Submitted:
02 April 2025
Posted:
03 April 2025
You are already at the latest version
Abstract
We report an unusual case of a nonsmoker and hypertensive 72 years old male who was admitted in the Neurology Department of Clinical County Emergency Hospital Bihor, with a second transient ischemic attack. He was diagnosed two years before, with the occasion of the first stroke, with paroxismal atrial fibrillation and was treated with anticoagulants, on top of his antihypertensive medication. At that time carotid echocardiography revealed nonobstructive atherosclerosis and statin therapy was initiated in an intend to lower the initial 70 mg/dl LDL-cholesterol level under 55 mg/dl, as indicated by current guidelines. Cardioembolism was considered the mechanism of stroke at that time. Despite the medication and the LDL under 50 mg/dl, carotid atherosclerosis evolved to an important left internal carotid stenosis and transient ischemic attack reappeared two years later. It was difficult to know its mechanism, but probably carotid stenosis was the cause. The patient underwent medical treatment and endarterectomy with good outcome. To elucidate the reason of progressive atherosclerosis and to apply preventive treatment in this case was challenging. No chronic diseases were detected during the postoperative evaluation of the patient, except for early-stage periodontal disease, for which adequate preventive measures were applied. Considering that subclinical inflammation induced by periodontal disease can induce the progression of atherosclerosis, chronic treatment with colchicine was added, with favorable outcome.
Keywords:
carotid stenosis
; stroke
; atherosclerosis
; subclinical inflammation
; dyslipidemia target
; colchicine
; periodontal disease
1. Introduction
Stroke is a disabling disease that reduces quality of life. Transient ischemic attack is a type of stroke with transitory functional disability but with the same prognostic importance. It can precede or follow the stroke and is thus an alarm signal, to which we must pay special attention. In terms of secondary prevention, the approach to the patient with transient ischemic attack is similar to that of the patient with stroke [1,2].
When faced with a stroke patient, it is important to elucidate its mechanism, in order to treat it according to guidelines and to prevent a new one. The most common mechanism of stroke is cardio-embolism, mainly due to atrial fibrillation. A cause of at least equal importance is carotid atherosclerosis [1,2,3]. Atherosclerosis is the basis of many cardiovascular diseases. In order to reduce cardiovascular mortality and morbidity, it is necessary to control its risk factors. It also can be the hidden hallmark of a systemic disease and a multidisciplinary approach is necessary to reduce its consequences.
The treatment of a transient ischemic attack or stroke patient can be a real challenge in clinical practice. Quite often, despite a treatment considered effective and according to guidelines, patients return with a second episode [3,4]. Making a decision regarding treatment and especially secondary prevention can be difficult.
2. Detailed Case Description
We present the case of a 72 years old nonsmoker and hypertensive man who was admitted in The Clinical County Emergency Hospital Bihor, at Neurology Department, for two episodes of global aphasia of 10 minutes each, with complete remission. The clinical examination revealed a normal weight man, with normal teguments, osteoarticular, muscular and digestive systems, without any particular sign. The cardiopulmonary examination did not show any changes, the blood pressure was 180/103 mmHg, the heart rate was 46 bpm. No cardiac and vascular murmurs were detected. Neurological exam was normal, too. The laboratory exam is showed in Table 1.
Shortly after presentation, the medical staff performed an electrocardiogram, which revealed sinus bradycardia, with a heart rate of 46bpm and no ST/T changes. Cranial computed tomography showed several chronic infarction areas in the left frontal, parietal and in the left internal capsule (Figure 1).
The medical history of this patient is interesting. Two years ago, he presented in the emergency department after a short episode of aphasia, with complete remission. Physical examination was normal, like now and the computed tomography looked almost the same, with an old stroke and small changes due to hypertension. The case was interpreted as a transient ischemic attack, the patient was not admitted in the hospital and was deferred to ambulatory evaluation. Of note, he is an occasionally- three times a week- tennis player, with a good effort tolerance. The medication for hypertension was Olmesartan 40mg/day, Amlodipine 10mg/day, Rilmenidine 1mg/day and had taken this for four years and his blood pressure was between 120-130 systolic and 75-80 diastolic. The laboratory from that time is showed in Table 2.
The electrocardiogram revealed sinus bradycardia with a rate of 50 bpm. The echocardiography showed a slight increased left atrium volume, a slight left ventricular hypertrophy with a normal left ventricular ejection fraction. No thrombus was detected in the left atrium. Abdominal echography did not reveal pathological changes. The Doppler echography showed slight nonobstructive atherosclerosis of the left and right internal carotid arteries and no changes of the peripheral arteries. Keeping in mind the symptoms, the volume of the left atrium, the results of the computed tomography, the normal LDL-cholesterol levels and slight atherosclerosis of the both internal carotid arteries, the patient performed an ambulatory electrocardiographic monitoring, which revealed sinus bradycardia with a minimum heart rate of 32 bpm, even in the daytime, and short episodes of atrial fibrillation with a high ventricular rate (Figure 2).
