
Submitted:
01 April 2025
Posted:
02 April 2025
You are already at the latest version
Abstract
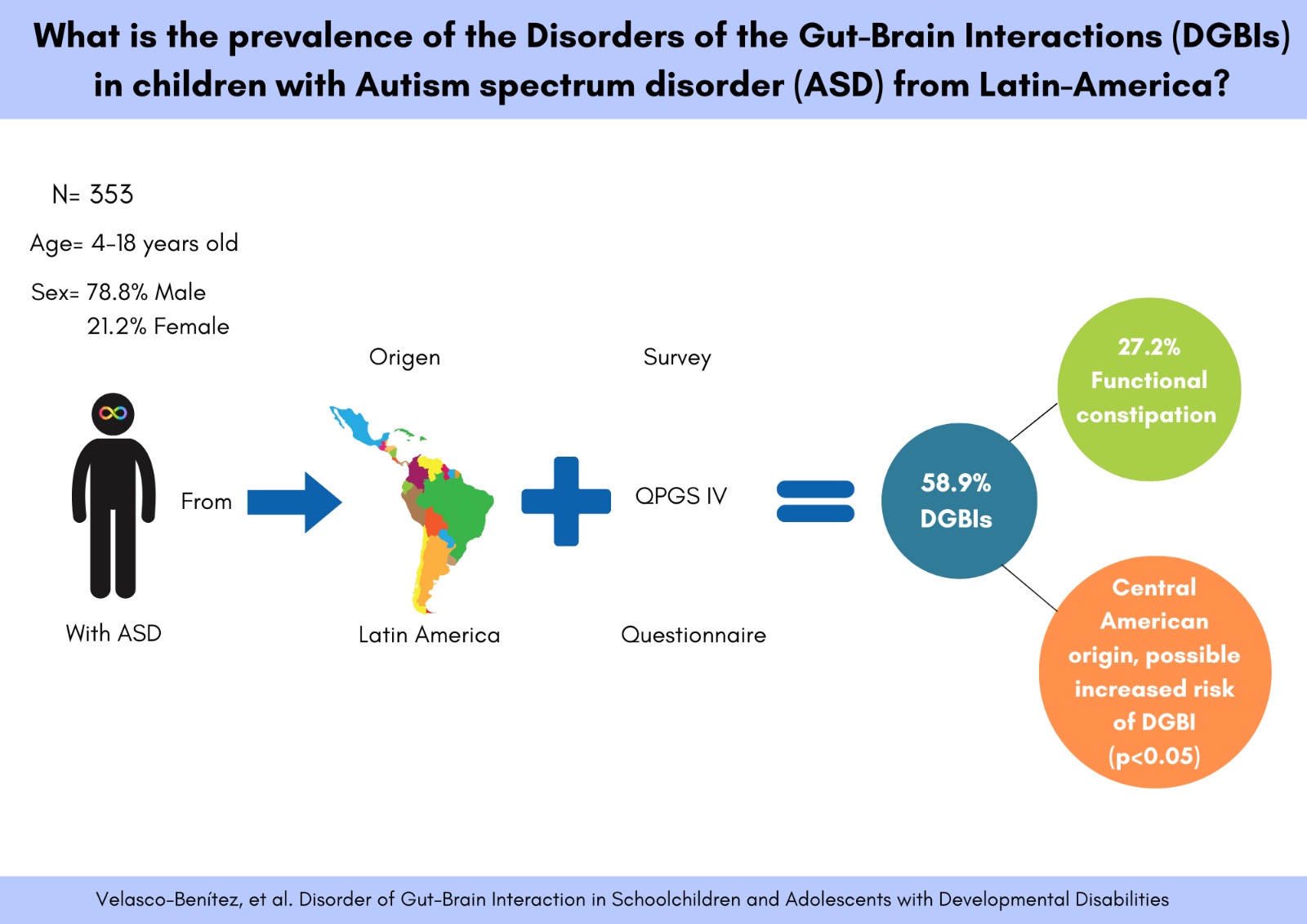
Background: Disorders of Gut-Brain-Interaction (DGBIs) are present in 22%-23% according to Rome IV. Latin American (LA) prevalence of DGBIs in children with Autism Spectrum Disorder (ASD) is unknown. The aim was to determine the prevalence of DGBIs and possible associations in schoolchildren and adolescents with ASD, from LA. Methods: observational analytical study conducted in six LA cities. Caregivers of children with ASD completed Rome IV Questionnaire for Pediatric Gastrointestinal Symptom to identify DGBIs. Sociodemographic, clinical, and family variables were included. Statistical analysis involved central tendency measures, univariate and bivariate analysis, calculation odds ratios (OR), 95% confidence intervals (95%CI), with p<0.05 significant. Results: The study included 353 children with ASD. Predominantly male (78.8%), white (56.1%), attending private schools (85.4%), normal nutritional status according BMI (58.8%) and height-for-age (85.6%), born by c-section (57.5%), firstborn (54.7%), and level 1 autism (45.0%). A total of 58.9% presented some DGBI. Functional constipation (FC) was the most frequent (27.2%). Those from Central America (CA) had higher likelihood of presenting a DGBI (OR=1.98, 95% CI=1.25–3.12, p=0.0018). Conclusions: Over a half of LA schoolchildren and adolescents with ASD presented some DGBI, with FC being the most common, and higher likelihood of DGBI for those from CA.
Keywords:
Autism Spectrum Disorder
; Disorders Gut-Brain interaction
; Functional Constipation
; Prevalence
; Latin America
; Rome IV
; Schoolchildren
; Adolescents
1. Introduction
Disorders of Gut Brain Interaction (DGBIs) are a group of functional gastrointestinal conditions that affect the interaction between the immune, endocrine, and nervous systems, causing discomfort and potentially localising at various levels of the digestive system [1]. The global prevalence of DGBIs in schoolchildren and adolescents is approximately 23.0% [2]. The diagnosis of these disorders, according to the Rome IV Criteria, is made through questionnaires focusing on the patient's symptoms [3]. On the other hand, Autism Spectrum Disorder (ASD), whose multifactorial aetiology is still not fully understood, is characterised by atypical neurological development affecting communication skills, social interaction, learning, and behaviours, which tend to be repetitive, restrictive, and selective; the last two being a barrier in terms of their food selectivity and the problems that their diet will bring [4]. The treatment for these patients should be early, interdisciplinary, individualized and adapted to the specific needs of each child and its family [5].
DGBIs have been studied in children with ASD due to the high prevalence of gastrointestinal symptoms reported in this population, which is approximately 33.0% [6]. There are several hypotheses regarding the cause of autism and its association with gastrointestinal manifestations; one of the most studied aspects of these are the DGBIs and their correlation with an imbalance in the gut microbiota, which could affect the release of proinflammatory cytokines and serotonin, factors that may help explain the behavioural manifestations observed in children diagnosed with ASD [7].
