru T.; Nakano A.; Hasegawa K.; Kimura E.; Tajima S.; Yoshikawa T.; Nemoto H. Association between workplace social support and use of health-promoting wearable devices: a prospective cohort study of Japanese employees. J UOEH 2023, 45, 95–103. [CrossRef]
- Inoue A.; Kawakami N.; Shimomitsu T.; Tsutsumi A.; Haratani A.; Yoshikawa T.; Shimazu A.; Odagiri Y. Development of a short questionnaire to measure an extended set of job demands, job resources, and positive health outcomes: the new brief job stress questionnaire. Industrial Health 2014, 52, 175–189. [CrossRef]
- Fujita E.; Kuno E.; Kato D.; Kokochi M.; Uehara K.; Hirayasu Y. Seishin no Kenko Kanri heno Sekkyokusei Hyoka Syakudo Nihongoban no Kaihatsu [Development and validation of the Japanese version of the patient activation measure 13 for mental health]. Seishin Igaku 2010, 52, 765–772. [CrossRef]
- Okuyama T.; Akechi T.; Kugaya A.; Okamura H.; Shima Y.; Maruguchi M.; Hosaka T.; Uchitomi Y. Development and validation of the cancer fatigue scale: a brief, three-dimensional, self-rating scale for assessment of fatigue in cancer patients. J Pain Symptom Manage 2000, 19, 5–14. [CrossRef]
- Furukawa T.A.; Kawakami N.; Saitoh M.; Ono Y.; Nakane Y.; Nakamura Y.; Tachimori H.; Iwata N.; Uda H.; Nakane H.; Watanabe M.; Naganuma Y.; Hata Y.; Kobayashi M.; Miyake Y.; Takeshima T.; Kikkawa T. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int J Methods Psychiatr Res 2008, 17, 152–158. [CrossRef]
- Kobayashi K.; Takeda F.; Teramukai S.; Gotoh I.; Sakai H.; Yoneda S.; Noguchi Y.; Ogasawara H.; Yoshida K. A cross-validation of the European Organization for Research and Treatment of Cancer QLQ-C30 (EORTC QLQ-C30) for Japanese with lung cancer. Eur J Cancer 1998, 34, 810–815. [CrossRef]
- Mayo S.J.; Lustberg M.; Dhillon H.M.; Nakamura Z.M.; Allen D.H.; Von Ah D.; Janelsins C.M.; Chan A.; Olson K.; Tan C.J.; Toh Y.L.; Oh J.; Grech L.; Cheung Y.T.; Subbiah I.M.; Petranovic D.; D’Olimpio J.; Gobbo M.; Koeppen S.; Loprinzi C.L.; Pang L.; Shinde S.; Ntukidem O.; Peters K.B. Cancer-related cognitive impairment in patients with non-central nervous system malignancies: an overview for oncology providers from the MASCC Neurological Complications Study Group. Support Care Cancer 2021, 29, 2821–2840. [CrossRef]
- Suzuki T.; Miyaki K.; Song Y.; Tsutsumi A.; Kawakami N.; Shimazu A.; Takahashi M.; Inoue A.; Kurioka S. Relationship between sickness presenteeism (WHO-HPQ) with depression and sickness absence due to mental disease in a cohort of Japanese workers. J Affect Disord 2015, 180, 14–20. [CrossRef]
- Schermelleh-Engel K.; Moosbrugger H.; Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods of Psychological Research Online 2003, 8, 23–74. [CrossRef]
- Endo M.; Muto G.; Imai Y.; Mitsui K.; Nishimura K, Hayashi K. Predictors of post-cancer diagnosis resignation among Japanese cancer survivors. J Cancer Surviv 2020, 14, 106–113. [CrossRef]
- Fowles J.B.; Terry P.; Xi M.; Hibbard J.; Bloom C.T.; Harvey L. Measuring self-management of patients’ and employees’ health: further validation of the Patient Activation Measure (PAM) based on its relation to employee characteristics. Patient Educ Couns 2009, 77, 116–122. [CrossRef]
- Cousins R.; MacKay C.J.; Clarke S.D.; Kelly C.; Kelly P.J.; McCaig R.H. ‘Management Standards’ work-related stress in the UK: practical development. Work Stress 2004, 18, 113–136. [CrossRef]
- Hakanen J.J.; Lindbohm M.L. Work engagement among breast cancer survivors and the referents: the importance of optimism and social resources at work. J Cancer Surviv 2008, 2, 283–295. [CrossRef]
- Yang T.; Ma T.; Liu P.; Liu Y.; Chen Q.; Guo Y: Zhang S.; Deng J. Perceived social support and presenteeism among healthcare workers in China: the mediating role of organizational commitment. Environ Health Prev Med 2019, 24, 55. [CrossRef]
- Baeriswyl S,; Krause A.; Elfering A. Berset M. How workload and coworker support relate to emotional exhaustion: The mediating role of sickness presenteeism. Int J Stress Manag 2017, 24, 52–73. [CrossRef]
- Overview of the Basic Plan to Promote Cancer Control Programs. Available online: https://www.mhlw.go.jp/english/wp/wp-hw3/dl/2-078.pdf (accessed on 5 Dec 2022).