Of note, after a slight daytime effort, the ventricular rate grew gradually to 100-110 bpm. The patient received apixaban 5mg twice a day (CHA2DS2-VA score 4) and atorvastatin 20mg once a day on top of his chronic treatment, to prevent future episodes of embolic ischemic attacks and to lower the LDL-cholesterol under 55mg/dl, as needed according to guidelines. The next two years the patient presented three times a year at neurologist and cardiologist. He was free of symptoms. During the visit at cardiologist, lower heart rates, usually below 40 bpm were observed. The patient was told that he needs a pace-maker, but he refused, because his effort tolerance was good and the heart rate grew during practicing tennis. The LDL-cholesterol levels lowered under 55 mg/dl and the treatment remained the same during the following two years.
During the present hospitalization, a Doppler echography of the precerebral vessels was done, revealing a pre-occlusive stenosis of the left internal carotid artery, which was not present two years ago. This stenosis was confirmed by computed tomography angiography of the supra-aortic arteries (Figure 3).
The transient ischemic attack appeared despite the correct anticoagulation and the level of LDL-cholesterol under 50 mg/dl. Very probably it was due to the left internal carotid stenosis. Aspirin was added to the treatment and the dose of atorvastatin was increased to maximum of 80 mg, given the pleiotropic effects of statin in atherosclerosis.
Keeping in mind the severity of carotid stenosis, the patient was deferred to vascular surgery.
Before the surgery, electrocardiogram was monitored for 24 hours, showing a minimum heart rate of 32 bpm in the night and 42 bpm during the daytime. Echocardiography looked almost the same like the old one and transesophageal echocardiography did not show any thrombus in the left atrium, nor in the left atrial appendage. The patient agreed pace-maker insertion, but the multidisciplinary team, consisting in neurologist, cardiologist, anesthesiologist and vascular surgeon decided that procedure to be postponed because of the risk of stroke. However, it is known that the manipulation of the carotid artery during the surgery could produce further bradycardia, but there is a high probability for it to respond to atropine, given the fact that it responds to effort. The patient was prepared for surgery and apixaban was replaced by enoxaparin for 48 hours.
The patient underwent endarterectomy of the left internal carotid artery (Figure 4), with complete anesthesia. During the intervention, a 3rd degree sinoatrial block was observed, with heart rate of 26 bpm. After intravenous atropine, the normal sinus rhythm reappeared.
The postoperative evolution was very good and after a week, a pacemaker was implanted. On top of his treatment, including apixaban, the patient received clopidogrel 75 mg/zi a la long. He will be reevaluated by vascular surgeon, cardiologist and neurologist once at 3 months for the first year and then annually.
After a month of recovery, the patient was referred to the internist for evaluation of a possible chronic disease which could be a trigger for the evolution of his atherosclerotic carotid disease. Laboratory tests, which included inflammatory markers and lipoprotein(a), chest radiography, abdominal ultrasound, gastroscopy and colonoscopy did not reveal the presence of such a condition. The same happened in the case of the otorhinolaryngological examination.
The dental evaluation revealed the presence of gingivitis, the first stage of periodontal disease, in which only the soft tissue of the gum is affected and the patient may be asymptomatic. The patient followed the preventive treatment according to the dentist's instructions. Considering the presence of periodontal disease as a cause of subclinical inflammation which could be involved in the mechanism of progression of atherosclerosis, we decided to add colchicine treatment. The ultrasound evaluation one year after the surgery did not reveal the evolution of carotid atherosclerosis, so the patient will follow chronic anti-inflammatory treatment, on top of his anti-hypertensive, anticoagulant, antiplatelet and high-dose statin therapy.
3. Discussion
Treating a patient with a history of atrial fibrillation and ischemic stroke despite oral anticoagulation is challenging. First of all, we had to discover the potentially mechanism of the second stroke in order to prevent the third.
Our patient presented in the Emergency Department after a second transient ischemic attack. One in every five strokes is caused by atrial fibrillation. This patient’s medical history included atrial fibrillation and according to the guidelines, the risk of ischemic stroke was substantially elevated, and the subjects had to be evaluated regarding the CHA2DS2-VA score [1]. This score includes congestive heart failure (one point), hypertension (one point), age ≥ 75 years (two points), diabetes mellitus (one point), prior stroke/transient ischemic attack/arterial thromboembolism (two points), vascular disease (one point), and age 65–74 years (one point) [1,2]. Our patient had a score of 4 and received apixaban, together with his antihypertensive medication and a statin, because nonobstructive carotid atherosclerosis was present, intending to lower the cardiovascular risk together with the LDL-cholesterol under 55mg/dl. Despite receiving anticoagulant and statin, he had a second transient ischemic attack. Of note, no significant vascular disease was diagnosed at that time.