Despite the high medical comorbidity in children with ASD, there are no studies in Latin American schoolchildren and adolescents demonstrating the presence of DGBIs in these groups. This lack of knowledge represents a challenge for the accurate diagnosis and treatment of the paediatric population with ASD in the region. Therefore, the aim of this study was to determine the prevalence and possible associations of DGBIs in Central and South American schoolchildren and adolescents between 4-18 years diagnosed with ASD.
2. Materials and Methods
An observational analytical study was conducted in which caregivers of schoolchildren and adolescents aged 4 to 18 years, diagnosed with ASD, were invited to participate from capital cities in South America (SA) and Central America (CA), including Buenos Aires (Argentina), Cali (Colombia), San José (Costa Rica), San Salvador (El Salvador), Puebla (Mexico), and Panama City (Panama). All participants were diagnosed with ASD according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) [5]. This study was carried out by the Functional International Digestive Epidemiological Research Survey (FINDERS) group, consisting of paediatric gastroenterologists from the Working Group DGBI of the Latin American Society of Paediatric Gastroenterology, Hepatology, and Nutrition (LASPGHAN). The focus of the study was on DGBIs in schoolchildren and adolescents with ASD. To enhance the external validity of the results, a diverse racial, ethnic, socio-economic, and regional approach was used. This allowed for a more equitable representation of the populations from these six countries, which together account for approximately 37.0% of the total population of Latin America.
To ensure consistency and enable comparisons across multinational cross-cultural studies, the research was systematically conducted following the same methods used in previous studies by the international FINDERS consortium [8]. Additionally, the Rome Criteria were used for interviews to determine DGBIs in schoolchildren and adolescents with a diagnosis of ASD through the Questionnaire for Pediatric Gastrointestinal Symptom Rome IV (QPGS-IV), which had previously been validated by the FINDERS group in Latin American schoolchildren and adolescents [8,9]. Children with ASD included in the study were referred from paediatric gastroenterology or neurology clinics or from foundations for children with ASD in each participating country. Caregivers of schoolchildren and adolescents aged 4 to 18 years with a diagnosis of ASD were interviewed once they authorised participation in the study. The variables considered included sociodemographic (age, sex, race, origin, school), clinical (caesarean birth, prematurity, autism severity, nutritional status, comorbidities), and family related (only child, firstborn, separated or divorced parents, intra-family DGBIs, family history of autism) factors.
Regarding ethical considerations of each country, prior to providing a description of the study, its purpose, and the voluntary nature of participation, the parents or caregivers of the schoolchildren and adolescents signed an informed consent form, in which they declared their voluntary participation and adherence to the commitments previously outlined. The study was approved by the ethics committees of Argentina (Facultad de Medicina, Universidad de Buenos Aires, July 12, 2021), Colombia (Act 007-2021, Hospital Universitario del Valle “Evaristo García”, March 12, 2021), and El Salvador (CNEIS/2022/19, September 20, 2022).
Data collection was carried out through interviews conducted between March 1, 2021, and February 28, 2023. The data were entered into an electronic database using Excel, and to ensure accuracy in the transfer, 10% of the completed questionnaires were reviewed. The statistical analysis included information on the prevalence in each of the participating countries for initial analysis, along with central tendency measures. Additionally, the data were analysed using the two tailed Student's t test, chi square test, and Fisher's exact test where applicable (Stata 16 version software, College Station, Texas). To assess possible associations for DGBIs, univariate and bivariate analyses were performed, with the calculation of Odds Ratios (OR) and their respective 95% Confidence Intervals (95% CI) for each exposure variable of interest (sociodemographic, clinical, and family related variables) and the outcome variable (presence or absence of DGBIs). A p-value <0.05 was considered statistically significant. The present study assesses the internal consistency and validation of the QPGS-IV in caregivers of schoolchildren and adolescents diagnosed with ASD using Cronbach's alpha (interpretation of Cronbach's alpha values: very high= 0.91-1.00, high= 0.61-0.80, moderate= 0.41-0.60, low= 0.21-0.40 and very low= 0.01-0.20) [10] [11].
3. Results
Four hundred and twenty-one parents or, in some cases, caregivers of schoolchildren and adolescents aged 4 to 18 years (mean age 9.0 ± 3.7 years) with a diagnosis of ASD were invited to participate in this study. Participants were recruited from various Latin American medical centres, foundations and hospitals during outpatient appointments. It should be noted that all parents and caregivers had previously consented to participate in the study.
Ten parents or caregivers did not want to participate. Data from respondents with inconsistent answers (n=20) and children under 4 years of age (n=10) were excluded. After the exclusions, N=353 participants were analysed, of which 290 (82.2%) were schoolchildren (aged 4 to 12 years old) and 63 (17.8%) were adolescents (aged 13 to 18 years old). The population was divided into two age groups: 4-10 years old (n=242, 68.6%) and 11-13 years old (n=111, 31.4%) (Figure 1).
Regarding sociodemographic variables, it was found that 78.8% of the participants were male, with a male to female ratio of 1:3.7. The majority of participants were of white ethnicity (56.1%) followed by mixed race (40.8%). In terms of education, 85.4% of the children attended private educational institutions. Geographically, CA contributed 58.1% of the total population, mainly from Panama (15.9%), while SA contributed 41.9%, primarily from Argentina (23.2%) (Table 1).
Among the clinical variables, 57.5% of the participants were born by caesarean section, 17.3% were preterm, and 45.0% had level 1 of autism. Regarding height-for-age, 85.6% were classified as eutrophic, and 58.8% had a normal weight according to the Body Mass Index (BMI) according to the World Health Organization. Additionally, 24.1% of the children had some comorbidity. Finally, in the family environment, 32.6% were only children, 54.7% were firstborn, and 26.1% had separated or divorced parents. A small percentage of children, 4.0%, had a family history of any DGBI, while 5.1% had a family history of autism (Table 2).
3.1. Prevalence
Among the 353 schoolchildren and adolescents with ASD assessed using the Rome IV Criteria, more than half (58.9%) met the criteria for at least one DGBI. The most frequent DGBI was functional constipation (FC) (27.2%), followed by functional dyspepsia (FD) (21.8%), unspecified abdominal pain (4.5%) and disorders associated with nausea and vomiting (2.9%) (Table 3).
3.2. Possible Associations
A possible association was found between the factors assessed and geographical location. Specifically, schoolchildren and adolescents with ASD from CA were more likely to have some DGBIs (OR = 1.98, 95% CI = 1.25-3.12, p = 0.0018) compared to those from SA. Within SA, Mexico also showed a significant association (OR = 1.95, 95% CI = 0.98-4.09, p = 0.0425). However, no significant differences were observed when analysing other sociodemographic, clinical and family variables (p > 0.05) (Table 4).
3.3. Validation and Internal Consistency of the QPGS IV in Spanish for ASD.
Validation and internal consistency analysis of the questionnaire, designed for parents and caregivers of schoolchildren and adolescents with ASD, showed a Cronbach's Alpha of 0.7818 (high). When analyzed the QPGS IV by section, interpretations ranged from moderate to high (Table 5).
3.4. Main Digestive Symptoms Identified
When evaluating the main digestive symptoms according to the Rome IV questionnaire, it was found that most children presented flatus (50.4%), followed by painful stools (35.7%), large stools (30.6%), history of large fecal mass in rectum (26.6%) and hard stools (23.8%) (Table 6).