- Yahaya N.A.; Abdullah K.L.; Ramoo V.; Zainal N.Z.; Wong L.P.; Danaee M. Effects of Self-Care Education Intervention Program (SCEIP) on activation level, psychological distress, and treatment-related information. Healthcare (Basel) 2022, 10, 1572. [CrossRef]
- Knoerl R.; Lee D.; Yang J.; Bridges C.; Kanzawa-Lee G.; Smith L.G,; Smith L.E.M. Examining the impact of a web-based intervention to promote patient activation in chemotherapy-induced peripheral neuropathy assessment and management. J Cancer Educ 2018, 33, 1027–1035. [CrossRef]
- National Cancer Center Japan: Cancer statistics in Japan 2021. Available online: https://ganjoho.jp/public/qa_links/report/statistics/2021_en.html (Accessed on 25 Nov 2021).
- Education at glance 2021: OECD indicators. Available online: https://www.oecd-ilibrary.org/sites/1426642c-en/index.html?itemId=/content/component/1426642c-en (Accessed on 5 Dec 2022).
- Lerner D., Amick B.C. 3rd.; Rogers W.H.; Malspeis S.; Bungay K.; Cynn D. The work limitations questionnaire. Med Care 2001, 39, 72–85. [CrossRef]
Figure 2.
Multiple-group SEM of the relationship between patient activation, cancer-related symptoms, and job performance. Note. The results of multiple-group SEM in (a) the low support group and (b) the high support group are shown. The latent variable “e” implies the error of each variable. Significant paths are in bold. * p < 0.05. ** p < 0.01.
Figure 2.
Multiple-group SEM of the relationship between patient activation, cancer-related symptoms, and job performance. Note. The results of multiple-group SEM in (a) the low support group and (b) the high support group are shown. The latent variable “e” implies the error of each variable. Significant paths are in bold. * p < 0.05. ** p < 0.01.
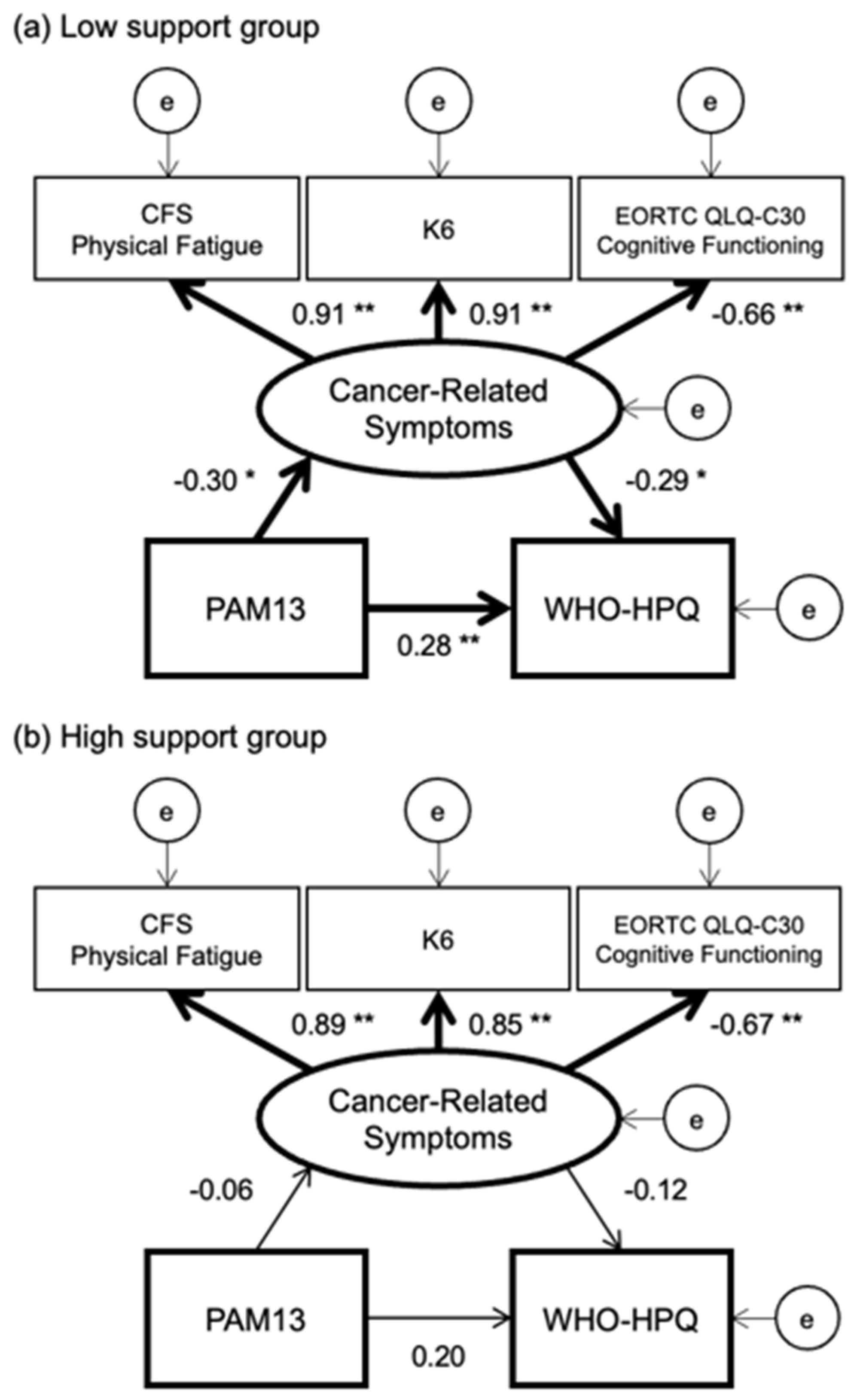

Table 1.
Demographic and clinical characteristics of participants.
| N = 202 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Low Support Group (n = 97) | High Support Group (n = 105) | WHO-HPQ | ||||||
| n | % | n | % | n | % | p a | η2 b | p b | |
| Age | 0.07 | 0.14 | 0.29 | ||||||
| 20–24 years | 7 | 3 | 2 | 2 | 5 | 5 | |||
| 25–29 years | 27 | 13 | 19 | 20 | 8 | 8 | |||
| 30–34 years | 61 | 30 | 28 | 29 | 33 | 31 | |||
| 35–39 years | 107 | 53 | 48 | 49 | 59 | 56 | |||
| Gender | 0.06 | 0.06 | 0.40 | ||||||
| Male | 45 | 22 | 16 | 16 | 29 | 28 | |||
| Female | 157 | 78 | 81 | 84 | 76 | 72 | |||
| Educational Level | 0.89 | 0.19 | 0.11 | ||||||