The possible mechanism of stroke in this type of patients includes: competing mechanism, other than atrial fibrillation-related embolism, non-adherence to anticoagulant or insufficient dose, or cardio-embolism related or not to atrial fibrillation [3,4]. Polymeris et al [3] reported competing mechanism in 24%, insufficient anticoagulation in 32% and cardio-embolism despite anticoagulation in 44% among 2946 patients. In our patient, competing mechanism of transient ischemic attack is more reasonable, keeping in mind the positive result of computed tomography angiography and the negative one of transesophageal echocardiography.
Another challenge in this case is the evolution of carotid atherosclerosis, despite the levels of LDL-cholesterol lower than 50 mg/dl after statin treatment. Amarenco et al [5]concluded that after an ischemic stroke- including transient ischemic attack- patients treated with statin who had LDL- cholesterol target less than 70 mg/dl had a lower risk of subsequent cardiovascular events than those treated to LDL-cholesterol target of 90 to 110 mg/dl. In our patient carotid atherosclerosis developed with LDL-cholesterol level going under target. Considering the unilateral presence of the chronic neurological condition, we agree that the atherosclerotic mechanism could have been involved from the beginning in the etiology of the stroke and that perhaps we should have initiated antiplatelet therapy at that time, in addition to anticoagulant and statin therapy. Maybe other factors were implicated in this evolution.
It is important to say that the same experienced neurologist performed both the carotid echography. He used the NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria based on peak systolic velocity in the carotid arteries to diagnose severe carotid artery stenosis [6]. According to the guidelines [6,7], the patient has to receive dual antiplatelet therapy with aspirin and clopidogrel and carotid endarterectomy is indicated within 14 days because medical therapy alone is not sufficient to prevent stroke in patients with significant carotid stenosis [6,7,8].
During carotid endarterectomy, transitory bradycardia without hemodynamic compromise appeared, due to intraoperative carotid manipulation. Lauro et al [9] reported that intraoperative bradycardia and hypotension not responding to atropine and requiring vasopressors during and after carotid surgery was associated with major cardiovascular events. Our patient responded to intraoperative atropine and was hemodynamically stable during the postoperative period. Cardiovascular monitoring in the first 24 hour after surgery is needed [9]. After surgery, the patient received a pacemaker, as indicated.
According to guidelines, aspirin or clopidogrel is recommended long time after internal carotid artery revascularization It is necessary to assess neurological and cardiological symptoms, risk factors for atherosclerosis, hematological, renal and hepatic parameters and adherence to therapy [6,7]. The hypertension and dyslipidemia should be treated properly, to lower the risk of future cardiovascular events [10]. Our patient needs oral anticoagulation, antiplatelet therapy and a more carefully assessment, because of higher risk of bleeding.
The most important issue in this case was the unknown mechanism of the evolution of carotid atherosclerosis. From this point of view, we considered subclinical inflammation as a mechanism of atherosclerosis evolution, so that the maximum dose of statin in the treatment of this patient was desirable, due to its pleiotropic effect, even though the LDL-cholesterol value was under 50 mg/dl with a lower dose. Knowing that inflammation of the arterial wall may play a role in the evolution of atherosclerosis, anti-inflammatory therapy would be pivotal [11,12]. Maybe a lower LDL-cholesterol target is needed to certain individuals [13]. We must take into account other risk factors for atherosclerosis than the classic ones, too. Lipoprotein(a) should be one of them [14]. In this case, lipoprotein(a) was in the normal range
As the patient did not have apparently an inflammatory disease, he was recommended an evaluation for an autoimmune or another one, even though he has not any symptoms, with negative results. A dental evaluation was desirable, too, knowing that periodontitis is one of the most common underdiagnosed inflammatory disease and is associated with an increased cardiovascular risk [15]. After the detection of the first stage of periodontal disease, the patient was treated by a dentist, in order to prevent the evolution of his dental problem. In this case, the only explanation for the development of atherosclerosis was subclinical inflammation in the context of periodontal disease, and we choose to add colchicine to the chronic treatment because nowadays, colchicine proved its important role in the management of atherosclerosis [6,16,17].
4. Conclusion
There is always room for an unexpected evolution in the medical field, even though the therapy is according to guidelines. Atherosclerosis underlies many cardiovascular events and is one of the most surprising entities in medicine. Not all its faces are known yet. To treat and prevent future cardiovascular events, in this patient and perhaps in all, a multidisciplinary approach is mandatory, taking into account all clinical features, mechanisms, classical and novel risk factors for atherosclerosis and atherothrombosis.
Author Contributions
Conceptualization, C.C. and AC1; methodology, C.C., AC.1B.R. and I.T.I.; software, C.C., A.C2. and C.B.R; validation, C.C., A.C.1 and I.T.I.; formal analysis, C.C. and I.T.I.; investigation, C.C., A.C1., C.B.R.and I.T.I.; resources, C.C and C.B.R; data curation, C.C., C.B.R.and I.T.I..; writing—original draft preparation, C.C., I.T.I. and A.C2; writing- review and editing, C.C.,C.B.R.,I.T.I. and A.C2; visualization, C.C., A.C1., C.B.R. and I.T.I.; supervision, C.C.; project administration, C.C. and I.T.I.; funding acquisition, C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This APC was supported by University of Oradea, Romania.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of ORADEA COUNTY EMERGENCY CLINICAL HOSPITAL, ROMANIA (protocol number 10198/27.03.2025), for studies involving humans.