4. Discussion
In the present study, we aimed to determine the prevalence of DGBIs in adolescents with ASD from Central and South America. Due to the inherent limitations in administering the questionnaires to the target population, it was the parents or guardians who completed the QPGS-IV, which demonstrated high validity and reliability (Cronbach’s alpha of 0.7818 ) (Table 5). This questionnaire, is considered the gold standard for diagnosing DGBIs in children and adults, despite being viewed as subjective [3], has adequate construct validity [9], a sensitivity of 75% (95% CI = 59.0-79.0), and a specificity of 90% (95% CI = 83.0-98.0) [8], and it is recommended that it be guided to improve internal reliability [12].
We found that Latin American schoolchildren and adolescents diagnosed with ASD had a prevalence of 58.9% for presenting some type of DGBI according to the Rome IV Criteria. This figure is higher than those reported in similar age groups of children without ASD: A systematic review of European, North American and Latin American children between the ages of 4 and 18, analyzed according to Rome IV criteria, found that the global prevalence of DGBI was 23.0%. (95% CI = 21.0-25.0%, I² = 99%) [2], in a cross sectional study made in Colombia, the prevalence of these disorders was 21.2% [13], 22.3% in Ecuador [13], 25.0% in the United States [14], 31.2% in Bosnia and Herzegovina [15], and between 26.2%-26.4% in Italy [16]. Some authors had compared the prevalence of these disorders according to the Rome III Criteria and the prevalence ranged from 13.4% to 29.9% (higher compared to Rome IV prevalence) in Latin American countries such as Mexico, Colombia, El Salvador, Ecuador, and Panama [13].
Our prevalence of DGBIs is lower than that reported by Gülpınar, et al. [17], who, in a case-control study conducted with Turkish children aged 4 to 10 years old, found a prevalence of 76.5% in children with ASD using the Rome III Questionnaire. Even when made a subanalysis to compared with our Latin American children of the same age (76.5% versus 59.1%, p = 0.006), the difference is notable and could be due to the questionnaire they applied or to cultural factors that may influence the prevalence of these DGBIs, such as eating habits.
In the present study and according to Rome IV, the most prevalent DGBI in Latin American schoolchildren and adolescents with ASD was FC, which occurred in 27.2%. This was higher than reported in neurotypical children of the same age according to Rome IV in European countries, Latin American, and the United States of America [2,13,14,15,16], and according to Rome III for Latin American countries [13], but lower than the figures found in Bosnia and Herzegovina [15] according to Rome IV, and those identified by Gülpınar, et al. [17], who found 38.2% in Turkish children with ASD [17].
Our second most prevalent DGBI was FD with 21.9%, higher than those reported according to Rome IV in healthy children without ASD [2,13,15,16] and with ASD [17], as well as according to Rome III Criteria in healthy Latin American children without ASD [13]. These differences could be explained by the hypothesis of a bidirectional interaction between the central nervous system and the digestive tract [18], as well as methodologically, by the type of questionnaire and its interpretation, the coexistence of DGBIs, the sample size or regional, cultural, nutritional and lifestyle differences, among others.
In future research, it would be beneficial to investigate the potential causes of the high prevalence of FC in children with ASD. These causes may include, but are not limited to, the child's diet and lifestyle. Furthermore, it may be advantageous to propose new non-invasive and cost-effective therapies that have demonstrated encouraging results in children with FC, such as transcutaneous tibial nerve stimulation [19,20] or novel drugs such as Linaclotide [21,22,23].
Regarding a drug treartment for the most prevalent DGBI, a 3-phase study proved that Linaclotide is safe and effective in treating FC. It evaluated multiple doses and response in patients aged between 6 and 17 years old. It also evaluated the dose and response in patients aged between 2 and 5 years old. And concluded with a double-blind, placebo-controlled, multicentre trial in children aged 6 to 17 years [21,22,23]. Subsequent to these findings, the drug has been approved by the Food and Drugs Administration in the United States of America, as a treatment for children suffering from FC, and the only adverse effect found was moderate to mild diarrhea in some of the patients [21,22,23].
The only possible association that we found in this group of Latin American schoolchildren and adolescents with ASD was the relevance of the geographical region they came from, as there was a higher prevalence of DGBIs in Central America (OR = 1.98, 95% CI = 1.25–3.12, p = 0.0018), specifically in Mexico, and a lower prevalence in SA, particularly in Colombia. Several hypotheses could explain this, including nutritional, psycho-affective factors, and the role of the microbiota. From a nutritional standpoint, we did not find differences in their nutritional status, even in the most prevalent DGBI, FC. However, it is worth noting that nearly one-third of the children with both FC and ASD (26.0%) were overweight or obese. Regarding what we previously mentioned, there is a theory that neurotypical children, no matter their sex, who are overweight or obese may experience FC, and the risk of obesity is higher in children with FC; those risk were observed specially in developed countries (95% CI = 1.49–3.46; p = 0.000), but not in developing countries [24]; however, these results have not been confirmed in Colombian children without ASD with certain DGBI, such as FC [25].
Despite the absence of any possible psycho-affective associations in these Latin American schoolchildren and adolescents with ASD and DGBI, there was a higher percentage of divorced or separated parents in Latin American adolescents with ASD compared to schoolchildren (38.7% vs. 20.2%, p = 0.000). This finding may be indicative of the psychosocial and familial strain involved in raising children with ASD in a society that is poorly adapted to the needs of this population. In correlation with our findings, one study showed that parents of children with ASD had lower scores than parents of neurotypical children on the WHOQOL-BREF quality of life scale and the QOL [26,27].
In future research, it would be beneficial to design and conduct a study that assesses family quality of life in the Latin American population. This study should be conducted before and after the diagnosis of the child with ASD, as well as following the diagnosis and interventions for both the family and the child.
Research related to alterations in the microbiota and behaviour in patients with ASD commenced reporting in 2015 [28], following the case report of a young individual from the United States of America, who exhibited behavioural improvements regarding social interaction, such as eye contact, speech improvement, and motricity, after undergoing common antibiotic treatment [28]. Subsequent studies have demonstrated significant disparities in the microbiota of children with ASD in comparison to those with typical development [29,30], and the prospective therapeutic benefits of pre- and probiotics [31,32], as well as faecal transplants [33,34], meticulously tailored to the individual requirements of each patient [29]. All of these points to the importance of advancing future research to uncover potential risk factors.
In these Latin American schoolchildren and adolescents with ASD, between 4.5% and 50.4% presented one or more symptoms based on the Rome IV Pediatric Digestive Symptom Questionnaire (Table 6). Children with ASD are 2 [35] to 4 times [36] more likely to present digestive symptoms, as well as multiple digestive symptoms (30.6% versus 5.4%, p < 0.05) [37], compared to children without ASD, which impacts both their quality of life and that of their families [38]. As a result, non-verbal scales have been proposed to identify digestive symptoms and assess their psychometric characteristics, for both research and clinical purposes [39]. Many of the digestive symptoms in patients with ASD are linked to their stereotyped behaviours, with a marked food selectivity and a strong preference for carbohydrates and specific foods [40]. In a case control study comparing typically developing children and children with ASD, gastrointestinal symptoms were associated, in both groups, with an increase in self-injurious behaviour, restricted stereotyped behaviour, aggressive behaviour, sleep problems, attention problems, somatic complaints and an increase in parasomnias [37]. Children with ASD and gastrointestinal symptoms were also more likely to experienced the problems listed above, than children with ASD but without gastrointestinal symptoms [37].