| Junior-High School | 4 | 2 | 2 | 2 | 2 | 2 | |||
| High School | 43 | 21 | 20 | 21 | 23 | 22 | |||
| College/Vocational School | 42 | 21 | 18 | 19 | 24 | 23 | |||
| University/Graduate School | 110 | 54 | 56 | 58 | 54 | 51 | |||
| Others | 3 | 1 | 1 | 1 | 2 | 2 | |||
| Type of Employment | 0.01 | 0.07 | 0.66 | ||||||
| Permanent | 135 | 67 | 55 | 57 | 80 | 76 | |||
| Temporary | 58 | 29 | 37 | 38 | 21 | 20 | |||
| Self-Employed | 9 | 4 | 5 | 5 | 4 | 4 | |||
| Type of Occupation | 0.80 | 0.18 | 0.37 | ||||||
| Technical | 38 | 19 | 17 | 18 | 21 | 20 | |||
| Managerial | 17 | 8 | 8 | 8 | 9 | 9 | |||
| Clerical | 76 | 38 | 35 | 36 | 41 | 39 | |||
| Sales | 20 | 10 | 9 | 9 | 11 | 10 | |||
| Production | 16 | 8 | 7 | 7 | 9 | 9 | |||
| Services | 25 | 12 | 14 | 14 | 11 | 10 | |||
| Others | 10 | 5 | 7 | 7 | 3 | 3 | |||
| Cancer Sites | 0.04 | 0.24 | 0.07 | ||||||
| Gastric Cancer | 16 | 8 | 6 | 6 | 10 | 10 | |||
| Colorectal Cancer | 16 | 8 | 8 | 8 | 8 | 8 | |||
| Breast Cancer | 18 | 9 | 11 | 11 | 7 | 7 | |||
| Female Genital Cancer | 85 | 42 | 50 | 52 | 35 | 33 | |||
| Thyroid Cancer | 17 | 8 | 7 | 7 | 10 | 10 | |||
| Lymphoma/Leukemia | 15 | 7 | 4 | 4 | 11 | 10 | |||
| Others | 35 | 17 | 11 | 11 | 24 | 23 | |||
| Period from Diagnosis | 0.02 | 0.11 | 0.27 | ||||||
| < 1 year | 32 | 16 | 15 | 15 | 17 | 16 | |||
| 1– < 5 years | 98 | 49 | 38 | 39 | 60 | 57 | |||
| ≥ 5 years | 72 | 36 | 44 | 45 | 28 | 27 | |||
| Treatment c | |||||||||
| Surgery | 122 | 60 | 54 | 56 | 68 | 65 | 0.19 | 0.00 | 0.97 |
| Chemotherapy | 50 | 25 | 22 | 23 | 28 | 27 | 0.51 | 0.02 | 0.76 |
| Radiation | 26 | 13 | 9 | 9 | 17 | 16 | 0.14 | 0.01 | 0.87 |
| Hormone Therapy | 18 | 9 | 10 | 10 | 8 | 8 | 0.50 | 0.05 | 0.44 |
| Mean | SD | Mean | SD | Mean | SD | p a | r d | p d | |
| Job Demands on New BJSQ | 2.6 | 0.7 | 2.5 | 0.7 | 2.7 | 0.7 | 0.16 | -0.08 | 0.25 |
| Workplace Support on New BJSQ |
2.5 | 0.8 | 1.9 | 0.5 | 3.2 | 0.4 | 0.02 | 0.27 | <0.01 |
Note. New BJSQ, New Brief Job Stress Questionnaire; SD, standard deviation; WHO-HPQ, World Health Organization Health and Performance Questionnaire. a The differences in characteristics between groups were tested by the chi-squared test for categorical variables and the Welch’s t-test for continuous variables. b The correlation ratio between characteristics and WHO-HPQ, and p-values were calculated. c Multiple answers allowed. d The Spearman’s ranked order correlation coefficients between characteristics and WHO-HPQ, and p-values were calculated.