Informed Consent Statement
Informed consent was obtained from the subject involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request. The data are not publicity available due to privacy reasons.
Acknowledgments
We highly appreciate the work of the staff from Vascular Surgery Department- especially Dr. Mihaela Ecsedi and Ștefania IonelaSije-Clinical County Emergency Hospital Bihor.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; Casado-Arroyo, R.; Caso, V.; Crijns, H.J.G.M.; De Potter, T.J.R.; Dwight, J.; Guasti, L.; Hanke, T.; et al. 2024 ESC Guidelines for the Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal 2024, 45, 3314–3414. [Google Scholar] [CrossRef] [PubMed]
- Rienstra, M.; Tzeis, S.; Bunting, K.V.; Caso, V.; Crijns, H.J.G.M.; De Potter, T.J.R.; Sanders, P.; Svennberg, E.; Casado-Arroyo, R.; Dwight, J.; et al. Spotlight on the 2024 ESC/EACTS Management of Atrial Fibrillation Guidelines: 10 Novel Key Aspects. Europace 2024, 26, euae298. [Google Scholar] [CrossRef] [PubMed]
- Polymeris, A.A.; Meinel, T.R.; Oehler, H.; Hölscher, K.; Zietz, A.; Scheitz, J.F.; Nolte, C.H.; Stretz, C.; Yaghi, S.; Stoll, S.; et al. Aetiology, Secondary Prevention Strategies and Outcomes of Ischaemic Stroke despite Oral Anticoagulant Therapy in Patients with Atrial Fibrillation. J Neurol Neurosurg Psychiatry 2022, 93, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Galea, R.; Seiffge, D.; Räber, L. Atrial Fibrillation and Ischemic Stroke despite Oral Anticoagulation. JCM 2023, 12, 5784. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P.; Kim, J.S.; Labreuche, J.; Charles, H.; Abtan, J.; Béjot, Y.; Cabrejo, L.; Cha, J.-K.; Ducrocq, G.; Giroud, M.; et al. A Comparison of Two LDL Cholesterol Targets after Ischemic Stroke. N Engl J Med 2020, 382, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Mazzolai, L.; Teixido-Tura, G.; Lanzi, S.; Boc, V.; Bossone, E.; Brodmann, M.; Bura-Rivière, A.; De Backer, J.; Deglise, S.; Della Corte, A.; et al. 2024 ESC Guidelines for the Management of Peripheral Arterial and Aortic Diseases. European Heart Journal 2024, 45, 3538–3700. [Google Scholar] [CrossRef] [PubMed]
- Naylor, A.R.; Ricco, J.-B.; De Borst, G.J.; Debus, S.; De Haro, J.; Halliday, A.; Hamilton, G.; Kakisis, J.; Kakkos, S.; Lepidi, S.; et al. Editor’s Choice – Management of Atherosclerotic Carotid and Vertebral Artery Disease: 2017 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). European Journal of Vascular and Endovascular Surgery 2018, 55, 3–81. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, P.; Hobeanu, C.; Labreuche, J.; Charles, H.; Giroud, M.; Meseguer, E.; Lavallée, P.C.; Gabriel Steg, P.; Vicaut, É.; Bruckert, E.; et al. Carotid Atherosclerosis Evolution When Targeting a Low-Density Lipoprotein Cholesterol Concentration <70 Mg/dL After an Ischemic Stroke of Atherosclerotic Origin. Circulation 2020, 142, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Bogniotti, L.A.C.; Teivelis, M.P.; Cardozo, F.A.M.; Caramelli, B.; Wolosker, N.; Puech-Leão, P.; De Luccia, N.; Calderaro, D. Hemodynamic Depression after Carotid Surgery: Incidence, Risk Factors and Outcomes. Clinics 2022, 77, 100090. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. European Heart Journal 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Joseph, P.; Ishai, A.; Mani, V.; Kallend, D.; Rudd, J.H.F.; Fayad, Z.A.; Tawakol, A. Short-Term Changes in Arterial Inflammation Predict Long-Term Changes in Atherosclerosis Progression. Eur J Nucl Med Mol Imaging 2017, 44, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; Fernández-Ortiz, A.; Fernández-Friera, L.; García-Lunar, I.; Andrés, V.; Fuster, V. Progression of Early Subclinical Atherosclerosis (PESA) Study. Journal of the American College of Cardiology 2021, 78, 156–179. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. European Heart Journal 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Rehberger Likozar, A.; Zavrtanik, M.; Šebeštjen, M. Lipoprotein(a) in Atherosclerosis: From Pathophysiology to Clinical Relevance and Treatment Options. Annals of Medicine 2020, 52, 162–177. [Google Scholar] [CrossRef] [PubMed]
- Leng, Y.; Hu, Q.; Ling, Q.; Yao, X.; Liu, M.; Chen, J.; Yan, Z.; Dai, Q. Periodontal Disease Is Associated with the Risk of Cardiovascular Disease Independent of Sex: A Meta-Analysis. Front. Cardiovasc. Med. 2023, 10, 1114927. [Google Scholar] [CrossRef] [PubMed]
- González L, Bulnes JF, Orellana MP, Muñoz Venturelli P, Martínez Rodriguez G. The Role of Colchicine in Atherosclerosis: From Bench to Bedside. Pharmaceutics 2022, 14, 1395. [CrossRef] [PubMed]
- Tucker B, Goonetilleke N, Patel S, Keech A. Colchicine in atherosclerotic cardiovascular disease. Heart. 2024, 110, 618–625. [CrossRef] [PubMed]
Figure 1.