We consider the strengths of our study to be the diversification of the population, which represents approximately 37.0% of the total population of Latin America. Upon calculating Cronbach’s Alpha for the questionnaire completed by the parents or caregivers of children with ASD, we concluded that this method of administering the questionnaire to third parties was valid and reliable (Cronbach’s Alpha = 0.7818). We acknowledge that one area for improvement is the need to expand the sample size in certain countries. Additionally, we cannot rule out that the results obtained may not be fully generalisable to all of Latin America. As this is the first Latin American study to evaluate the prevalence of DGBIs in children with ASD, the lack of previous similar research makes it difficult to compare our findings. We propose, in the future, to conduct a case-control study at the Latin American level to more accurately identify the risk factors affecting the school-aged and adolescent population with ASD.
5. Conclusions
In conclusion, through this study and in comparison with literature reviews of studies conducted on Latin American children and those from other continents, the hypothesis can be confirmed that there is a higher prevalence of DGBIs in children with ASD compared to those with neurotypical development. In this group of Latin American schoolchildren and adolescents with ASD, regardless of their level of autism, 6 out of every 10 children present some form of DGBI, with FC being the most frequent. Additionally, children from CA have a higher likelihood of presenting any DGBI.
Author Contributions
Conceptualization, CAV, CAR, CJO, DAV, CZ, JF, RB, AZ, RC, CG, FAR and RZ; Methodology, CAV, CAR, CJO, DAV, CZ, JF, RB, AZ, RC, CG, FAR and RZ; Software, CAV and DAV; Validation, CAV and DAV; Formal analysis, CAV and DAV; Investigation, CAV, CAR, CJO, DAV, CZ, JF, RB, AZ, RC, CG, FAR and RZ; Resources, CAV, CAR, DAV, CZ, JF, RB, AZ, RC, CG, FAR and RZ; Data curation, CAV, DAV and MCJ; Writing—original draft preparation, CAV, DAV and MCJ; writing—review and editing, CAV, CAR, CJO, DAV, MCJ, CZ, JF, RB, AZ, RC, CG, FAR and RZ; Visualization, CAV and DAV; Supervision, CAV, DAV and MCJ; Project administration, CAV and DAV. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Hospital Universitario del Valle “Evaristo Garcia” in Cali, Colombia (Act 007-2021.12th March 2021), by Argentina (Facultad de Medicina, Universidad de Buenos Aires, 12th July 2021), and El Salvador (CNEIS/2022/19th September 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Acknowledgments
No support of any kind, including administrative, technical, or in-kind donations, was received for the completion of this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DGBIs | Disorders Gut-Brain Interaction |
| ASD | Autism Spectrum Disorder |
| SA | South America |
| CA | Central America |
| OR | Odds Ratio |
| BMI | Body Mass Index |
| FC | Functional Constipation |
| QPGS IV | Questionnaire for Pediatric Gastrointestinal Symptoms Rome IV |
| FINDERS | Functional International Digestive Epidemiological Research Survey |
| DSM-V | Diagnostic Statistical Manual of Mental Disorders |
| LASPGHAN | Latin America Society of Paediatric Gastroenterology Hepatology and Nutrition |
| FD | Functional Dyspepsia |
| FAP | Functional Abdominal Pain |
References
- Kasarello, K.; Cudnoch-Jedrzejewska, A.; Czarzasta, K. Communication of gut microbiota and brain via immune and neuroendocrine signaling. Front Microbiol 2023, 14, 1118529. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Benítez, C.A.; Collazos-Saa, L.I.; García-Perdomo, H.A. A systematic review and meta-analysis in schoolchildren and adolescents with functional gastrointestinal disorders according to Rome IV criteria. Arq Gastroenterol 2022, 59, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.A. Functional gastrointestinal disorders: History, pathophysiology, clinical features and Rome IV. Gastroenterology 2016, 150, S0016-5085, 00223-7. [Google Scholar] [CrossRef]
- Dargenio, V.N.; Dargenio, C.; Castellaneta, S.; De Giacomo, A.; Laguardia, M.; Schettini, F.; Francavilla, R.; Cristofori, F. Intestinal barrier dysfunction and microbiota-gut-brain axis: Possible implications in the pathogenesis and treatment of autism spectrum disorder. Nutrients 2023, 15, 1620. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed.; American Psychiatric Publishing: Washington 2014, United States of America.
- Lasheras, I.; Real-López, M.; Santabárbara, J. Prevalence of gastrointestinal symptoms in autism spectrum disorder: A meta-analysis. An Pediatr (Engl Ed) 2023, 99, 102–110. [Google Scholar] [CrossRef]
- Morton, J.T.; Jin, D.-M.; Mills, R.H.; Shao, Y.; Rahman, G.; McDonald, D.; Zhu, Q.; Balaban, M.; Jiang, Y.; Cantrell, K.; et al. Multi-level analysis of the gut-brain axis shows autism spectrum disorder-associated molecular and microbial profiles. Nat Neurosci 2023, 26, 1208–1217. [Google Scholar] [CrossRef]
- Velasco-Benítez, C.A.; Ortíz-Rivera, C.J.; Sánchez-Pérez, M.P.; Játiva-Mariño, E.; Villamarín-Betancourt, E.A.; Saps, M. Utilidad de los cuestionarios de Roma IV en español para identificar desórdenes gastrointestinales funcionales en pediatría. Grupo de trabajo de la Sociedad Latinoamericana de Gastroenterología, Hepatología y Nutrición Pediátrica (SLAGHNP). Acta Gastroenterológica Latinoamericana 2019, 49, 259–296. [Google Scholar]
- Saps, M.; Nichols-Vinueza, D.X.; Mintjens, S.; Pusatcioglu, C.K.; Velasco-Benítez, C.A. Construct validity of the pediatric Rome III criteria. J Pediatr Gastroenterol Nutr 2014, 59, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.M. Research Design and Methods; Elsevier Inc.: Pennsylvania State University, University Park, PA, USA, 2007; pp. 419–429. [Google Scholar]
- Barbosa, E.Y. A neurodidactic model for teaching elementary EFL students in a college context. English Lang. Teach. 2021, 14, 42. [Google Scholar] [CrossRef]
- Baaleman, D.F.; Velasco-Benítez, C.A.; Méndez-Guzmán, L.M.; Benninga, M.A.; Saps, M. Can we rely on the Rome IV questionnaire to diagnose children with functional gastrointestinal disorders? J Neurogastroenterol Motil 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Velasco-Benítez, C. Trastornos Digestivos Funcionales En Pediatría, 1st ed.; Grupo Distribuna: Bogota, Colombia, 2022; pp. 4–5. [Google Scholar]
- Robin, S.G.; Keller, C.; Zwiener, R.; Hyman, P.E.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Shulman, R.J.; Hyams, J.S.; Palsson, O.; et al. Prevalence of pediatric functional gastrointestinal disorders utilizing the Rome IV criteria. J Pediatr 2018, 195, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Selimović, A.; Mekić, N.; Terzić, S.; Ćosićkić, A.; Zulić, E.; Mehmedović, M. Functional gastrointestinal disorders in children: A single centre experience. Med Glas (Zenica) 2024, 21, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Cenni, S.; Pensabene, L.; Dolce, P.; Campanozzi, A.; Salvatore, S.; Pujia, R.; Serra, M.R.; Scarpato, E.; Miele, E.; Staiano, A.; et al. Prevalence of functional gastrointestinal disorders in Italian children living in different regions: Analysis of the difference and the role of diet. Dig Liver Dis 2023, 55, 1640–1646. [Google Scholar] [CrossRef]