Table 2.
Cancer-related symptoms, patient activation, and job performance of participants.
| N = 202 | |||||||
|---|---|---|---|---|---|---|---|
| Total | Low Support Group (n = 97) | High Support Group (n = 105) | |||||
| Mean | SD | Mean | SD | Mean | SD | p a | |
| Patient activation score on PAM13 | 55.0 | 14.7 | 54.9 | 15.9 | 55.1 | 13.6 | 0.92 |
| CFS Physical Fatigue subscale | 9.0 | 7.4 | 9.0 | 7.3 | 9.0 | 7.5 | 0.95 |
| K6 | 6.5 | 6.4 | 6.4 | 6.2 | 6.7 | 6.6 | 0.74 |
| EORTC QLQ-C30 Cognitive Functioning subscale |
67.5 | 26.3 | 69.1 | 26.5 | 66.0 | 26.1 | 0.41 |
| WHO-HPQ | 63.9 | 17.4 | 59.4 | 18.0 | 68.1 | 15.8 | <0.01 |
Note. CFS, Cancer Fatigue Scale; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30; K6, Kessler-6; PAM13, Patient Activation Measure-13; SD, standard deviation; WHO-HPQ, World Health Organization Health and Performance Questionnaire. a The differences in scores between groups were tested by the Welch’s t-test.
Table 3.
Comparisons of the model fit indicators between the models.
| N = 202 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Models a | CMIN | Change b | p c | CMIN/df | CFI | GFI | AGFI | RMSEA | AIC |
| Model without any path constraints |
3.11 | NA | NA | 0.389 | 1.000 | 0.994 | 0.977 | 0.000 | 47.112 |
| Model with path constraints | |||||||||
| PAM13 to Cancer-Related Symptoms |
5.11 | 2.00 | 0.16 | 0.567 | 1.000 | 0.974 | 0.954 | 0.000 | 47.107 |
| PAM13 to WHO-HPQ | 3.26 | 0.15 | 0.70 | 0.362 | 1.000 | 0.978 | 0.961 | 0.000 | 45.261 |
| Cancer-Related Symptoms to WHO-HPQ |
4.55 | 1.43 | 0.23 | 0.505 | 1.000 | 0.975 | 0.956 | 0.000 | 46.545 |
| All paths | 7.02 | 3.91 | 0.27 | 0.638 | 1.000 | 0.971 | 0.954 | 0.000 | 45.201 |
Note. AIC, Akaike Information Criterion; CMIN, chi-square statistics; CFI, Comparative Fit Index; df, degrees of freedom; GFI, Goodness-of-Fit Index; AGFI, Adjusted Goodness-of-Fit Index; PAM13, Patient Activation Measure-13; RMSEA, Root Mean Square Error of Approximation; WHO-HPQ, World Health Organization Health and Performance Questionnaire. a Equality constraints was placed between the low and high support groups. b Changes of chi-square statistics comparing to the chi-square of the model without any path constraints. c p-values were calculated to indicate the significance of chi-square change.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