Computed tomography of the head.
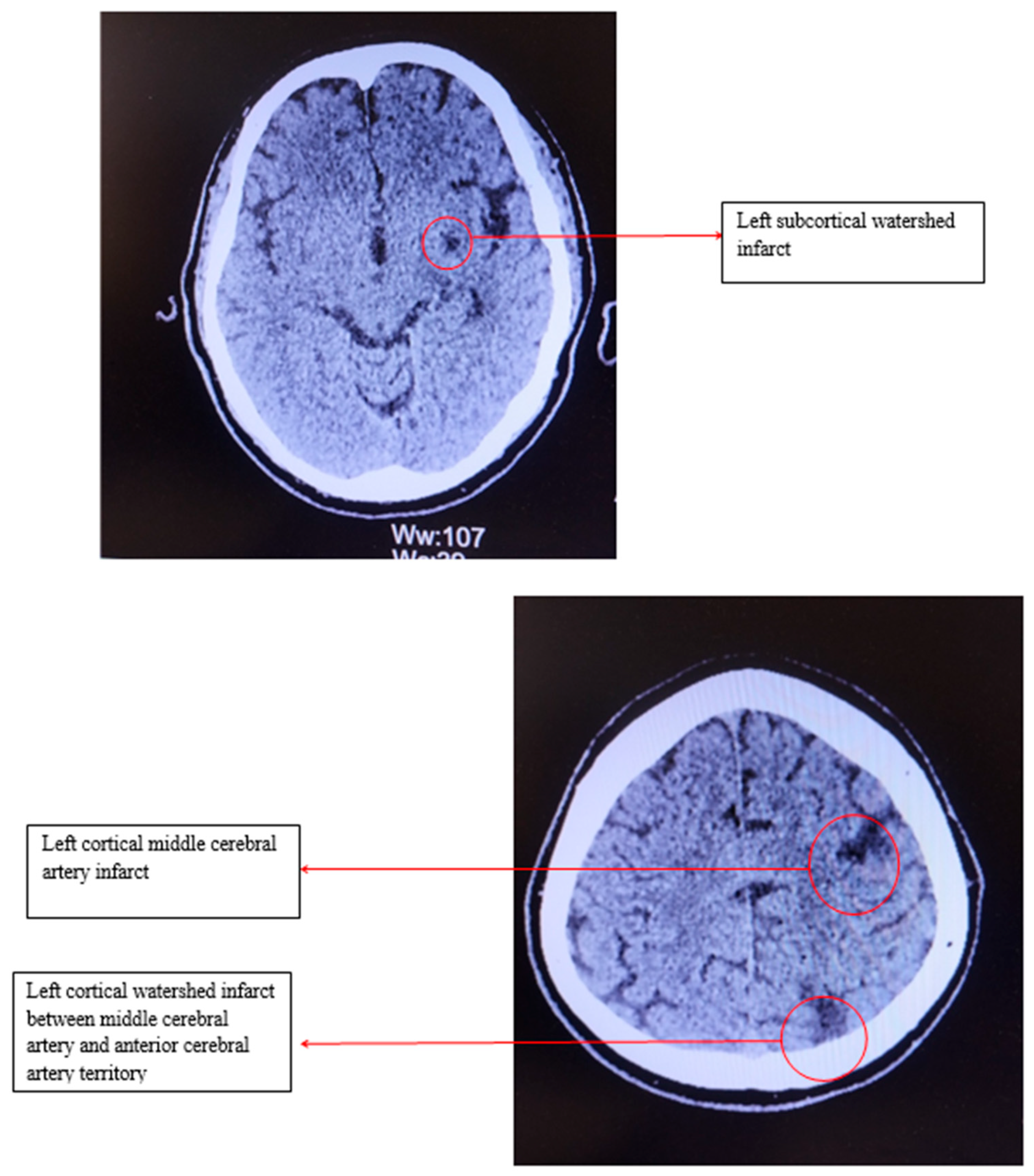
Figure 2.
Holter EKG Report.