- Aydın, Ö.G.; Baykara, H.B.; Akın, K.; Kahveci, S.; Şeker, G.; Güler, Y.; Öztürk, Y. Evaluation of functional gastrointestinal disorders in children aged 4-10 years with autism spectrum disorder. Turk J Pediatr 2024, 66, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Saurman, V.; Margolis, K.G.; Luna, R.A. Autism spectrum disorder as a brain-gut-microbiome axis disorder. Dig Dis Sci 2020, 65, 818–828. [Google Scholar] [CrossRef]
- Rego, R.M.P.; Machado, N.C.; Carvalho, M.A.; Graffunder, J.S.; Ortolan, E.V.P.; Lourenção, P.L.T.A. Transcutaneous posterior tibial nerve stimulation in children and adolescents with functional constipation: A protocol for an interventional study. Medicine 2019, 98, e17755. [Google Scholar] [CrossRef]
- Yu, A.T.; Song, J.M.; Qiao, L.; Wang, Y.; Chen, Y.; Weng, E.H.; et al. A randomized, double-blind, controlled trial of percutaneous tibial nerve stimulation with pelvic floor exercises in the treatment of childhood constipation. Am J Gastroenterol 2023, 118, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, C.; Nurko, S.; Hyams, J.S.; Rodriguez-Araujo, G.; Almansa, C.; Shakhnovich, V.; Saps, M.; Simon, M. Randomized controlled trial of linaclotide in children aged 6-17 years with functional constipation. J. Pediatr. Gastroenterol. Nutr. 2024, 78, 1059–1068. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Robert, J.; Rodriguez-Araujo, G.; Shakhnovich, V.; Xie, W.; Nurko, S.; Saps, M. Safety and efficacy of linaclotide in children aged 2-5 years with functional constipation: Phase 2, randomized study. J. Pediatr. Gastroenterol. Nutr. 2024, 79, 510–518. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Khlevner, J.; Rodriguez-Araujo, G.; Xie, W.; Huh, S.Y.; Ando, M.; Hyams, J.S.; Nurko, S.; Benninga, M.A.; Simon, M.; et al. Efficacy and safety of linaclotide in treating functional constipation in paediatric patients: a randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. Lancet Gastroenterol Hepatol 2024, 9, 238–250. [Google Scholar] [CrossRef]
- Wang, G.N.; Zhang, K.; Xiong, Y.Y.; Liu, S. The relationship between functional constipation and overweight/obesity in children: a systematic review and meta-analysis. Pediatr Res 2023, 94, 1878–1886. [Google Scholar] [CrossRef] [PubMed]
- Koppen, I.J.N.; Velasco-Benítez, C.A.; Benninga, M.A.; Di Lorenzo, C.; Saps, M. Is there an association between functional constipation and excessive bodyweight in children? J. Pediatr. 2016, 171, 178–182.e1. [Google Scholar] [CrossRef]
- Raju, S.; Hepsibah, P.E.V.; Niharika, M.K. Quality of life in parents of children with Autism spectrum disorder: Emphasizing challenges in the Indian context. Int. J. Dev. Disabil. 2023, 69, 371–378. [Google Scholar] [CrossRef]
- Musetti, A.; Manari, T.; Dioni, B.; Raffin, C.; Bravo, G.; Mariani, R.; Esposito, G.; Dimitriou, D.; Plazzi, G.; Franceschini, C.; et al. Parental Quality of Life and Involvement in Intervention for Children or Adolescents with Autism Spectrum Disorders: A Systematic Review. J. Pers. Med. 2021, 11, 894. [Google Scholar] [CrossRef] [PubMed]
- Rodakis, J. An n=1 case report of a child with autism improving on antibiotics and a father's quest to understand what it may mean. Microb Ecol Health Dis 2015, 26, 26382. [Google Scholar] [CrossRef]
- Iglesias-Vázquez, L.; Van Ginkel Riba, G.; Arija, V.; Canals, J. Composition of gut microbiota in children with autism spectrum disorder: A systematic review and meta-analysis. Nutrients 2020, 12, 792. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.; Zhang, Q.; Sun, J.; Li, Q.; Li, D.; Zhu, M.; Fu, X.; Zhao, L.; Wang, M.; Lou, X.; et al. A comparison between children and adolescents with autism spectrum disorders and healthy controls in biomedical factors, trace elements, and microbiota biomarkers: A meta-analysis. Front Psychiatry 2024, 14, 1318637. [Google Scholar] [CrossRef]
- Sanctuary, M.R.; Kain, J.N.; Chen, S.Y.; Kalanetra, K.; Lemay, D.G.; Rose, D.R.; Yang, H.T.; Tancredi, D.J.; German, J.B.; Slupsky, C.M.; et al. Pilot study of probiotic/colostrum supplementation on gut function in children with autism and gastrointestinal symptoms. PLoS One 2019, 14, e0210064. [Google Scholar] [CrossRef]
- Patusco, R.; Ziegler, J. Role of probiotics in managing gastrointestinal dysfunction in children with autism spectrum disorder: An update for practitioners. Adv Nutr 2018, 9, 637–650. [Google Scholar] [CrossRef]
- Dossaji, Z.; Khattak, A.; Tun, K.M.; Hsu, M.; Batra, K.; Hong, A.S. Efficacy of fecal microbiota transplant on behavioral and gastrointestinal symptoms in pediatric autism: A systematic review. Microorganisms 2023, 11, 806. [Google Scholar] [CrossRef]
- Yu, Y.; Wang, W.; Zhang, F. The next generation fecal microbiota transplantation: To transplant bacteria or virome. Adv Sci (Weinh) 2023, 10, e2301097. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.Y.C.; Leung, P.W.L.; Hung, S.F.; Shea, C.K.S.; Mo, F.; Che, K.K.I.; Tse, C.Y.; Lau, F.L.F.; Ma, S.L.; Wu, J.C.Y.; et al. Gastrointestinal problems in Chinese children with autism spectrum disorder. Neuropsychiatr Dis Treat 2020, 16, 1807–1815. [Google Scholar] [CrossRef]
- Gan, H.; Su, Y.; Zhang, L.; Huang, G.; Lai, C.; Lv, Y.; Li, Y. Questionnaire-based analysis of autism spectrum disorders and gastrointestinal symptoms in children and adolescents: A systematic review and meta-analysis. Front Pediatr 2023, 11, 1120728. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, B.; Angkustsiri, K.; Taylor, S.L.; Rogers, S.J.; Cabral, J.; Heath, B.; Hechtman, A.; Solomon, M.; Ashwood, P.; Amaral, D.G.; et al. Developmental-behavioral profiles in children with autism spectrum disorder and co-occurring gastrointestinal symptoms. Autism Res. 2020, 1, 1778–1789. [Google Scholar] [CrossRef]
- Holingue, C.; Poku, O.; Pfeiffer, D.; Murray, S.; Fallin, M.D. Gastrointestinal concerns in children with autism spectrum disorder: A qualitative study of family experiences. Autism 2022, 26, 1698–1711. [Google Scholar] [CrossRef] [PubMed]
- Holingue, C.; Kalb, L.G.; Musci, R.; Lukens, C.; Lee, L.-C.; Kaczaniuk, J.; Landrum, M.; Buie, T.; Fallin, M.D. Characteristics of the autism spectrum disorder gastrointestinal and related behaviors inventory in children. Autism Res 2022, 15, 1142–1155. [Google Scholar] [CrossRef]
- Bandini, L.G.; Curtin, C.; Phillips, S.; Anderson, S.E.; Maslin, M.; Must, A. Changes in food selectivity in children with autism spectrum disorder. J Autism Dev Disord 2017, 47, 439–446. [Google Scholar] [CrossRef]
Figure 1.