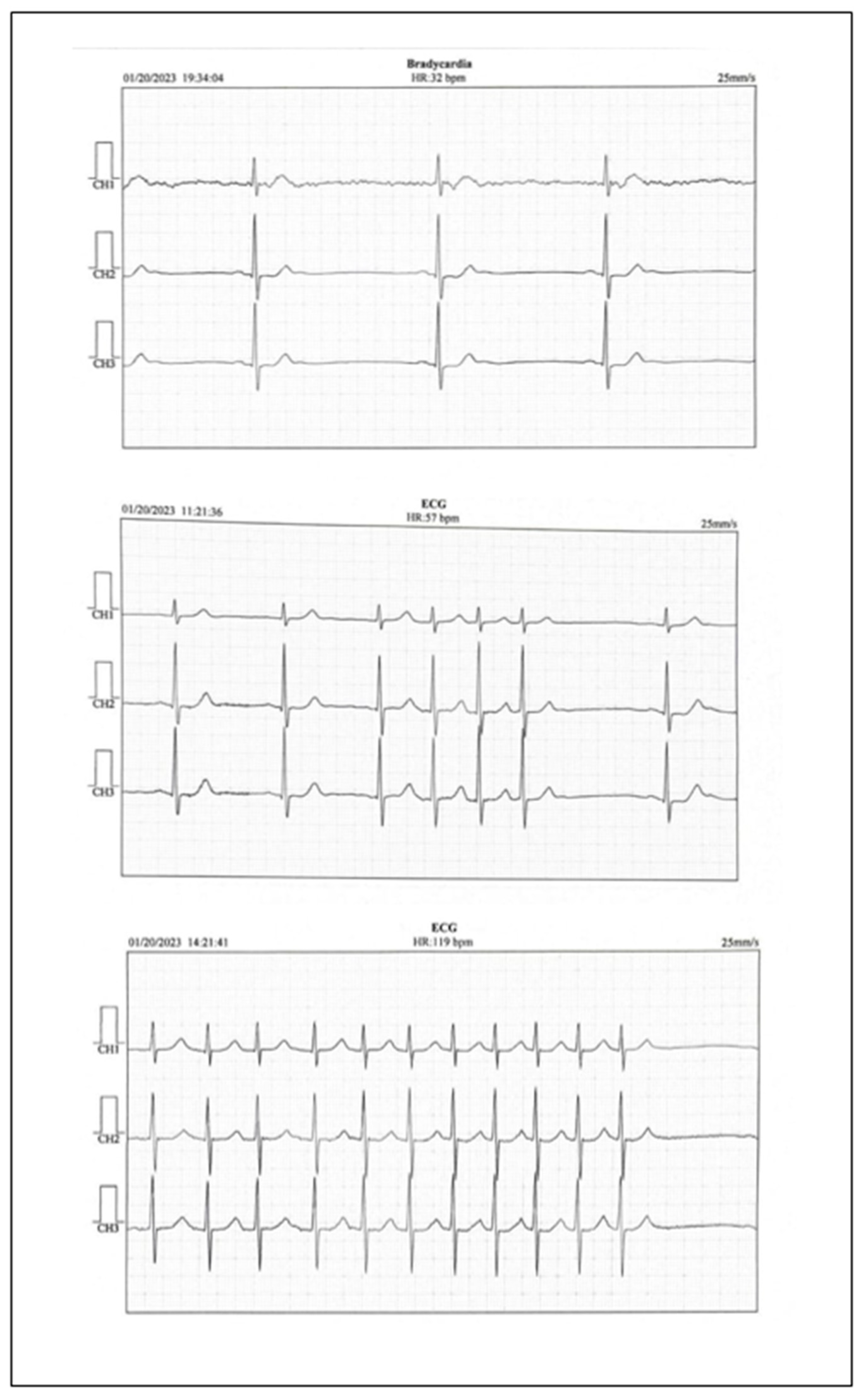
Figure 3.
Computed tomography angiography (CTA) of the supra-aortic arteries.
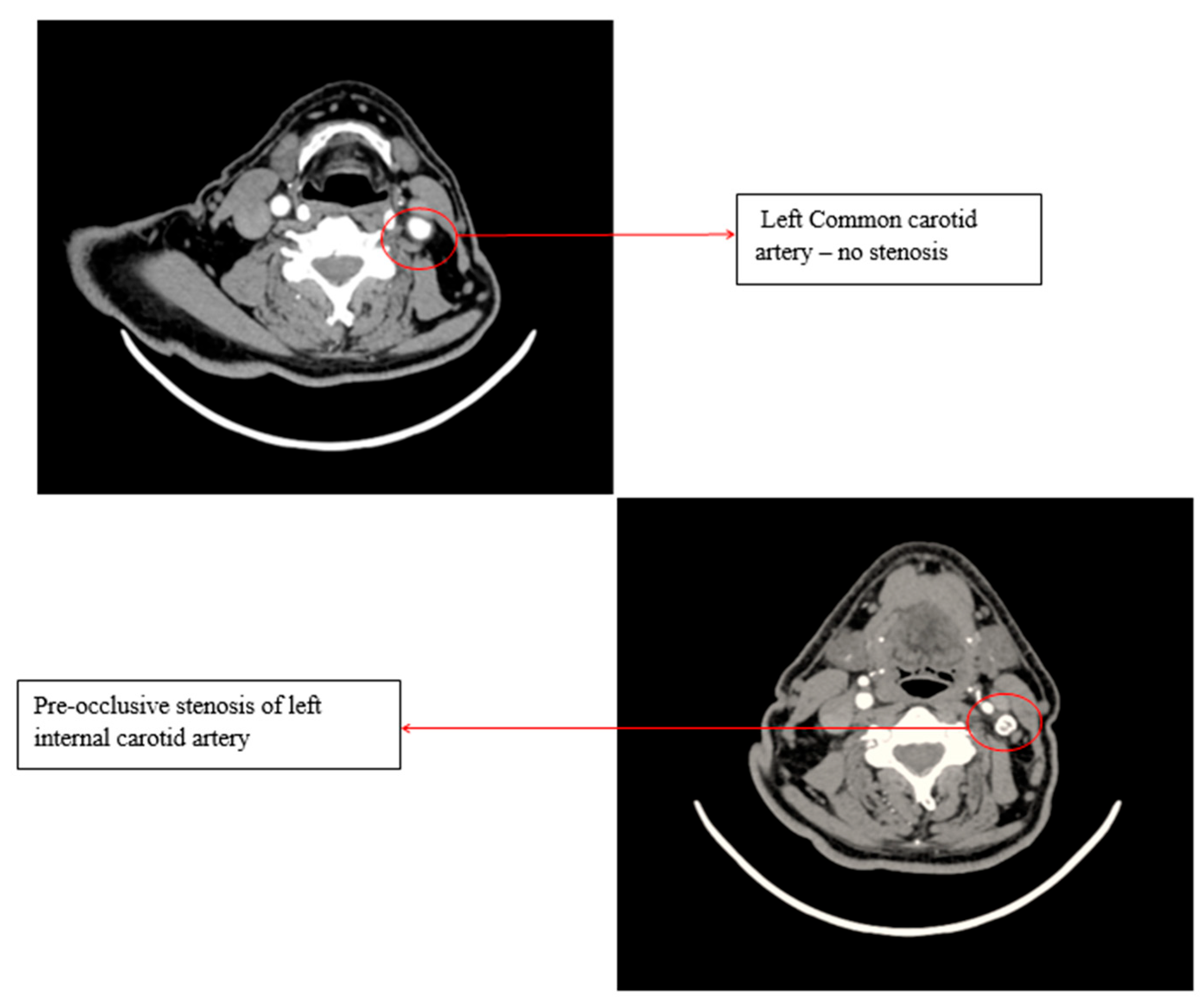
Figure 4.
Atheroma removed from left internal carotid artery.
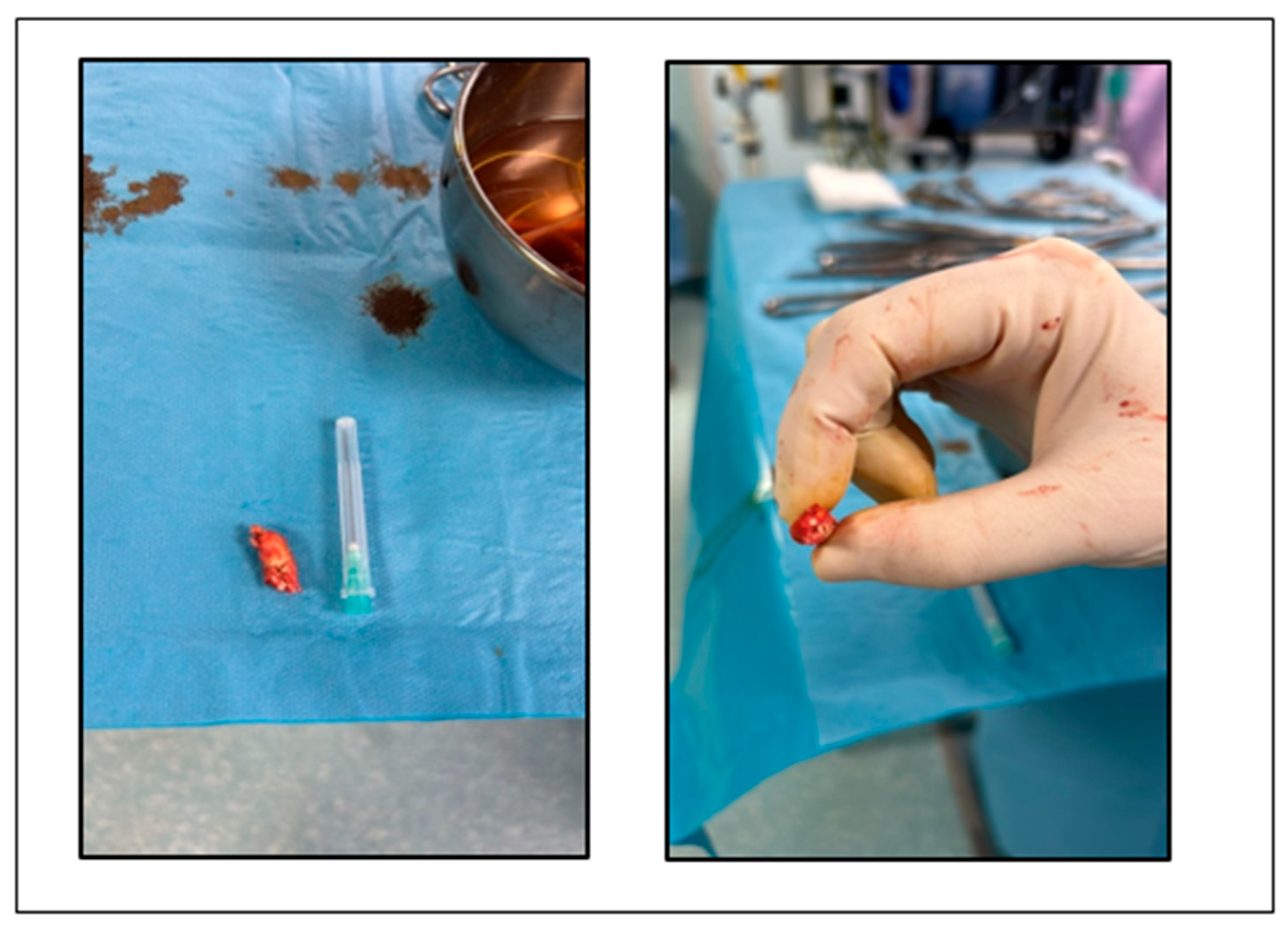

Table 1.
Blood and Urine Tests – Neurology Admission.
| Test | Result | Reference range |
| White Blood Cell Count | 9.81 10*3/uI | 4.00-10.0 10*3/uI |
| Hemoglobin | 14.1 g/dl | 12.6-17.4 g/dl |
| Platelet Count | 203 g/dl | 150-450 g/dl |
| Blood glucose | 94 mg/dl | 82-115 mg/dl |
| Total Cholesterol | 117 mg/dl | 0-200 mg/dl |
| Triglycerides | 108 mg/dl | 0-150 mg/dl |
| High-Density Lipoprotein Cholesterol | 49 mg/dl | 40-60 mg/dl |
| Low-Density Lipoprotein Cholesterol | 48.71 mg/dl | 10-100 mg/dl |
| Aspartate Transaminase | 30 U/L | 5-34 U/L |
| Alanine Transaminase | 13 U/L | 0-55 U/L |
| Total Bilirubin | 0.51 mg/dl | 0.2-1.2 mg/dl |
| Serum Urea | 25.00 mg/dl | 8.4-2.57 mg/dl |
| Serum Creatinine | 1.47 mg/dl | 0.72-1.25 mg/dl |
| Serum Uric Acid | 7.00 mg/dl | 3.5-7.2 mg/dl |
| C-Reactive Protein | 4.60 mg/L | 0-5.0 mg/L |
| Potassium | 4.50 mmol/L | 3.50-4.50 mmol/L |
| Sodium | 140 mmol/L | 135-145 mmol/L |
| Glomerular Filtration Rate | 51 mL/min/1.73m2 | 90-120mL/min/1.73m2 |