Population flowchart of the study.
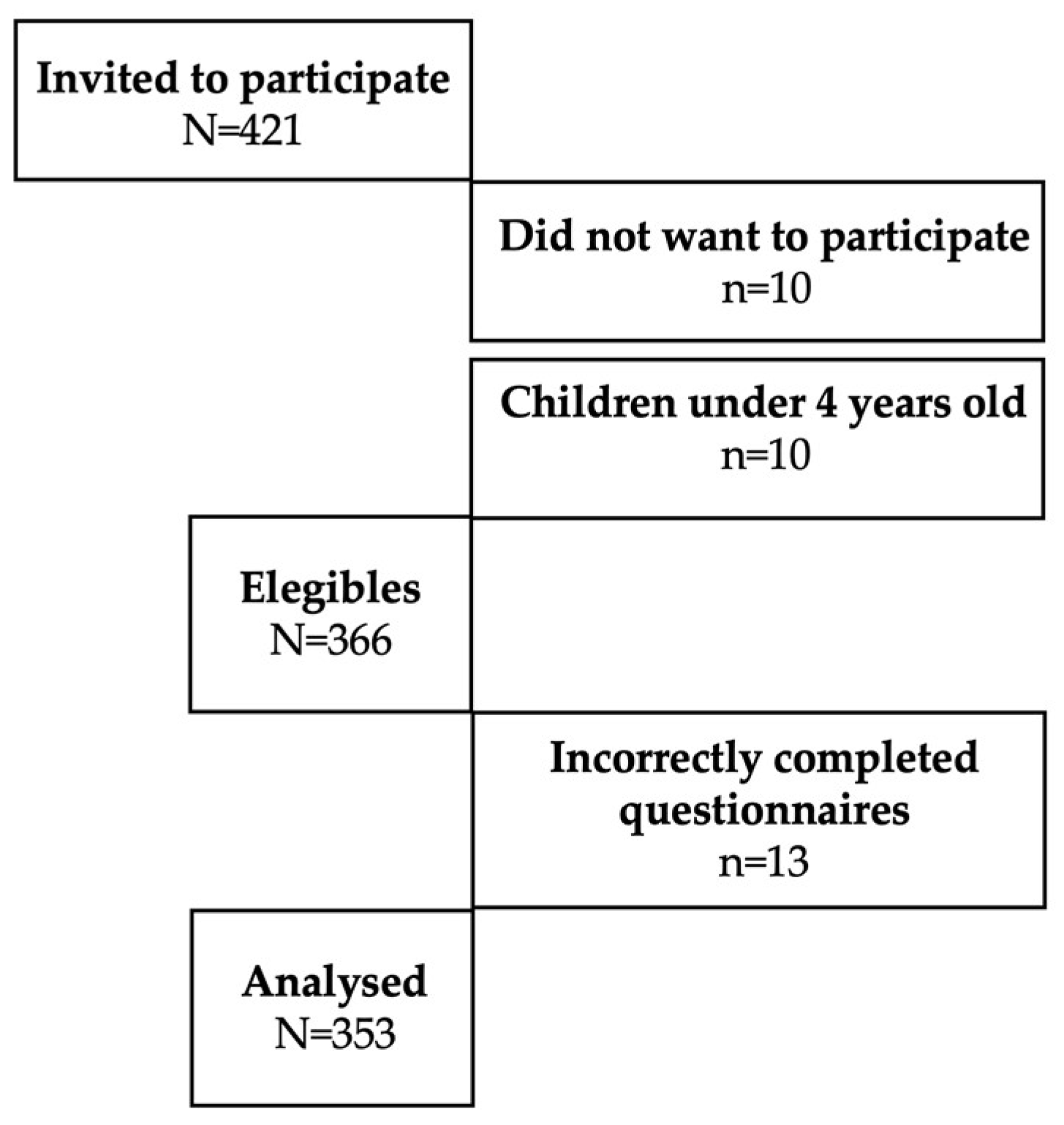

Table 1.
Demographics.
|
All (N=353) |
4-10 Years old (n=242) |
11-18 Years old (n=111) |
|
| Sociodemographic variables | |||
| Age (years) | |||
| Mean SD | 9.0+/-3.7 | 6.8+/-1.8 | 13.7+/-2.4 |
| Range | 4-18 | 4-10 | 11-18 |
| Age groups (years) | |||
| Schoolchildren (8-12) | 290 (82.2) | 242 (100.0) | 48 (43.2) |
| Adolescents (13-18) | 63 (17.8) | 0 (0.0) | 63 (56.8) |
| Sex | |||
| Female | 75 (21.3) | 47 (19.4) | 28 (25.2) |
| Male | 278 (78.8) | 195 (80.6) | 83 (74.8) |
| Race | |||
| White | 198 (56.1) | 132 (54.5) | 66 (59.5) |
| Mixed | 144 (40.8) | 100 (41.3) | 44 (39.6) |
| Afro-descendant | 7 (2.0) | 7 (2.9) | 0 (0.0) |
| Indigenous | 4 (1.1) | 3 (1.2) | 1 (0.9) |
| Country | |||
| South America | 148 (41.9) | 102 (42.1) | 46 (41.4) |
| Argentina | 82 (23.2) | 61 (25.2) | 21 (18.9) |
| Colombia | 66 (18.7) | 41 (16.9) | 25 (22.5) |
| Central America | 205 (58.1) | 140 (57.9) | 65 (58.6) |
| Costa Rica | 52 (14.7) | 33 (13.6) | 19 (17.1) |
| El Salvador | 47 (13.3) | 39 (16.1) | 8 (7.2) |
| Mexico | 50 (14.2) | 30 (12.4) | 20 (18.0) |
| Panama | 56 (15.9) | 38 (15.7) | 18 (16.2) |
| School (n=328) | (n=328) | (n=223) | (n=105) |
| Public | 48 (14.6) | 31 (13.9) | 17 (16.2) |
| Private | 280 (85.4) | 192 (86.1) | 88 (83.8) |
*SD=Standard Deviation.