| Microalbuminuria | 10 mg/L | 0-10mg/L |
| Urinary Sediment Test | Negative | Negative |
Table 2.
Blood and Urine Tests – Cardiology Admission.
| Test | Result | Reference range |
| White Blood Cell Count | 8.56 10*3/uI | 4.00-10.0 10*3/uI |
| Hemoglobin | 15.6 g/dl | 12.6-17.4 g/dl |
| Platelet Count | 197 g/dl | 150-450 g/dl |
| Blood Glucose | 96 mg/dl | 82-115 mg/dl |
| Total Cholesterol | 146 mg/dl | 0-200 mg/dl |
| Triglycerides | 75 mg/dl | 0-150 mg/dl |
| High-Density Lipoprotein Cholesterol | 61 mg/dl | 40-60 mg/dl |
| Low-Density Lipoprotein Cholesterol | 70 mg/dl | 10-100 mg/dl |
| Aspartate Transaminase | 25 U/L | 5-34 U/L |
| Alanine Transaminase | 15 U/L | 0-55 U/L |
| Total Bilirubin | 0.70 mg/dl | 0.2-1.2 mg/dl |
| Serum Urea | 22.00 mg/dl | 8.4-2.57 mg/dl |
| Serum Creatinine | 1.41 mg/dl | 0.72-1.25 mg/dl |
| Serum Uric Acid | 7.00 mg/dl | 3.5-7.2 mg/dl |
| C-Reactive Protein | 2.20 mg/L | 0-5.0 mg/L |
| Glomerular Filtration Rate | 54 mL/min/1.73m2 | 90-120mL/min/1.73m2 |
| Microalbuminuria | 9 mg/L | 0-10mg/L |
| Urinary Sediment Test | Negative | Negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