Table 2.
Clinical and family variables.
|
All (N=353) |
4-10 Years old (n=242) |
11-18 Years old (n=111) |
p | |
| Clinical variables | ||||
| Caesarean section | ||||
| No | 150 (42.5) | 98 (40.5) | 52 (46.9) | 0.158 |
| Yes | 203 (57.5) | 144 (59.5) | 59 (53.1) | |
| Prematurity | ||||
| No | 292 (82.7) | 202 (83.5) | 90 (81.1) | 0.341 |
| Yes | 61 (17.3) | 40 (16.5) | 21 (18.9) | |
| Level of autism | ||||
| Level I | (n=180) | (n=122) | (n=58) | |
| No | 99 (55.0) | 67 (54.9) | 32 (55.2) | 0.552 |
| Yes | 81 (45.0) | 55 (45.1) | 26 (44.8) | |
| Level II | (n=180) | (n=122) | (n=58) | |
| No | 110 (61.1) | 74 (60.7) | 36 (62.1) | 0.494 |
| Yes | 70 (38.9) | 48 (39.3) | 22 (37.9) | |
| Level III | (n=180) | (n=122) | (n=58) | |
| No | 151 (83.9) | 103 (84.4) | 48 (82.8) | 0.466 |
| Yes | 29 (16.1) | 19 (15.6) | 10 (17.2) | |
| Nutritional status | ||||
| According to Body Mass Index | ||||
|
Normal |
(n=318) 187 (58.8) |
(n=228) 135 (59.2) |
(n=90) 52 (57.8) |
0.456 |
| Malnutrition | 131 (41.2) | 93 (40.8) | 38 (57.8) | |
| According to Height for age | ||||
|
Normal |
(n=320) 274 (85.6) |
(n=228) 196 (86.0) |
(n=92) 78 (84.8) |
0.469 |
| Height altered | 46 (14.4) | 32 (14.0) | 14 (15.2) | |
| Comorbidity | ||||
| No | 268 (75.9) | 188 (77.7) | 80 (72.1) | 0.156 |
| Yes | 85 (24.1) | 54 (22.3) | 31 (27.9) | |
| Family variables | ||||
| Only child | ||||
| No | 238 (67.4) | 158 (65.3) | 80 (72.1) | 0.127 |
| Yes | 115 (32.6) | 84 (34.7) | 31 (27.9) | |
| Firstborn | ||||
| No | 160 (45.3) | 113 (46.7) | 47 (42.3) | 0.259 |
| Yes | 193 (54.7) | 129 (53.3) | 64 (57.7) | |
| Separated/divorced parents | ||||
| No | 261 (73.9) | 193 (79.8) | 68 (61.3) |
0.000 |
| Yes | 92 (26.1) | 49 (20.2) | 43 (38.7) | |
| DGBIs intra-family | ||||
| No | 339 (96.0) | 232 (95.9) | 107 (96.4) | 0.536 |
| Yes | 14 (4.0) | 10 (4.1) | 4 (3.6) | |
| Autism in the family | ||||
| No | 335 (94.9) | 230 (95.0) | 105 (94.6) | 0.521 |
| Yes | 18 (5.1) | 12 (5.0) | 6 (5.4) | |
*DGBIs=Disorders Gut Brain Interaction.
Table 3.
Prevalence of DGBIs.
|
All (N=353) |
4-10 Years old (n=242) |
11-18 Years old (n=111) |
|
| DGBIs | |||
| No | 145 (41.1) | 99 (40.9) | 46 (41.4) |
| Yes | 208 (58.9) | 143 (59.1) | 65 (58.6) |
| Associated with nausea and vomiting | 10 (2.9) | 6 (2.4) | 4 (3.6) |
| Functional vomiting | 6 (1.7) | 2 (0.8) | 4 (3.6) |
| Cyclic vomiting | 1 (0.3) | 1 (0.4) | 0 (0.0) |
| Rumination | 2 (0.6) | 2 (0.8) | 0 (0.0) |
| Aerophagia | 1 (0.3) | 1 (0.4) | 0 (0.0) |
| Associated with abdominal pain | 100 (28.3) | 69 (28.5) | 31 (27.9) |
| Functional dyspepsia | 77 (21.8) | 55 (22.7) | 22 (19.8) |
| Postprandial | 74 (21.0) | 53 (21.9) | 21 (18.9) |
| Epigastric | 2 (0.6) | 1 (0.4) | 1 (0.9) |
| Irritable bowel syndrome | 5 (1.4) | 5 (2.1) | 0 (0.0) |
| IBS with diarrhea | 1 (0.3) | 1 (0.4) | 0 (0.0) |
| IBS with constipation | 4 (1.1) | 4 (1.7) | 0 (0.0) |
| Abdominal migraine | 2 (0.6) | 1 (0.4) | 1 (0.9) |
| Functional abdominal pain not otherwise specified | 16 (4.5) | 8 (3.3) | 8 (7.2) |
| Associated with defecation | 98 (27.8) | 68 (28.1) | 30 (27.0) |
| Functional constipation | 96 (27.2) | 67 (27.7) | 29 (26.1) |
| Non-retentive faecal incontinence | 2 (0.6) | 1 (0.4) | 1 (0.9) |
*DGBIs=Disorders Gut-Brain Interaction; IBS=Irritable bowel syndrome.
Table 4.
Possible associations with DGBIs.
| DGBIs |
OR |
95% CI |
p |
DGBIs |
OR |
95% CI |
p |
||||
| No | Yes | No | Yes | ||||||||
| Sociodemographic variables | Clinical variables | ||||||||||
| Age groups | Caesarean section | ||||||||||
| Schoolchildren | 120 (82.8) | 170 (81.7) | 1.00 |
0.8040 |
No | 58 (40.0) | 92 (44.2) | 1.00 |
0.4289 |
||
| Adolescents | 25 (17.2) | 38 (18.3) | 1.07 | 0.59-1.95 | Yes | 87 (60.0) | 116 (55.8) | 0.84 | 0.53-1.32 | ||
| Sex | Prematurity | ||||||||||
| Female | 31 (21.4) | 44 (21.2) | 1.00 |
0.9594 |
No | 118 (81.4) | 174 (83.7) | 1.00 |
0.5782 |
||
| Male | 114 (78.6) | 164 (78.8) | 1.01 | 0.58-1.75 | Yes | 27 (18.6) | 34 (16.4) | 0.85 | 0.47-1.55 | ||
| Race | Level of autism (n=180) | ||||||||||
| White | Level I | (n=65) | (n=115) | ||||||||
| No | 64 (44.1) | 91 (43.8) | 1.00 |
0.9424 |
No | 37 (56.9) | 62 (53.9) | 1.00 |
0.6966 |
||
| Yes | 81 (55.9) | 117 (56.2) | 1.01 | 0.64-1.59 | Yes | 28 (43.1) | 53 (46.1) | 1.12 | 0.58-2.18 | ||
| Mixed | Level II | (n=65) | (n=115) | ||||||||
| No | 91 (62.8) | 118 (56.7) | 1.00 |
0.2569 |
No | 39 (60.0) | 71 (61.7) | 1.00 |
0.8182 |
||
| Yes | 54 (37.2) | 90 (43.3) | 1.28 | 0.81-2.03 | Yes | 26 (40.0) | 44 (38.3) | 0.92 | 0.47-1.82 | ||
| Afro-descendant | Level III | (n=65) | (n=115) | ||||||||
| No | 138 (95.2) | 208 (100.0) | n/a | No | 54 (83.1) | 97 (84.4) | 1.00 |
0.8237 |
|||
| Yes | 7 (4.8) | 0 (0.0) | Yes | 11 (16.9) | 18 (15.6) | 0.91 | 0.37-2.30 | ||||
| Indigenous | Nutritional status | ||||||||||
| No | 142 (97.9) | 207 (99.5) | 1.00 |
0.1655 |
According to Body Mass Index | ||||||
| Yes | 3 (2.1) | 1 (0.5) | 0.22 | 0.004-2.89 | Normal |
(n=132) 53 (40.2) |
(n=186) 78 (41.9) |
1.00 |
0.7501 |
||
| School (n=328) | (n=134) | (n=194) | Malnutrition | 79 (59.8) | 108 (58.1) | 0.92 | 0.57-1.49 | ||||
| Public | 23 (17.2) | 25 (12.9) | 1.00 |
0.2813 |
According to Height for age | ||||||
| Private | 111 (82.8) | 169 (87.1) | 1.40 | 0.71-2.71 | Normal |
(n=134) 18 (13.4) |
(n=186) 28 (15.1) |
1.00 |
0.6835 |
||
| Origin | Altered H/A | 116 (86.6) | 158 (84.9) | 0.87 | 0.43-1.73 | ||||||
| South America | Comorbidity | ||||||||||
| No | 70 (48.3) | 135 (64.9) | 1.00 |
0.0018 |
No | 112 (77.2) | 156 (75.0) | 1.00 |
0.6280 |
||
| Yes | 75 (51.7) | 73 (35.1) | 0.50 | 0.31-0.79 | Yes | 33 (22.8) | 52 (25.0) | 1.13 | 0.66-1.93 | ||
| Argentina | Family variables | ||||||||||
| No | 110 (75.9) | 161 (77.4) | 1.00 |
0.7358 |
Only child | ||||||
| Yes | 35 (24.1) | 47 (22.6) | 0.91 | 0.54-1.56 | No | 97 (66.9) | 141 (67.8) | 1.00 |
0.8604 |
||
| Colombia | Yes | 48 (33.1) | 67 (32.2) | 0.96 | 0.59-1.55 | ||||||
| No | 105 (72.4) | 182 (87.5) | 1.00 |
0.0003 |
Firstborn | ||||||
| Yes | 40 (27.6) | 26 (12.5) | 0.37 | 0.20-0.67 | No | 67 (46.2) | 93 (44.7) | 1.00 |
0.7813 |
||
| Central America | Yes | 78 (53.8) | 115 (55.3) | 1.06 | 0.67-1.66 | ||||||
| No | 75 (51.7) | 73 (35.1) | 1.00 |
0.0018 |
Separated/divorced parents | ||||||
| Yes | 70 (48.3) | 135 (64.9) | 1.98 | 1.25-3.12 | No | 110 (75.9) | 151 (72.6) | 1.00 |
0.4916 |
||
| Panama | Yes | 35 (24.1) | 57 (27.4) | 1.18 | 0.70-1.99 | ||||||
| No | 126 (86.9) | 171 (82.2) | 1.00 |
0.2359 |
DGBIs intra-familiar | ||||||
| Yes | 19 (13.1) | 37 (17.8) | 1.43 | 0.76-2.77 | No | 142 (97.9) | 197 (94.7) | 1.00 |
0.1273 |
||
| El Salvador | Yes | 3 (2.1) | 11 (5.3) | 2.64 | 0.67-14.98 | ||||||
| No | 123 (84.3) | 183 (88.0) | 1.00 |
0.3909 |
Familial autism | ||||||
| Yes | 22 (15.2) | 25 (12.0) | 0.76 | 0.39-1.49 | No | 138 (95.2) | 197 (94.7) | 1.00 |
0.8464 |
||
| Costa Rica | Yes | 7 (4.8) | 11 (5.3) | 1.10 | 0.37-3.43 | ||||||
| No | 130 (89.7) | 171 (82.2) | 1.00 |
0.0522 |
|||||||
| Yes | 15 (10.3) | 37 (17.8) | 1.87 | 0.95-3.83 | |||||||
| Mexico | |||||||||||
| No | 131 (90.3) | 172 (82.7) | 1.00 |
0.0425 |
|||||||
| Yes | 14 (9.7) | 36 (17.3) | 1.95 | 0.98-4.09 | |||||||
* DGBIs=Disorders Gut-Brain Interaction; H/A=Heigh for age.
Table 5.
Validation and internal consistency of the QPGS IV in Spanish designed for parents and caregivers of schoolchildren and adolescents with ASD.
Table 5.
Validation and internal consistency of the QPGS IV in Spanish designed for parents and caregivers of schoolchildren and adolescents with ASD.
| Alpha de Cronbach | Interpretation | |
| Total questionnaire | 0.7818 | High |
| Section A | 0.7331 | High |
| Section B | 0.4706 | Moderate |
| Section C | 0.6535 | High |
| Section D | 0.6110 | High |
| Section E | 0.6367 | High |
* QPGS IV=Questionnaire for Pediatric Gastrointestinal Symptoms Rome IV.
Table 6.
Main digestive symptoms identified using QPGS IV.
| Symptom | n (%) |
| Flatus | 178 (50.4) |
| Painful Stool | 126 (35.7) |
| Large stools | 108 (30.6) |
| History of large fecal mass in rectum | 94 (26.6) |
| Hard stools | 84 (23.8) |
| Belching | 84 (23.8) |
| Stool Retention | 78 (22.1) |
| Soiling | 73 (20.7) |
| Abdominal pain around and below belly button | 68 (19.3) |
| Early satiation | 66 (18.7) |
| Abdominal pain above belly button | 53 (15.0) |
| Abdominal distention | 48 (13.6) |
| Watery stools | 28 (7.9) |
| Swallowing air | 26 (7.4) |
| Nausea | 25 (7.1) |
| Heartburn | 16 (4.5) |
* QPGS IV=Questionnaire for Pediatric Gastrointestinal Symptoms Rome IV.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



